
Abstract
Healthy lifestyles are commonly associated with improved physical and mental health. Sleep patterns, nutrition, physical exercise, consumption of psychoactive substances, among others, can strongly influence positive mental health. The aims are: characterize lifestyles based on positive mental health clusters, considering the cross-sectional cohort sample of higher education students, and analyse the lifestyles associated with positive mental health. A cross-sectional, descriptive, correlational and multicentric study of quantitative approach was conducted. The Positive Mental Health Questionnaire was applied. Through the k-means method, four clusters were obtained based on positive mental health levels. The sample of 3647 higher education students was mostly female (78.8%), single (89.5%), with an average age of 23 years (SD = 6.68). Differences were found between clusters based on the sociodemographic characteristics and lifestyles. Findings in Cluster 1 were highlighted because they included students with a higher level of positive mental health, which was associated with greater satisfaction in affective relationships, higher recreational and sports activities, better sleep quality, a healthy diet, and lower medication and illicit drugs consumption. These key findings emphasize the promotion of healthy lifestyles and highlight the importance of positive mental health in promoting the health of higher education students.
Introduction
The perspective on life and human development has been changing. Human development takes place from a succession of developmental stages. The end of adolescence and entry into adulthood corresponds to a remarkable and demanding period, since it involves several dimensions, biological, cognitive, social, environmental and personality (1).
Several studies show that the age group 18 to 25 is a transitional stage from adolescence to adulthood, characterized by a distinct period of development, a phase with a changeable, fluid and transitional character (1). Erikson (2) observed cases of prolonged adolescence, which he considers to be a typical phenomenon of modern societies that allows young people to be offered a period of exploration that allows the young person to find themselves and find their place in society and coincides with attending higher education.
Academic life implies a daily life guided by autonomy, responsibility and autonomous decisions, in contrast to parental dependence (1). It is mostly in the early years that students face and feel the greatest demands, as students have to adapt to an extensive and complex set of roles, in addition to achieving academic success. This circumstance favours a condition of greater vulnerability, which can lead to situational crises or putting the student’s mental health at risk (3).
The World Health Organization (WHO) (4) defines mental health as a state of well-being, wherein each individual perceives his/her potential, copes with everyday life stressors, works productively and fruitfully, and actively contributes to the community. This definition has raised an interesting debate among mental health researchers, pointing to a consensus that not having a mental illness necessarily confers psychological well-being (5). From a salutary perspective, the variables promoting mental health are significant, with mental health viewed as an indicator of integration and adaptation (6).
Positive mental health is currently an important issue for scientific literature, policy-making and clinical practice (7), attracting a growing interest in health research (8).
Two major theories describe the main components of positive mental health and the concept of well-being. The hedonistic tradition comprises the emotional element, for example, happiness and life satisfaction, while the eudemonic tradition includes human potential and optimal functioning. The interconnectedness of these approaches enables the conceptualization of positive mental health as a mental health approach involving the emotional, psychological, and social well-being dimensions (9).
Among European countries, Portugal has the second-highest prevalence of psychiatric diseases. Anxiety disorders are the most prevalent (16.5%), followed by mood disorders (7.9%) (10). With the increasing number of higher education students, the prevalence of mental disorders poses significant concerns, especially about anxiety and depression symptoms (11). Moreover, the onset of many of these disorders occurs during the university years. The literature shows higher rates of mental disorders in university students than in the general population (12).
Entry into higher education is an important stage of the individual’s life, which represents, for most young people, a goal achieved (situational transition) but also corresponds to a period of consolidation or completion of the processes of ‘developmental transition’. This situation can intensify health imbalances and disturbances due to its cumulative effect, which Chick and Meleis (13) call multiple transitions.
Some studies conducted with higher education students highlighted a tendency towards risky behaviours such as sedentarism, unhealthy sexual behaviour, tobacco and alcohol consumption and poor eating habits (14,15). Also, students exposed to stress or with low resilience are more likely to use alcohol as a coping strategy (12). In Portugal, higher education students often experience nervousness, sometimes extreme sadness, emotional deregulation and intense concerns (10). An analysis of the factors associated with mental health problems does not explicitly point to changes in family or socio-economic factors. However, it emphasizes the increased stress observed in university contexts and concerns about education and career opportunities (16). Educational institutions are important environments for health promotion initiatives because of the intrinsic relationship between health and learning (8).
According to the WHO in 2005, a healthy lifestyle means regular physical activity, no smoking, limited alcohol consumption, a healthy diet to prevent overweight, maintaining normal body mass index parameters and engaging in cultural or mental activities (5). The literature identifies a two-way relationship between lifestyle and mental health variables (17,18).
Thus, this study was prompted by acknowledging the association between different lifestyles and positive mental health. The aim was to explore different profiles likely to combine interaction effects or synergies between sociodemographic and lifestyle variables among higher education students. These study findings will greatly contribute to improving the understanding of lifestyles associated with positive mental health of this population. Thus, this study aimed to a) characterise lifestyles based on positive mental health clusters, considering the cross-sectional cohort sample of higher education students, and b) analyse the lifestyles associated with positive mental health.
Methods
Study design
This study was a project, developed by the NursID group of the Center for Health Technology and Services Research. A cross-sectional, descriptive, correlational and multicentric study of quantitative approach was conducted. Data collection was carried out between October 2019 and March 2020 in higher education institutions (public and private) in Portugal, using a self-administered questionnaire.
Setting and participants
The sample comprised 3647 students from 20 higher education institutions who freely agreed to participate in the study. Students in Portugal aged 18 years or older were eligible to participate. Most were women (n = 2861; 78.8%), single (n = 3250; 89.5%), attending their first and second academic years (n = 1153; 32.1% and n = 888; 24.8%) and had an average age of 23.17 years (SD = 6.68).
Ethical procedures
This study followed the Helsinki Declaration and the Oviedo Convention’s recommendations, and the project was approved by the Ethics Committee. Participants were provided with information about the study objectives, which ensured anonymity, and were informed that they were free to withdraw from the study at any point.
Data collection
The questionnaire comprised 29 sociodemographic, clinical and lifestyle assessment questions and the Positive Mental Health Questionnaire (PMHQ), translated and validated for the Portuguese population in 2014 by Sequeira et al. (6). Lifestyle was assessed through questions about eating habits, sports or physical exercise, the number of sleeping hours and its quality, the use of anxiolytic therapy and the consumption of substances such as tobacco, alcohol and illicit drugs. This questionnaire followed the recommendations of the Portuguese Directorate-General of Health (18) and content validation was performed by a group of 25 experts.
The PMHQ consists of 39 items grouped into six factors that define the construct of positive mental health underlying the multifactorial model of positive mental health: Personal satisfaction; Prosocial attitude; Self-control; Autonomy; Problem-solving and Self-actualization; and Interpersonal relationship skills. The questionnaire uses a four-point Likert scale, with answers including ‘always or almost always’; ‘quite often’; ‘sometimes’; ‘rarely or never’. Scores range from 39 to 156 points, and the higher the score, the better the positive mental health.
Positive mental health shows good internal consistency (Cronbach α = 0.92), with a similar factorial structure to the original study (Spain); the six factors’ internal consistency varies between 0.60 and 0.84. The instrument has good stability (0.98), assessed by the test–retest performed at two-month intervals. In the present study, a Cronbach α of the overall scale also reached (0.92) and the internal consistency of the six factors varied between 0.55 and 0.86.
Procedure
Following the data collection, all questionnaires were submitted for analysis, eliminating those incomplete or incorrectly filled. The coding of valid questionnaires was then processed.
Data analysis
To group participants according to their positive mental health, a cluster analysis was applied through the k-means method. The analysis was performed using the six factors/variables that define the positive mental health construct (Personal satisfaction; Prosocial attitude; Self-control; Autonomy; Problem-solving and Self-actualization; and Interpersonal relationship skills). Standardized variables (z-scores) were included in the procedure, and solutions of two to six clusters were examined. The η2 values were calculated by dividing the sum of all between-subjects sum of squares by the sum of the total sum of squares. The results of η2 for the different solutions were two clusters: 0.362; three clusters: 0.448; four clusters: 0.505; five clusters: 0.531; and six clusters: 0.563. Based on these results, a four-cluster solution was chosen. Subsequently, six analysis of variance (ANOVA) tests were performed to compare the four clusters obtained in the selected dimensions, although statistically significant differences were expected. The Levene test was used for homogeneity of variances, and in case the test was significant, the Welch correction was performed. The chi-square test was applied to analyse the association between clusters belonging and sociodemographic variables and lifestyles. All the statistical analyses were carried out using the SPSS (Statistical Package for Social Science) program, version 25.0 (IBM Co., Armonk, NY). The measures of the magnitude of effect η2 for the ANOVA case and Pearson’s Phi or Cramer’s V for the chi-square test were presented. The results are considered statistically significant, with a 5% significance level.
Results
Clusters and positive mental health
From the sample of 3647 students, four distinct groups were identified, distributed across the four clusters: C1 (n = 1356, 37%); C2 (n = 976, 27%); C3 (n = 872, 24%) and C4 (n = 443, 12%). This distribution sought to group similar students within the same cluster and distinctive between clusters according to the positive mental health dimensions (Figure 1).
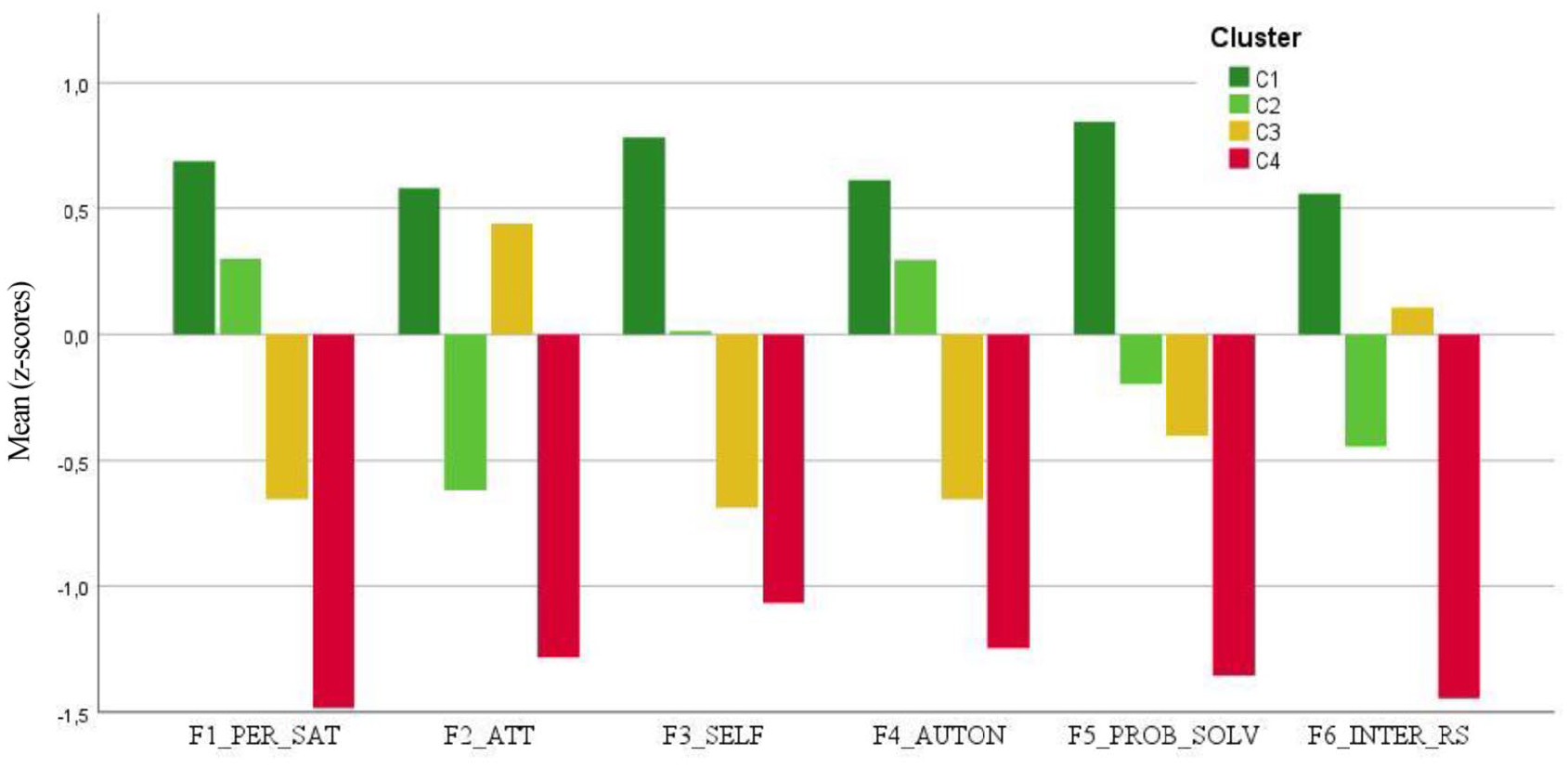
Cluster analysis. Mean performance z-scores by cluster in the positive mental health dimensions.
According to the results displayed in Table 1, through the ANOVA test with the Games–Howell post hoc test, statistically significant differences were found between clusters according to each positive mental health dimension.
Mean and standard deviation of the positive mental health dimensions by cluster.
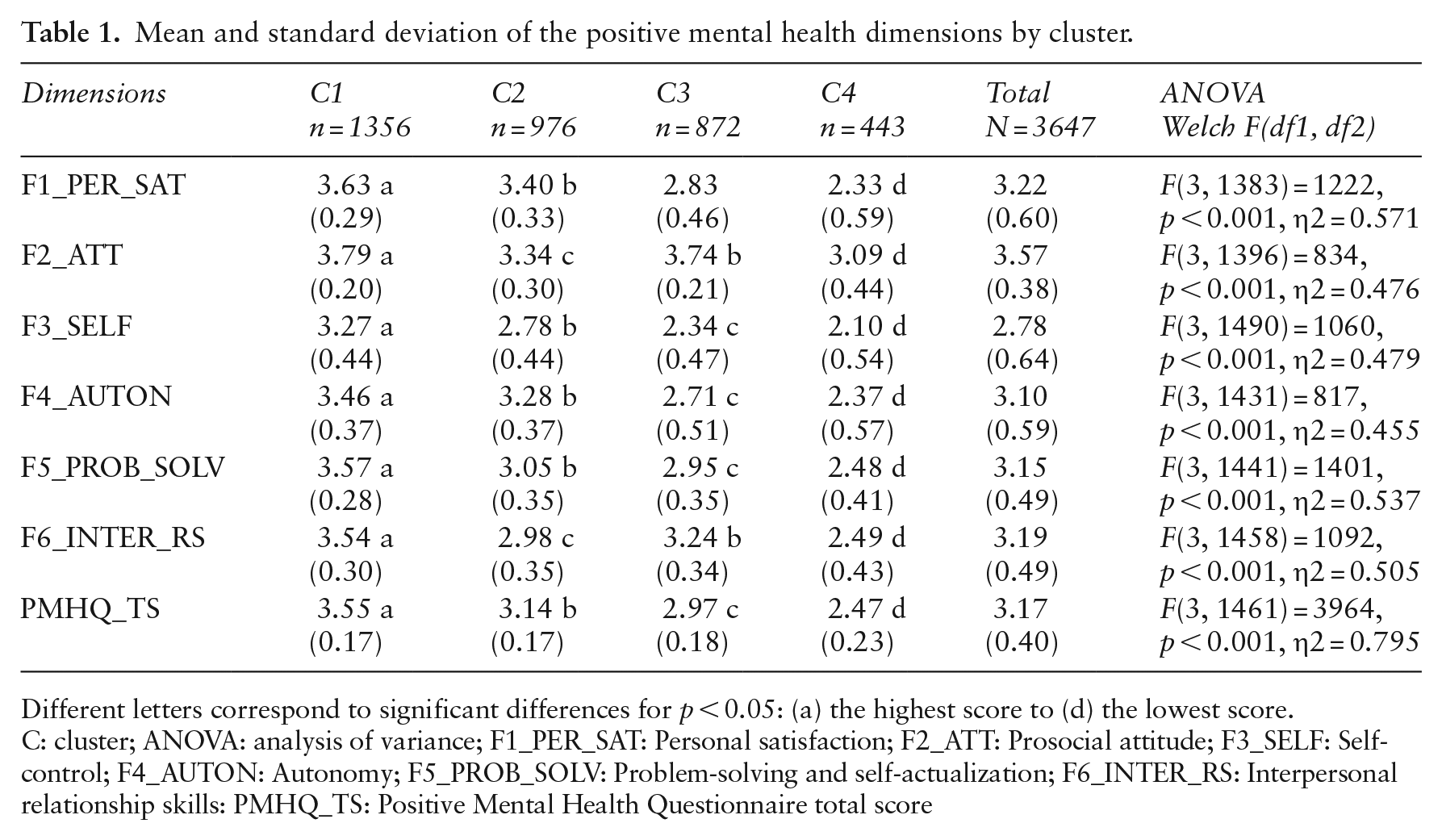
Different letters correspond to significant differences for p < 0.05: (a) the highest score to (d) the lowest score.
C: cluster; ANOVA: analysis of variance; F1_PER_SAT: Personal satisfaction; F2_ATT: Prosocial attitude; F3_SELF: Self-control; F4_AUTON: Autonomy; F5_PROB_SOLV: Problem-solving and self-actualization; F6_INTER_RS: Interpersonal relationship skills: PMHQ_TS: Positive Mental Health Questionnaire total score
The variables contributing to cluster differentiation were Personal satisfaction; Self-control; Problem-solving; Self-actualization; and Interpersonal relationship skills.
The clusters were ordered by classification of the dimensions of Personal satisfaction; Self-control; Autonomy; Problem-solving; and Self-actualization: C1 > C2 > C3 > C4. Regarding the Prosocial attitude and Interpersonal relationship skills dimensions, the clusters were ordered according to their classification C1 > C3 > C2 > C4. C1 participants showed greater personal satisfaction, autonomy, self-actualization, problem-solving ability and self-control compared with other clusters. Students from C1 presented higher overall positive mental health, followed by C2 > C3 > C4.
From the assessment of positive mental health factors in the various clusters, C1 included more participants (1356). This cluster also showed higher average levels of positive mental health in all dimensions. The Prosocial attitude was highlighted in this cluster, but Self-control and Autonomy potentially needed to be further developed.
C4, composed of 443 students, showed lower average levels of positive mental health in all dimensions. Also, the Prosocial attitude showed a higher average compared with other dimensions. Self-control and Personal satisfaction were the dimensions that needed to be further developed in students. Both C4 and C1 showed higher averages for Prosocial attitude, which can be explained by the students’ disposition towards social engagement and their altruistic social attitude towards others, accepting individual differences and social factors.
C2, composed of 976 students, showed behavioural similarities to C1. However, C2 scored lower averages on all dimensions, mainly for Interpersonal relationship skills and Prosocial attitude.
Finally, C3, with 873 students, showed a behaviour similar to C4 but scored higher averages for positive mental health dimensions. Moreover, the Prosocial attitude and Interpersonal relationship skills, and Self-control and Autonomy scored higher mean values.
An analysis was performed on the sociodemographic characteristics and lifestyles to further investigate the characterization of clusters.
Clustering related to the sociodemographic indicators
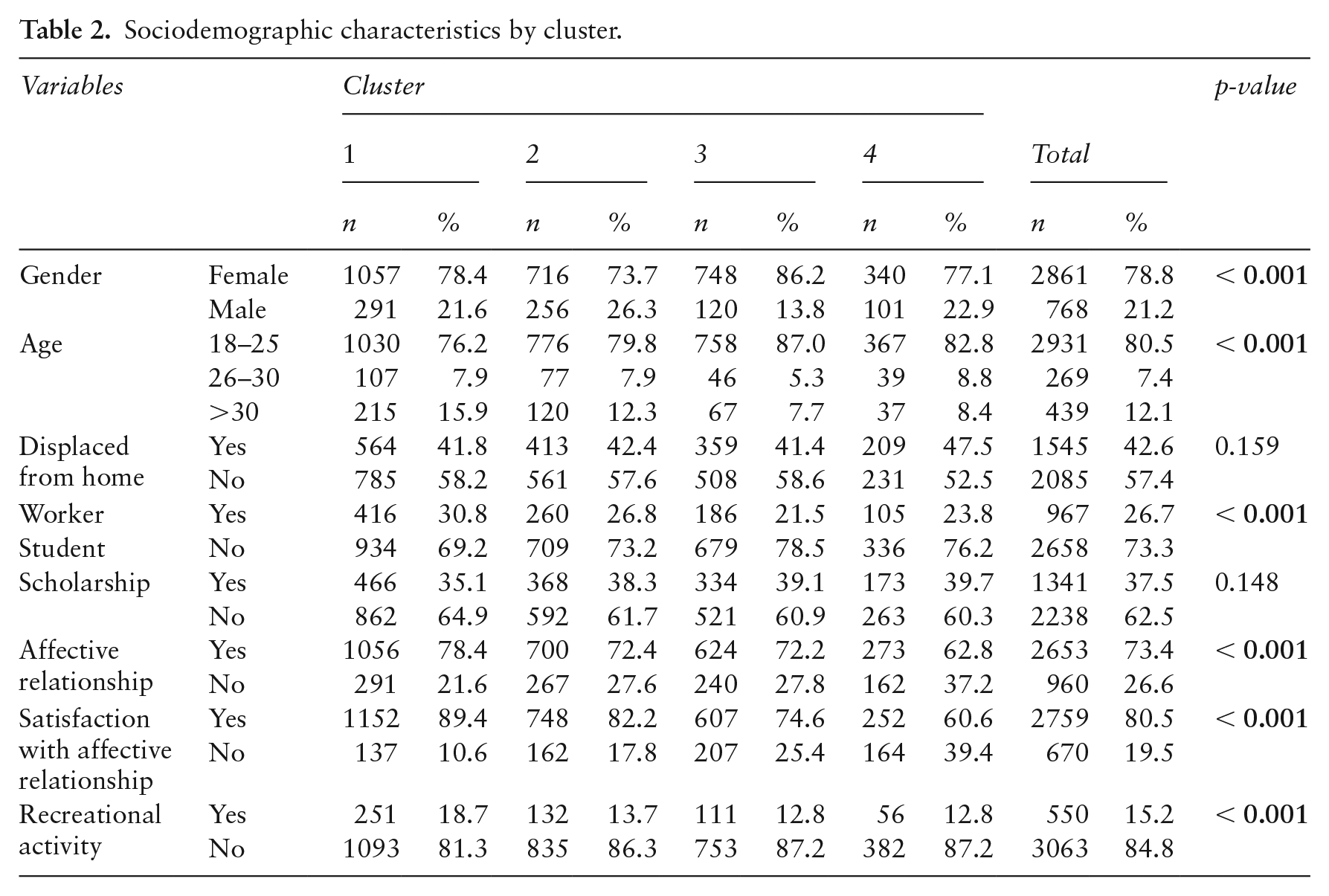
Table 2 presents the analysis of the sociodemographic characteristics and lifestyles by cluster through the chi-square test. Some important outcomes were obtained:
the existence of statistically significant associations between clusters and most sociodemographic variables (gender, age, being a student worker, having an affective relationship, satisfaction with the affective relationship, and engaging in recreational activities), except between being displaced from home and having a scholarship;
a larger percentage of female students in C1 and C3, compared with C2 and C4;
groups mainly composed of students aged between 18 and 25 years. C1 is the oldest group, with an average age of 24.22 years (SD = 7.83). The one-way ANOVA test was used to determine differences in ages between groups. Since the homogeneity of variances test was violated, the Welch correction was applied, and statistically significant differences were found, Welch F(3, 1650) = 28.6, p < 0.001. Using the Games–Howell Post-Hoc test, only C3 and C4 showed no significance;
the majority of the students were living with their families and did not practise physical activity. When comparing C1 and C3, these included fewer students displaced from home, and C1 had more student workers;
in every cluster, the majority of students did not have a scholarship;
most participants had an affective relationship and were satisfied with it. C1 showed higher percentages of students having an affective relationship and were satisfied, contrary to C4;
most did not practise recreational activities. However, C1 presented the highest percentage for recreational activities.
Sociodemographic characteristics by cluster.
Clustering related to the lifestyles indicators
The analysis of lifestyles through the chi-square test (Table 3) showed:
statistically significant associations in the four identified profiles (clusters), between most lifestyle variables (perception of a healthy diet, physical exercise, sleep satisfaction, no consumption of medication or illicit drugs), except for tobacco and alcohol;
most students did not practise physical exercise. However, C1 students were the ones exercising the most, while the C4 students exercised the least;
a good perception of a healthy diet, with C1 revealing the highest percentage of students, and C4 the lowest;
students had an average of 6.82 h of sleep (SD = 2.91). C4 reported sleeping fewer hours on average and C3 more sleeping hours. However, the differences in the average daily sleeping hours per group were not statistically significant (p = 0.06); Furthermore, C4 and C3 revealed the highest levels of dissatisfaction with the number of hours of sleep, but they were also the ones that most consumed sleeping pills. More specifically, students in C1 showed higher sleep satisfaction and lower consumption of medication. On the other hand, students in cluster C4 reported less sleep satisfaction and higher consumption of sleep medication;
most of the participants had no smoking or illegal substance consumption habits. Despite this result, no significant differences were found between the clusters.
Lifestyles by cluster.

Moreover, statistically significant differences were found between clusters for the consumption of illicit drugs. C1 showed the least consumption of illicit drugs, while C4 reported the highest consumption.
Discussion
After the cluster analysis, four distinct groups were obtained. C1 showed a better positive mental health profile in all dimensions, contrary to C4.
Students in cluster C1 showed greater personal satisfaction, demonstrating a high prosocial attitude based on strongly developed self-control and autonomy. These aspects, associated with the enormous ability to establish interpersonal relationships, are likely to promote a good problem-solving capacity and influence students’ self-actualization. Notably, students in C1 revealed a higher percentage of stable affective relationships. In the meta-analysis by Lyubomirsky et al. (19), the individuals’ positive emotions were perceived to make them better at resolving conflicts and becoming more sociable. Also, in the same research involving longitudinal studies, the authors found that happiness generated better relationships and work outcomes, implying a greater positive mental health.
In the present study, the students in C1 showed a better perception of positive mental health. This perception was associated with a higher age group, being a student worker, and having affective relationships with a certain degree of satisfaction. Also those were engaging in more recreational activities. On the contrary, C4, with the worst positive mental health, showed more students displaced from their usual residence, less satisfaction with affective relationships and less recreational activities. Our results do not corroborate the findings of another study, which concluded that the older the students, the less capacity they had to perceive emotional support and the more difficult it was to find and maintain affective relationships (20,21).
Regarding lifestyles, our study found that positive mental health was associated with physical exercise, the perception of a healthy diet, greater sleep satisfaction, and lower consumption of medication and illicit drugs.
The literature indicates that attitudes such as regular physical activity, good sleep hygiene, abstaining from consuming psychoactive substances and health surveillance are associated with better mental health, being indicators of positive behavioural health (14,22,23).
Concerning a healthy diet, current systematic reviews confirm a relationship between diet quality and positive mental health in adolescents. This evidence suggests the importance of taking nutrient-rich food between meals to help brain development and build a healthy adult life (24). In a study with 12,389 Australian people, Mujcic and Oswald (24) found that an increase in fruit and vegetable intake over two years resulted in a significant improvement in life satisfaction and positive mental health.
The literature also emphasizes sleep as an important element for the maintenance of general health. Recent studies have documented that the number of sleeping hours and sleep quality is related to the prevalence of physical and mental illness (25,26).
This present study showed that sleep promotes positive mental health. The difficulty in starting and maintaining sleep is common in students (27). This is an alarming signal because unhealthy sleep has proved to be associated with low academic performance (28), and/or poor mental health, such as depressive symptoms and anxiety (29).
Also, positive mental health was negatively associated with illicit drug use. However, the relationship between illicit substance and alcohol consumption with positive mental health is still controversial. While some studies have identified a non-linear relationship (with high risks for depression and anxiety for light/moderate users) (29), other studies did not find a significant correlation between alcohol and drug consumption with positive mental health (18). Most of our study participants had no smoking or illegal substance consumption habits, but many students consumed alcohol. The literature reveals that smoking is a risk factor for positive mental health (5).
In general, this present study has shown that students with better positive mental health had better lifestyles. Personal satisfaction and Prosocial attitude were highlighted with higher averages for positive mental health, and self-control, with autonomy, registering lower averages in C1. C4 was characterized by the worst lifestyle, with self-control and personal satisfaction showing lower averages for positive mental health.
Conclusion
Given that behaviours are easily influenced and modifiable, health education is an important vehicle for promoting mental health, and a unique opportunity to increase the mental health potential of higher education students, namely in the adoption of healthy behaviours. Knowledge about the determinants of mental health is extremely important, as it can and should be transferred and integrated into Health Policies.
These study results suggest an association between the analysed variables (sociodemographic characteristics and lifestyles), with practical implications for positive mental health. The findings also show that, in general, lifestyles, affective relationships and recreational activities should be carefully considered in a mental health promotion plan.
Lifestyles such as healthy diet, physical exercise, sleep satisfaction, not consuming medication or illicit drugs, having satisfactory affective relationships, maintaining the habitual residence, and recreational activities showed a strong influence on positive mental health. All these indicators act as promoters of overall positive mental health, especially Personal satisfaction and Prosocial attitude.
We stress the importance of interventions to promote self-control and autonomy, such as the students’ ability to deal with stress/emotions, frustration and anxiety. Importantly, interventions promoting personal satisfaction in students with a C4 profile should enhance self-concept, self-esteem, satisfaction with personal life and the belief of a better future.
Last, we suggest the design and implementation of intersection programmes between positive mental health and healthy lifestyle literacy among higher education students, demonstrating the relevance of the factors associated with the clusters identified in this study.
The student is an open system in interdependence with its context (family, academic and social). The family can act as a protective system for the individual in crisis situations, helping him to face adversity and manage anxiogenic situations related to higher education. So a systemic approach to promoting mental health seems particularly promising for enhancing student well-being and success.