
Abstract
Introduction
The aim of this study was to compare hand impairment and function in a cohort of patients with rheumatoid arthritis and matched healthy participants.
Methods
A matched case comparison research design comparing hand impairment and functional ability between patients with rheumatoid arthritis and healthy participants (males or females, aged ≥ 50 years). Functional ability was assessed using the Michigan Hand Questionnaire, power and pinch grip strength and the nine-hole peg test.
Results
A total of 100 participants (50 patients with rheumatoid arthritis and 50 matched healthy participants) were recruited. Patients with rheumatoid arthritis reported significantly lower overall hand function, activities of daily living, work, aesthetics, satisfaction (p < 0.001) and significantly higher pain scores when compared with healthy controls. The patients with rheumatoid arthritis had significantly lower maximum power and pinch grip strength in both left and right hands (p < 0.001) when compared with healthy controls. The rheumatoid arthritis group took significantly longer to complete the nine-hole peg test using both right and left hands compared with healthy controls (p < 0.001, respectively). Additionally, in rheumatoid arthritis patients, a significant moderate, positive correlation between power grip strength and activities of daily living (r = 0.584, n = 50, p < 0.01) and a weak-to-moderate, significant negative correlation between power grip strength and pain (r = −0.314, n = 50, p < 0.05) were reported.
Conclusion
Despite the recent substantial improvement of drug therapy and disease control, the functional impact of rheumatoid arthritis on hand pain and function remains significant.
Introduction
Rheumatoid arthritis (RA) is a chronic, systemic autoimmune disease characterised by associated inflammatory processes; 1 however, the disease pathogenesis remains unclear. Clinical diagnosis of RA requires a minimum of four of the following criteria: morning stiffness, arthritis of ≥3 joint areas, arthritis of hand joints, symmetric arthritis, rheumatoid nodules, positive rheumatoid factor test, and radiographic changes. 2 Incidence rates of RA in the UK are 54/100,000 for women and 25/100,000 for men 3 with symptoms including declining functional hand ability, increased pain, and often a reduced quality of life.4,5 In RA, controlling joint inflammation early with the aggressive use of disease modifying anti rheumatic drugs (DMARDs) and biological agents is advocated and has led to substantial improvements in control of disease activity and resulting structural damage. 6 Despite the routine use of DMARDs and biological agents in recent times, RA patients nevertheless endure declining functional ability and subsequent impact on their quality of life and ability to work.6,7
Hand function is essential for daily living and contributes to individuals’ quality of life, with successful participation in activities requiring accurate sensory input and interaction of anatomical and physiological characteristics. It has been demonstrated that function, grip strength and dexterity decline with age in and between healthy and RA populations8–11 and vary significantly between males and females.12,13 In RA, disease duration has been shown to have a significant negative association with grip strength 11 and hand stiffness. 14 With analysis of current cohorts of people with RA, it is evident that hand pain and activity limitation remain a significant problem. 15
A variety of valid and reliable measures have been developed for assessing hand impairment and function for patients with RA. These range from self-reported questionnaires (e.g. Michigan Hand Outcomes Questionnaire (MHQ), 16 and Disabilities of the Arm, Shoulder and Hand Questionnaire (DASH) 17 to ‘objective’ clinical tests (e.g hand grip strength, Grip Ability Test (GAT), arthritis hand function test and the nine-hole peg test (9HPT).18–20
What is not clear from the literature is what the differences are between healthy and RA populations for both self-reported and objective measurements of hand impairment and function when accounting for age and gender. An opportunity arose to analyse this with the collection and publication of a comprehensive set of contemporaneous self-reported and objective measurements. These hand function data measurements were known to be robust having been collected using standard operating procedures and checked by clinical trial quality assurance procedures for a cohort of patients with RA in the UK within a recent large-scale randomised controlled trial – the Strengthening And stretching for Rheumatoid Arthritis of the Hand (SARAH) trial. 21
This present study aimed to recruit healthy participants matched on age and gender to the SARAH trial cohort of patients with RA in order to: (i) compare hand impairment and function using standardised outcome measures and standard operating procedures; and (ii) examine the association between power grip strength and both pain and activities of daily living (ADL) as assessed by the MHQ.
Methods
A matched case comparison research design comparing hand impairment and functional ability between patients with RA recruited onto the SARAH trial 21 and healthy participants was employed. Based on the findings of Fraser et al. 22 comparing grip strength between RA and healthy individuals, a sample size calculation was conducted using the difference in grip strength between RA and healthy controls. It was calculated that 50 healthy controls would provide >80% power to detect statistical significance at p < 0.05, with a medium effect size of 0.40.
Recruitment and selection of healthy participants
Healthy participants were included in this study if they were males or females, aged ≥ 50 years and could be matched to SARAH participants on age (±2 years) and gender. Potential participants were excluded if they had a history of any rheumatological conditions, oesteoarthritis of the hand, previous hand surgery, or self-reported reduction in functional hand ability/pain. Potential participants were opportunistically recruited (posters/promotional stand) at three community and leisure centres in the South West and South East of England. In addition, a study information and recruitment email to the staff at Faculty of Health Sciences at University of Southampton was sent. All participants received written information about the study, and were given time to think about and discuss their involvement with family before agreeing to take part. Data collection occurred at one of the three recruiting centres.
Recruitment and selection of RA comparison cohort data
The RA comparison cohort was obtained from the SARAH trial database (ISRCTN 89936343:REC reference 08/H0606/47). 21 The SARAH trial was a pragmatic, randomised controlled trial involving 490 participants, aiming to evaluate the effectiveness of an individually tailored progressive hand and arm exercise programme, in addition to best practice usual care. RA patients were included in the SARAH study having met the American College of Rheumatology clinical and immunological criteria, 2 in addition to reporting active pain and dysfunction of hands, were either not on a DMARD regimen, or had been on a stable DMARD regimen for three months or more. 21 A data sharing agreement was completed between the sponsors of the two studies (Universities of Warwick and Oxford) and data were transferred via encrypted electronic transfer. The database was visually checked to identify all complete outcome measure data-sets. All incomplete data-sets were excluded from analysis. RA data-sets were randomly assigned to healthy participants using a set formula “=rand()” in Microsoft Excel, for which the lowest calculated number was used to select the RA patient. If multiple healthy participants were of the same age, previously matched RA patients were excluded from subsequent matching.
Data collection tools
Standardised operating procedures from the SARAH trial were followed for all data collection on matched healthy controls. 23 All participants provided written informed consent and full ethical approval (Ref:12600/14.10.2014) was obtained for all data collection. Functional hand ability was assessed using the MHQ, power and pinch grip strength, and a commercially bought wooden 9HPT using standardised assessment procedures that matched those for the SARAH trial.
Michigan Hand Outcomes Questionnaire
The MHQ is a reliable, validated and responsive self-reported questionnaire of RA patients’ perceptions of hand function.24–26 It is relatively quick to complete (approximately 10 min); however, assessor burden for scoring is considerably greater. 16 Thirty-seven questions of ordinal scale rating (1–5) evaluate six categories: overall hand function, activities of daily living (ADL), work performance, pain, aesthetics, and satisfaction with hand function. Additionally, an overall summary score of hand function is calculated based on all six categories. Responses are scored in line with the standardised MHQ algorithm to provide quantitative data; 27 all responses, except pain are scored positively. In brief, responses were added from each question and each category score was normalised to a scale ranging from 0 to 100. A high pain scale score indicates greater pain experienced; however in contrast, higher scores in the five remaining scales represent better hand performance.
Grip strength
Power and pinch grip strength were measured in Newton’s of force (N) using a recently calibrated MIE Digital Grip Analyser (MIE Medical Research Ltd, Leeds, UK). The MIE digital grip analyser is a reliable, valid and responsive measure of grip strength in an RA population. 28 Measurements were conducted using a standard operating procedure with participants positioned in a straight backed chair (without armrests) with feet flat on the floor, arms unsupported with shoulder in adduction (neutral), elbow flexed, forearm neutral and wrist 0–30° dorsiflexion and 0–15° ulnar deviation. 29 Starting with the dominant hand, three consecutive efforts of power and three-point pinch grip were completed; a rest period of 60 s between consecutive measurements was given to limit effect of fatigue. 30
Dexterity
Hand dexterity was assessed using a commercially bought 9HPT, a timed measure of dexterity and fine motor control, and was conducted using a square wooden board with nine wooden round pegs.18,31 As per standardised instructions, starting with their dominant hand, participants were required to insert and remove all nine pegs from the wooden board as quickly as possible.
All outcome measures used have been shown to be valid and reliable in an RA population. A pilot study was conducted to assess intra-rater reliability for the collection of healthy participant data and involved a single tester assessing seven healthy students (aged ≥ 18 years) from the Faculty of Health Sciences, University of Southampton. Students were required to complete testing on two occasions, separated by 4–7 days. The test–retest reliability of power and pinch grip strength, and 9HPT was assessed using 95% limits of agreement (LOA). The LOA for power grip for the left and right hand was 1 ± 41 N and −1 ± 30 N, respectively. The LOA for pinch grip for the left hand was −5 ± 9 N and the right hand was −2 ± 14 N. For the 9HPT, LOA for the left hand was 1 ± 2 s and right hand was 0 ± 3 s. These were deemed to be within acceptable reliability ranges for data collection. The data collection procedures for the SARAH patient trial did not report individual reliability testing of the 48 assessors, due to practical geographical limitations of a national multi-centre trial. This is not unusual for a UK study; however, standard operating procedures and quality assessment checks were conducted on all SARAH assessors throughout the trial.
Data analysis
Data were analysed for the healthy participants using SPSS version 22 statistical software (IBM SPSS Statistics for Windows, Version 22.0, IBM Corp, Armonk, NY). Histograms were plotted to visually assess data distribution. If data were normally distributed a paired t-test was used to compare MHQ, grip strength and dexterity between RA and healthy groups, while a Wilcoxon signed rank test was used if data were not normally distributed. Pearson’s correlation was used for normally distributed data to assess the relationship between MHQ and grip strength in the RA group. If data were not normally distributed, a Spearman’s rank correlation was used to assess these associations. Statistical significance was set a priori at p < 0.05.
Results
Baseline characteristics of rheumatoid arthritis and healthy control groups.
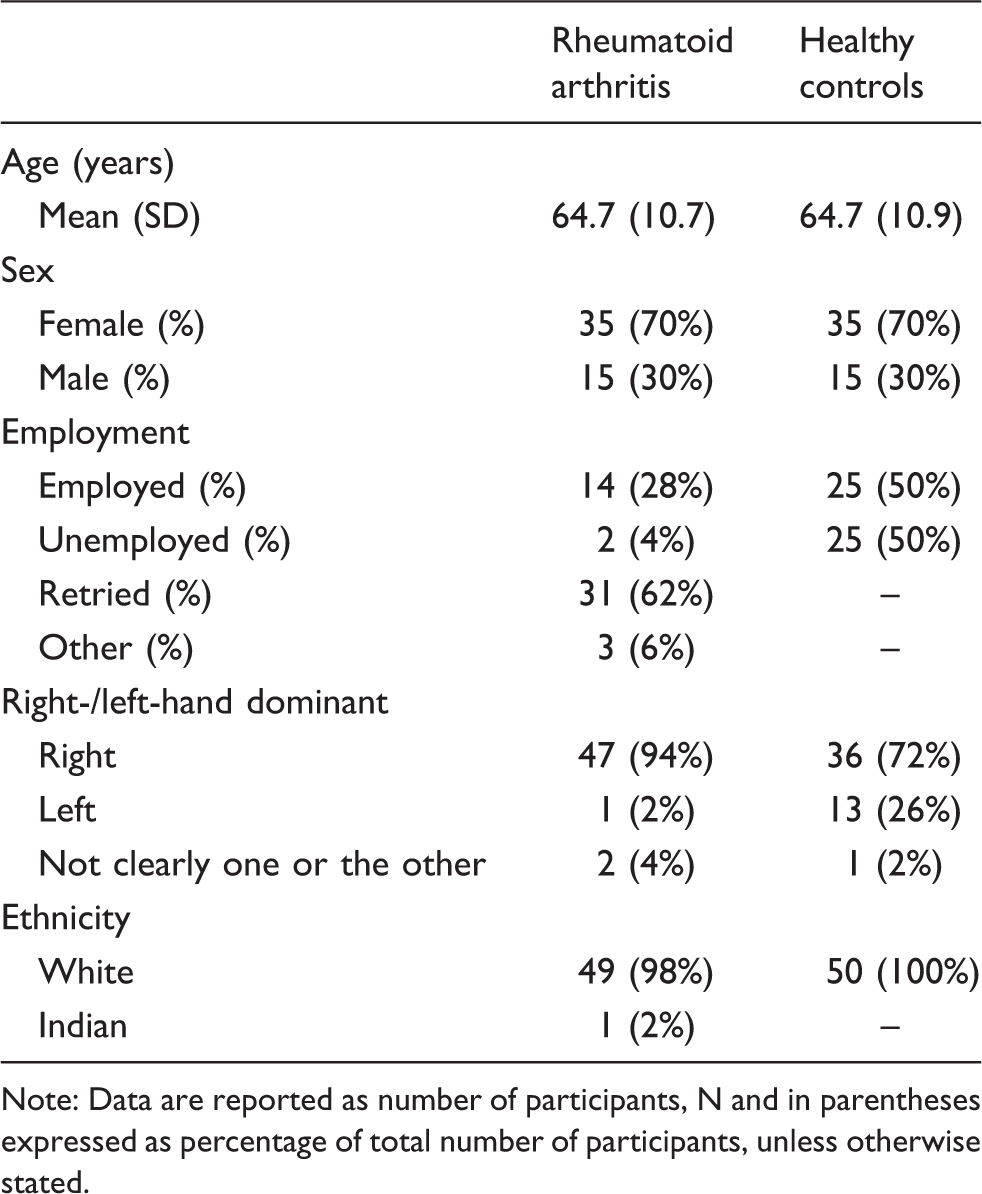
Note: Data are reported as number of participants, N and in parentheses expressed as percentage of total number of participants, unless otherwise stated.
Characteristics of healthy participants
Sixty-two healthy controls volunteered to participate in the study, 50 healthy participants (15 males and 35 females) were recruited and 50 patients with RA matched (15 males and 35 females). Eight healthy participants were excluded from the study. Four emailed/telephoned and were not suitable due to Dupuytren’s contracture and previous hand/finger fractures with associated impact on functional hand ability, four were screened verbally/visually and excluded due to cervical radiculopathy with associated impact on functional hand ability, fixed finger(s) due to previous fracture, Heberden’s nodes with associated pain. A further four withdrew due to availability.
Characteristics of the RA comparison cohort
The RA comparison cohort identified from the SARAH database had a mean disease duration of 15.0 ± 12.8 years. Drug history for RA patients was inconsistently reported across all drug subgroups; however, 26 participants consistently reported using Non-Steroidal Anti Inflammatory Drugs (NSAIDs, n = 10), DMARDs (n = 22), oral corticosteroids (n = 3) and biologic anti-tumour necrosis factor drugs (n = 2). However, all 50 RA patients consistently reported other drug history, with other medications (n = 36), extra NSAIDs (n = 2), steroid tablets (n = 2) and steroid injection into joint (site not specified) (n = 1).
Self-reported hand function (MHQ)
Group mean and median responses for MHQ, grip strength and dexterity for both the rheumatoid arthritis and healthy controls groups.
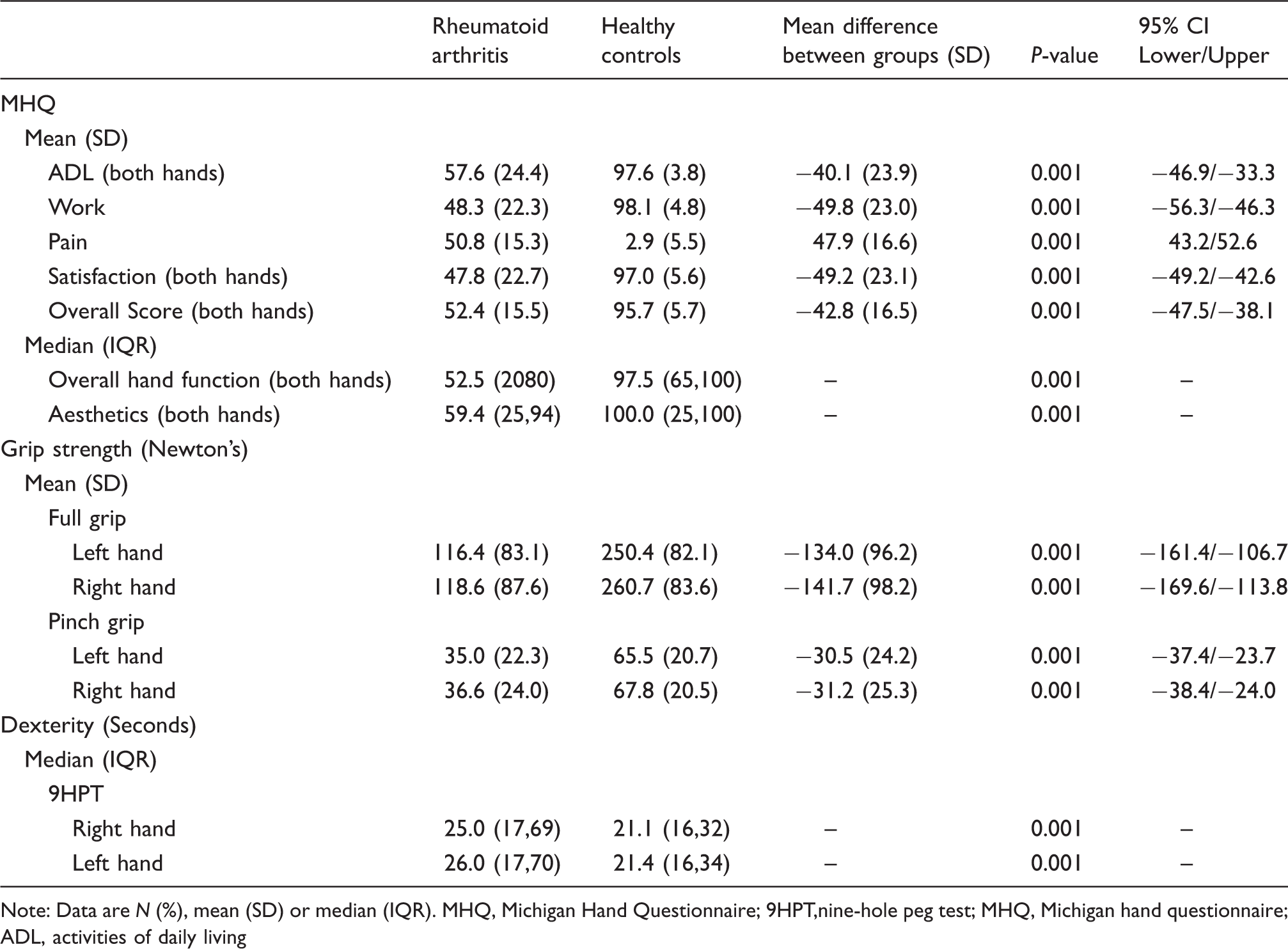
Note: Data are N (%), mean (SD) or median (IQR). MHQ, Michigan Hand Questionnaire; 9HPT,nine-hole peg test; MHQ, Michigan hand questionnaire; ADL, activities of daily living
Therapist measured outcomes (grip strength and dexterity)
The mean maximum power grip strength for the RA group was significantly lower in both the left (mean difference = −134.0 ± 96.2 N, p < 0.001) and right hands (mean difference = −141.7 ± 98.2 N, p < 0.001) when compared with healthy controls. The RA group also demonstrated significantly lower mean maximum pinch grip strength in both the left (mean difference = −30.5 ± 24.2 N, p < 0.001) and right hands (mean difference = −31.2 ± 25.3 N, p < 0.001) when compared with healthy controls. The time taken to complete the 9HPT with both the right and left hand was significantly longer (indicating worse function) in the RA group compared with healthy controls (z = −4.287, p < 0.001 and z = −4.923, p < 0.001, respectively).
Correlations
Spearman’s rank correlation revealed a significant moderate, positive correlation between power grip strength (right hand) and ADL (r = 0.584, n = 50, p < 0.01) in the RA group. The results of the present study also demonstrated a weak to moderate, significant negative correlation between power grip strength (right hand) and pain (r = −0.314, n = 50, p < 0.05) in the RA group (Figure 1).
(a) Individual participant values for grip strength and ADL in RA patients, with a line of best fit (r = 0.584, p < 0.01). (b) Individidual subject values for grip strength and pain in RA patients, with a line of best fit (r = −0.314, p < 0.05).
Discussion
This study is the first to compare a contemporaneous UK cohort of RA patients referred to hand therapists for hand treatment with age- and gender-matched healthy controls. We have reported that despite patients with RA being classified as medically stable, they demonstrated lower hand performance compared to healthy controls across all outcomes measures. This is one of few studies to show that RA patients have an overall lower hand performance across all domains, which encompass measurement of both objective and subjective patient-reported outcomes.
In the current study, power and pinch grip strength was 50% lower in the patients with RA compared with healthy age- and gender-matched controls, suggesting that inflammatory pathology reduces grip strength. Our results also indicate that the lower grip strength observed in RA is independent of the aging process and occurs at a greater rate of decline than natural aging. This is supported by previous evidence showing significantly lower grip strengths in patients with RA when compared with a population of similar age, and age-matched healthy controls.11,32
However, in interpreting our results, we acknowledge limits in the conclusions that can be drawn from this small RA study sample of n = 50. The RA study sample randomly selected from the SARAH trial included only two participants (4%) receiving anti-TNF biological therapy. This was not representative of the total SARAH population where 21% were receiving anti-TNF biological therapy. This differential could impact on the results in two opposing ways. First, if people recruited with stable disease into the SARAH trial had not fulfilled criteria to have been prescribed biological therapy, then our SARAH-matched sample could represent the most able of the SARAH population or conversely this matched sample could represent the least able if individuals were experiencing symptoms that had not been triaged yet to receive biological therapy. Whichever the case, it should be noted that the SARAH sample randomly selected for this analysis differed from the SARAH population in terms of biological therapy received. Although it should also be noted that another recent study examining the one-year impact of RA on hand function for people who also received biological therapy also indicated that ongoing hand pain and hand dysfunction were identified in spite of optimal drug management. 15
So whilst our data suggest that in the RA population current drugs are not effective at retaining and/or restoring hand function as patients continue to demonstrate significant functional problems, we acknowledge that the sample recruited differed on this variable from the SARAH trial population.
The lower grip strength seen in RA individuals is a likely consequence of multiple factors32,33 and despite many of these factors being evident within normal aging, the reduction seen within RA exceeds that seen in age- and gender-matched counterparts. The same argument can be applied to hand dexterity, where our data suggest that there is a reduction in speed and accuracy of fine motor hand function that is independent of the aging process. This is supported by previous findings that show RA patients have hand grip and global upper limb weakness, in addition to proprioceptive deficits. 33 In addition to handgrip differences, lower overall hand performance (as assessed by the MHQ) was observed in the RA sample, compared to healthy controls. Despite previous findings that hand performance decreases with age, 8 in RA these characteristics are affected to a greater extent than aging alone.
Limitations
Our study is not without limitations. Screening of the healthy controls for symptoms of hand osteoarthritis was done verbally and visually by a physiotherapy student and novice researcher and the use of more clinically robust measures may have benefitted this study. In the SARAH trial, there was no recording of affected hand(s) of participants, and so it was therefore assumed that both hands were affected. Consequently, it was not possible to analyse differences in relation to hand dominance and affected hand(s) due to the inability to identify if one or both hands were affected. Therefore, analysis for correlations was completed using power grip (right hand) as 94% of the group were right-hand dominant. Cross-sectional cohort studies can only provide a clinical picture at a single point in time, and fail to identify a wider clinical picture on progression over time and its relationship with baseline measurements. The full discrimination ability of the MHQ is not fully documented for RA populations, and for a healthy population it is unknown whether ceiling effects in this patient-reported outcome could have impacted on findings.
Future longitudinal research, e.g. one-year follow-up, of these groups would provide further insight and we would recommend studies that attempt to recruit a more ethnically diverse population to widen the generalisability of findings.
Conclusions
Grip strength, hand dexterity, and function can be reduced by up to 50% for patients with RA. Furthermore, reductions in grip strength, hand dexterity and function for this sample of people with RA is greater than can be expected from the ageing process alone. In spite of improvements in drug therapy and disease control, the functional impact of RA remains significant in terms of hand pain and function when compared to age- and gender-matched controls.
Footnotes
Acknowledgement
We would like to thank both the SARAH trial participants and the healthy participants for taking part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SARAH Trial was funded by NIHR HTA (grant no. HTA – 07/32/05).