
Abstract
Introduction
The Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire is a self-administered region-specific outcome questionnaire developed to measure upper extremity disability and symptoms. The aim of this study was to translate, culturally adapt and validate the Igbo version of the DASH in order to enhance its use in the Igbo-speaking population.
Method
This cross-sectional survey involved 100 participants (56 males, 44 females) with upper extremity musculoskeletal disorders, in the South-Eastern part of Nigeria. Participants completed both English and Igbo versions of the DASH on two occasions. Internal consistency was evaluated with Cronbach’s alpha. Test–retest reliability was analysed by intraclass coefficient (ICC) and the Bland and Altman method. Construct validity was investigated with the Spearman rank correlation coefficient, and a principal component analysis was performed. Alpha was set at 0.05.
Results
Test–retest reliability was excellent (ICC = 0.99). The Cronbach’s alpha coefficient was high (0.979) for the entire items on the scale. There was a significant strong correlation (r = 0.994; p = 0.001) between the scores obtained on the English and Igbo versions of the DASH indicating excellent construct validity. Thirty linear components were identified within the data set. The communalities were above 0.4.
Conclusion
Principal component analysis of the Igbo DASH revealed a two-factor structure, having fulfilled all necessary conditions. The Igbo version of the DASH questionnaire is a valid and reliable outcome measure for individuals with upper extremity musculoskeletal disabilities.
Introduction
Musculoskeletal disorders (MSDs) are highly prevalent Worldwide. 1 Huissetede et al., 2 estimated a range of 1.6 to 53% and 2.3 to 41% for the point and 12-month prevalence of upper extremity MSDs, respectively. MSDs affecting the shoulder constitute the third most common reason for consultation in medical practice after back and neck pain. 3
The development and use of disease-specific questionnaires for every musculoskeletal condition may, however, not be practical.4,5 Region-specific outcome questionnaires have therefore been introduced. One of these is the Disabilities of Arm, Shoulder and Hand (DASH) questionnaire, which was developed and validated in 1994 by the American Academy of Orthopaedic Surgeons (AAOS), the Council of Musculoskeletal Specialty Societies and the Institute for Work and Health (IWH). 6 This questionnaire focuses on functional status and symptoms rather than on one specific anatomic region or specific disease entity. The rationale for the development of the DASH was that the upper extremity is to be considered as one functional unit. 4
The DASH was developed to measure physical disability and symptoms of the upper limb in a heterogeneous population comprising both genders and a range of severities in a wide variety of upper extremity disorders. 7 The DASH allows comparison across different upper extremity disorders and provides a uniform outcome measure to evaluate conservative and surgical interventions, as well as for research purposes. 6
It is a patient-reported questionnaire that contains 30 items covering symptoms and functional status, especially physical function. Each item is rated on a 5-point Likert scale and includes 21 items that evaluate physical function, five items evaluating symptoms and four social role/function items. The values of all questions are averaged, and this value is then converted to a 0–100 scale by subtracting one and multiplying by 25. Higher scores indicate greater disability. An optional work module and sports or music module can evaluate respective functions. 6
Cross-cultural adaptation of validated outcome questionnaires has been advocated to facilitate their use in international multi-centre clinical trials, which would also reduce the need for developing new questionnaires with the same purpose.8,9 To maintain the validity of the original questionnaire while taking into consideration important cultural differences, a specific methodology has been developed for the adaptation process.10–12
According to Willams et al., 13 Nigeria is a multi-cultural country, with the South-Eastern region (Igbo-speaking population and one of the main indigenous languages), having 18% of the total population of 177 million or approximately 32 million people.
In Nigeria, a Yoruba version of the DASH has been translated, adapted and validated in Yoruba language, but this can only be used in the South-Western region of Nigeria. 14 Nigeria has three major indigenous languages: Hausa, Igbo and Yoruba. 14 The Igbo monolinguals in Nigeria lack a standardised uniform outcome measure for different upper extremity disorders. There is a need for translation, cross-cultural adaptation and validation of the DASH for Igbo monolingual individuals with upper extremity MSDs in Nigeria.
The purpose of this study was to translate and culturally adapt and validate the Igbo version of the DASH.
Methods
Permission to translate and cross-culturally adapt the DASH to the Igbo language was obtained from the developers the IWH and the AAOS Outcomes Research Committee. Ethical approval was sought and obtained from the Ethical Committee of Nnamdi Azikiwe University Teaching Hospital (NAUTH), Nnewi before commencement of the study. Nine tertiary hospitals were randomly selected for this study from the five south-eastern states of Nigeria. The procedure employed in this study followed the guidelines for translation and cross-cultural adaptation by Beaton et al. 15 The procedure for the study was in three phases: Phase 1 – translation phase, Phase 2 – adaptation phase and Phase 3 – validation phase.
The purpose and procedure of the study were explained to patients who met the following inclusion criteria: patients with upper-extremity musculoskeletal conditions managed at the orthopaedic surgery and hand therapy units of the selected health facilities in the South-Eastern region in Nigeria, aged 18 years and above and who were literate in both English and Igbo language.
Their participation in the study was voluntary, and they were free to withdraw from the study at any point. Patients with upper-extremity musculoskeletal conditions who gave fully informed written consent participated in the study. The sociodemographic characteristics (age, gender, marital status, highest educational attainment and occupation) and information on part(s) of the upper extremity affected were obtained from all participants. Participants were asked to rate their ability to perform activities over the past week and give only one answer per question. They were also encouraged to complete at least 27 of the 30 items. The scores of all items were used to calculate a summed score ranging from 0 (no disability) to 100 (severest disability).
Phase 1 – Translation phase
The translation phase involves translation of the original English version of the DASH to the Igbo version of DASH (I-DASH). The original English version of the DASH was translated by two bilingual translators whose first language is Igbo, with one having a medical background and the other having no medical background (forward translation). It produced two different Igbo versions of DASH (T1 and T2). The two forward translations were reviewed and discussed by the two translators and a synthesised version was formed (T-12), any differences were resolved by consensus. The synthesised version (T-12) was translated back to the English language (back translation – B1 and B2) by two other bilingual translators who speak and understand both English and Igbo languages and are graduates of English language, as specified by DASH translation guidelines, were blinded to the concepts being investigated and had no medical background.
Phase 2 – Adaptation phase
The translations (T1, T2, T-12, B1 and B2) were reviewed by members of an expert committee comprising of translators (forward and back translators), health professionals and an outcome methodologist. Discrepancies were resolved by consensus to achieve semantic equivalence, idiomatic equivalence, experiential equivalence and conceptual equivalence of the pre-final I-DASH. The pre-final version was created and subjected to field testing on patients. The findings of the field testing were reviewed by the expert committee in a second meeting to produce the final I-DASH.
Phase 3 – Validation phase
The final Igbo version of the DASH and the original English version of the DASH were distributed to individuals with upper-extremity MSDs for self-administration attending physiotherapy clinics or orthopaedic units of the eight hospitals in the five South-Eastern States of Nigeria. The order of administration of the two questionnaires was randomised using a simple randomisation method. The I-DASH questionnaire was re-administered on 55 of the participants one week after the first administration by the researcher.
Data analysis
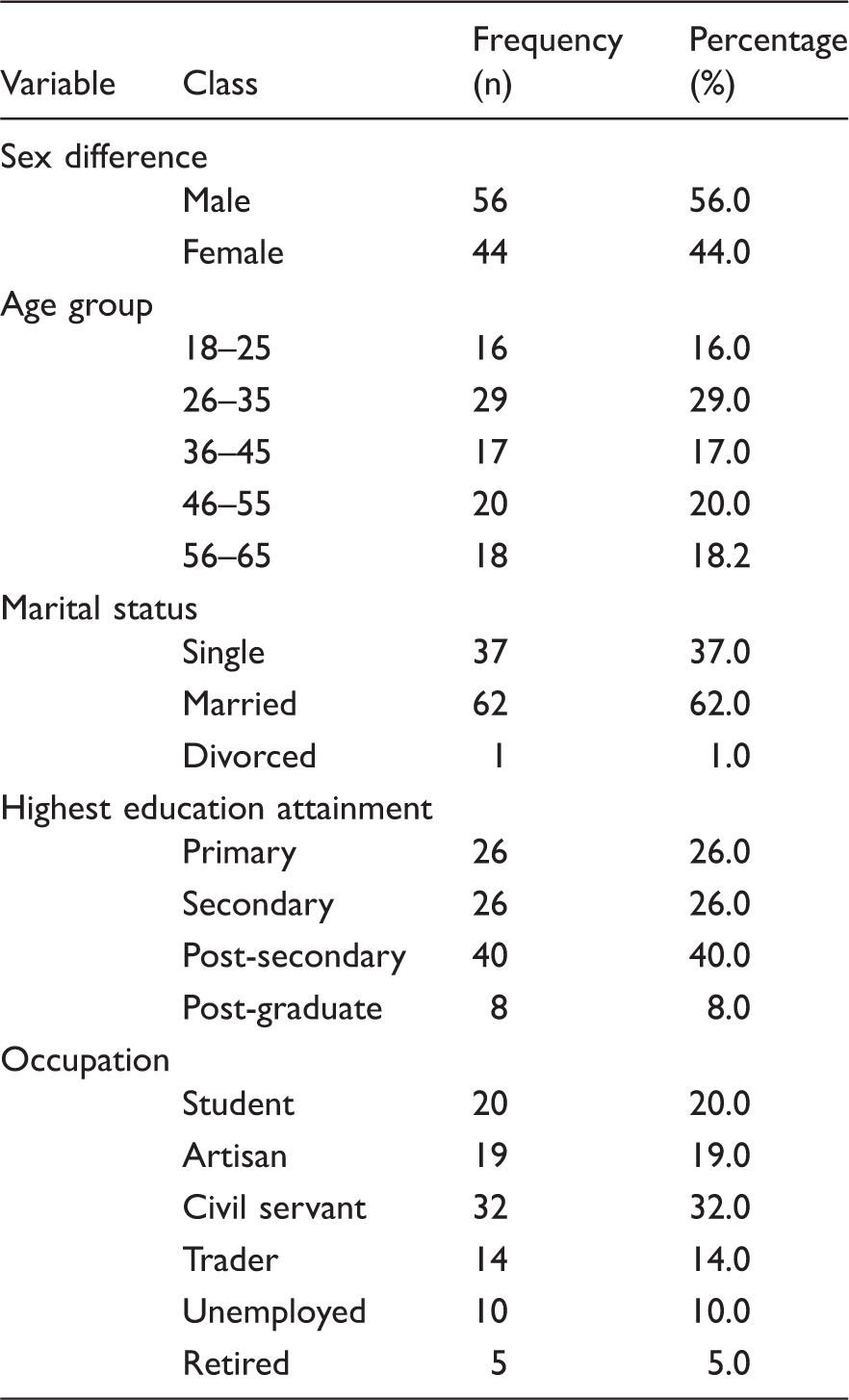
The demographic and clinical variables as well as the scores of the I-DASH and the English version of DASH (E-DASH) were summarised using frequency counts and percentages, means and standard deviation.
The Spearman rank order correlation coefficient was used to analyse the strength of association between participants’ total scores on the E-DASH and I-DASH (to determine concurrent validity), and between the items in the English and I-DASH (to determine construct validity). The intraclass correlation coefficient (ICC) and Bland and Altman plotting method were used to compare the scores on the I-DASH at the two different occasions in order to determine the test–retest reliability of the I-DASH. Cronbach’s alpha was used to determine the internal consistency of the I-DASH. Principal component analysis (PCA) was used to assess the structural validity of the I-DASH. All analyses were conducted using the Statistical Package for Social Sciences (SPSS) version 20.
Results
Socio-demographic distributions of participants.
Cross-cultural adaptation process of the DASH into Igbo culture and environment
Summary of words and phrases modified in adapting the DASH to Igbo culture and environment.
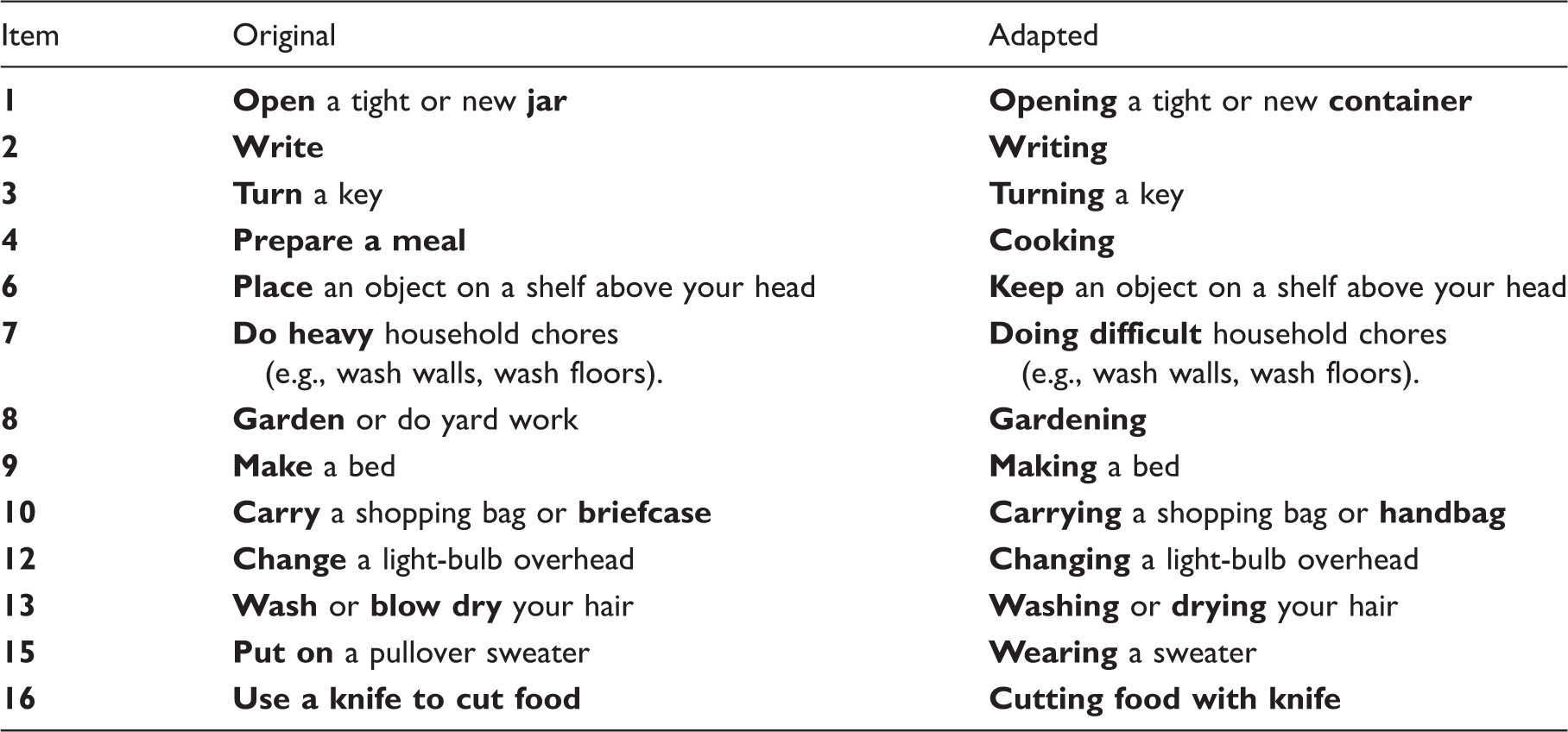
Note: Modified words/phrases are bold.
Twenty patients with upper-extremity MSDs (12 males and 8 females) with mean age of 39.3 ± 28.03 years participated in the pretesting and cognitive debriefing interview of this study. Most of the participants were employed and 16 had at least secondary education. The patients stated that the items were clear and that most of them were relevant to their upper extremity condition. The average time taken by the patients to answer all items was about 10 min. No other adjustment was made by the expert panel.
Test–retest reliability
Test–retest was analysed for 55 patients (32 males, 23 females) who were randomly selected. Their mean age was 37.59 (SD = 12.25) years. The I-DASH scores at the first and second visit were 70.83 (SD = 19.32) and 70.48 (SD = 19.36), respectively. Test–retest reliability analysis gave an ICC of 0.99 (95% CI = 0.996 to 0.998), indicating excellent reliability. However, graphic analysis by the Bland and Altman plotting method revealed that the test–retest results were not strictly centred (mean: 0.35, SD = 1.08). The limits of the agreement for the two scores were −1.8 and 2.5 (Figure 1). The numbers of outliers were only four.
Bland Altman plot of test–retest scores of the I-DASH.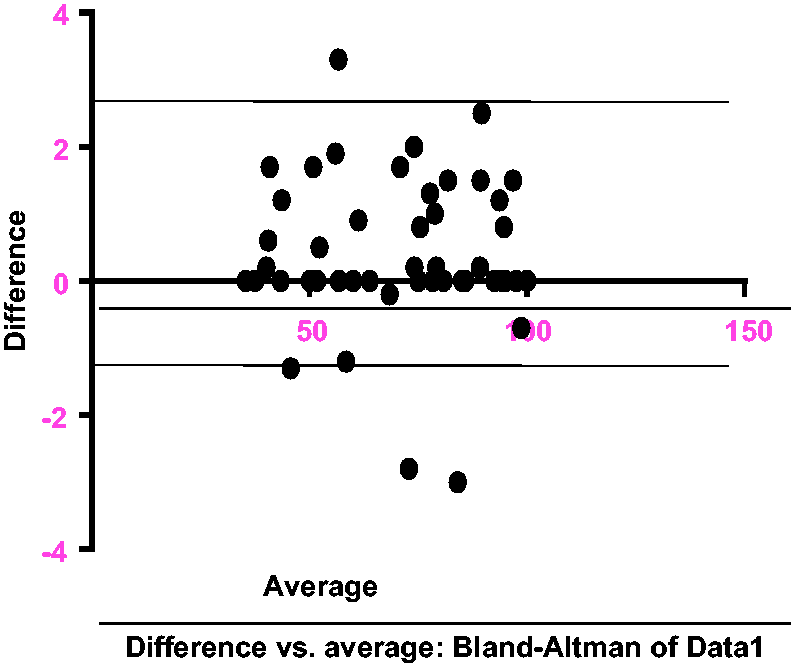
Internal consistency
Internal consistency was high with a Cronbach’s alpha coefficient of 0.98.
Concurrent validity
The correlation between the scores obtained on the English and cross-culturally adapted Igbo version was used to assess the known-groups validity of the DASH. Spearman’s correlation coefficient, r = 0.99 (p = <0.01) was obtained, thus indicating a significant strong association between the two questionnaires. The I-DASH mean score is 55.7 (SD = 25.7) and the E-DASH mean score 54.7 (SD = 24.7). The finding of similar scores in both English and Igbo DASH supports the linguistic and conceptual equivalence of the Igbo version. 11
Structural validity
The 30 items of the Igbo DASH were subjected to PCA using SPSS version 20. Prior to performing the PCA, the suitability of the data for factor analysis was assessed. Inspection of the correlation matrix revealed the presence of many coefficients of 0.3 and above. The Kaiser-Meyer-Olkin (KMO) value was 0.87, exceeding the recommended value of 0.6 16 and Barlett’s test of sphericity reached statistical significance (χ2 (2724) = 435, p = 0.001) supporting the factorability of the correlation matrix. 17
Part 1: PCA
Principal component analysis and Monte Carlo PCA for parallel analysis of the I-DASH.
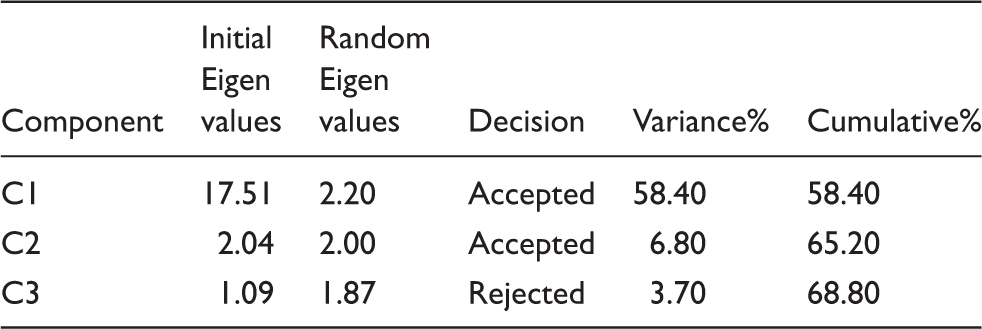
C1: Component 1; C2: Component 2; C3: Component 3; I-DASH: Igbo version of DASH.
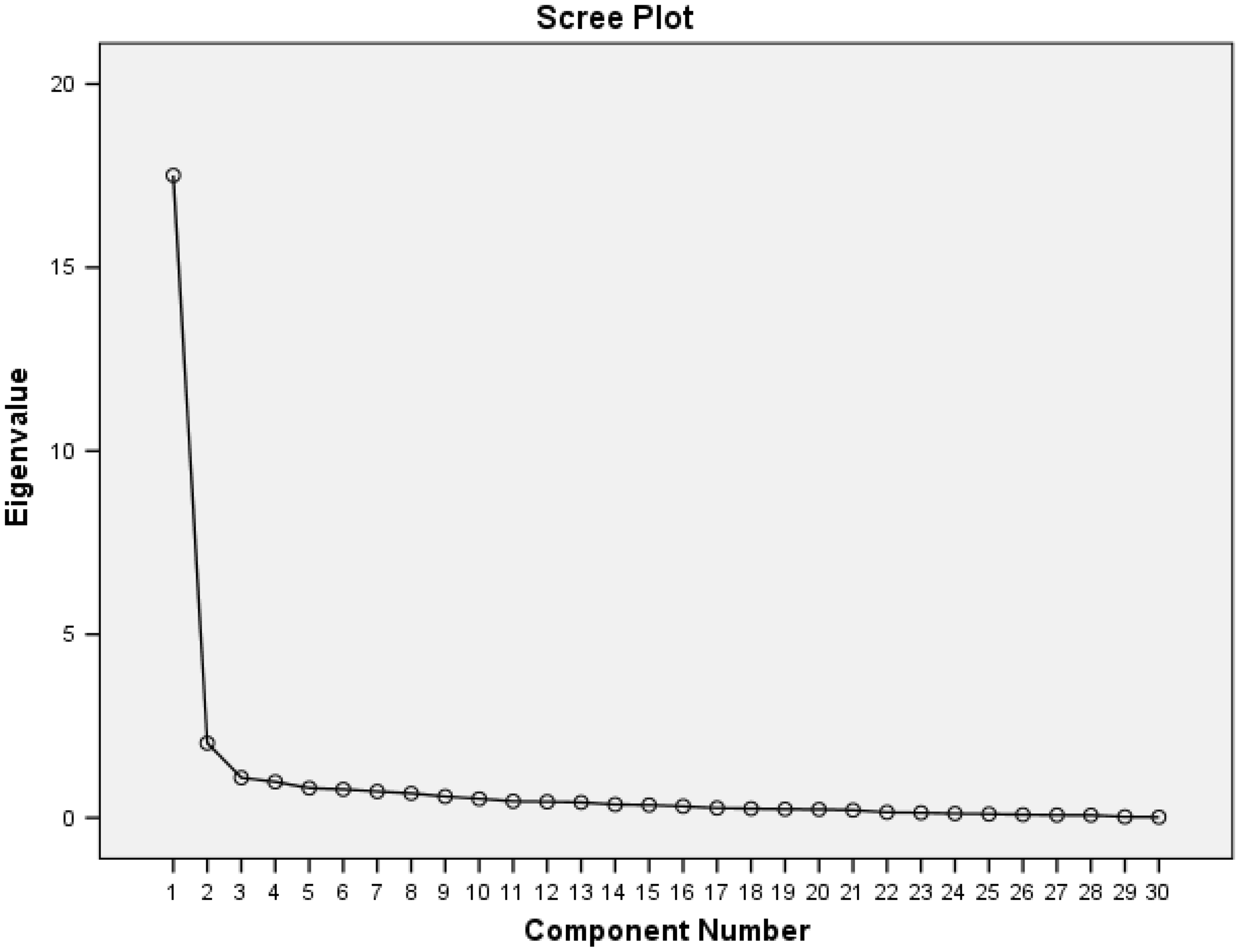
Scree plot of items on I-DASH.
Pattern and structure matrix for PCA with Oblimin rotation of two-factor solution of I-DASH items.
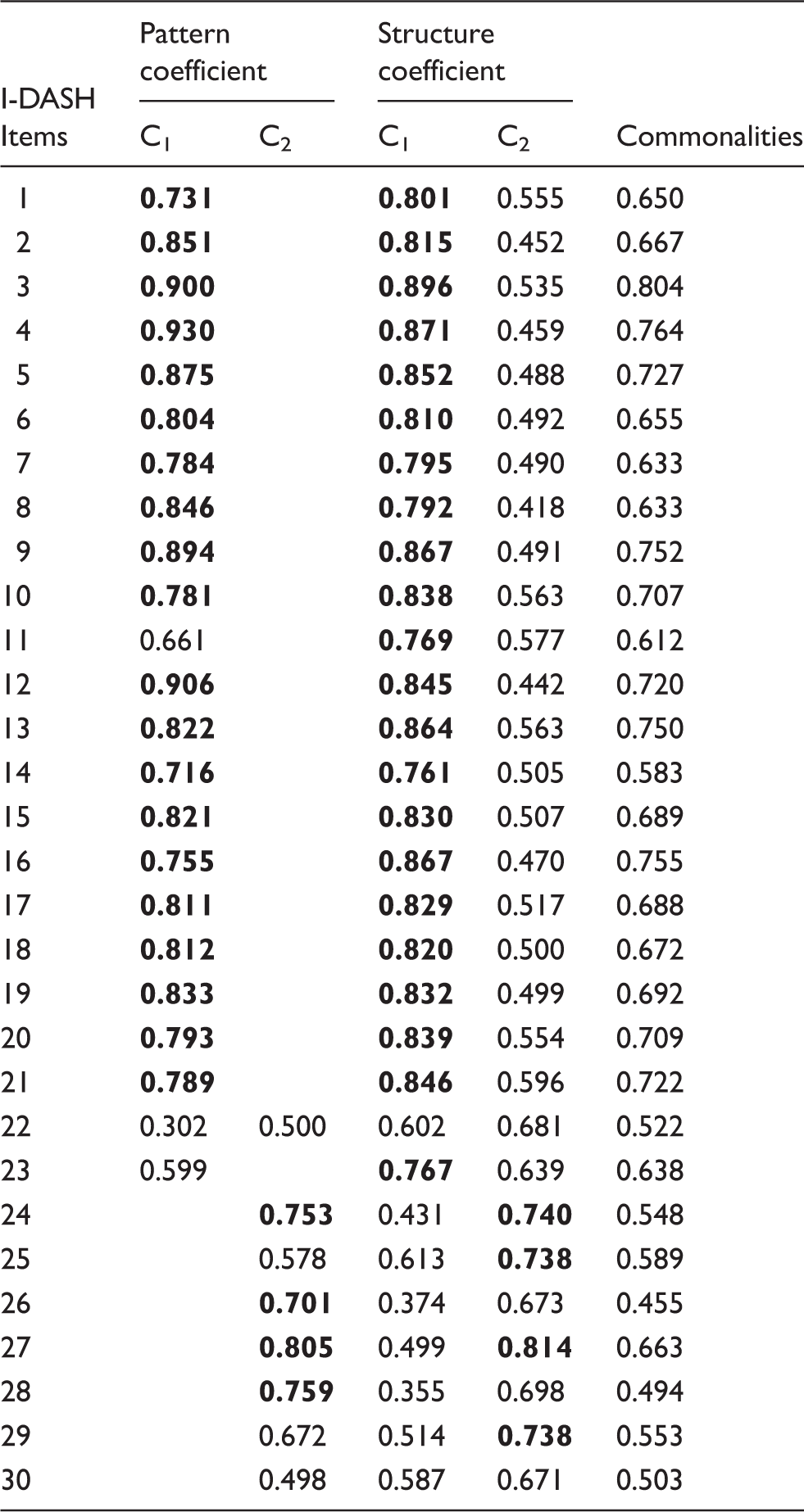
Note: The highest loading of each item is in bold.
PCA: Principal Component Analysis; C1: Component 1;
Part 2: Oblimin rotation of the two-factor solution
The component correlation matrix shows a strong correlation between the two components (0.6). The structure matrix which is unique to the Oblimin output provides information about the correlation between variables and components. The pattern matrix shows the loading of each item on the components (Table 4). The items that have the highest loading on the first component (strength-based) are 4, 16, 12, 3, 9, 5, 2, 8, 19, 13, 15, 18, 17, 6, 20, 21, 7, 11, 1 and 14. The main items on the second component (pain-based) are 27, 28, 24 and 26.
Commonalities with low values (less than 0.3) could indicate that the item does not fit well with the other items loading on the same component. However, all items fit well as none of the items is less than 0.3 (Table 4). The percentage of the variance explained for the two components is 65.2% compared to the 68.8% of the previous three components.
Correlation between the items in the English and Igbo versions of DASH
The correlation coefficient between the items of the English and Igbo versions of the DASH was very high, statistically significant and ranged from 0.888 to 0.995, with item 27 (weakness) having the highest correlation coefficient (r = 0.995; p < 0.001) and item 7 (doing heavy household chores) having the lowest correlation coefficient (r = 0.888; p < 0.001).
Discussion
Adaptation of DASH into Igbo culture and environment was performed following a systematic standardised approach. All the items on the original version of DASH were judged by the experts’ panel to be relevant in clinical research of upper extremity MSDs and for clinicians managing patients with such disorders, living in South-Eastern Nigeria or Igbo land. However, some modifications were made in order to ensure semantic, experiential and conceptual equivalence of the terms and examples in an Igbo environment. 11
This study showed that there is excellent test–retest reliability (ICC = 0.99) of the I-DASH. As expected, this high reliability coefficient is similar to those reported by Fayad et al. 20 of the French version of DASH (ICC = 0.95) and Odole et al., in their study on the Yoruba version of DASH (ICC = 0.96). 14 Portney and Watkins state that a coefficient above 0.75 indicates a good to excellent reliability. 21
Although the ICC for test–retest can be considered excellent, graphic representation of the test–retest scores by the Bland–Altman method revealed that despite a marginal number of outliers, the scores were not all centred, with a systematic trend observed. This graphic representation is consistent with the French version of DASH by Fayad et al. 20
The internal consistency of I-DASH was similar to that of the original English version, Swedish version, Korean version, German version, Spanish version, French version and Yoruba version.14,15,22–28 This indicates that the items on the I-DASH are homogenous and are all assessing different aspects of disability. This supports the alternate hypothesis that the items on the I-DASH would show significant internal consistency (homogeneity). It should be noted, however, that if alpha is too high, it may suggest that some items are redundant as they are testing the same question but in a different guise. 29 A maximum alpha value of 0.90 has been recommended. 30
There was a strong significant correlation between the scores obtained on the E-DASH and I-DASH. This correlation is similar to that reported by Odole et al. in the validation of Yoruba version of DASH and Fayad et al. (French version) with correlation coefficients of 0.99 and 0.78, respectively, indicating concurrent validity.20,28 This suggests that the I-DASH is a valid questionnaire for patients with upper-extremity musculoskeletal disability in the South-Eastern region (Igbo speaking) of Nigeria. The test of difference between the E-DASH and I-DASH revealed that there was no significant difference (p = 0.96) between the two questionnaires indicating that the I-DASH was excellently translated and culturally adapted to the Igbo culture and environment. This is the first item by item correlation of the E-DASH and test of difference with other language versions. It could be of interest to apply this technique to other language versions of the scale to confirm these findings.
PCA, according to Matsunaga, is intimately involved with the question of validity and at the heart of the measurement of psychological constructs. 31 In other words, PCA provides a diagnostic tool to evaluate whether the collected data are in line with the theoretically expected pattern, or structure of the target construct and thereby determines if the measures used, have indeed captured what they are supposed to measure. The choice of PCA was informed by the fact that the scale had already been established on an existing theory by the original authors of the English version and there is no need for exploratory factor analysis.32,33 Kaiser recommends accepting values of KMO greater than 0.5. 16 Values below this should lead to either collection of more data or a rethink of which variable to include. The KMO measure of sampling adequacy was 0.87, which is better than the results from the Yoruba version (0.61) and they are all above the recommended value of 0.6. The Barlett’s test of sphericity was highly significant (χ2 (2724) = 435, p = 0.001) similar to the result by Odole et al. 14 The communalities were all above 0.4, thus confirming that each item shared some common variance with the other items. The factorability of the 30 items on I-DASH was investigated, and this revealed that all the items correlated at 0.5 and above with at least one other item on the scale. This suggests reasonable factorability.34,35
PCA of the I-DASH scale revealed one major factor accounting for 58.37% of the total variance, which was consistent with findings of other authors, in their studies on the Dutch, Japanese, Chinese, French and Yoruba versions of DASH, respectively.25,28,31,36,37 The component matrix of the variables before rotation in this present study revealed that the matrix contains the loading of each variable on each factor. However, all loadings below 0.4 were suppressed in the output. At this stage, two factors have been extracted by Kaiser’s criterion, and the scree plot begins to tail off after two factors before a stable plateau is reached. There was a strong correlation between the two factors (r = 0.60). The rotated factor matrix shows that the questions that load highly on each factor and help us to identify what the construct might be, thus identifying common themes. All items retained in each factor have a high loading (>0.4) in each of the factors. The loading of 22 items were over 0.6 which is similar to the Yoruba DASH with loading of 21 items >0.6. 28 These findings further validate the relevance of all the items on the I-DASH and that there could be two themes in the I-DASH. The loading on factor 1 seems to relate to strength-based items, while factor 2 relates to pain-based items. The sub-themes show that it can actually measure what it is set to measure, which are two sub-components within the 30 components. The Igbo DASH is therefore fit to measure, what it was developed to measure.
The level of disability of the upper extremity among the participants in this study was average (I-DASH score = 55.7) and is similar to that reported by Beaton et al. 15 in a study involving diseases affecting the wrist, hands and shoulders, with DASH scores of 43.9 and also Jain et al. 38 with DASH scores ranging from 21 to 99. 38 The finding of similar scores in the present study supports the linguistic/conceptual equivalence of the I-DASH. 11 However, this is in contrast with the study done by McConnel et al., 39 where the original DASH was administered to 368 patients with different upper-extremity disorders and reported a mean DASH score of 38. The difference in findings could be as a result of the number of patients that participated in the study. It is important to note that the higher the score, the poorer the condition of patients.
Limitations
This work is limited in its scope as it concentrated on concurrent, content and construct validity and some aspects of reliability like temporal stability, internal consistency, equivalent and scorer’s reliability only.
Conclusions
The findings of this study validate the relevance of all the items on the I-DASH. There could be two themes in the I-DASH. The first theme relates to strength-based items, while the second theme relates to pain-based items. Since the DASH has to do with assessing disabilities of the shoulder, arm and hand, the sub-themes show that it can actually measure what it set out to measure, which are two sub-components within the 30 items. This is the first study to provide some psychometric evidence to support the use of the I-DASH. It can be concluded that the Igbo DASH is fit to measure, what it was developed to measure. Clinicians and researchers may use the I-DASH to assess the level of disability and symptoms among Igbo-speaking patients with upper-extremity musculoskeletal conditions in the South-Eastern part of Nigeria. Translation of the DASH questionnaire into other major Nigerian languages should be done to enhance its utility across various cultures in the country. It can be incorporated for use in the management of Igbo-speaking patients with upper-extremity musculoskeletal condition in the South-Eastern part of Nigeria. Further research testing other psychometric properties needs to be done with the Igbo version.
Footnotes
Acknowledgements
We acknowledge all subjects who participated in this study. We would like to thank Mr E.C Okoye and Mrs A.I Amaechi for their assistance during the translation of the questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from all the subjects before the study.
Ethical approval
Ethical approval for this study was obtained from Nnamdi Azikiwe University Teaching Hospital Ethics committee, Nnewi, Anambra State, Nigeria. (NAUTH/CS/66/VOL.7/48)
Guarantor
IB.
Contributorship
POI and ACO conceived the research. POI and ACE researched literature, developed protocol, gained ethical approval, recruited patients. COA was involved in protocol development and gaining approval. POI conducted the data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.