
Abstract
Introduction
Using meaningful activities as a treatment modality is characteristic of occupation-based intervention (OBI). The benefits of OBI have been described, but not the effectiveness thereof. The aim of this review was to assess the effectiveness of OBI in relation to the type, commencement, duration and outcomes as reported in literature.
Methods
A comprehensive search of electronic databases was conducted, including EBSCOHost, PubMed, Cochrane Register for Controlled Trials, Web of Science, OTSeeker, PEDro and Google Scholar. Search terms included ‘occupation-based’, ‘occupation-centered’, ‘intervention’, ‘upper limb’ and ‘outcome measures’. Studies including OBI for neurological or paediatric cases were excluded.
Results
Twelve studies met the inclusion criteria. Using the PEDro scale, three of the studies, all randomised controlled trials (RCTs), were viewed as high quality, one of fair and one of poor quality. Due to the heterogeneity of the studies, a meta-analysis was not possible, and a narrative synthesis is presented. Five studies used interviewing together with the Canadian Occupational Performance Measure (COPM) to determine the client’s occupational profile when choosing meaningful activities. The commencement and duration of OBI varied amongst the studies, and a variety of outcome measures were used to determine the effectiveness of OBI.
Discussion
OBI used together with biomechanical approaches shows promising effectiveness. Outcome measures such as the COPM and the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) that measure activity and participation, should be employed in client-centered practice. More robust scientific evidence regarding the effectiveness of OBI is needed.
Introduction
Clients with upper limb conditions frequently experience restrictions during participation in daily occupations such as self-care, leisure activities and work.1,2 Individuals’ levels of functioning is often indicated by their ability to participate in meaningful activities, within their context. 3 Given the impact of upper limb conditions, therapists have to direct therapy towards restoring function to enable return to daily occupations. Occupation-based intervention (OBI) is an approach fit for this purpose. OBI in upper limb therapy has made inroads in recent years. Fisher 4 defines ‘occupation-based’ as a method of making use of the individuals’ engagement in occupation, during assessment and intervention. Che Daud et al. 5 found consensus among therapists in defining OBI as ‘an intervention on occupational performance that is meaningful (and), matches the client’s goal’5:700.
The International Classification of Functioning, Disability and Health (ICF) is a framework employed during upper limb therapy, which emphasises aspects of body functions and structures,6–8 based on the premise that function will improve with treatment of physical symptoms. 6 Routinely used occupation-based therapy has therefore been uncommon, as hand therapy has largely been dominated by biomedical and protocol-driven approaches.9–11 This can however, detract from practising client-centred therapy. 11
Despite acknowledging the importance of the client-centred nature of OBI, many therapists report challenges with the implementation of occupation-based upper limb therapy, for example, time constraints, costs involved, resources available, reliance on treatment protocols and a lack of knowledge about the implementation of OBI.7,12,13 Of these challenges, ‘lack of time’ was reported most frequently, 7 as therapists found the measurement and treatment of body functions and structures to be more time-efficient, neglecting a client-centered approach. ‘High caseloads’ in acute settings and ‘reimbursement issues’ around insurance claims 10 were also put forward as reasons for not addressing each client’s individual occupational needs.
According to Amini, 11 OBI includes long-term goals related to the clients’ performance areas. It further connects activities to the area of occupation that they intend to treat, and uses activities that simulate real-life situations. Whilst awaiting tissue healing and continued application of biomechanical approaches, limitations in clients’ occupational performance areas are addressed through the use of adaptive equipment and compensatory techniques.11,13 Outcome measures should be used routinely to determine the effectiveness of intervention and to ensure the provision of evidence-based practice. 14
In a systematic review conducted by Weinstock-Zlotnick et al., 15 instruments for determining the benefits of OBI ranged between clinician-reported outcome measures (ClinROMs), performance-based outcome measures (PerBOMs) and patient-reported outcome measures (PROMs). However, ClinROMs, focussing on body function and structures, are often used as the only outcome measure by therapists in the field of upper limb therapy and do not provide outcome data on improvement in occupational performance. 16 Stakeholders, such as insurance companies and employers, place more emphasis on outcomes reflective of aspects of activity and participation, rather than incremental increases in range of movement. 9 The use of appropriate outcome measures can therefore not only illustrate the value of therapeutic services within the health sector, 14 but also show the clinical effectiveness of OBI. 17
The purpose of this systematic review was to collate and appraise the available literature, reporting on the effectiveness of OBI used in upper limb therapy practices (including type, commencement, duration and outcomes).
The objectives of this systematic review were to (i) identify research on occupation-based upper limb therapy approaches and interventions, used in the clinical setting; (ii) evaluate the methodological quality and bias in the identified studies; (iii) analyse the results of the identified studies (through narrative synthesis) and (iv) draw conclusions regarding the type of occupation-based approaches and the effectiveness thereof in occupation-based therapy for upper limb conditions.
Methods
The systematic review protocol was designed using Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement 18 and was registered with the International Prospective Register of Systematic Reviews (PROSPERO) as CRD42020157050.
With the assistance of an expert librarian, a search strategy was applied between February 2020 to June 2020. A comprehensive search of electronic databases (i.e. EBSCOHost, PubMed, the Cochrane Register for Controlled Trials, Web of Science, PEDro, OTSeeker and Google scholar) was done. Possible sources of grey literature, theses and dissertations (completed and/or unpublished), Open Grey (references of European grey literature), WHO Library and OpenDOAR were also considered. No language exclusions were applied.
An example of a search string (used in PubMed Medline) included: “occupation-based”[All Fields] AND (((((“upper extremity”[MeSH Terms] OR (“upper”[All Fields] AND “extremity”[All Fields])) OR “upper extremity”[All Fields]) OR (“upper”[All Fields] AND “limb”[All Fields])) OR “upper limb”[All Fields] AND ((((((“therapeutics”[MeSH Terms] OR “therapeutics”[All Fields])) OR “therapies”[All Fields]) OR “therapy”[MeSH Subheading) OR “therapy”[All Fields]) OR “therapy s”[All Fields]) OR “therapys”[All Fields]))
The search strategy described was used in a similar way when searching EBSCOHost, Google Scholar, PubMed, Web of Science and Grey literature.
Eligibility
All intervention studies were included in the search, irrespective of their design. Articles were screened for relevance by title and abstract. Following the initial screening, the full texts were retrieved, and the eligibility criteria were applied.
Criteria for inclusion were: Intervention studies which included the use, type and duration of occupation-based upper limb therapy; intervention studies which included the use of outcome measure towards reporting on the outcome of occupation-based therapy to the upper limb in the treatment of persons with musculo-skeletal hand and upper limb conditions. Studies were excluded if they made use of outcome measures or assessment instruments during the first treatment session only and if studies focussed on neurological and/or paediatric upper limb conditions.
Screening
Between July and August 2020, the title and abstract screening was conducted by the first author (EV) and duplicate articles were removed. Full text screening was conducted by both the first author (EV) and the second reviewer (MJ) independently, in order to limit bias. The PRISMA flow diagram
18
(Figure 1) depicts the search and selection process. Covidence
19
was used to upload and manage the searches, and enable sharing of references between the two reviewers (EV and MJ). PRISMA flow diagram.
18

Assessment of methodological quality
Two reviewers (EV and MJ) assessed the quality of the selected studies independently, by making use of the Physiotherapy Evidence Database (PEDro scale) and the JBI Critical Appraisal Checklist for Case Reports. Notes on the administration of both checklists were provided to both reviewers to ensure clarity and consistency of administration.
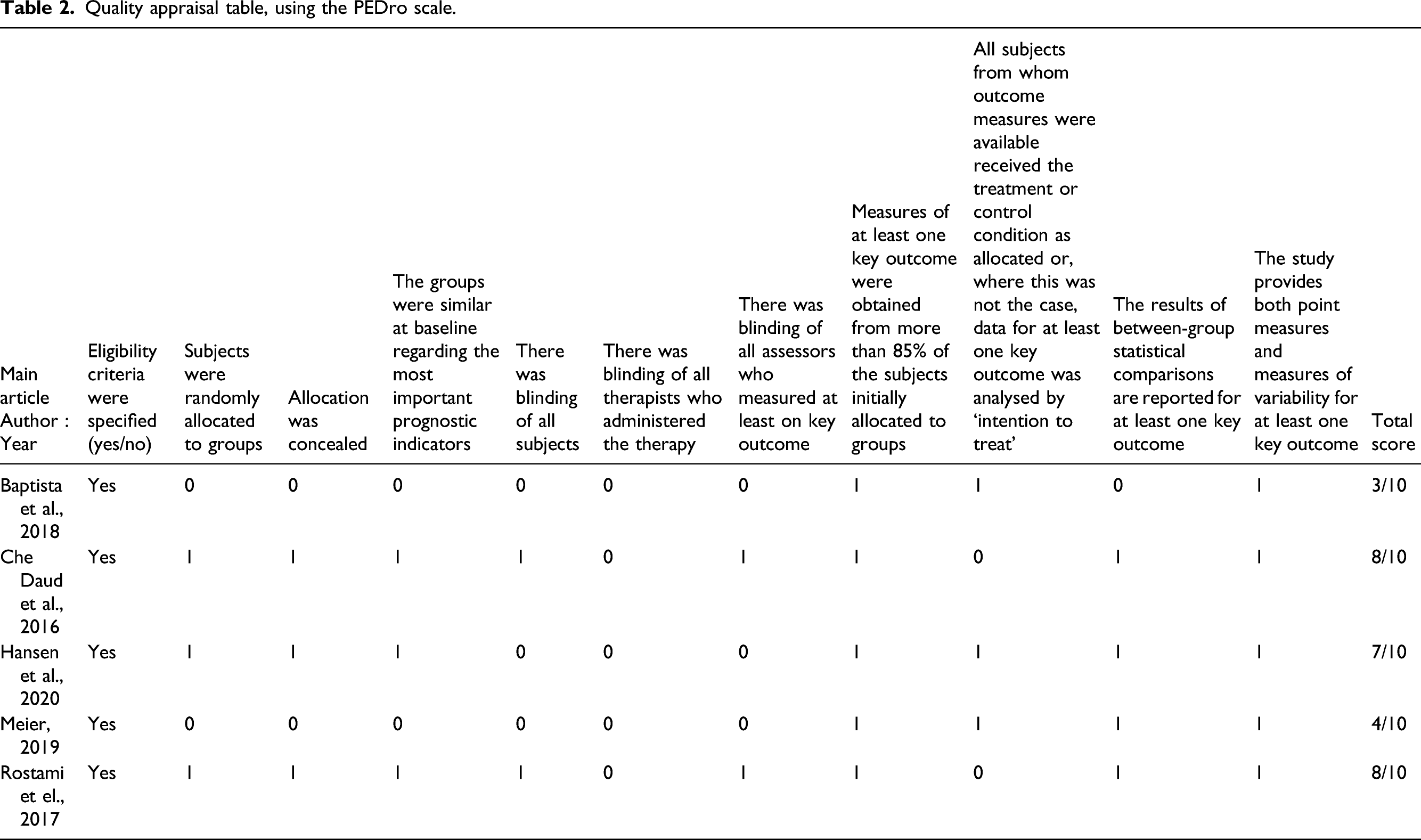
The PEDro scale was developed to examine the methodological quality of intervention studies, using an 11-item checklist. For item one to item 11, a score of 1 (‘yes’) was allocated when the criterion was met, and a score of 0 (‘no’) was allocated when the criterion was not met. 15 If the study did not report that a specific criterion was met, it was scored as if the criterion was not met. 20 The PEDro scale was initially developed to assess the quality of randomised controlled trials (RCTs),15,21 but has also been found to assess the quality of non-randomised studies,15,22 making it an appropriate tool to use.
The quality of intervention studies’ PEDro scores were evaluated as follows 23 : ≤3, were viewed as poor quality, 4 or 5, were viewed as fair quality, 6 to 10, were viewed as moderate to high quality.
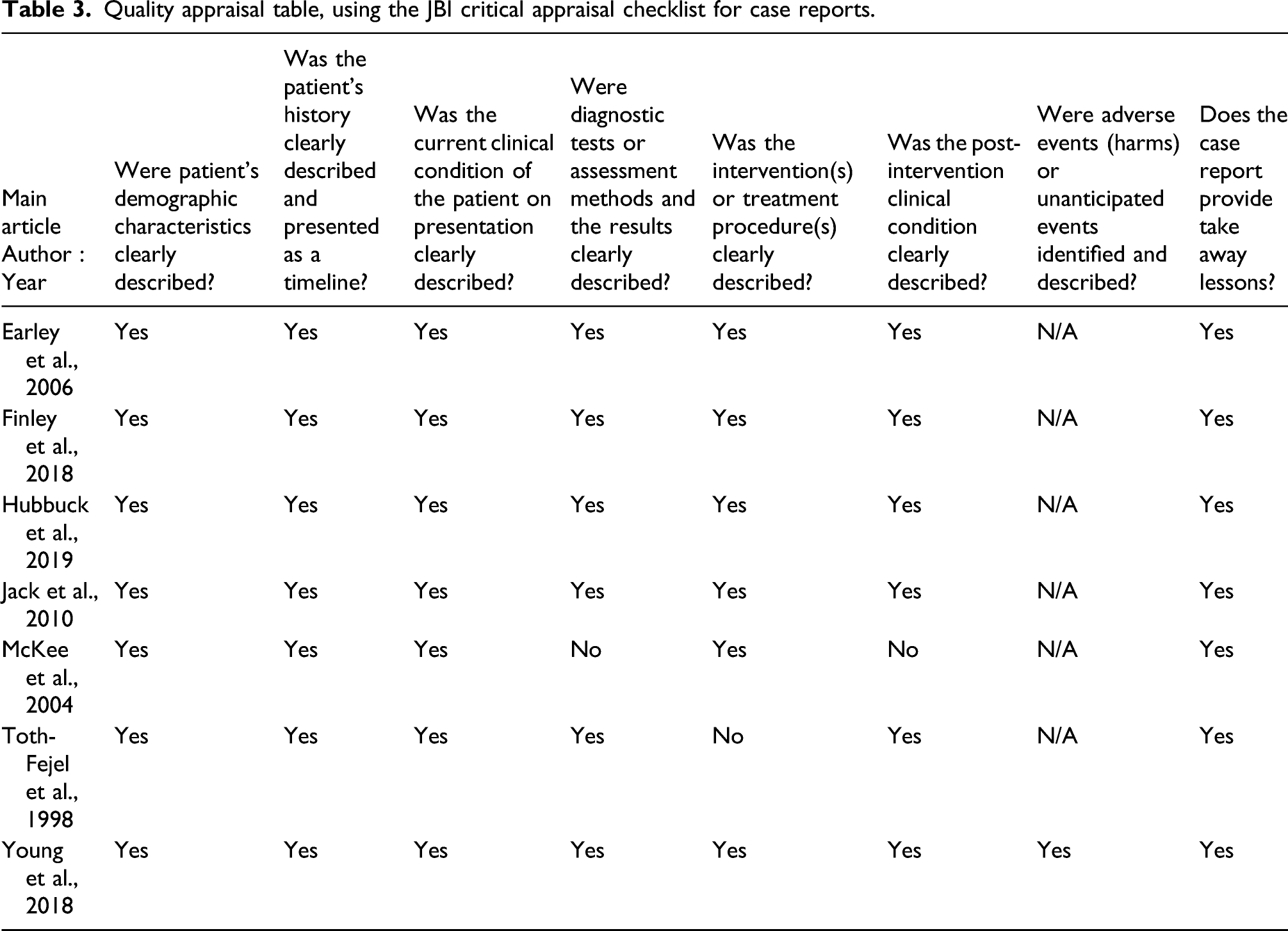
The PEDro scale cannot be used to assess the quality of case reports. 15 The JBI critical appraisal checklist for case reports, is reported to be the only tool that can be used to assess their quality. It comprises eight questions for which the reviewer can indicate ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’.
Following independent assessment of methodological quality, the reviewers (EV and MJ) disclosed their findings and discrepancies were discussed until agreement was reached. A third reviewer (SdK) was available, but was not needed.
Data extraction
Quality appraisal and characteristics of studies.
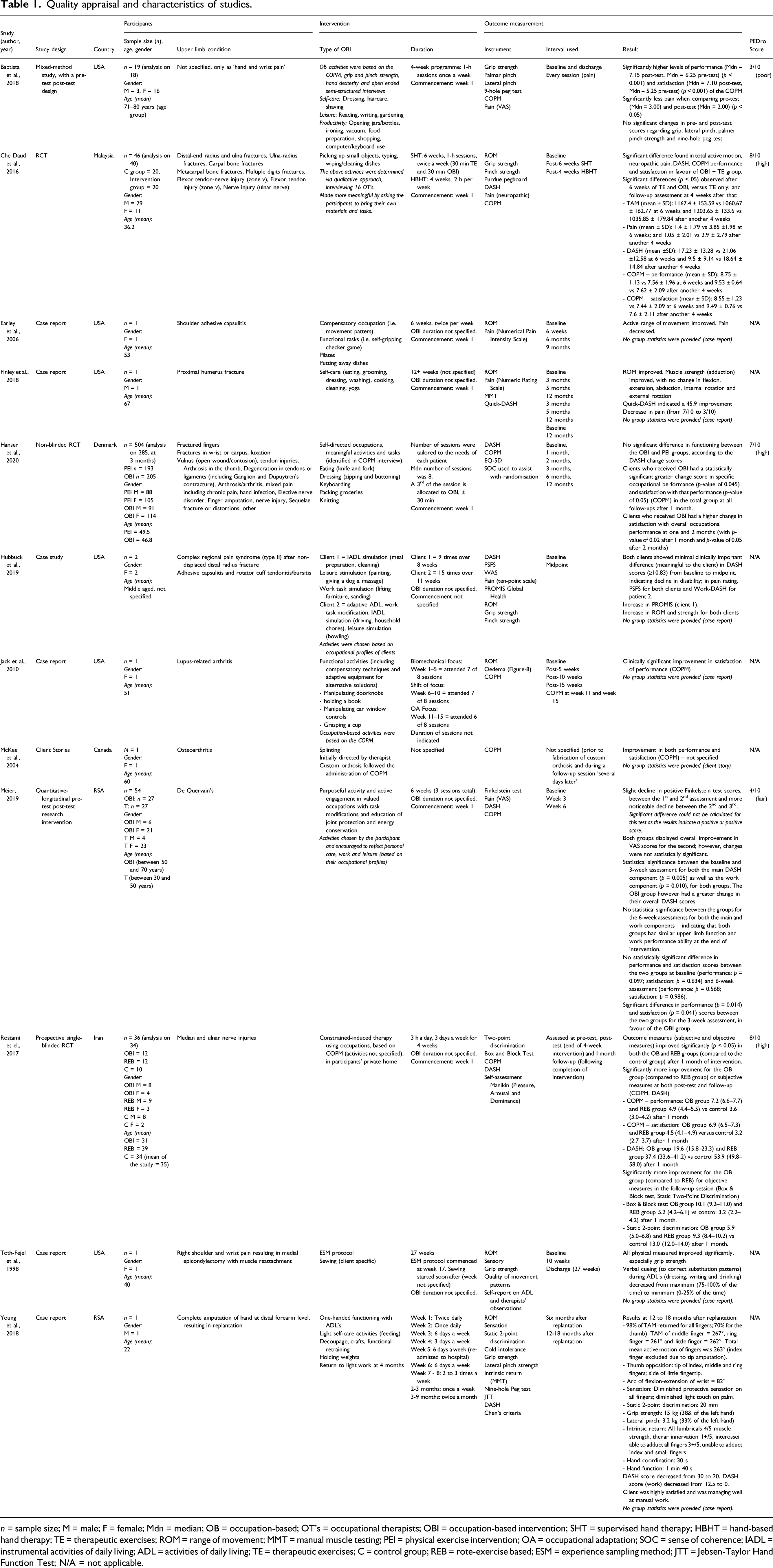
n = sample size; M = male; F = female; Mdn = median; OB = occupation-based; OT’s = occupational therapists; OBI = occupation-based intervention; SHT = supervised hand therapy; HBHT = hand-based hand therapy; TE = therapeutic exercises; ROM = range of movement; MMT = manual muscle testing; PEI = physical exercise intervention; OA = occupational adaptation; SOC = sense of coherence; IADL = instrumental activities of daily living; ADL = activities of daily living; TE = therapeutic exercises; C = control group; REB = rote-exercise based; ESM = experience sampling method; JTT = Jebsen-Taylor Hand Function Test; N/A = not applicable.
For accuracy, each data entry was reviewed on two separate dates by the first author, and spot-checks were conducted by the second reviewer (MJ).
Results
Twelve studies were included in the review (Figure 1 and Table 1).
Methodological quality
Quality appraisal table, using the PEDro scale.
Quality appraisal table, using the JBI critical appraisal checklist for case reports.
Data synthesis
Relevant data aligned to the review objectives were extracted in order to collate and summarise the findings (Table 1). • OBIs used were extracted and described, with regard to the type of intervention, as well as the commencement and duration thereof. • The outcome measures used in each of the studies were identified, defined and subsequently framed within the ICF to provide an overview of domains measured.
As studies were not heterogeneous in terms of the upper limb condition/injury, the type of OBI provided, and the variety of outcome measures used, meta-analysis of the data was not suitable. Results were therefore summarised and presented in narrative format.
Data extraction
Characteristics of studies included
Of the 12 studies included in this review, three1,24,25 were high quality RCTs, one 26 was a quantitative longitudinal pre-test post-test research intervention study of fair quality and one 27 was a mixed method study of poor quality. Three of the studies were considered as being limited due to non-blinding of therapists, 24 small sample size and the inability to blind therapists, 25 and small sample size and lack of double-blinding. 1 Two studies were viewed as poor 27 and fair 26 quality studies respectively, due to lack of random and concealed allocation and lack of blinding of clients, therapists and assessors. Seven of the studies included in the review were case reports and case studies.9,28–33 Case reports were included in the review as it can increase the evidence and strengthen the credibility of a review in emerging disciplines, such as OBI. 34
A total of 667 participants were included across the twelve studies, with sample sizes ranging from 19,28–31,33 to 504 participants. 24 Study participants presented with various upper limb conditions, as shown in Table 1. Most studies included in the review originated in high income countries, namely the USA (n = 6)9,27,28,30–32, Denmark (n = 1) 24 and Canada (n = 1) 33 . The remaining four studies originated in low and middle income countries, namely Malaysia (n = 1) 1 , Iran (n = 1) 25 and South Africa (n = 2)26,29.
Interventions
Type
Activities chosen by the various studies included that of ADL self-care tasks, leisure activities, IADL and productivity tasks and are reflected in Table 1. Three studies made use of meaningful activities, which were based on the COPM semi-structured interview.24,25,31 Others determined the clients’ occupational profile through interview and gave the client the opportunity to choose their activity.26,32 It was noted that consultation with the client, facilitated by the COPM, resulted in a positive outcome of splinting for CMCJ osteoarthritis, especially after initial splinting (as decided by the therapist) did not offer adequate pain relief. 33
Finley et al. 30 developed a rehabilitation protocol (post-proximal humerus fracture), incorporating various graded participation in ADL’s, IADL’s, work and leisure. Compensatory/adaptive techniques and adaptive equipment were also included towards enabling participation in their chosen occupations.27–32 The importance of regaining normal movement patterns, after prolonged use of compensatory methods, were also addressed by Toth-Fejel et al. 9
Duration
The three RCTs1,24,25 commenced OBI using specific time frames, varying from four to 10 weeks, based on their respective trial periods. All three studies made use of OBI from the onset of therapy. Two studies1,24 incorporated ±30 min of OBI to therapy sessions that lasted ±1 hour, where the use of preparatory/therapeutic exercises (e.g. active range of movement [AROM] and strengthening exercises) were also included. Even though some studies indicated that they made use of OBI from the start of therapy, the duration of sessions (or time spent on occupation-based activities) was unclear.25,26,28,30–32 In three of the case reports9,31,33 the commencement of occupation-based upper limb therapy, within their respective treatment protocols, seemed to occur only when clients expressed frustration with lack of functional progress.
Outcome measures
Two of the high quality studies1,25 made use of ClinROMs, PerBOMs and PROMs to evaluate the effectiveness of their interventions. The third high quality study, 24 however, made use of PROMs only. Outcome measures were used throughout the intervention process, at various intervals. The majority (n = 9) of the studies made use of outcome measures at baseline and at discharge.1,9,24–28,30,31 Hubbuck et al. 32 only made use of baseline and midpoint intervals and Young et al. 29 conducted their baseline assessment at 6 months after the arm replantation of their client, and again at discharge.
Clinician-reported outcome measures
The majority of the studies made use of physical measures, such as goniometry,1,9,28–32 the Jamar hand dynamometer1,9,27,29,32 and a pinch gauge.1,27,29,32 Three studies assessed sensation, that is, static two-point discrimination,25,29 monofilaments 29 and the Hand Dowel Test. 9 Two studies made use of manual muscle testing,29,30 one the Finkelstein test, in a study specifically focussing on the treatment of De Quervain’s 26 and one used figure of eight oedema measurement. 31
Performance-based outcome measures
Four of the twelve studies made use of PerBOMs. Two studies made use of the Nine-Hole Peg Test,27,29 one the Purdue Pegboard Test, 1 one study 25 used the Box and Block Test, and one study made use of the Jebsen-Taylor Hand Function Test (JTT). 29
Patient-reported outcome measures
Seven of the twelve studies made use of the COPM1,24–27,31,33; not only as a method to determine which occupation-based activities to use,25,27,31 but also to determine change with regards to occupational performance and client satisfaction. Six studies made use of the DASH1,24–26,29,31 and one the Quick-DASH. 30 One study each respectively made use of the Self-assessment Manikin, 25 the EQ-5D, 24 Patient Specific Function Scale, 32 the Work Ability Score 32 and the PROMIS Global Health score. 32 Various pain scales (i.e. Visual Analogue Scale [VAS], Graphic Numerical Rating Scale, Numerical Pain Intensity Scale) were also used in six of the twelve studies.1,26–28,30,32
Discussion
The aim of this systematic review was to review the quality of the current evidence on the effectiveness of occupation-based hand and upper limb intervention. Few high quality studies have been identified that investigate the effectiveness of OBI. There is heterogeneity at various levels (in accordance to the PEDro scale) including the fact that groups were not similar at baseline. In addition, even though studies evaluated with the PEDro scale achieved high ratings for items eight to 11 (see Table 2), there was heterogeneity in terms of the key outcomes, outcome measures used and the between-group statistical comparisons, making a meta-analysis not feasible. Our results suggest that the evidence available on the effectiveness of OBI, from studies evaluated with the PEDro scale, is inconclusive overall. As for the studies evaluated with the JBI Critical Appraisal Checklist, comparison is not feasible as the checklist cannot be summed into a total score. It does however inform synthesis and interpretation of the results of the studies. 35 The studies evaluated with the JBI Critical Appraisal Checklist all demonstrated promising outcomes, including but not limited to improvements in pain, ROM, muscle strength, client satisfaction and activity participation when using an OBI approach. This could inform future research.
In two studies, both high quality,1,25 it was noted that OBI allow clients to practise their targeted occupation during therapy sessions and transfer these skills to their home and work environment. Making use of OBI therefore not only results in transference to their daily occupations, but also results in compliance with therapy and increased motivation to use their injured limb, 25 preventing avoidance.15,28 Similarly, Amini 11 found clients to be more invested in their treatment as the goals are collaborative in nature and thus provide meaning. They further describe the effect of meaningful activities as alleviating depression and excessive loss in function, leading to improved functional outcomes. 11
In the mixed method study, 27 viewed as a poor quality study, authors report similar findings; stating that group attendance (where participants could share ideas based on a common functional limitation) and discussing content that was meaningful to them, increased their motivation to follow through on the recommended functional adaptations and home exercises. This was the only study to highlight the benefit of peer support and the participants’ experience of knowing that others are going through the same experiences.
When choosing meaningful activities, various studies24,25,27,31,32 made use of interviewing and the COPM to determine the clients’ occupational profile. The benefit of making use of the COPM is that insight is gained into the clients’ priority issues by means of a semi-structured interview, therefore employing a client-centered approach. 36 This is the essence of OBI, as the clients’ perspectives are sought in relation to concerns related to self-care, productivity and leisure. 36 By making use of meaningful occupations the treating therapist therefore facilitates clients to maintain a positive connection to important life roles, their responsibilities and their daily activities that have been negatively affected by their upper limb condition. 12
The commencement and duration of OBI varied amongst the studies. Jack et al. 31 recommended that OBI should not only be introduced in the event that the biomechanical approach is not successful or dissatisfaction with therapy is indicated, but should occur simultaneously with the biomechanical approach. By supplementing the biomechanical approach with an OBI approach,9,31 progress, meaningful to the client, is noted and results in satisfaction with therapy.
Various outcome measures were used to determine the effectiveness of OBI in the respective studies, but lacked homogeneity. When framing these outcome measures within the ICF, measures of body function and structure were often used as the only outcome measure, as seen in the case report of Earley et al. 28 Change in body function and structures however may not be a true reflection of the change in occupational performance brought about by OBI. For example, it is understood that joints do not require full AROM, while performing activities of daily living, implying that function can be retained despite loss of motion.
When measuring aspects of activity and participation, PerBOMs (i.e. box and block test, the JTT, the Purdue Pegboard Test and the Nine-hole Peg Test) apply. Four of the twelve studies1,25,27,29 made use of PerBOMs. These outcome measures are timed performance tests, implying that the faster the performance, the greater the participant’s hand dexterity.27,37 Che Daud et al. 1 and Baptista et al. 27 both noted no significant difference with regards to scores on the Purdue Pegboard Test and the Nine-hole Peg Test whilst demonstrating significant improvement as measured with the COPM. This demonstrates that PerBOMs such as the JTT do not necessarily correlate with improvement as measured with PROMs. 38 Sears et al. 38 found that even though the JTT demonstrated reliability, it is not validated as a measure of activities of daily living and hand function and is not responsive to clinical change. Sears et al. 38 therefore conclude that it should not be used as a measure of disability or clinical change and found PROMs to be more sensitive to change, following intervention. Quality of completion may be more important to the clients, than the speed of completion. In client-centered practice, instruments have to assess outcomes that are meaningful to the client, for example, reflecting their perspectives, values and preferences with regards to occupational performance. 39
Powell et al. 16 found PROMs such as the COPM and DASH to be linked with the ICF in assessing across all the ICF domains. The majority of the included studies either included the use of the COPM1,24–27,31,33 and/or the DASH1,24–26,30,32 in addition to other PROMs. Seven of the twelve studies1,24–27,31,33 made use of the COPM as an outcome measure. All of these studies indicated that the COPM demonstrated significant improvement with regards to occupational performance and satisfaction, following intervention that included OBI. The COPM provides client-centered information that is not obtained with outcome measures with predefined test items. 39 In addition, it is considered to have good test-retest reliability and validity for clients with upper limb conditions1,11,16,24,27 and is therefore a suggested choice to demonstrate the effectiveness of OBI in future research. Meier 26 indicated that the administration of the COPM contributed to the participants understanding of OBI and assisted with gaining insight into their needs. The COPM is therefore an instrument that assists both the therapist and the client to formulate therapy goals and expectations of treatment. 39
Six of the twelve studies1,24–26,29,32 made use of the DASH questionnaire, and Finley et al. 30 made use of the Quick-DASH questionnaire. All of these studies indicated that the DASH demonstrated minimal 32 to clinical significant1,24–26,30 functional improvement in clients, following intervention that included OBI. The DASH questionnaire differs from the COPM as it has predetermined test items, measuring aspects of the ICF. 26
Two studies39,40 supported the notion that functional assessment as well as measures of body function and structure should be used towards a complete picture of improvement in function following OBI. This review however demonstrates that the evidence across included studies is inconclusive in terms of the commencement, the type of OBI approach, the duration thereof and which outcome measures best reflect the effectiveness of the intervention. The COPM and the DASH do however show promise in demonstrating the effectiveness when an OBI approach is used.
Limitations of the review
With due consideration of the objectives of the review, studies that used OBI terminology only were included. Terms broader than occupation-based/occupation-centered have to be included in future research to include a wider variety of studies that reports on the effectiveness of OBI. The authors suggest including terms such as, for example, client-centered, activity-based, activity-focused.
Despite the motivation provided for including case reports/case studies in the current review, some may consider this a limitation as the specific scores obtained do not revert to a level of quality of the case reports. A lack of, for example, comparison group, randomisation and blinding in case reports/studies means these are considered a low level of evidence.
The review was prospectively registered, but not assessed for eligibility by PROSPERO (due to the COVID-19 pandemic), which could be seen as a limitation.
Conclusion
This review supports the use of OBI for upper limb conditions, although few high quality studies indicated its effectiveness. OBI in upper limb therapy is an emerging field of study, and with growing evidence to support its use in clinical practice, therapists may confidently incorporate OBI in their daily practice. This review further revealed that a more consistent use of OBI terminology in research will assist in drawing conclusions regarding its effectiveness. More high quality studies (i.e. RCTs) which incorporate the use of outcome measures such as the COPM and the DASH questionnaire could further demonstrate the effectiveness of OBIs.
Although various studies incorporated both biomechanical and occupation-based approaches, it was evident that this combination did not result in better client performance than those receiving only biomechanical intervention. It was, however, clear that those receiving OBI had a statistically significant improvement in occupational performance when measured with the COPM. Commencement and the types of OBI employed varied amongst the studies. It was however noted that OBI only commenced when clients expressed dissatisfaction with their progress. This review demonstrated that outcome measures used to determine the effectiveness of OBI as reflected in PROMs, such as the COPM and the DASH, should be implemented rather than focussing on ClinROMs alone, as the latter do not assess function and activities meaningful to the client.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
EV
Contributorship
EV researched literature and conceived the review. EV, SdK and LJNK were involved in the protocol development, data analysis and drafting of the manuscript. EV and MJ were involved in full text screening of studies and risk of bias assessment. All authors reviewed and edited the manuscript and approved the final version of the manuscript.