
Abstract
Background:
Immune checkpoint inhibitors (ICIs) have shown limited efficacy in unselected advanced sarcomas. Drug-eluting bead transarterial chemoembolization (dTACE) may enhance antitumor immunity through localized chemotherapy and immunogenic cell death.
Objectives:
This study aimed to evaluate the clinical benefits of combining dTACE with ICIs-based therapy in locally advanced or metastatic sarcomas.
Design:
This was a retrospective study.
Methods:
In this retrospective, exploratory cohort study (May 2019–July 2024), patients receiving ICIs-based therapy (ICIs ± chemotherapy ± tyrosine kinase inhibitors) were stratified into two groups: systemic therapy alone (ICIs-based therapy) or combined with dTACE (ICIs-dTACE). Propensity score matching (PSM) was used to address selection bias and balance baseline characteristics.
Results:
A total of 213 patients were included (167 in the ICIs-based therapy group and 46 in the ICIs-dTACE group), yielding 44 matched pairs after PSM. The ICIs-dTACE group was associated with significantly superior median progression-free survival (PFS) compared to the ICIs-based therapy group (7.9 vs 4.5 months; hazard ratio (HR) = 0.532, 95% confidence interval (CI) 0.339–0.836; log-rank p = 0.005). This association remained consistent after PSM (7.9 vs 4.7 months; HR = 0.533, 95% CI 0.312–0.910; log-rank p = 0.019). The disease control rate was also higher in the ICIs-dTACE group both before (87.0% vs 71.9%, p = 0.036) and after PSM (88.6% vs 70.5%, p = 0.034). Multivariate analysis identified ICIs-dTACE as an independent predictor for improved PFS (post-PSM: HR = 0.522, 95% CI 0.284–0.959; p = 0.036). Notably, 16 patients (34.8%) in the ICIs-dTACE group underwent surgical resection, achieving an R0 resection rate of 87.5% (14/16) and a major pathological response (⩾90% necrosis) in 50.0% (8/16). The safety profiles were comparable between groups, with grade ⩾3 adverse events (AEs) primarily attributable to chemotherapy. No grade 3 or higher AEs were attributed to dTACE.
Conclusion:
In this exploratory analysis, the addition of dTACE to ICIs-based therapy was associated with improved PFS and enabled surgical resection in a subset of patients with advanced sarcoma, without introducing additional severe toxicity. These findings suggest the synergistic potential of this combined modality and warrant prospective validation.
Plain language summary
This study looked at a new treatment approach for patients with advanced sarcoma, a type of cancer that is often difficult to treat. The approach combines two types of treatments: a targeted procedure called drug-eluting bead transarterial chemoembolization (dTACE) and immunotherapy drugs known as immune checkpoint inhibitors (ICIs). dTACE is a minimally invasive procedure where tiny beads loaded with chemotherapy are injected directly into the blood vessels feeding the tumor. This delivers a high dose of medicine to the cancer while blocking its blood supply. Immunotherapy drugs help the patient’s own immune system recognize and attack cancer cells. Researchers compared patients who received immunotherapy-based therapy (ICIs with or without chemotherapy or other targeted drugs) alone to those who received the same immunotherapy-based therapy plus the dTACE procedure. They found that adding dTACE was associated with improved outcomes:
- Patients lived longer without their cancer getting worse (median 7.9 months vs. 4.7 months).
- The cancer was better controlled in a higher percentage of patients.
- More patients underwent surgery after treatment (about 35% in the combination group vs. 6% in the immunotherapy-alone group). Among those who had surgery, most achieved complete tumor removal, and half showed a very strong response to treatment in the removed tissue.
- The combined treatment was well-tolerated, with no severe side effects attributed to the dTACE procedure. The side effects seen were mainly related to the chemotherapy or immunotherapy components.
In summary, this study suggests that adding the targeted dTACE procedure to immunotherapy-based therapy is associated with better disease control, longer time before the disease progresses, and more opportunities for surgery in patients with advanced sarcoma, without adding major new risks. This offers a promising new option for managing this challenging cancer.
Keywords
Introduction
Sarcomas represent a diverse spectrum of mesenchymal malignancies with distinct biological behaviors and molecular profiles. 1 While localized disease may be managed through multimodal approaches, patients with metastatic or unresectable lesions face dismal outcomes, typically demonstrating median progression-free survival (PFS) of 4–6 months with conventional therapies.2,3 Immune checkpoint inhibitors (ICIs), targeting PD-1/PD-L1 or CTLA-4 pathways to restore antitumor immunity, have revolutionized oncology, especially in melanoma and nonsmall cell lung cancer.4,5 ICIs have shown modest efficacy in select sarcoma subtypes or patients.6,7 Notably, alveolar soft part sarcoma (ASPS) stands out among sarcomas for its relative clinical susceptibility to ICIs, as demonstrated in several clinical trials. For instance, the combination of axitinib and pembrolizumab and atezolizumab monotherapy have both shown promising efficacy in patients with advanced ASPS.7,8 This culminated in the recent U.S. Food and Drug Administration approval of atezolizumab for metastatic ASPS, marking a significant regulatory milestone for immunotherapy in sarcoma. This contrasts sharply with the limited responses observed in most other sarcoma subtypes.9,10 While the exact mechanistic basis for this differential responsiveness remains incompletely defined, the generally poor outcomes in unselected sarcomas have been attributed to potential factors such as immunosuppressive tumor microenvironments and low/absent PD-L1 expression. 10 Recent advances have highlighted the importance of the tumor immune microenvironment in determining immunotherapy responses. Emerging evidence suggests that tertiary lymphoid structures (TLS) within the tumor microenvironment may serve as predictive biomarkers for ICI efficacy in sarcoma, with TLS-rich tumors demonstrating more favorable responses to PD-1 blockade. 11
Current strategies combining ICIs with tyrosine kinase inhibitors (TKIs) or cytotoxic agents show modest success,12,13 underscoring the necessity for innovative therapeutic synergies. Transarterial chemoembolization (TACE), particularly with drug-eluting beads (dTACE), delivers high-dose chemotherapy directly to tumors while embolizing their blood supply.14,15 dTACE presents a dual mechanism—localized chemotherapy delivery and vascular occlusion—with demonstrated efficacy in chemotherapy-refractory sarcomas. 14 Beyond its cytoreductive effects, dTACE may enhance systemic antitumor immunity by inducing immunogenic cell death (ICD) and releasing tumor-associated antigens, thereby potentially synergizing with ICIs. This synergy has been preliminarily validated in hepatocellular carcinoma (HCC) models showing enhanced treatment responses with combined approaches.16,17 Similarly, cholangiocarcinoma suggests that combining ICIs with regional therapies may yield superior outcomes compared to systemic therapy alone. 18 Despite promising preclinical and clinical data in HCC and other solid tumors, the role of dTACE combined with ICIs in sarcomas remains underexplored. Critically, such synergy could enable surgery—downstaging initially unresectable tumors to resectability—a pivotal goal in locally advanced/metastatic sarcoma where R0 resection remains the sole curative opportunity. 19
The synergy between dTACE and ICIs may enable surgery for unresectable sarcomas by combining rapid cytoreduction and immunogenic priming. While demonstrated in other solid tumors, 20 sarcoma-specific evidence remains limited to case reports. 21 The rarity and heterogeneity of locally advanced/metastatic sarcomas pose challenges for randomized controlled trials, necessitating robust real-world analyses. Propensity score matching (PSM) provides methodological rigor to address selection bias in retrospective cohorts, enabling more reliable evaluation of combination therapies. 22 It is important to note that this study’s retrospective design carries inherent limitations, including potential selection bias and unmeasured confounding factors, which are addressed in the discussion. This study investigates whether dTACE potentiates ICIs-based therapy to improve survival, disease control, and rates of surgery in locally advanced/metastatic sarcomas, while maintaining acceptable toxicity.
Materials and methods
Study design and ethical approval
This single-institution retrospective, exploratory cohort analysis evaluated combined ICIs-based therapy (ICIs ± chemotherapy ± TKIs) with dTACE in locally advanced/metastatic sarcomas. The study utilized clinical data from the orthopedic oncology database of a tertiary tumor referral center. The requirement for obtaining individual informed consent was waived by the Institutional Review Board of Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (No. 2026-KY-034K). The Declaration of Helsinki was strictly followed in this study. The reporting of this study conforms to the STROBE statement (Supplemental Material 1). 23
Patients
Patients with locally advanced/metastatic sarcoma who received ICIs-based therapy between May 2019 to July 2024 were screened retrospectively. The final follow-up data were updated through November 2024. Inclusion criteria included: (1) Histologically or radiologically confirmed locally advanced or metastatic sarcoma. Locally advanced disease was defined as unresectable tumors due to extensive local involvement, invasion of critical structures, or recurrent disease after prior therapy precluding curative-intent surgery; (2) ⩾1 measurable lesion through Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1; (3) Received ICIs-based therapy (ICIs ± chemotherapy ± TKIs). Exclusion criteria included (1) Received locoregional therapies (including radiotherapy) other than dTACE concurrently; (2) Incomplete clinical data; (3) >8 weeks interval between ICIs initiation and dTACE; (4) Received systemic therapies other than ICIs, chemotherapy, TKIs. The final cohort comprised two cohorts: ICIs-based therapy cohort and ICIs-dTACE cohort (ICIs-based therapy and dTACE).
Baseline variables were included as follows: demographics (age, sex), disease characteristics (clinical stage, histology, tumor size, metastatic sites), and treatment history (prior lines, chemotherapy/immunotherapy/TKIs exposure). Histology was categorized based on ICI sensitivity according to NCCN Guidelines: ASPS was classified as ICI-sensitive; myxofibrosarcoma, undifferentiated pleomorphic sarcoma, dedifferentiated liposarcoma, cutaneous angiosarcoma, and undifferentiated sarcoma as potentially ICI-sensitive; and all other sarcoma subtypes—including all bone sarcomas and soft tissue sarcomas without established ICI sensitivity—as “other subtypes. 24 The cut-off of tumor size was different between bone sarcoma (⩽8 vs >8 cm) and soft tissue sarcoma (⩽5 vs >5 cm). Collection of race/ethnicity data was waived because 98% of the regional population self-identifies as Han based on national census records.
Clinical stage was defined according to the AJCC 8th Edition staging system. For bone sarcoma, stage III was defined as high-grade tumors (G2–G3) larger than 8 cm (T3) without nodal or distant metastasis (N0, M0). Stage IV included any tumor with lung metastasis, regional lymph node metastasis, or other distant metastases, regardless of T or G status. For soft tissue sarcoma, stage III comprised locally advanced, high-grade tumors (G2–G3) larger than 5 cm (T2–T4) without nodal or distant metastasis (N0, M0). Stage IV included any tumor with regional lymph node metastasis or distant metastasis, regardless of T or G status.
Systemic therapy
ICIs (PD-1/PD-L1 inhibitors or PD-1/CTLA-4 bispecific antibodies) were administered via subcutaneous (envolimab) or intravenous routes per institutional protocols. The selection of concomitant systemic therapy (chemotherapy and/or TKIs) was individualized based on sarcoma histology, prior treatment exposure, and performance status. The most commonly used chemotherapy included gemcitabine-based combinations. The specific choice of TKI was influenced by drug accessibility within our regional healthcare system and patient tolerance. ICIs and TKIs were continued until progression, intolerable toxicity, or up to 24 months for ICIs. Chemotherapy cycles (typically ⩽6) were adjusted according to patient tolerance and clinician discretion.
dTACE procedure
Patients with large unresectable tumors or identified vascular shunts may be more willing to undergo dTACE. The decision to perform dTACE was determined through multidisciplinary team (MDT) consensus based on pretreatment imaging (dynamic contrast-enhanced MRI/CT) and clinical parameters. Patients with hypervascular tumors exhibiting dominant feeding arteries and no uncorrectable vascular shunts were considered candidates. Intraoperative angiography further validated tumor vascularity; cases with hypovascular patterns or unsafe vascular anatomy were either converted to arterial infusion chemotherapy or aborted, with such patients excluded from the dTACE cohort.
It is important to characterize the inherent differences in cohort formation for transparency. The ICIs-dTACE cohort comprised patients who were anatomically selected for the procedure, based on MDT assessment of hypervascular tumors with suitable feeding arteries. Moreover, dTACE was performed on anatomically suitable tumors regardless of whether the target was primary or metastatic, supported by evidence that locoregional treatment of metastases may confer similar benefits as primary tumor treatment in patients with HCC. 25 In contrast, the ICIs-based therapy cohort represents a broader, unselected population of patients receiving systemic immunotherapy, which included individuals with varying tumor vascularity, some of whom would not have been optimal candidates for dTACE. This reflects the real world, exploratory intent of the study: to evaluate the outcomes of the combined modality in the technically eligible subgroup against contemporary outcomes with systemic therapy alone in a heterogeneous advanced sarcoma population.
dTACE was performed using epirubicin-loaded CalliSpheres® beads (Jiangsu Hengrui Pharmaceuticals, China), with a diameter of 100–300 or 300–500 μm. Perioperative management included hydration, antiemetics, and analgesics as needed. The procedure followed standardized protocols: (1) Drug loading: Beads were loaded with 60–70 mg epirubicin per vial via ion exchange; (2) Catheterization: Under local anesthesia for adults and general anesthesia for children, a 5-French catheter was inserted via left or right femoral artery, and super-selective embolization of tumor-feeding arteries was performed; (3) Embolization endpoint: Complete occlusion of the tumor blood supplying artery. For large tumors, staged embolization may be required to achieve optimal devascularization while minimizing procedural risks.
Surgery
Postsystemic therapy resectability was reevaluated by MDT upon achieving radiographic response. Surgery encompassed curative-intent resections (limb-sparing/amputation) and select palliative procedures for controlled diseases, excluding surgeries performed for outright progression. Surgical eligibility was determined by the MDT based on confirmed improvement in local disease control, even in the presence of persistent metastases or marginal resectability. Histopathological assessment of resection margins and treatment response followed standardized protocols. Surgical decisions were made through MDT consensus based on two distinct scenarios. Curative-intent or conversion surgery was considered when radiographic response suggested that the primary tumor and/or limited metastases had become technically resectable with clear margins. Additional requirements included disease control at other sites and the ability to safely interrupt or continue systemic therapy perioperatively. Palliative surgery was considered for symptomatic patients when tumor-related symptoms required intervention, with the goal of symptom relief rather than complete disease eradication. Therefore, all surgeries reported in this study were performed after systemic therapy (with or without dTACE), and include both curative-intent resections and palliative procedures. Detailed surgical outcomes are presented in Table 4.
Follow-up and assessments
Treatment efficacy and safety were assessed via imaging and laboratory monitoring at clinical intervals. All radiological evaluations underwent independent dual-review by blinded radiologists using RECIST v1.1. The imaging schedule was tailored to clinical practice: initial assessments were typically performed every 6–8 weeks (approximately 2 treatment cycles), with intervals extending to 2–3 months for patients demonstrating prolonged disease stability. Imaging was conducted immediately upon clinical suspicion of disease progression. For surgery patients, surgery type, resection margins (R0/R1), and pathological response26,27 were recorded. PFS was defined from the start of protocol-defined therapy to radiographic progression or death from any cause. The time origin was defined as follows: for patients in the ICIs-dTACE group, PFS was calculated from the date of the first dTACE procedure; for patients in the ICIs-based therapy group, PFS was calculated from the date of first ICIs administration. Tumor responses were classified as CR (complete response), PR (partial response), SD (stable disease), or PD (progressive disease), with ORR (objective response rate; CR + PR) and DCR (disease control rate; CR + PR + SD) calculated. Adverse events (AEs) were graded per National Cancer Institute Common Terminology Criteria for Adverse Events v5.0.
Notably, the surgical complications of surgery were excluded from this analysis as they represent discrete procedural risks rather than inherent treatment toxicity. This approach aligns with the primary objective of characterizing the systemic safety profile of the investigational regimen.
Statistical analysis
Analyses used SPSS software, version 26 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism, version 10 (GraphPad Soft-ware Inc., Boston, MA, USA). Categorical data were expressed as n (%). Between-group comparisons used χ2 or Fisher’s exact tests. PSM was performed using nearest-neighbor matching with a caliper of 0.05. The propensity score was estimated via logistic regression incorporating the following clinically relevant covariates simultaneously: clinical stage (III vs IV), histology categorized by sensitivity to ICIs (ASPS, potentially sensitive subtypes, other subtypes), tumor size (stratified by AJCC thresholds for bone and soft tissue sarcomas), treatment lines of ICIs (first-line vs second-line or beyond), chemotherapy exposure (yes/no), and TKI exposure (yes/no). Survival was analyzed via Kaplan–Meier/log-rank tests. Multivariable Cox proportional hazards models incorporated significant variables and covariates demonstrating borderline significance (p < 0.10) in preliminary univariate analyses. The reverse Kaplan–Meier method was used to calculate the median follow-up time. Significance was set at two-sided α = 0.05.
Results
Patient characteristics and treatment patterns
A total of 322 patients with locally advanced/metastatic sarcoma receiving systemic therapy (ICIs ± chemotherapy ± TKIs) were screened between May 2019 and July 2024. After applying exclusion criteria, 213 patients (median age 33 years, IQR 19–52; 57.3% male) were included, with follow-up data updated through November 2024. In total, 167 patients were included in ICIs-based therapy cohort (systemic therapy), and 46 in ICIs-dTACE cohort (ICIs-based therapy and dTACE). In the ICIs-dTACE group, all dTACE procedures were performed within 8 weeks of ICIs initiation, confirming adherence to the study protocol. The median time from ICIs initiation to dTACE was 14 days (range 0–42 days). PSM (caliper = 0.05) balanced baseline covariates (clinical stage, histologic subtypes, tumor size, treatment lines, chemotherapy, and TKIs), resulting in 44 matched pairs (Figure 1). The median follow-up time was 10.1 months (95% confidence intervals (CI), 6.3–13.9).
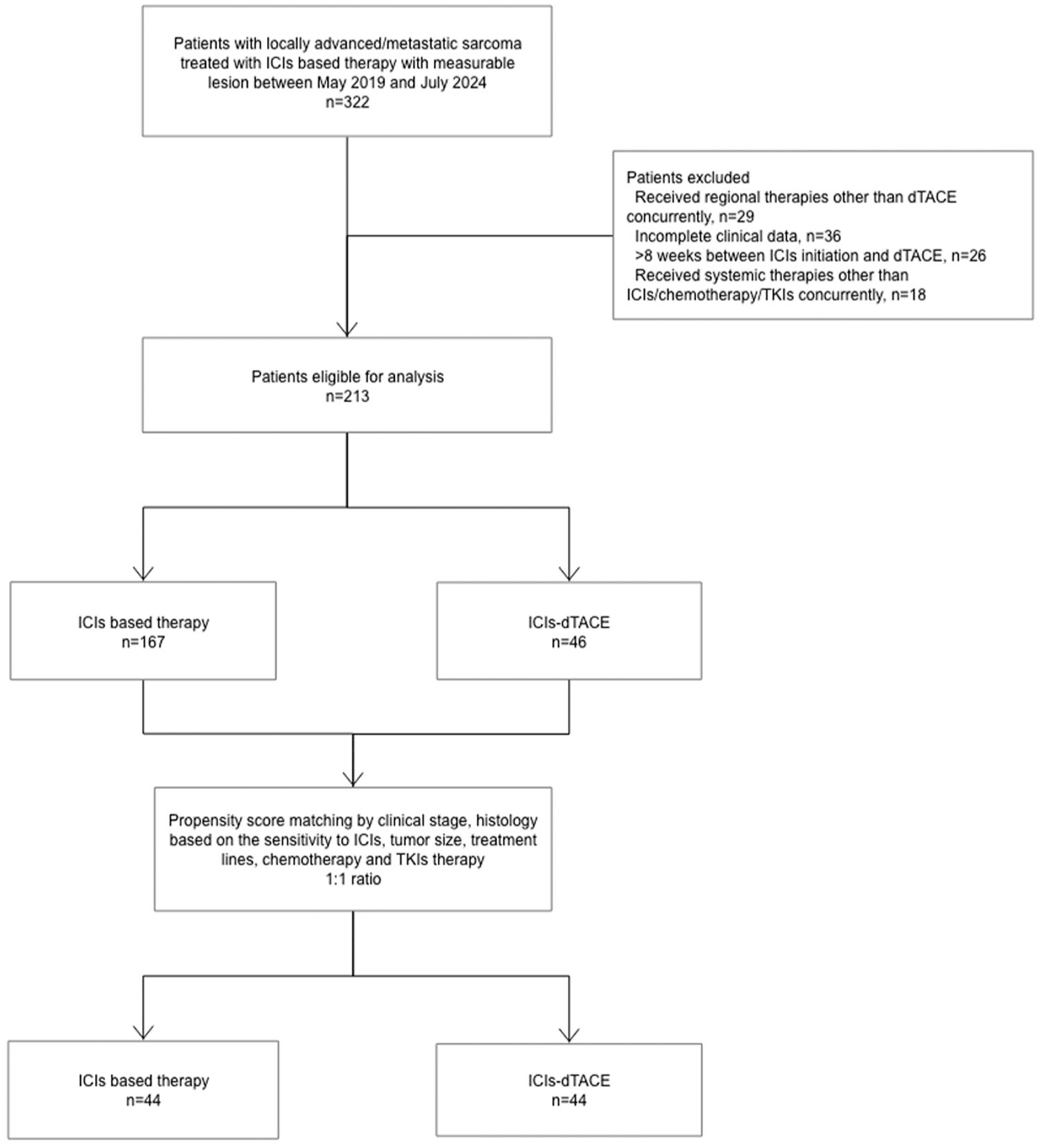
Flow diagram of patient enrollment.
The median number of prior lines of systemic therapy was 3 (range 1–6) for the overall population, with detailed prior treatment exposure summarized in Table 1 by therapeutic class. Before matching, ICIs-dTACE cohort had more patients with large tumor size than ICIs-based therapy cohort (89.1% vs 52.1%, p < 0.001; Table 1). In the ICIs-dTACE cohort, 17.4% of patients (8/46) had previously received ICIs therapy, whereas none of the patients (0/167) in the ICIs-based therapy cohort had prior ICIs exposure (Table 1). There was no difference between the two cohorts among the other baseline characteristics (Table 1). Except the characteristic of ICIs therapy, the other baseline characteristics were balanced (p > 0.05) after PSM, confirming the robustness of matching (Table 1).
Baseline characteristics and treatment patterns.

Patients received standard treatment for locoregional disease.
Surgery refers to procedures performed after systemic therapy.
ASPS, alveolar soft part sarcoma; DDLPS, dedifferentiated liposarcoma; dTACE, drug-eluting beads transarterial chemoembolization; ICIs, immune checkpoint inhibitors; LN, lymph node; STS, soft tissue sarcoma; TKIs, tyrosine kinase inhibitors; UPS, undifferentiated pleomorphic sarcoma.
A detailed summary of TKIs used in both cohorts is as follows: In the ICIs-dTACE group (n = 46), anlotinib was the most frequently used TKI (30.4%, 14/46), followed by apatinib (15.2%, 7/46), fruquintinib (13.0%, 6/46), cabozantinib (4.3%, 2/46), and lenvatinib (2.2%, 1/46). In the ICIs-based therapy group (n = 167), anlotinib was also the most common (32.3%, 54/167), followed by apatinib (21.6%, 36/167), fruquintinib (10.8%, 18/167), lenvatinib (6.0%, 10/167), and cabozantinib (1.8%, 3/167). Pazopanib and regorafenib were used in a small proportion of patients in the control group only (1.2%, 2/167 and 0.6%, 1/167, respectively). Approximately one-third of patients in the ICIs-dTACE group (34.8%, 16/46) and one-quarter in the ICIs-based therapy group (25.7%, 43/167) did not receive any TKIs. This detailed breakdown, along with the ICI distribution, has been added to Table S1.
The most frequently used ICIs were sintilimab (n = 67), camrelizumab (n = 54), and tislelizumab (n = 39; Table S1). In the ICIs-dTACE group, the most common ICIs were camrelizumab (32.6%), sintilimab (30.4%), and tislelizumab (17.4%); in the ICIs-based therapy group, the most common were sintilimab (31.7%), camrelizumab (23.4%), and tislelizumab (18.6%). PD-1 inhibitors were the predominant class in both groups, with PD-L1 inhibitors (envafolimab, adebrelimab, atezolizumab) used in a smaller proportion of patients. PD-1/CTLA-4 bispecific antibodies (cadonilimab) were used in 4.8% of patients in the control group. As shown in Table 1, the distribution of ICIs classes was well balanced between groups after PSM.
Tumor response evaluation
ORR remained comparable between arms both before (ICIs-dTACE: 13.0% vs ICIs-based therapy: 12.6%, p = 0.933) and after matching (13.6% vs 25.0%, p = 0.177). DCR numerically favored ICIs-dTACE cohort across analyses (pre-PSM: 87.0% vs 71.9%, p = 0.036; post-PSM: 88.6% vs 70.5%, p = 0.034). CR was absent in the study population (Table 2).
The overall response before and after propensity score matching.

CR, complete response; DCR, disease control rate; dTACE, drug-eluting beads transarterial chemoembolization; ICIs, immune checkpoint inhibitors; ORR, objective response rate; PD, progressive disease; PR, partial response; SD, stable disease.
Survival analysis
ICIs-dTACE cohort demonstrated superior PFS compared to ICIs-based therapy cohort, with median PFS (mPFS) of 7.9 months (95% CI 6.0–9.8) versus 4.5 months (3.3–5.7) in the overall cohort (log-rank = 7.807, p = 0.005). Kaplan–Meier analysis revealed significant stratification between arms, a benefit maintained postmatching (7.9(6.2–9.6) vs 4.7(2.5–6.9) months, log-rank = 5.517, p = 0.019; Figure 2).

Kaplan–Meier analyses of PFS in the two cohorts before (a) and after (b) PSM.
In the entire cohort, a total of 138 events contributed to the PFS analysis. Within the ICIs-dTACE group (n = 46), all 23 events were either radiographic progression (n = 21) or death without prior progression (n = 2). In the ICIs-alone group (n = 167), the 115 events consisted of 105 radiographic progressions and 10 deaths without prior progression.
Two illustrative cases are presented to demonstrate the potential of this combination strategy. The first case (Figure 3) shows a 38-year-old patient with pelvic malignant giant cell tumor with spindle cell sarcomatous transformation (pMMR/MSS/low TMB) who achieved durable response >16 months following dTACE combined with camrelizumab-based therapy. The second case (Figure S1) describes a 15-year-old patient with chemotherapy-refractory extraskeletal Ewing sarcoma/PNET of the right chest wall who underwent resection after achieving near-CR with dTACE combined with cisplatin + irinotecan, anlotinib, and camrelizumab, with durable disease control at 1-year postresection.

Durable clinical response to ICIs-dTACE in metastatic refractory pelvic malignant giant cell tumor with spindle cell sarcomatous transformation (pMMR/MSS/low TMB). Baseline hypermetabolic lesions (PET-CT), (a) and enhancing pelvic mass (MRI), (b) indicated active disease. Following multiline doxorubicin-based therapy failure (MRI), (c), epirubicin-loaded dTACE (d) combined with camrelizumab and the original therapy (chemotherapy-anlotinib) induced rapid tumor necrosis (MRI), (e) and durable anatomic regression (MRI), (f, g). Metabolic partial response (PERCIST), (h) coexisted with RECIST 1.1 partial response. Maintenance therapy (camrelizumab-anlotinib) sustains >16-month PFS (grade 1–2 toxicities).
Prognostic factors analyses
Table 3 showed the prognostic factors analyses in the whole population. Treatment cohort (ICIs-dTACE cohort, hazard ratio (HR) = 0.532, 95% CI 0.339–0.836; p = 0.006), histology based on the sensitivity to ICIs (other subtypes vs ASPS, HR = 2.791, 95% CI 1.288–6.047; p = 0.009), treatment lines (⩾2nd lines, HR = 2.446, 95% CI 1.428–4.189; p = 0.001), and chemotherapy history (HR = 2.316, 95% CI 1.445–3.711; p < 0.001) were significant predictors. Furthermore, multivariable analysis identified treatment cohort (ICIs-dTACE cohort, HR = 0.407, 95% CI 0.247–0.670; p < 0.001) as independent predictor of PFS.
Prognostic factors associated with PFS before and after propensity score matching.

ASPS, alveolar soft part sarcoma; CI, confidence interval; DDLPS, dedifferentiated liposarcoma; dTACE, drug-eluting beads transarterial chemoembolization; HR, hazard ratio; ICIs, immune checkpoint inhibitors; LN, lymph node; PFS, progression-free survival; PSM, propensity score matching; STS, soft tissue sarcoma; TKIs, tyrosine kinase inhibitors; UPS, undifferentiated pleomorphic sarcoma.
After PSM adjustment, the prognostic factors analyses were shown in Table 3. Treatment cohort (ICIs-dTACE cohort, HR = 0.533, 95% CI 0.312–0.910; p = 0.021) showed significance. Moreover, treatment cohort (ICIs-dTACE cohort, HR = 0.522, 95% CI 0.284–0.959; p = 0.036) was identified as the independent prognostic factor for PFS. A sensitivity analysis using a stratified Cox model accounting for matched pairs yielded a consistent point estimate (HR = 0.490) but with a wider CI (95% CI 0.220–1.091, p = 0.081). Of note, surgical resection was not included as a covariate in the multivariable model because it represents a posttreatment outcome rather than a baseline characteristic. Including such time-dependent variables would introduce immortal time bias and violate proportional hazards assumptions. Therefore, surgery was appropriately analyzed as a treatment outcome in Table 4.
Clinical characteristics of advanced sarcoma patients who underwent surgery after systemic therapy.

OS data are reported for patients who underwent curative-intent surgery only, as of the data cutoff date (November 2024).
ASPS, alveolar soft part sarcoma; CSC, clear cell sarcoma; DDCS, dedifferentiated chondrosarcoma; dTACE, drug-eluting beads transarterial chemoembolization; ERMS, embryonal rhabdomyosarcoma; HG sarcoma with F/MF differentiation, high-grade sarcoma with fibroblastic/myofibroblastic differentiation; ICIs, immune checkpoint inhibitors; Malignant SFT, malignant solitary fibrous tumor; OS, overall survival; PFS, progression-free survival; PR, partial response; SD, stable disease; TKIs, tyrosine kinase inhibitors; UPS, undifferentiated pleomorphic sarcoma; NR, not reported.
Surgery
Following ICIs-dTACE therapy, 34.8% (16/46) of locally advanced/metastatic sarcoma patients underwent surgery, significantly higher than the 6.0% (10/167) in the ICIs-based therapy cohort (p < 0.001; Table 1). This study reports all patients who underwent posttreatment surgery, including both curative-intent and palliative procedures. Detailed individual-level data for each operated patient, including histology, surgical margins, and pathological response, are provided in Table 4.
Among the 16 patients who underwent surgery after ICIs-dTACE therapy, 9 received curative‑intent/conversion surgery and 7 received palliative procedures. For the nine curative‑intent/conversion surgery patients, seven were initially deemed unresectable due to locally advanced disease (massive tumor volume and/or involvement of critical neurovascular structures, where R0 resection would have caused unacceptable functional loss), while the remaining two had limited metastatic disease that was controlled by systemic therapy, allowing subsequent curative resection of all sites. The seven palliative surgery patients all had metastatic disease at baseline. In most of these patients, surgery was performed for symptom relief (e.g., pain, bleeding, or neurological compromise) or for cytoreduction (tumor debulking). In a minority of cases, surgery was initially intended as curative; however, due to intraoperative findings or final pathological assessment, complete resection was not achieved, and these cases were therefore classified as palliative procedures.
In the ICIs-dTACE group (n = 16), R0 resection was achieved in 87.5% (14/16), and 50% (8/16) exhibited tumor necrosis rates ⩾90%. Femoral tumors (n = 5) emerged as the most prevalent resection site. Notably, all five cases, which would have historically required amputation, successfully underwent limb-sparing curative surgery with R0 resection. Among pelvic tumors (n = 4), two achieved exceptional pathologic necrosis rates ⩾90%.
In the ICIs-based therapy group (n = 10), R0 resection was achieved in 70% (7/10), with tumor necrosis rates ⩾90% observed in 20% (2/10). The 10 operated patients included various histologies: ASPS (n = 3), osteosarcoma (n = 2), Ewing sarcoma (n = 2), and one each of chondrosarcoma, malignant solitary fibrous tumor, and well-differentiated liposarcoma. Surgical sites included primary tumors (n = 5), pulmonary metastases (n = 2), bone metastases (n = 1), and recurrent tumors (n = 2).
At data cutoff, 62.5% (10/16) of operated patients in the ICIs-dTACE group maintained PFS beyond 6 months, including one sternal osteosarcoma case (Patient 11) with ongoing PFS exceeding 57 months, compared to 40% (4/10) in the ICIs-based therapy group.
Safety
Treatment-related AEs are detailed in Table 5. No fatal events occurred during follow-up. AEs of any grade were reported in 28 patients (60.9%) in ICIs-dTACE cohort and 99 patients (59.3%) in ICIs-based therapy cohort. Grade 3–4 AEs occurred in 10 patients (21.7%) in ICIs-dTACE cohort and 39 (23.4%) patients in ICIs-based therapy cohort. No patients in ICIs-dTACE cohort and 2(1.2%) of patients in ICIs-based therapy cohort undergoing ICIs-based therapy discontinued ICIs due to drug-related toxicity. The most common drug attributed AEs reported in ICIs-dTACE cohort and ICIs-based therapy cohort were myelosuppression (including leukopenia, thrombocytopenia, and anemia) and nausea/vomiting, consistent with the AEs of chemotherapy. Notably, no grade ⩾3 complications arose from dTACE procedures. The most common dTACE-attributed AEs in the ICIs-dTACE cohort were pain (54.3%) and fever (17.4%), followed by skin rash (15.2%) and skin necrosis (6.5%). This AE profile is consistent with the known localized effects of dTACE.
Treatment-related adverse events.

dTACE, drug-eluting beads transarterial chemoembolization; HFSR, hand-foot skin reaction; ICIs, immune checkpoint inhibitors; RCCEP, reactive cutaneous capillary endothelial proliferation.
Discussion
This study suggests that combining dTACE with ICIs-based therapy is associated with improved outcomes in advanced sarcoma, doubling mPFS (7.9 vs 4.7 months, p = 0.019) compared to systemic therapy alone. Beyond survival benefit, the regimen enabled surgical resection in 34.8% of patients—transforming palliative scenarios into opportunities for durable disease control—while maintaining a manageable safety profile. The safety profile remained manageable, with no grade ⩾3 AEs attributed to dTACE, aligning with the tolerability observed in other locoregional-immunotherapy combinations. 16 The PSM was employed to minimize selection bias and improve the comparability of the cohorts. The finding of a significant PFS benefit in the more balanced postmatch analysis strengthens the evidence for the efficacy of the combined approach. This methodological approach enhances causal inference by minimizing selection bias, 22 while the observed surgical interventions with high R0 resection rates further validate the clinical relevance of this treatment strategy. These findings highlight the potential of locoregional-systemic therapy synergy to improve outcomes for advanced sarcoma patients.
Single-agent ICIs have shown modest activity in sarcomas, with mPFS rarely exceeding 6 months in unselected cohorts. 28 The SARC028 trial reported the efficacy of pembrolizumab in unselected sarcomas with the mPFS of 18 weeks for soft tissue sarcoma and 8 weeks for bone sarcoma. 9 Chemotherapy agents and TKIs may synergize with ICIs by depleting immunosuppressive cells or normalizing tumor vasculature. However, current strategies combining chemotherapy or TKIs with ICIs in advanced sarcoma also show limited clinical synergy, likely due to immunosuppressive tumor microenvironments and heterogeneous responses.12,29–31 ICIs-based therapy cohort in our study exhibited a mPFS of 4.7 months, consistent with these reports. This underscores the need for combination strategies to amplify immune activation.
The proposed synergistic mechanism—dTACE-induced ICD potentiating ICIs—is plausible but remains speculative. Preclinical studies suggest that locoregional therapies like TACE enhance systemic immune responses by releasing tumor antigens and upregulating PD-L1 expression, thereby potentiating ICIs. 32 dTACE delivers localized chemotherapy while occluding tumor-feeding vessels, causing hypoxia and necrosis. 33 This process releases tumor-associated antigens, damage-associated molecular patterns, and cytokines, which recruit dendritic cells and prime T-cell responses,34,35 potentially overcoming the immunosuppressive tumor microenvironment characteristic of sarcomas.36,37
However, emerging evidence highlights that additional factors may critically influence immunotherapy responses in sarcoma. TLS—ectopic lymphoid aggregates that facilitate local B-cell maturation and T-cell priming—have been identified as key determinants of ICIs efficacy. Fu et al. 11 recently demonstrated that in patients with pretreated advanced sarcoma receiving sintilimab plus anlotinib, TLS presence correlated with improved outcomes, suggesting TLS may serve as a predictive biomarker for immunotherapy responsiveness in sarcoma. Other microenvironmental features, including tumor-associated macrophages, myeloid-derived suppressor cells, and specific chemokine signaling pathways, likely modulate responses to combined locoregional-immunotherapy approaches.
Our observation of durable responses in immunologically “cold” tumors (Microsatellite Stable/Proficient Mismatch Repair/Tumor Mutational Burden-low) following dTACE-ICI therapy (Figure 3) suggests that dTACE may overcome certain immune resistance mechanisms through antigen release and microenvironment remodeling. However, without paired pre- and posttreatment tissue analysis, the exact mechanisms remain undefined. Prospective studies with systematic tissue collection are needed to characterize changes in TLS density, immune cell infiltration, and other microenvironmental features before and after dTACE-ICI therapy.
Our findings align with emerging evidence supporting the combination of locoregional and immunotherapies. For instance, several studies had reported improved PFS with TACE plus ICIs in HCC,16,17 though sarcoma-specific data remain scarce. In this context, dTACE offers a critical advantage over conventional transarterial chemoembolization (cTACE) by minimizing systemic drug exposure, thereby reducing treatment-related AEs while preserving immunogenic tumor cell death—a feature essential for enhancing systemic immune responses when integrated with ICIs, potentially explaining the absence of severe dTACE-related AEs. The safety profile of the dTACE combination was comparable to ICIs-based therapy alone, with pain and skin injury related to TACE procedures being the primary added toxicity.
This ICIs-dTACE regimen achieved a mPFS of 7.9 months. This outcome compares favorably with a historical benchmark of 3.9 months for conventional TACE alone at our center 15 and approaches the 9.5 months reported for intensive dTACE monotherapy 14 which required a median of 3.6 procedures in a highly selected cohort. The ability of our combination to achieve substantial disease control with only 1–2 dTACE sessions underscores its clinical efficiency, leveraging well-tolerated local therapy to potentiate systemic immunotherapy and reduce procedural burden.
The ICIs-dTACE regimen was associated with surgical resection in 34.8% (16/46) of patients, achieving high R0 resection (87.5%) and major pathological response (50%) rates. While Long et al. 38 reported higher resection rates (85.7%) with a different combination therapy, this discrepancy likely reflects fundamental differences in patient populations. Our cohort predominantly consisted of metastatic and heavily pretreated patients, who inherently have lower surgical eligibility. The efficacy of dTACE may stem from its dual mechanism of epirubicin-mediated rapid cytoreduction and reversal of the immunosuppressive microenvironment, as illustrated by the durable response in a pMMR/MSS/low-TMB patient (Figure 3). These results establish a new benchmark for locoregional-systemic synergy in a difficult-to-treat population.
Unlike HCC studies reporting higher ORR with combination therapy,17,25 our study observed comparable ORR between cohorts. Notably, the lack of significant differences in ORR between cohorts, despite improved PFS, mirrors findings in other solid tumors.29,39 This apparent paradox likely reflects the unique mechanism of dTACE-ICI combination: dTACE-induced tumor necrosis (50% of resected specimens exhibited ⩾90% necrosis) may not be captured by RECIST criteria, while localized cytoreduction can render marginally resectable tumors technically operable even without systemic PR. Furthermore, immunotherapy may prolong disease control through delayed immune effects that extend beyond conventional tumor shrinkage. Thus, PFS may better capture the biological activity of this combination than ORR alone. Subgroup analysis by histology (categorized by ICI sensitivity) demonstrated that the PFS benefit was observed across a histologically diverse cohort, though the wide CIs preclude precise prognostic estimates for individual subtypes.
After PSM, the ICIs-based therapy group contained a higher proportion of soft tissue sarcomas than the ICIs-dTACE group (72.7% vs 54.5%, p = 0.076). Given evidence that soft tissue sarcomas may be more responsive to immunotherapy, 9 this imbalance would bias results against the ICIs-dTACE group, suggesting our observed PFS benefit may be underestimated. The balanced distribution of ICI-sensitive subtypes (p = 0.736) and multivariable adjustment further support the robustness of this finding. Tumor size cutoffs were stratified by histologic origin (5 cm for soft tissue, 8 cm for bone sarcomas) according to AJCC prognostic thresholds40,41; the observation that larger tumors exhibited superior response may reflect their greater vascularity enhancing susceptibility to embolization and subsequent antigen release.
This study has several limitations inherent to its retrospective, exploratory design. The sample size and histological heterogeneity preclude robust subgroup analyses and may lead to model overfitting. While PSM was employed, the fundamental difference in treatment eligibility between cohorts—wherein the control group included patients ineligible for dTACE—represents the principal limitation, cautioning against direct causal inference. Sensitivity analysis using a stratified Cox model accounting for matched pairs yielded a consistent point estimate (HR = 0.490) but with a wider CI (95% CI 0.220–1.091, p = 0.081), reflecting the loss of power inherent in matched-pair designs and the sensitivity of statistical significance to the analytical method used. Given that the upper bound of the primary analysis CI approached 1.0 (0.959), the statistical significance of the PFS benefit should be interpreted with caution. These factors, alongside the selection bias toward hypervascular tumors (a poor prognostic feature itself 42 ), underscore the hypothesis-generating nature of our findings. The overall AE rate in this retrospective study is lower than that typically reported in prospective trials, likely reflecting underdocumentation of mild, self-limited events in routine clinical records. However, grade ⩾3 AEs requiring medical intervention were reliably captured and are accurately reported.
Conclusion
This exploratory, retrospective study suggests that combining dTACE with ICIs-based therapy significantly improves survival and enables surgery in patients with advanced sarcoma, transforming palliative scenarios into opportunities for durable disease control. These findings warrant prospective validation to standardize protocols and identify predictive biomarkers.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261450424 – Supplemental material for Drug-eluting bead transarterial chemoembolization combined with immune checkpoint inhibitors is associated with improved progression-free survival in locally advanced or metastatic sarcoma: a retrospective propensity score-matched analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359261450424 for Drug-eluting bead transarterial chemoembolization combined with immune checkpoint inhibitors is associated with improved progression-free survival in locally advanced or metastatic sarcoma: a retrospective propensity score-matched analysis by Chenliang Zhou, Hongtao Li, Guowei Qian, Wenxi Yu, Shuier Zheng, Zan Shen and Yonggang Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-2-tam-10.1177_17588359261450424 – Supplemental material for Drug-eluting bead transarterial chemoembolization combined with immune checkpoint inhibitors is associated with improved progression-free survival in locally advanced or metastatic sarcoma: a retrospective propensity score-matched analysis
Supplemental material, sj-jpg-2-tam-10.1177_17588359261450424 for Drug-eluting bead transarterial chemoembolization combined with immune checkpoint inhibitors is associated with improved progression-free survival in locally advanced or metastatic sarcoma: a retrospective propensity score-matched analysis by Chenliang Zhou, Hongtao Li, Guowei Qian, Wenxi Yu, Shuier Zheng, Zan Shen and Yonggang Wang in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.