
Abstract
Background:
Three-quarters of non-communicable disease (NCD) mortality occurs in low- and middle-income countries. However, in most developing countries, quality and reliable data on morbidity, mortality and risk factors for NCD to predict its burden and prevalence are less well understood and availability of these data is limited. To better inform policymakers and improve healthcare systems in developing countries, it is also important that these factors be understood within the context of the particular country in question. Objective: The aim of this study is to further inform practitioners in Ethiopia about the availability and status of NCD information within the Ethiopian healthcare system.
Method:
A mixed method research design was used with data collected from 13 public referral hospitals in Ethiopia. In phase 1 quantitative data were collected from 312 health professionals (99 physicians; 213 nurses) using a cross-sectional survey. In phase 2, qualitative data were collected using: interviews (n = 13 physician hospital managers); and one focus group (n = 6 national health bureau officers).
Results:
Results highlighted the lack of NCD morbidity, mortality and risk factor data, periodic evaluation of NCD data and standardised protocols for NCD data collection in hospitals. The study also identified similar discrepancies in the availability of NCD data and standardised protocols for NCD data collection among the regions of Ethiopia.
Conclusion:
This study highlighted important deficiencies in NCD data and standardised protocols for data collection in the Ethiopian healthcare system. These deficiencies were also observed among regions of Ethiopia, indicating the need to strengthen both the healthcare system and health information systems to improve evidence-based decision-making.
Implications:
Identifying the status of NCD data in the Ethiopian healthcare system could assist policymakers, healthcare organisations, healthcare providers and health beneficiaries to reform and strengthen the existing healthcare system.
Keywords
Introduction
The incidence of non-communicable diseases (NCDs) has increased, resulting in the death of 38 million people in 2012, of which 28 million occurred in low- and middle-income countries, causing an estimated US$7 trillion economic loss (WHO, 2014). A significant number of NCDs, such as cardiovascular disease, diabetes, hypertension and obesity, can be avoided by addressing the major behavioural and metabolic risk factors associated with such conditions (Mwai and Muriithi, 2015). Their prevention and treatment requires reliable, accurate and timely information on their symptoms and associated risk factors. Therefore, the availability and use of credible data to identify current and potential NCD morbidity, mortality and related risk factors has become increasingly important (Mishra et al., 2016).
Research indicates that the availability of NCD data at local, regional and national levels is helpful for decision makers to prioritise prevention, asset distribution and budget allocation in the healthcare system (Mishra et al., 2016). It has been demonstrated that strengthening the health system is a possible way to resist the growing burden of NCD and ensure enhanced health results (Nutley and Reynolds, 2013). An effective health system is built on a well-functioning information system that collects accurate, reliable, timeous and relevant health data for optimal healthcare delivery and decision-making (Ledikwe et al., 2014; Mpofu et al., 2014). The lack of data in the healthcare system is a hindrance to planning, allocating resources and implementing appropriate NCD intervention strategies (Cresswell and Sheikh, 2015). Studies have indicated that the effective prevention of NCD is based on having consistent morbidity, mortality and related risk factors data to plan, design and implement evidence-based decision-making and its preventive strategies at regional and national levels. NCD surveillance data can be best collected by establishing and implementing data collection standardised protocols in the healthcare system (Mishra et al., 2016). Such standardised protocols are data collection forms used to obtain morbidity, mortality and risk factor data (Ledikwe et al., 2014). A study by Wandai et al. (2017) indicated that collecting NCD data alone is not enough for their effective prevention and intervention, but that a well-organised healthcare system needs to periodically evaluate the data quality, timeliness and accuracy of mortality, morbidity and related risk factors to ensure effective decision-making (Mpofu et al., 2014). While progress has been made to lead the development of national NCD monitoring programmes, most developing countries are still struggling to adequately establish robust information systems to help with their intervention, treatment and related risk factors (Ranck and Ranck, 2011).
Health information systems (HIS) store information that is obtained from patient records, surveys, health plans and other data sources (Oluwafemi and Ameenah, 2014). Most developed countries, such as the United States, Australia and Europe, have established standards and processes in their healthcare sector to obtain ongoing information on morbidity, mortality, NCD risk factors as well as determinants of their care services (Brattig Correia et al., 2013). Middle-income countries, such as South Africa (Mphatswe et al., 2012), and low-income countries, such as Ghana, Mozambique, Rwanda, Tanzania and Zambia, have conducted studies to investigate the capacity of their national HIS, which resulted in them developing strong disease surveillance systems to better understand their disease profiles (Mutale et al., 2013). The availability of health information in the healthcare system enabled these countries to exchange health-related data between healthcare providers, organisations and health service consuming communities (Dixon et al., 2013).
According to Kumar (2011) and Diamantidis and Becker (2014), the availability of public health data in the healthcare system enables: timely and appropriate healthcare decisions to be made, quick information retrieval, fast information sharing, improved data storage and improved information screening and reporting, all of which enhance the quality of healthcare. Furthermore, having NCD mortality, morbidity and risk factor information about their population helps policymakers and healthcare providers to establish relevant preventive strategies in the national healthcare system. In a healthcare system with accessible, accurate, reliable, timely and cleaned health information, it is possible to predict the future burden of NCD in that country (Ranck and Ranck, 2011). Globally, various countries have established healthcare strategic plans in order to address the burden of NCD by specifically focusing on the four major lifestyle risk factors, these being an unhealthy diet, physical inactivity, tobacco use and excessive alcohol consumption (Tsolekile et al., 2014). The Ethiopian Ministry of Health has made a concerted effort to improve the health status of its inhabitants, particularly regarding preventing and treating infectious communicable diseases, such as HIV/AIDS and tuberculosis (Letebo and Shiferaw, 2016). This was achieved by training thousands of health extension professionals who were responsible for educating the public on these diseases.
However, little attention has been devoted to preventing and treating NCD in Ethiopia (Teklehaimanot and Teklehaimanot, 2013), which has resulted in an increased burden of such conditions on individuals, communities and the healthcare system, as is the case in most low-income countries. Despite the growing evidence of NCD in this population, the operating healthcare system predominantly focuses on preventing and treating infectious communicable diseases, with little evidenced-based research that evaluates the availability of their morbidity, mortality and associated risk factors. Therefore, the present study aimed to establish a knowledge base for practitioners in relation to the availability and status of NCDs information in the Ethiopian healthcare system.
Method
Research design
A mixed method sequential explanatory research design was used for this study, which included questionnaires and focus group discussions (FGDs) that aimed to ascertain the knowledge of practitioners regarding the availability and status of NCD data, and the standardised protocols for data collection in the Ethiopian public referral hospitals. The study was conducted at 13 purposively selected public referral hospitals in Ethiopia that provide tertiary level healthcare services for NCD. Ethical clearance was obtained from the University of KwaZulu-Natal’s Biomedical Research Ethics Committee (reference number HSS/0683/015D). Additionally, administrative permission to conduct the study in Ethiopia was obtained from the Ethiopian Ministry of Health after the concerned bodies ethically reviewed the proposal. Informed consent was obtained from each participant after explaining the purpose of the study.
Participants
The study was conducted in two phases due to the explanatory sequential design, the first being quantitative and the second qualitative. In phase I, 99 physicians were purposively selected; and 213 nurses proportionately and randomly selected from their respective hospitals for the first (quantitative) phase of the study. For the second (qualitative) phase, 13 hospital managers, who are all qualified medical doctors, and 6 national health bureau officers were purposively selected to participate. Purposive sampling ensured accurate and reliable results and sampling bias in this case was eliminated by setting specific inclusion and exclusion criteria. The randomisation of the sample of nurses also served to mitigate potential sampling bias. Participants were considered for inclusion in the study if they had had 3 years or more work experience treating NCD-related conditions in a hospital setting.
Materials and data collection
After an extensive literature review, prior to the main study and data collection, self-administered questionnaires were developed and validated by conducting a pilot study on 30 practitioners from two other hospitals not included in this study. Questionnaire items were scored on a five-point Likert-type scale, with a significance level of (p < 0.05) selected. A Cronbach’s α of 0.80 was obtained. Qualitative data were thematically analysed.
In phase I, healthcare professionals who provided consent to participate and met the inclusion criteria completed the questionnaires, which consisted of two sections. The first section obtained the participants’ demographic characteristics, and the second addressed the practitioners’ knowledge of (a) the availability of NCD morbidity, mortality and risk factor data; (b) the presence of mechanisms to periodically evaluate NCD data quality, reliability and timeliness; (c) and the availability of standardised protocols for NCD morbidity, mortality and risk factor data collection. Regional discrepancies regarding these issues were explored.
In Phase II, interviews and one focus group were conducted to investigate participants’ personal opinions and knowledge of NCD data availability, quality, timeliness and the link between the data and prevention of NCDs in the Ethiopian healthcare system (Box 1). The interviews (n = 13 physician hospital managers) and one focus group (n = 6 national health bureau officers who work for the NCD Department of the Ethiopian Ministry of Health) were taped and conducted by two researchers (MDK & JMG). Due to geographical variation and distance between the hospitals, it was impossible to undertake focus groups with all hospital managers. In addition, the records and HIS were examined at all 13 hospitals by checking the availability of NCD data.
Questions for Phase II of the study on non-communicable disease (NCD) related data.

Data analysis
In phase I, the Statistical Package for Social Science (SPSS) version 24 was used to analyse the quantitative data. Descriptive statistical analyses included frequencies for the socio-demographic characteristics of participants. Statistical measures, such as means, standard deviations and a sample t-test, where applicable, were used to measure the practitioners’ knowledge of the availability of NCD data and standardised protocols in the hospitals. The bivariate analysis, analysis of variance (ANOVA; Welch where conditions for ANOVA are not met), was used to establish the differences in the knowledge of the practitioners on the availability of NCD data and standardised protocols across regions. One-way ANOVA Robust Tests of Equality of Means, a test for several independent samples that compare two or more groups of cases in one variable, was applied to determine the practitioners’ knowledge of the availability of NCD data and standardised protocols across regions. All tests were conducted to show a 95% confidence interval and to recognise a 5% level of significance, with all means being considered significantly different at p <0.05. In Phase II, qualitative data from the interviews and focus group were transcribed and transferred into the NVivo 11 software program (NVivo, 2015) with data being analysed with a thematic content analysis method.
Results
Phase I
Phase I results were obtained from the 99 purposively selected physicians and the proportionately and randomly selected 213 nurses to address the three study objectives: (i) availability of NCD morbidity, mortality and risk factor data; (ii) presence of mechanisms to periodically evaluate NCD data quality, reliability and timeliness; and (iii) availability of standardised protocols for NCD morbidity, mortality and risk factor data collection.
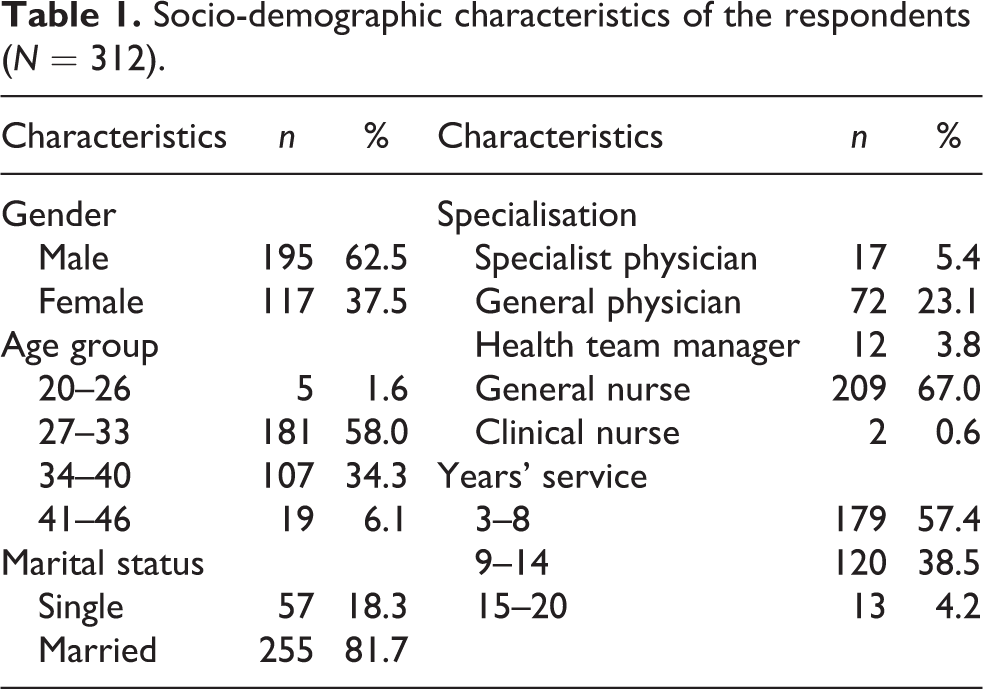
Socio-demographic characteristics of the participants (Table 1) showed that the majority were male (n = 195, 62.5%), over half were between 27 and 33 years of age (n = 181, 58.0%), the majority were married (n = 255, 81.7%) and 209 (67.0%) were general nurses. Specialist physicians accounted for 5.4% (17), with general physicians making up 23.1% (72) of respondents. Over half of the respondents (n = 179, 57.4%) had 3–8 service years, with very few (n = 13, 4.2%) having more than 15 years of service.
Socio-demographic characteristics of the respondents (N = 312).
Availability of NCD morbidity, mortality and risk factor data
Mean ratings of practitioner knowledge of availability of NCD data in the HIS of the 13 hospitals are depicted in Table 2. The availability of morbidity-related NCD data (presence of NCD-related disease or other adverse health events, including illness, injuries or disability associated with NCD) (M = 2.51, SD = 1.033, t (311) = −8.329, p < 0.0005); NCD risk factors data report (M = 2.78, SD = 1.195, t (311) = −3.316, p = 0.001); case-specific mortality-related data (M = 3.25, SD = 1.506, t (311) = 2.971, p = 0.003); and case-specific morbidity-related data (M = 2.35, SD = 0.990, t (311) = −11.670, p < 0.000) were all found to be significant. Other aspects related to the availability of NCD data were significantly below the mean value of 3 on the five-point Likert-type scale (Table 2).
Practitioners’ knowledge of availability of NCD data in the Ethiopian HIS.

NCD: non-communicable disease; HIS: health information systems; CI: confidence interval; SD: standard deviation.
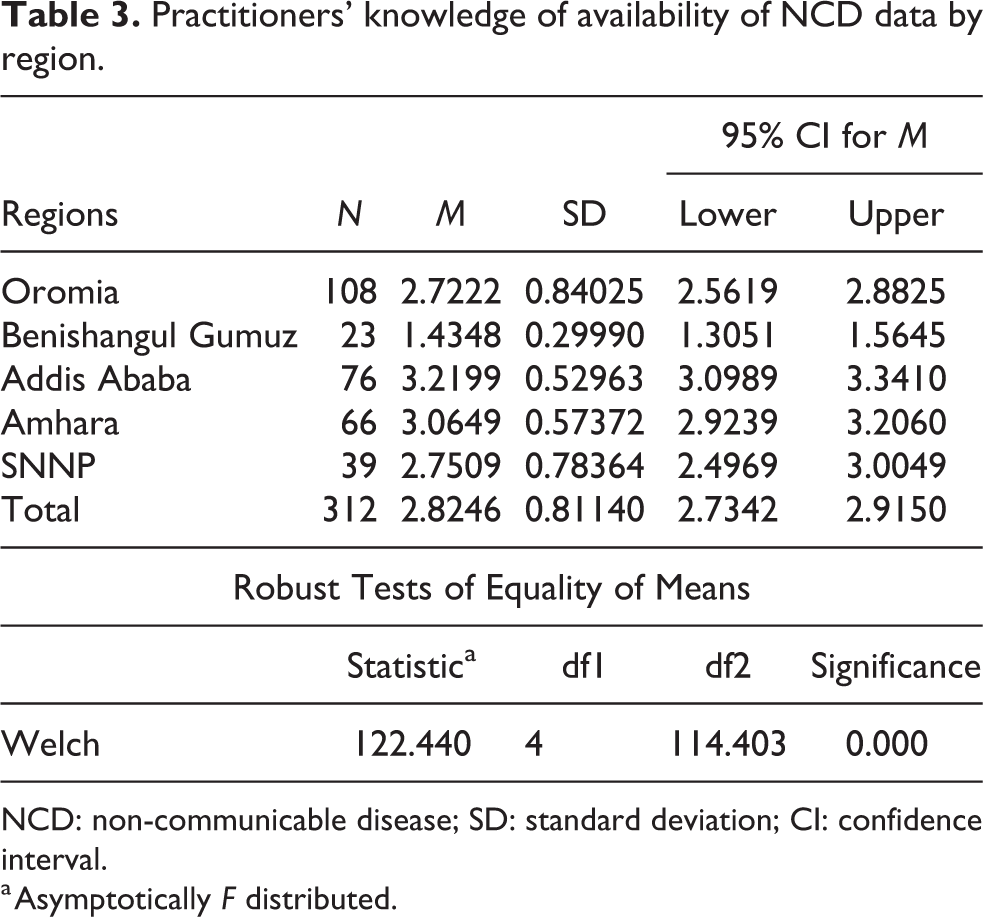
The regional comparison of the practitioners’ knowledge of the availability of NCD data (Table 3) using the one-way ANOVA average score showed statistically significant differences across regions, Welch (df1 = 4; df2 = 114.403) = 122.440, p < 0.0005, illustrating that not all regions had comparable regular score.
Practitioners’ knowledge of availability of NCD data by region.
NCD: non-communicable disease; SD: standard deviation; CI: confidence interval.
a Asymptotically F distributed.
Results of the Robust Tests of Equality of Means (Table 3) revealed that Addis Ababa (M = 3.22, SD = 0.53) and Amhara region (M = 3.06, SD = 0.57) had a significantly higher average score on the measure of the knowledge of the practitioners on the availability of NCD data compared to SNNP (M = 2.75, SD = 0.78), Oromia (M = 2.72, SD = 0.84) and Benishangul Gumuz regions (M = 1.43, SD = 0.29). Higher and lower average scores on the measure of practitioners’ knowledge of availability of NCD data are reported in Addis Ababa (M = 3.22, SD = 0.53) and Benishangul Gumuz region (M = 1.43, SD = 0.29), respectively.
Established mechanisms to periodically evaluate NCD data quality, reliability and timeliness
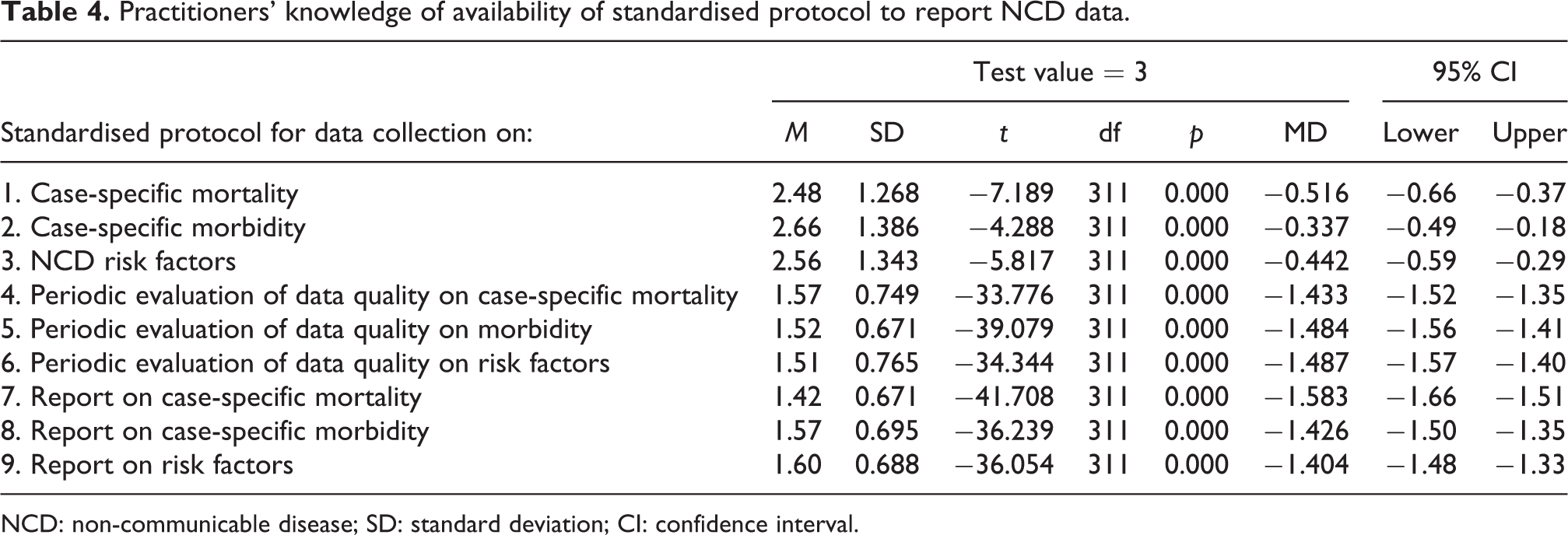
The presence of an established mechanism to periodically evaluate NCD data quality, reliability and timeliness is indicated in Table 4, with the following results below the mean value: case-specific mortality related to NCD (M = 1.57, SD = 0.749, t (311) = −33.776, p < 0.001), morbidity related to NCD (M = 1.52, SD = 0.671, t (311) = −39.079, p < 0.001) and NCD risk factors (M = 1.51, SD = 0.765, t (311) = −34.344, p < 0.001).
Practitioners’ knowledge of availability of standardised protocol to report NCD data.
NCD: non-communicable disease; SD: standard deviation; CI: confidence interval.
Availability of standardised protocols for NCD morbidity, mortality and risk factor data
The mean rating on the availability and use of a standardised protocol for NCD data collection in all 13 hospitals (Table 4) were significantly below the mean value across all the aspects, with the p values all being 0.000.
Regional comparisons of availability of standardised protocol used in hospitals for NCD data collection are depicted in Table 5, with the one-way ANOVA of regions average score indicating statistically significant differences across all the regions, Welch (df1 = 4; df2 = 126.312) = 115.615, p < 0.000. Robust Tests of Equality of Means demonstrated a relatively higher average score on the measure of availability of standardised protocol used for NCD data collection in Addis Ababa (M = 2.24, SD = 0.38) and lower average score in Benishangul Gumuz region (M = 1.19, SD = 0.13).
Practitioners’ knowledge of availability of standardised protocols for NCD data collection in hospitals by region.

NCD: non-communicable disease; SD: standard deviation; CI: confidence interval.
a Asymptotically F distributed.
Phase II
Results from the 13 interviews with physician hospital managers (2 questions) and the focus group with six Ministry of Health national health bureau officers (5 questions) are presented below under the interview and focus group questions with quotes reflecting responses. In addition, the records and HIS were examined at all 13 hospitals by checking the availability of NCD data that were further analysed. However, none of the hospitals provided adequate NCD data based on the examination.
Results from the interviews regarding perceptions of physician hospital managers regarding NCD data collection in the hospitals and the link between lack of NCD data and disease prevention
Question 1: What is the status of current NCD data in your hospital?
When asked about the status of NCD data in their hospital, the respondents indicated that the Ethiopian healthcare system was operating with limited resources and a small budget to meet the health demands of the public. Physician Hospital Manager 13 (PHM: 13) reported, “in my experience, most public hospitals lack well-trained professionals in the area of health information, networked health systems, standardised data collection protocols related to NCD morbidity, mortality and risk factors.” They indicated that the existing poor healthcare system, together with the lack of NCD policy, contributed to the lack of quality NCD data in the hospitals: In my view, there is no well-organised and recorded NCD related mortality, morbidity, and risk factor data in hospitals. I believe this may make decision-making and the delivery of healthcare difficult, as well as to predict the magnitude of NCD in the public (PHM: 5, as agreed to by PHM: 7, PHM: 9, and PHM: 10). Undoubtedly, the existing patient medical examination data registration forms in hospitals are mainly prepared for an infectious communicable disease. Despite the rising number of patients admitted due to NCD, the effort made to record NCD related morbidity, mortality and associated NCD risk factor data is poor in most hospitals (PHM: 1, as agreed to by PHM: 4, 6, 8, and PHM: 12).
They also referred to the current healthcare system as being poorly designed, and in the absence of a strong NCD policy, the availability of related morbidity, mortality and risk factor data had remained poor: I feel that the exclusion of NCD from the national demographic and health survey, and the lack of follow-up on the morbidity and death registration in the healthcare system, are the main reasons for the lack of NCD data in hospitals (PHM: 2, as agreed to by PHM: 3, 7, 11, and PHM: 12).
Question 2: How does the lack of data affect NCD prevention?
Participants indicated that there was an inverse relationship between the availability of NCD-related data and disease prevention, stating: “For me, where there is accurate and timely NCD related information, the healthcare system can make the appropriate decision and provide effective healthcare on time” (PHM: 1, as agreed to by PHM: 2-9). They indicated that having reliable NCD data was important for healthcare providers and organisations, policymakers, the community and even individuals. “If you think, quality health data is the source where the public, healthcare providers, healthcare organisations and donors can get sufficient amount of information related to NCD risk factors, prevalence, and mortality for decision-making” (PHM: 5, as agreed to by PHM: 10-13). The participants underlined quality health data as the building block of the healthcare system and stated that most hospitals in Ethiopia lacked an NCD data hub due to the existing weak HIS. “I think there is not a good enough system that coordinates hospitals with regional and national health centres to record, interpret and broadcast NCD mortality, morbidity and risk factors information to the public” (PHM: 3, as agreed to by PHM: 7, and PHM: 11).
Results from the focus group regarding Ministry of Health national health bureau officers regarding NCD data collection and the link between lack of NCD data and disease prevention
Question 1: How do you evaluate the availability of NCD-related data in the current Ethiopian healthcare system?
The discussants stated that the existing healthcare system was poorly organised and networked regarding both human and material resources, which affected the availability of NCD data. “In my opinion, the data that must provide effective healthcare delivery is lacking in the healthcare system due to a lack of networked health systems,” according to the FGD with participant 1 (FGD: P1). They also agreed that the NCD prevention demanded information that could only be obtained if the patient, the healthcare provider and the leading organisations functioned cohesively. “Honestly speaking, the availability of accurate data is lacking on NCD mortality, morbidity, and risk factors. The existing reports on NCD are made based on non-factual data, from WHO national estimations of disease and surveillance” (FGD: P2).
The focus group (FG) participants agreed to the introduction of a computerised patient medical history recording system in the Addis Ababa hospitals that was mainly designed for communicable disease-related data collection and recording, not for NCD. “For me, poor NCD data is only available at a local and regional level so that it is difficult to indicate the exact epidemiologic transition of disease at a national level, and NCD remain untreated,” according to the focus group discussion (FGD: P3, as agreed to by P4-P6).
Question 2: What should be done to secure quality NCD-related data?
Participants agreed that quality NCD data are associated with a strong healthcare system and the availability of human, financial and material resources, and its ongoing monitoring and evaluation. “In my opinion, political commitment, sufficient financial resources, trained healthcare workers, and cooperation amongst workers are required to effectively extract quality NCD related data” (FGD: P4). They indicated that quality data on NCD can be accessed through policy revision and joint working with donors, healthcare providers, policymakers and politicians. “For me, it is clear that NCD prevention strategic plans are required and the healthcare system should be equipped with health information and human resources” (FGD: P1). The participants also noted that as a member of the World Health Organization, the Ethiopian Ministry of Health must conduct population-based national NCD surveys to determine the prevalence of NCD and related risk factors. “Population based-national surveys, standardised protocols for NCD data collection, and a death registrar is required in the healthcare system” (FGD: P2, as agreed to by P5 and P6).
Question 3: How do you associate the lack of NCD-related data with its prevention?
The perception of participants was that NCD disease prevention and related information were two sides of the same coin, with data being the source of information for the healthcare system. “It is obvious that the healthcare system, with better data and information, can function optimally in decision-making and disease prevention than healthcare systems with inadequate data” (FGD: P2, P5 and P6).
Question 4: Do you have a NCD prevention policy in the current healthcare system?
According to the FG participants, the existing healthcare policy targeted infectious communicable diseases, such as HIV/AIDS, malaria, tuberculosis and reproductive issues such as contraceptive issues, child and maternal mortality. NCDs were not addressed in the current healthcare policy, with only road traffic accidents being included under this category. “Major NCD, like cardiovascular disease, diabetes, hypertension, respiratory disease, and cancer, are marginalised. However, tobacco preventive strategic plan was designed in 2015 but not yet implemented” (FGD: P1, as agreed to by P2-P5).
Question 5: What is your opinion on the effect of lack of policy on NCD prevention?
The discussants indicated the necessity of an all-encompassing and flexible national health policy, with the lack of an NCD preventive strategy resulting in many such conditions remaining undetected and inadequately managed: “I can say that the lack NCD preventive strategies in the national healthcare policy make public health remain under the burden of disease” (FGD: P3); and “I believe that a NCD preventive strategy is required and will soon be included in the national healthcare system” (FGD: P6).
Discussion
The results of our study showed a lack of mortality, morbidity, NCD risk factor and case-specific morbidity-related NCD data to be reported and recorded in the Ethiopian hospitals. Even though these results are consistent with previous studies in low- and middle-income countries (Chipps and Uys, 2014; Mareike et al., 2015), they differ from a study in Rwanda, which described a complete availability of an NCD data health report (Nisingizwe et al., 2014). The total absence of a report on mortality, morbidity and NCD risk factor data in the Ethiopian healthcare system can be attributed to the lack of standardised protocols for data collection, poor level of HIS utilisation, lack of a functioning HIS and lack of a NCD prevention policy and strategy in Ethiopia.
Our study revealed that NCD mortality data and NCD risk factor data are lacking in hospitals, which corroborates previous results that reported on the lack of mortality and risk factor data on NCD in developing countries (Naghavi et al., 2015). However, in their research, Naghavi et al. did indicate the presence of age-, sex- and case-specific deaths related to NCD in the health reports of developing countries. The difference in the findings by Naghavi et al. and the present study can be attributed to the absence of a death registration system, the scarce technical capacity to conduct NCD surveillances and poor networking in the Ethiopian healthcare system. In accordance with our study, Krishna (2016) found a lack of morbidity information, absence of a death registrar, inadequate NCD data collection processes, analyses and dissemination of NCD data. These factors, combined with the absence of an available platform to interpret the data, are possible reasons for the lack of NCD mortality and risk factor data in the healthcare systems of developing countries. However, our investigation indicated the availability of case-specific mortality-related NCD data in the Ethiopian hospitals. This could be attributed to the fact that road traffic accidents and related deaths have been recognised and regarded as NCD in the Ethiopian health policy, which is a significant limitation to the usefulness of such data. Studies in the SNNP region (Abegaz et al., 2014) and Addis Ababa (Hailemichael et al., 2015) confirmed that road traffic accidents were registered and reported as NCD in Ethiopian hospitals.
The results of our study exemplified differences across regions regarding the availability of more NCD data in Addis Ababa than in Oromia, Benishangul Gumuz and SNNP regions. The justification for the regional differences in the knowledge of practitioners on the availability of NCD data could be attributed to the special attention given by the Ethiopian Government to health investment, including healthcare services and facilities, in Addis Ababa as it is the capital city of the country and the headquarters of the African Union. Other possible reasons for the differences in the practitioners’ knowledge of availability of NCD data across regions could be the lack of skilled health information experts, inadequate and poor accessibility of computers and the Internet, lack of data, a poor HIS, inadequate resource allocation and the lack of accountability in other regions compared to Addis Ababa. The findings of our study also showed that the practitioners’ knowledge on the availability of NCD data in the Amhara region was more comprehensive as compared to the Oromia, Benishangul Gumuz and SNNP regions. The observed difference in the knowledge of practitioners on the availability of NCD data could be attributed to the regional variation in trained and qualified healthcare workers, inequitable distribution of facilities and the attention given to NCD and health information by the regional health bureau. Other possible reasons for the regional variation of NCD data could be attributed to the differences in the developmental status of the region, or the proximity of the regions to the capital city of Addis Ababa, as the regions nearer to Addis Ababa have greater access to adequate human and material resources than do the emerging and remote regions such as Benishabgul Gumuz. A study by Mousavi et al. (2016) in Iran illustrated the existence of disparities among its counties regarding health indicator data. Thus, the findings of our study are in line with the results of researchers in North African countries (Boutayeb and Helmert, 2011), in Tunisia (Ben Romdhane et al., 2014) and in Iran (Mousavi et al., 2016).
The results of our study also showed the lack of standardised protocols for data collection on NCD case-specific mortality, NCD case-specific morbidity and NCD risk factors in Ethiopian hospitals. The apparent lack of a standardised protocol for NCD data collection in Ethiopia can be ascribed to the low emphasis given to the prevention of NCD, lack of NCD policies and the over-attention given to infectious communicable disease. Another possible reason for the lack of a standardised protocol for NCD data collection could be attributed to inadequate numbers of trained and qualified human resources, the absence of processes, and of a networked computerised system in the Ethiopian healthcare system. A study in Benin confirms an association between poor data quality and the availability of resources in the healthcare system (Glele Ahanhanzo et al., 2014). This may result in a skewed presentation of the actual figure and burden of NCD, forcing healthcare organisations to use estimations for decision-making. The findings of our study also indicated the lack of periodic evaluation of data quality on case-specific NCD mortality, NCD morbidity and NCD risk factors. This substantiates previous findings (Krishna, 2016; Ndabarora et al., 2013) which reported the lack of periodic evaluation of health data in low- and middle-income countries. However, the finding of our study contrasts with a study by Nisingizwe et al. (2014) in Rwanda which reported the presence of follow-up and periodic evaluation of health data. A poor healthcare system, the absence of a HIS and NCD surveillance system are possible reasons for the different findings in our study compared to the study in Rwanda on the apparent lack of periodic evaluation of data quality on case-specific mortality, morbidity and NCD risk factors in Ethiopia.
Our study revealed a regional discrepancy in the availability of standardised protocols for NCD data collection with a standardised protocol relatively available in Addis Ababa and SNNP regions that were not available in Amhara, Benishangul Gumuz and Oromia regions. The revealed differences among regions can be accounted for in part by the variance in the unequal distribution of assets, healthcare professionals, healthcare finance and the attention given to the prevention of NCD. This confirms that Addis Ababa has more likely given attention to NCD prevention and treatment than other regions. The observed differences among the regions could be ascribed to the capacity of the regional health bureau in planning, and implementing regional-based standardised NCD data collection processes. Another possible reason could be attributed to the escalating inequality of healthcare among the regions as well as the increasing social inequalities among the regions. A study by Boutayeb and Helmert (2011) indicted an uneven distribution of human, material and economic resources for healthcare resulting in social inequalities, regional disparities and health inequality in North African countries.
Conclusion
In this study, we assessed the knowledge of practitioners on the availability of NCD information and standardised protocols for data collection in the Ethiopian public referral hospitals and its regional variations. Identifying the status of the existing NCD-related data assists effective service delivery, evidence-based decision-making and assessment of the operating healthcare system to sustain a high quality of healthcare. Our study highlighted the lack of NCD-related data, lack of periodic and timely evaluation of NCD-related data as well as the lack of standardised protocols for NCD-related data collection in the Ethiopian public referral hospitals. The study also scrutinised the deviating discrepancies in NCD data and standardised protocols for NCD data collection among the different regions of Ethiopia. An important result from our study was participants’ perceived link between NCD data quality and NCD prevention. Our study showed that disease prevention policies and strategies can be better designed and targeted with accurate and timely information about NCDs. To ensure quality and timely NCD data for decision-making, leading healthcare organisations need to strengthen the existing HIS and should establish and implement NCD preventive strategic policies. Similarly, the healthcare system requires standardised protocols for NCD data collection, funding and human resources to conduct population-based NCD surveillance. The important deficiencies highlighted in this study indicate the need to strengthen both the healthcare system and HIS to facilitate evidence-based decision-making.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.