
Abstract
Background:
Documentation of patient health information (PHI) is a regulatory requirement and hence a standard procedure in allopathic healthcare practice. The opposite is true for African traditional medicine (ATM) in most African countries, including South Africa, despite legal and policy frameworks that recognise and mandate the institutionalisation of ATM. Developing good practice standards for PHI documentation is an essential step in the institutionalisation of ATM.
Objective:
This study examined the knowledge and practices of documentation of PHI by traditional health practitioners (THPs) in Durban, eThekwini Municipality, KwaZulu-Natal Province, South Africa.
Methods:
In this quantitative cross-sectional study, snowball sampling was used to identify and recruit THPs. An interviewer-administered questionnaire was used to gather data. Chi-square tests and logistic regression were used to assess associations of knowledge and practice of documentation of PHI with potential predictors; age, gender, education, type of practitioner, experience, number of patients seen per day and location of the practice.
Results:
Of the 248 THPs who participated, 71.8% were female. Mean (SD) age was 47.4 (14.2), ranging 18–81 years. The majority (65.7%) were Izangoma (diviners). Overall, 42.9% of the THPs reported knowledge of patient medical records (PMRs). In logistic regression, only number of patients seen per day remained a significant predictor of knowledge about PMR. THPs who reported seeing 6–10 patients were five times more likely (Odds Ratio (OR): 5.164, 95% Confidence Interval (CI): 1.270–20.996; p = 0.022) to report knowledge of PMR than those seeing <6 patients per day. Overall, 25.0% of THPs reported that they were documenting some PHI. Documentation was associated with having knowledge of PMR (OR: 29.323, 95% CI: 10.455–82.241; p < 0.0001) and being an Isangoma (OR: 3.251, 95% CI: 1.092–9.679; p = 0.02). Not knowing what (56.5%) and how (50.5%) to record were the most commonly cited reasons for not documenting.
Conclusion:
Knowledge of PMR is low, and the practice of documenting PHI is even lower among THPs in eThekwini. That knowledge of PMR was a strong predictor of documentation practice, and the most common reason for not documenting was lack of knowledge about what and how to document suggests that training could improve PHI documentation in traditional medicine practice.
Keywords
Introduction
Documentation of patient health information (PHI) is an essential practice and professional requirement in every healthcare practice (Hussein et al., 2018). PHI describes all phases of patient care and can be used to continually assess, plan, intervene and evaluate the health of a patient and or community in an effort to provide optimal care (Alfoghi and Ramadan, 2017). Despite its significance, there is limited evidence of the practice of documenting PHI in African traditional medicine (ATM) in South Africa and other African countries. ATM is fully recognised in South Africa as a health discipline, mainly for primary healthcare (Moshabela et al., 2016). Traditional health practitioners (THPs) offer services of patient care in ATM.
The practice of PHI recording in ATM in South Africa is undocumented. Integrated PHI can be used to monitor and evaluate ATM diagnostic and treatment approaches as well as treatment outcomes. Such information is essential for standardisation of diagnosis and treatment by THPs. Documentation could enable the beginning of identifying single or combination chemical entities on specific treatments, which could lead to the development of standards for such treatments (Ngarivhume et al., 2015). The standardisation of PHI documentation can allow for interregional and international comparison of diagnosis and treatments. Observing progress, and the evolution of an efficient framework for such research, can provide a firm foundation for future WHO strategies (Bodeker and Burford, 2007). Further, it is conceivable that records of PHI from ATM can provide useful data for clinical and epidemiological studies of ATM. Records of PHI can also contribute to the body of evidence of safety, efficacy and quality of care provided by THPs and possibly enable the development of a specialised health information system (HIS) for ATM, which does not exist at the moment in South Africa.
Efforts have been made to include ATM in health programs such as the HIV and AIDS responses in affected countries including South Africa (Peltzer et al., 2008). However, there has been no systematic efforts to establish sustainable HISs for ATM in South Africa. The role that THPs continue to play in South Africa’s response to HIV/AIDS and its efforts to build up its health system have largely been ignored. HISs, including documentation of PHI, are well developed and documented in biomedicine (Wreford, 2005). There has been considerable advancement in biomedicine, transforming from paper to electronic patient medical records (PMRs) (Gesulga et al., 2017; Ryu, 2012). There has also been considerable support promoting this advancement, and a number of developed countries have had success stories (WHO, 2011). Use of mobile technology devices in supporting patient management through collecting and displaying PMR has become more prevalent (WHO, 2011). There is ample evidence of the value and effectiveness of electronic PMR in improving patient health management in biomedicine health system (Miriovsky et al., 2012). PMRs include relevant facts, findings and observations about a patient’s health history, including past and present illnesses, examinations, laboratory tests, treatments and outcomes (Luthuli and Kalusopa, 2017).
On the contrary, there is paucity of information on HIS in ATM practice (Wreford, 2005). Mafuva and Marima-Matarira (2014) also noted that there is marginalisation of ATM by the modern healthcare system. The lack of discrete policies being followed and implemented by ATM, concerns about lack of monitoring the safety of herbal medicines and the lack of documentation of ATM and its practices contribute significantly to the gap between the two health systems. For adequate cross-referral and patient management to occur, ATM practitioners will need to have some way of recording health information and communicating this information across different systems of healthcare, as is the case within the biomedical system itself. ATM has been in existence parallel to the main health systems for decades in South Africa, as in many African countries. The main goal as mentioned by WHO is to integrate ATM into the main healthcare system, either fully or selectively, intending to enhance general healthcare (Bodeker and Burford, 2007). However, the pace of integration has remained slow and erratic in most African countries, as there is a wide gap between these two health systems that still needs to be addressed. While China, India and other Asian countries have had successful stories of integration of traditional medicine and the allopathic health system, the same is not true for most African countries. Bodeker and Burford (2007) stated that the WHO traditional medicine strategy 2014–2023 focused on four areas that needed attention: policy; safety, efficacy and quality; access; and rational use. Safety, efficacy and quality can be partially addressed by the existence of PMR in ATM. Despite the WHO strategy and the recognition of the importance of ATM, especially in low-income contexts such as much of Africa, there is almost no information on how, if at all, THPs keep PMRs, and what is recorded. This underinvestment risks continuing marginalisation and poor standards of practice and products of ATM (Bodeker and Burford, 2007).
There is a dearth of literature on practices of documentation of PHI by THPs in South Africa with the exception of the study published by Gqaleni et al. (2011). The existence of such activity in ATM practice in eThekwini Municipality has not been studied. The South African National Health Act No. 2 of 2000 (RSA, 2003) requires all healthcare practitioners, including THPs, to document PHI (Laws et al., 2013) in the form of PMRs. There are discrepancies in THPs practice, and there has not been any formal training known to be offered to the THPs. A wide gap exists between the education levels of THPs, from those who are illiterate to those with higher education. Thus, regarding the issue of PMRs, THPs need the support, education and cooperation that formal healthcare systems might be able to offer for them, to execute it appropriately. The government has not yet followed up on implementation and reinforcement of such practice in ATM, hence the need for strategic interventions, including awareness building and training in documentation, should be put in place.
This study, which forms part of a larger project on health information and record-keeping among THPs in Kwa-Zulu Natal, South Africa, presents the first step to begin to address this gap. The overarching aim of this study was to collect comprehensive data from THPs on their current knowledge of PMR, together with information on how the THPs document, including reasons for not documenting, and how and what they document, to contribute to the overall appreciation of ATM practice of documentation.
Method
Research paradigm
A quantitative positivist paradigm design approach was best suited to this study as the focus was to explore, confirm and predict patterns of behaviour of THPs towards the practice of documenting PHI (Aliyu et al., 2014). This was the approach to the study of ATM to reveal the true nature of how the THPs operate (when it comes to documentation of PHI) in their practice. The positivist paradigm mainly makes use of first-hand data obtained objectively and interpreted in a statistical manner.
Study setting
The study design was an analytical cross-sectional study conducted from April 2018 to June 2018 at Umlazi Township and surrounding rural areas of eThekwini Municipality, KwaZulu-Natal Province, South Africa. Umlazi Township is situated on the south-west of Durban and is the fourth largest township in South Africa. Umlazi Township was conveniently selected as it is the largest township in eThekwini Municipality and thus there was a high probability of recruiting enough THPs for the study. THPs were enrolled from Umlazi Township (urban) and rural areas surrounding the Township, namely: Adams, Folweni, KwaMakhutha, Maphumulo, Mbokodweni, Mgababa, Ngonyameni and Umbumbulu. The maps in Figure 1 show the locations of the areas from which the THPs were drawn.

Maps of KwaZulu-Natal in (a) South Africa, (b) Durban and (c) Umlazi and surroundings. Available at: http://www.turkey-visit.com/map/south-africa/umlazi/map_of_Umlazi.jpg.
{kind=link}
Sampling, eligibility and recruitment
To be eligible for participation in the study, THPs had to be living and practising (no time limit was checked) in the Umlazi Township and the surrounding rural parts. THPs visiting the location (for training, to consult, visiting relatives) were excluded. Respondents came from the four categories of THPs that are practiced in South Africa and can be freely consulted by patients: herbalists (Inyanga), diviners (Izangoma), faith healers (abathandazi) and traditional birth attendant (ababelethisi) 1 (Sodi et al., 2011). We also included THPs who were in their first year of training for each of the above-listed categories and still under the supervision of an experienced THP – these are referred to as amathwasa. Amathwasa also work as assistants to most THPs. Those who were willing to participate in the study through written consent were enrolled. The four categories of THPs were determined from those available and willing to participate.
The leaders of eThekwini THPs Forum provided an initial list of THPs residing or practising in Umlazi Township and the surrounding areas. From this list, we sampled participants using the snowballing technique, a form of non-probability sampling method where participants were asked to identify other THPs in the defined areas who would be eligible for participation (Laws et al., 2013). THPs were then contacted and briefed about the study and, if consenting to participation in the study, were interviewed in IsiZulu. Respondents were recruited until saturation (n = 248).
Data collection
Data were collected from April 2018 to June 2018. We used a structured questionnaire with both open- and close-ended questions that had been developed by the research team. The questionnaire was designed in English and translated to IsiZulu (the most common first language for most THPs practicing in eThekwini) by a professional translator. The questionnaire was divided into four sections, sections A to D. Section A focused on biographical information, section B on knowledge of PMRs and practice of documentation of PMRs, section C on attitudes to PMRs and section D focused on perceptions of PMRs.
The questionnaire was piloted with five THPs in February 2018, in Umlazi Township, at the THPs council office, in eThekwini Municipality, before the study commenced and underwent several iterations to ensure it captured the information we were looking for. All interviewers who were fluent is IsiZulu were trained on how to conduct the interviews and expand on the meaning of each question when necessary. The interviews were conducted face-to-face in a private space and lasted for about 45–60 minutes. PMR knowledge was defined as yes or no, based on the response to one item unprompted and prompted question: “Do you know about patient medical records?”
Documentation of PHI was defined as yes or no if a THP self-reported keeping a hard copy or electronic record of an interaction with a patient and that record was directly linked to the patient’s health-seeking behaviour. For those who were not documenting any PHI, there were possible reasons listed, and THPs were asked to choose yes or no for various reasons. In an open-ended question, they were also asked which information they documented. Information was grouped according to content (e.g. address, contact details, full name, date of birth, identification number, gender, age, date, marital status and next of kin constituted “Patient Identification Information”). The previous visit to the doctor, if the patient was on any chronic condition treatment, if the patient had any note from the clinic (written by doctor or nurse), family history, history of illness, weight or any information of previous medication fell under “Patient History.” “Diagnosis” included nature of illness, treatment and instruction for medication. “Fee” included the cost or the charge of THPs to the patient. “Notes” included all the extra information that could be put down by the THPs concerning the visiting patient. “Traditional Knowledge Preservation” included all traditional treatments, such as ingredients mixed to form the traditional medication or concoction given to patients. “Referral Notes” included all notes THPs wrote for the patient to take to any referred Centre by the THPs.
Ethics and other approvals
Ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee, approval number BE570/17. Another approval was obtained from the eThekwini Municipality Health Department Research Committee. Gatekeepers’ approval was obtained from the eThekwini THP Forum. The nature of the study was explained to the participants and if they consented to take part, they gave written consent before the start of the interviews.
Data analysis
Data were analysed using the statistical program for social sciences (SPSS) version 25.0 (IBM Corp, 2017). Descriptive statistics were used to summarise the study population, showing the mean and standard deviation (SD), median and interquartile range, as applicable. Proportions were used to summarise categorical variables. Pearson χ2 was used to determine associations of knowledge and practice of documentation of patient health (dependent variables) and the potential explanatory (independent) variables (age, gender, education, location of practice, type of THP, type of THP qualification, experience, number of patients seen per day, full or part-time). Chi-square test was also used to test for associations between documenting any PHI and the speculated reasons. Binary logistic regression was used to separately assess the association between (i) knowledge of PMRs and (ii) practice of documenting PHI and the explanatory variables while controlling for confounding variables. All potential predictors assessed in bivariate analysis were included in the separate regression models for knowledge and practice of documentation. For the practice of documentation model, knowledge of PMR was also included. All predictor variables were categorical. Collinearity of explanatory variables was assessed using correlation coefficients in the correlation matrix (Midi, Sarkar, and Rana, 2010). None of the variables were collinear. The questionnaire was analysed with χ2 analysis to test associations among subgroups and analysis of variance and t-tests to compare subgroup scores.
Results
Baseline characteristics of study participants
A total of 248 THPs participated into the study. The majority practiced as Izangoma (65.7%) and the remainder as Izinyanga (34.3%; herbalists). Just over a third (36.8%) of the Izangoma representing 24.2% of the THPs also practiced as Abathandazi. The majority of the THPs (71.8%) were female. As expected, the majority of females (84.7%) were Izangoma or Izangoma/Abathandazi practitioners (χ2 = 40.013, p < 0.0001). Most of the THPs (66.1%) were practicing in urban areas, 19.4% in peri-urban/rural and 14.5% in both localities. There was no association between category of practitioner and location of practice (χ2 = 3.485, p = 0.480). The mean age (SD) of the THPs was 47.4 (14.2), ranging 18–81 years. The majority (59.3%; n = 146) had secondary school education, 27.2% (n = 67) primary level, 5.3% (n = 13) tertiary and 8.1% (n = 20) no formal education. Nearly all THPs were trained by indigenous senior practitioners, named (Ogobela) in local language, with only 2% reporting self-training. Nearly half (47.6%) of the THPs had more than 10 years of experience (range: 0–59 years), and for the majority (82.7%), the practice was full time. Most THPs (83.9%) saw up to 5 patients per day, while 10.5% reported seeing more than 10 patients per day.
Knowledge of THPs on PMR
Associations between level of knowledge about PMR and demographic and practice-related factors among the THPs are presented in Table 1. Overall, 42.9% of the THPs reported knowledge of PMR. In bivariate analysis, only age and experience were statistically significantly associated with knowledge of PMR. Highest levels of knowledge were reported by THPs between 45 years and 54 years (58.1%) and between 35 and 44 years (44.7%) of age. The lowest level of knowledge (21.6%) was reported by THPs 25–34 years old. THPs with 11–24 years of experience had the highest levels of knowledge (55.0%), while lowest knowledge was reported among those with 6–10 years of practice (p = 0.044). THPs who reported seeing 6–10 patients per day reported highest knowledge (78.6%) about PMR compared to those who reported <6 (40.8%) and >10 (40.0%) patients (p = 0.021). However, there were no statistically significant differences found for other variables examined. In logistic regression with knowledge of PMR as a dichotomous dependent variable and all explanatory variables included, only number of patients seen per day remained a significant predictor of knowledge about PMR. THPs who reported seeing 6–10 patients were five times more likely (OR: 5.164, 95% CI: 1.270–20.996; p = 0.022) to report knowledge of PMR than those seeing <6 patients per day.
Knowledge of PMRs by THPs.
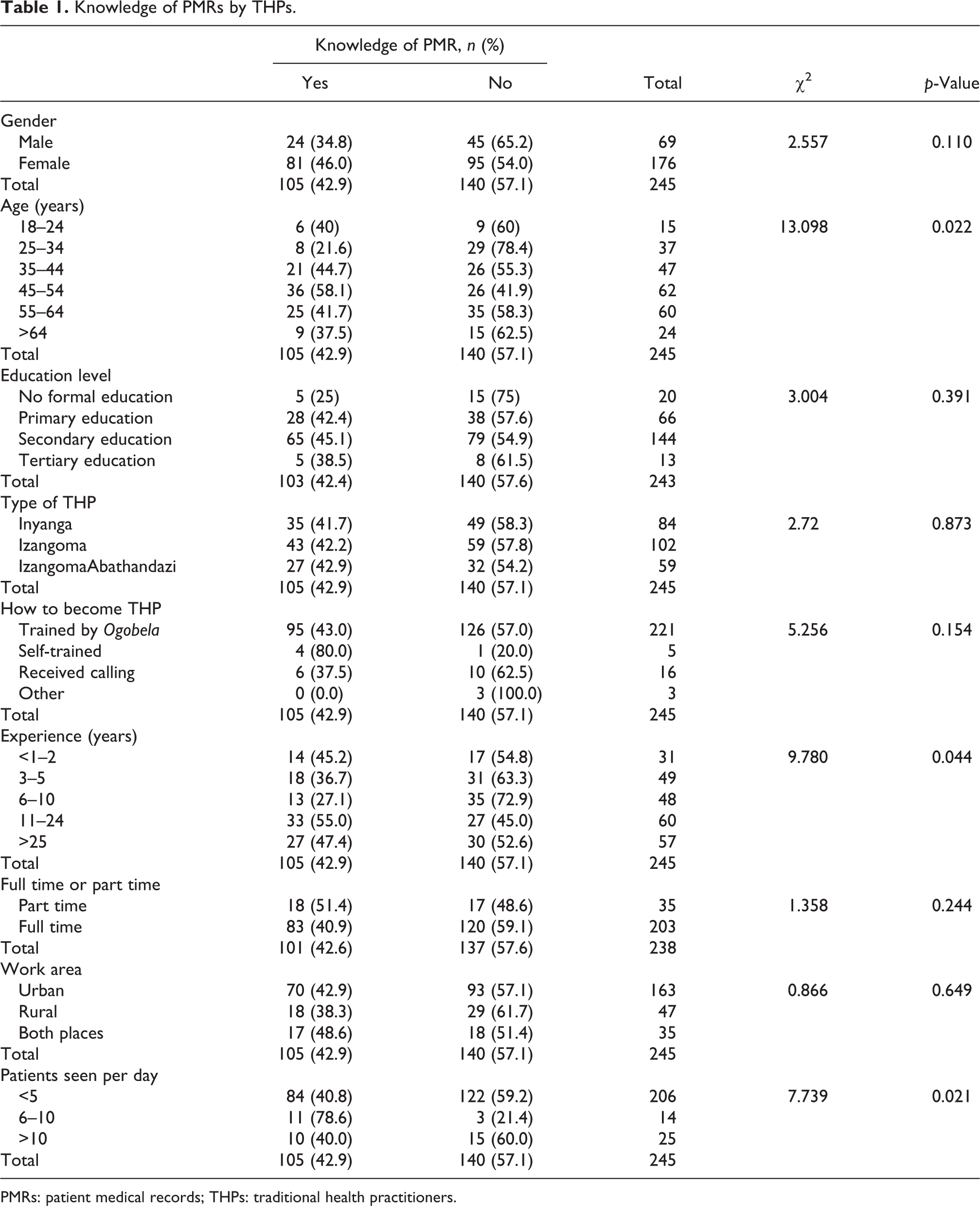
PMRs: patient medical records; THPs: traditional health practitioners.
Documentation of PHI
Table 2 presents the association between practice of documentation of PHI and several potential explanatory variables, including knowledge of PMR. Overall, 25% of THPs reported that they were practicing some form of PHI documentation. As expected, practice of documentation was higher among THPs who reported knowledge of PMR compared to those who did not (51.7% vs. 5.1%; p = 0.001). There were also no significant differences in documentation practice by gender, age, education, category of practitioner, type of training and locality. Similarly, there was no difference in documentation practice whether the THP was full time or part time or in the years of experience as THPs.
THPs’ practice of documentation of patient health information.

THPs: traditional health practitioners; PMR: patient medical record.
In logistic regression analysis with practice of documentation of PHI as a dichotomous dependent variable and all explanatory variables plus knowledge of PMR as independent variables, only knowledge of PMR and type of practitioner were significantly associated with PHI documentation practice. As expected, THPs with knowledge of PMR were nearly 30 times more likely to document PHI (OR: 29.323, 95% CI: 10.455–82.241; p < 0.0001) than those without. Izangoma were three times more likely (OR: 3.251, 95% CI: 1.092–9.679; p = 0.02) to report documenting PHI than Izinyanga.
Type of information THPs document in their practice
Figure 2 shows the types of PHI documented by the THPs. Patient identification information was the most common variable documented by the THPs. THPs were not documenting significant information on patient health management but were focusing on the general information about the patient. Male THPs reported not documenting referral notes, traditional knowledge preservation, notes or fees in any PMR file.

Information traditional health practitioners currently document.
Reasons for not documenting PHI
THPs who were not documenting any PHI in their practice were asked to choose from a list and note which possible reasons best described their reasoning. The reasons are presented in Table 3. Just over half of the THPs (56.5%) reported that they did not know how to record, and 50.5% did not know what to record. Younger THPs (18–24 years) claimed that they had no formal training in documenting PHI. Location of practice was significantly associated with not knowing what to record (p = 0.002). Nearly 80% of THPs operating in both urban and rural areas reported lack of knowledge of what to record compared to 59.5% and 41.7% operating in rural and urban areas, respectively.
Possible reasons for not documenting PHI in ATM.

PHI: patient health information; ATM: African traditional medicine.
Discussion
The South African Government invested support in ATM by endorsing functional structures for the practice to be guided and regulated as is the case with allopathic health system (Moshabela et al., 2016). However, the efforts are contradictory as they seem to have under-funded this health sector (Rees, 2015) and not much has advanced in this sector. Hence, there exist gaps between these two health systems, currently operating in parallel, but failing to share or exchange health information. An apparent limitation of the effort to improve ATM is evident in the lack of funding towards implementation of a constitutional requirement provided in National Health Act (RSA, 2003). This Act requires all healthcare practitioners, including THPs, to document PHI in the form of PMRs. However, for the THPs to be able to fully embrace the standard practice of documentation of PHI in their practice, there is a need for financial support and training in how to document effectively. This study has shown that the majority of the THPs who participated had some basic education that could enable training in documentation to be instituted. A general framework that can be used in the ATM for guidance in proper and effective documenting is vital. This would standardise information documented by all THPs.
Gesulga et al. (2017) reported that user resistance and lack of knowledge and training were predominant barriers to electronic health record system implementation in the conventional health system. Our study has shown that lack of knowledge of what and how to document is a more important barrier to documentation than resistance by THPs. Training of the THPs on how to document PHI is necessary for them to appreciate the significance of PHI in and standardisation of patient management. The supreme goal is to contribute to the institutionalisation of ATM through capacitating THPs to document their treatment approaches and care and develop an HIS for ATM. This enables scientific evaluation of processes and outcomes of treatment and care in ATM. The Medical Protection Society (MPS) stipulated compulsory elements of clinical records that have to be followed (Anthony, 2012) when documenting PHI. Thus, THPs need to be proficient in documenting and creating standard PMR. Contributing towards the institutionalising and professionalising of ATM could also help to bridge the divide between the two health systems (De Roubaix, 2016).
The results of this study have demonstrated that the majority of THP participants lacked knowledge of PMRs, did not keep any form of patients records and were unaware of the importance of documenting the PHI in their practice. A few THPs showed they had knowledge of PMR and were keeping PMRs in their practice. A study by Chege et al. (2015) found similar results in Kenya, where THPs registered knowledge of PMRs and documented PHI. Some THPs were knowledgeable about PMRs but were currently not documenting any PHI in their practice as they lacked the tools to document and the knowledge on how to document precisely in their practice, considering ATM has always been passed on through oral traditions. Level of education seemed to have little influence on the knowledge of PMR. Seventy-nine (79%) of the THPs in this study, with secondary level education, had no knowledge of PMR. However, in terms of level of education of THPs, clearly these practitioners could be trained to be able to document PHI in their practices.
Chege et al. (2015) established that THPs who were managing diabetes patients were using different tools to document PHI in Kenya. In the same way, in the current study, it emerged that THPs were using different tools to document PHI. Each THP was using what was available, or affordable for them to maintain, in order to continue documenting. Ho et al. (2014) reported that the process of documenting patient visits was affected by many factors, which determined how each provider chose to document and contributed to a lack of standardisation across the providers.
All THPs who were documenting PHI were documenting patient identification information. However, only 6% of THPs in this study were documenting patient medical history, which is a significant part of PHI records in the allopathic health system. PMRs are often viewed as the ideal source of health data for measuring patient illness, processes of care and outcomes (Tisnado et al., 2006). Ho et al. (2014) maintained that both healthcare providers and administrators in their study believed that documentation serves five primary domain purposes: clinical, administrative, legal, research and education. However, the prevailing practice of documentation by THPs highlights many gaps as they are failing to document all essential information in their practice as stipulated in the MPS guide (Anthony, 2012). They also lack reliable standardised tools to document PHI. There is no standard practice of documentation of PHI among the THPs as they tend to document differently, in terms of the information they document.
A specialised documentation framework for THPs to allow them to capture the fundamental elements of health information as per the MPS guide of medical records Anthony (2012) could go a long way in promoting the practice of documentation in ATM. Isola (2013) noted that inadequate documentation was listed as one of the major shortcomings of ATM practice. Many medical errors have been noted in diagnosis and prescription when the practitioner relies on memory (Isola, 2013). This has also been reported in biomedical healthcare systems, where documentation was being done poorly (Alfoghi and Ramadan, 2017). Documentation of PHI by THPs in this study was not comprehensive and remained at minimal levels. Similar observations have also been reported by Chege et al. (2015).
In general, there are different ways and styles in documenting PHI, varying from institution to institution. Even in the formal health systems, this may vary from practitioner to practitioner or health centre to health centre (Ebirim and Buowari, 2013). For health information to be valuable, it is critical that it be comprehensively documented. Therefore, THPs need to be educated in this aspect of PMR and how to document comprehensively. PMRs could positively support the two parallel health systems that currently exist in South Africa to merge and work more closely. It is essential for THPs to improve their knowledge on PMRs and professionalise their practice by initiating dedicated documentation of PHI in their practice. Institutionalisation of ATM practice and enabled development or streamlining of HISs of ATM in South Africa is possible.
Conclusion
Documentation of PHI can promote validation and evaluation of ATM. A formal framework to document PHI for the effective contribution of ATM to mainstream healthcare is essential. Therefore, it is important to consider improving the knowledge of PMR in ATM by introducing a bespoke documenting tool for the THPs to use in their practice. Lack of knowledge of PMR and documentation tools tailored for ATM perpetuate non-documentation and the oral transmission of information, resulting in continued marginalisation of ATM and ATM potential risk to patient safety. Despite the lack of knowledge about PMR and their poor documenting practices, there is clearly a considerable interest among THPs when it comes to exploring the use of patient record systems in their practice. However, there is also a need to enhance knowledge and skills of THPs about PHI documentation and the issues of confidentiality around PHI.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to THPs for participating in the study, University of Kwa-Zulu Natal, College of Health Sciences and National Research Foundation (NRF) for funding the project. The funding agency did not participate in the process of designing the study, data collection, analysis, report writing and selection of the journal. The authors extend their heartfelt gratitude to the British Academy Writing Programme 2018 for funding and associated workshops which supported the development and submission of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from College of Health Sciences, University of Kwa-Zulu Natal and National Research Foundation (NRF). The funding agency did not participate in the process of designing the study, data collection, analysis, report writing and selection of the journal. The authors extend their heartfelt gratitude to the British Academy Writing Programme 2018 for funding and associated workshops which supported the development and submission of this manuscript.