
Abstract
Background:
The Uganda Government, together with development partners, has provided continuing support services (including protection, food, nutrition, healthcare, water and sanitation) to refugee-hosting Districts to successfully manage refugees from different neighbouring countries in established settlements. This service has increased the need for timely and accurate information to facilitate planning, resource allocation and decision-making. Complexity in providing effective public health interventions in refugee settings coupled with increased funding requirements has created demands for better data and improved accountability. Health data management in refugee settings is faced with several information gaps that require harmonisation of the Ugandan National Health Management Information System (UHMIS) and United Nations High Commission for Refugees (UNHCR) Refugee Health Information System (RHIS). This article discusses the rationale for harmonisation of the UNHCR RHIS, which currently captures refugee data, with the UHMIS. It also provides insights into how refugee health data management can be harmonised within a country’s national health management information system.
Method:
A consultative meeting with various stakeholders, including the Ugandan Ministry of Health, district health teams, representatives from UNHCR, the United Nations Children Education Fund (UNICEF), United States Government and civil society organisations, was held with an aim to review the UHMIS and UNHCR RHIS health data management systems and identify ways to harmonise the two to achieve an integrated system for monitoring health service delivery in Uganda.
Results:
Several challenges facing refugee-hosting district health teams with regard to health data management were identified, including data collection, analysis and reporting. There was unanimous agreement to prioritise an integrated data management system and harmonisation of national refugee stakeholder data requirements, guided by key recommendations developed at the meeting.
Conclusion:
This article outlines a proposed model that can be used to harmonise the UNHCR RHIS with the UHMIS. The national refugee stakeholder data requirements have been harmonised, and Uganda looks forward to achieving better health data quality through a more comprehensive national UHMIS to inform policy planning and evidence-based decision-making.
Keywords
Background
Refugee response in Uganda
As of February 2019, Uganda has hosted approximately 1.31 million refugees from South Sudan, Democratic Republic of Congo, Burundi, Somalia, among others (United Nations High Commission for Refugees (UNHCR), 2018a, 2019), which has necessitated major funding requirements to enable the Government of Uganda and partners such as United Nations agencies and non-governmental organisations to provide minimum services. Progress has been made to ensure refugees are protected and live in safety and with dignity in host communities in Uganda; that they are welcomed, placed in demarcated settlements or land plots and provided with basic services (e.g. education, health, food, water and sanitation); and included in strategic planning and resource allocation for national disease prevention and control efforts (UNHCR, 2017a, 2017b, 2018b). Public health services in refugee settlements and settings have been integrated into the district local government health services and implemented in line with national health policy and the Health Sector Development Plan III (UNHCR, 2018a, 2018b). One hundred health facilities currently offer healthcare services to refugees hosted in settlements, although about 30% of people who visit these health facilities are nationals (UMoH, 2018).
Uganda adopted the 2016 New York Declaration’s evolutionary Comprehensive Refugee Responsive Framework (CRRF), a model that facilitates hosting countries to address refugee situations (UNHCR, 2017c). Uganda’s CRRF stipulates implementation of a minimum healthcare service package for all refugees as a key priority, with emphasis on preventive and promotion of health care (UNHCR, 2017a). This applies to new refugee arrivals at entry points, in transit and in reception centres during their initial stay in settlements. The package includes vaccinations, nutrition screening, emergency referrals and provision of life-saving primary healthcare services, in addition to surveillance and response measures for disease outbreaks.
Full integration of health services within the Ugandan Ministry of Health (UMoH)’s national system has been designed to provide the following: accreditation of health facilities in refugee-hosting areas; refugee health workers’ licensing by the UMoH; capacity building of the district local government health system to reinforce its resilience to respond to increasing refugee influxes; coordination with and leadership of UMoH and District Health Offices to ensure that refugees are part of government plans; review of humanitarian partners’ approach to delivery of healthcare services, with a stronger focus on supporting existing government systems as opposed to creating parallel mechanisms; and greater support to UMoH in districts receiving new refugee arrivals (UMoH, 2018). Additionally, increasing efforts by the Office of the Prime Minister, the UMoH, and development partners to include refugees in national planning exercises also comes with associated demands. These include timely and quality information pertaining to settlements for the purposes of monitoring and evaluation together with improved accountability and reporting to the Government of Uganda, United Nations agencies and other partners.
Importantly, for the health sector to adequately plan for the Ugandan population, refugee population health conditions, disease burden and logistics consumption (among others) must be monitored and tracked to inform planning and decision-making for better health services delivery. Collection of health data when refugees access health services either within the settlements or health facilities across the country is also required in an efficient way to achieve this end. This was the major driver for harmonisation of the Ugandan National Health Management Information System (UHMIS) with the UNHCR Refugee Health Information System (RHIS) for refugee health data management.
Refugee health data management in Uganda
In Uganda, there are currently 13 settlements in 11 districts across the country, serving about 1.3 million refugees (UMoH, 2018). Uganda has been one of the refugee-hosting countries where separate information systems or software applications are used for refugee and host population health data management. The UNHCR RHIS and the national UHMIS are used to manage refugee and host population health data, respectively. The UHMIS is an integrated reporting system used to: routinely collect relevant and functional information to aid monitoring of the national Health Sector Strategic Plan indicators; enable evidence-based planning and/or decision-making; and to monitor and evaluate the healthcare delivery system by the UMoH (2014). The national UHMIS is a comprehensive toolkit including all data required by the technical programs (vertical disease programs) and departments within the UMoH. The UHMIS is populated with data routinely collected from communities and health facilities through the electronic District Health Information System (DHIS), which the Districts then submit to the UMoH. The UHMIS is divided into pre-primary (patient management tools, e.g. treatment client cards); primary tools (tools that are used to summarise the data from pre-primary tools, e.g. registers); secondary tools (reporting forms for weekly, monthly, quarterly and annual reporting); and management tools, such as infrastructure, and equipment management tools. Conversely, the national UHMIS and the DHIS do not cater for refugee data needs (i.e. the ability to disaggregate by refugees and nationals). This is what propelled the implementation of the disaggregation in Uganda’s UHMIS to facilitate health data management while appropriately meeting refugee data needs.
As mentioned earlier, the UNHCR RHIS is currently being used alongside the national UHMIS primary tools (registers) to capture data and report information in health facilities that provide healthcare services in the refugee settlements and settings. For instance, health facilities in Uganda’s refugee settings use the UHMIS primary tools (registers) to record refugee health data and then summarise and report these data using UNHCR RHIS tally sheets and reporting forms. The UNHCR RHIS is one of the key paper-based and electronic systems used mainly in refugee-hosting districts in Uganda to collect, tally, aggregate, analyse and report refugee health data (UMoH, 2018; UNHCR, 2010). The main objective of the UNHCR RHIS is to facilitate reporting of health services data for refugees, disaggregated from nationals, to the UNHCR and other partners. The strengths of using the UNHCR RHIS include: an ability to disaggregate by refugee and national status; flexibility to accommodate change in health services provided to refugees that may not be routinely available from the UMoH; and flexibility to reduce or modify reporting requirements at short notice, given the emergency nature of refugee settings (Haskew et al., 2010).
Despite the strengths of the UNHCR RHIS in refugee settings, a number of gaps have been identified, including: lack of sustainability, given it necessitates dedicated human and financial resources mostly provided by donors (evidenced in some host districts where support has been withdrawn and the UNHCR RHIS has collapsed (UMoH, 2018); variance in health data quality as the same health workers collecting data for the UNHCR RHIS also collect data for the national UHMIS; and wide disparities in the ability of end users to use the data housed in the RHIS due to lack of comprehensiveness (has fewer indicators) compared to the national UHMIS. Most importantly, data from the UNHCR RHIS are not readily available to the host districts, the UMoH and other stakeholders, thus making evidence-based decision-making impossible (UMoH, 2018). Furthermore, the UNHCR RHIS has increased the burden of data collection on health workers since they have to work with (analyse and report) two parallel systems (UMoH, 2018). Given the value of refugee data to the UMoH and other stakeholders, coupled with the challenges of using two parallel systems, harmonisation of national stakeholder health data needs was seen as the only means of solving some of these challenges.
Comparison of the UHMIS to the UNHCR RHIS
The UHMIS and the UNHCR RHIS are similar in that both are characterised by: Reporting frequency: This refers to the standard periods within which both systems are used to report health data by respective end users; both systems follow standard reporting frequencies. Indicators: This refers to the priority health and nutrition indicators defined and measured periodically depending on national and/or organisational strategic, monitoring and evaluation goals; both systems constitute health and nutrition indicators. Reporting structure: This refers to the lines or levels through which reporting of health data occurs either using the UHMIS or the UNHCR RHIS; both systems follow a reporting structure. Data collection tools: This refers to the pre-primary (such as client cards), primary (such as registers) and secondary tools (such as tally sheets, summary tables and reporting forms) used to collect, summarise and report health data/information; both systems constitute data collection tools categorised as pre-primary, primary and secondary health data collection tools.
However, the two systems differ in relation to population type disaggregation, health accessibility and the technology platform on which they are built (Table 1). For instance: The standard reporting frequency in the UHMIS context is weekly, monthly, quarterly and annually, whereas that of the UNHCR RHIS is only weekly. National, subnational and international stakeholders are able to easily access aggregate data generated from UHMIS, whereas aggregate data managed by the UNHCR RHIS are not easily accessible. The UHMIS constitutes over 200 indicators and 2286 data elements in the categories of emergency medical services, specialised services (cancer and heart services), mental health, child and school health, immunisation, HIV/AIDS, reproductive health, environmental health (e.g. the Uganda Village Project, Water, Sanitation, and Hygiene (WASH)), tuberculosis and leprosy, supply chain management, quality assurance and planning indicators, community health, nutrition, disability, vector control, mortality, laboratory and blood transfusion services. Conversely, the UNHCR RHIS constitutes fewer indicators in the following categories: population, mortality, morbidity, inpatient and referral services, laboratory, disease control, expanded programme of immunisation, nutrition, reproductive health and HIV/AIDS. The reviewing frequencies for the UHMIS and the UNHCR RHIS differ. The UHMIS is reviewed every 5 years, while the UNHCR RHIS was last updated in 2010. The UHMIS and the UNHCR RHIS differ in the reporting structure. Reporting lines when using the UHMIS run from the community through the health facility through to the district and finally to the national levels. In contrast, the reporting lines are from the health facility to UNHCR in parallel to the UHMIS. The UHMIS does not provide for disaggregation of health data by national or host and refugee populations, whereas the UNHCR RHIS does. The UHMIS is built on the “District Health Information System 2” (DHIS2), which is an open source aggregate information system technology, whereas the UNHCR RHIS is built on spreadsheet software or technology (Microsoft Excel).
Summary of UHMIS and UNHCR RHIS comparison.
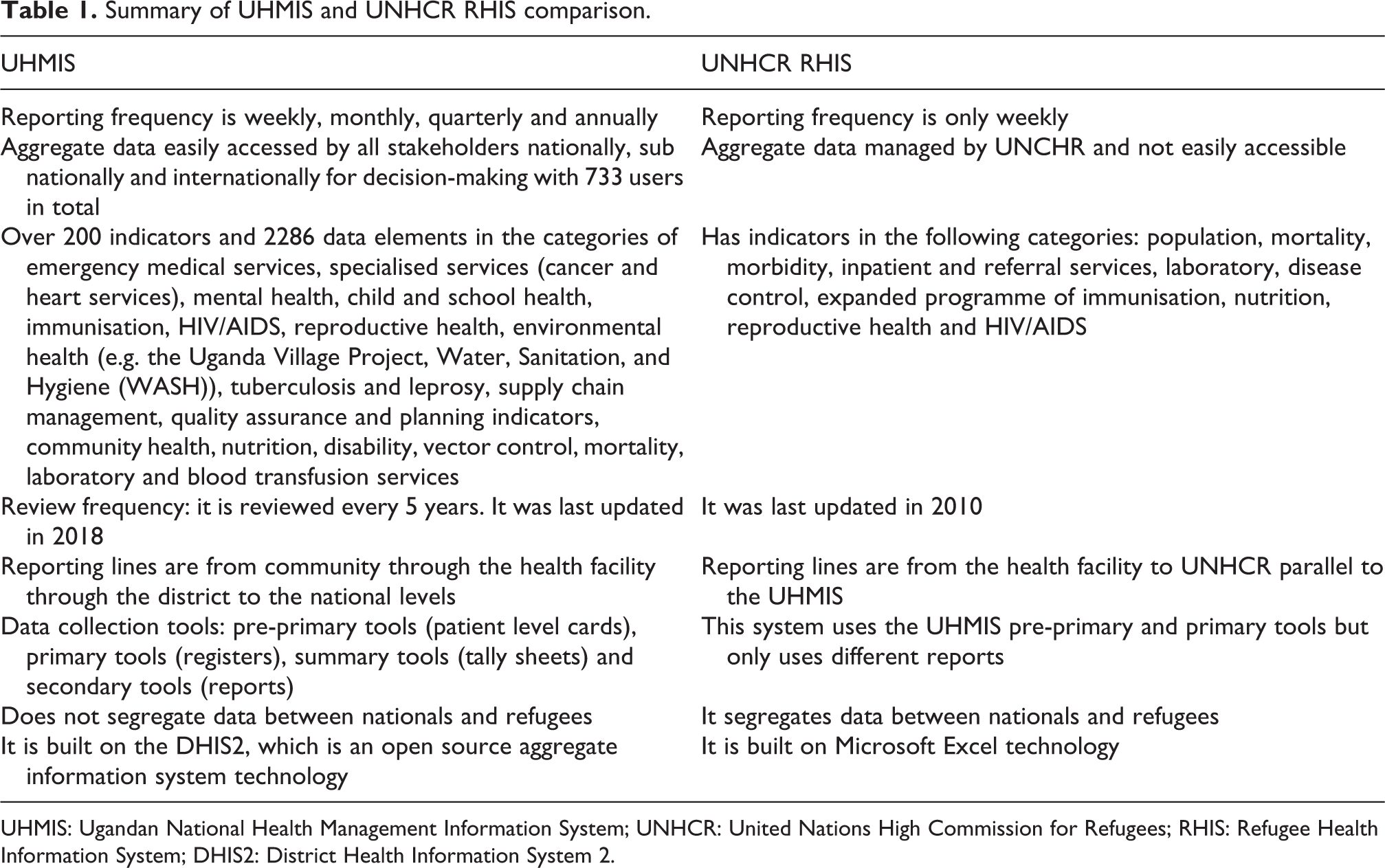
UHMIS: Ugandan National Health Management Information System; UNHCR: United Nations High Commission for Refugees; RHIS: Refugee Health Information System; DHIS2: District Health Information System 2.
Method
The UHMIS and UNHCR RHIS integration process
In May 2018, the UMoH held the UHMIS Review Refugee Stakeholder Consultative Meeting. Its purpose was to review the refugee health data management systems with the intent of establishing ways to harmonise national stakeholder data needs to achieve an integrated system for monitoring health service delivery in Uganda. In this meeting, current practices and refugee data requirements were presented by the various participants including refugee-hosting districts and development partners including UNHCR, the United Nations Children Education Fund (UNICEF), United States Agency for International Development (USAID), centres for disease control and prevention, Doctors with Africa (CUAMM) and civil society organisations to inform harmonisation of UNHCR RHIS recording and reporting tools with the UHMIS. The specific objectives were to present an overview of the 2018 UHMIS review process and highlights from what had transpired thus far; to appreciate the refugee data management situation; to understand data management processes under refugee health services; to identify unique data needs for the refugee-hosting communities; and to develop data collection tools for use in refugee-hosting communities in order to ably feed into the national system (UHMIS and/or DHIS).
Results
Key outputs of the stakeholder consultative meeting were as follows. A clear description of the refugee data management processes and data flow, later translated into current and suggested workflows is illustrated in Figures 1 and 2. The current refugee data management process begins by collecting both nationals’ and refugees’ detailed patient data using the national paper-based UHMIS pre-primary and primary tools (client cards and registers). Data are summarised using paper-based UNHCR RHIS tally sheets and reporting pads, captured in the electronic UNHCR RHIS excel-based system and cleaned for purposes of analysis, reporting and storage for retrieval. Reports are generated and submitted to UNHCR. It is important to note that data are not shared with host districts and neither are they entered into the routine UHMIS. The current health data management process in refugee-hosting Districts is demonstrated in Figure 1. After harmonisation of national refugee stakeholder health data needs, the health data management process in refugee-hosting districts is expected to change. The process will start by collection of all detailed patient data (both national and refugee) using the paper-based UHMIS pre-primary and primary tools (client cards and registers). Data will then be aggregated/summarised using the UHMIS tally sheets, and compilation of separate reports for refugees and nationals will be achieved using the revised reporting forms for refugees and nationals, respectively. Thereafter, all health data (refugee and national) will be captured in DHIS at subnational or district level and submitted to the UMoH. It is expected that all national refugee stakeholders are able to access and use these data for planning and evidence-based decision-making. The suggested workflow or new health data management process is demonstrated in Figure 2. Identification of challenges currently facing refugee data management. Recommendations geared towards harmonisation national refugee stakeholder health data requirements. Draft harmonised UHMIS tools and indicators.
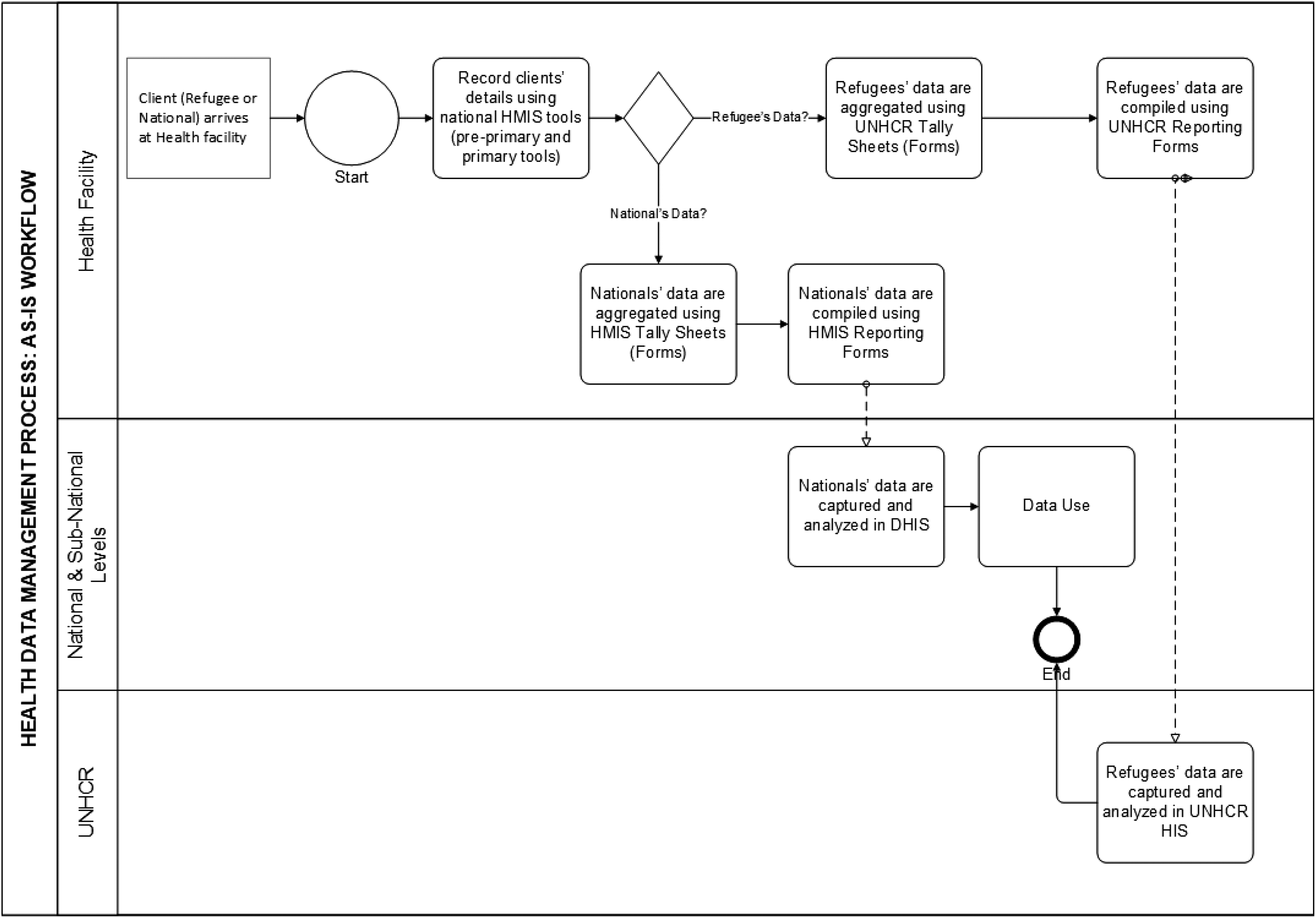
Current health data management process/workflow. UNHCR: United Nations High Commission for Refugees; DHIS: District Health Information System.
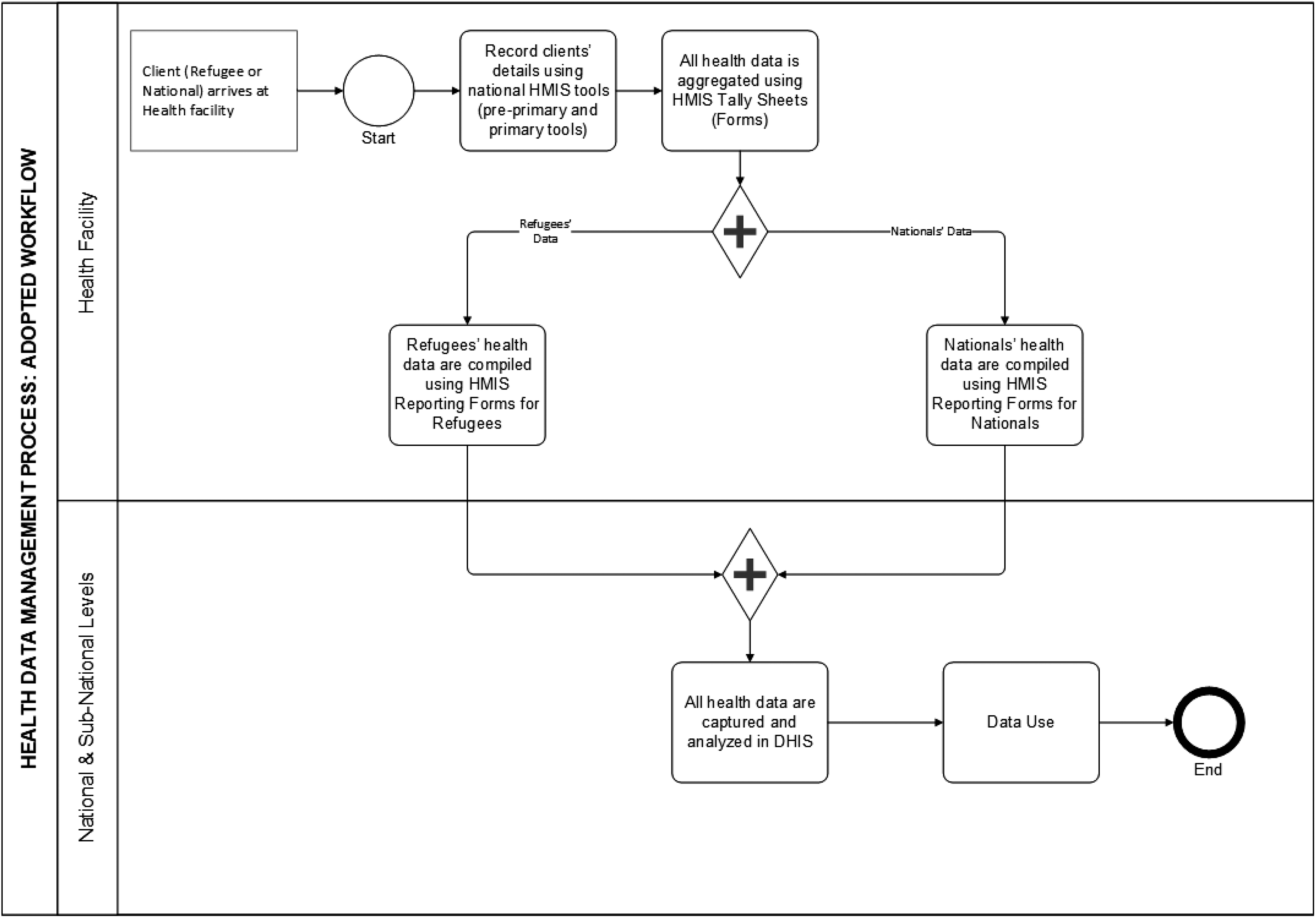
Adopted health data management process/workflow. DHIS: District Health Information System.
Discussion
Stakeholder consultative meeting proceedings
Remarks were made by various representatives from the UMoH, UNHCR, UNICEF, United States Government, district health officers from the 11 districts hosting refugees (Adjumani District, Arua District, Hoima District, Isingiro District, Kamwenge District, Kiryandongo District, Koboko District, Kyegegwa District, Lamwo District, Moyo District and Yumbe District) and other partners supporting refugee-hosting districts. Remarks made were centred on current practices, challenges and recommendations for action. The majority of stakeholders expected that collection of health data disaggregated by refugee and host population would occur while minimising duplication of client records; strategies to ensure data quality would be developed; and ways to address other challenges that affect data collection and reporting, like accreditation of health facilities offering health care to refugees, would be identified and addressed. It was proposed that the UMoH and UNHCR draft a Memorandum of Understanding to ensure that the harmonisation of refugee health data needs be implemented. One of the key priorities was to quickly update the tools and have them piloted in the refugee-hosting districts before December 2018.
Key challenges facing refugee data management in Uganda
Some key challenges noted by the refugee-hosting districts in regard to data management were as follows. Parallel use of UNHCR RHIS and UHMIS is tedious and often translates into duplicate over- and under-reporting, especially in high-volume facilities with heavy workloads, hence affecting the quality of data. Variance in data collected using the two systems. Data housed in the UNHCR RHIS and the UHMIS are different in terms of how diagnoses are classified and indicators defined. The UNHCR RHIS lacks data on crucial services regarding aspects such as laboratory services, viral load (unsuppressed/suppressed) and other national data, such as Hepatitis B tests and cervical cancer, which are not captured. Moreover, UNHCR RHIS data collection and reporting tools do not have some of the data elements and indicators included in the UHMIS, which makes it hard to compare and reuse the data. The UNHCR reporting periods are different from those stipulated by the UMoH; hence, there are discrepancies in data, especially at the time of triangulation. For instance, the UNHCR epidemiological week runs from Saturday to Friday as opposed to the UHMIS week, which runs from Monday to Sunday. This increases the burden on health workers when it comes to data collection, analysis and surveillance reporting. Lack of inclusiveness in capacity building plans for the district staff in terms of building their capacity to use the UNHCR RHIS. Refugee-specific data are not readily accessible by districts and the UMoH resulting in late submission of UHMIS reports because health workers have to report using two parallel systems.
Recommendations from the stakeholder consultative meeting
The meeting unanimously agreed to a reporting system that commanded the harmonisation of refugee stakeholder data requirements. It was agreed that the UHMIS be adopted for all health programming, regardless of the environment (i.e. whether in refugee or host population settings), because, according to the majority of stakeholders, harmonisation of refugee health data needs would answer almost 98% of refugee health data demands; provide all the stakeholders with the required data; enable refugee-hosting districts to provide accountability amidst high consumption of commodities; and coordinate capacity-building activities for all health facilities, including those offering services to refugees.
The general recommendations from the meeting were to redesign data collection and reporting tools that disaggregate health data by nationals and refugees; update the electronic UHMIS or DHIS2 to aid this disaggregation and analysis; train health workers on how to use the redesigned tools (both paper-based UHMIS and DHIS2); ensure adequate supply of UHMIS data collection and reporting tools especially to health facilities that offer services to refugees and therefore register high consumption of tools; establish a strong and effective coordination mechanism for health service delivery and data management; and offer support supervision to the health facilities in refugee-hosting districts for purposes of supporting them in timely reporting of disaggregated data.
Integration framework
Figure 3 demonstrates an integration framework or model that can be used by countries that desire to harmonise their national and refugee population health data systems. The components of the proposed integration framework include the stages, activities and outputs of harmonising the UHMIS and the UNHCR RHIS.

Integration framework for harmonising UHMIS and refugee data systems. UHMIS: Ugandan National Health Management Information System; DHIS2: District Health Information System 2.
Conclusion
Complex challenges and increased funding in providing effective public health interventions in refugee settings have resulted in related demands for better data and improved accountability. This necessitates an improved data collection and reporting system that can disaggregate health data by refugees and nationals to ensure more transparent management of funds as well as aid. All the same, as the refugee influx into Uganda increases, there is a need to reinforce the existing healthcare system with a full package of interventions, including staffing, medical and nutrition supplies, infrastructure, equipment and referral capacities, as well as skills training of existing medical personnel. Uganda is one of the first countries to successfully achieve consensus among stakeholders as far as harmonising national refugee stakeholder needs are concerned. As one of the key priorities, the process of updating both the paper-based and electronic tools has been completed, and plans are underway to start implementation, with financial and technical support from the donors and implementing partners. The integration framework suggested here could be adopted by other countries that aim to follow a similar direction.
Footnotes
Acknowledgements
The authors would like to thank the UMoH leadership, the Health Management Information Division, which coordinated the efforts of the UHMIS integration, as well as acknowledge support from UNICEF for funding the stakeholders consultative meeting. The authors also extend their sincere thanks and appreciation to all the national level partners, including UNHCR, US Mission, Monitoring and Evaluation Technical Support (CDC-METS) program and Strategic Information Technical Support (USAID-SITES). They also thank various participants from the refugee-hosting districts (Adjumani District, Arua District, Hoima District, Isingiro District, Kamwenge District, Kiryandongo District, Koboko District, Kyegegwa District, Lamwo District, Moyo District and Yumbe District) and Implementing Partners, including Infectious Disease Institute (IDI), Medical Teams International, AVSI, Doctors with Africa (CUAMM), IRC and RMF who participated in this meeting.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.