
Abstract
To promote workers’ health and boost corporate productivity and national competitiveness, workplace health promotion is an international trend and a vital part of national policies. Prior to 2000, Taiwan’s workplace issues focused on industrial hygiene and safety improvements. Since 2003, the Health Promotion Administration (HPA) at the Ministry of Health and Welfare has established coaching centers for workplace health promotion and dispatched trained experts for teaching health promotion skills; including promoting the tobacco control program, preventing important chronic diseases, driving comprehensive programs, advocating workplace health promotion with the Ministry of Labor, establishing certification mechanisms for workplace health promotion, recognizing outstanding health-promoting workplaces, and conducting a nationwide survey for monitoring the practices of healthy behaviors and health conditions of workers. Through 2014, 12,439 workplaces have been accredited.
Since 2003, the efforts of the HPA in workplace health promotion projects has shifted society’s focus on workplace health from occupational diseases and injury prevention to workplace health promotion, resulting in the revision of the Occupational Safety and Health Act in 2013 by the Ministry of Labor to detail employers’ responsibilities in protecting and promoting employees’ health and well-being.
Introduction
International trend of healthy workplaces
The workplace is an important environment, affecting the mental and physical well-being of workers, economy, and society; it also indirectly affects the health conditions in households, communities, and society levels. The global workforce accounts for approximately half of the world’s population (1), making it the foremost socioeconomic contributor for each nation. Rapid changes in business environments have recently resulted in enterprises seeking novel ways to boost their productivity. Contrastingly, the increasing number of people with chronic diseases has decreased productivity and increased medical costs. Hence, methods for preventing work-related illnesses and boosting workers’ well-being are important (2).
Prior to the 1980s, occupational safety and health emphasized the recognition, evaluation, and control of workplace environmental risk factors. However, with the rising awareness of global health promotion, the workplace has evolved as an ideal health promotion site. In 1997, at the Symposium on Healthy Workplaces at the 4th International Conference on Health Promotion, the World Health Organization (WHO) recognized the workplace as an important health promotion domain and proposed the Jakarta Statement on Healthy Workplaces. It explicitly outlined the four main principles of a healthy organization: health promotion, occupational health and safety, human resource management, and sustainable (social and environmental) development (3). In the same year, the European Union (EU) established the Luxembourg Declaration on Workplace Health Promotion, stating that promoting a healthy workplace depends on cumulative efforts of employers, employees, and society for adapting to future changes (4).
In the process of the push for workplace health promotion among developed countries, workers’ health and lifestyle, workplace safety and hygiene, organizational culture, and workplace mental health are closely associated; it is incumbent on the government and enterprises to collaborate and devise comprehensive plans. Canada, Japan, America, Australia, and the EU support this notion; in 2010, WHO launched ‘Healthy Workplaces: A Global Model for Action’ (5), which integrates core values, promotion approaches, and execution steps, forming the crux of healthy workplace promotion.
Workplace health situations and issues
Taiwan launched a labor insurance program in 1950, and the Labor Insurance Act was effective in 1960 for ensuring the economic stability of workers. The act was amended 15 times to increase coverage, provide workers with more protection and compensate more workers; in 2009, the Labor Insurance Pension program was implemented. Previously, cash benefits from labor insurance included maternity, injury/sickness, disability, old age, and death. However, since the implementation of this program, monthly pension claims for disability, old age, and death have been integrated to better care for workers and their families.
Taiwan enacted the Occupational Safety and Health Act (OSHAct) in 1974, amended over four times prior to 2013, to prevent occupational hazards and protect the safety and health of workers. However, revisions were mostly centered on accountable departments, improvement of environment safety and sanitation, and fine regulations (Occupational Health and Safety Act, 2013) (6).
To identify occupational diseases and provide post-accident security and retraining, the Act for Protecting Workers from Occupational Accidents was enacted in 2002, with one regulation specifying the compensation offered to uninsured workers by the government. The act also aims at reducing the incidence of occupational injury by implementing research, education, and training programs.
Apart from the aforementioned labor protection measures, Occupational Safety and Health Administration, Ministry of Labor (OSHA) established the Voluntary Protection Program and Taiwan Occupational Safety and Health Management System (TOSHMS) to assist companies to introduce health and safety self-management systems. TOSHMS was formulated and integrated based on the framework and requirements of global management systems ILO-OSH 2001 and OHSAS 18001:2007, which help enterprises to comply and integrate these systems into their business strategy and operations, creating a safe and comfortable working environment. Starting in 1994, in addition to labor inspections of high-risk workplaces, a nationwide randomized survey of perceptions of safety and health at workplaces has been conducted every three years as a reference for possible policy adjustments.
During the 1990s, Taiwan businesses were mostly concerned with workplace safety and hygiene. A survey concerning the status of medical and health management in Taiwanese factories by Jin-Huei Hsu in 2005 revealed that the main topic of pre-occupational education of labor workers was ‘emergency rescue and disaster response’ and that it focused less on risk factors for health, such as smoking cessation, stress, and nutrition (7). That same year, a study on promoting workplace health in Taiwan’s businesses by Fen-Ling Chen revealed that the priorities of health promotion in domestic businesses still centered on regulations and labor safety, such as regular health check-ups, recreational activities, and seminars on occupational hazards (8).
Hazards have been minimized by improving occupational safety and hygiene, and changing labor population and operation patterns. However, adverse health factors from unhealthy lifestyles and insufficient physical activity because of work pressure and industry change, as well as the incidence of eating out and consuming sugary drinks, are important considerations in combating musculoskeletal disorders, mental health problems, and obesity.
To promote workers’ health, the Health Promotion Administration (HPA) began promoting a nationwide ‘Smoke-free Workplace’ project in 2003. While it was based on tobacco hazard prevention at workplaces, the project emphasized promoting workplace health beyond hygiene and safety. In 2004, the HPA proposed the following goals: (1) promotion of health risks and occupational health; (2) establishment of an occupational health service network; (3) establishment of a reporting system for occupational injuries and diseases; (4) promotion of workplace health building; and (5) improvement of the mental, physical, and social health status in employees (9). In 2006, the HPA included other health promotion issues, such as breastfeeding and betel-nut hazard prevention, transforming the project into a comprehensive workplace health promotion program.
Since 2007, the HPA has organized annual activities for healthy workplace certification. There are two types of certification: 1) the Tobacco Hazard Prevention Label; and 2) the Health Promotion Label. In 2009, the Health Promotion Label was further differentiated into the Health Activation Label and the Comprehensive Health Promotion Label. The purpose of this differentiation is to encourage all workplaces to move toward a Comprehensive Health Promotion Label. Li-Hui Yu stated that one of the key factors affecting health promotion quality in workplaces is the Healthy Workplace Certification category; workplaces awarded with the Comprehensive Health Promotion Label often scored higher in quality of health promotion in the workplace than those with the Health Activation Label (10).
Methods
Establishing coaching centers for workplace health promotion
To enhance health promotion capacity building in enterprises, the HPA has established workplace health promotion coaching centers in northern, central, and southern Taiwan (11,12). Each center has a consultation team consisting of about 10 experts from the fields of public health, occupational health, nutrition, tobacco hazard prevention, physical activity, and healthy behaviors. Multidisciplinary representatives are able to strengthen the bridges between science, policy, and practice. Figure 1 shows the organization of the coaching centers, which are commissioned by the HPA and supported by the Ministry of Labor, and have established collaboration with local governments, academia, medical institutions, and the Institute of Labor, Occupational Safety and Health. The coaching centers also tutor enterprises, associations, and unions.
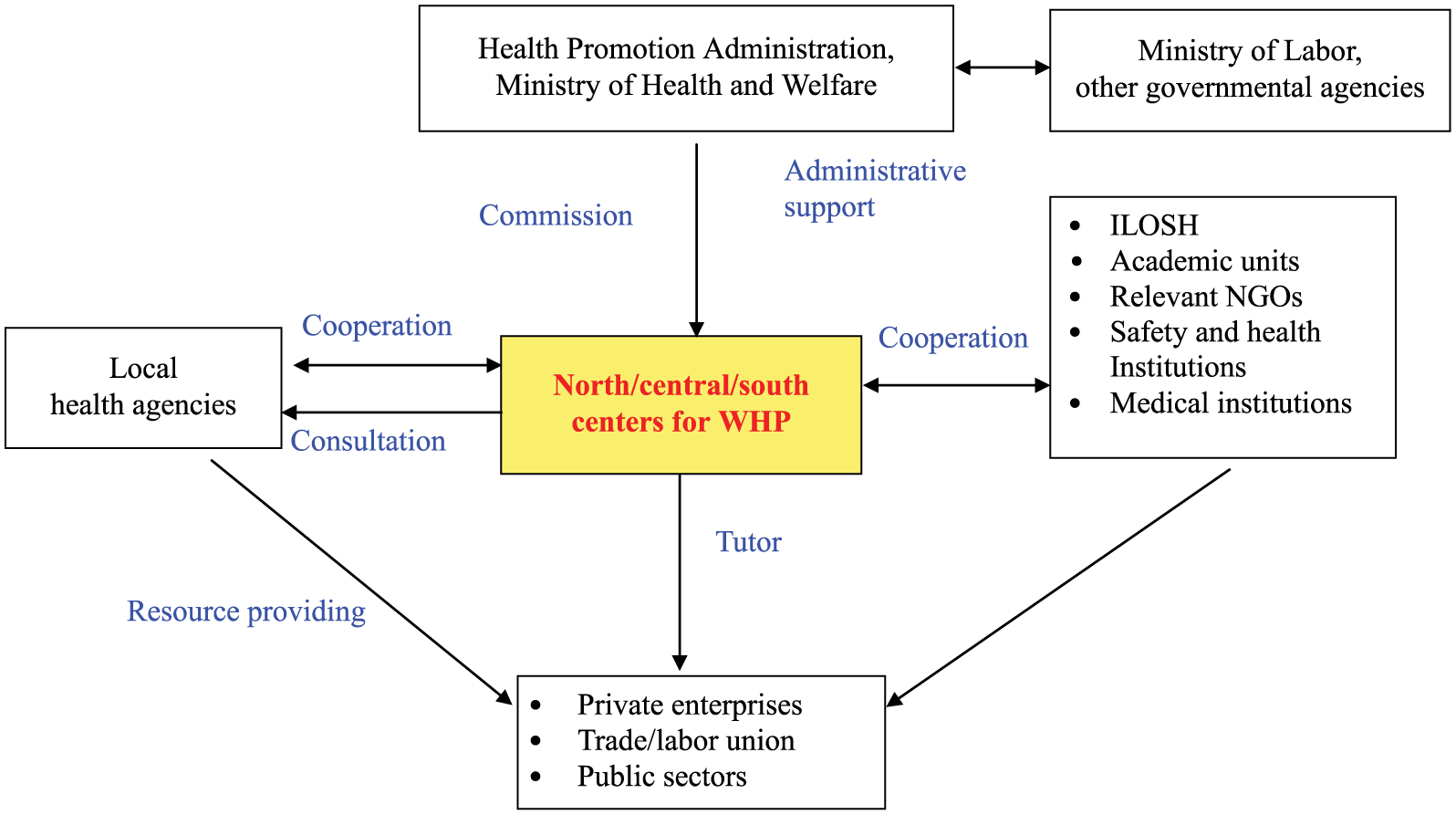
Structure framework of workplace health promotion.
Three coaching centers aim to provide consultations for health promotion programs, conduct seed personnel training courses for local health agencies and enterprises, develop educational tools, organize annual self-management certification activities, and conduct annual nationwide surveys that will provide the basis for future promotion and adjustments for the program.
The promoting strategies of Centers for Workplace Health Promotion (CWHP) are in accordance with the five Health Promotion Actions of the Ottawa charter for health promotion. Industries are advised to establish health policies to foster a healthy environment, support healthy eating and on-site exercise programs, and recommend paid time-off for participation in behavioral health programs. The local health agencies and CWHP provide many on-site educational classes for strengthening personal skills. CWHP is crucial in helping health agencies to conduct the Cancer Screening Program and Healthy Weight Management Program.
Implementing workplace health promotion
Anti-smoking programs have been globally implemented for protecting human health since European and American medical communities confirmed that smoking is hazardous. In 2003, the Nationwide Tobacco Hazards Prevention Program in the Workplace was launched in Taiwan, aiming to achieve smoke-free workplaces. The program included a counseling project comprising education, policy interventions, smoking area restrictions, and smoking cessation aids. Personnel at industrial safety and health departments were offered training courses on national tobacco control policy, workplace promotion strategies, tobacco hazards, and health promotion. Tobacco control policies were integrated into the management systems of every enterprise and were individually tailored to their needs based on prior visits, including suggestions regarding the optimal locations for smoking rooms or areas and other workplace improvements. The project also provided numerous resources, including posters, flyers, stickers, a telephone helpline, and smoking cessation aids, to the counseled workplaces.
The Comprehensive Healthy Workplace Model implemented in 2010 aims to encourage smoke-free workplaces and promote occupational injury/disease prevention and health promotion programs, paving the way to a healthy workplace. This model not only addresses the core values of leadership engagement and worker involvement but considers the four avenues of influence for a healthy workplace. Furthermore, the eight steps (i.e. mobilize, assemble, assess, prioritize, plan, do, evaluate, and improve) of the continual improvement process which proposed by WHO were followed to guide enterprises in establishing a healthy workplace.
The government budget of workplace health promotion is funded by the Health and Welfare Surcharge on Tobacco Products. Increasing the cost of tobacco products in terms of price and tax increases has been helpful in controlling tobacco consumption in many countries. The Health and Welfare Surcharge on Tobacco Products, launched on March 24, 2000 in Taiwan, and the designated tobacco surcharge revenue are directed for use in health promotion and care.
Advocating workplace health promotion with the Ministry of Labor
The Institute of Labor, Occupational Safety and Health (ILOSH), Ministry of Labor, had collated international literature on issues of workplace health promotion in the labor administration system, along with different approaches for health promotion, but was not involved in the workplace health programs. The HPA and Ministry of Labor reached a consensus to promote healthy workplaces and named 2008 as the first year of workplace health promotion.
Despite efforts by the Ministry of Health and Welfare and the Ministry of Labor to promote a healthy workplace, the 2013 National Healthy Working Environment survey indicated that 42% of the companies did not previously organize any health-related promotional activities. This revealed a discrepancy compared with the North American counterparts, where about 80% of enterprises actively participated in providing health services for their employees. Furthermore, during counseling for healthy workplace promotion at each center, it was clear that most companies were yet to propose health policies, allocate budget, or present a sustainable health promotion plan.
The Ministry of Labor has markedly revised the occupational health, safety, and hygiene programs. The Occupational Safety and Health Act has replaced the Labor Safety and Health Act, expanding its coverage to all industries. The act entails employers’ responsibilities in the areas of: 1) prevention of musculoskeletal disorders because of repetitive tasks; 2) prevention of work-related diseases because of anomalistic workloads from work shifts, night shifts, and long working hours; 3) prevention of unlawful physical or mental injuries from others while on the job; and 4) protection of maternal health for female workers during pregnancy and breastfeeding. Moreover, to effectively promote the relevant policies, employers should follow regulatory guidelines for recruiting workers and on-site physicians to aid in preventative medical care. The Occupational Safety and Health Act was officially enacted on July 3, 2013 and it fosters a more aggressive health care and health promotion campaign at workplaces.
Encouraging enterprises to participate in the Workplace Health Promotion (WHP) program
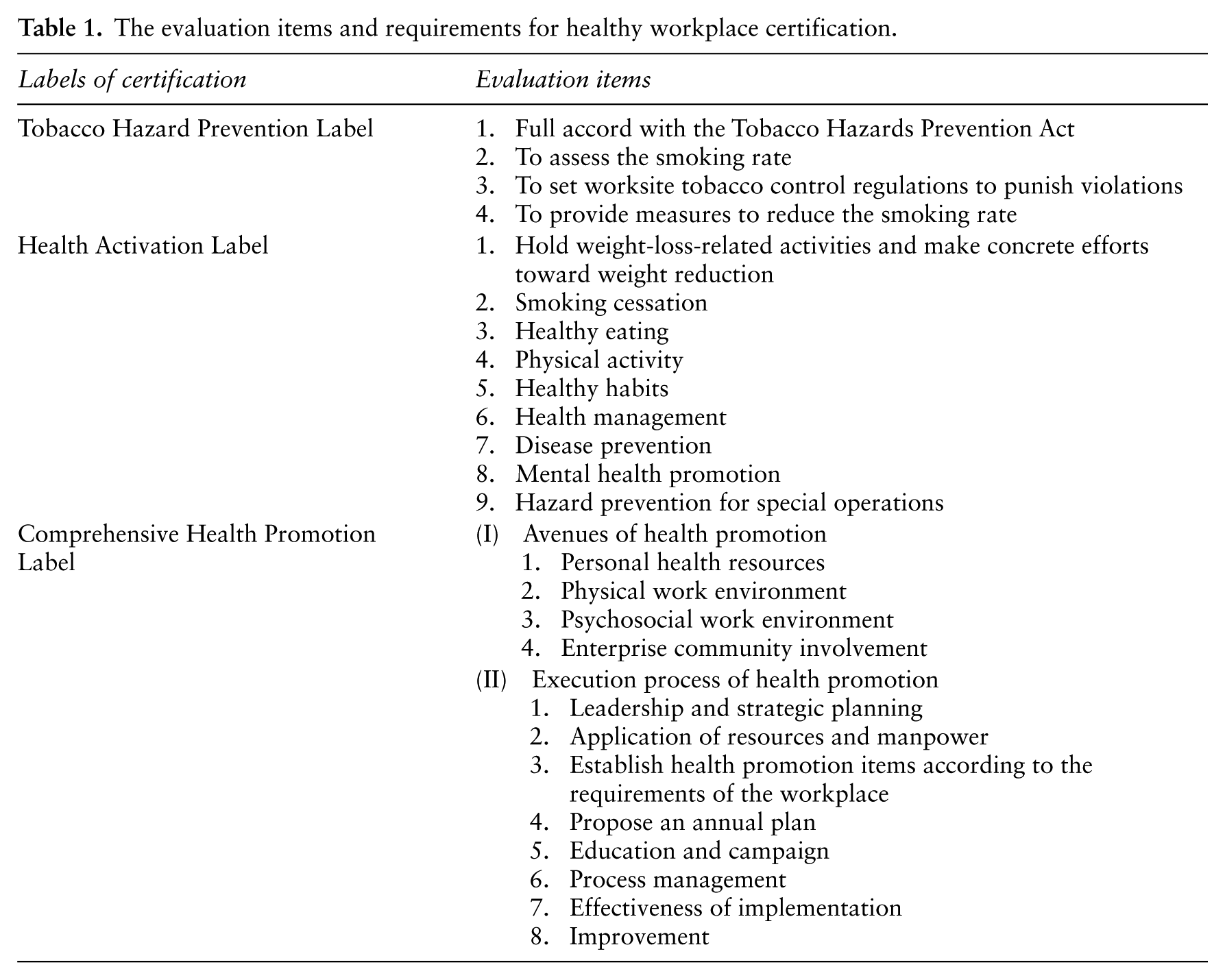
In order to encourage enterprises to participate in health promotion, since 2007, the HPA has organized annual activities for healthy workplace certification. There are two types of certification: 1) the Tobacco Hazard Prevention Label, which evaluates the prevention of tobacco use at workplaces; and 2) the Health Promotion Label, which evaluates the implementation of health promotion activities at workplaces. In 2009, the Health Promotion Label was further differentiated into the Health Activation Label and the Comprehensive Health Promotion Label. The Health Activation Label was added to encourage workplaces that implement at least two or more employee health promotion activities to participate in the certification. The criteria for the Comprehensive Health Promotion Label amplify the value of regular employee health check-ups and systematic planning of employee health promotion. Table 1 shows the assessment items and requirements for the three labels.
The evaluation items and requirements for healthy workplace certification.
Enterprises participating in the healthy workplace certification have increased year by year since 2007. There were only 673 workplaces that had passed the certification the first year; however, by 2014, 12,439 workplaces had been accredited, with Smoke-free labels awarded to 6957 companies, the Health Activation Label awarded to 3490 companies, and the Comprehensive Health Promotion Label awarded to 1992. Up to 432 companies have been discreetly evaluated and commended for their active efforts and are the learning models for other enterprises.
Recognizing outstanding workplaces as a paradigm of enterprises
To speed up health promotion at workplaces and to offer bench-marking learning opportunities for industries, the HPA has carried out nationwide health excellence workplaces recognition since 2006. Each year, awards are set based upon the policy targets of the year, and 30 outstanding workplaces are awarded. The eligibility criteria include application for the certification of a healthy workplace (Health Activation and Comprehensive Health Promotion labels) and submission of special achievements and outcomes as the accompanying proof of excellence. Workplaces that have been awarded the label are nominated by local health bureaus or coaching centers and are judged by experts assembled by the HPA through document reviews and on-site visits. To illustrate the creativity and experiences of health promotion at workplaces, different award categories, including the Health Pilot Award (healthy workplace as one of the core values of the enterprise), the Health Benchmark Award (a comprehensive health promotion plan that can be a model for other workplaces to learn from), and the Health for All Award (for every employee to encourage a healthy lifestyle), were established. In 2014, two new categories were added: the Decade Excellence Award and the Promotion Staff Excellence Award. Between 2006 and 2014, 412 workplaces achieved recognition.
Results and discussion
Achievements and challenges in workplace health
The Labor Safety and Health Act was enacted in 1974, and it has resulted in the following noteworthy achievements. A gradually increasing tendency of pre- and on-job physical examinations and occupational safety and health education was found among respondents from seven consecutive surveys between 1994 and 2013. Moreover, the numbers of occupational accidents sharply declined from 4.898 to 3.453 per thousand workers, with a rate of reduction of 29.5% between 2001 and 2014, similar to data from advanced countries.
Conventional environmental hazards have been minimized with improved occupational safety and hygiene as well as the change in labor population and operation patterns. However, risk factors associated with unhealthy lifestyles and insufficient physical activities because of work pressure and industry changes are important for combating musculoskeletal disorders, mental health problems, and obesity (13). Table 2 shows the numbers and the major causes of compensation for occupational diseases in recent years. We found the numbers of workers compensated due to occupational diseases were low compared with most developed countries. According to data of the compensation of labor insurance for occupational diseases, the most commonly seen occupational diseases in Taiwanese workers include: arm, neck, and shoulder disorders; occupational lower back pain; coal worker pneumoconiosis and its complications; as well as brain and cardiovascular diseases. More than 60% of the causes of the compensation of labor insurance for occupational diseases were musculoskeletal disorders, although brain and cardiovascular diseases ranked fourth, and they ranked first according to disease severity, because almost half of the cases led to death or disability. Therefore, preventing work-related musculoskeletal and brain and cardiovascular diseases is important in workplace health promotion. The reasons for low compensation application and payment cases in occupational diseases included the complex legal system and compensation process, the lack of work exposure data, employers’ unwillingness to report, as well as uninsured labors in small businesses (15,16). In order to foster the quality of prevention and treatment services of occupational injury and diseases, and to minimise the underestimation of occupational disease issues in Taiwan, OSHA established centers and clinics in 2003. These included the Center of Occupational Disease and Injury Service and outpatient clinics at network hospitals, and currently there are nine major prevention and treatment centers and 66 network hospitals. The reference guide to identified occupational injuries and diseases has been updated yearly, with 61 presently verified as harm caused by chemical, physical, biological, human nature, or social psychological reasons.
Compensation of labor insurance for occupational diseases.
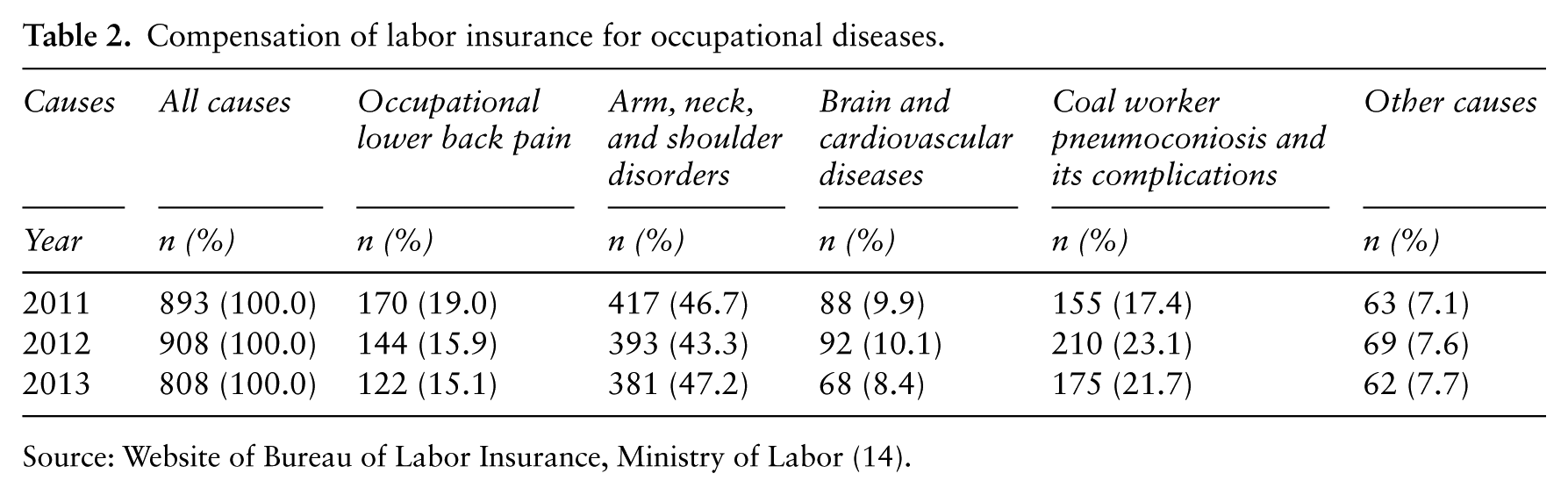
Source: Website of Bureau of Labor Insurance, Ministry of Labor (14).
In addition, to prevent new occupational diseases, such as burnout, and musculoskeletal and mental disorders due to long working hours and stress, the OSHA amendment act requires that all employers implement prevention programs. Meanwhile, OSHA and the HPA both provide funding to occupational health services programs and healthy workplace promoting programs, respectively, but the two programs complement each other, and meet to discuss the content of the programs. The occupational health services programs focus on health and environment assessment, high-risk group identification, occupational injury and disease-related consultations, and health management; the healthy workplace programs follow the WHO Healthy Workplace Model to guide workplaces to establish health policies and prevent health problems arising from work or unhealthy lifestyles.
OSHA has tried their best to improve the physical working environments for several decades and has also turned their attention to the emerging work-related diseases. With the enactment of the Occupational Safety and Health Act, more enterprises will be encouraged to foster health promotion plans in compliance with regulations. Moreover, HPA and OSHA continuously advocate for corporations to pay more attention to corporate social responsibility, and argue that impetus for a healthy workplace can be elevated when more emphasis is placed on the value of the enterprise and its duty to take care of the employees.
Achievements and challenges in workplace tobacco control
The achievements brought about through the workplace tobacco control program have been significant. This program was simultaneously launched with other national tobacco control programs in 2003, and owing to the efforts of the involved enterprises, most workers recognized the hazardous effects of tobacco smoke, with many employers agreeing to restrict or completely prohibit smoking areas. This may have been the driving force behind the amended Tobacco Hazards Prevention Act enacted five years later. The amendment completely prohibited smoking at indoor workplaces with three or more workers.
Figure 2 shows the results from national surveys conducted between 2004 and 2014. A 10% smoking rate reduction (from 24.2% to 14.2%) was found among all respondents over 10 years; the decreasing trend in male workers was particularly sharp, with the smoking rate decreasing from 42.4% to 27.9%. Second-hand smoke exposure rates were also remarkably reduced, from 29.9% to 14.0%. However, after the implementation of the Tobacco Hazards Prevention Act, second-hand smoke exposure rates annually increased because of laxity in workplace tobacco control issues. Table 3 reveals that the percentage of tobacco control classes in 2010 was only half of that in 2007 in SMEs (Small and Medium Enterprises, enterprises with less than 300 employees). Furthermore, after implementation of a reinforcing strategy, the second-hand smoke exposure rate fell by 1% in 2014 after four years of successive increases; the exposure rate needs to be continuously observed.
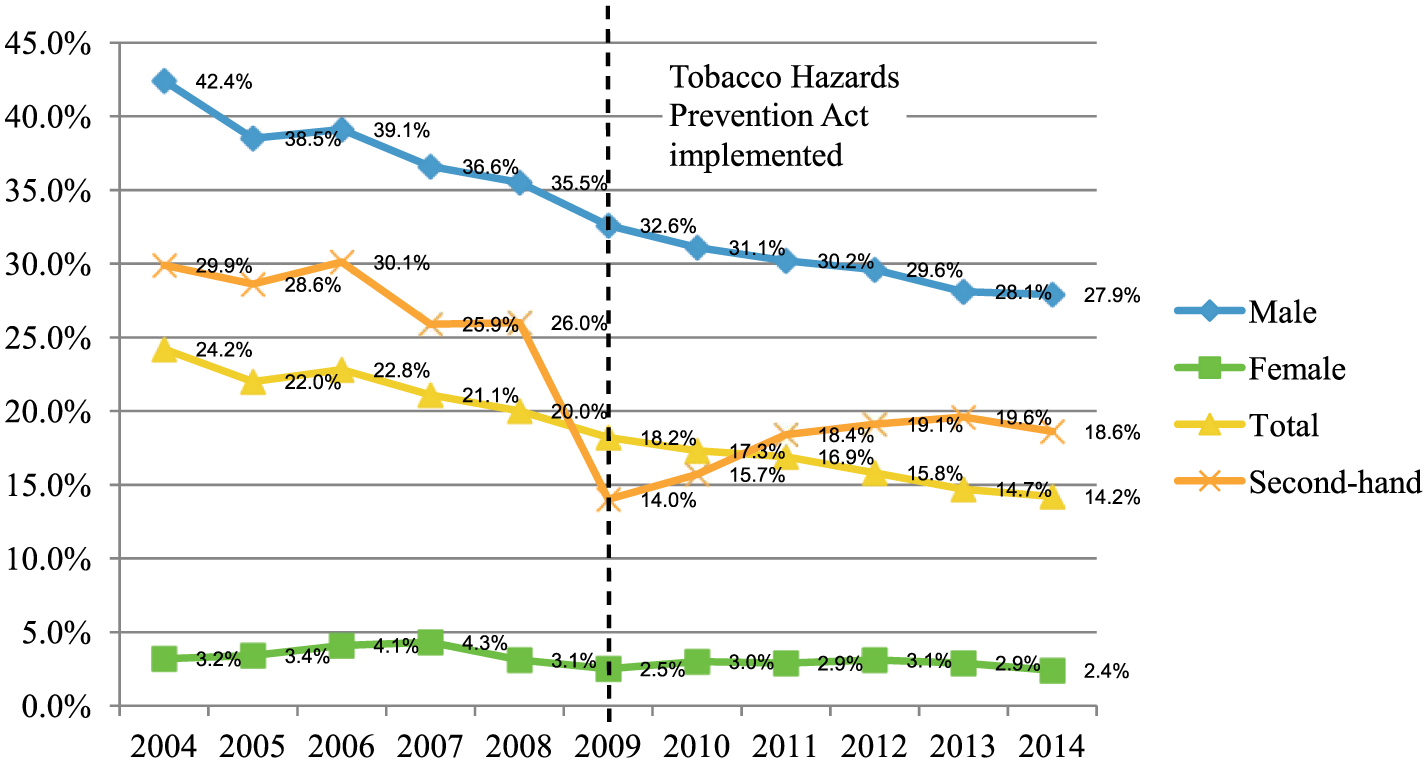
Changes in smoking rates and second-hand smoke exposure rates, 2004–2014.
Health promotion classes or activities at workplace among respondents.
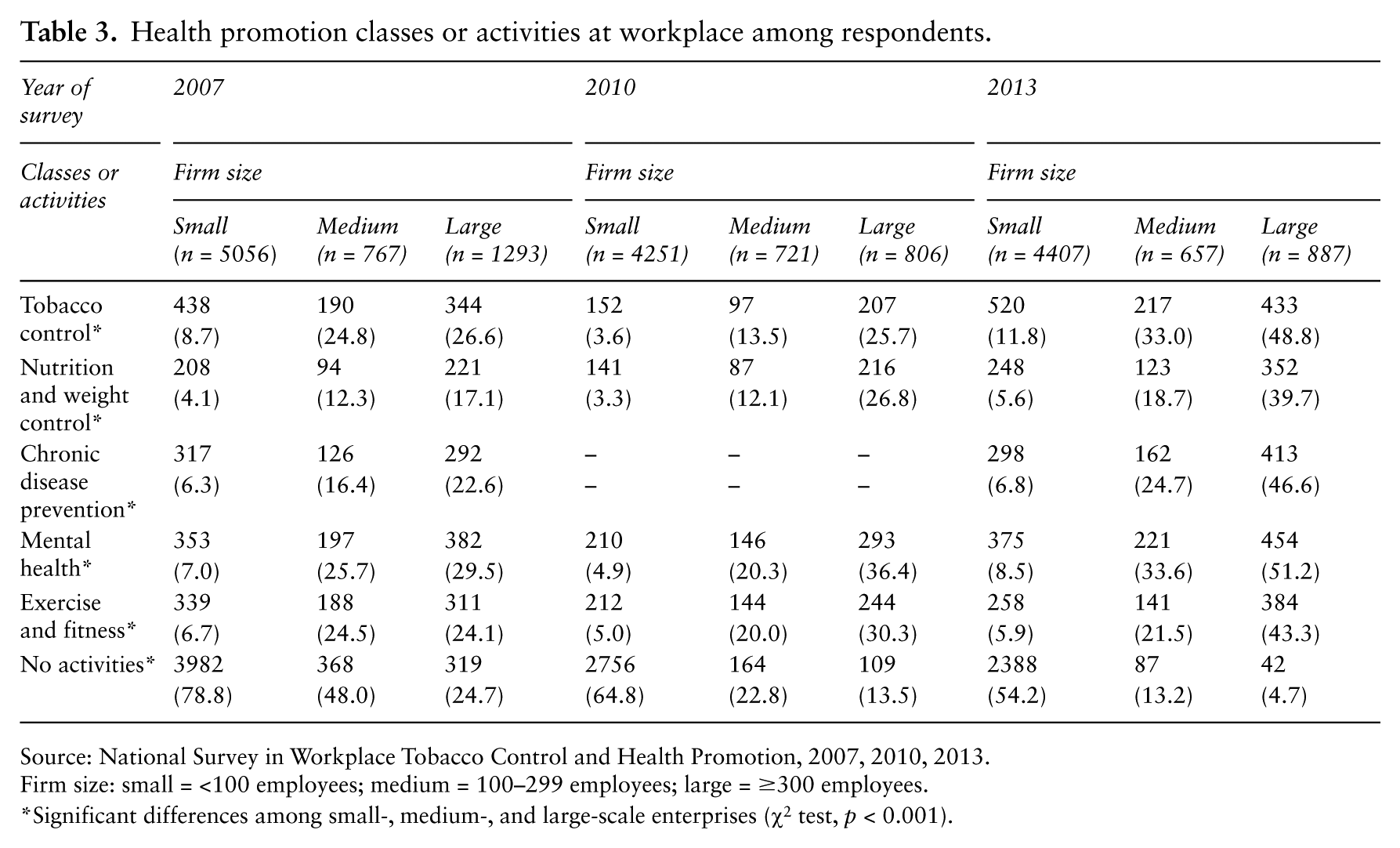
Source: National Survey in Workplace Tobacco Control and Health Promotion, 2007, 2010, 2013.
Firm size: small = <100 employees; medium = 100–299 employees; large = ≥300 employees.
Significant differences among small-, medium-, and large-scale enterprises (χ2 test, p < 0.001).
Although smoking rates among employees sharply decreased, the smoking rates of male workers needs to be reduced, and more attention needs to be paid to resolve issues associated with second-hand smoke exposure. The workplace tobacco control program remains a complicated concern.
Achievements and challenges in advocating and implementing workplace health promotion
Since 2006, CWHP has provided impetus for multiple issues for the WHP program.
Table 3 reveals a continuously increasing prevalence of activities in large firms, with only 4.7% not offering any training classes about health promotion in 2013. However, progress in small companies was less significant. In addition to health promotion activities, the health promotion facilities offered by employers were also improved. Annually increasing penetration rates were found at all facilities, except at sport venues. Because of space constraints in Taiwan, sport venues are not available at many companies; therefore, a strategy for promoting regular exercise must be implemented at workplaces.
To achieve sustainable healthy workplaces, we initiated the workplace health promotion program through multiple activities, such as health seminars, exercise campaigns, and weight loss campaigns. Once awareness is raised in the workplace, further health promotion programs are introduced to assist workplaces in policy establishment, resources integration, needs assessment, program formulation, program execution, and effectiveness evaluation. Through years of advocacy, the external resource provision can be a boost to the initial stage of health promotion; however, it is the commitment of the higher levels of the company that ensures its sustainability. Their participation in health policy formulation, manpower and fund provision, as well as other important factors, including physical environment, working condition, organizational culture, and health services, are the key to a comprehensive healthy workplace.
In Taiwan, the HPA has devoted major efforts in WHP for over 10 years, and positive outcomes in tobacco control and other topics of health promotion have been found. However, as of 2014, 38.1% of enterprises or organizations that did not offer any health promotion project were present. Further, the percentage of healthy lifestyle practice among workers remains low. Data from the national survey in 2014 reveals that only one-third of respondents ate enough vegetables and fruits (i.e. three and two portions of vegetables and fruits, respectively), with more than half the respondents not exercising enough (i.e. at least 150 min of medium-level exercise/week); 27.9% male workers are current smokers. The situation emphasizes the importance of the WHP program. Approximately 40% respondents suffered from musculoskeletal disorders, 30% usually felt fatigue, 20% suffered from headache and insomnia, and 10% had emotional problems. Merely 7.8% of respondents had taken sick leave in the past three months. Contrastingly, 15.6% respondents were present while ailing. Because of the association between presenteeism and productivity loss, enterprises should consider better-paid sick leaves or paid vacations.
According to the latest report conducted by the Buck Consultants Company (17), the percentage of organizations offering health promotion to employees – by region – was as follows: North America 79%, Latin America 46%, Europe 46%, Africa/Middle East 38%, Asia 46%, and Australia/New Zealand 47%. The percentage of WHP in Taiwan was about 60% (13), estimated from nationwide representative samples, placing it just below North America; however, the percentage of firms offering comprehensive health promotion was lower than 19% (18).
In the United States, the employer feels the direct impact of poor employee health; this has led to a higher prevalence of WHP programs in the United States. While in Taiwan and most European countries, because of the existence of universal health insurance coverage, employers mainly feel the impact of poor health through absenteeism and presenteeism. But there is a lack of research on the relationship between absenteeism, presenteeism, and productivity in Taiwan (19). It is thus recommended that in the near future, more studies be undertaken to encourage employers to offer the WHP and ultimately, promote employee health and productivity (20).
In addition, it is shown that whether a workplace promotes health-promoting activities is correlated to its magnitude. For instance, health-promoting activities are more commonly seen in medium- and large-sized enterprises rather than small-sized enterprises. In Taiwan, the requirements of the Occupational Safety and Health Organization and the numbers of personnel by OSHA are according to the numbers of employees. In large-sized enterprises, there are well-established occupational safety and health departments and enough personnel, including industrial hygienists and occupational nurses, to facilitate the health promotion programs. On the other hand, because of the shortage of manpower and financial support, there is a need for more external resources to promote worksite health promotion among Taiwan’s small-sized enterprises.
Taiwan has a well-developed health administrative system to carry out the WHP program. WHP programs executed by the HPA, when integrated with other healthcare resources and other settings (such as health promotion schools, health promotion hospitals, health promotion military, health promotion correctional facilities, etc.), would bring about accelerated penetration rates and effective results. The experience in the push for healthy workplaces is becoming more mature, and with experience sharing of accredited workplaces and promotion by counseling centers, these can greatly assist in the implementation of subsequent campaigns.
The authority for worker safety, health, and well-being is the Ministry of Labor, although the concepts of health protection and health promotion have been introduced into OSHAct, and active communication and cooperation between health and labor departments require further strengthening. In response to the OSHAct and the HPA’s chronic disease prevention strategies, both health and labor departments should have a clearer division of work and collaboration.
On the grounds of enhancing quality of public service, countries in Europe take the lead in advocating health promotion in public sectors. By contrast, since our public servants are not covered under the Occupational Safety and Health Act, and relevant manpower and funding are not allotted, the penetration rate of health promotion in public services is not high enough to become a trend.
Conclusion
The Ministry of Labor in Taiwan has been devoted to the improvement of the physical working environment for several decades. Like most countries, Taiwan’s workplace also faces challenges such as an aging workforce, increasing prevalence of lifestyle-related diseases, and mental disorders. OSHA has revised the Occupational Safety and Health Act recently to entail employers’ responsibilities in preventing work-related cardio-cerebrovascular diseases, musculoskeletal disorders, and mental problems; nonetheless, the penetration rate of employers’ implementing health promotion has yet to be proven.
The HPA’s eagerness in pushing for workplace health promotion has given rise to amendments in the Tobacco Hazards Prevention Act and the Occupational Safety and Health Act, and has corporations paying more attention to the health issues of its employees. With the gradual increases in health promotion activities and facilities, approximately 60% of workplaces now engage in at least one health promotion activity.
In an attempt to achieve the optimal state of employees’ mental and physical health, authorities should continue to offer incentives and assistance to enterprises and enhance inter-departmental collaboration within government sectors.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.