
Abstract
Background:
Anaplastic lymphoma kinase-targeted tyrosine kinase inhibitors (ALK-TKIs) have revolutionized the treatment of non-small-cell lung cancer (NSCLC). However, several key issues remain unresolved. Specifically, the impact of prior chemotherapy on ALK-TKI efficacy is unclear, the impact of MET overexpression on ALK-TKI efficacy remains unclear, and the dynamic changes in programmed death ligand 1 (PD-L1) expression during the development of TKI resistance are not fully understood.
Objective:
This study aimed to evaluate the efficacy of ALK-TKIs across different treatment lines, analyze the impact of MET expression on treatment outcomes, and investigate changes in PD-L1 expression before and after the development of resistance.
Design:
Retrospective cohort study.
Methods:
A retrospective analysis was conducted on 259 patients with ALK-positive NSCLC treated at Zhejiang Cancer Hospital between 2011 and 2022 to compare the efficacy of ALK-TKIs administered as first-line therapy versus after chemotherapy. Immunohistochemical staining was used to assess MET and PD-L1 expression. Survival analysis was performed using the Kaplan–Meier method and the log-rank test.
Results:
Crizotinib showed no significant difference in progression-free survival (PFS) or overall survival (OS) between first-line and post-chemotherapy use (PFS: p = 0.803; OS: p = 0.761). For second-generation ALK-TKIs, first-line treatment had numerically longer PFS compared to post-chemotherapy (alectinib: 41 vs 24 months; ceritinib: 30 vs 8 months), but these differences were not statistically significant after adjustment (p = 0.120 and 0.284, respectively). OS did not differ significantly between the two treatment sequences for either drug. Notably, among patients treated with alectinib, those with MET overexpression had significantly shorter PFS (12 vs 42 months; p = 0.011) and OS (41 months vs not reached; p = 0.001) compared with MET-negative patients. There was no significant change in PD-L1 expression following resistance (p = 0.248).
Conclusion:
ALK-TKIs have shown a tendency to improve patient survival in both first-line and post-chemotherapy settings. Among patients treated with alectinib, there appears to be a trend toward shorter PFS and OS in those with MET overexpression. In a limited number of matched samples, PD-L1 expression did not change significantly after TKI resistance, although a slight increase was observed.
Introduction
Lung cancer is the most common malignancy worldwide and remains the leading cause of cancer-related death. 1 Non-small-cell lung cancer (NSCLC) accounts for most cases, with adenocarcinoma as the predominant subtype. Advances in molecular medicine and targeted therapies have shifted the treatment of NSCLC from conventional chemotherapy to personalized therapy and immunotherapy. Despite these improvements, the overall prognosis for patients with NSCLC remains poor. Anaplastic lymphoma kinase (ALK) is an important therapeutic target in NSCLC. In 2007, Soda et al. 2 first identified the EML4-ALK fusion gene, marking the beginning of targeted therapy for this molecular subtype. ALK rearrangements are observed in approximately 5% of NSCLC patients, primarily among non-smokers or light smokers with adenocarcinoma, constituting a molecular subgroup with unique clinical and pathological characteristics.3–6 ALK-targeted tyrosine kinase inhibitors (TKIs) can significantly prolong patients’ progression-free survival (PFS),7,8 making ALK one of the key targets for precision therapy. Currently available ALK-TKIs have expanded from the first-generation drug crizotinib to include second-generation inhibitors such as alectinib, brigatinib, ceritinib, and ensartinib, as well as the third-generation drug lorlatinib. 9 Large-scale clinical trials have demonstrated that second-generation TKIs are superior to first-generation drugs in the first-line setting, and second-generation drugs, such as alectinib, have become the standard of care for first-line therapy.10,11 Within this treatment landscape, research on sequential therapy has naturally focused on strategies for switching between different TKIs. In real-world practice, chemotherapy followed by ALK-TKIs is another commonly used sequential strategy. This may occur due to delayed pathological testing at initial diagnosis, limited drug availability, or patient preference. There is currently a lack of sufficient evidence-based data to determine whether prior chemotherapy diminishes the efficacy of subsequent ALK-TKIs. In the PROFILE 1014 study, 12 84.2% of patients in the first-line chemotherapy group crossed over to crizotinib after disease progression. Their overall survival (OS) reached 49.5 months, which was comparable to that of the first-line crizotinib group. ALK-TKIs administered following chemotherapy continued to confer meaningful survival benefit.
While second-generation ALK-TKIs, such as alectinib, have become the standard first-line treatment, research on the impact of prior chemotherapy on their efficacy remains limited. This study aimed to investigate the impact of prior chemotherapy on the efficacy of sequential ALK-TKI therapy using a real-world cohort analysis, to provide guidance for clinical decision-making.
The MET receptor is encoded by the MNNG HOS Transforming gene (MET) on chromosome 7 (7q21-31),13,14 with hepatocyte growth factor as its ligand. Although MET activation supports wound healing and embryonic development, persistent MET signaling in advanced cancers promotes proliferation, motility, migration, and invasion.15,16 This aberrant activation often results from genetic alterations or dysregulation of MET, 17 with common mechanisms including MET amplification, mutation, and overexpression. Significant progress has been made in targeted therapies for MET gene alterations (such as MET exon 14 skipping mutations and MET amplification). In China, several selective MET inhibitors have been approved for the treatment of NSCLC with MET exon 14 skipping mutations, including savolitinib, glumetinib, bozitinib, capmatinib, and tepotinib. 18 In addition, crizotinib, a first-generation ALK-TKI, is recommended by the NCCN guidelines for the treatment of NSCLC with high-level MET amplification or METex14 skipping mutations due to its concurrent anti-MET activity. However, the clinical significance and therapeutic value of MET protein overexpression—a more common phenomenon—in NSCLC remain unclear. This observation may be of particular clinical relevance in ALK-positive patients. Feng et al. 19 found that MET overexpression was more common in ALK-positive NSCLC than in ALK-negative NSCLC (66.7% vs 37.3%; p = 0.04), suggesting that this co-expression may have specific clinical significance. In epidermal growth factor receptor (EGFR)-mutated NSCLC, previous studies have explored the therapeutic value of MET overexpression. Scagliotti et al. 20 studied patients with EGFR-mutated NSCLC. They found that in those with MET overexpression, adding emibetuzumab to erlotinib significantly prolonged median PFS (20.7 vs 5.4 months).
This suggested that patients with MET overexpression may be a potential subgroup to benefit from the combination of EGFR-TKIs and MET inhibitors. Whether MET overexpression in ALK-positive NSCLC represents a viable therapeutic target remains unclear. Theoretically, given that crizotinib possesses dual inhibitory activity against both ALK and MET, it may offer unique therapeutic advantages in ALK-positive patients with MET overexpression. Preliminary research by Chen et al. 21 provided supporting evidence for this, as they reported that crizotinib achieved higher objective response rates (ORR) and longer PFS in ALK-positive patients with MET overexpression. However, as clinical practice has evolved, second-generation ALK-TKIs (such as alectinib) have gradually replaced crizotinib as the standard first-line treatment. Unlike crizotinib, these second-generation drugs lack anti-MET activity; therefore, their efficacy in this specific subgroup with MET overexpression remains uncertain. Currently, there is a lack of research on whether MET overexpression affects the efficacy of second-generation ALK-TKIs. By analyzing the association between MET overexpression and the efficacy of alectinib, this study aimed to provide preliminary real-world evidence addressing this clinical question. Programmed death receptor-1 (PD-1) is an immune checkpoint molecule expressed on T cells. When PD-1 binds to its ligand PD-L1, it suppresses T-cell activity and induces T-cell exhaustion.22,23 This mechanism allows tumor cells to evade recognition and elimination by the immune system, thereby promoting tumor progression. Immune checkpoint inhibitors (ICIs) that block the PD-1/PD-L1 signaling pathway have demonstrated encouraging efficacy in advanced or metastatic NSCLC by reactivating the antitumor immune response.24–28 However, the efficacy of immunotherapy in ALK-driven NSCLC is generally limited. Recent studies have shown that the ORR for pembrolizumab combined with chemotherapy in ALK-positive patients was only 29%, with a median PFS of just 2.9 months. 29 Consequently, international guidelines now explicitly exclude ALK-positive patients from the primary indications for immunotherapy. 30 Nevertheless, a small number of case reports suggest that some ALK-positive patients may benefit from immunotherapy following TKI resistance.31,32 Further investigation is warranted to determine whether ALK-TKI resistance alters the tumor immune microenvironment and induces dynamic changes in PD-L1 expression. It also remains unclear whether these changes can guide the selection of subsequent immunotherapy.
This retrospective study analyzed ALK-positive NSCLC patients treated with targeted therapy at Zhejiang Cancer Hospital. This study aimed to compare the efficacy of different ALK-TKIs, examine the effect of prior chemotherapy on treatment outcomes, evaluate MET expression and its influence on ALK-TKI efficacy, and assess PD-L1 expression before and after resistance. These findings may help guide more precise treatment strategies and support clinical decision-making.
Materials and methods
Study cohort
This study included 259 ALK-positive NSCLC patients treated with ALK-TKIs at Zhejiang Cancer Hospital (Hangzhou, China) from November 2011 to February 2022. The inclusion criteria were as follows: (1) NSCLC confirmed by histology or cytology; (2) ALK rearrangement confirmed by immunohistochemistry (IHC) or next-generation sequencing (NGS) testing; (3) prior treatment with at least one ALK-TKI (crizotinib, alectinib, or ceritinib); and (4) availability of clinical follow-up data. Patients with other driver gene mutations (e.g., EGFR, ROS1) or a history of prior immunotherapy were excluded. This study included not only stage IV patients but also some stage IIIB/IIIC patients who were unsuitable for or refused curative chemoradiotherapy. For these unresectable locally advanced cases, the treatment intent aligns with that of stage IV disease; therefore, systemic ALK-TKI therapy is a clinically appropriate option in routine practice. Given the retrospective design and the inclusion of deceased patients, the Ethics Committee waived the requirement for individual written informed consent.
Of the 259 patients included in the study, some received ALK-TKIs as first-line therapy, while others began ALK-TKI treatment only after chemotherapy. The latter group included patients who switched to ALK-TKIs either while remaining progression-free during chemotherapy or after disease progression on chemotherapy. The remaining patients began ALK-TKI treatment in later lines of therapy. Archived tumor specimens from 103 ALK-positive NSCLC cases were evaluated for MET expression using IHC. PD-L1 expression was further assessed in 17 patients with paired tissue samples collected before ALK-TKI treatment and after acquired resistance. Due to the retrospective design and the lengthy study period, records of specific chemotherapy regimens, including drug types, cycles, and maintenance therapy, were incomplete in some earlier medical records. Therefore, a detailed stratified analysis of prior chemotherapy was not conducted in this study.
Immunohistochemistry
MET immunohistochemical analysis was carried out on the BenchMark XT automated system (Ventana, Tucson, AZ, USA) following the standard manufacturer’s protocol. Tissue sections underwent deparaffinization with EZ Prep and heat-induced epitope retrieval with CCI buffer, then were incubated with the CONFIRM Anti-Total MET primary antibody (clone SP44). Detection was performed using the ultraView DAB detection system, followed by counterstaining with Hematoxylin II and Bluing Reagent. MET expression was graded using a four-tier scale: 0 (no staining or staining in <50% of tumor cells), 1+ (>50% of tumor cells with weak intensity or <50% with moderate/strong intensity), 2+ (>50% with moderate/strong intensity and <50% with strong intensity), and 3+ (>50% with strong intensity). In line with published criteria, 33 MET overexpression was defined as moderate or strong staining in >50% of tumor cells.
PD-L1 IHC was performed following the protocol outlined by Fan et al. 34 The tumor proportion score (TPS) was determined by a board-certified pathologist from a commercial laboratory and categorized as negative (TPS 0%–1%), low (TPS 1%–49%), or high (TPS ⩾50%), based on existing classification guidelines. 35 Two pathologists independently evaluated all IHC results. A sample was considered PD-L1 positive if TPS was ⩾1%, while those showing no staining or a TPS <1% were classified as negative.
Statistical analysis
Categorical variables, including the number of treatment lines and MET status, were assessed for their association with clinical characteristics using the Pearson Chi-square test. Survival analyses were performed with Kaplan–Meier curves and log-rank tests. Univariable and multivariable Cox proportional hazards models were used to identify prognostic factors; variable selection for the multivariable Cox regression model was based on prior clinical knowledge and existing literature. The included covariates comprised clinically relevant factors such as age, sex, smoking history, TNM staging, sites of metastasis (brain, bone, liver, lung, and pleura), surgical history, and number of treatment lines. Results were presented as hazard ratios (HRs) with 95% confidence intervals (CI), and the proportional hazards assumption was assessed using the Schoenfeld residual test. The rank-sum test was employed to assess differences in PD-L1 expression before and after the onset of resistance. The Benjamini–Hochberg method was used to correct the false discovery rate for multiple comparisons in the primary survival analysis. p-Values in the baseline characteristics table were for descriptive purposes only and are not adjusted for multiple comparisons. Due to the limited sample size, no formal tests were conducted for interaction terms. Statistical significance was set at p < 0.05. All analyses were performed using SPSS (Version 29.0, IBM Corp., Armonk, NY, USA) and R (Version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria). This observational study report adheres to the Statement on Reporting Observational Studies in Epidemiology (STROBE). 36 The complete STROBE checklist is provided as Supplemental Table 1.
Sensitivity analysis
To ensure the robustness of the study results, we conducted the following sensitivity analyses as part of our primary statistical plan. First, because the number of treatment lines violated the proportional hazards assumption in the initial PFS model (Schoenfeld residual test, p < 0.05), we adjusted for it as a stratification factor rather than a conventional covariate in the final model. Second, to minimize potential time-related bias, the start of follow-up for survival analysis was defined as the TKI initiation date rather than the chemotherapy initiation date. Third, to control for the risk of Type I errors resulting from multiple comparisons, the Benjamini–Hochberg correction was applied to p-values from survival-related comparisons between first-line and post-chemotherapy treatments. p-Values in the baseline characteristics table were not corrected, as they were used for descriptive purposes only.
Treatment and follow-up
As of the last follow-up date (December 31, 2023), disease progression or death had occurred in 87 patients, while 172 remained alive. PFS was calculated from the start of ALK-TKI treatment until either disease progression or death. OS was measured from the initial diagnosis of NSCLC to the date of death or the last confirmed follow-up. To avoid bias due to survival time, the follow-up period for the survival analysis began at the start of ALK-TKI treatment, rather than at the start of prior chemotherapy. For patients who switched to ALK-TKI without progression during chemotherapy, the risk period was calculated from the date TKI treatment began.
Results
Patient characteristics
This study included 259 ALK-positive NSCLC patients (124 males and 135 females) with a median age of 65 years. According to the 9th edition TNM staging system, 56 patients had stage III disease and 203 had stage IV disease. The non-smoker-to-smoker ratio was approximately 9:5. All cases were lung adenocarcinoma. Of the patients, 140 (54.1%) received ALK-TKIs as first-line therapy. Among the 80 patients with prior chemotherapy, 18 (7.0%) switched to ALK-TKIs after ALK mutation detection without progression, and 62 (23.9%) started ALK-TKIs as second-line therapy after progression on chemotherapy. The remaining 39 patients received ALK-TKIs in later treatment lines. Crizotinib was administered to 62 patients (23.9%), alectinib to 159 (61.4%), and ceritinib to 38 (14.7%). ALK fusion types included EML4-ALK in 127 patients (49.0%). Another 126 patients (48.6%) had ALK mutations identified by IHC only, without NGS, which prevented further classification. Rare fusion types included one SETD2-ALK, one CNOT11-ALK, and one HIP1-ALK case (each 0.3%). Three patients (1.2%) exhibited multiple ALK fusions, including EML4-ALK, KIF5B-ALK, KLC1-ALK, and TFG-ALK. Baseline characteristics of patients receiving first-line ALK-TKIs and those treated after chemotherapy are summarized in Table 1.
Baseline characteristics of ALK-positive NSCLC patients receiving first-line versus post-chemotherapy ALK-TKIs.
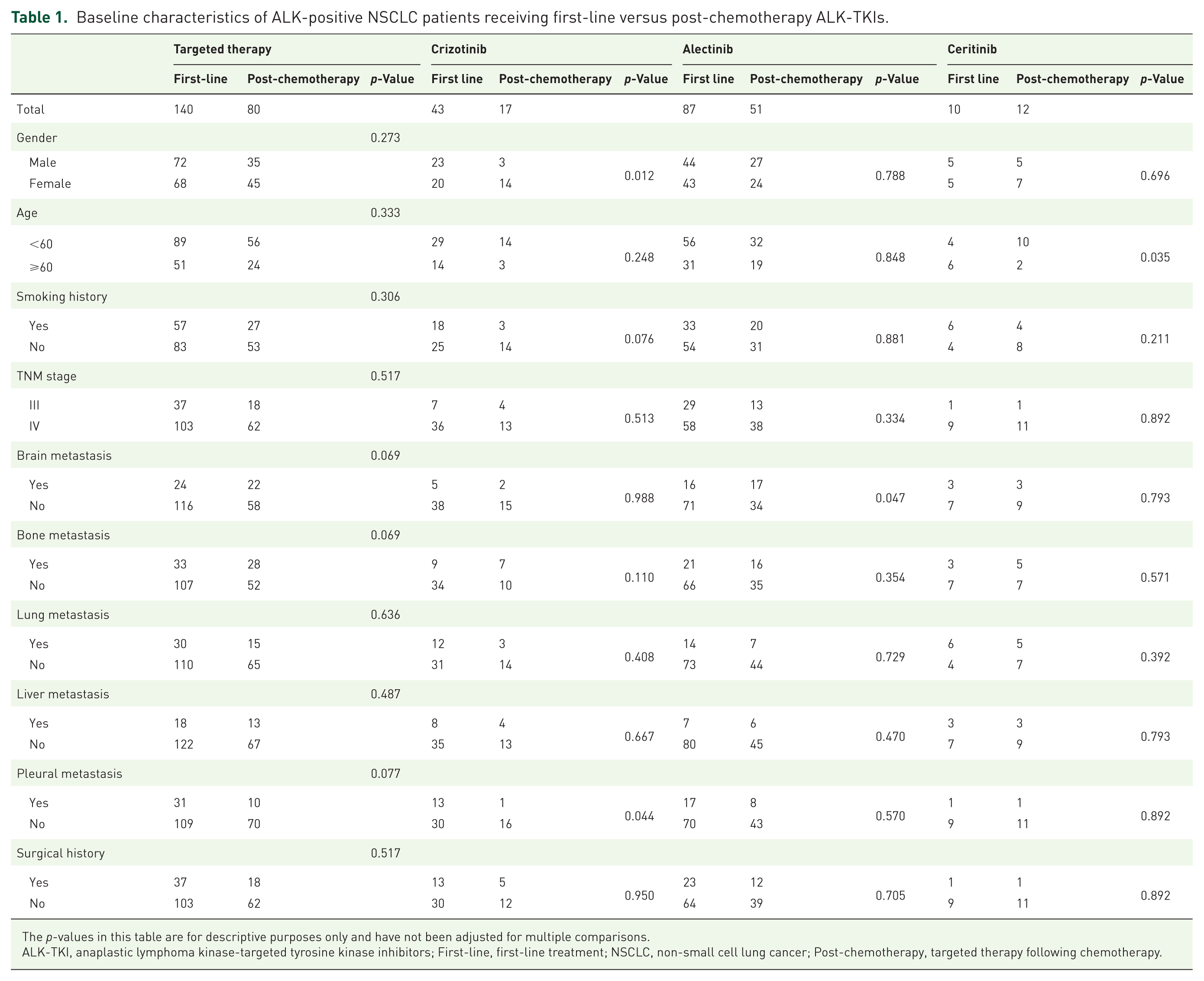
The p-values in this table are for descriptive purposes only and have not been adjusted for multiple comparisons.
ALK-TKI, anaplastic lymphoma kinase-targeted tyrosine kinase inhibitors; First-line, first-line treatment; NSCLC, non-small cell lung cancer; Post-chemotherapy, targeted therapy following chemotherapy.
Clinical outcomes and correlation factors of TKI efficacy
In the first-line ALK-TKI group, median PFS was 29 months (95% CI: 20.224–37.776), with 3- and 5-year PFS rates of 32% and 25%, respectively. Median OS reached 93 months (95% CI: 80.115–105.885), and the 3- and 5-year OS rates were 76% and 66%. Among patients with a history of prior chemotherapy, the median PFS was 18 months (95% CI: 12.586–23.414), and the 3- and 5-year PFS rates were both 26%. Their median OS was 87 months (95% CI: 61.220–112.780), with 3- and 5-year OS rates of 70% and 59% (Supplemental Table 2). PFS showed a significant difference between groups (HR: 1.484; p = 0.022), but after adjustment, the p-value was 0.11, indicating the difference was no longer statistically significant. Similarly, OS did not show a significant difference between the two groups (HR: 1.315; p = 0.274; adjusted p = 0.422).
Crizotinib demonstrated comparable efficacy whether used as first-line or subsequent therapy: median PFS was 16 months (95% CI: 11.808–20.192) in first line and 15 months (95% CI: 11.023–18.977) after chemotherapy, with no significant difference in PFS (HR: 1.116; p = 0.723; adjusted p = 0.803) or OS (71 months (95% CI: 41.570–100.430) vs not reached (NR; 95% CI: not estimable (NE)); HR: 0.800, p = 0.609, adjusted p = 0.761). In patients treated with alectinib, a comparison of efficacy between first-line treatment and treatment following chemotherapy showed that the median PFS was 41 months (95% CI: 36.585–45.415) in the first-line treatment group and 24 months (95% CI: 19.704–28.296) in the treatment-following-chemotherapy group. Unadjusted analysis suggested a significant difference between the two groups (HR: 1.651; p = 0.030); however, after adjustment for multiple comparisons, this difference was no longer statistically significant (adjusted p = 0.120). Regarding OS, the median OS in the first-line treatment group was 87 months (95% CI: 63.043–110.957), while it had not yet been reached in the post-chemotherapy treatment group; the difference between the two groups was also not statistically significant (HR: 1.826; p = 0.108; adjusted p = 0.240). In the ceritinib group, median PFS was 30 months (95% CI: 21.052–38.948) with first-line use and 8 months (95% CI: 2.908–13.092) after chemotherapy, with no statistically significant differences in either PFS (HR: 2.832; p = 0.051; adjusted p = 0.170) or OS (42 months (95% CI: NE) vs 36 months (95% CI: 28.190–43.810); HR: 4.129, p = 0.142, adjusted p = 0.284). Survival curves were generated in Figure 1(a)–(f). Although the adjusted p-values in each drug subgroup did not reach statistical significance, the numerical trends and survival curves suggested a potential trend toward superior survival outcomes with first-line ALK-TKI therapy compared to targeted therapy following chemotherapy. This observational finding suggests that prior chemotherapy may have some impact on the efficacy of subsequent ALK-TKI therapy; however, due to limitations in sample size and baseline differences, further research is needed to validate these findings.
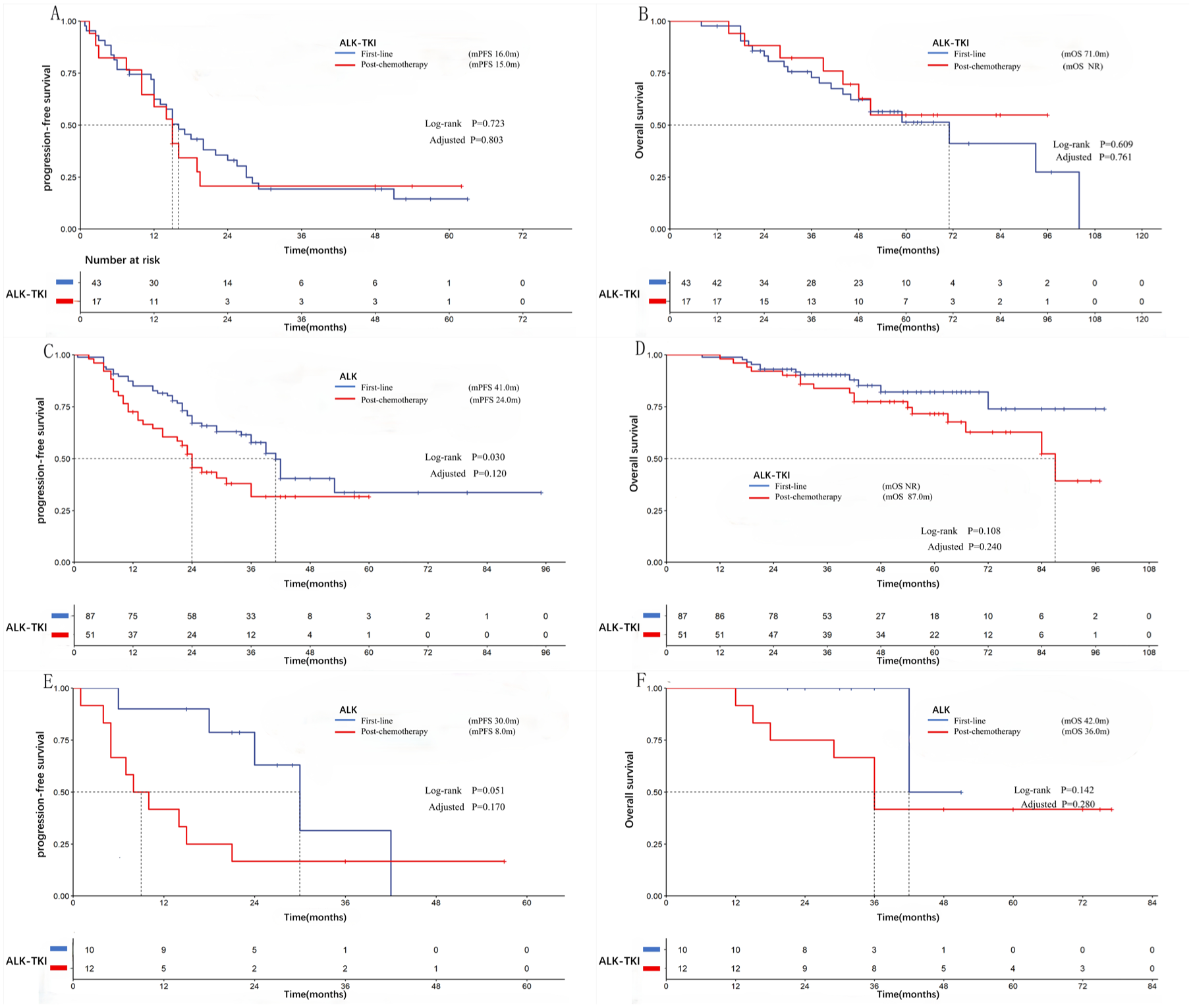
Kaplan–Meier estimates of PFS and OS comparing first-line versus post-chemotherapy use of ALK-TKIs: crizotinib (a, b), alectinib (c, d), and ceritinib (e, f).
Survival outcomes were compared across three treatment strategies: first-line ALK-TKIs, second-line ALK-TKIs initiated after progression on chemotherapy, and switching to ALK-TKIs before progression during chemotherapy. The first-line group achieved a median PFS of 29 months (95% CI: 20.224–37.776) and a median OS of 93 months (95% CI: 80.115–105.885). In the second-line post-progression group, median PFS was 15 months (95% CI: 9.566–20.434) and median OS was 84 months (95% CI: 52.348–115.652). The pre-progression switch group showed a median PFS of 24 months (95% CI: 22.302–25.698), with median OS not reached (95% CI: NE). Statistical analysis indicated a significant PFS difference between the first-line and second-line post-progression groups (29 vs 15 months; HR: 1.676, p = 0.004, adjusted p = 0.027), although OS did not differ significantly (93 vs 84 months; HR: 1.446, p = 0.159, adjusted p = 0.289). No significant differences in PFS (29 vs 24 months; HR: 0.929, p = 0.832, adjusted p = 0.876) or OS (93 months vs not reached; HR: 0.835, p = 0.708, adjusted p = 0.833) were observed between the first-line and pre-progression switch groups. Similarly, comparisons between the second-line post-progression and pre-progression switch groups showed no significant differences in PFS (15 vs 24 months; HR: 0.550, p = 0.091, adjusted p = 0.260) or OS (84 months vs not reached; HR: 0.548, p = 0.228, adjusted p = 0.380). Corresponding survival curves are presented in Figure 2(a)–(f). Based on the numerical trends, survival outcomes appear to be better with first-line targeted therapy than with targeted therapy following chemotherapy, regardless of whether the latter is initiated after disease progression or as a pre-progression switch. However, due to limitations in sample size and study design, this observational finding requires further validation in larger-scale prospective studies.
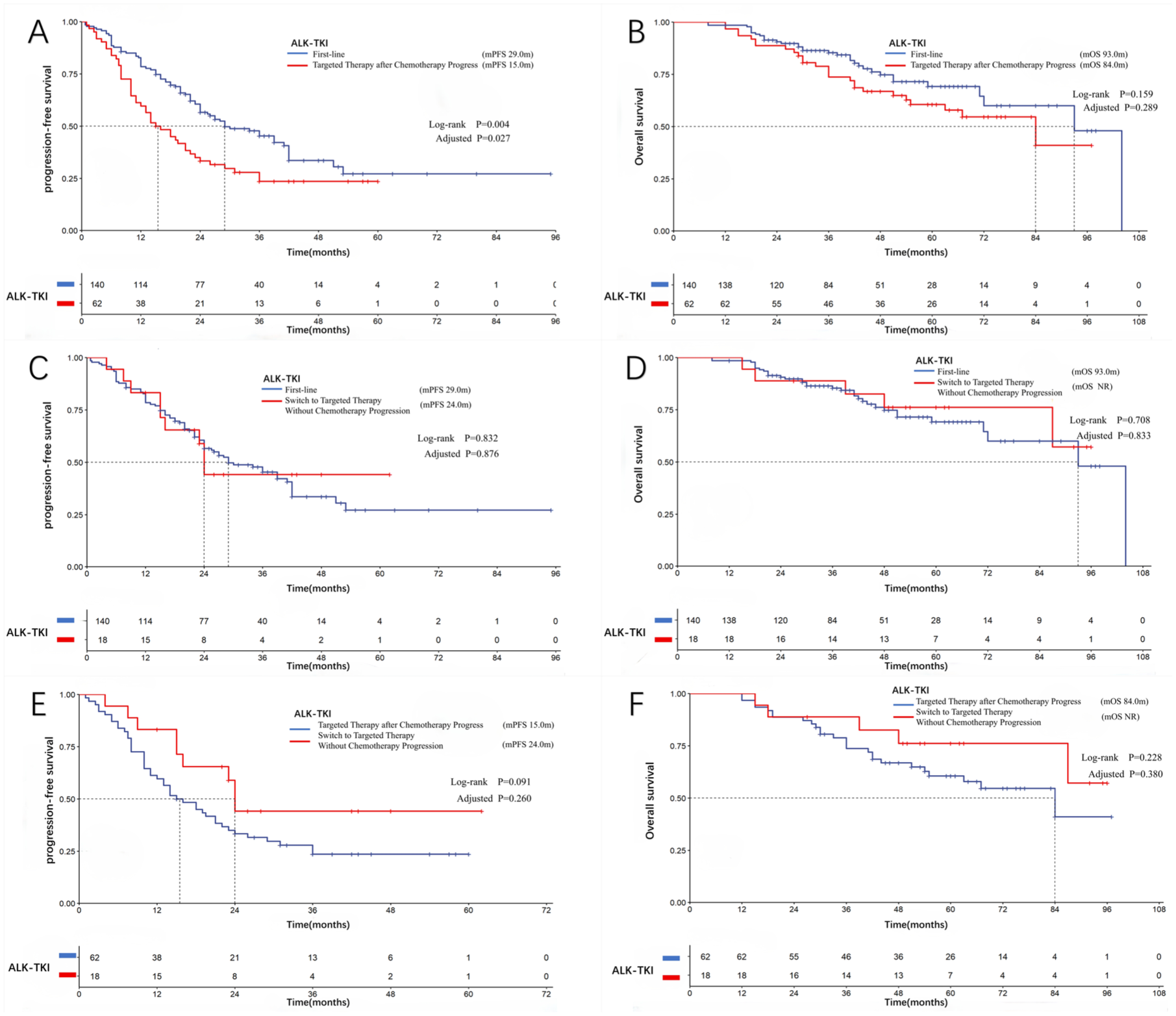
First-line versus second-line targeted therapy (after chemotherapy). (a, b) First-line targeted therapy versus first-line chemotherapy followed by targeted therapy. (c, d) Targeted therapy after chemotherapy with versus without prior progression (e, f).
Survival outcomes were also compared across different first-line ALK-TKIs. Patients receiving crizotinib had significantly shorter PFS (16 months (95% CI: 11.808–20.192) vs 41 months (95% CI: 36.585–45.154); HR: 0.379, p = 0.001, adjusted p = 0.02) and OS (71 months (95% CI: 41.570–100.430) vs NR (95% CI: NE); HR: 0.331, p = 0.002, adjusted p = 0.020) than those treated with alectinib. No significant differences were found between crizotinib and ceritinib in PFS (16 months (95% CI: 11.808–20.192) vs 30 months (95% CI: 21.052–38.948); HR: 0.472, p = 0.105, adjusted p = 0.263) or OS (71 months (95% CI: 41.570–100.430) vs 42 months (95% CI: NE); HR: 0.398, p = 0.355, adjusted p = 0.507). Similarly, no significant differences were observed between alectinib and ceritinib in PFS (41 months (95% CI: 36.585–45.154) vs 30 months (95% CI: 21.052–38.948); HR: 1.424, p = 0.449, adjusted p = 0.599) or OS (NR (95% CI: NE) vs 42 months (95% CI: NE); HR: 1.073, p = 0.947, adjusted p = 0.947).
A Cox proportional hazards model was used to evaluate prognostic factors for PFS in 220 ALK-positive patients treated with ALK-TKIs as first-line therapy or following chemotherapy. Detailed results are included in Supplemental Table 3. Univariable analysis revealed that the number of treatment lines (HR: 1.484; 95% CI: 1.052–2.094; p = 0.025) and liver metastases (HR: 1.892; 95% CI: 1.216–2.945; p = 0.005) were significantly associated with PFS. Multivariable analysis further confirmed that liver metastasis is an independent adverse prognostic factor for PFS (HR: 1.777; 95% CI: 1.121–2.817; p = 0.014). During model validation, we performed the Schoenfeld residual test to assess the proportional hazards assumption. The results showed that when the number of treatment lines was included as a covariate in the model, the proportional hazards assumption was violated for both the number of treatment lines and surgical history (p for proportional hazards assumption test <0.05). This finding suggested that their effects on survival risk may be time-dependent. Therefore, in the final model, we adjusted for the number of treatment lines as a stratification factor. After adjustment, the p-values for the Schoenfeld residual tests of all included variables were greater than 0.05, indicating that the model satisfied the proportional hazard assumption. Diagnosis of multicollinearity showed that the variance inflation factors (VIF) for all variables were less than 3, suggesting no significant multicollinearity issues. The C-index of the final model was 0.780 (95% CI: 0.721–0.840), indicating acceptable discriminatory power for PFS. Although the number of treatment lines reached statistical significance in the multivariable analysis (p = 0.032), violation of the proportional hazards assumption made it unsuitable for inclusion as a conventional covariate in the final model. Consequently, it cannot be considered an independent prognostic factor in the traditional sense. We accounted for this effect using stratified analyses. To investigate prognostic factors for OS, we constructed a Cox proportional hazards model based on clinical a priori knowledge and literature reports. Supplemental Table 4 presents the results of univariable and multivariable analyses, as well as proportional hazards assumption tests and diagnostics for multicollinearity. Univariable analysis revealed that TNM staging (HR: 3.690; 95% CI: 1.591–8.555, p = 0.002), bone metastasis (HR: 1.935; 95% CI: 1.161–3.225, p = 0.011), liver metastasis (HR: 1.983; 95% CI: 1.076–3.654, p = 0.028), and a history of surgery (HR: 0.404; 95% CI: 0.211–0.775, p = 0.006) were significantly associated with OS. Multivariable analysis further confirmed that a history of surgery was an independent protective prognostic factor for OS (HR: 0.489; 95% CI: 0.248–0.962; p = 0.038), indicating that patients who underwent surgical treatment had a significantly reduced risk of death. Regarding model validation, the Schoenfeld residual test showed that the p-values for all included variables were greater than 0.05, indicating that the model satisfied the proportional hazards assumption. Multicollinearity diagnostics revealed that the VIF for all variables was less than 3, suggesting no significant multicollinearity issues. The model’s C-index was 0.555 (95% CI: 0.521–0.589), slightly higher than the random prediction level (0.5), suggesting that the model’s predictive ability for OS is limited. This may be related to factors such as heterogeneity in subsequent treatment regimens and the long duration of follow-up. Therefore, the analysis of prognostic factors indicates that liver metastasis is an independent risk factor for disease progression, while a history of prior surgery is significantly associated with longer OS. Furthermore, while the PFS prediction model performed well, the OS prediction model demonstrated limited discriminatory power, suggesting that OS may be influenced by a combination of complex factors, including subsequent treatments.
No standardized approaches currently exist for managing rare ALK rearrangements. This study identified six cases with uncommon ALK fusions: one SETD2-ALK, one CNOT11-ALK, one HIP1-ALK, and three involving EML4-ALK, KIF5B-ALK, KLC1-ALK, or TFG-ALK fusions (Table 2). All patients showed positive responses to ALK-TKIs, highlighting the importance of accurate fusion detection by NGS to guide treatment and prognosis.
Rare ALK fusion types and treatment efficacy.
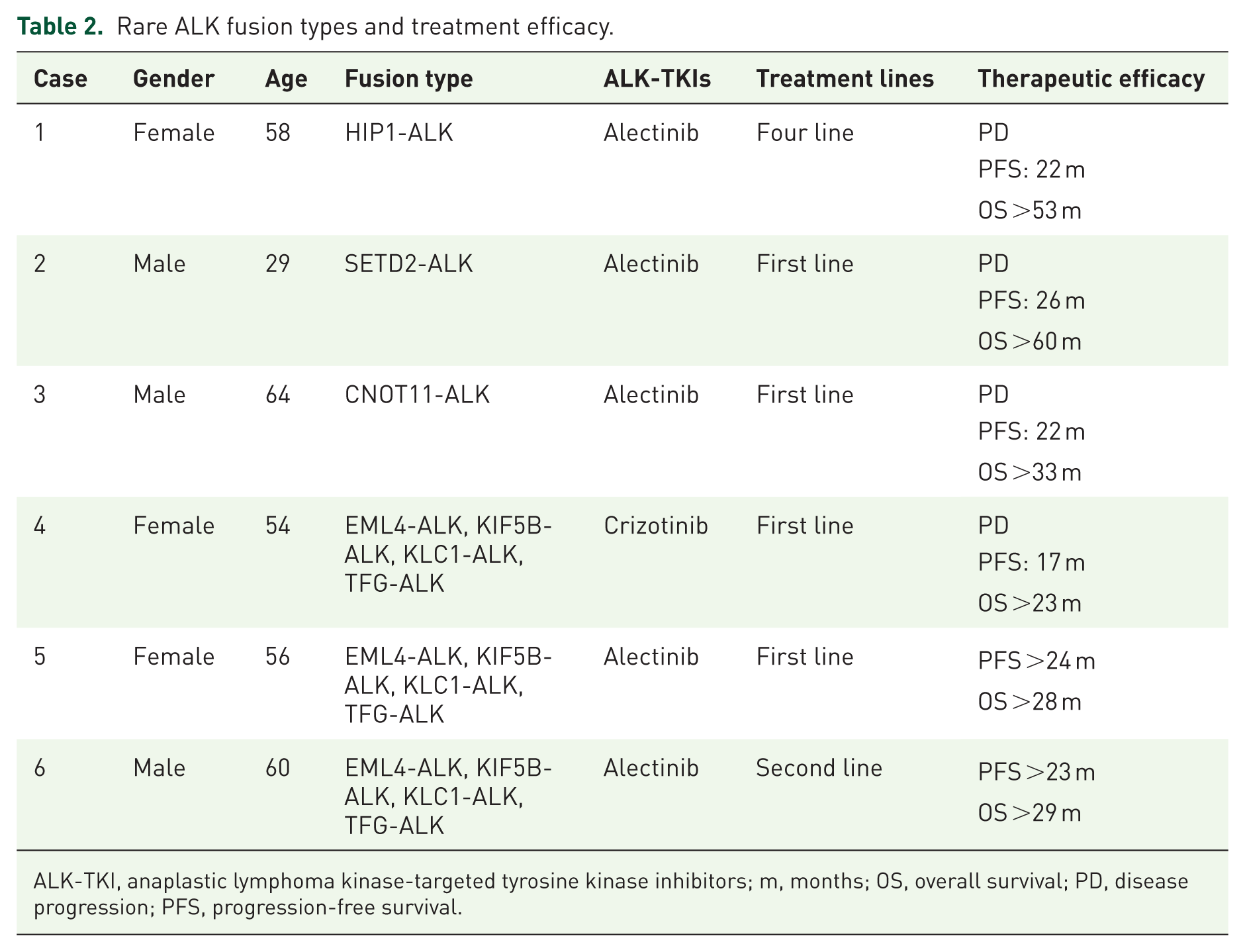
ALK-TKI, anaplastic lymphoma kinase-targeted tyrosine kinase inhibitors; m, months; OS, overall survival; PD, disease progression; PFS, progression-free survival.
Although ALK-positive NSCLC patients typically respond well to ALK-TKIs, resistance eventually develops. We retrospectively analyzed NGS results from resistant ALK-positive patients at our institution (Figure 3). Among these patients, six developed the G1202R missense mutation, five exhibited MET gene amplification, and two had TP53 nonsense mutations. Additional mutations were detected in other individual cases.
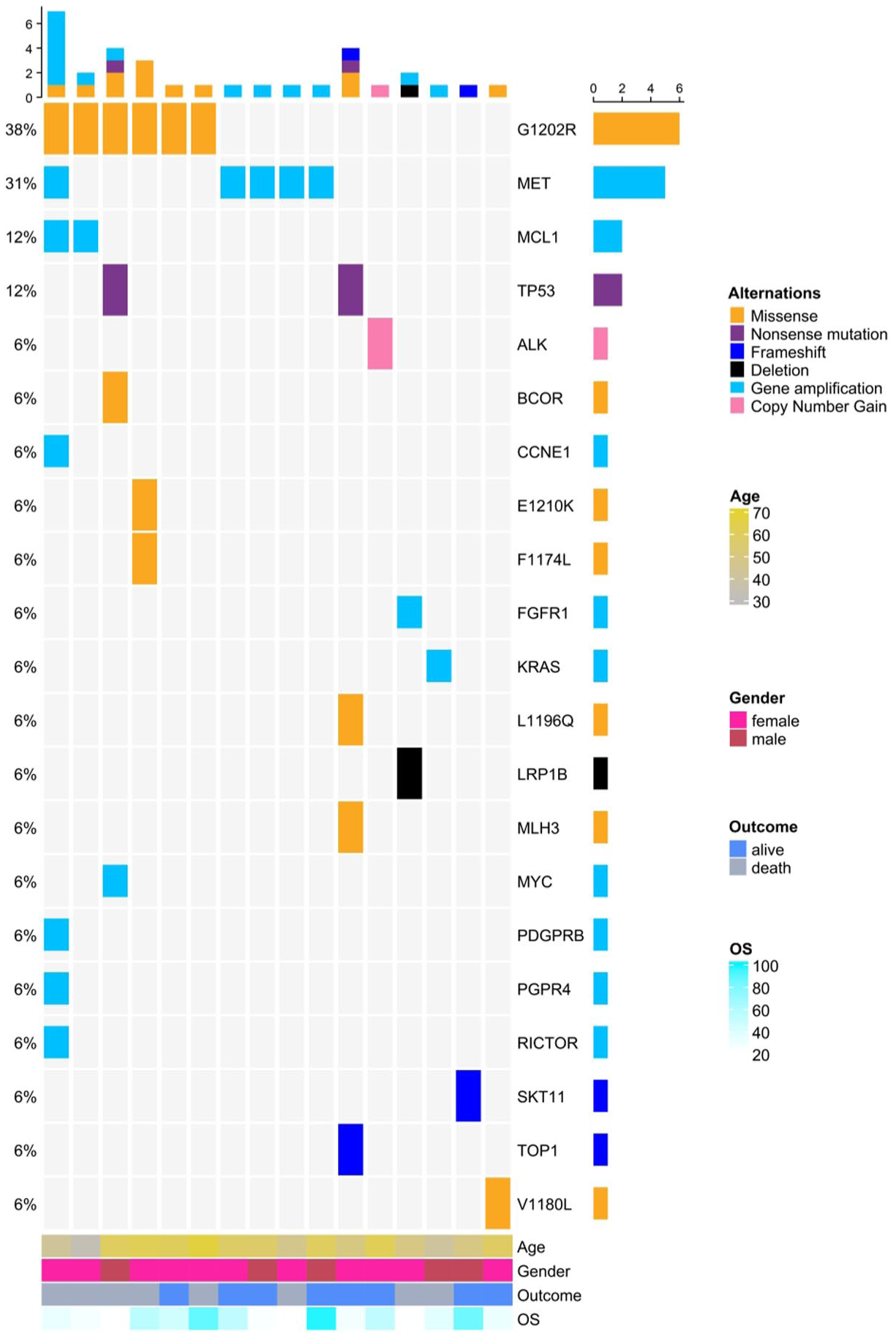
NGS testing at drug resistance in ALK-positive NSCLC.
Impact of MET expression on targeted therapy efficacy in ALK-positive NSCLC
Among the 259 ALK-positive NSCLC patients, 103 had preserved tissue specimens at Zhejiang Cancer Hospital. After the IHC evaluation, 18 samples were excluded due to insufficient tumor content. Among the remaining specimens, 11 showed MET overexpression, and 74 were MET-negative, resulting in a MET overexpression rate of 13.1%. Patient demographics and treatment details are summarized in Table 3. In the MET-overexpressing subgroup, three patients received first-line crizotinib, six received first-line alectinib, and two received alectinib as second-line therapy after progression on initial chemotherapy. The median PFS for first-line crizotinib was 17 months (95% CI: 13.799–20.201), with median OS not reached (95% CI: NE). In the first-line alectinib group, the median PFS was 12 months (95% CI: 0.000–27.603) and the median OS was 41 months (95% CI: 24.069–57.931). No significant differences in PFS (HR: 0.608; p = 0.544) or OS (HR: 1.904; p = 0.574) were found between these two treatment groups. However, due to the extremely small sample size, these comparisons lack statistical power. Therefore, the absence of a statistically significant difference should not be interpreted as evidence of equivalence in efficacy between the two treatments.
Characteristics and survival outcomes of ALK-positive patients with MET overexpression treated with ALK-TKIs.

ALK-TKI, anaplastic lymphoma kinase-targeted tyrosine kinase inhibitors; IHC, immunohistochemistry; m, months; OS, overall survival; PFS, progression-free survival.
In addition, 81 ALK-positive, MET-negative patients received first-line alectinib, along with 6 MET-overexpressing patients also treated with first-line alectinib. No significant differences were observed between the two groups in gender, age, smoking history, disease stage, metastasis sites (bone, brain, liver, and lung), or surgical history (Supplemental Table 5). However, clinical outcomes differed significantly: Compared with the MET-negative group, the MET-overexpressing group had a significantly shorter median PFS (12 months (95% CI: 0.000–27.603) vs 42 months (95% CI: 38.618–45.382); HR = 0.315, p = 0.011), and median OS was also significantly shorter (41 months (95% CI: 24.069–57.931) vs not reached (95% CI: NE); HR = 0.145, p = 0.001; Figure 4). Although the differences were statistically significant, the small number of patients with MET overexpression and the retrospective design of the study preclude definitive conclusions. These findings suggest that MET may have prognostic value, but this needs to be validated in larger prospective cohorts.

Kaplan–Meier estimates of PFS (a) and OS (b) for first-line alectinib in ALK-positive NSCLC patients, stratified by MET overexpression status.
Exploratory analysis of changes in PD-L1 expression
Among ALK-positive NSCLC patients with available tissue samples, 17 had paired specimens collected before ALK-TKI treatment and after the development of resistance. PD-L1 expression was assessed using the H-score method. After resistance, 5 patients (29.4%) showed increased PD-L1 expression, 10 (58.8%) exhibited no significant change, and 2 (11.8%) had reduced expression. Comparative analysis demonstrated no statistically significant difference in PD-L1 levels before and after resistance (p = 0.248). The dynamic changes in PD-L1 expression are shown in Figure 5. Due to the limited sample size (n = 17) and inconsistent direction of change among individuals, this study did not observe statistically demonstrable alterations in PD-L1 expression following ALK-TKI resistance.

PD-L1 expression in ALK-positive NSCLC pre- and post-ALK-TKI resistance.
Illustrative cases: Immunotherapy after ALK-TKI resistance
Despite the efficacy of ALK-TKIs, acquired resistance remains a clinical challenge. Among 259 ALK-positive NSCLC patients, 2 individuals received ICIs following ALK-TKI resistance.
The first case was a 49-year-old male (Supplemental Figure 6) with a 2-month history of cough and hoarseness. Imaging showed a soft-tissue mass behind the inferior vena cava invading the right lower lobe. Biopsy confirmed adenocarcinoma, and NGS detected an EML4-ALK fusion. He began crizotinib but switched to alectinib due to liver injury. After 19 months, pulmonary metastases developed, and he started tislelizumab (200 mg every 3 weeks), achieving a partial response (PR) sustained for more than 2 years.
The second case was a 28-year-old male non-smoker (Supplemental Figure 7) with a persistent cough. CT imaging showed bronchial stenosis, extensive lymphadenopathy, bilateral lung nodules, pleural thickening, pleural and pericardial effusion, and multiple bone lesions. Pleural biopsy confirmed lung adenocarcinoma, and NGS identified two ALK fusions: EML4-ALK (E14:A21, allele frequency 14.05%) and SETD2-ALK (S12:A21, allele frequency 25.20%). Diagnosed with stage IVB lung adenocarcinoma with widespread metastases, he started alectinib (600 mg twice daily), achieving stable disease (SD). After 26 months, chest tightness and dyspnea indicated resistance. A liquid biopsy revealed no mutations. In January 2021, he received six cycles of pemetrexed with carboplatin and toripalimab. Due to side effects and patient preference, treatment transitioned to toripalimab maintenance. At 16 months of follow-up, mild progression was noted. Six additional cycles of pemetrexed and toripalimab were administered, followed by continued toripalimab maintenance, achieving SD for 34 months.
Previous studies have demonstrated a lower overall response rate to immunotherapy in ALK-positive patients. However, these findings are mainly derived from treatment-naïve or first-line combination therapy settings, and the efficacy of immunotherapy following acquired resistance remains uncertain. In light of this, we present the treatment courses of these two patients as exploratory observations, aiming to describe the clinical phenomena that may arise in this specific post-resistance setting and to provide a foundation for generating hypotheses for future research. As case observations, the results are subject to inherent limitations, such as extremely small sample size and publication bias, and should not be extrapolated to the overall efficacy in the ALK-positive population.
Discussion
These findings provided real-world insights into the current debate over the optimal sequential treatment regimen for ALK-TKIs. Univariable analysis suggested that first-line alectinib was associated with longer median PFS than its use after chemotherapy (41 vs 24 months). However, this difference was not statistically significant after adjusting for baseline imbalances (e.g., brain metastases) and multiple comparisons. These adjusted analyses suggested that the poorer efficacy of alectinib following chemotherapy may be attributable to the higher prevalence of adverse prognostic factors in this population, such as a higher baseline rate of brain metastases.
Although this difference was not statistically significant, the higher PFS observed in the first-line setting remains clinically meaningful. Current guidelines consistently recommend potent second-generation ALK-TKIs as the standard first-line treatment. These agents provide robust systemic efficacy and excellent intracranial control from the outset, thereby reducing the risk of early central nervous system progression. 37 Therefore, whether prior chemotherapy has a substantial impact on the efficacy of subsequent TKI therapy or not, early initiation of alectinib remains the more prudent and optimal choice. The treatment landscape for ALK-positive NSCLC is rapidly evolving, although the present work focused on the sequential use of the second-generation TKI alectinib in combination with chemotherapy. With the third-generation TKI lorlatinib having demonstrated superior efficacy to second-generation drugs in first-line treatment, 38 clinical practice now faces a new dilemma: should first-line therapy consist of a second- or third-generation TKI? How will this decision influence the subsequent profile of resistance mechanisms and sensitivity to other drugs? These questions represent the principal focus of current research on “sequential strategies.” The primary objective is to design a long-term treatment pathway that maximizes OS in the context of an expanding range of available drugs. Despite the inherent limitations of retrospective studies, these real-world data provide insights into the current second-generation TKI-based sequential treatment model. They also support the exploration of more complex regimens involving third-generation TKIs.
The application of NGS technology has greatly expanded our understanding of the ALK fusion spectrum. In addition to the predominant EML4-ALK variant, which accounts for approximately 95% of ALK-positive NSCLC cases, 39 more than 92 rare ALK fusion partners have been reported to date. 40 Although most rare fusion types exhibit some sensitivity to ALK-TKIs, evidence-based data regarding their clinical efficacy remains limited. Taking HIP1-ALK as an example, Hong et al. 41 first reported this fusion type in NSCLC in 2014. A subsequent study involving 11 Chinese patients demonstrated that the ORR with crizotinib treatment reached 90%, with a median PFS of 17.9 months. 42 In our cohort, one HIP1-ALK patient achieved a 22-month PFS with fourth-line alectinib. This finding supported the sensitivity of this fusion type to targeted therapy. However, the diversity of fusion partners also leads to high heterogeneity in treatment responses. Different fusion partners and breakpoints may affect drug binding affinity or downstream signaling pathways. This can lead to different clinical outcomes. 43 For example, Du et al. 44 reported a case of a patient with a CMTRI-ALK fusion who was primary resistant to crizotinib. This finding suggests that not all rare ALK fusions benefit from targeted therapy, and treatment efficacy may be fusion-partner-specific. Currently, there are no standardized treatment strategies for rare ALK rearrangements 45 ; therefore, precise identification of fusion subtypes via NGS is of great value for predicting drug sensitivity and guiding personalized treatment selection. Only six patients with rare ALK fusions were included, representing an extremely limited sample size. Furthermore, as the cases were derived from retrospective data at a single center, selection bias may be present. Therefore, the above observations are primarily based on case reports and are intended to provide preliminary insights for future research; their conclusions cannot yet be generalized to all patients with rare fusions.
According to the 2023 Chinese Expert Consensus, 33 MET overexpression is defined as moderate to strong staining in ⩾50% of tumor cells, with a detection rate of 13.1% in this cohort. Existing studies suggest that patients with MET overexpression may benefit from treatment with MET inhibitors, with some studies reporting ORR as high as 50%.46,47
Crizotinib, as a multi-targeted inhibitor, simultaneously inhibits ALK and MET, demonstrating unique advantages in ALK-positive patients with MET overexpression. Chen et al. 21 found that among ALK-positive patients treated with crizotinib, the median PFS was longer in the MET-overexpressing group than in the MET-negative group (15.2 vs 11.0 months), although the difference was not statistically significant (p = 0.263). Meanwhile, the median OS had not yet been reached in the MET-overexpressing group, whereas it was 33.5 months in the MET-negative group. Feng et al. 19 further reported that among six patients with ALK-rearranged NSCLC and MET overexpression, two achieved complete remission (CR) and four achieved PR following crizotinib treatment. In this cohort, three ALK-positive patients with MET overexpression received first-line crizotinib treatment, with a median PFS of 17 months and OS not yet reached.
Unlike crizotinib, the second-generation ALK-TKI alectinib lacks anti-MET activity, and its efficacy in patients with MET overexpression remains unclear. Six patients with MET overexpression received first-line alectinib. Their median PFS was only 12 months. This was significantly shorter than that of MET-negative patients (42 months) and lower than real-world data (45.5 months 48 ), suggesting MET overexpression might negatively affect alectinib efficacy. MET amplification is widely recognized as one of the mechanisms underlying resistance to EGFR and ALK inhibitors, 49 and MET overexpression may similarly contribute to treatment failure. Basic research indicates that in ALK-positive NSCLC cells, MET activation can serve as a bypass signaling pathway following alectinib treatment, whereas inhibition of MET signaling can enhance the efficacy of alectinib. 50 Clinical cohort studies have further confirmed that MET alterations are a common mechanism of early resistance to first-line alectinib therapy. 51 Some patients with MET overexpression exhibited significantly shorter PFS following alectinib treatment, and one patient tested negative for MET after developing resistance. MET overexpression may be associated with acquired resistance and could play a role in the mechanism underlying alectinib resistance.
However, there is currently a lack of high-quality evidence regarding the clinical value of MET protein overexpression in ALK-positive patients, and relevant studies are extremely limited. Current research in this field is primarily constrained by two major challenges. First, criteria for interpreting MET overexpression have only recently become standardized, resulting in substantial heterogeneity among earlier studies. Second, cases simultaneously meeting the criteria of ALK-positive status, well-preserved tissue specimens, and complete TKI treatment follow-up data are rare, making the collection of clinical data and biological samples extremely difficult. Against this backdrop, our real-world cohort with standardized assessment represents the first analysis of how MET overexpression affects alectinib efficacy in Chinese patients. It provides preliminary real-world evidence on this clinical issue. Although the sample size was limited, MET overexpression was significantly associated with shorter PFS and OS during first-line alectinib treatment. This result suggested that MET overexpression remains a potential biomarker of poor prognosis, even with current standard therapy. Given that alectinib itself lacks anti-MET activity, these patients may struggle to derive maximum survival benefit from second-generation TKI monotherapy. They represent a clinical subgroup that requires urgent identification and intervention.
From a mechanistic perspective, MET overexpression promotes tumor proliferation, migration, invasion, and angiogenesis by activating the MET pathway, which may underlie the poor prognosis observed in patients. Therefore, interventions targeting the MET pathway hold clear therapeutic value. Currently, several selective MET inhibitors (including savolitinib, tepotinib, capmatinib, and vebreltinib) are in clinical development, and their efficacy in MET-positive NSCLC is gradually being elucidated. Evidence indicated that combined EGFR and MET inhibition provided substantial clinical benefit in patients with EGFR-mutant NSCLC. In the SACHI study, patients harboring EGFR mutations with MET amplification achieved significantly longer PFS with the combination of the MET inhibitor savolitinib and osimertinib compared with chemotherapy (mPFS 9.8 vs 5.4 months; HR 0.34) 52 EGFR and ALK are distinct driver genes, and their combined treatment strategies cannot be directly extrapolated. Nevertheless, the success of the SACHI study indicates that dual-inhibition strategies may offer clinical benefit in cases of targeted therapy resistance driven by MET alterations. Multiple case reports have also confirmed that in patients with MET-amplification-mediated resistance to alectinib, the dual inhibition strategy combining alectinib and crizotinib can yield significant clinical benefits. 53 However, its efficacy and applicability in patients with ALK-positive tumors exhibiting MET overexpression remain to be confirmed in prospective clinical studies.
Although limited by its single-center, retrospective design and small sample size, this analysis cannot establish causality, yet its mechanistic hypothesis remains clinically meaningful. In the precision medicine era of ALK-positive NSCLC, MET overexpression warrants clinical attention as a potential biomarker of poor prognosis. In the future, our team plans to continue collecting such rare cases through multicenter collaboration to expand the sample size. A combination of these efforts with more precise detection methods (such as NGS and FISH) will help elucidate the genetic status underlying MET overexpression. This approach will lay the groundwork for the precise identification of patients with a potentially poor prognosis.
Regarding changes in PD-L1 expression in patients with ALK-positive NSCLC following TKI resistance, existing research findings are inconsistent. Gainor et al. 54 reported that, among patients with ALK-positive NSCLC, the PD-L1 positivity rate was 25% in samples collected after crizotinib resistance. This rate was lower than the 47% observed in treatment-naïve patients, suggesting a potential decline in PD-L1 expression following the development of resistance. Koh et al. 55 found that, among seven patients with paired biopsy samples, PD-L1 expression remained unchanged or increased in six patients following the development of crizotinib resistance compared to pre-treatment levels. However, Kim et al. 56 observed upregulation of PD-L1 expression in resistant cell lines, with the H-score in clinical samples rising from 6.5 to 35.0 (p = 0.163). Our observations suggested that PD-L1 expression increased in 5 cases, remained stable in 10 cases, and decreased in 2 cases following resistance (p = 0.248). Although statistical significance was not reached, an upward trend was observed. The aforementioned heterogeneity suggests that the effect of TKI resistance on PD-L1 expression may be regulated by multiple factors, and a unified conclusion cannot yet be drawn. Future large-scale prospective studies are needed to determine whether PD-L1 expression changes following ALK-TKI resistance and to identify patients who may benefit from subsequent immunotherapy.
Currently, multiple clinical studies have demonstrated the limited efficacy of ICIs in ALK-positive NSCLC. The ORR of ICI monotherapy in ALK-positive patients is only 0%–3.6%, 57 with a median PFS of 2–3 months. 58 In addition, subgroup analyses from the IMPower150 59 and IMPower130 60 trials indicated that ALK-positive patients did not experience meaningful benefit from chemotherapy combined with PD-(L)1 inhibitors. However, the aforementioned evidence primarily stems from clinical trials of first-line combination therapy. Whether patients who have developed resistance to ALK-TKIs can benefit from ICI therapy remains a question requiring further investigation. In recent years, real-world studies have begun to explore this clinical issue. A real-world study conducted by Wang et al. 61 was the first to systematically evaluate the efficacy of immunotherapy following resistance to ALK-TKIs. The results showed that the median PFS was significantly longer in patients who received immunotherapy than in those who did not (5.3 vs 2.5 months, p = 0.009). Of particular note, among patients who tested PD-L1-positive upon re-biopsy after resistance, the median PFS in the immunotherapy group reached 7.8 months, significantly outperforming the 2.7 months observed in the non-immunotherapy group (p = 0.002). This finding suggests that screening for PD-L1-positive patients via re-biopsy after treatment resistance may help identify potential beneficiaries of immunotherapy.
In addition to PD-L1 expression status, other molecular factors may also influence the efficacy of immunotherapy following resistance to ALK-TKIs. One patient exhibited dual EML4-ALK and SETD2-ALK fusions at baseline. Following progression on alectinib, liquid biopsy confirmed the loss of both ALK fusions, and sequential chemotherapy combined with immunotherapy resulted in disease stabilization lasting up to 34 months. This case suggests that the loss of driver genes may represent a new mechanism of sensitivity to immunotherapy following TKI resistance. Similar cases demonstrating long-term benefit have also been reported. Fu et al. 62 reported a case of an ALK-positive patient harboring a TP53 mutation, with a PD-L1 TPS of 85%. The patient developed rapid resistance to crizotinib and alectinib but subsequently achieved a PR with pemetrexed combined with platinum-based chemotherapy and toripalimab. Notably, the response duration exceeded 45 months. Yang et al. 32 reported a patient who developed acquired ALK fusion loss and high PD-L1 expression following TKI progression; after receiving pembrolizumab, the patient achieved PFS of over 29 months and CR.
Although these rare cases represent only a small fraction of the ALK-positive population, they reveal a potential mechanism by which immunotherapy may confer benefit. Clonal evolution of the tumor following resistance, such as loss of the ALK fusion or acquisition of TP53 mutations, can remodel the immune microenvironment. This process may convert a tumor initially characterized by a “cold” microenvironment into a “hot” tumor that is responsive to ICIs. Although these observations are derived from a very small number of cases and are insufficient to support general conclusions, they offer valuable insights. Specifically, they may guide future efforts to identify patient subgroups that could benefit from immunotherapy following resistance. Identifying patient subgroups with specific molecular characteristics through post-resistance re-biopsy may offer a potential breakthrough to overcome the current limitations in the efficacy of immunotherapy for ALK-positive patients.
Several limitations inherent to the retrospective design should be considered; these biases must be fully considered when interpreting the study results.
First, selection bias was one of the major limitations of retrospective studies. Treatment decisions were made by treating physicians according to clinical characteristics, performance status, comorbidities, and treatment guidelines rather than through random assignment. As a result, baseline characteristics may have differed systematically between groups. For example, the proportion of patients with baseline brain metastases was significantly higher in the post-chemotherapy alectinib group than in the first-line treatment group (p = 0.047), and brain metastases are a known poor prognostic factor for NSCLC. 63 Therefore, the shorter PFS in the post-chemotherapy group (24 vs 41 months) may be partly attributable to a higher burden of brain metastases, rather than solely reflecting the effects of prior chemotherapy. Furthermore, selection bias was present in the composition of the study population. The stage III patients included in this study constituted a specific subgroup who were unsuitable for or refused curative chemoradiotherapy due to factors such as high tumor burden, involvement of critical sites, comorbidities, or personal preference. Their inherent prognosis differs from that of the typical stage III population, which may limit the generalizability of the results.
Second, although the multivariable regression model adjusted for known prognostic factors, the retrospective design still carries the risk of unmeasured confounding. Due to limitations in historical medical records, some potential confounding factors could not be included in the analysis, including performance status (ECOG/KPS), dose adjustments, treatment interruptions, and adherence during TKI therapy. In particular, the absence of performance status data warrants special attention, as ECOG/KPS is a recognized independent prognostic factor for NSCLC 64 ; its omission may introduce residual confounding and affect the interpretation of survival outcomes. In real-world clinical practice, dose reductions or treatment interruptions due to adverse events occur frequently; these treatment adjustments may affect actual drug exposure and treatment duration, thereby becoming potential confounding factors for PFS and OS. Regarding survival bias, patients who switched from chemotherapy to TKI during the progression-free period (n = 18) had to survive the chemotherapy phase to receive TKI treatment, creating a “survival window.” Although the follow-up start date was set at TKI initiation to reduce this bias, residual bias remains possible.
Third, the long study duration introduced temporal bias. During this period, the availability of ALK-TKIs and treatment guidelines evolved continuously, and there was significant heterogeneity in the chemotherapy regimens patients had previously received. Due to limitations of retrospective data, these factors could not be systematically collected or adjusted, potentially introducing confounding effects on the assessment of subsequent TKI efficacy. This limitation should be considered when interpreting “the impact of prior chemotherapy on the efficacy of subsequent TKI therapy.”
Fourth, the small sample size introduced notable sampling bias and limited statistical power in the analysis. Although the overall cohort included 259 ALK-positive NSCLC patients—a relatively large sample size—the sample size for specific subgroups was limited, which significantly reduced statistical power and limited the ability to draw definitive conclusions. First, sample size limitations were particularly evident in the biomarker analysis. Only 103 patients had tissue samples available for MET IHC testing, which may have led to sampling bias, as patients from whom tissue samples could be obtained may represent a selective subgroup with better physical condition and greater tolerance for biopsy, thereby limiting the generalizability of the study results. In the MET-overexpression subgroup (n = 11), the comparison between crizotinib (n = 3) and alectinib (n = 6) carries a high risk of Type II error, with wide CIs for survival outcomes (95% CI: 0.000–27.603 months) and significant interpatient heterogeneity (PFS ranging from 6 to 39 months, as shown in Table 3), suggesting poor stability of the estimates. Preliminary observations suggest that MET overexpression may be associated with poor response to alectinib; however, due to the limited sample size, these findings require confirmation in larger-scale studies. Furthermore, the analysis of changes in PD-L1 expression before and after resistance was based on only 17 paired samples. The results showed that although PD-L1 expression exhibited an upward trend in some patients following ALK-TKI resistance, the overall difference was not statistically significant (p = 0.248). Due to the limited sample size and consequent lack of statistical power, no reliable conclusions can be drawn regarding whether PD-L1 expression changes after resistance develops. Similarly, with only two cases receiving immunotherapy, inferences regarding the efficacy of immunotherapy must be made with extreme caution and can only serve as preliminary evidence for describing phenomena and generating hypotheses. A systematic evaluation is required through prospective studies involving larger sample sizes and combined with dynamic biomarker monitoring. In the ALK-TKI efficacy subgroup analysis, the sample size for the ceritinib group was small (n = 38), particularly in the subgroup analysis of first-line treatment (n = 10) and post-chemotherapy treatment (n = 12). This limited sample size substantially reduced statistical power. As a result, the numerically notable difference in PFS (30 vs 8 months, p = 0.051) did not reach statistical significance. Similarly, the small sample size in the post-chemotherapy subgroup (n = 12) also limited a reliable assessment of the impact of prior chemotherapy. For patients with rare ALK fusions (n = 6), the sample size was extremely small, making it impossible to conduct comparative analyses of efficacy across different fusion types or to assess prognostic differences compared to the common EML4-ALK fusion. Although all six patients responded to ALK-TKIs, these results are limited to case reports and are not generalizable to the broader population with rare ALK fusions.
Several important limitations should be considered in the MET detection method used. The assessment of MET status relied solely on IHC, which measures protein expression levels but cannot distinguish the specific molecular mechanisms underlying MET overexpression—which may include gene amplification, exon 14 skipping mutations, transcriptional upregulation, or epigenetic alterations. 65 Sensitivity to MET inhibitors may vary significantly depending on the underlying mechanism. Furthermore, IHC interpretation criteria are subject to subjectivity and heterogeneity: although the current analysis adhered to the 2023 Chinese expert consensus, 33 defining MET overexpression as moderate or strong positive staining in ⩾50% of tumor cells, differences among pathologists, antibodies, and staining platforms may lead to varying results. Moreover, the absence of a unified international positive threshold currently limits comparability across studies. Therefore, conclusions regarding MET overexpression derived from IHC should be interpreted with caution when translating them into clinical decision-making. Findings from this study suggested that MET overexpression may be linked to poor prognosis in ALK-positive patients; however, it cannot be used to determine whether patients should receive combination therapy with MET inhibitors. Future studies should adopt multimodal MET detection strategies to more accurately identify patient subgroups that may benefit from combination therapy with ALK-TKIs and MET inhibitors.
Finally, detailed information regarding patients’ radiotherapy was unavailable. This included whether radiotherapy was administered, the treatment objective (curative or palliative), the size of the radiation field, the sequence relative to systemic therapy, and the radiation dose. In patients with ALK-positive NSCLC, because ALK-TKIs can lead to long-term survival, patients are more likely to undergo radiotherapy during the course of their disease; radiotherapy may interact with TKI therapy in complex ways, and therefore, this missing data may constitute a significant unmeasured confounding factor. Furthermore, the role of radiotherapy differs according to disease stage. For patients with unresectable stage III disease, radiotherapy is a cornerstone of treatment; common approaches include consolidation immunotherapy following concurrent chemoradiotherapy (cCRT) or synchronous chemoradiotherapy (sCRT). Recent real-world studies have shown 66 that the frequency of use of cCRT and sCRT in clinical practice is currently roughly equivalent (each accounting for approximately 37.7%). The choice of cCRT was primarily based on tumor location, while sCRT was more commonly used in patients with larger tumor volumes, rather than solely based on TNM staging. This implies that even among patients with stage III disease, there are significant differences in their overall treatment regimens. In specific molecular subgroups (such as EGFR-mutant NSCLC), curative radiotherapy may precede or be integrated with targeted therapy (such as osimertinib 67 ). Similar treatment heterogeneity may also exist in our ALK-positive cohort. Radiotherapy may be combined with ALK-TKIs in different sequences and for different purposes. This may further increase unmeasured confounding.
For stage IV patients, the use of radiation therapy is no longer limited to palliative care. In patients with oligometastatic or oligoprogressive disease, radiation therapy is often used as a means to achieve a cure or alter the course of the disease. As noted in current prospective trials (such as RISE 68 ), Kuncman et al. administered high-dose consolidation radiotherapy to patients with up to 10 metastatic lesions. This strategy challenges the traditional definition of metastatic disease and highlights the biological significance of local treatment, particularly during immunotherapy or in the late stages following chemotherapy. These findings indicate that the scope of radiation therapy for stage IV patients extends far beyond conventional understanding and that there is significant variation among patients in terms of whether they receive radiation therapy, the treatment objectives, and the extent of the radiation field. Furthermore, emerging evidence suggests that certain characteristics of radiation therapy—particularly the treatment volume and low-dose exposure of immune-related organs (such as the lungs and heart)—may trigger radiation-induced lymphocytopenia (RIL). Early lymphocyte levels and low-dose radiation exposure to the chest have been shown to predict clinically significant lymphocytopenia during radiation therapy for lung cancer. This condition may, in turn, affect the efficacy of subsequent or concurrent systemic therapy. 69 This means that even if two groups of patients receive the same systemic treatment regimen, differences in their radiation therapy plans may lead to different treatment outcomes through the RIL mechanism. Because radiation therapy dose and volume data were unavailable in the dataset, the potential impact of RIL on ALK-TKI efficacy could not be assessed, representing another important unmeasured confounding factor.
Conclusion
Preliminary results from this study indicated that ALK-TKIs were associated with favorable survival outcomes, regardless of whether they are used as first-line or subsequent-line therapy. The trend toward benefit was more pronounced with first-line treatment. Among ALK-positive patients with MET overexpression, the PFS and OS in the first-line alectinib group were numerically inferior to those in the crizotinib group; however, given the limited sample size, these findings require further validation. Furthermore, although a trend toward increased PD-L1 expression was observed following ALK-TKI resistance, the overall change was not significant. Therefore, the role of immunotherapy in ALK-TKI-resistant disease remains to be further elucidated.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-1-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-2-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-3-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-4-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-4-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-5-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-5-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-6-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-6-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-7-tam-10.1177_17588359261458657 – Supplemental material for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status
Supplemental material, sj-docx-7-tam-10.1177_17588359261458657 for The efficacy of targeted therapy in ALK-positive non-small-cell lung cancer patients and analysis of MET/PD-L1 expression status by Xinyuan Wang, Yi Chen, Dong Chen and Hongyang Lu in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank Zhejiang Cancer Hospital for supporting this study. We also thank all the patients and their families, as well as all investigators involved in this work.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.