
Abstract
Introduction
In 2020, the COVID-19 pandemic caused a rapid uptake of virtual consultations (VCs) to minimise disease transmission and for this reason, research into telerehabilitation has been expanding. This review aimed to map and synthesize evidence on the use of VCs in upper limb musculoskeletal rehabilitation, describe key characteristics, and identify gaps in the research.
Methods
This scoping review investigated synchronous rehabilitation consultations performed over VC. All asynchronous, wearable or pre-recorded technology was excluded. CINAHL Complete, Medline, PEDro, Google Scholar and grey literature sources were searched. Screening and data extraction were done by a single researcher. Frequency counts were used to analyse the data.
Results
Nineteen studies were identified, with patients with shoulder injury/pain most frequently studied. Most sources (n = 9) used bespoke video programmes. Range of motion (ROM) was the most common assessment (n = 10) and exercise prescription (n = 7) was the most common treatment. Benefits included time and cost savings, maintaining therapeutic relationships and increasing patient independence. Most diagnostic assessments, except joint and nerve tension tests, were found to be reliable and valid. Studies noted increased function in activities, decreased pain and increased ROM after VCs. Limitations included restricted ‘hands-on’ treatment, resource and training concerns and limiting patient factors.
Conclusions
This review mapped available evidence and identified several gaps in the literature. Further robust research into VCs for hand/wrist disorders, ROM assessment and cost-effectiveness is needed.
Introduction
Outpatient hand therapy and musculoskeletal (MSK) physiotherapy departments play an ever-increasing role in the management of upper limb (UL) MSK diagnoses. 1 Historically, most outpatient services were delivered in person. However, many patients struggle to access rehabilitation due to costs, travel distances and mobility restrictions. 2 As a result, there has been a movement towards using technology to improve the accessibility of these services by incorporating telerehabilitation.3,4
Telerehabilitation is defined as the provision of rehabilitation services at a distance using telecommunication technology. 5 This can be synchronous (in real time) or asynchronous (pre-recorded or automatic) and involves the use of technology such as telephone and video-conferencing platforms or virtual reality. 5 In this review, virtual consultations (VCs) included telephone and/or video consultations that are performed in real-time between the patient and the therapist.
Prior to 2020, the UK’s National Health Service (NHS) included telerehabilitation in their Five Year Forward View and Long-Term Plan.3,4 Although these recommendations were in place, the uptake of VCs was still slow within rehabilitation. 6 However, with the beginning of the COVID-19 pandemic in March 2020, all outpatient departments in the UK were instructed to convert most sessions to VCs in order to minimise disease transmission and protect patients and staff. 7 Therefore, the global pandemic brought about a rapid uptake of VCs.
Research into the use of VCs has identified comparable treatment outcomes, fair patient and therapist satisfaction and evidence for cost savings across multiple disciplines8–10 and within MSK rehabilitation.11,12 However, researchers noted that there is limited, heterogenous and weak to moderate level evidence for the use of VCs in the management of patients with upper limb conditions. 13 Therefore, a scoping review was deemed more appropriate than a systematic review.
The objective of this scoping review was to map and synthesize the evidence of how VCs have been used in upper limb MSK rehabilitation, describe trends and key characteristics, as well as to identify gaps in the research base.
Review question
How have VCs been used in outpatient upper limb MSK rehabilitation? Questions that were addressed included: 1. How have VCs been delivered and structured within upper limb MSK rehabilitation? a. What target groups of patients have been studied? b. What type of technology has been used? c. What assessment and treatment tools are commonly used? 2. What are the reported benefits and limitations of upper limb MSK VCs from a therapist’s perspective? 3. What are the reported benefits and limitations of upper limb MSK VCs from a patient’s perspective? 4. Are upper limb MSK VCs comparable to face-to-face sessions in terms of the following? a. Assessment reliability and validity b. Health outcomes c. System-level outcomes
Methods
This scoping review was conducted in accordance with the guidance published by the Johanna Briggs Institute (JBI) 14 and the PRISMA-ScR Checklist. 15 Scoping reviews are useful when the information on a topic has not yet been comprehensively reviewed16,17 as they provide a rigorous and transparent method of mapping out the information in order to allow policy-makers and practitioners easy access to the information. 18
Eligibility criteria
This review investigated studies of adults (18 years+) involved in telerehabilitation for upper limb MSK diagnoses, including occupational therapists, physiotherapists or patients. Synchronous telerehabilitation sessions, with two-way, real-time communication, performed over any internet programme were included.
This scoping review focused on empirical evidence only, including a range of study designs. Systematic reviews were checked to ensure all relevant articles were included. Studies with applicable discrete data which could be clearly separated from the whole study were included in the analysis. Grey literature, including conference presentations, was included. Text and opinion papers, trial registries and protocols were excluded.
In order to obtain a view of how research into this topic has developed over the last few years, this study did not set a date limit. Any international studies were included, provided that they were published in English. Any studies investigating diagnoses other than upper limb MSK diagnoses were excluded, as were any studies that investigated asynchronous information sharing, virtual reality (VR) games or wearable devices. This was because the structure of information provision, feedback and personalisation of rehabilitation tasks in virtual and face-to-face consultations is generally similar, whereas pre-recorded or web-based information is not individualised. Additionally, VR tasks were considered to have a different structure from traditional rehabilitation sessions.
Search strategy
An initial search of CINAHL, MEDLINE, Google Scholar and The Cochrane Library was undertaken from February to March 2021 to identify relevant articles, useful search keywords and MeSH terms, and to identify journals for hand searching. The text words contained in the titles, abstracts and index terms were used to develop a full search strategy (included in supplementary materials).
The databases searched were CINAHL Complete, Medline, PEDro and Google Scholar. Sources of grey literature included PROSPERO, Open Science Framework and Ethos. If any relevant protocols were found, an attempt was made to request the full paper and/or results. Backwards and forward citation searching of relevant articles’ reference lists was performed and, when needed, authors were contacted for clarification.
The Journal of Hand Therapy, Hand Therapy, International Journal of Telerehabilitation and Journal of Telemedicine and Telecare (JTT) were hand searched. The search strategy, including all identified keywords and index terms, was adapted for each included database and/or information source as necessary.
Source of evidence screening and selection
Following the search, the relevant citations were collated into Endnote™ 20 (Clarivate Analytics, USA) and duplicates were removed. The titles and abstracts were initially screened by the first author (AM) for assessment against the inclusion criteria. Following this, AM assessed the selected full texts against the inclusion criteria before a second reviewer (SW) carried out a calibration exercise. SW randomly sampled 10% of the full texts (n = 2), checked these against the inclusion criteria and confirmed the selection of the sampled articles.
Data extraction
Data were extracted by the first author (AM) using a specifically developed data extraction tool, based on the JBI template 14 and adjusted to include findings pertaining to the specific review questions.
The data extraction tool was modified and revised as necessary. The review questions guided the development of categories (eg. “Assessment tools used”) and sub-categories were added in an iterative process when they were presented in the studies (DASH, sensory testing etc). See supplementary materials for the original and completed tool.
Critical appraisal of included sources
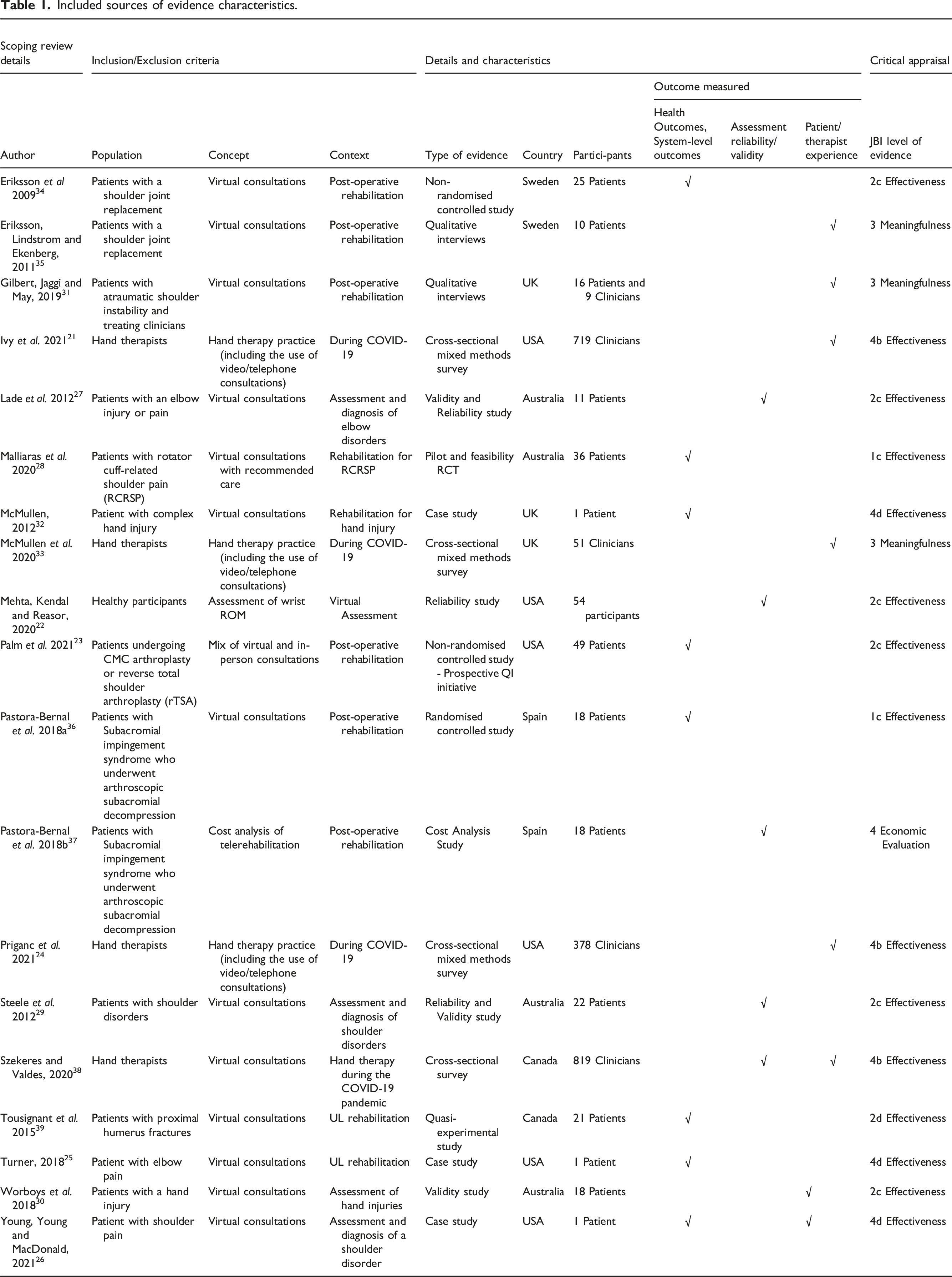
Included sources of evidence characteristics.
Data analysis
The data for VC delivery and structure (Q1) and comparability of VCs vs. face-to-face (Q4) were analysed with simple frequency analysis. The benefits and limitations of upper limb MSK VCs (Q2 & 3) were analysed by identifying key findings within the study results, creating a descriptive label (e.g. ‘no hands-on treatment’) and performing a frequency count of the times similar statements appeared in the texts.
Results
The systematic search was performed six times between 4th April and 20th October 2021 and records were identified from database searches (n = 104), hand searching (n = 12), citation searching (n = 11) and other sources (n = 8).
After duplicates were removed, 104 abstracts were screened and 77 excluded. After full-text screening of the remaining 27 articles, four were included only in part due to relevant discrete data. Eight further articles were excluded, of which two were protocol-only records. The authors were contacted via email, but no replies were received. Therefore, 19 studies overall were included in the data analysis (Figure 1). PRISMA 2020 Flow Diagram (Page et al., 2021).
The data from the 19 sources are summarised in Table 1.
Countries where studies were performed
Six studies were performed in the United States of America.21–26 Four studies were performed in Australia27–30 and three in the United Kingdom.31–33 Two studies each were performed in Sweden,34,35 Spain36,37 and Canada.38,39
Types of evidence sources included
Two RCTs were found,28,36 which were the only studies appraised as Level 1c for effectiveness. 19 Two qualitative studies (Meaningfulness: Level 3)31,35 were included and only one cost-analysis study was found (Economic Evaluation: Level 4). 37 The most frequently performed were cross-sectional surveys (n = 4) and reliability and validity studies (n = 4), followed by quasi-experimental studies and case studies (n = 3). See Table 1 for respective JBI Levels of Evidence. 19
Delivery and structure of virtual consultations
Most sources studied the use of video consultations versus face-to-face sessions (n = 16). Few studied the use of both telephone and video consultations (n = 3) and none studied telephone-only consultations. From the clinical perspective, this can be understood as it is much more difficult to determine a patient’s movement, function or healing without a visual component. Thomas et al. 40 also noted that videos enhance the therapeutic interaction by allowing gauging of non-verbal cues and visualising of physical signs.
Nine of the included sources used bespoke programme software, while fewer used well-known programmes such as Zoom (Zoom Video Communications, USA) (n = 3), Facetime (Apple Inc., USA) (n = 2) and Skype (Microsoft Corporation, USA) (n = 2). One study noted the use of various platforms 38 and four studies did not state which software was used.24,33–35
Bespoke programmes were used because they incorporated specialised software23,27,29 or because they had increased security.25,30,39 While well-known programmes are easy to use and familiar to patients, there are concerns about their usability in telehealth provision as they may not meet national privacy and security standards, such as the EU’s General Data Protection Regulation. 41 For healthcare providers, assurance that the software is secure aligns with legal requirements, as well as core ethical principles of using secure and effective communication methods. 42
The most frequent participants studied were patients with shoulder injuries or pain (n = 5) and rehabilitation therapists (n = 5), followed by joint replacements (n = 3). Elbow and hand pain/injuries were studied in two sources, while humerus fractures, joint instability and healthy participants were each studied in one source. See Table 1. Note that some studies included one or more participant groups (thus, n > 19).
Assessment and treatment tools used
Assessment and treatment tools.

While visual estimation has always been viewed with hesitancy, a reliability study by Hayes et al. 44 found fair to good inter- and intra-rater reliability of visual estimation. Mehta et al. 22 also found that all visual estimations over VC were within five degrees of the goniometer measurement. However, this study only tested wrist flexion and extension, which can be more easily estimated. No included studies investigated the reliability and validity of using a goniometer held over the screen, despite it being commonly used.
The use of subjective patient-reported outcome measures (PROM) were reported frequently among the included sources. The visual analogue scale (VAS) and numerical rating scale (NRS) pain scales and Disabilities of the Arm, Shoulder and Hand (DASH) and Quick-DASH 45 were the most commonly used due to their speed, ease, effectiveness over VCs, and appropriateness for a range of UL diagnoses.
Prescribing exercise was the most common treatment (n = 7), followed by patient education and activity modification (n = 4 each).
Use of Virtual Consultations due to COVID-19
The 2020-2021 surveys21,24,33,38 showed an increase in the use of VCs during the COVID-19 pandemic. During COVID-19, the percentage of therapists using VCs more than quadrupled, with the exception of the survey by Priganc et al.,
24
which was conducted after the first wave of COVID-19 (Figure 2). This indicated a gradual return to normal practice, albeit with higher VC use compared to pre-COVID-19. Therefore, it’s likely that therapists and managers may have been led by policies such as the UK’s Second Phase of the NHS Response,
46
to continue the use of VCs, while allowing for gradual increase of face-to-face contact. The use of virtual consultations due to COVID-19.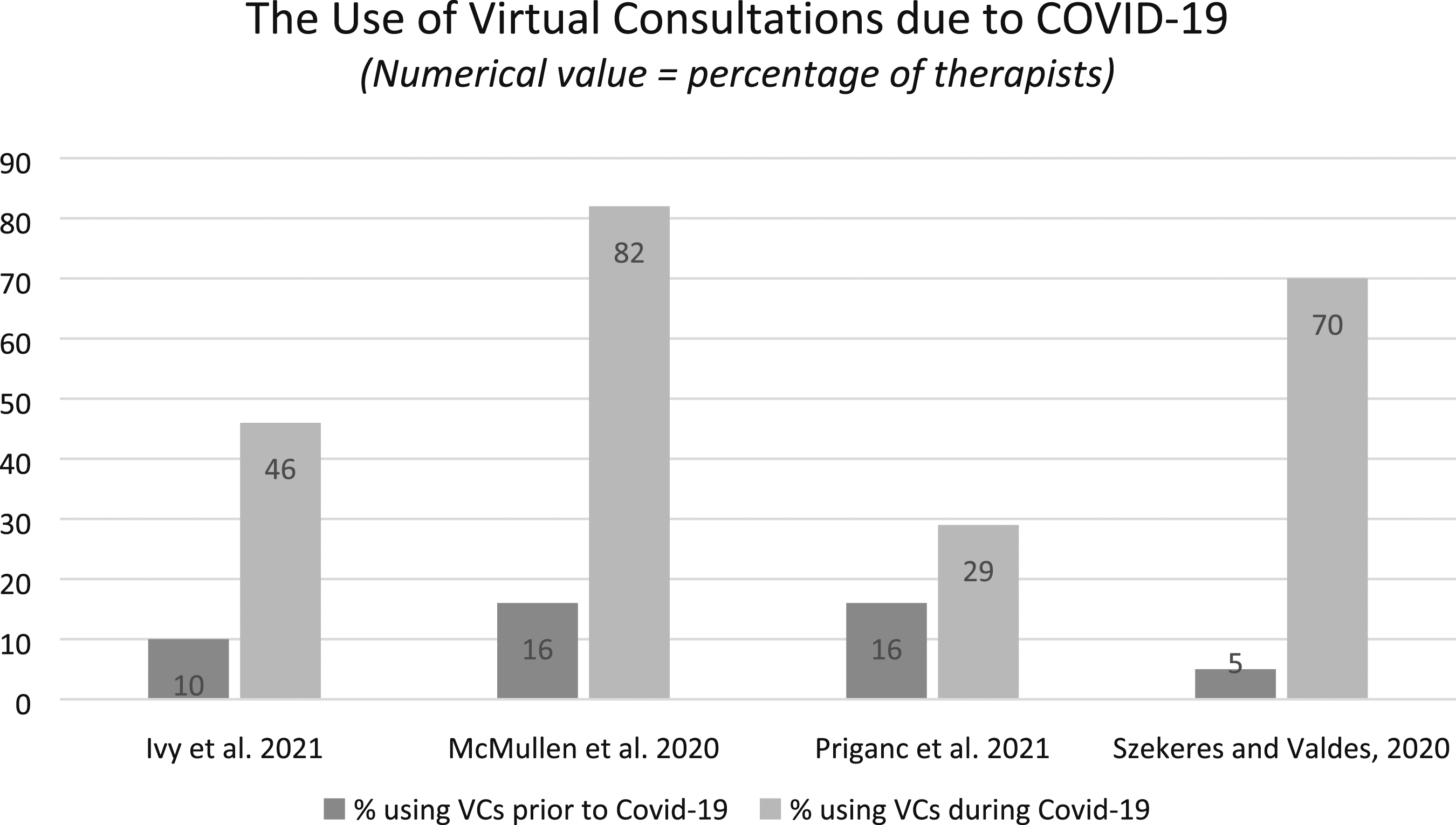
Ivy et al. 21 and Priganc et al. 24 found that post-operative patients were more likely to receive in-person treatment during COVID-19, and non-traumatic, non-operative cases and patients over the age of 65 years were more likely to be seen virtually.
Ivy et al. 21 found that of 294 respondents, only slightly more therapists reported receiving training on the use of VCs (n = 171) than those that did not (n = 123).
Benefits of virtual consultations
Two qualitative studies investigating patient experience both noted the decrease in travel costs and time as a benefit of VCs.31,35 Patients also described feeling safe and secure in their home environment and reported that the therapeutic relationship was the same as, or better than, in-person sessions.31,35 In Eriksson et al., 35 patients reported the perception of having received more regular and immediate feedback from therapists, which assisted with moving from dependence to independence post-operatively. This is due to necessitating increased patient engagement to perform and self-manage their exercises and was echoed in a systematic qualitative review by Gilbert et al., 47 which found that VCs change the dynamic of being a patient by transferring the responsibility of rehabilitation back to the patient. Therefore, the patient takes a more active role in their rehabilitation and experiences greater independence faster. Gilbert et al. 31 found that therapists felt able to progress, advise and problem-solve appropriately over VCs. Therapists also enjoyed the unique opportunity to assess patients’ activities of daily living (ADLs) in their home environment. In two sources21,24 therapists felt that telerehabilitation is ‘the future’ and could see it being incorporated into therapy long term.
Limitations of virtual consultations
The most frequent limitation noted by patients was that it was not ‘hands-on’ therapy.31,35 This was echoed in three of the studies investigating therapist opinion.21,31,33 Eriksson et al. 35 found that patients considered VCs as a useful supplement to in-person treatment, but not a replacement for it.
Therapists in two studies24,33 reported that certain diagnoses, assessments or treatments, such as muscle strength measures or splinting, cannot be performed over VCs. Therefore, they felt that VCs were not as effective as in-person treatment.24,31
Therapists also reported concerns about patient factors that could influence the success of VCs. 33 Key factors were patient anxiety, motivation levels and other mental health factors. Social risk factors, such as self-employment, financial limitations or reliance on family members to assist with technology set-up could cause difficulty with VCs. Therefore, many therapists would then see these patients in person. 33
Gilbert et al. 31 found that many therapists believed the therapeutic relationship over VC was better when the patient was already known to the therapist and that therapists were more comfortable with offering both in-person and VCs. In two surveys21,24 therapists stated concerns that VCs might replace in-person treatment completely.
Finally, therapists highlighted issues regarding access to and training for the technology used.21,31,33
Comparability of VCs and face-to-face consultations
This review looked at whether VC outcomes were comparable to in-person treatment. This was divided into assessment reliability and validity, health outcomes and system-level outcomes.
Three sources found that diagnostic assessments performed over video were valid and comparable to in-person assessments.27,29,30 These investigated the full assessment, including various outcome measures such as ROM, pain scales, patient-reported outcome measures (PROMs) and special orthopaedic tests (SOTs). Lade et al. 27 found high levels of validity (>68%) for all outcome measures performed over VCs, except nerve tension testing (NTT) and joint assessments, which Steele et al. 33 also noted as having poor agreement between in-person and VC.
Three sources22,27,29 found significant intra-rater reliability between a range of in-person and video assessments. Two sources22,29 found significant inter-rater reliability of assessments. Lade et al. 27 specifically noted that they found intra-rater percentage agreement (90%, p = 0.001) to be better than inter-rater agreement (64%, p = 0.11 non-significant) when measuring ROM over VC.
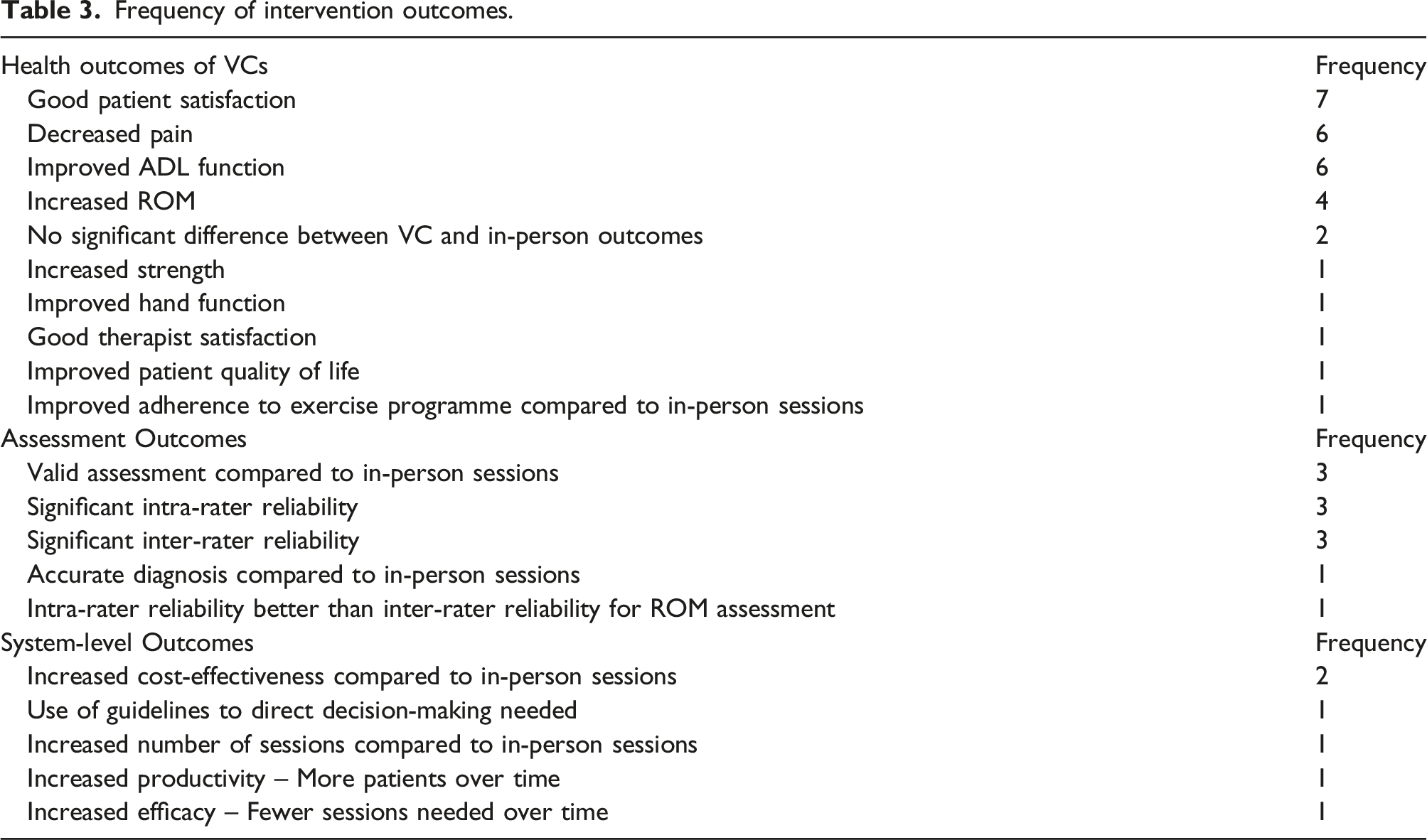
Generally, the health outcomes of the studies were positive, with improvements in ROM, ADL function and decreased pain most common.25,28,32,34,36,39 While three of the sources were case studies or not controlled,25,32,39 both Eriksson et al. 34 and Pastora-Bernal et al. 36 were well-performed, low-bias controlled trials. They found pain, function and ROM to be either similar or significantly better than in-person treatment, therefore supporting the efficacy of VCs. Although Palm et al. 23 also stated this finding, their study had a high risk of bias and so should be interpreted with caution. Two studies23,36 noted no significant difference between VC and in-person outcomes.
VCs were found to be a cost-effective intervention by Pastora-Bernal et al. 37 This was a high-quality cost-analysis study, 37 and supported within the greater MSK field.48–50 However, it was a single study on post-operative shoulder injury, so further investigation of the economic implications of hand/wrist rehabilitation is needed.
Frequency of intervention outcomes.
Discussion
The aim of this scoping review was to explore how VCs have been used in UL MSK rehabilitation, synthesise key characteristics and identify the evidence gaps to inform future research.
This review found limited empirical research in the field of VCs for upper limb MSK rehabilitation (n = 19), with very few of those studies being high quality RCTs. Therefore, further robust RCTs are needed to compare in-person and VC interventions for upper limb MSK conditions.
One of the most prominently studied patient groups was shoulder injury or pain (n = 5), which often falls into the MSK physiotherapy field. As hand and wrist injuries likely require a greater demand for in-person techniques (ie. splinting), similar studies in hand therapy may provide different results, which could indicate potential bias in the pooled review results. This highlights the need for further research into VCs in hand therapy.
Regarding assessment of patients over VCs, the included studies found good reliability and validity for most outcome measures performed over video.22,27,29 However, care should be taken when performing nerve or joint assessments, as these were found to be less valid,27,29 a finding which was echoed in a systematic review of general MSK assessments. 51
PROMs were also commonly used amongst the included studies. When choosing PROMs for use in VCs, therapists should consider the standardisation of the measures, the validity and reliability of the tool, and its ease of use. Finally, research is needed into the reliability and validity of the commonly used method of measuring ROM over the screen.
The benefits of using VCs in upper limb MSK rehabilitation were noted by both patients and therapists. Patients largely had a positive experience of using VCs, with the most regularly mentioned benefit being the decrease in travel costs and time. Therapists also reported success with session outcomes such as progressing exercises, advising and problem-solving with their patients.
The included studies found that health outcomes, such as pain, function and ROM, were generally similar or significantly better than in-person treatment,35,36 indicating that VCs can be an effective tool for MSK rehabilitation.
Finally, only one study explored the cost-effectiveness of VCs in upper limb MSK rehabilitation. 37 While it had positive outcomes, further cost-effectiveness studies are needed for the use of VCs in hand and wrist rehabilitation to assist with policy development.
The most commonly mentioned limitation was understandably the lack of ‘hands-on’ treatment, which was also noted within the wider field of VC research.52–54 Therapists were concerned about not being able to perform some assessments and techniques such as splinting or manual joint mobilisation techniques, virtually.21,31
Within the included studies, both therapists and patients believed that VCs were more successful when the therapist was already known to the patient.31,35 Hence, an argument can be made for offering a mix of virtual and in-person appointments, possibly with an in-person first contact as standard for patients with higher care needs. This idea has been supported by researchers within the MSK field.55–58
A notable finding from this review is the importance of deciding which patients are appropriate for VCs. There are certain patient factors which can negatively impact VC success, including the patient’s diagnosis and clinical presentation. Post-operative patients were more likely to receive in-person treatment,21,24 due to the increased risk of complications such as infection, oedema and contractures, and the need to use manual techniques, such as splinting, to avoid them. 33 Non-traumatic, non-operative cases and patients over the age of 65 were more likely to receive VCs during COVID-19.21,24 As patients with these types of diagnoses often do well with education and self-management, they are well suited to VCs.
While these broad categories are a starting point, the holistic view of the patient, including diagnosis, social and patient factors, needs to be considered to ensure the allocation of patients to VCs is safe and effective. Clinical decision-making tools can be very helpful for guiding therapists when making these decisions. However, as McMullen et al. 33 found, very few therapists (35%) were using such a tool and were instead relying on their own discretion. Therefore, this review agrees with McMullen et al. 34 that evidence-based decision-making tools should be developed, tested and implemented to ensure safe and appropriate standards of care.
Finally, a significant impact on the therapist’s opinion of VCs was the lack of time to receive adequate training on VC skills and technology. In a repeated measures survey, Cottrell et al. 59 found that clinician confidence and acceptance of VCs improved significantly with training and repeated exposure. Appropriate training is, therefore, paramount to ensure increased uptake and confidence in the use of VCs.
This review has several strengths, as noted: a clearly structured and rigorous search strategy, broad search boundaries and a deep examination and extraction of the heterogeneous outcomes in each evidence source. A detailed protocol was also published online at https://osf.io/d38vt/.
The greatest limitation of this study was one researcher performing the search and data extraction, due to the nature of the Masters Independent Study requirements. Measures such as the use of the calibration exercise and checklists were put in place to mitigate the risk of bias that this introduced, but there is still an increased risk of bias in the study results. Secondly, the paucity of research in this field led to a small number of evidence sources being included. Finally, limiting the search to English sources only may have excluded valuable information within this field.
Conclusions
This scoping review found limited evidence for the use of VCs in upper limb MSK rehabilitation, despite the increased uptake during COVID-19. Included studies reported both benefits and limitations for VC use, as well as positive health outcomes, assessment reliability and validity and limited evidence for cost-effectiveness. This review emphasises the importance of assessing patients’ appropriateness for VCs and suggests the use of clinical decision-making tools to assist with this process.
Further research into the use of VCs within upper limb MSK rehabilitation is needed specifically for hand and wrist disorders, investigating cost-effectiveness and ROM measurement over VCs.
Supplemental Material
Supplemental Material - The use of telephone and video consultations in upper limb musculoskeletal rehabilitation: A scoping review
Supplemental Material for The use of telephone and video consultations in upper limb musculoskeletal rehabilitation: A scoping review by Amy Maltby, Ann Underhill and Sarah Woodbridge in Hand Therapy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements
We would like to thank Ian Shelton and Nikki Daniels for their assistance and guidance in this research.
Author contributions
AM researched literature and conceived the study with the help of SW as part of an Independent Study dissertation for Master's level study. AM and SW developed the protocol. AM performed the literature search with assistance from SW for the calibration exercise. AM performed the data extraction and analysis. AM wrote the first draft of the manuscript and AU assisted with reviewing and editing the manuscript. AM and AU reviewed and approved the final version of the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AM
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.