
Abstract
Introduction
Several barriers challenge the use of occupation-based interventions in hand therapy. An outpatient clinical setting can be prepared in such a way as to address the most common occupational performance problems which might promote an occupation-based intervention. To this end, more knowledge is needed about which problems patients with hand-related disorders consider most important.
Methods
Interviews using the Canadian Occupational Performance Measure (COPM)were conducted with 507 patients. Data were entered into Microsoft Excel in the COPM categories: Self-care, productivity and leisure and analysed using descriptive statistics. Data concerning main problem areas were categorized according to the Taxonomic Code of Occupational Performance (TCOP). The analysis included the number of prioritized occupational performance problems (NPOPP) in each COPM category/subcategory; the NPOPP in each category is relative to gender and age and the most frequent problems.
Results
The total NPOPP was 2384. Problems within productivity and self-care constituted the largest proportion, respectively, 46% and 40%. Gender or age affected the NPOPP in each category to a limited extend. Problems were expressed at all levels in the TCOP, except the lowest level. The most frequently expressed problem was use of utensils when eating.
Conclusion
The problems mostly concern productivity and self-care, regardless of gender or age. Patients consider problems at the levels of occupation, activities, tasks and actions to be important and meaningful to address in their intervention. This study provides useful knowledge that can be applied when preparing a setting to address the most common problems, which could lead to the promotion of occupation-based interventions.
Keywords
Introduction
Hand-related disorders are quite common1,2 and affect people of all ages.2–4 Patients with hand-related disorders report that the disorder impacts on their performance of activities of everyday life, such as dressing, meal preparation, toileting and driving.5–9 The disorder can continue to have an impact on paid work, domestic work, leisure activities, and health-related quality of life many years after the injury has taken place.7,8,10–15 At Odense University Hospital, Denmark, where this study was conducted, about 10,000 patients are treated at the accident and emergency department each year. 1 Several are in need of rehabilitation to manage their activities of everyday life, both during and after recovery.
A focus in occupational therapy is to enable patients’ engagement in occupations they want to do, need to do or are expected to do – by improving their occupational performance. 16 Occupational performance is the dynamic interaction between a person, occupation and environment. 17 The problems to be addressed in an intervention are identified through a client-centred approach, which includes a proviso that the patient and therapist collaboratively select the occupational focus for the intervention. 18
One way of gaining insight into patients’ priority issues is by applying the Canadian Occupational Performance Measure (COPM). 19 COPM is a standardized outcome measure designed to identify occupational performance problems. During a semi-structured interview performed by an occupational therapist (OT), the patient identifies their problems within the areas of self-care, productivity and leisure. 19 The patient rates the importance of the problems on a scale from 1 to 10. At the end of the interview, the patient prioritizes up to five problems that are most important to them and rates them on a scale from 1 to 10 in terms of performance and satisfaction with performance. The psychometric properties of COPM have been investigated in a number of countries and populations,20–28 including patients with hand-related disorders.24,25,27,29,30 Adequate levels of reliability and validity have been reported, together with a strong responsiveness and utility.20–28,31
Occupation-based interventions have been shown to be effective in several patient groups, from paediatric to geriatric, in increasing patients’ occupational performance,32–38 and it is reported that this intervention is more meaningful, motivating and satisfying for the patient. 39 To practise an occupation-based intervention, the occupational performance problems experienced by the patient must be analysed in detail, since occupations can be complex and consist of several underlying activities and tasks. The different levels in the Taxonomic Code of Occupational Performance (TCOP) can be used to distinguish the different complexity of the chosen problems. TCOP describes occupational performance on five levels, with increasing complexity.17,40 At the top level, occupation is defined as: ‘An activity or set of activities that is performed with some consistency and regularity that brings structure, and is given value and meaning by individuals and a culture’ (p. 19). 17
Thus, only the individual patient can decide if an activity is an occupation or not. An activity is described as a set of tasks with a specific endpoint; a task is described as a set of actions, while voluntary movements are placed at the lowest level of the taxonomy. 17
According to the literature, occupation-based interventions are sparsely used in hand therapy,39,41 despite the fact that OTs working as hand therapists have acknowledged the value of this intervention.39,42 Several explanations and barriers are reported that challenge the use of occupation-based interventions in hand therapy.39,42 The main challenge is that hand therapy is dominated by the biomedical approach and its focus on body impairments.39,43,44 Logistical issues are also mentioned, such as limited time, space and available supplies for all the different occupations in which people are engaged.39,45 By meeting the logistical barriers, it might be easier to change the focus and increase the use of occupation-based interventions in hand therapy. Thus, clinical settings need to be prepared in such a way as to address the most common occupational performance problems that arise when using the COPM.
The aim of this study was to explore occupational performance problems that patients with hand-related disorders in need of rehabilitation consider to be the most important at the beginning of their rehabilitation at an outpatient hand therapy clinic. The insights gained may increase the chances that occupation-based interventions are included in rehabilitation of hand-related disorders.
Methods
This study was an explorative and descriptive cross-sectional study using baseline data from a randomized controlled trial investigating the effectiveness of an occupation-based intervention versus a physical exercise-based and occupation-focused intervention, for patients with hand-related disorders. 46 All participants were informed about the project verbally and in writing before enrolment of the main trial 46 and they all gave their written consent. The main trial was approved by the Regional Scientific Ethical Committee for Southern Denmark, Project-ID 20120123.
Participants
Participants were recruited into the trial between February 2014 and December 2016 reported elsewhere. 46 Enrolment was at the time of referral to rehabilitation at the specialized outpatient hand therapy clinic at Odense University Hospital (OUH) in Denmark. Patients were referred to rehabilitation by the hand surgeons, based on clinical evaluation. They had a broad spectrum of hand-related disorders, such as fractures of the wrist and fingers, tendon and nerve injuries, dislocations, wounds, arthrosis, arthritis, Dupuytren’s, pain and infections. Patients were excluded from the main study if they had a shoulder disability with <100 degree flexion or abduction, epicondylitis, or burn injuries. They were also excluded if they had trivial injuries with minor influence on occupational performance, such as impaired extension in fifth finger of the non-dominant hand or hyper-sensitivity of a scar as the only disability, or if they had no described or prioritized occupational performance problems. This was done to maintain the internal validity of the main study. In this study, 46 56.4% of the 507 participants were women (n = 286), (mean age 47.2 year, range 18–92). Most participants had a vocational education or medium-length, third-level education; however, they were educated along a spectrum from elementary school to long-term, third-level education.
Data collection
Data used in this study were derived from COPM interviews collected at baseline in the main trial. 46 The day the patients started occupational therapy, COPM interviews were conducted in accordance with the Danish manual, 31 by specialized hand therapists experienced in using the COPM. In the trial, patients had to select three to five occupational performance problems and rate them.
Data analysis
The three to five prioritized occupational performance problems of each patient were entered into Microsoft Excel and divided among the three COPM categories: Self-care, productivity and leisure, as described in the Danish version of COPM. 31 Problems that could be categorized within more than one category, e.g. “using a computer,” were categorized according to the patient’s decision during the interview. Descriptive statistics were used in the analysis. Included in the analysis were the number of prioritized occupational performance problems (NPOPP) in each COPM category/subcategory, the NPOPP in each category relative to gender and age and the most frequently expressed problems. Furthermore, data concerning the most commonly mentioned occupations, activities, task or actions were categorized according to the TCOP.
Results
The total NPOPP formulated by the 507 patients were 2384. Each patient prioritized, on average, 4.7 problems. Problems within productivity and self-care constitute the largest proportion, respectively, 46% and 40%. The proportion of problems identified in leisure amounted to 14%.
Occupational performance problems in relation to gender and age
Women accounted for 56.4% (n = 286) of the patients, and 57.6% of the NPOPP identified. The proportion of problems in relation to women and men was, respectively: self-care (38.7%, 41.9%), productivity (47%, 43.5%) and leisure (14.3%, 14.5%). The main differences within the categories were: Within productivity, 76.6% of the problems expressed by the women concerned household management and 20.9% were about paid/unpaid work. For the men, 55.9% of the problems were about household management and 42.3% concerned paid/unpaid work. Within leisure, 28.6% of the problems expressed by the women were about quiet recreation, e.g. needlework. By comparison, 12.9% of the problems expressed by the men were about quiet recreation.
The NPOPP in relation to age is shown in Figure 1. The dispersions of NPOPP per patient for all the age groups were, respectively, 1.83–1.92 (self-care), 1.88–2.28 (productivity) and 0.53–0.92 (leisure).

The number of prioritized occupational performance problems (NPOPP) per patient in each age group and within each COPM category.
Occupational performance problems in COPM categories and subcategories
The NPOPP in each of the three COPM categories and their subcategories is shown in Table 1. Occupations that represented the majority of a subcategory are specifically mentioned in the table.
Number of prioritized occupational performance problems (NPOPP) within the COPM categories, the subcategories and the most commonly mentioned occupations within a subcategory.
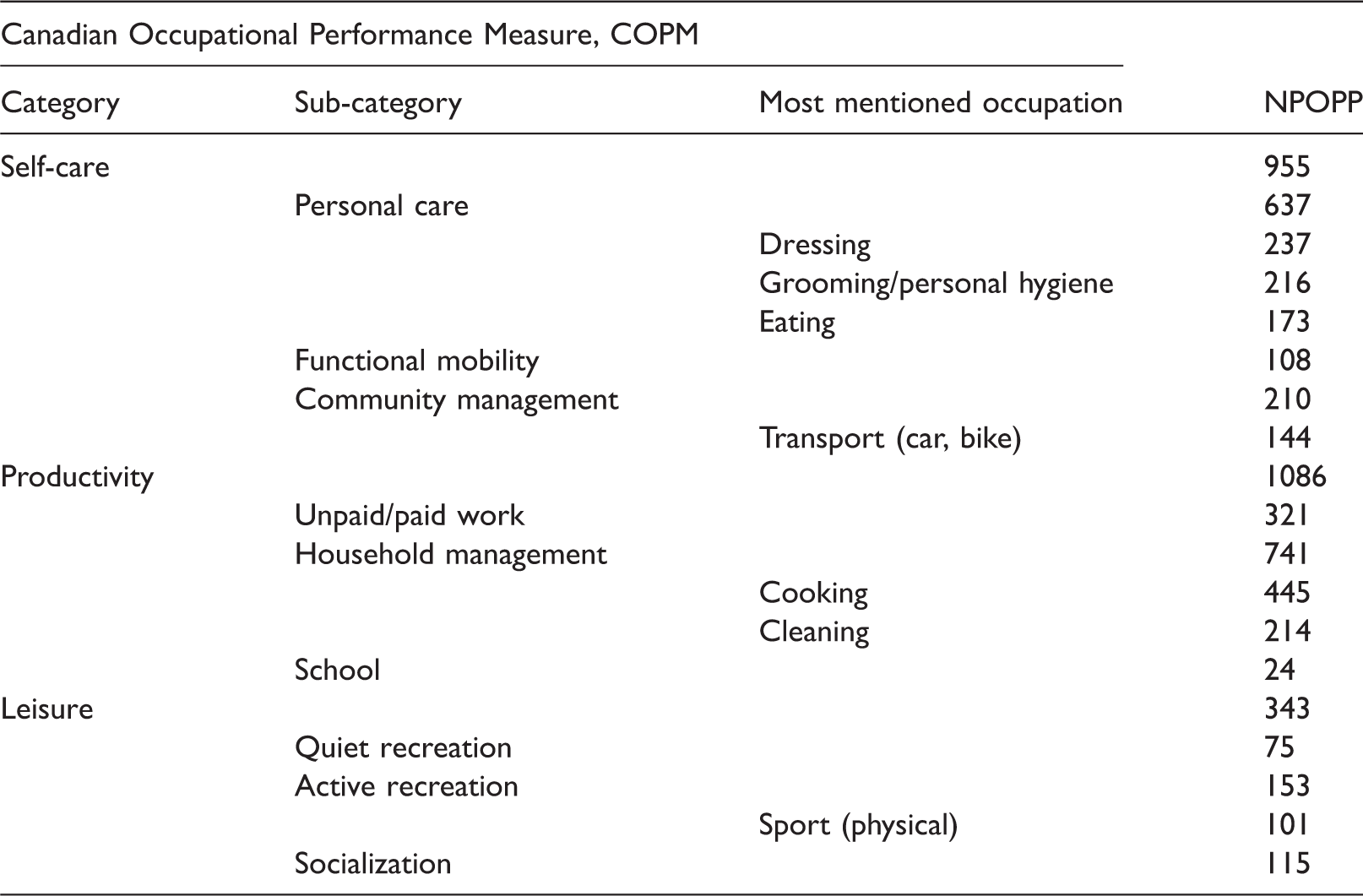
NPOPP: number of prioritized occupational performance problems.
In self-care, 443 participants (87.4%) prioritized 1 to 4 problem(s), giving an NPOPP of 955. The problems especially concerned dressing, grooming/personal hygiene and eating, within the subcategory personal care and about transport, within the subcategory community management.
In productivity, 475 participants (94.7%) prioritized 1 to 5 problem(s), giving an NPOPP of 1086. Most problems were about cooking and cleaning, within the subcategory household management. The subcategory paid/unpaid work showed a big variation in problems, which reflects the fact that the patients had different professions, e.g. within the care, retail, skilled or manual work sectors.
The category with the lowest NPOPP was leisure, where 239 participants (47.1%) chose to prioritize 1 to 3 problem(s), giving an NPOPP of 343. The largest subcategory was active recreation: NPOPP = 153 (45%), e.g. physical sport such as fitness, handball and horse-riding. Twenty-five per cent of the 507 participants (131 participants) prioritized 1 to 2 problem(s) in active recreation.
In detail, the most often expressed problems in self-care were using utensils when eating (NPOPP = 149), driving a car, within transport (NPOPP = 73), doing up buttons when dressing (NPOPP = 58) and washing one’s hair – under grooming/personal hygiene (NPOPP = 44), as shown in Table 2. In productivity, the most frequently expressed problems were cutting while cooking (NPOPP = 115) and wringing a cloth when cleaning (NPOPP = 101). In the subcategory paid/unpaid work, problems related to the use of a specific tool, such as a screwdriver, were common (NPOPP = 48). In leisure, the most frequently expressed problem was doing physical exercises, in the subcategory active recreation (NPOPP = 42).
The most frequently expressed problems (NPOPP > 40).
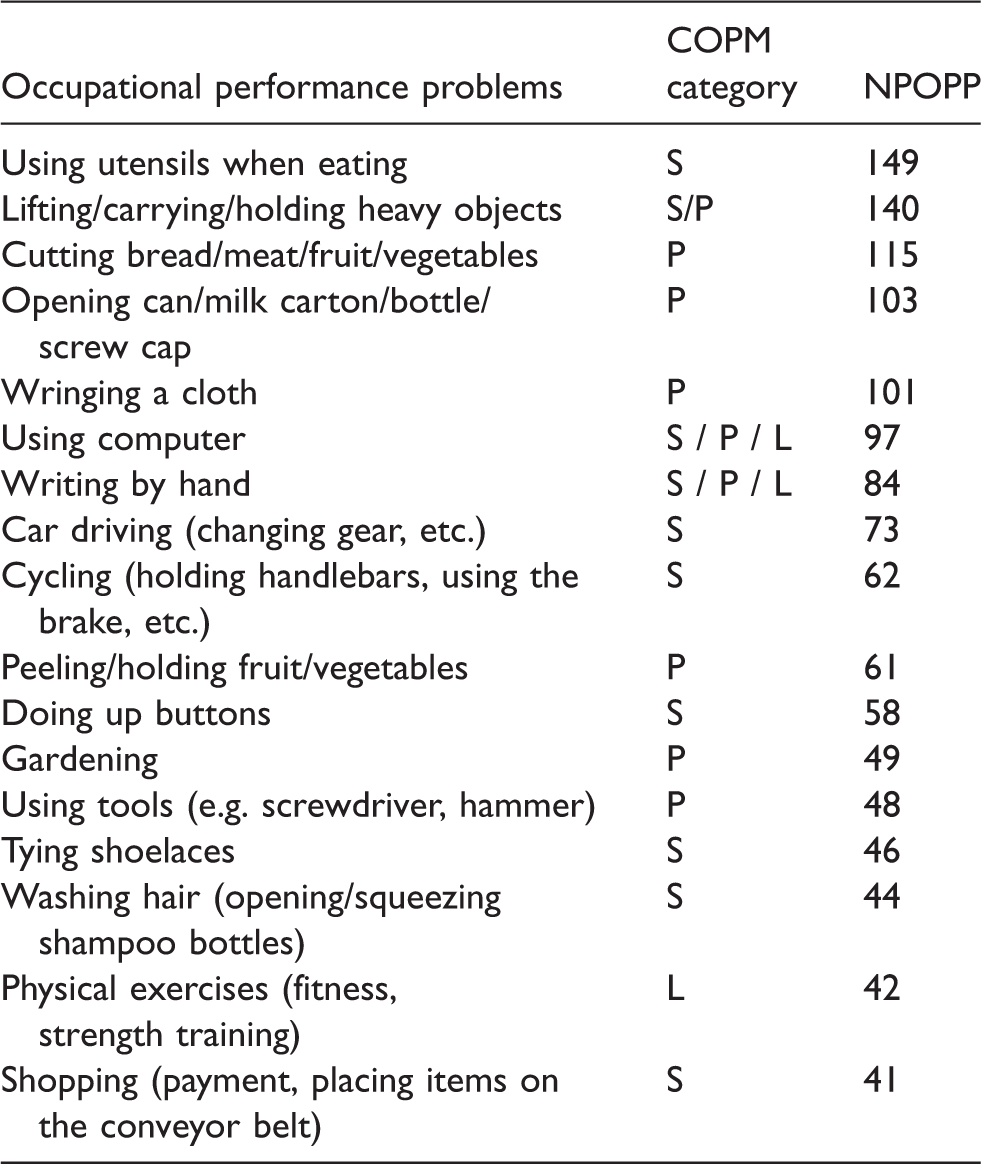
Note: Some problems were represented in more than one COPM category.
S: self-care; P: productivity; L: leisure; NPOPP: number of prioritized occupational performance problems.
Furthermore, three problems were mentioned in more than one COPM category, respectively, lifting/carrying/holding heavy objects (NPOPP = 135), using a computer (NPOPP = 97) and writing by hand (NPOPP = 84). The first problem was especially represented in the subcategories household management in relating to cooking (NPOPP = 73) and in the subcategory paid/unpaid work (NPOPP = 46). The occupational performance problems with an NPOPP >40, shown in Table 2, represent 55.1% of the total number of problems.
Occupational performance problems and the TCOP
The occupational performance problems that patients found most important to them are expressed at all levels in the TCOP, except the lowest level – voluntary movement. Examples are shown in Table 3. In the self-care and productivity categories, a few patients expressed their problems at the level of occupation, e.g. dressing (NPOPP = 10) and cooking (NPOPP = 16) or cleaning (NPOPP = 4). The problems are mostly expressed at the activity, task and actions levels. The action level is typically represented in occupations involving handling instruments or tools, e.g. eating, cooking and cleaning. Some problems are expressed accurately: ‘Holding a fork when eating’ and others are expressed more widely: ‘Lifting something heavy, e.g. a pan’. In the leisure category, the problems are mostly expressed at the activity level, e.g. playing the guitar and knitting.
Examples of expressed performance problems at each level in the TCOP.
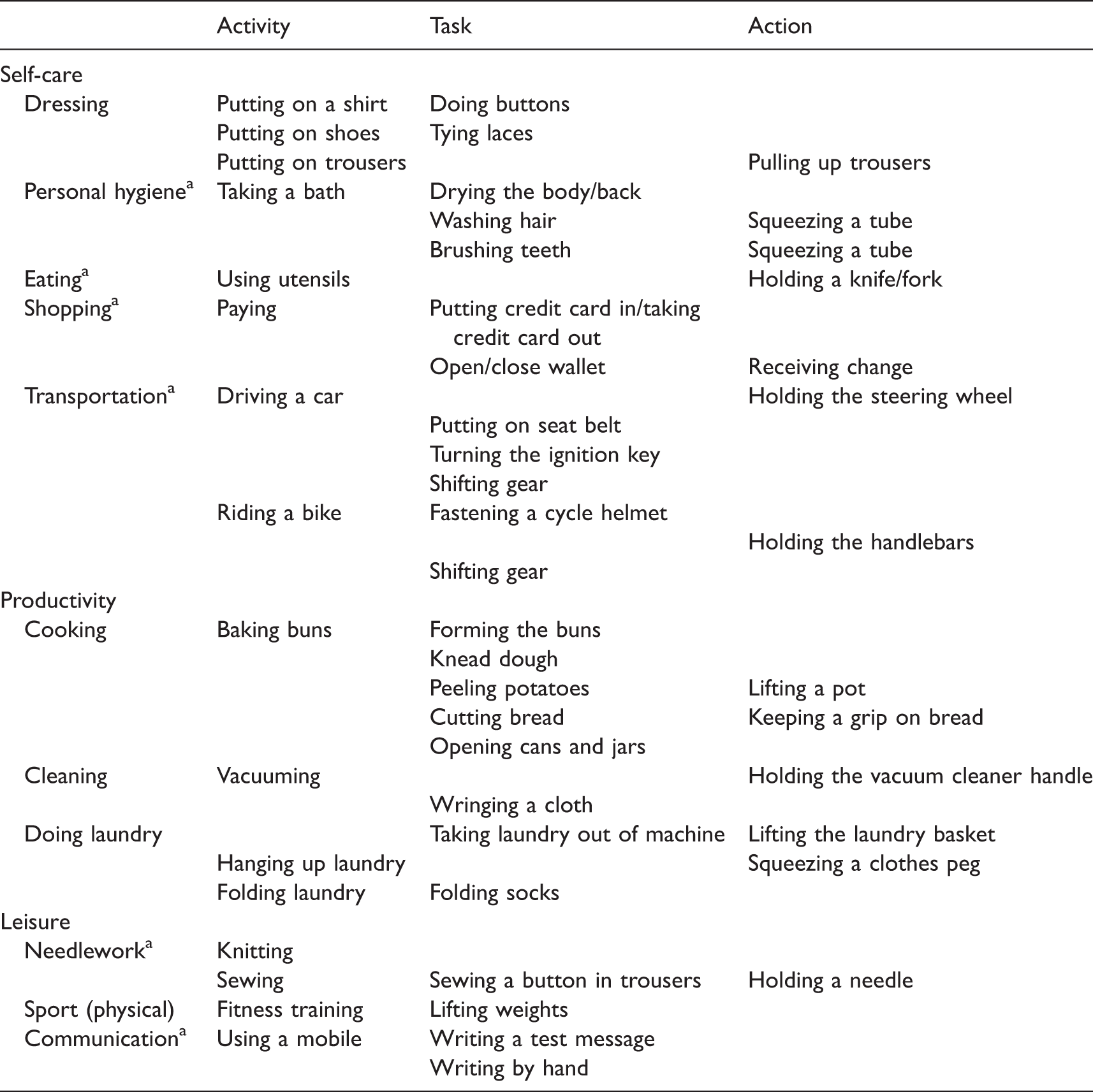
aNot expressed by the patients. Applied when categorizing data.
Discussion
The aim of this study was to explore occupational performance problems that patients with hand-related disorders considered to be the most important at the beginning of their rehabilitation. This insight can be used when preparing an outpatient clinical setting in order to address the most common problems which might promote an occupation-based intervention in hand therapy.
In this study, patients with hand-related disorders primarily considered occupational performance problems within productivity and self-care as most important to regain in their rehabilitation. However, 46% and 40% of the expressed problems concerned these categories. These findings indicate that both categories are important to address at the beginning of the rehabilitation which is supported by Nielsen and Dekkers. 47 Since OTs in hospitals or clinics often focus on self-care,20,48 attention must be paid to the fact that problems within work, cooking, shopping and transportation are just as important.
Women accounted for 56.4% (n = 286). Since 57.6% of the NPOPP were mentioned by women, the number of prioritized problems appears to be fairly equal between the two genders. Furthermore, the distribution of NPOPP between the genders is almost the same in the three main COPM categories. In the subcategories, a bigger variation between the genders was found regarding the prioritized problems. Women typically found that problems to do with household management and quiet recreations were more important to them. Men typically prioritized work-related problems more than the women did. The dispersion of NPOPP per patient is small for all age groups in each COPM category. However, there was a slight tendency for patients in the youngest age group (18–29) to weight problems in leisure higher and problems in productivity lower than do the other age groups. These considerations need to be kept in mind for practice.
According to Killian, 49 the availability of treatment areas where occupations can be performed in a common natural environment is important when implementing occupation-based practice, e.g. a housekeeping area. 50 In the two largest categories, productivity and self-care, the most expressed problems concern cooking, cleaning, dressing, grooming/personal hygiene, eating and transportation (car driving and cycling). These findings indicate that the setting must be organized with functional stations (as far as possible) where these types of problems can be addressed. In relation to functional stations, the five most expressed problems in Table 2 can be addressed in a kitchen area (using utensils, lifting/holding heavy objects, cutting, opening something and wringing a cloth). Activities like spreading butter on bread and making coffee are easily accessible and accommodate the issues mentioned. A station where patients with problems using a computer or writing by hand can practise would be appropriate. Furthermore, an area for personal care where problems like doing up buttons and tying shoelaces can be addressed. For these issues, patients could be asked to bring some of their own belongings. Performing tasks or activities in areas prepared for this will make it easier for the patient to transfer the treatment to their own environment, which in turn will support their rehabilitation.
An important finding in this study is that patients with hand-related disorders prioritize problems at all levels in the TCOP, apart from voluntary movement, in choosing their most important problems. This finding is supported by a study by Larsen et al., 20 in which it is reported that patients with orthopaedic conditions identify tasks or actions when describing their most important occupational performance problems. The fact that problems are expressed on several levels in the TCOP indicates that occupation-based interventions do not necessarily have to consist of performing occupations at the highest level in the TCOP – given that patients also highlight problems at the level of activities, task and actions to be meaningful and important. This might reflect that they are able to analyse their occupations themselves and distinguish which activities, tasks or actions are the main ones before being able to perform the occupations they would like to do. This assumption is supported by Dekkers and Nielsen. 5
The described tasks and actions (Table 2) can guide the preparation of boxes as suggested by Killian 49 to support an occupation-based intervention. Boxes are collections of supplies and equipment that are commonly used in an occupation or activity 42 and that can be used right away in the interventions without spending time on preparation. When preparing the boxes, the context – where the activity, task or action is typically performed – should be taken into consideration. For example, wringing a cloth is not just about wringing a dry cloth. It is about wringing a wet cloth and wiping a table. Furthermore, it can be noted that some problems at the action level are specifically linked to an activity or occupation, e.g. to be able to hold a fork. Other problems are more generally formulated, e.g. to be able to squeeze a tube – an action which is required in a wide range of self-care activities, such as hair washing, applying lotion and brushing teeth.
In this study, it has also been seen that problems in the leisure category often are described at a higher level than those involved in self-care or productivity. It may be due to the fact that, at the beginning of their rehabilitation at the outpatient hand therapy clinic, the patients only have had to perform the occupations that they used to doing every day. Through these occupations, they learn their limitations and from this experience they can express their problems at lower levels in the TCOP, while as yet they have not tried to perform their leisure occupations.
Limitations
There are some potential limitations to this study. The COPM interviews were conducted by several OTs, which might have introduced variation in interview style and thereby affected the level of occupational performance problems mentioned. Furthermore, the data were entered and categorized only by the first author and therefore could be at risk of being biased. However, any questions in doubt were discussed with the co-author. It might also be a limitation that the patients were asked to fill in the COPM at their first visit to the outpatient clinic, since the chosen occupation performance problems might have been different if they had had time to reflect on them. However, the results show what they found important on the day they started rehabilitation.
Conclusion
This study has provided insight into which occupational performance problems that 507 patients with hand-related disorders in need of rehabilitation consider as most important at the beginning of their rehabilitation at an outpatient hand therapy clinic. It turns out that the prioritized problems mostly concern productivity and self-care, irrespective of gender or age. Furthermore, the problems are expressed at all levels in the TCOP, apart from voluntary movement, which indicates that occupation-based interventions do not necessarily have to involve performing occupations. For patients, it is also meaningful and important to perform activities, task and actions.
Finally, this study provides useful knowledge that can be used when preparing a clinic setting, addressing the most common occupational performance problems which will promote an occupation-based intervention.
Footnotes
Acknowledgements
We would like to thank all patients and occupational therapists who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main trial was supported by the University of Southern Denmark, the Region of Southern Denmark, the Danish Occupational Therapist Association, Bevica Foundation and Odense University Hospital. Funding sources did not have any role in the design of this paper.
Ethical approval
The main trial was approved by the Regional Scientific Ethical Committee for Southern Denmark, Project-ID 20120123.
Guarantor
HP.
Contributorship
The data used in the present study were collected in a main trial, 1 led by AOH. HP and AOH researched the literature and planned the present study. HP entered, categorized and analysed the data; and wrote the draft of the introduction, results and discussion section. AOH wrote the draft of the method section. Both authors reviewed and edited the article and approved the submitted version.
Informed consent
All patients were informed about the project orally and in writing before enrolment in the main trial. Written informed consent was obtained from the patients for their anonymized information to be published in articles.