
Abstract
Introduction
Early sensory re-education techniques are important strategies associated with cortical hand area preservation. The aim of this study was to investigate early cortical responses, sensory function outcomes and disability in patients treated with an early protocol of sensory re-education of the hand using an audio-tactile interaction device with a sensor glove model.
Methods
After surgical repair of median and/or ulnar nerves, participants received either early sensory re-education twice a week with the sensor glove during three months or no specific sensory training. Both groups underwent standard rehabilitation. Patients were assessed at one, three and six months after surgery on training-related cortical responses by functional magnetic resonance imaging, sensory thresholds, discriminative touch and disability using the Disabilities of the Arm, Shoulder and Hand patient-reported questionnaire.
Results
At six-months, there were no statistically significant differences in sensory function between groups. During functional magnetic resonance imaging, trained patients presented complex cortical responses to auditory stimulation indicating an effective connectivity between the cortical hand map and associative areas.
Conclusion
Training with the sensor glove model seems to provide some type of early cortical audio-tactile interaction in patients with sensory impairment at the hand after nerve injury. Although no differences were observed between groups related to sensory function and disability at the intermediate phase of peripheral reinnervation, this study suggests that an early sensory intervention by sensory substitution could be an option to enhance the response on cortical reorganization after nerve repair in the hand. Longer follow-up and an adequately powered trial is needed to confirm our findings.
Introduction
Soon after a peripheral nerve injury, the cortical hand map no longer receives sensory input from the injured area. 1 At the end of the reinnervation process after a nerve repair, the cortical hand map presents a spatial configuration that can be totally different from the original one. This process is due to brain plasticity, which includes neurochemical changes, functional alterations of excitatory and inhibitory connections, atrophy and degeneration of normal substrates, sprouting of new connections and reorganization which contribute to the sensory dysfunctions observed in the hand after nerve lesion. 2
A nerve injury in the hand causes a de-afferentation followed by disappearance of the cortical hand representation, with rapid expansion of adjacent cortical territories. This period is termed phase 1 and it lasts about three to four months before the first signs of re-innervation in the hand occur. Phase 2 follows which represents the beginning of the peripheral re-innervation process, when ‘classic’ and late sensory re-education usually begins. 3 Considering the influence of cortical changes after peripheral nerve injury and repair, different strategies for early sensory re-education, applying the concepts of the brain cross-modal plasticity, sensory substitution and integration have been proposed in an attempt to optimize the recovery of sensory function of the hand, still in phase 1.4,5
The use of sensory substitution to provide the brain afferent impulses from visual or auditory sources has a potential basis for the early sensory re-education of the hand. 4 Protocols have shown that the extensive cortical reorganization can be modulated by the brain capacity for visuo-tactile and audio-tactile interactions, during the initial phase following nerve repair. 3
Lundborg et al. 6 developed a sensor glove model, called the sensor glove system, which aims to preserve the cortical map of the hand after peripheral nerve injury. Mendes et al. 7 also developed a similar model of the sensor glove with the same principles, and tested it in healthy volunteers to compare an auditory stimuli training with promised cortical reported results. Both sensor glove models6,7 can during the initial and early stage after nerve repair, when no return of sensibility has yet occurred in the affected area of the hand, give the possibility of hearing the sound generated by the stimulus that the hand should feel. It provides an alternative input to the brain which needs to be interpreted and decoded by the somatosensory area representative of the hand. It has been demonstrated, through functional magnetic resonance imaging (fMRI), that this is an effective alternative pathway to activate the cortical hand map and thus prevent maladaptive cortical reorganization of the somatosensory map, contributing also to better sensory results, related to tactile gnosis, in the long term after injury.1,8–10
The objective of this study was to evaluate and compare the initial cortical responses, sensory and hand function from an early protocol of sensory re-education of the hand with a sensor glove model in patients with median and/or ulnar nerve repairs.
Methods
This is a non-randomized controlled clinical trial and the present study was approved by the local research Ethics Committee.
Participants
This study included patients of both genders, over 18 years old, with an injury of the ulnar and/or median nerves at the wrist or distal forearm level, surgically repaired, within 15 days after trauma, in a tertiary university hospital. All patients had tendon and artery injuries associated with a peripheral nerve injury.
Patients presenting with neurological or systemic diseases, which affected either directly or indirectly the central or peripheral nervous system, or with extensive trauma in the upper limbs were excluded from the study.
The patients selected to participate in the study were allocated into two groups by convenience: those who lived in the same city of the Rehabilitation Center and could come to rehabilitation more often, were allocated to the Training Group (TG) for an early sensory re-education, and those who lived in other cities and could come only for pre-scheduled returns, were allocated to the Control Group (CG). Patients were blinded to group allocation in terms of the intervention.
TG patients underwent three-month early sensory re-education of the hand using the sensor glove model developed by Mendes et al. 7 No home sensory re-education program was used with either group and the CG did not receive early sensory re-education of the hand during these three initial months.
Intervention
Protocol for early sensory re-education of the hand
The early sensory re-education protocol was applied twice a week, always after the rehabilitation sessions, for 15 min for each patient, during the first three post-operative months.
The sensor glove model 7 had mini-microphones attached to a fabric glove, a mini-amplifier and headphones, allowing the individual to hear the sound (amplified) generated by the touch of their fingers in different objects and textures (Figure 1).

Components of the sensor glove model: earphones, miniature microphones, amplifier and glove.
During the cast immobilization period after nerve repair surgery, only microphones were coupled to the volunteer's fingers, without the use of the fabric glove.
The application sequence was as follows: in the initial 5 min, the patient listened to a sound and observed the touch of different textures on the microphones coupled to the fingers. Next, with eyes closed, the patient listened only to the touch sound for another 5 min and, in the final 5 min, the patient tried to identify, still with eyes closed, which texture the listened sound was coming from. As the patient became adjusted to the sensory relearning program and equipment, new textures and objects from day-to-day activities were gradually introduced.
After the early phase of the protocol, once reinnervation was identified by touch threshold testing with monofilaments, all patients were instructed to initiate late phase 2 or ‘classic’ sensory re-education, 3 at home.
Both groups received standard rehabilitation based on motor re-education, oedema and scar management. The treatment adopted in the immediate post-operative period was based on Duran's modified protocol of early passive mobilization for flexor tendon injuries for all patients. 11 All patients received standard programs (supervised and for home) for scar management and progressive active and resistive therapeutic exercises to prevent tendon adhesion and improvement of range of motion and grip strength, until six months after surgery.
Outcomes
Assessment of hand sensory function
The sensory function of the hand (touch thresholds and discriminative touch) was assessed at the first (A1), third (A3) and sixth (A6) months after the nerve repair. The touch threshold test (TTT) was applied with monofilaments and discriminative touch was assessed by static two-point discrimination test (2PD) and the shape and texture identification test (STI™). Disability was assessed by Disabilities of the Arm, Shoulder and Hand (DASH) patient-reported questionnaire. Assessments and scoring were performed according to standardized procedures described by the American Society of Hand Therapy (ASHT), 12 Rosén and Lundborg13,14 and Beaton et al. 15
Assessments were carried out by the same therapist who applied the full protocol, with no blinding procedure.
Functional magnetic resonance imaging exam
At the third post-operative month, all TG and CG patients had an fMRI exam, which was carried out by experienced technicians, and always in the researcher’s presence.
Image acquisition
Images were acquired in a Philips Achieva 3T MRI equipment (Best, Holland). The exams included one structural T1-weighted image acquisition and functional echo-planar acquisitions during two sensory tasks. One of the tasks was called ‘tactile task’, and the other, ‘auditory task’; both were accomplished in four blocks of stimulation interspersed with five blocks of rest; each block lasted for 30 s.
The tactile task was carried out as follows: in the exam room, the researcher stood up next to the volunteer and in the task blocks applied a stimulus with a stick lined with a rough texture on the volar area of the second finger for median or both nerve repair or fifth finger for ulnar nerve repair. For synchronization between tactile stimulation and the task block, throughout the exam the researcher would view a monitor screen, which indicated the exact moment to start and stop the stimulation.
As for the auditory task, it was carried out from the transmission of a recording of the sound generated by touching the rough texture to the volunteer. The recording was transmitted during the exam to the earphones used by the volunteer also in synch with the task blocks.
The whole synchronization of the tactile and auditory stimulations with the corresponding task blocks was intermediated by the Esys (Invivo, USA) system.
Thus, structural images were acquired using a gradient-echo 3D (GRE) type sequence, T1 weighted (TR = 7.2 ms, TE = 3.3 ms and 8° rotation angle), FOV 240 × 240×180 mm to totally cover the head and with a sagittal orientation to optimize the acquisition array. The array dimensions were 240 × 240×180 mm to ensure a 1 mm isotropic resolution, thus generating 180 sagittal sections. A high Turbo Field Echo factor (TFE = 240) and a SENSE = 2 factor was defined; therefore, the total sequence time was 4 min 13 s. Two sets of functional images of the Echo Planar (135 volumes) type with TR = 2000 ms, TE = 40 ms were also acquired, with 30 sections 4 mm wide and with no spacing, to cover the whole brain, with an intraplane resolution of 1.8 mm and a 128 × 128 array.
Image processing
The functional images were processed using the software Brain Voyager™ QX 1.8 (Brain Innovation, Maastricht, the Netherlands) and the plugins (GCM 2.5 and Cluster Threshold Estimator). Images were pre-processed for motion correction and enhancement of the signal-noise ratio by applying a tri-linear interpolation, a 4 mm full-width at half-maximum Gaussian spatial filter.
Statistical analysis
Sensory function
A comparison between groups was performed by a blinded person, at one month as baseline, and at three- and six-month follow-up using Mann–Whitney test (p < 0.05).
fMRI
An experienced blinded assessor conducted image analysis. The association among BOLD signal oscillations in different cortical areas over time was checked by performing a difference Granger Causality Map (dGCM).
Granger Causality mapping indicates whether the signal in a brain site (seed region) is useful to predict signal variations in other locations. 16 For this analysis, the reference area chosen (seed region) was the Brodmann 3 area (BA3), at post-central gyrus, that includes the somatosensory hand representation area in the brain cortex. After calculating Granger’s causality generated the differential maps for each group and tested against zero (p < 0.01, corrected). Resulting regions-of-interest (ROIs) served as probes to verify Granger values and, again, to compare between groups (t-test, bicaudal, p < 0.05).
Granger’s causality positive values indicate that the activity in a cortical area succeeds the activity occurring in seed region; negative values indicate that the activity in the areas in question precedes the activity occurring in the seed region. 16
Results
Trial participants
A total of 33 patients met the inclusion criteria; 16 patients dropped out of the study by non-attendance and 17 were included in the final sample. The TG had eight patients and the CG nine patients. Three patients (two from TG and one of CG) were excluded from fMRI analysis due to the presence of motion artefacts at the images and four patients from CG quit the final sensory evaluation and were excluded from sensory function analysis as shown Figure 2.

Flowchart of participants.
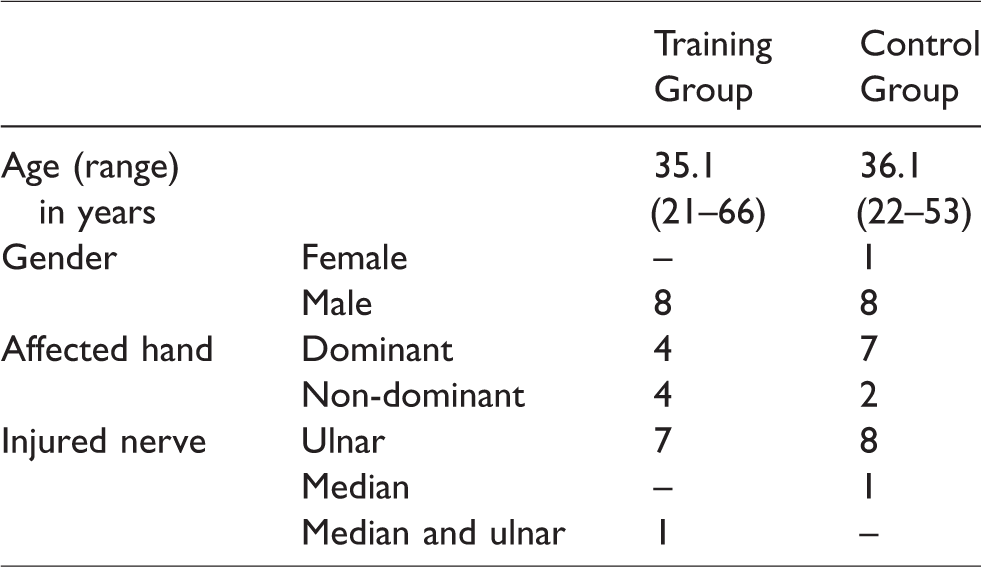
A description of the sample based on age, gender, affected hand and injured nerve is shown in Table 1.
Baseline data of study sample.
Sensory function
At the first month, at baseline evaluation, patients from both groups presented poor results related to touch threshold test, discriminative touch tests and high scores in DASH questionnaire, indicating substantial disability in that period after the nerve injury and repair.
Over time, in the comparison between groups, there were no statistically significant differences between groups at any timepoint and for any sensory test or DASH questionnaire (Table 2).
Median outcomes (min–max) and differences at first (A1), third (A3) and sixth (A6) month after nerve repair.

2PD: two-point discrimination; STI: shape and texture identification; DASH: Disabilities of the Arm, Shoulder and Hand.
Cortical responses
In the TG patients, during the auditory task, Granger's Causality mapping indicated that lower temporal gyrus (BA21); right supramarginal gyrus (BA40, BA13 and BA3); right lingual gyrus (BA18) and upper right frontal gyrus (BA10) were effectively connected with BA3. For the CG patients, medial cuneus (BA19), left fusiform gyrus (BA37) and left insula (BA13) presented effective connectivity with BA3. Then, during auditory stimulation in TG patients, effective connectivity of BA3 with secondary and tertiary associative areas of the brain cortex were observed, related for instance to the auditory process and recognition memory (BA21), executive functions and working memory (BA10), image interpretation (BA18) and phonological relationships (BA40). 17 All areas, except BA40, presented negative Granger's causality values, indicating that cortical activity in those regions preceded the activity in BA3. In CG patients, areas related to image processing, semantic and phonological relationships (Insula, BA19, BA37) presented effective connectivity with BA3, always with positive Granger's causality values, indicating that the activity in BA3 preceded it or Granger-caused the activity in those areas. 17
During tactile stimulation, we observed effective connections between BA3 and areas such as the cerebellum (uvula) and thalamus (pulvinar), whose activity succeeded the activity occurring in the somatosensory cortex in trained patients (TG). We also observed effective connections between BA8, whose activity preceded that one occurred in BA3. All those areas are related to the onset of motor responses, since the thalamus is a mandatory way for the structural connection of the somatosensory pathways. For the CG, during tactile stimulation, we also observed effective connectivity between BA3 and the contralateral pre-central gyrus (BA6), also related to the planning of motor routines. 17
Granger's causality values (dGCM) for each group and task are shown in Tables 3 and 4.
Granger’s Causality values (dGCM) during auditory task in ROIs effectively connected with BA3 and comparison of the dGCM values founded in these areas for each group (t-test, p < 0.05).
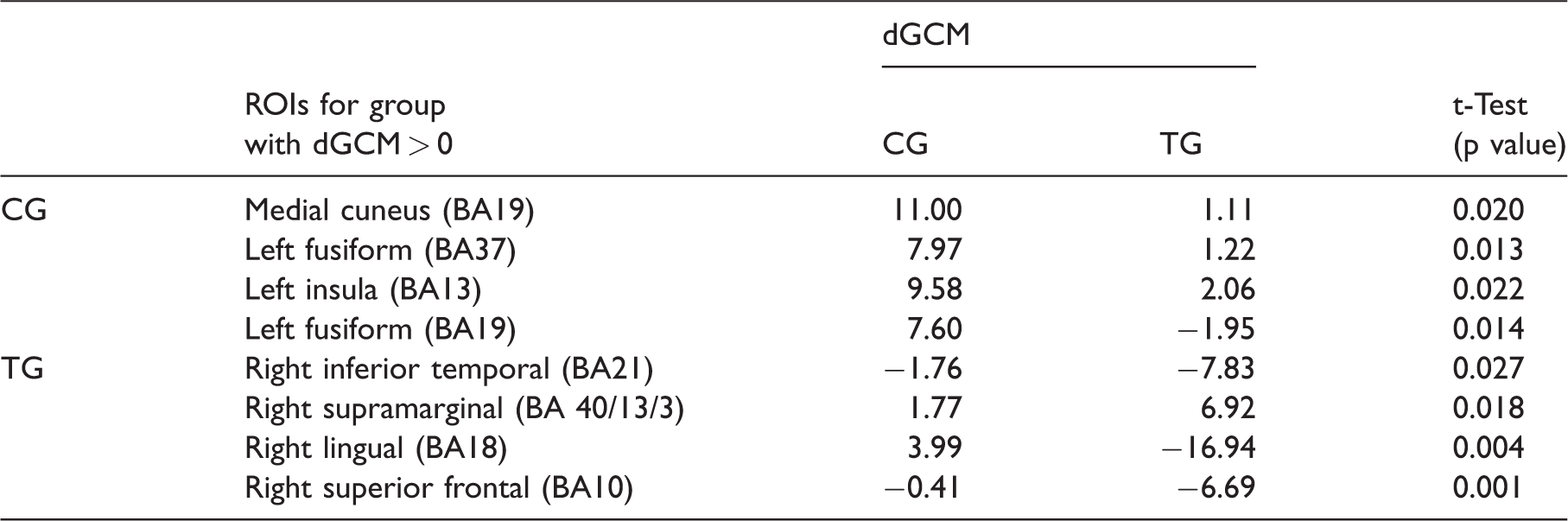
dGCM: difference Granger Causality Map; CG: Control Group; TG: Training Group; ROIs: regions-of-interest.
Granger’s Causality values (dGCM) during tactile task in ROIs effectively connected with BA3 and comparison of the dGCM values founded in these areas for each group (t-Test, p < 0.05).
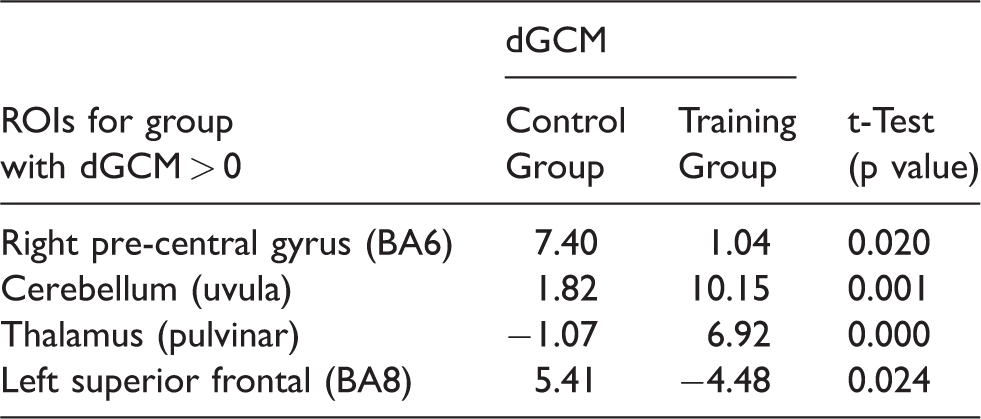
dGCM: difference Granger Causality Map; ROIs: regions-of-interest.
Discussion
Patients undergoing early training with the sensor glove auditory stimulation protocol presented a more specific connectivity and directed towards the auditory task, between BA3 and other cortical areas, leading to the formation of neural networks related to more complex cognitive processes in those patients. Therefore, it seems that in trained patients, a greater engagement occurs between the associative areas of the cortex, which indeed relate to the auditory stimulation and to the area of cortical projection of the hand in BA3. There seems to be an association between the audio-tactile training used in this study, and the cortical responses to the auditory stimulation, involving the BA3 and the frontal cognitive areas. Besides no direct activation of the cortical area of representation of the hand in BA3 by auditory or tactile stimuli during fMRI exam, yet, Granger's causality analysis allowed the identification of this effective connectivity initiated during each stimulation mode (tactile or auditory) and thus the major differences between the groups relate to the cortical areas which effectively connect with the BA3 somatosensory area. Conversely, patients in the control group presented effective connectivity with primary cortical areas in the auditory task and this was a non-specific response to this type of stimulation.
During the tactile task, in spite of the sensory stimulation, a connection between BA3 and the areas related to motor planning was observed in patients from both groups. This was an expected result in view of the fact that, during the third post-operative month, after a complete peripheral nerve injury at the wrist level, most of the patients were still unable to detect or identify such a stimulus. 18 The connection between BA3 and areas related to the planning of motor responses might also be related to minor finger movements that occurred during such stimulation mode, which, when captured by the articular receptors, triggered a sequential cortical response.
Previous studies also assessed cortical activity by fMRI in patients with different nerve lesions and exposed to some kind of auditory stimulation training such as sensor glove system or similar devices.8,9,19,20 All of them applied different types of training with auditory stimuli and studies differed in terms of time after injury, duration or frequency of stimulation patterns during the fMRI exam, making it difficult to compare the results. Nonetheless, in all these studies it was observed in those individuals who were trained that there was a relationship between plastic cortical changes in the hand representation area and auditory stimulation.
Our study did not demonstrate any significant improvement related to the recovery of touch threshold, tactile gnosis or disability outcomes after three-month protocol of early sensory re-education of the hand with a sensor glove model, neither after six months of follow-up. Considering a nerve outgrowth rate of 1 to 2 mm per day in humans, nerve injuries at wrist level may require three to four months until the first signs of reinnervation can be observed and an even longer period to tactile gnosis recovery.3,18 So, probably we observed only short-term outcomes in this study at the beginning of phase 2 of re-innervation process 3 and longer follow-up is necessary. Rosén and Lundborg, 10 in a randomized controlled clinical trial, found only after a 12-month follow-up a significant improvement in tactile gnosis of patients that used their sensor glove in the early period after nerve injury and repair at the wrist level. However, at six months, they found 10 similar results to our study, corroborating our findings. The main difference between the studies was the frequency of training with the sensor glove. Rosén and Lundborg 10 proposed a daily-based training; in our study, the participants trained only twice a week with the sensor glove model. To have more control over the sensory re-education protocol, the TG patients used the sensor glove only in the research environment, so the frequency of training was restricted. This training frequency might have influenced the cortical responses to our early protocol of sensory re-education of the hand. Although, we did follow a standard regime based on clinical practice. 21
Our sample consisted mostly of median and ulnar nerve repair, representative of this kind of trauma with high incidence in young males globally.22–26
Limitations
Despite promising results of this study, the following limitations should be considered. The small sample size, the non-randomization of the participants that could complete the proposed protocol, the patients' training frequency with the sensor glove model and the short-term follow-up may explain why we did not observe any significant change in sensory results. Our patients were referred from several towns, to the University Public Hospital, which is a regional centre for hand trauma, and treats patients with lower incomes. A further limitation is the outcome measures we used. We could have used the STI™ and 2PD tests and calculated the Rosén score, a composite impairment score for nerve repair.27,28
Implications for practice and future study
The glove system is not yet an available tool in rehabilitation for clinical practice. Nevertheless, its principles should be added as an early approach still in phase 1 of sensory relearning for maintenance of the cortical representation of the hand by brain plasticity, before peripheral reinnervation. In a previous study, Mendes et al. 9 also found signs of cortical audio-tactile interaction after use of the same sensor glove model in subjects without sensory loss, but, in that case, the training was daily, for seven days, 15 min each. Whilst none of the models of the sensor glove are commercially available yet, a home program of sensory re-education of the hand using simple techniques may be necessary to increase cortical sensory input in the early postoperative period in order to stimulate and preserve the cortical map of the hand. Some of these simple techniques use the same principles of cortical audio-tactile integration and other use visual-tactile integration like mirror training, sensory imagery and observation of touch.18,29–32
Systematic reviews remain inconclusive on what are the best techniques of sensory re-education of the hand and highlight the need for more high-quality studies to define protocols for each recovery phase after surgical repair of peripheral nerve injuries. Finally, documentation of outcomes also needs standardization in order to compare treatments and clinical findings.33,34
As protocols are standardized and tested by a larger number of participants, it will be possible to investigate how audio-tactile integration occurs after early sensory re-education of the hand using sensor glove models or similar equipment and/or stimulation.
Conclusions
In this study, patients undergoing surgical repair of median and/or ulnar nerve traumatic injuries and trained with a sensor glove model in the early post-operative period showed more complex cortical responses to the auditory stimulation than untrained patients, They also, presented a more specific effective connectivity between the cortical area of representation of the hand and cortical associative areas indicating some type of cortical audio-tactile interaction. In terms of clinical findings and recovery of sensory function, after three-month training with the sensor glove model in the early period after nerve injury and after six months of follow-up, no differences between groups were observed.
Footnotes
Acknowledgements
The authors would like to give special thanks to Birgitta Rosén and Anders Björkman for the valuable feedback during the discussion about the results of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received financial aid from the Foundation for the Support of Teaching, Research and Assistance of the Faculty Hospital (FAEPA) and from the Foundation to support the research of the state of Sao Paolo (FAPESP).
Informed consent
Written informed consent was obtained from all subjects before the study.
Ethical approval
Ethical approval was obtained from: Research Ethics Committee from the University Hospital, Faculty of Medicine of Ribeirão Preto, Brazil (HCFMRP/USP – 6393/2011).
Guarantor
Raquel Metzker Mendes.
Trial registration
Contributorship
RMM, CR, CEGS, NM, and CHB conceived the study. RMM also recruited the patients, applied the protocol and collected data. CR analyzed fMRI data. RMM, MCRF, and RIB wrote the first version of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.