
Abstract
Introduction
Children with Down syndrome present with joint laxity, hypotonia and shortened hands resulting in reduced grip and pinch strength. Limited information on grip and pinch strength in children with Down syndrome motivated this study.
Methods
A convenience sample of 30 children with Down syndrome (9–16 years) from special schools and 30 age- and gender-matched healthy school children was studied. Grip and pinch strength were measured according to ASHT standard procedure using JAMAR® dynamometer and B&L pinch gauge. Anthropometric data of upper limb and subject characteristics were recorded.
Results
Children with Down syndrome had significantly lower values for grip, palmar and key pinch strength (p < 0.001) (6.3 kg, 1.91 kg, 2.75 kg) compared to healthy children (15.9 kg, 2.86 kg, 3.52 kg), respectively. A positive moderate correlation was observed between right hand grip strength and body height (r = 0.67), bodyweight (r = 0.69), total arm length (r = 0.68), upper arm length (r = 0.68), forearm length (r = 0.63), hand length (r = 0.68) and hand breadth (r = 0.66) in children with Down syndrome.
Conclusions
Children with Down syndrome presented with 60% less grip strength, 33% less palmar pinch strength and 22% less key pinch strength when compared to children without Down syndrome. Positive moderate correlation was observed between grip strength, body height, body weight and upper limb anthropometric variables in children with Down syndrome.
Introduction
The World Health Organization South East Asia has reported an estimated frequency of 1:800 and 34,000 births/year of Down syndrome (DS) in India. 1 DS is characterised by various clinical symptoms including orthopaedic, neurological and cognitive impairments affecting muscular strength. 2 The physical impairments include hypotonia, hyperflexibility of joints, ligamentous laxity, dysplasia of middle-phalanx of fifth finger, short broad hands and single transverse palmar crease. Cognitive impairments include mild-to-moderate mental retardation, attention deficit and mild behavioural problems. Reduced hand grip and pinch strength in children with DS could be due to interaction between various physical and cognitive factors. 3
Hand function comprises prehensile and non-prehensile skilled movements. Prehensile activities require power grip and precision handling; 4 hence, evaluation of grip and pinch strength is an integral component of hand function assessment. Grip and pinch strength are simple clinical tests with a standard protocol and can be done with readily available equipment. Children with DS have impaired grip and pinch strength and are believed to improve with training. Hence, assessment of hand strength is essential to plan goal-oriented therapy and monitor the outcome of therapy.
However, there is limited information on grip and pinch strength in children with DS. Priosti et al. 5 reported an approximately 40% reduction in grip strength and gross dexterity in 7- to 9-year-old children with DS compared to healthy age-matched controls. However, it may not be appropriate to use findings from Brazilian children with DS as reference values for Indian children with DS owing to variations in genetic, anthropometric characteristics, nutritional and environmental factors which influence grip and pinch strength. 6
The present study was conducted in an attempt to explore both power grip and pinch strength in Indian children with DS. The primary aim was to compare grip and pinch strength of children with DS to age- and gender-matched healthy children. Secondary aims were to study the influence of dominance on grip strength and explore association between grip strength and anthropometric variables.
Methods
The study was conducted after obtaining approval from the University ethics committee (MGMUDPTEC; approval number: 2012/IP/03). The nature and purpose of study was explained and consent was obtained from the head of school and parents. Thirty children with DS from two special schools were studied. Children who were unable to follow commands or had any injury to upper extremity or cervical region were excluded. Thirty age- and gender-matched healthy school children were included in control group.
The JAMAR® (Sammons Preston, USA) hand dynamometer and B&L Pinch gauge (PINSCO, Inc.), supplied by ElectroMedical Control, Mumbai, India, were used to measure grip, key pinch and palmar pinch strength and recorded in kilograms. Tip pinch strength was not recorded in children with DS as they were not able to perform the testing position. The JAMAR® hand dynamometer is a valid and reliable tool for measurement of grip strength. 7 The B&L pinch gauge was used to measure key and palmar pinch strength. Grip and pinch strength were recorded according to recommendations of American Society of Hand Therapist described in detail elsewhere. 8
Grip and pinch strength were also recorded in 30 healthy age- and gender-matched children. Demographic data and physical examination of children in both groups were recorded. Hand dominance was selected as per the records maintained in school. All recorded anthropometric measurements were performed by single tester. Measurements were recorded according to methodology described by Singh
9
using weighing scale, sliding caliper and flexible inelastic tape. Bony landmarks identified for measurement were total arm length (measured between acromion and tip of middle finger), upper arm length (measured from acromion along the posterior aspect of arm until acromion), forearm length (measured from medial epicondyle to the ulnar styloid), hand length (measured from distal crease at wrist to the tip of middle finger) and hand breadth (measured from edge of hand on one side, across palm to edge of hand on other side, at level of metacarpophalangeal joints, with fingers parallel and extended) (refer Figure 1). Data were collected over two-month duration by one of the researchers who did not participate in data analyses.
Anthropometric measurements of upper limb: (a) total arm length; (b) upper arm length; (c) forearm length; (d) hand length; and (e) hand breadth.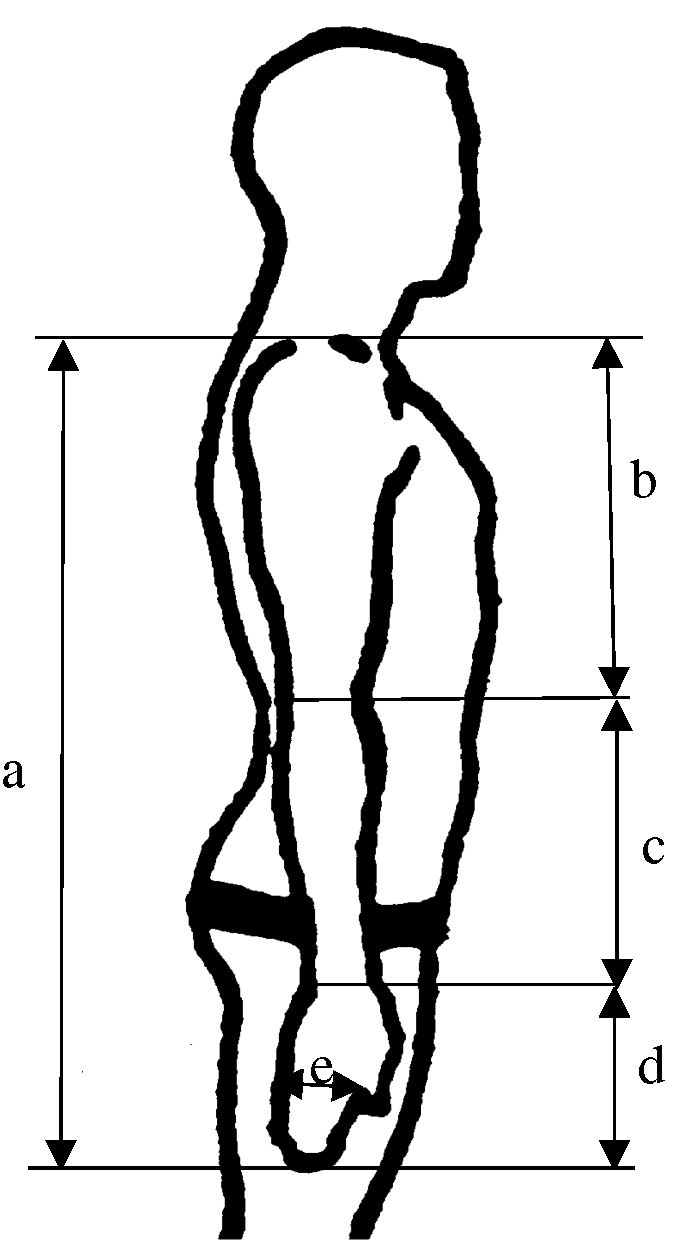
Data were analysed descriptively using SPSS (version 16). Tests for normality (Kolmogorov–Smirnov, Shapiro–Wilk, Histogram and Q–Q plot) were conducted and data fulfilled the assumptions for normal distribution. Unpaired sample t-test was used to compare hand grip and pinch strength between groups (p < 0.05). Independent sample t-test was used to compare hand grip and pinch strength between dominant and non-dominant hands in children with DS (p < 0.001). Data from right hand were used to correlate grip strength with various anthropometric measures (body height, body weight, total arm length, upper arm length, forearm length, hand length and hand breadth) using Pearson’s correlation coefficients.
Results
Demographic data.
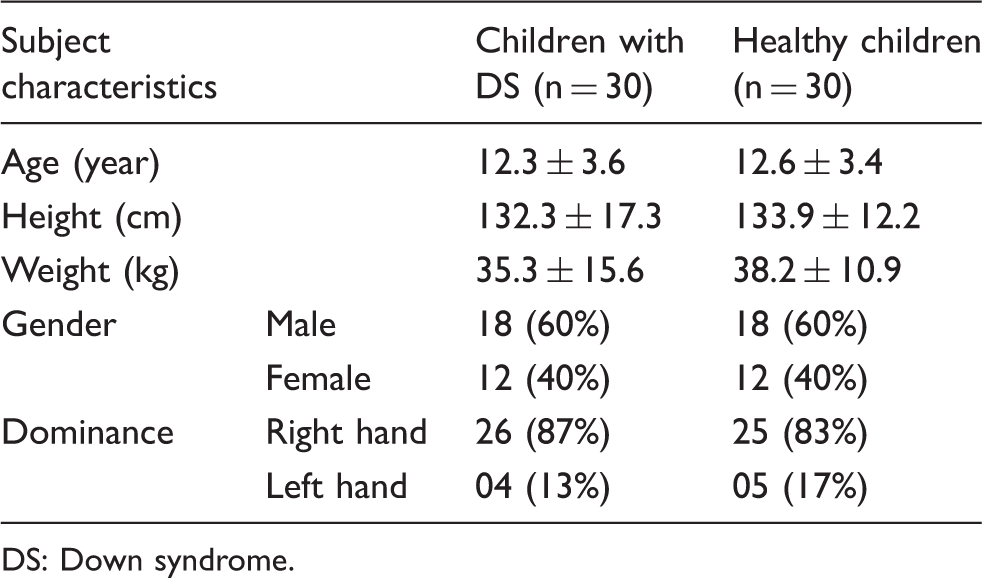
DS: Down syndrome.
Comparison of grip and pinch strength in children with DS (n = 30) and healthy children (n = 30).
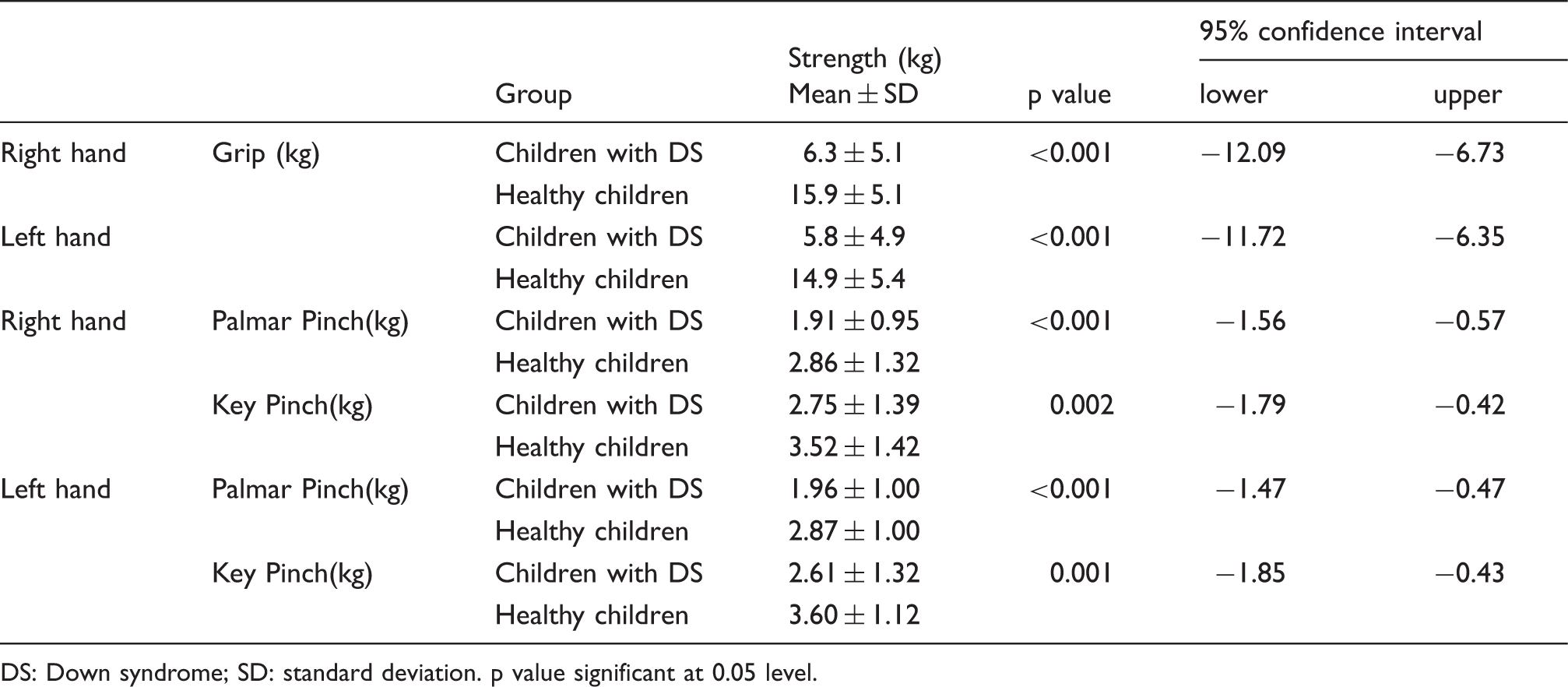
DS: Down syndrome; SD: standard deviation. p value significant at 0.05 level.
Comparison of dominant and non-dominant hand grip and pinch strength in children with DS.
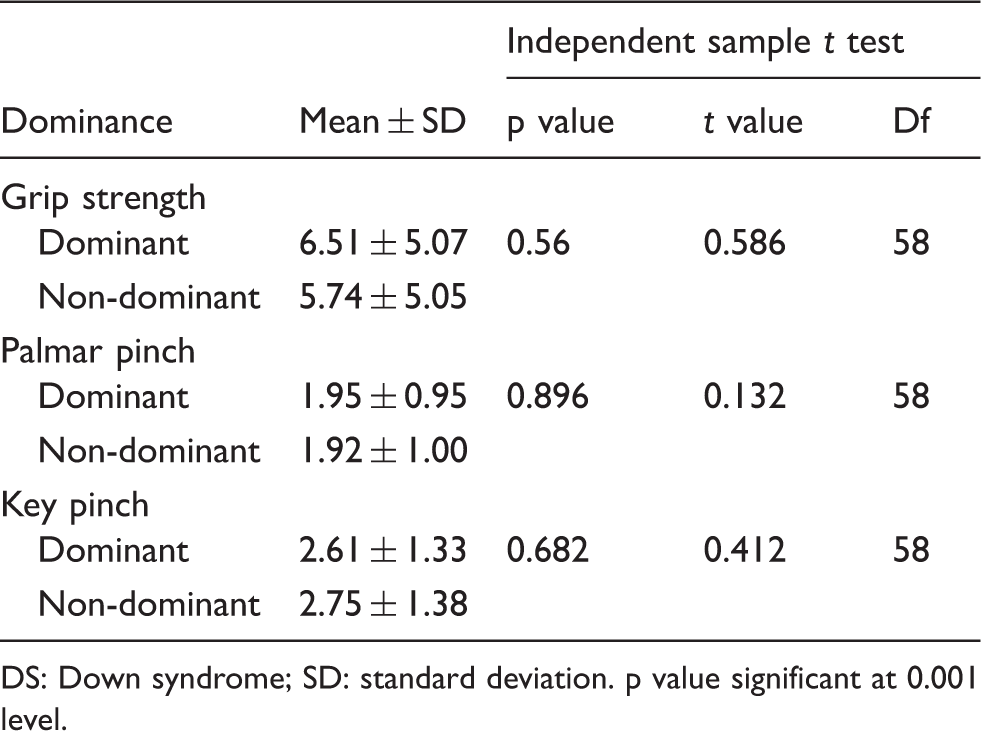
DS: Down syndrome; SD: standard deviation. p value significant at 0.001 level.
Pearson correlation coefficient of grip strength with anthropometric variables.
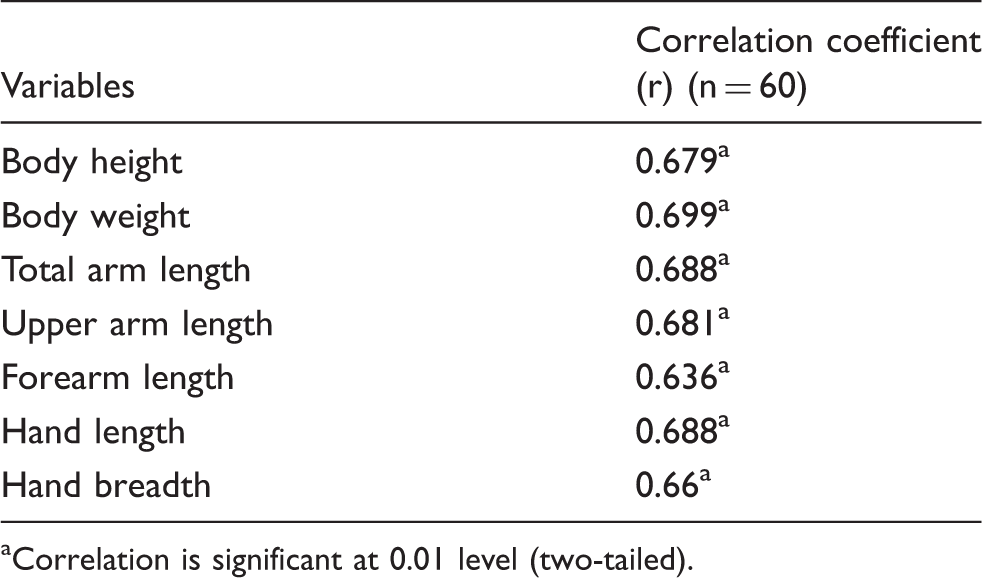
Correlation is significant at 0.01 level (two-tailed).
Discussion
Children with DS presented with less grip and pinch strength compared to healthy children in both hands. Right hand grip, palmar and key pinch strength in children with DS was less by 60%, 33% and 22%, respectively, compared to controls. Similarly, grip, palmar and key pinch strength of left hand was less by 60%, 32% and 28%, respectively, in children with DS. Present findings agree with a previous study by Priosti et al. 5
Children with DS presented with more than half reduction in grip strength, one-third reduction in palmar pinch and slightly less than one-third in key pinch strength compared to healthy. It needs to be emphasised that children in our study were trained regularly at special schools but despite therapy they demonstrated less hand grip and pinch strength. Children with DS who are not trained for hand functions are speculated to present with still lesser grip and pinch strength.
Grip and pinch strength are influenced by generic factors such as age, gender, anthropometric characteristics, nutritional status and socio economic status. 6 In addition to these factors, children with DS present with hypotonia, hyper-flexibility of joints and ligamentous laxity which can reduce muscle strength and effectively hand grip strength. Additionally, it is known that grip strength reduces with hypermobility owing to abnormal proprioceptive acuity. 10
However, grip and pinch strength did not vary between dominant and non-dominant hand probably because children of this age group are most likely using both their hands equally for self-grooming and play bimanually. Children with DS assume atypical grip using fewer fingers and hyperextending them while gripping objects, leading to reduced grip and pinch strength from altered biomechanics. 11 It is speculated that optimal lever arm and length tension relationship of contracting muscles are crucial for efficient force production. This relation is altered in DS as finger flexors are stretched rather than shortened due to hyperextension, therefore not able to produce maximal force.
Anthropometric variables such as body height, body weight, arm and forearm length and hand length and breadth are known to have a direct association with grip and pinch strength. 12 We observed moderate correlation between grip strength and all anthropometric variables. It is speculated that no single variable emerged with strong association because DS affects the normal growth pattern of the whole appendicular skeleton, leading to short stature and hands. 13
Studies across various countries including India have explored the association of grip strength with relevant anthropometric variables in healthy population.12,14–16 The authors of the present study have also reported positive correlation between grip and upper limb anthropometric variables in; healthy Indian population. 17
Our findings provide information on hand strength in children with DS in India. As children with DS respond positively to training,18,19 it is important to include grip and pinch strength training in routine rehabilitation along with conventional exercise therapy. Our findings will also help to monitor outcome of rehabilitation in case of injury to upper limb in children with DS.
In addition to attempts to improve hand function in a clinical setting, these results indicate a need to incorporate therapeutic measures to improve grip and pinch strength both at school and at home to improve overall performance of children with DS. It may not be unreasonable to speculate that children with DS may perform better in fine hand activities such as writing, drawing and other fine activities of hand as a result of grip and pinch strength training.
However, further studies are necessary with a larger sample and long-term follow-up after implementation of exclusively designed exercise program for improving hand function to allow exploration of positive effects of training.
Limitations of study
Various biological age groups within paediatric population were not studied exclusively and data for grip and pinch strength were not compared gender wise.
Conclusions
Children with DS presented 60% less grip strength, 33% less palmar pinch strength and 22% less key pinch strength compared to children without DS. Positive moderate correlations were observed between grip strength, body height, body weight and upper limb anthropometric variables (total arm length, upper arm length, forearm length, hand length and hand breadth) in children with DS.
Footnotes
Acknowledgement
The authors thank all their volunteers for their co-operation and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no external financial support for the research, authorship, and/or publication of this article.