
Abstract
Background:
Social media is used in health communication by individuals, health professionals, disease centres and other health regulatory bodies. However, varying degrees of information quality are churned out daily on social media. This review is concerned with the quality of Social Media Health Information (SMHI).
Objective:
The review sought to understand how SMHI quality issues have been framed and addressed in the literature. Health topics, users and social media platforms that have raised health information quality concerns are reviewed. The review also looked at the suitability of existing criteria and instruments used in evaluating SMHI and identified gaps for future research.
Method:
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses and the forward chaining strategy were used in the document search. Data were sourced according to inclusion criteria from five academic databases, namely Scopus, Web of Science, Cochrane Library, PubMed and MEDLINE.
Results:
A total of 93 articles published between 2000 and 2019 were used in the review. The review revealed a worrying trend of health content and communication on social media, especially of cancer, dental care and diabetes information on YouTube. The review further discovered that the Journal of the American Medical Association, the DISCERN and the Health on the Net Foundation, which were designed before the advent of social media, continue to be used as quality evaluation instruments for SMHI, even though technical and user characteristics of social media differ from traditional portals such as websites.
Conclusion:
The study synthesises varied opinions on SMHI quality in the literature and recommends that future research proposes quality evaluation criteria and instruments specifically for SMHI.
Keywords
Introduction
Social media is described as a group of Internet-based applications that build on the foundations of Web 2.0 to allow for the creation and exchange of user-generated content. Different forms of social media such as social networking sites, blogs, content communities, collaborative projects, virtual game worlds and virtual social worlds have been created to idealise the engagement, immediacy and interactivity that Web 2.0 offers (Kaplan and Haenlein, 2010; Smailhodzic et al., 2016). Today, the diverse range of social media tools impact the way people create, seek and share information. People of diverse backgrounds and cultures freely share all manner of information on social media including health contents. Ranging from benign to malignant health issues, consumers search the web for information on symptoms and conditions of ailments, communicate in real time with health experts, learn to administer drugs and complete online personal health assessment questionnaires (Doherty-Torstrick et al., 2016; Finney Rutten et al., 2019; Fox and Duggan, 2013; Zhang et al., 2019). Similar to other information shared on social media, health information also comes from varied sources and channels including generalist information platforms, lay users, healthcare professionals and institutions (Crook et al., 2016; Şahin et al., 2019). For instance, several studies in the United States report of a growing use of social media in health communication among adults (Chou et al., 2009; Jacobs et al., 2017; Jones and Fox, 2009; Tennant et al., 2015). In the United Kingdom, social media has become one of the popular sources of health information among young people (Fergie et al., 2016a, 2016b). Social media is also used in health communication by hospitals, clinics, disease centres and other health regulatory bodies (Moorhead et al., 2013). During and after recent pandemics such as Covid-19 (Chan et al., 2020) and H1N1 (Ding and Zhang, 2010) or epidemics such as Ebola (Nagpal et al., 2015), social media platforms have been used as timely information dissemination sources by the World Health Organization, Centers for Disease Control and Prevention and national health agencies (Househ, 2016).
Motivated by reasons such as public safety (Antonius and Rich, 2013), well-being and wellness of people (Zhang et al., 2020), financial considerations as well as fame (Eysenbach, 2008), these information sources (actors) capitalise on the network effect of social media to share and reshare health information. In the end, ascertaining information quality becomes a challenge especially for health-anxious individuals who are often nervous and fretful, and therefore rarely question the credibility and accuracy of the information (McManus et al., 2014; Te Poel et al., 2016). According to Baumgartner and Hartmann (2011), health-anxious people tend to have a negative response towards trustworthy health information sources such as from government health agencies. Because these organisations present more factual information, they may increase anxiety about health conditions for individuals who undertake searches for reassurance.
Perhaps one critical source of health misinformation on social media is through self-disclosure. According to Lin et al. (2016), when individuals self-disclose medical information on digital platforms such as social media, it creates a reciprocal tendency to compel recipients to also share their health information or reshare other related information within their friend network. This creates a cycle of misinformation sharing among friend networks if such medical information is fake or miscommunicated. Note that unlike information obtained from traditional health media outlets such as books, journals and health magazines which not only are produced by recognised institutions and individuals but also come with metadata such as disclaimers, author information, year of publication, the publisher and the target audience, Social Media Health Information (SMHI) is often informal and largely authored by non-health professionals and therefore raises quality concerns. The casual, unregulated nature of social media poses risks especially to online health information seekers who are often novices and anxious in seeking answers (Deng and Liu, 2017; Li et al., 2018; Strekalova, 2016). Moorhead et al. (2013), Orizio et al. (2010) and Adams (2010) affirm that while social media presents a potent means of disseminating health information, quality of the content, its reliability and misapplication are real concerns. There are also associated limitations such as non-disclosure of the source of shared documents, especially because of the background of authors.
In view of the above concerns, this study sets out to review how SMHI quality issues have been framed and addressed in the literature. We define information quality in this study as “the fitness to use or the sufficient value provided to the user of that information” (Miller, 1996; Naumann and Rolker, 2005). While several literature reviews have been conducted on social media health communication, none so far has been dedicated to SMHI quality. For instance, Moorhead et al. (2013) provided a review of the uses, benefits and limitations of social media for health communication, and Ventola (2014) conducted a review of the benefits, risks and best practices of social media use for healthcare professionals. The review by Grajales et al. (2014) focused on social media applications in medicine and healthcare. Others such as Best et al. (2014) and Yonker et al. (2015) focused on adolescents’ use of social media, their health and well-being, while Charles-Smith et al. (2015) conducted a literature review of the role of social media in disease surveillance and outbreak management. We hypothesise that whether considering the benefits and risks of social media health communication, its application in healthcare or how adolescents use it in health promotion and well-being, the quality of the information is paramount. The investigators therefore reviewed research works with a focus on health topics, users and social media platforms that are raising health information quality concerns as well as the suitability of existing criteria and instruments used in evaluating quality of SMHI using the following Review Questions (RQs) as a guide:
Methodology
The article adopted the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the forward chaining strategy, also known as citation searching (Booth, 2008), to track relevant papers for the review. PRISMA (Moher et al., 2009) was used in this study because of its transparent way of reporting reviews as well as its popularity in healthcare systematic reviews and meta-analyses. The forward chaining strategy, which begins with a highly cited paper on a subject of interest and searches for relevant cited papers in a forward direction, was used to complement PRISMA. Moorhead et al. (2013), Neiger et al. (2012) and Adams (2010) were the publications used in the forward chaining approach via Google Scholar. The search strategy was used in five electronic databases, namely Scopus, Web of Science, Cochrane Library, MEDLINE and PubMed Central. Three search strategies were used in the PRISMA review. In each strategy, the Boolean “OR” and “AND” operators were combined with the key search terms “social media,” “social network,” “social networking,” “Web 2.0,” YouTube, “Facebook,” “Twitter,” “Instagram” and WeChat.
In the first PRISMA strategy, the above search terms were combined with “Health Information Quality” or “Medical Information Quality” in searching for relevant publications. An example of such combination is the search term “Social media Health Information Quality” or “YouTube medical information.” The second search strategy combined five information quality criteria (i.e. the attributes, principles, characteristics or features that guide users when accessing health information), namely “credibility,” “content,” “disclosure,” “design” and “interactivity,” with the above search terms to widen the scope of the article search. Thus, the search terms “social media,” “social network,” “social networking,” “Web 2.0,” YouTube, “Facebook,” “Twitter,” “Instagram” and so on were combined with the terms “health information credibility,” “health information content,” “health information disclosure,” “health information design” or “health information interactivity (see Box 1). The five criteria and their related sub-criteria were selected from notable evaluation instruments such as the Journal of the American Medical Association (JAMA) benchmark (Silberg et al., 1997; Winker et al., 2000), the DISCERN instrument (Charnock et al., 1999), the Health on the Net Foundation (HONcode) principles (Boyer et al., 1998), the Agency for Health Care Policy and Research (AHCPR, 1999) (now the Agency for Healthcare Research and Quality (AHRQ)), LIDA and Flesch–Kincaid grade level (FKGL) that are relevant to the evaluation of SMHI quality. Most of the sub-criteria have different names in the JAMA, DISCERN, HONcode, AHRQ, LIDA or FKGL instruments even though they share the same meaning. For instance, while the HONcode uses the term authoritative to describe the credibility of the Internet information, the JAMA benchmark and the AHRQ respectively use authorship and source to describe the same criteria. Therefore, such criteria that generally describe the trustworthiness of the source of the information were labelled credibility. Typically, after a set of health information quality criteria has been established, a methodological or procedural instrument is designed to demonstrate how to evaluate or measure information quality. In the final full article review, and guided by RQ3, we assessed the popularity and use of each of the quality criteria in Box 1 together with the evaluation instruments that are often used in determining SMHI quality. For the PRISMA flow diagram, see Figure 1.
Internet health information quality criteria.
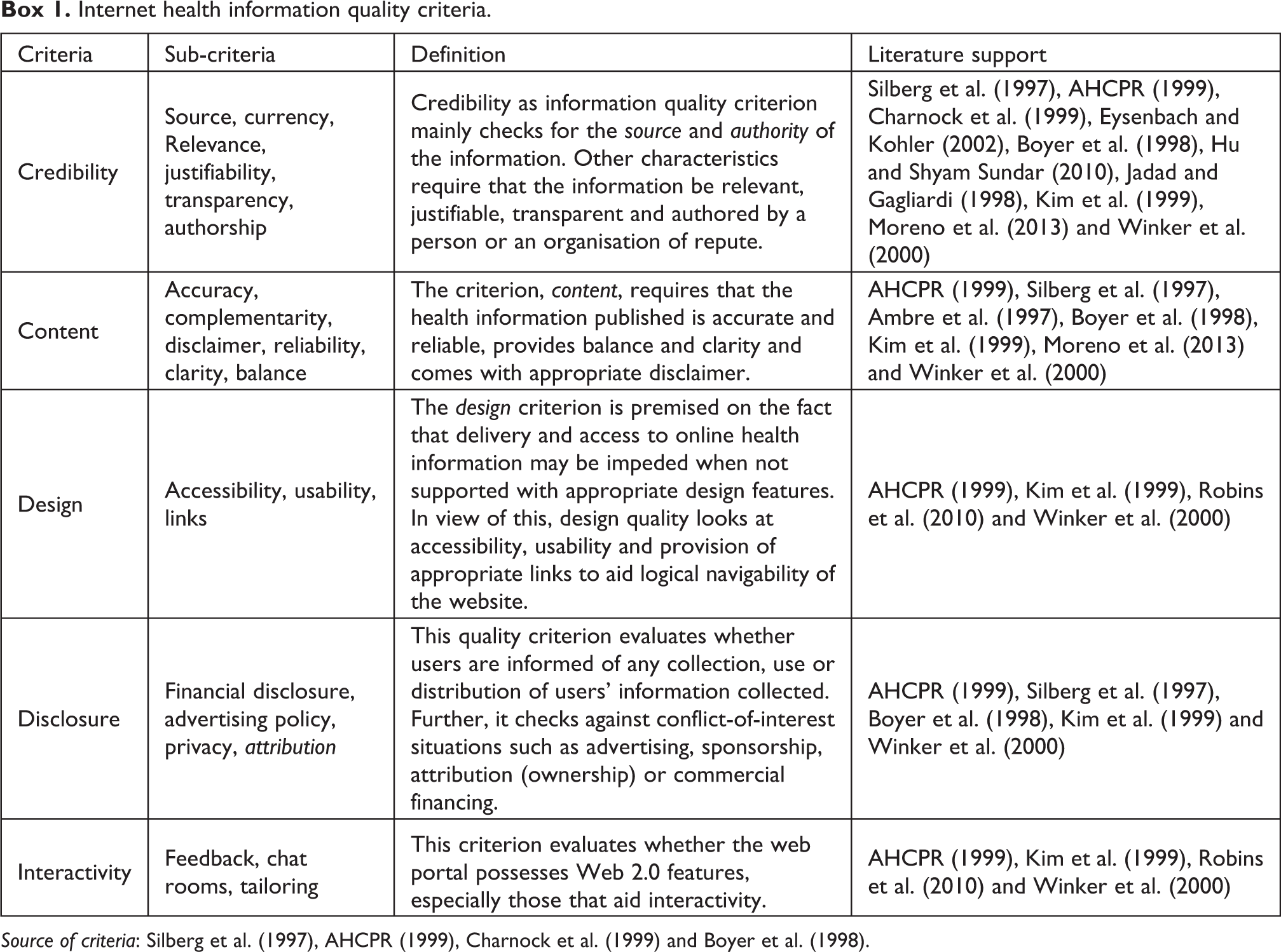
Source of criteria: Silberg et al. (1997), AHCPR (1999), Charnock et al. (1999) and Boyer et al. (1998).
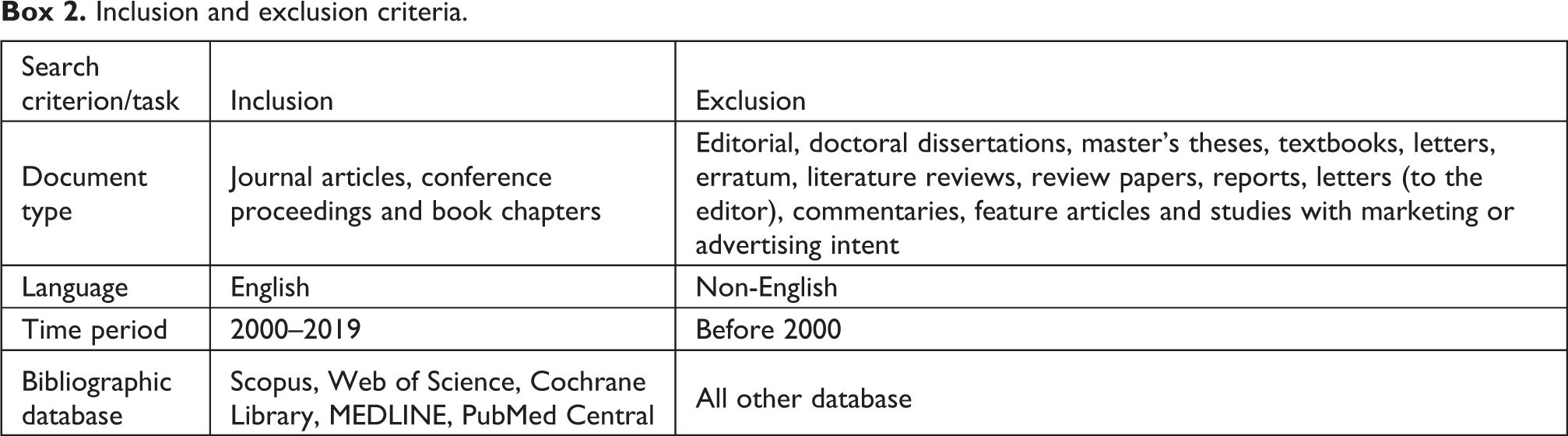
Inclusion and exclusion criteria.
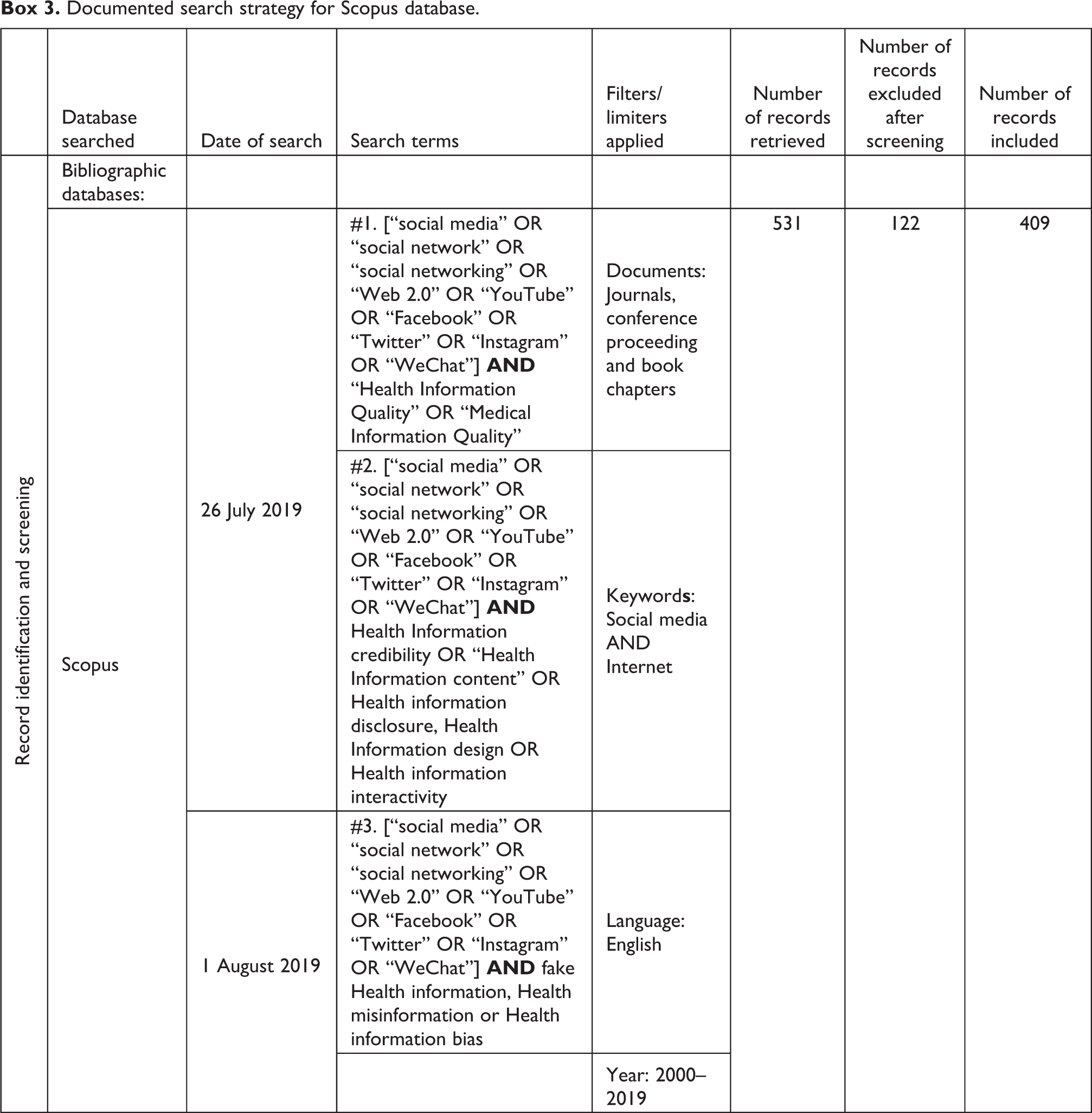
Documented search strategy for Scopus database.

PRISMA flow diagram. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The third and final search strategy anticipated that the absence of information quality could result in descriptions such as fake information, misinformation or information bias. These terms were also combined with “social media,” “social network,” “social networking,” “Web 2.0,” YouTube, “Facebook,” “Twitter” and “Instagram” to extract other relevant publications. In all, 796 articles were initially identified by SBE and EAD. Titles and abstracts were screened by EAD to determine their eligibility. After applying the exclusion and inclusion criteria, a total of 198 articles were included for full-text review. SBE was tasked to retrieve the full-text articles. AAD and EAD independently reviewed the selected articles. Ultimately, 93 articles qualified for inclusion in the final content analysis – qualitative studying of the documents. The search period was limited to years 2000–2019 since major social networking sites that have survived to date were launched in the 2000s. The search inclusion and exclusion criteria are shown in Box 2; the full electronic search strategy used for the Scopus database is presented in Box 3.
Results
The results of the review have been reported in accordance with the RQs.
Health topics
In reference to RQ1, this section addressed quality concerns relating to SMHI on a range of health topics. Two sub-themes, diseases, disorders and ailments and treatments, were created to review the health topics (Table 1). As shown in Table 1, cancer was the most investigated health issue on social media, followed by dental care and diabetes. Though cancer was the most investigated health issue (cited by 18 papers), there were actually only four unique information quality concerns raised in total, namely source, relevance, accuracy and reliability. However, while diabetes was cited by only seven articles, there were five unique information quality concerns raised: source, currency, relevance, accuracy and reliability. This means that while cancer was the most discussed disease in the literature, diabetes had the greatest number of unique information quality concerns. Apprehensions relating to information quality were mostly about inaccuracies and misleading cancer self-medications and treatment videos on YouTube. There were other diseases and disorders whose information quality concerns on social media were sparingly mentioned (single publications) such as Robillard et al. (2013) on dementia, Harber and Leroy (2017) on lung disease, Taggart et al. (2015) on HIV, Singh et al. (2012) on arthritis, Ng et al. (2017) on scoliosis, Erdem and Karaca (2018) on kyphosis, Bora et al. (2018) on Zika disease, Larouche et al. (2016) on urethral slings, Nour et al. (2016) on schizophrenia, Lenczowski and Dahiya (2018) on psoriasis (skin disease), Garg et al. (2015) on kidney disease and Thapa et al. (2018) on attention deficit hyperactivity disorder (ADHD).
Health topics raising information quality concerns on social media.
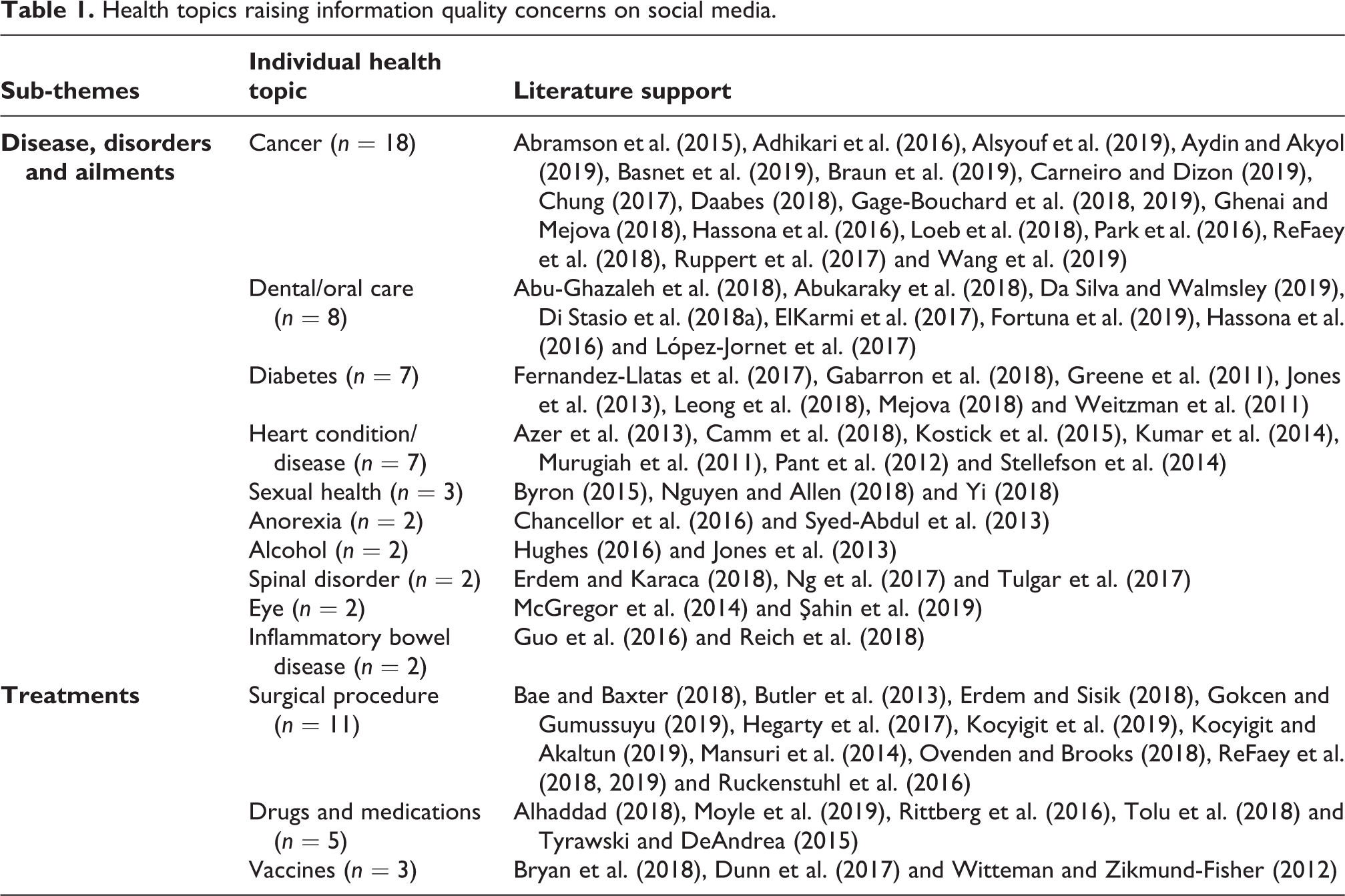
On health topics relating to medical treatments, surgical procedures were the subject of the majority of publications in terms of information quality (Table 1). For instance, a YouTube quality analysis of cataract surgery and disc herniation (Bae and Baxter, 2018; Gokcen and Gumussuyu, 2019) revealed a worrying trend of misinformation. There were also information quality concerns relating to drugs/medications and vaccines as shown in Table 1. For example, Tyrawski and DeAndrea (2015) reported of an increase in social media pharmaceutical information that have commercial intent. To affirm the impact of health misinformation on people, Dunn et al. (2017) described how misinformation and conspiracies in some states in the United States resulted in low vaccine coverage. Articles reviewed across various health topics were critical of SMHI quality, with some being categorical in condemnation using terms such as fake, misinformation, misleading or low-quality information (Alsyouf et al., 2019; Chou et al., 2018; ElKarmi et al., 2017; Ghenai and Mejova, 2018; Goobie et al., 2019; Loeb et al., 2019; Qi et al., 2016; Syed-Abdul et al., 2013). Though overall most articles expressed grave concern with the quality of SMHI, Henderson et al. (2019), Aboelmaged (2018), Kumar et al. (2014) and Esquivel et al. (2006) were exceptions – positing that the quality of SMHI in their respective studies was satisfactory. For instance, according to Esquivel et al. (2006), most of the information shared by users in a breast cancer social group was accurate. However, in instances where statements were misleading and inaccurate, participants sought to correct them in their subsequent postings.
The literature also highlighted diverse groups of people to whom health topics on social media are normally targeted. For instance, information quality concerns were raised in the literature about the content of YouTube videos which focus on oral care in children. Di Stasio et al. (2018a, 2018b) examined parents’ concerns of YouTube videos on oral thrush (oral candidiasis) and mouth sores in children and described them in general to be unsatisfactory. According to Di Stasio et al. (2018b), videos on oral thrush and mouth sores in children offered by generalist information channels (which are the main sources of these videos) on YouTube were misleading. Thapa et al. (2018) also bemoaned the quality of YouTube videos on ADHD in children.
Information quality concerns relating to women had two common themes, namely breast and cervical cancer, on three social media platforms, YouTube, Facebook and Twitter (Abramson et al., 2015; Chung, 2017; Esquivel et al., 2006; Himelboim and Han, 2014; Tan et al., 2014). All the authors with the exception of Esquivel et al. (2006) bemoaned the quality of breast cancer information on social media. One major concern centred on information provided by lay users, generalist information channels and advertisers who have no specific medical training. To address such concerns, Di Stasio et al. (2018a) suggested that social media platforms could flag health information as emanating from either a trusted source or otherwise. There were also calls by authors advocating for healthcare professionals and organisations to take active role in correcting misconceptions, especially those that are authored by generalist information channels (Antheunis et al., 2013; Şahin et al., 2019).
Quality evaluation criteria and social media platforms
This section addresses RQ2 and RQ3 by focusing on health information quality criteria that have been discussed in the literature in relation to social media platforms. Guided by the quality criteria in Box 1, the focus was to understand (1) quality criteria that have received regular mention in the literature and are used in evaluating health information quality on social media and (2) social media platforms that have had specific quality criteria concerns. In all, the most frequently studied health information quality criterion in relation with SMHI is the source (Table 2). The sub-criterion, source, which is part of a set of criteria used in determining credibility of Internet health information generally looks at the provision of key metadata such as the individual author’s qualification or the official logo of the institution providing the health information, as a way of defusing user doubts about the credibility of the information. Other sub-criteria found in the literature under the major criterion credibility were currency, relevance and authorship (Table 2). By far, these four sub-criteria were the ones widely studied in relation to SMHI credibility. Note that there were instances where two or more evaluation criteria were used to evaluate the quality of SMHI (see references with * under Table 2). For instance, Şahin et al. (2019) evaluated the quality of health information on YouTube using the criteria source, credibility, content and reliability in the examination, diagnosis and the treatment of retinopathy of prematurity.
Information quality criteria.a
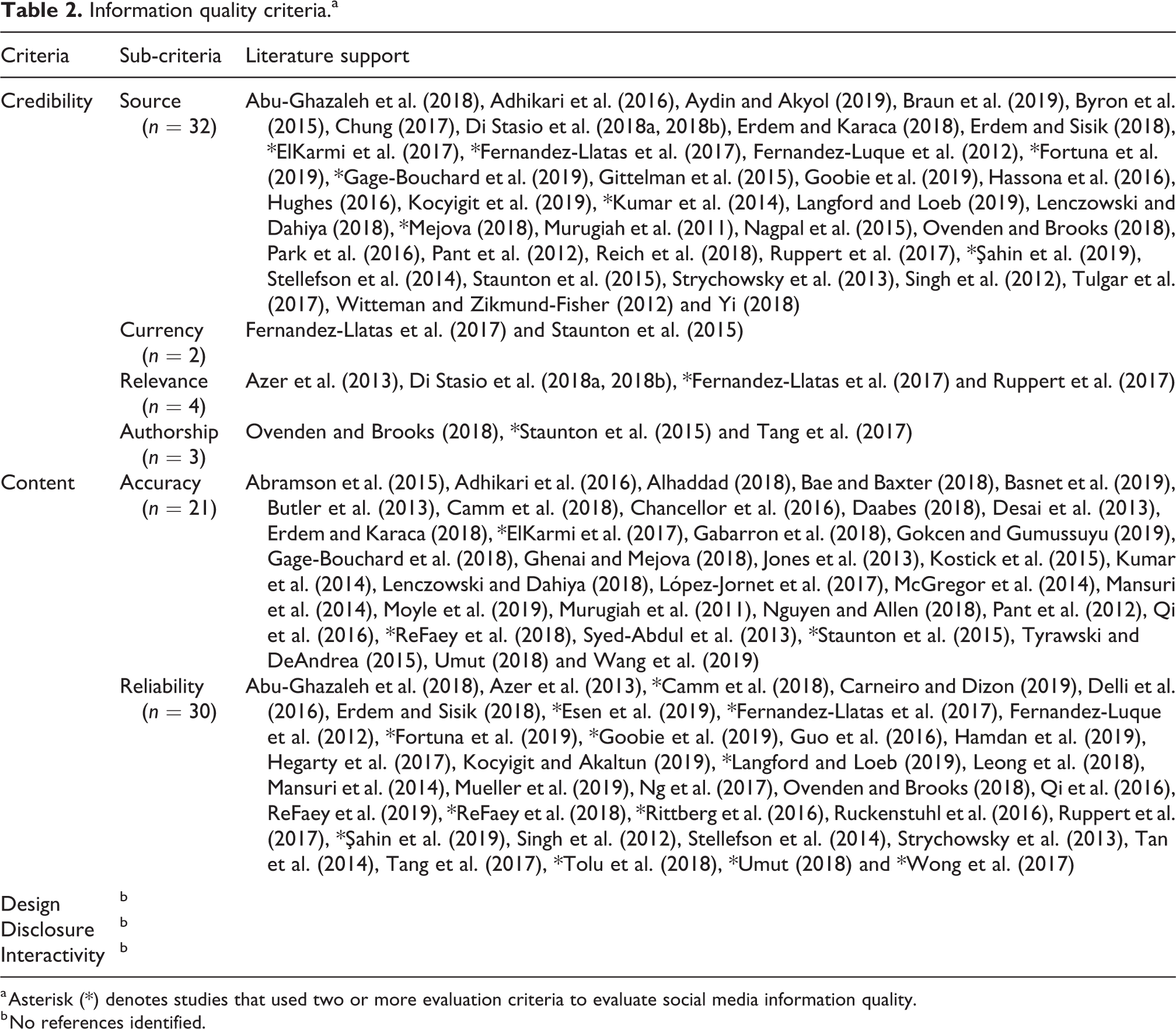
a Asterisk (*) denotes studies that used two or more evaluation criteria to evaluate social media information quality.
b No references identified.
In respect of the major criterion, content, the most studied information quality sub-criterion used in determining the quality of SMHI was accuracy, followed by reliability (Table 2). YouTube, Twitter, Facebook, Instagram and WeChat were social media platforms studied in relation to health information quality. A number of studies empanelled scientific experts to evaluate accuracy of health contents, especially those published on YouTube. Issues of poor video content, misinformation, half-truths as well as contents with commercial intent were frequently discussed. Studies by ElKarmi et al. (2017) and Şahin et al. (2019) compared YouTube content published by generalist information platforms and health professionals and strongly advocated for health professionals to play active role on social media so as to help correct misleading health information. In all, YouTube was the most discussed social media platform, followed by Facebook and Twitter, in relation to SMHI quality criteria. An observation in the review was that while the credibility of SMHI has been extensively studied on YouTube, it has received little or no attention on Facebook, Instagram and WeChat (Table 2).
Quality evaluation instrument
In this section, the literature review focused on evaluation instruments that have been applied to SMHI and how the evaluation is methodically carried out. Besides popular evaluation instruments such as JAMA, DISCERN, HONcode, LIDA, AHRQ and FKGL, other evaluation instruments were found in the literature. These were the Global Quality Scale (GQS), HealthTrust (Fernandez-Luque et al., 2012), Patient-Provider Communication Composite Score
Quality evaluation instruments.a
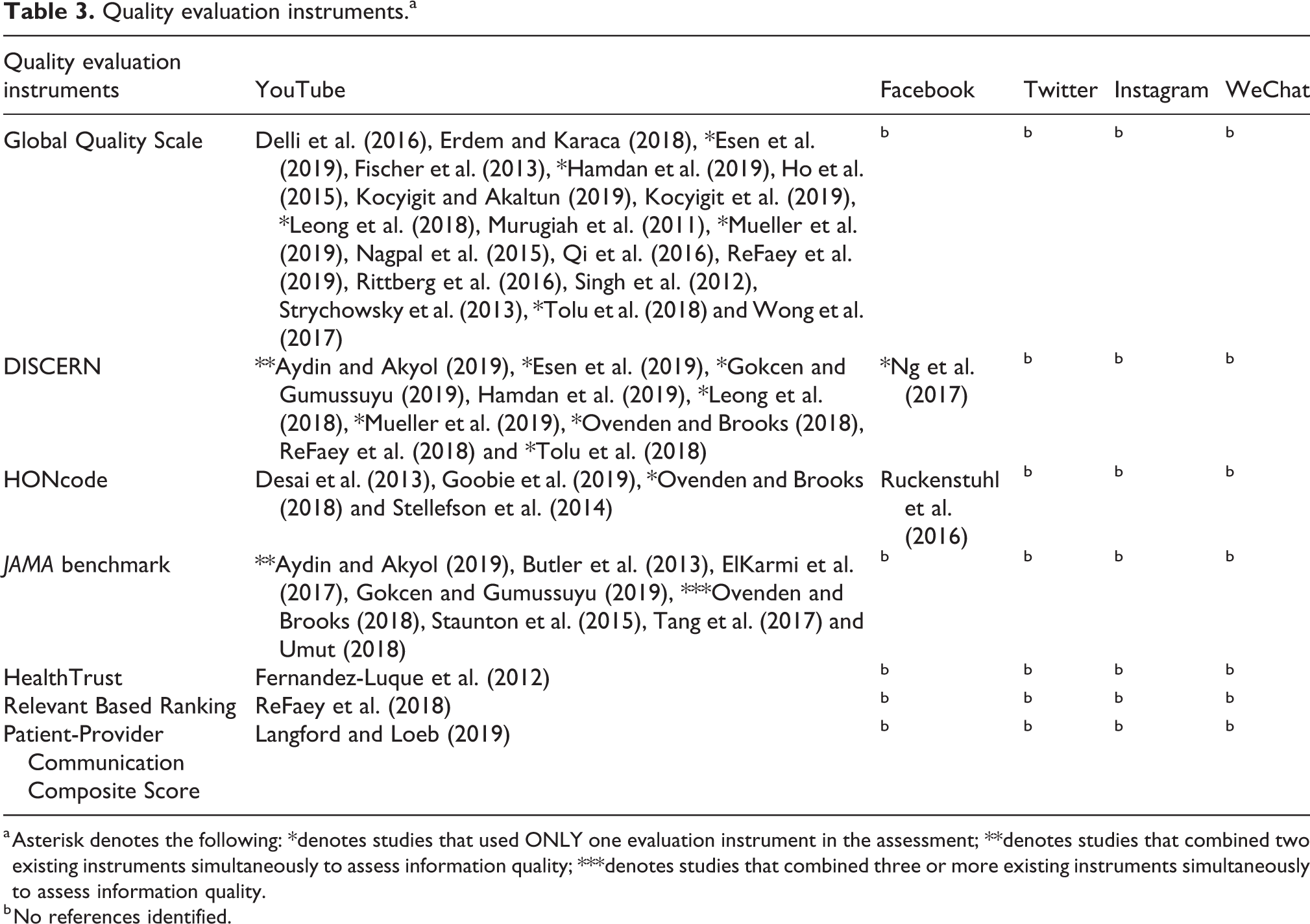
a Asterisk denotes the following: *denotes studies that used ONLY one evaluation instrument in the assessment; **denotes studies that combined two existing instruments simultaneously to assess information quality; ***denotes studies that combined three or more existing instruments simultaneously to assess information quality.
b No references identified.
Discussion
Overall, the literature review found worrying concerns about the quality of SMHI. As expected, diseases that are life-threatening such as cancer and diabetes and which often bring anxiety to people raise the most quality concerns about SMHI. However, dental care, though not life-threatening, also received regular mention in terms of its poor information quality on social media. The literature uses terms such as fake, misinformation, misleading, inaccuracy, misapplication, half-truths, low-quality, poor content to describe SMHI, with the majority of such low-quality contents emanating from YouTube, as well as other generalist health information platforms and lay users. In view of this, health professionals, especially physicians, have been urged to (1) probe to find the kinds of information patients access on social media in order to help ascertain the quality and direct them to reliable sources; (2) educate patients and the general public on how to assess quality of health information resources; and (3) be active on social media to help defuse the spread of low-quality contents generated mostly by lay users and generalist information sources. The call on health professionals to be active agents in social media health communication is to help stop the cycle of health misinformation sharing among friend networks on social media (Antheunis et al., 2013; Şahin et al., 2019).
We also note that though attempts have been made to evaluate the quality of SMHI by researchers, few of the quality evaluation criteria (Box 1) have been a subject of focus in research studies. For instance, the results in this review show that while credibility and content have received mention in the literature, design, disclosure and interactivity criteria have yet to be studied in relation to SMHI. Currently, the criteria for evaluating SMHI are drawn from the JAMA, DISCERN, HONcode, AHRQ, LIDA and FKGL which were originally designed for traditional online platforms such as websites. It is therefore not surprising that most studies are not able to find use for other criteria since they appear not a good fit for SMHI quality evaluation. For instance, given the architectural design of social media, criteria such as design and interactivity may appear irrelevant for evaluation since they are fundamental to the concept of Web 2.0 applications and therefore are provided by default. However, unlike websites, social media information platforms do not often come with metadata such as author information, source of funding, year of publication, disclaimers and so on. In view of this, disclosure as a quality criterion may be suitable for SMHI quality evaluation and can be enforced. We therefore argue that given these disparities in terms of features between traditional websites and social media platforms, there is the need for separate evaluation criteria and appropriate instruments that focus solely on social media. Such SMHI evaluation criteria and instruments will take into consideration the nature and architecture of social media to propose criteria that are applicable to SMHI.
Major gaps in the literature identified in this study
Major information quality gaps in the literature pertaining to SMHI were identified in this review: The literature is so far silent on the appropriate use of hybrid quality evaluation instruments (use of two or more quality evaluation instruments). For instance, when is it appropriate to combine quality criteria such as the JAMA, DISCERN, HONcode in a single study and how reliable would the results be? We argue that since each evaluation instrument, whether JAMA, DISCERN or HONcode, has a slightly different objective, future research has to demonstrate when and how such hybrid evaluation instruments are appropriate. Additionally, there are a number of predetermined platform-specific quality metrics that are arbitrarily used by authors. For instance, while some studies use video metrics such as video length, total views, number of comments, likes and dislikes to determine quality of the information, other studies use the nature of the video, whether professionally produced or amateur, and the source of the video, whether it has commercial intent or otherwise, to determine quality. These platform-specific attributes must be standardised. Additionally, instances where YouTube video metrics such as number of views, likes or comments are used to determine information quality must be further investigated since such metrics are in most cases only indicative of the “popularity” of the content and not a measure of the quality of the content in terms of either its accuracy or reliability for a health condition. The review revealed that current SMHI quality evaluation is skewed or biased towards YouTube and Facebook. As other platforms emerge for social media health communication such as WhatsApp, Instagram, WeChat and other country-specific social media platforms, more research needs to be carried out to bring other perspectives to SMHI quality issues. Given that existing online health information quality evaluation criteria and instruments were designed before the advent of social media, future research must explore designing and testing criteria and instruments that match the technical and user characteristics of social media platforms. The abundance of SMHI may naturally lead to sophisticated information seekers. There would then be the need to study how SMHI users make decisions regarding quality information. Thus, focus could be on the decision-making abilities of the SMHI consumer and how they find and evaluate quality health information.
Conclusion
The casual, loose and self-disclosing nature of social media results in varying degrees of information quality, especially in health communication. Social media’s capacity to present content in new contextual forms and from varied authors makes it even more difficult to determine the authority, reliability and accuracy of its health information. This review, which focuses on health information quality concerns on social media, was therefore intended to stir up interest and illuminate discussion on health information quality on social media. Overall, researchers have shown grave concerns about the quality of SMHI, especially on cancer treatments and surgical procedures. YouTube received the most traction in the literature as far as the quality of its health information and communication was concerned. Health information authored by lay users and generalist information portals on social media raised the most information quality concerns. In view of this, a significant number of the articles reviewed have called on medical practitioners and health institutions to be actively involved in health communication on social media, not only to create awareness but also to dispel false medical information that has the potential of spreading in a social network. The review also sheds light on the information quality criteria and instruments currently being used in determining quality of SMHI. Thus, we argue that future studies need to focus on designing unique quality evaluation criteria and instruments specific to social media. Lastly, the review opens up the space for other researchers to investigate the information quality dimensions of other diseases, disorders and ailments as well as health treatment options that continue to generate discussion among social media users. Though YouTube health videos have been extensively studied in the literature, this review posits that future research needs to investigate whether the platforms by their design also contribute to information quality abuses and general concerns.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Queen Elizabeth II Diamond Jubilee Scholarship (QES) at McGill and Carleton University, Canada.