
Abstract
Background:
Perihilar cholangiocarcinoma (pCCA) is a highly aggressive malignancy that persists even after curative resection. Although serum gamma-glutamyl transferase (GGT) is associated with cancer prognosis, most studies have evaluated its prognostic role only at a single time point. However, the prognostic value of perioperative dynamic trajectories remains unclear.
Objectives:
To evaluate perioperative GGT trajectories as prognostic markers in patients with pCCA undergoing radical resection.
Design:
This retrospective multicentre study included 765 patients with pCCA who underwent curative resection at two centres.
Methods:
Perioperative GGT trajectories were modelled using latent class mixed models. Patients were categorised according to trajectory patterns, and associations with overall survival (OS) were evaluated using multivariate Cox regression with clinical covariates. Model discrimination was assessed using time-dependent receiver operating characteristic analysis.
Results:
Two distinct perioperative GGT trajectories were identified: flat and V-shaped. The model showed an adequate fit (Bayesian Information Criterion (BIC) = 35818.61) and good classification quality (entropy = 0.69). The two classes accounted for 48.32% and 51.68% of the patients, respectively. Patients in the flat trajectory group had significantly longer OS (HR = 0.603, 95% CI: 0.450–0.808, p < 0.001), independent of other factors. The model yielded AUCs of 0.729 (0.658–0.801) and 0.805 (0.721–0.881) for 3- and 5-year OS, respectively.
Conclusion:
Perioperative GGT trajectories independently predicted pCCA prognosis. Monitoring GGT dynamics may offer a simple and practical tool for postoperative risk stratification.
Plain language summary
Perihilar cholangiocarcinoma is a rare and aggressive cancer of the bile ducts. Surgery is currently the only treatment that can offer long-term survival, but outcomes vary widely between patients. For this reason, doctors are interested in simple ways to estimate a patient’s risk after surgery. Gamma-glutamyl transferase (GGT) is a routine blood test related to liver function and is commonly measured before and after surgery. Most previous studies have examined GGT at a single time point. In clinical practice, however, GGT levels often change during the perioperative period, and it is uncertain whether these changes are related to patient survival. In this retrospective multicentre study, we analysed data from 765 patients who underwent curative surgery for perihilar cholangiocarcinoma at two hospitals. We examined how GGT levels changed from before surgery to the early postoperative period and grouped patients according to similar patterns over time. We then assessed whether these patterns were associated with overall survival, taking other clinical factors into account. Two main patterns of GGT change were identified. One group showed relatively stable GGT levels, while the other showed a V-shaped pattern, with levels decreasing and then rising after surgery. Patients with stable GGT levels generally survived longer after surgery, even after adjustment for other factors. The model showed reasonable performance in predicting survival at three and five years. These findings suggest that changes in GGT over time may provide useful information beyond a single measurement. Because GGT testing is simple and widely available, monitoring perioperative GGT trends may help support postoperative risk assessment in patients with this disease.
Introduction
Perihilar cholangiocarcinoma (pCCA) originates from the bile ducts at the hepatic hilum and represents approximately 50%–60% of all cholangiocarcinomas.1,2 The complexity of pCCA largely stems from its anatomical position at the hepatic hilum, where the confluence of the right and left hepatic ducts poses considerable challenges for both resection and management. 3 Surgical resection remains the only potentially curative treatment. However, even when negative margins are achieved, outcomes remain poor, with a 5-year overall survival (OS) ranging from 13% to 50% and a disease-free survival (DFS) of approximately 30%.4,5 Thus, identifying reliable prognostic biomarkers to improve outcome prediction and guide treatment decisions has become a key research priority. Accumulating evidence suggests that cholangiocarcinoma is a multifactorial disease, with contributing factors including metabolic influences, 6 conditions associated with bile stasis and chronic biliary inflammation, 7 and enteric microbiota dysbiosis with biliary tract bacterial colonisation. 8 This complex pathogenesis suggests that reliance on single time-point biomarkers may be insufficient. However, most existing studies have concentrated on static measurements, potentially overlooking the dynamic nature of disease evolution. Most existing studies have concentrated on biomarkers measured at a single point in time, potentially overlooking the dynamic nature of disease evolution.
Gamma-glutamyl transferase (GGT) is a liver enzyme that catalyses the hydrolysis of gamma-glutamyl groups from glutathione and its conjugates. 9 Clinically, GGT is a well-established marker of hepatobiliary dysfunction and excessive alcohol consumption.9–12 In addition to liver function, GGT has been linked to systemic inflammation 13 ; chronic diseases, such as cardiovascular disease 14 and chronic kidney disease 15 ; and multiple malignancies, including gastrointestinal,10,16–20 breast 21 and lung cancers. 22 Recently, increasing attention has been directed towards the prognostic potential of GGT in patients undergoing surgical resection for gastrointestinal malignancies.16,20 Nevertheless, most studies have examined GGT at a single time point without considering the prognostic relevance of its dynamic temporal trajectories.
During the perioperative stage, encompassing both preoperative and postoperative intervals, patients with pCCA often undergo substantial surgical stress accompanied by fluctuations in systemic inflammation. 23 Considering the physiological vulnerability during this phase, this study sought to determine whether changes in GGT levels across the perioperative window could serve as a practical marker of prognosis in patients who underwent radical resection. To characterise these variations, a latent class mixed model (LCMM) was used to describe the dynamic perioperative profiles of serum GGT levels in patients with pCCA. Subsequently, the relationship between different trajectory patterns and patient outcomes was examined. A multivariate prognostic model was then constructed, combining trajectory classification with key clinical factors, to facilitate individualised postoperative risk evaluation and clinical decision-making.
Materials and methods
Data collection
We used the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline 24 to draft this manuscript, and the STROBE reporting checklist when editing, included in the Supplemental Checklist.
Data for this study were retrospectively collected from Henan Provincial People’s Hospital and Third Military Medical University Southwest Hospital. The clinical dataset included perioperative GGT levels, key demographic variables and critical pathological parameters, such as histological differentiation, Bismuth classification, surgical margin status, vascular and perineural invasion and tumour–node–metastasis (TNM) stage defined according to the eighth edition of the American Joint Committee on Cancer (AJCC) classification. Overall survival information was obtained through routine postoperative follow-up, including scheduled outpatient visits and telephone interviews. Eligibility for the study required a histopathologically confirmed diagnosis of pCCA based on postoperative examination of resected surgical specimens, which served as the diagnostic gold standard. The exclusion criteria were as follows: distant metastasis, a history of other malignancies, undergoing secondary surgery or noncurative resection, missing preoperative GGT values (within 2 weeks before surgery), and fewer than three recorded GGT measurements spanning from 2 weeks preoperatively to 2 months postoperatively. Patients who met the eligibility criteria and did not meet any of the exclusion criteria constituted the final cohort for the GGT trajectory analysis. Patients lost to follow-up were excluded from the prognostic analysis, whereas cases with unavailable dates of death were treated as having missing outcome data.
Model construction
Because the distribution of GGT values was markedly skewed, standard transformations (such as log or square root) did not adequately satisfy the assumption of normally distributed random effects. Therefore, an LCMM was employed to characterise the heterogeneity in GGT trajectories. 25 Modelling was performed using the lcmm function in the lcmm package in R (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria), and the main steps were as follows:
1. Overall temporal trends of GGT were plotted to obtain an initial impression of the potential trajectory patterns.
2. Model specification and parameter configuration.
We explored models with two to four latent GGT trajectories. Linear, quadratic and natural-spline forms were examined to approximate the most suitable trajectory pattern. As biomarker measurements are influenced by patient-level heterogeneity, fixed-effect-only formulations may not adequately capture this variation. Therefore, we compared random-intercept and random-intercept-with-slope models. To promote model convergence and maintain numerical stability, estimates obtained from a single-class model (ng = 1) were used as initial values when fitting multiclass models (ng = 2–4) through argument B.
3. Model selection
The optimal LCMM was selected based on predefined criteria balancing model fit, classification accuracy and interpretability. The main criteria were as follows: (1) successful model convergence (conv = 1); (2) the smallest Bayesian Information Criterion (BIC); (3) entropy >60%, indicating acceptable classification certainty; and (4) ⩾10% of individuals per class to avoid sparsity. Taken together, these criteria helped to identify what we regarded as a reasonably robust and interpretable latent class structure.
Survival outcomes
OS and 3- and 5-year survival rates were assessed as the main study endpoints. OS was defined as the interval between surgery and death or, for censored patients, the date of the last follow-up. The survival dataset was updated on 31 December 2024.
Statistical analysis
For patients with incomplete covariate information, multiple imputation was applied using chained equations implemented in the mice package in R. The imputation approach varied according to variable type: multinomial logistic regression (polyreg) for categorical variables, proportional odds logistic regression (polr) for ordinal variables, and predictive mean matching (pmm) for continuous variables. Variables without missing values were not imputed but were still included in the analysis model. Five imputed datasets were generated using maximum likelihood estimation with a fixed random seed to maintain reproducibility across runs. Patients lacking information on the main outcome (event) were excluded from the survival analysis, and no imputation was applied for these cases. A brief comparison of the datasets before and after imputation was conducted (Table S3).
Comparisons between the trajectory groups were performed using the raw dataset before imputation. Continuous variables that were not normally distributed are summarised as medians (interquartile ranges) and were compared using the Mann–Whitney U test. For ordinal data, values are shown as counts and percentages and were analysed using the Mann–Whitney U test. Nominal variables are described in the same way and were examined using either a χ2 test or Fisher’s exact test, depending on the sparsity of the cells. Effect sizes were also reported, including rank-biserial correlation for continuous data, Cliff’s δ for ordinal data and Cramér’s V for categorical data. Kaplan–Meier curves illustrated the survival trends among the trajectory groups, and group differences were examined using the log-rank test. Prognostic factors were screened using the least absolute shrinkage and selection operator (LASSO) approach, in which trajectory class membership was entered as a covariate. Based on the selected variables, a Cox proportional hazards model was built to estimate OS. To reduce the potential influence of intervention-related effects on perioperative GGT trajectories, a sensitivity analysis was performed after excluding patients who underwent preoperative biliary drainage or developed postoperative biliary/infectious complications, including biliary leakage, cholangitis, postoperative liver failure and intra-abdominal infection. Time-dependent receiver operating characteristic (ROC) curves were drawn to assess the 3- and 5-year survival rates. All statistical analyses were two-sided, and statistical significance was set at p < 0.05. Analyses were performed using R (version 4.5.1).
Results
Study population
Between January 2012 and December 2024, 765 patients who underwent surgical treatment for pCCA at the two participating hospitals were identified. Of these, 15 had distant metastases, 5 had undergone repeat surgery, 11 had a history of malignancy and 66 had undergone non-radical procedures. GGT measurements were available for 566 patients; however, not all records were complete. Twelve extreme values were removed according to the IQR rule; values lying more than twice the IQR from either quartile were excluded. In addition, 159 patients had no documented GGT results within 2 weeks before surgery, and 37 had fewer than three available tests from the preoperative to the early postoperative period (approximately 2 months). After these exclusions, 358 patients remained for trajectory modelling. For survival analysis, patients lost to follow-up were further excluded, leaving 286 patients in the final analysis cohort. Regarding missing covariate data, Bismuth classification was unavailable for four patients, TNM stage for 32 patients and histological differentiation for 23 patients. Overall survival data were missing for 12 patients. The overall screening and selection processes are summarised in Figure 1.
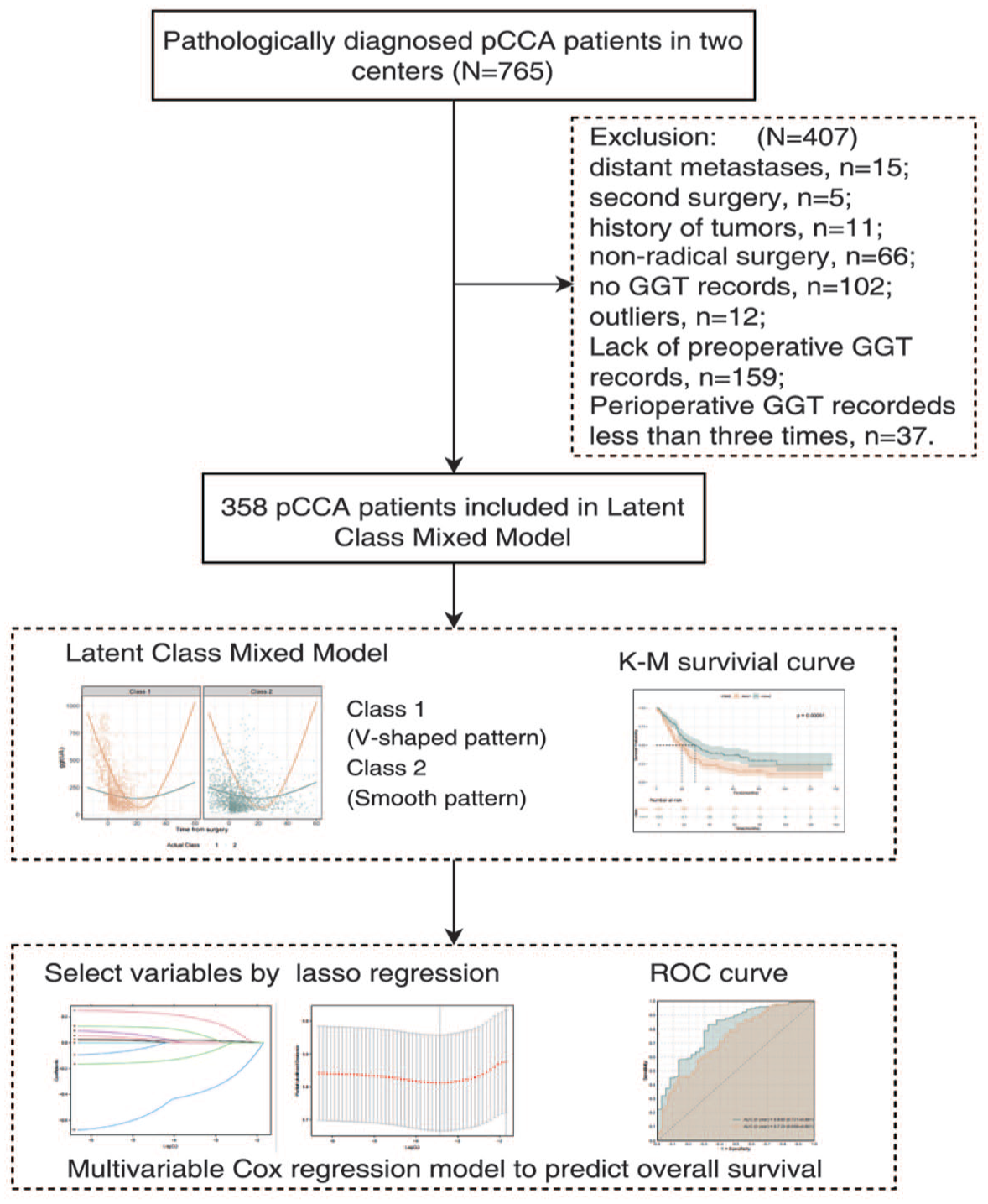
The study flowchart.
Latent class mixed model construction
Prior to model construction, the perioperative GGT trajectories of all included patients were plotted to explore the potential patterns in GGT changes (Figure S1). Eighteen model configurations were tested. The models assuming a random intercept and a linear fixed component for the two to four trajectory classes were denoted as m2a, m3a and m4a, respectively. Those that included a random slope under the same linear structure were named m2b, m3b and m4b. When a quadratic term was introduced, models with only random intercepts were tagged as m2c, m3c and m4c, whereas those that also allowed random slopes became m2d, m3d and m4d. A similar setup was applied to the spline-based specifications: m2e, m3e and m4e for the random-intercept models, and m2f, m3f and m4f when both the intercept and slope were random. The model fit indices for these 18 versions are summarised in Table S1.
According to predefined criteria, the m2f model appeared to provide the best fit, distinguishing between the two main patterns of GGT change. This model incorporated both random intercept and slope terms and used natural-spline functions as fixed effects (Figure 2).

Perioperative GGT trajectories identified by the m2f model.
Convergence was reached after 26 iterations and appeared to be stable across the starting values. The first class, representing roughly half of the cohort (48.32%), showed a rather pronounced V-shaped curve, with a sharp drop (β = –14.56, SE = 0.93, p < 0.001) followed by an evident rebound (β = 8.17, SE = 1.07, p < 0.001). By contrast, the second class had a flatter overall shape, with only mild fluctuations—an initial small drop (β = –1.53, SE = 0.68, p = 0.025) and a later modest rise (β = 1.39, SE = 0.66, p = 0.034; Table S2). The estimated variance components for intercept and slope were 1.99 and 0.01, respectively, with a covariance of -0.07 between them. The baseline profiles of the two trajectory groups are presented in Table 1. All subsequent analyses were based on the original non-imputed dataset. Except for the survival outcomes (OS and event status), no major baseline differences were observed between the two groups (all p > 0.05).
Baseline characteristics and outcomes stratified by GGT trajectory class.
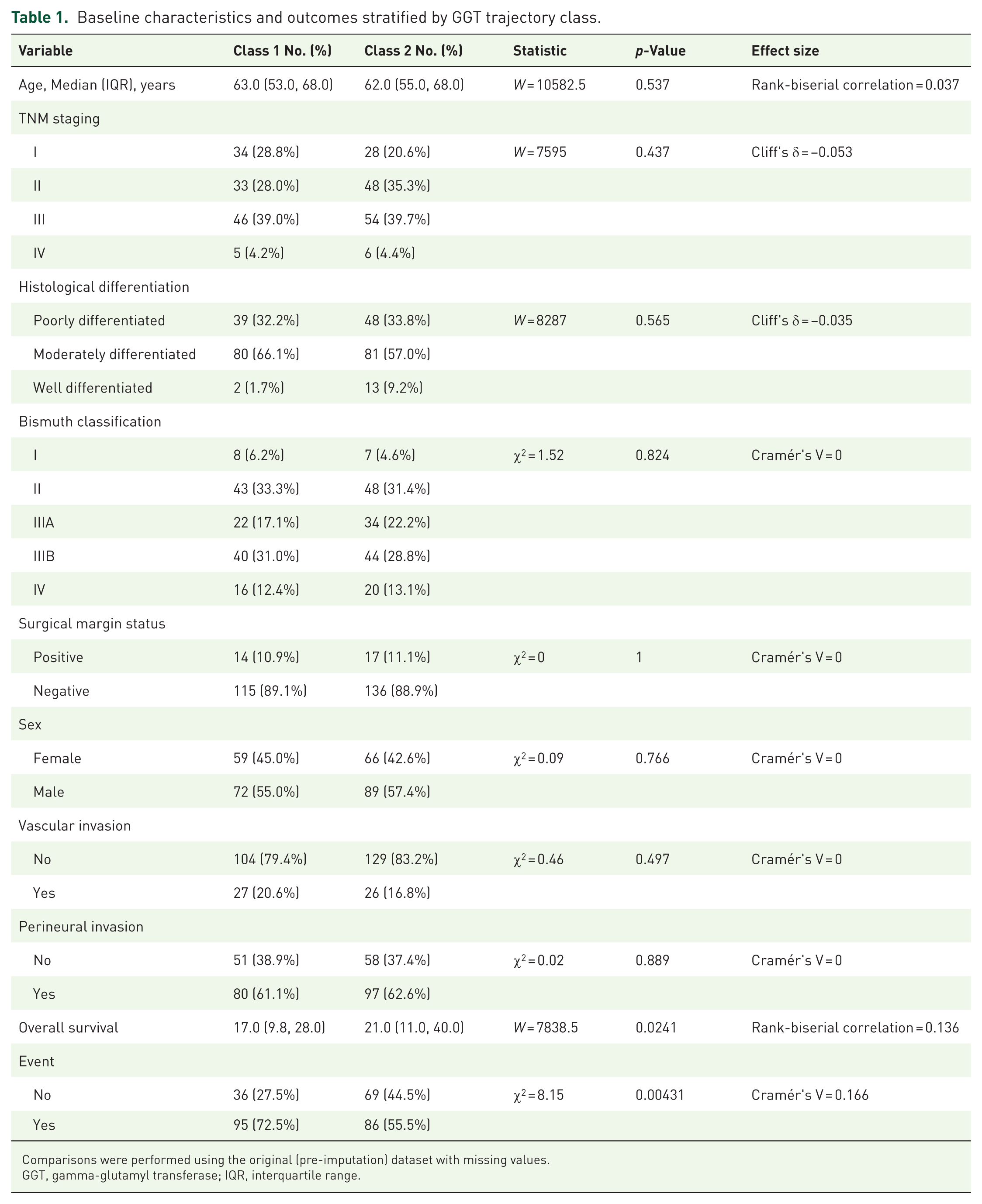
Comparisons were performed using the original (pre-imputation) dataset with missing values.
GGT, gamma-glutamyl transferase; IQR, interquartile range.
Prognosis prediction
For the prognostic analysis, patients lost to follow-up were excluded, leaving 286 patients with pCCA.
Trajectory classes and OS
Trajectory class was included as a covariate to examine its association with prognosis. The Kaplan–Meier curves (Figure 3(a)) suggested that patients in class 2 (flat trajectory) experienced better survival than those in class 1 (V-shaped trajectory; HR = 0.60, 95% CI: 0.45–0.81, p < 0.001). In the subgroup analysis, the association remained significant in the Henan Provincial People’s Hospital cohort (HR = 0.61; 95% CI: 0.41–0.89; p = 0.011; Figure 3(b)). In the Third Military Medical University Southwest Hospital cohort, the trend was similar but did not reach statistical significance (HR = 0.70; 95% CI: 0.44–1.12; p = 0.14), possibly because of the smaller sample size (N = 135; Figure 3(c)).

Kaplan–Meier survival curves stratified by GGT trajectory classes in the overall study cohort and the two study centres. (a) Kaplan–Meier survival curves stratified by GGT trajectory classes in the overall study cohort. (b) Kaplan–Meier survival curves stratified by GGT trajectory classes in the Henan Provincial People’s Hospital cohort. (c) Kaplan–Meier survival curves stratified by GGT trajectory classes in the Third Military Medical University Southwest Hospital cohort.
Multivariable prognostic model
LASSO regression was employed for variable selection. Figure S2(A) shows the coefficient paths of the candidate variables, and Figure S2(B) depicts the model selection using 10-fold cross-validation. The model with the lowest mean squared error was selected. Five factors (trajectory class, TNM stage, histological differentiation, age and perineural invasion) were incorporated into a multivariate Cox proportional hazards model. Table 2 presents the results of the univariate and multivariate regression analyses. Time-dependent ROC curves for 3- and 5-year survival were plotted (Figure 4) based on the multivariate Cox model. The curves showed acceptable discrimination, especially for long-term survival, with AUCs of 0.729 (95% CI: 0.658–0.801) and 0.805 (95% CI: 0.721–0.881), respectively.
Association of clinical variables and GGT trajectory classes with overall survival: univariate and multivariate Cox regression analyses.

CI, confidence interval; GGT, gamma-glutamyl transferase; HR, hazard ratio.

ROC curves of the multivariable Cox model for predicting 3-year and 5-year overall survival.
Sensitivity analysis
To further evaluate whether the identified perioperative GGT trajectories were influenced by intervention-related factors, we performed a sensitivity analysis (Table S4) after excluding patients who underwent preoperative biliary drainage and developed postoperative biliary or infectious complications, including biliary leakage, cholangitis, postoperative liver failure and intra-abdominal infection. After exclusion, the association between GGT trajectory patterns and overall survival remained largely unchanged. In multivariate Cox regression analysis, trajectory class 2 remained independently associated with improved overall survival compared with class 1 (HR 0.567, 95% CI: 0.404–0.796, p = 0.001), with effect estimates comparable to those observed in the primary analysis.
Discussion
This multicentre retrospective analysis showed that perioperative GGT trajectories may help stratify patients with pCCA who underwent radical resection into two prognostic groups. Patients whose GGT levels followed a relatively flat trajectory appeared to show better OS than those whose trajectory was V-shaped (HR = 0.603; 95% CI: 0.450–0.808; p < 0.001). This association remained after adjusting for clinical covariates in the multivariable model, suggesting that GGT trajectories could act as independent prognostic indicators. Besides, given that serum GGT levels are highly sensitive to biliary obstruction, decompression procedures and postoperative inflammatory events, we further performed a sensitivity analysis excluding patients with preoperative biliary drainage and postoperative biliary or infectious complications. The association between GGT trajectory patterns and overall survival remained stable, suggesting that the observed trajectories were not primarily driven by intervention-related effects. Furthermore, a prognostic model combining trajectory classes with clinical variables showed reasonable discrimination, particularly for longer-term survival, with AUCs of 0.729 (95% CI: 0.658–0.801) at 3 years and 0.805 (95% CI: 0.721–0.881) at 5 years, indicating potential clinical applicability.
In previous studies, elevated preoperative GGT levels have been associated with worse prognosis in gastrointestinal cancers. These levels have been linked to advanced tumour stage, vascular invasion and poor differentiation.16–19,22 In a retrospective multicentre study involving 699 patients with hepatitis B-related hepatocellular carcinoma, a preoperative serum GGT level ⩾38 U/L independently predicted higher postoperative all-cause mortality (HR 1.73; 95% CI: 1.06–2.84). 20 Among patients with colorectal cancer, one review noted that elevated serum GGT levels were linked to an increased risk of cancer onset, lymph node metastasis, tumour progression and reduced OS. 16 However, these studies predominantly used single time-point GGT measurements and did not address dynamic trajectories over time.
Previous studies have suggested that changes in tumour marker levels around the time of surgery may be related to patient prognosis. For instance, among patients with pancreatic adenocarcinoma, those whose CA199 normalised during neoadjuvant therapy tended to have better post-resection survival: 2-year RFS of 47% versus 28% (p = 0.01) and OS of 75% versus 49% (p = 0.01). 26 Among patients with extrahepatic bile duct cancer, those who failed to achieve postoperative CA199 normalisation appeared to have a lower 5-year OS rate (17.9% vs 39.2%, p < 0.001). 27 Among patients with gallbladder carcinoma, persistently high perioperative CA199/total bilirubin ratios (the non-normalisation group) were linked to worse 3-year OS (24.2% vs 72.0% and 58.4%, respectively, p < 0.001) and RFS (11.8% vs 54.5% and 25.5%, respectively, p < 0.001) compared with the normal or normalisation groups. 28 Building on this prior work, we applied an LCMM to explore heterogeneity in perioperative GGT trajectories, aiming to move beyond subjective classification towards a more objective and statistically grounded approach. To our knowledge, this is the first study to examine the prognostic value of perioperative GGT trajectories in patients with pCCA, a type of cancer known to have generally poor outcomes, even after curative resection. Incorporating longitudinal measurements could provide a more detailed understanding of patient responses to surgery and might help better predict long-term survival outcomes.
The biological mechanisms underlying the observed GGT trajectories remain unclear; however, a few plausible explanations can be considered. GGT participates in the glutathione cycle, hydrolysing extracellular GSH into glutamate and cysteinylglycine. Cysteinylglycine may then be cleaved by dipeptidases to yield cysteine, a rate-limiting precursor for intracellular GSH and protein synthesis. 29 By influencing GSH availability, GGT may modulate the cellular redox status30,31 and contribute to the detoxification of ROS and xenobiotics. 32 These processes are considered important for liver regeneration 33 and the tumour microenvironment. 34 Higher GGT activity has been suggested not only as a marker of oxidative stress but also as an active contributor to tumour progression. According to Bansal et al., 35 inhibition of the GGT1/GSH pathway suppresses the growth of clear cell renal carcinoma by inducing cell cycle arrest, inhibiting migration and reducing proliferation. Similarly, Xie et al. 36 found that increased GGT1 expression might enhance the immunosuppressive activity of myeloid-derived suppressor cells (MDSCs), potentially promoting tumour progression. During the perioperative period, a flat GGT trajectory might indicate relatively successful restoration of redox balance, more effective resolution of surgical inflammation and better hepatic functional reserve, which could improve survival. Conversely, a V-shaped trajectory showing an early decline followed by rebound might reflect unstable oxidative stress, lingering cholangiocyte injury, or maladaptive redox recovery, which could worsen postoperative inflammation, hinder tissue repair and possibly promote tumour recurrence.
Our findings have several clinical implications that may be relevant for the management of patients with pCCA. At present, the prediction of prognosis in patients with pCCA depends largely on traditional clinical staging approaches, such as the TNM classification; however, in clinical practice, neither the seventh nor the eighth AJCC staging edition clearly distinguishes prognostic outcomes among patients undergoing curative surgery. 37 Including GGT trajectories in prognostic evaluations might offer a more dynamic and individualised perspective, reflecting not only tumour-related factors but also aspects of the patient’s physiological status. Tracking perioperative GGT trajectories could help clinicians estimate recurrence tendencies, tailor postoperative follow-up, and adjust treatment decisions when necessary. In particular, patients with a V-shaped perioperative GGT trajectory may be considered a higher-risk subgroup and could benefit from intensified postoperative surveillance, including more frequent imaging and shorter follow-up intervals, to facilitate earlier detection of recurrence. In addition, these patients may warrant closer evaluation in multidisciplinary discussions regarding the potential role of adjuvant therapy, even in the absence of clear radiological evidence of disease progression. By contrast, patients with a relatively stable trajectory may be managed with standard surveillance protocols. GGT is a relatively simple and cost-effective biomarker, making it a practical tool for routine clinical use, particularly in resource-limited settings where advanced molecular tests may be unavailable.
Although this study offers new insights, it has a few limitations. First, an important limitation of this study relates to the substantial sample attrition during cohort selection, which may potentially affect the generalizability of the findings. To address this concern, we performed a comprehensive comparison of baseline clinical, surgical and tumour characteristics between included and excluded patients. Most variables showed generally comparable distributions between the two groups, suggesting limited systematic differences. Although a modest imbalance was observed in the Bismuth classification, the corresponding effect size remained small, indicating only minor differences in biliary anatomical complexity. Nevertheless, because not all potential confounders could be fully controlled for, residual selection bias cannot be entirely excluded and the generalizability of our findings may therefore be limited when extrapolating to broader pCCA populations. Moreover, although our model showed encouraging predictive behaviour, the biological basis for the different GGT trajectories remains unclear. Further experimental work would be helpful to confirm these findings and clarify the role of GGT in tumour development and recovery after surgery. Likewise, larger prospective studies involving multiple centres would be valuable to verify the prognostic relevance of perioperative GGT trajectories.
Conclusion
The current study demonstrated that perioperative GGT trajectories were independently associated with long-term survival in patients with pCCA undergoing radical resection. Patients with a flat GGT trajectory showed significantly better postoperative outcomes than those with a V-shaped trajectory, suggesting that dynamic perioperative changes in GGT may provide prognostic information beyond single time-point measurements. These findings improve the understanding of the clinical significance of perioperative biochemical dynamics and support the potential utility of trajectory-based monitoring for postoperative risk stratification. Although prospective validation and mechanistic investigations are still required, perioperative GGT trajectory analysis may represent a simple and practical approach for identifying high-risk patients after curative resection.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261461750 – Supplemental material for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study
Supplemental material, sj-docx-1-tam-10.1177_17588359261461750 for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study by Huiyuan Tian, Haotian Hu, Qiankun Luo, Zhipeng Liu, Zhiyu Chen and Tao Qin in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359261461750 – Supplemental material for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study
Supplemental material, sj-docx-2-tam-10.1177_17588359261461750 for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study by Huiyuan Tian, Haotian Hu, Qiankun Luo, Zhipeng Liu, Zhiyu Chen and Tao Qin in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261461750 – Supplemental material for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study
Supplemental material, sj-pdf-1-tam-10.1177_17588359261461750 for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study by Huiyuan Tian, Haotian Hu, Qiankun Luo, Zhipeng Liu, Zhiyu Chen and Tao Qin in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-2-tam-10.1177_17588359261461750 – Supplemental material for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study
Supplemental material, sj-pdf-2-tam-10.1177_17588359261461750 for Prognostic value of perioperative gamma-glutamyl transferase trajectories in perihilar cholangiocarcinoma: a multicentre retrospective cohort study by Huiyuan Tian, Haotian Hu, Qiankun Luo, Zhipeng Liu, Zhiyu Chen and Tao Qin in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.