
Abstract
Health information systems (HIS) in India, as in most other developing countries, support public health management but fail to enable healthcare providers to use data for delivering quality services. Such a failure is surprising, given that the population healthcare data that the system collects are aggregated from patient records. An important reason for this failure is that the health information architecture (HIA) of the HIS is designed primarily to serve the information needs of policymakers and program managers. India has recognised the architectural gaps in its HIS and proposes to develop an integrated HIA. An enabling HIA that attempts to balance the autonomy of local systems with the requirements of a centralised monitoring agency could meet the diverse information needs of various stakeholders. Given the lack of in-country knowledge and experience in designing such an HIA, this case study was undertaken to analyse HIS in the Bihar state of India and to understand whether it would enable healthcare providers, program managers and policymakers to use data for decision-making. Based on a literature review and data collected from interviews with key informants, this article proposes a federated HIA, which has the potential to improve HIS efficiency; provide flexibility for local innovation; cater to the diverse information needs of healthcare providers, program managers and policymakers; and encourage data-based decision-making.
Background
A country’s health system usually involves a two-pronged approach: Provider-driven healthcare services offered directly to patients and public health system–driven healthcare for communities. However, the health information systems (HIS) of India and other developing countries have largely focused on collecting quantitative population data because of the prominence of infectious and communicable diseases. Although most routine public health data are generated during patient–provider encounters at health facilities or in communities, aggregated data flow upward through multiple parallel HIS (National Health Systems Resource Centre, 2011) to the central program–monitoring agencies, with limited use of data by healthcare providers.
In the context of developing countries, many parallel central program–based HIS exist, which leads to fragmentation of the HIS landscape. For example, the Health Management Information System (HMIS), the Mother and Child Tracking System (MCTS) and the Integrated Disease Surveillance Program are three different HIS in India. Further, these parallel HIS fail to provide accurate, timely and complete health information (Chilundo and Aanestad, 2004; Kimaro and Nhampossa, 2005). The call for creating integrated HIS has reaffirmed the value of an enabling health information architecture (HIA) (National Health Systems Resource Centre, 2011). In some African countries, an enterprise architecture approach is proposed for the integration of HIS (Mwanyika, 2014). An architecture framework that focuses on standards and guidelines for improving the interoperability of South Africa’s HIS is recommended (Mudaly et al., 2013). A good architecture produces a system that is scalable, sustainable, cost-effective, flexible for innovations, available for use and has acceptable performance and functional processes for testing and change (Payne and Beckton, 2015). Experiences in Sierra Leone and many other countries show that a scalable and comprehensive architecture can meet both public health and patient care data needs (Braa et al., 2010). China is among the developing countries that are also implementing health information exchange, that is, technologies or frameworks to facilitate better patient care and population health outcomes (Vest, 2012). The HIS framework developed by the Health Metrics Network (WHO, 2008) encompasses all the health data sources of a country pertinent to managing both population and clinical healthcare services. An enabling HIA is required to meet the information needs of healthcare providers, program managers and policymakers. Such an architecture would allow providers to generate, capture, share, analyse and use clinical data to improve both patient health outcomes and the quality of public health monitoring data. HIAs that enable providers and public health decision makers do exist in developed country hospital settings (McMurry et al., 2007). However, these are needed in the decentralised and heterogeneous health systems of developing countries (Moodley et al., 2012). For instance, while Bihar and other Indian states have a constitutional mandate to address the healthcare needs of their populace, national health agencies can also plan and implement health programs across several states. This means that financial allocations for health programs vary from one state to another, owing to the states’ differing financial capacity and the scale of national programs in a state.
The national health system of India comprises sub-health systems at the state, district, sub district and block levels, which manage their own HIS. These systems involve several types of healthcare providers, both public and private (including non-profit), whose roles, skill sets, functions and facilities vary. They also have differing data needs and use differing tools, processes and systems to collect, report and access data for decision-making. Among these data categories are antenatal care, pregnancy outcomes, postnatal care, disease outcomes, laboratory test results, immunisation history, inpatients and outpatients and surgical procedures (Ministry of Health and Family Welfare, Government of India, 2014−2015). Even though individual healthcare data are communicated with increasing efficiency to national public health databases for analysis and policymaking in India, clinics’ patient information still tends to be stored in multiple non-standard paper formats. The situation is especially problematic when clients visit multiple clinics or even multiple providers, because this results in the fragmentation of individual patient records and cost and quality of care.
The inconsistent HIS landscape, lack of standards and interoperability and architectural gaps are well-documented in India (National Health Systems Resource Centre, 2011). As part of the overall digital health ecosystem, national health policymakers hope to create and roll out a federated architecture to link systems at the national and state levels (Box 1) and have outlined key principles and strategies for an integrated HIS. However, there is lack of in-country evidence on HIS research (Rao et al., 2014) and a design of integrated HIS, given that this is a relatively new focus of the national health policy (Ministry of Health and Family Welfare, Government of India, 2017).
Integrated health information systems: Principles and strategies
Adoption of national electronic health record standards and metadata and data standards Federated architecture to roll out and link systems at the state and national levels Progressive use of Aadhaar (a 12-digit unique identification number [ID/UID]) for identification Creation of a health information exchange platform and a national health information network Use of existing/planned national and state-level information technology Smartphones/tablets for capturing real-time data Setting up of dedicated governance structures
Source: Adapted from National Health Policy 2017, Ministry of Health and Family Welfare, Government of India (2017).
Case study objective
The purpose of this case study was to analyse the health system and HIS of a single Indian state, Bihar, and use the findings to propose an HIA that could enable healthcare providers, policymakers and program managers of public health agencies to use data for decision-making.
Method
We conducted a literature review and collected primary data using interviews with key informants. The literature search was conducted using PubMed and Web of Science, with these key terms: ‘health information exchange’; ‘health information systems’; ‘health information architecture’; ‘health information exchange’ OR ‘health information architecture’ OR ‘integrated health information architecture’; ‘health information systems’ AND ‘developing countries’; ‘health information exchange’ AND ‘developing countries’; ‘health information architecture’; and ‘integrated health information architecture’. We also analysed relevant reports and program documents available in the digital repositories of relevant India-based organisations to understand and describe the HIS landscape of India and the health systems of Bihar. For this purpose, the websites of the Ministry of Health and Family Welfare (MOHFW), the National Health Systems Resource Centre (NHSRC), the National Institute of Health and Family Welfare (NIHFW), the Society for Health Information Systems Program (HISP) and the South-East Asia Regional Office of the World Health Organization were searched. Secondary research was followed by 11 interviews with health administrators, public health practitioners, physicians and e-health professionals at the state level. Because this study was conducted as part of the Master of Public Health degree program and involved primary data collection, a study proposal was submitted to the Institutional Review Board of the University of North Carolina at Chapel Hill. The study received a waiver from the Board.
Case study
The literature review and interview findings were used to describe the health system of Bihar state and to propose a federated HIA (FHIA). We have organised this section under two subsections: the health system of Bihar and the proposed HIS innovation (i.e. FHIA).
Health system of Bihar
Bihar is India’s third most populous state, with a total population of more than 104 million (Office of the Registrar General and Census Commissioner, 2011). The administrative structure of Bihar consists of 9 divisions (each comprising several districts), 38 districts (each comprising many blocks and subdivision), 101 subdivisions and 533 blocks (each comprising several villages) (Ministry of Health and Family Welfare, Government of India, 2013). This administrative structure is responsible for delivering, monitoring and reviewing public services, including healthcare. The state public health system in Bihar is complex and involves multiple stakeholders at both the national and state levels (Figure 1). Besides the national MOHFW, which oversees the National Health Mission (NHM), national agencies such as the NHSRC, the NIHFW and the National Informatics Centre provide technical assistance to the state health programs. These agencies also have state-level counterparts that support health programs. In addition, the state of Bihar has its own state-, division-, district- and block-level health departments and units. While all these national- and state-level institutions facilitate the delivery of healthcare services, lack of a horizontal or pyramidal structure and interagency reporting leads to duplication of effort and underlines the lack of a coherent strategy.

Health System of Bihar: Organisational linkages. IT: Information Technology; Dept.: Department; MOHFW: Ministry of Health and Family Welfare; NHSRC: National Health Systems Resource Centre; NHM: National Health Mission; NIHFW: National Institute of Health and Family Welfare; MCTS: Mother and Child Tracking System; HISP: Health Information Systems Program; NGO: Non-governmental Organization; HMIS: Health Management Information System; DHIS 2: District Health Information Software 2.
Population health status
The NHM has expanded Bihar’s health infrastructure, helping to increase access to healthcare services. However, given the state’s population size, socioeconomic inequality and geographic spread, functional public health infrastructure is still lacking in many areas (Ministry of Health and Family Welfare, Government of India, 2015). Furthermore, a shortage of healthcare workers and a lack of financial resources limit the state’s capacity to innovate and increase dependence on donors, non-governmental organisations and the federal government.
The state has a high decadal population growth (25.07%) and total fertility rate (3.5) in comparison with the national averages of 17.64% and 2.4%, respectively (Office of the Registrar General and Census Commissioner, 2011). In addition, maternal mortality (219/100,000 live births) and infant mortality (44/1000 live births), combined with a lack of availability of and access to healthcare services in socially and geographically remote regions, continue to be challenges. The health system is struggling to respond effectively, owing to a lack of financial and technical resources, infrastructure, leadership and governance (Ministry of Health and Family Welfare, 2011: 55−58).
Public health agencies
The state health system’s complexity (Figure 1), in terms of the number of actors and their roles and responsibilities, authority and accountability, communication and organisational relationships, influences the performance of HIS. The State Health Society, Bihar (SHSB), is primarily responsible for implementing the NHM. The SHSB is an autonomous organisation that was created under the National Rural Health Mission (NRHM), which is now part of the NHM, to lead the implementation of NRHM programs. An important point to note is that SHSB decisions are strongly influenced by the state health department, which oversees all health programs in the state, including those funded by the national government. Other state-based public health institutions, such as the State Health Systems Resource Centre and the State Institute of Health and Family Welfare, provide technical assistance to the SHSB and the Department of Health. However, they are in turn influenced by their national counterparts. In terms of health information technology (IT) support, the SHSB has an in-house team of three people. Each health facility at the primary health centre level and above has a data centre to support data entry activities. Technology support for national HIS initiatives implemented in the state is provided by the National Informatics Centre—a government IT agency—and its state counterparts, in addition to the in-house team of the SHSB. Private technology companies, such as Tata Consultancy Services, and non-governmental organisations, such as the Society for Health Information Systems Program, also offer technology support and maintenance for specific products.
HIS in Bihar
Bihar has several HIS that use the web, mobile phones or a combination of information and communication tools. However, only a few of these systems are operational throughout the state; among them, the national HMIS portal and the MCTS. The state-specific systems are the human resources information system (HRIS) for Health and Sanjeevani (a web—enabled ambulatory care information system). Both national and state governments fund these two systems, with financial and technical assistance from the development partners. The HRIS is used primarily to assess the availability of health workers at various facilities in the state.
The national HMIS portal is designed to aggregate data on the basis of health indicators compiled by rural healthcare workers. At the system’s core are approximately 200 indicators related to the areas of child and maternal health and infectious diseases. The data are collected at service delivery sites (health sub-centre, additional primary health centre, primary health centre, community health centre or district hospital) and fed progressively up to block-, district-, state-, and national-government levels (Figure 2), where they can be analysed and used to make decisions. The MCTS tracking system collects individual patient data. This system is used to track antenatal care, pregnancy outcomes and postnatal care services to women of reproductive age and to track immunisation services provided to children under 5 years of age at the health sub-centre level. It collects data on more than 100 data elements. The HMIS portal and the MCTS were developed and are maintained by different organisations. While the MCTS was developed by the Gujarat state informatics centre, a government agency, the HMIS portal is built on a proprietary software application by a private IT firm.

Data flow in the health management information system.
The web-enabled Sanjeevani system is perhaps the only information system designed to capture individual clinical data. Ambulatory care services data are captured on paper but also online through Sanjeevani (Box 2). However, data pertaining to pathology tests, radiology diagnosis, medication, and patient admission, discharge, and transfer are collected primarily on paper. Sanjeevani is implemented across the state to capture patient registration and drug distribution data.
Key features of Sanjeevani
Primary purpose: to record the number of outpatient visits (and drug distribution) Patient registration data entry done by data entry operators employed by the government Drug distribution data and disease name entered by pharmacist Physician/clinician does not access or enter any data Lab test data available in paper form and sometimes entered in ‘remarks’ section of the application Lab test data entry module under development Web-enabled but also allows offline data entry for later synchronisation Currently hosted on cloud server; a new vendor identified for in-state hosting Software built .NET Developed by state-based developers State Program Implementation Plan (2014–2015) provides conditional approval by the Government of India until the nationally approved software application (Java-based) is put in place and data migrated to the new application
Sanjeevani is a locally developed system dependent on federal funding and will most likely be replaced by a more comprehensive system developed by the Centre for Development of Advanced Computing (CDAC), a national IT agency. Bihar’s approved state health program implementation plan (2014–2015) highlights conditional budget approval for the continuation of Sanjeevani, which means that the national government is willing to fund a clinical information system developed in consultation with the CDAC and according to the government’s electronic health record (EHR) standards (Ministry of Health and Family Welfare, Government of India, 2014–2015: 106).
Because the funding and decision for operating the Sanjeevani system is conditional, the system will most likely close out, and a new system is expected to replace it. The new system is expected to import existing patient data from Sanjeevani before the latter is phased out. The situation in private hospitals is similar to that in government health facilities with respect to electronic systems for data capture. Even private hospitals lack a system for capturing ambulatory and inpatient data over the life cycle of a patient. One large private hospital uses the picture archiving and communications system.
Not surprisingly, in the absence of national- or state-level health IT policies, regulations and standards, each health department or program uses the technology of its choice and is managed by a department or program. There is a lack of coordination among these departments in the design, implementation and use of HIS. Even though individual patient data are collected and reported across the state, no policy or regulation exists to protect and secure patient data.
Proposed HIS innovation: FHIA of Bihar
This article has drawn insights from the theory of information infrastructure (Hanseth and Monteiro, 1998) to define ‘FHIA’, which refers to an HIA that integrates the health information needs of local or sub-health systems with those of the central or state health system while enabling providers and public health leaders to use data for decision-making, creating a shared information infrastructure and offering local autonomy to address contextual health issues. Even though the centralised architecture offers economies of scale through a central data repository and reduces redundant costs, it is less responsive to local needs and has a longer implementation timeline (Eckerson, 2011; Ziesemer and Hoyt, 2009). And although a decentralised architecture is quick to deploy and offers local adaptability, it leads to redundancies and higher overall cost while limiting the ability to create an organisational perspective on a health information need (Eckerson, 2011; Ziesemer and Hoyt, 2009). The advantage of an FHIA is that it can create a balance between the autonomy and information needs of local health units and the information needs of policymakers and program managers. Such an architecture utilises available standards and offers the flexibility to build user-centred decision support tools to aid decision-making at both the provider and management levels.
Data elements, data collection and sharing processes and data collection and sharing systems are key aspects of an FHIA. These three aspects are discussed next, using the example of a district hospital in Bihar to demonstrate how they function in the existing context and how their functions will change after the FHIA has been implemented.
Data elements
Current situation
Government health facilities report facility-wide data on outpatient and inpatient care, institutional deliveries, caesarean sections and major and minor surgeries (Ministry of Health and Family Welfare, Government of India, 2014−2015). The data categories are antenatal care, pregnancy outcomes, postnatal care, disease outcomes, laboratory test results, immunisation history, inpatients and outpatients and surgical procedures, including those conducted in vertical disease-control programs such as blindness control. The study found that broad categories of data collected and reported (Box 3) in different HIS at the primary health centre and a district hospital are almost the same.
Data categories
Demographic data Health worker profile Antenatal care services Deliveries Number of caesarean sections performed Pregnancy outcomes and newborn details Pregnancies with complications Postnatal care services Medical termination of pregnancy Reproductive tract infections/sexually transmitted infections Family planning services Child immunisation Number of cases of childhood diseases Blindness control services Patient services (ambulatory and inpatient care; mortality) Laboratory test results Mortality and causes
Post-FHIA situation
The foundation for the proposed FHIA has already been laid by the EHR standards document, which recommends not only a minimum dataset (MDS) for an EHR system but also the use of semantic standards such as the Systematized Nomenclature of Medicine—Clinical Terms and the International Classification of Diseases 10 (Ministry of Health and Family Welfare, Government of India, 2013). These standards will enhance data quality and analysis and prevent misinterpretation. The MDS includes such demographic information as unique patient identifier, date of birth and address. The clinical dataset covers past health history, clinical encounter details, provider information, clinical summary, diagnosis and treatment plans (Ministry of Health and Family Welfare, Government of India, 2013). The FHIA can reduce duplication of effort and allow health facilities to collect these data elements, which are now collected and reported only sometimes. Additionally, architectural flexibility can enable the implementation of selected EHR modules and standardised interfaces. A modular approach to the implementation of an EHR keeps the system flexible and agile enough to address any gaps resulting from changing organisational information needs (Bush et al., 2010; Sabherwal et al., 2003; Tiwana and Konsynski, 2010) if supported by appropriate governance mechanisms (Tiwana and Konsynski, 2010). For example, two of the modules critical for improved patient care are computerised physician order entry and clinical documentation (Figure 3). Adding these modules will allow providers to collect and analyse important quantitative and qualitative data in a coherent way. The data from a modular system can feed into a repository that will allow providers to query clinical data and respond to the healthcare needs of individual patients. These datasets can also serve the aggregate needs of program managers and policymakers.
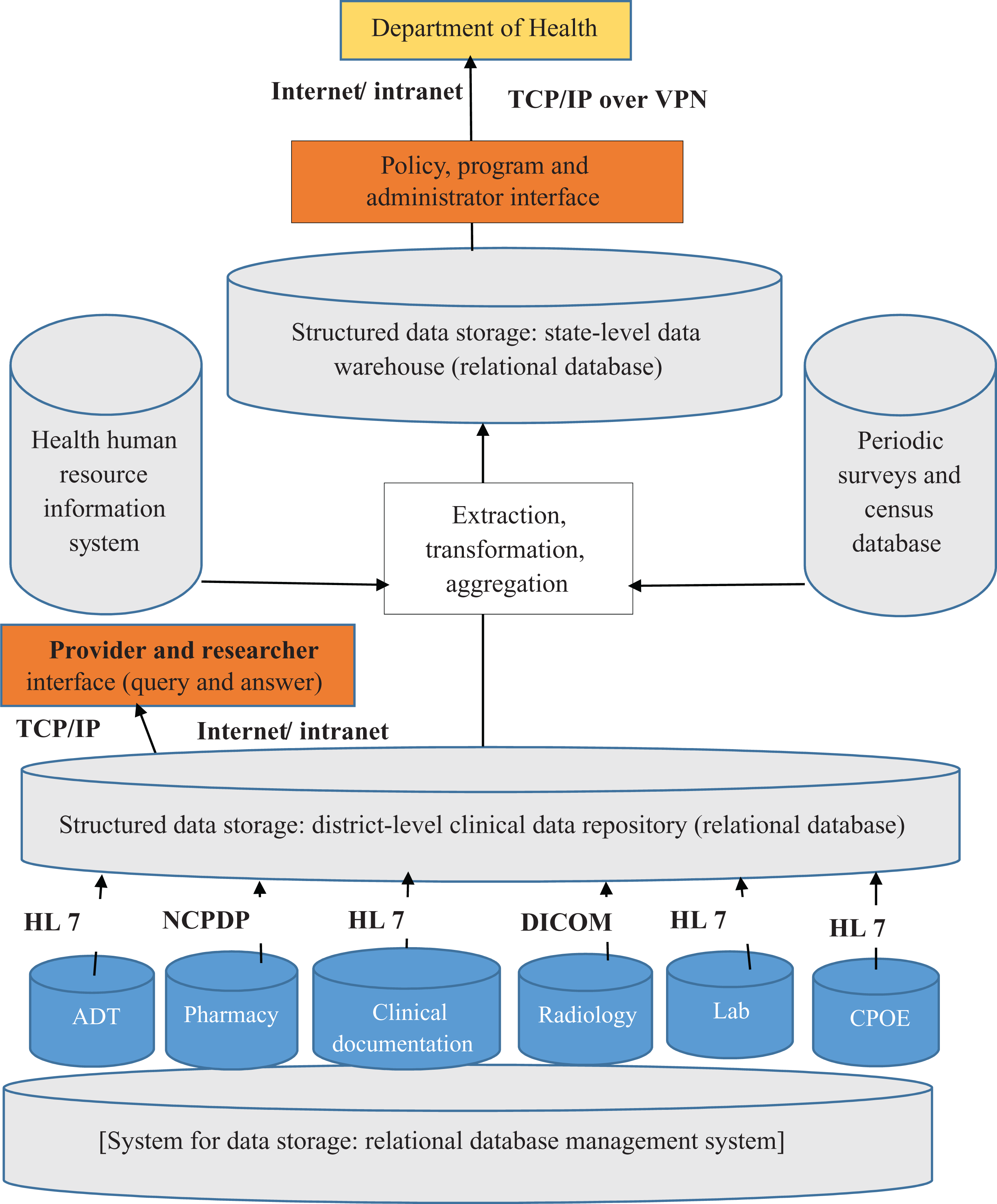
Proposed Federated Health Information Architecture of Bihar. TCP/IP: Transmission Control Protocol/Internet Protocol; VPN: Virtual Private Network; ADT: Admission, Discharge and Transfer; CPOE: Computerised Physician Order Entry; HL 7: Health Level 7; NCPDP: National Council for Prescription Drug Programs; DICOM: Digital Imaging and Communications in Medicine.
In the future, data collection and reporting requirements are likely to expand once Bihar adopts the Indian Public Health Standards (Ministry of Health and Family Welfare, Government of India, 2012). The FHIA can effectively respond to the need for data on patient safety, sexual harassment and patient privacy. Achieving these requirements without losing granular patient data is an important feature of the proposed FHIA.
Data collection and reporting processes
Current situation
Clinical and administrative data are captured manually on paper at the health facilities. Patient admission, discharge and transfer data are made available on paper, but a patient receives only a discharge summary, which is not a standard process in the district hospitals. The ambulatory care system also generates a lot of data, but the dataset reported in the Sanjeevani system is limited. Clinical data collection on paper forms lacks a systematic approach and standardisation. Data are collected in many different paper-based registers and formats at district health facilities and lower level health facilities, such as the reproductive and child health register at the health sub-centre level. Although different types of clinical data—medication data, use of diagnostic tests and surgical procedures and their outcomes—are collected at district health facilities, these datasets fail to support quality management practices for improved clinical outcomes at either the individual or the population level. A big reason for this failure is ineffective clinical documentation. To make sound clinical decisions, enough information must be captured from each encounter to support continuity of care over a patient’s lifetime.
Standard reporting formats for each type of system are made available and used to report data electronically, through spreadsheets and online in different HIS. For example, individual data are reported in the MCTS and in the Sanjeevani system; aggregate data are reported in the national HMIS portal. Reporting periodicity also varies across systems. Aggregate data are reported monthly at the primary health centre, but at the district hospital, they are reported monthly, quarterly and annually to the HMIS. Most aggregated healthcare service data are reported online, though paper-based reports are also shared within the facility and at the district level during monthly review meetings.
Post-FHIA situation
Many MDS data elements are already collected on paper and also reported online. Therefore, data collection requirements may not increase significantly, although the standardisation of data collection formats is essential, and electronic data collection and reporting uptake can take time because of the limited capacity of Bihar’s health system. But over a period, the FHIA will ensure the standardisation of data collection and reporting formats and standards for data interchange to facilitate meaningful use. Data standards allow the consistent, accurate and reproducible capture of clinical, administrative, diagnostic and drug data across diverse HIS. Therefore, the use of standards such as Health Level 7 data interchange standards, the National Council of Prescription Drug Program and Digital Imaging and Communications in Medicine can facilitate data interchange between modular systems and the clinical data repository, which in turn can enable structured data storage. The FHIA will offer an opportunity to reduce duplication in data collection and sharing, solve inconsistency and improve efficiency and quality (Davenport, 1998). The provision of evidence-based healthcare services will be possible once the FHIA is in place and adequate capacity has been built. The transfer and interchange of data can take place over secure networks to ensure privacy and confidentiality. The process of extracting, transforming and aggregating data will allow data to be pulled from different systems, such as HRIS and the census database, and organised in a data warehouse. Program managers can then access the data from the data warehouse through an appropriate user interface. In addition, creating user-centred data analytics and visualisation programs will enable healthcare providers, policymakers and program managers to use data for decision-making.
Data collection and reporting systems
Current situation
As discussed earlier, to collect and report data, Bihar now uses national- and state-specific systems, some of which are paper based and some of which are electronic.
Post-FHIA situation
An FHIA can overcome the challenges posed by the stand-alone use of different HIS in Bihar. The MDS is partially captured through the MCTS and the Sanjeevani system. Because Sanjeevani is ad hoc system, Bihar will be able to shed the burden of its existing fragmented system by adopting an FHIA, which will use a relational database management system to support each of the modular components. This system will allow the storage of structured data in a clinical data repository. Use of the TCP/IP over a VPN will enable secure communication among different information systems in the FHIA.
The proposed FHIA offers Bihar a unique opportunity to harmonise data collection and reporting and data use efforts to accomplish both individual and public healthcare objectives.
Conclusions
Most of the developing world is grappling with the challenge of managing and using multiple vertical HIS. These fragmented systems lead to inefficiency, poor data quality, limited data use and the neglect of healthcare providers’ information needs. The policy directive to create an integrated HIS in India is an important step in the right direction that has the potential to overcome the barriers to data use created by fragmented HIS. The FHIA proposed in this article is an effort to present an architectural option that will improve HIS efficiency; provide flexibility for local innovation; cater to the diverse information needs of healthcare providers, program managers and policymakers; and enable data-based decision-making. However, it is important to note that institutional leadership is required to promote evidence-based decision-making. This article is an important contribution to the knowledge base in India, and we hope that it will stimulate further research in this domain.
Footnotes
Acknowledgements
The authors acknowledge the support received from government officials at the state and national levels in India during the fieldwork for this article. The authors are thankful to Dr Christopher M. Shea, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, for his feedback on the first draft of this article. They thank Dr Hanimi M. Reddy, Save the Children—India, and Dr John Stanback, FHI 360, Chapel Hill, North Carolina, for their useful feedback on the second draft of this article. They also thank Martha Spaulding and Debbie McGill, both MEASURE Evaluation, for their copy-editing support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.