
Abstract
Background:
Triplet therapy with androgen deprivation therapy (ADT), docetaxel, and androgen receptor pathway inhibitors (ARPIs), either darolutamide or abiraterone, is one of the standard treatments for metastatic hormone-sensitive prostate cancer (mHSPC); however, no randomized trial has directly compared both ARPIs within this regimen. Given practical and financial constraints, a head-to-head randomized trial directly comparing these ARPIs may be unlikely.
Objective:
To compare the real-world effectiveness of darolutamide- versus abiraterone-based triplet therapy in patients with mHSPC.
Design:
Retrospective cohort study using a multinational electronic health record network.
Methods:
We conducted a retrospective cohort study using the TriNetX research network. Patients with mHSPC treated with darolutamide- or abiraterone-based triplet therapy were identified and balanced using propensity-score matching. The primary outcome was overall survival (OS), and the secondary outcome was time to next treatment (TTNT), defined by treatment switch. Prespecified subgroup analyses focused on age, cardiometabolic comorbidities, and polypharmacy-related medication use.
Results:
Among 1607 eligible patients, 1252 were included after propensity score matching (626 per group). Darolutamide-based triplet therapy was associated with longer OS compared with abiraterone (hazard ratio (HR) 0.42). A favorable difference in TTNT was also observed (HR 0.66). These associations were consistent across clinically relevant subgroups, including patients aged ⩾65 years and those with ischemic heart disease or diabetes mellitus. In polypharmacy-enriched subgroups, darolutamide-based therapy was consistently associated with more favorable OS and TTNT.
Conclusion:
In this large real-world analysis, darolutamide-based triplet therapy was associated with longer OS and TTNT compared with abiraterone-based triplet therapy in patients with mHSPC, particularly among older individuals and those with comorbidities. These findings are hypothesis-generating, suggesting that ARPI selection within triplet therapy may have clinically relevant implications, supporting the need for prospective studies.
Plain language summary
Advanced prostate cancer is often treated with a combination of three drugs: hormone therapy, chemotherapy, and a hormone-blocking medicine. Two commonly used hormone-blocking drugs are darolutamide and abiraterone. Although both are recommended treatments, no clinical trial has directly compared these two options when used together with chemotherapy. In this study, we used a large international health database to compare these two treatment approaches in real-world clinical practice. We included over 1,200 patients and used statistical methods to make the two groups as similar as possible. We found that patients treated with darolutamide lived longer and had a longer time before needing another treatment compared with those treated with abiraterone. These benefits were also seen in older patients and in those with other medical conditions, such as heart disease or diabetes. However, because this was not a randomized clinical trial, other factors that we could not fully measure may have influenced the results. In addition, the follow-up period was relatively short. Overall, our findings suggest that darolutamide may be a more effective option than abiraterone when used as part of three-drug therapy for advanced prostate cancer. Further studies are needed to confirm these results.
Keywords
Introduction
Prostate cancer (PC) remains the second most prevalent malignancy in men worldwide, with 1,466,680 new cases, as well as 396,792 deaths in 2022. 1 An estimated 1.5 million new male patients are diagnosed with PC globally each year; approximately 10% of them present with metastatic disease, harboring a 5-year survival rate of 37%. Within the last decade, the treatment landscape of metastatic prostate cancer (mPC) has evolved rapidly, 2 and androgen deprivation therapy (ADT) alone cannot prolong patients’ life span as long as treatment intensification strategy for metastatic hormone-sensitive prostate cancer (mHSPC). In addition to ADT, androgen receptor pathway inhibitors (ARPIs) become another backbone of mPC management. Undeniably upfront chemohormonal therapy with docetaxel changed the treatment paradigm for metastatic stage, especially in high-volume disease, 3 doublet combination with ADT and ARPIs has been recognized as the standard and optimal treatment of mPC, improving patient survivals and additional patient-relevant end points, regardless of disease burden. 4
In 2021, Fizazi et al. 5 reported at the European Society for Medical Oncology (ESMO) congress that adding abiraterone to docetaxel and ADT significantly improved radiographic progression-free survival in men with de novo mPC, providing an absolute median benefit of approximately 2.5 years, without introducing additional clinically significant short-term toxicity. The Prostate Cancer Consortium in Europe-1 (PEACE-1) trial ushered in a new era of intensification with triplet therapy in mHSPC, demonstrating an 18% overall survival (OS) benefit, with a medical follow-up of 4.4 years. Later, based on the American Society of Clinical Oncology (ASCO)Genitourinary Cancers Symposium 2022 presentation of the ARASENS trial, 6 the Food and Drug Administration approved darolutamide use in combination with docetaxel for patients with mHSPC. The new triplet regimen reduced the risk of death by 32.5% and showed consistent advantages in secondary endpoints and similar safety compared with ADT plus docetaxel alone. As evidence continues to accumulate,7 –12 triplet systemic therapy has been shown to confer substantial OS advantages in mHSPC patients.
The triplet combination therapies are composed of ADT with docetaxel and ARPI, either darolutamide or abiraterone. A variety of network meta-analyses have reported that triplet therapy prolonged longer survival in patients with mHSPC compared with standard doublet regimens, especially in high-volume disease.8,9,13 –15 Irrefutably, contradictory results16 –18 were also presented to suggest an equipoise on how triplet combinations compare with ARPI doublet regimens. A trend has been observed that intensified triplet therapy with darolutamide provided more pronounced OS survival benefits in mHSPC patients with visceral disease 19 and even older ages. 20 Despite these advances, no head-to-head randomized controlled trials (RCTs) currently compare darolutamide directly against abiraterone within a triplet regimen. This leaves an unmet evidence need regarding the optimal choice of ARPI.
In addition, patients with mHSPC were frequently older and poly-medicated due to age-related comorbidities. In this context, the pharmacological profiles of ARPIs might become one decisive factor. Specifically, abiraterone acetate is a moderate inhibitor of the CYP2D6 isozyme and requires concomitant prednisone, whereas darolutamide shows a lower potential for drug–drug interactions (DDIs) and does not require corticosteroid co-administration. 21 These differences in DDI profiles and toxicity may influence real-world outcomes outside of the strictly controlled environment of clinical trials. To bridge the evidence gap, we utilized aggregated and anonymized patient data from the TriNetX Global Collaborative Network to perform a large-scale retrospective study. We aimed to explore which ARPI—darolutamide or abiraterone—could offer superior real-world effectiveness when incorporated into a triplet regimen for treating mHSPC.
Materials and methods
Data source
We obtained data from the TriNetX Global Collaborative Network, a federated research platform comprising de-identified longitudinal electronic health records from 165 health care organizations across six continents. The network provides harmonized data on demographics, diagnoses International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), procedures Current Procedural Terminology (CPT), prescriptions (RxNorm), and laboratory measurements Logical Observation Identifiers Names and Codes (LOINC). All data were fully de-identified in compliance with the Health Insurance Portability and Accountability Act and applicable privacy regulations. Detailed coding definitions used for cohort identification, exposure ascertainment, exclusion criteria, and outcome definitions are provided in Supplemental Table 1.
Study design and population
We conducted a retrospective cohort study of men 18 years of age or older with a diagnosis of PC and evidence of metastatic disease, defined using ICD-10-CM codes for secondary malignant neoplasms (C77–C79), who had been treated with docetaxel and subsequently initiated darolutamide or abiraterone therapy between August 1, 2022, and December 31, 2024. To reflect real-world implementation of triplet therapy, receipt of docetaxel was required to occur within 3 months before or after the first prescription of darolutamide or abiraterone. Patients were assigned to the darolutamide cohort or the abiraterone cohort according to the first agent prescribed after the diagnosis of PC. The index date was defined as the date of the initial prescription of the assigned agent. Eligibility assessment, treatment initiation, and start of follow-up were aligned at the index date (time zero) to minimize immortal time bias.
To avoid treatment contamination and confounding from prior lines of therapy, patients were excluded if they had received the comparator ARPI within 5 years before or after the index date. Furthermore, patients with prior exposure to other advanced PC therapies—specifically enzalutamide, apalutamide, poly(ADP-ribose) polymerase (PARP) inhibitors, radium-223, or lutetium-177—before the index date were excluded. The alignment between the hypothetical target trial protocol and its observational emulation is summarized in Supplemental Table 2. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 22 The completed STROBE checklist has been provided as a Supplemental Table S3.
Propensity-score matching
We used propensity-score matching (PSM) to minimize confounding arising from differences in baseline characteristics between treatment groups. Propensity scores were estimated using logistic regression models that included age, race, body mass index (BMI), and relevant baseline coexisting conditions. Patients in the two cohorts were matched in a 1:1 ratio using greedy nearest-neighbor matching with a caliper width of 0.10 of the standard deviations of the logit of the propensity score. Standardized mean differences (SMD) were calculated to evaluate covariate balance after matching, with an SMD < 0.10 considered indicative of good balance.
Follow-up and outcomes
Follow-up began on the index date and continued until the earliest occurrence of an outcome event or December 1, 2025, whichever came first. The primary outcome was OS, defined by death records within the TriNetX system. The secondary outcome was time to next treatment (TTNT), a composite endpoint defined as the subsequent initiation of enzalutamide, apalutamide, PARP inhibitors, radium-223, or lutetium-177, representing a treatment switch because of disease progression. This definition had been used in prior real-world studies where radiographic outcomes were unavailable. The primary estimand of this study was the intention-to-treat (ITT) effect of initiating darolutamide-based versus abiraterone-based triplet therapy, defined as the effect associated with treatment initiation at time zero regardless of subsequent treatment modification or discontinuation. Patients were analyzed according to their initial ARPI assignment.
Subgroup analyses and effect heterogeneity
Prespecified subgroup analyses were conducted to explore potential effect heterogeneity across clinically relevant demographic, disease-related, and pharmacologic variables. Subgroups were defined at baseline (time zero) unless otherwise specified. Demographic subgroups included age (18–65 vs >65 years) and body mass index (BMI < 30 vs ⩾30 kg/m2). Comorbidity-related subgroups included hypertension, diabetes mellitus, hyperlipidemia, and ischemic heart disease, defined by ICD-10-CM codes. Additional sensitivity analyses were performed by stratifying patients based on metastatic sites (e.g., bone-only vs others) to evaluate the consistency of treatment effects across different disease distributions.
To explore potential DDI–related effects, additional subgroups were defined according to baseline exposure to selected concomitant medications with known CYP-mediated metabolism or cardiovascular relevance. Concomitant medication exposure was defined as an active prescription before the index date. These medications included β-blockers, statins, renin–angiotensin system inhibitors, selected antidepressants, opioids, antipsychotics, antiarrhythmics, and other agents with potential CYP2D6 or CYP3A4 involvement. Within each subgroup, treatment effects were estimated using Cox proportional-hazards models. Subgroup analyses were exploratory in nature, and no formal interaction testing was performed. Therefore, subgroup findings should be interpreted as hypothesis-generating.
Statistical analysis
Baseline characteristics were compared between the treatment cohorts before and after matching, and SMD were used to assess covariate balance. Cox proportional-hazards models were fitted to estimate hazard ratios (HRs) and 95% confidence intervals (CI). The proportional-hazards assumption was assessed using Schoenfeld residuals. Kaplan–Meier curves were generated to illustrate time-to-event outcomes, and survival distributions were compared using the log-rank test. Subgroup-specific hazard ratios were estimated using stratified Cox models as described above. All analyses were performed with the TriNetX Analytics Platform (accessed in December 2025).
Results
Patient characteristics
The initial search identified 1607 eligible patients; the darolutamide cohort consisted of 746 patients, and there were 861 patients in the abiraterone group. Owing to disparity in baseline characteristics, a 1:1 PSM was performed, and 1252 patients remained (626 per arm). The median follow-up was 590 days in the darolutamide cohort and 545 days in the abiraterone cohort. The matching process successfully balanced both cohorts (Table 1). The mean age was 66.7 ± 8.43 years for the abiraterone group and 67.0 ± 7.72 years for the darolutamide group. Racial distribution was similar, with approximately 64% White and 15%–16% Black or African American participants in both groups. Comorbidities such as hypertension, type 2 diabetes mellitus, and secondary malignancies were well-balanced with SMDs < 0.10. Baseline laboratory parameters, including prostate-specific antigen (PSA) levels, were assessed at index. In the propensity-score matched cohorts, the median PSA level was 33.6 ng/ml (IQR, 208) in the darolutamide group and 8.3 ng/ml (IQR, 72.1) in the abiraterone group. Although the darolutamide cohort showed a significantly higher median PSA, the distributions were highly skewed across both treatment arms, as evidenced by the wide interquartile ranges.
Baseline characteristics of patients receiving darolutamide- versus abiraterone-based triplet therapy before and after propensity-score matching.
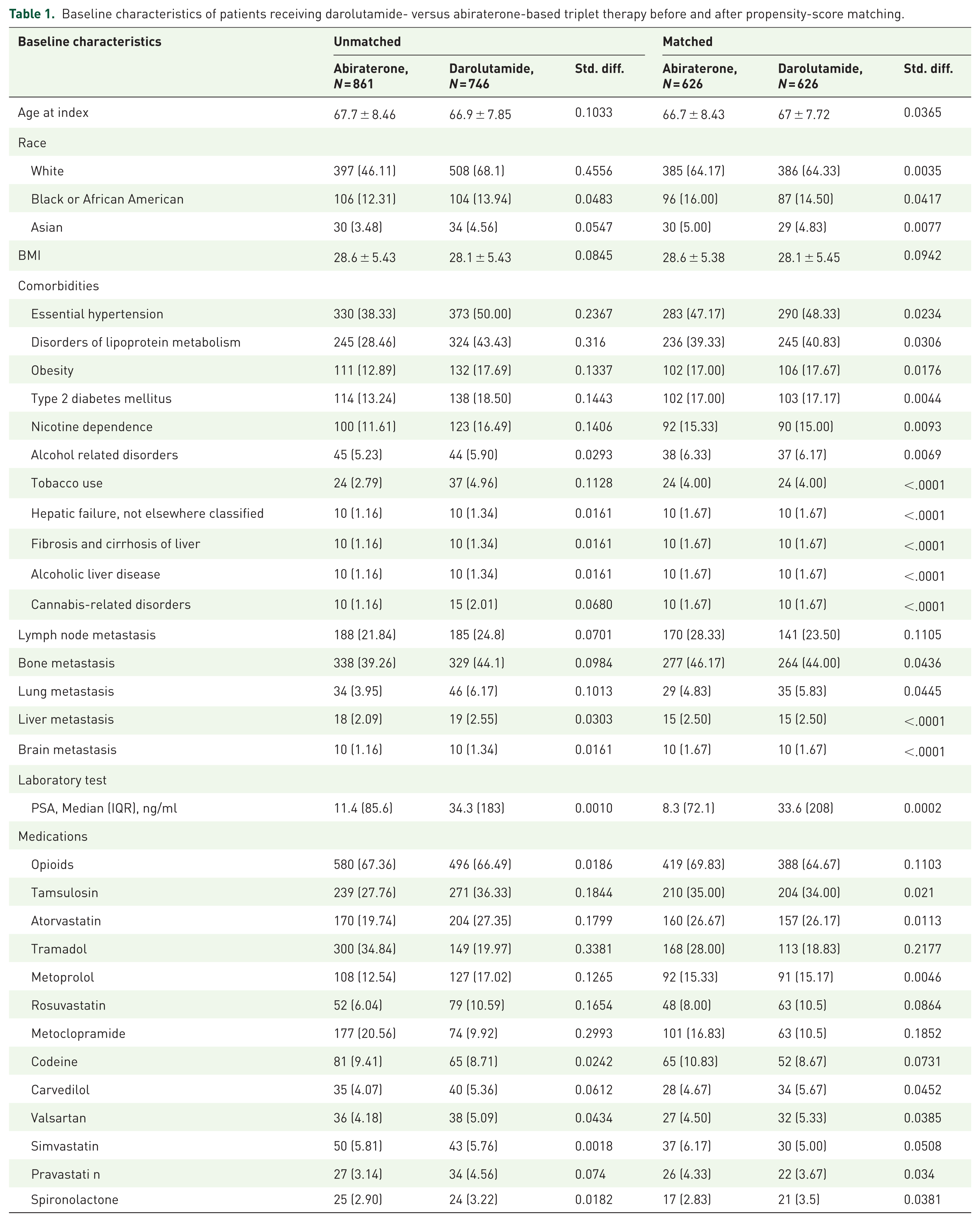

PSA, prostate-specific antigen.
Primary outcome: OS
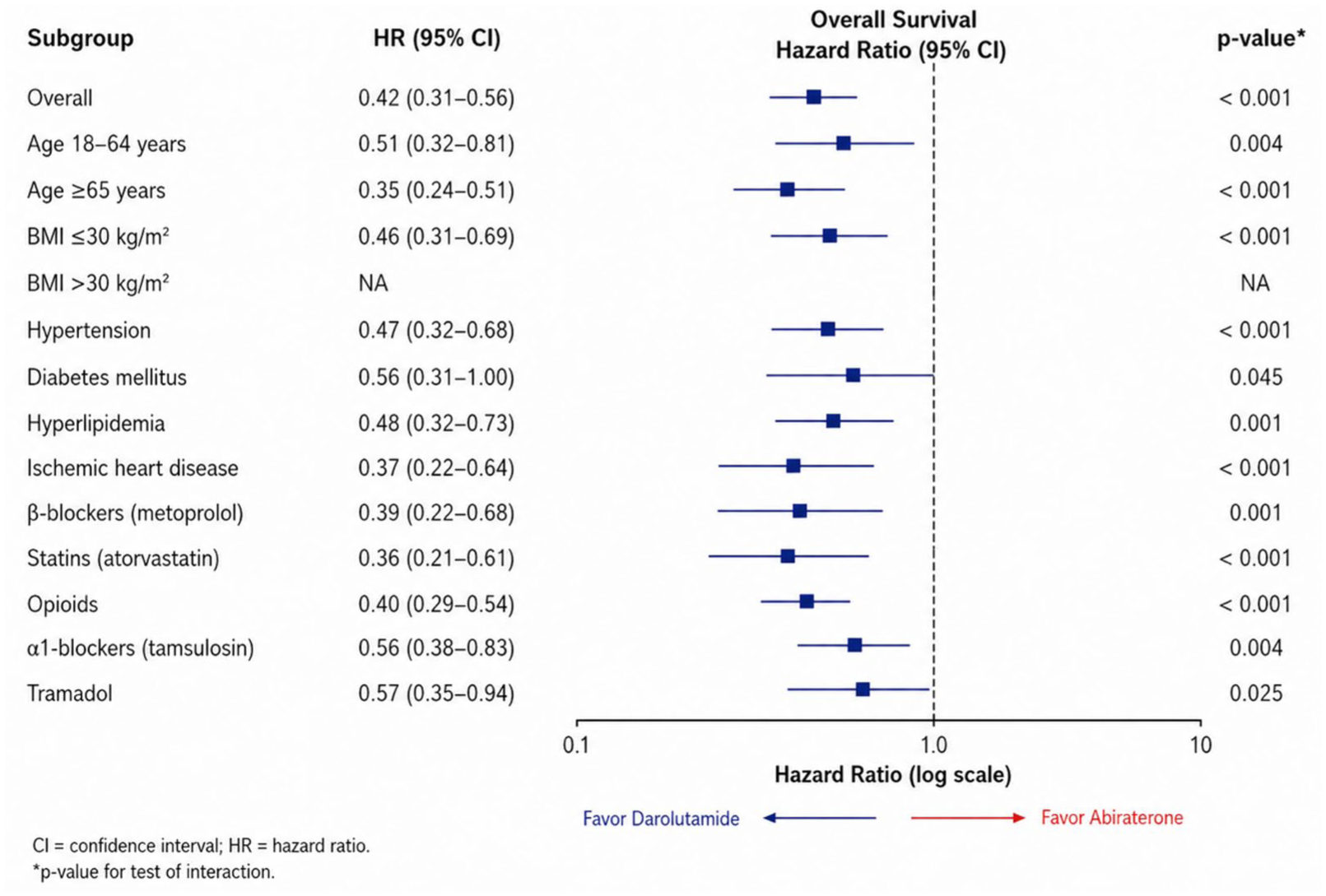
Darolutamide was associated with a significant improvement in OS compared to abiraterone. The HR for all-cause mortality was 0.42 (95% CI: 0.31–0.56; p < 0.0001). Kaplan–Meier survival estimates (Figure 1) showed a sustained divergence, with the darolutamide arm maintaining survival probabilities above 80% at 36 months, whereas the abiraterone arm dropped to approximately 65%. Subgroup analysis for survival (Figure 2) demonstrated consistent benefits for darolutamide, particularly in patients with the age of ⩾65 years (HR 0.35, 95% CI 0.24–0.51), ischemic heart disease (HR 0.37, 95% CI 0.22–0.64), and concomitant exposure to atorvastatin (HR 0.36, 95% CI 0.21–0.61) and opioids (HR 0.40, 95% CI 0.29–0.54). To further evaluate whether the survival benefit was influenced by disease volume, we performed sensitivity analyses stratified by metastatic patterns. Darolutamide-based triplet therapy demonstrated a consistent survival benefit in patients with bone-only metastasis (HR 0.473, 95% CI 0.304–0.738, p = 0.0007) and those with non-visceral metastasis (HR 0.431, 95% CI 0.321–0.577, p < 0.0001; Supplemental Table S4). Analysis for other subgroups, such as multiple organ involvement, was limited by small sample sizes (Supplemental Table S5).
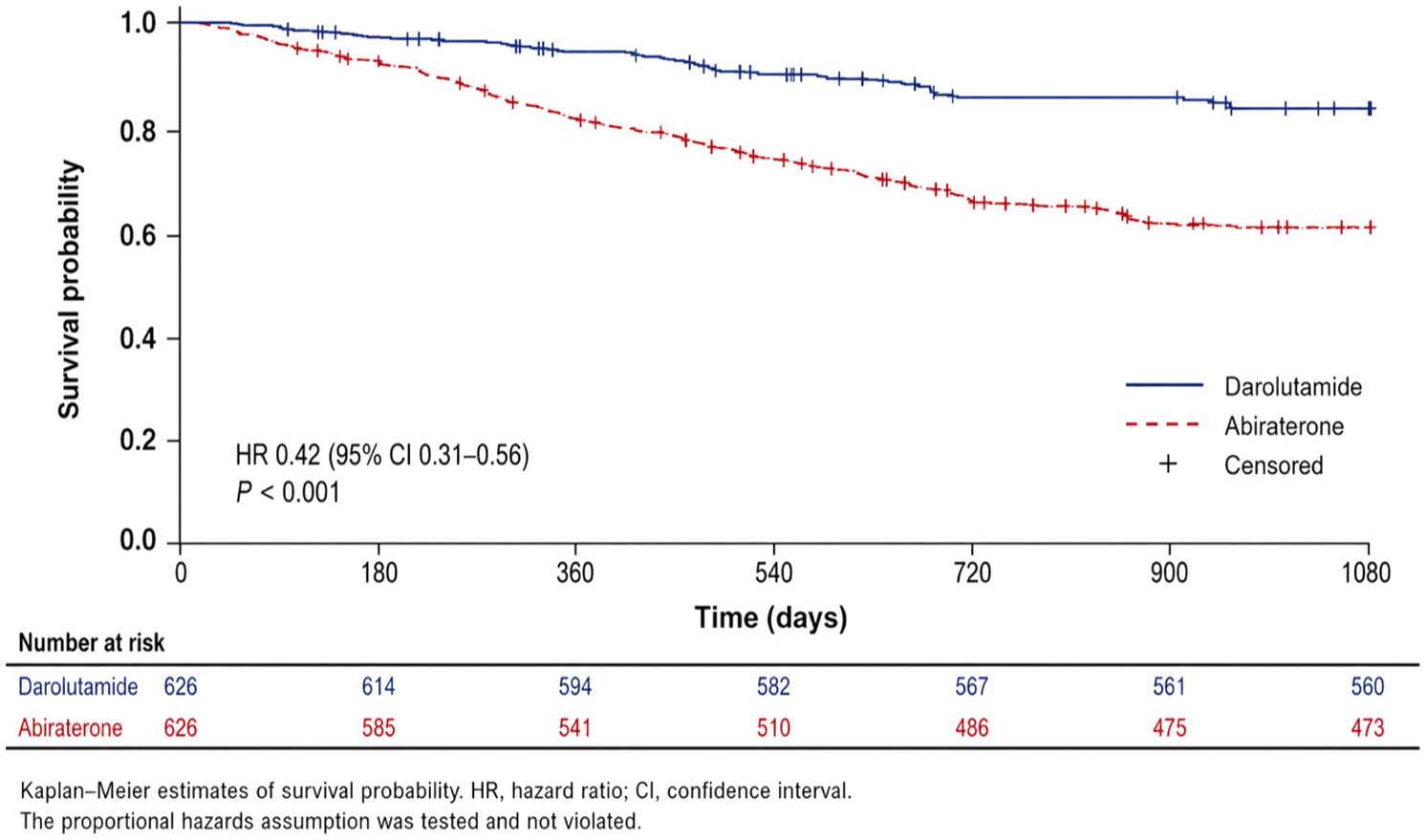
Kaplan–Meier estimates of overall survival in patients receiving darolutamide- versus abiraterone-based triplet therapy.
Subgroup analyses for overall survival comparing darolutamide- versus abiraterone-based triplet therapy.
Secondary outcome: TTNT
The darolutamide cohort demonstrated a statistically significant improvement in time to next treatment compared with the abiraterone cohort (HR, 0.66, 95% CI, 0.48–0.91; p = 0.010). The Kaplan–Meier curves began to separate approximately 6 months after treatment initiation, with the abiraterone group exhibiting a higher cumulative probability of progression-related events, defined as switch to next-line therapy, over the 36-month follow-up period (Figure 2). Subgroup analysis of the secondary endpoint (Figure 3) favored darolutamide across most strata. Notable statistically significant benefits for darolutamide in preventing treatment switch were seen in patients with diabetes mellitus (HR 0.42, 95% CI 0.20–0.88), as well as concomitant exposure to metoprolol (HR 0.38, 95% CI 0.18–0.80) and tamsulosin (HR 0.51, 95% CI 0.32–0.82; Figure 4).
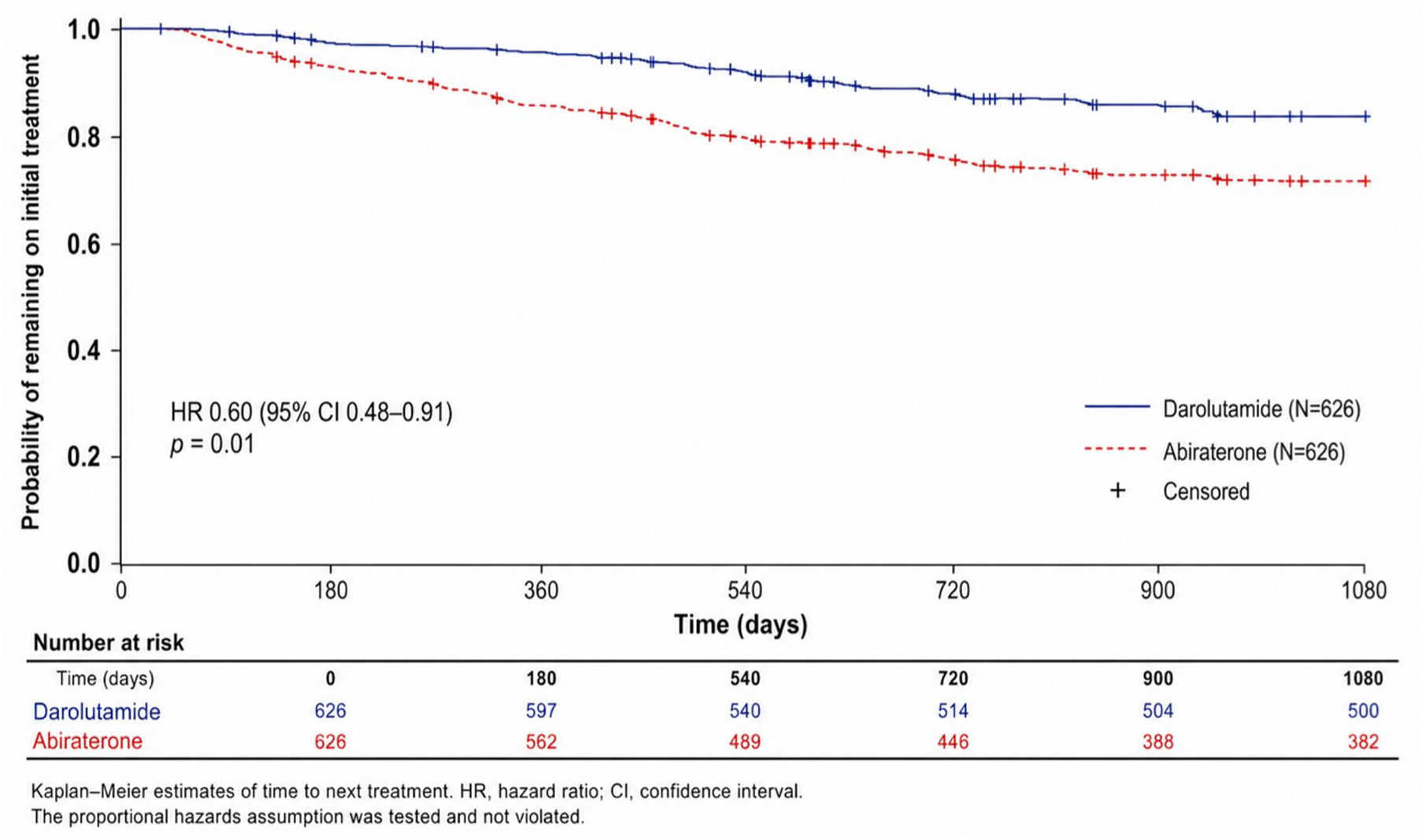
Kaplan–Meier estimates of time to next treatment in patients receiving darolutamide- versus abiraterone-based triplet therapy.
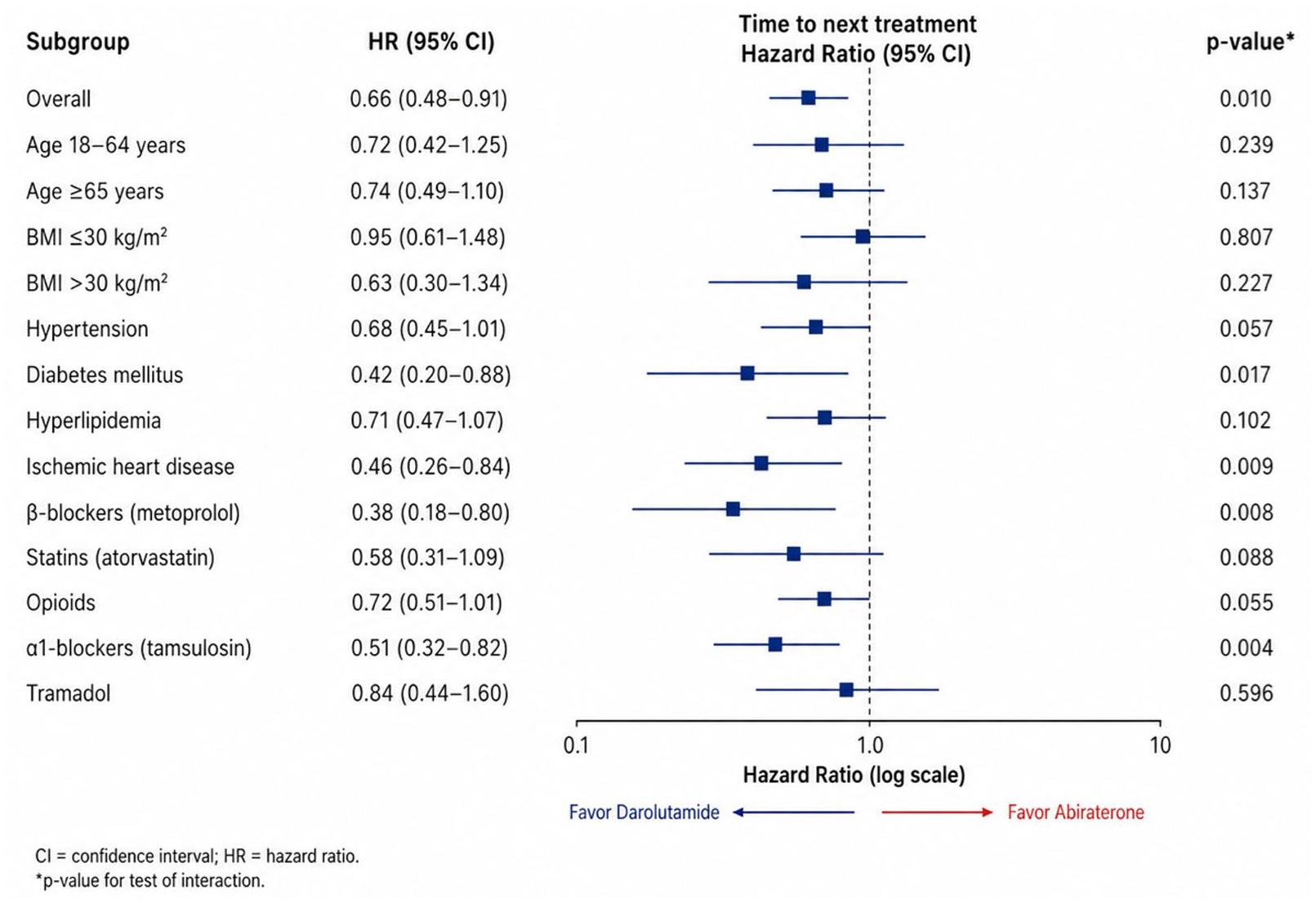
Subgroup analyses for time to next treatment comparing darolutamide- versus abiraterone-based triplet therapy.
Discussion
To the best of our knowledge, this large-scale PSM real-world analysis represents an early effort to compare darolutamide and abiraterone within a triplet regimen for mHSPC. While RCTs such as PEACE-1 and ARASENS have established the benefit of treatment intensification with ARPIs, docetaxel, and ADT, none were designed to directly evaluate the relative outcomes associated with different ARPIs within a triplet strategy. This evidence gap persists despite the increasing adoption of intensified regimens in routine clinical practice. Our findings provide hypothesis-generating real-world evidence suggesting that outcomes associated with darolutamide- and abiraterone-based triplet therapy may differ, particularly among older patients and those with cardiometabolic comorbidities.
Our results are broadly consistent with and extend the growing body of literature supporting treatment intensification in mHSPC. Multiple network meta-analyses encompassing large patient populations across global randomized trials have consistently ranked triplet regimens among the most effective first-line therapeutic strategies for improving survival outcomes.7 –15,23,24 These analyses further suggest that the greatest OS and TTNT benefits are observed in patients with high-volume disease, supporting the biological rationale that early and sustained suppression of androgen signaling, combined with upfront cytotoxic therapy, may alter the disease trajectory of aggressive mPC. Within these comparative frameworks, darolutamide-based triplet regimens have frequently been ranked highly in indirect comparisons, with signals suggesting more favorable outcomes relative to other ARPI-based triplets.14,23 Notably, a recent systematic review focusing on patients with visceral metastases reported more favorable OS outcomes associated with darolutamide-based strategies in this high-risk subgroup. 19 Similar trends have also been described in older populations, suggesting that darolutamide may offer a more favorable therapeutic index in patients with increased vulnerability to treatment-related toxicity. 20
Emerging observational evidence beyond the triplet setting provides complementary context for our findings. A retrospective analysis from Sichuan Provincial People’s Hospital comparing darolutamide plus ADT with abiraterone plus ADT in a doublet setting reported longer time to metastatic castration-resistant PC, deeper PSA responses, and more favorable secondary outcomes associated with darolutamide, with comparable safety profiles. 25 In addition, McKay and colleagues evaluated real-world triplet therapy outcomes using the ConcertAI Patient360 database and reported higher PSA90 response rates, lower treatment discontinuation, reduced progression to metastatic castration-resistant disease, and longer OS among patients receiving darolutamide-based triplet therapy compared with abiraterone-based triplets. 26 In aggregate, these findings are directionally concordant with our results and indicate that outcomes may differ according to ARPI selection within similarly structured intensified regimens. Most notably, a recent study by Chu and colleagues in a real-world US veteran cohort further corroborates our findings; they reported that among patients receiving triplet therapy, darolutamide was associated with improved OS compared to abiraterone (HR 0.52, 95% CI 0.30–0.91). 27 The consistency between their observed survival benefit and our reported HR of 0.42—both favoring darolutamide in a triplet setting—reinforces the potential clinical superiority of this agent, particularly in patients with high-volume or synchronous disease presentation.
From a DDI perspective, subgroup analyses in our study offer additional clinical context for the observed outcome differences between darolutamide- and abiraterone-based triplet therapies. In polypharmacy-enriched subgroups—including patients receiving β-blockers (metoprolol), α1-blockers (tamsulosin), statins (atorvastatin), or opioids—darolutamide-based therapy showed directionally consistent associations with more favorable overall and progression-free survival compared with abiraterone-based therapy. These medications are commonly prescribed in older individuals with cardiovascular or metabolic comorbidities and may serve as pragmatic proxies for patient populations particularly vulnerable to clinically relevant DDIs.
These observations are biologically plausible in light of the distinct pharmacokinetic profiles of the two ARPIs. 21 Abiraterone acetate is a clinically relevant inhibitor of CYP2D6 and CYP2C8 and requires concomitant prednisone administration, factors that may increase the risk of adverse interactions and treatment intolerance in poly-medicated patients. In contrast, darolutamide demonstrates minimal CYP2D6 inhibition and does not require corticosteroid co-administration, which may reduce the likelihood of pharmacokinetic interactions that could compromise treatment adherence or exacerbate non–cancer-related morbidity. Undeniably, darolutamide is not entirely devoid of DDIs—its exposure may be influenced by strong CYP3A4 or P-glycoprotein modulators, and it may affect select transporter substrates such as BCRP and OATP1B1/1B3—these interactions are generally predictable and clinically manageable through dose adjustment or monitoring.
Cardiovascular and neurologic safety considerations provide additional context for these findings. In a network meta-analysis by Aziz et al., 28 abiraterone-based triplet therapy was associated with a higher risk of hypertension and arrhythmias compared with doublet therapy, whereas such increases were not observed with darolutamide-based triplet regimens. In our cohort, patients receiving β-blockers or statins showed directionally more favorable survival outcomes with darolutamide-based therapy, suggesting that treatment tolerability and cardiovascular safety profiles may be particularly relevant in individuals with pre-existing cardiovascular risk. Moreover, Matsukawa et al. reported that darolutamide was associated with fewer central nervous system adverse events, including cognitive impairment and falls, compared with other ARPIs, likely related to its limited blood–brain barrier penetration. 29 Preservation of functional status and reduced fall risk may be especially important in older patients and could partially explain the age-specific outcome patterns observed in our analyses.
Several limitations should be acknowledged. As with all real-world database analyses, residual confounding, heterogeneity in treatment delivery, and incomplete capture of performance status, metastatic burden, and physician decision-making cannot be fully excluded. A formal sample size calculation was not performed because of the retrospective nature of the study using an available global database; this should be considered a limitation. Furthermore, TTNT was defined based on treatment modification rather than radiographic progression, reflecting a commonly used but imperfect surrogate in real-world studies. In addition, death may act as a competing event for treatment escalation; however, formal competing risk modeling was not performed because of platform constraints. This may have led to overestimation of progression risk in the presence of early mortality. With a median follow-up of approximately 1.6 years, our OS data remains relatively immature for mHSPC. Given that median survival in this population often exceeds 5 years, longer-term follow-up is necessary to confirm the observed survival advantage. Detailed metastatic characteristics—such as de novo versus metachronous disease and high- versus low-volume status according to CHAARTED criteria—were unavailable. Although the lack of CHAARTED/LATITUDE criteria remains a limitation, our proxy-based sensitivity analyses demonstrated that the OS benefit of darolutamide was preserved in both bone-only and non-visceral subgroups. These findings mitigate the concern that the observed superiority of darolutamide was solely driven by an imbalance in patients with low-volume disease. Nevertheless, because of the limited number of patients with visceral or multi-organ involvement in our real-world cohort, we were unable to perform meaningful statistical comparisons for these high-burden strata, and further validation in larger cohorts is required.
Regarding baseline characteristics, the darolutamide group had a significantly higher median PSA level compared to the abiraterone group (33.6 vs 8.3 ng/ml). Although higher PSA levels are often associated with greater disease burden in mHSPC, the observed survival benefit of darolutamide remained consistent after propensity-score matching. However, residual confounding cannot be excluded. Importantly, this analysis does not replace the need for a prospective, adequately powered head-to-head randomized trial comparing darolutamide- and abiraterone-containing triplet regimens, which remains an essential next step.
Nevertheless, several strengths merit emphasis. Utilization of the TriNetX platform enabled the inclusion of a large, multinational, and clinically heterogeneous population that more closely reflects routine clinical practice than traditional randomized trials. The inclusion of older adults, patients with multiple comorbidities, and poly-medicated individuals—groups often underrepresented in clinical trials—enhances the external validity of our findings. The consistency of OS and TTNT findings across clinically relevant subgroups lends support to the robustness and generalizability of these results.
Conclusion
This real-world PSM analysis suggests that darolutamide-based triplet therapy may be associated with more favorable OS and TTNT compared with abiraterone-based triplet therapy in patients with mHSPC, particularly among older individuals and those with cardiometabolic comorbidities. Differences in pharmacologic properties, DDI burden, and tolerability profiles may contribute to the observed outcome differences. While prospective head-to-head trials are required to establish definitive comparative evidence, our findings provide timely, practice-relevant insights to inform ARPI selection in treatment intensification strategies for mHSPC.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261463076 – Supplemental material for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study
Supplemental material, sj-docx-1-tau-10.1177_17562872261463076 for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study by I-Hsuan Alan Chen, Ren-In Chang, Chia-Cheng Yu, Tzu-Ping Lin and Chih-Yu Yang in Therapeutic Advances in Urology
Supplemental Material
sj-docx-2-tau-10.1177_17562872261463076 – Supplemental material for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study
Supplemental material, sj-docx-2-tau-10.1177_17562872261463076 for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study by I-Hsuan Alan Chen, Ren-In Chang, Chia-Cheng Yu, Tzu-Ping Lin and Chih-Yu Yang in Therapeutic Advances in Urology
Supplemental Material
sj-docx-3-tau-10.1177_17562872261463076 – Supplemental material for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study
Supplemental material, sj-docx-3-tau-10.1177_17562872261463076 for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study by I-Hsuan Alan Chen, Ren-In Chang, Chia-Cheng Yu, Tzu-Ping Lin and Chih-Yu Yang in Therapeutic Advances in Urology
Supplemental Material
sj-docx-4-tau-10.1177_17562872261463076 – Supplemental material for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study
Supplemental material, sj-docx-4-tau-10.1177_17562872261463076 for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study by I-Hsuan Alan Chen, Ren-In Chang, Chia-Cheng Yu, Tzu-Ping Lin and Chih-Yu Yang in Therapeutic Advances in Urology
Supplemental Material
sj-docx-5-tau-10.1177_17562872261463076 – Supplemental material for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study
Supplemental material, sj-docx-5-tau-10.1177_17562872261463076 for Real-world comparative outcomes of darolutamide- versus abiraterone-based triplet therapy for metastatic hormone-sensitive prostate cancer: a retrospective cohort study by I-Hsuan Alan Chen, Ren-In Chang, Chia-Cheng Yu, Tzu-Ping Lin and Chih-Yu Yang in Therapeutic Advances in Urology
Footnotes
Acknowledgements
The authors would like to thank Dr. Chang-Bi Wang for his assistance with access to the TriNetX data and support in statistical analyses for this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.