
Abstract
Introduction
The Upper Limb Functional Index (ULFI) is a patient-reported outcome measure (PROM) designed to evaluate both the functional status and the level of participation in patients with upper limb musculoskeletal disorders (ULMSDs). The purpose of this study was translation, cross-cultural adaptation, and psychometric evaluation of the original ULFI into Persian (ULFI-Pr).
Methods
The original ULFI was translated into Persian through double forward and backward translations. Consecutive symptomatic upper limb patients (n = 180, male = 60%, age = 38.21 ± 7.13) were recruited and completed the ULFI-Pr and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaires. Internal consistency and test-retest reliability were determined using Cronbach’s Alpha and the Intra-class Correlation Coefficient (ICC2.1). Criterion validity was analyzed by evaluating the Pearson’s r correlation coefficient between the ULFI-Pr and DASH questionnaires. Construct validity was examined through exploratory factor analysis (EFA) using Maximum Likelihood Extraction with Promax rotation.
Results
The original ULFI was translated and cross-culturally adapted into Persian with only minor wording changes. The ULFI-Pr demonstrated high levels of internal consistency (α = 0.91) and test-retest reliability (ICC2.1=0.92). The correlation between the ULFI and DASH was high (r = 0.71). The EFA demonstrated a one-factor structure that explained 38.2% of total variance. No floor or ceiling effects were observed.
Conclusion
The ULFI-Pr can be considered as a region-specific, single-factor structure PROM for evaluation of patients with upper limb disorders for clinical and research purposes in Persian language populations.
Introduction
Upper limb musculoskeletal disorders (ULMSDs) are a common health problem in the general population, children and in patients referred to orthopaedic clinics.1–4 The point prevalence range of ULMSDs in different populations is reported as ranging from 1.6% to 53% at any one time, while the annual prevalence ranges from 2.3% to 41%.2,5,6 Upper limb problems affect between 24% and 30% of the working population, being second only to the spine region at 37% to 52%, as the most affected region.2,7 This results in a heavy economic and social burden on both the health care systems and society generally.2,8 Additionally, ULMSD patients have reduced activities of daily living (ADL), along with reduced participation in social, work and leisure activity, all of which may initiate a harmful cycle of pain-disability.3,9,10 The ability to reduce pain coupled with improved function and return to work, are critical considerations in the management of symptomatic patients in the clinical setting, for both the physician and rehabilitation provider.
In contrast to traditional physical, biomechanical and physiological parameters, self-report evaluation from patient-reported outcome measures (PROMs) has the ability to provide greater reliability and accuracy. 11 Moreover, physical dimensions such as range of motion (ROM), hand grip strength, and tactile sensation have only weak correlation with activity limitations in such affected populations. 7 To quantify function and limitations in these patients, reliable and valid instruments are critical. Over recent decades PROMs have gained greater attention and use, due to their capacity to provide concise evaluation of a patient’s functional ability and limitations. 12 Among the five categories of PROMs (generic, condition-specific, disease-specific, region-specific and joint-specific), 13 region-specific PROMs have several advantages. These include simple to use, 14 smaller error margins enabling a smaller sample size, 15 reduced burden for therapists, and patients,7,15–17 and more feasible and applicable in both the research and clinical settings.18,19
There are several PROMs for the evaluation of functional status of the upper limb that are applicable in the health care context. The Disabilities of the Arm, Shoulder and Hand (DASH) is the most commonly recognised and used PROM in different research and clinical settings.20,21 However, there are significant concerns with the DASH and its shortened version the QuickDASH. 22 The DASH has a comparatively lengthy administration time, potential item redundancy, dimensionality concerns,20,23 and variation in responsiveness.14,24,25 Therefore its applicability in some clinical contexts is reduced. The QuickDASH, though shortened, has several concerns around perspectives from both classical test theory (CTT) considering factor structure, and modern test theory (MTT) using Rasch analysis, 20 that may potentially limit its use as a single summated instrument. 26 The Upper Extremity Functional Index (UEFI) 27 is another region-specific instrument, however it too has notable clinimetric concerns, particularly around limited generalisability due to its development methodology on a specific working population in a small data set.14,28 A similar instrument is the Upper Extremity Functional Scale (UEFS), however its reliability has shown contradictory results.29,30 The Neck and Upper Limb Index (NULI), as with the DASH, has several similar items which cause a high level of internal consistency and suggests item redundancy as too many items ask a similar question. The noted problems, in each of these upper limb regional PROMs, affect the ability of these instruments to accurately represent a broad spectrum of different activities in varied populations such as employed and unemployed persons, and to encompass the idea of looking at the function of the upper limb as a single kinetic chain.6,14,17
A more recent alternative upper limb PROM is the Upper Limb Functional Index (ULFI), a 25-item regional PROM designed to evaluate the functional status and level of participation for ULMSD patients.14,23,29,31,32 Some clinimetric advantages of the ULFI include a short completion time, functionality in a clinical setting, 33 simple scoring that does not require a computational aid, 9 ease of reading and interpretation on the Flesch-Kincaid scale for most patients,7,34,35 strong psychometrics properties, and a client-centred focus. 33 Due to these positive psychometric and practical characteristics, the ULFI appears to be a preferred substitution for the other instruments such as the DASH, Quick DASH14,34 and UEFS. 14 The ULFI is shown to be both valid and reliable in English, 14 Spanish, 29 French-Canadian, 7 Korean, 33 Italian, 32 and Turkish. 31 It has however been critiqued for potential factor structure issues, 22 though the study’s sample size was insufficient to fully verify the final findings.32,36
The ULFI has not been linguistically and culturally adapted or validated in Persian to date. Such an adaptation can subsequently be compared with the original and other language versions in terms of clinimetric properties to ascertain its validity and potential application in Persian speaking populations. Therefore, the aim of this study was to translate and cross-culturally adapt the ULFI to Persian, and to measure validity, reliability, standard error of measurement (SEM), internal consistency, and factor structure using exploratory factor analysis (EFA), in a Persian population. Confirmatory factor analysis (CFA) was not measured due to the limitation of the recruitment sample being below the required level. 37
Methods
This study was conducted in two phases. The first phase included the translation and cross-cultural adaption of the ULFI into Persian. The second phase included the evaluation of the following psychometric properties: test-retest reliability, internal consistency, and validity including face, content and construct. In addition, criterion validity was evaluated using the Persian (Iranian) version of the DASH 38 as the external standard.
Questionnaires
Upper Limb Functional Index (ULFI)
The ULFI questionnaire is a self-reported, single page 25-item PROM that assesses the individual’s self-perceived problem/s with their upper limb, and how their functional capacity and ADL is affected. 14 It has a single factor structure as reported under EFA using CTT;23,31,39 however there is uncertainty in the CFA as inadequate sample sizes have been used to date.22,36 The original ULFI was developed in 2006 as a dichotomous response PROM according to the World Health Organisation’s definition of activity limitation, impairment and participation.14,40 The ULFI demonstrated a single dimensional structure that contained four factors within two functional themes: those related to ADL; and those that were upper limb specific. 7 In 2010 the ULFI was modified to a 3-point response option of ‘Yes’=1, ‘Partly’=0.5 and ‘No’=0 in order to improve reliability and reduce cognitive load. 22 The ULFI requires less than a minute to complete with the total score calculated by summing the response items (a maximum raw score of 0 to 25 points), then multiplying by four (to a 100 point or percentage scale indicating disability), then subtracting this total from 100 to give the patient a functional score relative to their normal status.14,23,29 The scores range from 0% (maximum limitation) to 100% (normal/ability/preinjury status). Up to two missing responses are permitted.
Disabilities of the Arm, Shoulder, and Hand (DASH)
The DASH is a 30-item PROM that evaluates the level of difficulty in performing some physical ADL (21 items), severity of pain and symptoms related to ULMSDs (5 items), and the effects of the condition on social activities, work (3 items) and confidence in abilities (1 item). Response options are on a 5-point Likert scale (1–5) with a subsequent raw score of 120 ranging from 30 to 150.41,42 A transformation is performed on the score using 100/120 (0.8333) to convert the raw score to a 0 to 100, or percentage scale, which makes it easier to compare to other PROMs and measures. The Persian DASH has been shown to have good test-retest reliability (ICC2.1=0.82) and convergent validity. 38
Translation and cross-cultural adaptation of the ULFI
The procedure of translation and cross-cultural adaptation of the original ULFI English version into Persian followed the established published research and guidelines.15,43–45 Forward translation was performed by two independent native Persian speakers: a physical therapist (T1), familiar and aware of the questionnaire concept, and a professional translator (T2) who was not. An expert review committee consisting of one physical therapist, one hand therapist, one ergonomist, one psychometrician, all of the translators, and the authors produced a synthesis of both translations. After discussing any discrepancies, a consensus draft Persian version of the ULFI was developed.
Backward translation was performed by two additional independent and blinded translators whose native language was English with no knowledge of the ULFI. The new English versions were compared with the original version, and demonstrated semantic and grammatical equivalence. The expert review committee then produced a pre-final version of the Persian-ULFI (ULFI-Pr) which facilitated the determination of face and content validity.
Cultural adaptation, face and content validity of the pre-final version
The ULFI-Pr was pilot tested on 30 patients (20 males and 15 females, mean age 32.05 years (SD = 6.76) with ULMSDs to detect the alternative wording, understandability, interpretation, and cultural relevance of the translation in order to verify both face and content validity.
46
This was further supported by the expert committee discussions and consensus agreement.
47
Each patient answered the questionnaire and was encouraged to highlight (for the test administrators) any items that were difficult to understand. Most patients found the questionnaire easy to understand and applicable to their conditions, but some changes were made due to differences in interpretation of the linguistic and cultural perspectives. The following changes were made prior to the final ULFI-Pr consensus questionnaire being established, and then used for the validity and reliability components of the research.
Item 15, “my body is weaker” was inserted instead of “weaker” alone as it was otherwise not interpreted and understood by Iranian patients. In item 7 and 3, the 10lb was changed to 5kg as Persian culture uses the metric system. In item 20 the chop stick was removed because it is not applicable in Persian language. In item 21 the “tea glass” was added to the examples.
After pilot testing, we provided the questionnaire to 14 experts and invited them to complete a ‘content validity questionnaire’ based on the established standard. 46 The experts were asked to rate each draft item for its relevance to the construct, typically on a 4-point scale as follows: 1= not relevant, 2 = somewhat relevant, 3 = quite relevant, and 4 = highly relevant. 37 We assessed the content validity quantitatively through calculating the content validity index (CVI) at the item-level (I-CVIs) and scale-level (S-CVI).37,46,48 The CVI we used in this assessment is preferable to others available because: (1) it provides expert assessment data at both the item and scale level; (2) it is easy to compute; and (3) it is the only index that captures agreement within a single context.
Participants
A total of 180 (108 female and 72 male, mean age 35.24 years [SD = 8.95]) native Persian speaking patients with ULMSDs were recruited to participate in the study from individuals referred to three separate clinics in Tehran, Iran for physical therapy, hand therapy and rehabilitation. Face validity was assessed with the 30 patients in the pilot study and the feedback and discussions of the expert committee. Test-retest reliability was also conducted but on a different set of 30 patients, randomly selected from the original group, who completed the questionnaires with an interval of 3–7 days during a non-treatment period.
The eligibility criteria for participation in the study were: age ≥18 years; being native Iranian and fluent in the Persian language; enrolled in a rehabilitation or physiotherapy program for a hand/wrist, elbow, or shoulder injury or musculoskeletal disorder condition); symptoms duration of ≤12 weeks; and a diagnosis by a medical practitioner.7,14,32 The exclusion criteria were: upper limb involvement as a result of recent surgery of <6 weeks, infection, tumour, cancer, or other systemic disease. Written informed consent was completed by all patients which had been part of the ethical approval by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (USWR) (IR.USWR.REC.1395.171).
Statistical analysis
Descriptive analyses were performed to calculate means and standard deviations (SD) of demographic variables. Distribution and normality of the ULFI and DASH were determined by the one-sample Kolmogorov-Smirnov tests (significance >0.05). Reliability was examined through test-retest reliability and internal consistency. Test-retest reliability was determined by calculating the Intraclass Correlation Coefficient type 2,1 (ICC2,1) and the corresponding two-sided 95% confidence interval (CI) 14 in the randomly selected sub-sample of n = 30. An ICC2,1 value >0.80 was considered as ‘good’ and >0.90 as ‘excellent’.49,50 Internal consistency was assessed using Cronbach’s-α where a value between 0.70 and 0.95 is considered high with values >0.95 considered excessive and suggestive of redundancy and potential non-validity.51,52 The standard error of measurement (SEM) was calculated to estimate the absolute reliability and the minimal detectable change at the 90% CI (MDC90).
Content validity was assessed by calculating the CVI at the item-level (I-CVIs) and scale-level (S-CVI) 37 using a 4-point (1–4) questionnaire based on that of the recommended 10 item standard in 3 themes of relevance, comprehensiveness and comprehensibility. 46 The I-CVIs were computed as the proportion of experts who agreed that the item is either “quite” or “highly” relevant to all experts. The average of all I-CVIs was considered as the S-CVI. The I-CVI value >0.78 is considered as an adequate item of relevance and the S-CVI values of >0.90 provides evidence of strong content validity of the overall scale. 37
Criterion or concurrent validity for the ULFI was assessed using the Pearson’s correlation test performed between the ULFI-Pr and the Persian versions of the DASH. A correlation of 0.70 is interpreted as good and acceptable.51,53 All patients simultaneously completed both PROMs.
In this study, construct validity was evaluated by means of factor analysis. If a clear hypothesis regarding the factor structure is approved or confirmed for other versions of the instrument, CFA should be used. But if the same results are not observed in the different versions the exploratory factor analysis should be performed to detect the latent factors.48,52 The EFA determines the dimensionality of the items of a questionnaire. The EFA was used with Promax rotation and a loading suppression at 0.3 with Maximum likelihood extraction (MLE) 51 to detect the number of ULFI dimensions. The factor extraction had three a-priori requirements: an Eigenvalue >1.0, variance >10%, and the scree plot inflexion at the second point. 36 A CFA was not possible due to the limitations on sample size as an appropriate CFA would require an absolute minimal sample of a 10:1 patients to item ratio, n = 250 and ideally 20:1, n = 500.54,55
The sensitivity or error score of the questionnaire was calculated through the MDC90 interval of analysis.
56
First the SEM was determined for the ULFI using the formula of [SD
Floor and ceiling effects were considered present if more than 15% of the respondents achieved the lowest or highest possible score, respectively. 52
All statistical analysis were performed using the statistical package for social science version 16 (SPSS 16) for windows. The level of significance was set at p < 0.05.
Results
A total of 180 patients with shoulder (n = 66), elbow (n = 29), wrist or hand (n = 49) and multi-region disorders (n = 36) participated in this study. Of these 30 (14 male and 16 female) were randomly selected to participate in the test-retest analysis. Demographic characteristics and patients’ diagnosis by the referring medical practitioner are reported in Tables 1 and 2, respectively.
Demographic characteristics of the patients.

Diagnosis of upper limb dysfunction based on the region within the study population.

Translation process and cultural adaptation
Although the process of translation is performed based on the recognised guidelines, 43 the cultural-linguistic adaptation must also be considered in order to ensure that any new version of an instrument is appropriate for the intended population. 15
The Persian ULFI questionnaire translation was performed without major language difficulties or other conceptual misunderstandings. Some minor changes were applied in the Persian version to meet the cultural relevance. In item-7 the lb was changed to kg because it was not familiar for Iranian people and not commonly used in daily life in Iran. None of the patients reported any problems or difficulties in completing the ULFI-Pr. Moreover, there was no missing data and all items received a response.
Content validity
The findings from the CVI were that all items exceeded the minimum required cut-off, which indicated suitable content validity. The specific relevance for each of the items determined: item 8 was 0.79, items 1, 5, 14, was 0.86, items 15, 22 was 0.93, and for the remaining items was 1. The S-CVI was 0.96 indicating excellent content validity.
Floor and ceiling effects
There were no floor or ceiling effects as no respondent achieved the lowest or highest score.
Internal consistency
Cronbach’s-α value for ULFI-Pr was 0.91 with individual item ranges of 0.90 to 0.92 indicating a high level of internal consistency, but below the cut-off for item redundancy.
Test-retest reliability
The 30 patients completed the ULFI-Pr questionnaire twice with no significant difference between the test and re-test mean scores. The high ICC value (0.92) with an individual range of 0.87 to 0.94 indicated excellent test-retest reliability.
Measurement error
Measurement error, calculated from the SEM and MDC90, were respectively 3.11% and 7.25%.
Concurrent validity
Concurrent validity between the ULFI-Pr and Persian DASH total scores was ‘good’ and acceptable (r = 0.71; p < 0.001), which exceeded the 0.70 cut-off threshold for this classification.
Factor analysis structure
The MLE and Promax rotation was conducted on the 25 ULFI-Pr items. The Kaiser-Meyer-Olkin (KMO) measure was 0.71, well above the acceptable limit of 0.5. 57 This verified the sampling adequacy for the analysis. Bartletts’s test of Sphericity [x2 (300) = 4812.63, p < 0.001] indicated that correlations between items were sufficiently large for factorial analysis to be made. In an initial analysis, Eigenvalues for six factors were >1, however only one factor accounted for >10% variance (38.23%). This was supported by the visual inspection of the scree plot showing the inflection at the second point, hence suggestive that the ULFI has a one or unidimensional factor structure (Figure 1). The three a-priori requirements were satisfied which supported the factor loading for the one factor solution as shown in Table 3.
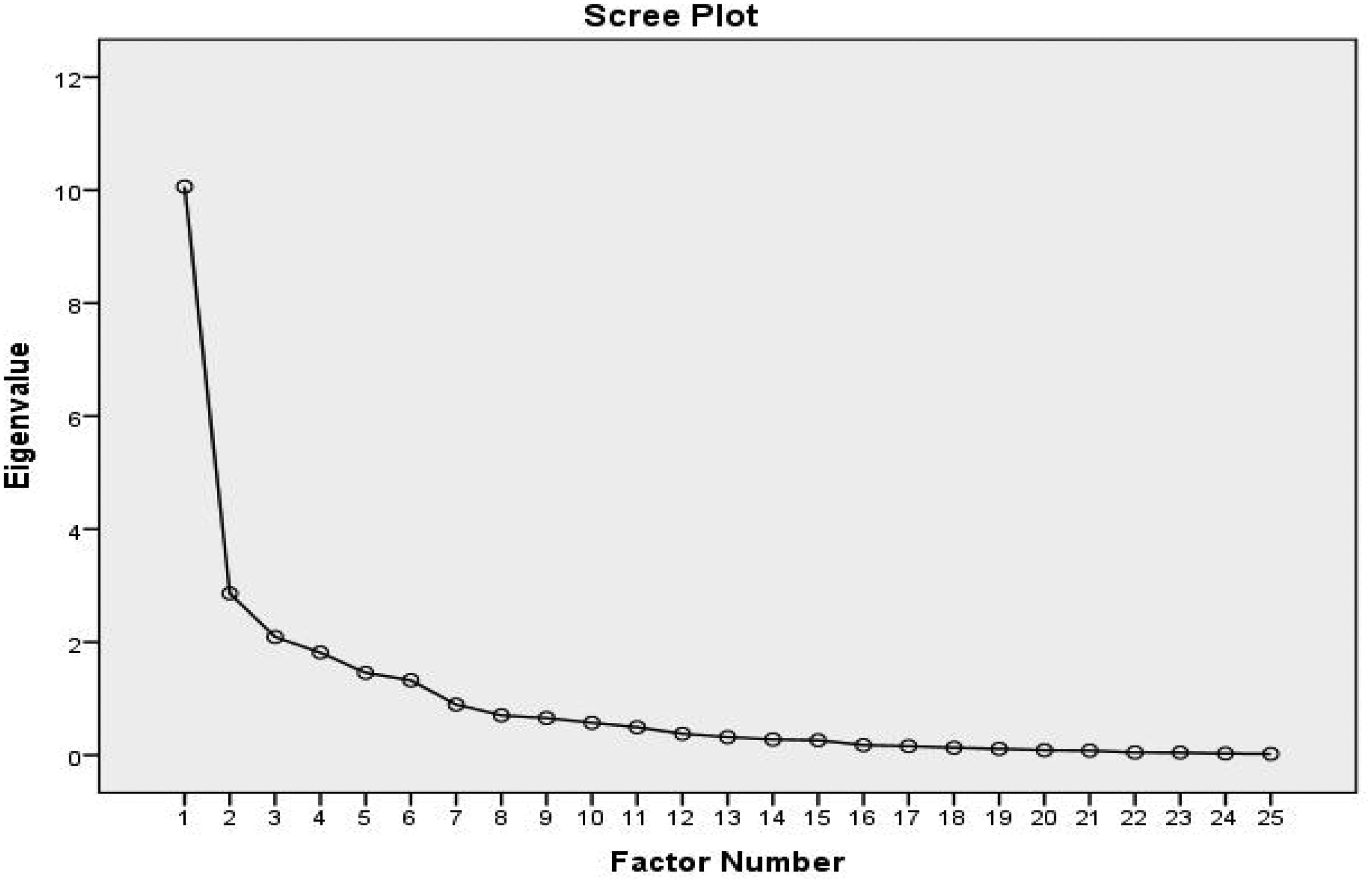
The scree plot supported a one-factor solution.
Factor loading items for the one-factor solution and average score of items.

Discussion
The purpose of this study was to develop a Persian version of the ULFI and to test its clinimetric properties. The cross-cultural adaptation procedure was adopted from suggested and recognised guidelines. 43 In relation to studies of the psychometrics of any PROM developed in different languages and cultures, such as the ULFI in different non-English populations, the content validity at the conceptual level must be maintained. To achieve this purpose, the instrument’s translation and cultural adaptation must be completed simultaneously.15,58 During the cultural adaptation phase some changes are often suggested by, either or both, the patients and the expert review committee. Such suggestions are a consequence of the differences in culture and daily customs between the original country, which was Australia for the original ULFI, and those of the Iranian people.
In item 15, the exact meaning of “weaker” alone was not understood by the Persian speaking patients, and they wanted to know what was weaker. Consequently the phrase “my body is weaker” replaced that of “weaker” alone. This reflection of the interpretation of “weaker” was also found in the Turkish version of the ULFI and a similar change was made. 59 Iranian and Turkish people are neighbours and their cultures are relatively similar, which reflects the consistency of this finding. In items 3 and 7, the 10lbs was removed and the 5 kg was maintained. The unit of pound is not used in Iranian culture. In item 20, the chop stick was removed as this eating implement is not common in Iran, and consequently of limited applicability to the Persian language and culture. This change in the Persian version was also reported in the Turkish version, which is again because of the similarity of the two cultures and countries. 59 A final cultural change in the questionnaire was related to item 21 in which the term ‘mugs and jars’ was omitted due to lack of cultural relevance, and as with the Turkish version the “tea glass” was added to the examples. 59
Our factor analysis showed six factors with Eigenvalues >1.0, but only one factor had variance >10% which accounted for ∼38% of variance, and corresponded to the Scree plot ‘elbow’ or inflection point. This supports the findings of previous research on the original 14 and Spanish 29 versions. The ULFI considers the functional status of the upper limb as a single kinetic chain with a single summated score. In the English version, seven factors with Eigenvalues >1.0 were found, but only one with variance >10% (33.4%). 14 In the Spanish version, four factors showed Eigenvalues >1.0, but only one with >10% variance, which accounted for 49% of total variance, with the scree plot ‘elbow’ at the second point, the same finding as this study. 29 In contrast to our results the Turkish version had seven factors extracted with Eigenvalues >1.0. Among them two factors showed variance >10% that explained 31.2% of total variance. 31 The Korean 33 and French-Canadian 7 versions did not report factor analysis results. The Italian version 22 reported a multi-factor structure on CFA, but the sample size was below the normally required minimum of n = 250–500.54,55
Four further critical psychometric properties of the ULFI-Pr were shown to be well supported. The Cronbach’s α coefficient (α = 0.91) showed strong internal consistency and no item redundancy, the same finding as all other versions. This α value was very close to the other five versions, the original (α = 0.89), 14 Turkish (α = 0.88), 31 French-Canadian (α = 0.93), 7 Spanish (α = 0.94), 29 and Korean (α = 0.94) 33 versions.
A high test-retest reliability (ICC2,1=0.92) was also shown for the ULFI-Pr. The ICC2.1 was lower than the original ULFI (0.98) 14 and Spanish versions (0.93), 29 identical to the French-Canadian version (0.92), 7 and higher than the Turkish (0.72) 31 and Korean versions (0.90). 33 Sensitivity to change, as measured by MDC90, indicated that ULFI-Pr minimal changes are about 7.25%, which is higher than the Turkish version (5.35%), 31 but lower than the Spanish (8.03%) 7 version, while in the Korean 33 and French-Canadian 7 versions MDC90 was not reported. To detect the treatment effect and assessment results, sensitivity of the measured values are important, which in this study were comparable with previous versions. Further, in this study floor and ceiling effects were not observed, which was consistent with the other sensitivity results and critical as it helps determine if any changes after interventions and assessment are genuine.
Concurrent validity determined from the relationship between the ULFI-Pr and DASH (r = 0.71) was ‘good’. The correlation between the DASH and ULFI in the other versions was also considered ‘good’, but varied from a lower value in the Turkish version (r = 0.68) 31 to comparable in the Korean (r = 0.72) 35 and notably higher in the French-Canadian (r = 0.85) 7 and the original (r = 0.85) 14 versions respectively. In the Spanish version, the EuroQol Health Questionnaire 5 Dimensions (EQ-5D-3 L) was used to assess concurrent validity, with a finding that was fair and inversely correlated (r=-0.59). This was consistent with the use of a quality of life assessment instrument rather than a region-specific criterion standard. 29 The relative similarity in findings with the Asian population instruments from Turkey and Korea31,33 may be attributed to the relative similarity in cultural features of the selected patients based on their geographical situations. In these three countries, the populations are mostly mono-cultural compared to Australia and Spain, with greater diversity in cultural background and language.
Limitations and strengths of the study
Limitations in this study include the inability to measure responsiveness and CFA, both of which are related to the study’s time duration. As a cross-sectional design with a focus on sub-acute patients, responsiveness could not be determined as the design lacks the required minimum time interval to consider such longitudinal aspects; and this also impacts the capacity to ensure a larger sample size, as required for CFA. Further, there is the potential to consider, in greater depth, the normal response distribution related to the individual joints of the hand, wrist, elbow and shoulder. Generalisability is also potentially impacted by patient recruitment, as patients were limited to specific therapy clinics, and only from within Tehran City.
The strengths of the study are that we used the standard methods of translation and cultural adaptation, and the assessment of the critical psychometric properties. This consequently expands the available specific number of PROMs, particularly for the upper limb, for Persian speaking patients and professions.
Conclusions
The development and adaptation of the ULFI-Pr for a Persian speaking population has not been done prior to the present study. The results demonstrated that it is possible to translate this upper limb regional questionnaire into Persian without loss of the original clinimetric properties. We found a one factor structure which supported the findings in previous studies and suggests the use of a single summated score is appropriate. However, CFA on a larger sample is recommended. Consequently, the ULFI-Pr can be applied as a specific upper limb functional status assessment instrument for clinical and research studies in Persian language populations.
Supplemental Material
sj-pdf-1-hth-10.1177_1758998320986832 - Supplemental material for Cross-cultural adaptation, validity, and reliability of the Persian version of the Upper Limb Functional Index
Supplemental material, sj-pdf-1-hth-10.1177_1758998320986832 for Cross-cultural adaptation, validity, and reliability of the Persian version of the Upper Limb Functional Index by Hamid Reza Mokhtarinia, Armin Zareiyan and Charles Philip Gabel in Hand Therapy
Footnotes
Acknowledgements
The authors are grateful to the volunteers for their participation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The ethics committee of the University of Social Welfare and Rehabilitation Sciences (USWR) approved the study (IR.USWR.REC.1395.171).
Funding
The author(s) disclosed receipt of the following financial supportfor the research, authorship, and/or publication of this article: This study was supported by grant No 1255 in University of Social Welfare and Rehabilitation Sciences.
Guarantor
HRM.
Contributorship
All the authors have made contributions to conception of this study. HRM, AZ and PCG participated in the analysis and interpretation of data and were involved in drafting the manuscript or revising it critically for important intellectual content. HRM helped with collecting data and technical support. All the authors have given final approval of the version to be published.
Informed consent
A written informed consent was gained for all participants.
Supplementary file
Persian ULFI is available as an online supplementary file.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.