
Abstract
Introduction
Limited research exists on the post-operative treatment of extensor pollicis longus (EPL) repair (tendon transfer and direct repair). Early active motion (EAM) and dynamic extension splinting (DES) are becoming more common compared to static casting. The aim of this systematic review was to determine whether EAM was superior to DES post EPL direct repair or tendon transfer. Outcomes of interest included range of motion, strength, and adverse events.
Methods
A systematic search of AMED, EBSCO health database (CINAHL, MEDLINE, and SPORTDiscus), and Scopus was completed. Randomised control trials or cohort studies were included if they followed either an EAM or DES rehabilitation protocol and assessed total active motion, grip strength, pinch strength, or range of motion post EPL surgical repairs. Data extracted included the surgical procedure, rehabilitation protocols, and results. The Downs and Black checklist for clinical trial quality assessment was utilised to assess the methodological quality.
Results
Six studies met the inclusion criteria. Five studies included DES and two studies included EAM. Both interventions resulted in improvements in ROM, grip strength and pinch strength with neither intervention being superior. There was no increase in adverse outcomes by using EAM or DES. The risk of bias following assessment of methodological quality of included studies ranged from good to poor.
Discussion
The use of EAM should be considered post EPL repair or tendon transfer. EAM does not result in superior outcomes post EPL repair compared to DES, equally EAM does not appear to be inferior compared to DES.
Keywords
Introduction
Extensor pollicis longus (EPL) is the main extensor of the thumb. It is responsible for extending the thumb at the interphalangeal joint (IPJ), metacarpophalangeal joint (MCPJ), and carpometacarpal joint (CMCJ). 1 Patillo and Rayan 2 reported thumb injuries to be the most common extensor injury comprising 26% of extensor tendon injuries followed by the index finger at 25%, with laceration to the dominant hand being the most common cause of tendon injury to the thumb. Zone TV was most injured with 69% of thumb injuries occurring in this zone. EPL repairs are commonly grouped with digital extensor tendon injuries even though the anatomy and function of these tendons differ.3,4 Furthermore, these studies reported low numbers of EPL injuries and a limited number of studies focused specifically on EPL repairs in isolation. 4 This makes the assessment of treatment protocols for EPL tendon injuries challenging.
Post-operative treatment, historically, has focused on full immobilisation of the thumb in extension for 3-6 weeks3,5 Immobilisation after direct repair can cause tendon tethering and adhesions particularly in the extensor tendons due to their extra-synovial position and their close proximity to bone and other tissues.3,5,6 Tendon tethering and adhesions cause restrictions to tendon gliding and limit thumb movement,7,8 making these adverse events difficult to treat.
9
To prevent such post-operative complications, treatment has included passive tendon mobilisation at the wrist and thumb
10
through dynamic extension splinting (DES) (Figure 1).
4
Wood et al.
4
completed a systematic review comparing rehabilitation protocols following EPL surgical repair to zones TI - VIII and found DES to have a superior outcome than static splinting (Figure 2) with greater range of motion (ROM), total active motion (TAM), grip strength, and pinch strength 4-6 weeks post-operatively. In addition, the results showed that DES shortened rehabilitation time and reduced complications.
4
In this systematic review only one article looked at EAM, this study showed 83% of patients had good-excellent results for TAM.
4
An example of a dynamic extension splint. An example of a static splint.

Early active motion (EAM) is also used to help prevent adverse events associated with immobilisation. EAM is being used more frequently following extensor digitorum communis repairs,11–13 however EAM is less commonly reported for EPL repairs. Discussing two case studies, Burr and Pratt 14 reported that EAM provided faster recovery of active ROM compared to immobilisation post EPL repair in Zone TIII. In addition, EAM led to an earlier discharge (4 weeks) compared to immobilisation (12 weeks). 14 A case series by Van Veenendaal and Moate 15 showed that EAM post EPL repair in Zone TII led to excellent IPJ extension and good TAM of the thumb by 8 weeks, with no adverse outcomes reported. EAM allows tension and motion to be applied across the surgical site and this has been shown to increase tendons strength through an upregulation of collagen deposit. 16 EAM has also been shown to generate greater tendon excursion than passive movement 17 reducing the risk of adhesions. DES only applies passive movement to the repaired tendon, which may provide inferior outcomes. However, when DES is compared to EAM for extensor direct repairs zone IV–VII in the digits they are equally effective. 18 Collocott et al. 19 have shown EAM type protocols to be safe, with no tendon ruptures, following extensor digitorum communis direct repairs.
Considering the trend towards EAM protocols following digital extensor direct repairs and the benefit of movement on tissue healing, the present review aimed at determining whether EAM results in better outcomes post EPL repair compared to DES. In particular, ROM, grip strength, pinch strength, and adverse events such as rupture, adhesions, tethering or infection were outcomes of interest. With the significant benefits of active motion compared to passive motion on healing tissues it would be expected that EAM protocols would be more beneficial than DES.
Method
Study design
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 20
Search strategy
Search strategy.
Note. A summary of search terms used in database searches.
Study selection
Studies were included if they were randomised controlled trials (RCTs) or cohort studies that assessed patients post EPL surgical repairs (repair or tendon transfer); if post-operative treatment included EAM or DES; and if they assessed grip strength, pinch strength, TAM/ROM, or adverse events as outcome measures. Studies were excluded if they were not in English, included extensor digitorum communis direct repairs, were cadaveric studies, or were case studies/series. Inclusion and exclusion criteria were applied during title, abstract and full text screening. The reference list of the studies included was checked for additional eligible studies following which inclusion and exclusion criteria were applied to these studies also.
Data extraction
The primary author (CB) extracted the following data from all included studies: authors, date, study design, participant number and characteristics, eligibility criteria, intervention, length of follow-up, results, and adverse events.
Quality evaluation method
The Downs and Black checklist, which can be used for assessment of risk of bias for both RCT and non-randomised studies, was utilised to assess the methodological quality of each study. 21 The Downs and Black checklist has been found to be suitable for use in systematic reviews and it has been shown to be have high reliability and validity. 22 O'Connor et al. 23 have shown excellent inter-rater reliability for the Downs and Black checklist.
Five areas were assessed using the Downs and Black checklist: reporting, external validity, internal validity, selection bias, and power. The maximum score for the tool is 32. Scores can be described as excellent (26-32); good (20-25); fair (15-19); and poor (<14). 24 Two authors (CB and NM) scored all included papers independently. Where disagreements occurred, the third author (RE) was asked to moderate until consensus was reached. Cohen’s Kappa was employed to assess the level of agreement among reviewers when scoring research papers. The calculated Kappa statistic provided a quantitative measure of inter-rater reliability, helping to gauge the consistency of assessments beyond what would be expected by chance alone. 25
Statistical analysis
A Bayesian framework was employed to estimate the posterior probabilities of tendon rupture rates across different surgical techniques and post‐surgical rehabilitation protocols. Two primary groups were considered: direct repair and tendon transfer. For each group, patients were assumed to be equally distributed between two post‐surgical protocols—EAM and DES—with prior probabilities set at 0.5 for each protocol.
For the direct repair group (n = 120), the rupture rates were assumed to be 0.001 under the EAM protocol and 0.02 under the DES protocol. In the tendon transfer group (n = 66), the corresponding rupture probabilities were 0.09 for EAM and 0.036 for DES. The observed number of ruptures for each subgroup was modelled using a binomial likelihood. A non‐informative Beta(1, 1) prior was used for all subgroups, leading to posterior distributions of the form:
For each repair method, the overall rupture probability was calculated by taking a weighted average (with equal weights of 0.5) of the posterior estimates from the two protocols. To compare the two surgical groups, 10,000 samples were drawn from the overall posterior distributions for both direct repair and tendon transfer. The proportion of simulations in which the rupture probability for tendon transfer exceeded that for direct repair provided an estimate of the probability that tendon transfer is associated with a greater rupture risk.
Results
A total of 178 studies were identified following the search (Figure 3). After duplicate removal and exclusion of non-English studies, 115 studies remained. Screening of titles and abstracts of these studies led to the exclusion of 83 studies. The remaining 32 studies underwent full text review. Five studies were included, and the reference lists were checked for additional studies. One further study was identified through reference search, and it met the inclusion/exclusion criteria. A total of six studies were included in this systematic review. Prisma diagram.
Participant characteristics
Study and participant characteristics.
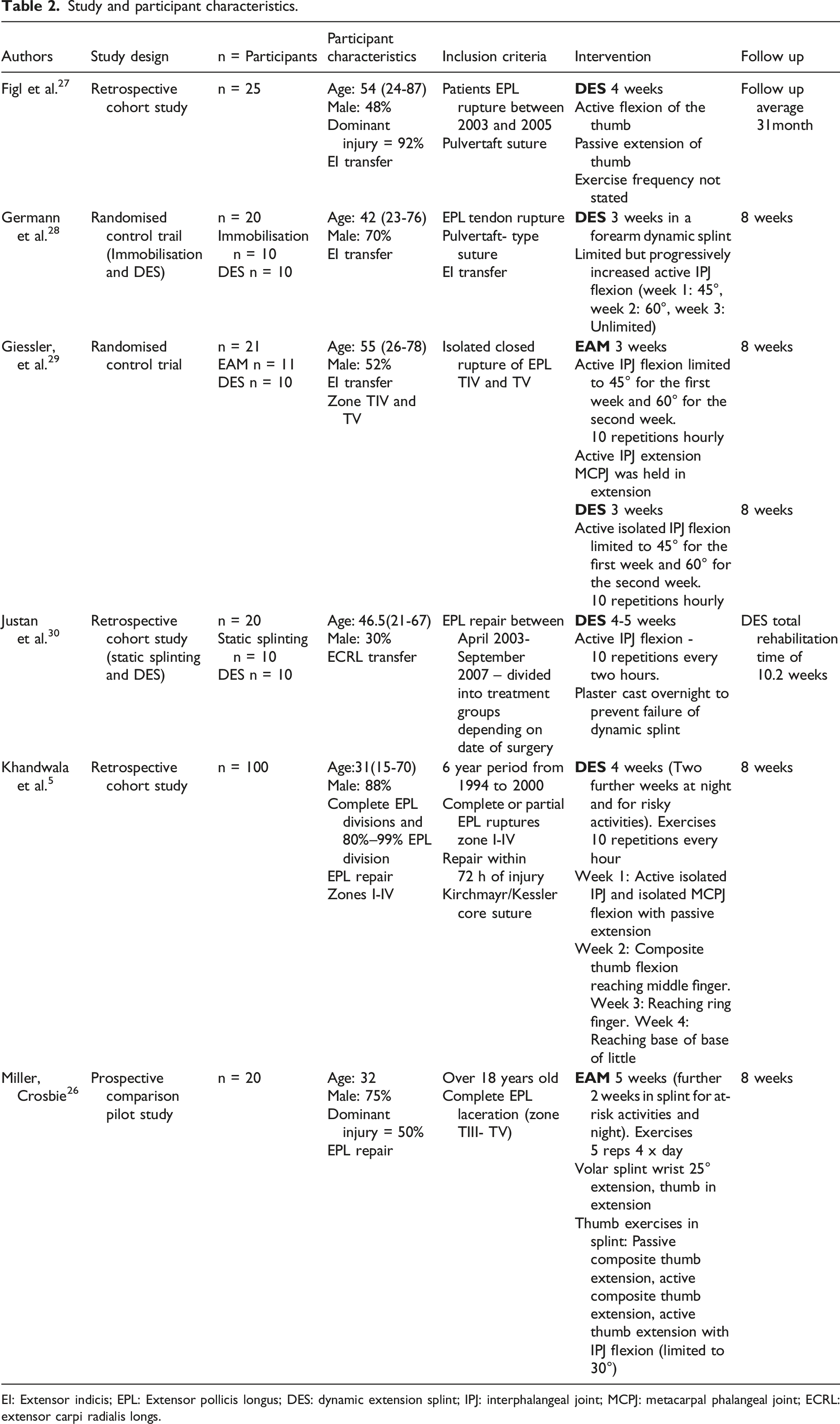
EI: Extensor indicis; EPL: Extensor pollicis longus; DES: dynamic extension splint; IPJ: interphalangeal joint; MCPJ: metacarpal phalangeal joint; ECRL: extensor carpi radialis longs.
All participants had EPL ruptures and no other injury to the hand. The cause of EPL rupture varied between studies as did the zone of injury. The participants reported by Miller and Crosbie 26 all had complete lacerations to the EPL in zone TIII-TV and had surgery within 14 days of the injury occurring. The participants of Figl et al. 27 all had EPL ruptures due to metalware after surgical management of distal radius fractures but did not report how long participants waited for EPL repair or the zone injured. Due to the mechanism of injury being metalware on the distal radius it can be assumed zone VII or VIII was where the injury occurred. Distal radius fracture as well as rheumatoid arthritis and insidious tendon rupture were reported as causes of EPL rupture in two studies.28,29 The EPL ruptures reported by Giessler et al. 29 occurred in Zone TIV and V. Justan et al. 30 reported EPL rupture due to falls, fracture, injury, arthritis, and from iatrogenic causes but did not report which zones were injured. They also had a significant delay in receiving treatment, 20.7 weeks (1 day – 2 years). 30 Delayed presentation results in a tendon transfer being required instead of direct repair. 31 Khandwala et al. 5 was the only study that reported including 80%–99% EPL divisions in their study. Eighteen participants had partial divisions and 82 participants had complete EPL ruptures. The cause of injury was laceration (90%), crushing/blunt trauma, and motor vehicle accidents. Injures occurred in Zone TI- TIV and were repaired within 72 h of injury. 5
Surgical repair technique’s used were Pulvertaft suture,27–29 modified Kessler or horizontal mattress, 26 and Tajima variant of the Kirchmayr/Kessler suture. 5 Justan et al. 30 did not state the suture technique used in the repair. Tendon transfers were performed in four studies, extensor indicis was used in three studies27–29 and extensor carpi radialis longus in one study. 30
Study intervention
Table 2 summarises individual interventions used for each included study. In all studies DES allowed some active flexion of the thumb IPJ with extension being applied passively by the dynamic component of the splint. This was isolated to the IPJ in all studies except Khandwala et al. 5 who allowed active isolated MCPJ flexion as well as isolated IPJ flexion by changing how the splint was fitted for each exercise. EAM protocols included various active extension of the thumb, Giessler et al. 29 allowed this at the IPJ whereas Miller and Crosbie 26 allowed composite thumb extension. In two studies the DES was worn full time for 3 weeks and exercises consisted of isolated active IPJ flexion which was initially restricted to 45° and gradually increased.28,29 Justan et al. 30 and Khandwala et al. 5 both used DES for slightly longer post-operatively, 4 weeks. Both studies allowed active IPJ flexion.5,30 Khandwala et al. 5 also allowed active isolated MCPJ flexion. This was progressed in the second week to include composite flexion, gradually increasing from reaching the middle finger, then the ring finger in the third week and base of little finger by the end of the fourth week. The DES was used to control MCPJ extension in zones TII-IV and in zone TI injuries it was fitted to control IPJ extension. 5 Figl et al. 27 also used DES that allowed active thumb flexion with passive extension, but did not state specific joints that were moved or the frequency of exercises making comparisons to this study difficult.
Miller and Crosbie 26 used EAM as their intervention, patients rested and performed their exercises in a volar splint (wrist in 25° extension and thumb extended) for 5 weeks (which was the longest immobilisation time of the included studies). During this time participants did exercises four times a day. Exercises included passive composite thumb extension, active composite thumb extension, active thumb extension with combined flexion of the IPJ (limited to 30°). Each exercise was repeated five times. 26 In Giessler et al. 29 the EAM group were splinted for 3 weeks and exercises were performed more frequently, 10 times every hour and included active IPJ flexion and extension with the MCPJ remaining blocked.
Methodological quality and risk of bias
Downs and Black scoring.

Results from CB and NM scoring the Downs and Black, with RE assisting if a consensus could not be reached.
Studies scored low on internal validity and selection bias, no study was able to blind their participants, two studies used independent people to measure the main outcome measures.29,30 Two studies used randomisation of their subjects in their studies.28,29 Miller and Crosbie 26 did not report random allocation of participants instead the rehabilitation protocol was selected by the surgeon, and this could have created significant bias if there was a perception of likely prognosis by the surgeon.
Non-adherence was reported by Khandwala et al. 5 where they had two EPL tendons re-rupture by participants not following post-operative protocol. No other studies reported issues with compliance to the intervention.
All studies, except Khandwala et al., 5 had low sample sizes meaning they may not be sensitive enough to pick up changes and adverse events. No studies undertook power or sample size calculations. Although Khandwala et al. 5 had 100 participants they had high loss to follow-up (23%).
Two studies did not use the unaffected side for comparison.28,30 Considering that ROM between participants varies, including the unaffected side for comparison would have allowed for a more accurate measurement. All other studies included the unaffected side for comparison.
Individual study results and outcome measures
Study results.

DES: Dynamic extension splinting; MCPJ: metacarpal phalangeal joint; TAM: total active motion; IPJ: interphalangeal joint; EAM: early active motion; ASSH: American Society for Surgery of the Hand.
Grip strength was assessed in three studies at 8 weeks27–29 and improved by a similar amount in all studies. Figl et al. 27 was the only study to report hand dominance with 92% of participants dominant hands affected. Without knowing hand dominance it is difficult to compare improvements between studies, the expectation would be that dominant hands would get greater improvements in strength. Giessler et al. 29 showed grip strength to be 66% of the unaffected side in DES group and 63% of the unaffected side in the EAM group. Figl et al. 27 and Germann et al. 28 both showed grip strength in DES groups to return to 75% of the unaffected side. Two studies examined pinch strength.28,29 DES and EAM had similar pinch strength at 8 weeks, 73% and 71% respectively 29 and 78% 28 when compared to the unaffected side.
Adverse events
Common adverse events post direct repair include rupture, adhesions, and infection.9,32 Tendon rupture’s were reported in two of the included studies.5,29 Khandwala et al. 5 DES group had two ruptures in the second week but these were due to participants being non-adherent and not wearing their splint. Giessler et al. 29 had one rupture which occurred 5 months post-operatively in the DES group, no cause was given but it was noted that the patient had a history of rheumatoid arthritis. Adhesions resulting in loss of ROM were reported in two studies.27,29 One occurred in the DES group in Figl et al. 27 and one in the EAM group in Giessler et al. 29 Germann et al. 28 and Miller and Crosbie 26 both reported there were no adverse events in their studies, these studies looked at DES and EAM respectively. Miller and Crosbie 26 was the only study to specifically mention infection as a possible adverse event and reported no cases of infection.
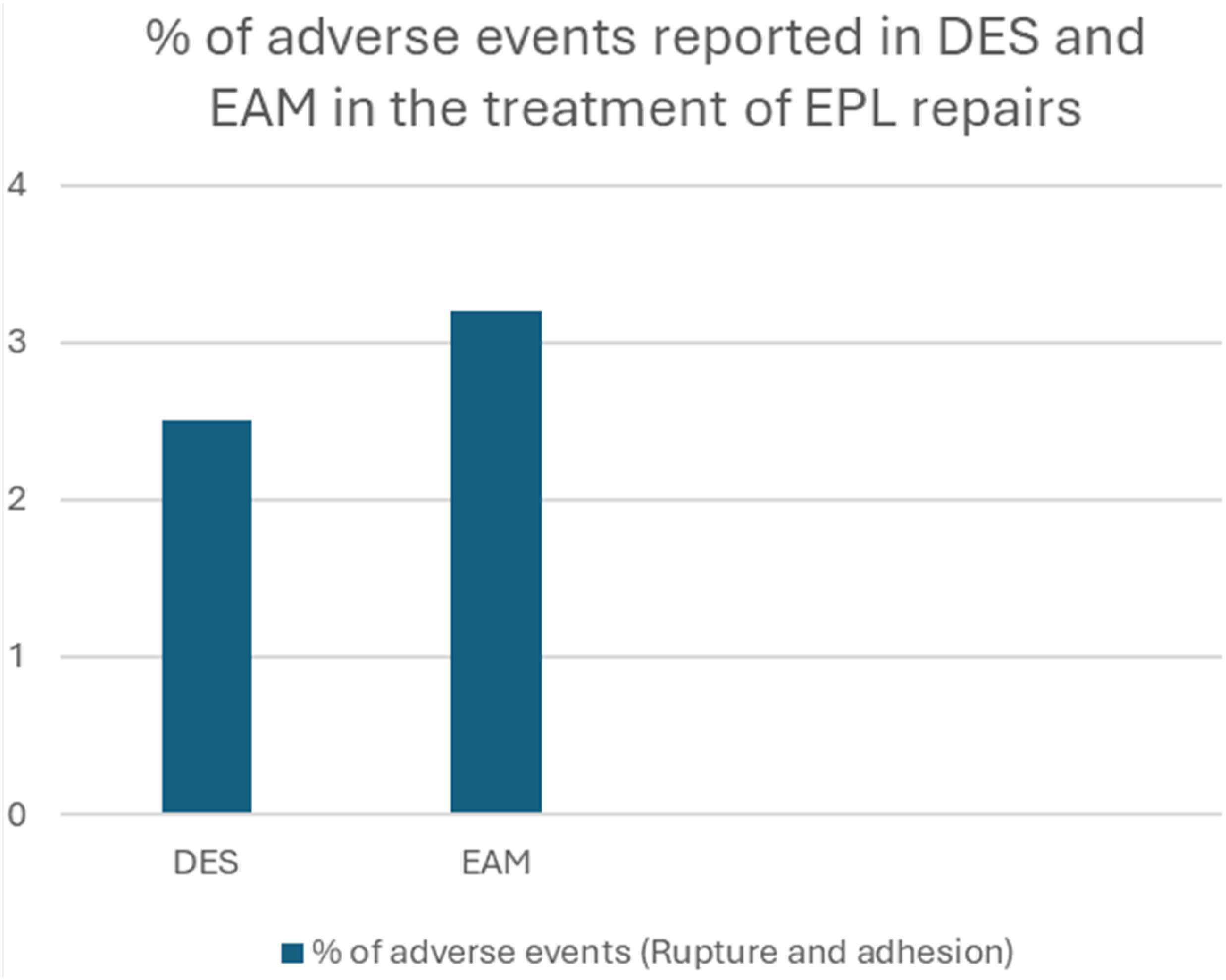
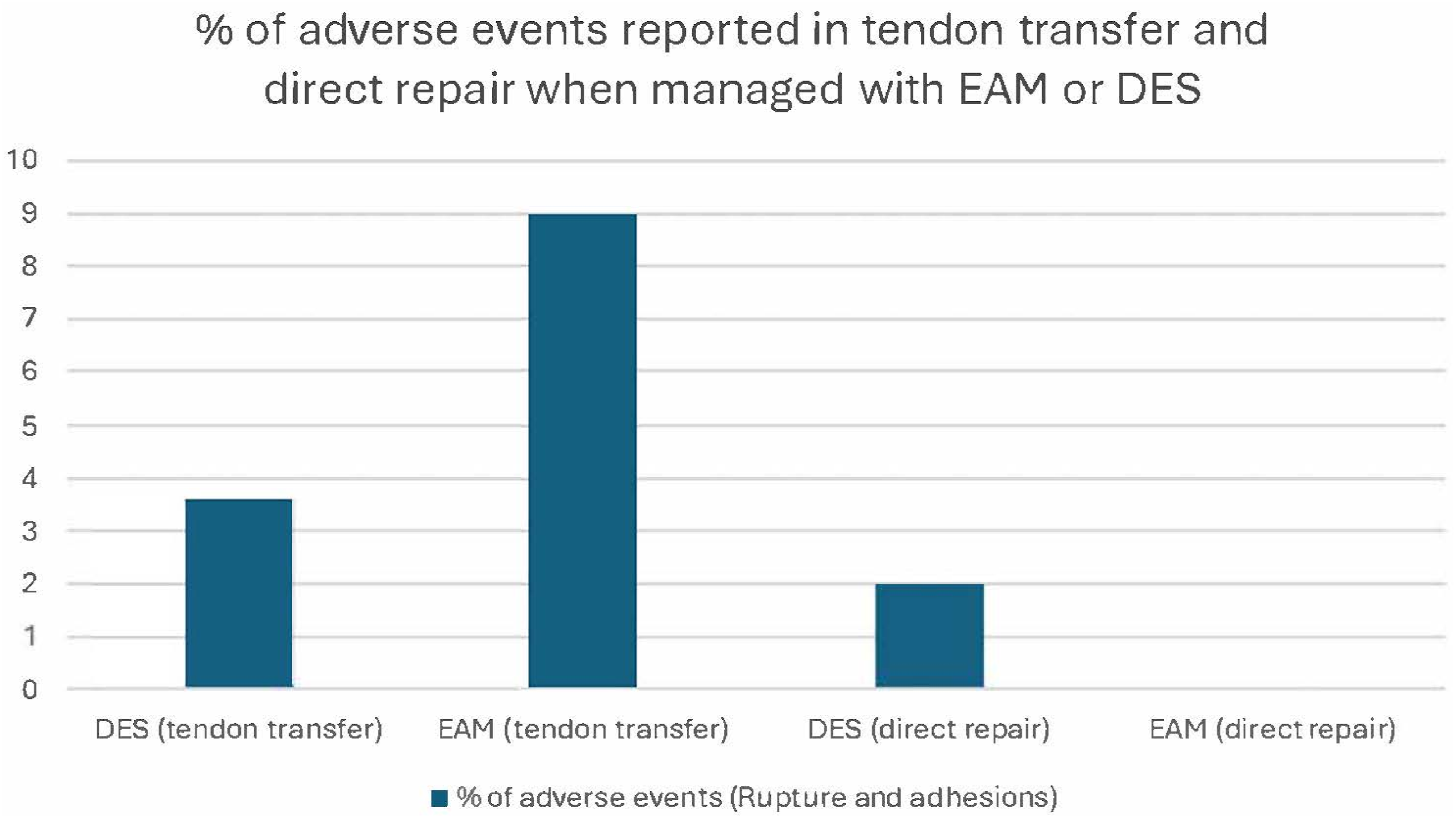
A Bayesian analysis was performed to estimate the posterior distributions of tendon rupture probabilities for the direct repair and tendon transfer groups. As illustrated in Figure 4, the posterior distribution for the direct repair group is centred at a lower probability of rupture, while the tendon transfer group exhibits a distribution shifted toward higher rupture probabilities. Based on 10,000 posterior samples, the probability that the tendon transfer group has a higher rupture rate than the direct repair group is 0.98. These findings suggest that, given the data and model assumptions, tendon transfer is more likely to be associated with an increased risk of tendon rupture compared with direct repair. The type of post-surgical approach had inconsistent effects on post-surgical adverse events (see Figures 5 and 6). Histograms providing a visual comparison of the uncertainty associated with each group’s rupture probability. Graph providing percentage of adverse events for DES and EAM. Graph providing percentage of adverse events for specific surgical techniques, tendon transfer and direct repair with respect to the post-operative treatment (DES or EAM).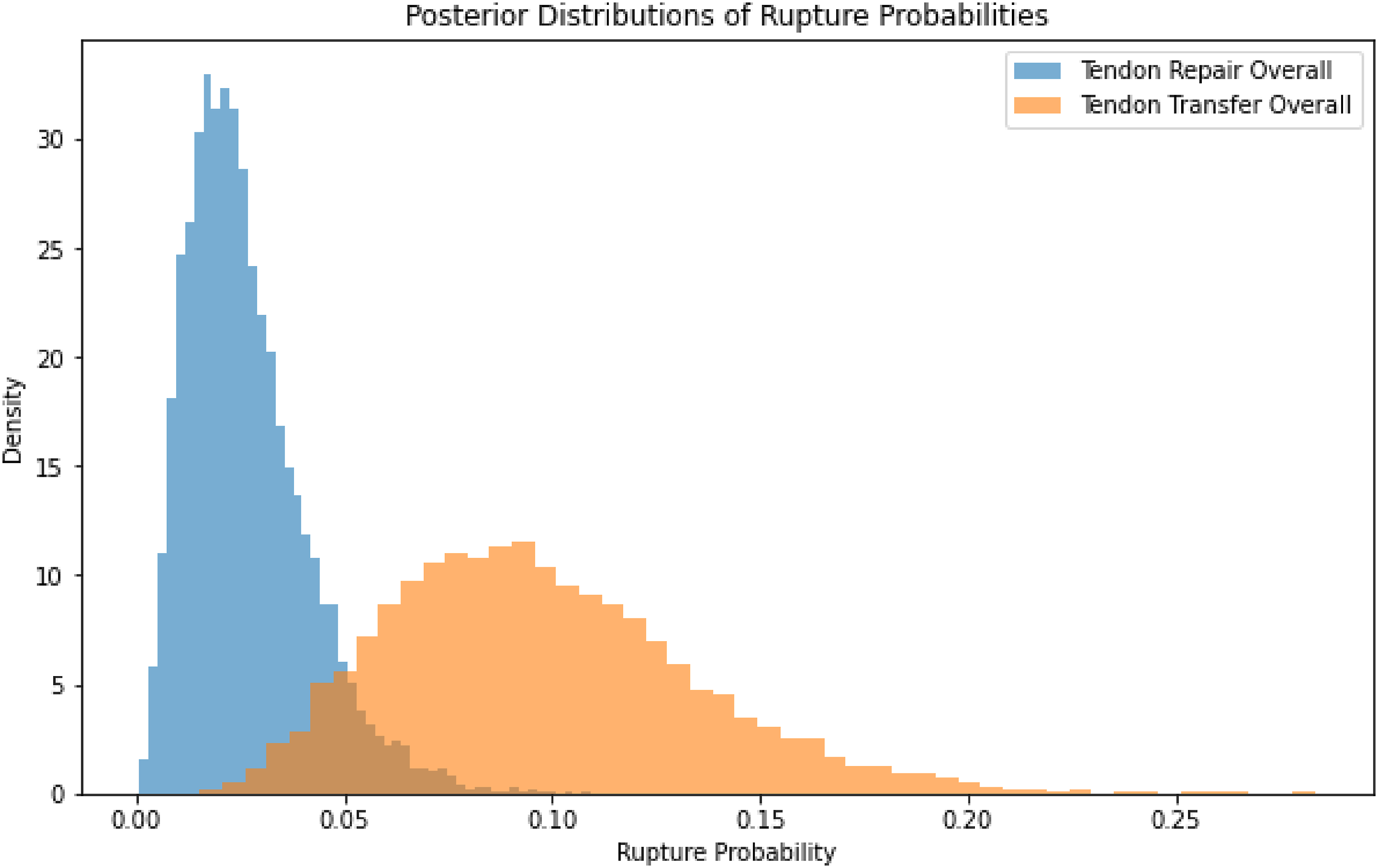
Discussion
The aim of this review was to assess whether EAM results in better outcomes compared to DES post EPL repair. The results showed that there is a small number of low to moderate quality studies on the topic. The findings of the current review suggest that there is not enough evidence to say that EAM results in better outcomes post EPL repair than DES. However, EAM does not appear to be inferior. All studies, regardless of intervention, reported improvements in numerous outcome variables including, ROM, pinch strength, and grip strength.
No ruptures were reported in any of the EAM studies. In the DES studies ruptures were reported in two studies (n = 3).5,29 Two of these, were due to participants removing their splint and one was 5 months after the surgery. Another adverse event was tendon adhesions. One participant in the DES group from Figl et al. 27 and one in the EAM group from Giessler et al. 29 reported tendon adhesions. When compared as a percentage, DES had 2.5% adverse events compared to EAM 3.2% (see Figure 5). Based on our Bayesian analysis, it appears that the greatest risk of adverse events is driven by the type of surgery (i.e. tendon transfer having higher risk than repair) rather than the post-surgical rehabilitation protocol.
With the known benefits of motion maintaining the health of tissues such as articular cartilage, dense connective tissue and joint mobility, 33 whenever possible motion should be maintained. Although motion is the aim of DES, this only allows passive movement, whilst EAM allows active tendon gliding. EAM had reduced rupture rates and no increase in adverse events, this indicates that some form of movement is possible post-operatively, particularly if the amount of motion applied is within the limits of the repair. 32 Motion and tension are beneficial for tendon healing with increased break strength and cellular activity. 16 This supports the use of EAM over DES.
Three studies stated the zones that were repaired.5,26,29 TIV was the only zone that was consistently mentioned in all three studies. These studies included DES and EAM as treatment. Two of the studies5,29 reported adverse events but it is not reported if these were related to specific zones. Due to the limited reporting of zones, conclusions cannot be drawn as to which zones may do better with DES or EAM.
Giessler et al. 29 was the only study that directly compared EAM and DES. The results from this study indicated that EAM does not accelerate recovery and had comparable results in IPJ ROM, pinch strength and grip strength when compared to DES. It was reported that participants in the EAM group may not have followed their protocol fully due to fear of doing something wrong or damaging the repair. It is important to consider the patients understanding and level of adherence when selecting patients for EAM protocols.
The exercises performed in the EAM group reported by Giessler et al. 29 were isolated IPJ flexion and extension. Other EAM protocols for the thumb or digits have included active composite extension and active extension with active IPJ flexion18,26 which would generate more tendon gliding and load through repaired site. 34 It is also worth considering that whilst performing passive extension in a dynamic brace, some active motion may be occurring, which would reduce the difference between the two interventions.
Thumb retropulsion was assessed by two studies. It had greater return in the EAM group in the study by Miller and Crosbie 26 compared to the DES group from the Figl et al. 27 study. The EAM group did exercises into thumb extension including passive composite thumb extension, active composite thumb extension, active thumb extension with combined flexion of the IPJ 26 and may indicate this is beneficial for greater return of thumb retropulsion. Figl et al. 27 did not state what exercises were preformed making it hard to compare and for this reason we cannot say that the improvements in retropulsion were solely due to the EAM protocol. More studies need to assess retropulsion as it is a key movement of EPL.
Both EAM studies showed an increase TAM of the IPJ at 8 weeks26,29 Participants of the Giessler et al.
29
study had regained more movement at the 8 weeks mark in IPJ motion (82%) compared to those involved in the study by Miller and Crosbie
26
(73%). Giessler et al.
29
had patients doing 10 repetitions every hour and had a shorter splinting time of 3 weeks, compared to the protocol of Miller and Crosbie
26
where exercises were done 4 times a day and 5 repetitions and splinted participants for 5 weeks. Although these results cannot be directly compared, it may indicate more frequent EAM and reduced splinting time may result in slightly better IPJ movement
Two studies looked at pinch and grip strength and had comparable improvements at 8 weeks post-operatively.28,29 Grip strength was also shown to be similar in the study by Figl et al. 27 but it was not stated when this measurement was taken. Longer follow-up is needed to assess for difference in strength to allow time for strength to be regained.
Although no studies documented low levels of compliance to splinting and exercises, future research would benefit from participants keeping a diary of exercise completion and splint wearing to ensure groups follow protocols as directed. If participants are being non-adherent this may cause results to be inaccurate for example people using a DES protocol removing their splints and preforming active movement. It may also lead to adverse events which are not directly related to the treatment. Blinding of participants was not possible in studies due to the use of a splint and specific exercises that participants had to perform. Blinding of assessors was not done in any of the studies but would be possible if participants had their splints removed and not visible whilst being assessed at follow-up. This would help reduce measurement bias in future studies
Four studies used tendon transfers to treat EPL rupture. Figl et al., 27 Germann et al., 28 and Giessler et al. 29 used EI transfers and Justan et al. 30 used ECRL transfer. EPL was repaired in the two other studies reviewed.5,26 In the EPL direct repair groups, EAM resulted in no adverse events compared to DES having two ruptures, 2% (see Figure 6). This may indicate that EAM is more beneficial for direct EPL repairs. In comparison, the tendon transfer studies reported adhesions being an adverse event with both the DES and EAM groups reporting 1, it was not documented if these were confirmed by ultrasound scan. In addition, a tendon rupture was reported in the DES tendon transfer group. This results in 3.6% adverse events in tendon transfer treated with DES compared to 9% when treated with EAM (see Figure 6). Overall, a greater number of adverse events were reported in the tendon transfer studies compared to direct EPL repair. Due to the limited number of studies it is difficult to determine whether the type of surgery is a more important factor than they post-surgical rehabilitation approach but it appears direct repairs do better with both DES and EAM than tendon transfers having lower percentage of adverse events. Further research would be beneficial to focus on whether direct repair or tendon transfer perform better from EAM or DES.
This review showed EAM and DES to have comparable results for ROM, grip strength, pinch strength and adverse events. There are other benefits of EAM that need to be considered. These include reduced cost of splint making, a less bulky splint which is easier to wear, and lower number of follow-up appointments for splint modifications. 36 Splint satisfaction and cost of treatment need to be considered in future research.
Clinical implications
Based on the current findings, EAM provides similar functional outcomes as DES with no significant difference in adverse events (DES 2.5% and EAM 3.2%). It may be a useful alternative to DES for suitable patients. For this reason, EAM should be considered as a treatment option post EPL repair particularly considering its reduced cost and ease of splint making. This may be beneficial for patients who cannot regularly attend clinic appointments.
Limitations
There are several limitations to this study. Firstly, grey literature was not searched and included. Only English studies were included. There were only a small number of studies that met the search criteria and the quality of these studies was low when assessed on the Downs and Black checklist. There were more studies looking at DES than EAM and significantly more participants in the DES groups, 155 participants versus 31 participants in EAM. Sample sizes were small in most included studies, reducing the overall strength of the evidence available, and no meta-analysis was conducted due to heterogeneous samples. Not all studies stated the zones where the EPL tendon was repaired. For this reason, conclusions cannot be made about what zones may do better with EAM or DES. Finally, this review was not registered a priori.
Conclusion
The findings from the present review show that EAM does not present with superior outcomes for ROM or strength when compared to DES and does not have a significant increase in adverse events. Additional reasons for the use of EAM are reduced splinting costs and potential greater patient satisfaction. There is need for a larger RCT to compare DES and EAM to assess whether one intervention is superior, assess the cost of treatment, and patient comfort/satisfaction associate with each approach.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.