
Abstract
Background:
While trifluridine/tipiracil (FTD/TPI) is approved for refractory metastatic colorectal cancer (mCRC), its clinical benefit may vary based on molecular and clinical characteristics.
Objectives:
To identify clinical and molecular factors associated with overall survival (OS) in patients with refractory mCRC treated with FTD/TPI.
Design:
Retrospective, multicenter study.
Methods:
A retrospective multicenter cohort study of 591 mCRC patients treated with FTD/TPI was conducted. Cox regression was used to identify independent prognostic factors for overall survival (OS).
Results:
Median OS was 7.8 months in the overall cohort. Patients with deficient mismatch repair (dMMR) had significantly longer OS than those with proficient MMR (p = 0.001). Body mass index (BMI) (hazard ratio (HR) = 0.96), neutrophil-to-lymphocyte ratio ⩾3 (HR = 1.94), and dMMR status (HR=0.29) were independent predictors of OS (all p < 0.001).
Conclusion:
In this retrospective multicenter cohort, MMR status, BMI, and neutrophil-to-lymphocyte ratio (NLR) were identified as factors independently associated with OS among patients with refractory mCRC treated with FTD/TPI. These findings support the integration of molecular and clinical factors for prognostic stratification in later-line treatment settings
Plain language summary
Colorectal cancer that has spread to other organs and does not respond to standard treatments is difficult to treat. Trifluridine/tipiracil is a medicine commonly given to such patients late in their treatment journey, but not all patients benefit equally. In this study, we looked at 591 patients with advanced colorectal cancer who received trifluridine/tipiracil in routine clinical practice to understand which factors were linked to how long patients lived after treatment. We found that patients whose tumors had a specific molecular defect called deficient mismatch repair (dMMR) tended to live longer after receiving this treatment than patients without this feature. We also found that body mass index (BMI) and a simple blood marker of inflammation, the neutrophil-to-lymphocyte ratio (NLR), were associated with survival: patients with higher inflammation levels tended to have shorter survival. These measurements can be taken easily during routine care. These findings suggest that looking at tumor biology and simple clinical factors could help doctors better estimate prognosis and personalize treatment decisions for patients receiving trifluridine/tipiracil. In particular, testing tumors for dMMR and evaluating inflammation markers may help identify patients who are more likely to benefit from this therapy. Future research should confirm these findings and explore how this information can be used to guide treatment choices.
Keywords
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide, accounting for 10% of the 19.3 million newly diagnosed cancer cases in 2020, according to GLOBOCAN estimates. 1 It also ranks as the second leading cause of cancer-related deaths globally, with most deaths resulting from metastatic colorectal cancer (mCRC).1,2 Despite advances in screening and systemic therapies, a substantial proportion of patients develop metastatic disease, which remains associated with poor prognosis, particularly in later-line treatment settings. The first- and second-line treatments for most unresectable mCRC cases typically involve fluoropyrimidine-based doublet or triplet regimens, such as FOLFOX (folinic acid, fluorouracil, and oxaliplatin) and FOLFIRI (folinic acid, fluorouracil, and irinotecan), with or without antivascular endothelial/epidermal growth factor pathway blockers, depending on predictive and driver gene mutation status.2–5 For mCRC patients with microsatellite instability-high (MSI-H) tumors, also known as mismatch repair deficiency (dMMR), first-line treatment includes immune checkpoint inhibitors.2–5
For mCRC patients who have progressed beyond prior treatments, prognosis often becomes less favorable, with therapeutic goals focused on extending survival and maintaining quality of life. 6 Trifluridine/tipiracil (TAS-102, FTD/TPI), regorafenib, and fruquintinib have been tested in the third- and fourth-line settings and have since received approval for the treatment of heavily refractory mCRC.7–9 FTD/TPI is an oral combination of FTD, a cytotoxic thymidine analog, and tipiracil, which inhibits thymidine phosphorylase to enhance the bioavailability of FTD. 10 The pivotal Phase III RECOURSE trial demonstrated significant benefits of FTD/TPI in progression-free survival (hazard ratio (HR) 0.48) and overall survival (OS) (HR 0.68) compared to placebo in refractory mCRC. 8 A subsequent Phase III SUNLIGHT trial examining the efficacy of FTD/TPI plus bevacizumab versus FTD/TPI alone in the nonfirst-line setting showed a significant OS benefit, with the combination group achieving an approximately 3.3-month longer OS (HR 0.61). 11 These results from the SUNLIGHT trial led to the approval of FTD/TPI plus bevacizumab as a treatment option for previously-treated mCRC patients.
Apart from investigating the effectiveness of FTD/TPI alone or in combination with bevacizumab as a later-line therapy, recent studies have explored other potential FTD/TPI combinations, dosing regimens, and the use of FTD/TPI in earlier-line settings, especially for special populations such as those intolerant to intensive chemotherapy or elderly patients.12–17 While FTD/TPI has demonstrated efficacy in patients with refractory mCRC, clinical outcomes remain heterogeneous, and reliable biomarkers to guide treatment selection in real-world practice are lacking. Emerging molecular biomarkers have also been explored to refine prognostic stratification in colorectal cancer, further highlighting the complexity and heterogeneity of disease biology. 18 In particular, the impact of mismatch repair (MMR) status on outcomes with FTD/TPI remains unclear, as existing studies are limited by small sample sizes or insufficient representation of patients with deficient mismatch repair (dMMR). Given the increasing importance of molecular stratification in mCRC, there is an unmet need to better characterize prognostic factors, particularly dMMR status, in patients receiving FTD/TPI in routine clinical settings. Therefore, this study aimed to investigate the effectiveness of FTD/TPI in real-world mCRC patients and to identify clinical and molecular predictors of OS for FTD/TPI treatment.
Methods
Study design and patients
This multicenter retrospective study was conducted across four branches of Chang Gung Memorial Hospital, including Linkou, Keelung, Kaohsiung, and Chiayi branches. An electronic search was performed to identify patients who received FTD/TPI for metastatic CRC between December 10, 2018 and December 31, 2022, across the participating institutions. Clinical data were obtained from linked, de-identified real-world data sources within the Chang Gung Medical Foundation research database. Patients with incomplete medical records during FTD/TPI treatment were excluded from the analysis. Before study initiation, ethics approval was obtained from the Institutional Review Board of Chang Gung Medical Foundation (IRB No. 202301099B0 and 202400603B0), which oversees all participating institutions. The study was conducted in accordance with the Declaration of Helsinki.
The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement. 19 The completed STROBE checklist is provided as Supplemental Table S3.
Treatment
Patients received oral FTD/TPI on a 28-day regimen at 35 mg/m² twice daily for 5 consecutive days (days 1–5 and 8–12), followed by 2 days off (days 6, 7, 13, and 14) in the first 2 weeks. This was administered alone or in combination with oxaliplatin (85 mg/m² intravenously on day 1 every 2 weeks), irinotecan (100 mg/m² intravenously on day 1 every 2 weeks), and bevacizumab (5 mg/kg intravenously once every 2 weeks), until disease progression, intolerance, or death.
Data collection and outcome
Data collected included baseline demographic data, including age, sex, body mass index (BMI), primary tumor location, MMR status, KRAS mutation status, and neutrophil-to-lymphocyte ratio (NLR). BMI and NLR were calculated using measurements obtained within seven days prior to initiation of FTD/TPI treatment. MMR status was determined by immunohistochemistry (IHC) for mismatch repair proteins, including MutL homolog 1 (MLH1), MutS homolog 2 (MSH2), MutS homolog 6 (MSH6), and PMS1 homolog 2, mismatch repair system component (PMS2), according to institutional pathology protocols. Loss of nuclear expression of any of these proteins in tumor cells, in the presence of intact staining in internal control cells (e.g., stromal cells or infiltrating lymphocytes), was interpreted as deficient mismatch repair (dMMR). Retained nuclear expression of all four proteins was classified as proficient MMR (pMMR). All IHC assessments were performed as part of routine clinical practice and interpreted by board-certified pathologists at each participating institution. KRAS mutation status was determined using MassARRAY (Agena Bioscience)-based polymerase chain reaction (PCR) assays, according to institutional molecular pathology protocols. The primary outcome was OS. Survival was determined by linking to the Taiwan Death Registry database, which is available in our data source. The secondary outcome was time to treatment failure (TTF), which was defined as discontinuation of treatment for any reason, including progression of disease, treatment toxicity, and death. Patients were followed until December 31, 2022.
Statistical analysis
Patients received either monotherapy or combination therapy with FTD/TPI. Differences between groups were analyzed using independent sample t-test for continuous variables (i.e., age and BMI), Mann–Whitney U test for NLR, and chi-square test for categorical variables. The survival rates were estimated using the Kaplan–Meier estimator along with the log-rank test to compare groups (e.g., combination vs monotherapy; left side vs right side; KRAS mutation vs wild type; dMMR vs pMMR). The association of prognostic predictors with OS was assessed using univariate and multivariable Cox proportional hazard models. A two-sided p value of <0.05 was considered statistically significant. Statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC, USA). No formal sample size calculation was performed, as this was a retrospective study including all eligible patients during the study period.
Results
A total of 591 patients with metastatic colorectal cancer who received FTD/TPI were included in the study. Baseline demographic and clinical characteristics are summarized in Table 1. Male patients accounted for 55.0% of the cohort, and the mean age was 61.8 years. Most patients had left-sided primary tumors (78.8%), and approximately half had KRAS mutations (48.2%). Patients with dMMR tumors accounted for a small proportion of the cohort (n = 18, 3.0%). A detailed comparison according to MMR status is presented in Table 1. Overall, baseline characteristics were generally comparable between the dMMR and pMMR groups, although patients with dMMR tumors had a higher proportion of elevated neutrophil-to-lymphocyte ratio (NLR ⩾ 3), a higher rate of right-sided tumors, and a higher rate of primary site resection. A total of 127 patients (21.5%) received combination therapy . Treatment modality, either FTD/TPI monotherapy or combination therapy, was determined at the discretion of the treating physician. The median follow-up duration for the total cohort, monotherapy group, and combination therapy group was 5.7, 6.3, and 4.7 months, respectively. Detailed baseline characteristics according to treatment modality are provided in Supplemental Table S1. Only a small proportion of patients received immune checkpoint inhibitors (ICIs) during the study period (n = 6), including 5 patients in the pMMR group and 1 patient in the dMMR group.
Baseline characteristics of patients according to MMR status.
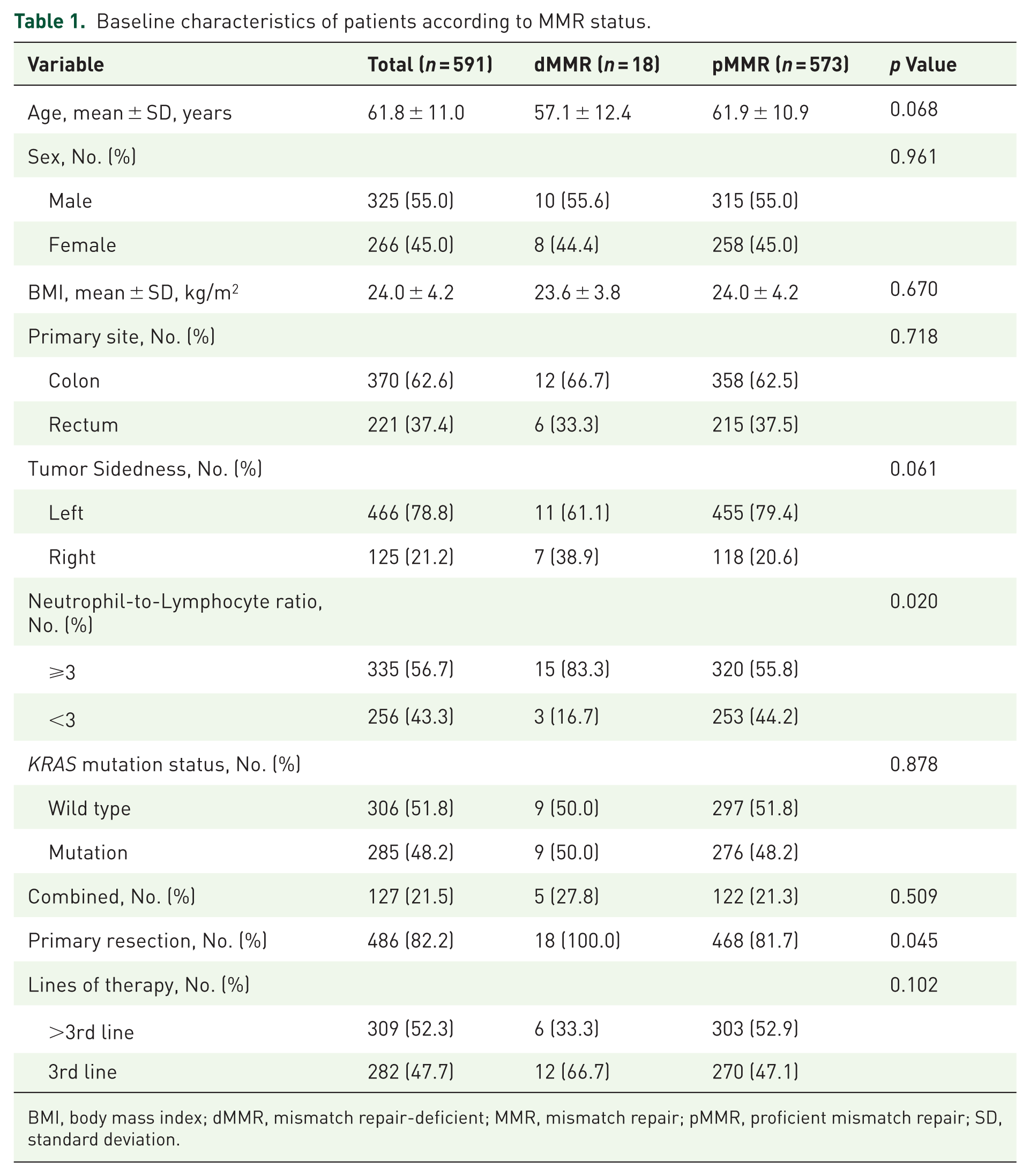
BMI, body mass index; dMMR, mismatch repair-deficient; MMR, mismatch repair; pMMR, proficient mismatch repair; SD, standard deviation.
Figure 1 illustrates the Kaplan–Meier curve of OS for the entire group. The median OS was 7.8 months (95% confidence interval (CI) 7.0–8.6 months). A difference in OS between patients receiving FTD/TPI monotherapy and combination therapy was observed (p = 0.03; Supplemental Figure S1). Subgroup analyses according to clinical factors showed that OS was comparable between left- and right-sided tumors (p = 0.83; Supplemental Figure S2). Higher body mass index (BMI ⩾ 24), lower neutrophil-to-lymphocyte ratio (NLR < 3), and earlier line of therapy at FTD/TPI initiation were associated with longer OS (Figure 2). Subgroup analyses according to molecular characteristics showed no significant difference in OS between KRAS-mutant and wild-type tumors (p = 0.79; Supplemental Figure S3). In contrast, patients with dMMR tumors experienced significantly longer OS compared to those with pMMR tumors (p = 0.001; Figure 3(b)). Patients with dMMR tumors also had longer TTF than those with pMMR tumors (Figure 3(a)).
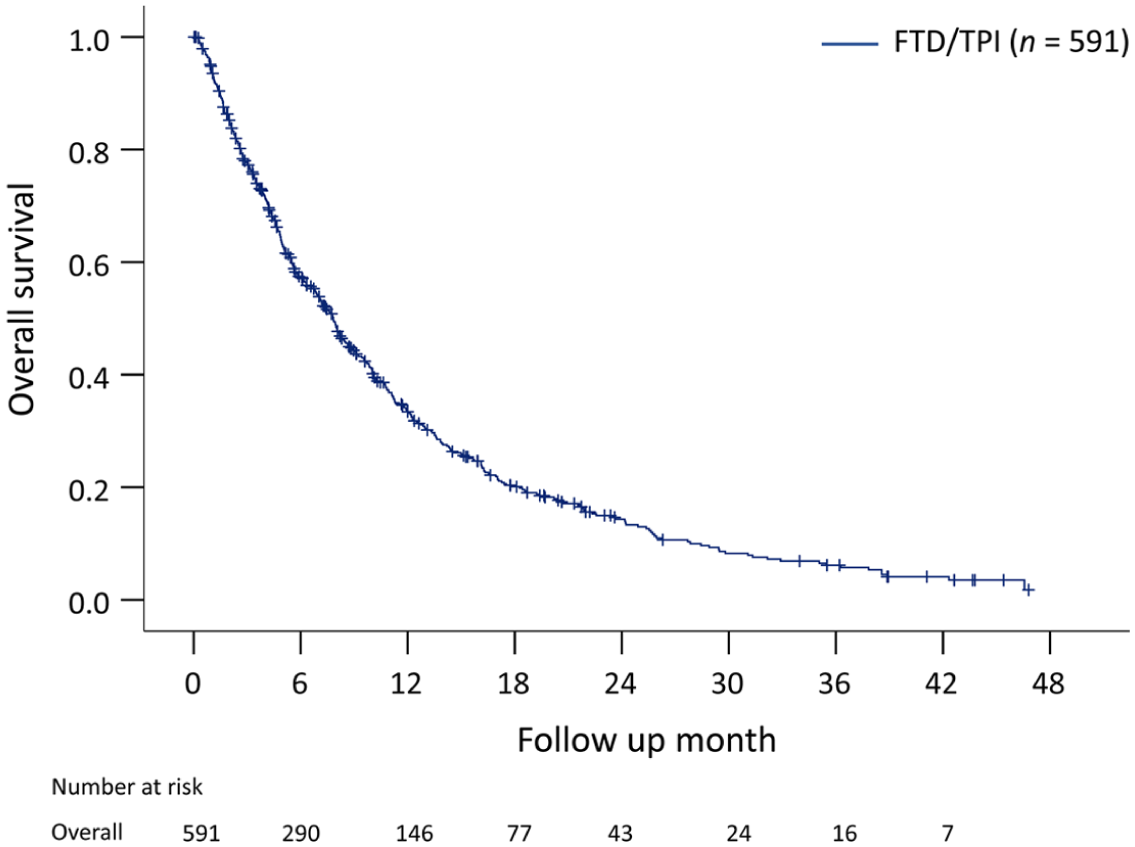
Kaplan–Meier curve of overall survival in the entire cohort.

Kaplan–Meier curves of overall survival, stratified by: (a) body mass index, (b) neutrophil-to-lymphocyte ratio, (c) lines of therapy.

Kaplan–Meier curves of survival, stratified by MMR status: (a) time to treatment failure, (b) overall survival.
Detailed subgroup analyses of median OS are provided in Supplemental Table S2.
The association between clinical factors, tumor characteristics, treatment modality, and OS was further evaluated using Cox regression analysis (Table 2). In univariate analysis, dMMR status, BMI, NLR, line of therapy, and treatment modality were associated with OS (all p < 0.05). In multivariable analysis, dMMR status (HR 0.29, 95% CI 0.14–0.60), BMI (HR 0.96, 95% CI 0.93–0.98), and NLR ⩾3 (HR 1.94, 95% CI 1.60–2.36) remained independently associated with OS (all p < 0.001).
Univariate and multivariable Cox regression analyses of overall survival.
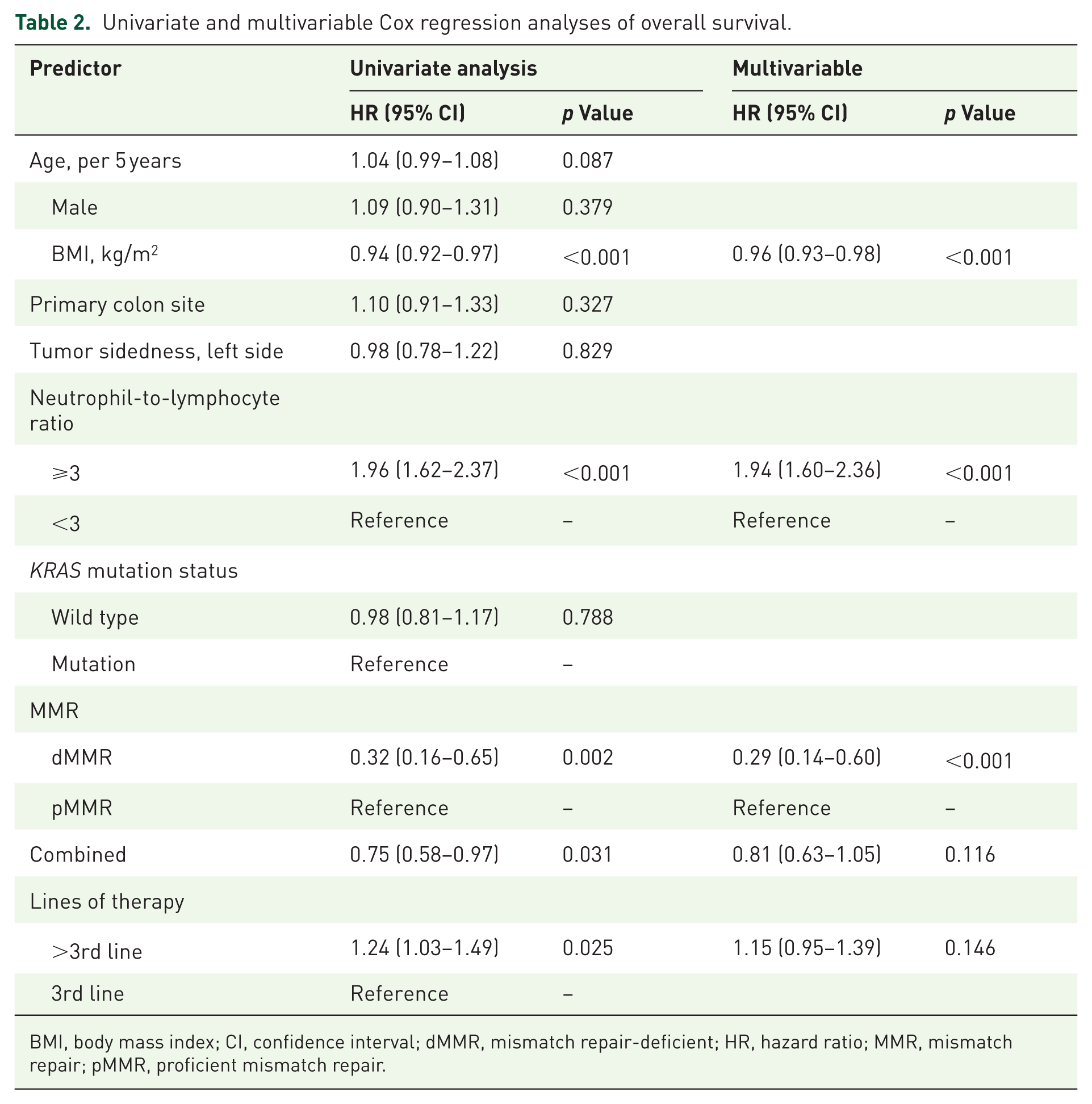
BMI, body mass index; CI, confidence interval; dMMR, mismatch repair-deficient; HR, hazard ratio; MMR, mismatch repair; pMMR, proficient mismatch repair.
Discussion
In this multicenter retrospective study, patients with mCRC treated with FTD/TPI had a median OS (mOS) of 7.8 months. MMR status, BMI, and NLR were independently associated with OS. Patients with dMMR tumors had significantly longer OS compared with those with pMMR tumors, whereas tumor sidedness and KRAS mutation status were not significantly associated with OS. Earlier line of therapy at FTD/TPI initiation and combination therapy were associated with longer OS in univariate analysis, but neither remained independently associated with OS in the multivariable model. Therefore, these findings should be interpreted as exploratory and may reflect underlying patient selection or treatment-sequencing factors. To our knowledge, this study represents one of the largest real-world cohorts evaluating outcomes according to MMR status among patients with mCRC treated with FTD/TPI. The efficacy of FTD/TPI in mCRC was first demonstrated in the pivotal RECOURSE Phase III trial, with a mOS of 7.1 months in the FTD/TPI arm, compared to 5.3 months in the placebo arm. 8 Several meta-analyses and real-world studies also demonstrated the effectiveness of FTD/TPI monotherapy (pooled HR = 0.61; mOS range 6.6 to 14.4 months from meta-analysis studies20–22; mOS range 6.6–9.97 months in real-world studies).23–29 More recently, the SUNLIGHT study 11 established FTD/TPI plus bevacizumab as a standard later-line treatment option, demonstrating a significant survival benefit over FTD/TPI monotherapy. Several studies with FTD/TPI combination therapy reported mOS as high as 16.7 months compared to 6.7 months for monotherapy.30–32 In our study, a numerically longer overall survival was observed in patients receiving combination therapy. However, this association was not statistically significant in the multivariable analysis and may be influenced by residual confounding. This study reflects real-world treatment patterns in the pre-SUNLIGHT era (2018–2022), during which combination strategies were not yet standardized and treatment selection was based on physician discretion. Therefore, the observed differences in survival may reflect underlying patient characteristics rather than a true treatment effect and should be interpreted with caution.
Earlier studies have assessed predictive factors for FTD/TPI treatment outcomes, including patient physical performance, type and number of metastases, prior treatments, disease duration, blood biomarkers, inflammation-associated indices, and genetic mutations.23–27,29,33–37 Genetic mutations in RAS or BRAF have been associated with OS in FTD/TPI monotherapy, though the direction of impact on survival has been inconsistent.23,24,29 Pooled analyses have shown that subgroups with RAS mutations or prior bevacizumab exposure may benefit from FTD/TPI plus bevacizumab combination therapy. 37 Our findings were consistent with prior clinical trials, which showed KRAS mutations had no significant impact on survival outcomes with FTD/TPI treatment. 36 NLR has increasingly been considered a biomarker to predict response to systemic chemotherapy in patients with mCRC. 35 Consistent with previous studies that reported a negative association between pretreatment NLR and survival, 35 our multivariable analysis also indicated that patients with an NLR ⩾3 had lower OS compared to NLR < 3. Similarly, lower BMI may reflect poorer nutritional reserve or cancer-related cachexia, which could contribute to inferior outcomes in later-line treatment settings. These findings support the potential value of readily available clinical markers for prognostic assessment in patients receiving FTD/TPI.
The approval of ICIs as first-line therapy reflects the fact that mCRC with dMMR or MSI-H typically responds poorly to conventional chemotherapies.2–5 Recent Phase II trials have also explored the efficacy of ICIs in previously treated MSI-H/dMMR mCRC, though indirect modeling has suggested it is not as cost-effective as FTD/TPI, primarily due to the high cost of ICIs. 38 Preclinical studies have highlighted the potential efficacy of FTD/TPI in dMMR and MSI-H mCRC due to the MBD4 frameshift mutation, 39 although the clinical evidence for this is currently limited. The MBD4 frameshift mutation occurred frequently in CRC with dMMR and impaired DNA mismatch repair in CRC cells.40–43 A few prior clinical studies on FTD/TPI treatment response have explored the impact of MMR status on treatment outcomes, and those with small patient numbers have reported no significant association.25,44 Only one retrospective study reported that FTD/TPI ± bevacizumab showed promising results for efficacy and safety in mCRC with dMMR. 45 In contrast, our study observed significantly longer OS for patients with dMMR compared to those with pMMR. Importantly, our cohort represents the largest real-world dataset of dMMR mCRC patients treated with FTD/TPI, surpassing previous studies in sample size. Furthermore, the proportion of dMMR mCRC patients in our cohort aligns with a recent review estimating the prevalence of MSI-H and dMMR in advanced CRC at 4.1% (95% CI 2.5–6.0%) and 6.9% (95% CI 5.4–8.5%), respectively. 46 Our findings suggest that dMMR status may define a subgroup with favorable survival outcomes among patients receiving FTD/TPI. Although clinical evidence remains limited, the C-TASK FORCE study reported a notable case of long-term response in an MSI-H patient treated with FTD/TPI plus bevacizumab, supporting the need for further investigation in this molecular subgroup. 47 These observations underscore the necessity of routine molecular profiling to optimize late-line treatment selection. Given the observed survival association, prospective validation is warranted to refine patient selection criteria and further elucidate the therapeutic role of FTD/TPI in this molecularly distinct mCRC subset.
Several limitations should be acknowledged. First, this was a retrospective study, which may restrict the generalizability of the findings and introduce residual confounding. Second, data on BRAF mutation status, tumor burden, metastatic sites, and performance status were not uniformly available, limiting our ability to assess their impact on survival following FTD/TPI treatment. In particular, information on performance status (e.g., ECOG) was not consistently captured in the linked, de-identified real-world data sources and could not be retrieved from electronic medical records. Given the established prognostic role of performance status in metastatic colorectal cancer, this may represent an important source of residual confounding. Third, although line of therapy was incorporated into the multivariable analysis, the potential impact of other unmeasured clinical factors cannot be fully excluded. In addition, only a small proportion of patients received ICIs, all of which occurred after FTD/TPI treatment (5 in the pMMR group and 1 in the dMMR group). This reflects the study period (2018–2022), during which ICIs were not yet widely reimbursed or routinely used as earlier-line therapy in Taiwan. Given the very limited number of cases and their distribution, the impact of immune checkpoint inhibitor use on survival outcomes is expected to be minimal in this cohort. Finally, no formal sample size calculation was performed because this was a retrospective study including all eligible patients during the study period.
Our findings have potential clinical implications. In addition to readily available clinical parameters such as BMI and NLR, our results highlight the importance of molecular factors, particularly MMR status, in prognostic stratification. The integration of clinical and molecular features may provide a more comprehensive approach to risk assessment in patients receiving later-line treatment. These factors may help clinicians better stratify patients, estimate prognosis, and support more individualized treatment planning and patient counseling in real-world practice.
Conclusion
This study indicated that MMR status, along with BMI and NLR, is associated with overall survival in patients with refractory mCRC treated with FTD/TPI. These findings highlight the potential role of integrating molecular and clinical factors to refine prognostic stratification in later-line settings. Further prospective studies are warranted to validate these findings and to explore their potential role in guiding treatment strategies.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261458757 – Supplemental material for Trifluridine/tipiracil and survival in mismatch repair-deficient metastatic colorectal cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359261458757 for Trifluridine/tipiracil and survival in mismatch repair-deficient metastatic colorectal cancer by Pei-Hung Chang, Wen-Kuan Huang, Yu-Li Su, Feng-Che Kuan, Jason Chia-Hsun Hsieh and Hung-Chih Hsu in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors gratefully acknowledge the invaluable support of all members of the Taiwan Association of Cancer Research (TACR). This work was supported by grant TACR_S0002 to C.H.H.
Declarations
Supplemental material
Supplemental material for this article is available online.
Meeting presentation
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.