
Abstract
Introduction
Proprioceptive assessments of the wrist inform clinical decision making. In wrist rehabilitation, joint position sense has emerged as one way of assessing conscious proprioception with varying methods and minimal psychometric analysis reported. The purpose of this study was to standardise the wrist joint position sense test method for clinical use and to determine its test–retest reliability in a healthy population.
Methods
Four wrist positions (20° and 45° flexion, 20° and 45° extension) were measured twice in a random order, by a single rater, using a universal goniometer on the same day. The absolute error in degrees between each position and reposition was calculated. For relative reliability analysis, the intraclass correlation coefficient (3,1) was calculated. For absolute reliability the standard error of the measurement was calculated and Bland–Altman plots visually inspected.
Results
Fifty-five healthy volunteers (mean age 31.1 SD±10.25 years) were assessed. The mean absolute error, summarised for all positions for test and retest, was 3.98°. The intraclass correlation coefficients were poor to fair (0.07–0.47), and standard error of the measurement was 2° (rounded) for all positions. The limits of agreement were fairly narrow, and the Bland–Altman plots showed random distribution of errors for each position, therefore the measurement error was clinically acceptable.
Conclusions
The active wrist joint position sense test using goniometry demonstrated poor to fair test–retest reliability and acceptable measurement error in healthy volunteers. The wrist joint position sense angle of 20° flexion was the most reliable.
Introduction
In rehabilitation, using psychometrically sound measures is an important aspect in delivering best practice. There is a constant challenge to use standardised tests with known reliability, validity and responsiveness. 1 Initial testing of a new measure is usually advocated on healthy volunteers, and reliability is a prerequisite to validity. 2 Investigating reliability of assessments is needed to ensure reproducibility in repeated trials on the same individuals3,4 and to determine whether the measurement error is small enough to detect clinical changes. 5
Proprioception is the perception of movement, posture and joint position, acknowledged as three senses: the conscious sensations of joint position awareness and kinaesthesia relating to joint movement detection as well as the unconscious sense of neuromuscular control pertaining to activation of dynamic joint restraints in response to joint position and anticipation of joint motion.6–8 Proprioceptive mechanisms are complex and still not completely understood. 7 However, evidence suggests that ligament mechanoreceptors influence proprioceptive reflexes mediated by the central nervous system.9–12
Over the last decade there has been growing support for proprioceptive and sensorimotor rehabilitation in hand therapy.6,7 This has been driven by increasing knowledge and understanding of the proprioceptive pathways and their role in dynamic stability 6 and related disturbances found in populations with wrist conditions such as osteoarthritis (OA), 13 instability, 14 distal radius fracture (DRF) 15 and age-related muscle weakness.11,16
Wrist instability results in an inability to bear physiological loads and is associated with a loss of normal carpal alignment. 17 Functional joint stability involves static stabilisers including normal joint surfaces, ligaments (often manipulated in surgery) and muscles supporting dynamic proprioceptive mechanisms. 9 In the wrist the scapholunate interosseous ligament, dorsal intercarpal and radiocarpal ligaments have been shown to be highly innervated.18,19 Consequently, any disruption to these structures, from wrist injury or OA, will result in proprioception disturbance.6,13,14 This forms the basis of proprioceptive rehabilitation used in addition to, or instead of, surgery for enhancing wrist stability.6,11,20
An unpublished UK therapists' scapholunate injury management survey (led by the Pulvertaft Hand Centre) reported 39% (of 72) wrist pain specialists assess proprioception, although only 35% explained how by measuring joint position sense (JPS). Interestingly, however, 82% completed proprioceptive rehabilitation. This demonstrates proprioceptive rehabilitation is gaining clinical credence, even though wrist joint proprioceptive assessments are still in their infancy.
Measurement of proprioception has been widely investigated in peripheral joints such as the knee,12,21 ankle, 22 shoulder23,24 and elbow. 25 However, there are few studies in the wrist and hand.16,26,27 Present methods of proprioceptive testing at the wrist include kinaesthesia requiring lab-based sensors and JPS assessment.6,11,28
JPS is defined as ‘the conscious sensation of joint position’ and, for measurement ‘the ability to accurately reproduce a specific joint angle’. 6 The magnitude of error is generally accepted as being a useful proprioceptive acuity indicator.8,29
No ‘gold standard’ for assessing wrist JPS has been reported in the literature. The earliest studies testing wrist JPS used custom-made jigs30–32 or laboratory-based sensors and equipment 33 which reduced clinical setting transferability. Hagert 6 discussed a more clinically applicable concept of measuring position–reposition accuracy via manual goniometry. Position and repositioning can be assessed passively (the subject moved by operator) or actively (the subject moving independently).6–8,28
The concept was then investigated by Karagiannopoulos et al. 15 on 24 DRF patients and matched controls as part of a sensorimotor assessment. Although they reported high intra-rater reliability (intraclass correlation coefficient (ICC)= 0.85) they only tested JPS at 20° extension on a single occasion.
Only one published article has investigated test–retest reliability of wrist JPS (termed joint position error) 34 ; JPS was measured three times on two occasions. Their goniometry method lacked detail and no power calculation was reported. In the 25 healthy volunteers studied, JPS error was demonstrated to have poor to good test–retest reliability (ICC= 0.11 for 45° flexion, ICC= 0.58 at 45° extension). 34
Both Khamwong et al. 34 and Karagiannopoulos et al. 15 found varying wrist JPS reliability despite using passive position active reposition methods that are common practice in JPS testing in a clinical setting.6–8 It is difficult to separate and evaluate the specific attributing factors as both studies investigated JPS simultaneously with other tests causing potential proprioceptive interference. 8 In addition, the reliability findings are potentially influenced by and challenging to compare due to variation in reliability type, JPS test method, position angles and populations studied. To the best of the authors’ knowledge no previous study has reported reliability of wrist JPS in isolation in a healthy adult population across a variety of angles.
The primary aim of this study was to create a standardised wrist JPS test protocol utilising goniometry measurement, selected for clinical utility. The secondary aim of this study was to determine if the wrist JPS test had acceptable test–retest reliability in healthy adults (ICC >0.75 as considered excellent, according to guidelines by Fleiss 35 ).
Methods
A test–retest experimental study design was undertaken to examine wrist JPS reliability, between two trials on the same day, of four wrist positions measured twice in a random order, by a single rater. Ethical approval was obtained and all participants gave informed written consent.
Study sample
To provide a desired confidence interval (CI) width of 0.2 around an ICC of 0.8, in two-way ANOVA models a sample size of 55 was needed. 36 Participants were recruited via posters displayed at the authors’ work locations.
Inclusion criteria were set to reduce known proprioceptive or JPS influences reducing sampling error by increasing heterogeneity. 7 Inclusion criteria were age 18–50 years, able to comprehend verbal and written English, no existing pathology (arthritis), no previous wrist injury or pain in the last two years, no neurological disorders or traumatic or post-surgical conditions involving the upper limbs.
Rater
The study was performed by a registered and chartered physiotherapist (CP) with 13 years postgraduate and nine years hand speciality experience. To reduce rater recall and analysis bias, separate test–retest trial record sheets were used. Data entry and analysis occurred after data collection was completed.
Wrist JPS test protocol rationale
Standardisation of the wrist JPS test was undertaken using available literature on goniometry and understanding of JPS influences. In line with other JPS studies15,23,30,34 a passive position–active reposition method was used.
Ipsilateral position–reposition is the most commonly found method in JPS testing.12,15,24,26,30,34 This reflects ipsilateral proprioceptive pathways including local receptor stimulation6,11 and may reduce influence from central unconscious feedback control.9,10
Wrist target positions of 20°, 45° flexion and 20°, 45° extension were selected as representative of functional mid and inner ranges 37 and to enable comparison with previous wrist JPS studies.15,34
Rest between test and retest was dependent on participant availability with a minimum time difference of 10 min and maximum within the same day. To minimise order or learning effects, randomisation of wrist position test order was undertaken, using a computerised random numbers generator 21 prior to data collection. The allocation concealment was provided by opaque sealed envelopes 2 held in a locked cabinet accessible only by the rater during testing. Participants were blinded to the wrist position test order.
Instrumentation
Wrist joint angles were measured using a plastic Jamar® goniometer with a 360° central scale marked in 2° increments and two 8 cm arms. The arms were long enough to allow accurate measurement but reduce sensory interference.
Volar–dorsal goniometer placement is American Society of Hand Therapists recommended 38 and is the most reliable method for wrist extension–flexion.39,40 To ensure consistent measurement, the capitate 39 provided the midcarpal and radiocarpal joint axis marker with the goniometer arms parallel to the radius and middle finger metacarpal. 38
Wrist JPS test procedure
Each participant sat facing a narrow hand table opposite the rater. Test instructions and demonstration were given. A blindfold removed visual cues 29 and was placed over the participants’ eyes prior to the allocation of the random test positions.
The dominant side was measured with the elbow approximately 90° flexed resting on the table, forearm vertical6,15 in mid-pronation and fingers relaxed. 38
During passive target positioning with goniometry alignment, rater contact with the volunteers’ hand and wrist was minimal, followed by a 3 s hold to allow the volunteer to memorise the position. A verbal prompt of ‘concentrate on the position of your wrist and hand in space’ by the rater was given. The volunteer returned their wrist to a neutral position before actively repositioning in the target position. The angle was measured and recorded by the rater to the accuracy of 1° (Figure 1).

Goniometry measurement of wrist JPS.
Data analysis
There is controversy in the literature on how best to calculate reliability or measurement error, 4 with a single analysis being insufficient.5,41 Therefore, relative and absolute reliability measures were calculated.
Wrist JPS angle was expressed as absolute error (AE), the difference in degrees between the target and reposition angle, because it is more reliable than constant error in JPS testing 25 and is consistent with other wrist JPS studies.15,34 Mean AE was calculated from the two measurements for test and retest for each wrist JPS angle separately.
Test–retest relative reliability was assessed using ICCs, traditionally determining test stability.
42
Specifically, ICC type 3,1 a two-way mixed ANOVA with absolute agreement was applied, as the test angle was the only test angle of interest (fixed variable) with the focus on random error (volunteers random variable).43,44 Ninety-five per cent CIs were calculated, indicating precision.
1
It is recognised that ICCs can be positively influenced by high interperson variability despite poor test–retest consistency error,
41
therefore further reliability analysis was undertaken. Standard error of the measurement (SEM) formula was used to provide an absolute index of reliability.
41
SEM is expressed in actual units not influenced by between-subject variability.

In addition, Bland–Altman plots and 95% limits of agreement (LoA) between the mean AE for test–retest for each test angle were drawn to provide a visual indication of measurement error.5,45
The statistical analysis was undertaken using Statistical Package for Social Sciences Version 12.0 (SPSS Chicago IL).
Results
Fifty-five healthy volunteers, 37 females and 18 males, with a mean age of 31.1 years (SD = 10.25 years) completed the study. Forty-four (74.5%) were right hand dominant. All data were collected on seven separate days in two University of Nottingham facilities (City Hospital, Nottingham and Royal Derby Hospital, Derby). The median test–retest time interval was 24 min (interquartile range 19–34 min).
The mean AE and SD for test and retest for each position angle, mean difference between test–retest and related reliability statistics of ICC and SEM are presented in Table 1.
Test and retest absolute error and reliability statistics for each wrist JPS position angle.
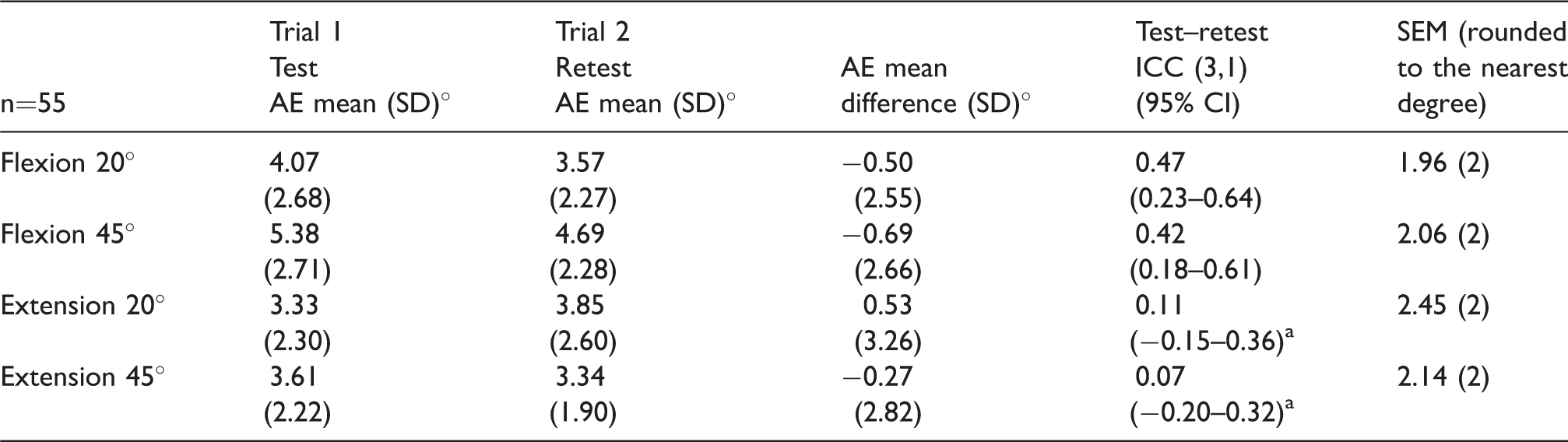
AE: absolute error; CI: confidence interval; ICC: intraclass correlation coefficient; SD: standard deviation; SEM: standard error of the measurement.
aThe ICC confidence intervals with minus values are out of range but are reported as SPSS calculated, for completeness. A value of 0 should be given in these cases. 44
The mean AE summarised for all position angles was 4.10° (SD 2.61°) for test and 3.86° (SD 2.33°) for retest. The mean AE improved (decreased) for all position angles between test and retest by a mean difference of −0.27 to −0.69° except for 20° extension which increased (0.53°) (Table 1). The ICCs ranged from 0.07 to 0.47 indicating very poor to fair relative test–retest reliability 35 with moderately wide CIs indicating low precision (Table 1). For example, the true ICC at 20° flexion lies between 0.23 and 0.64 with 95% certainty. The SEM was 2° rounded to the nearest degree for all position angles indicating the true AE being ±3.92° at 95% confidence (±1.96 × SEM). 41
Bland–Altman plots are presented in Figure 2(a) to (d) with upper LoA ranging from 4.60 to 7.06° and lower LoA ranging from −5.60 to −6.01°. The angle of 20° flexion has the narrowest LoA (4.60 to −5.60°). The mean difference between retest and test mean AE for all position angles has less than 1° negative bias except for 20° extension with a positive bias (0.53°). On visual inspection of the Bland–Altman plots (Figure 2(a) to (d)) there is no clear association between the retest–test differences and the mean of the test–retest position angles.
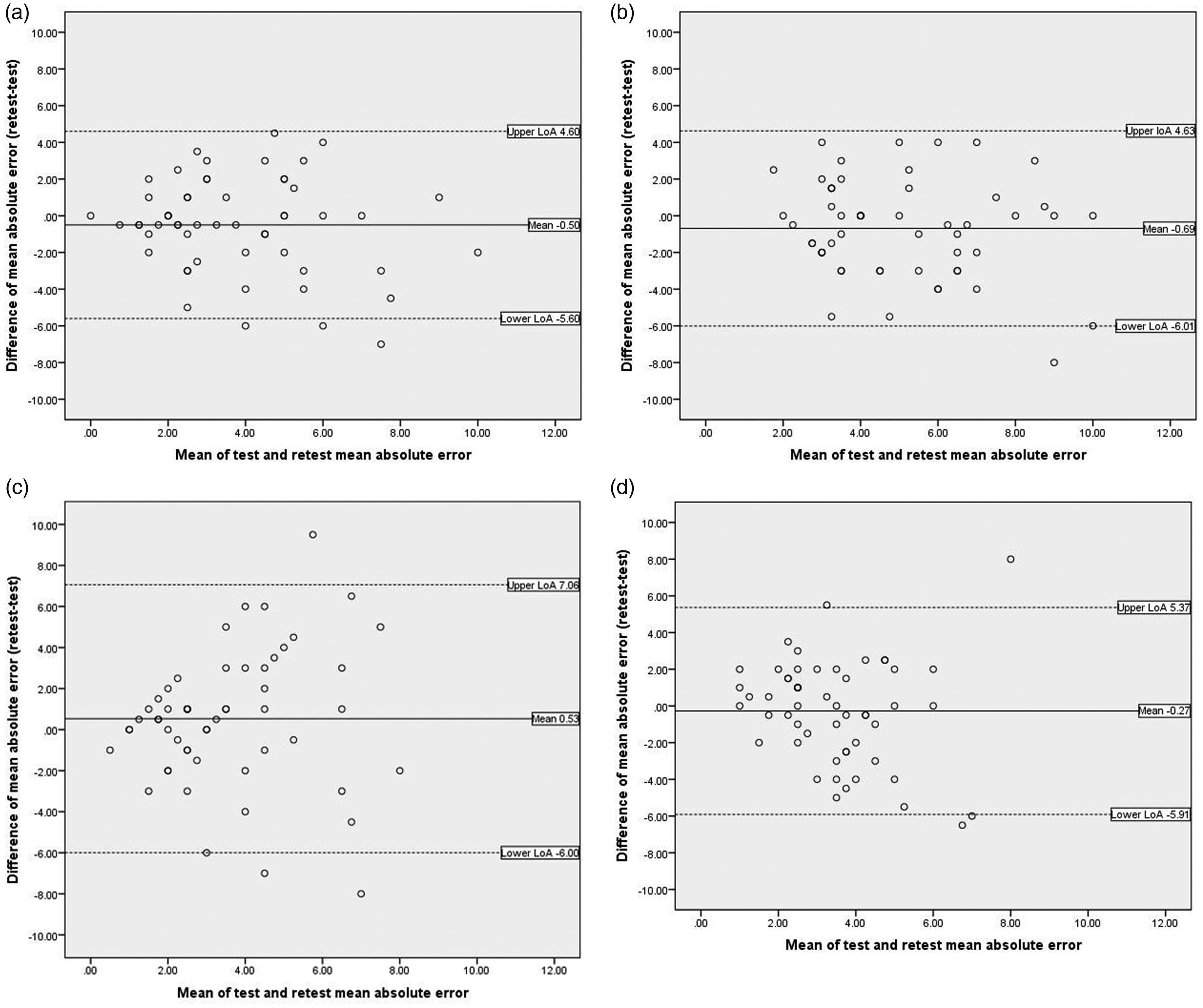
Bland–Altman plots for each wrist JPS position angle. Bland–Altman plots to illustrate the relationship between mean test and retest mean AE against the differences in retest–test mean AE at (a) 20° flexion, (b) 45° flexion, (c) 20° extension and (d) 45° extension. Solid line: the mean difference of the AE of the retest against the test (−0.50°, −0.69°, 0.53°, −0.27°, respectively); dashed line: the 95% LoA (−5.60 to 4.60°, −6.01 to 4.63°, −6.00 to 7.06°, −5.91 to 5.37°, respectively).
Discussion
This study demonstrated variable test–retest reliability for the wrist JPS test over four position angles in a convenience sample of healthy volunteers. The initial aim was to determine a standardised method for testing wrist JPS using goniometry. The second aim was to determine test–retest reliability.
Methodological differences and complex interactions in the sensorimotor system make attribution of JPS measurement variation across studies challenging. 7 The main contributors of AE and reliability variations in this study are considered to be heterogeneity in population, method of JPS testing and goniometry measurement.
A strength of this study was use of a sufficiently powered sample. However, a wide age range of 18–50 years may have reduced the relative reliability by limited clustering of volunteers’ mean AEs 41 reducing the ability to discriminate between volunteers, 46 despite the age parameters being set to avoid age-related JPS decline. 47 There is some evidence to suggest JPS error may increase earlier than age 50 in healthy populations shown in the ankle 22 and elbow. 29 In the hand, Kalisch et al. 16 showed significant age-related decrease in JPS between groups of 45 healthy volunteers (young adults 20–30 years, adults 33–63 years and 66–79 older adults).
A surprising finding was that our mean wrist JPS AEs at 20° extension for both trials were higher (3.33°–3.85°) compared to 2.87° in 24 healthy adults over 50 years reported by Karagiannopoulos et al. 15 when completing the same test. This suggests that age may not influence test ability. Their subsequent work reports mean AEs of 10.82° at baseline and 3.65° at 12 weeks after rehabilitation in 33 DRF patients, concluding that active wrist JPS test measured at 20° extension is responsive to change. 48 No wrist JPS AEs for the other angles tested in this study are reported in the literature.
In this study, standardising the wrist JPS procedure (position, instructions given, use of a blindfold and randomised order of target positions) reduced the risk of variation between test and retest conditions. Our low mean AE retest–test differences support this condition control; however, the small improvement over three position angles may indicate an overall learning effect. Reliability studies regularly employ practice trials to stabilise learning effect, test understanding and performance before measuring.23,25,29,42
Muscle fatigue has been reported to adversely influence muscle spindle activity with significant decrease in primary afferents 49 and increasing limb position and movement and therefore JPS error in human shoulders 50 and elbows. 51 In this study the time differences between test–retest were wide (minimum = 10 min and maximum = 300 min) and this may have increased the variation in fatigue affects and subsequent JPS AE between volunteers. Potential learning effects attributed to a small test–retest time difference were mitigated by randomising the order of target positions.
Relative reliability ICC values for both flexion position angles are markedly higher than the extension angles and all values are lower than 0.75, in the present study. This is in contrast to poor test–retest wrist JPS reliability (ICC −0.11) at 45° flexion and good reliability (ICC 0.58) at 45° extension as found by Khamwong et al. 34 They calculated the ICC from a mean of three measurements taken on two occasions within a 24 h period in 25 young healthy volunteers. JPS was tested alongside eight other wrist measures including active movement and grip strength that all produced ICCs over 0.85. 34 From their minimal description, the main difference in JPS method in comparison to this study is angle test order which was flexion followed by extension and may indicate a learning effect reflected in their ICCs.
Test–retest reliability of JPS has also shown variability when consecutively testing more than one position angle in the knee 21 and the elbow 25 in healthy populations, where high reliability is expected. Multiangles reproduction has been reasoned to require more attention, 34 creating a possible concentration fatigue effect.
Measuring proprioception via JPS ipsilateral testing heavily relies on subject memory to replicate the position angle8,29,52 but has been shown to have lower AE compared with contralateral testing that requires interhemispheric transfer. 29 We have no reason to believe our healthy volunteers had memory issues; however, testing different angles consecutively is likely to be inherently more difficult than testing a single angle and is reflected in the moderate AE across all positions (3.33–5.38°).
Karagiannopoulos et al. 15 demonstrated excellent intra-rater reliability (ICC 0.85) on investigation of a single angle (20° extension) in 24 DRF patients and matched controls. CIs were not reported. To allow intra-rater reliability comparison to this study an ICC of 0.42 was calculated for 20° extension, from the two test trial measurements. These intra-rater reliability results further support higher ICCs and lower AEs when testing single JPS angles.
Many JPS protocols use three to five measurements. 8 Higher ICC values have been demonstrated in the shoulder with three measurements (ICC 0.978) 24 and in the metacarpophalangeal joint with five measurements (ICC 0.92). 31 In this study, with only two measurements per angle any lapse in concentration could greatly influence the mean AE and risk large within-subject variability, potentially contributing to the low test–retest ICCs.
In considering position angle influence on reliability, outer ranges are reportedly more reproducible providing an overstretch protective mechanism12,53 possibly from cutaneous receptor influence at end of joint range. 9 This is supported in the knee with extreme test angles producing the lowest AE. 22 Khamwong et al. 34 reported their use of mid-range wrist positions may have contributed to low reliability due to lower joint mechanoreceptor firing rates and small change detection difficulty. Karagiannopoulos and Michlovitz 54 advocate testing wrist JPS at 20–30° extension due to it biomechanically providing optimal joint stability quoting a cadaver study. 55 Furthermore, they recommend not using outer range, stating that joint tissue strain may affect sensory feedback. This is not supported in Patterson et al.’s 32 study on wrist JPS, which measured seven specific flexion/extension angles in control volunteers with a custom-made jig; results indicate lowest AE neutral and 60° extension (1–3°). Furthermore, in two studies investigating knee JPS in pathological populations, one found no statistical difference in ICC between 20 and 60°, 53 and another reported lower ICC at 10° compared to 60° flexion. 56 It is unclear if these findings are joint specific or range related. This study’s results demonstrated similar ICCs and mean AE for inner and mid-range angles. However, it is worth noting the flexion angles have the higher ICC but higher AE, and in extension angles the opposite is true. This indicates that flexion angles have more relative reliability but poorer angle replication accuracy.
A critical review of proprioceptive methods 8 suggests active JPS repositioning has greater fusimotor activity and sensory feedback, predominantly from muscle spindles compared to passive positioning where cutaneous receptors provide most feedback. Second, active target repositioning is free where there is a physical stop on passive positioning, causing a mismatch in sensory feedback. Consequently, active positioning–repositioning has demonstrated significantly lower AE than passive in the knee, 53 shoulder 57 and hand, 28 and slightly lower AE (although not significant) in the wrist for both test (anaesthetic block) and control volunteers. 33 Studies support muscle spindles have reduced signalling in static positions 58 with joint and skin receptors stretch mechanisms responding to movement over position. 11 An efferent motor command is used to inform future positioning 52 and is influenced by estimation of movement extent interpreted by movement type and speed. 29 Motor command signals have been investigated in the hand to signal even when movement is prevented 59 and muscle contraction reduces JPS accuracy at the wrist but interestingly not at the elbow. 60 Therefore, during wrist JPS testing the movement component and muscle activity (during the three second hold) may affect error accuracy. However, it is unclear if some of these findings on JPS method are joint specific. Passive position with active repositioning is regularly used in JPS testing 29 and specifically at the wrist.15,34,48 The impact of this method is unknown, but may have contributed to the mismatch in mean AE and ICC scores we found and supports future active position–active reposition investigation of the wrist JPS test.
To gain appreciation of measurement error magnitude, absolute reliability or agreement was considered. The SEM was relatively low at 2° and the Bland–Altman plots show minimal AE bias, less than 1°, and moderate LoA between test–retest across all position angles. Khamwong et al. 34 reported SEM for wrist position error in 45° flexion at 3.01° and in 45° extension at 1.24° which is comparable to our findings. They report SEM (calculated further as a % related to the mean) as not in acceptable reliability ranges. This calculation was unclear and therefore not reproducible.
To determine if these SEM scores are clinically acceptable, comparison with wrist goniometry studies was made. Intra-rater SEM for passive flexion measured dorsally was 5.74° and extension measured volarly was 5.57° averaged across 141 patient wrists, eight clinics and 32 therapist raters. 40 Another wrist goniometry study demonstrated measurement accuracy within 7° on fixed cadaver specimens. 39 Our use of a standardised protocol for goniometry measurement and positioning is consistent with other studies.15,48 The only variant between these studies and this study is our goniometer had shorter arms, to reduce cutaneous proprioceptive feedback, which may have contributed to slightly higher mean AE difference at 20° extension. Multiple goniometry positioning for each position–reposition measurement is a more likely cause of this discrepancy.
The Bland–Altman plots analysis, 61 knowledge of goniometry and JPS error would support the wrist JPS test as having a clinically acceptable measurement error, especially at 20° flexion with demonstrating the lowest SEM and narrowest LoA. No previously published JPS reference was found using Bland–Altman plots. The authors recommend SEM should be considered with clinical interpretation of wrist JPS mean AE.
Further study is suggested to determine whether factors such as target position angles, number of trials, position–reposition method and multiple raters are important variables in wrist JPS reliability in healthy and pathological populations. There has been a recent call for neuromuscular rehabilitation in wrist instability patients 62 but to date no test–retest reliable method for assessing conscious JPS in a clinical setting has been reported.
Conclusions
This study is the first of its kind to investigate specifically the test–retest reliability of a standardised active wrist JPS test in a solely healthy population, in a clinical setting and analysed by a variety of reliability statistics.
Contrasting reliability was found with low ICC values indicating poor to fair relative reliability; however, low SEM and fairly narrow LoA indicate low measurement error, acceptable absolute agreement and reliability. Taking all reliability statistics into consideration, 20° flexion is considered to be the most reliable wrist JPS angle.
The wrist JPS test using goniometry is an easy, cheap and versatile tool with which to measure the conscious proprioceptive sense in a clinical setting. However, due to the low test–retest reliability found, caution is raised on using the wrist JPS test in isolation and it is recommended therefore that it should form part of a proprioceptive assessment.
Challenges in clinically measuring aspects of conscious proprioception, namely JPS at the wrist have been highlighted in this study. This supports future research to further understand and reliably measure the JPS phenomenon in healthy and patient populations to guide assessment and rehabilitation.
Footnotes
Acknowledgements
The authors wish to thank all the participants who took part in the study and Andrea Venn for her invaluable statistical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CP gained part funding towards her MSc dissertation fee to complete this project from: the Pulvertaft Hand Unit, Royal Derby Hospital (RDH); Rheumatology Department, RDH; Medical Education Department, University of Nottingham.
Ethical approval
This study was approved by the University of Nottingham Faculty of Medicine and Health Sciences Research Ethics Committee (FMHS REC ref: PT11082016).
Informed consent
Written informed consent was obtained from all participants.
Guarantor
CP
Contributorship
CP undertook this research towards an MSc in Physiotherapy at the University of Nottingham. CP conceived and implemented the research project including literature review, protocol development, gaining ethical approval, patient recruitment and data analysis. Permissible supervision and assistance with preparation for publication, proof reading and amendment of the final manuscript was provided by VHM.