
Abstract
Background:
Robot-assisted endoscopic submucosal dissection (RA-ESD) has been developed to address the ergonomic and technical limitations of conventional ESD (C-ESD). However, the current evidence base remains limited and is predominantly derived from preclinical studies.
Objectives:
To systematically evaluate the comparative efficacy and safety of RA-ESD versus C-ESD.
Design:
Systematic review and meta-analysis.
Data sources and methods:
A comprehensive literature search was conducted in major electronic databases in accordance with the PRISMA 2020 Statement. Comparative studies assessing RA-ESD versus C-ESD were included. Continuous outcomes were pooled using mean differences (MDs), and dichotomous outcomes were analyzed using odds ratios (ORs), both with 95% confidence intervals (CIs). Random-effects models were applied for all primary analyses.
Results:
Twelve studies (n = 581) were included, of which the majority were preclinical. In exploratory pooled analyses, RA-ESD was associated with shorter submucosal dissection time (min) (MD −6.62, 95% CI −9.38 to −3.86) and overall procedure time (min) (MD −6.00, 95% CI −9.13 to −2.86). Dissection speed (mm2/min) was higher with RA-ESD (MD 35.80, 95% CI 8.98 to 62.62), although heterogeneity was substantial. The blind dissection rate (%) was lower in the RA-ESD group (MD −22.64, 95% CI −31.49 to −13.78). RA-ESD was associated with a higher en bloc resection rate (OR 6.44, 95% CI 1.05 to 39.39) and a lower risk of muscular injury (OR 0.18, 95% CI 0.06 to 0.53). No significant difference in perforation was observed.
Conclusion:
RA-ESD demonstrates promising technical advantages over C-ESD, including improved procedural efficiency and reduced technical difficulty, without an apparent increase in major adverse events. However, given that the current evidence is predominantly preclinical and characterized by substantial heterogeneity, these findings should be interpreted as preliminary and hypothesis-generating. Further well-designed clinical studies are required to confirm the real-world effectiveness, safety, and long-term outcomes of RA-ESD.
Trial registration:
PROSPERO registration number: CRD420261336534.
Plain language summary
This study looked at whether robot-assisted endoscopic submucosal dissection (RA-ESD) works better than the standard technique (C-ESD). ESD is a minimally invasive procedure used to remove abnormal or early cancerous tissue from the digestive tract without open surgery. However, standard ESD can be technically difficult and physically demanding for the operator. We reviewed 12 studies involving 581 procedures and combined their results. Overall, robot-assisted ESD was linked to better technical performance. It shortened the time needed to remove tissue, increased the speed of dissection, reduced the amount of “blind” cutting, and improved the chance of removing the lesion in one piece. It was also associated with fewer injuries to the muscle layer. The risk of perforation was similar between the two approaches. These findings suggest that robot-assisted ESD may help doctors perform this difficult procedure more efficiently and with greater control, without reducing safety. This could potentially improve treatment quality for patients. However, the current evidence is still limited. Many of the included studies were performed in preclinical settings, such as animal or laboratory models, or were early-stage clinical studies. This means the results should be interpreted with caution. Larger, well-designed clinical trials in real patients are still needed to confirm whether robot-assisted ESD provides clear long-term benefits in routine medical practice.
Keywords
Introduction
Endoscopic submucosal dissection (ESD) has emerged as a crucial minimally invasive therapy for early gastrointestinal (GI) neoplasms. First developed in Japan in the late 1980s, ESD enables en bloc removal of premalignant and early malignant lesions throughout the GI tract. 1 Over the past two decades, it has become a standard treatment for early GI cancers, offering an organ-sparing cure with excellent long-term outcomes. 2
Despite its efficacy, traditional ESD is technically challenging. The procedure demands advanced endoscopic skill, a steady hand, and extensive training; it is associated with a steep learning curve and often prolonged procedure times, even for experienced endoscopists. 3 Maintaining a stable visual field is difficult when the endoscope must constantly reorient, and transmitting force to the resection plane via a flexible scope is suboptimal. 4 These technical hurdles contribute to higher risks of complications (such as perforation) and hinder the wider adoption of ESD in some regions. 5
Existing traction-assisted ESD techniques can improve submucosal exposure. However, many simple traction methods provide limited and often non-adjustable traction direction, may require repeated repositioning, and can interfere with endoscope maneuverability. 6 These limitations hinder procedural standardization and sustained visualization. Therefore, robot-assisted ESD (RA-ESD) has been introduced as an innovative solution to enhance endoscopic resection. 7 Several robotic or electromechanical platforms have been developed to augment the capabilities of the endoscopist during ESD. 8 These systems integrate advanced control mechanisms and additional instrument arms to provide greater precision, stability, and traction than a human operating a standard endoscope alone. 9 In general, robotic assistance aims to overcome the ergonomic and technical limitations of manual ESD by enabling finer movements, continuous tissue counter-traction, and a stable operative field. These enhanced dexterity and control are expected to translate into more precise dissections, better access to difficult lesion angles, and potentially greater efficiency during the procedure. 7
However, it is important to note that current evidence on RA-ESD remains preliminary. This technology remains at an early stage of clinical application, and most published data come from limited single-center experiences, small case series, or pilot trials often involving animal or ex vivo models. 8
Given the potential role of RA-ESD to address key limitations of conventional ESD, a systematic evaluation of its performance is warranted. Therefore, we conducted this systematic review and meta-analysis of all available comparative studies (covering various GI sites, robot types, and study designs) that directly evaluate RA-ESD versus traditional ESD, aiming to inform endoscopists and stakeholders about the current state of RA-ESD and guide future research and development in advanced endoscopic resection.
Methods
We conducted this meta-analysis based on the methodological recommendations of the Cochrane Handbook and reported following the PRISMA 2020 statement 10 . The review was prospectively registered in PROSPERO registration number (CRD420261336534).
Eligibility criteria for study selection
Inclusion criteria: (1) studies evaluating robot-assisted ESD; (2) prospective, retrospective, randomized, or non-randomized comparative studies evaluating RA-ESD versus C-ESD; (3) reporting outcomes of interest.
Exclusion criteria: (1) Review articles, editorials, conference abstracts, comments, and letters without original data; (2) Studies without extractable outcome data relevant to the predefined outcomes; (3) Non-comparative reports or technical descriptions that did not provide analyzable outcome data.
Search strategy
We searched electronic databases (PubMed, Embase, Cochrane, Web of Science) without applying a filter for publication date on December 24, 2025. We used relevant terms, including “Robotic-assisted,” “endoscopic submucosal dissection,” and other relevant outcome terms in both free-text form and medical subject headings. The details of our search strategy are given in the Supplemental Material.
Two authors (M.W. and Y.Z.) independently screened all records identified from the electronic databases using Rayyan, a web-based systematic review management tool. The study selection process was conducted in three sequential stages: (a) removal of duplicate records, (b) screening of titles and abstracts, and (c) full-text eligibility assessment. Initially, duplicates were automatically identified and removed within Rayyan, followed by an additional manual check during the title and abstract screening phase. Studies deemed potentially eligible were subsequently retrieved in full and assessed against the predefined inclusion and exclusion criteria. Any disagreements between the two reviewers were resolved through discussion until a consensus was reached.
Outcome definitions
The primary procedural outcomes included dissection time, dissection speed, procedure time, and blind dissection rate, while perforation, muscular injury, and en bloc resection rate were analyzed as safety and quality outcomes. Dissection time was defined as the duration from the initiation of submucosal dissection to the completion of lesion resection. Dissection speed was calculated as the area of the resected specimen divided by the submucosal dissection time and expressed as mm2/min. Procedure time was defined as the time from the start of the endoscopic procedure (mucosal marking or submucosal injection) to the completion of lesion removal. Blind dissection was defined as submucosal dissection performed without clear visualization of the dissection plane or the tip of the endoscopic knife, and the blind dissection rate was calculated as the ratio of blind dissection time to total dissection time. Perforation was defined as a full-thickness defect or direct endoscopic visualization of extraluminal structures during the procedure. Muscular injury refers to damage to the muscularis propria without full-thickness perforation. En bloc resection was defined as the complete removal of the lesion in a single piece without fragmentation.
Data extraction
Two authors (M.W. and Y.Z.) independently extracted data using a standardized data collection form. Information on study characteristics, type (human, animal, or ex vivo), sample size, and technical features of the robotic system was collected. Outcomes of interest included procedure time, dissection time, dissection speed, blind dissection rate, en bloc resection rate, and procedure-related complications, including perforation and muscular injury. Disagreements were resolved by consensus.
For quantitative synthesis, outcome data were harmonized prior to meta-analysis. When continuous variables were reported using different measurement units, values were converted to a unified scale to ensure comparability. For studies reporting continuous outcomes as medians with interquartile ranges, means and standard deviations were estimated using established statistical methods, assuming approximate symmetry of the data distribution. When outcomes were reported separately according to anatomical location (e.g., gastric vs colorectal lesions), data were combined to generate overall estimates when clinically and methodologically appropriate. In such cases, pooled means and standard deviations were calculated using standard weighted formulas based on subgroup sample sizes, thereby preserving the original variance structure. This approach was applied only when outcome definitions and measurement methods were consistent across anatomical subgroups.
Sensitivity analyses
Leave-one-out sensitivity analyses were conducted to evaluate the stability of the pooled results. Each study was sequentially excluded, and the meta-analysis was repeated using the remaining studies. The resulting pooled effect estimates and 95% confidence intervals (CIs) were compared with those of the primary analyses to determine whether any single study had a disproportionate influence on the overall findings.
Risk of bias assessment
For randomized controlled trials (RCTs), risk of bias was assessed using the Cochrane Risk of Bias tool (RoB 2). 11 Risk of bias in animal studies was assessed using the SYRCLE Risk of Bias tool, which is an adaptation of the Cochrane risk-of-bias framework tailored to preclinical animal intervention studies. 12 For ex vivo mechanistic studies, the OHAT (Office of Health Assessment and Translation) risk-of-bias tool was applied, which provides a comprehensive bias assessment across multiple study designs, including animal and laboratory studies. Disagreements were resolved by consensus.
Statistical analysis
Statistical analyses were performed using Review Manager (RevMan, version 5.4) and R software (version 4.4.2). Continuous outcomes were synthesized using mean differences (MDs) with corresponding 95% CIs. The primary outcome, dissection time, was pooled using the inverse variance method under a random-effects model. Dichotomous outcomes were pooled as odds ratios (ORs) with 95% CIs using a random-effects model. Random-effects models were applied to account for anticipated clinical and methodological heterogeneity. Statistical heterogeneity was assessed using the I2 statistic. A two-sided p-value <0.05 was considered statistically significant.
Result
A total of 306 records were identified through database searching. After removal of duplicates, 223 records remained for title and abstract screening, of which 201 were excluded. The full texts of 22 articles were assessed for eligibility, and 10 were further excluded because of systematic reviews (n = 1), unavailable full text (n = 4), or insufficient detail in gray literature (n = 5). Ultimately, 12 studies were included in the quantitative synthesis (Figure 1).

Flowchart of the study.
Characteristics and quality of included studies
Table 1 summarizes the characteristics of the included studies. A total of 12 studies published between 2019 and 2025 were included, comprising two clinical trials in humans (Fan, 2025; Zhang, 2025) and 10 preclinical studies (including ex vivo organ models, live porcine animal models, and one model-based study). Overall, the studies were conducted in China (n = 5), Korea (n = 5), and the USA (n = 2). The total sample size across all studies was 581, with 240 human participants and 341 preclinical models. Sample sizes ranged from 20 to 192.
Characteristics of the included studies.
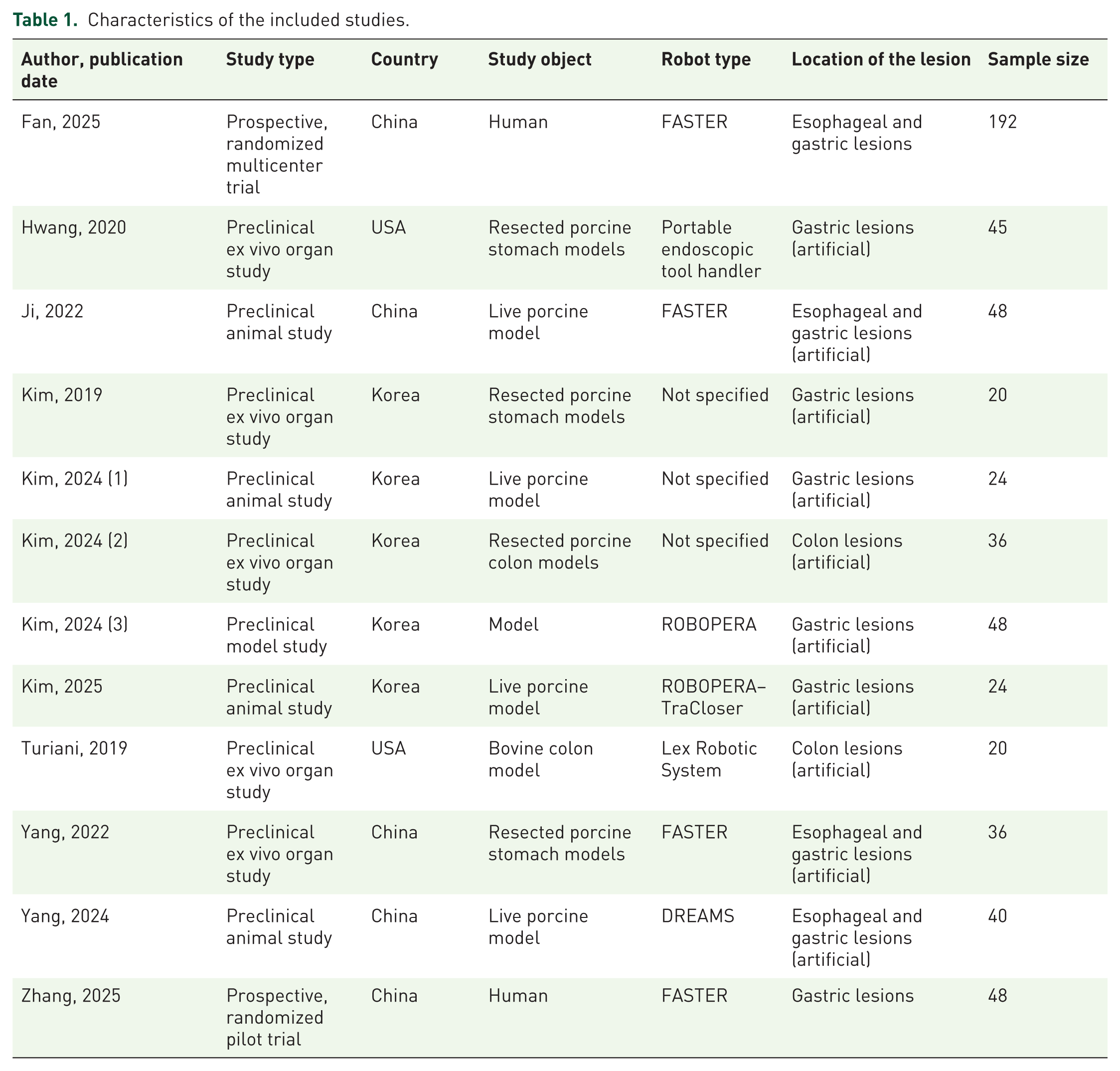
Regarding lesion location, most investigations focused on the upper gastrointestinal tract, including esophageal and gastric lesions (n = 4 studies) and gastric lesions alone (n = 6 studies), whereas colon lesions were evaluated in 2 studies. Several robotic or electromechanical platforms were assessed, most commonly FASTER (n = 4), followed by DREAMS (n = 1), ROBOPERA (n = 1), ROBOPERA–TraCloser (n = 1), Lex Robotic System (n = 1), and a portable endoscopic tool handler (n = 1); in 3 studies, the robot type was not specified.
Study outcome
Dissection time data were available from 12 studies. Overall, RA-ESD significantly reduced dissection time (min) compared with C-ESD (MD −6.62, 95% CI −9.38 to −3.86; I2 = 89%; p < 0.00001) (Figure 2). In addition, dissection speed (mm2/min) was reported in 8 studies. The pooled analysis showed a significant difference between groups (MD 35.80, 95% CI 8.98 to 62.62; I2 = 97%; p = 0.009). Similarly, procedure time (min) was available in 12 studies. RA-ESD was associated with a shorter procedure time than C-ESD (MD −6.00, 95% CI −9.13 to −2.86; I2 = 89%; p = 0.0002). For technical performance, blind dissection rate (%) was reported in 7 studies. The pooled estimate indicated that RA-ESD significantly reduced the blind dissection rate (MD −22.64, 95% CI −31.49 to −13.78; I2 = 97%; p < 0.00001). Finally, en bloc resection (%) was assessed in 8 studies. The pooled result suggested a higher en bloc resection rate with RA-ESD (OR 6.44, 95% CI 1.05 to 39.39; I2 = 0%; p = 0.04) (Figure 3).

Forest plot comparing submucosal dissection time between RA-ESD and C-ESD.

Forest plots comparing secondary outcomes between RA-ESD and C-ESD: (a) procedure time, (b) dissection speed, (c) blind dissection rate, and (d) en bloc resection rate.
Safety
Regarding safety outcomes, perforation (%) was reported in 8 studies. The pooled analysis found no significant difference between groups OR 0.35, 95% CI 0.09 to 1.31; I2 = 0; p = 0.12). In contrast, muscular injury (%) was reported in 6 studies. RA-ESD was associated with a significantly lower risk of muscular injury (OR 0.18, 95% CI 0.06 to 0.53; I2 = 41%; p = 0.002) (Figure 4).

Forest plots comparing safety outcomes between RA-ESD and C-ESD: (a) perforation, (b) muscular injury.
Subgroup analysis
In human studies, no significant differences were observed between RA-ESD and C-ESD in submucosal dissection time (MD 2.30, 95% CI −4.53 to 9.12; p = 0.51) or overall procedure time (MD 10.04, 95% CI −5.42 to 25.49; p = 0.20). However, RA-ESD was associated with significantly higher dissection speed (MD 51.47, 95% CI 20.53 to 82.41; p = 0.001). The blind dissection rate was numerically lower in the RA-ESD group, but the difference was not statistically significant (MD −18.22, 95% CI −49.42 to 12.98; p = 0.25) (Figure S5).
In animal and ex vivo model studies, RA-ESD significantly reduced submucosal dissection time (MD −7.53, 95% CI −10.43 to −4.63; p < 0.00001) and overall procedure time (MD −7.13, 95% CI −10.30 to −3.95; p < 0.0001) compared with C-ESD. RA-ESD was also associated with a significantly higher dissection speed (MD 51.47, 95% CI 20.53 to 82.41; p = 0.001) and a lower blind dissection rate (MD −24.42, 95% CI −34.23 to −14.61; p < 0.00001). In addition, RA-ESD achieved a higher en bloc resection rate (OR 8.91, 95% CI 1.01 to 78.95; p = 0.05) and a lower muscular injury rate (OR 0.18, 95% CI 0.04 to 0.80; p = 0.02), whereas no significant difference was observed in perforation (OR 0.35, 95% CI 0.09 to 1.30; p = 0.12) (Figures S5–S7).
Sensitivity analyses
Overall, leave-one-out sensitivity analyses showed that omission of any single study did not materially alter the direction or approximate magnitude of the pooled effect estimates for most outcomes, indicating that the main findings of this meta-analysis were generally stable and robust. For continuous outcomes, the direction of effect remained consistent with the original pooled results after sequential exclusion of individual studies, with no reversal in effect direction observed after removal of any single study, suggesting that these findings were not driven by any one study alone.
For binary outcomes, some results also demonstrated good robustness. For example, the pooled effects for en bloc resection rate (OR 6.436, 95% CI 1.052 to 39.386) and muscular injury (OR 0.185, 95% CI 0.064 to 0.533) remained directionally consistent in the leave-one-out analyses, supporting the reliability of these findings. In contrast, for perforation (OR 0.351, 95% CI 0.095 to 1.305), the confidence interval crossed the null value of 1, indicating that although a potential trend was observed, the statistical evidence for this outcome remained insufficient and should therefore be interpreted with caution.
Risk of bias
For the ex vivo model studies, most studies showed a high risk of bias, mainly due to the lack of blinding during experimental procedures. Several domains were rated as unclear because of insufficient methodological details. For the preclinical animal studies, the overall risk of bias was considered high. Baseline characteristics and outcome assessment were generally well reported, whereas blinding and allocation procedures were often unclear. For the RCTs, the overall methodological quality was good. Most domains were assessed as low risk of bias, although one study showed a high risk in allocation concealment (Figures S1–S3).
Discussion
This systematic review and meta-analysis suggest that robot-assisted ESD may offer potential advantages in procedural efficiency and technical performance compared with conventional ESD. In the exploratory pooled analyses, RA-ESD was associated with shorter submucosal dissection time and overall procedure time, a lower rate of blind dissection, a higher en bloc resection rate, and fewer muscular layer injuries, without a significant increase in perforation. However, these findings should be interpreted cautiously because the current evidence base is predominantly preclinical, with only two human clinical studies and substantial methodological heterogeneity across included studies.
Our primary finding is that RA-ESD significantly reduced dissection time. This result suggests that robotic assistance improves efficiency during the most technically demanding phase of ESD rather than merely shortening peripheral procedural steps. A plausible explanation is that stable, controllable traction improves submucosal exposure and instrument targeting, allowing more continuous and precise dissection. 13 Importantly, this efficiency may reflect improved tissue exposure and instrument control provided by robotic assistance, indicating that RA-ESD not only accelerates performance but also reduces cognitive and manual burden. At the same time, we did not observe a corresponding increase in adverse events, suggesting that faster dissection with robotic assistance did not come at the cost of procedural safety. Taken together, these findings support a favorable balance between efficiency, ergonomics, and safety for RA-ESD. 14
A second key finding is the reduction in blind dissection rate with RA-ESD. Blind dissection is widely considered a major source of technical difficulty in ESD because loss of a clear submucosal view increases uncertainty in tissue-plane control and may predispose to unintended deep injury. By functioning as a stable “second hand,” robotic traction systems help maintain continuous visualization of the dissection plane and reduce view-dependent interruptions. 15 This mechanism is likely central to the observed reduction in perceived procedural difficulty and operator strain. 16 From a training perspective, lowering the frequency of blind dissection may reduce the technical barriers faced by less-experienced endoscopists, thereby decreasing learning costs and potentially shortening the pathway to procedural proficiency. 17 If validated in larger pragmatic studies, this advantage could facilitate broader and safer adoption of ESD, particularly in settings where uptake has been limited by steep technical learning curves. 18
Our results should be interpreted considering the current developmental stage of endoscopic robotics. The field of RA-ESD is still in its infancy, and most robotic platforms are prototypes evaluated in limited clinical trials or preclinical studies. 19 This reality was reflected in our included studies: out of 12 studies, 10 were preclinical (ex vivo models, animal experiments, or simulation-based), and only 2 were trials in human patients. While pooling data from preclinical research provides valuable insight into the theoretical benefits of RA-ESD, it may not fully capture real-world complexity.
Several limitations of this meta-analysis must be acknowledged. First, the included studies were clinically and methodologically heterogeneous, comprising human clinical studies, live animal experiments, and ex vivo models. Although these designs are all relevant to the development of RA-ESD, they differ substantially in biological context, procedural complexity, outcome meaning, and clinical applicability. Therefore, the overall pooled estimates should not be interpreted as direct evidence that RA-ESD improves clinical outcomes in routine patient care. Second, the evidence base was dominated by preclinical studies, whereas only two small human studies were available. This substantially limits external validity and prevents firm conclusions regarding clinically important outcomes such as R0 resection, delayed bleeding, perforation, recurrence, recovery, and cost-effectiveness. Third, substantial statistical heterogeneity was observed for several key outcomes, likely reflecting differences in study design, lesion location, robotic platform, operator experience, and experimental setting. To further explore the robustness of the findings, we conducted leave-one-out sensitivity analyses, which showed that the direction and magnitude of the pooled effects remained largely unchanged after sequential exclusion of individual studies. In addition, subgroup analyses according to study type (human, animal, ex vivo) were performed. Although subgroup analyses were limited by the small number of human studies, they suggested that treatment effects varied across experimental settings. In particular, the human subgroup showed a significant improvement in dissection speed but did not demonstrate significant reductions in dissection time, procedure time, or blind dissection rate. This lack of statistical significance may be partly attributable to the limited number of human studies and the relatively small sample size, which reduced statistical power and widened the confidence intervals. Therefore, the overall pooled findings should be interpreted primarily as exploratory evidence rather than definitive clinical evidence.
Looking ahead, larger high-quality studies are required to validate the potential advantages of RA-ESD. Future RCTs in clinical settings should better define their impact on procedural efficiency, safety, and long-term outcomes, including R0 resection, recurrence, and recovery. Evidence in technically challenging lesions (e.g., duodenal or fibrotic lesions) will be particularly informative, as these scenarios represent key limitations of conventional ESD. Beyond technical feasibility, future studies should also evaluate cost-effectiveness and the learning curve. Although robotic systems may improve procedural stability and reduce technical difficulty, their acquisition and maintenance costs, resource utilization, and training requirements remain important barriers to widespread implementation. Prospective studies incorporating economic evaluation and operator learning-curve analysis are therefore needed to determine whether the technical advantages of RA-ESD translate into sustainable clinical value.
Conclusion
In conclusion, robot-assisted ESD showed promising technical advantages over conventional ESD in the currently available evidence, including shorter procedure-related times, reduced blind dissection, lower operator burden, higher en bloc resection rates, and fewer muscular injuries. However, these findings are mainly derived from preclinical studies and are accompanied by substantial heterogeneity and limited human clinical data. Therefore, the results should be interpreted as preliminary and hypothesis-generating rather than definitive evidence of clinical superiority. Further well-designed, adequately powered clinical trials are needed to confirm whether the technical advantages of RA-ESD translate into meaningful improvements in patient-centered outcomes, safety, long-term efficacy, learning curve, and cost-effectiveness.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261458700 – Supplemental material for Robot-assisted versus conventional endoscopic submucosal dissection: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848261458700 for Robot-assisted versus conventional endoscopic submucosal dissection: a systematic review and meta-analysis by Menghan Wang, Yan Zhao, Yijun Chen and Wenhai Wang in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.