
Abstract
Objective:
The aim of this study was to validate the content and appearance of an educational game for children aged 7 to 10 years, focusing mainly on cardiovascular health promotion.
Method:
The study used methodological research, with a quantitative approach. The validation process included the participation of 17 specialists in children and/or cardiovascular health. A concordance index of at least 0.80 was considered for content validation and 0.75 for the appearance of the proposed educational material.
Results:
The proposal of the educational game was considered valid, through some suggestions, in view of the purpose of sensitizing children in relation to the promotion of cardiovascular health while still in childhood.
Final considerations:
As a relevant factor in the use of games as strategies to improve health education, we emphasize that the participant is the active agent and the protagonist of the health-disease process.
Introduction
Annually, an increasingly high number of people die prematurely as a result of chronic noncommunicable diseases (NCDs) when compared to other causes (1). It is estimated that 16 million people die each year before the age of 70. However, these early deaths can be significantly reduced through government policies that reduce tobacco use, alcohol abuse, unhealthy diets and a sedentary lifestyle. In Brazil, the mortality rate due to NCDs is decreasing by 1.8% per year, due in part to the expansion of primary health care (1).
In this context, cardiovascular diseases (CVDs) stand out as one of the main causes of deaths, morbidities and disabilities at a worldwide level (2). Overall, CVDs more often affect the elderly population, but the risk factors may originate in childhood. Therefore, the importance of educational actions in the school context is ratified, as it is the place with the best access for children and the young population. Among such actions, collective strategies that integrate physical and recreational activities, in addition to offering healthy snacks and meals, must be implemented (3).
It is known that health education practices carried out in a conservative way, such as educational lectures, are not so attractive to the child population and very often provoke disinterest in the child, making it necessary to develop playful educational strategies that are attractive to children and adolescents, such as educational games.
Particularly, it can be observed that games are consolidated every day as an important tool in health advice. It has been stated that the use of games as a health education strategy can result in changes in attitude and behavior among those who use them. However, in the development of any educational material, it is necessary for it to undergo a validation process aiming to guarantee the effectiveness of its use by the target population (4).
Considering the abovementioned facts, the question is: does the educational game contribute to the promotion of cardiovascular health in children aged 7 to 10 years? Therefore, the aim of this study was to validate the content and appearance of an educational game aimed at children aged 7 to 10 years, focused on promoting cardiovascular health.
Method
The present study used methodological research, which consists of the creation, evaluation and improvement of something that has been constructed (5). In this case, it is a board game in the format of a trail, which has a starting line and a finishing line. It consists of 18 squares made of ethylene vinyl acetate material, each measuring 50 cm × 50 cm, a dice measuring 30 cm × 30 cm, an hourglass and 25 cards. The illustrations in each game square, as well as in the overall format, came from a study that assessed children’s knowledge regarding life habits and risk factors for CVD (6). Other pictures were also present, especially in the ‘Challenge’ house, which were obtained from Google Images (2017).
The participating children (7 to 10 years old) begin by positioning themselves at the starting line, either individually or in pairs. The game starting order is decided by throwing the dice, and the participant with the highest score is the first to start the game. The game pathway consists of five domains: (1) ‘Healthy heart’, (2) ‘Risk factors for heart disease’, (3) ‘Challenge’, (4) ‘Healthy eating’ and (5) ‘Physical activity’. Each of these domains has five cards, which are to be chosen one at a time. Cards 1 to 5 include questions about the topic, expected answers and instructions to be performed for each domain. Moreover, there are five cards related to the ‘challenge’ of the game, for which the participant must perform practical activities. The game is over when everyone reaches the last square, ‘Getting a healthy heart’.
Upon reaching the last square (number 18: called ‘Getting a healthy heart’), the participant must give a summary of the knowledge acquired during the game. Based on this report, this and other teammates who reach this house will win a Meritorious Medal of Honor.
The criteria for selecting the group of expert judges were: having a minimum degree of specialist knowledge; having at least one publication in the area of child health and/or child cardiovascular health and/or child education; and having a minimum experience of 1 year in the field of child health and/or child cardiovascular health and/or early childhood education, from varied areas. To improve the content and appearance validation process, such as that in the study by Cruz et al. (7), a multidisciplinary group of judges should be included, for example from Education, Physical Education, Nursing, Medicine, Nutrition, Child Education and Occupational Therapy, among others.
The sample size of the specialist group required to validate the educational game was defined based on the information which states that there is no consensus on the number of specialists to constitute a group of judges (8). However, recruiting an odd number is recommended, considering the characteristic of what will be validated, the method of analysis of the findings from these judges and, also, the researcher’s preferences.
The survey of eligible specialists was initially carried out at the Database of Theses and Dissertations of the Coordination for the Improvement of Higher Education Personnel (CAPES, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) using the following keywords: ‘cardiovascular health’ AND ‘child’. From them, the first contact was initiated through the Lattes Platform of the CNPq Portal. Moreover, the indication of other professionals who met the selection criteria for the training of the judges was also requested, which resulted in some being selected by snowball sampling, an ideal method when one intends to study populations that are difficult to access or where there is no precision about quantity, as in the present study (9). The participants indicated through the snowball sampling technique were invited to participate in the group of experts by email and/or the WhatsApp application (9).
The recommended specialists had their Lattes curricula analyzed to verify they met the inclusion criteria. It is pointed out that there was a limitation regarding the fact that many education professionals do not have this type of curriculum, and it was necessary to ask early childhood and elementary education teachers for referral of professional colleagues.
To reach the sample size, 89 people from different regions of the country were invited. Of these, 72 did not respond to the initial contact and 17 responded to the evaluation of the educational game, using the Google Forms form.
The validation process took place between September and November 2019, with the participation of 17 specialists with experience in child health and/or child cardiovascular health, thus constituting a multidisciplinary group of judges who evaluated the educational game, in terms of its content and appearance.
For data collection, a form was made available via the internet with approval by the judges, accompanied by the invitation letter, the Free and Informed Consent Form and the educational game analysis protocol. The educational game analysis form and protocol were adapted from the literature (10).
The game analysis protocol was divided according to the proposed domains, evaluating in addition to them, the last square ‘Getting a healthy heart’. After the data collection was performed, these were extracted from the online form in the form of a Google data spreadsheet and the consistency of responses was analyzed. For the analysis of the five game cards for each domain, the validation variables were carried out as shown in Figure 1.
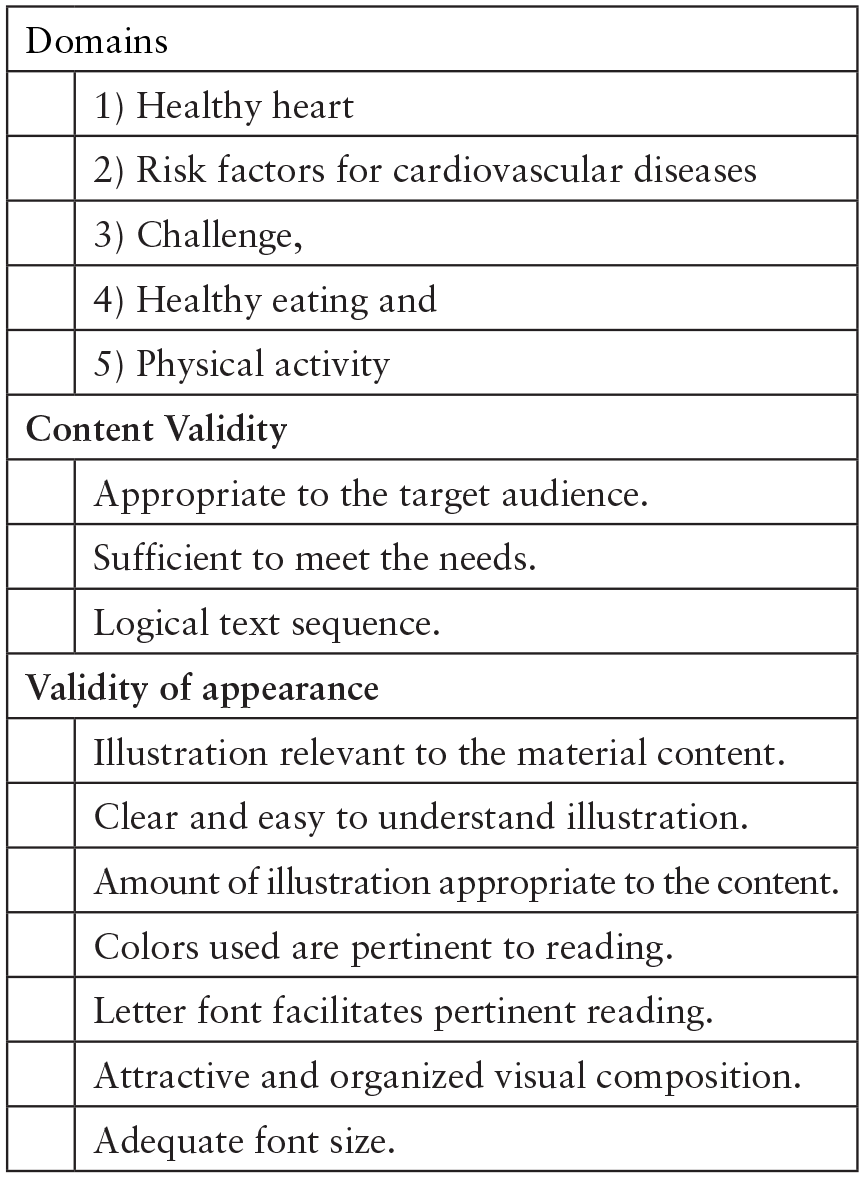
Domains related to the educational game squares and characterization of the assessment items considering the content and appearance validation.
To perform the analysis of the findings, a descriptive quantitative evaluation, represented as absolute frequency and the percentage of valid responses, was chosen.
The Likert scale was used in the educational game analysis protocol, including five options, with a rating range of: 1 – ‘totally disagree’ (TD), 2 – ‘disagree’ (D), 3 –‘neither disagree nor agree’ (ND/NA), 4 – ‘agree’ (A) and 5 – ‘totally agree’ (TA), in addition to spaces for comments and suggestions for the game. In the last session, the relevance of the educational game was evaluated, when the expert’s general opinion about the game was requested.
The evaluation was guided by the Content Validity Index (CVI) of the cards available for the first version of the educational game. The CVI calculation proposes the measurement of the proportion of judges who are in agreement with the material to be validated, with an agreement index of no less than 0.80 (8). For the validity of appearance, the recommendations were followed (11,12), considering the relevance criterion and agreement index between the judges of at least 0.75 (13).
Results
Selected evaluators
The group of specialists consisted of 17 people, including 11 nurses, three physical education professionals, one occupational therapist and two educators, of which 16 were female and one male. Their ages ranged from 28 to 60 years (mean (
Regarding the nurses (n = 11), considered specialists in the thematic area, after analysis of the Lattes curriculum, six had a PhD and five had a Master’s degree as their highest degree. The other professionals, who answered the instrument requirements to evaluate the proposed game, met the previously defined criteria.
Validation of content
All the evaluation results are shown in Table 1. In the evaluation of the ‘Healthy Heart’ domain, in the individual analysis of the cards in relation to the content, the cards 1 (0.90), 2 (0.84) and 3 (0.82) were shown to be adequate, while cards 4 (0.76) and 5 (0.76) did not reach the agreement value. When referring to Risk Factors for heart disease, cards 1 (0.86), 4 (0.88) and 5 (0.88) obtained a CVI > 0.80. Card 2 also reached its average >0.80 for content validation. Card 3, on the other hand, showed a lower agreement rate among the specialists in all its items, with an average of 0.51. As for the ‘Challenge’ domain, the agreement index was higher than the referenced minimum of 0.80 in all cards.
Judges’ assessment of the Content Validity Index in the cards according to each domain.

Mean rating of the Content Validity Index.
Cards 1 to 5 showed a variation in the average related to the validity index from 0.88 to 1. It is observed that Card 1 (1) obtained the highest level of agreement among the evaluators.
The ‘Healthy eating’ domain also had a CVI higher than 0.80 in all of its cards, corresponding to the agreement between the judges. However, some suggestions for changes were reported for this domain.
According to Table 1, the ‘Physical activity’ domain reached the CVI in relation to the content of 0.80, in all evaluated items, with an agreement value of 1 in some of these.
The last square, ‘Getting a healthy heart’, was also evaluated and obtained a mean CVI value of 1 for content validation.
Validation of appearance
Regarding the validation of appearance for the ‘Healthy Heart’ domain, all items reached a CVI > 0.75. When referring to ‘Risk Factors for heart disease,’ according to cards 1, 4 and 5, the CVI was >0.75, with the respective averages of 0.88, 0.86 and 0.87. Card 2, for one of its items, showed a value of 0.70, related to the topic ‘the illustration is clear and easy to understand’; however, even if this card had a lower index in one of its items, the card average was >0.75 (0.84).
Card 3, on the other hand, showed a lower agreement rate among the specialists for all its items, with an average of 0.49 for appearance validity.
As for the ‘Challenge’ domain, the agreement index was higher than the minimum of 0.70 in all cards.
It is observed that Card 1 obtained the highest level of agreement among the evaluators. Regarding the appearance validity index, the range was from 0.89 to 0.94. In contrast, for ‘Healthy eating’, all cards reached a CVI of 0.75, and in some items the agreement value was equal to 1. Cards 1 (0.92), 2 (0.95), 3 (0.87), 4 (0.88) and 5 (0.87) showed the mean CVI values.
According to Table 2, the ‘Physical activity’ domain reached the CVI in relation to the appearance of 0.75 in all assessed items, considering the agreement value of 1 in some of these.
Judges’ assessment regarding the Content Validity Index of the cards’ appearance in all domains.
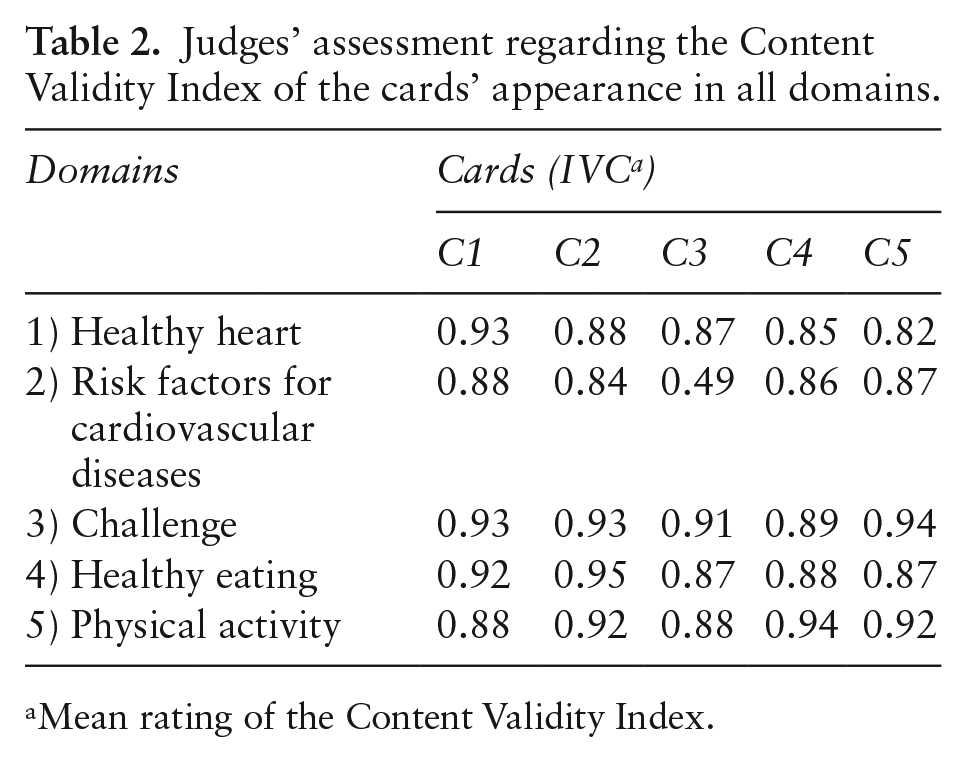
Mean rating of the Content Validity Index.
Square number 18, ‘Getting a healthy heart’, also obtained a higher than expected average of 0.75, obtaining a value of 0.95 of agreement among the judges.
Figure 2 shows the judges’ suggestions for changes in the cards and also demonstrates the reformulated ones.
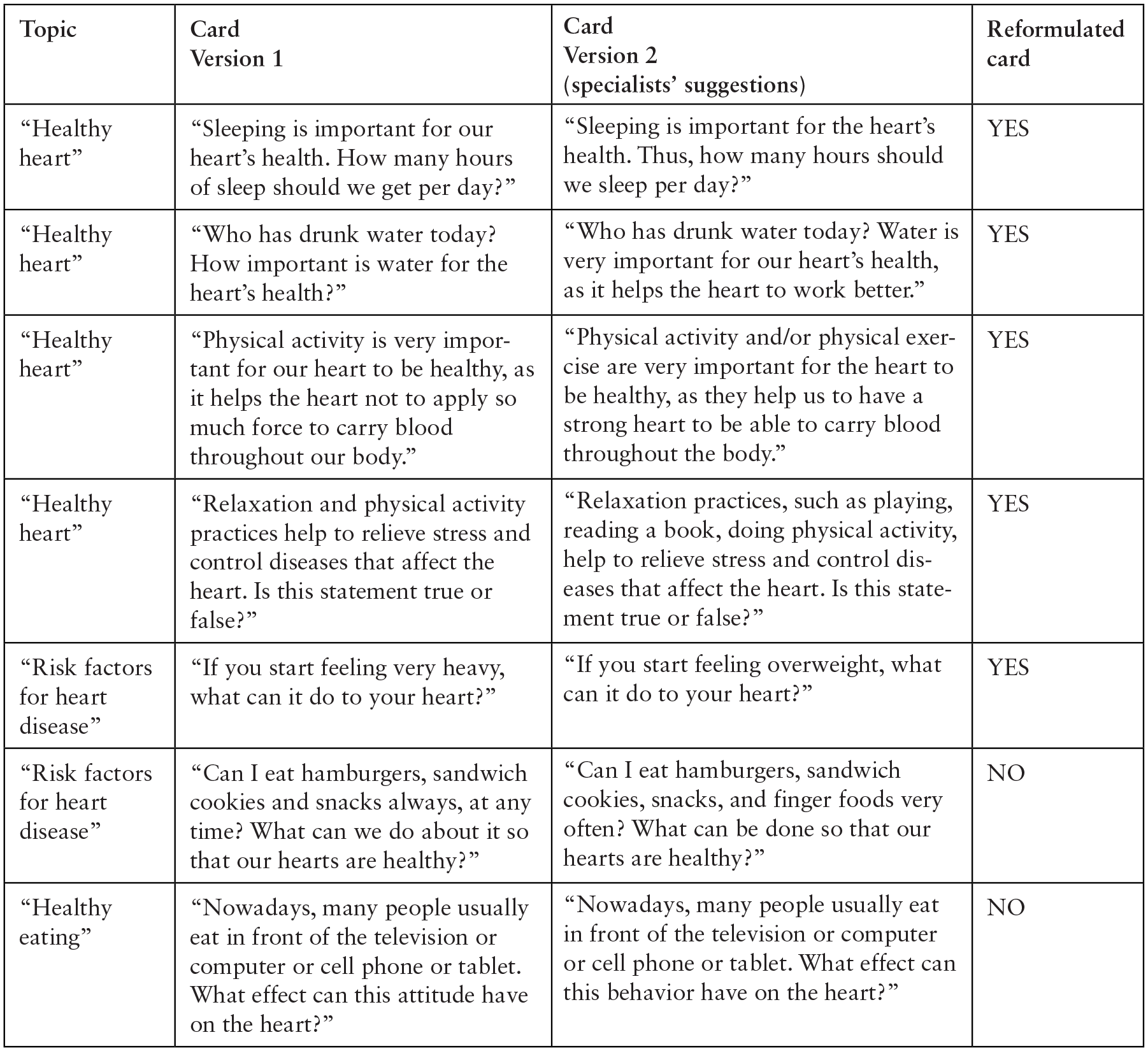
Judges’ suggestions for the ‘Game for Cardiovascular Health Promotion in Children’ cards.
Among the judges’ suggestions, modifications were suggested for two cards, corresponding to Card 2 of the ‘Risk factors for heart disease’ domain and Card 4, ‘Healthy eating’, one of which was accepted. The non-reformulation is due to the fact that the suggestion did not cover the association between the foods described in the card and the questioning.
Discussion
Among the judges’ responses, after analyzing the data, it was observed that the educational game proposal was considered valid, after some suggestions, to achieve its purpose of encouraging children to think about cardiovascular health promotion.
The suggestions for improving the educational game were taken into account, in relation to the content and appearance of some cards, such as in the ‘Healthy Heart’ domain, related to changes in the card written text, in addition to the color of the card and its design, aiming to make the game even more attractive for children. However, regarding the design, the suggested changes were not accepted, and this fact can be considered a limitation of this proposal, as the drawings used were obtained and adapted after the authors’ authorization (6).
The main objective of the first domain addressed in the ‘Healthy Heart’ game was to raise awareness among children about healthy behaviors to promote cardiovascular health, since it was observed, based on other studies, that the ideal time to start this awareness, as well as the prevention of CVD, is during childhood. This is because it is still possible to change risk factors that are modifiable, such as being overweight, physical inactivity, dyslipidemia and exposure to tobacco. By working with this child population, we can have healthy adolescents and adults with a lower risk of developing CVD (14).
As for the validated domain ‘Risk factors for heart disease’, changes were suggested for two cards, one of which was accepted. One of the cards was not reformulated because the suggestion did not include the association between the foods described in the question included in the letter and the questioning.
The purpose of presenting this topic to children was to provide knowledge about risk factors for heart disease, by demonstrating several risk factors for CVD, which can be grouped into two main groups: modifiable and non-modifiable (15). The same author also mentions as modifiable risk factors: dyslipidemia, tobacco exposure, lack of physical exercise/physical activity and body mass index (BMI) ⩾30 kg/m². Genetic predisposition, ethnicity, age and gender are risk factors for heart disease, but are characterized as non-modifiable.
Regarding the validated ‘Healthy food’ domain, only one card had suggestions for its reformulation, which were not accepted, as it is understood that the term attitude, which was requested to be replaced by behavior, is in agreement with the purpose of the educational game.
The attitude outweighs the behavior, by influencing it; thus, the attitude acts as a precursor for judgments and decisions (16).
The aforementioned domain reinforced the importance of starting healthy eating habits as early as during childhood, considering that it is at this stage of life that food acceptance is at its greatest. However, better eating habits must be encouraged, as they are an essential behavior for optimal physical, motor and cognitive development and energy supply (17). It was observed, based on the validation of the proposed game, that of the 25 cards, seven had suggestions for reformulations. However, only five of these were reformulated as a result of the experts’ recommendations.
Therefore, the validated game proposal fills a gap identified by other authors regarding the impact of CVD on society (18), by addressing risk factors as early as in childhood (19,20), 80% of which can be prevented (1).
Different studies have identified the importance of using educational games for the development of activities related to child health promotion (21,22). However, what can be observed in the literature is that individual educational programs are effective, but costly (23), whereas more conservative methods for providing education, such as lectures and pamphlets, are more accessible to the population, but do not significantly improve clinical outcomes (24). In this context, it is understood that educational technologies can be used as health education strategies, as they more easily provide advice and understanding among the participants (25).
Within the context that refers to the promotion of children’s cardiovascular health, increasingly early interventions must be implemented in the school space, aiming at the prevention of NCDs in adult life, including CVDs, as they will influence the population’s quality of life (26).
It is understood that an educational game, such as a health education strategy, must be something simple, yet playful, and attractive, as well as motivating. It must also have clear and understandable language, and the rhythm must be guided by the children.
Conclusion
The validation of a game with an educational purpose that is also playful is of utmost relevance, because the importance of the analysis of concepts seen from different perspectives and realities is understood.
As a limiting factor of the study, we emphasize the participation of only two professionals in early childhood education among the specialists. This fact should be reassessed for future validation of educational games.
It can be concluded that the educational game was validated and the suggestions for reformulations were accepted within the context of maximum use to guarantee its effectiveness, and for further evaluation with the target audience, as this is a health education strategy that can become more attractive, interesting, dynamic and motivating. Moreover, it has a low cost design and is easy to use, without the need for supplementary equipment or instruments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.