
Abstract
Introduction
Base of thumb osteoarthritis (OA) is a common degenerative condition, causing pain, stiffness, weakness and functional limitations. Most patients initially present to their GP. It is important that patients have timely access to therapy interventions. A base of thumb OA group was established within a U.K. inner-city location, as part of a community musculoskeletal therapy service. The group aligned with international clinical guidelines, providing a treatment package including exercise, educational advice and behaviour change strategies.
Methods
A prospective qualitative service evaluation was undertaken, with an aim of understanding patients’ experiences and views about the base of thumb OA group. Focus groups were undertaken with six patient participants and were recorded, transcribed and analysed thematically.
Results
Participants were positive about the impact of the group on self-management of their condition. Participants recognised the complex nature of base of thumb OA and felt that the group provided holistic support. Participants expressed a need for long term support. From a practical perspective participants described some lack of clarity regarding the clinical pathway and referral routes and a lack of support during the waiting period. Participants expressed a preference for face-to-face care delivery.
Discussion
Participants appeared supportive of the base of thumb OA group. It appears that such groups can be delivered in a community setting. Some practical service design and delivery lessons were learned. Further research would expand this relatively small scale, pragmatic service evaluation.
Introduction
Osteoarthritis (OA) of the base of thumb joint is a common degenerative disease, causing varying degrees of pain, stiffness, weakness and increased functional loss. 1 The prevalence of the condition can reach up to 7% of men and 15% of women over 50 years of age.1,2 Risk factors include age, jobs involving repetitive use of the thumb and the post-menopausal period. 2 As a result, in longstanding base of thumb OA, patients present with a loss of neuromuscular control of the joint and in more severe cases, subluxation and adduction contracture of the thumb. 3
Management of hand OA should aim to improve activity performance, pain and quality of life, with education as a core aspect for all patients. 4 Surgery, although potentially effective is considered the last treatment option due to the inherent risk of complications. Consequently, conservative treatment options are the most common first line interventions and should take a stepwise approach. 5 Previously published systematic reviews suggested that therapeutic exercises along with manual therapy and orthotic interventions can be effective in improving pain and function at short-term follow-up in patients with base of thumb OA.6,7 As a long-term condition, it is acknowledged in the NICE guidelines 8 that a treatment package could be considered. A treatment package could include exercise, manual therapy, devices and pharmacological treatments combined with behaviour-change approaches, including ways to reduce pain and straining when using joints, pain coping skills training, goal setting, motivational coaching, weight management counselling and workplace risk counselling. An education programme could be given by one or more healthcare professionals over multiple sessions, including those based on behavioural theory. 8 Evidence supports the use of a group to deliver effective interventions for base of thumb OA. 9 Such a programme was developed for patients attending a community musculoskeletal (MSK) service.
The aim of this qualitative service evaluation was to identify the value that patients attribute to the base of thumb OA group and identify patients’ experiences and views about pathways and processes pertaining to the group.
Methods
Context
A novel base of thumb OA group was established within a multidisciplinary community MSK therapy service. The service provides care to a U.K. inner-city population of over 300,000 and the service itself receives approximately 1500 referrals each month. Referrals are received via several routes including self-referral, GP referral and referral from first contact practitioner physiotherapists. The base of thumb OA group is delivered within a specialised clinical patient pathway for hand condition management. In addition to the above routes of referral, patients can also be referred to the base of thumb OA group via internal patient pathways, including from individual therapy sessions or the specialist hand interface clinic. The base of thumb OA group is delivered face-to-face by a therapist over four hour-long sessions. The group aligns with recognised clinical guidelines.4,8 The National Institute for Clinical Excellence suggests combining the non-pharmacological components of patient support within a package of treatment, combining therapeutic exercise with an education programme or behaviour change approaches in a structured programme. The base of thumb OA group achieved this by bringing together practical exercise sessions (based around those utilised in the OTTER II study 10 ) and educational sessions including information on condition, functional anatomy, splinting, lifestyle factors, joint protection and managing a flare-up.
Design
A qualitative evaluation of the base of thumb OA group was conducted between October 2023 and March 2024. As a service evaluation and in accordance with the Health Research Authority decision tool, ethical approval was not needed. Nevertheless, governance support was provided throughout the evaluation by the organisation’s Research and Evaluation team. Participants who took part were provided with information leaflets prior to the day of the focus group, and written informed consent was provided by all participants.
Participants and recruitment
Recruitment was purposive, with participants recruited from a database of patients who had indicated their willingness to be involved in the evaluation at the completion of the group: all had a clinical diagnosis of OA base of thumb.
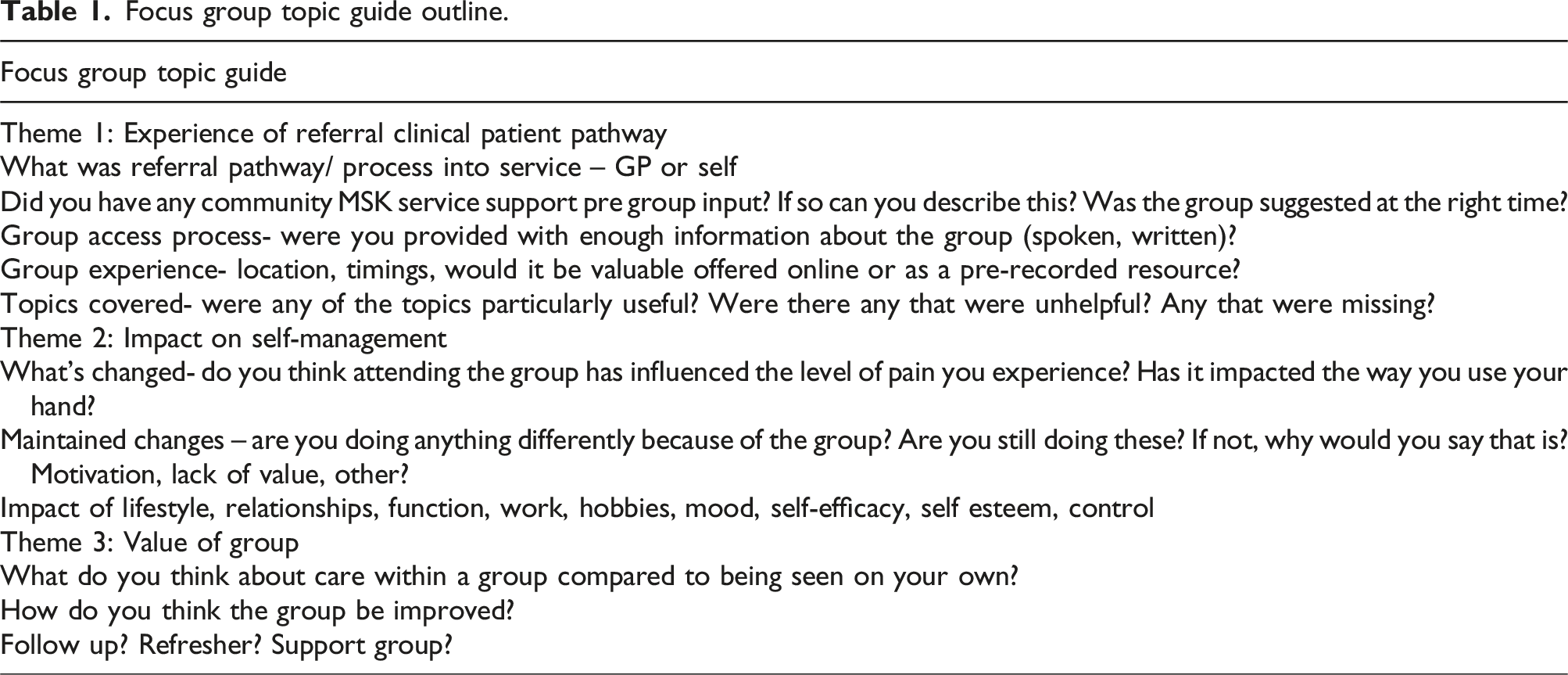
Group method and data collection
Focus group topic guide outline.
Researcher reflexivity
The evaluators were an advanced practice hand therapist (RB) and a clinical academic physiotherapist (RG). RB had been fundamental in the conception, design, and implementation of the base of thumb OA group. In addition, both evaluators had constructed the interview schedules and led the data synthesis process. Therefore, it was seen as essential that both evaluators were cognisant of their roles in the evaluation. Qualitative research findings are the result of a co-production between the evaluator and participants. 11 As such, evaluator reflexivity, acknowledging that the evaluators’ position may affect the research design, process and outcome is paramount. 12 Reflexivity was applied throughout in evaluator meetings. Nevertheless, the evaluators positionality, and their specialist knowledge, and experience, was an advantage. This experience is likely to have led to more iterative insights and a deeper exploration, and interrogation, of new topics as they emerged through the process. 13
Analytic procedure
Focus group data were digitally recorded and transcribed verbatim by an independent professional. A copy of the audio-file was saved in a secure digital folder. Initial analysis was undertaken by two evaluators (RB and RG) independent of each other, who then came together and collaborated on the generation of themes.
Inevitably, because of their positionality, the evaluators brought their own theories into the focus groups. As such, the evaluation sought to interrogate these ‘a priori’ theories and a component of the analysis was deductive. However, flexibility was also applied to allow for the inductive generation of new themes. As such, a hybrid approach to thematic analysis was used.10,14
Results
Three distinct themes were synthesised with reference to the evaluation aims; to understand patients’ experiences and views about the base of thumb OA group. and are reported as follows.
Excerpts from the transcripts are presented to authenticate the themes (coding: P=participant, F=facilitator).
Theme 1: Pathways
The participants’ experiences of patient pathways were explored with several subthemes emerging.
Referral methods
It was apparent that participants could be unclear who had referred them to the thumb OA group. Even when participants cited their referral originating from a doctor, they appeared unclear as to whether this was their own GP, the GP with special interest (who worked within the specialist hand interface clinic, or indeed a doctor at all. Overall, there was lack of clarity/recall on the referral processes involved: “I think I was referred by the doctor to the group, I think. Or it could have been one of the other people I’d seen” (P1)
There appeared to be a clear lack of awareness of the self-referral option. Indeed, participants were under the impression that a referral was a pre-requisite of attending. Most participants reported being referred by someone or being given details on how to self-refer. Only one participant reported using the self-referral system of their own volition having been made aware of this option during a previous course of physiotherapy. For most self-referral was not an option, or invisible to them.
Protocol driven
Data from participants suggested the referral process and access to the MSK Service (and the base of thumb OA group therein) was seen as a fixed, protocol driven process that they found frustrating: “It’s a protocol you have to follow, you can’t just bypass it..the protocol is GP, [health centre], you go through that. You have to go through the physio even though you don’t gain anything out of the physio, but it’s part of the protocol you have to follow.” (P6) “….And she gave me the exercises. And I asked about the injections, and she said I couldn’t have the injections unless I went to …. the four-week course.” (P4)
Waiting times from point of referral into MSK Service
Participants described prolonged waiting times that they found frustrating. Some participants were more consilient about the long waiting times in the context of the wider NHS. However, there were suggestions that information while waiting would be useful, both in term of timelines and self-management advice during the waiting period. “NHS under stress, and you’re always thinking you don’t want to put upon them….But obviously when it’s sort of okay, we’ll refer you here, and then you wait, and there's nothing in that in between. Like when you’re in the groups, you would get a text or an email to say, here’s a couple of exercises, try these.” (P1)
Members at different stages of their journey
Participants reflected that there was one single pathway that made no distinction for duration of symptoms. As such, the OA thumb group had a wide variation in symptom duration, clinical intervention exposure and symptom severity/ disability. Despite initial concerns about this heterogeneity, participants described this a being beneficial. “ what I found really interesting within the group, what that the other two people had as I say, their problems were much more severe. But both of them had had operations…to my recollection, they almost wish they hadn’t had the operations….that for me was a big lesson actually, not to necessarily think surgery would be the best thing.” (P2)
Theme 2: Group process/content
This theme describes the participant experiences around the processes and delivery of the group intervention.
Pre-group information
There was often a period of waiting following the internal referral to the start date of the thumb OA group. Participants described the information they were provided about the group, what the group involved and how to contact the service, if needed, as satisfactory.
Group accessibility and format
There was a strong feeling that the group was less accessible for people when English was not their first language: “Definitely, yeah… that's a tricky one...you can’t really do it without interpreters.” (P2)
In terms of delivery style, participants felt strongly that the group should be face-to-face. It was felt that if the group was face to face it facilitated relational interaction and practical issues such as supervising exercises. Challenges such as public transport and timing of the group during the day were also discussed. “ I have to say, I don’t think online would have been nearly as helpful. You know, when you’re interacting with the people, and you know like you say, you can see when someone’s in pain. And quite often they are holding, rubbing you know. So yeah, I felt the support was fine, I’m very glad it was face to face.” (P2) “10 o’clock is a bit early, because you know, it’s the transport network …definitely face to face…It was worth coming, I mean I made the effort, I came.” (P5)
Benefits of being in a group
Aligning with the consensus of holding the group face to face, participants also felt this facilitated the benefits of the group. “I think on a Zoom thing it’s just like, it’s just not the same, not the same as being in that room with other people.” (P5)
The group format allowed participants to share their common experiences of this condition: “Do you think being in the group might be helpful?(F2) “Yeah, it does, because you bring… because when [clinicians] talk about different things, you share your experience….and someone else will say something different…and you think, oh okay, that sounds a good idea, I might try that. So you do learn from other people.” (P3)
Benefits of the base of thumb OA group
Several participants highlighted that having the opportunity to modify tasks through hands on experience with assistive devices was a valuable aspect of the group process. For others, sharing ideas with each other and the associated psychological support were valuable: “It was very useful, very useful, because there’s things I have to say, you’re not really familiar with. And you know, such that that jar key, because I just avoided jars or had to get somebody to open them for me.” (P5) “I think there is something to be said about a group giving you that psychological support, you know. Whether you realise it or not you know, I think is something to be said.” (P2) “I think I would still be wearing the [splint] on my hand if I hadn’t been to the group, because I wouldn’t have done the exercises to be honest...I’ve used my thumbs more in the last few weeks than I have done in the last few months.” (P4)
Participants were aware of the long term nature of base of thumb OA and the challenge to maintain the management approaches they had adopted.
Theme 3: Living with OA
Participants described the experience of living with base of thumb OA, the relationship between activity and symptoms, and maintaining changes in behaviour learned throughout the group.
Psychological impact
Participants widely acknowledged the biopsychosocial complexity of living with base of thumb OA. Participants spoke of the relationship between their symptoms and their psychological and emotional state, such as feeling isolated and low in mood. They also acknowledged how the emotional impact could influence their sleep and activity levels. For some this meant adapting activities of daily living and for others this had resulted in them moving out of employment. “...it affects your sleep patterns, it does affect your mood. I mean today would be a day of, I just wouldn’t venture anywhere.” (P5) “I was working as a carer, and that's how I’d fell across my problem. And I gave up, because I thought, oh I just can’t; do this anymore. And that was I think, before I came to the group even, probably.” (P2)
Making and maintaining changes
In terms of changes arising from attending the group, participants spoke about use of devices and task modification. There were mixed responses in terms of using principles such as pacing or continuing with existing activity levels (“You don’t think, you just do” (P1)).
There was a strong feeling amongst the group, that to assist with living with a long-term condition such as OA, there needed to be some long-term support. Their feeling was this would support motivation and the application of the self-management principles. Participants proposed drop-in groups, ideally facilitate by a member of the community MSK service, as a way to address this need. “The group’s great, but I need it sort of as an ongoing therapy...I wondered about an arthritis drop-in centre once a month or something. Where there is somebody, you know, that can be on hand that people can come to.” (P2)
Discussion
Summary
Base of thumb OA is a common degenerative disease, causing varying degrees of pain, stiffness, weakness and increased functional loss. 1 Most patients will initially present to their GP. It is important that patients have timely access to the most appropriate therapy interventions, 15 however the evidence shows that at the point of referral to interface services, many patients newly diagnosed with base of thumb OA have been managed with analgesics. 16
It was apparent, from the participant data, that the referral pathway was unclear. Participants had limited knowledge of the community MSK service in general and almost no prior knowledge of the base of thumb OA group. It appeared that the self-referral route was invisible to participants, unless they had previous exposure to it. This is problematic, particularly within a healthcare system that is overburdened. Self-referral has the potential to alleviate demand on general practice and simplify the patient pathway, and experience. Neither of these objectives appears to have been realised in this evaluation. In addition, this unclear pathway, and the long waits associated with it are frustrating to patients. Furthermore, the participants’ perspective was that the pathway was protocol driven. Participants felt unsupported during, what were, long waiting times and made suggestions as to how this could be improved.
Participants were positive about the group structure and content. Participants recognised the biopsychosocial nature of base of thumb OA and acknowledged. Participants felt that the group content and the group structure supported the management of their condition. Participants were clear in their views about the benefits of the group being face-to-face, rather than offered online.
Nevertheless, alongside this strong opinion regarding the face-to-face nature of the group there were some other access considerations. For some, the travelling involved presented a potential barrier and thought attention should be paid to location and timings of the group to facilitate attendance. Importantly, equality, diversity and inclusion could be improved and there was a suggestion that the service considered this in the future.
In addition, participants expressed a need for further follow up, or support to assist with maintaining behaviour changes learned within the group.
Comparison with existing literature
There are several parallels with existing literature. Fundamentally, the base of thumb OA group was efficacious, with patients describing various positive attributes of the group and positive outcomes. This aligns with previous research examining combined conservative management for base of thumb OA. 9 Furthermore, it was clear from the participants comments that base of thumb OA is a complex, long-standing health condition that sits within a biopsychosocial framework and, as such, requires an approach in keeping with this complexity.4,8
It was evident that access to the group was somewhat unclear to the participants. The apparent and potentially problematic lack of awareness related to self-referral access has been reported elsewhere; despite the participants positive narrative about physiotherapy, awareness and understanding of the role and access was poor.17,18 Patient perception of beneficial strategies for hand OA at the point of contact with a GP and subsequent access to specialist therapy skills can be limited. 15
In this evaluation, it was also evident that access to all population groups was inequitable. Concordant with previous evidence, access may be compromised for patients whose first language is not English. 19
Strengths, limitations, and future research
This evaluation was novel in its intent to specifically assess the patient perception of a community base of thumb OA group. A limitation is that only two focus group with six participants were recruited to this evaluation. It is possible that alternative insights may have been elucidated had a larger and more diverse sample been recruited. Furthermore, participants were drawn from one service in one specific geographical location and as such the results are context specific. Future research could focus on a larger, controlled trial and considering many of the base of thumb OA population are managed initially by their GP, an evaluation whereby the base of thumb OA group is accessed earlier in the MSK pathway would be indicated. As a pragmatic service evaluation, resources were limited and consequently participant numbers were quite low although the evaluation team were satisfied that, for their interview schedule, the topics under discussion did reach saturation. 20
Implications for practice
There are several important implications for practice that can be drawn from this evaluation. The first is that the base of thumb OA groups appears to be efficacious and well received by patients. As such, the service provider can be confident in this treatment approach. Nevertheless, the groups may remain invisible to some (where referral pathways are unclear) and inaccessible to others- most specifically those who cannot travel and those who do not have English as their first language. The organisation should work with partner organisations- GPs, commissioners, and patient representatives- to better understand these access issues. Waiting well and long-term support were important themes raised through discussion. The above implications for practice will all be incorporated into the quality improvements made as a result of this service evaluation.
Conclusion
In conclusion, our results provide support for the base of thumb OA group. Further research is needed to build upon what is a small, pragmatic service evaluation. Issues of access, both generally and within underrepresented populations needs consideration at a service provider level to increase equity of provision. Longer term follow-up or support options should be explored. This group is a comprehensive intervention which was described as efficacious and well received by patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.