
Abstract
Background:
Health information technology (IT) solutions can aid healthcare reform efforts, but without proper information management, these efforts are futile. In this study, we used Kuwait as an example of a high per-capita gross domestic product country that faces information management challenges to draw insights that can be generalised to other developed countries.
Objective:
(i) to uncover the status quo of information management practices in public hospitals and (ii) to offer recommendations to improve them.
Method:
This study analysed qualitative and quantitative accreditation-related data pertaining to the compliance with the information management standard at all secondary care public hospitals over two accreditation cycles.
Results:
Overall, public hospitals had made positive progress in their compliance with the information management standard. However, issues still existed with (i) developing and implementing an information management plan, (ii) involving the appropriate stakeholders in selecting health IT solutions and (iii) access to the Internet by staff and patients.
Conclusion:
Evidence underscored the importance of proper information management driven by clear centralised strategic plans.
Implications:
With the rapid adoption of digital health systems, the role of health information management leaders should not be undervalued. Embracing health IT solutions with strong information management practices can aid healthcare reform efforts.
Keywords
Introduction
Healthcare systems around the globe face grand challenges that hinder their efforts to deliver care services effectively and efficiently while improving the health of the population (Vos et al., 2017). Globally, the toll of chronic non-communicable diseases (e.g. diabetes and hypertension) has become virtually insupportable, and the proliferation of these diseases among the growing populations threatens the economies of many countries (Arredondo and Aviles, 2015). Even in developed countries with universal health coverage, an affluent population and a high per-capita gross domestic product, these challenges persist (Tordrup et al., 2013). Similar to many developed countries, the demand for healthcare services in the oil-rich State of Kuwait has been on the rise as its population continues to grow older and live longer (Gulseven, 2016; Younis et al., 2015). Additionally, the dramatic changes in the population’s socio-economic status in the post-oil era have promoted a sedentary lifestyle and a high-calorie diet (Al-Haifi et al., 2013; Allafi et al., 2014). Such lifestyle promotes the wide spread of non-communicable diseases such as diabetes (Awad and Alsaleh, 2015; Shaltout et al., 2017), hypertension (Channanath et al., 2013, 2015) and cardiovascular diseases (Alarouj et al., 2013), which are creating huge financial costs and more importantly, the lives of many people (Mokdad et al., 2014).
In light of these challenges, the status quo of universal access to healthcare cannot be sustained. Hence, healthcare reform efforts have become a top priority for healthcare system leaders globally, including resource-rich countries (Behbehani, 2014; Conway et al., 2014). Better quality of care, improved health outcomes and reduced costs are important targets for all healthcare reform efforts (Berwick et al., 2008). To achieve these targets, the successful and effective adoption of health information technology (IT) solutions, such as electronic health records (EHRs), by healthcare institutions becomes paramount (Buntin et al., 2010; Koru et al., 2016). These solutions can enable the healthcare organisation to better manage the information and improve care coordination among healthcare providers (Williams et al., 2017). Additionally, health IT solutions can collect and monitor dynamic quality measures over time (Buntin et al., 2010) as well as eliminate duplication and waste in healthcare by making the results of prior diagnostic tests and interventions available at all points of care (Koppel et al., 2005).
Unfortunately, recent evidence highlights limitations and quality issues related to data associated with these solutions such as incomplete records (Wright et al., 2015) or miscoded data (de Lusignan et al., 2010). Merely having an electronic record for a patient does not mean that the information in that record is sufficient for safe and effective healthcare practice (Weiskopf et al., 2013). Therefore, the adequate management and governance of health information is a necessary precursor to the effectiveness of health IT solutions. Ineffective information management will not aide healthcare reform efforts but rather create additional problems, increase hazards and introduce additional barriers to realising the benefits of healthcare reform (Zeng et al., 2009).
Background
The healthcare system in the State of Kuwait offers universal access to healthcare services with 70% of healthcare services being provisioned by the public or government sector represented by the Ministry of Health (MoH, 2015). This public healthcare system is distributed across Kuwait’s six governorates and is organised into three levels: primary, secondary and tertiary. The primary healthcare centres, conveniently located in the residential areas across the country, provide the first line of primary care services and the entry point into the healthcare system. Secondary care is provided through six general hospitals, while tertiary care is provided via specialised and diseases-focused hospitals and centres (Regional Health Systems Observatory – EMRO, 2006). The workforce, clinicians and administrators working in this system are multinational and come from diverse educational and cultural backgrounds (Katoue and Ker, 2018).
To better manage health information, Kuwait has made a significant investment in digital health infrastructure since 2000 (Weber et al., 2017). A variety of health IT solutions have been implemented at MoH facilities (Alhuwail and Barnes, 2011), including EHRs at primary healthcare centres (Al-Azmi et al., 2006; Al-Jafar, 2013) and hospitals (Alquraini et al., 2007), as well as picture archiving and communication systems (Buabbas et al., 2016). However, the maturity and adoption levels of these solutions vary greatly among healthcare facilities, and to our knowledge, no formal evaluation has been performed to assess them. The higher education institutions in Kuwait, namely Kuwait University and the Public Authority for Applied Education and Training, train health information management professionals who will work in the medical records departments at the healthcare institutions. However, the remaining health and allied health professionals receive minimal information management training throughout their academic curriculum.
An important aspect of moving health IT and health information management towards having a more influential role in health delivery is reaching certain maturity milestones established by globally recognised standards. The National Accreditation Program for Hospitals (NAPH) in Kuwait, established by the Quality and Accreditation Directorate (QAD) at MoH, provides the means to facilitate improvements in health information management. The NAPH is concerned with improving care quality and enhancing patient safety through creating, implementing, monitoring and evaluating programs and standards of quality and safety across all sectors of the MoH.
The NAPH was established in 2008 and originated from Accreditation Canada’s Client Centred Accreditation Program (Ladha-Waljee et al., 2014). The program is tailored to make it appropriate and applicable to the context of Kuwait’s healthcare system and the nature of care services provisioned by MoH hospitals. The program provides a process for hospitals to assess, monitor and improve their performance on an ongoing basis. The program is composed of 12 standards that cover a wide range of important areas and services, such as human resources, clinical services and information management. Currently, there are debates in the literature about the value of accreditation and whether it is worth the time and money. Yet, many healthcare organisations and systems around the world are engaged in accreditation activities (Lam et al., 2018; Mumford et al., 2013). However, there is still no definitive evidence suggesting that accreditation is fruitless (Algahtani et al., 2017).
The current research
To date, little is known about the pressing challenges, gaps and opportunities concerning information management practices in Kuwait’s healthcare institutions. The aim of this empirical research was to (i) discover the status quo of information management practices in public hospitals and (ii) offer recommendations to improve these practices. The evidence from this research will inform several key stakeholders such as hospital administrators, health information management professionals, informaticians, governments and policymakers. We focused on the benefits of compliance with the standards as a result of engaging in accreditation activities and not necessarily the benefits or value of accreditation. We acknowledge that while compliance with accreditation standards does not guarantee the attainment of superior quality, it establishes a baseline of minimum expectations that are required.
Method
Research design and data sources
The convergent-design mixed methods approach was used to gain a comprehensive, context-specific and rich understanding of the research topic (Guetterman et al., 2015). This approach allows for an integrative collection and analysis of both quantitative and qualitative data at similar times (Bazeley, 2012). Prior to data collection, the required ethical approvals were granted from the ethical review board at MoH. This study analysed accreditation-related data from hospitals providing secondary care services, specifically, anonymous data collected by QAD at MoH pertaining to the compliance with the information management standard at each hospital (refer to the Online Appendix for detailed information about the standard and its related criteria). The dataset contained numerical self-assessment scores and surveyors’ scores in addition to the surveyors’ comments over nine criteria, as illustrated in Box 1. Overall, the dataset covered two accreditation cycles with cycle 1 taking place in 2012–2013 and cycle 2 in 2016–2017. 1 The indicators of performance for safety, designated as criterion 10 (10.0–10.2), were not included because they were only introduced in the second accreditation cycle; therefore, comparative analysis could not be performed.
Criteria of the information management standard considered in this study.

aDescriptions are extracted from the information management standard. Refer to the Online Appendix.
Accreditation process
Initially, the organisations began by completing a self-assessment survey evaluating their compliance with the set forth national standards on a predetermined five-point scale ranging from “no compliance” to “substantial compliance.” This was followed by an on-site survey conducted by an expert team of healthcare professionals or surveyors. The surveyors were MoH healthcare providers trained on the accreditation-related assessments and evaluations. The on-site surveys validated the hospitals’ self-assessment scores and served as a means of external peer review and validation. The surveyors’ visits entailed team interviews, touring the hospital, reviewing all relevant documentation, facilitating various focus group interviews and finally completing the survey report. After the survey, the organisations received a report highlighting the results of the survey, the hospital’s strengths, recommendations for improvement and an accreditation decision. Organisations were encouraged to follow up on the recommendations from the report and continue to make ongoing improvements to their services.
Participants
All public hospitals providing secondary care services were included in the study (N = 6). For this reason, the hospitals have not been identified by name to protect their anonymity. For comparative purposes, a compound measure was developed to classify hospitals by size. This measure considered the number of beds and outpatient visits. The hospitals were ranked as small (n = 2), medium (n = 2) and large (n = 2); Small hospitals had less than 400 beds and reported less than 150,000 outpatient visits, whereas large hospitals had 800+ beds and reported 250,000+ outpatient visits.
Data analysis
A basic descriptive analysis was performed on the numerical surveyor-reported scores. Across the two accreditation cycles and for each criterion along with its sub-parts, the differences in surveyors’ scores were calculated. The surveyor scores were considered for calculations because these scores represented an evaluation by external experts and were based on evidence supplied by the hospital. Investigating the surveyor team scores was more reliable since scores were evidence-based. The qualitative data formed by the surveyors’ comments were used to support the evidence and justify the results. The framework method (Gale et al., 2013) was used to analyse the qualitative data. The analysis was iterative, and the data were sorted, summarised and synthesised into key themes according to the information management criteria.
Results
Information management practices
For an overview of hospitals’ performance in each criterion of the information management standard spanning the two accreditation cycles, refer to Table 1. To protect the anonymity of hospitals, the size information cannot be disclosed. Interestingly, the results indicated no meaningful patterns related to the hospital’s size or even the scope of services it provided. Overall, results showed that public hospitals in Kuwait had made positive progress in their information management practices over the span of accreditation cycles. Notably, criterion 1.00, 3.00, and 8.00 remained below partial compliance over the two accreditation cycles. These three criteria referred to establishing and implementing an information management plan, instituting policies for data privacy and security and Internet accessibility for staff. With respect to contributing data to external databases in accordance with laws or regulations, the majority of hospitals did exceptionally well and had either maintained their high level of compliance or improved on it; only H62 remained partially compliant. To illustrate the magnitude of change across the two cycles for each hospital, refer to Figure 1.
Rate of compliance with information management criteria for each hospital between accreditation cycles.
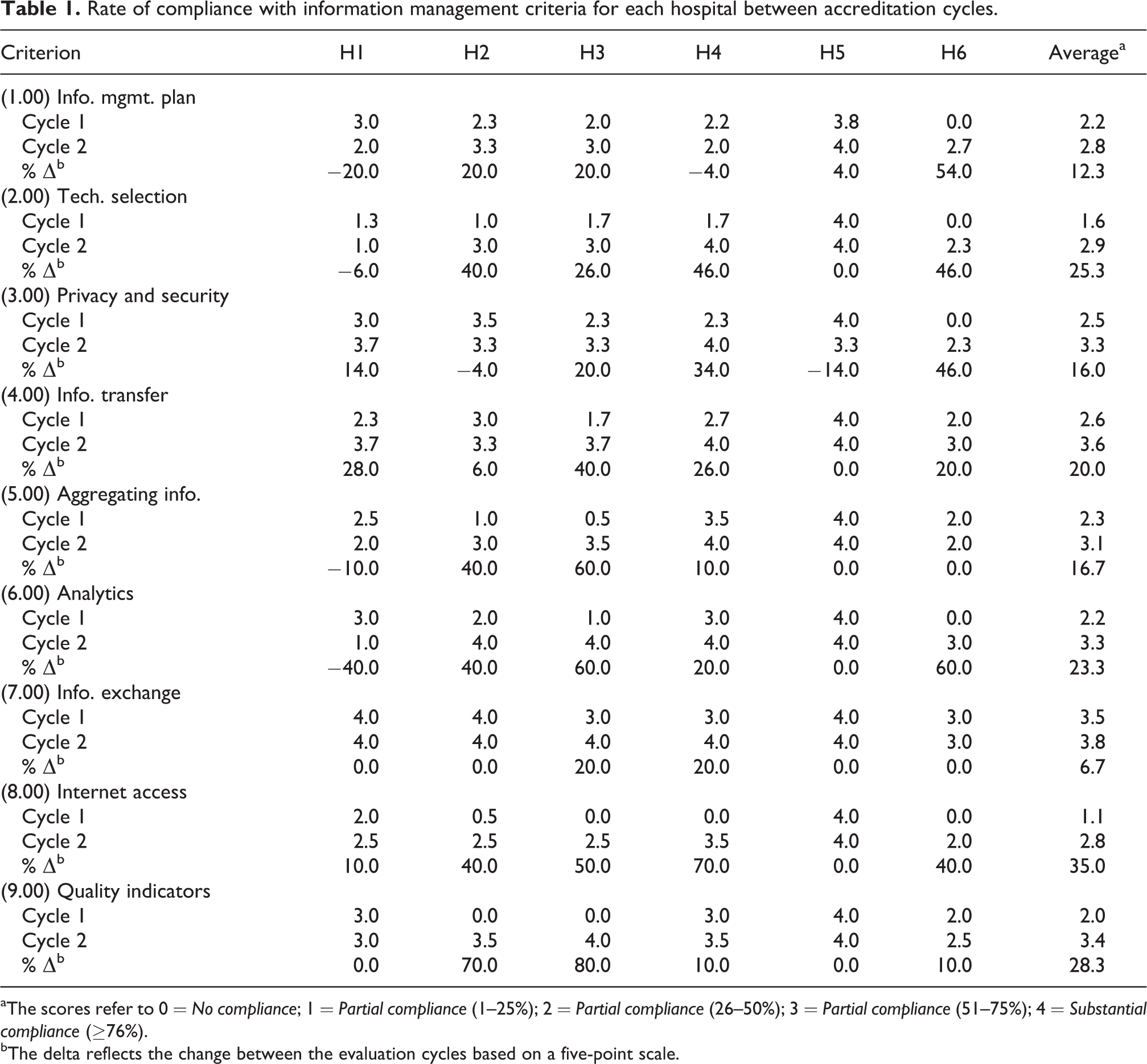
aThe scores refer to 0 = No compliance; 1 = Partial compliance (1–25%); 2 = Partial compliance (26–50%); 3 = Partial compliance (51–75%); 4 = Substantial compliance (≥76%).
bThe delta reflects the change between the evaluation cycles based on a five-point scale.
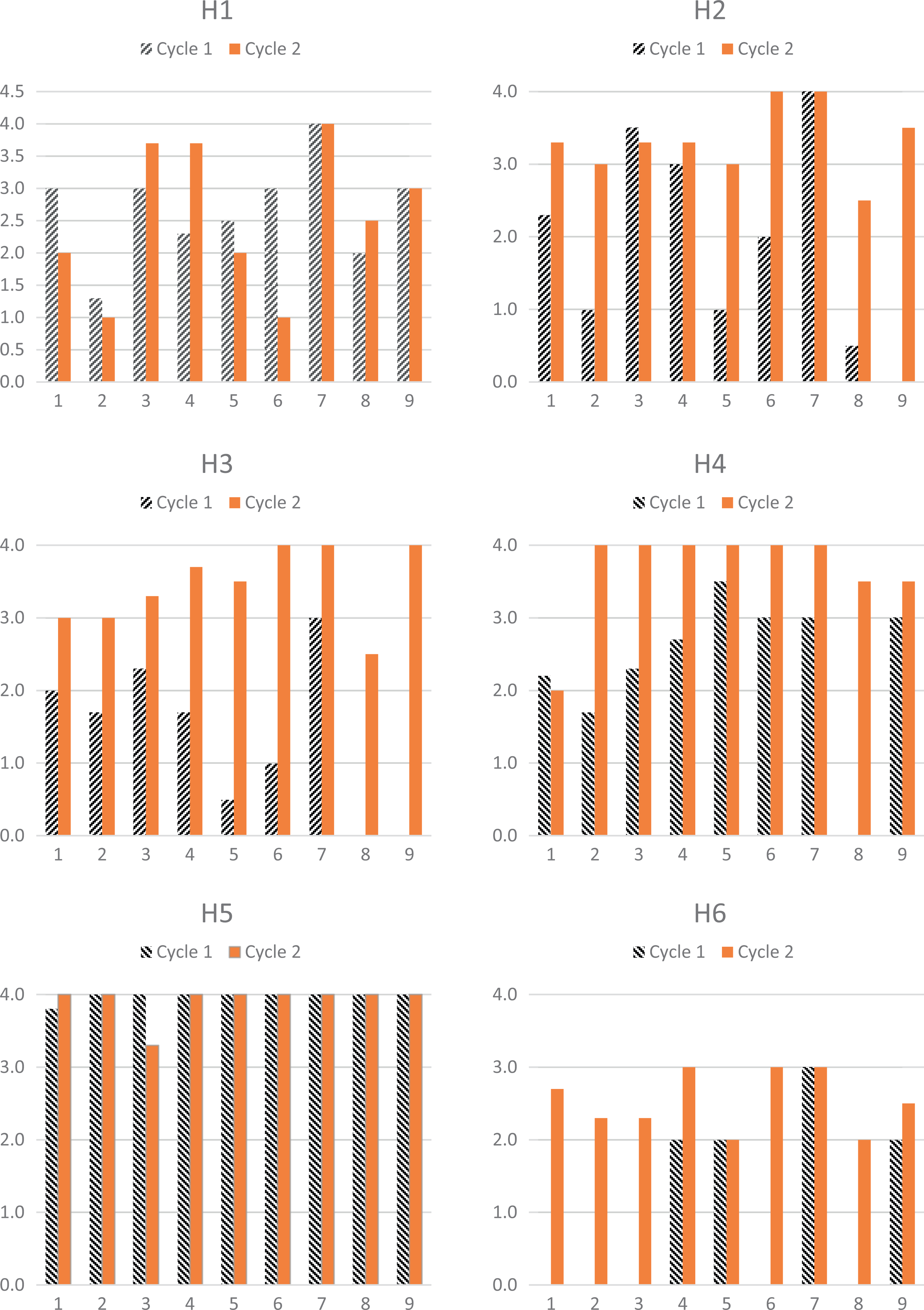
Column chart for each hospital with respect to its progress in attaining the criteria in the information management standard across the two accreditation cycles.
Review of findings related to each criterion across hospitals
Information management plan
The majority of hospitals struggled to develop and implement an information management plan to meet their information needs. H1 and H4 had a deteriorating rate of improvement in complying with this criterion. Only H5 had substantial compliance in this regard. One issue was the need to engage all the relevant departments in developing this plan. One survey team suggested that the “information management plan needs to be developed in collaboration with other clinical and professional departments” – (s4). 3 There was also a need to “integrate the information management with clinical and administrative services” – (s2). Another survey team noted that “comprehensive plans, policies and protocols need to be written down, and communicated to staff and later monitored” – (s3). The data also indicated that some hospitals needed to improve and increase the availability of training about information management to all staff members, both clinical and non-clinical staff; “The team is encouraged to develop comprehensive schedule for education and training in information management” – (s6).
Technology selection
Only two hospitals, H4 and H5, achieved full compliance in this criterion by involving the appropriate clinical, managerial and IT staff in the selection and integration of health IT systems for the hospital. The remaining hospitals showed partial improvements in compliance with this criterion, apart from H1, which regressed. The survey teams were encouraged to “involve the departments appropriately in the selection of information technology” – (s2).
Data privacy and security
The majority of hospitals had good levels of compliance in protecting the privacy and security of the information. Only H6 remained at a medium compliance with this criterion. Interestingly, H2 and H5 showed declining rates of compliance in this matter. Some of the issues noted by the survey team included the lack of policies that restrict unauthorised access to patients’ records; “Develop and implement a policy to ensure a restricted access for authorized staff to medical records” – (s6). Additionally, the data about some hospitals indicated the absence of a backup system for patient records, whether paper or electronic. The survey teams suggested the “establishment of a back-up data system” – (s2). Surveyors also advised that clients’ trust in the hospital’s ability to protect information was critical; “To gain the trust of the hospital client, hospital should improve medical record management.” – (s4).
Information transfer
On this criterion, all hospitals improved their processes related to transmitting data effectively and efficiently. Only H3, H4 and H5 had functioning EHRs, and hence their high levels of compliance with this criterion were noted by the surveyors. The lack of electronic systems such as EHRs, laboratory information systems and radiology information systems contributed to lower levels of efficiency and sometimes ineffective information transfers; “Lack of the electronic medical file system or Hospital Information System is a challenge to share information” – (s6).
Aggregating information
Three hospitals showed improvements in compliance with this criterion, which in turn was concerned with aggregating information and data to support patient care, administrative decision making and quality improvement initiatives. Only H5 remained substantially compliant while H1 showed a decline in compliance, and H6 showed no improvement and remained partially complaint. This was largely attributed to the lack of electronic informatics solutions; “No comprehensive computerized hospital wide system yet” – (s2). Survey teams suggest that “electronic data management need to be implemented to improve acquisition of data” – (s4)
Analytics for decision-making
For this criterion, nearly all hospitals improved their compliance attainment. However, for H1, the level of compliance decreased (from up to 75% to up to 25%). One survey team indicated that the “data collected is not fully utilized towards generating more reports to improve decision-making by administration” – (s3).
Information exchange
All hospitals showed improvement with respect to contributing data and information to serve the various statistical reports generated by MoH as well as external databases in accordance with laws or regulations. Only H6 remained in medium compliance with this criterion. One survey team suggested that an integrated informatics solution across the hospital could “help improve efficiency and communication” – (s5).
Access to internet
All hospitals indicated improvements with providing access for staff to obtain information that could support safe patient care. Only H5 was substantially complaint with this criterion. The remaining hospitals reported minor to medium compliance. One survey team indicated issues with monitoring and enforcing appropriate use policies for the Internet; “We recommend compliance and monitoring Internet use policy” – (s1). Another team suggested that access to the Internet should be also made available to patients; “To provide Internet to staff and clients” – (s1).
Quality performance indicators
Evidence suggested that all hospitals identified the required indicators of performance for quality in their information management efforts and monitored them as part of their quality improvement activities. Only H3 and H5 were substantially compliant, while H6 remained in minor compliance with the criterion.
Other issues
Survey teams reported several other challenges that were relevant to information management. The diversity of the languages spoken by the hospital’s staff could be a barrier to the effective implementation of information management; “Challenges: There are language barriers, especially for information management, human resources pose challenges” – (s6). The evidence also suggested misalignment between strategic and operational plans, which in turn could negatively impact information management; “Area for Improvement: The linkage between strategic and operational plans among the senior leaders and staff” – (s3).
Discussion
The results from this study indicated an overall positive improvement in compliance with the information management standard by hospitals providing secondary care services. This improvement could have been the result of becoming more aware of the standard and the attempts by hospitals to attain higher levels of compliance (Devkaran and O’Farrell, 2014).
The effectiveness of information management practices is dependent on formulating, communicating and adhering to a clear strategic plan. Evidence from this study suggests that hospitals without clear or comprehensive information management plans that were inclusive of all the stakeholders were not able to attain the desired levels of compliance with the information management standard. This demonstrates the importance of having a comprehensive information management plan that aligns with existing national strategies.
Currently in Kuwaiti public hospitals, there is no designated leadership position responsible for information management practices across the hospital. While the information systems and technology vendors or departments at hospitals often assume this function, they remain mainly focused on supporting the technology infrastructure. In turn, this creates a huge gap in supporting safe patient-centred care via good health information management (Snyder et al., 2011).
Additionally, the results of this study indicate that some hospitals need to improve the availability and accessibility of information management training to all staff members. Without properly investing in training the staff on the important aspects of information management practices as well as the proper use of technology tools and systems, hospitals will not reap the benefits and their information management efforts will likely be wasted or at best underutilised (McAlearney et al., 2012). Ongoing professional training and mentorship should also be available to the professionals working in the medical records department (Bates et al., 2014).
Preserving the security and confidentiality of data and information is a primary concern for hospitals globally. With rising rates of adopting health informatics solutions, cybersecurity has been a major topic of interest (Kuo et al., 2014; Perakslis, 2014). While the evidence indicated that hospitals had improved their security practices, it is nevertheless concerning that some hospitals were still facing issues with unauthorised access to patients’ physical records. Adopting EHRs with the appropriate privacy and security mechanisms in place would be an effective solution (Fernández-Alemán et al., 2013).
As highlighted from the surveyors’ comments, organisations that adopted and deployed integrated informatics solutions, such as EHRs, had better scores compared with their peers who did not. However, the current levels of adoption and maturity of health informatics solutions in Kuwait are limited (Weber et al., 2017). While some hospitals had some electronic solutions such as EHRs or laboratory information system, these solutions were operating in a silo and did not interface with other systems in or outside the hospital. Hospitals should adopt, implement and maintain integrated health informatics solutions to support the various functions within the hospital as well as outside of the hospital and across the nation.
Towards more digitally mature healthcare systems
With the rapid advances in the adoption of digital health tools and systems, it has become paramount that healthcare leaders develop and embrace a digitally enabled health informatics strategy. If not already in place, regulators should spearhead and develop a national strategic digital health and informatics plan that encompasses information management. Throughout its lifecycle, the plan should be inclusive of all relevant stakeholders, including patients and their advocates.
Additionally, healthcare institutions should be involved in continuous assessments to uncover their digital health maturity. These assessments would allow the institutions to discover their strengths, highlight areas for improvement and aid in prioritising issues or areas to focus on. The HIMSS EMRAM evaluation (Pettit, 2013) and the NHS Digital Maturity assessment (Johnston, 2017) are examples of such assessments that could be used.
Moreover, clinical informatics leadership roles (i.e. Chief Clinical Informatics Officer and Chief Nursing Informatics Officer) should be clearly defined and integrated into the organisational structure of the healthcare institution (Kannry et al., 2016). Academic institutions should also prepare to meet the demand for these roles and integrate health information management and informatics training into the academic curriculum for all health and allied-health disciplines (Cooper, 2009). This will help prepare the future workforce to work with digital health solutions and truly embrace the power that these solutions provide for enhancing healthcare delivery.
Strengths and limitations
The evidence uncovered in this study was captured by healthcare professionals with a wealth of experience working at MoH and was performed consistently over two cycles with several years between the cycles. The dataset was rich with both quantitative data (self-reported hospital score and surveyors’ score) and qualitative data (comments from survey teams). However, some interesting phenomena could not be further explored, such as reasons why a hospital did not comply with a specific criterion. Additionally, the dataset did not systematically evaluate the informatics infrastructure and setup at the time of the survey to better understand the information management context and the level of its automation. Rich feedback from the healthcare organisations and their views about information management challenges and opportunities can be valuable. Lastly, the results can be informative for policymakers and hospital administrators in Kuwait when evaluating their information management practices. Given the similarities between the healthcare system in Kuwait and many of the developed countries (e.g. many of the Economic Co-operation and Development (OECD) countries), the findings can potentially be applicable more broadly. However, careful consideration of the contextual determinants is required before assuming generalisability.
Conclusion
The socio-economic context and the challenges facing the healthcare system in the State of Kuwait, as well as many developed countries, necessitate careful consideration of information management practices in healthcare institutions. The evidence from this study illustrates that Kuwait’s public hospitals have been making positive progress overall in their compliance with information management standards as part of the NAPH. However, issues remain concerning the development and implementation of an information management plan as well as involving the appropriate stakeholders in selecting the appropriate health IT solutions for the hospital. The results also highlight the fact that the role of health information management in aiding healthcare reform efforts can no longer be postponed or ignored. Today, digital health solutions that are governed by strong health information management act as the circulatory system of the modern healthcare system, transporting the necessary information to the various parts of this system. When the arteries of this system are constricted or clogged with absent, fragmented, inefficient or isolated information management practices or systems, the consequences are dire! It is time to reform healthcare through strong information management governance powered by informatics.
Supplemental material
Supplemental Material, Appendix1InformationManagement - Understanding health information management practices in public hospitals in Kuwait
Supplemental Material, Appendix1InformationManagement for Understanding health information management practices in public hospitals in Kuwait by Dari Alhuwail in Health Information Management Journal
Footnotes
Acknowledgements
The author wishes to thank the Ministry of Health in Kuwait, especially the Quality and Accreditation Directorate, for their invaluable assistance on the project. The author also wishes to acknowledge the Kuwait Foundation for the Advancement of Sciences and the Kuwait Programme, Middle East Centre at the London School of Economics and Political Science for their in-kind support. The author would also like to thank Dr Yousef Abdulsalam for his valuable feedback and review of the manuscript prior to submission.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.