
Abstract
Background:
Autoimmune (AI) comorbidities are common in people with multiple sclerosis (MS) and may complicate therapeutic management, particularly when dual immunosuppression is required. Cladribine, an immune reconstitution therapy approved for relapsing MS, has shown potential benefit in selected autoimmune disorders.
Objectives:
To evaluate the prevalence of AI comorbidities in a large French MS cohort and explore the potential efficacy of cladribine in MS patients with concomitant autoimmune diseases.
Design:
Retrospective multicenter registry analysis combined with a descriptive case series and literature review.
Data sources and methods:
Data were retrospectively extracted from the European Database for MS across five French tertiary MS centers. Adults with MS and documented autoimmune comorbidities were identified, including a subgroup treated with oral cladribine. In addition, eight detailed clinical cases of MS associated with autoimmune diseases treated with cladribine were reviewed to assess outcomes on both MS and the associated autoimmune condition.
Results:
Among 11,410 people with MS, 901 had at least one autoimmune comorbidity, corresponding to a prevalence of 7.9 ± 0.25% (age 50.8 years), with a predominance of women. Of 385 cladribine-treated patients, 39 (10.1% ± 1.54%) had concurrent autoimmune disorders, although this proportion did not significantly differ from the overall cohort (p = 0.11). Eight cases involving ankylosing spondylitis (n = 3), psoriatic arthritis (n = 2), psoriasis (n = 1), rheumatoid arthritis (n = 1), and sarcoidosis (n = 1) were analyzed. Cladribine was consistently associated with MS stability, while efficacy on associated autoimmune conditions was variable, with more favorable outcomes observed in ankylosing spondylitis, psoriasis, and sarcoidosis.
Conclusion:
Autoimmune comorbidities affect approximately 8% of the French MS population and are more frequent in women. Cladribine may represent a useful therapeutic option in selected patients with concomitant autoimmune disorders, potentially limiting prolonged dual immunosuppression. Larger prospective studies are required to confirm efficacy and safety.
Trial registration:
OFSEP/EDMUS registry, ClinicalTrials.gov: NCT02889965.
Plain language summary
A French study involving more than 11,000 people with multiple sclerosis (MS) found that around 8% also had another autoimmune disease, with women more commonly affected. Because treating both conditions can require multiple long-term immune-suppressing therapies, researchers explored whether cladribine, an approved MS treatment, could help control both diseases simultaneously. Among patients receiving cladribine, about 10% had an additional autoimmune disorder. Researchers closely reviewed eight patients with MS plus conditions including ankylosing spondylitis, psoriatic arthritis, psoriasis, rheumatoid arthritis, or sarcoidosis. The study found that MS remained stable in patients treated with cladribine. Some associated autoimmune conditions, especially ankylosing spondylitis, psoriasis, and sarcoidosis, also appeared to improve, although results were mixed for other diseases. Overall, the findings suggest that cladribine could be a useful treatment option for certain patients with both MS and autoimmune comorbidities, potentially reducing the need for multiple therapies. However, current evidence remains limited, and larger clinical studies are needed to confirm its safety and effectiveness for these additional autoimmune conditions.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease driven by an immune attack against the myelin of the central nervous system (CNS). As frequently observed for immune-mediated disorders, people with MS (PwMS) have an increased risk of developing other autoimmune (AI) conditions compared to the general population,1,2 suggesting shared pathophysiological mechanisms and genetic susceptibility between these different entities. 3
Epidemiological studies over the years have provided information on the prevalence of a double diagnosis of MS plus other AI disorders, showing that the frequency of comorbid autoimmune diseases is higher in PwMS than in healthy individuals.4,5 Several works have estimated this number across the MS population, with an observed prevalence after MS diagnosis spanning from 3% to 26.1% in a meta-analysis of multiple studies. 6 In more detail, according to cohorts and sample sizes, the calculated proportions vary from 4.5% 7 to 11.2% 8 and up to 17.2%. 5 Women with MS are more affected by concurrent AI disorders than men, because of biological factors, including genetic and hormonal susceptibility.4,5 Most common AI comorbidities are rheumatoid arthritis (RA), psoriasis, and inflammatory bowel diseases.9–11 Narrowing the focus to rheumatologic AI diseases, a significantly higher rate of MS diagnosis compared to matched controls is found in subjects with ankylosing spondylitis (AS, 0.5% vs 0.3%, p = 0.008). 12 Similar data confirming a greater incidence of MS are reported for psoriatic arthritis (PsA, hazard ratio 2.86, 95% CI 1.81–4.50). 13 Regarding the association between MS and RA, heterogeneous prevalence findings have been reported in epidemiological studies.3,14–16
Noteworthy, the presence of additional AI disorders can significantly impact MS outcomes—acting via multiple processes—and influence treatment decisions. RA, for instance, through a dysregulated immune system and the worsening of motor functions/walking abilities, has been shown to increase the risk of MS disability progression. 17 In an Italian study of 873 people with relapsing-remitting MS (RMS), of whom 215 (24.7%) had at least one comorbidity, individuals with AI ones, compared to the reference group, exhibited older age at MS onset and MS diagnosis and higher Expanded Disability Status Scale (EDSS) score at diagnosis and after 36 months. 18 A recent large-scale meta-analysis of data from 16.794 patients across 17 phase III clinical trials found that a higher burden of concurrent disorders, including AI conditions, was associated with greater disease activity in PwMS, highlighting the importance of addressing these comorbidities in clinical practice. 19
Looking at treatment choices, in the aforementioned Italian cohort, 18 people with AI comorbidities were more frequently treated with glatiramer acetate, natalizumab, and rituximab. Nonetheless, a non-negligible point is that some Disease modifying therapies (DMTs) used to treat MS may exacerbate, or even trigger, other AI conditions. 20
In recent years, the management of MS has seen a significant shift toward early use of high-efficacy therapies (HETs). This change was mainly driven by findings demonstrating that early initiation of HETs is associated with lower long-term disability, compared to the later switch seen with classical escalation approaches. 21 However, gathering evidence on HET efficacy in PwMS with concomitant AI disorders remains challenging due to case complexity. For these reasons, in such a context, clinical and therapeutic decision-making mainly relies on retrospective data and case series. A few years ago, a report discussed the off-label use of subcutaneous cladribine, an immune reconstitution therapy (IRT), for PwMS who were ineligible for licensed DMTs, including those with comorbidities such as AI ones. 22 Indeed, IRT approaches like cladribine, by resetting the immune system toward a more tolerogenic environment, may offer a valuable treatment option when MS and other AI disorders coexist, particularly in resource-limited settings where access to expensive biologics is restricted.
In the present work, we aimed at assessing the prevalence of AI comorbidities in a large French cohort of PwMS. We then focused on cladribine use through some clinical examples of its prescription in MS with concomitant AI diseases, additionally providing, for each MS-associated condition, an up-to-date literature review of data on cladribine’s potential therapeutic effect. A viewpoint on the added value of cladribine as a treatment option to avoid continuous double immunosuppression and minimize safety concerns in these scenarios is discussed in the manuscript.
Methods
To assess the frequency of AI comorbidities in a French cohort of PwMS, we performed a retrospective study of the local European Database for MS (EDMUS) registry (https://www.plateforme-edmus.org), developed by the Observatoire Français de la Sclérose en Plaques (OFSEP). The EDMUS is a powerful software tool that facilitates the medical monitoring of PwMS and supports research initiatives. It is populated both retrospectively and prospectively by clinical research associates and physicians, ensuring the collection of standardized information that can be easily extracted for statistical analyses. Data were extracted from five French tertiary MS centers: Strasbourg University Hospital, Fondation Adolphe de Rothschild Hospital, Paris-Saclay Hospital, Amiens University Hospital, and Gonesse Hospital, during the period from December 24, 2025, to February 3, 2026. To analyze registry data, inclusion criteria were (i) Diagnosis of MS according to actual criteria at the time of patients’ entry in the registry (McDonald’s 2010, 2017, or 2024 revised criteria) and, for AI/cladribine subgroups, (ii) Concomitant, well-defined diagnosis of one or more associated AI condition, (iii) Having received a complete two-year cycle with cladribine. Exclusion criteria included the absence of a precise diagnosis for the associated AI disorder. We quantified the number of PwMS with AI comorbidities and the proportion treated with oral cladribine.
Regarding the case series, clinical follow-up was assured until November 2025, while radiological follow-up was reported until the most recent MRI available in the records. When discussing disease reactivation, “MS activity” was defined as either clinical (relapse) or radiological (new MRI lesion) or both, while recurrence of the associated AI condition (“AI activity”) was defined as uncontrolled immune reactivation, for example, inflammation affecting previously healthy joints or immune-mediated attacks necessitating treatment intensification/switch.
The systematic literature review on selected AI comorbidities presented here was conducted through PubMed search, using the following search terms: “multiple sclerosis (or MS) and psoriasis,” “multiple sclerosis (or MS) and psoriatic arthritis,” “multiple sclerosis (or MS) and ankylosing spondylitis’, “multiple sclerosis (or MS) and rheumatoid arthritis”, “multiple sclerosis (or MS) and sarcoidosis”. The extracted list of articles was carefully reviewed for validation. Epidemiological findings from the EDMUS database, individual cases, and literature data were then discussed during a multidisciplinary expert meeting held in Paris, France.
Statistical analysis
Prevalence precision–calculated from the analysis of the EDMUS registry–was expressed as standard error (SE), as usually done for epidemiological studies. A two-proportion z-test was used to compare the difference in the prevalence of AI comorbidities between the general MS cohort and the cladribine-treated group. Significance was set at p < 0.05.
Results
Prevalence of concurrent autoimmunity and cladribine treatment in people with MS in France
In a cohort of 11.410 individuals with MS across five MS centers, 901 exhibited a concomitant AI disease, yielding a prevalence of 7.9% (SE = 0.25%). As expected, sex distribution in this subgroup was more skewed toward females (76.9%); mean age was 50.8 ± 13.4 years, with a median EDSS of 2.5 (range 0–6.5).
Three hundred eighty-five PwMS received cladribine tablet therapy, of which 10.1% (SE = 1.54%) presented with concurrent AI disorders, a proportion numerically larger than that observed in the general cohort, but this difference was not statistically significant (p = 0.11). The distribution of AI disorders among cladribine-treated patients and in the general MS cohorts demonstrated significant heterogeneity, including diabetes mellitus, Hashimoto’s thyroiditis, psoriasis, Sjögren’s syndrome, and various other autoimmune conditions. Notably, some patients presented with 2 or more AI comorbidities in addition to MS.
Clinical cases
Cladribine in MS with psoriasis and psoriatic arthritis
Case report 1
A 34-year-old female with a history of PsA treated with methotrexate experienced a right lower limb paresis in 2020 without consulting a neurologist, followed by right-sided sensorimotor deficits in mid-2022. The spinal cord MRI exam performed in November 2022 revealed a C2 myelitis. In early 2023, she experienced a new neurological event with a cerebral lesion on MRI, and RMS was diagnosed. Her EDSS score was 3.5. After intravenous corticosteroid treatment and vaccinations, she was started on cladribine treatment in May 2023. By March 2024, 10 months post-initiation, she showed no clinical or radiological MS activity, and her dermatological condition remained stable, although she reported cervical pain. However, at 20 months post-cladribine introduction, she experienced a recurrence of PsA activity with new inflammation in previously unaffected joints. Conversely, on the MS side, follow-up MRI at 23 months post-cladribine introduction remained stable, with no neurological disease activity (Table 1).
Demographic and clinical characteristics of the eight cases presented in more detail below.
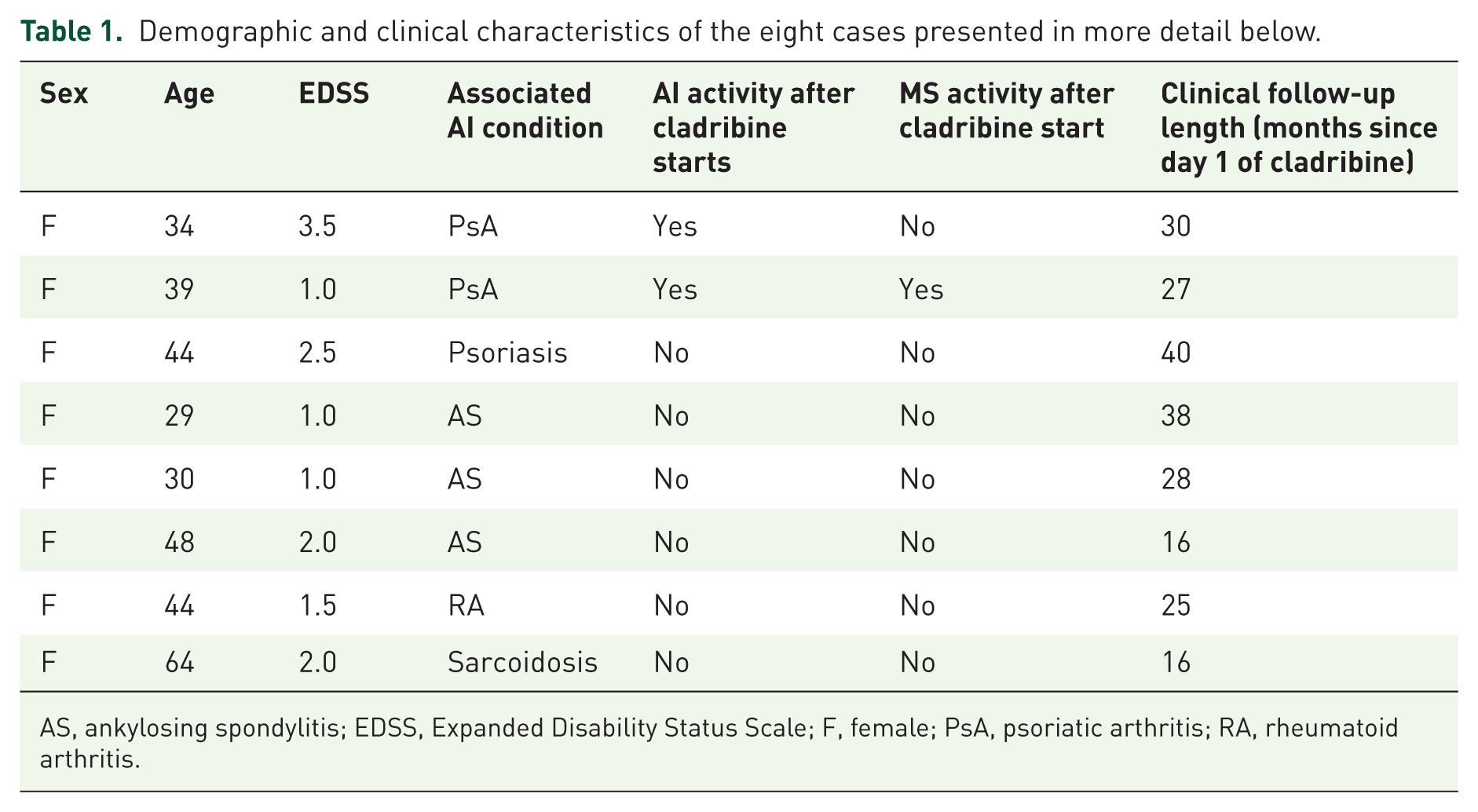
AS, ankylosing spondylitis; EDSS, Expanded Disability Status Scale; F, female; PsA, psoriatic arthritis; RA, rheumatoid arthritis.
Case report 2
A 39-year-old female with a personal and family history of autoimmune disorders, including PsA and MS in a cousin, was diagnosed with MS. Her initial symptoms appeared in January 2019 with mild left-sided sensorimotor deficits and facial involvement. Initial tests, including spinal MRI, cerebrospinal fluid (CSF) analysis, evoked potentials, and autoimmune markers, were normal. In May 2023, she experienced lower limb paresthesia with reduced vibration sense. Spinal MRI revealed thoracic and cervical T2 lesions, with concomitant supratentorial lesions on brain MRI. At that time, she had an EDSS of 1.0 and was started on cladribine in August 2023. However, in late October 2023, approximately 2 months post-initiation, she had an MS relapse with right-sided hypoalgesia. Follow-up MRIs in December 2023 showed a new C4–C5 lesion that was treated with intravenous corticosteroids. By July 2024, while free from MS relapses, she was experiencing significant disability because of uncontrolled PsA attacks and pain. In late December 2024, the 2-year MRI post-cladribine initiation showed stable MS lesions.
Case report 3
A 44-year-old female with RMS and psoriasis had a history of dyslipidemia and obesity. MS onset occurred in November 2004 with symptoms including four-limb paresthesia. MRI showed white matter hyperintensities and positive oligoclonal bands. After starting interferon beta-1a in April 2005, treatment was suspended in April 2007 for pregnancy planning. During her pregnancy in June 2008, she developed right hemiparesis, treated with methylprednisolone. Subsequent relapses included right optic neuritis in May 2009 and a spinal cord event in May 2010. Because of positive John Cunningham virus (JCV) testing, Natalizumab was not an option, leading to glatiramer acetate treatment in October 2010, which was stopped for a second pregnancy. After a four-year follow-up gap, she returned in November 2016 with bilateral lower limb deficits. Dimethyl fumarate and glatiramer acetate were tried but interrupted due to side effects. In February 2020, she experienced sensory disturbances treated with methylprednisolone. Glatiramer acetate was resumed in March 2020, but a gadolinium-enhancing lesion was found in December 2021. Following a COVID-19 infection in March 2022, she developed vertigo and diplopia, treated with methylprednisolone. Cladribine therapy was initiated in July 2022, and as of November 2025, she has been relapse-free with an EDSS score of 2.5 while continuing ustekinumab for psoriasis.
Cladribine in MS with ankylosing spondylitis
Case report 1
A 29-year-old woman with AS was diagnosed with RMS in January 2019 based on MRI and CSF testing after presenting with lower limb hypoesthesia and an EDSS score of 2.0. A platform treatment was introduced, but in 2022, MRI findings revealed a new T2 lesion, multiple black holes, and increasing atrophy. In the same year, she experienced electric discharge sensations in the left limbs and dysuria, along with mild neurocognitive symptoms confirmed by the neuropsychological assessment. Since she did not want a daily treatment, she was JCV positive with a high index (2.3) and had a pregnancy plan in the medium term. Cladribine tablets were proposed and started in September 2022, with the second year’s dose administered as scheduled. At the most recent evaluation in the summer of 2025, clinical assessment revealed an EDSS score of 1.0 with no new relapses, although she reported ongoing AS-related chronic pain without new inflammatory attacks. Radiologically, the lesion load remained stable.
Case report 2
A 30-year-old female presented with comorbid MS and AS. Her MS history began in 2020 with right optic neuritis confirmed by altered right visual evoked potentials, leading to a diagnosis of MS in September 2020. At that time, the EDSS score was 1.0. The therapeutic decision favored cladribine tablets, considering her difficulty with daily medication due to changing work schedules (which led to pushing forward treatment introduction until acceptance of cladribine in July 2023) and taking into account the potential for therapeutic adjustment for AS after 18 months if necessary. At 28 months post-initiation of cladribine, she showed no MS activity or AS inflammatory attacks but experienced disabling AS-related chronic pain.
Case report 3
A 48-year-old female with a diagnosis of AS presented to the emergency department in January 2022 with progressive binocular horizontal diplopia, following a suspension of adalimumab treatment for AS since December 2021. MRI showed a small contrast-enhancing lesion in the posterior fossa, and CSF analysis revealed 12 oligoclonal bands. Follow-up brain and spine MRI in 2022 showed a new contrast-enhancing right temporal juxtacortical lesion and a small left juxtaventricular hyperintensity, with an EDSS score of 2.0 at that time. In 2023, a neurology-rheumatology multidisciplinary team recommended an anti-CD20 treatment to control both conditions. However, due to inadequate control of AS symptoms, the treatment was later switched to cladribine tablets in the summer of 2024. Notably, at 16 months post-initiation of cladribine, the patient showed no disease activity in either MS or AS.
Cladribine in MS with rheumatoid arthritis
Case report
A 44-year-old female presented in June 2023 with gait instability, dizziness, and dysarthria. She had a history of RA diagnosed at 38, treated initially with methotrexate and later with rituximab, which was stopped in 2021 due to relapse. A brain MRI prior to starting anti-tumor necrosis factor (TNF) therapy (adalimumab) revealed a single periventricular white matter lesion, leading to the choice of abatacept instead. By summer 2023, she developed new focal neurological symptoms, and a contrast-enhanced MRI showed nine inactive lesions and one active plaque in the posterior fossa, confirming a diagnosis of RMS. Cladribine was initiated to avoid double immunosuppression, with the first course given in October-November 2023 and the second in October-November 2024. A follow-up MRI 6 months post-treatment showed no progression, and by 2025, she remained clinically stable with an EDSS of 1.5, continuing treatment for RA with abatacept.
Cladribine in MS with sarcoidosis
Case report
A 64-year-old female with a history of sarcoidosis involving ocular, mediastinal, and lymph nodal regions was diagnosed in 2012 based on clinical presentation and histological analysis. In February 2015, she developed right leg numbness and weakness, leading to brain and spinal cord MRIs that revealed multiple lesions and positive oligoclonal bands in the lumbar puncture. Initially interpreted as neurosarcoidosis, she was treated with methotrexate, achieving clinical stability. In 2020, she experienced decreased visual acuity and arm numbness, with investigations showing granulomatous uveitis and a new cervical lesion. After switching to infliximab for uncontrolled neurosarcoidosis, she remained stable. However, a radiological assessment in November 2023 revealed three new enhancing brain lesions, prompting further evaluation that concluded a diagnosis of MS. Consequently, anti-TNF treatment was stopped, and methotrexate was restarted. Cladribine was chosen for MS treatment, with the first course initiated in July 2024. A follow-up MRI in February 2025 showed stability; her EDSS remained unchanged at 2.0, and no clinical/radiological reactivation of neurosarcoidosis occurred.
Discussion
Autoimmune comorbidities in the MS population
Comorbidities may negatively impact the MS clinical course by worsening clinical symptoms, delaying diagnosis, and limiting therapeutic options. Since the presence of another AI condition necessitating steroid treatment or immunosuppressants is almost invariably an exclusion criterion from clinical trials for MS, there is a lack of evidence-based guidance for managing patients with coexisting autoimmune comorbidities using approved disease-modifying treatments. The absence of valuable data eventually results in treatment retardation or interruption, underuse of certain immunosuppressant agents, and increased risk of adverse events. 23 In more detail, when autoimmune diseases coexist, therapeutic decisions for PwMS are significantly affected if the additional diagnosis justifies the introduction of an immunosuppressive therapy or a biologic treatment. This is often the case for inflammatory rheumatic diseases (such as rheumatoid arthritis, ankylosing spondylitis, and psoriatic arthritis) and inflammatory bowel diseases (such as Crohn’s disease and ulcerative colitis). 19
The optimal scenario is when both MS and the concurrent autoimmune disease can be treated with the same medication. Examples include anti-CD20 therapies for rheumatoid arthritis or natalizumab for Crohn’s disease. 20 A more challenging situation arises when different medications are required, which may increase the risk of adverse effects. Notably, some treatments for autoimmune disorders, such as anti-TNF-alpha therapies, might potentially increase the risk of MS relapses. 24 This raises important questions about the safety of these therapies in patients with concurrent MS. In complex cases, clinicians often need to prioritize treating one condition, which may adversely affect the other. However, in these rapidly evolving therapeutic fields, there is a lack of information regarding the impact of new biologic therapies on MS progression or the efficacy of combination therapies. The complex interplay between MS and other autoimmune diseases highlights the need for personalized treatment strategies and further research into the effects of emerging therapies on concurrent autoimmune conditions.
Treating MS with comorbid autoimmune disorders using cladribine: Considerations on transient immunosuppression and immune reconstitution
Cladribine tablets represent a significant advancement in the treatment of RMS, with over 131.000 patients treated worldwide since their approval in 2017.25,26 This therapy operates through a unique mechanism of transient immunosuppression, selectively depleting B and T lymphocytes, which leads to a qualitative reconstitution of the immune system. This process not only reduces pathogenic lymphocytes but also promotes the emergence of a naïve lymphocyte population, contributing to long-term disease control and sustained efficacy. The treatment allows for extended periods free from therapy, providing patients with opportunities for family planning and vaccinations while maintaining a favorable safety profile characterized by manageable side effects. 27 Less than 1% of severe infections are reported 28 and no new safety signals are emerging over time, even in older patients. 29 Cladribine’s “reset” effect on the immune system suggests its potential application beyond MS to other autoimmune diseases, including inflammatory bowel diseases (IBD) such as Crohn’s disease.30,31 For instance, a recent case report highlighted a 33-year-old female with both primary sclerosing cholangitis and MS, who achieved resolution of liver and neurological symptoms, along with stable brain imaging and normalized liver parameters, during a 2-year follow-up after treatment with oral cladribine. 32 In our case series, we present eight PwMS with different AI conditions associated with MS: psoriasis, psoriatic arthritis, ankylosing spondylitis, rheumatoid arthritis, and sarcoidosis. All patients were female, mirroring the broader cohort sex distribution of MS plus AI comorbidities in the registry, where female sex was overrepresented (with almost 80% being women). Among them, positive effects of cladribine were observed in PwMS with concomitant RA, AS, psoriasis, or sarcoidosis.
Literature review on the impact of cladribine for selected AI conditions other than MS
Psoriasis and psoriatic arthritis
Psoriasis is a chronic, immune-mediated inflammatory skin disorder characterized by well-demarcated erythematous plaques covered with silvery scales. It results from dysregulated T cell activation and cytokine overproduction, where activated dendritic cells present skin antigens, leading to the differentiation of CD4+ T cells into Th17 cells influenced by cytokines such as IL-23, IL-6, and TGF-β. These Th17 cells secrete pro-inflammatory cytokines, including IL-17, IL-22, TNF-α, and IFN-γ, causing abnormal keratinocyte proliferation and inflammatory cell infiltration.33–35 In psoriatic arthritis (PsA), similar mechanisms trigger synovial inflammation and joint damage.36,37 Limited data exists on cladribine’s efficacy in psoriasis or PsA, with early evidence suggesting some benefit in refractory PsA. 38 Subsequent reports indicated psoriasis regression following cladribine treatment for various conditions.39–41 A recent study 42 showed significant improvement in a murine model of psoriasiform dermatitis, indicating a potential therapeutic effect. However, the varied impact of cladribine on psoriatic manifestations in clinical cases indicates the need for further investigation to clarify its role in treating associated psoriatic disorders.
Ankylosing spondylitis
AS is a chronic inflammatory rheumatic disease primarily affecting the sacroiliac joints and spine. 43 The 2019 American College of Rheumatology (ACR) guidelines recommend physical activity, nonsteroidal anti-inflammatory drugs, and TNF inhibitors for refractory cases. 44 However, concerns exist regarding the potential role of anti-TNFα therapies in developing demyelinating lesions.24,45,46 The association between AS and MS has been debated, with conflicting studies on shared genetic risk factors.47,48 This dual diagnosis presents therapeutic challenges due to the lack of effective treatments for both conditions. Leflunomide showed limited efficacy in AS, benefiting peripheral arthritis but not axial symptoms, 49 and these results were not confirmed in later trials. 50 Treatments effective in AS, such as secukinumab and anti-IL12/23 agents, have not met primary endpoints in MS trials.51,52 Cladribine emerges as a potential therapeutic alternative, offering long-term efficacy in MS while allowing for AS-specific treatments to be initiated later, thus avoiding continuous combined immunosuppression. Moreover, a recent Australian study reported an incidence of de novo spondyloarthritis in anti-CD20 mAb-treated PwMS being over nine times greater than the highest estimates for the general population, encouraging testing alternative medications, such as cladribine, as potential rescue treatment in these cases. 53
Rheumatoid arthritis
RA is a chronic autoimmune inflammatory disease characterized by synovial inflammation and joint destruction. Its pathogenesis involves the activation of antigen-presenting cells, leading to the differentiation of naïve CD4+ T cells into Th1 and Th17 subsets, which secrete pro-inflammatory cytokines such as IFN-γ, IL-17, and TNF-α.54,55 Both MS and RA share similarities in their pathogenesis, including the roles of T and B lymphocytes, genetic predisposition, and overlapping therapeutic options. However, significant immunological differences complicate treatment choices, as TNFα inhibitors may benefit RA patients but worsen MS. 20 Data on cladribine’s efficacy in RA is limited to intravenous or subcutaneous formulations, with no systematic studies on oral tablets.56–58 A study performed in five patients refractory to over three disease-modifying drugs 57 showed that cladribine administration led to effective B and T lymphocyte depletion in RA patients. Moreover, continuous cladribine infusion has been shown to induce rapid monocyte disappearance, suggesting potential for broader use in refractory cases.59,60 Although cladribine demonstrated a favorable safety profile, its clinical efficacy remains inconclusive, and larger studies are needed to better estimate the efficacy of this therapeutic option. Moreover, other molecules, such as anti-CD20, have proven effective against moderate to severe MA resistant to anti-TNF treatments and could therefore be used in the case of MS plus RA.61,62 Nonetheless, safety concerns about serious infections in these cases 63 encourage looking for alternative, safer strategies. In this scenario, the commercialization of oral cladribine raises interest in its use for both MS and RA, given some shared pathophysiological mechanisms 64 and a more favorable safety profile.
Sarcoidosis
Sarcoidosis is a multisystem inflammatory disease characterized by non-caseating granulomas, primarily affecting the lungs and lymph nodes, with an unclear etiology linked to an abnormal immune response. 65 Approximately 5%–15% of cases involve the central nervous system, termed neurosarcoidosis, which complicates treatment. Corticosteroids are the first-line therapy, but refractory cases may require additional immunosuppressants. Managing patients with both sarcoidosis and MS necessitates careful coordination to avoid exacerbating either condition. Rituximab has been historically used as an off-label, third-line option for refractory sarcoidosis. 66 While being effective in anecdotal reports, studies suggest limited efficacy, with cases of worsening/no benefit in refractory pulmonary sarcoidosis, occasionally leading to death. Interestingly, a prospective, open-label trial involving 10 individuals with treatment-refractory pulmonary disease did not show a clear benefit and potentially increased harm (one death). 67 In addition, it should be kept in mind that sarcoid reactions can also occur as a consequence of anti-CD20 treatment. 68 Regarding cladribine, in our case study, this medication was used to treat MS while methotrexate managed sarcoidosis, with some literature suggesting cladribine’s potential benefits for both disorders. Moreover, previous reports (limited to three cases published between 2004 and 2015) indicate that intravenous cladribine has effectively treated neurosarcoidosis, providing significant responses without the need for ongoing immunosuppressive therapy.69,70 Given its mechanism of inhibiting DNA synthesis in lymphocytes, 58 cladribine may offer a safer alternative for managing both conditions. However, further research using the oral formulation of cladribine is needed to evaluate its efficacy in patients with concurrent MS and sarcoidosis.
Conclusion
In conclusion, AI comorbidities are frequent in patients with MS. Pharmacological treatment with immunoactive medications in these cases may raise efficacy and safety concerns for either or both disorders. Cladribine’s mechanism of action and administration scheme make it a potential option in this scenario. Its ability to induce selective immune reconstitution and tune immune system functioning, coupled with a favorable safety profile and cyclic administration, could allow
- co-efficacy on the AI condition other than MS in certain cases (e.g., psoriasis, AS, and sarcoidosis), with the advantage of using one molecule for two disorders;
- avoidance of double immunosuppression and greater risk of adverse events if the associated AI comorbidity requires its own continuous immunotherapy.
Some limitations must be considered in interpreting our findings. First, given the respective nature of the analysis of national MS registry data, information on autoimmune comorbidities—particularly milder ones—that was not entered by clinicians could not be retrieved; this might have led to slightly underestimating the real prevalence of concurrent AI disorders in PwMS. Second, the case series collection design limits causal inference and may have introduced selection/reporting bias related to the description of favorable outcomes. Third, it must be acknowledged that the description of single cases may give a hint at the potential benefit of cladribine on the associated AI condition. The collected series explores this hypothesis of using a single immune-active molecule in similar scenarios, but does not provide solid evidence to defend it. Indeed, the low number of patients and the absence of validated outcome measures that could transversally apply to all descriptions limit the generalizability of our conclusions. Further research—notably larger-scale, prospective studies with longer follow-up periods—is needed to understand its impact and possible use in these clinical scenarios.
A multidisciplinary, personalized approach to treatment decision remains essential when AI disorders coexist: this should consider disease-underlying pathways and mechanisms that are shared by different immune-mediated conditions and could therefore benefit from a common therapeutic intervention. This treatment-selection strategy would allow one to choose the best options, not to undertreat (therapeutic inertia for the fear of multiplying adverse events) or to worsen (inappropriate treatment combination) either disease.
Supplemental Material
sj-docx-1-tan-10.1177_17562864261458568 – Supplemental material for Cladribine use for multiple sclerosis with autoimmune comorbidities: retrospective analysis of the French MS registry, case series, and therapeutic considerations
Supplemental material, sj-docx-1-tan-10.1177_17562864261458568 for Cladribine use for multiple sclerosis with autoimmune comorbidities: retrospective analysis of the French MS registry, case series, and therapeutic considerations by Vito A. G. Ricigliano, Ines Masmoudi, Marine Boudot de la Motte, Eric Manchon and Jérôme De Seze in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.