
Abstract
Objective:
To calculate average savings of using health information exchange (HIE) for demographic and treatment requests for chlamydia and gonorrhoea in Western New York, specifically the Erie County Department of Health and its catchment area.
Method:
We conducted a mixed-method case study. Qualitative methods included interviews, document review, and workflow mapping, which were used as the inputs to identify time savings. Case rates, time savings, and salary averages were used to calculate average savings.
Results:
The avoided demographic information requests resulted in time and money savings (range of USD$2312–USD$4624 for chlamydia and USD$809–USD$1512 for gonorrhoea) as did avoided treatment requests (range of USD$671–USD$2803 for chlamydia and USD$981–USD$1635 for gonorrhoea).
Discussion:
HIE supported sexually transmitted infection (STI) treatment by making it easier for public health staff to identify and act upon STI diagnoses. Availability of information online resulted in less reliance on provider offices for demographic and treatment information.
Conclusion:
Results indicated that using HIE to support treatment and management of STIs can save public health staff time spent on obtaining demographic and treatment information. Other public health departments could use HIE for this and other types of disease surveillance activities. Considering public health needs in HIE development and use can improve efficiency of public health services and enhance effectiveness of activities.
Keywords
Background and significance
Among the many functions of public health departments in the United States is identification, prevention and treatment of patients with sexually transmitted infections (STIs) (Jajosky and Groseclose, 2004). Treatment of patients with STIs is complicated by locating patients and partners (CDC, 2014). Patients requiring additional treatment following a positive test result are frequently difficult to locate, and obtaining information about sexual contacts for contact tracing is an even greater challenge. Public health staff often have incomplete or incorrect information obtained from the clinical laboratory or provider’s office that reports a positive reportable test result. Consequently, locating patients is very time-consuming and is frequently unsuccessful (Gamache et al., 2010). Health information exchange (HIE) across healthcare settings could ameliorate these challenges.
In Western New York (WNY), public health officials use the local HIE, HEALTHeLINK, to support a variety of functions including receiving and processing reporting to public health agencies; receiving and acting upon alerts; and supporting for clinical care, investigations and quality measurement (Haque et al., 2016). Public health staff use the HIE to query clinical records to obtain patient and partner information such as addresses and phone numbers. Staff can also access recent visits, medication histories, lab reports, radiology reports, and pharmacy histories, including prescriptions written and medications dispensed. These are data that staff had access to prior to HEALTHeLINK implementation but required cumbersome, manual processes to access.
HEALTHeLINK serves eight counties in WNY. The HIE enjoys 100% hospital participation and has 4009 participating providers, and 98% of lab records and 90% of radiology reports are available through the HIE. HEALTHeLINK was founded by local hospitals and payers, who maintain it and are responsible for it financially. Additional funding was provided by the Beacon Community demonstration program (Beacon, 2014). While the Erie County Department of Health (ECDOH) is involved in HEALTHeLINK, the relationship is not financial.
Access to clinical records on HEALTHeLINK requires patient consent but approved local and state health department personnel and emergency care providers are granted exemptions to this consent requirement (Haque et al., 2016; Kass-Hout et al., 2007; Massoudi et al., 2014). This is in line with HIPAA and other policies that exempt public health departments from standard consent rules. HEALTHeLINK is not a database or repository. Rather, it provides a mechanism for querying records. The Board of Directors is responsible for role-based access control and monitoring those who access records in order to protect patient privacy and prevent unauthorised access (Haque et al., 2016; Massoudi et al., 2014).
After public health staff receive notification of positive communicable disease test results via the NYS Electronic Clinical Laboratory Reporting Surveillance (ECLRS) system, they access HEALTHeLINK to obtain additional clinical, administrative, and demographic data. These data support communicable disease investigations, leading to timely and accurate identification and treatment of affected patients (Beacon, 2014). An increase in efficiency can lead to improved partner management, which is paramount in controlling the spread of these infections. Improved management of individual patients and their contacts can result in improved outcomes in populations as a whole (Maenpaa et al., 2011; Shapiro, 2007; Shapiro et al., 2011).
Objective
The objective of this study was to identify and quantify the benefits of using HEALTHeLINK in WNY. We hypothesised that with HEALTHeLINK use, we would be able to increase reported treatment rates of both gonorrhoea and chlamydia, the most commonly reported communicable diseases. Furthermore, we expected to see a significant cost savings with less staff time devoted to completing these disease investigations, getting cases into the appropriate care and notifying partners.
Method
Research design
We used a mixed-method approach to more fully understand the impact of HEALTHeLINK on STI treatment and management in Erie County (Massoudi et al., 2014). Data collection and analysis included document review, interviews, thematic analysis and time-saving estimates. Institutional Review Board (IRB) oversight was through the RTI International IRB, which considered this work exempt (IRB ID #13211).
Qualitative data collection and analysis
We conducted in-person and telephonic semi-structured interviews with staff from the ECDOH, the New York State Department of Health and HEALTHeLINK. Interviews followed a discussion guide tailored to the role of the participant. The hour-long interviews were audio-recorded with permission and transcribed. The interviewed staff represented a variety of functional roles, including public health commissioners, nurses, epidemiologists, investigators and information technology specialists. We followed up with ECDOH professionals to obtain detailed information on how HEALTHeLINK changed the workflow across disease investigations and interventions.
Interview transcripts were uploaded into NVIVO, a qualitative software analysis program, for thematic analysis. The documents were coded and 25% of interviews were double coded to assess interrater reliability. The two coders achieved an average κ coefficient of 0.8 or greater on codes on the double-coded interviews.
Quantitative data collection analysis
We used inputs from interviews, time motion data, epidemiologic reports and workflows to estimate the impact of HEALTHeLINK in Erie County. This information coupled with wage and labour data was used to develop a model of potential savings based on the following categories of benefits: resource savings for disease investigations and interventions and improved disease surveillance.
Benefits from time savings were derived through interviews with ECDOH staff to construct a detailed description of workflows with and without HEALTHeLINK and identifying time savings. Workflows were validated with ECDOH staff. Time-saving categories included avoiding home visits, more efficient data collection and avoiding manual processes. Time savings were not absolute but were provided in ranges. To value these time savings, we use publicly available data to estimate the cost of employment for epidemiologists employed by local governments. In 2012, the mean hourly wage for epidemiologists employed by local governments was USD$29.99 (May 2012). To adjust the hourly wage to reflect the total cost of employment, we adjust the wage to reflect that 40% of the cost of employment for state and local government employees goes toward benefits (2013) and also include an additional 17% of the hourly wage to reflect overhead costs of employment(C, 2002). Under these assumptions, we estimate the fully loaded hourly cost of employment for epidemiologists employed by local governments to be USD$55.08. Applying this value to the estimate of time savings annually, we calculated rates for savings based on the cost of employment and ranges of time savings.
ECDOH provided data regarding the quarterly success rate of following up with individuals and their partners before and after HEALTHeLINK implementation. These data included quarterly summaries of all interviews for patients with chlamydia, gonorrhoea and syphilis and their elicited partners between April 2009 and September 2013. Treating each quarterly report by individual who followed up and disease as an individual data point, we ran two regression models to estimate the change in success rate before and after HEALTHeLINK adoption.
Results
Treatment rates for chlamydia and gonorrhea
HEALTHeLINK was implemented in WNY in 2012. After implementation, ECDOH significantly increased reported treatment rates for both chlamydia and gonorrhoea. Reported chlamydia treatment rates increased from 77.5% in 2011 to 92.6% in 2013 (p < 0.05; Figure 1). Reported gonorrhoea treatment rates increased from 79.2% in 2011 to 94.7% in 2013 (p < 0.05; Figure 2).
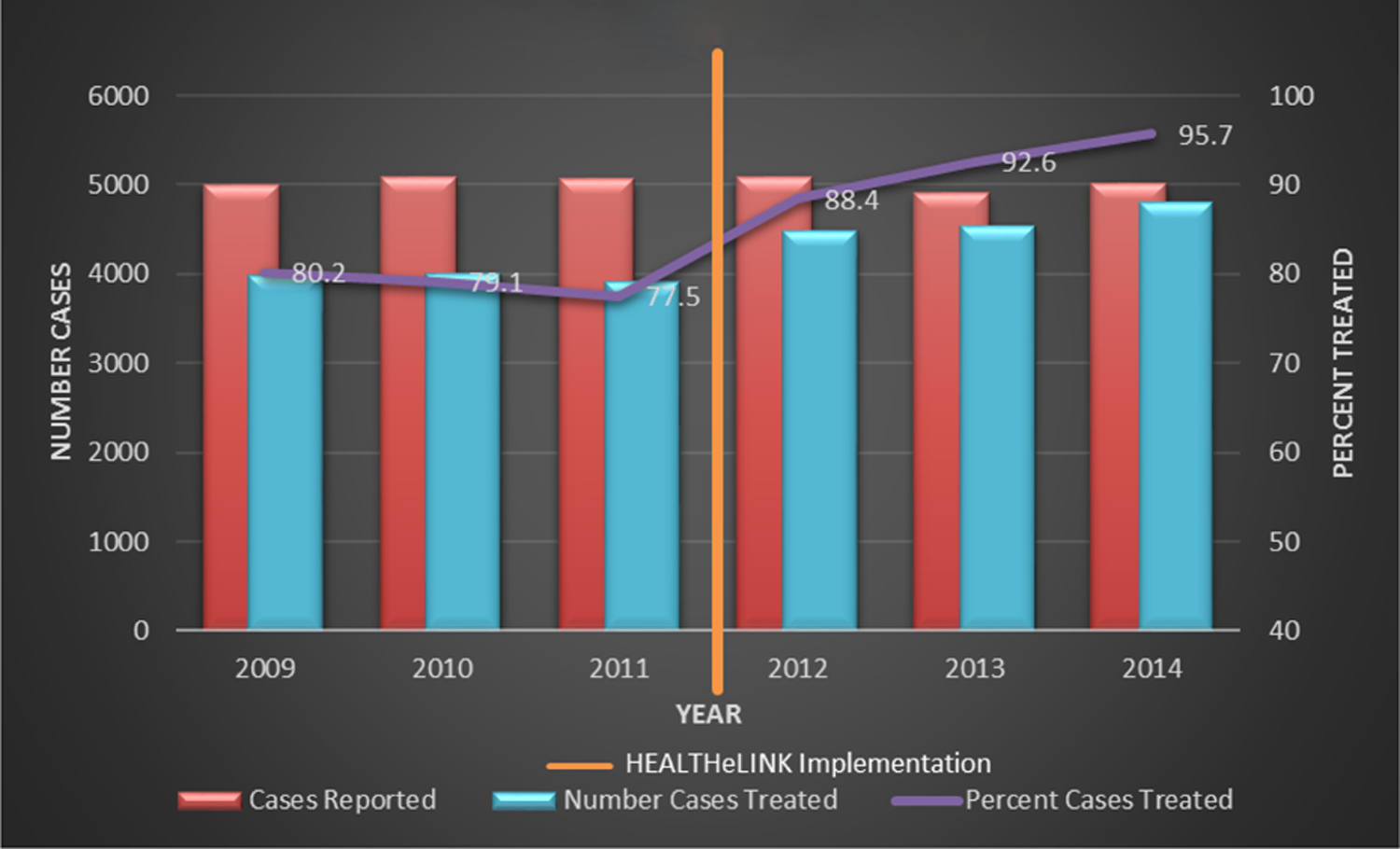
Reported chlamydia treatment by year in Erie County, New York.

Reported gonorrhoea treatment by year in Erie County, New York.
Resource savings for tracking and reporting STIs
In 2012, 5088 chlamydia cases were reported in Erie County. ECDOH epidemiologists estimated that between 5 and 10% of ECLRS reports contain incomplete demographic information and that this information can be found in HEALTHeLINK for 99% of cases. Through interviews with ECDOH staff and calculating time savings, we estimate HEALTHeLINK obviates additional demographic data collection for 378 cases.
ECDOH epidemiologists estimate that obtaining demographic information in HEALTHeLINK rather than contacting the laboratory or ordering physician saved approximately 10 min of their time per case. Based on the number of demographic informational requests for chlamydia cases in 2012, we estimated that using HEALTHeLINK to obtain cases’ demographic information saved 63 epidemiologist hours, leading to an estimated USD$3468 of salary savings (Table 1).
Estimated annual savings of avoided demographic information requests and avoided treatment requests for chlamydia cases from HEALTHeLINK in 2012.
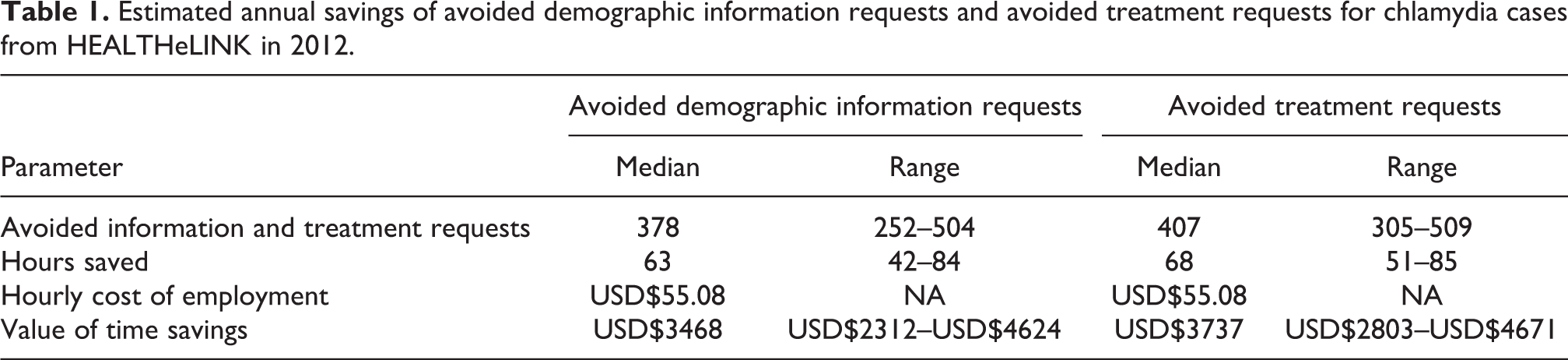
ECDOH staff estimate that in approximately 20% of chlamydia cases, providers do not document treatment. ECDOH epidemiologists estimate that when treatment can be confirmed in HEALTHeLINK, they save approximately 10 min of time per case. Based on our estimate of the number of treatment requests for chlamydia cases in 2012, we estimated that using HEALTHeLINK saved 68 epidemiologist hours, leading to an estimated USD$3737 of salary savings (Table 2).
Estimated annual savings of avoided demographic information requests and avoided treatment requests for gonorrhea cases from HEALTHeLINK in 2012.

In 2012, 1781 gonorrhoea cases were reported in Erie County. Based on the number of demographic informational requests for gonorrhoea cases in 2012, we estimated that using HEALTHeLINK to obtain cases’ demographic information saved 22 epidemiologist hours leading to an estimated USD$1214 of salary savings (Table 2). Based on our estimate of the number of treatment requests for gonorrhoea cases in 2012, we estimated that using HEALTHeLINK saved 24 epidemiologist hours, leading to an estimated USD$1308 of salary savings in 2012 (Table 2).
Discussion
STI management is a significant challenge for public health agencies. Rapid STI case identification, treatment and contact tracing of partners is a key component of STI management. One of the biggest challenges is the inability to quickly and accurately obtain patient information once a positive clinical laboratory test is reported. Delays in obtaining patient information can lead to delays in treatment, which can result in increased disease severity and disease transmission. This may lead to cost savings due to early detection and treatment.
By providing the ability to access patient information from almost any source in a given area, HIE has the potential to increase the level of efficiency in tracking and treating affected patients and their partners. With the use of HEALTHeLINK, ECDOH was able to significantly increase both reported chlamydia and gonorrhoea treatment rates to over 90% in 2013, only 1 year after implementation of routinely accessing HEALTHeLINK.
HEALTHeLINK allows public health staff to obtain accurate patient demographic and treatment information more efficiently. In addition, it saves provider staff time in responding to demographic and treatment requests. Prior to HEALTHeLINK access, obtaining these data was a manual process with limited ability to look at multiple data sources. For each incomplete chlamydia and gonorrhea case report, using HEALHTeLINK resulted in an estimated staff time savings of 10 min for each demographic request and 10 min for each treatment confirmation. These time savings translate to ECDOH epidemiologist staff time reduction of a total 131 hours per year for chlamydia surveillance and an additional 46 hours per year for gonorrhoea surveillance, for a total of almost 4.5 weeks of epidemiology staff time saved per year.
HEALTHeLINK’s time savings improved productivity that allowed for caseload expansion. Prior to HEALTHeLINK implementation, ECDOH only investigated gonorrhoea and chlamydia cases diagnosed in the ECDOH STD Clinic. In 2014, ECDOH was able to expand their caseload to also investigate all gonorrhoea cases and certain high-risk chlamydia cases (e.g. younger than 16 years of age, pregnant, repeat positive test within 90 days or provider request for assistance finding patient location and treatment) in one high morbidity Buffalo City zip code. By 2015, two additional zip codes were also added to the coverage area, which improved reach. Because of the increased efficiency afforded by HEALTHeLINK, ECDOH was able to expand its area of disease investigation without any increase in work hours. As a result, without any increase in budget, ECDOH was able to expand effective disease control and partner services to a large number of additional residents who may have been missed prior to HEALTHeLINK use. It is likely that significant savings resulting from fewer untreated patients with fewer long-term complications improved partner identification and treatment also ensued. However, time savings and increased surveillance are not additive.
Limitation
There could have been other relevant contextual factors that may potentially have contributed to increased treatment rates that were not included in the study. However, interview data overwhelmingly linked the above changes to HEALTHeLINK implementation.
Conclusion
While we have demonstrated that an HIE, such as HEALTHeLINK, can be an excellent tool for gonorrhea and chlamydia surveillance and disease investigation, this is far from the only possible use of these systems. Other possibilities include HIV partner management, hepatitis surveillance, rabies investigations, tracking food-related outbreaks and syndromic surveillance for genetic diseases. HEALTHeLINK may also have other advantages. Computerised services have the advantage of 24 hr access, compared to most medical offices which are only open during business hours. Also, an HIE can lessen the burden on providers in the community. Rather than calling a clinician or hospital, using the health exchange system, public health staff can look up records on their own. This can lessen the time office staff spends on the phone. In addition, chart reviews can be conducted remotely rather than at participating hospitals, eliminating travel time and expense. These advantages can be translated to other areas of disease surveillance and outbreak management. HIE can be used to promote more efficient, accurate and complete tracking and monitoring.
Through the use of an HIE, ECDOH was able to improve surveillance efficiency and accuracy, which led to improved ECDOH reported gonorrhoea and chlamydia treatment rates and cost savings in staff time. HIE has great promise to support public health activities. The experience using HIE to support STI treatment and management can be expanded to other types of disease surveillance and outbreak management. Considering public health needs in HIE development and use can improve efficiency of public health services and enhance effectiveness of activities.
Footnotes
Authors’ note
The views expressed are solely those of the authors and do not reflect the official positions of the institutions or organisations with which they are affiliated or the views of the project sponsors.
Acknowledgements
The authors are grateful to the staff of the Erie County Department of Health, the New York State Department of Health and HEALTHeLINK for their time and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (contract 200-2011-F-40207).