
Abstract
Background:
The All Patient-Refined Diagnosis-Related Groups (APR-DRGs) system has adjusted the basic DRG structure by incorporating four severity of illness (SOI) levels, which are used for determining hospital payment. A comprehensive report of all relevant diagnoses, namely the patient’s underlying co-morbidities, is a key factor for ensuring that SOI determination will be adequate.
Objective:
In this study, we aimed to characterise the individual impact of co-morbidities on APR-DRG classification and hospital funding in the context of respiratory and cardiovascular diseases.
Methods:
Using 6 years of coded clinical data from a nationwide Portuguese inpatient database and support vector machine (SVM) models, we simulated and explored the APR-DRG classification to understand its response to individual removal of Charlson and Elixhauser co-morbidities. We also estimated the amount of hospital payments that could have been lost when co-morbidities are under-reported.
Results:
In our scenario, most Charlson and Elixhauser co-morbidities did considerably influence SOI determination but had little impact on base APR-DRG assignment. The degree of influence of each co-morbidity on SOI was, however, quite specific to the base APR-DRG. Under-coding of all studied co-morbidities led to losses in hospital payments. Furthermore, our results based on the SVM models were consistent with overall APR-DRG grouping logics.
Conclusion and implications:
Comprehensive reporting of pre-existing or newly acquired co-morbidities should be encouraged in hospitals as they have an important influence on SOI assignment and thus on hospital funding. Furthermore, we recommend that future guidelines to be used by medical coders should include specific rules concerning coding of co-morbidities.
Keywords
Introduction
The quality of coded clinical data is a relevant issue in the context of healthcare management. The accuracy and completeness of reporting all additional diagnoses in a hospital stay is of most concern as appropriate and fair hospital funding may depend upon the reliability of grouping coded inpatient episodes into clinically homogeneous groups with similar resource use, the so-called Diagnosis-Related Groups (DRGs) (Cheng et al., 2009; Mathauer and Wittenbecher, 2013). The DRG classification was designed at the Yale University in the late 1960s (Busse et al., 2011) and was first used in 1983 as part of a prospective payment system for reimbursing Medicare patients (Langenbrunner et al., 1989). The original DRGs were redesigned afterwards, resulting in the creation of the Medicare Severity Diagnosis-Related Groups, which added three distinct complication levels (major complication and co-morbidities, complications and co-morbidities and no complications and co-morbidities) in order to obtain smaller and more clinically homogenous groups (Centers for Medicare and Medicaid Services (CMS), 2016). A new methodology of DRG stratification was later introduced with the All-Patient Refined Diagnosis-Related Groups (APR-DRGs) classification, which modified the basic DRG structure by including four levels of severity of illness (SOI) (Aiello and Roddy, 2017), which refers to the degree of loss of function or physiologic decompensation of an organ system, and risk of mortality (ROM), which reflects the likelihood of dying (Averill et al., 2013). Both SOI and ROM are characterised by a score ranging from 1 to 4 (1 – minor; 2 – moderate; 3 – major; 4 – extreme), representing increasing reimbursement demands. The APR-DRG classification is currently employed for reimbursement purposes in some European countries, such as Belgium, Spain, Portugal and Italy, some Arab countries and in over 30 states in the United States (Dewilde et al., 2018). Figure 1 shows the overall APR-DRG grouping logic.
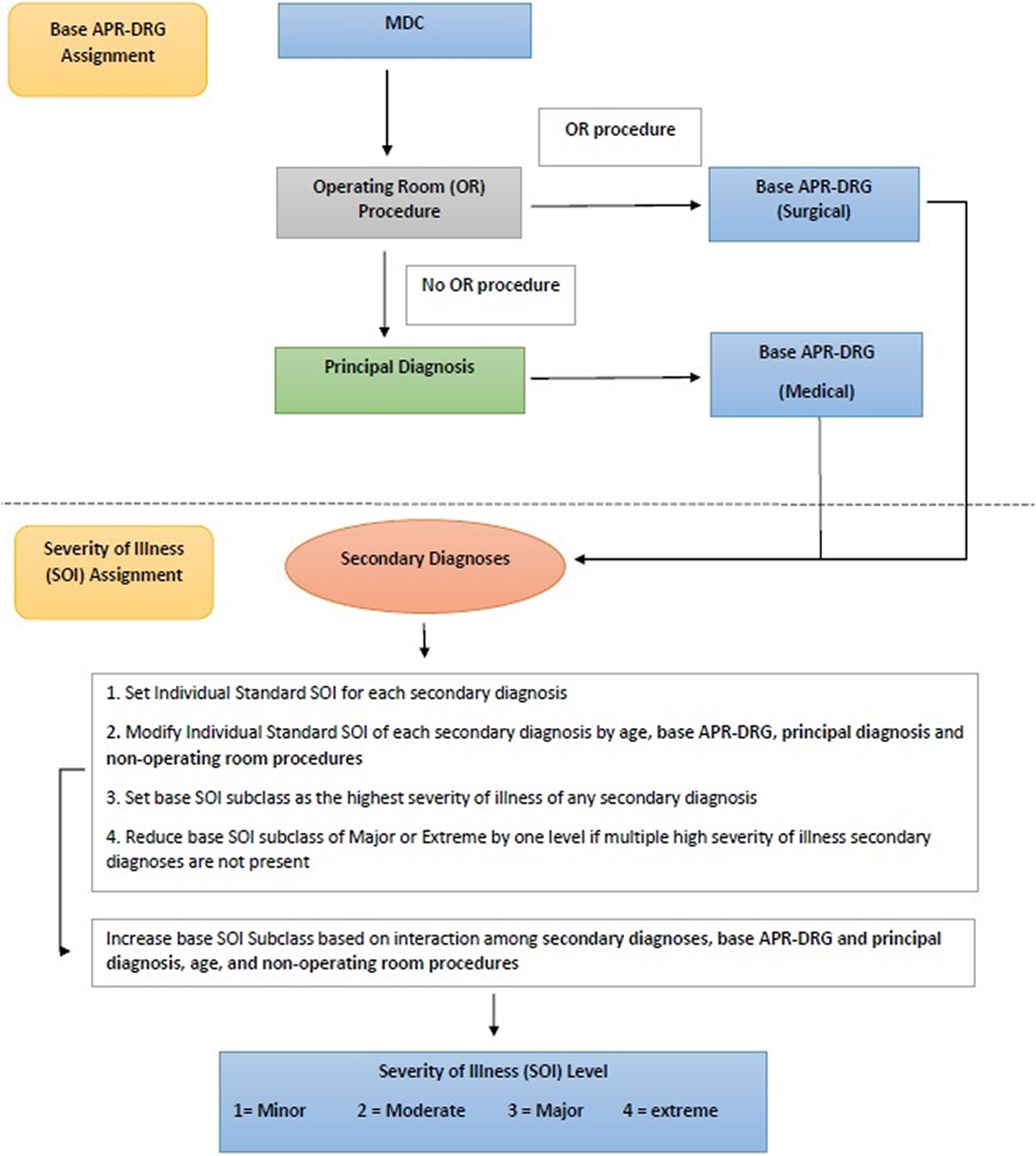
Overview of the APR-DRG grouping logic. APR-DRG: All Patient-Refined Diagnosis-Related Group.
In the APR-DRG classification, episodes within a given Major Diagnostic Category (MDC), which correspond to a specific diagnosis area, will be assigned to a disease- or procedure-specific base APR-DRG. Medical episodes will be grouped into a base APR-DRG mostly according to the principal diagnosis, whereas surgical episodes will be grouped according to an operating room procedure (Averill et al., 2013). The base APR-DRG is further stratified into SOI and ROM levels considering combinations of base APR-DRG, diagnoses, age and procedures (Averill et al., 2013). Despite the influence of nearly all patient features, secondary diagnoses representing co-morbidities and complications are what typically drive SOI and ROM levels (Aiello and Roddy, 2017). In fact, episodes with higher SOI levels usually present multiple co-morbidities affecting different organ systems (Averill et al., 2013). Thus, accurate and complete coding of co-morbidities is particularly important in APR-DRG classification as the patient’s SOI has a significant role in hospital payment (Spurgeon et al., 2011). For instance, in Portugal, a hospital that treats a patient assigned to APR-DRG 1944, which represents heart failure patients (base APR-DRG 194) with an extreme SOI, will be paid with an amount about five, three and two times higher than cases assigned to the same base APR-DRG with SOI levels 1, 2 and 3, respectively (Administração Central do Sistema de Saúde, 2017).
Due to their important role on determining patient outcomes, several methods have been developed to measure co-morbidities, with Charlson and Elixhauser scores being the two most commonly used (Chang et al., 2016; Li et al., 2008). The Charlson’s method was developed by reviewing inpatient hospital charts and assessing the relevance of several clinical conditions in the prediction of mortality and a total of 17 co-morbid categories were created. A weighted score was assigned to each of 17 co-morbidities and the Charlson index was developed as an indicator of disease burden. The Elixhauser investigated groups of ICD-9-CM diagnosis codes to identify categories of co-morbidities and further measured their association with mortality. The performance of the Charlson and Elixhauser measures in predicting poor outcomes has been evaluated and validated by several studies and are regarded as good predictors of patient outcomes (Li et al., 2008).
Despite their clinical significance, evidence elsewhere has shown that certain co-morbidities are generally under-reported in administrative databases (Austin et al., 2005), while the prevalence of others is overestimated when compared with the information of medical charts (Blumenthal, 1996; Chong et al., 2011; Hawker et al., 1997; Humphries et al., 2000; Iezzoni et al., 1992; Kieszak et al., 1999; Malenka et al., 1994; McCarthy et al., 2000; Mears et al., 2002; Newschaffer et al., 1997; Normand et al., 1995; Powell et al., 2001; Preen et al., 2004; Romano et al., 1994; Sarfati et al., 2010; Spurgeon et al., 2011; Waite et al., 1994). Overall, asymptomatic conditions tend to be under-reported in administrative datasets (Powell et al., 2001; Romano et al., 1994), while certain acute medical conditions or complications tend to be regarded by medical coders as more important than others, thereby originating this coding bias (Iezzoni et al., 1992). In this context, several studies have evaluated the degree of agreement between the information on co-morbidities obtained from administrative datasets and that obtained from medical charts. The prevalence of co-morbidities obtained from administrative data was found to be typically lower than that obtained from medical charts for most of the evaluated conditions (Chong et al., 2011). Comparing with chart review data, Quan et al. (2002) demonstrated that administrative data from a Canadian hospital discharge under-reported 29 of 32 Charlson and Elixhauser co-morbidities when ICD-9-CM (International Statistical Classification of Diseases and Related Health Problems, 9th Revision, Clinical Modification) is used, whereas this number increased to 31 with ICD-10-CM (International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Clinical Modification) data (Quan et al., 2002).
In this article, we present a machine learning approach to explore the technical structure of the APR-DRG classification in order to characterise the impact of under-reporting secondary diagnoses representing Elixhauser and Charlson co-morbidities on APR-DRG classification and hospital funding.
Methods
Inpatient data
Inpatient data used in this study were extracted from Portugal’s national DRG database, which currently does not impose a limit on the number of secondary diagnoses to be reported per episode and contains coded hospitalisation data provided by all National Health Service (NHS) public hospitals in mainland Portugal. We collected data of all inpatient episodes assigned to MDC 4 (Diseases and Disorders of the Respiratory System) and 5 (Diseases and Disorders of the Circulatory System) that occurred between 2011 and 2016, which corresponded to the period in which APR-DRG data were available. We applied this methodology on respiratory (MDC 4) and cardiovascular diseases (MDC 5) because they were the two diagnosis areas with the highest number of hospitalisations among all MDCs, accounting for over 1 million hospitalisations during the studied period, with a total of 577,313 episodes assigned to MDC 4 and other 526,611 episodes in MDC 5. Thus, we believe that both areas are relevant for hospitals and public authorities due to this high hospitalisation burden.
Each inpatient episode contained all variables required for APR-DRG grouping, namely principal diagnosis and up to 30 secondary diagnoses, up to 30 operating and non-operating room procedures (as the original APR-DRG grouper only considers the first 30 secondary diagnoses and procedures), discharge status, sex and age. All diagnoses and procedures were coded in ICD-9-CM classification system. Our sample included hospitalisations grouped across 49 base APR-DRGs (version 31), 17 respiratory APR-DRGs (MDC 4) and 32 cardiovascular APR-DRGs (MDC 5).
SVM classification models for simulating APR-DRG classification
We employed support vector machine (SVM) algorithms on Portuguese inpatient data originally grouped with the 3M APR-DRG grouper software to programmatically learn how these hospitalisations were assigned to their APR-DRGs. SVM models learn how to group episodes by finding a separating boundary between them, the so-called hyperplanes (Son et al., 2010), to segregate the different classes (APR-DRGs). The main advantage of this algorithm is that it can overcome high dimensionality problems occurring when there is a large number of input variables relative to the number of available observations (Verplancke et al., 2008), which is the case with APR-DRG assignment, as its algorithm relies on several input variables such as discharge status, a wide variety of diagnosis and procedure codes and other intrinsic patient characteristics (e.g. age and sex) (Averill et al., 2013). Additionally, SVM has demonstrated high performance in solving classification problems in bioinformatics (Chu et al., 2008).
For each studied MDC, we built two classification models: one for assigning the coded episodes to a base APR-DRG and the other one to attribute the SOI level. As ROM subclass is not used for payment and we were interested in investigating the individual impact of co-morbidities on hospital payments, we did not assess changes in ROM levels in our study. All variables required for APR-DRG assignment were used to build the SVM models. The first model (base APR-DRG assignment) included age as a numeric variable, sex and discharge status as categorical variables, as well as all ICD-9-CM diagnosis and procedure codes present in the dataset. As the SOI algorithm does not consider sex and discharge status, the second model (SOI assignment) only included age as a numeric variable, the base APR-DRG itself as a categorical variable and all diagnosis and procedure codes. In both models, each diagnosis and procedure code was treated as a separate binary variable (1 if the episode reported the code, 0 otherwise). We trained SVM classifiers on two-thirds of the inpatient data for the period 2011–2015 (training set) and evaluated their performance on the remaining third (testing set). As evaluation metrics, we estimated the percentage of correctly classified episodes, recall and precision. Although the testing phase provides us with a reasonable estimate of the model performance, we tested the models on data from 2016 and estimated the percentage of correctly classified episodes to add critical validation to the models and assess their capacity of generalisation. The evaluation metrics of the SVM models are presented in Box 1, in supplementary online material.
Sensitivity analysis
Using the previously constructed SVM models, we performed a first classification phase using the complete dataset, with all available codes. A second classification phase was conducted afterwards, but all secondary diagnosis codes representing Charlson and Elixhauser co-morbidities were individually removed to assess grouping changes. We calculated and compared the model’s sensitivity before and after removing each co-morbidity. We further employed paired-sample Wilcoxon signed-rank test to verify whether differences in sensitivity before and after removing each co-morbidity were statistically significant. We considered each APR-DRG combined with a respective SOI level as a unit of analysis to employ this statistical test. We also assessed the proportion of episodes that changed their base-APR-DRGs or SOI level as a result of missing co-morbidities. All co-morbidity codes were selected through Charlson and Elixhauser ICD-9-CM-enhanced definitions presented by Quan et al. (2005). Those definitions identify a set of conditions characterised by high-prevalence or severity and have been extensively used as alternatives to the complexity of acute episodes (Jackson et al., 2015). All 17 Charlson’s co-morbidities and all 30 Elixhauser’s co-morbidities were considered in this study.
Besides evaluating changes in APR-DRG classification, we also studied the financial impact of under-reporting for each studied co-morbidity by estimating the total hospital payments that could have been lost when these co-morbidity codes are missing. For this analysis, we used official APR-DRG prices derived from the 2017 APR-DRG prices and weights table defined for NHS public hospitals in Portugal (Administração Central do Sistema de Saúde, 2017).
Ethical considerations
Since inpatient data used in this study were completely anonymised and only contained the discharge year, diagnosis and procedure codes, sex, age, discharge status and an arbitrary episode identification number, there was no need for ethical approval.
Results
A total of 935,139 inpatient episodes were included in our sample for constructing and testing the SVM models, which corresponded to all inpatient episodes assigned to MDC 4 (485,233 episodes) and MDC 5 (446,906 episodes) between 2011 and 2015. Overall, the SVM models showed a good sensitivity when employed on the complete dataset (first classification phase), with overall rates above 0.8 (Table 1). Using hospitalisation data from the whole year of 2016, we verified that SVM models presented a high capacity of generalisation, achieving a percentage of correctly classified cases of more than 90% for nearly all base APR-DRGs and over 80% for all SOI levels (see Box 1, in supplementary online material).
Overall rates of sensitivity (true positives/total number of episodes) and percentage change in sensitivity for respiratory APR-DRGs classification.
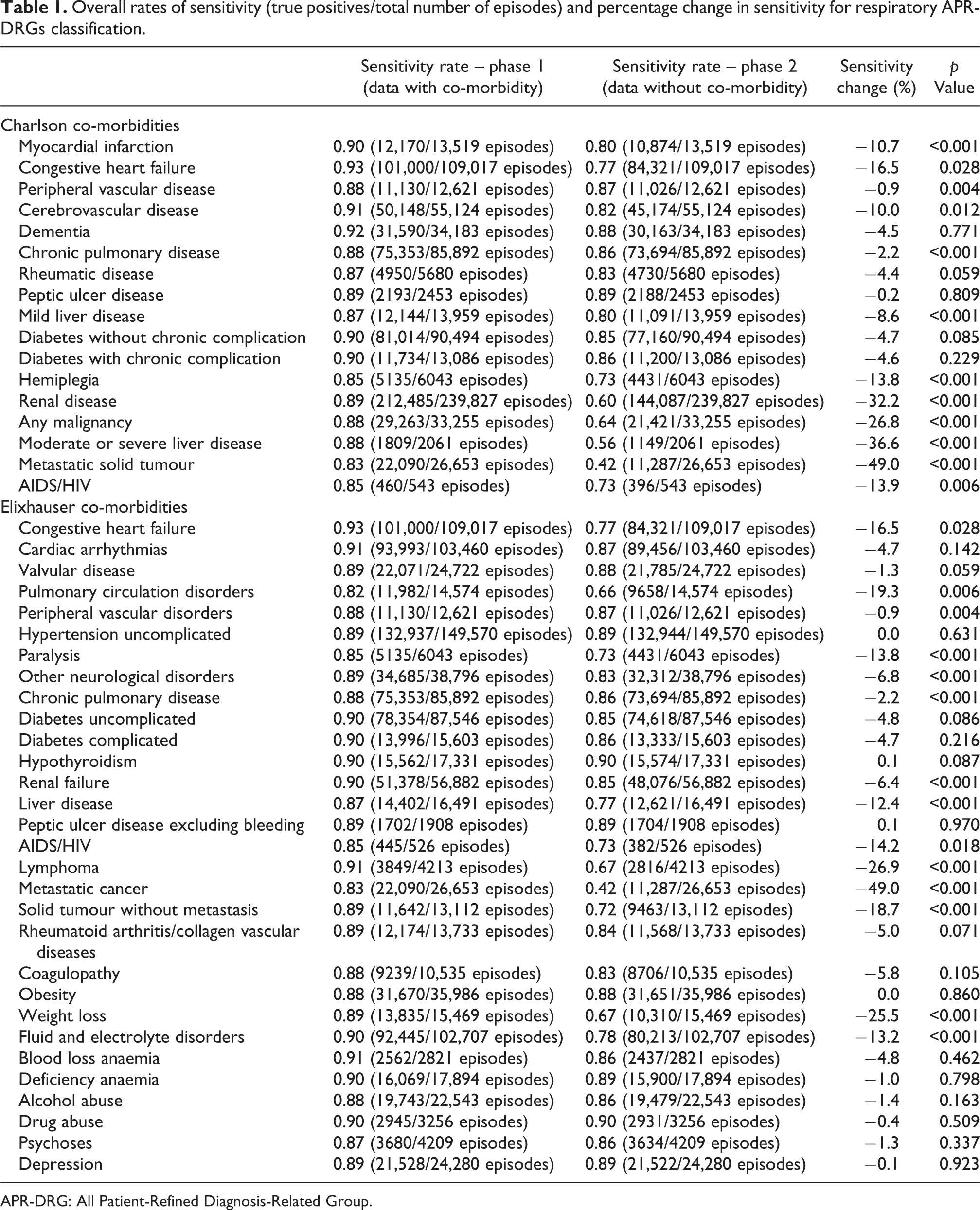
APR-DRG: All Patient-Refined Diagnosis-Related Group.
The removal of most co-morbidities caused a reduction in the model’s sensitivity in both studied MDCs (Table 1). Metastatic solid tumour/metastatic cancer accounted for the highest impact in both MDCs, reducing the model’s sensitivity by almost a half (49.0%) (Tables 1 and 2). Furthermore, the removal of most Charlson co-morbidities (12 of 17) and nearly half of the Elixhauser co-morbidities (14 of 30) caused a significant reduction in sensitivity (p value < 0.05). In general, the same co-morbidities significantly impacted APR-DRG assignment in both MDCs, apart from the following: Charlson’s diabetes, either with or without complication, which only significantly impacted the sensitivity for cardiovascular APR-DRGs; and AIDS/HIV, which only significantly impacted the sensitivity for respiratory APR-DRGs (Tables 1 and 2). A total of 2 Charlson’s co-morbidities and 16 Elixhauser’s co-morbidities did not cause any significant impact on APR-DRG classification (see Tables 1 and 2).
Overall rates of sensitivity (true positives/total number of episodes) and percentage change in sensitivity for cardiovascular APR-DRGs classification.

APR-DRG: All Patient-Refined Diagnosis-Related Group.
In terms of financial impact, we observed that removing any co-morbidity would cause a considerable difference in the total amount to be reimbursed to hospitals (Table 3). Considering the entire period of 2011–2015, the absence of Charlson’s co-morbidity renal disease alone would account for a difference of more than 107 million euros in the total hospital payments for treating MDC 4 patients (Table 3). This same co-morbidity also presented the highest impact on reimbursement for MDC 5 patients, with an estimated difference in hospital payments of more than 45 million euros (Table 3). The top-5 co-morbidities that would have accounted for the highest differences in hospital payments for charging MDC 4 patients included metastatic solid tumour/metastatic cancer (−22.2%), renal disease (−18.3%), moderate or severe liver disease (−17.8%), pulmonary circulatory disorders (−14.1%) and weight loss (−13.7%) (Table 3). The top-5 co-morbidities accounting for the highest differences in hospital payments for charging MDC 5 patients were moderate or severe liver disease (−16.9%), metastatic solid tumour/metastatic cancer (−15.1%), renal disease (−11.5%), congestive heart failure (−10.7%) and any malignancy or fluid and electrolyte disorders (−9.7%) (see Table 3).
Overall percentage change in hospital charges, by MDC.
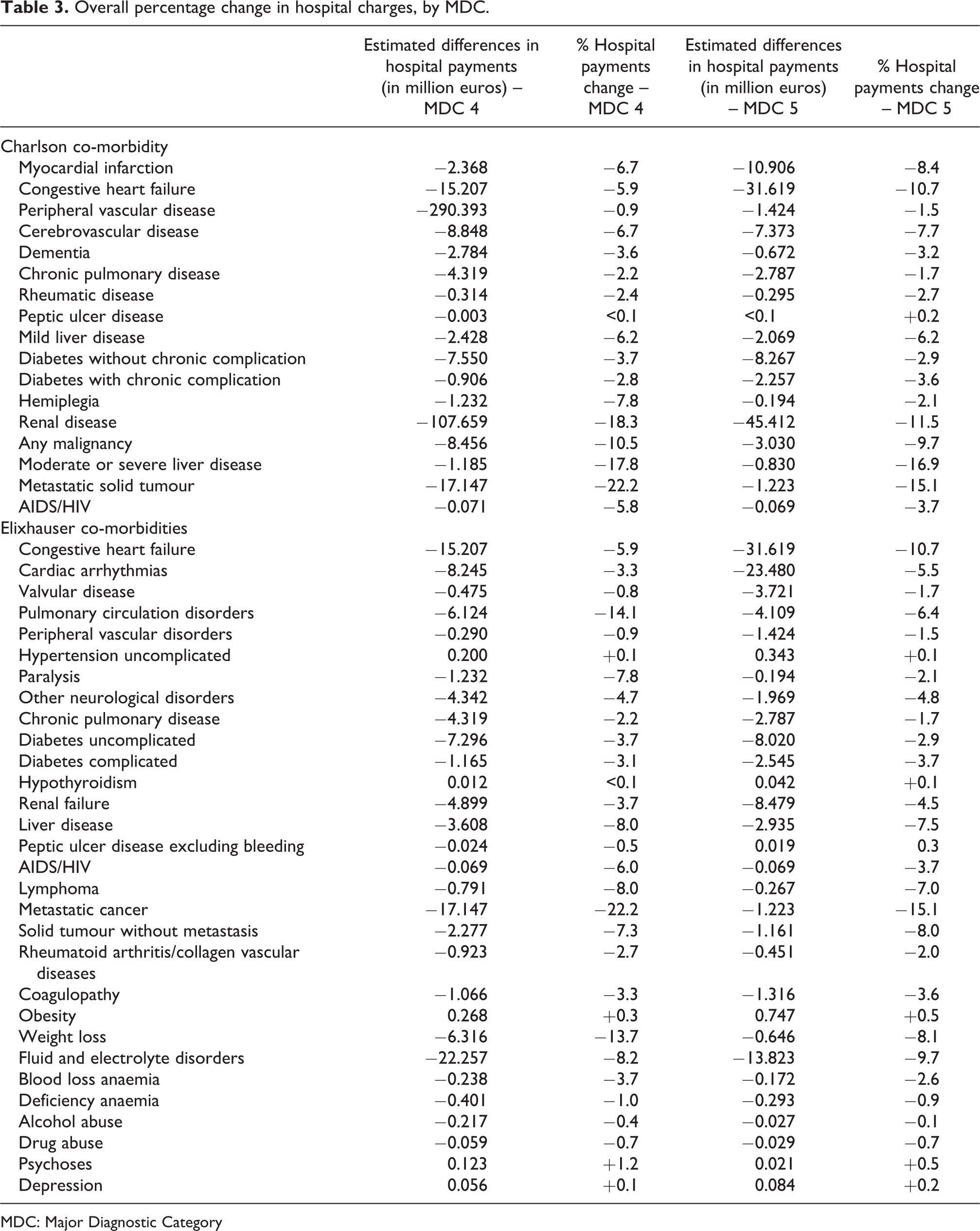
MDC: Major Diagnostic Category
Moreover, removing either Charlson or Elixhauser co-morbidities had a much higher impact on SOI assignment than on base APR-DRG assignment, regardless of the diagnosis area, as a very small percentage (close to zero) of episodes changed their base APR-DRG in the absence of co-morbidities (Tables 4 and 5, in supplementary online material). Tables 4 and 5 (in supplementary online material) present the number of episodes (and the percentage of total) that changed their base-APR-DRG or SOI level when a given co-morbidity was missing in MDC 4 and 5 data, respectively. The classification results obtained with the SVM models using the complete dataset were used as reference. SOI columns correspond to cases that maintained their base-APR-DRG but changed their SOI level, whereas the last column corresponds to cases that changed to another base APR-DRG.
Overall, the highest percentage of episodes that changed their SOI level were those initially grouped into the higher SOI levels, though the magnitude of change varied considerably according to the co-morbidity. Among MDC 4 episodes, the top-5 co-morbidities that accounted for the highest percentage changes in SOI 4 were renal disease (64%), pulmonary circulation disorders (53.3%), moderate or severe liver disease (48.8%), weight loss (43.2%) and myocardial infarction (35.8%). In SOI 3, the top-5 co-morbidities were renal disease (61.4%), moderate or severe liver disease (45.6%), metastatic solid tumour/metastatic cancer (45.6%), weight loss (35.8%) and any malignancy (27.7%). Among MDC 5 episodes, the top-5 co-morbidities for SOI 4 were renal disease (48.1%), moderate or severe liver disease (44.5%), fluid and electrolyte disorders (33.0%), myocardial infarction (27.0%) and liver disease (25.4%). In SOI 3, the top-5 co-morbidities were metastatic solid tumour/metastatic cancer (47.9%), renal disease (42.2%), weight loss (37.1%), moderate or severe liver disease (30.4%) and myocardial infarction (27.4%). Under-coding these co-morbidities would thus lead to the highest changes in the proportion of episodes grouped into higher SOI levels.
To evaluate the influence of each co-morbidity across the different base APR-DRGs, considering that their influence is disease-specific, we presented in s. Table 4 and s. Table 5 (in supplementary online material), by each base APR-DRG, the number of episodes (and the percentage of the total) that changed their SOI levels or shifted to another base APR-DRG following the removal of each studied co-morbidity. Table 4 (in supplementary online material) shows the results for each respiratory APR-DRG, while Table 5 (in supplementary online material) contains the same analysis for each cardiovascular APR-DRG. Overall, even when assessing at base APR-DRG level, higher SOI levels were still the most affected and little to no changes in base AR-DRG were observed (Tables 4 and 5, in supplementary online material). Moreover, the percentage change in SOI level varied greatly according to the base APR-DRG for most co-morbidities. Certain co-morbidities, however, were crucial for SOI assignment, regardless of the base AR-DRG, such as renal disease, which considerably influenced the classification into higher SOI levels for all respiratory APR-DRGs and almost all cardiovascular APR-DRGs (Tables 4 and 5, in supplementary online material). On the other hand, co-morbid conditions such as uncomplicated hypertension or depression little influenced SOI assignment in any respiratory or cardiovascular APR-DRG (Tables 4 and 5, in supplementary online material). Other co-morbidities were against the trend and did considerably impact base APR-DRG assignment, such as the case of co-morbidity myocardial infarction, which changed the base APR-DRG in 29.3% of the episodes initially grouped into APR-DRG 190 (acute myocardial infarction) (Table 5, in supplementary online material).
Discussion
Pursuing higher quality of clinical administrative data and investing in medical coding are highly needed for ensuring that the correct amount of hospital funding will be allocated, especially in countries that employ DRG-based payment systems. The APR-DRG classification has provided means to achieve this goal by subdividing base APR-DRGs into SOI levels to obtain smaller and more homogeneous clusters in terms of resource use. SOI assignment is highly dependent on all necessary diagnosis codes, as its complex algorithm considers the interactions between all diagnoses, age and procedures (Averill et al., 2013). In this context, a comprehensive report of all relevant diagnoses, namely the patient’s underlying co-morbidities, can be a key factor for ensuring that SOI level and thereby hospital funding will be adequate.
Since January 2015, Portugal uses APR-DRGs for budget allocation and reimbursement of hospital care (Administração Central do Sistema de Saúde, 2014), with a percentage share of hospital revenues related to DRGs at about 80% (Mihailovic et al., 2016). In Portugal, each inpatient episode should be coded by a trained coder based upon a discharge summary, which is mandatory in all hospitals within the NHS, complemented by other information from daily medical reports, emergency room records, as well as surgical and pathological anatomy reports (Administração Central do Sistema de Saúde_B, 2014). Medical coding of diagnoses in Portugal is based on the official guidelines provided by the CMS and the National Center for Health Statistics, two departments within the US Federal Government’s Department of Health and Human Services (Centers for Disease Control and Prevention, 2011). Those guidelines do not contain specific rules for coding co-morbidities, but they provide specific information on coding additional diagnoses, including pre-existing conditions, which can thereby influence coding of co-morbidities. In those guidelines, additional diagnoses mean “all conditions that coexist at the time of admission, that develop subsequently, or that affect the treatment received and/or the length of stay. Diagnoses that relate to an earlier episode which have no bearing on the current hospital stay are to be excluded.” Furthermore, these guidelines clearly state that additional diagnoses to be coded are those requiring clinical evaluation, therapeutic treatment, diagnostic procedures, extended length of stay or increased nursing and monitoring care, which can be the case with co-morbidities (Centers for Disease Control and Prevention, 2011).
Using the same database employed in our study, Freitas et al. (2016) found that the number of co-morbidities reported by inpatient episode has increased, with the average number of Elixhauser and Charlson co-morbidities by episode increasing, respectively, by 81% and 48% in the period 2000–2010 (Freitas et al., 2016), though this increasing trend was not equal for all co-morbidities. The proportion of episodes with Charlson’s AIDS/HIV and peptic ulcer disease, as well as Elixhauser’s drug abuse, blood loss anaemia, peptic ulcer disease excluding bleeding and complicated diabetes, has decreased over the studied period (Freitas et al., 2016). On the contrary, the proportion of episodes with Charlson’s myocardial infarction, dementia and renal disease, as well as Elixhauser’s complicated and uncomplicated hypertension, uncomplicated diabetes, hypothyroidism, renal failure, coagulopathy, obesity and depression, have increased above 100% (Freitas et al., 2016). Those discrepancies in reporting certain co-morbidities found by Freitas et al. (2016), which was also described elsewhere in the literature (Chong et al., 2011), should be more closely watched. Thus, investigating and acknowledging how each co-morbidity affects the different base APR-DRGs and knowing whether and which co-morbidities are key within the grouping logic is a relevant matter to improve medical coding. To the best of our knowledge, this was the first study to employ a machine learning approach to explore the APR-DRG classification in order to provide information on the individual impact of each Charlson and Elixhauser co-morbidity on APR-DRGs, raising awareness on the importance of a comprehensive report of these conditions.
We first built SVM models to simulate the APR-DRG classification and assess the model’s sensitivity to the removal of each studied co-morbidity. As removing these codes caused little to no impact on base APR-DRG classification, our analyses focused on changes in SOI levels. Our findings were consistent with the general grouping logic of the APR-DRG as the sensitivity for calculating higher SOI levels was clearly the most negatively affected by the removal of co-morbidities and base APR-DRG classification, which is mainly determined by the principal diagnosis or operating-room procedure, was little affected by the absence of co-morbidities (Tables 2 and 3). Dewilde et al. (2018) also found that certain co-morbidities were strongly associated with higher SOI levels and thus with higher funding. Moreover, while Dewilde et al. (2018) focused on ischemic stroke APR-DRG, our results strengthened these previous findings on the role and importance of co-morbidities regarding SOI determination by adding evidence that included all respiratory and cardiovascular APR-DRGs. We initially considered, however, that the impact of removing co-morbidities was disproportional and specific to the base APR-DRG, which was later confirmed when assessing grouping changes at base APR-DRG level (Tables 4 and 5, in supplementary online material), indicating that certain co-morbidities might be crucial for attributing a SOI level within a given APR-DRG, while it would not influence SOI in others. Thus, these findings are in accordance with the basic clinical principle of the APR-DRG classification as our scenario showed that the role of co-morbidities for the calculation of SOI levels was disease-specific and the significance of co-morbidities depends on the underlying problem, which is characterised by the base APR-DRG. The consistency of our results strengthens the methodology based on the constructed SVM models.
In APR-DRG, the subcategorisations into SOI levels were created to achieve more correct funding within each base APR-DRG, considering that the mix of resources used at different SOI levels leads to substantial differences in total costs. Hospitals that admit proportionally more patients with higher SOI would be underfunded when clinical data fail to provide a more precise SOI calculation. In fact, the distribution of episodes across the different SOI levels might have a substantial impact on hospital budgets. Measuring how under-coding of co-morbidities alone can affect hospital payment is thereby relevant for hospitals and medical coders as such conditions usually drive SOI assignment. Thus, we estimated the amount of hospital payments in the period 2011–2015 that could have been lost when each co-morbidity is not present in the data. We found that all co-morbidities would lead hospitals to receive less money (see Table 3).
In summary, our findings clearly showed how incomplete coding of co-morbidities alone could substantially affect SOI assignment and thus hospital funding. In addition to that, we should also keep in mind that incomplete reporting of co-morbidities could make unfeasible the reutilisation of clinical data for healthcare quality measurement, which often relies on coded clinical data for the calculation of quality indicators (e.g. risk-adjusted in-hospital mortality), for biomedical research, namely for studies that employ more sophisticated methodologies, such as the calculation of risk-adjusted health outcomes, and for other tasks related to healthcare management, as the use of APR-DRGs in conjunction with SOI can be applied for evaluating resource use and establishing patient care guidelines (Averill et al., 2013). Therefore, collecting information on pre-existing or acquired co-morbidities should always be encouraged in hospitals and the construction of specific guidelines for coding of co-morbidities is highly recommended to achieve a more comprehensive report of such conditions and thus improve quality of clinical data and hospital funding in APR-DRG-based payment systems.
Limitations of the study
We used clinical data from an administrative database as gold standard and thus our findings are limited to the reality abstracted from this data. Certain co-morbidities might have had little or no significant impact on APR-DRG grouping because they could have been under-reported and thus the SVM models, which were constructed through patterns learned from the data, would minimise their importance in terms of classification, being less sensitive to their absence. Another important limitation is that our methodology is mostly based on results obtained from the SVM models, as we used their classification results obtained with the complete dataset as baseline to estimate and compare changes in APR-DRGs and hospital payments. Therefore, possible errors or shortcomings associated with the original SVM models may have influenced or been replicated in our results.
Conclusion
Using a machine learning approach, we found that most Charlson and Elixhauser co-morbidities did considerably influence SOI assignment and the absence of all studied conditions may lead to losses in hospital payments to some extent. The degree of influence of each co-morbidity, however, is quite specific to the base APR-DRG. Furthermore, our results based on the SVM models were consistent with overall APR-DRG grouping logic. Our findings reinforced that a comprehensive reporting of the patient’s underlying co-morbidities is relevant for APR-DRG grouping as our findings, in line with previous research, showed that such groups of diagnoses have an important influence on SOI determination, potentially undermining the correct identification of most resource-consuming patients and thus hospital funding. Better documentation of co-morbidities should enable more accurate and complete medical coding, which in turn should lead to more accurate grouping into higher SOI levels. In this sense, hospitals should be oriented to collect all information on any pre-existing or newly acquired co-morbidity and we recommend that future guidelines to be used by medical coders should include specific rules concerning medical coding of co-morbidities.
Supplemental material
Supplemental Material, Box_1_(Supplementary_Material) - Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases
Supplemental Material, Box_1_(Supplementary_Material) for Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases by Julio Souza, João Vasco Santos, Veronica Bolon Canedo, Amparo Betanzos, Domingos Alves and Alberto Freitas in Health Information Management Journal
Supplemental material
Supplemental Material, Table_4_(Supplementary_Material) - Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases
Supplemental Material, Table_4_(Supplementary_Material) for Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases by Julio Souza, João Vasco Santos, Veronica Bolon Canedo, Amparo Betanzos, Domingos Alves and Alberto Freitas in Health Information Management Journal
Supplemental material
Supplemental Material, Table_5_(Supplementary_Material) - Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases
Supplemental Material, Table_5_(Supplementary_Material) for Importance of coding co-morbidities for APR-DRG assignment: Focus on cardiovascular and respiratory diseases by Julio Souza, João Vasco Santos, Veronica Bolon Canedo, Amparo Betanzos, Domingos Alves and Alberto Freitas in Health Information Management Journal
Footnotes
Acknowledgements
Project “NORTE-01-0145-FEDER-000016” (NanoSTIMA) is financed by the North Portugal Regional Operational Programme (NORTE2020), under the PORTUGAL 2020 Partnership Agreement, and through the European Regional Development Fund (ERDF). The authors would also like to thank the Central Authority for Health Services, I.P. (ACSS), for providing access to the data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would also like to thank The Brazilian National Council for Scientific and Technological Development (CNPq) for providing financial support. Moreover, DA would like to thank the Sao Paulo Research Foundation (FAPESP) for financial support (Process number 2018/00307-2).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.