
Abstract
Introduction
The C-Trac splint has been designed to mechanically stretch the transverse carpal ligament and is advertised as an alternative to surgical Carpal Tunnel Decompression. The purpose of the study is to compare the effectiveness of the C-Trac splint with standard splinting in mild to moderate idiopathic carpal tunnel syndrome.
Methods
This is a pilot parallel randomised controlled trial. Forty-nine patients with clinically and neurophysiologically proven carpal tunnel syndrome were randomised into the two treatment groups, C-Trac and Beta Wrist Brace, and reassessed clinically for one year.
Results
Patients were generally satisfied with both splints, but two out of the 24 C-Trac patients developed problematic side effects possibly due to using the splint: De Quervains tenosynovitis and basal joint arthritic pain. There was no clinically relevant or statistically significant difference in the success and failure rates of the two splints by eight weeks, six months or at one year. Three of the 25 C-Trac splints (costing £130 each) used during the one-year study required replacement, compared with eight of the Beta Wrist Braces (costing approximately £10 each).
Conclusions
These results suggest that C-Trac splint is not dissimilar in efficacy to a resting Beta Wrist Brace. The reported side effects raise questions as to the wisdom of its unregulated use.
Introduction
Carpal tunnel syndrome (CTS) is a very common condition affecting approximately 10% of the female population,1,2 and most cases occur without obvious cause. 3 The gold standard treatment, Carpal Tunnel Decompression (CTD), costs approximately £800 ($1100) per operation. At the Pulvertaft Hand Centre in Derby, 600 such operations are performed each year. Surgery exposes patients to the risk of pillar pain, nerve damage, scar tenderness and reduced grip strength, 4 and some patients are reluctant to proceed with operative management if their symptoms are not too intrusive. 5
In recent years, a new form of splint (C-Trac; MeDevice Corp, Miami, FL) has been marketed which is purported to stretch the transverse carpal ligament, obviating the need for surgery.6,7 The single-patient-use C-Trac splints are available for purchase without the need for a prescription for £130 in the UK and $149.99 in the USA.6,7
A small non-comparative outcome study conducted by the designers of C-Trac and published in the American Journal of Hand Therapy concluded that C-Trac was a very effective treatment for CTS resistant to treatment with non-steroidal anti-inflammatory drugs (NSAIDS), resting hand splints during the night, acupuncture and hand therapy. Patient satisfaction with the C-Trac was high. 8
Beta Wrist Brace (BWB) resting splints (Promedics) have been shown to be effective for the management of mild to moderate CTS. 9 These resting splints are thought to act by limiting wrist movement, particularly flexion or extension, thereby maximising carpal tunnel volume and minimising median nerve compression within the carpal tunnel. 10 The BWB is available without prescription and retails at approximately £10.
A pilot randomised controlled trial was therefore initiated at the Pulvertaft Hand Centre to ascertain the safety of the C-Trac and BWBs, to compare the effectiveness of the splints for managing mild and moderate idiopathic CTS and to evaluate patient satisfaction with the splints.
Materials and methods
Trial design
This is a pilot, parallel, randomised controlled trial to assess the safety and side effects of the C-Trac splint for treating idiopathic CTS and to assess whether the new C-Trac device is effective enough to warrant further research. Recruitment and consenting of patients followed ICH-GCP guidelines (The International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use – Good Clinical Practice). No changes were made to the methods after trial commencement.
Participants
Patients were included if a diagnosis of CTS was established from a history and clinical examination and confirmed with nerve conduction studies in keeping with usual clinical practice. Clinical assessments were made by two surgically qualified doctors supported by three senior hand therapists.
Patients with severe CTS, as evidenced by wasting of abductor pollicis brevis (APB), were excluded before consent or randomisation, as were patients with nerve conduction study results not indicative of CTS. Patients were also excluded before consent or randomisation if they had non-idiopathic CTS: a history of gout, hypothyroidism, previous fragility fracture, symptomatic basal joint arthritis, septic or rheumatoid arthritis of the hand, previous wrist fracture, diabetes mellitus, current pregnancy, amyloidosis, acromegaly, renal dialysis, current oral steroid use or regular use of hand-held vibrating tools. The exclusion criteria extended to patients having had previous CTD or steroid injection of the affected wrist and patients aged 65 years or older.
After commencement of the trial, three other exclusion criteria were added: the second hand of patients with bilateral CTS, patients with vibration white finger and patients with evidence of double crush phenomenon were also excluded.
Patients with nerve conduction studies in keeping with CTS were contacted by the research team and if interested in taking part in the study, were sent an information leaflet and a consent form and an appointment was made at the research clinic for them to request additional information and to undergo further assessment after formal consenting.
Interventions
The C-Trac splint consists of a C-shaped, tubular, semi-rigid frame made of Duraplast© (Smith & Nephew) contoured around the dorsum of the wrist and hand. On the palmar aspect, its free edges grip the thenar and hypothenar eminences. There is an opening in the tube for the thumb. On the inside of the tubular C-shaped frame is an air bladder attached to a pressure gauge and a hand-pump identical to those found on a sphygmomanometer. This bladder is in contact with the dorsum of the carpus. Inflation of the bladder to 180–190 mmHg creates pressure on the dorsum of the hand, and the free edges of the splint pull the thenar and hypothenar eminences apart. This inflation is maintained for 2 min. A minutes rest is followed by a further 2 min of inflation. Patients in the C-Trac group were prescribed treatment with the splint three times per day for the first four weeks, and as necessary thereafter.
The BWB group were prescribed to wear their splint at night and during activities that provoke symptoms during the first four weeks, and as necessary thereafter. The bend in the aluminium palmar bar was straightened before use. All patients were given a chart to document their usage after week four.
Outcomes
This is a pilot randomised controlled trial allowing assessment of the safety and any side effects of the splints. Our primary clinical outcome was the Levine 11 symptom and function score at eight weeks. The secondary outcomes were Levine symptom and function score at four, 26 and 52 weeks, and Semmes–Weinstein monofilament© scores, grip and pinch strengths, and splint satisfaction visual analogue scale (VAS) scores at four, eight, 26 and 52 weeks. Problems, side effects (to assess splint safety) and compliance were also recorded. Participants hand size and body mass index (BMI) were also measured, and the size of splint used was recorded.
Telephone contact was made with all the participants at two and six weeks, and clinic appointments were conducted in the Pulvertaft Hand Centre at a specially created research clinic at zero, four, eight, 26 and 52 weeks. The phone calls entailed set questions regarding any problems or side effects and took approximately 5 min, and the clinic appointments involved history and clinical examination using a pro forma, and lasted on average 45 min.
The decision to continue with the splint (treatment success), or to proceed to invasive treatment and therefore leave the trial (treatment failure), was at the discretion of the patients.
Sample size
Our sample size was determined by the 25 C-Trac splints donated by Heritage Medical. There was no previous information at the trial commencement about the effectiveness of the C-Trac when compared to BWB to guide the power calculation for the sample size. Therefore, it was conducted as pilot study to assess the safety of the interventions and to collect data on clinical outcomes for planning future definitive research.
Randomisation
Patients were randomised to C-Trac or BWB using sequentially sealed envelopes. Random sequences of block size of 10 were used. The randomisation list was generated using the ClinStat software. Block size were concealed from the research team until completion of the trial.
Blinding
The decision was made not to blind this study, due to it being a Phase 1 clinical trial primarily aimed at assessing the safety and any side effects of the splints. No attempt was made to blind the assessors, as it was felt that this would impede their ability to detect the safety and any side effects of the splints.
Statistical methods
All the statistical analysis was performed using SPSS v16. Statistical analysis was done based on complete cases at each time point. Initial descriptive analysis was done using all the variables of the pilot study. The distribution of the continuous variables was tested using their histograms. Independent T-test or Mann–Whitney U test was performed for comparing the continuous demographics, the Levine scores, pinch, grip, satisfaction scores and sensation scores between the two splint groups. Moreover, the Fisher's Exact test was constructed to test the association between the treatment success rate, the categorical demographics and the two splints.
Registration
The study received backing from the Derby Research and Development Department (DHRD/2006/037) and received ethical approval from the Derbyshire Ethics Committee (06/Q2401/77). The trial's International Standard Randomised Controlled Trial Number is ISRCTN26618585.
Results
Participant flow
Figure 1 illustrates the patient flow through this trial. Five patients were excluded prior to randomisation, as their nerve conduction studies suggested severe CTS. Six patients were excluded following randomisation, one from the C-Trac group and five from the BWB group. The second hand of two bilateral CTS patients was initially included before it was realised that this was impractical. Three patients had other pathology not included in the exclusion criteria but which interfered with their assessment: two patients had had exposure to vibration and symptoms in keeping with vibration white finger, and one patient had a small middle finger laceration. One patient had concomitant cervical spine-related symptoms which had initially been missed. These scenarios and conditions were added to the exclusion criteria. The contra-lateral hand of patients with bilateral CTS was managed in the same way as their study hand.
CONSORT diagram: participant flow over one year, (n = number of patients).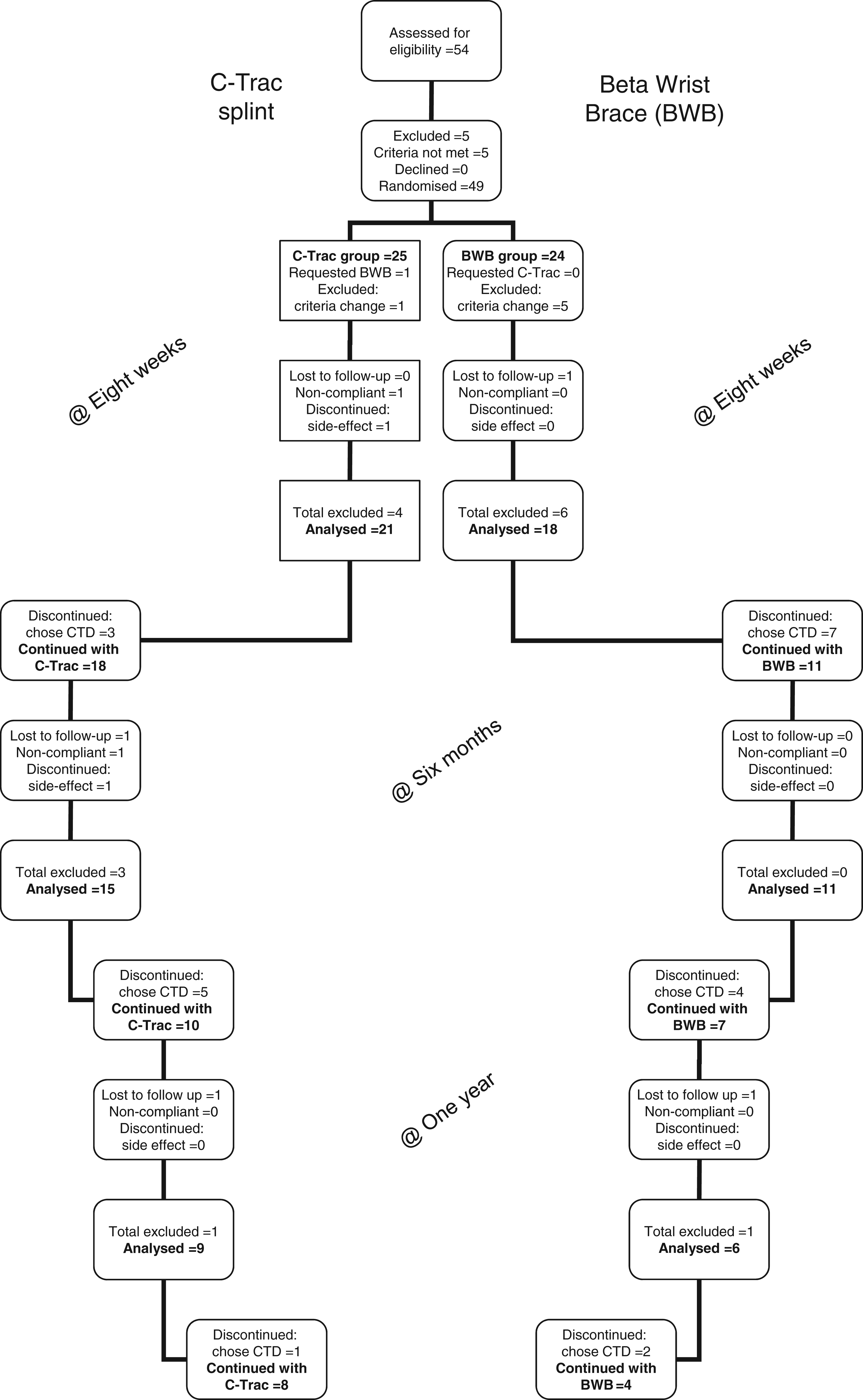
Recruitment
Recruitment to this trial occurred between September 2006 and August 2007, and ended when 25 patients had been randomised to the C-Trac group.
Baseline data
Baseline characteristics of C-Trac and BWB groups.
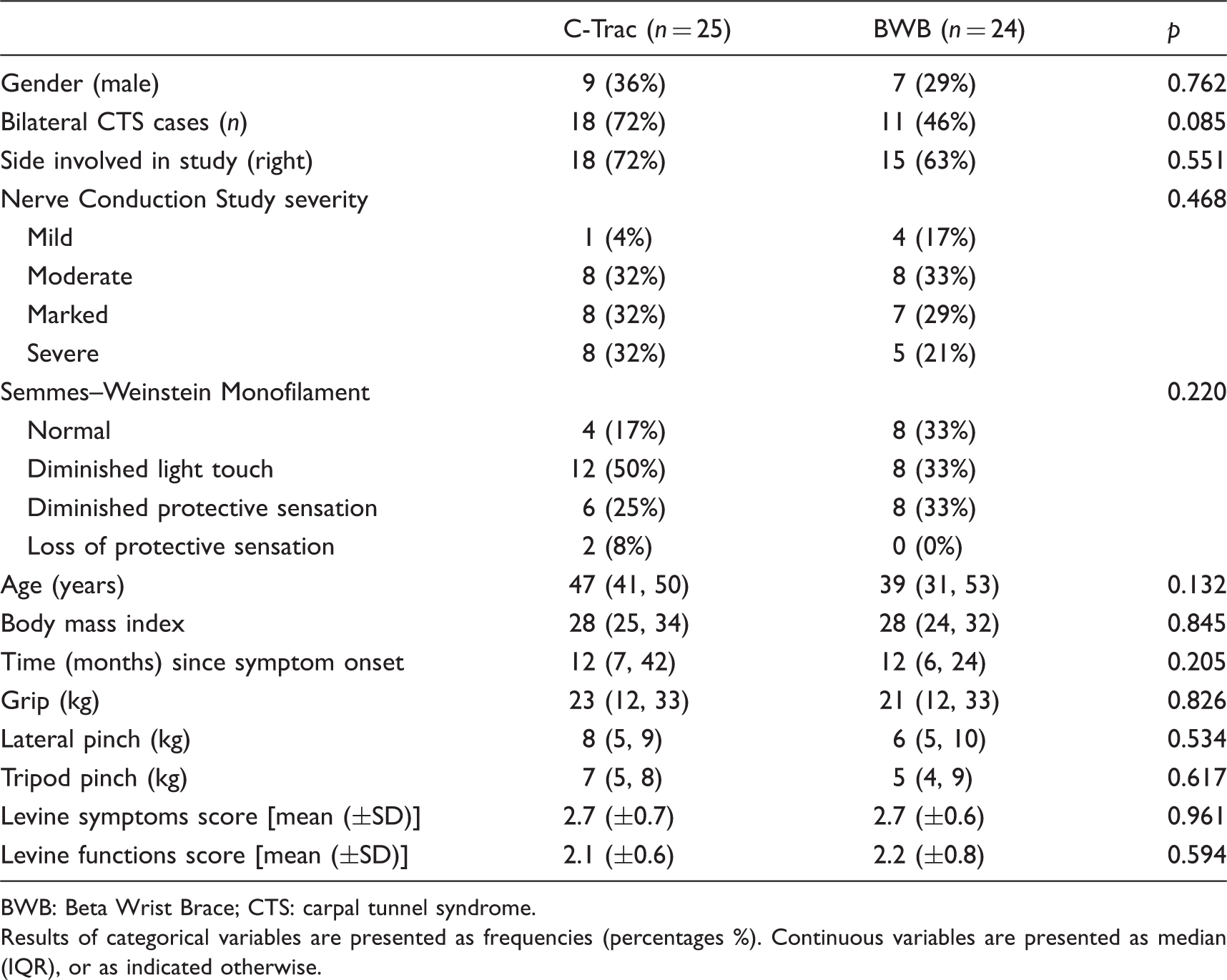
BWB: Beta Wrist Brace; CTS: carpal tunnel syndrome.
Results of categorical variables are presented as frequencies (percentages %). Continuous variables are presented as median (IQR), or as indicated otherwise.
Numbers analysed
Figure 1 shows the numbers of patients that continued with each splint who were analysed at each follow-up time.
By one year, four patients (two in each group) had been lost to follow up, giving a dropout rate of 9.3%.
Harms
During the course of the year, there were two significant side effects possibly attributable to C-Trac splint use: one patient experienced an exacerbation of a quiescent de Quervains tenosynovitis and had therefore discontinued C-Trac use after one week; a second patient developed basal thumb joint pain between weeks four and eight and a radiograph confirmed early basal joint arthritis.
There were three cases of non-compliance in the C-Trac group: one patient decided to stop using the C-Trac after one week as his CTS symptoms had deteriorated; a second patient attended the follow-up clinic at four weeks requesting a BWB; and a third patient had discontinued use of the C-Trac splint by week eight despite clear directions. Two patients were unable to wear the BWB whilst at work, and five patients described this splint as being ‘sweaty’ but continued to use it.
The valves of three of the C-Trac splints failed necessitating splint replacement, and eight of the BWBs were exchanged for new ones.
Outcomes
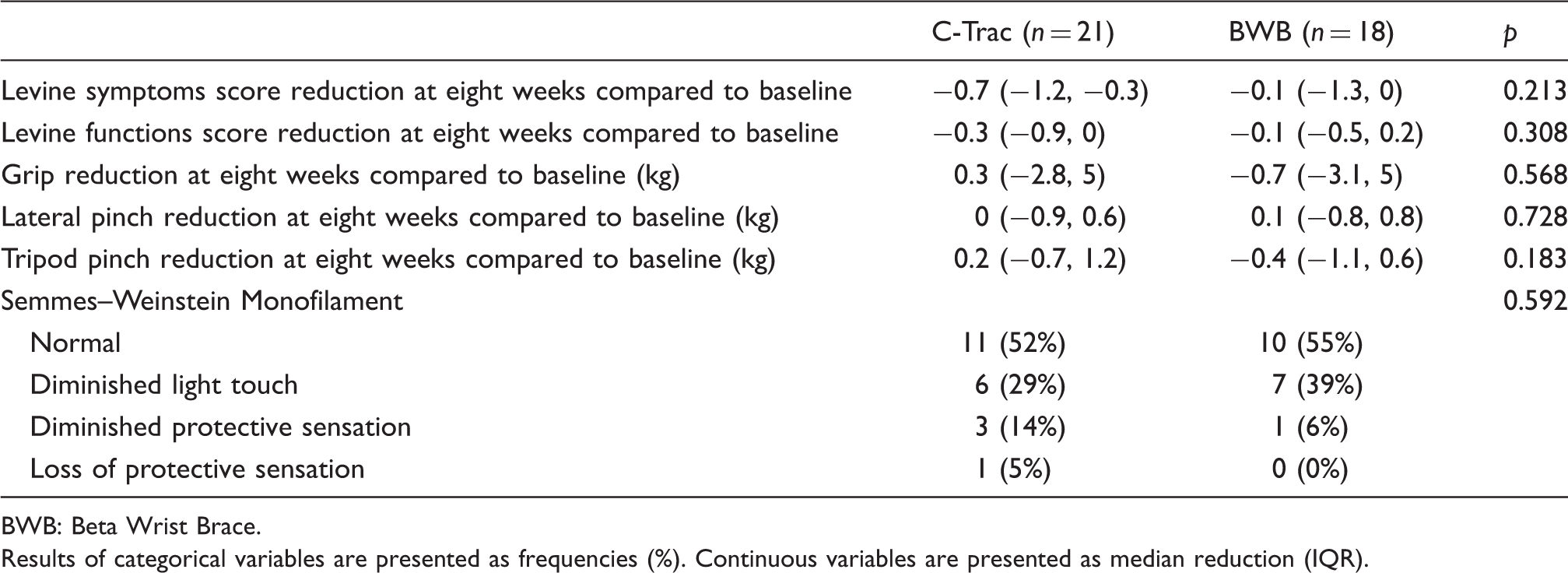
There was no significant difference between the two groups in the primary clinical outcome of Levine symptom and function scores by week eight as illustrated in Table 2 (p = 0.213 and p = 0.308, respectively, n = 39). In terms of the secondary clinical outcomes at week eight, there was no significant difference between the two groups in Semmes–Weinstein monofilament scores (p = 0.567, n = 39); grip and pinch strengths changed little, and there was no significant difference between the two groups (grip strength p = 0.568, lateral pinch p = 0.728, tripod pinch p = 0.183, n = 39); there was no difference in the treatment success rates between the two splints (p = 0.309, n = 39), as illustrated in Table 2; and satisfaction with the splints was also comparable (p = 0.888, n = 39), as shown in Figure 2.
Splint satisfaction (visual analogue scale, VAS) at eight weeks, (n = 39). C-Trac and BWB group outcomes at eight weeks. BWB: Beta Wrist Brace. Results of categorical variables are presented as frequencies (%). Continuous variables are presented as median reduction (IQR).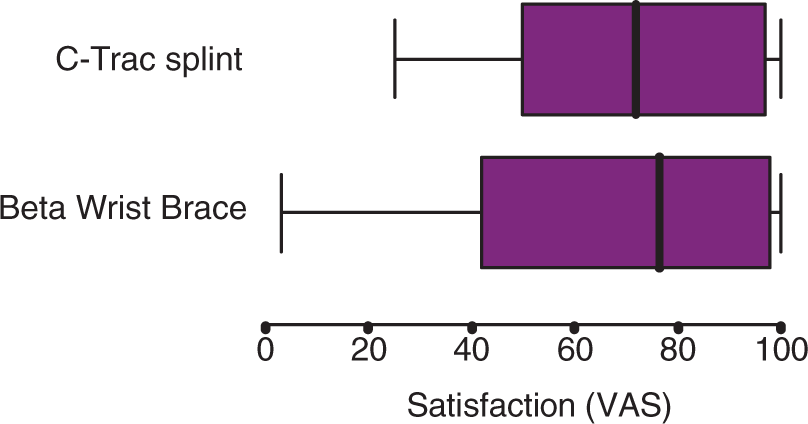
There was no difference in the success and failure rates of the two splints by six months (n = 26, p = 0.873) or one year (n = 15, p = 0.525), Figure 1. Twelve out of 39 patients were successfully managed non-operatively for one year. At one year, eight patients in the C-Trac group elected to continue with their splint to control their CTS compared with four patients in the BWB group. Of these, four patients in the C-Trac group had not recently used their splint compared with one patient in the BWB group.
Discussion
Limitations
The small numbers in this trial increase the likelihood of a Type 2 statistical error. However, the previous non-randomised study 8 concluded that the C-Trac splint obviates the need for CTD. It was on this basis that our pilot study was performed. If C-Trac is as effective as CTD at treating CTS, 8 its effectiveness should be vastly superior to the BWB, and a small study of this nature should therefore have shown a difference between the two splints.
The lack of assessor blinding was also a weakness in this trial, potentially resulting in bias. The large number of exclusions following randomisation was disappointing, but in keeping with a pilot study.
Generalisability
This study was limited to patients between 18 and 65 years of age with mild to moderate idiopathic CTS: no evidence of APB wasting.
Interpretation
CTD surgery exposes patients to an operative intervention with the risks of pillar pain, nerve damage, scar tenderness and reduced grip strength. 12 Surgery will inevitably oblige a patient to take time off work and may intrude on leisure activities. Some patients are reticent to proceed with operative management. CTD in the United Kingdom has a tariff of approximately £600–£800 ($900–$1100) per operation. The C-Trac splint is marketed as offering a solution to these clinical, social and financial issues.6,7
Potential patients requesting use of the splint must be advised of the possible side effects of C-Trac. Its unregulated use is brought into question: at present, it is freely available for purchase without guidance from a clinician. The side effects described in this study perhaps resulted from compression of the first extensor compartment and the basal thumb joint by the C-Trac splint.
The reliability and durability of the C-Trac splint design is also brought into question by the fact that three of the 25 splints used during the one-year study required replacement. There is a cost issue, as it retails at £130 compared with about £10 for the BWB. The C-Trac is more complicated to use than the BWB and requires a degree of intelligence, dexterity and acuity to operate. There is no research published by the manufacturers outlining the rationale for their suggested treatment regime as used in this study.
There will always be patients who do not want to proceed with surgery for a variety of reasons, and given a thorough investigation to exclude the conditions exacerbated by use of the C-Trac splint, we have shown that it is an alternative to the BWB for the non-operative management of idiopathic CTS in patients aged between 18 and 65 years. We have not been able to reproduce the results published by the manufacturers. 8 There is no doubt that several patients in this study were very glad of a splint which did not require constant use, and which for 5 min use three times each day, kept their CTS at bay.
We have decided not to continue with research into the efficacy of the C-Trac splint, but would welcome other groups to confirm or refute the findings of this study.
Footnotes
Funding
Heritage Medical Ltd contributed 25 C-Trac splints to the study, at the then retail cost of £5000.
Conflict of interest
The C-Trac splints were provided by Heritage Medical Limited, the UK Company with the splint manufacturing rights. Beyond providing the splints, Heritage Medical Limited was not in any way involved in the research project.