
Abstract
In an era characterised by the adverse impacts of climate change and environmental degradation, health promotion programmes are beginning to actively link human health with environmental sustainability imperatives. This paper draws on a study of health promotion and sustainability programmes in Australia, providing insights to evaluation approaches being used and barriers and enablers to these evaluations. The study was based on a multi-strategy research involving both quantitative and qualitative methods. Health promotion practitioners explained through surveys and semi-structured interviews that they focused on five overarching health and sustainability programme types (healthy and sustainable food, active transport, energy efficiency, contact with nature, and capacity building). Various evaluation methods and indicators (health, social, environmental, economic and demographic) were identified as being valuable for monitoring and evaluating health and sustainability programmes. Findings identified several evaluation enablers such as successful community engagement, knowledge of health and sustainability issues and programme champions, whereas barriers included resource constraints and competing interests. This paper highlights the need for ecological models and evaluation tools to support the design and monitoring of health promotion and sustainability programmes.
Keywords
Introduction
There is a plethora of evidence that underscores the negative human health impacts of climate change and environmental degradation (1,2). Leading health and environmental science authorities, including the Intergovernmental Panel on Climate Change and World Health Organization (3,4), identify multiple social, economic and environment consequences of climate change and impacts on global burden of disease. The association between poor health outcomes related with degraded environments exacerbate existing health inequities evident in low-income and disadvantaged communities (4,5).
Since the 1980s, Western constructs of health have evolved from purely medical origins, shifting to approaches that recognise environmental and social determinants of health (6). Health promotion mandates have supported this, as is evident in the Ottawa Charter for Health Promotion and the Bangkok Charter of Health Promotion in a Globalized World (7,8). The Ottawa Charter advocated for stable ecosystems and sustainable resources to inspire a holistic, inter-sectoral approach to health (7). One theoretical framework moving towards a holistic, systems thinking and sustainability imperative is the ecological model of health, encapsulated within the Mandala of Health Model (9). This model emphasises the intertwining of natural, medical and social sciences and their impacts on individuals and communities (10). Health from an ecological perspective acknowledges that the health of individuals and communities are dependent upon the health of the planet (11).
Despite critiques that health promotion has not fully embraced an ecological perspective (12–14), there is evidence to suggest the field is engaging with relevant global environmental and social challenges and strategies like participatory governance, risk assessment and inter-sectorial partnerships (15–17). As such a paradigm appears to be emerging, that recognises the significance of our ecosystems (18,19), which may be broadly defined as ecological health promotion, public health ecology or ecosystem approaches to health (20–22). Within this paradigm, strategies to promote environmental sustainability are seen as integral to promoting human health, equity and wellbeing (23,24).
However, to date there is scant documentation of where health promotion and environmental sustainability have merged and therefore embraced these ecological perspectives in practice and within planning and evaluation processes. Research in Australia has documented the benefit of the merging of health promotion and sustainability programmes (23–25). This research demonstrated that community level health promotion practitioners are endeavouring to incorporate concerns for the environment, in particular climate change, into their practice. This research also revealed a number of barriers to this work, including: a limited evidence base for effective health and sustainability strategies; a lack of health and sustainability planning and evaluation tools ; and practitioner knowledge of relevant evaluation indicators and measures (23).
This paper identifies health promotion and sustainability programmes across Australia, highlight-ing the evaluation approaches being used and barriers and enablers to evaluating such initiatives. The paper aims to stimulate thinking and debate about the extent to which ecological models are guiding health promo-tion practice and evaluation design.
Methodology
This study, which was guided by the principles of ethnography (26), applied multi-strategy research combining both quantitative and qualitative methods (27). This approach enabled data triangulation and an understanding of programme evaluation strategies being applied within health promotion and sustainability programmes at a community level in Australia (28). The research project was conducted with approval of the Human Research Ethics Committee (Human Research Ethics Committee of Deakin University: Code H96_2013).
Purposeful sampling strategies, namely snowball and maximum variation sampling, guided participant recruitment. Snowball sampling leverages existing networks to recruit study participants was appropriate given the database of contacts developed in the author’s previous studies (29). Maximum variation sampling supported the researchers in attempting to gain the widest range of participant diversity in the sample population (i.e. participants working in different types of agencies, settings and geographical locations of Australia), and because it has been recommended for health promotion research (28). Participation in the survey and interviews was open to health promotion practitioners delivering health and sustainability programmes at the community level in Australia.
Survey
The survey was a cross-sectional design (28,31), developed from the variables and patterns identified within the authors qualitative case study research previously implemented in Victoria, Australia (references withheld). The survey design was based on a combination of structured, semi-structured and demographic questions (32). The survey instrument was pre-tested by five colleagues (fortnightly over two months) to check for meaning and measure its effectiveness in responding to the aims of the study. The pre-test participants included three academics with qualifications in ecological health promotion and experience working in the sector and two health promotion practitioners working in the sector. The 23 questions were structured across five themes: consent to participate; demographic information; organisational priorities; programme profiles; and evaluation tools and indicators. Once all inter-observer reliability tests were complete the final 23-question survey instrument was launched via Survey Monkey.
Survey participants were recruited via the research team’s existing database of health and sustainability professional associations in Australia. Working from an initial list of thirty, the researchers contacted each association to request that they distribute the survey to their membership list. Fifteen organisations/associations agreed to distribute the survey, including the national and state level branches of the professional associations working in the health promotion and public health space. The survey was open online for eight weeks with 82 individuals participating in this component of the study. The final sample consisted of:
Gender: 21 males; 61 females
Age ranges: 4 (18–25 years); 28 (25–35 years); 16 (35–45 years); 19 (45–55 years); 13 (55–65 years); 2 (65+)
Locations: 33 Victoria; 17 New South Wales; 10 Queensland; 2 Australian Capital Territory; 6 Tasmania; 6 Western Australia; 4 Northern Territories; 4 South Australia
Agency types: 33 non-government (e.g. primary health care agencies); 34 government (e.g. local government); 15 other (including health and sustainability consultancy).
After the data collection period the data was cleaned, tested on SPSS and Excel. Due to a statistically low number of participant responses (and a decline in response rate as the survey progressed) the data was handled as and used for descriptive purposes only to develop a broader understanding of the topic. The results were analysed, coded in tables and for participant quotes, NVivo was applied.
Interviews
Semi-structured interviews were applied to strengthen the survey results and build a richer picture of health and sustainability programmes and evaluation approaches. Potential interview participants were identified via three mechanisms: invitation to participate at the end of the survey; through direct contact with potential participants from the researchers’ existing database; and referrals from other participants. Twenty participants were contacted in order to assess their interest and suitability for participation, with 11 interviews undertaken. Although the sample was intended to be nationwide participants were all from eastern states. The participant profiles consisted of:
Gender: 5 males; 6 females
Age ranges: 3 (25–35 years); 6 (35–45 years); 2 (45–55 years)
Locations: 6 Victoria; 2 New South Wales; 2 Queensland; 1 Australian Capital Territory
Agency types: 4 non-government; 5 government; 2 other.
Eight interviews were undertaken via telephone and three face-to-face at the participant’s agencies. The semi-structured interview schedule included demographic and open-ended questions to understand the experiences of participants. The interview questions were structured around five themes: participant demographics; current or planned health and sustainability programmes; evaluation activities/tools for these programmes; barriers and enablers to programme evaluation; and evaluation framework recommendations. All interviews were audio-recorded and transcribed verbatim. De-identified transcripts were then sent to individual participants for ‘member checking’ (31). Transcripts were then uploaded too and analysed within NVivo.
The analysis was guided by techniques used in ethnographic analysis, for example, the identification of ‘patterned regularities’ and ‘rich points’ (33). Wolcott’s ethnographic framework for data analysis was applied (26), including description, analysis and interpretation. The description stage involved developing a profile of each programme and the evaluation techniques being used by reading transcripts, highlighting themes and making notes. The analysis stage highlighted themes based on ‘patterned regularities’ emerging from the various data sources (33), including overarching programmes types. This process resulted in the identification of several ‘rich points’ (e.g. contradictions, departures from expectations, repackaging of ideas and repetition) (33), which were considered to inform the findings. These findings were then represented as a thematic narrative supported by participant quotes.
After analysis of the qualitative component was completed the data from the survey and interviews was triangulated using thematic and content analysis (28,29). The outcome was a representation of the programmes and evaluation approaches being used within Australia through a narrative, replete with tables and participant quotes. In the interpretation stage, the triangulated data was considered in relation to evaluation and health promotion literature.
Results
Programme types
The interview and survey data revealed five overarching health and sustainability programme types in Australia:
Sustainable and healthy food (community gardens; food co-operatives; farmers’ markets; and food security initiatives);
Active transport (cycling and walking initiatives in schools, workplaces and public housing estates; and cycling infrastructure/policy);
Energy efficiency (household and organisation energy efficiency programmes; renewable energy; and greenhouse gas (GHG) emission reduction campaigns);
Contact with nature (green volunteering; environmental stewardship initiatives; and health promotion in open space); and
Capacity building (partnerships; and workforce/organisational development).
Five survey questions prompted descriptions of these programmes and the interviews provided the context. The results indicated that populations targeted were based on variable geographies (urban, rural and regional), age (children and the elderly) or socio-economic status (public housing residents). ‘Geographical community’ was the primary setting but some participant’s specified schools, workplaces or health services. Strategies spanned risk assessments and traditional community level ‘midstream’ health promotion approaches like behaviour change, education and training. ‘Upstream’ interventions including community action, policy development and advocacy were also described.
Evaluation approaches
The survey revealed that most evaluations of health and sustainability programmes were conducted in-house by programme staff (48%). Approximately 29% of programme evaluations were undertaken by academics from research institutions, 14% by evaluation consultants and 19% led by the community. Interview participants indicated a similar range of inputs to evaluation. One participant highlighted the complexity and variability surrounding who leads these evaluations:
Typically get an independent third party to do it, a research institution like a university, or occasionally a consultancy. There were some that we did in-house when we didn’t have the required resources to engage a research institution. (Practitioner 5)
The research highlighted that surveys were the most popular evaluation tool followed by qualitative approaches like interviews, case studies and administering focus groups. Participatory research techniques (characterised by active involvement of programme participants in research planning, design and outcomes) were used by 38% of the survey respondents. This quote from a practitioner highlights multiple methods were often applied:
We use a mix of pre and post surveys, participant interviews or sometimes focus groups. We are now starting to look more to participatory methods. (Practitioner 3)
Survey questions demonstrated that most evaluations were mixed methods. The majority of participants reported the collection of quantitative data (86%) followed by qualitative data (69%) and case studies (62%). Anecdotal evidence (48%), document reviews (43%) and narratives (38%) were also popular whereas only 17% of data was collected on a longitudinal basis. The survey questions identified the types of indicators used in these evaluations (Table 1) with demographic, health and social indicators prioritised over environmental and economic indicators.
Indicators used in health and sustainability programme evaluations.

The interview data also established the range of key indicators and tools being used to evaluate health and sustainability programmes. Common to all interviewees testimonies were the use of ‘process’ (reach of the programme, participant satisfaction) and ‘impact’ (short to medium term effects on humans and environment) indicators. This participant quote demonstrates that programme logic was a popular tool:
Our evaluations are guided by programme logic because it’s still the preferred framework. (Practitioner 1)
Table 2 demonstrates the methods being used by participants as categorised by five overarching programme types. Table 2 suggests that the common method for evaluations were surveys that measured participation and satisfaction rates along with changes in behaviour and knowledge.
Programme type versus evaluation methods and indicators used.

Barriers and enablers to programme evaluation
In both the survey and interviews, participants were asked to identify barriers and enablers to health and sustainability programme evaluations. In the survey the key enablers were: ‘interest from the community, agency, partners, team’ (61%: n = 50); ‘knowledge and awareness of key health and sustainability issues’ (59%: n = 48) and ‘programme champions’ (50%: n = 41). The major barriers to evaluation were ‘resource constraints’ and ‘competing priorities’ (83%; n = 68). Participants were unsure whether ‘understanding of climate science’ (46%; n = 38) was an enabler or barrier to evaluation. ‘Planning/evaluation tools & frameworks’, ‘evidence base’ and ‘organisational mandate to do this work’ were factors that were primarily considered as enablers but none-the-less more evenly spread across ‘not sure’ or ‘barrier to evaluation’.
The interview participants’ responses elicited more detailed explanations of the conditions that support evaluation. Table 3 highlights themes that emerged with indicative quotes (refer parenthesis). The table demonstrates interview participants oscillated between describing generic barriers and enablers to health promotion evaluation and more specific challenges of the nexus between health promotion and environmental sustainability programme evaluation work.
Enablers and barriers to evaluation of health promotion and sustainability programmes.
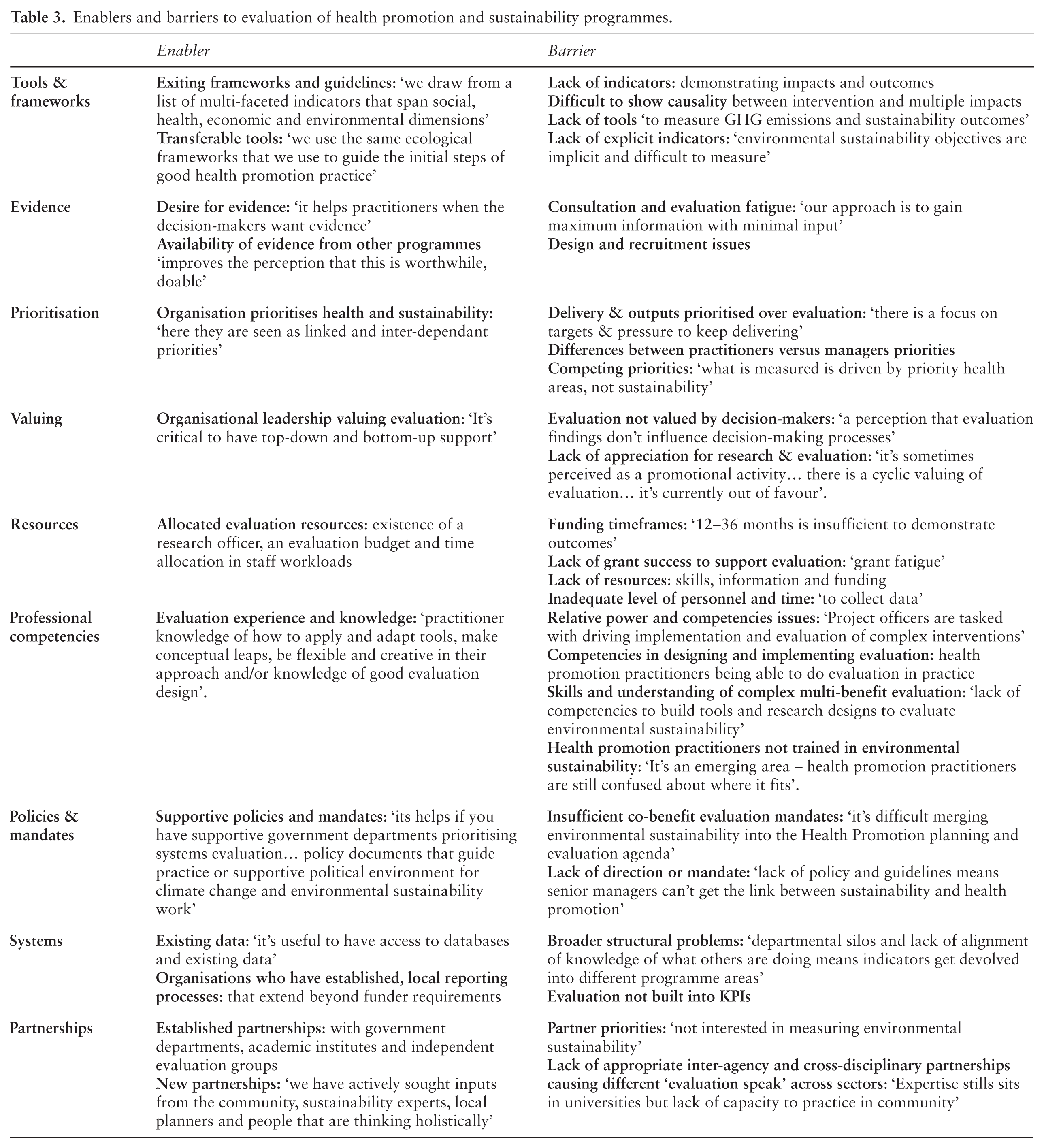
Table 3 suggests there are multiple barriers to evaluation that sit outside of the current influence of health promotion practitioners. For this work to become embedded, larger scale system/structural level barriers need to be overcome. The findings emphasise the need for greater collaboration across sectors and disciplines.
Discussion
The study illustrated in ecological health promotion practice there were five overarching programme types through which practitioners were engaging with individuals, communities and systems that applied biomedical, lifestyle and social-environmental approaches (34). This research was consistent with previous studies (23,24,35,36), which emphasised that community-level health promotion programmes were beginning to address sustainability and climate change imperatives, however, there were barriers to this incorporation. These same barriers make evaluation of these initiatives challenging.
Practitioners in the study were transferring or extending existing health promotion frameworks, including evaluation mechanisms, to support work at this nexus. The evaluation tools (surveys, interviews, observations) and methods (qualitative, quantitative, experimental, participatory) were atypical of the diversity and richness of conceptualisations and methods currently used in health promotion evaluation (37). Evaluation designs reflected the plurality of accepted practices in the field of evaluation and those applied in the complex and value-based practice of health promotion (37). Not surprisingly, given its status in Australian government evaluation practice and within public health traditions, the programme logic-based approach to programme evaluation was a commonly used framework. Participants also reported the routine collection of demographic information and the use of traditional health promotion impact indicators linked to physical, mental and social health.
Perhaps more pertinent though, was that participants testified to grappling with ‘sustainability’ indicators (Table 1) conveying their endeavours to build in ‘environmental domains’ into their health and sustainability programme evaluations. This was significant given calls by ecological public health practitioners, Brown and colleagues (38), to observe the complex and interactive health-environment system over time, allowing for feedback throughout the programme delivery (formative evaluation) as well as evaluation of the final outcome (summative evaluation). Notably some participants in the study were actively fostering new partnerships, bringing together multiple experts and community stakeholders in an attempt to devise a more holistic set of programme indicators. These practitioners were doing what numerous authors believed was essential when working in the nexus of health and sustainability (21,24,38), i.e. incorporating different constructions of knowledge through constructive collaboration and the development of socio-ecological based evaluation frameworks which more adequately embrace complexity.
Worthy of note was the fact that in their endeavours to organise the complexity, participants were plagued by familiar concerns for ‘certainty’ in collecting evidence, in that they prioritised deductive thinking in an attempt to quantify programme results (38). These were considered existing barriers to evaluation and the participants’ opinions were consistent with the argument that there are numerous methodological issues inherent to the health promotion evaluation that reach beyond the normal problems of programme evaluation (37). Participants testified to multiple barriers (Table 3), which were further complicated by the new layer of complexity presented by designing and resourcing programme evaluation at the nexus of health and sustainability. Participants implicitly acknowledged that existing approaches to evaluation fall short in addressing future-oriented and complex problems – which is characteristic of health and sustainability work (38).
There were various enablers identified in this study. The main enablers included: stakeholder interest/understanding of key issues and evaluation design; programme champions willing and able to make the conceptual leaps; and practitioners committed to working collaboratively with diverse stakeholder. The enablers identified were also consistent with research (23,36) that found a range of enablers across the health system (individual professional competencies through to supportive government policy) were required to positively reinforce programme planning and evaluations.
A strength of the present study was that it provided a snapshot of health and sustainability programs in Australia by using a mixed methods approach. Conversely, limitations of the study were that the authors were unable to obtain an overall response rate for the survey; and ensure representation nationwide (the findings were skewed to eastern states). The study findings would have been strengthened had the study been able to garner the views of practitioners equally across Australia.
Conclusion
It is promising that health promotion practitioners in Australia are engaging with health and sustainability issues. However, this study identified a triple layer of difficulty in evaluation practice (conducting basic evaluation is difficult and when coupled with health promotion and then sustainability, it becomes more complex) and the need for holistic ecological models to guide practice. Even with compelling scientific evidence and the emergence of ecological health promotion, there is no codebook to guide early adopters. Practitioners are faced with the monumental task of problem-solving and solution generation for complex health and sustainability issues inside a system oriented toward linear thinking and single issue approaches. To achieve the necessary shift in practice, there needs to be continued commitment to developing holistic ecological models that are both theoretically sound and can be readily applied to support practice. This could be enabled through increased engagement between health promotion and sustainability practitioners and the development of evaluation tools to support monitoring of community level programmes.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Teresa Capetola, Rebecca Koss and the research participants.
Conflict of interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by Deakin University’s Faculty of Health.