
Abstract
Antonovsky’s salutogenesis is a theoretical perspective on health development that explores physical, mental, and social factors that contribute to a ‘healthy life orientation’ and also a theoretical approach to behavior change. Previous studies applying salutogenesis show that a high sense of coherence (SOC), a composite measure from salutogenesis indicating one’s capacity to cope with stress, is associated with a healthy life orientation and lifestyle behaviors, including healthy eating patterns. However, limited evidence exists on the factors that underlie SOC, which could be used to strengthen this capacity as a means to enable healthier eating. Dutch adults (N = 781) participated in a cross-sectional study examining the relationship between SOC and a set of individual, social-environmental, and physical-environmental factors. The main findings indicate that high SOC was associated with a diverse set of factors including lower doctor-oriented health locus of control; higher satisfaction with weight; higher perceived levels of neighborhood collective efficacy; higher situational self-efficacy for healthy eating; lower social discouragement for healthy eating; and higher neighborhood affordability, accessibility and availability of healthy foods. These findings can inform the design of nutrition interventions that target these factors that strengthen SOC and provide the building blocks for a healthier life orientation.
Introduction
Diet-related diseases such as obesity and diabetes have reached epidemic proportions worldwide (1). As a result, there has been a push within nutrition research to better understand the risks and benefits of certain nutrients and foods on physical health (2), and the study of risk factors leading to poor dietary behaviors (3). Such research comes from a biomedical model, which is driven by the search for causes and prevention of disease and ill-health (4). However, the biomedical approach insufficiently addresses the complex, multifaceted factors influencing eating. As a result, there is decreased relevance and applicability of research findings for everyday life (5). For instance, eating is much more than only a health behavior (6). In everyday life, it is a complex, multifaceted practice influenced by many aspects (7), including, amongst others, personal belief systems and the wider social context (8,9). Moreover, we know that people’s physical health concerns are not the only force driving people’s food choices (10). In everyday life, people do not just eat to fulfill physiological needs; they also strive for quality, pleasure, and goodness (11). Lastly, it assumes healthful eating is a central concern in people’s lives. Yet in everyday life, healthy eating is only one of the many concerns to accomplish health and it is integrated within daily practices. Eating practices are socially embedded into daily life; food is often shared with others and provides opportunities for making social contacts (12).
Taking this all into account, biomedically-oriented nutrition research, which emphasizes risks to individual physical health, is too narrowly focused and should be complemented with a contextualized orientation, relevant and applicable to people’s everyday life (13). Salutogenesis, Antonovsky’s theoretical perspective on health development (14), offers an appropriate starting point. It is a theoretical perspective on health development that explores physical, mental, and social factors that contribute to a ‘healthy life orientation’ and also a theoretical approach to behavior change. Rather than a static state, health is defined through this framework as a life-long process and healthy means an active and productive life, a ‘good life’. The salutogenic approach differs from the described biomedical approach in several ways. Instead of having a focus on physiological factors involved in illness and the prevention of disease, it has an emphasis on the positive aspects of health and well-being (15), taking into account the diverse physical, mental, social, and factors that promote health (16). Furthermore, rather than studying individual health separately from the physical and social context, it studies how health is developed through resources found within people and their everyday life context (17). Another key difference is that salutogenesis assumes health-related practices – such as eating – are a resource for living rather than a central goal in life (18).
Within the salutogenic framework, the central construct is what Antonovsky called ‘sense of coherence’ (SOC). SOC is described as a ‘sixth sense’ for survival and helps in generating health-promoting abilities (17). The strength of one’s SOC is a crucial factor in facilitating and developing health. A higher SOC score is associated with better physical and mental health outcomes (19). Furthermore, evidence suggests that SOC is also a predictor of healthy lifestyle practices. High SOC is associated with dietary patterns more in line with dietary recommendations (13), higher intake of fruits and vegetables (20,21), and lower intake of sugars and saturated fats (22).
Given that SOC is a strong predictor of health and healthy lifestyle practices, health promotion should consider strengthening SOC within interventions (23,24). Evidence from a limited number of studies suggests that socio-demographic factors (25,26) and work and living conditions (27,28) relate to SOC. However, evidence remains limited and we lack a comprehensive picture and deeper understanding of the building blocks which support the development of SOC (29). As a result, it remains unknown what is needed in health promotion activities to strengthen SOC (30). By gaining greater insight into the factors that underlie SOC, we can help inform the development of future health promotion interventions.
The purpose of this study was to determine in a cross-sectional sample of Dutch adults if a set of individual, social-environmental, and physical-environmental factors are associated with SOC. Since our study was part of a larger project interested in promoting healthy eating and preventing obesity, we identified eating-specific factors from the literature that support healthy dietary behaviors and healthy weight. In addition, we included factors arising from the individual and social- and physical-environment that have been found in previous studies to be associated with SOC (25–28). This led to the inclusion of the following eleven factors: body weight, satisfaction with weight, nutrition knowledge, flexible restraint of eating, situational self-efficacy for healthy eating, multidimensional health locus of control, social support and discouragement of healthy eating, neighborhood collective efficacy and perceived neighborhood affordability, availability and accessibility of healthy foods, and socio-demographic factors.
Methods
Study population
Participants for the study were recruited from the CentERdata Long-term Internet Studies for the Social Sciences (LISS) panel. We used a sub-group from the research panel involved in an ongoing weight monitoring project. In this project, participants weigh themselves regularly and complete questionnaires on a regular basis regarding weight and dieting habits. Furthermore, participants complete a yearly survey that collects general health and socio-demographic data. Panel members (N = 1001) 18 years and older who had measured their weight between August 2011 and January 2012 were invited to complete the internet-based survey in January 2013. The survey was completed by 944 panel members (response rate 94%). Participants with missing data, who were either pregnant, currently being treated for an eating disorder, following a modified diet due to a health problem or who had a serious illness that caused weight loss or gain were excluded from the analysis. This left a total of 781 people (78% of total sample) that were included in the final analysis.
Survey instrument
The survey instrument measured respondents SOC as well as individual, social-environmental and physical-environmental factors.
Scales chosen for the study were from pre-existing, pre-validated scales and when necessary, were translated from English into Dutch. Table 1 provides a complete overview of variables in the survey including an example question, scale content, scale measurement, internal reliability (Cronbach’s α) as found in our study, and the references to the pre-existing, pre-validated scales that they came from.
Survey measures.
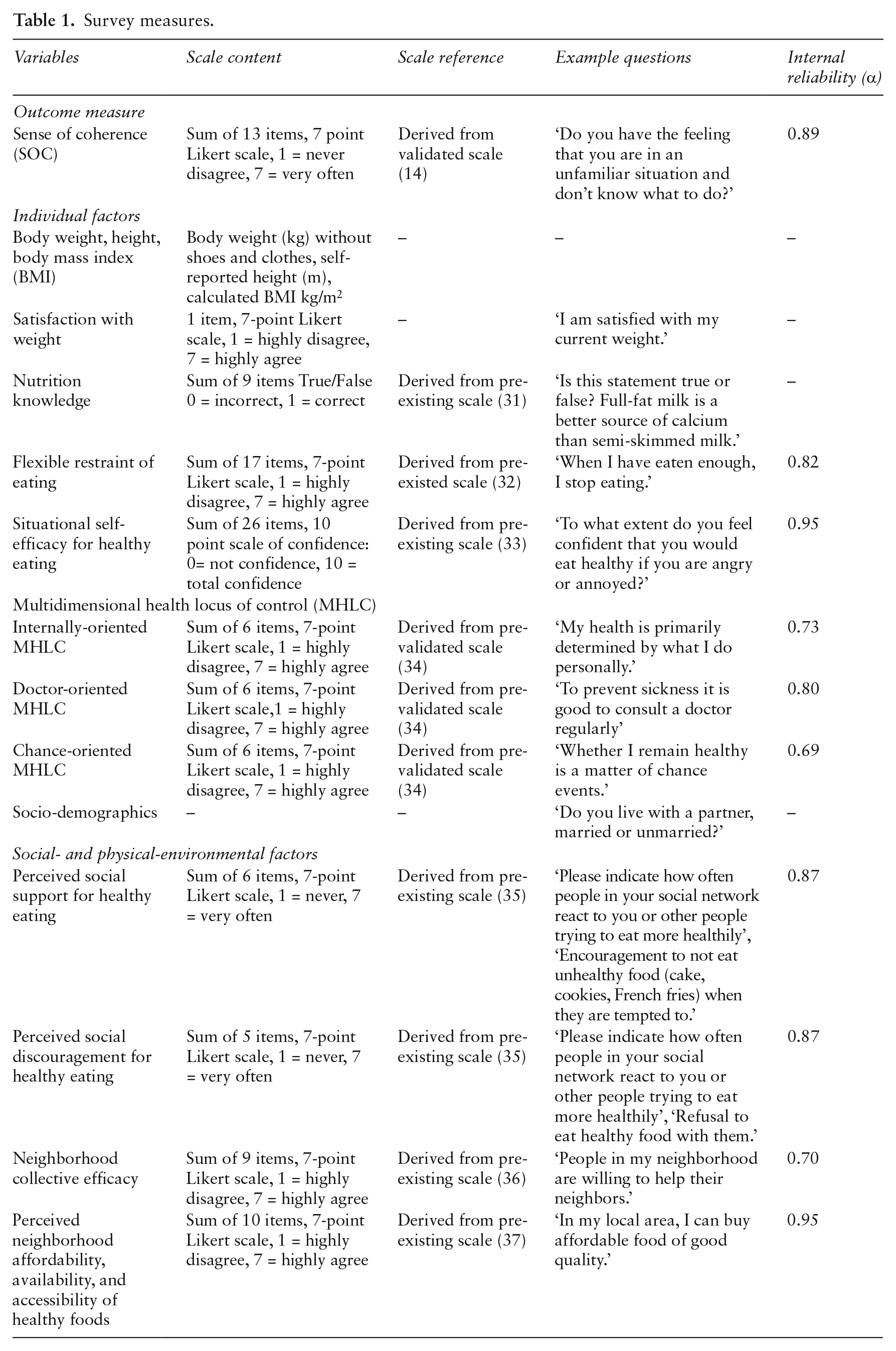
The constructs and their related definitions are given below:
Outcome measure
Sense of coherence (SOC) is a key concept the salutogenic framework to health development and is defined as an ‘orientation to life’. A high SOC makes it easier for people to perceive their lives as consistent, structured and understandable. Participants’ SOC was measured using the Dutch version of the validated English SOC-13 item scale (SOC-13) (14).
Individual factors
Weight data. Data were available on participants most recently measured weight in kilograms (kg) and body mass index (BMI).
Satisfaction with weight. Respondents’ body satisfaction was measured with one item that asked how satisfied respondents are with their current weight.
Nutrition knowledge in this study was defined as how well participants understand the relationship between nutrition and physical health. The nutrition knowledge scale used for this study asked participants to respond with either true or false on statements regarding consumption of different food items and its impact on physical health (31).
Flexible restraint of eating is defined as a balanced and sensible approach to dietary intake that includes flexible restraint behaviors such as eating slowly and taking small helpings (32).
Situational self-efficacy for healthy eating measures one’s confidence in carrying out healthy eating under a variety of circumstances and impediments (33).
Multidimensional health locus of control (MHLC) refers to the extent that individuals feel to have control over their own health either internally (e.g. my health is decided by my own actions), or externally through doctors (e.g. doctors determine my health) or by chance (e.g. whether I remain healthy is a matter of chance events) (34).
Social-environmental factors
Social support and discouragement of healthy eating defined in our study as the perceived levels of support or sabotage for healthy eating that participants observe in their everyday social contexts, e.g. at home, work, social engagements (35).
Neighborhood collective efficacy. This construct encompasses two main elements: perceived social cohesion and informal social control present in a neighborhood. It describes the willingness of community members to look out for one another (36).
Physical-environmental factors
Perceived neighborhood affordability, availability, and accessibility of healthy foods measures perceived ease or difficulty experienced in undertaking healthy eating in local environments in terms of affordability, availability, and accessibility (37).
Socio-demographic factors
Data were collected about participants’ gender; age; whether or not they live with a partner (married or unmarried); income level (in Euros); and highest level of education (elementary school, high school, vocational school, university degree).
Statistical analysis
Data were analyzed using SPSS 19.0 for Windows (SPSS, Chicago, IL). The internal reliability was tested by calculating Cronbach’s α of each individual survey scale. Firstly, linear regression analysis was performed to determine associations between individual, social-environmental, and physical-environmental factors, with the SOC-13 score as the dependent variable. Multiple logistic regression analysis was subsequently performed to assess the association between individual, social-environmental, and physical-environmental factors and the outcome measure SOC. Based on the median 50th percentile mark of scores, participants’ SOC-13 scores were stratified into either low SOC (score of ≤67, n = 395) or high SOC (score of 68 or higher, n = 386) groups for the multiple logistic regression analysis. SOC was examined as a dichotomous variable since previous research examining SOC and health outcomes (38), and healthy eating practices (13), also examined it as a dichotomous variable and we were interested to confirm these findings and see if a high SOC would also be related to the individual, social-environmental, and physical-environmental factors in a Dutch study population. Only factors that were found to be statistically significant (p < 0.05) in the linear regression analysis were entered into the multiple logistic regression model.
Results
The mean age of respondents was 55 years and 55% were male and 45% were female. The mean BMI was 25.5 kg/m2, which falls in the overweight category based on the international classification status of BMI. The majority of respondents (75%) reported that they live with a spouse or significant other. For the highest level of education completed, 34% reported high school, 27% reported vocational school and 32% reported university. The mean net monthly income in euros was €2842.
Table 2 shows the results from the linear regression analysis. For the individual factors, the following variables were positively correlated with SOC: satisfaction with weight, flexible restraint of eating, situational self-efficacy for healthy eating, age, living with a partner, educational level and monthly income. Moreover, doctor-oriented MHLC was inversely correlated with SOC. For the social-environmental factors, perceived social discouragement for healthy eating was inversely correlated with SOC whereas neighborhood collective efficacy was positively correlated with SOC. The physical-environmental factor of perceived affordability, accessibility and availability of healthy foods was also positively correlated with SOC. The following factors were not significant: sex, BMI, nutrition knowledge, internally oriented MHLC, chance oriented MHLC, and perceived social support for healthy eating.
Linear regression analysis investigating association between SOC-13 score and individual, social-environmental and physical-environmental factors for respondents (n = 781).

Abbreviations: MHLC – multidimensional health locus of control, BMI – body mass index (kg/m2), *Significance < 0.05; **Significance < 0.0001.
Table 3 shows the results from the multiple logistic regression analysis. In total, eight of the ten individual, social-environmental, and physical-environmental factors entered into the model were statistically significant. For the individual factors, those with a high SOC were more likely to have a higher situational self-efficacy for healthy eating, have a higher satisfaction with weight, have a lower doctor oriented MHLC, be older in age, and report higher monthly incomes. For the social-environmental and physical-environmental factors, those with a high SOC were significantly more likely to perceive lower social discouragement for healthy eating, perceive higher neighborhood collective efficacy, and perceive higher neighborhood affordability, accessibility and availability of healthy foods. Flexible restraint of eating and education level were not statistically significant in the model. The logistic multiple regression analysis with SOC delivered an explained variance of between 20.5% (Cox and Snell R square) and 27.4% (Nagelkerke R square). The Omnibus Tests of Model Coefficients showed that the full model containing all the predictors was statistically significant, X2 =179.533, (9, n = 781), p < 0.00001. This indicates an acceptable goodness of fit in the model and that it was able to distinguish between respondents reporting a high and a low SOC.
Multiple logistic regression analysis with odds ratios (OR) and 95% confidence intervals (CI) for low and high SOC score and individual, social-environmental, and physical-environmental factors of respondents.
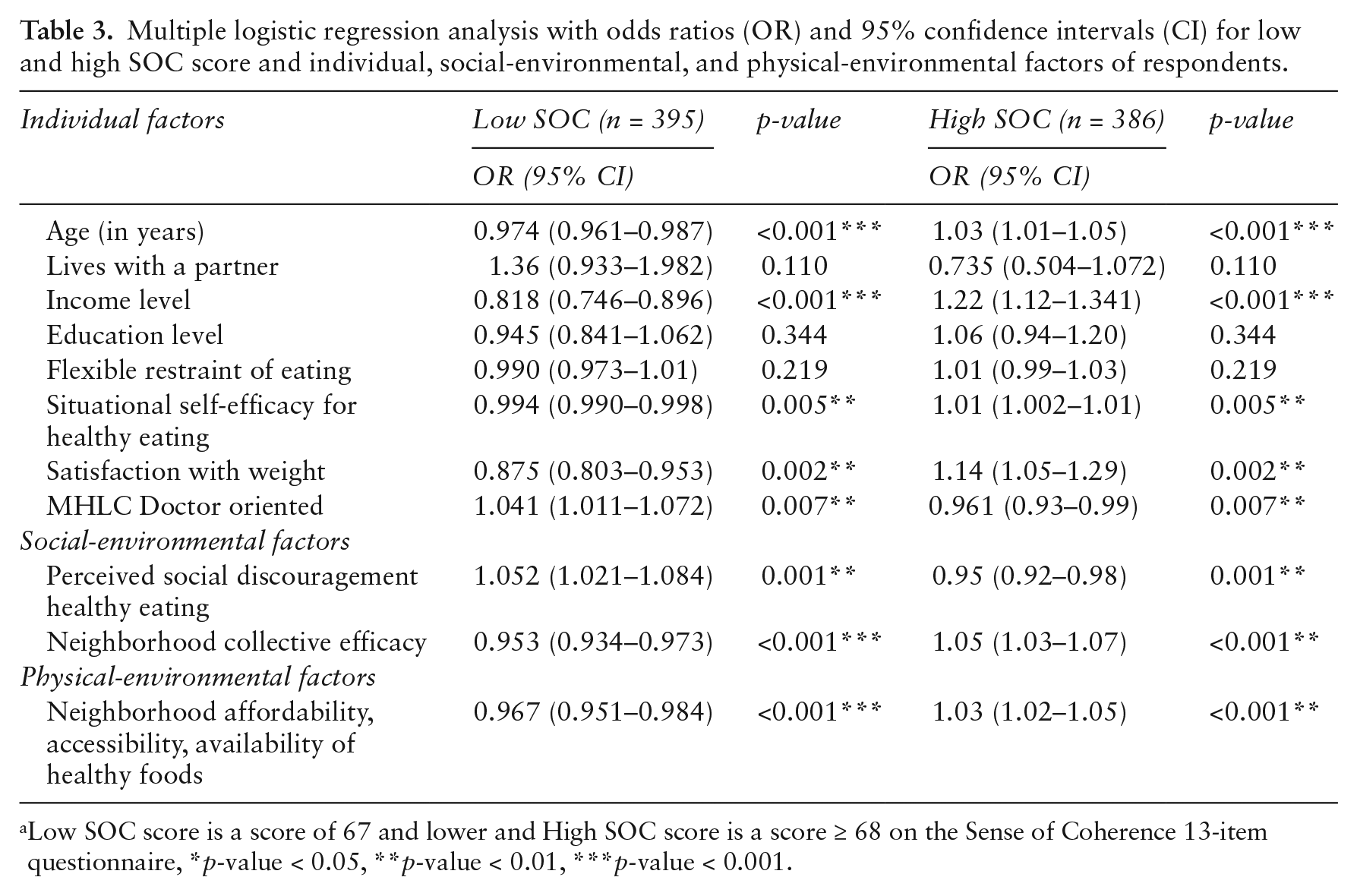
Low SOC score is a score of 67 and lower and High SOC score is a score ≥ 68 on the Sense of Coherence 13-item questionnaire, *p-value < 0.05, **p-value < 0.01, ***p-value < 0.001.
Discussion and conclusion
Our study brings forth new and significant findings since it is the first to identify a number of individual, social-environmental, and physical-environmental level factors that relate to SOC. The relationship between a limited number of factors including socio-demographic characteristics and living and working conditions and SOC had been explored in previous research; however, it was not known whether other factors also underlie SOC. Specifically, SOC was positively correlated to individual, social-environmental, and physical-environmental characteristics including satisfaction with weight, neighborhood collective efficacy, age, and income level and negatively related to doctor-oriented MHLC. Furthermore, SOC was positively correlated to a number of individual, social- and physical-environmental characteristics with a specific food or eating-related component including situational self-efficacy for healthy eating and perceived neighborhood affordability, accessibility and availability of healthy foods and inversely correlated to social discouragement for healthy eating. The findings are relevant as they shed light on the types of factors that health promotion should consider when developing interventions to strengthen SOC.
The factors of relevance we found can be referred to as generalized resistance resources (GRRs) (14). Specifically, Antonovsky described GRRs as physical, biochemical, material, cognitive, emotional, attitudinal, interpersonal, or macro sociocultural characteristics of an individual or group (14). The stronger a person’s SOC, the greater his or her ability to identify and use GRRs in a health-promoting manner (39). It is this reciprocal process that enables people, when under the threat of various stressors, to use GRRs in a health-promoting way and therefore supports them to have a healthy life orientation (40).
Our findings are important since they shed light on the types of resources that health promotion should consider when developing interventions to strengthen SOC. However, it is important to consider that this is not as straightforward as providing a set of GRRs to strengthen SOC. For instance, such an intervention may run the risk of only benefiting those with a high SOC who are more likely to mobilize GRRs for their health, whereas those with a low SOC will not and remain in ill health. This could even perpetuate the widening gap in health inequalities. Therefore, this will require further considerations. For instance, empowerment, which is a supporting process whereby groups or individuals are enabled to change a situation, given skills, resources, opportunities and authority, could be seen as a tool for the enhancement of SOC (18,41). Furthermore, governmental policies should focus on enabling participation in life experiences that allow people to identify and apply resources to support SOC. Participation is widely recognized in health promotion and one of the most fundamental elements that stands central to the empowerment concept (41). Yet current nutrition promotion efforts insufficiently allow for active involvement of people themselves. Therefore, there is a need for change in expert-driven approaches towards a co-evolutionary development process. Through this, policy makers can identify sustainable GRRs that take advantage of the community’s existing resources, which enable active involvement and participation, and empowerment.
It should also be noted that although social discouragement for healthy eating was inversely associated with SOC, social support for healthy eating was not associated. This is an interesting finding, particularly given that social support plays such a large role in promoting health. Future research should examine this relationship further as the reason for this outcome is not entirely clear.
Previous studies in Finnish and Japanese populations have found that being married or living with a partner contributed to a strong SOC (27,28), but this was not the case in our study population. However, the quality of this relationship is probably what contributes more to SOC than partnership status alone. Volanen et al. found that those perceiving a poor relationship with their spouse or partner had a low SOC (28). Due to limitations in the number of survey items, we were only able to ask whether the person lived with a partner and not about the nature of the relationship.
Antonovsky theorized that SOC is developed until 30 years of age and thereafter it remains relatively stable until retirement, after which it decreases (14). However, findings from longitudinal studies have suggested that SOC can be subject to change in adulthood (42,43). Future longitudinal research should examine this further by tracking the growth and stability of SOC over the life course, from early childhood into adulthood. In addition, Antonovsky proposed that SOC is developed and shaped through meaningful and coherent life experiences (39). Future research should study those with a high SOC and explore the breadth and nature of these experiences in relation to food, eating and health.
This study has a number of strengths. The survey instrument designed for this study included an extensive number of diverse factors. Further strengths included the study’s significant sample size, a high survey response rate of 94% and the use of pre-tested, validated scales to measure the constructs in our survey instrument. Another strength was that the survey instrument had a good to excellent internal reliability and performed well indicated by the Chronbach’s α scores ranging from 0.69–0.95.
It is important to mention that due to the cross-sectional nature of this study, we are not able to make conclusions in regards to cause and effect relationships. Future studies should be carried out in different populations and contexts, particularly given the fact that Antonovsky argued that factors underlying SOC can differ from culture and context (14). The explained variance of the logistic regression model of between 20.5% and 27.4% was not strong but moderate. However, given the exploratory nature of this study, such a value was expected. Ideally we would have included more factors in the survey instrument but we were restricted in the number of survey items that could be asked to the research panel. Future research should examine a wider number of factors to see whether or not these could be of further relevance in explaining SOC.
In conclusion, our study brings forth new insights because it shows that GRRs arising from the individual and the social and physical environment relate to SOC. Advancing knowledge of GRRs that shape SOC is important as it can inform the development of health promotion interventions that strengthen SOC. This study’s findings also complement what is already known from biomedical research models by bringing forth new knowledge of the complex, multidimensional factors that can contribute to a healthy orientation to eating and life. Future nutrition research should consider integrating both salutogenic and biomedical approaches within research methodologies in order to gain a more complete picture of factors driving both healthy and unhealthy eating practices. Furthermore, this study’s findings provide the impetus for the further application of the salutogenic framework within health promotion research to gain deeper understanding of how these factors contribute to a healthy life orientation.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received funding from the Dutch Dairy Organization (NZO) and Wageningen University.