
Abstract
Background:
Hemorrhage is one of the most significant complications of percutaneous nephrolithotomy (PCNL) and may lead to clinically significant persistent hematuria requiring digital subtraction angiography (DSA) and transcatheter arterial embolization (TAE). Identifying predictors of TAE may improve perioperative planning and risk stratification.
Objectives:
To determine predictors of need for TAE in patients evaluated with DSA for persistent post-PCNL hemorrhage.
Design:
Single-center retrospective observational study.
Methods:
From 2021 to 2024, a total of 2947 tubeless PCNL procedures were performed at our institution. Consecutive adult patients who developed clinically significant persistent post-PCNL hemorrhage and underwent DSA were assessed. Persistent hematuria was operationally defined as severe visible hematuria persisting for >24 h despite conservative management or recurrent severe hematuria after initial stabilization. DSA referral followed predefined escalation criteria after failure of conservative measures, including hemodynamic instability, Hb drop ⩾3 g/dL within 24 h or progressive decline, transfusion requirement ⩾2 units within 24 h, and/or recurrent clot retention requiring clot evacuation and/or continuous bladder irrigation. TAE was performed only when DSA demonstrated a culprit vascular lesion.
Results:
The mean age of the study population was 55.1 ± 10.6 years, and 68% were male. Among the 100 patients who underwent DSA for persistent post-PCNL hemorrhage, 36 (36%) required TAE, while 64 (64%) had normal angiographic findings and were managed conservatively. On multivariable logistic regression analysis, diabetes mellitus (odds ratio (OR) 7.42), larger stone size (OR 1.27 per mm), higher stone density (OR 1.007 per Hounsfield unit), greater skin-to-stone distance (OR 1.14 per mm), and longer operative time (OR 1.18 per minute) independently predicted the need for TAE. Pseudoaneurysm was identified in 77.8% of embolized patients and arteriovenous fistula in 22.2%. Selective coil embolization achieved 100% clinical success without the need for repeat embolization, surgical exploration, or nephrectomy.
Conclusion:
Among patients undergoing DSA for clinically significant persistent post-PCNL hemorrhage, diabetes mellitus, larger stone size, higher stone density, greater skin-to-stone distance, and longer operative time were independently associated with the need for TAE.
Plain language summary
This study highlights key predictors for the need for AE following PCNL, including diabetes, larger stone size, higher stone density, longer operative time, and increased skin-to-stone distance. The presence of stones in parenchyma appeared protective.
Introduction
Percutaneous nephrolithotomy (PCNL) is recognized as the gold standard treatment for large or complex renal calculi. 1 Recent guidelines and cohort studies highlight the safety and effectiveness of PCNL in treating staghorn and other large calculi, establishing it as the preferred intervention for complex stone disease.2,3 Despite advances in procedural techniques, PCNL remains an invasive procedure that can potentially damage renal vessels and surrounding organs, so anticipating complications is crucial.4,5
Overall, PCNL is a safe procedure; however, a risk of complications exists in a minority of patients. Among these, bleeding is the most concerning major complication. 5 Significant post-PCNL hemorrhage can happen immediately or may arise after a delay. 6 The incidence of transfusion varies between 1% and 11%, while the rate of required angiographic embolization to control bleeding vessels ranges from 0.6% to 2.6%.7,8 In one large series, massive renovascular bleeding, often leading to persistent hematuria, was observed in approximately 0.3% to 1% of patients.9,10 The most common underlying issues include renal pseudoaneurysms and arteriovenous fistulas (AVF), which most commonly present within the early postoperative period, typically within the first days to 2 weeks after PCNL. 10
When significant hematuria persists after PCNL, the initial approach is conservative. It includes bed rest, adequate hydration, bladder irrigation, correction of coagulopathy, and blood transfusions if necessary.11,12 However, in case of persistent bleeding after these measures, additional evaluation is warranted. Cross-sectional or angiographic imaging is used to detect the cause of bleeding. In hemodynamically unstable patients who require greater than 2 units of blood transfusion, have a hemoglobin (Hb) drop of greater than 3 g/dL (≈30 g/L) despite conservative management, or have vascular lesions such as pseudoaneurysm, AVF, or active extravasation on imaging, the treatment of choice is transcatheter arterial embolization (TAE).12–16 Embolization is safe and extremely successful, with technical success of approximately 92% to 100% in the ability to arrest post-PCNL bleeding described in recent publications. There is a consensus of specialists that TAE must be performed urgently for persistent post-PCNL hemorrhage, since conservative care alone is typically insufficient. 17 Nevertheless, embolization is required only in a small subset of PCNL cases. Given that these complications can lead to significant morbidity, a major challenge is identifying which patients with persistent hematuria will need embolization. 18
Given the potentially life-threatening nature of persistent hematuria after PCNL, it is crucial to identify high-risk patients. Current guidelines and expert recommendations emphasize the importance of early angiographic evaluation in cases of ongoing bleeding accompanied by hemodynamic instability. 16 Practically, a number of factors, such as patient factors, stone composition, renal anatomy, and procedural aspects, can be utilized to assist in the decision to have angiography. In our research, the specific focus is on patients who have developed persistent hematuria after PCNL and would like to know which factors most accurately predict the need for TAE. Through the incorporation of recent human evidence and judicious analysis, we aim to offer enhanced risk stratification and perioperative planning. Our primary objective is to minimize major bleeding complications and ensure prompt treatment for patients at high risk of hemodynamic instability.
Materials and methods
Study design and setting
This retrospective observational study was conducted at Sina Hospital, Tehran University of Medical Sciences (Tehran, Iran). The study period spanned January 2021 to December 2024. The study was performed in accordance with the Declaration of Helsinki and was approved by the institutional ethics committee of Tehran University of Medical Sciences (Approval Code: IR.TUMS.SINAHOSPITAL.REC.1404.076). Patient identifiers were removed before analysis to ensure confidentiality. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational studies. 19 A completed STROBE checklist is provided as Supplemental File 1.
Study population
We reviewed adult patients who underwent tubeless PCNL during the study period. The study population consisted of consecutive patients who developed persistent post-PCNL hemorrhage meeting predefined criteria for escalation beyond routine postoperative management and therefore underwent digital subtraction angiography (DSA) to evaluate suspected renal vascular injury. Patients with transient or self-limited hematuria that resolved with routine postoperative care and did not meet escalation criteria were not included. Patients were excluded if essential variables required for analysis were missing or if severe renal impairment/acute renal failure was documented (e.g., Estimated Glomerular Filtration Rate (eGFR) < 30 mL/min/1.73 m2 where available).
Bleeding severity and referral criteria
Persistent hematuria was operationally defined as severe visible hematuria persisting for more than 24 h despite standardized conservative management, or recurrent severe hematuria after initial stabilization. 16 Conservative management included bed rest, hydration, correction of coagulopathy when present, hemostatic drugs, transfusion support as clinically indicated, clot evacuation when indicated, and continuous bladder irrigation when required. Referral for DSA was based on predefined escalation criteria after failure of conservative measures, including one or more of the following: hemodynamic instability (systolic blood pressure < 90 mmHg or persistent heart rate > 100 bpm), Hb drop ⩾3 g/dL or progressive decline within 24 h, transfusion requirement ⩾2 units packed red blood cells within 24 h, or recurrent clot retention requiring clot evacuation and/or continuous bladder irrigation. TAE was performed only when DSA identified a culprit vascular lesion (pseudoaneurysm, AVF, or active contrast extravasation).6,16,20
Imaging strategy
At our institution, contrast-enhanced CT angiography (CTA) is not routinely performed for persistent post-PCNL hemorrhage when patients meet criteria for urgent angiographic evaluation. This approach avoids two separate iodinated contrast administrations and minimizes delay to definitive management because DSA serves as both a diagnostic and therapeutic modality, allowing immediate selective TAE during the same session when a lesion is identified. CTA was reserved for selected situations, such as when immediate DSA was not available or when the clinical scenario suggested a low likelihood of endovascular intervention and stable patients.6,12,16,20
Data collection
Data were extracted from operative reports, anesthesia records, radiology reports, laboratory results, and interventional radiology documentation. Collected variables included age, sex, BMI, diabetes mellitus (DM), hypertension (HTN), cardiovascular disease, smoking status, alcohol consumption, and past medical history. Antiplatelet/anticoagulant use at the time of PCNL and documented coagulopathy were assessed. Hemangioma refers to an incidental superficial/subcutaneous hemangioma documented in the past medical history.
Stone characteristics included maximum stone diameter, stone density in Hounsfield units (HU), laterality, calyceal location, and number of involved calyces. Skin-to-stone distance (SSD) was measured on preoperative CT as the distance from the skin surface to the center of the target stone using standardized angles (0°, 45°, and 90°), with the mean value used for analysis. 21 The hydronephrosis grade was also recorded as mild (pelvic dilatation only), moderate (enlargement of pelvis and calyx, and blunting of the calyceal fornices), and severe (ballooning of the pelvicalyceal system accompanied by renal parenchymal atrophy), diagnosed by CT. 22
Operative and perioperative variables included operative time, number and location of access tracts, transfusion requirement and transfused units, ICU admission, and analgesic consumption expressed as morphine milligram equivalents (MME). Hemoglobin drop (ΔHb) was calculated as preoperative hemoglobin minus the lowest post-bleeding/pre-angiography hemoglobin value. Postoperative complications were classified using the Clavien–Dindo system and reported categorically according to available records.
Angioembolization procedure
Expert Interventional radiologists performed Angioembolization under aseptic conditions after local anesthesia. The femoral artery was accessed retrogradely through the groin using the routine method. The artery was punctured with a needle, and a guidewire was inserted. Using the Seldinger technique, a 6-French sheath was introduced over the wire. A 5-French diagnostic catheter was then guided through the sheath and slowly positioned within the suspected artery under fluoroscopic guidance. A nonionic iodinated contrast agent (approximately 300 mgI/mL) was injected, and DSA images were obtained to identify lesions such as pseudoaneurysms or AVFs. If a lesion was detected, a 2.7 to 2.8 French microcatheter was super-selectively guided to the involved branch, and embolization with a metal coil was performed until blood flow at the location of the lesion was completely occluded. The final DSA image revealed a confirmed total occlusion. The sheath and catheter were removed following the procedure, and the entry site was closed by vascular closure or direct pressure. The patient was kept in the supine position for 4–6 h, with vital signs monitored and the puncture site examined for any bleeding or hematoma. The distal pulse was also checked, and renal function was observed following the contrast injection.
Outcomes
The primary outcome was the need for TAE among patients undergoing DSA for clinically significant post-PCNL hemorrhage. Clinical success of TAE was defined as resolution or control of hematuria following selective embolization without the need for repeat angiography/re-embolization, surgical exploration, or nephrectomy during index hospitalization.
Statistical analysis
Analyses were performed using SPSS (version 28; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± SD and categorical variables as number (percentage). Normality was assessed using the Shapiro–Wilk test. Between-group comparisons were performed using an independent-samples t-test or Mann–Whitney U test for continuous variables and chi-square or Fisher’s exact test for categorical variables, as appropriate. Variables significant in univariable comparisons and clinically relevant factors were entered into multivariable logistic regression to identify independent predictors of TAE. To reduce the risk of model overfitting, given the limited number of embolization events, the number of variables included in the final multivariable model was restricted to clinically relevant predictors. Adjusted odds ratios (OR) with 95% confidence intervals (CI) are reported. A two-sided p-value < 0.05 was considered statistically significant.
Results
During the study period, 2947 patients underwent tubeless PCNL. Among these, 103 developed persistent post-PCNL hemorrhage meeting predefined criteria and underwent DSA. After excluding three patients due to incomplete records (n = 2) or acute renal failure (n = 1), 100 patients comprised the final study cohort. Of these, 36 patients (36%) required TAE due to an identified vascular lesion, while 64 patients (64%) had normal angiography and were managed conservatively. A flow diagram summarizing patient selection and study inclusion is presented in Figure 1.
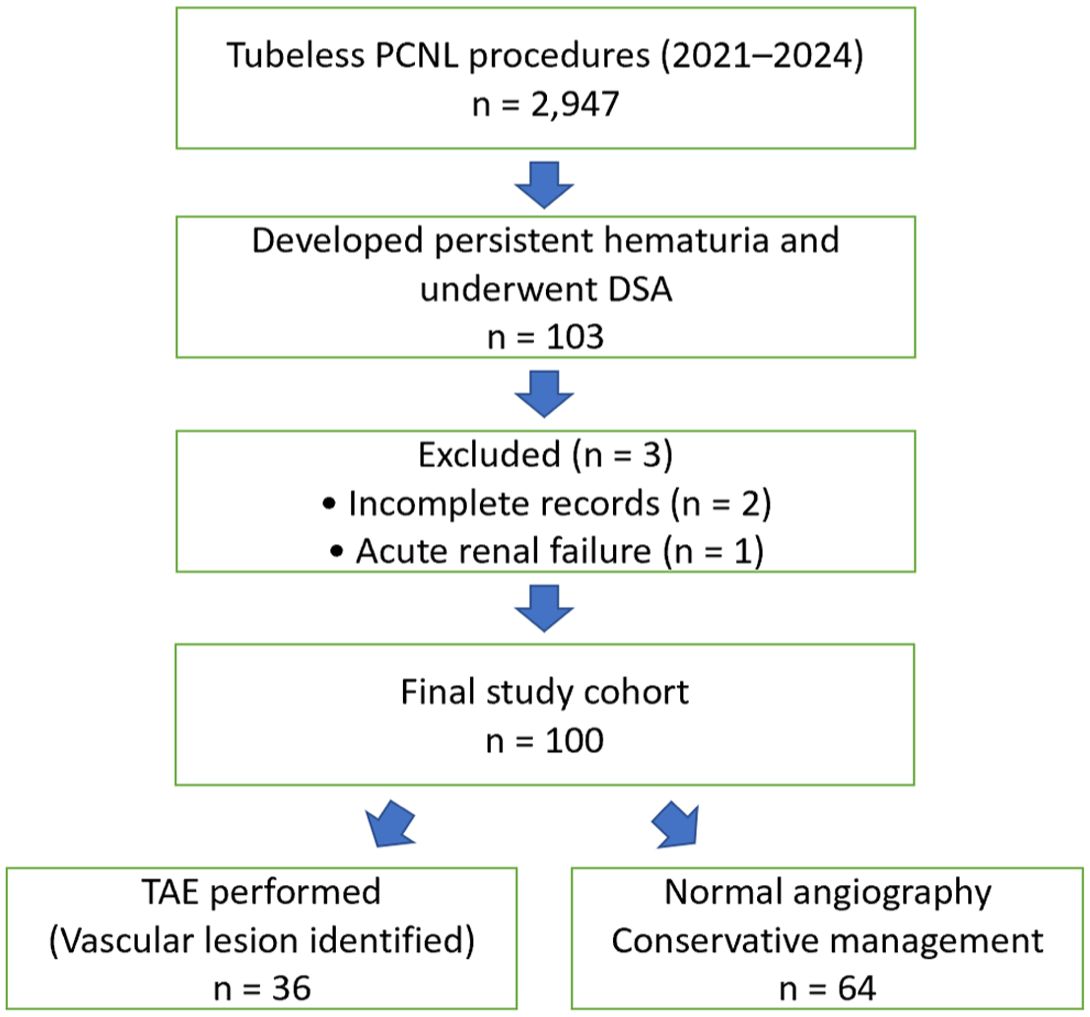
STROBE flow diagram of patient selection process.
The mean age of the patients was 55.12 ± 10.63 years, and 68% were male. Baseline demographic and clinical characteristics stratified by need for TAE are shown in Table 1. Baseline characteristics were comparable between groups with respect to age, sex, BMI, HTN, cardiovascular disease, smoking status, prior renal surgery, and history of embolization. DM was significantly more prevalent in the TAE group than in the non-TAE group (69.4% vs 23.4%, p < 0.001). Alcohol use was also more frequent in the TAE group (16.7% vs 3.1%, p = 0.017). Hydronephrosis grade was not significantly associated with the need for TAE (p = 0.726). Angiographic lesions in the TAE group consisted predominantly of pseudoaneurysm (77.8%) and AVF (22.2%; Table 2).
Baseline demographic and clinical characteristics according to need for TAE.
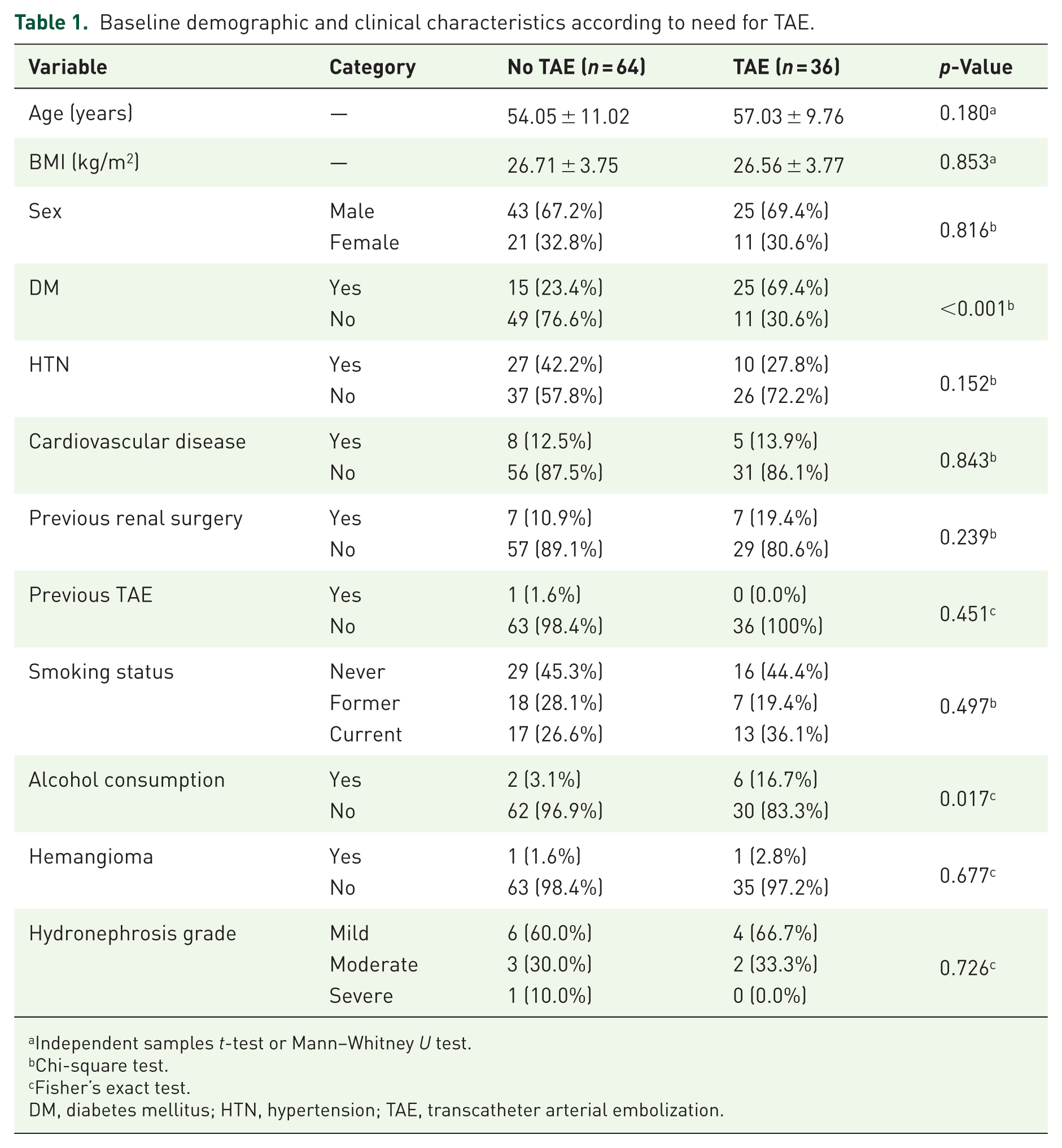
Independent samples t-test or Mann–Whitney U test.
Chi-square test.
Fisher’s exact test.
DM, diabetes mellitus; HTN, hypertension; TAE, transcatheter arterial embolization.
Perioperative, postoperative, and procedural characteristics according to need for TAE.
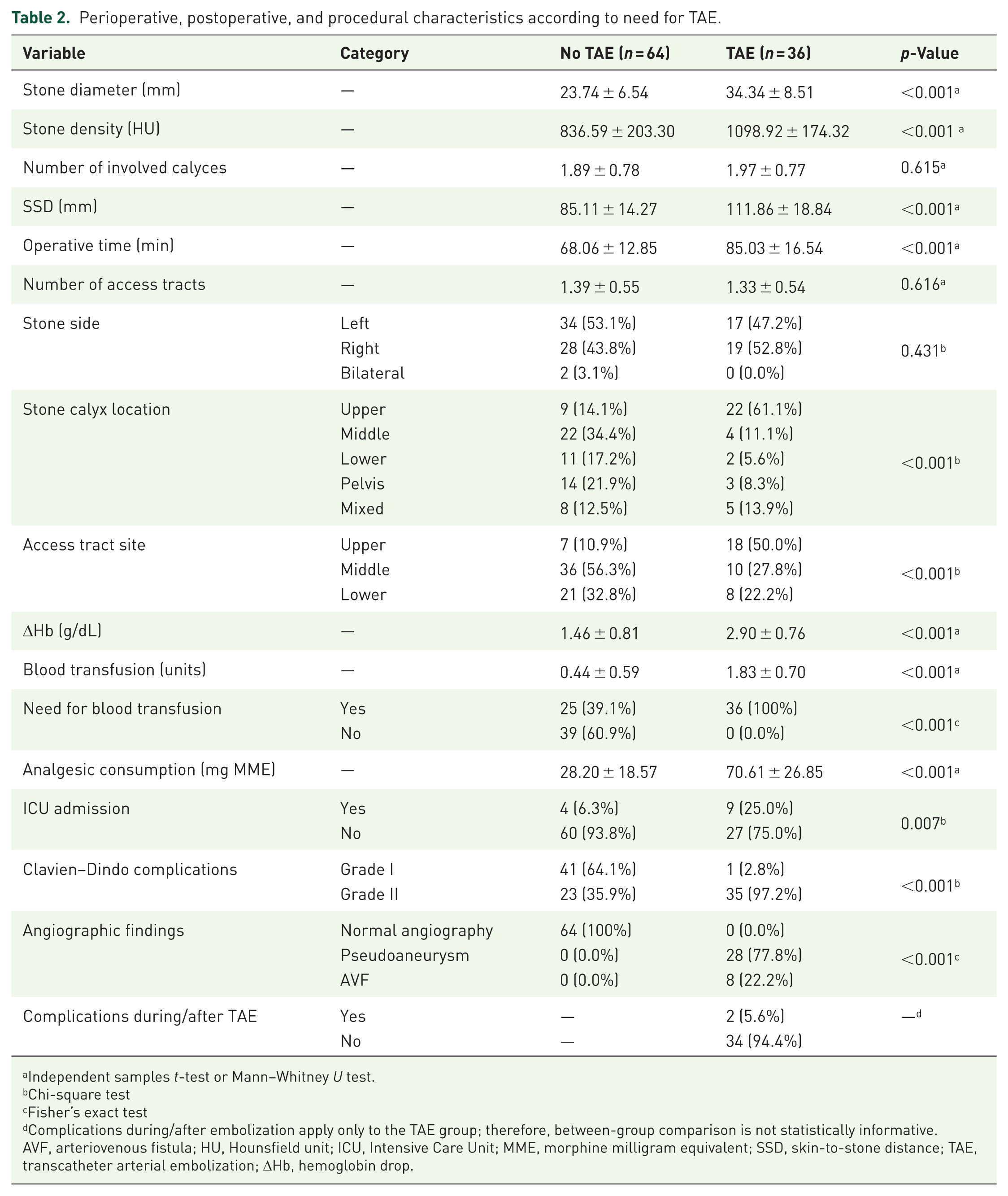
Independent samples t-test or Mann–Whitney U test.
Chi-square test
Fisher’s exact test
Complications during/after embolization apply only to the TAE group; therefore, between-group comparison is not statistically informative.
AVF, arteriovenous fistula; HU, Hounsfield unit; ICU, Intensive Care Unit; MME, morphine milligram equivalent; SSD, skin-to-stone distance; TAE, transcatheter arterial embolization; ΔHb, hemoglobin drop.
Perioperative and stone-related characteristics are summarized in Table 2. Patients requiring TAE had larger stones (p < 0.001) and higher stone densities (p < 0.001). SSD was also greater in the TAE group (p < 0.001). Upper calyceal stone location and upper pole access tract were more frequent among patients requiring TAE (both p < 0.001). Operative time was longer in the TAE group (p < 0.001).
Bleeding severity and postoperative outcomes are also detailed in Table 2. A total of 61% of patients required transfusion overall. ICU admission was more common in the TAE group (25.0% vs 6.3%, p = 0.007). Postoperative analgesic consumption was higher in the TAE group (p < 0.001). Clavien–Dindo grades are presented descriptively in Table 2. Because transfusion requirement contributes to grade II classification and was part of the escalation pathway, these data were not interpreted as independent predictors of TAE.
On multivariable logistic regression analysis, DM (OR 7.42, 95% CI 2.97–18.54, p < 0.001), larger stone size (OR 1.27, 95% CI 1.08–1.50, p = 0.003), higher stone density (OR 1.007 per HU, 95% CI 1.003–1.012, p = 0.003), greater SSD (OR 1.14, 95% CI 1.06–1.22, p < 0.001), and longer operative time (OR 1.18 per minute, 95% CI 1.03–1.36, p = 0.019) remained independently associated with the need for TAE (Table 3). The model demonstrated adequate calibration (Hosmer–Lemeshow p = 0.504).
Multivariable logistic regression analysis identifying independent predictors of TAE.

adjusted OR, adjusted odds ratio; CI, confidence interval; DM, diabetes mellitus; HU, Hounsfield unit; SSD, skin-to-stone distance; TAE, transcatheter arterial embolization.
Clinical success was achieved in all embolized patients. No patient required repeat embolization, and no nephrectomy was performed. Minor procedure-related complications occurred in two patients (5.6%).
Discussion
In this study, we evaluated predictors of persistent hematuria after PCNL requiring TAE. We identified both patient-related and procedural factors independently associated with embolization. DM emerged as a strong predictor (OR 7.42), consistent with prior reports linking metabolic comorbidities to increased post-PCNL bleeding risk. Du et al. 23 and Irani et al. 24 demonstrated a significant association between diabetes and delayed hemorrhage requiring embolization. Hu et al. 8 confirmed this finding in a recent meta-analysis (OR 3.27). The relationship may be explained by microvascular fragility and impaired vascular healing in diabetic patients, predisposing them to pseudoaneurysm or AVF formation.25,26
We also noted that stone complexity and size were significantly higher in patients who underwent embolization in our case series. This is consistent with the seminal work of Srivastava et al. 27 and El-Nahas et al., 28 who showed that larger and staghorn stones had an association with vascular injury and embolization requirement. Arora et al. 13 also revealed that higher stone complexity is an independent predictor of severe hemorrhage. Recent meta-analytic data found that staghorn and multiple stones remain independent predictors of major bleeding. 8 Increased stone burden likely necessitates more extensive manipulation and prolonged instrumentation, increasing the probability of vascular trauma. In addition, we observed that higher stone density independently predicted TAE requirement. Although prior studies have emphasized stone complexity, few have evaluated stone density as a separate parameter. Although HU itself is unlikely to directly cause vascular injury, it may reflect harder stones requiring more prolonged fragmentation, greater intrarenal manipulation, and potentially higher cumulative parenchymal trauma. 29 Therefore, stone density should be interpreted as a procedural complexity marker rather than a direct causal factor.
Access characteristics may influence the likelihood of clinically significant vascular injury after PCNL. Previous studies have identified upper calyceal puncture and multiple access tracts.28,30 In the present cohort, upper calyceal stone location and upper-pole access were more common among patients who underwent TAE. One possible explanation is that upper-pole access may increase the risk of posterior segmental arterial injury compared with lower-pole approaches.30,31 In addition, more oblique punctures may pass through a larger volume of renal parenchyma and thereby increase the possibility of vascular trauma.6,31 However, because the access site was not retained in our final multivariable model, this finding should be interpreted cautiously. Operative time was likewise independently associated with embolization, supporting findings by Zeng et al., who identified prolonged PCNL duration as a bleeding predictor. 32 Longer procedures may reflect technical complexity and cumulative parenchymal trauma.
A novel finding in our study was the association between increased SSD and the risk of embolization. While previous research has examined tract size and multiplicity, SSD has not been systematically evaluated.13,31,33 Greater SSD was independently associated with TAE requirement. One possible explanation is that a greater SSD may necessitate a longer access tract through perinephric tissue, which can make tract alignment and instrument control more difficult during PCNL. 34 However, increased SSD may also act as a surrogate marker for obesity, body habitus, and associated comorbidity burden.35–37 This parameter may offer an additional anatomical consideration for preoperative planning, particularly in obese individuals.
Angiographic findings in our cohort were consistent with established literature, with pseudoaneurysm and AVF accounting for nearly all vascular lesions.12,27,28,32,37 The predominance of pseudoaneurysms reflects the typical mechanism of partial arterial laceration with contained extravasation. TAE achieved complete bleeding control in all embolized patients, comparable to previously reported technical success rates ranging from 81.5% to 100%.12,13,24,31–33,37 Prior studies have also highlighted additional predictors of embolization, underscoring the multifactorial nature of post-PCNL vascular complications. He et al. showed urinary infection (OR 11.21) and hypertension (OR 5.69) to strongly predict embolization, and Kim et al. highlighted precise puncture (OR 3.82) as critical.38,39 Meanwhile, Surag et al. 31 determined that only tract size independently predicted in a tubeless group during PCNL. Another finding was that Postoperative analgesic consumption was higher among patients requiring TAE. This outcome shows that patients with more pain than others have more uncontrolled hematuria that requires embolization. However, this variable was considered a postoperative marker of clinical severity rather than an independent predictor.
This study has several limitations. Its retrospective single-center design introduces potential selection and information bias and may limit generalizability to other institutions. Although all consecutive eligible patients were included, a formal a priori sample size calculation was not performed, and the relatively small number of embolization events may reduce statistical power and increase the risk of model overfitting. Given the relatively small number of embolization events, the multivariable model was limited to a restricted number of predictors, and residual confounding cannot be excluded. Certain potentially relevant variables, including preoperative urine culture status, Guy’s Stone Score, and cortical thickness, were not consistently available and therefore could not be analyzed. No patients had renal anatomical anomalies, coagulopathy, or active antiplatelet/anticoagulant use, which may further limit applicability to broader or higher-risk populations. Additionally, long-term outcomes such as renal functional trajectory and quality of life after embolization were not assessed. Prospective multicenter studies with larger cohorts and standardized reporting are needed to externally validate these findings.
Conclusion
In this single-center retrospective study of patients undergoing DSA for persistent hemorrhage after tubeless PCNL, diabetes mellitus, larger stone size, higher stone density, greater skin-to-stone distance, and longer operative time were independently associated with the need for transcatheter arterial embolization. These findings highlight the importance of preoperative stone burden and anatomical factors in predicting severe post-PCNL bleeding requiring endovascular intervention. Early identification of high-risk patients may facilitate closer monitoring and timely angiographic evaluation. Prospective multicenter studies are warranted to externally validate these predictors.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261458089 – Supplemental material for Predisposing factors for angioembolization in persistent hematuria after percutaneous nephrolithotomy: a retrospective analysis
Supplemental material, sj-docx-1-tau-10.1177_17562872261458089 for Predisposing factors for angioembolization in persistent hematuria after percutaneous nephrolithotomy: a retrospective analysis by Ali Alfiel, Abdolreza Mohammadi, Mohammad Mahdi Mehrabi, Sara Ashtari, Farshid Alaedini, Fateme Guitynavard, Parsa Nikoofar and Seyed Mohammad Kazem Aghamir in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.