
Abstract
İntroduction
In hand injuries involving thumb impairment, rehabilitation must be conducted meticulously as it is essential for restoring hand function and facilitating return to daily life and work. The aim of this study is to investigate the effects of prescribing mobile games as home exercises on recovery outcomes in patients with thumb involvement due to thumb injuries and/or carpal tunnel syndrome.
Method
This randomized controlled trial included 31 patients who were randomly assigned to either the routine rehabilitation (RR) group or the mobile game (MG) group. The primary outcome measure was functional status, assessed using the Quick Disabilities of the Arm, Shoulder, and Hand (Q-DASH) questionnaire. Secondary outcomes included hand function evaluated with the Duruöz Hand Index (DHI), activity-related pain assessed using the Visual Analog Scale (VAS), range of motion (ROM) measured with a goniometer, edema assessed with a tape measure, and adherence to home exercises monitored using a home exercise tracking form.
Results
In both groups, statistically significant improvements were observed in all parameters after treatment compared to baseline (p < 0.05); however, no differences were found in the primary outcome measure (p > 0.05). In the between-group comparison, a significant difference in favor of the MG group was observed only for total active motion of the metacarpophalangeal joint and adherence to home exercises (p < 0.05).
Conclusion
Mobile game–assisted home exercises appear feasible for patients with thumb involvement. While MCP joint motion improved significantly, no differences were found in pain or function. Further research is needed to confirm clinical relevance.
Introduction
All fingers of the hand are involved in various manipulative abilities and contribute to many activities in our daily lives. 1 Considering that the thumb plays approximately 40% of the role in hand functionality, it can be stated that the thumb holds a key role in daily manipulative skills compared to the other four fingers.1,2 Therefore, in hand injuries involving thumb impairment, rehabilitation must be carried out meticulously, as it is crucial for restoring hand functionality and facilitating a return to daily life and work.
The time spent in clinical sessions is not sufficient for quality and rapid recovery. In fact, patients spend significantly more time at home than in the clinic. Therefore, home exercises play a foundational role in achieving effective rehabilitation outcomes,3,4 ensuring the continuity of treatment when access to a therapist is not possible. Additionally, they offer several advantages, such as reducing healthcare costs by spacing out clinical sessions. However, the lack of immediate feedback and supervision remains their most significant disadvantage. 5 Home exercises prescribed for hand therapy often consist of written exercise instructions. However, this method may lead to irregular exercise performance or complete discontinuation of the exercises. 6 Poor adherence to home exercise programs and failure to perform the prescribed exercises reduce the effectiveness of rehabilitation, thereby negatively impacting recovery outcomes. 7
In contemporary clinical practice, the use of technological support is increasingly prevalent in various therapy fields, including hand rehabilitation. However, home-based exercise programs typically do not incorporate technological support. 6 This is because technology-supported devices used in clinics often require equipment such as gaming consoles and monitors. This, in turn limits patients’ ability to perform exercises anywhere they wish. 8 Since technological devices such as smartphones and tablets are widely used and accessible across all age groups,9,10 their integration into the rehabilitation process presents an opportunity for technology-supported home exercise programs. 6
In most applications used on smartphones, thumb function is predominant: this is also true for many mobile games. The majority of games played on phones require controlled thumb movements, rapid responses, fine motor skills, and precise thumb positioning. Additionally, each game provides sensory feedback through touch interaction. 11 Therefore, when used for appropriate durations, mobile games may particularly enhance thumb joint range of motion. To the best of our knowledge, no studies have investigated the use of mobile games in thumb rehabilitation. So, the aim of this study is to incorporate mobile games as home exercises into the rehabilitation of patients with impaired thumb function and to evaluate their impact on functionality, normal joint range of motion, pain, edema, and adherence to home exercises.
Methods
Study design
This study was a randomized controlled trial. The experimental group consisted of patients received mobile game (MG) intervention, while the control group received routine rehabilitation (RR). Blinding was not implemented for interventions or assessments; however, blinding was ensured for the individual conducting the statistical analysis. All assessments in both groups were conducted for each patient on the first day of rehabilitation and on the final day before discharge.
This study protocol was reviewed and approved by the Ethics Committee of Clinical Research and conducted in accordance with the principles stated in the Declaration of Helsinki. Before to treatment, all participants were provided with both written and verbal information about the study. They also gave their informed consent in writing to participate. The research was carried out between November 2024 and March 2025. This study has been registered on ClinicalTrials.gov under the ID: NCT06731972.
Participants
A total of 31 patients were included in the study. The inclusion criteria were as follows: being between 18 and 65 years of age, having adequate communication skills, and experiencing pain and/or functional impairment in the thumb (e.g., thumb fractures, tendon injuries, nerve injuries, osteoarthritis, trigger finger, carpal tunnel syndrome, ligament injuries, soft tissue damage, etc.). In addition, voluntary participation was required.
Patients who were illiterate, did not own a smartphone, were in the acute phase and/or had activity limitations, had a neurological, chronic orthopedic, or rheumatologic condition affecting the relevant limb, or had undergone carpal tunnel surgery were excluded from the study (Figure 1). Flow chart of the patients.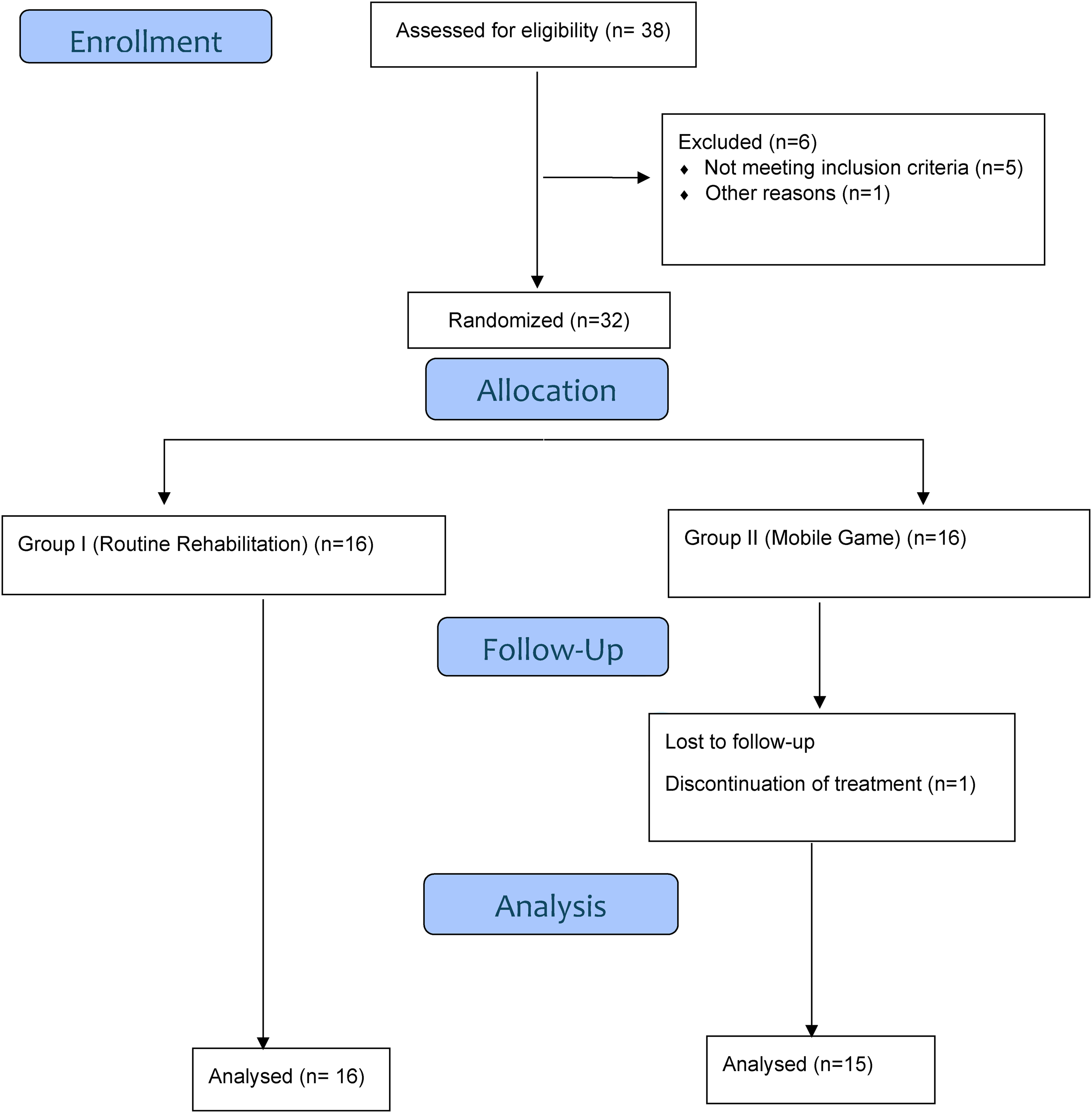
Patient enrollment and randomization
In order to ensure balanced distribution of diagnostic groups between the intervention and control groups, a minimization randomization method was used. This adaptive randomization technique takes into account participants’ diagnostic characteristics and assigns them to groups in a way that minimizes imbalance across predefined variables.
Interventions
Summary of the in-clinic rehabilitation program applied for patients.
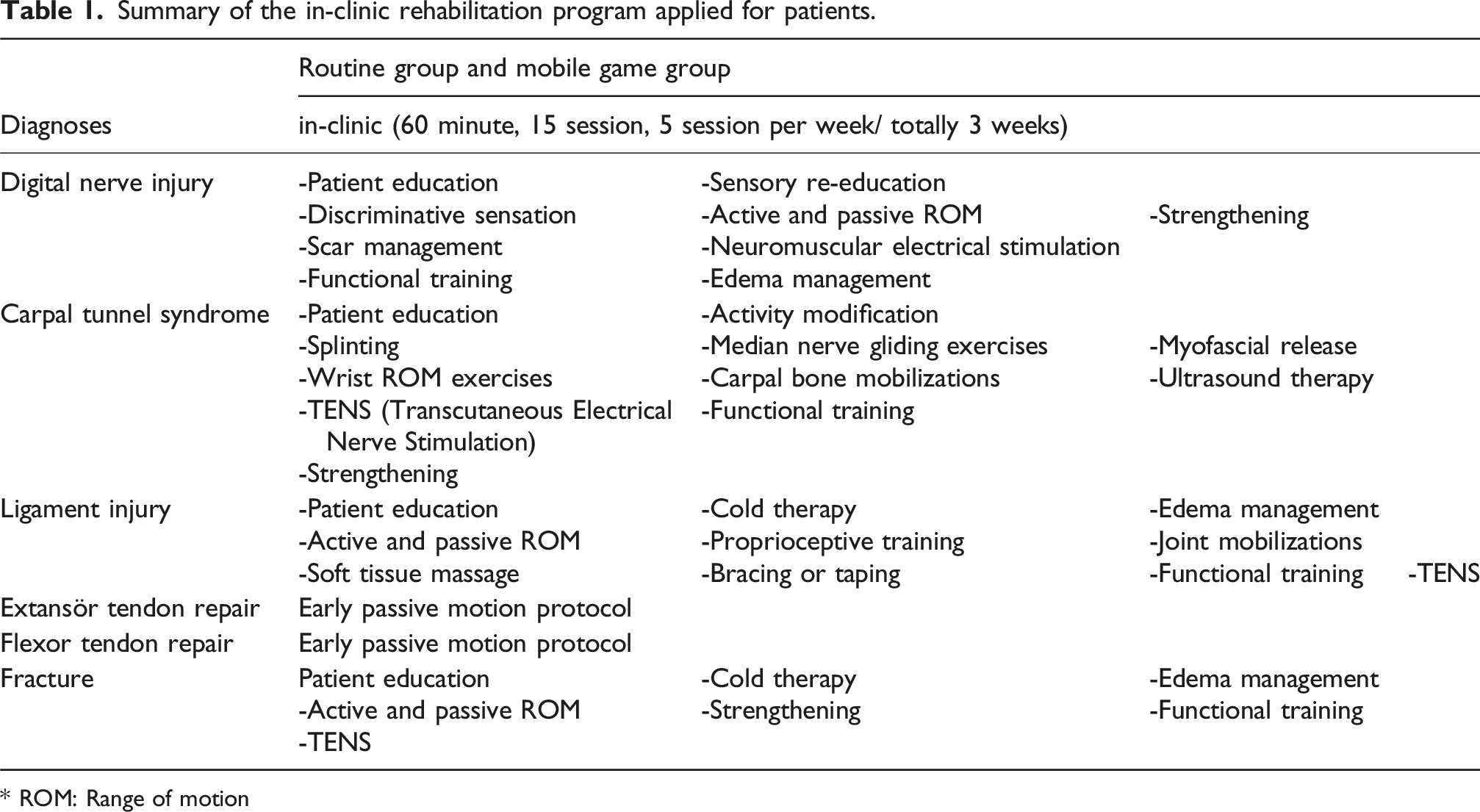
* ROM: Range of motion
Summary of the home exercise programs prescribed to patients.

* ROM: Range of motion
The MG group also received routine treatments that were specifically adapted and applied according to the diagnosis in the hand rehabilitation clinic during the sessions. However, unlike the RR group, routine home exercises were not prescribed. Instead, in the first session, a mobile game appropriate for the patient’s current functional status was recommended and taught. It was ensured that the patients had learned the game and were playing it correctly for the intended purpose. The routine treatments and home exercise programs applied to the MG group are summarized in Tables 1 and 2.
The games selected for the study, based on the literature, included Angry Birds, Temple Run, Piano Tiles, Perfect Piano, and Fruit Ninja 4 .
Outcome measures
Before initiating treatment, demographic data—including age, gender, occupation, education level, smoking status, injured hand, and history of surgery—were collected from all patients in both groups. Additionally, all patients were evaluated prior to the start of treatment sessions and again following the completion of all sessions. Assessments included activity-related pain using the Visual Analog Scale (VAS), normal joint range of motion (ROM) of the metacarpophalangeal (MCP) and interphalangeal (IP) joints using goniometry, functional status using the Duruöz Hand Index (DHI) and Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) questionnaire, and edema using circumferential measurement. Adherence to the home exercise program was also assessed at the end of treatment using a home exercise tracking form. All measurements were conducted by a single examiner to ensure consistency.
According to healthcare policies in Turkey, patients in this group are entitled to a maximum of 30 free physical therapy sessions per year. Although an initial recommendation of 15 sessions is typically made, this number can be increased up to 30 depending on the severity of the condition. To standardize the intervention across all participants, the 15th session was designated as the endpoint of treatment, and final assessments were conducted during this session.
Primary outcome
The Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) Questionnaire is a valid and reliable 11-item scale that assesses functional status and symptoms in individuals with upper extremity disorders and injuries. It is a shortened version of the original DASH questionnaire. Each item has five response options (1: no difficulty, 5: unable to perform). To calculate the score, at least 10 out of the 11 questions must be answered. The total score is calculated on a scale of 0 to 100, with higher scores indicating greater levels of disability. 12 In this study, since various diagnoses affecting thumb function were included, the QuickDASH provides a comprehensive assessment by covering the overall upper extremity functionality. Although some items (e.g., “carrying a shopping bag” or “tingling sensations”) may not be exclusively thumb-specific for all diagnoses, they reflect the patients’ general functional status in daily activities. Additionally, items such as opening a tight or newly sealed jar, performing heavy household chores, washing one’s back, and using a knife to cut food specifically evaluate tasks that involve significant thumb activity.
Secondary outcomes
Assessment of range of motion
The most commonly used objective method for evaluating joint motion in the literature is goniometric measurement, which has been proven to be valid and reliable. Although the universal goniometer is the most frequently used tool, finger goniometers are also among the available types. The selection of a suitable, adaptable, and reliable goniometer should be based on the specific assessment needs. 13 In this study, the total active motion of the MCP and IP joints (active flexion-extension loss) was measured using a finger goniometer.
Duruöz Hand Index (DHI)
The Duruöz Hand Index (DHI) is an 18-item scale designed to assess hand function in activities such as cooking, dressing, personal hygiene, and other daily tasks. Unlike some other functional scales, it does not evaluate pain, numbness, social life, or psychological state. The assessment takes approximately 3 minutes to complete. The total score is calculated out of 90 points, with higher scores indicating greater difficulty and restrictions in daily living activities. 14
Assessment of pain intensity
The Visual Analog Scale (VAS) is a widely used tool for assessing pain intensity, represented by a 10 cm horizontal line anchored by two extremes: 0 cm signifying “no pain” and 10 cm denoting “the worst imaginable pain.” Participants were asked to place a mark on the line that best reflected their current level of pain, and the distance from the zero point to the marked location was measured in centimeters and recorded for data analysis. 15 In a study conducted on a patient population undergoing non-shoulder hand and upper extremity surgery, the estimated Minimal Clinically Important Difference (MCID) for the VAS-Pain scale was calculated to range from 1.6 to 1.9, while the Substantial Clinical Benefit (SCB) was estimated to range from 2.2 to 2.6. 16
Assessment of edema
In clinical hand rehabilitation settings, finger circumference is typically assessed using either a standard flexible measuring tape or a custom-made gauge composed of a six-inch ruler with an attached measuring strap. In this study, edema was measured at the level of the proximal phalanx. Using a flexible tape measure, the circumference was assessed at the midpoint of the proximal phalanx, ensuring that the tape was in contact with the skin without applying compression. The measurement results were recorded in centimeters.
Assessment of adherence to home exercise program
All patients were asked to record the days on which they performed their home-based exercises. For this purpose, each patient was provided with a home exercise tracking chart prior to the initiation of the rehabilitation program. These charts were collected and documented during the post-treatment assessment following the completion of all rehabilitation sessions.
Each patient marked on the form whether they had performed the exercises on a given day, in accordance with the prescribed frequency and duration. Compliance scores were calculated based on the number of days the patient completed the prescribed exercises. For instance, a patient who performed the exercises on 13 out of a 15-days program received a score of 13, whereas a patient who exercised on 10 days received a score of 10.
Partial adherence (e.g., performing only 30 min of a prescribed 60-min session) was not included in the evaluation. Only whether the full daily exercise session was completed or not was considered. Therefore, the compliance scores reflect full-day participation only.
Statistical analysis
Statistical analyses were performed using SPSS software (version 25). The normality of variable distributions was assessed through visual methods (histograms and probability plots) and analytical tests (Shapiro-Wilk test). Descriptive statistics were presented as mean and standard deviation for normally distributed variables, while categorical variables were expressed as frequencies and percentages. Group comparisons of continuous variables were conducted using the independent samples t-test, whereas categorical variables were compared using the Pearson chi-square test. To evaluate changes over time and group-time interactions in measurement-based variables, a mixed-design repeated measures ANOVA was applied. For single-time point comparisons, the Mann-Whitney U test was used for non-normally distributed data. A p-value of <0.05 was considered statistically significant.
Sample size
The variable used in the sample size calculation was QuickDASH. Considering the minimal clinically important difference (MCID) of 15.91 and a standard deviation of 18 17 a power analysis was conducted using G*Power 3.1.9.4 with a significance level of 0.05 and 80% power. The analysis determined that a total of 34 patients were required. Accounting for a 10% dropout rate, the final required sample size was 38 patients, with 19 participants in each group.
Results
Comparison of the baseline values and descriptive characteristics of the groups.
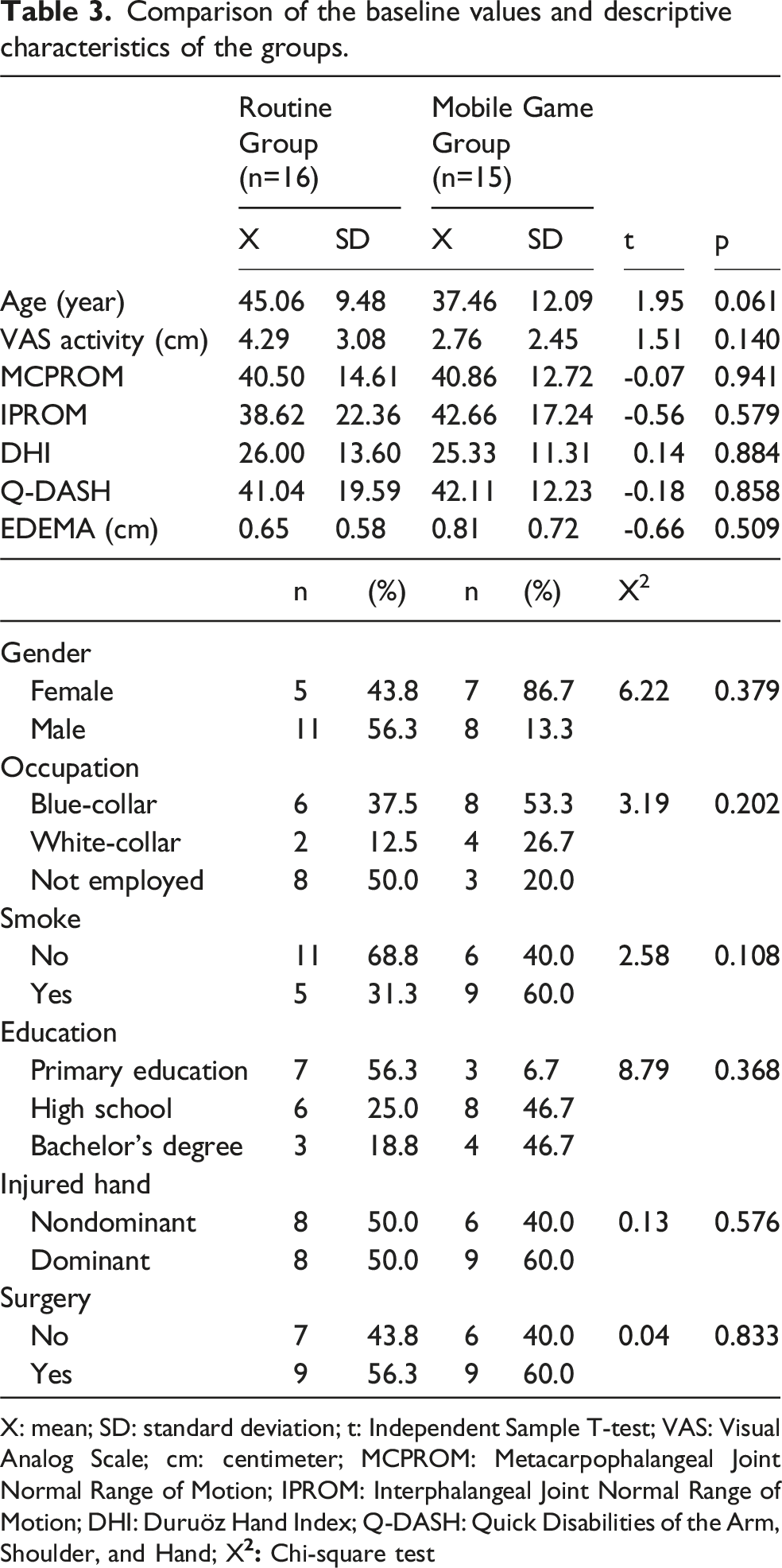
X: mean; SD: standard deviation; t: Independent Sample T-test; VAS: Visual Analog Scale; cm: centimeter; MCPROM: Metacarpophalangeal Joint Normal Range of Motion; IPROM: Interphalangeal Joint Normal Range of Motion; DHI: Duruöz Hand Index; Q-DASH: Quick Disabilities of the Arm, Shoulder, and Hand; X
In the RR group, the distribution of diagnoses was as follows: one digital nerve injury, 2 cases of carpal tunnel syndrome, two ligament injuries, four fractures, four extensor tendon injuries, and three flexor tendon injuries. In the MG group, the distribution included one digital nerve injury, 2 cases of carpal tunnel syndrome, two ligament injuries, three fractures, four extensor tendon injuries, and three flexor tendon injuries (Figure 2). Distribution of diagnoses among patients.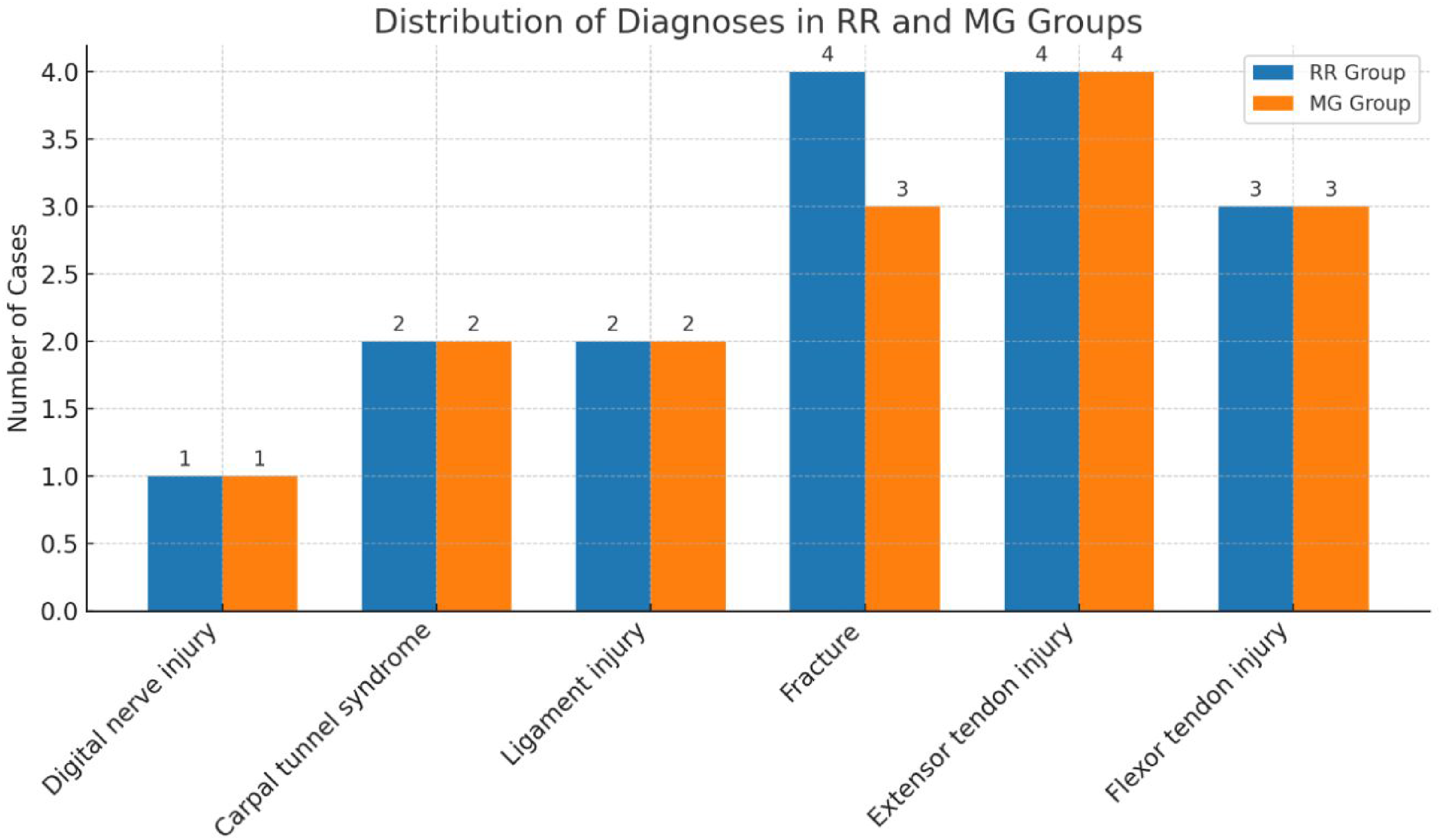
Comparison of the pre- and post-test values of VAS activity, MCPROM, IPROM, DHI, Q-DASH Edema, and AHEP measurement data between the Routine and Mobile game groups.

Mixed Design Repeated Measures ANOVA; X: Mean; SD: Standard Deviation; η2: Effect Size, T1: pre-treatment assessment, T2: post-treatment assessment; VAS: Visual Analog Scale; MCPTAM: Metacarpophalangeal Joint Total Active Motion (metacarpophalangeal joint flexion - metacarpophalangeal joint extension loss; IPTAM: Interphalangeal Joint Total Active Motion (interphalangeal joint flexion - interphalangeal joint extension loss); DHI: Duruöz Hand Index; Q-DASH: Quick Disabilities of the Arm, Shoulder, and Hand; cm: centimeter; ˜X: Median; min: Minimum; max: Maximum; *: Mann-Whitney U Test; AHEP: Adherence to Home Exercises Program
Both the routine rehabilitation (RR) group and the mobile game (MG) group demonstrated a statistically significant improvement in Q-DASH scores from pre-to post-treatment (p < 0.05), indicating improved upper extremity function over the course of rehabilitation.
However, in the between-group comparisons, no statistically significant difference was found in Q-DASH scores (p > 0.05). This suggests that while both approaches contributed to functional improvement, neither method was superior in terms of enhancing Q-DASH outcomes.
According to this table, when examining the within-group changes over time for MCPTAM (Metacarpophalangeal Joint Total Active Motion), IPTAM (Interphalangeal Joint Total Active Motion), DHI, VAS activity, and edema measurement data in the routine and mobile game groups, statistically significant differences were found for all parameters (p < 0.05). This indicates that the comparisons between the pre-treatment and post-treatment measurements for these parameters were statistically significant in both groups.
A statistically significant difference in favor of the mobile game group was found in the intergroup comparison of MCPTAM measurements. However, no statistically significant differences were observed between the groups in terms of IPTAM, DHI, VAS activity, and edema measurements. Additionally, a statistically significant difference in favor of the mobile game group was found in the intergroup comparison regarding adherence to home exercise.
Discussion
This study investigated the effects of integrating mobile games as a home exercise component into the rehabilitation process of patients with thumb involvement due to conditions such as tendon repair (FPL, EPL), carpal tunnel syndrome (non-operative), fractures, digital nerve repair, and ligament injuries. The outcomes of functionality, normal joint range of motion, pain, edema, and adherence to home exercises were compared with those of a group following a standard home exercise program. Improvements were observed in all parameters at the end of the treatment in both groups compared to baseline. However, no significant difference was found between the groups in the primary outcome measure, the QuickDASH. While the MG group showed greater improvement in MCP joint range of motion compared to the RR group, this difference was not observed in IP joint measurements. Similarly, no significant differences were found between the groups in additional functional outcomes such as the DHI, activity-related pain, or edema measurements. Notably, adherence to home exercises was significantly higher in the MG group than in the RR group.
The target population for inclusion initially encompassed all patient groups with thumb involvement, including conditions such as thumb osteoarthritis, thumb replantation, and similar pathologies. However, during the course of the study, the actual patient profile presenting to the clinic was limited to cases involving flexor pollicis longus (FPL) and extensor pollicis longus (EPL) tendon repairs, non-operative carpal tunnel syndrome, fractures, digital nerve repairs, and ligament injuries. This study included various diagnoses that result in thumb involvement, and this diversity may be considered valuable as it reflects the nature of real-world clinical practice. Since all patients experienced a common functional limitation, the mobile game-supported exercise program was designed with shared therapeutic goals. Diagnostic variability was accounted for in the statistical analyses, baseline functional levels were kept comparable, and randomization ensured homogeneous distribution of diagnoses between the groups. Nevertheless, this diversity may serve as a foundation for future studies focusing on diagnosis-based subgroup analyses.
Although no significant difference was found between the groups in the primary outcome measure (Q-DASH), both groups demonstrated improvements at the end of treatment. These findings suggest that mobile game–based home exercise programs may be considered a potentially effective option in thumb rehabilitation and, at the very least, not inferior to standard home exercise programs. Future studies with larger sample sizes and longer follow-up periods, preferably designed as non-inferiority trials, could further examine this possibility and determine whether functional differences may emerge over time.
A study incorporating therapeutic activities post-wrist fracture, with the addition of smartphone games requiring wrist movements, found that the experimental group engaging in exercises involving wrist movements exhibited greater improvement in wrist extension. 3 Similar to these studies, our research also found superior results in the group that performed home exercises via mobile games, particularly in terms of thumb MCP joint range of motion. There is considerable variability in the flexion and extension ROM of the thumb MCP joint in the general population. However, most individuals typically exhibit an MCP joint ROM between 35° and 55°. 18 Considering the approximately 6° greater ROM observed in favor of the mobile game group, this improvement corresponds to roughly 10% to 20% of the total average motion range. We believe this proportion represents a clinically meaningful gain within a relatively short period. The mobile games used in our study generally required swipe and tap functions, which are associated with the thumb’s MCP joint flexion/extension and abduction/adduction movements. Therefore, this may have contributed to the greater improvement in MCP joint motion in the gamification group. Additionally, considering the age group in our study, the fun and motivational aspects of the mobile games could also be another contributing factor.
Although no significant differences were found between the groups in terms of functionality and activity-related pain, a statistically significant improvement of approximately 6° in total MCP joint range of motion was observed in favor of the mobile game group. This increase in joint mobility did not appear to translate into improved functional performance or reduced pain levels, which may be attributed to the relatively short duration of follow-up in this study. With a longer follow-up period, the observed gains in joint ROM may potentially facilitate greater engagement in daily activities, ultimately leading to functional improvements and reductions in pain over time.
Moreover, functional ROM has been defined as the arc of movement required at each joint to perform 90% of daily tasks. In a prior study, the average functional ROM necessary to complete 90% of the Sollerman hand function test activities was reported to be approximately 48%, 59%, and 60% of the active ROM for the MCP, PIP, and DIP joints, respectively. 19 In the present study, it is assumed that the pre-treatment average joint range of motion in both groups had already met the functional thresholds required for performing daily living activities. This may explain the absence of significant differences in functional outcomes between the groups.
A systematic review examining the effect of digital interventions on adherence to home exercises found that seven out of the 10 studies reviewed suggest that digital aids can enhance exercise compliance. This is because digital interventions are user-friendly, provide feedback, and thereby encourage regular usage. 20 In a study conducted to understand patient preferences, when patients were presented with the options of a mobile phone video or a paper brochure for home exercises, it was found that 72% of participants preferred the mobile phone video option. Participants who chose the mobile phone video reported finding it more visually appealing, understandable, and effective. 21 Similarly, in our study, the adherence rate to home exercises was found to be higher in the group that performed home exercises through a mobile gaming application compared to the group that followed a routine home exercise program.
The advantages of incorporating digital interventions into home exercise programs via smartphones or tablets include easy accessibility, the ability to be performed anytime and anywhere, increased motivation, and an enjoyable experience.3,21 In summary, playing a game on a smartphone or tablet for a few minutes can serve as an effective hand exercise. However, digital interventions also present certain disadvantages that may negatively impact long-term adherence to exercises, such as technical difficulties like freezing, software incompatibility with certain operating system versions, and other usability issues. 20 Additionally, excessive smartphone use may lead to musculoskeletal problems such as “text neck syndrome” and “SMS thumb,” which should not be overlooked.22,23 For this reason, when recommending a mobile game–based application as a home exercise, it is essential to educate the patient on the correct usage posture and to provide appropriate warnings regarding excessive use.
The limitations of our study include the failure to reach the sample size calculated based on the power analysis, the short follow-up duration, the absence of an assessment of patient satisfaction with home exercises, and the reliance solely on patient self-reports to evaluate adherence to the home exercise program. The discrepancy in sample size may have reduced the statistical power of the study, increasing the risk of Type II error—meaning that potentially meaningful differences or effects may not have reached statistical significance simply due to an insufficient number of participants. As a result, while the findings are promising, they should be interpreted with caution. Future studies with larger sample sizes are recommended to confirm the results and further investigate the impact of mobile game–based rehabilitation on thumb function recovery. With regard to adherence, patients were asked to complete daily exercise logs and return them at the end of the session. However, some patients may have forgotten to fill in the forms on a daily basis and instead completed them retrospectively, which could have introduced recall bias. In addition, the use of self-reports as the sole source of adherence assessment may have introduced self-reporting bias. Another limitation of this study is the lack of assessment of thumb opposition, a movement that uniquely characterizes thumb mobility and function. Considering the clinical importance of opposition in hand performance, we believe that its inclusion as an outcome measure in future studies would provide valuable insights. On the other hand, to the best of our knowledge, our study is the first to incorporate mobile games into home exercise programs for thumb rehabilitation, which stands out as a key strength.
Conclusion
This study explored the feasibility of incorporating mobile game–based home exercise programs in patients with thumb involvement. Although a statistically significant improvement in MCP joint range of motion was observed in the intervention group, the clinical relevance of this finding remains uncertain. No significant differences were identified between the groups in primary and secondary outcomes, including pain and function. The results suggest that mobile games may offer potential benefits as an alternative to conventional home exercise programs in thumb-related conditions and may enhance adherence. However, larger-scale and longer-term studies are needed to determine the practical effectiveness and clinical implications of this approach.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by This work was supported by the TUBITAK 2209-A- University Students Research Projects Support Program- 1919B012314029
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trail Registeration
Clinical Trials ID: NCT06731972-167638: https://register.clinicaltrials.gov/prs/app/template/Preview.vm?epmode=Edit&uid=U0007WRZ&ts=1&sid=S000F6HI.