
Abstract
Cancer of unknown primary (CUP) is an aggressive malignancy with a persistently poor prognosis. Renal metastases from an occult primary adenocarcinoma are exceptionally rare and diagnostically challenging, frequently mimicking primary kidney cancer. This case report details a rare instance of metastatic adenocarcinoma to the kidney from an occult primary origin, initially misclassified as primary renal cell carcinoma. A 60-year-old male patient was admitted to our department for further evaluation of a cystic-solid right renal mass. Staging revealed synchronous extrarenal metastases. Subsequent immunohistochemical analysis indicated gastrointestinal differentiation, yet exhaustive diagnostic workup failed to identify the primary tumor site. The patient underwent radical nephrectomy followed by biomarker-guided FLOT (fluorouracil, leucovorin, oxaliplatin, and docetaxel) chemotherapy combined with camrelizumab immunotherapy, achieving a progression-free survival of approximately 7 months, accompanied by a temporary decline in tumor markers. Tumor recurrence manifested at 11 months postoperatively as pulmonary progression, at which point retrospective molecular profiling of the archived specimen revealed an ERBB2 amplification, providing a molecular rationale for subsequent targeted therapy. This case highlights the crucial roles of multidisciplinary collaboration and molecular technology in resolving diagnostic dilemmas and identifying actionable targets in CUP. It offers two key clinical takeaways: diagnostically, a solitary kidney mass with other metastases should prompt consideration of a renal metastasis, even though primary kidney cancer is more common. Therapeutically, while the identified biomarker provided a rationale for precision therapy, the resulting clinical benefit was limited and transient. This suggests that the aggressive biology and spatial heterogeneity typical of CUP can attenuate the long-term efficacy of biomarker-guided interventions.
Introduction
Cancer of unknown primary site (CUP), accounting for 3%–5% of all malignant neoplasms, represents the seventh to eighth most prevalent malignancy. 1 The clinical profile of CUP is defined by its aggressive behavior and rapid metastatic progression. 1 Nevertheless, conventional treatment strategies often lack precision due to an undetermined tissue of origin, resulting in substantially inferior clinical outcomes compared to metastatic malignancies with established primary sites.
As an uncommon site of metastatic involvement, the kidney often presents diagnostic challenges due to the subtle and nonspecific clinical manifestations associated with renal metastases. Most cases are incidentally detected through imaging examination rather than clinical symptoms, and the majority of patients remain asymptomatic even with extensive parenchymal infiltration. It has been reported that fewer than 20% of cases manifest with hematuria or proteinuria. 2 This clinically silent growth pattern contributes significantly to diagnostic delay. While renal metastases typically demonstrate characteristic imaging features of small bilateral multifocal lesions, exceptions occur as solitary large masses that may radiographically mimic primary renal cell carcinoma (RCC),3–6 further compounding the diagnostic challenge.
Herein, we report a challenging case of renal metastasis from an occult primary malignancy, despite extensive multimodal diagnostics. Immunohistochemistry (IHC) indicated gastrointestinal differentiation, yet no primary site was identified. We systematically analyze the diagnostic dilemmas encountered throughout the clinical trajectory and detail our therapeutic decision-making process. Given the paucity of documented evidence on renal metastases with an unknown primary site in the contemporary literature, this case serves as an instructive paradigm for navigating such diagnostic complexities and proposes a structured multidisciplinary approach. This case report has been prepared in accordance with the CARE guidelines (Supplemental Materials). 7
Case presentation
A 60-year-old male patient was admitted to our department (Department of Urology, the First Affiliated Hospital of Xi’an Jiaotong University) in December 2023 for further evaluation of a cystic-solid right renal mass. The lesion was incidentally identified on a computed tomography (CT) scan performed at a local hospital for perineal discomfort. The patient reported no abdominal/flank pain, gross hematuria, or systemic symptoms such as fever or night sweats. His medical history was significant only for hypertension with no history of smoking, alcohol consumption, other chronic diseases, or familial malignancy. Physical examination revealed a right-sided varicocele, with absence of renal region distension or costovertebral angle tenderness.
Abdominal CT suggested the presence of a large (155.1 × 171.2 × 169.1 mm), oval-shaped, cystic-solid hypodense lesion in the right renal region, containing punctate hyperdense foci. On contrast-enhanced imaging, mild enhancement was observed in the cystic components with a mean attenuation of 42.3 HU, a value suggesting complex contents rather than simple fluid, while the solid portion exhibited heterogeneous enhancement predominantly in the mid-to-inferior regions, demonstrating a hypervascular washout pattern with an attenuation of 92.9 HU in the arterial phase that decreased to 75.4 HU in the delayed phase (Figure 1(a)–(c)). Tortuous vessels were identified at the inferior pole of the mass, with no significant perilesional lymphadenopathy noted. Computed tomography angiography (CTA) further delineated complex vascular anatomy, including a tripartite right renal artery with displacement of all branches and a small penetrating tumor-feeding artery originating from the superior branch (Figure 1(d)). These imaging characteristics were highly suspicious for a malignant neoplasm. Chest CT demonstrated a solid micronodular opacity within the apical segment of the right upper lobe. Prompted by this suspicious pulmonary finding, concurrent elevation of the serum alkaline phosphatase (ALP) level (130 U/L; detailed below) and the substantial tumor burden, a comprehensive metastatic workup was initiated. 8 Whole-body bone scintigraphy combined with three-dimensional CT reconstruction of the ribs revealed multiple metastatic lesions involving the ribs.

Imaging findings of the metastatic renal mass. (a–c) Contrast-enhanced abdominal CT scans (a: coronal, b: axial, c: sagittal planes) reveal a large cystic-solid mass in the right kidney with associated hydronephrosis. (d) Representative image of CTA. (e) Postoperative PET-CT reveals no abnormal glucose metabolic foci in the resection bed.
The patient’s other test results were unremarkable. However, to exclude the possibility of renal metastasis from extra-renal primaries (e.g., gastrointestinal or prostate origin), given the patient’s age, the complex nature of the mass, and its close anatomical proximity to the digestive tract, a panel of serum tumor markers was assessed. This analysis revealed striking elevations in gastrointestinal-associated markers, notably carbohydrate antigen 19-9 (CA 19-9, 4421.0 U/mL; reference range: 0.0–39.0 U/mL) and carcinoembryonic antigen (CEA, 236.0 ng/mL; reference range: 0.0–5.0 ng/mL). Mild to moderate elevations were also observed in neuron-specific enolase (NSE, 27.0 ng/mL; reference range: 0.0–16.3 ng/mL), alpha-fetoprotein (AFP, 21.5 ng/mL; reference range: 0.0–7.0 ng/mL), AFP-L3% (27.1%; reference range: 0.0–10.0%), carbohydrate antigen 72-4 (CA 72-4, 57.6 U/mL; reference range: 0.0–6.9 U/mL), and alkaline phosphatase (ALP, 130.0 U/L; reference range: 45.0–125.0 U/L). Following these findings, the patient underwent esophagogastroduodenoscopy and colonoscopy at an external medical institution, which revealed no pathological abnormalities.
A multidisciplinary team (MDT) involving specialists from medical oncology, radiology, orthopedics, and hepatobiliary surgery was convened to formulate a diagnostic and therapeutic strategy for the right renal tumor with synchronous bone metastases. In light of the massive tumor burden, the potential risks associated with percutaneous biopsy of the cystic-solid lesion, and the unremarkable gastrointestinal (GI) workup, the MDT recommended upfront surgical intervention to prevent local complications and provide the necessary tissue for a definitive diagnosis. On December 29, 2023, the patient underwent transperitoneal laparoscopic-assisted radical right nephrectomy. The resected specimen revealed an intact, sharply circumscribed, round-to-oval tumor mass measuring approximately 20 cm in greatest dimension (Figure 2(a)). The postoperative histopathological examination of the right renal tissue demonstrated infiltration by a moderately to poorly differentiated adenocarcinoma with necrosis (Figure 2(b) and (c)). Although other sites could not be excluded, morphological evaluation combined with IHC analysis supported a metastatic origin, most consistent with a gastrointestinal primary. The tumor exhibited strong positivity for GI lineage markers (CDX2 (+), Villin (+), CK20 (focal +), and SATB2 (partially +)), while remaining entirely negative for characteristic renal and urothelial markers (PAX8 (−), RCC (−), Vim (−), and CA9 (−)). Other notable markers included a high Ki-67 proliferation index (80%), P504S (+), CD10 (focal +), CK7 (−), S100P (−), and GATA3 (−) (see Figure 2(d)–(j) for representative stains).
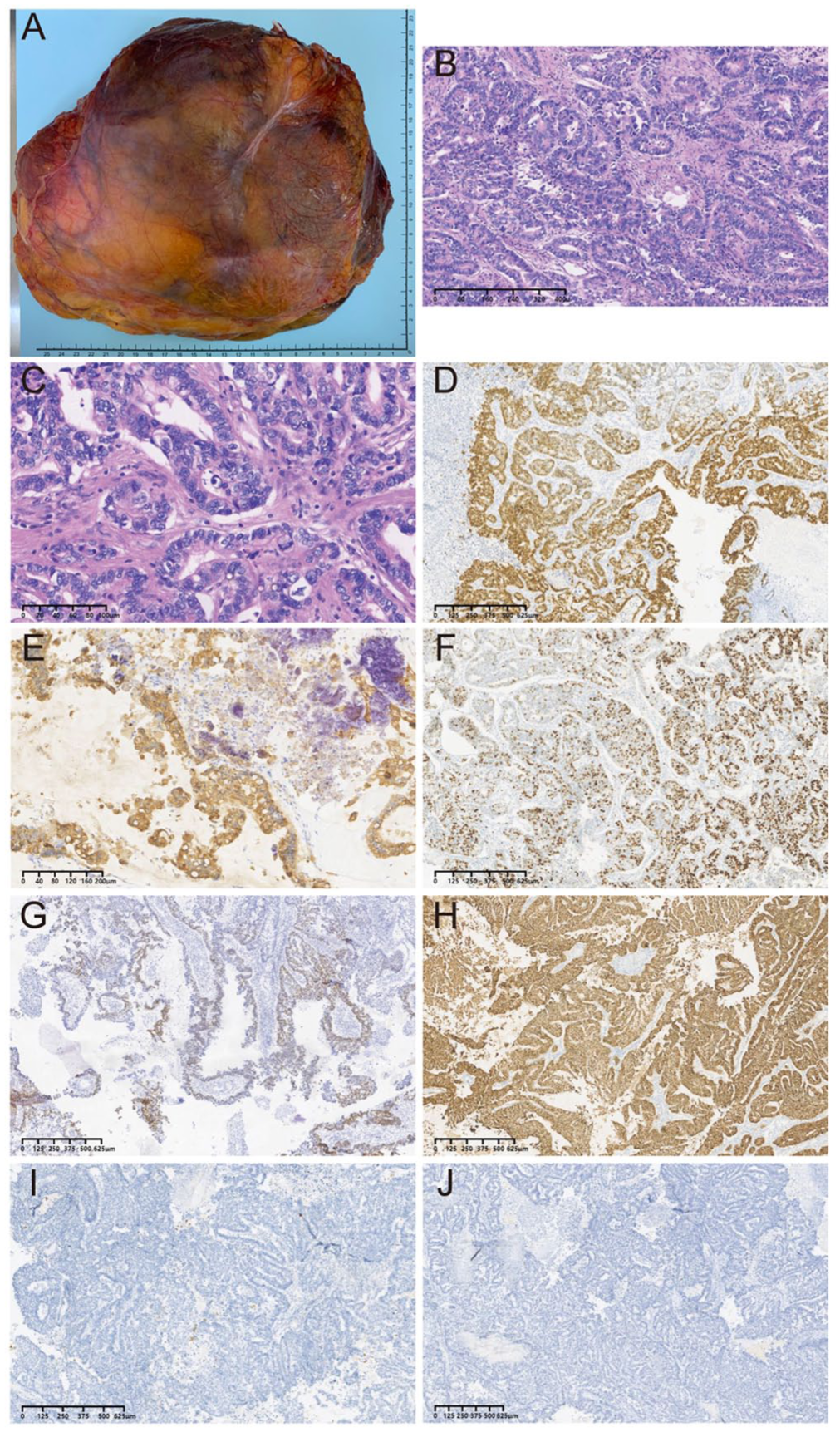
Histopathological features and immunohistochemical profile. (a) Gross photograph of the resected right kidney and the massive tumor (measuring 20 cm in its greatest dimension). Histological examination at low (b) and high (c) magnification reveals malignant epithelial cells with increased nuclear-to-cytoplasmic ratio, round-to-oval nuclei, and conspicuous nucleoli. Immunohistochemical staining of the renal tumor tissue for CDX2 (d), CK20 (e), Ki-67 (f), SATB2 (g), Villin (h), CA9 (i), and PAX8 (j).
To further investigate the primary tumor origin, a positron emission tomography-computed tomography (PET-CT) scan was performed 2 weeks after the operation. The scan revealed no abnormal fluorodeoxyglucose (FDG) avidity in the surgical bed (Figure 1(e)). In addition, non-FDG-avid small nodules were noted in the right lung (apical and posterior-basal segments), for which interval follow-up was recommended. Similarly, multiple foci of increased bone density in the ribs were noted, with no significant glucose metabolic abnormalities at the corresponding sites; however, based on other imaging examinations, bone metastasis was suspected. In February 2024, a follow-up endoscopic ultrasonography (EUS) was performed to reassess the previous findings, revealing chronic atrophic gastritis and a 3-mm gastric body polyp. To assess potential hereditary cancer predisposition, next-generation sequencing (NGS) analysis of a 474-gene pan-solid tumor panel (Illumina Nextseq550Dx platform) was performed in May 2024. However, the analysis yielded no informative clues. Despite a series of examinations, we were unable to locate the primary tumor site.
After a multidisciplinary evaluation, the patient received further systemic therapy in the department of medical oncology of our hospital. Four cycles of FLOT (fluorouracil, leucovorin, oxaliplatin, and docetaxel) chemotherapy regimen combined with camrelizumab, an anti-PD-1 immune checkpoint inhibitor, were administered from May to July 2024. Zoledronic acid was concurrently initiated to mitigate the risk of skeletal-related events. Throughout the therapeutic course, the patient underwent systematic follow-up assessments, including contrast-enhanced CT scans of the chest and abdomen, whole-body bone scintigraphy, and tumor marker tests. Contrast-enhanced abdominal CT revealed postoperative right nephrectomy status, with no evidence of recurrence or complications in the surgical bed or perinephric tissues. Most tumor marker levels normalized postoperatively, except for persistently mild elevations in CEA and CA 72-4 (Figure 3(a) and (b)). In November 2024, while the patient was being evaluated at another institution for lumbar spinal stenosis, disease progression was incidentally noted, presenting as enlarging pulmonary nodules and elevated CEA and CA 19-9 levels (Figure 3(b)). Prompted by this clinical progression and the need for actionable targets, retrospective molecular re-evaluation was performed on the archived primary renal tumor specimen. On December 3, 2024, tumor molecular profiling revealed ERBB2 copy number amplification by fluorescence in situ hybridization (FISH), with HER2 overexpression confirmed by IHC (3+). Based on these findings, the patient received targeted therapy with disitamab vedotin in December 2024 and January 2025. However, clinical progression continued despite this intervention, as re-examination at a local hospital revealed rising tumor markers. The patient subsequently continued supportive therapy at that institution, demonstrating significant systemic deterioration with massive ascites, which raised a high clinical suspicion of peritoneal metastasis. Late-stage clinical details were partially limited by inter-institutional care fragmentation, with the terminal trajectory reconstructed from available local summaries and familial reports. The complete chronological sequence of the patient’s clinical course, including all key diagnostic evaluations, therapeutic interventions, and clinical outcomes, is summarized in Figure 4.
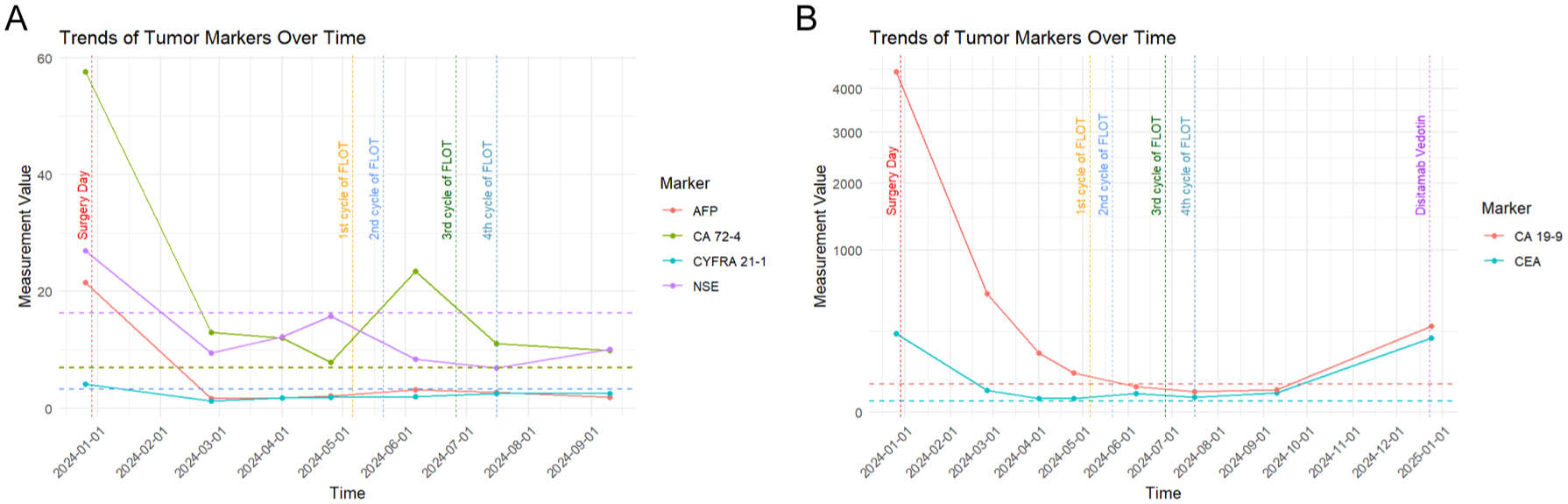
Serial serum tumor marker dynamics during the clinical course. (a) Trends of AFP, CA72-4, CYFRA21-1, and NSE levels over time (months). (b) Trends of CEA and CA19-9 levels over time (months).

Clinical timeline of the patient.
Discussion
The clinical management of this case was initially complicated by the tumor’s radiological presentation, which closely mimicked primary renal cell carcinoma. In the context of suspected metastatic disease, percutaneous core biopsy is the recommended standard of care to establish a histological diagnosis prior to surgical intervention. We acknowledge that our decision to proceed directly with upfront cytoreductive nephrectomy (CN) may deviate from current guidelines; furthermore, considering that upfront CN remains controversial in the targeted therapy era, this constitutes a notable limitation in our clinical management.9,10 This non-standard approach was carefully deliberated by our MDT based on the patient’s specific clinical circumstances. Primarily, the negative GI workup increased the clinical probability of a primary renal tumor. Furthermore, the massive size (>15 cm) and heterogeneous cystic-solid architecture of the lesion precluded percutaneous biopsy due to potential hemorrhage, a non-negligible risk of needle tract seeding, and a high risk of sampling error—notably, such complex masses carry a non-diagnostic rate of up to 40% secondary to low cellularity.11,12 Supported by the patient’s good performance status (Karnofsky Performance Status score > 80), CN was deemed necessary to prevent impending local complications, such as rupture, and to obtain a definitive histological diagnosis. In retrospect, while the initial clinical assessment pointed toward primary RCC, the aggressive surgical strategy served as the critical diagnostic step to unmask the occult metastasis. However, we emphasize that this upfront surgery was an individualized necessity driven by extreme local tumor characteristics. As a specific deviation from standard clinical practice, it should not be generalized as a routine pathway for suspected renal metastases.
This case profoundly illustrates the diagnostic conundrum inherent to CUP—a clinical entity typically diagnosed only after systemic metastasis, where comprehensive investigations fail to localize the primary tumor. Biologically, CUP is distinguished by a uniquely aggressive profile, exhibiting an exceptionally high mutational burden and active angiogenesis driven by factors mediating neovascularization (e.g., vascular endothelial growth factor (VEGF)) and matrix degradation (e.g., matrix metalloproteinases (MMPs)).13,14 This genetically complex phenotype often drives rapid, atypical dissemination that clinically mimics other primary malignancies. Specifically, secondary renal malignancy is a rare manifestation whose diagnostic obscurity primarily stems from a predominantly subclinical course.3,15 Although renal metastases typically present as bilateral, multifocal small lesions, they can also manifest as large, unilateral, solitary masses depending on the primary tumor characteristics.3–6 Given that the molecular features of our case strongly suggested a gastrointestinal lineage, this atypical presentation is further supported by our review of 28 previously reported cases of renal metastases of gastrointestinal origin (Table 1). This review reveals a primary tendency for unilateral renal involvement (26/28 cases) and a strong male predominance. Most of these patients, similar to our case, demonstrated synchronous extrarenal disease.
Summary of reported cases of renal metastases originating from primary gastrointestinal malignancies.

Data sources for each entry are indicated in the “Case” column. Refs 16–41 are cited only in this table.
HCC, hepatocellular carcinoma; OS, overall survival; SCC, squamous cell carcinoma; TAE, transcatheter arterial embolization.
In our patient, the concurrent metastatic involvement of the lung and bone—which represent the most frequent metastatic sites for primary RCC (70.9% and 30.7%, respectively)—created a striking clinico-radiological overlap. 42 Exclusive reliance on these conventional clinical parameters, coupled with the large, solitary nature of the renal mass, predictably led to the presumptive, albeit incorrect, diagnosis of primary RCC.
Although initially approached as a suspected primary renal malignancy, our diagnostic trajectory reflects the diagnostic principles outlined in the 2023 ESMO Clinical Practice Guideline for CUP. Phase I (Initial Clinical Work-up) involved standard clinico-radiological and endoscopic evaluations. Because the massive renal lesion radiographically mimicked primary RCC, phase II (Pathological Adjudication) commenced with upfront cytoreductive nephrectomy to mitigate hemorrhage risk, a decision consistent with recommended algorithms for suspected renal lesions. On the resected tissue, differentiating this morphologically ambiguous mass from an occult metastasis required a stepwise IHC approach. Initial clinico-radiological differentials included clear cell RCC (ccRCC), papillary RCC (pRCC), and urothelial carcinoma. However, tumor negativity for PAX8, CA9, Vimentin, and GATA3 excluded these urological primaries. Although the tumor expressed P504S—a marker common in pRCC and prostate adenocarcinoma—concurrent negative PAX8/CK7 staining and normal clinical prostate parameters ruled out these etiologies. The diagnosis of a gastrointestinal (GI) lineage CUP was definitively confirmed by the expression of enteric markers (CDX2, Villin, focal CK20, and partial SATB2). Following this pathological confirmation, we proceeded to phase III (Comprehensive Genomic Profiling). An initial 474-gene NGS panel yielded no actionable targets. However, repeat profiling upon disease progression using the same archived nephrectomy specimen revealed ERBB2 amplification (confirmed by FISH, with corresponding HER2 overexpression by IHC 3+), an established actionable alteration in this setting. The delayed identification of ERBB2, alongside the absence of canonical GI variants (e.g., KRAS/BRAF), demonstrates the spatial heterogeneity of CUP. This discrepancy highlights a known technical limitation: targeted NGS relies on read-depth algorithms, rendering it susceptible to false-negative copy number results when sample tumor purity is compromised by extensive necrosis. 43 By contrast, FISH provides direct single-cell in situ evaluation, effectively bypassing these dilution effects. 44 This objective finding provided the precise rationale for subsequent targeted therapy with disitamab vedotin and supports the clinical utility of complementary molecular testing methodologies when initial broad-panel NGS is unrevealing.
Conclusion
This report presents a challenging diagnostic and therapeutic scenario in the management of CUP. From a diagnostic perspective, in patients presenting with a solitary renal mass and extrarenal metastases, the renal lesion should be considered a potential metastatic site. Although primary renal cancer is more prevalent, the renal parenchyma can be a “silent target” for metastasis, especially with multisystemic involvement or non-renal differentiation suggested by IHC. Therapeutically, this case illustrates the utility and inherent limitations of a biomarker-guided precision strategy in CUP. Although molecular profiling identified an actionable ERBB2 amplification, the subsequent clinical response was limited and transient. This suggests that identifying molecular targets may not consistently yield durable efficacy, as the aggressive biology and spatial heterogeneity of CUP can significantly attenuate the benefits of precision interventions. Simultaneously, the persistence of latent metastatic foci continues to pose a substantial progression risk, compromising long-term survival and warranting further investigations into resistance mechanisms and novel multi-modal strategies.
Supplemental Material
sj-pdf-1-tau-10.1177_17562872261458108 – Supplemental material for Renal metastasis of adenocarcinoma of the gastrointestinal tract with unknown primary site: a case report and review of the literature
Supplemental material, sj-pdf-1-tau-10.1177_17562872261458108 for Renal metastasis of adenocarcinoma of the gastrointestinal tract with unknown primary site: a case report and review of the literature by Jiacheng Li, Xiaoyuan Ren, Zhiyuan Wang, Yanxin Zhuang, Yelinaer Baoerbieke, Yishuai Zhang and Jin Zeng in Therapeutic Advances in Urology
Footnotes
Acknowledgements
We sincerely thank Dr. Ting Liang from the Department of Radiology at the First Affiliated Hospital of Xi’an Jiaotong University for his assistance in providing and interpreting the imaging data for this study. We also extend our gratitude to Dr. Hua Liang from the Department of Pathology at the First Affiliated Hospital of Xi’an Jiaotong University for conducting the pathological review.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.