
Abstract
Introduction
The purpose of this study was to evaluate a newly developed trapeziectomy rehabilitation protocol. Variability in trapeziectomy rehabilitation protocols and the arrival of new surgeons in our hospital required a uniform protocol.
Methods
Fifty hands in 44 patients (32 women/12 men) were immobilised for 4 weeks in a plaster cast after a trapeziectomy. A carpometacarpal splint immediately followed for 2 weeks, taken off for exercises and self-care. Patients were assessed preoperatively and at 3, 6 and 12 months using: a pain visual analogue scale (VAS), grip, tip pinch and lateral pinch strength, goniometry, the Modified Kapandji Index (MKI), the Quick Disabilities of the Arm, Shoulder and Hand questionnaire (Q-DASH, Dutch version) and the Short Form 36 (SF-36, Dutch version). At 3, 6 and 12 months, patient’s satisfaction with the operation was rated on a satisfaction VAS.
Results
The correlation between pain and patient satisfaction was significant (ρ = −0.80). VAS pain improved from a median of 75 mm preoperatively to 20 mm at 12 months (p < 0.01). The Q-DASH improved from a median of 48 preoperatively to 20 at 12 months (p < 0.01). Median grip, tip pinch and lateral pinch strength increased at 12 months by 19%, 8% and 24%, respectively from the baseline measurement.
Conclusions
Patients participating in a standardised protocol after trapeziectomy with 4 weeks immobilisation demonstrated improvements in pain, Q-DASH, grip strength, tip pinch and lateral pinch grip. They were satisfied with the results. Further research into the optimal immobilisation time after trapeziectomy surgery is needed.
Introduction
The pathogenesis of osteoarthritis (OA) remains elusive although it is predominantly believed to occur spontaneously. 1 OA can be painful and greatly impair hand function.1–4 OA symptoms in the first carpometacarpal (CMC I) joint often starts to show from about 50–60 years in both men and women. A younger onset of CMC I OA can also be observed due mainly to generalised ligamentous laxity and joint hypermobility.1–5 There are occasional causal factors leading to CMC I OA, for example infection, trauma, Rolando or Bennett’s fractures or repetitive use injuries resulting from work-related mechanical loading.6,7 Instability with subsequent CMC I OA has a higher incidence rate in women compared to men. 8 This is thought to be due to a more shallow and less congruent trapezium bone form covered with a thinner layer of cartilage.9,10 In addition, hormonal changes may also increase the incidence of OA with a prevalence of OA found in 33% of postmenopausal women. 3
The CMC I joint surfaces have most contact with each other during opposition when it is stable and tightly congruous.8,11 Large forces are transmitted through the thumb during pinching, which is an essential grip for many daily activities. 12 Progression of OA degenerating the CMC I joint can lead to deformity of the thumb, resulting in subluxation of the first metacarpal (MC I).2,8 As the MC I subluxes, the web space reduces and the metacarpophalangeal (MCP I) thumb joint begins to hyperextend.8,11 The increased mechanical instability reduces joint surface contact. Subsequently, compressive shear forces can over time result in trapeziometacarpal joint OA. 13
Pain and resulting loss of function are the main reasons patients with CMC I OA seek treatment.1,6 Initially, conservative interventions are usually offered which include painkillers, steroid or hyaluronidase injections, functional aids, splints and hand therapy.1,8 Once conservative treatments have been exhausted surgery may be proposed. Surgical techniques for this condition vary, including: trapeziectomy alone, trapeziectomy with ligament reconstruction and tendon interposition (LRTI), arthrodesis or joint replacement. None of these techniques appear superior based on comparative outcome measures.6,7,14,15
Various arguments have been given for the use of immobilisation, for example: cast immobilisation has been used as a method to prevent loss in trapezial height following a trapeziectomy. Lins et al. 16 and Downing and Davis 17 have questioned concerns of thumb height loss. Although height may be lost due to a trapeziectomy, it may not lead to poorer patient outcomes.14,16,17 It has been suggested the only reason for longer immobilisation is to protect the capsular closure. 18 Horlock and Belcher 19 however, stated that splintage might have been introduced to prevent reoccurrence of a thumb adduction contracture. In their study no extra benefits for prolonged splintage for a trapeziectomy were found. It has been argued that a longer splintage time after a trapeziectomy is neither necessary nor desirable as it is recognised that this can cause stiffness.18,19
Immobilisation times and methods of postoperative treatment after CMC I surgery vary greatly. A lack of agreement was found in studies that describe the period of immobilisation after an operation for CMC I OA: cast removal at 1 week and a splint fitted, which was to be removed for regular mobilising; 5 weeks in a plaster of Paris then start exercises; immobilisation in a cast and splint for a total of 6 weeks before mobilising.18–21 In a systematic review carried out by Li et al., 14 immobilisation practices differed between randomised controlled trials. The options included immediate mobilisation, support in a soft bandage or immobilisation in a thumb cast or splint. 21 In the study by Belcher and Nicholl 18 patients were immobilised for 2 weeks, then wore a splint until 6 weeks. Early mobilisation (1 week) has been found to be more convenient and comfortable than late mobilisation (4 weeks).18,19 In contrast, Davis and Pace 21 immobilised patients after a trapeziectomy in a soft bulky bandage for 3 weeks leaving the fingers free. However, 4 out of the 65 patients experienced a complication of dorsal subluxation of the pseudoarthrosis. It was subsequently suggested that immobilisation in a plaster cast may be preferred by some surgeons. 21
While many studies started mobilising at 6 weeks, others started earlier with acceptable results.18–20 Belcher and Nicholl 18 began gentle mobilisation out of the splint at 4 weeks. Patients in their study reported an improved perception of hand function and reduction in pain at a median of 13 months postoperatively. In another study, Horlock and Belcher 19 comparing two groups instructed patients in their early mobilisation group to take their custom splint off after 1 week for light activities and wear it for protection at night until 6 weeks. The late protection group however, started gentle use and mobilisation out of the splint at 4 weeks, stopping use of the splint at 6 weeks. There was no significant difference in outcomes (function, ROM, grip strength, pulp pinch and key pinch) between the two groups. There was also no evidence that early mobilisation predisposed to subluxation. 19
Hand therapy is often started after the immobilisation period following a trapeziectomy. Hand therapists can provide education, assist with functional recovery of the hand after surgery and treat complications (e.g. prolonged pain, oedema, stiffness). Few studies addressing postoperative treatment for CMC I OA include specific referral to a hand therapist or rationale for a cast immobilisation period.
Based on the experience of the participating surgeons and the average time found in the literature, consensus of the immobilisation time in a plaster cast was decided to be 4 weeks.6,18,22 In addition to some pain control, it provided uniformity of treatment. It was agreed that all patients should be referred to a hand therapist preoperatively. At 4 weeks a splint (Figure 2) was fitted, with mobilisation and self-care immediately started out of the splint. The purpose of this prospective cohort study was to evaluate the effect of a newly developed standardised protocol on clinical outcomes at a 1-year follow-up.
Methods
Demographic and clinical data of cohort.
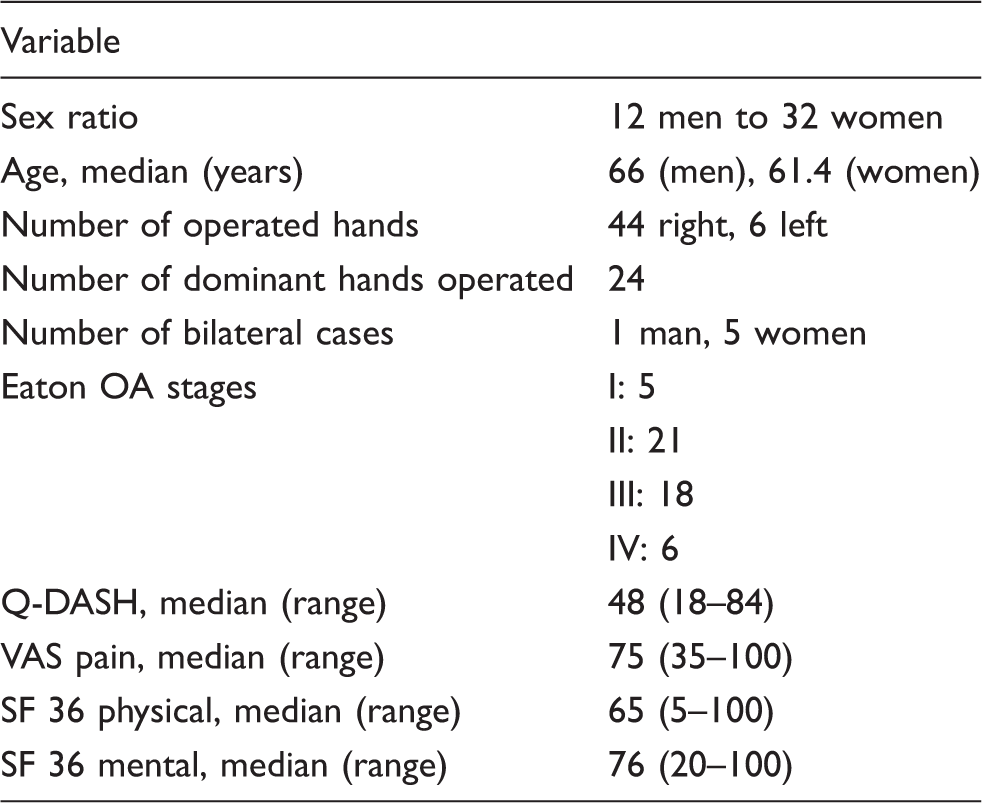
Note: OA: osteoarthritis; Q-DASH: Quick Disabilities of the Arm, Shoulder and Hand questionnaire; SF-36: short-form questionnaire.
Outcomes
All patients were evaluated preoperatively and at 3, 6 and 12 months. Patients were asked to complete the Quick Disabilities of the Arm, Shoulder and Hand (Q-DASH) and the Short Form 36 (SF-36) questionnaires (Dutch versions) as well as indicate the level of their pain on a 0–100 mm Visual Analogue Scale (VAS).24–26 In addition at 3, 6 and 12 months patients were asked to rate their satisfaction of the operation on a VAS of 0–100 mm: 0 was totally unsatisfied and 100 mm was completely satisfied with the operation.
Hand therapists recorded active range of movement (AROM) using the Modified Kapandji Index (MKI) and goniometry (Smith & Nephew Rolyan, Inc.). 27 Grip strength was measured with the Jamar® Hydraulic Hand Dynamometer following a set procedure. Tip pinch and lateral pinch were measured using the Baseline® Mechanical Pinch Gauge following the Pinch Gauge Operating Instructions.
Rehabilitation
The pre-admission assessment by the hand therapist included preoperative measurements and clinical scoring. A leaflet and verbal information about the rehabilitation process were given and the patients’ short and long-term goals were evaluated. 28 Light daily activities without experiencing pain or using force through the hand were started 4 weeks postoperatively while wearing the splint as shown in Figure 2. In addition to self-care, the splint was removed four times a day for light proprioceptive thumb and active wrist exercises. The splint maintained the thumb in a functional position protecting the joint. 29 The rehabilitation was progressed at week 5. This included range of movement exercises for extensor pollicis brevis (EPB), flexor pollicis brevis (FPB), abductor pollicis longus (APL) and the first lumbrical muscle. Ten repetitions of the exercises were to be performed four times a day without pain.
Splint usage was stopped at week 6 except for protection with heavier tasks. Exercises were continued and progressed with an increase in repetitions as tolerated. Specific use of the hand for the patient’s lifestyle was reviewed and begun as appropriate. Patients were educated how best to position their thumb including avoiding positions of deformity, especially hyperextension of the MCP I.2,30
Light pinch strength training using therapy putty was started at week 8. Exercises were to be carried out 2–4 times a day progressing from 10 repetitions to 2 sets of 10, then 3 sets of 10 without pain. Functional use of the hand and strengthening exercises continued to be progressed weekly within pain. The rehabilitation process is shown in Figure 1.
The rehabilitation process.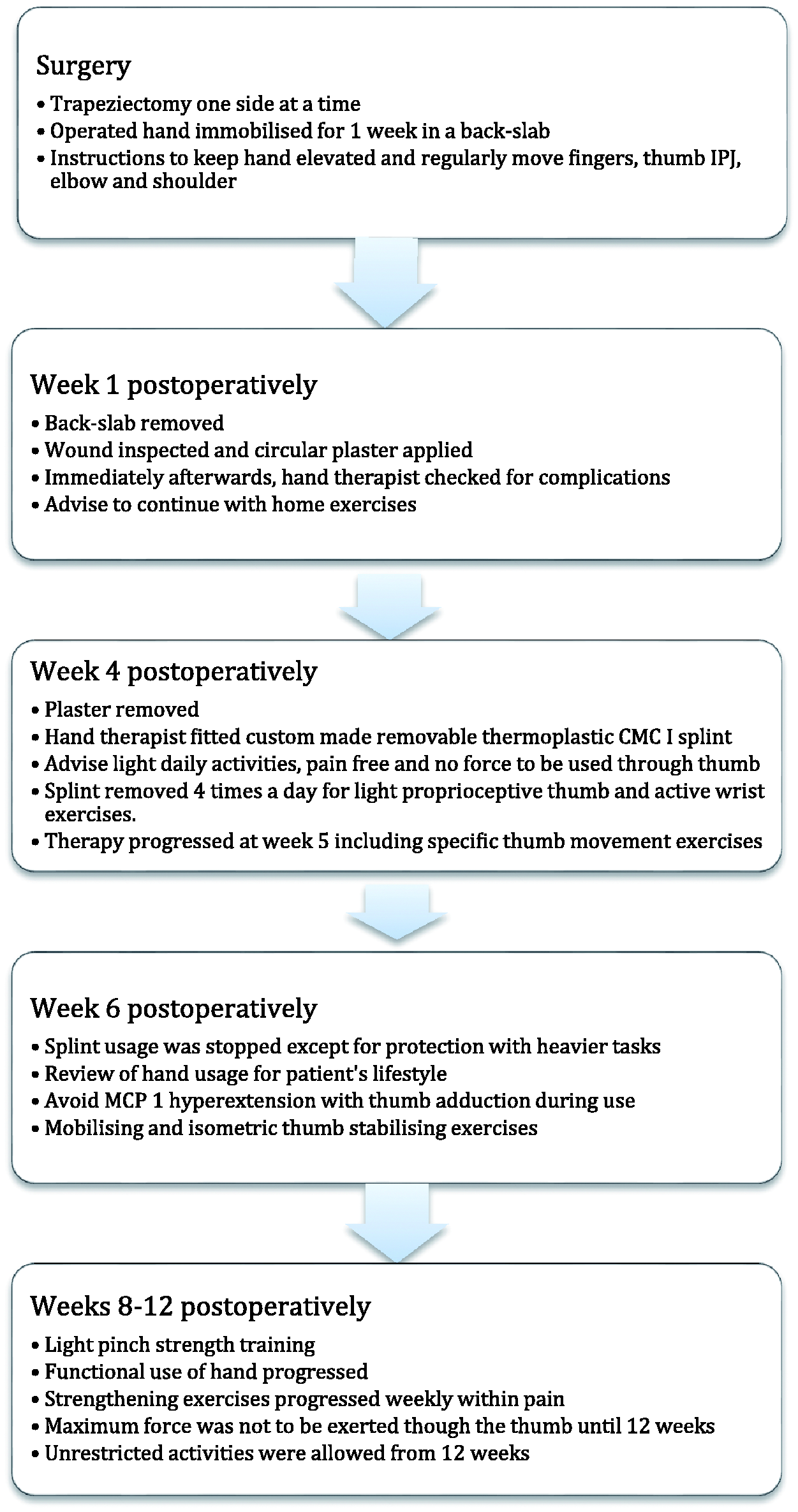
Data analysis
The statistical Package for Social Sciences (SPSS) software version 21 (SPSS Inc., Chicago, IL) was used for the statistical analysis. Results are presented as a median (range) as all variables were not normally distributed and non-parametric tests were used to determine the correlation and differences between measurements. Differences were considered statistically significant with a p-value <0.05. To compare changes between the time intervals, median grip and pinch strength as a percentage of the baseline value (shown as 100%) were calculated.
Results
Median (range) results of outcome measures preoperatively, 3, 6 and 12 months.
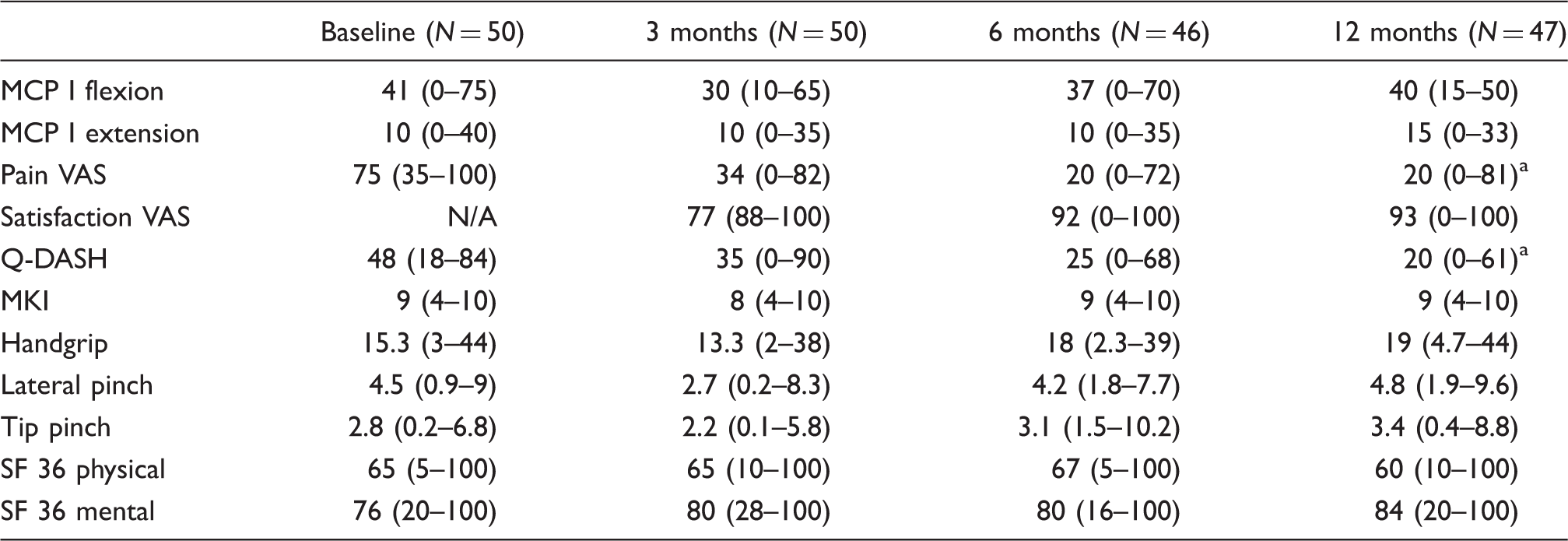
Note: MCP I: metacarpophalangeal; VAS: visual analogue scale; Q-DASH: Quick Disabilities of the Arm, Shoulder and Hand questionnaire; MKI: modified Kapandji index; SF-36: short-form questionnaire; N/A: not applicable.
Significant difference between the baseline and 12 months measurements.
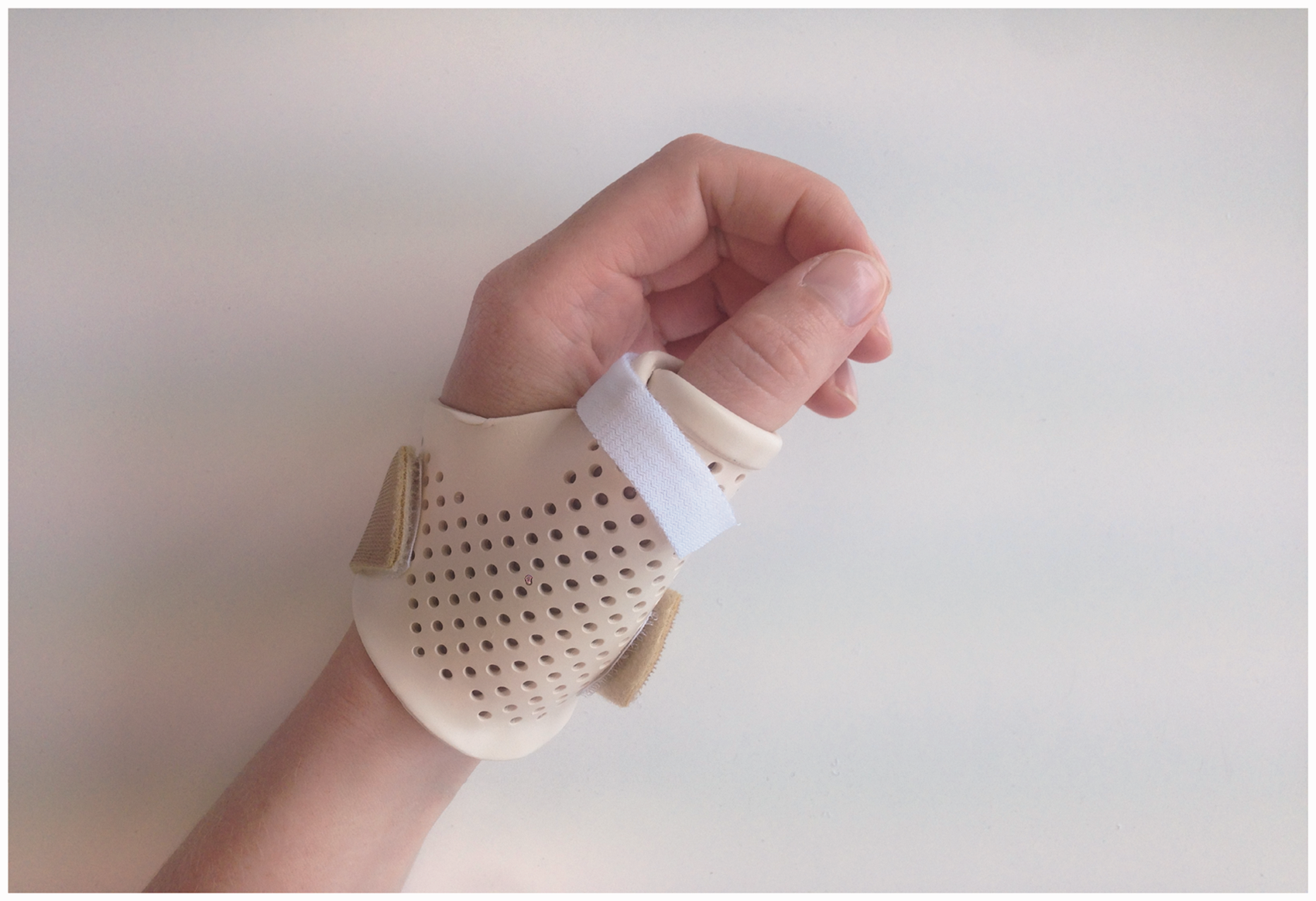
Carpometacarpal 1 splint.
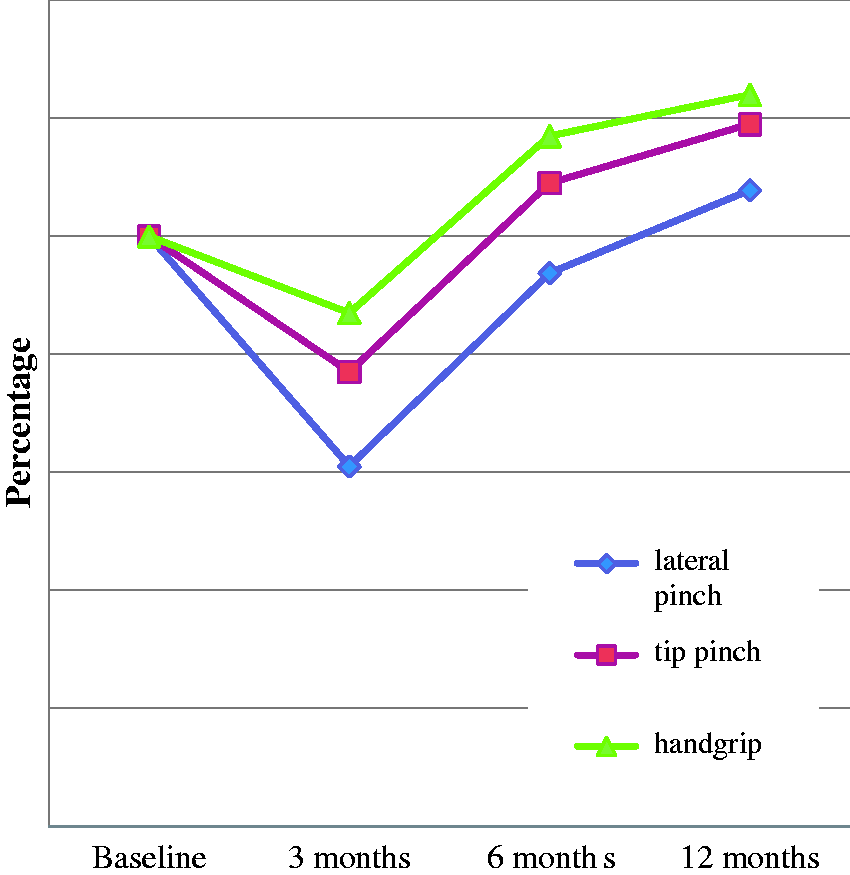
Percentage grip and pinch results preoperatively, 3, 6 and 12 months, as a calculated proportional ratio of the pre-operative baseline values (100%).
Discussion
The aim of the present investigation was to develop a trapeziectomy rehabilitation protocol. With the arrival of new surgeons in our hospital we encountered variability of trapeziectomy protocols which included different immobilisation times and logistics including hand therapy referrals.
Pain in an osteoarthritic thumb can dramatically limit daily life becoming a common reason for individuals to seek surgery.5,8 As the purpose of a trapeziectomy is to reduce pain for the return of acceptable hand function, it may be one of the most important outcomes to be used.6,8,18,22 Therefore, we used the pain VAS as a subjective patient-rated outcome measure as well as satisfaction VAS, the Q-DASH and SF-36. A main finding of our study was the significant correlation (ρ = −0.80), between pain perception and satisfaction with the operation at 12 months. These results support the findings of Belcher and Nicholl 18 who treated 43 patients for either a trapeziectomy alone or with a LTRI. As with our investigation they found that as the perception of pain reduced satisfaction with the operation increased. 18
A significant improvement in hand function was revealed in our study. This was shown by the change, (48–20) in the Q-DASH from preoperative to 12 months follow up (p < 0.01). There were no significant changes within the SF-36. The SF-36 questionnaire is a well-known, valid but general quality of life tool. The results in the physical domain of SF-36 may be influenced by other medical conditions in our patient population: for example arthritis in other joints, rheumatoid arthritis. Despite no significant difference in the physical domain, hand function still improved.
Some of the objective findings (MCP I flexion, MKI, grip, tip pinch and lateral pinch strength), relatively worsened at 3 months which could be expected. Patients were aware that these changes might occur as they had been informed prior to the operation. By 12 months these outcomes had improved to their baseline level or higher. The grip, tip pinch and lateral pinch strength results are comparable to the findings of previous studies.18–20 Although the measures in our study showed an improvement, as with some earlier studies there were no significant differences at 12 months relative to the base line measures.18,20,21
Key to the structure of our protocol were the uniform referral system, the preoperative assessment and consensus of the immobilisation time. These factors were intended to minimise logistical problems and inconsistencies. 31 A preoperative assessment was introduced for patient’s transparency and education. In addition to a leaflet, the assessment provided an opportunity for clarification of patients concerns. We also discussed their responsibilities in self-management during the rehabilitation process. Patients were informed about the postoperative treatment pathway and rationale behind steadily increasing the use of their hand. Throughout the rehabilitation this information was regularly tailored to the individual’s work, home and hobby contexts. Education is known to support patients’ psychological state enabling them to make better health care decisions for themselves. 28
All patients in our study were immobilised for 4 weeks in a plaster cast based on the average time found in the literature and experience of the surgeons involved. 22 In daily practice some patients expressed their discomfort with being immobilised for 4 weeks while others complained of pain or stiffness in the wrist and/or MCP I after the plaster cast was removed. Appropriate exercises and advice were subsequently given by the hand therapists to help reduce the problem. Pain and stiffness after immobilisation for a trapeziectomy have previously been reported.18,19 Similarly to our study, Horlock and Belcher 19 found that prolonged splintage is less convenient for patients. They suggested that regimes should be adjusted for patient convenience and comfort while protecting the thumb in the early days after surgery. 19 Our subjective findings with patients’ comments questions the need for prolonged immobilisation. Few studies are available for comparison due to heterogeneous and/or inconsistent use of outcome measures. 7 Further research using comparable subjective outcomes are needed to clarify the optimal length of immobilisation time after a trapeziectomy.
A survey carried out by Brunton and Wilgis 22 found that while over 75% of respondents fully immobilised their patients for 4 weeks or more, of the surgeons who immobilised patients for 2 weeks or less, 62% had more than 10 years experience. The differing immobilisation choice highlights the importance of expert opinion. Similar operations performed by different surgeons with varying postoperative treatment have had acceptable results. While evidence based medicine is essential it is not always possible to apply in practice. The use of expert opinion therefore, is necessary to bridge the gap for provision of optimal medical care. 32
Wolfe et al. 33 recently described considerable variation found in postoperative immobilisation, exercise, therapist referral patterns and returning to full activity in trapeziectomy procedures. Patients in our study began unrestricted activities from 12 weeks after their operation. This was based on surgeons experience and healing times, however few studies address when patients can return to full activities. 33 The variety of both immobilisation protocols and surgical techniques makes it difficult to draw clear conclusions in terms of clinical effectiveness. 18 Careful preoperative evaluation and planning, correct surgical technique and appropriate postoperative care are considered essential to the success of trapeziectomy surgery. 34 Long-term prospective studies for treatment of CMC I OA are needed to address these issues.
Relatively few complications occurred in our study consistent with other investigations. Trapeziectomy alone is considered as safe as other surgical procedures for CMC I joint arthritis. 7 In addition to some patients experiencing pain or stiffness after the plaster cast was removed, complications also included: eight patients experiencing slight sensory loss or hypersensitivity from the superficial radial nerve, which recovered between 2 and 6 months. Five patients developed chronic regional pain syndrome type 1 (CRPS 1) in their hand and wrist. At 3 months, three patients had very mild symptoms that had resolved by 6 months. At 12 months, the fourth patient was fully recovered, the other patient had residual stiffness in her hand. One patient’s first metacarpal proximally migrated and a loose bone fragment was found. The loose body was removed at 9 months postoperatively. The patient was very satisfied with the resulting hand function. Two male patients complained about loss of lateral grip- and tip pinch strength due to >2 mm proximalisation of the first metacarpal; both had a pain VAS score of 6.5. One of these patients required a revision (LRTI), with a good result at one and a half years after surgery.
Limitations of the study include: its study design, a prospective cohort with a lack of a control group; we have no previous results for data comparison with the present research; the last outcome measures were recorded at 12 months, which limited findings for long-term results. Adherence to the exercises was not formally recorded which might be a limitation. However, patient’s exercises were reviewed at every treatment session. The majority of patients progressed as planned through the rehabilitation programme. This included a preoperative assessment then starting from 4 weeks postoperatively, once a week until 3 months postoperatively. This varied depending on patients needs. Some patients had fewer appointments as they could self manage between rehabilitation stages. Other patients required more appointments as they needed, for example more support with exercises or developed complications.
In future, research into adherence of exercises and stages of progression should be recorded.
The maximum web space was linearly measured from the nail corner of the index finger to the nail corner of the thumb. This method was found to be unreliable so the measurements were not included in the results. Davis and Pace 21 found measurement of the radial and palmar abduction of the trapeziometacarpal joint difficult to measure and inaccurate. Palmar abduction is important to measure as it is a movement required for restoration of functional grip. 35 In future studies, a validated measurement for CMC I palmar abduction could be used, such as the Pollexograaf®. 36
Extrapolation of the present protocol to a population of patients treated with LRTI could be considered. During our study, a few patients received a LRTI and were treated with the same protocol. However, due to low numbers it is not yet possible to draw conclusions. In the future, a prospective study could be carried out in a group of patients treated with a LRTI compared to a group treated with trapeziectomy alone, using the same rehabilitation protocol. We intend to modify the immobilisation time of the present protocol based on the good results of the pain VAS and patients satisfaction with the operation. In addition, while patients complained about plaster time and stiffness in the hand once it was removed, we have no real evidence of a detrimental influence on patients’ outcomes with a shorter immobilisation time. Therefore, we propose a back slab for one week followed by a removable CMC I splint over the wrist until 4 weeks postoperatively. Starting at week 1, patients should be instructed to move their wrist and thumb gently and pain free out of the splint 3–5 times a day. Experienced hand therapists are capable of adapting the splint to the patients needs (e.g. only the CMC I supported) and tailor the immobilisation period to a maximum of 4 weeks based on individual requirements. The results from the study with the new protocol could then be compared with the present results in a non-inferiority study. It would be expected that patients have the same improvement in pain with less inconvenience from longer immobilisation.
Financial implications were not considered with this study and have rarely been mentioned in previous studies. 14 With the increasing cost of healthcare the cost effectiveness of trapeziectomy protocols should also be investigated.
Conclusion
The present study describes a standardised trapeziectomy rehabilitation protocol with a 4 weeks immobilisation time. It has been shown that pain is reduced and good satisfaction with the operation and hand function are achieved using: a univocal referral system, appropriate pre-education and immobilising patients for 4 weeks postoperatively. Trapeziectomy and associated procedures with regard to surgical techniques and results appear to be widely written about with only limited consideration of pre- and postoperative rehabilitation procedures or immobilisation time frames.
Future studies of good methodological quality are required with the focus on an appropriately tailored immobilisation time with pre- and post-operative rehabilitation pathways concerning trapeziectomy. The use of objective and subjective outcome measurements should be less heterogeneous to facilitate pooling of data.
Footnotes
Acknowledgements
The author would like to give special thanks to Annemiek Hol for her untiring support during the study and valuable advice and feedback. The author also gratefully thanks Peer Konings for his support and feedback during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Rijnstate Hospital Ethics Committee, Arnhem, The Netherlands, (LTC 817/231211).
Guarantor
Lucy Henstridge.
Contributorship
Not applicable.
Informed consent
Written informed consent was obtained from all subjects before the study.