
Abstract
Introduction
Dexterity assessment is an integral component of hand function evaluation. The Minnesota Rate of Manipulation Test is a valid and reliable tool to evaluate manual dexterity and has been used to study prognosis of therapy. Information available on its reference values is limited. Reference values are required to interpret, set realistic treatment goals, and assess the ability to return to employment. Therefore, manual dexterity was studied in healthy Indian adults to generate reference values.
Methods
A descriptive study was conducted on 900 subjects divided into three groups: Group 1: 18–30 years (n = 300): Group 2: 31–60 years (n = 300), and Group 3: ≥61 years (n = 300). The Minnesota Rate of Manipulation Test was used to evaluate manual dexterity. All subjects performed three trials (one practice + two test trials) of the five subtests. The average of two test trials was used to compute the Minnesota Rate of Manipulation Test score.
Results
The total score of the Minnesota Rate of Manipulation Test in Groups 1, 2, and 3 was 275.7 ± 24.1 s, 299.3 ± 31.9 s, and 357.4 ± 48.6 s, respectively. Manual dexterity was moderately associated with age (r = 0.707, p < 0.001); however, differences between males and females were nonsignificant (p = 0.306).
Conclusion
Manual dexterity declined with advancing age; however, differences between genders were not significant. These reference values of manual hand dexterity for healthy adult Indian people will be relevant for clinical assessment of hand function.
Introduction
An interest in identifying valid and reliable outcome measures within the context of the International Classification of Functioning, Disability, and Health (ICF) for hand assessment is growing considering its relevance.1,2 Accordingly, the multidimensional concepts of functioning and disability are expressed in terms of body structures and functions, activity, participation, personal and environmental factors.2,3.In the same context, fine hand use (d440) is a component of mobility within the domains of activity and participation.1,2 Therefore, dexterity is considered an integral constituent of fine hand use and hand function. 4 Dexterity is defined as “manual skill requiring rapid coordination of fine and gross movements based on certain number of capacities developed through learning, training and experience.” 5 Assessment of dexterity has functional implications based on age, health impairments, and vocation of people.6–10 In children dexterity assessment helps predict development of their manual abilities, 6 while among geriatrics it assists in interpreting functional independence. 7 In chronic stroke, patients’ dexterity correlates significantly with manual skills influencing choice of therapy. 8 Dexterity assessment is used to observe prognosis of therapy 9 and helps in vocational evaluation of potential manual workers.9,10 Therefore, evaluation of dexterity is necessary to assess capacity of hand function.
Dexterity is of two types i.e. finger and manual. 5 It has been observed that adults from different continents are likely to present dissimilar normative values for finger dexterity owing to differences in cultural practices and socioeconomic conditions.11,12,13 For instance, American adults were faster 12 with their dominant hand on the Purdue pegboard test as compared to age-matched Indian counterparts. 13 Similarly, children from different continents showed a difference in manual dexterity. 14 It is evident that healthy adults and children from different continents vary in manual dexterity. Besides geography, manual dexterity is known to be influenced by sociocultural background, age, gender, occupation, skin temperature, environmental temperature, and practice.14–20 While reference values are available for manual dexterity for different age groups of people in the western hemisphere,20–22 it may not be appropriate to use these reference values influenced by various extraneous and intrinsic factors for Indian people.23
In current routine clinical practice, manual dexterity is assessed by standardized tests like the Box and block test, the Jebsen hand function test, and functional dexterity test.4,5,24–26 Among these, the Minnesota Rate of Manipulation Test (MRMT) demonstrates good psychometric properties; is valid and reliable and thus recommended to evaluate manual dexterity.10,11,24,25 The MRMT is successfully used for disability evaluation, 27 screening for employment purposes,28,29 and to evaluate prognosis of therapy. 11 Moreover, MRMT scores along with other data were used to plan employment options for psychiatric patients. 10 The MRMT was also validated to assess manual dexterity in individuals with moderate mental retardation. 9 Also, the MRMT can be performed in standing as well as sitting position making it convenient to use.9,30
Therefore, the purpose of this study was to generate reference values for manual dexterity in healthy Indian adults using the MRMT. In addition to this, the study explored the association of manual dexterity with age and job, and compared values between genders. Reference values generated from testing people from India are required to interpret, set realistic treatment goals, and assess ability to return to employment in an Indian clinical setting. 23
Methods
Ethical approval was obtained from the institutional review board. Each participant signed voluntary informed consent. A convenience sample of 900 subjects aged ≥18 years was recruited from students, staff members, and residential complexes in the vicinity of the institute. People with higher function deficits,9,29,31 musculoskeletal impairment,32,33 traumatic injuries, 34 and systemic inflammatory disorders 35 were excluded as these conditions are known to decrease manual dexterity. All subjects were classified into three groups based on age. Group 1 included young adults (n = 300) aged 18–30 years, 23 Group 2: middle-aged adults (n = 300) aged 31–60 years, and Group 3: older adults (n = 300) aged 61 years and above. 36 Each group had an equal number of male (n = 150) and female (n = 150) participants.
The MRMT kit was used to evaluate manual dexterity. The test kit is a wooden rectangular peg board with 60 color coded pegs. The 60 pegs are arranged in 15 columns and 4 rows. The pegs have one blue surface and other red. 10 The board and pegs were constructed precisely as per dimensions reported earlier. 21
The MRMT consists of five subtests: placing, turning, displacing, one hand turning and placing, two hand turning and placing.21,22 All tests were explained to individual participants in a comprehensible local language (Marathi or Hindi) in addition to demonstration of the tasks they were expected to perform. On account of the diversity of the participants’ reading abilities, this was easier than providing written instructions. Every subject was provided one trial test for practice, followed by two repetitions for each subtest.11,21 Time taken for the practice trial was not accounted in the total score. Time was recorded in seconds after the last peg was inserted into the hole using a stopwatch. An average of two repetitions was computed for the final score.11.Total score was obtained by computing the sum of time taken for all subtests in seconds.
Each participant was tested in a standing position. 21 For the placing test, the subject was instructed to place pegs from the top board into holes of the bottom board using only the dominant hand.21,22,37 In the turning test, the subject was instructed to pick up pegs, one at a time, with their dominant hand as fast as they could and transfer the peg to the nondominant hand. The peg was replaced into the original hole, with the reversed surface, based on color using the nondominant hand.21,22,37 For displacing, the subject was instructed to remove the peg from top hole on upper left-hand corner in the first column and put it in an empty hole on other side of the board. The following 59 pegs were displaced one hole at a time in the standard manner. 22 In one hand turning and placing test, the participant picked pegs from top board, turned the pegs over based on color, and placed them into holes of bottom board all performed using only the dominant hand. 22 In the two hands turning and placing test, the subject picked pegs from the top board as quickly as possible, two at a time (one in each hand), turned the pegs over, thus showing the other color of the peg, and placed them into holes of the bottom board closer to them with both hands engaged in this subtest. 22
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 16.0 for Windows 7 (IBM, New York, USA). Subject demographics were presented with frequency distribution, mean, and standard deviations wherever appropriate. Central tendency and spread of total score were reported with mean and standard deviation for all age groups. Differences in manual dexterity scores between the three age groups were compared using one-way analysis of variance (ANOVA). Linear polynomial contrast was used to investigate decline in manual dexterity from young to older adults. The association of manual dexterity with advancing age was explored with Pearson’s correlation coefficient. Decrement of manual dexterity with advancing age was presented graphically. Manual dexterity scores between males and females were compared using Student’s unpaired t-test. Job demand was classified according to the Dictionary of Occupational titles.38,39 MRMT score variation with different occupations was represented graphically. Differences were considered significant at p ≤ 0.05 for all analyses.
Results
The study included 900 participants (450 women and 450 men) stratified in three groups of 18–30 years, 31–60 years, and ≥61 years. Among them 96.1% were right-hand dominant and 3.9% were left-hand dominant. The majority of men and women were engaged in professional, technical, and managerial occupations (74.4%), followed by sales and clerical occupations (16.8%), and homemakers (7.3%). Remaining were in agricultural, fishery, forestry and related occupations (0.6%), bench-work occupations (0.1%), structural work occupations (0.2%), and miscellaneous occupations (0.6%). The recruited population did not include people engaged in processing and machine trades occupations.
Values of manual dexterity of people engaged in various jobs, classified according to Dictionary of Occupational Titles are described as follows: Professional, technical, and managerial jobs (314.9 s), clerical and sales (299.5 s), service (297.8 s), agricultural, fishery, forestry (284.6 s), bench-work (324.5 s), structural work (288.2 s), and miscellaneous jobs (307.7 s). Variation in MRMT scores was not observed across different jobs. It is speculated that large differences in the number of participants in each occupation, may have resulted in nonsignificant differences.
Execution time(s) for Minnesota Rate of Manipulation Test (MRMT) and its subtests among females and males.

Differences in total mean scores between three age groups were statistically significant (p < 0.1; Table 1). Significant linear contrast indicates linear decline in manual dexterity from young to middle to old adults (p < 0.001). Correlation analysis revealed that with increasing age, participants took longer time to complete the MRMT test (r = 0.708; Figure 1). To summarize, while age had a detrimental effect on manual dexterity, no association was noted between MRMT scores and gender in Indian adults.
Association of time duration for manual dexterity with advancing age.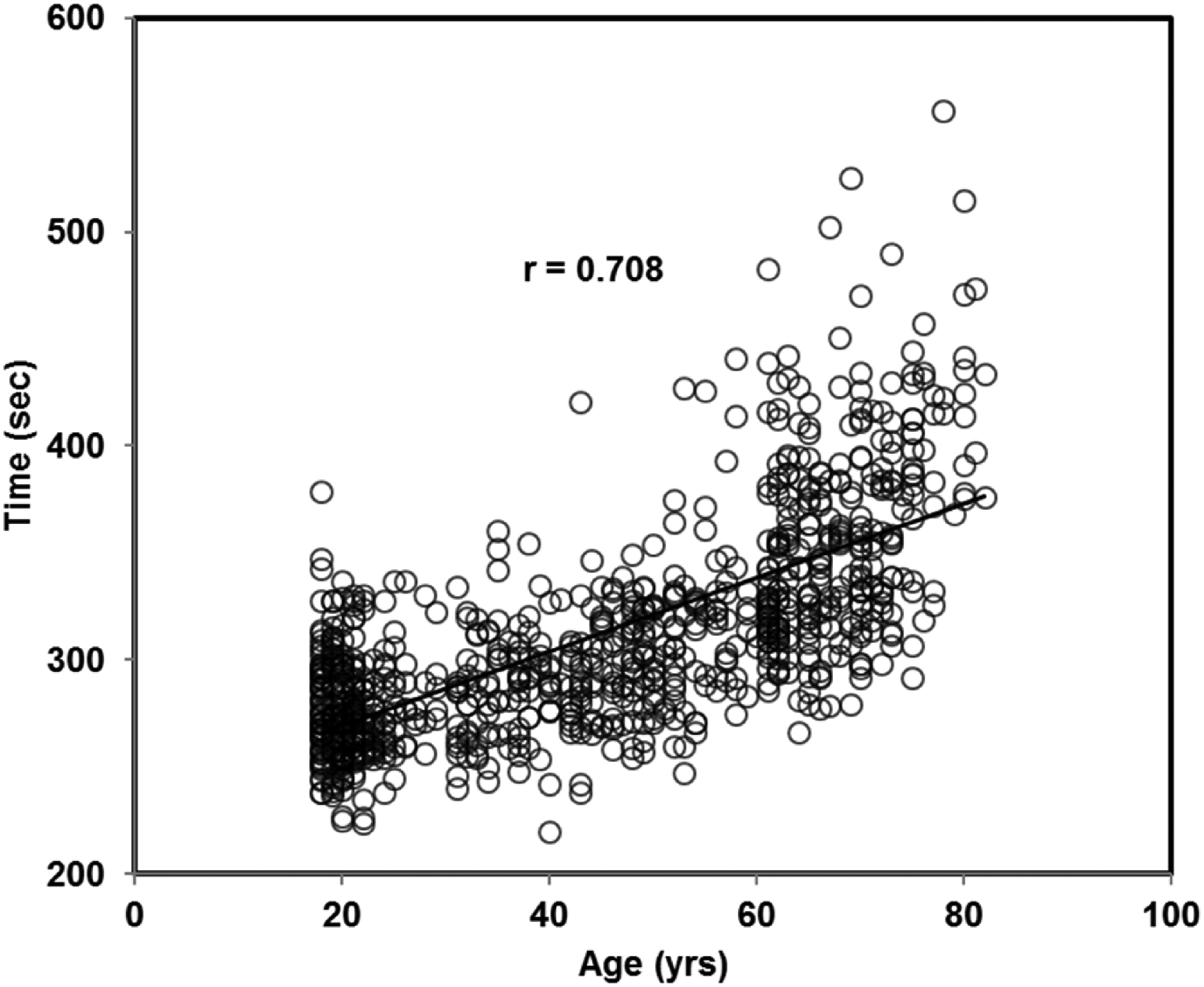
Discussion
The present study established reference values for manual dexterity using MRMT among Indian adults across different age groups. It was observed that as age advanced, there was a decline in manual dexterity, especially after fourth and sixth decade of life. In addition, this study found no influence of gender on manual dexterity among Indian adults.
Comparison of Minnesota Rate of Manipulation Test (MRMT) scores between Indian and populations across different geographical locations.
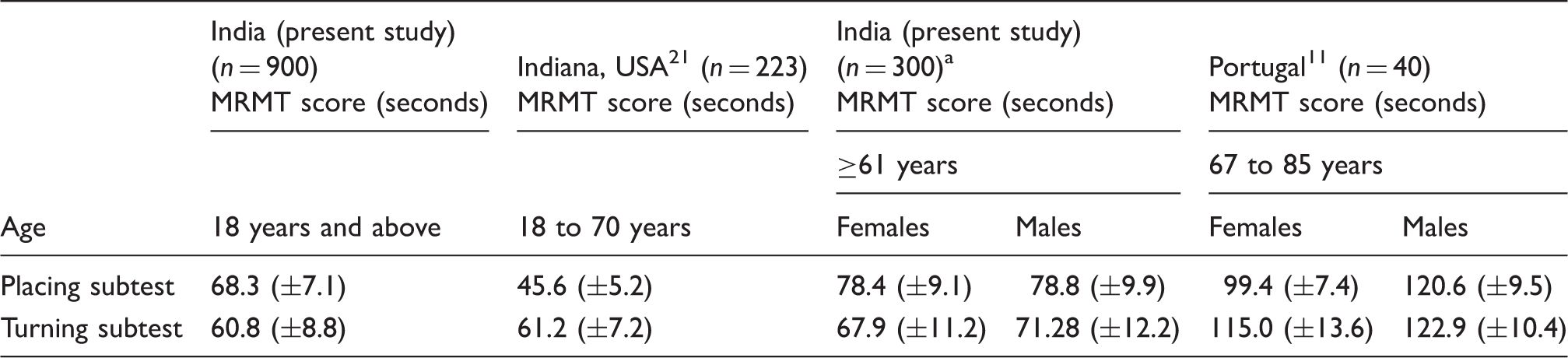
Participants in age group of ≥61 years were 300 in number.
A study from Indiana, USA reported by Surrey et al., examined performance outcomes between the MRMT and the Minnesota Manual Dexterity Test (n = 223) 21 (Table 2). Direct comparison of MRMT scores is not possible, as the MRMT scores were reported for subjects with ages ranging from 18 to 70 years without age stratification. However, a cursory comparison of both studies reveals that Indian subjects were slower in the placing subtest and had similar scores than American counterparts. Another study available for comparison from Portugal, reported manual dexterity scores using the MRMT in 67–85 years’ age group11 (Table 2). Direct comparison of manual dexterity scores in the age group 61 years and above is not possible due to limited details about the test procedure and small sample size (n = 40). Despite accounting for likely differences, it was observed that Indian males and females completed the placing and turning subtest earlier compared to the Portuguese subjects.
The MRMT scores obtained from Indian adults revealed that their manual dexterity was different compared to age-matched individuals of other geographical locations, reiterating importance of generating age and gender-based reference values of manual dexterity for Indian healthy adults ≥18 years. In addition to this, the study explored the association of manual dexterity with age and job and compared values between genders.
Exploration of manual dexterity with age revealed a strong influence of age. As age advanced, time taken to complete MRMT increased. These findings were consistent with previous studies despite use of alternate tools for evaluation of manual dexterity i.e. the Box and Block test, Jebsen test of hand function, and Grooved pegboard test.20,42,43 Decline in manual dexterity commenced gradually in the fourth decade of life, which can be attributed to brain atrophy in the forties and association of brain atrophy with deterioration of mental function. As age advanced beyond sixties, a rapid decline in manual dexterity was noted (Figure 1). The older adults demonstrated approximately 30% decline in manual dexterity as compared to young adults, which can be explained by reduced finger mobility, selective atrophy of fast twitch muscles, significant reduction in action potentials, and diminution in number of viable motor units.20,44–46 Other factors contributing to decline in manual dexterity in older adults are peripheral decrement in tactile sensibility, degenerative changes in motor cortex, cerebellum, and basal ganglia.44,46 In addition to these, loss of small neurons in the intermediate zone of the spinal cord,46–49 deferring of hand-associated afferent information processing44,45 and loss of visual acuity 46 lead to difficulties with fine precision and grip movements subsequently affecting manual dexterity. 46 Hence, manual dexterity of Indian adults was observed to decline with increasing age, especially in the forties with a rapid decline after sixties.
The study also investigated the effect of gender on manual dexterity in Indian adults. An earlier study conducted in Portugal has reported a significant difference in manual dexterity between males and females (p < 0.05). 11 However, the present study did not demonstrate an influence of gender on manual dexterity. This can be explained as follows: dexterity is quantified as an ability to produce pinch force with two digits to perform manipulations with small objects 50 and it is already reported that there is no difference in generation of pinch force and peg placing time between males and females. 51 Secondly, tactile sensitivity that is pivotal in dexterity was reported to have no variation between genders. 4 Findings of the present study concur with previous studies, which did not demonstrate influence of gender on manual dexterity. 19 However, this does not exclude the likely possibility of variations in finger dexterity between both genders as the females are known to be involved in fine dexterous activities such as chopping, sewing, knitting, braiding, and cooking. 51 Descriptive analysis revealed that females in middle age and older adults performed marginally better.
This study observed marginal variation in MRMT scores across people of different jobs; however, differences were nonsignificant probably because the participants did not include an equal number of people from different job categories. The majority of participants were performing similar jobs such as professional, technical, and managerial categories i.e. lightweight activities.
The reference values for MRMT will provide clinicians with a range while evaluating manual dexterity in healthy adult Indian subjects across different age groups. These values should be useful to guide clinical decision making and monitor hand function in rehabilitation and injuries.21,23 However, the clinician should be conscious that the MRMT scores give insight into the highest level of functioning (i.e., capacity). These scores do not necessarily translate into functional independence in performing activities of daily living and related to work (i.e., performance).2,52 Hence along with MRMT, clinicians should consider evaluating activities of daily living 4 or specific work-related activities, as the MRMT does not assess all routine activities.
A major limitation of study includes lack of a random sampling strategy. Therefore, we recommend further research on normative values for MRMT among Indians be conducted using a large random sample stratified by age group, gender, and job.
Conclusion
This study established reference values for manual dexterity using MRMT among Indian adults across different age groups. Reference values generated from the study can be used for clinical reference in the evaluation of hand function of adult Indian people. Findings suggest that as age advances, manual dexterity declines after fourth decade with a rapid decline after sixth decade of life. Manual dexterity did not differ between men and women.
Although reference values for manual dexterity using MRMT reported in this study cannot be considered as normative values for Indian adults, these values can provide baseline reference, which can be used by clinicians to compare performance of patients in different occupations and daily living activities pre- and post-therapeutic intervention.
Footnotes
Acknowledgements
Authors wish to thank all participants for cooperation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from “Mahatma Gandhi Mission, Medical College and Hospital, Institutional Ethics Review Committee.”
Guarantor
SR.
Contributorship
SR, AP, and RM conceived and designed the study. SR and AP collected the data. RM and SR were involved with statistical analysis of the data. The manuscript was written and edited by RM, SR, and AP.
Informed consent
Written informed consent was obtained from all participants before the study.