
Abstract
Background:
While clinician attitudes towards electronic prescribing (e-prescribing) systems have been widely studied, little is known about the perspectives of patients, despite being the primary beneficiaries of these systems.
Objective:
The objective of this study is to explore and compare patient and clinician attitudes towards an integrated e-prescribing and dispensing system, in order to guide improvements in system implementation, service delivery and enhancements to system functionality.
Method:
A cross-sectional survey was developed and administered to patients and multidisciplinary clinicians at a multisite Australian metropolitan teaching hospital network in all areas where e-prescribing was fully implemented. Participants’ views on perceived impact and valued features of the e-prescribing system were elucidated.
Results:
Overall, 783 participants (400 patients and 383 clinicians) completed the survey. Although 98% of clinicians were aware of the transition to e-prescriptions, only 36% of patients were aware prior to the study. Over 80% of patients and clinicians perceived improvements in prescribing and dispensing safety and clinician workflow; 90% of patients were comfortable with information privacy associated with e-prescriptions; and 86% of patients preferred e-prescriptions to handwritten prescriptions. Although over 80% of patients valued features that improved access to information and medication safety, clinicians were more discerning about valued system features.
Conclusion:
The majority of patients and clinicians reported a positive impact of e-prescribing on safety and efficiency. Both groups valued safe and effective use of medicines, although differences existed in the importance placed on key system features. A greater focus on patient engagement and communication is needed to optimise the delivery of patient-centred care.
Keywords
Introduction
A fundamental process in the implementation of an electronic prescribing (e-prescribing) system is the engagement of key stakeholders to ensure successful adoption and acceptance of changes in workflow and processes (Day et al., 2011). Key stakeholders of an e-prescribing system include medical, nursing and pharmacy clinician users, information technology staff and patients. As clinicians are the primary users of any clinical information system, their perspectives on e-prescribing systems have been widely studied in the literature (Ayatollahi et al., 2015; Bramble et al., 2013; Devine, Williams and Martin et al., 2010; Lapane et al., 2011; Nanji et al., 2014). Other studies have also defined features of e-prescribing systems that clinicians expect will maximise benefits and minimise potential harms (Georgiou et al., 2009; Sweidan et al., 2010). Recognising and integrating these views into the design, implementation and evaluation process can have an important influence on clinicians’ attitudes and adoption of e-prescribing. Positive attitudes are more likely to lead to favourable adoption of e-prescribing, while lack of clear understanding about potential benefits and required changes to workflow may result in dissociation from technology and regression to paper-based systems (Crosson et al., 2008).
Including patients as stakeholders in the design, implementation and evaluation stages of e-prescribing systems complements the focus on clinician engagement. Patients offer a unique perspective as the primary beneficiaries of these systems. Patient satisfaction and healthcare outcomes are influenced by the safety and quality of care received, which in turn reflects the impact of e-prescribing systems on medication error rates (Westbrook et al., 2012). Additionally, the direct interaction and exchange of information between patients and clinicians is central to the function of the e-prescribing system in supporting the provision of healthcare. For healthcare organisations, patient-centred care is one of the three core principles for ensuring safe and high-quality care in the Australian Safety and Quality Framework for Health Care (Australian Commission on Safety and Quality in Health Care, 2010: 1). Aligned with this, a key focus of the Australian National Safety and Quality Health Service (NSQHS) Standards (Australian Commission on Safety and Quality in Health Care, 2012: 22) is working in partnership with patients and consumers, which can result in improved safety, quality and efficiency of healthcare. Ensuring patients actively participate and contribute to the design of care as well as service planning, measurement and evaluation can help achieve this.
However, currently little is known about patients’ perspectives on e-prescribing. A systematic review (Gagnon et al., 2014) of literature published between 2002 and 2012 included 28 studies focussed on user experience of e-prescribing implementation across a range of primary, secondary and tertiary settings. Most studies in this review centred on the perspectives of clinicians; mainly medical, pharmacy and nursing staff. Although one of the factors identified as relevant to e-prescribing implementation was patient attitudes and preferences towards e-prescribing, none of the studies in this review included patients. Another systematic review (Liu et al., 2013) of literature published between 1995 and 2011 included eight studies focussed on patient satisfaction with electronic health records and clinical information systems. However, only three studies explored patient satisfaction in the context of systems with e-prescribing functionality. While literature in this area has examined patient satisfaction with quality of care provided, there is very limited information on patient attitudes and preferences. Consequently, minimal consideration of patients’ perspectives has been afforded in the design, functionality and implementation of clinical information systems (Lapane et al., 2007; Liu et al., 2013). Furthermore, most studies in this area were undertaken in the United Kingdom or United States (US), with no published studies in the Australian setting. The inclusion of an integrated e-prescribing and dispensing system within the functionality of the intervention used in this study provides an additional perspective and contributes further narrative to the evidence currently reported in the literature.
This study aimed to explore and compare patient and clinician attitudes towards an integrated e-prescribing and dispensing system implemented for discharge, outpatient clinic and emergency department prescriptions. This knowledge provides insights for guiding improvements in system implementation, service delivery and enhancements to system functionality, which will optimise the delivery of patient-centred care that truly meets the needs and expectations of both patients and clinicians.
Method
Setting
An integrated e-prescribing and dispensing system (Pharmhos MerlinMAP e-prescribing and Merlin dispensing) was implemented from June 2013 to January 2016 in a multisite Australian metropolitan teaching hospital network. The organisation had 1950 beds (Monash Health, 2016: 18–19) at more than 40 locations including major tertiary and secondary hospitals, aged residential care centres and an extensive network of rehabilitation, community health and mental health facilities. As the organisation did not have an electronic medical record (EMR) in place at the time of the study, the home-grown integrated e-prescribing and dispensing system functioned independently. However, it interfaced with the patient administration system and scanned medical records. The e-prescribing system incorporated both active (medicines interaction and adverse drug reaction (ADR) alerts) and passive (pre-populated prescribing and Pharmaceutical Benefits Scheme information) clinical decision support (CDS) features. A separate tab provided access to the hospital formulary and restrictions. While alternative commercial e-prescribing systems often require additional configuration to interface prescribing and dispensing processes, the system used in this study was unique because it was fully integrated, utilising one shared database of information, including a common medication dataset.
Security to access the e-prescribing system functionality was tailored to the different roles and scope of practice of various groups of clinicians using the system. Prescribing capability was restricted to doctors and nurse practitioners. Recording allergies/ADRs and anthropometric measurements, for example, patient weight and height, was limited to doctors, nurse practitioners, pharmacists, nurses and midwives. Patients’ medication prescribing and dispensing history, allergy/ADR status and anthropometric measurements could be viewed by all clinician groups, including pharmacy technicians. Security to access dispensing system functionality was restricted to pharmacists and pharmacy technicians only.
A cross-sectional survey of patients and clinicians was conducted over 5 weeks (25 January 2016–26 February 2016) across the five major hospital sites of the organisation in all wards, outpatient clinics and emergency departments where e-prescribing was fully implemented. Outpatient clinics at one site were excluded from the study as e-prescribing was not yet fully implemented during the data collection period.
Survey design
Two different survey instruments for patients and clinicians were developed, based on initial interviews with the e-prescribing project team and users. The patient experience survey (Online Appendix 1) was assessed for usability and readability by the organisation’s patient review group, comprised of patient liaison advisers and patients. The clinician experience survey (Online Appendix 2) was piloted on medical, pharmacy and nursing clinicians. Questions aligned with a subset of themes (impact on patient care, clinician workflow and key features valued in an e-prescribing system) were incorporated into both patient and clinician surveys to allow comparison of attitudes, although question wording was slightly different in consideration of the different context, usability and health literacy needs of the two groups. The project was reviewed by the organisation’s Human Research and Ethics Committee Co-ordinator on 13 January 2016 and was authorised to proceed as a quality and service improvement activity to be conducted within the organisation only.
Patient survey
The patient survey consisted of four sections: characteristics, attitudes and experiences with e-prescribing, key features valued in an e-prescribing system and the opportunity for open-ended comments. Eight statements examined attitudes and experiences (such as clarity of the prescription, medication safety, impact on waiting time and privacy concerns) using a six-point Likert-type scale ranging from “strongly disagree” to “strongly agree” with a “not sure” option included. One question provided 11 statements exploring key features valued relating to safety, efficiency and convenience, from which participants could select any, or multiple or none. An open-ended question was available for additional responses and general comments.
Clinician survey
The clinician survey consisted of six sections: characteristics, attitudes and experiences with e-prescribing on both patient safety and clinician workflow, key features valued in an e-prescribing system, satisfaction with training and support and the opportunity for open-ended comments. For sections related to patient safety and clinician workflow, 15 statements examined attitudes and experiences using a six-point Likert-type scale ranging from “strongly disagree” to “strongly agree,” with two statements also having “not applicable” options. One question provided eight statements exploring key features valued relating to medication safety, CDS and accessibility of information, from which participants could select any or multiple or none. An open-ended question was available for additional responses and general comments.
Participants and recruitment
Participation in the study was voluntary and anonymous. Consent was requested when introducing the survey to participants and inferred if the survey was completed. The research team (e-prescribing project pharmacists and pharmacy students) visited 95 areas across the five major hospital sites of the organisation to recruit participants using convenience sampling.
Patients
Patients were included in the study if they had received an e-prescription during a current or previous episode of care and identified by verbal confirmation for outpatients and by review of the e-prescribing history for inpatients. The e-prescription may not have been generated during the data collection period. Paper copies of the survey were given to potential participants by a member of the research team. Patients were excluded if too clinically unwell or cognitively impaired or were from a non-English speaking background without a professional interpreter, carer or relative immediately available to interpret or translate the survey.
Clinicians
Clinicians (doctors, nurse practitioners, nurses, midwives, pharmacists and pharmacy technicians) involved in the provision of medicines management for patient care were included in the study. The survey was available in paper form and on the Internet (via SurveyMonkey®). Clinicians were invited to participate in the study via email distribution lists and online newsletters, during staff meetings and ad hoc if a member of the research team and clinician were present in the study areas.
Data analysis
Data were included from fully completed surveys only, and responses were analysed using Stata software version 11 (StataCorp, College Station, Texas, USA). Survey results were presented as percentages of aggregated positive or negative responses for categorical variables or medians and interquartile ranges for ordinal variables. For the aligned questions in both the patient and clinician surveys, results were compared using the χ 2 test for categorical variables and the Wilcoxon rank-sum test for ordinal variables, with p < 0.05 considered statistically significant. Responses to training and support (including those provided in open-ended questions) were specific to the organisation and used to improve local implementation processes and service development; these results were excluded from this study article as they were not generalisable to other settings.
Results
Characteristics of participants and awareness of transition to e-prescribing system
Overall, 783 participants (400 patients and 383 clinicians) completed the survey. Participant characteristics are summarised in Table 1.
Characteristics of participants.a
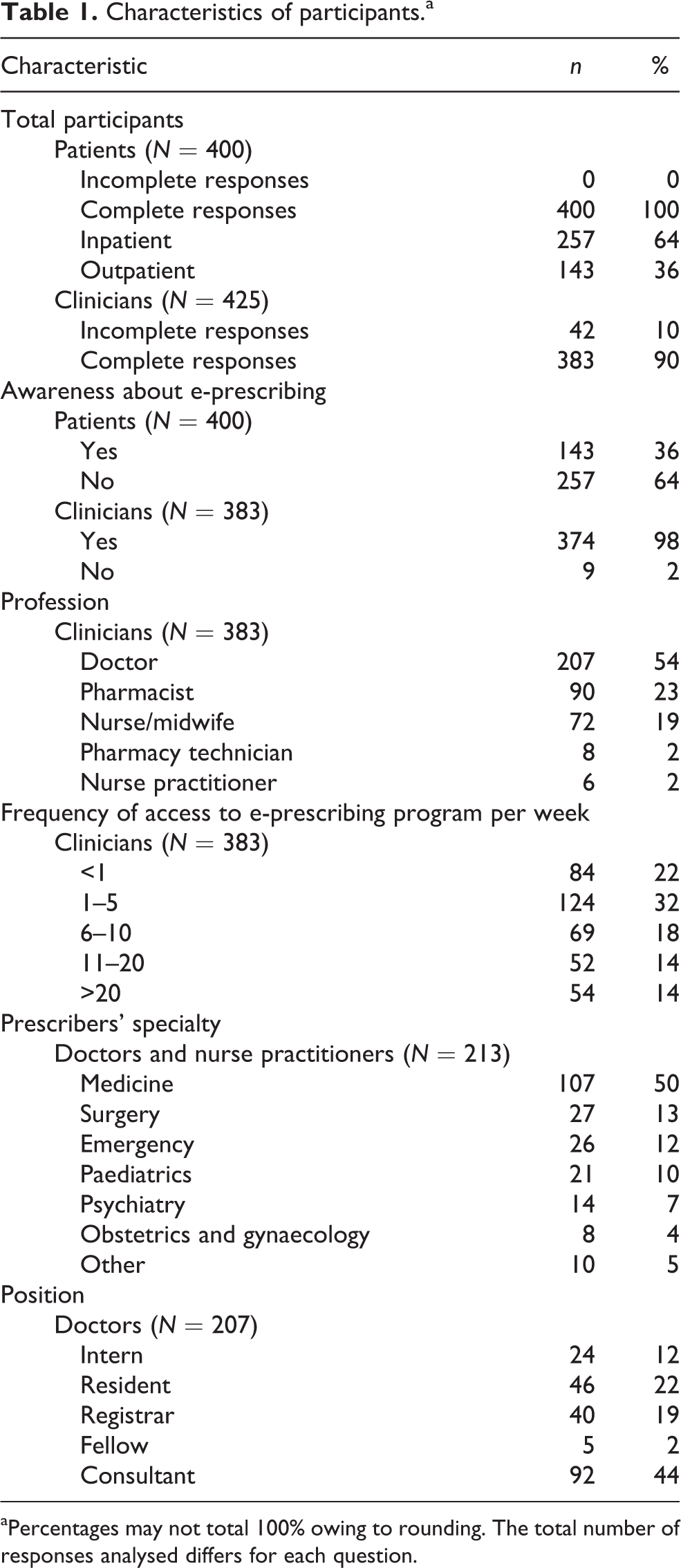
aPercentages may not total 100% owing to rounding. The total number of responses analysed differs for each question.
All patients (n = 400) completed the survey on paper. Clinicians completed the survey on paper (n = 214) and online (n = 169). Of the 524 patients invited to participate, 400 completed the survey (76% response rate). During the data collection period, e-prescriptions were generated for 13,648 unique patients. Our sample size represented 2.9% of this actual patient population. Among 425 clinicians who attempted to participate, 383 completed the survey and were included (90% response rate). The number of clinicians who received an invitation to complete the survey was unable to be determined, due to the indirect distribution methods during participant recruitment. During the data collection period, there were 1284 unique prescribers (doctors or nurse practitioners) who generated an e-prescription. Our prescriber sample size (n = 213) represented approximately one-sixth (17%) of this prescriber population. Almost all prescribers were doctors representing a broad range of over 30 sub-specialties and evenly distributed across junior and senior doctors.
Attitudes and experiences with the e-prescribing system
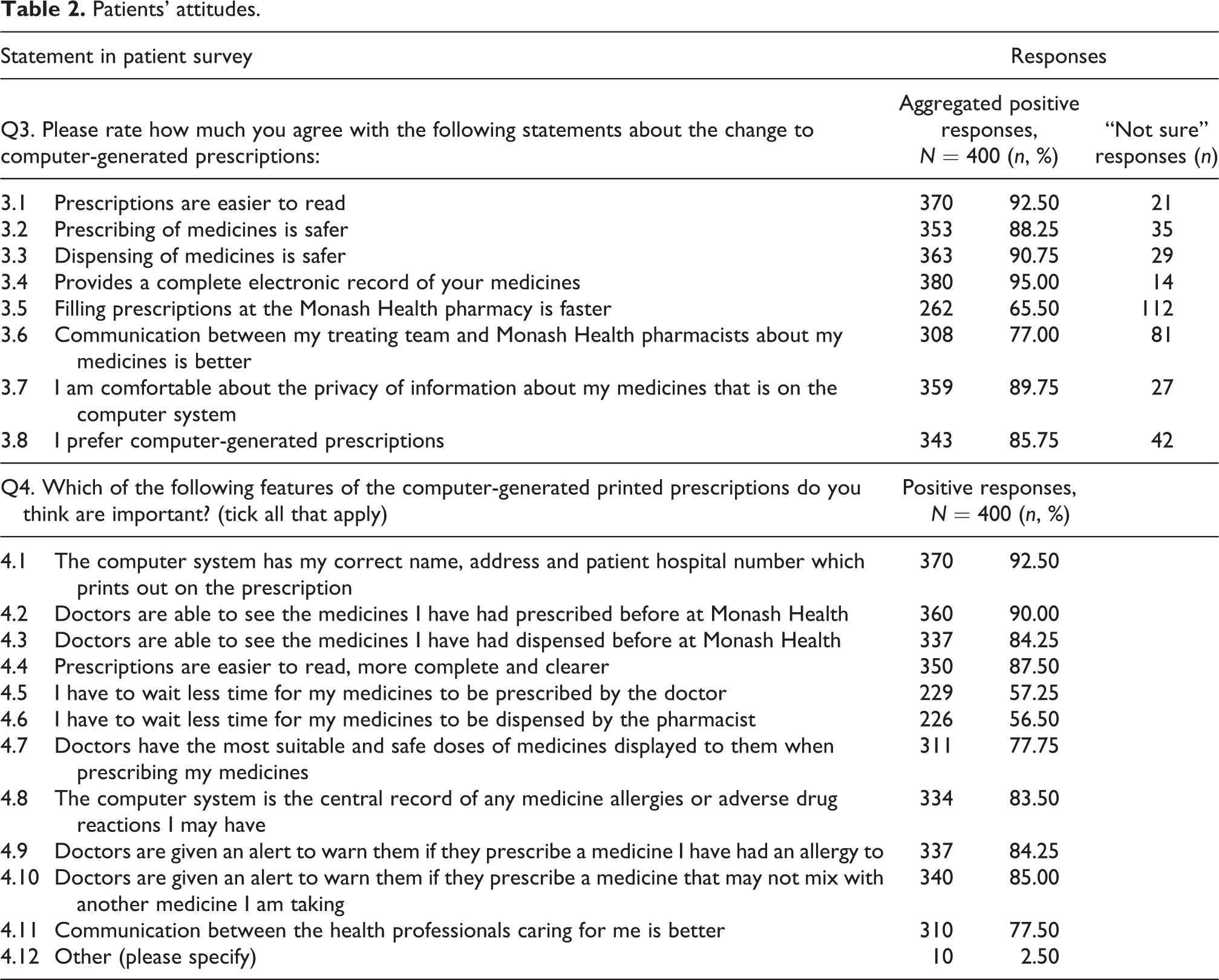
Participants’ attitudes towards the impact of e-prescribing on medication safety, efficiency and access to information were explored. Results for patients and clinicians are presented in Tables 2 and 3. Patient and clinician attitudes towards aligned questions are compared in Table 4.
Patients’ attitudes.
Clinicians’ attitudes.
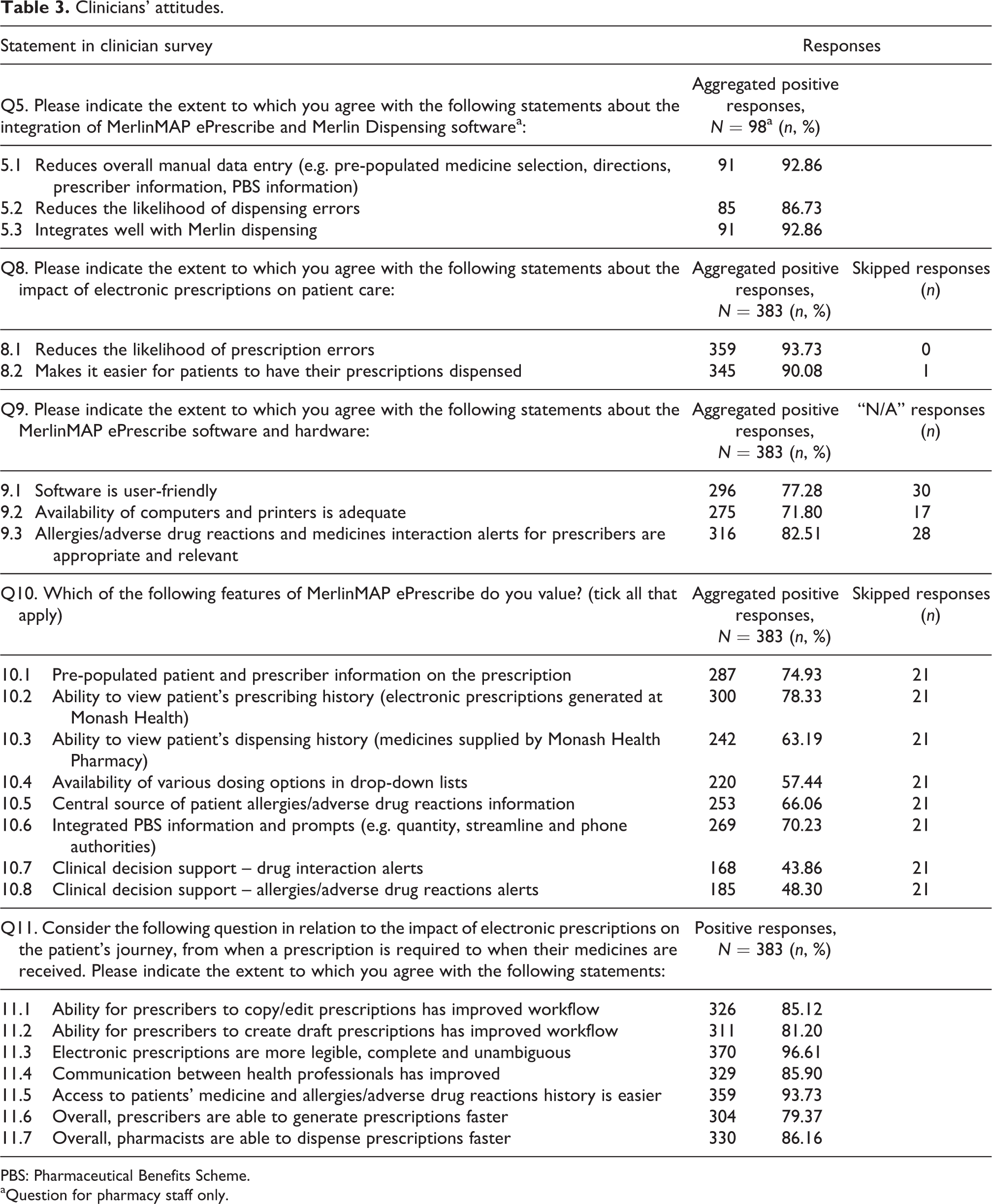
PBS: Pharmaceutical Benefits Scheme.
aQuestion for pharmacy staff only.
Comparison of perspectives (patient compared to clinician).a
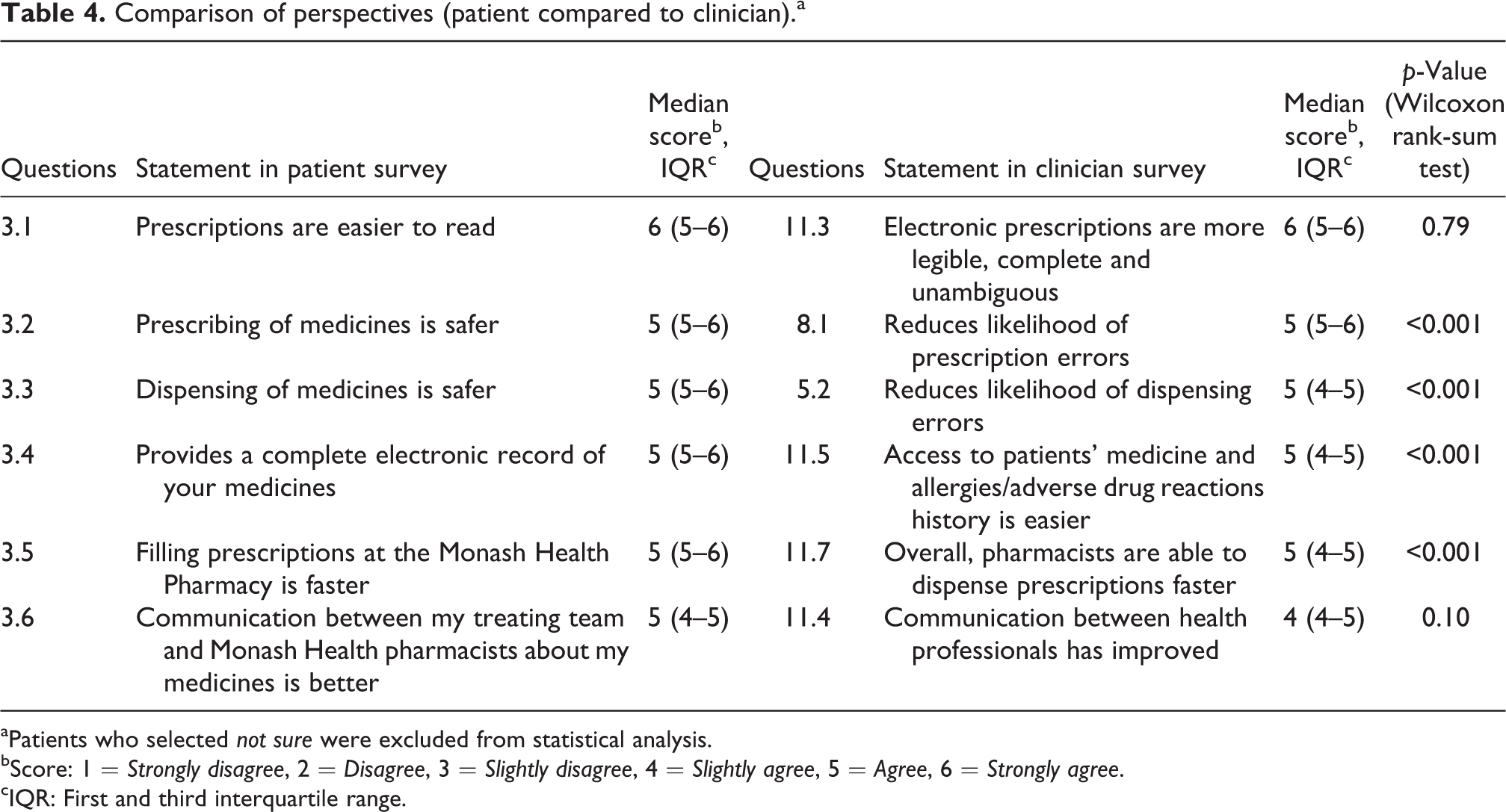
aPatients who selected not sure were excluded from statistical analysis.
bScore: 1 = Strongly disagree, 2 = Disagree, 3 = Slightly disagree, 4 = Slightly agree, 5 = Agree, 6 = Strongly agree.
cIQR: First and third interquartile range.
A large majority of patients believed e-prescribing improved safety of prescribing and dispensing (88% and 91%), legibility of prescriptions (93%) and were also comfortable about the privacy of electronic records (90%). However, 28% of patients were uncertain whether there was a positive impact on prescription waiting times at the pharmacy. Most clinicians perceived that the system reduced prescribing and dispensing errors (94% and 87%) and that there were improvements in communication (86%) and workflow (85% and 81% related to copy/edit and draft functionality, respectively). Comparison of patient and clinician perspectives showed that both groups were similarly aligned in attitudes and provided positive responses by mostly agreeing to the same extent with the survey statements, with minimal variation (Figure 1).
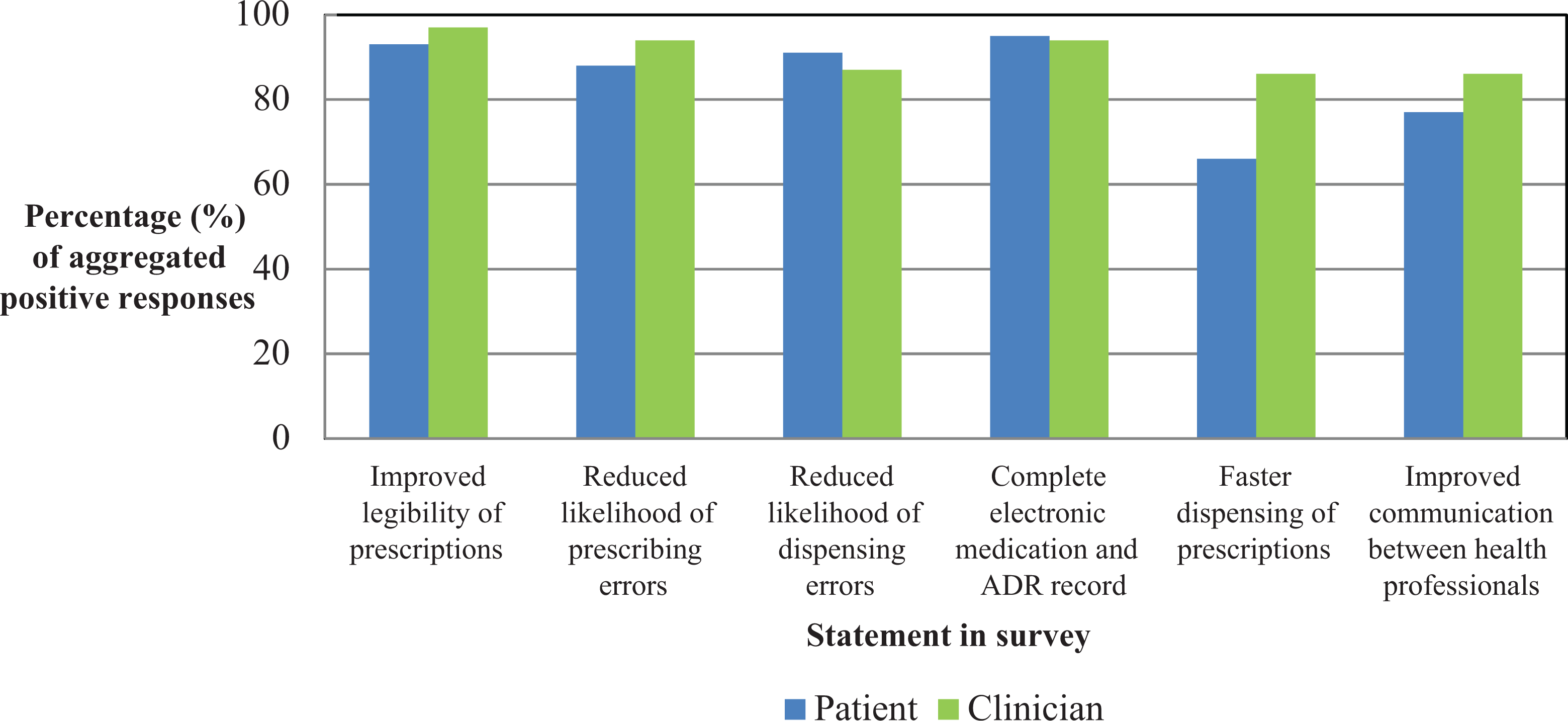
Comparison of patient and clinician perspectives. ADR: adverse drug reaction.
For the general open-ended questions at the end of both surveys, 75 patients (19%) and 134 clinicians (34%) responded. Most comments were brief and corroborated answers to closed questions or related to local implementation, training and support. However, the following statements provided further insight into patient and clinician perspectives: Using computers will introduce new system errors; beware the law of unintended consequences. (Patient x) Ability to see which items are stocked in the hospital pharmacy, so that I don’t end up waiting for something that isn’t even kept here. (Patient y) Having a current list of active medications (not repeated 47 times in the dispensing history) would be enormously useful. (Clinician x) Please include a feature that highlights which drugs are available at the hospital. It is not always practical to get a doctor to rewrite a prescription because the hospital does not keep the stock. (Clinician y)
Features valued in an e-prescribing system
Participants’ attitudes towards features valued in an e-prescribing system were also explored. Results for patients and clinicians are presented in Tables 2 and 3. Patient and clinician attitudes towards aligned questions are compared in Table 5.
Comparison of features valued (patient compared to clinician).a
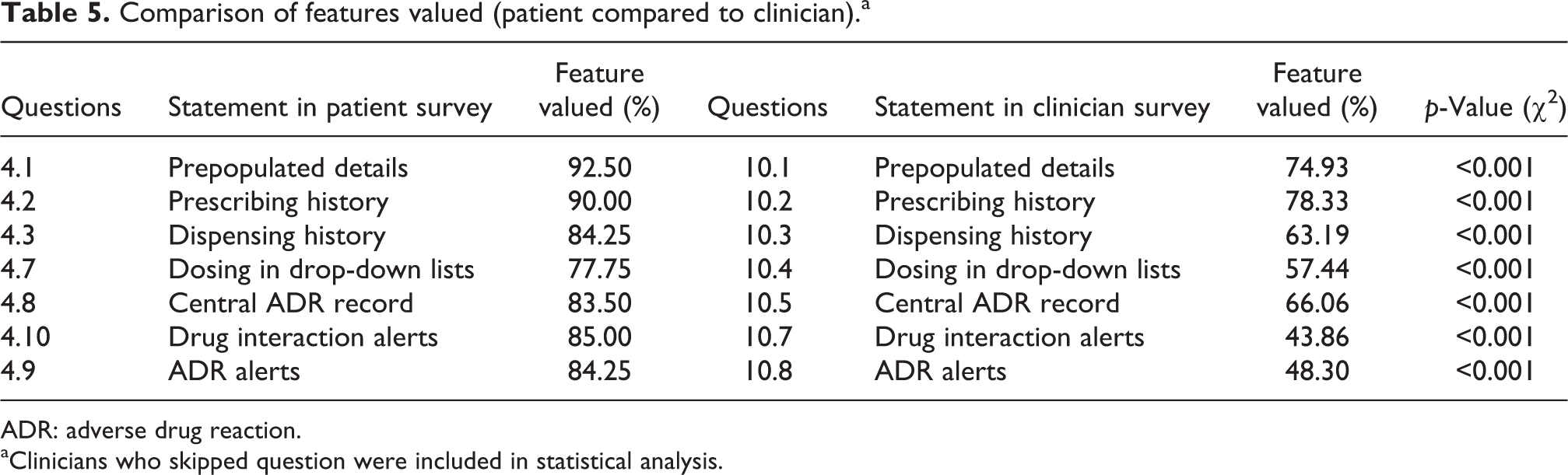
ADR: adverse drug reaction.
aClinicians who skipped question were included in statistical analysis.
Most patients valued the importance of system features that improved access to information, such as administrative details (93%), previous medication prescribing and dispensing history (90% and 84%) and allergy/ADR status (84%). CDS features were similarly regarded as important, including display of standard safe doses (78%) and interaction and allergy/ADR alerts (85% and 84%). However, only half of all patients (57%) considered reduced waiting times with either the doctor or at the pharmacy as important. For clinicians, while 75% regarded availability of administrative details as useful, a much lower emphasis was placed on the value of CDS features such as display of standard safe doses (57%) and interaction and ADR alerts (44% and 48%). Comparison of patient and clinician responses identified significant differences in the importance placed on various system features; a greater proportion of patients believed each feature to be important – in particular, the percentage of patients who valued active CDS was almost double that of clinicians (interaction alerts 85% vs. 44% and ADR alerts 84% vs. 48%, respectively; Figure 2).
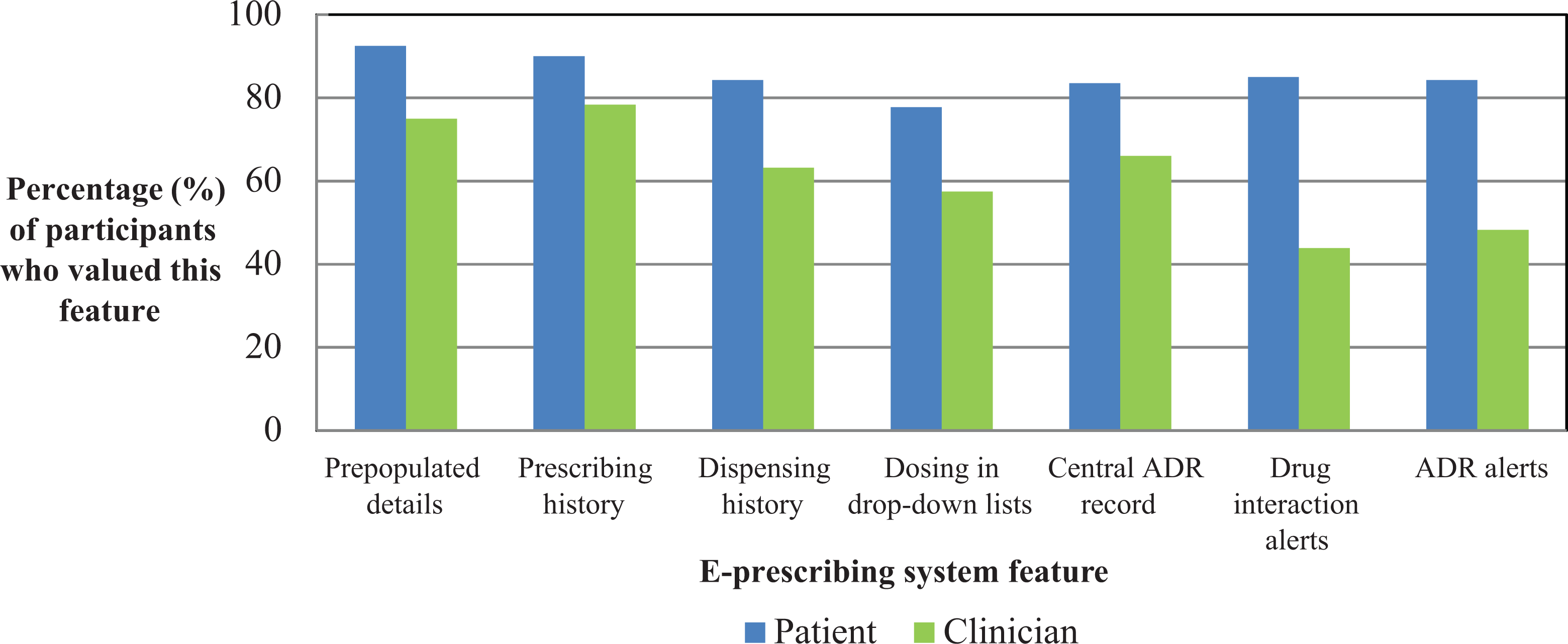
Comparison of features valued by patients and clinicians. ADR: adverse drug reaction.
Discussion
Characteristics of participants and awareness of transition to e-prescribing system
As the primary users of the system, almost all clinicians (98%) were aware of the transition to e-prescriptions. Clinician engagement is widely recognised as an essential element in the successful implementation of electronic medication management systems (Day et al., 2011; Gagnon et al., 2014). In contrast, only about one-third (36%) of patients were aware of the transition to e-prescriptions prior to the study. Although lower, this was consistent with other studies and indicated that many patients may be unaware of the use of e-prescribing, as in one US study where only 58% of patients in a primary care setting were aware of the use of e-prescribing in private practices (Hakim, 2010) or another US study where 25% of patients were unfamiliar with the process involved in e-prescribing (Frail et al., 2014). While innovation and advances in technology transform the delivery of healthcare services and provision of medicines, patients remain the primary beneficiaries of electronic medication management systems. However, patient perspectives are not always considered during project design, implementation and evaluation phases (Hordern et al., 2011). Patient and consumer-centred care should be a key priority for all healthcare organisations, and partnering with consumers is one of the Australian NSQHS standards (Australian Commission on Safety and Quality in Health Care, 2012: 22). These results highlight opportunities to partner with patients by sharing information and providing patient-centred communication and education about initiatives designed to improve the quality use of medicines and healthcare provided.
Attitudes and experiences with the e-prescribing system
Overall, attitudes were aligned between patients and clinicians regarding the perceived impact of e-prescribing on the clarity of the prescription, safety of prescribing and dispensing, access to medicines and allergy/ADR history and communication between healthcare professionals.
Medication safety
The large majority of patients agreed that the e-prescribing system improved the safety of prescribing and dispensing (88% and 91%). This is comparable to a study in a primary care setting (Hakim, 2010), which reported that 79% of patients believed that e-prescribing significantly or somewhat improved medication safety.
Similarly, many clinicians agreed the e-prescribing system reduced prescribing and dispensing errors (94% and 87%) and that medicines interaction and allergy/ADR alerts were appropriate and relevant (83%). This is higher than reported in a study of physicians in the outpatient setting where 50% reported they had avoided a potentially dangerous drug interaction or prescribing despite known allergy as a result of the e-prescribing system alerts (Desroches et al., 2010). Other studies have reported clinicians experiencing “alert fatigue” using e-prescribing systems (Payne et al., 2015; Weingart et al., 2009; Xie et al., 2014). However, these results indicate this is not a particular concern for the majority of clinicians with the e-prescribing system used in this study. This is likely due to alert functionality being set to only trigger interaction alerts with moderate to severe significance and is further explored in the discussion.
An objective, qualitative measurement of the impact of the e-prescribing and dispensing system used in this study on medication errors was outside the scope of this study, with positive outcomes already reported elsewhere (Hodgkinson et al., 2017) and with other e-prescribing systems (Bates et al., 1998; Donyai et al., 2008; Franklin et al., 2007; Westbrook et al., 2012). However, the subjective and positive patient and clinician attitudes regarding the impact of this system on medication errors identified in this study are supported by these previous objective study results.
Efficiency related to workflow and prescription turnaround time
The majority of clinicians believed the system improved workflow due to the ability to copy or edit prescriptions (85%) and create draft prescriptions (81%) and facilitated faster generation of prescriptions (79%). This is consistent with other studies that have found that physicians and nurses believe the use of e-prescribing systems improves workflow and efficiency (Ayatollahi et al., 2015; Khajouei et al., 2011; Lapane et al., 2011).
Determining the time required to generate prescriptions was outside the scope of this study. The actual impact of e-prescribing systems on prescription turnaround time can be highly variable. Some studies of local e-prescribing systems have suggested a slight increase in prescribing time per patient of 20–30 s (Devine, Hollingworth and Hansen et al., 2010), although this may be offset by time saved due to a reduction in the number of orders requiring clarification and other efficiencies gained by access to accurate information at the time of prescribing (Porterfield et al., 2014). Another study reported an initial increase in time of 26 s per patient; however, this was reversed over time as users gained experience interacting with the system and eventually resulted in a time saving of almost 4 min per patient (Overhage et al., 2001). However, these were based on ambulatory or primary care settings in the US.
With respect to the time required to fill a prescription at the hospital pharmacy, 86% of clinicians believed that pharmacists were able to dispense prescriptions faster with e-prescribing. However, only 66% of patients considered the process faster and 28% were unsure of the impact. This suggests that some patients were uncertain about the process involved in the dispensing of an e-prescription at the pharmacy and the overall impact on prescription turnaround time. These results highlight that patient-centred communication and education is needed to improve pharmacist–patient interactions and patient care (Devine, Williams and Martin et al., 2010), particularly as a previous before and after study (Hodgkinson et al., 2017) conducted at the same organisation had identified a reduction in median patient waiting time for outpatient clinic and emergency department e-prescriptions to be dispensed of 52% (from 27 min to 13 min). Total prescription turnaround time is influenced by many other factors apart from the time required to generate a prescription; unexpected delays can occur due to various reasons such as issues with stock availability or high prescription volume (Raghuvanshi and Choudhary, 2013). Approaches to improve patients’ understanding and expectations may involve ensuring transparent communication between health professionals and patients about the dispensing process, current capacity and existing demands on efficient and timely supply of medicines.
Privacy and overall preferences
The large majority of patients (90%) in this study were comfortable with the level of privacy and security around e-prescriptions. Historically, patients have been concerned about confidentiality of computerised personal health records maintained by healthcare providers (Ridsdale and Hudd, 1994). Similarly within the last decade, patients have reported mixed views about the privacy of electronically stored personal health information, with some studies reporting 50% of patients expressed no opinion when asked about the perceived confidentiality of an EMR system (Freeman et al., 2009) and 37% of patients reported concerns about loss of privacy with electronic medical files (Strayer et al., 2010; Vodicka et al., 2013). More recently with the development of the personally controlled electronic health record in Australia, a study of general public perspectives (Andrews et al., 2014) identified a moderate level of concern about privacy and confidentiality of electronic health records, which could influence patient and consumer adoption and acceptance of technology.
There was also a high overall patient preference for e-prescribing over handwritten prescriptions, with 86% of patients preferring e-prescriptions in this study. Another study (Freeman et al., 2009) reported only 63% of patients felt e-prescriptions were better than handwritten prescriptions at an ambulatory care practice with an EMR. The results suggest many patients have a high level of confidence in and acceptance of the e-prescribing system used in this study. This is aligned with patients’ positive attitudes towards the perceived benefits of the systems. However, there is likely to be an ongoing, albeit reducing, proportion of patients who prefer the previous handwritten prescription system. Over time, as these systems become further embedded in routine practice, overall preference for e-prescribing over handwritten systems may improve.
Features valued in an e-prescribing system
The importance placed on key e-prescribing system features varied widely between patients and clinicians. While features designed to improve access to timely and relevant medicines information were generally well regarded, responses related to active and passive CDS functionality demonstrated differences between patients and clinicians.
Access to information
Timely availability of relevant information was highly valued by both patients and clinicians, including pre-populated patient and prescriber details and previous prescribing and dispensing history. These features are among other e-prescribing software features that are rated as having medium to high positive impact on safety, quality and usefulness to clinicians and patients by a multidisciplinary group of Australian experts (Sweidan et al., 2010).
Integration of the prescribing and dispensing system in this study by utilising one shared database of information (including a common medication dataset) allowed display of pharmacy dispensing history within the e-prescribing system and enabled automatic population of prescription details in the pharmacy dispensing software. Some studies have shown that direct transfer of medicines information from prescribing to dispensing may result in reduction of certain types of dispensing errors (Franklin et al., 2014). Other aspects of the integrated system included electronic transfer of recorded allergy/ADR information from the e-prescribing system to patient medication lists and electronic alerts in hospital scanned medical records.
Potential strategies to further develop access to timely and relevant medicines information include the integration of hospital formulary restrictions and stock availability into the e-prescribing system. Provision of accurate and up-to-date formulary information has been shown to influence both patient perspectives (Frail et al., 2014) and perceived efficiencies in clinician workflow (Lapane et al., 2011). These enhancements in system functionality would streamline the prescribing process for clinicians and reduce delays in prescription turnaround time due to conflicts with hospital formulary restrictions or stock availability. Perceptibly, the availability of this functionality was also suggested by patient and clinician participants through open-ended comments in this study.
Medication safety
In this study, participants’ views on active CDS were explored using statements describing medicines interaction and allergy/ADR checking capability. While over 80% of patients valued alerts for medicines interactions and ADRs (85% and 84%), less than half of clinicians believed these were important (44% and 48%). Another statement regarding passive CDS described restricted dosing options in drop-down lists when prescribing. While 78% of patients valued this feature, it was only considered important by 57% of clinicians. These were also features rated as having medium to high positive impact on safety, quality and usefulness to clinicians and patients by a multidisciplinary group of Australian experts (Sweidan et al., 2010).
The significant differences in attitudes between patients and clinicians are not surprising, as only clinicians’ experiences would be based on direct user interaction with CDS system features. Additionally, CDS features that required users to actively override electronic alerts had a greater impact on clinician attitudes compared to passive functions that did not involve direct intervention. While medicines interaction alerts and allergy/ADR checking capability provides clinical guidance to prescribers, concerns about “alert fatigue” have been well documented in the literature (Payne et al., 2015; Weingart et al., 2009; Xie et al., 2014). Factors such as alert volume and level of clinical significance can have a major impact on the usefulness of CDS features, and override rates can be as high as 88% and 69% for medicines interaction and ADR alerts, respectively (Payne et al., 2002). While CDS systems can enhance decision-making within clinical workflow, careful refinement of software functionality related to interaction checking logic and frequency of displayed alerts is needed to optimise relevance and effectiveness in practice for clinicians.
Convenience
Patients’ attitudes towards the impact of the e-prescribing system on the length of time required to obtain their prescription were explored. Only 57% of patients placed importance on the speed of obtaining a prescription, when generated by a prescriber or when dispensed by the pharmacy, which may challenge previous assumptions held by other stakeholders regarding patients’ priorities. In contrast, the large majority of patients valued other aspects of an e-prescribing system, such as those designed to improve medication safety and access to relevant information. This suggests that patients highly value system features that promote the effective and safe use of medicines; a primary outcome that clinicians similarly aim to achieve.
Limitations
This study describes the attitudes and experiences of patients and clinicians towards the e-prescribing system. As these were attitudes identified using survey methodology, they may not necessarily reflect the actual evidence quantifying the impact on medication errors or waiting times. However, reductions in waiting time and prescribing and dispensing errors at the same organisation have been reported in a separate study using objective measurements (Hodgkinson et al., 2017). Other limitations included the timing of the study, as changeover of junior medical staff occurred during the data collection period, and the survey was conducted early in the year when many new staff had recently been recruited to the organisation and may not have developed familiarity with the e-prescribing system. Also, while the research team visited 95 areas during participant recruitment, three outpatient areas at one site were excluded as e-prescribing had not been fully implemented. For participants included in the study, a possibility of recall bias existed as they may not have used e-prescribing or received an e-prescription immediately before completing the survey. For those who did not participate, non-response bias may have been present as even though response rates were reasonable, the views of the sample population may not necessarily reflect the entire population. Confirmatory factor analysis was not performed as direct comparison of responses between patients and clinicians occurred only if a statement in the patient survey aligned to a specific statement in the clinician survey.
Conclusion
This study revealed a diverse range of perspectives from patients and clinicians towards the e-prescribing system. Overall the transition to the e-prescribing system resulted in a positive impact on perceived medication safety and availability of information and a high level of patient satisfaction and acceptance of e-prescriptions. It was apparent that patients valued safe and effective use of medicines, synonymous with the primary purpose of an electronic medication management system. The home-grown system used in this study featured unique integration of e-prescribing and dispensing programs, which may not be applicable to e-prescribing systems in other organisations, particularly those integrating an EMR with a legacy dispensing system. However, the study findings on the value attributed to key e-prescribing system features by patients and clinicians, as well as patient perspectives about privacy, may be generalisable to other Australian and international settings where implementation of a new system or enhancements to an existing system are being considered. While patients and clinicians had similar attitudes towards the e-prescribing system used in this study, there were differences between each group in the value placed on key features. The study findings demonstrated the importance of gaining a better understanding of both patient and clinician attitudes. Patients’ attitudes may challenge assumptions made by other key stakeholders of electronic healthcare systems such as clinicians and software developers. Changes to improve service delivery, software functionality and patient-centred care should take into consideration the needs and expectations of both patients and clinicians. Moreover, engagement, communication and education strategies that include patients during the design, implementation and evaluation of these systems are needed to improve patient partnership and awareness of the impact on clinician workflow and patient care. Further research on patient attitudes towards EMRs and personal health records are necessary to appropriately inform future decisions and ensure that healthcare organisations fully engage in partnership with patients for optimal outcomes.
Supplemental material
Supplemental Material, Appendix_1_-_Patient_Survey_-720601 - Patient and clinician perspectives of an integrated electronic medication prescribing and dispensing system: A qualitative study at a multisite Australian hospital network
Supplemental Material, Appendix_1_-_Patient_Survey_-720601 for Patient and clinician perspectives of an integrated electronic medication prescribing and dispensing system: A qualitative study at a multisite Australian hospital network by Grace Lau, Jayde Ho, Susan Lin, Karen Yeoh, Tiffany Wan, and Marisa Hodgkinson in Health Information Management Journal
Supplemental material
Supplemental Material, Appendix_2_-_Clinician_Survey_720601 - Patient and clinician perspectives of an integrated electronic medication prescribing and dispensing system: A qualitative study at a multisite Australian hospital network
Supplemental Material, Appendix_2_-_Clinician_Survey_720601 for Patient and clinician perspectives of an integrated electronic medication prescribing and dispensing system: A qualitative study at a multisite Australian hospital network by Grace Lau, Jayde Ho, Susan Lin, Karen Yeoh, Tiffany Wan, and Marisa Hodgkinson in Health Information Management Journal
Footnotes
Acknowledgement
The authors would like to thank Danica Eng, Pharmacy Student, Monash University; Karina Fildes, Pharmacy Student, La Trobe University; Tran Le, Pharmacy Student, Monash University; Meghana Maduri, Pharmacy Student, RMIT University; and Roshny Stanly, Pharmacy Student, James Cook University.
Data access statement
All data supporting this study are provided in the results section and supplementary information accompanying this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.