
Abstract
Aims:
A major component of the National Health Service (NHS) Health Check in England is to provide lifestyle advice to eligible participants. The aims of the study were to explore the variations (in terms of uptake) in the NHS Health Check in Leicester and to determine its association with a healthy lifestyle.
Methods:
This cross-sectional study used data from the Leicester Health and Wellbeing Survey (2015).
Results:
The odds of having an NHS Health Check were found to be higher in Black and minority ethnic groups and in people of other religions. The odds were lower in people without a religion, residing in the fourth index of multiple deprivation quintile and in ex-smokers. No associations were found between having an NHS Health Check and describing a healthy lifestyle, following a healthy lifestyle, thinking of making lifestyle changes in the next 6 months, cutting down on/stopping smoking among current smokers, or amount of alcohol current drinkers would like to drink.
Conclusions:
In Leicester, a few variations in having an NHS Health Check were found among different socio-economic, demographic and behavioural groups. No association was found between the NHS Health Check and a healthy lifestyle. Thus, the improvement work should focus on reducing these variations in having the NHS Health Check and bringing its benefits on promoting a healthy lifestyle.
Introduction
In 2009, the National Health Service (NHS) Health Check programme was introduced in England to reduce the risk of developing conditions like heart disease, stroke, diabetes and kidney disease. People are invited for a free NHS Health Check every 5 years. Its target population is people in the age group of 40–74 years – they are at a higher risk of developing one of these conditions. Generally, people younger than this age range have a much lower risk of developing these conditions and thus, it is not an effective way for the NHS to spend its resources on providing the NHS Health Check for younger people. Those with a pre-existing condition (such as coronary heart disease, heart failure, atrial fibrillation, stroke, transient ischaemic attack, diabetes, chronic kidney disease, peripheral arterial disease, hypertension, and hypercholesterolaemia) or those on prescribed statins are excluded. It is made up of three main components: risk assessment, risk awareness and risk management. During the risk assessment, standardised tests are used to measure the key risk factors (such as age, gender, ethnicity, family history of these conditions, body mass index (BMI), waist circumference, smoking, alcohol consumption, physical activity, blood pressure, cholesterol and blood glucose) and establish the individual’s risk of developing these conditions. The outcome of the risk assessment is then used to raise awareness of the risk factors and to inform a discussion on, and agreement of, the lifestyle and medical approaches best suited in managing the individual’s health risk. It is usually carried out at general practitioner (GP) practices, but depending on the local authority, it can also be carried out at other settings such as pharmacies or non-NHS settings. Where it is conducted outside the individual’s GP practice, the results and other relevant information are passed on to the individual’s GP. It is carried out by a healthcare professional (e.g. a doctor, nurse, healthcare assistant or pharmacist) and takes around 20–30 min. The Department of Health modelling showed its average annual cost as £332m/year at full rollout and the benefit as £3.7bn with around £3,000 cost/quality adjusted life year (QALY). It is cost-effective with potential savings by the NHS of around £57m/year after 4 years, rising to £176m/year after 15 years. Its cost-effectiveness is based on an assumed uptake of 75%. It could prevent 1,600 heart attacks and strokes, saving at least 650 lives/year. It could prevent over 4,000 people/year from developing diabetes and detect at least 20,000 cases of diabetes or kidney disease earlier, allowing individuals to be better managed and improve their quality of life. 1
The above-mentioned health gains will only be achieved if eligible participants attend it and are compliant with the advice provided. There has been an ongoing debate regarding its uptake and impact. Because of the potential benefits, many professionals are enthusiastic about it, whereas others have raised concerns about the inequality of its uptake and its evidence-base.2–9 It is important to continue evaluating the NHS Health Check to provide the evidence base for future policy direction. While randomised controlled trials (RCTs) are extremely vital, other forms of evidence can also provide a legitimate basis for action, particularly for such a complex intervention which has multiple interacting components and non-linear causal pathways. 10 It is also complex because it targets a wide range of people, and there are complexities in its organisation and implementation, which requires a degree of flexibility. 1
Leicester is the largest city in the East Midlands region of England. 11 It is one of the most ethnically and religiously diverse cities.12,13 In England, cardiovascular disease is more common in people of South Asian, African or Caribbean origin. 1 The city is one of the most disadvantaged urban areas in England, exhibiting some of the most complex health needs and biggest health inequalities.11,14 Out of the 326 local authorities in England, Leicester is ranked 21st most deprived in the index of multiple deprivation 2015 (which combines seven domains of deprivation – income, employment, education, skills and training, health and disability, crime, barriers to housing and services, and living environment). In other words, it is ranked within the 10% most deprived local authorities in England. In the case of health deprivation and disability domain, it is ranked 52. This domain measures the risk of premature death and the impairment of quality of life through poor physical or mental health. It also measures morbidity, disability and premature mortality but not aspects of behaviour or environment that may be predictive of future health deprivation. In Leicester, 32 geographical areas (lower-layer super output areas) are experiencing high health and disability deprivation (i.e. within 10% most deprived nationally). 15 Some of the related health indicators are significantly worse in the city than the England average. For example, the life expectancy for men and women is 77 and 82 years, respectively; the under 75 mortality rate due to cardiovascular disease is 112 (rate per 100,000 population); the rate of alcohol-related harm hospital stays is 734 (rate per 100,000 population); and 60% of adults are physically active. 11
Leicester City Council is responsible for improving public health in Leicester. Public health services promote good lifestyle choices, help to prevent ill health and support people to live longer and healthier lives. Leicester City Council is working with Leicester City Clinical Commissioning Group to deliver the NHS Health Check. The NHS Health Check is available to eligible residents registered with a GP in Leicester City Council catchment area and is available at GP practices across this catchment area. 16 The study aims were to explore the variations (in terms of uptake) in the NHS Health Check in Leicester and to determine its association with a healthy lifestyle.
Methods
Study design and participants, and data source and collection procedure
This cross-sectional study used data from the Leicester Health and Wellbeing Survey (2015). The survey was commissioned by Leicester City Council (Public Health Division). The data were collected by an independent research agency, Ipsos MORI. Trained interviewers conducted face-to-face interviews with the participants using a quantitative questionnaire, under the Market Research Society Code of Conduct and the Data Protection Act, 1998. Most of the questions were asked by the interviewer and few were for self-completion. The survey was conducted from January to June 2015. A total of 2,321 residents, aged 16 and above, were interviewed in pre-assigned sample points across Leicester. Quotas were set by age, sex, ethnicity and work status to ensure demographic representativeness. The current study included those who were registered with a GP and were in the 40–74 years age range. 1
Study variables
The following variables were extracted from the survey dataset (please see supplemental material): age in years; sex; the index of multiple deprivation 2015 (5 quintiles with 1 and 5 representing the most and least deprived groups, respectively) 17 ; sexual orientation (heterosexual; lesbian, gay, bisexual and transgender (LGBT); and prefer not to say); ethnicity (White and Black and minority ethnic groups (BMEs)); religion (Christianity, other, no and don’t know/refused); English language skills – speaking, writing and reading (yes and no); smoker (never, ex-smoker and current smoker); alcohol drinker (never, ex-drinker, current drinker and prefer not to say/don’t know); describing a healthy lifestyle included a healthy diet (yes and no), regular exercise (yes and no), no smoking (yes and no) and not drinking too much alcohol (yes and no); following a healthy lifestyle included current diet – fruit and vegetables (⩾5 portions/day and <5 portions/day), 18 current physical activity – moderate intensity (⩾150 min/week and <150 min/week), 19 current smoking or tobacco usage (no and yes), current alcohol drinking (⩽14 units/week and >14 units/week), 20 and current BMI (normal (18.5–24.9 kg/m2), under (<18.5 kg/m2) and overweight/obese (⩾25 kg/m2)); 21 thinking of making lifestyle changes in the next 6 months included eat more healthily (yes and no), lose weight (yes and no), increase the amount of physical activity (yes and no), cut down or stop smoking (yes and no) and cut down the amount of alcohol (yes and no); cut down/stop smoking among current smokers (included smoking and other forms of tobacco usage) included trying to cut down or give up smoking completely (yes, no and don’t know), giving up smoking altogether (yes, no and don’t know) and ever tried to stop smoking (yes and no); amount of alcohol current drinkers would like to drink included like to drink alcohol (less than as at the moment, about the same as at the moment and more than as at the moment); and NHS Health Check (yes and no). Participants were asked, ‘Have you had an NHS Health Check from your GP practice?’
Ethics
The study was approved by the Research Ethics Committee, The University of Nottingham (UK).
Statistical analyses
For categorical variables, numbers and percentages were calculated. For normally distributed continuous variables, means and standard deviations (SD) were calculated. Simple logistic regression method was used to investigate the association between the NHS Health Check and other variables. The associations which were found significantly in simple logistic regressions were further adjusted for ‘a priori’ confounders (such as age, sex, the index of multiple deprivation, ethnicity or religion) in multiple logistic regression models. As the NHS Health Check is for people without a pre-existing condition, 1 sensitivity analyses were conducted by excluding those with any long-standing (over the last 12 months or the coming 12 months) illness, disability or infirmity. Odds ratios (OR)/coefficients and their respective 95% confidence intervals (CIs) were calculated. The results were considered significant when p values were ⩽.05. All data were analysed using Stata V.14 for Windows software.
Results
In all, 979 participants satisfied the inclusion criteria. 65% of them (n = 637) had an NHS Health Check. Table 1 shows the variations in having an NHS Health Check among different socio-economic, demographic and behavioural groups. There were no variations in having an NHS Health Check in terms of sex, sexual orientation and English language skills. The odds of having an NHS Health Check increased with age (coefficient 0.02, 95% CI: 0.01–0.03, p = .027). The odds were lower in people residing in the fourth index of multiple deprivation quintile (OR: 0.57, 95% CI: 0.35–0.93, p = .024), having no religion (OR: 0.66, 95% CI: 0.47–0.91, p = .013), in ex-smokers (OR: 0.60, 95% CI: 0.43–0.84, p = .003) and in current drinkers (OR: 0.70, 95% CI: 0.53–0.92, p = .011). The odds were higher in BMEs (OR: 1.66, 95% CI: 1.26–2.18, p < .001) and in people having other religions (OR: 1.54, 95% CI: 1.13–2.11, p = .007).
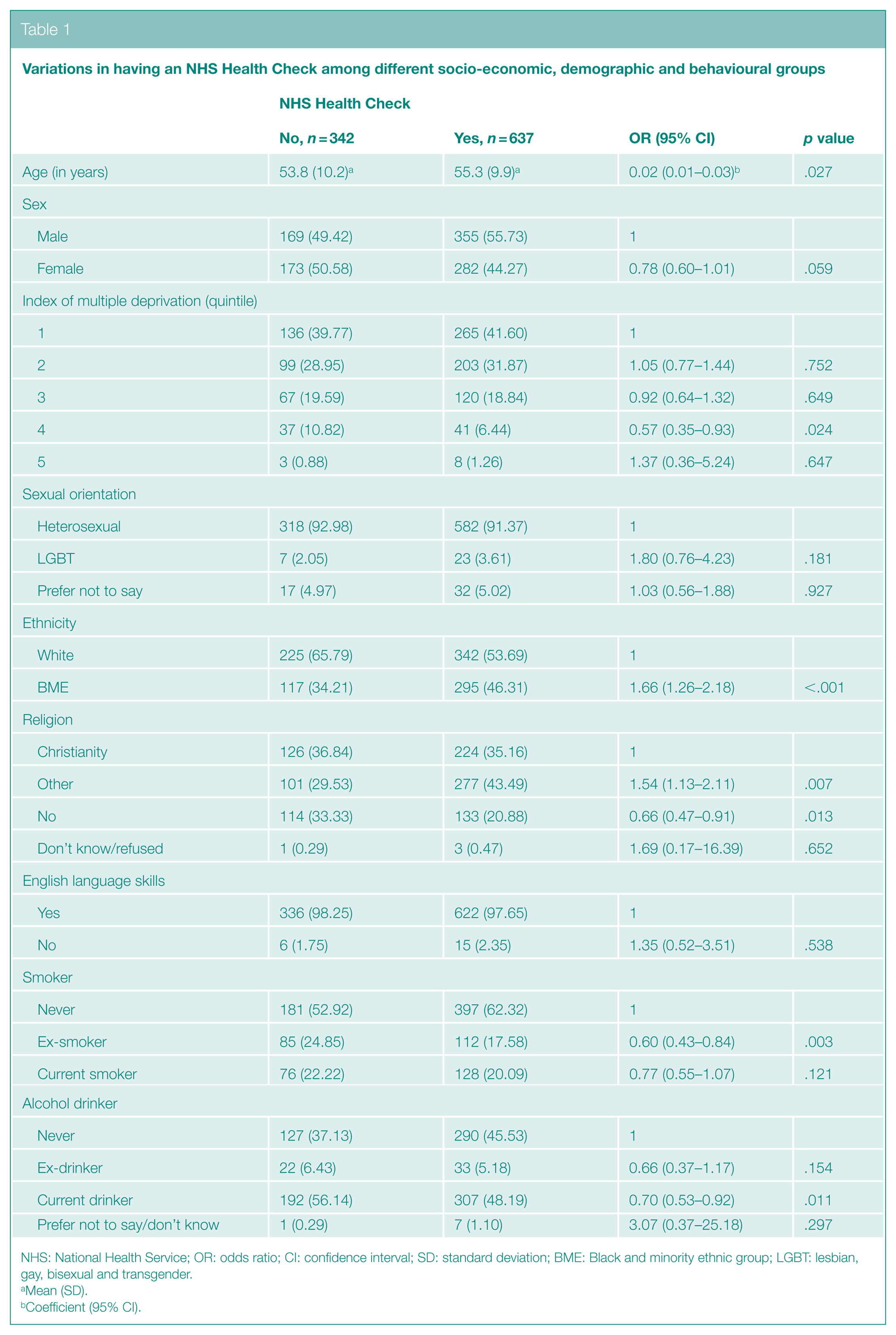
NHS: National Health Service; OR: odds ratio; CI: confidence interval; SD: standard deviation; BME: Black and minority ethnic group; LGBT: lesbian, gay, bisexual and transgender.
Mean (SD).
Coefficient (95% CI).
Table 2 reports any association between having an NHS Health Check and a healthy lifestyle. No associations were found between having an NHS Health Check and describing a healthy lifestyle, following a healthy lifestyle or thinking of making lifestyle changes in the next 6 months, except for eating more healthily. The odds of having an NHS Health Check were lower in people who were not thinking of eating more healthily in the next 6 months (OR: 0.72, 95% CI: 0.54–0.97, p=.028).
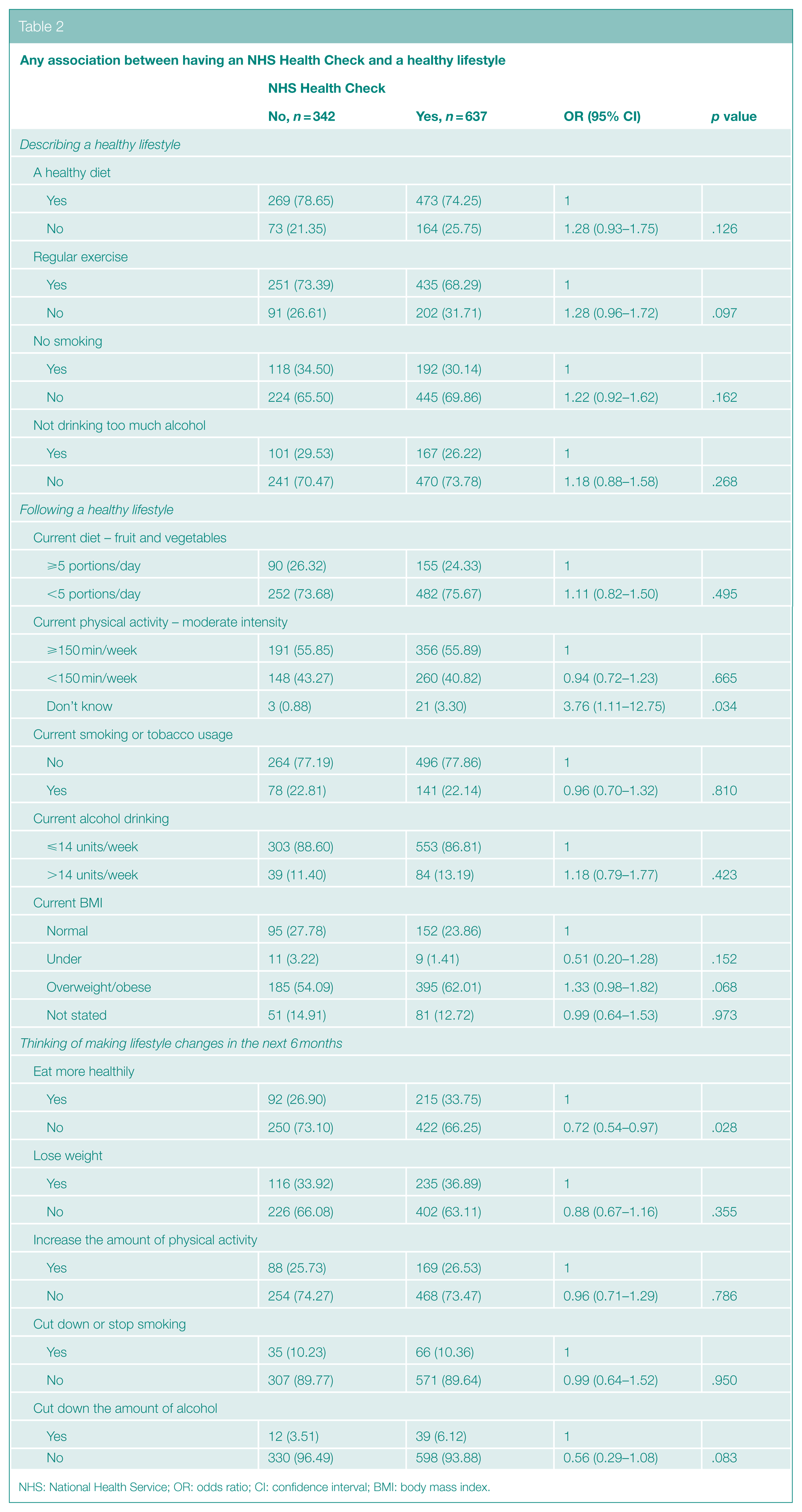
NHS: National Health Service; OR: odds ratio; CI: confidence interval; BMI: body mass index.
Table 3 shows any association between having an NHS Health Check and cut down/stop smoking among current smokers (n = 219) or amount of alcohol current drinkers (n = 499) would like to drink. No associations were found between having an NHS Health Check and cut down/stop smoking among current smokers or amount of alcohol current drinkers would like to drink.

NHS: National Health Service; OR: odds ratio; CI: confidence interval.
Table 4 reports the multiple logistic regression models, having adjusted for ‘a priori’ confounders. After adjustment for age, sex and the index of multiple deprivation, the odds of having an NHS Health Check were still higher in BMEs (OR: 1.74, 95% CI: 1.31–2.32, p < .001) and in people having other religions (OR: 1.61, 95% CI: 1.16–2.25, p=.005), and the odds were still lower in people having no religion (OR: 0.69, 95% CI: 0.49–0.98, p=.037). The odds were still lower in people residing in the fourth index of multiple deprivation quintile after adjustment for age, sex and ethnicity and age, sex and religion (OR: 0.55, 95% CI: 0.34–0.91, p=.019; and OR: 0.55, 95% CI: 0.33–0.90, p=.019, respectively). The odds were still lower in ex-smokers after adjustment for age, sex, the index of multiple deprivation and ethnicity (OR: 0.65, 95% CI: 0.45–0.92, p=.017) and age, sex, the index of multiple deprivation and religion (OR: 0.67, 95% CI: 0.47–0.97, p=.031). However, no variation was found in having an NHS Health Check among alcohol drinkers. No association was found between having an NHS Health Check and thinking of eating more healthily in the next 6 months.
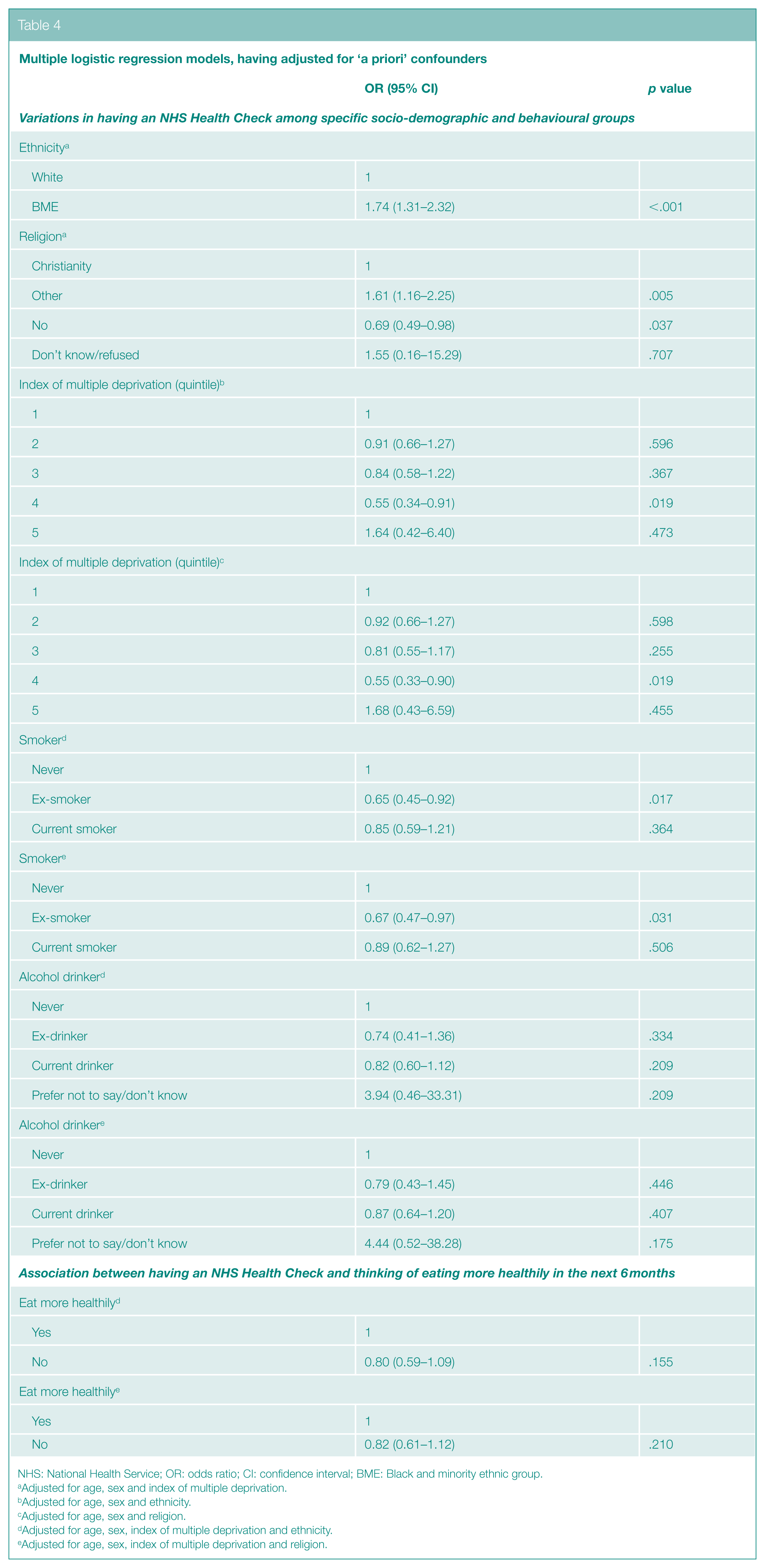
NHS: National Health Service; OR: odds ratio; CI: confidence interval; BME: Black and minority ethnic group.
Adjusted for age, sex and index of multiple deprivation.
Adjusted for age, sex and ethnicity.
Adjusted for age, sex and religion.
Adjusted for age, sex, index of multiple deprivation and ethnicity.
Adjusted for age, sex, index of multiple deprivation and religion.
In the sensitivity analyses, 523 participants were included. The findings remained the same, except for insignificant results for the fourth index of multiple deprivation quintile, no religion, ex-smoker, current drinker and thinking of eating more healthily in the next 6 months. The odds of having an NHS Health Check were lower in females (OR: 0.54, 95% CI: 0.38–0.77, p=.001).
Discussion
In all, 65% of participants had an NHS Health Check. The odds of having an NHS Health Check were found to be higher in BMEs and in people having other religions. The odds were lower in people having no religion, residing in the fourth index of multiple deprivation quintile and in ex-smokers. Apart from these, there were no variations in having an NHS Health Check. No associations were found between having an NHS Health Check and describing a healthy lifestyle, following a healthy lifestyle or thinking of making lifestyle changes in the next 6 months. Similarly, no associations were found between having an NHS Health Check and cut down/stop smoking among current smokers or amount of alcohol current drinkers would like to drink.
Studies have been conducted in different parts of England to explore the variations in attendance among different population groups. Older people had a higher uptake than younger people.22–29 In one study, males had a higher uptake than females and, in another study, the opposite was reported.24,27 Similarly, in terms of socio-economic deprivation and ethnicity, different results were reported in different studies. For example, some studies reported no variation, some reported a higher uptake in the most deprived areas and some reported a higher uptake in the least deprived areas.25–32 Some studies reported no ethnic variation, some reported a lower uptake in some BME sub-groups and some reported a lower uptake in Whites.22,25,26,30,32 In Leicester, the uptake among BMEs was reported as good. 30 Public Health England is working with the local authorities to address the inequality of its uptake. 33 If the NHS Health Check can motivate the under-served groups to improve lifestyle, it may reduce health inequalities therein. 30
Many qualitative studies have been conducted in different parts of England to explore the reasons for attending and not attending the NHS Health Check. Proactive attitudes towards health and a desire to prevent disease before the development of symptoms motivated many individuals to attend. The reasons for not attending include the lack of awareness, misunderstanding the purpose, aversion to preventive services, time constraints, the poor acceptability of the provider and the poor accessibility.34–37 A similar qualitative study needs to be conducted in our study area to explore the reasons behind having and not having an NHS Health Check. There is no ‘one size fits all’ blueprint for maximising the uptake among different population groups and different evidence-based strategies specific to the target group should be used for this purpose.27,35,36,38–42 There is a need to address the specific barriers to attending the NHS Health Check. This may include raising public awareness to ensure that people are informed about the aim and nature of the programme in order to reach an informed decision about taking up the invitation, emphasising the benefits of prevention of diseases that may encourage attendance in those who are reluctant to burden the public health-care systems, and extending outreach initiatives and increasing ‘out of hours’ provision at local community sites that may facilitate access.30,36,38,43,44
In terms of lifestyle advice provided as part of the NHS Health Check, some studies reported benefits, some reported no benefits and some reported mixed results.34,44–49 Some participants were satisfied with the lifestyle advice and some were not.34,35,45,47,49 Some participants found the lifestyle advice non-personalised, were confused about how it was communicated or were confused about the follow-ups.43,47,49 In addition, there were variations in the delivery of lifestyle advice between and within GP practices.50–52 Thus, there are a number of areas where improvements could be made. This includes a clear provision of personalised lifestyle advice, referral/access to appropriate services and adequate follow-ups; more standardisation in delivering the lifestyle advice between and within GP practices; and sufficient baseline and refresher training of staff to deliver the lifestyle advice effectively.38,44,47,49,52–55 In one RCT, the authors reported that there was no evidence of a further benefit of an additional lifestyle support by having the NHS Health Check. 56 It should be noted that the behaviour change process helps an individual to transition from an unhealthy lifestyle to a healthy one and to adhere to the healthy one in the longer term. Behaviour change techniques, such as information provision, exploration and reinforcement of motivation to change, goal setting, action planning, coping plans, and relapse prevention, are used for this purpose. 57 The lifestyle advice provided during the NHS Health Check can play an important role in this transition.
As far as we are aware, this is the first study of its kind conducted using an existing survey dataset. In terms of generalisability, the study findings could be valid in settings with similar populations. Several questions were adapted from the health and wellbeing measurement section of the UK census survey questionnaire, which has been used several times and has improved over time. This ensured the validity and reliability of the questionnaire. The trained interviewers used a standardised data collection protocol. Missing data could lead to bias, but it was nil in this study. It was not possible to calculate the ‘response rate’ as the survey was conducted using a quota sampling approach. Quota sampling has its own limitations (e.g. problems in making inferences from the sample to the population). The survey interviewed residents in pre-assigned sample points across Leicester. Quotas were set by age, sex, ethnicity and work status to ensure demographic representativeness. The interviewers continued to knock on the doors until they reached the target. Data were not collected on those who opted against taking part. Even if this information was available, the accurate ‘response rate’ would still be difficult to work out, as some people might have been willing to take part but did not fall into the right quotas. All the data were self-reported, and subjectivity, recall bias, and social desirability bias could have been an issue. Thus, studies incorporating existing records and objective measures could be used, which would cross-check our study findings and provide a complete picture. Around 98% of respondents were able to speak, write and read English, and language was an issue with only a few participants. In such cases, a family member or a professional interpreter was involved in the interview process, which might have influenced a small number of responses. The overarching BME and other religious groups are not homogeneous, and variations exist between BME and other religious sub-groups. However, in our study, these sub-groups were combined together as single overarching groups, as the sample size in each subgroup was not adequately large enough. Thus, further research is needed to explore the variations in these sub-groups. In our study, it was not possible to differentiate people who were already aware of/thinking of following/following a healthy lifestyle before attending the NHS Health Check from people who became aware of/started thinking of following/started following a healthy lifestyle after attending it. It was not possible to determine the causal association between the NHS Health Check and a healthy lifestyle, being a cross-sectional study. This would be better evaluated through a robustly designed RCT.
Conclusions
In Leicester, a few variations in having an NHS Health Check were found among different socio-economic, demographic and behavioural groups. No association was found between the NHS Health Check and a healthy lifestyle. Thus, the improvement work should focus on reducing these variations in having the NHS Health Check and bringing its benefits on promoting a healthy lifestyle.
Supplemental Material
10.1177_1757913919834584_Supplementary_material_appendix – Supplemental material for NHS Health Check and healthy lifestyle in Leicester, England: analysis of a survey dataset
Supplemental material, 10.1177_1757913919834584_Supplementary_material_appendix for NHS Health Check and healthy lifestyle in Leicester, England: analysis of a survey dataset by K Chattopadhyay, M Biswas and R Moore in Perspectives in Public Health
Supplemental Material
Appendix_LHWS_Relevant_Questions_Dec_2018 – Supplemental material for NHS Health Check and healthy lifestyle in Leicester, England: analysis of a survey dataset
Supplemental material, Appendix_LHWS_Relevant_Questions_Dec_2018 for NHS Health Check and healthy lifestyle in Leicester, England: analysis of a survey dataset by K Chattopadhyay, M Biswas and R Moore in Perspectives in Public Health
Footnotes
Acknowledgements
The authors thank the Leicester City Council (Public Health Division) and Ipsos MORI.
Conflict Of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Statement On Ethical Approval
The study was approved by the Research Ethics Committee, The University of Nottingham (UK).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.