
Abstract
Sex education in schools is an adolescents’ right, and can have health benefits, such as improved knowledge or increased condom use. In Asturias, a secondary school programme called Neither Ogres Nor Princesses educates pupils for four years with trained teaching staff and external workshops. This study examined whether this programme (a) improved adolescents’ sexuality knowledge, attitudes and skills, and (b) increased condoms use. A quasi-experimental survey was conducted, with comparison arm, with a pre-test in the first year of secondary school (12- to 13-year-olds), and two post-tests: after the intervention (15- to 16-year-olds) and two years later (17- to 18-year-olds). A questionnaire with socio-demographic, knowledge, attitude, skill and sexual behaviour variables was used. The impact was evaluated with ‘difference-indifferences’ analyses. There was a greater increase of knowledge in the intervention arm in both post-tests, and an increase in skills in the first post-test. Girls in the intervention arm reported less practices with penetration and greater condom use the first time, this also among boys. However, the impact was limited in time. Interventions that aim to increase sex education in curricula with quality and fidelity are a priority to guarantee children’s rights and their health.
Introduction
Sexual health, as defined by the World Health Organisation (WHO), is ‘a state of physical, mental and social well-being in relation to sexuality’, with ‘a positive and respectful approach, as well as the possibility of having pleasurable and safe sexual experiences’ (1). Additionally, sexual health among adolescents is crucial for their wellbeing and for global health. Globally, young people are at elevated risk of sexually transmitted infections (STIs) and unintended pregnancy through unprotected sexual intercourse (1); for example, worldwide, young people aged 15–24 represent nearly 20% of new HIV infections (2). In Spain, the highest incidence rates of HIV cases are found in 25- to 29-year-olds (3) and abortion occurs more commonly in women around 20–24 years of age (4). In light of this situation, there are effective interventions to reduce these risks (5, 6), such as sex education (7), which is a sexual right, recognized by international organisations (7, 8).
There is strong evidence to support that school sex education programmes can delay first intercourse and/or increase the use of condoms and other contraceptive methods, which as a result reduces STIs and unintended pregnancies (5–7, 9–11).
Sex education with a ‘rights and gender’ approach, which presents sexuality as a positive human value and source of pleasure, and with a gender and empowering perspective (7,12–14), is internationally recognized as being effective (7, 12–15).
At the same time, the United Nations Sustainable Development Goals (SDGs) prioritise sex education as a strategy to promote gender equity and sexual and reproductive health (16). The SDGs, signed by 193 countries in 2015, set 169 goals for 2030, some related to sex education, and which all the signatory countries, including Spain, should fulfil. There is, therefore, a commitment to the implementation, evaluation and extension of sex education programmes, adapted to each context, contributing to the fulfilment of the SDGs.
In Spain, this commitment has a legal framework (17), which establishes sex education in schools. However, several studies show that this is not effectively or universally incorporated (18–20). Proposals for its implementation are based on voluntary and external work (no mandatory job), and most of them eventually disappear (19). As an example, in our country, only 14% of schools have given their teachers training in sex education during the last 3 years (21).
In Asturias, since 2008, the Regional Ministry of Health promotes a sex education programme called Neither Ogres Nor Princesses (NONP) (22). Based on a rights and gender approach (13), this intervention seeks to generate conditions for people to make autonomous responsible decisions, and promotes that they can exercise their rights, fulfill their responsibilities and respect the rights of others. The program addresses knowledge, attitudes of respect and training of social and specific skills in relation to sexuality, in order to promote healthy and respectful behaviors. This programme was designed based on other effective programmes (7, 14) and targets pupils aged 12 through 16 who receive sessions taught by their teachers during compulsory secondary education (from 1st year to 4th year). Teachers receive 12 h of training beforehand and have the support of a didactical guide, with participative and active sessions to work in classroom (debates, role-playing, training techniques, etc.). The contents are organized into five thematic blocks: social skills (communication, emotion management, decision making, etc.), affectivity (self-esteem, friendship, family, love, etc.), anatomy and physiology (changes in puberty, menstruation, reproduction, etc.), pleasure and health (sexual practices, consent, prevention, etc.) and identities (gender, feminism, sexual diversity, etc.). The participating teachers assumed the commitment to teach at least 5 h in the classroom for each school year on these contents. Teaching is complemented with 2 h of external workshops per year, except in 4th year, where two students per classroom, previously trained, taught a 3-h workshop to their classmates (‘peers methodology’).
After 1 year of implementation, a process evaluation was conducted pointing out that it was a novel intervention, with a high level of execution, as well as a high level of participation, satisfaction and usefulness perceived both by pupils and teachers (23).
NONP is intended to improve the health and well-being of adolescents, increase self-esteem and personal autonomy, promote freedom of choice through knowledge, and ensure equality between women and men and respect for sexual diversity. Key objectives related to sexuality include increasing facilitators’ knowledge as well as developing positive attitudes and social skills. This aims at the acquisition of pleasurable, healthy, safe and responsible sexual behaviour adopted by young people, which will contribute to reducing STIs and unintended pregnancies.
Research questions
Does NONP (a) improve adolescents’ sexuality knowledge, attitudes and skills; and (b) increase condom use at first and last intercourse?
Methods
Study design
A quasi-experimental study was conducted with pupils who participated in the NONP programme and a comparison arm, using a pre-test, a post-test at the end of the intervention and a post-test in the medium term (2 years later) design.
Sample size was determined for 80% statistical power and bilateral significance of 5%, assuming a 50% prevalence of condom use in the comparison arm in the post-test and minimum significant differences of 10% in the intervention group.
Sampling was by cluster, and intervention schools were selected randomly until the established sample size was reached. In total, there were five secondary schools (out of 21 total with the programme), for which all their 1st year pupils participated. In order to choose controls, comparability was sought in the same context: for each intervention school, another school in the same geographical area that did not participate in NONP or any other sex education programme was randomly selected.
Data collection
Before the intervention (pre-test), the 1st year pupils (12- and 13-year-olds) completed an auto-administered and anonymous survey, previously piloted in four classrooms. Two post-intervention surveys were undertaken by an external team: at the end of the intervention, when the pupils were in 4th year (15- and 16-year-olds); and again in May 2016, 24 months after the intervention, when they were in 2nd baccalaureate year (17- and 18-year-olds). This study was not paired, for reasons of participation, organization and anonymity, and we assumed that the pupils would be the same, with minimal changes. For this reason, in post-tests, pupils who had not previously completed the four grades of secondary school in the same centre were excluded.
Ethical considerations
Ethical approval was granted by the Ministries of Education and Health, and with the consent of the centres’ management teams. Families and pupils were informed of the study and both gave their consent to participate.
Participants
The pre-test included 656 pupils (327 in the intervention and 329 in the control group). For the first post-test, the number of participants was 608 (310 intervention and 298 control) and 371 for the second post-test (186 intervention and 185 control). Response rates for pre-test and post-tests were 96%, 92% and 81%, respectively, with no differences by arm (Figure 1). Non-responses were due mainly to absences. Surveys poorly answered (no response or inconsistencies), which were less than 1% in each arm and at each time, were excluded.
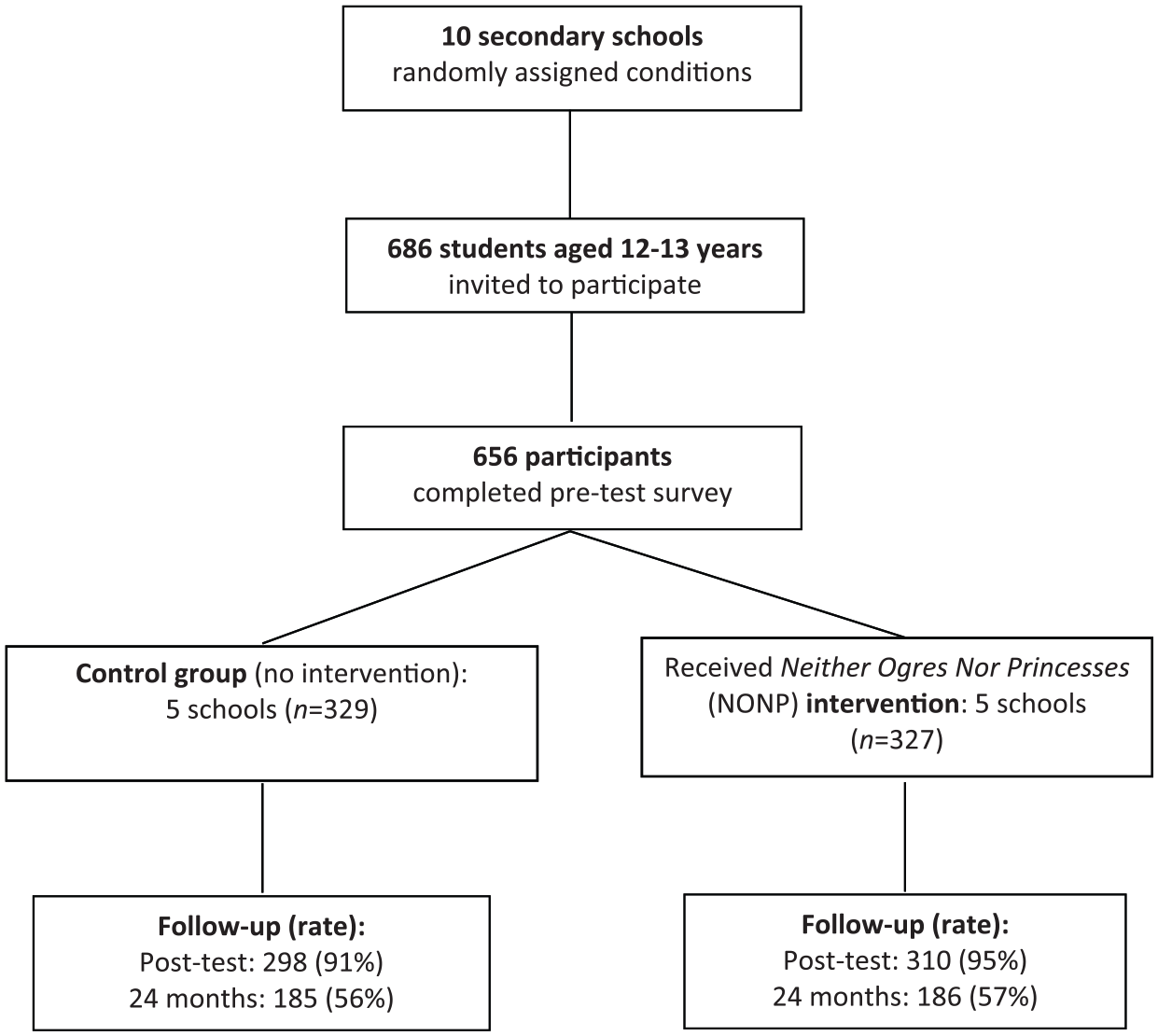
Flowchart for group-randomised, controlled design.
The interventions
Teachers in the NONP programme taught 20.7 h of sex education to their pupils during the 4 years of intervention. In those schools, workshops made up another 7.5 h. In total, pupils received an average of 28.1 h (range: 24–34) of intervention. In control schools, activities during those 4 years accounted for 4.2 h on average, all external (range: 2–8). The information was gathered annually with the collaboration of each school. Sex education included in the curricular contents was not taken into account; it was also assumed that there were no differences by arm.
Outcome measures
The variables were classified in five categories: socio-demographic, knowledge, attitudes, skills (ability to do), and sexual behaviour.
The socio-demographic consisted of gender, age and birth country. The average age of the participants at each intervention phase was 12, 16 and 17.5 years, respectively, with no differences by arm. There were no differences between the intervention and the control arm in relation to the participants’ sex and country of birth.
For the rest of the categories, questions that appeared in other studies were used (24, 25), with 15 items for knowledge (with a choice of a true/false), for attitudes (using a Likert-type scale) and for skills (using frequency scale or ‘yes/no’).
Following the pattern of other studies (26, 27), a total score (out of 10) for knowledge, attitudes and skills was obtained, with the sum of correct/desired responses regarding the following topics: sexuality, equity, sexual diversity, pregnancies and STIs.
Lastly, sexual behaviour variables were: sexual intercourse with penetration (penis in vagina/anus), condom use at first intercourse and condom use at last intercourse (responses ‘yes/no’). These aspects were not investigated in the pre-test, assuming that sexual activity is unusual at that age (24). On sexual behaviour, a declaration of sexual orientation (‘heterosexual’, ‘bisexual’, ‘homosexual’, ‘I don’t know’) was also included.
Analysis
A descriptive analysis was used, with the average and standard deviation for the quantitative variables and the distribution of absolute and relative frequencies for the qualitative variables.
Difference-in-differences (dif-in-difs) analyses were conducted to evaluate the impact of the intervention. Using a dif-in-difs analysis allowed us to simultaneously compare the difference between pre-test and post-tests in the intervention group versus the control group. The differences between the pre- and the post-tests in each group were expressed in terms of odds ratio (OR) and their confidence intervals at 95% (95% CI) obtained in the previous models. The modification of the difference between pre- and post-tests due to the intervention (interaction) was assessed using the difference in coefficients of the time between the groups, and was reported in terms of ratio of OR (ROR) at 95% CI.
In the same way, the global extent of the effect on each category using linear regression models was analysed, using the total score for each category as the dependent variable and the intervention group and time (pre-test or post-tests) in the control group and the intervention group as independent variables. Beta coefficients and their 95% CI were reported as a measure of the differences in the mean for each group, and the differences of these coefficients as a modification of the difference due to the intervention.
Values of p < 0.05 were considered to be statistically significant in all comparisons. The analysis was performed with the statistical software Stata version 14.
Results
Knowledge
There was an increase in knowledge: from 4.8 to 7.0 and 7.8 in the control group, and from 4.1 to 6.8 and 7.7 in the intervention group (Table 1). This increase was greater in the intervention group, with a difference between the groups at the limit of significance in the first post-test (p = 0.053) and significant in the second post-test (p = 0.022).
Knowledge, attitudes and skills.
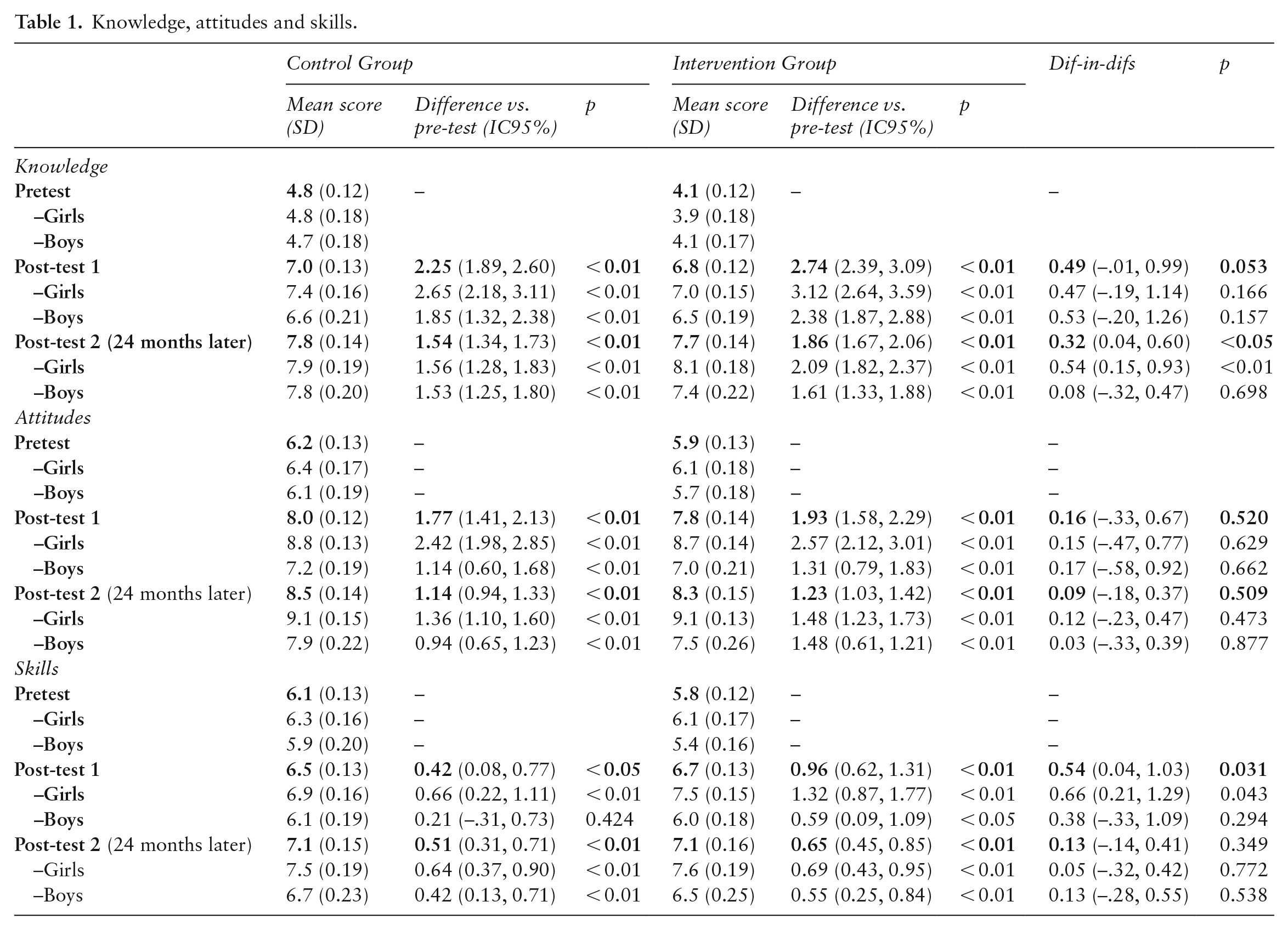
In the analysis by sex, girls in the intervention group started from the lowest average score in the pre-test (3.9) and obtained the highest in the second post-test (8.1), while boys from the same group started from a similar situation (4.1) but reached a lower final score (7.4). In the control group, there were no differences between boys and girls.
Attitudes
There were significant increases in the total score: 6.2 to 8 and 8.5 in the control group; 5.9 to 7.8 and 8.3 in the intervention group (Table 1). This evolution was similar in both groups, without significant differences.
The starting situation was similar in boys and girls, but girls evolved better in both groups, with an average of 9.1 in the second post-test vs. 7.9 for boys in the control group and 7.5 for boys in the intervention group.
Skills
The total score increased in both arms: 6.1 to 6.5 and 7.1 in the control group and 5.8 to 6.7 and 7.1 in the intervention group (Table 1). This increase was greater in the intervention group in the first post-test (p = 0.031).
Boys in the intervention group started with the lowest average (5.4 vs. close to 6.2 for the girls in both groups and 5.9 for boys in the control group) and also obtained the lowest final score: 6.5 in the second post-test vs. 7.6 of the girls in their group (6.7 and 7.5 in the control group, respectively).
Sexual behaviour
Declared sexual orientation was similar in both intervention and control groups at the different times of the study: around 95% of the pupils declared themselves to be heterosexual (Table 2).
Sexual behaviour.
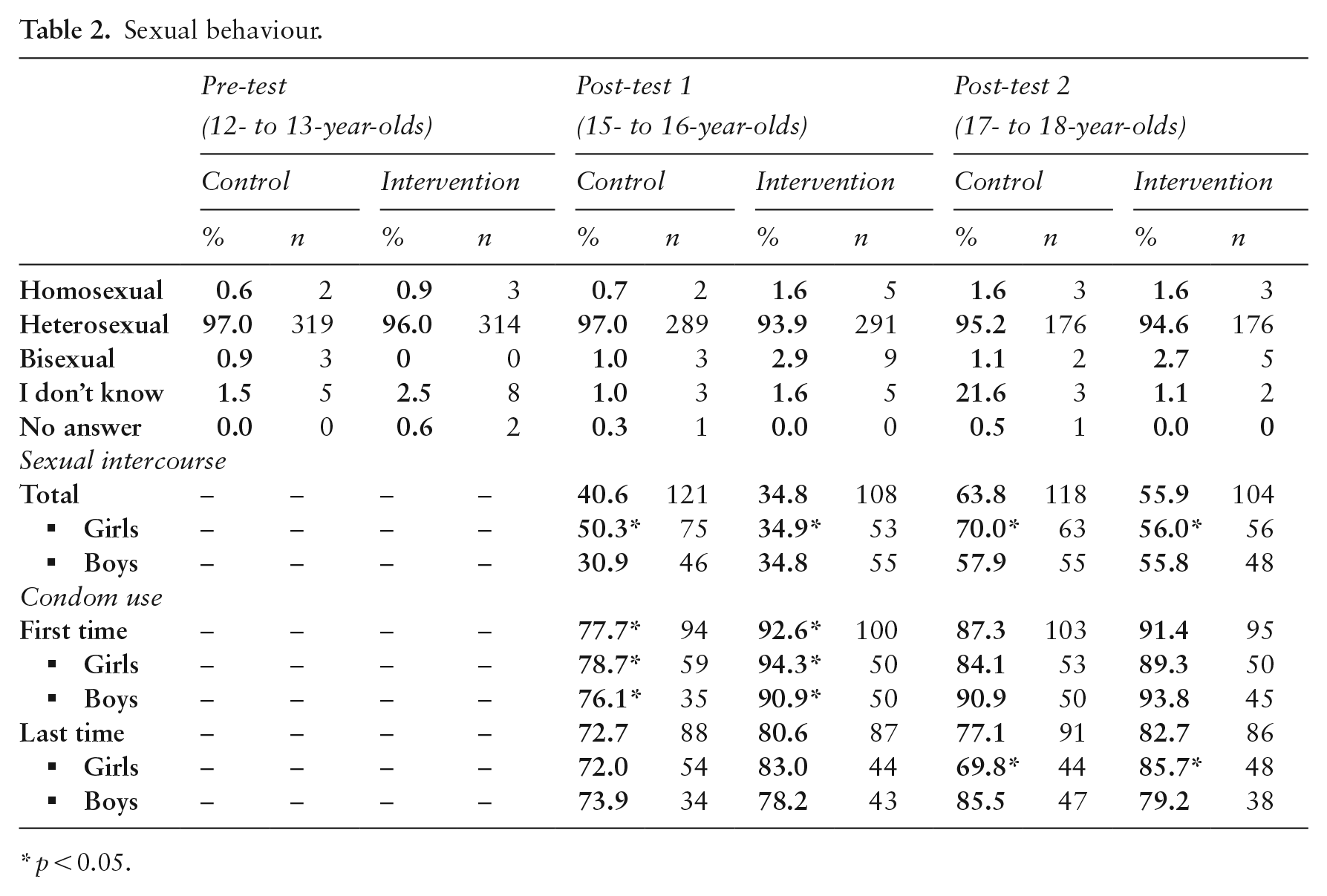
p < 0.05.
Sexual intercourse was more frequent in the control group (41 vs. 35% in the intervention group in the first post-test) and also in the second post-test (64 vs. 56%), but without statistical significance. In the analysis by sex, there were significant differences among girls, with lower rates in the intervention group.
Among those, condom use at first intercourse was significantly higher in the intervention group, among both girls and boys, at more than 90% compared with 78% in the control group. These differences disappeared in the second post-test where condom use increased in the control group up to 89%, while remaining at 91% in the intervention group.
Condom use at last intercourse was greater in the intervention group: 81 vs. 73% in the first post-test, and 83 vs. 77% in the second post-test, but without statistical significance. There were significant differences among girls in the analysis by sex: 70% in the control group vs. 86% in the intervention group in the second post-test.
Discussion
Boys and girls, in both arms, improved in sexuality knowledge, attitudes and skills. However, the intervention group experienced a significantly greater increase in knowledge and in skills (in the first post-test). There was also an impact on sexual behaviour: reduced sexual intercourse with penetration, with statistical significance in girls, and greater condom use at first intercourse in both sexes after the intervention. In the medium term, girls also declared greater condom use in their most recent sexual intercourse.
At the same time, the intervention had no impact on attitudes: variables evolved positively but without differences between the groups. These findings were similar to the results obtained by other sex education programmes (7, 26–28). This fact may have several explanations; for instance, the limited influence of schools (29, 30) in a context in which pupils are influenced on a massive scale, primarily through the media, which presents a model of sexuality based on gender stereotypes (29). This reality makes it extremely difficult for these interventions to achieve health outcomes and highlights the urgent need for action from different fields beyond school (6, 30).
These results are consistent with those found in other Spanish studies, which reported improvements in knowledge and skills, and sometimes in sexual behaviour (19, 25, 28). However, they should be interpreted wisely, taking into account the limitations of this investigation. On the one hand, the hours of intervention were within the recommendations (7, 14), it was superior even to other rigorously designed and evaluated programmes (25–28, 31), and the teachers fulfilled their commitment. But, on the other hand, the quality of the intervention relies on teachers and their experience, training and fidelity with the scheduled sessions, which are key aspects in these kinds of interventions (7, 32), yet were not controlled. Another possible bias could be the pupils’ socioeconomic, cultural and religious status, a non-collected variable, which could influence extracurricular sexual education, but which was sought to be controlled in the way in which similar centres in the same geographical area were selected. Finally, the sample size in the second post-test was smaller than expected, because absences were higher than initially expected, which decreased its statistical power.
Regarding sexual behaviour, note that data from this study is consistent with others recently conducted in Asturian young people. Specifically, the HBSC-2014 study (33) found that 59% of Asturian adolescents aged 17–18 had sexual intercourse with penetration (vs. 60% in the average of both groups of our study), 84% of whom used a condom at last intercourse (vs. 80% of our study). Compared with other regions (33), Asturias was one of the communities with safer practices at last intercourse (with 10 percentage points above the national average for condom use). Condom use at last intercourse declined by 4% in adolescent Asturians aged 17–18 in relation to HBSC-2006 study data (24), although there was a fall of 12% in the national average. According to the data obtained, we could say that the intervention, with 50% coverage from the 2012–2013 academic year, has perhaps helped to maintain the Asturian figures of condom use.
The findings of this study are also comparable to others recently conducted in Spain within young people (29, 34, 35), in which girls declared more practices with penetration and reduced condom use, which also occurred in the control group. This ties in with the fact that the impact of the intervention on sexual behaviour occurred mostly among girls: penetration was less frequent thanks to them, and girls also used more condoms. These differences seem to indicate that girls are more receptive to these kinds of interventions (9, 25, 28).
Therefore, it can be concluded that the NONP programme had a positive impact. In relation to the research questions, it increased condom use and improved knowledge and skills, although in a limited way, and more notably among girls. These findings are important because, despite the noted effects of sex education (5–7), not all studies have been able to find an impact on sexual behaviour (7, 19, 26–28, 32), which may have to do with the duration and quantity of this intervention (four school years, with almost 30 h). It would obviously be necessary to repeat this investigation in the future to demonstrate its validity.
Meanwhile, this intervention may be a good starting point to making sex education universal through compulsory education, as is internationally recommended and as is done in other countries (7, 10, 12, 14). In extending sex education, there are two key aspects to strengthen: teacher training (7–14), which would have an impact on commitment and quality of the intervention (7, 32); and the setting of a minimum curricular content, fully integrated into the school curriculum (7, 12). For example, in Estonia, with a sex education programme in curricula throughout 3 years, the improvement in youth sexual indicators since 2000 has been impressive. Such improvements include an unprecedented reduction in STIs and HIV infections rates and also sizeable downward trends in abortion and teenage birth rates due to a sharp increase in condom and contraceptive use among young people (10).
To improve the impact on sexual health goals, complementary interventions, involving families, media, and health services, are also essential, while taking into account social inequities as well as the huge influence of the internet’s social networks and pornography (5, 6, 10, 36–38). Thus, sex education is recommended from health services (in revisions programmed in childhood and adolescence), recreational actions at the community level (cinema, etc.) and free distribution of quality condoms (5, 6, 12, 39–40).
These are key aspects to fully achieve the rights of adolescents, the United Nations SDGs and, above all, improve the welfare, health and education of adolescents.
Footnotes
Acknowledgements
We would like to acknowledge the support of Eva Iraizoz, Mark Prunella-Miller, Mario Salas and Esther Arbesú, who provided advice, the pupils of this study (and their teachers) and of the NONP programme, the authentic protagonists of this paper and sex education.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the work in sexual education of the Regional Ministry of Health of Asturias.