
Abstract
Introduction
Cubital Tunnel Syndrome (CuTS) is a common condition of the elbow that is often treated with surgical decompression of the ulnar nerve but evidence for optimal management is unclear. A previous Cochrane review from 2016 identified very limited evidence to guide conservative management, in particular, night splints. The aim of this systematic review was to update the evidence related to the effectiveness of night splints in the treatment of CuTS.
Methods
We conducted an electronic search on January 15th 2025 of the MEDLINE, Embase, Emcare and CINAHL databases from the last 30 years, using a pre-defined protocol. Risk of bias was assessed using the RoB2 and ROBINS-I tools, with certainty assessed using GRADE.
Results
We identified only one randomised controlled trial (RCT), with high overall risk of bias, that compared night splints to a control arm of advice only. This under-powered trial with high loss to follow-up found no difference between groups. One additional RCT and three single-arm studies, all at high/serious/critical risk of bias, suggested the majority of patients with mild/moderate CuTS improve with night splinting but it is unclear whether the effect was due to treatment or time. Evidence certainty was very low.
Discussion
We identified a paucity of evidence, of low quality, regarding night splinting. The evidence identified by this review is currently insufficient to determine whether night splints should be recommended for the treatment of CuTS and there is a need for a high-quality research trial comparing night splints to a control intervention.
Introduction
Cubital Tunnel Syndrome (CuTS) is a common condition of the elbow, affecting 25 men and 19 women per 100,000 every year. 1 Surgery is commonplace when conservative treatments such as activity modification, physiotherapy or splints are not effective. 2 In 2023-4, according to Hospital Episodes Statistics data, 3751 cubital tunnel decompression surgeries were performed in England. 3
The UK guidance from the National Institute of Health & Care Excellence (NICE) accredited ‘Commissioning guide: treatment of painful tingling fingers’ makes recommendations for the management of both CuTS and carpal tunnel syndrome. 1 The carpal tunnel syndrome recommendations were updated in 2017 but the CuTS guidance has not been updated since the original publication in 2013. 1 It recommends referral to secondary care for consideration of surgery for patients with moderate or severe symptoms and initial conservative management of patients with mild symptoms before referring for surgery. The use of night splints is advised against, though this is based upon a single under-powered low-quality randomised controlled trial (RCT), conducted by Svernlov et al in Sweden & Denmark. 4 A subsequent Cochrane systematic review of treatments for CuTS, from 2016, only identified the same RCT. 2 It therefore remains unclear whether night splints should be recommended or not.
Similarly, the review found insufficient evidence to guide when to treat patients conservatively or surgically, in terms of clinical or symptom severity. 2 There is potential for night splints to reduce the numbers of patients undergoing surgery unnecessarily and therefore reduce waiting lists and healthcare costs. The aim of this systematic review was to update the evidence related to the effectiveness of night splints in the treatment of CuTS.
Methods
We conducted a systematic review using a protocol set a priori and registered on the PROSPERO database of systematic reviews (https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024622986) in accordance with the PRISMA statement. 5
Search strategys
Search strategy.

The search results were uploaded to the Rayyan online systematic review system (https://www.rayyan.ai/).
6
Two reviewers (MB & HS) then independently screened titles and abstracts, whilst blinded, to select full-text reports based on the following pre-defined inclusion criteria: • Adults (18+) diagnosed with Cubital Tunnel Syndrome (idiopathic). • Treatment involving any form of night splint. • Any form of comparator treatment or control including advice or physiotherapy. • All study types (e.g. randomised controlled trials, case series, cohort studies, service evaluations). • English language. • Main outcomes: Patient reported outcome measures that may include and not limited to: pain, disability, nerve symptoms, quality of life, treatment satisfaction. • Exclusions: studies of patients with cubital tunnel syndrome following trauma (e.g. fracture of the distal humerus).
The Rayyan software indicated when the process had been completed by both reviewers and would highlight any disagreements. A third reviewer (AT) was available for arbitration in the event of disagreement but in this case was not required as the two reviewers agreed.
Data extraction
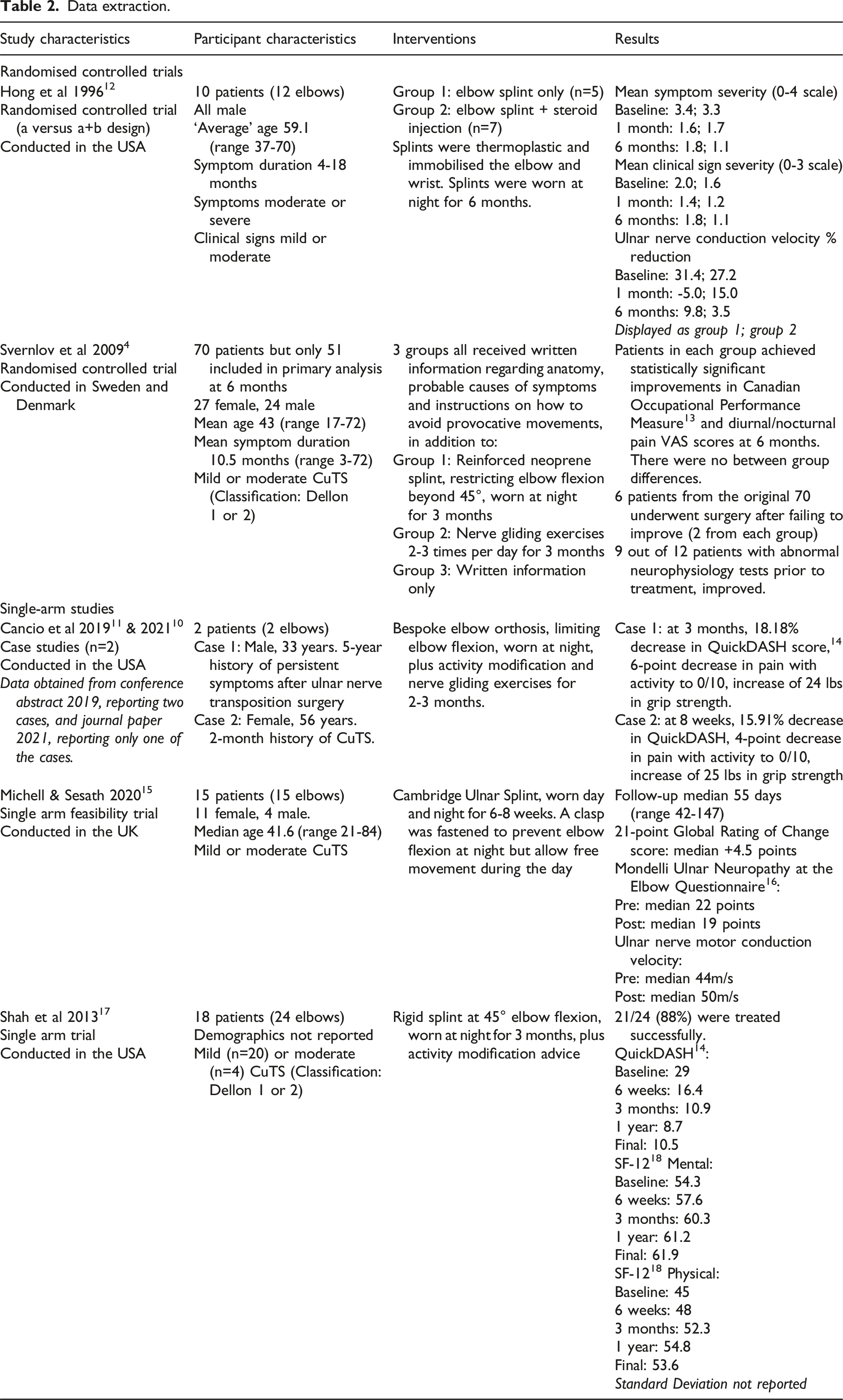
One reviewer (MB) extracted data in relation to study characteristics, participant characteristics, interventions and results before a second reviewer (AT) independently verified the findings.
Risk of bias assessment
Risk of bias assessment was conducted by MB and subsequently reviewed by HS and AT. RCTs were assessed using the RoB2 tool 7 and single arm studies were assessed using the ROBINS-I tool. 8 The RoB2 tool rates each study in terms of high risk, unclear risk and low risk of bias within five domains (see Table 3), to reach an overall conclusion. 7 The ROBINS-I tool rates each study in terms of low, moderate, serious and critical risk of bias within seven domains (see Table 4), to reach an overall conclusion. 8 Any discrepancies between reviewers were then discussed and resolved.
Evidence synthesis
We had intended to perform a meta-analysis of RCTs using similar outcome measures but this was not possible due to the lack of RCTs identified by the search. Similarly, there was heterogeneity of outcome measures across the single-arm studies identified. A narrative evidence synthesis was therefore performed. Certainty of evidence from RCTs was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) process via the GRADEpro online tool (https://www.gradepro.org/). 9 The tool assesses evidence in terms of risk of bias, inconsistency, indirectness, imprecision and treatment effect, to determine overall certainty.
Results
Initial searches identified 648 reports. After removal of duplicates and screening, six reports from five studies were included in the final analysis. One conference abstract was included in addition to the journal paper relating to the same case study, as it contained additional information (a second case study).10,11 The study selection process is detailed in the PRISMA flow diagram (Figure 1). PRISMA flow diagram. *One study includes a journal paper report and a conference abstract report that contains additional data.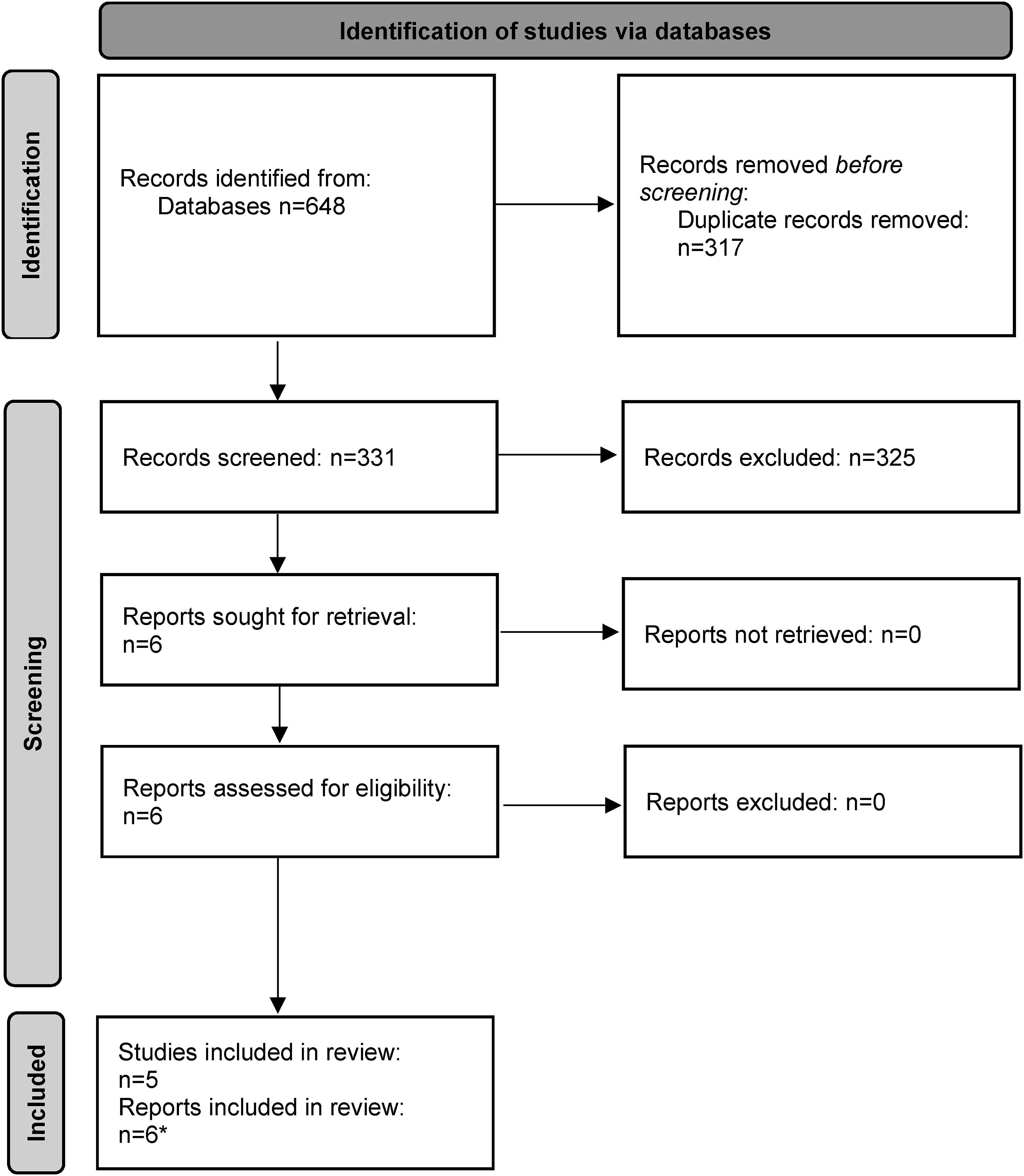
Data extraction.
RoB2 Risk of bias assessment.

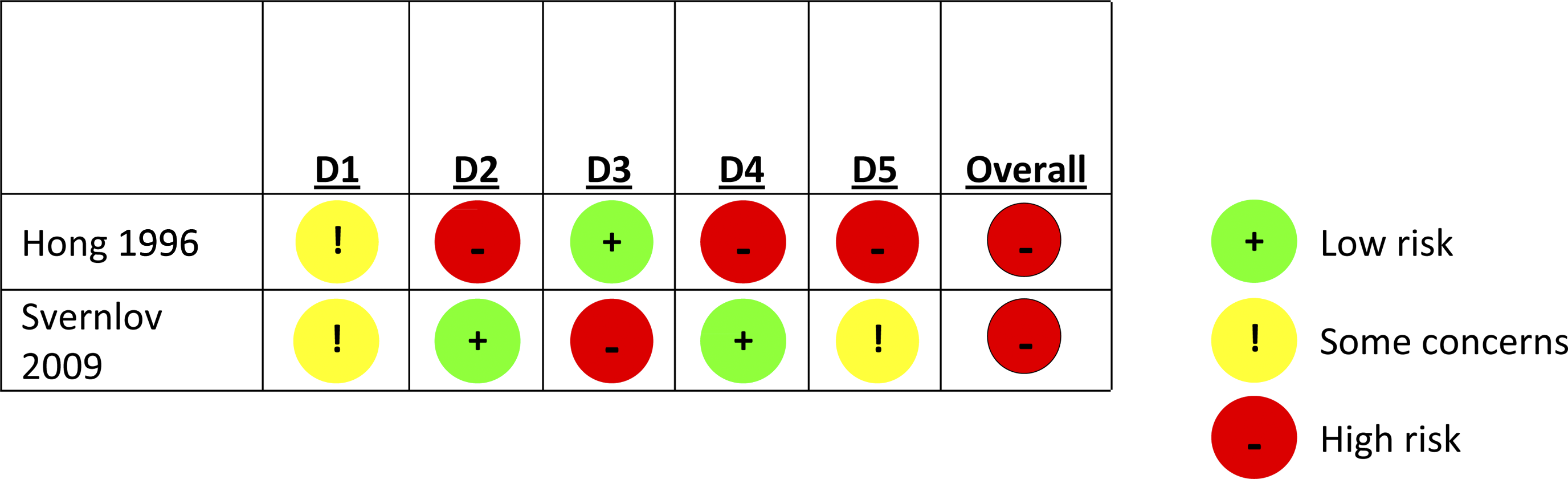
D1 Randomisation process.
D2 Deviations from the intended interventions.
D3 Missing outcome data.
D4 Measurement of the outcome.
D5 Selection of the reported result.
Another RCT, by Hong et al, again at high risk of bias, compared night splinting to a combination of night splinting and steroid injection. 12 Patients in both groups achieved statistically significant improvements in signs and symptoms at 1 and 6 months but there were no differences between groups. Similarly, nerve motor conduction velocity results improved in both groups at 6 months, although there were greater improvements at 1 month in the splint-only group. The authors conclude that there is no benefit in adding a steroid injection to night splinting. However, without a control group no conclusion can be drawn regarding the true effect of night splinting alone.
ROBINS-I Risk of bias assessment.
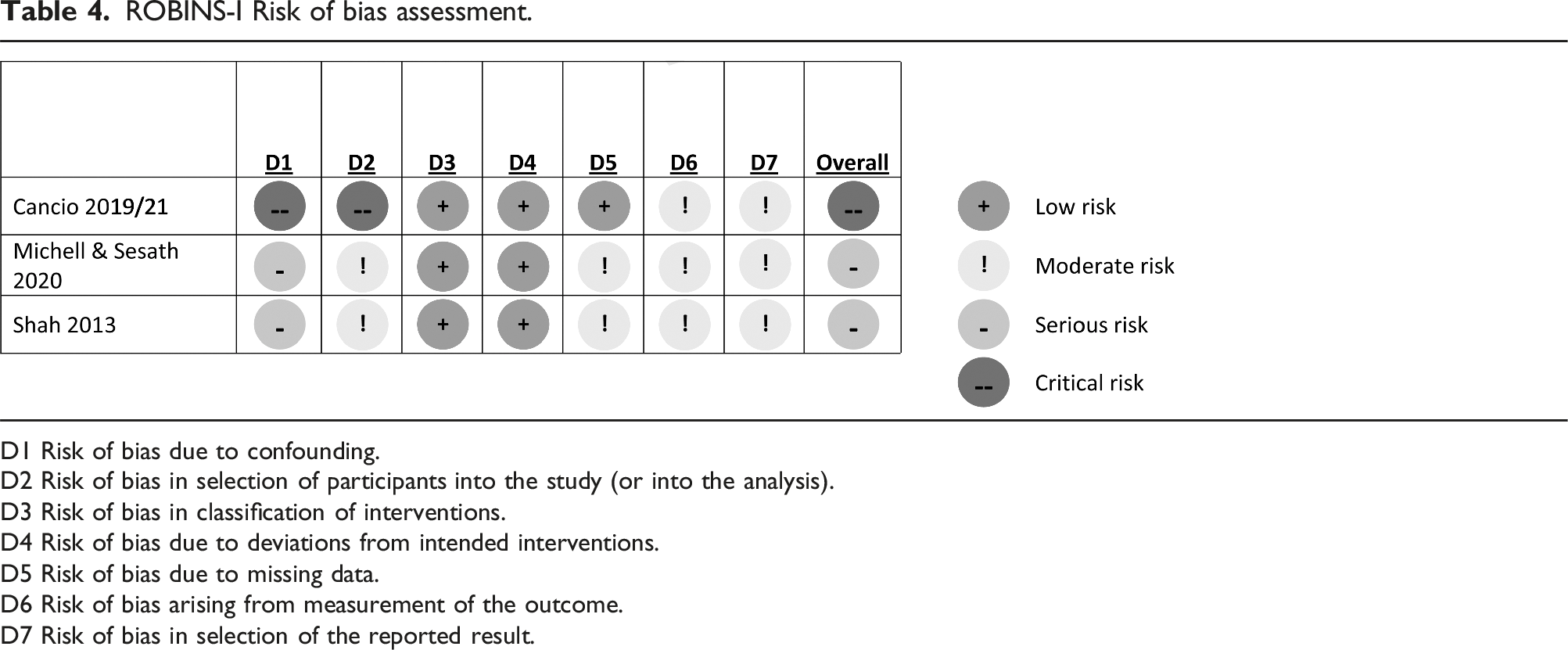

D1 Risk of bias due to confounding.
D2 Risk of bias in selection of participants into the study (or into the analysis).
D3 Risk of bias in classification of interventions.
D4 Risk of bias due to deviations from intended interventions.
D5 Risk of bias due to missing data.
D6 Risk of bias arising from measurement of the outcome.
D7 Risk of bias in selection of the reported result.
GRADE assessment of evidence certainty.
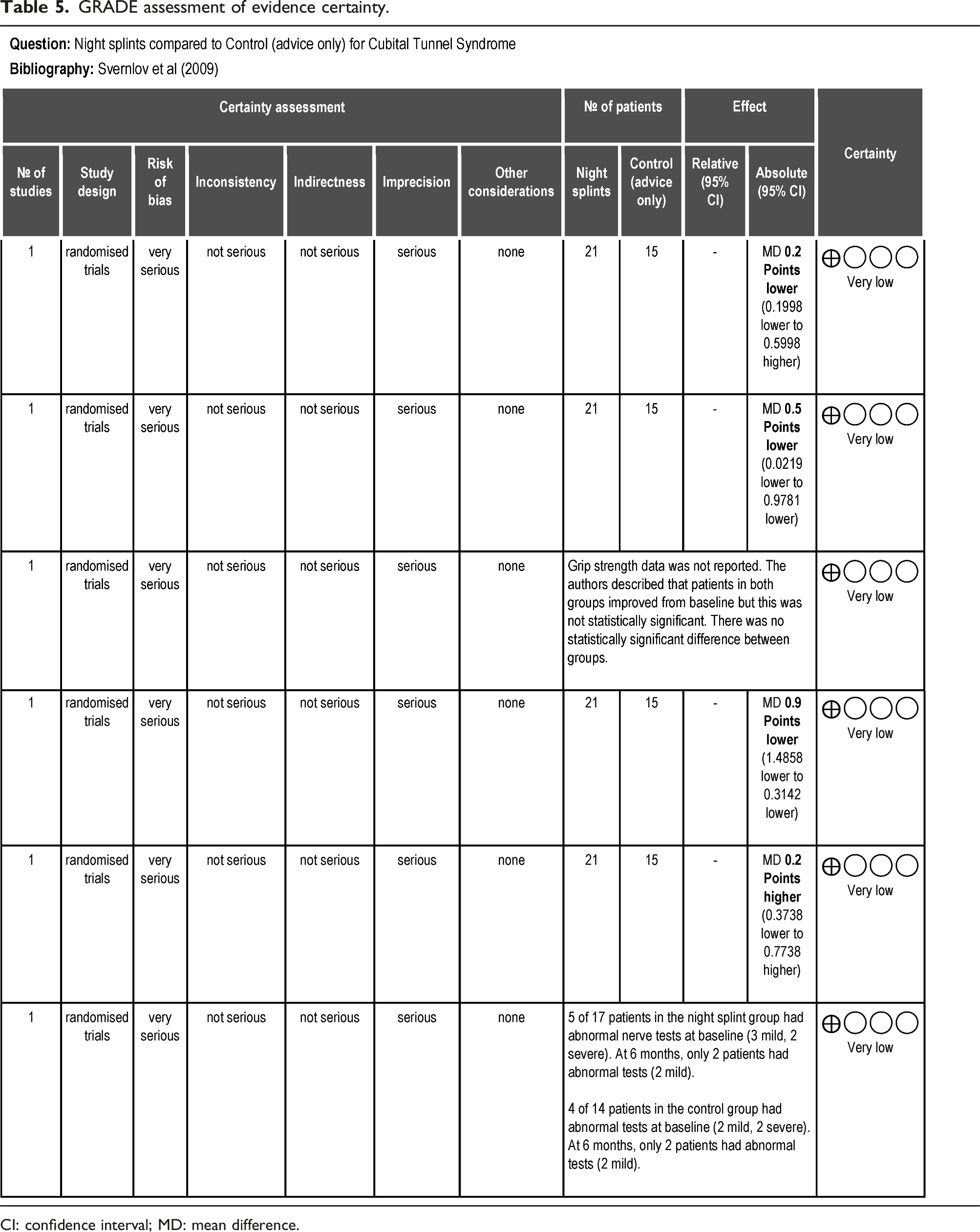

CI: confidence interval; MD: mean difference.
Discussion
The current evidence, identified by this systematic review, is not sufficient to determine whether night splints are an effective treatment for CuTS. We identified only one RCT that compared night splinting to a control intervention (advice only). 4 This was the same RCT referred-to in the NICE-accredited guidance and 2016 Cochrane review.1,2 The trial was under-powered and had a high loss to follow-up, so the conclusions must be treated with caution. Of the 70 patients recruited, only 51 were included in the primary analysis. The analysis was conducted per protocol, rather than by intention-to-treat, so increases the risk of bias. There were also differences in baseline characteristics of participants, with a greater proportion of males in the splint group (57%) compared to the control group (33%). Participants in the splint group also had longer symptom duration by a mean of 4 months compared to controls. These disparities highlight the lack of power in the trial and are potential confounding factors for the effectiveness of the interventions.
The only other RCT used an A versus A + B design, where night splinting was itself the control intervention. 12 Again, this study was under-powered and was at high risk of bias due to having an unclear method of randomisation and concerns around bias of outcome assessment, whereby patient-reported outcome questionnaires were completed by the co-authors whilst interviewing the patients. The trial was designed to assess the effectiveness of steroid injection, using night splints as the control, so has limited value in answering the aim of this systematic review. It did provide some evidence that patients with mild or moderate clinical signs of CuTS do improve with night splinting over the course of 6 months. It is unclear, however, whether they would have simply improved with time without using a splint.
Similarly, the three single-arm studies provide further data to suggest that the majority of patients using night splints do improve over time. Of the 35 patients (41 elbows) included across those studies, only seven did not improve (20%).10,11,15,17 It remains unclear whether patients would have improved without splinting and the lack of randomisation introduces a high risk of selection bias, so these findings must be treated with caution.
All of the studies included in this review selected patients with mild or moderate clinical signs of CuTS. Only two studies12,17 reported the breakdown of patients by severity, with a total of 25 mild severity and 11 moderate severity, as defined by the Dellon classification. 19 Shah et al reported results by severity, with 18/20 patients showing symptom improvement in the mild severity category and 3/4 in the moderate severity category. 17 Data extracted from the Hong et al study, shows that nerve conduction velocity across the elbow improved at 6 months in 5/5 patients with mild severity and 6/7 with moderate severity. 12 Similarly, Svernlov et al, reported that prior to splinting, 5/17 had abnormal nerve conduction velocity (3 mild, 2 severe). After 6 months, this had reduced to 2/17 (2 mild). 4 Graphical data from the Michell & Sesath suggests that 10/15 patients had improved nerve conduction velocity after 6-8 weeks of splinting. 15 These data suggest that conservative management (possibly due to the effect of night splinting or natural resolution over time) may benefit those with either mild or moderate symptoms, both in terms of symptomatic and neurophysiological improvement.
Outcome assessment varied across the studies identified in this review. Many used functional measures, such as the QuickDASH, SF-12 and Canadian Occupational Performance Measure, rather than condition-specific outcomes.13,14,18 It is unclear (beyond the scope of this review) whether these tools have been validated for CuTS and whether statistically significant changes correspond to meaningful clinical outcomes. Heterogeneity of outcome assessment is not conducive for future meta-analysis of studies, so there is a need for an agreed core outcome set for CuTS.
We also identified heterogeneity regarding splint use. The duration of recommended use ranged from 6 weeks to 6 months, with some studies using custom-made devices, some using off-the-shelf devices, some rigid and some reinforced neoprene. It is unclear, if effectiveness is determined by the type of splint and treatment duration.
This systematic review may be limited by only including English language studies from the last 30 years. There may be additional studies outside of that time period or studies reported in other languages that might provide further evidence on night splints. The evidence identified by this review is currently insufficient to determine whether night splints should be recommended for the treatment of CuTS and there is a need for a high-quality research trial comparing night splints to a control intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.