
Abstract
Objective:
To determine whether tranexamic acid (TXA) reduces blood loss and transfusion rate in single-stage bilateral combined surgery for developmental dysplasia of the hip (DDH) in children.
Methods:
A retrospective study was conducted on 148 children with bilateral DDH who underwent single-stage bilateral combined surgery between March 2021 and May 2025. Patients were categorized into a TXA group (n = 71) and a control group (n = 77) based on TXA administration. The TXA group received a single intravenous bolus of TXA 15 mg/kg preoperatively, while the control group received no intervention. Complete blood count tests were obtained preoperatively and at 24 h postoperatively. Estimated blood loss (EBL), transfusion rate, operative duration, and complications were compared.
Results:
The TXA group exhibited significantly lower EBL compared with the control group (117.5 ± 7.7 mL vs. 171.4 ± 11.3 mL; p < 0.001). The total transfusion rate was also lower in the TXA group (5.6 % vs. 16.9 %; p = 0.03), as well as the intraoperative transfusion rate (1.4% vs. 11.7%; p = 0.03). The median surgical duration was 2.3 h in both groups, with no significant difference (p = 0.29). One postoperative infection occurred in each group (1.4 % vs. 1.3 %; p = 1), and no cases of seizures or deep vein thrombosis were observed.
Conclusions:
TXA significantly reduces EBL and both total and intraoperative transfusion rates in children undergoing single-stage bilateral combined surgery for DDH, without affecting the risk of complications.
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is a prevalent pediatric orthopedic disorder and a common cause of adult-onset hip osteoarthritis and total hip arthroplasty if not treated appropriately.1 –3 This condition involves structural deformities, morphological alterations, and positional deviations of the acetabulum, femur, and surrounding soft tissues.4 –6 In 1961, Salter introduced the innominate osteotomy to address anterolateral acetabular deficiencies in DDH. 7 By rotating the acetabulum around the pubic symphysis, this technique enhances anterior-lateral coverage of the femoral head. Extensive clinical validation has established Salter innominate osteotomy (SIO) as one of the standard acetabular redirectional surgeries for DDH management. 5
Approximately 35.5% of children with DDH present with bilateral involvement. 8 For eligible patients, single-stage bilateral combined surgery, including SIO, open reduction, and femoral shortening osteotomy, offers several advantages over staged procedures, including shorter rehabilitation time, lower overall treatment costs, and greater parental satisfaction, while maintaining comparable therapeutic efficacy.9,10 A biomechanical study has also demonstrated no significant differences in pelvic stability between single-stage bilateral and unilateral SIO. 11 However, the bilateral combined procedure is associated with prolonged operative duration, increased intraoperative blood loss, and higher transfusion requirements. 9
Tranexamic acid (TXA), a synthetic lysine analog, competitively occupies the lysine-binding sites of plasminogen, thereby preventing the binding of plasminogen to fibrin and inhibiting fibrinolysis. 12 It has been shown to significantly reduce intraoperative blood loss in adult orthopedic procedures without increasing the risk of complications.13 –15 In pediatric orthopedic surgery, TXA has primarily been used in procedures related to cerebral palsy. However, its clinical applications in children with DDH remain inadequately explored. This study aims to investigate the efficacy of TXA in controlling blood loss in single-stage bilateral combined surgery for DDH in children.
Methods
This study was a retrospective cohort analysis approved by the Institutional Review Board of West China Hospital, Sichuan University (approval No. IRB 21-588). Due to its retrospective nature and the use of anonymized data, the requirement for informed consent was waived. We leveraged the hospital’s comprehensive big-data research platform—which houses the full medical records of every patient—to identify cases. By filtering for the diagnosis “bilateral DDH,” age “2–6 years,” and visit date “March 2021–May 2025,” we extracted the cohort and systematically reviewed each patient’s complete medical chart. Inclusion criteria: (1) bilateral DDH confirmed by standard anteroposterior pelvic radiographs; (2) single-stage bilateral combined procedure; (3) pelvic osteotomy performed as SIO; (4) Tönnis grade III or IV; (5) American Society of Anesthesiologists (ASA) classification of grade I or II; (6) age 2–6 years; (7) complete clinical data. Exclusion criteria: (1) revision surgery; (2) staged surgery; (3) non-combined procedure; (4) pelvic osteotomy performed as Pemberton; (5) pathological or neuromuscular hip dislocation; (6) history of hematologic disorders or coagulation abnormalities; (7) preoperative hemoglobin (Hb) less than100 g/L; (8) incomplete clinical data. After retrospective review of the medical records, patients were stratified into a TXA group and a control group according to whether the agent was administered.
The administration of TXA was determined by a combination of the surgeon’s recommendation and the anesthesiologist’s preference. For every patient, surgeons advised the anesthesiologists to administer TXA. However, some anesthesiologists remained concerned about its safety and declined to administer it. Therefore, the anesthesiologists made the final decision on whether to give TXA. Patients in the TXA group received a single intravenous bolus of TXA 15 mg/kg 10 min before skin incision, while the control group received no additional intervention. Three surgeons with comparable experience performed these procedures, each with more than 17 years of specialized pediatric orthopedic expertise and over 11 years of DDH surgical experience. All procedures were performed under general anesthesia. First, an adductor tenotomy was carried out. A bikini incision was then used to expose the ilium and hip joint. A T-shaped capsulotomy was performed, and intra-articular soft tissues obstructing hip reduction were excised. A proximal femoral shortening osteotomy was performed in every patient, with additional derotation when required. The acetabulum was reoriented using a SIO, with the osteotomy gap filled with autologous iliac bone grafts and stabilized using Kirschner wires. The identical sequence was repeated on the contralateral side. Both hips were immobilized in a hip-spica cast for 8 weeks.
A full blood count was obtained preoperatively and at 24 h postoperatively. For patients with suspected anemia, full blood count was performed immediately and a repeat test was still conducted at 24 h postoperatively. Demographic and clinical data, including gender, age, Tönnis classification, ASA classification, preoperative and postoperative Hb levels, transfusion requirement, and complications, were collected.
Primary outcome measures were estimated blood loss (EBL) and transfusion rate, and secondary outcomes included surgical duration and complications. EBL was calculated with the formula: 16 EBL (mL) = estimated blood volume (mL) × (preoperative Hb—postoperative Hb)/preoperative Hb + transfused blood volume (mL), where estimated blood volume (mL) = weight (kg) × 75 (mL/kg). Transfused blood volume was defined as the volume of packed red blood cells administered. The indication for blood transfusion was based on Hb levels less than 70 g/L or symptoms associated with anemia, such as dizziness, tachycardia, and hypotension. Perioperative fluid dilution was minimized via standardized fluid management: all patients received isotonic crystalloid intraoperatively, with the fluid infusion volume calculated as the sum of maintenance volume (4 mL/kg/h for the first 10 kg, 2 mL/kg/h for the subsequent 10 kg, 1 mL/kg/h for any weight exceeding 20 kg) and estimated fluid losses (4 mL/kg). Fluid intake was restricted to the maintenance volume during the first 6 h postoperatively. Oral intake was gradually initiated at 6 h postoperatively, with supplementation provided based on the deficit if intake was insufficient. Surgical duration was defined as the time from skin incision to wound closure.
Statistical analysis was conducted using SPSS27.0 (IBM Corporation, Armonk, NY, USA). Normally distributed continuous data were expressed as mean ± standard deviation and compared with the two-sample t test; nonnormally distributed continuous data were presented as median (interquartile range) and analyzed with the Mann–Whitney U test. Categorical variables were summarized as frequencies (%) and analyzed using the χ² test. A two-tailed p < 0.05 was considered statistically significant.
Results
During the study period, 156 patients underwent single-stage bilateral combined surgery (pelvic osteotomy performed as SIO). After excluding 8 with incomplete records, 148 patients were eligible for analysis: 71 in the TXA group and 77 in the control group. Mean age was 4.1 years in the TXA group and 4.3 years in the control group. No statistically significant differences were observed between groups in age, gender, weight, Tönnis classification, ASA classification, or preoperative Hb level (p > 0.05), confirming that baseline characteristics were well balanced (Table 1). All surgical procedures were completed successfully (Figure 1). The EBL in the TXA group was significantly lower than that in the control group (117.5 ± 7.7 mL vs. 171.4 ± 11.3 mL; p < 0.001). The total blood transfusion rate was also significantly lower in the TXA group (5.6% vs. 16.9%; p = 0.03). We further compared the intraoperative and postoperative transfusion rates. It demonstrated that the intraoperative transfusion rate was significantly lower in the TXA group (1.4% vs. 11.7%; p = 0.03), with no significant difference in the postoperative transfusion rate (4.3% vs. 5.9%; p = 0.97). The median surgical duration was 2.3 h in both groups, with no significant difference (p = 0.27). One patient in each group developed a postoperative infection, and no cases of seizures or deep vein thrombosis were reported in either group (Table 2).
Comparison of demographics between TXA group and control group.

TXA: Tranexamic acid; ASA: American Society of Anesthesiologists.
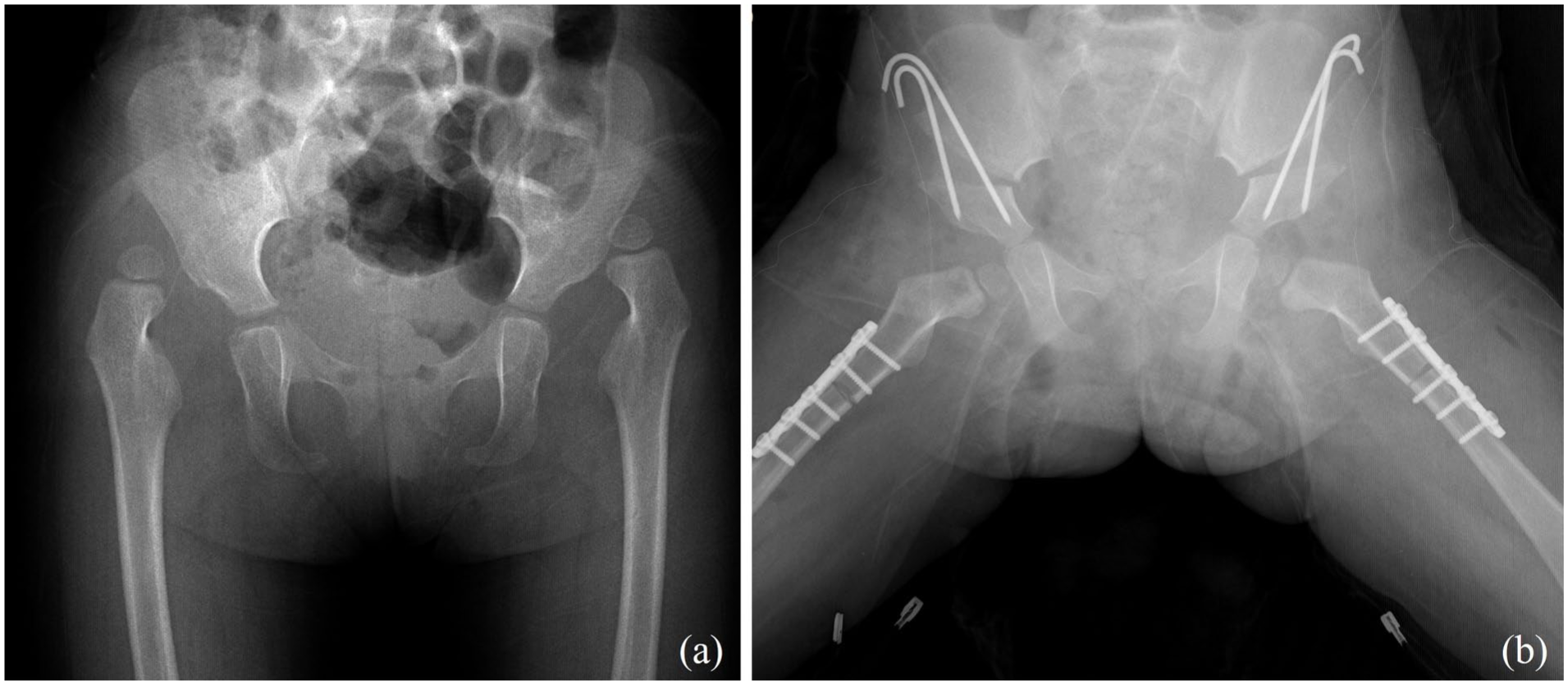
Anteroposterior pelvic radiographs of a 2.3-year-old girl with bilateral developmental dysplasia of the hip.
Comparison of outcome measures between TXA group and control group.

TXA: Tranexamic acid.
Statistically significant.
Discussion
Application of TXA in pediatric orthopedics is attracting growing interest, but its value remains contentious. A retrospective comparative study of proximal femoral varus derotational osteotomy in children with cerebral palsy reported lower overall and postoperative transfusion rates when TXA was used. 17 Similarly, a double cohort study found that TXA successfully reduced total blood loss and transfusion rates in cerebral palsy patients undergoing femoral varus derotational osteotomy. 16 A double-blind randomized controlled clinical trial demonstrated that TXA significantly reduced intraoperative bleeding in pediatric patients with cerebral palsy undergoing surgical treatment for hip instability. 18 Furthermore, a meta-analysis showed that TXA reduced the overall transfusion rate and total blood loss in children with cerebral palsy who underwent osteotomies. 19
Conversely, other work has failed to demonstrate a clear benefit. A study observed that while TXA showed a trend toward reducing transfusion requirements in cerebral palsy patients undergoing hip reconstruction, this effect does not reach statistical significance. 20 Besides, a matched comparative study indicated no significant differences in postoperative Hb levels, hospitalization duration, or transfusion rates between the TXA and control groups in children undergoing bony reconstruction for neuromuscular hip dysplasia. 21 These conflicting results suggest that the universal clinical benefits of TXA still require further validation.
In the present study, we administered TXA for patients undergoing single-stage bilateral combined surgery for DDH. We found that it significantly reduced the EBL, as well as the total and intraoperative transfusion rates. These findings support the efficacy of TXA in this specific setting, where bilateral simultaneous osteotomies impose a substantial hemorrhagic burden. The half-life of TXA is approximately 2 h, 22 whereas the duration of our surgical procedures generally exceeds that. The absence of a significant reduction in postoperative transfusion rate may be attributable to the use of a single preoperative bolus without a maintenance dose, allowing the drug effect to wane over time.
TXA is typically safe for use in pediatric orthopedic procedures and does not increase the risk of complications. 23 Similar to previous reports, our study found that TXA did not increase the risk of infection, seizures, or deep vein thrombosis. The fibrinolytic system and immune system are intertwined processes. The administration of antifibrinolytic agents in catheterized mice induces catheter-associated urinary tract infections and systemic dissemination. 24 Given the small sample size of both previous studies and our own, the infection risk requires continued monitoring in large cohorts. Additionally, a meta-analysis indicates that systemic TXA administration increases the risk of seizures, 25 though this complication was not observed in our study. In contrast, topical TXA, applied directly to the surgical site, achieves local haemostasis with minimal systemic absorption, potentially reducing seizure risk. Future studies could compare systemic and topical TXA in DDH surgery to determine the optimal route of administration.
The optimal TXA dosing regimen in pediatric orthopedics remains unclear. In hip or spinal surgeries for children with cerebral palsy, two TXA administration protocols are used. One protocol involves a single intravenous bolus before surgery begins, while the other includes a loading dose before surgery followed by an intravenous infusion during the procedure.17,18,20 The loading dose ranges from 5 to 100 mg/kg, and the maintenance dose ranges from 1 to 10 mg/kg/h. 23 The varying efficacy of TXA across studies may be related to these differences in administration protocols. A meta-analysis of 57 studies including 5698 adults showed that a single preoperative intravenous dose of TXA reduced the probability of transfusion by 72 %, and the most common dose employed across studies was 15 mg/kg. 26 In our study, we administered a single intravenous bolus of TXA at 15 mg/kg before surgery without a maintenance dose. This protocol effectively reduced EBL and transfusion rate in single-stage bilateral combined surgery for DDH. A double-blind randomized controlled trial of hip reconstruction in children with cerebral palsy found that a single preoperative intravenous dose of 10 mg/kg effectively reduced intraoperative blood loss. 18 Therefore, the optimal dose of TXA in pediatric orthopedic surgery still requires further investigation.
Our cohort consisted of 148 children with DDH who required combined surgery after a delayed diagnosis. This indicates that the neonatal screening program remains inadequate in the corresponding referral region. The neonatal screening particularly ultrasound screening, constitutes a crucial strategy to reduce the rate of late diagnosis, diminish the need for surgical intervention, and improve long-term clinical outcomes. Selective ultrasound screening reduced the late diagnosis rate of DDH from 2.2/1000 to 0.34/1000. 27 Since the nationwide universal ultrasound screening program was launched in Austria in 1992, prospective studies have confirmed that this initiative has decreased both the rate of open reduction and the incidence of subsequent revision surgery. 28 Although several economically developed Chinese cities have provided free DDH ultrasound screening program since 2008, an effective system remains absent in less-resourced regions, including our own. Establishing a standardized, region-wide DDH ultrasonographic screening program is therefore an urgent priority for our current practice. In addition, the large population base, together with the allure derived from the advantages of one-stage bilateral surgery, has also contributed to the concentration of bilateral DDH patients in our institution.
This study has several limitations. Despite modifications for transfusion and standardized fluid management, EBL was calculated using a Hb-based formula, which may not have accurately reflected the true blood loss. The 24-h postoperative Hb measurement reflects both intraoperative bleeding and early postoperative bleeding, as well as potential hemodilution from perioperative fluids. Thus, the EBL calculation cannot isolate intraoperative blood loss. Future studies using direct intraoperative blood loss measurement combined with serial Hb monitoring may provide more precise differentiation. The retrospective, nonblinded design raises the possibility of selection bias in transfusion decisions. However, transfusion indications were strictly protocolized and uniformly applied to both groups, minimizing this bias. Future prospective, double-blinded studies are needed to confirm our findings without potential observer bias. While some studies have indicated a significant relationship between TXA dosage and reductions in intraoperative blood loss and transfusion requirements, 29 this study did not explore the dose–response relationship, making it impossible to determine the optimal dose.
Despite these limitations, this study provides promising preliminary findings on the use of TXA in single-stage bilateral combined surgery for DDH. Preoperative administration of a single 15 mg/kg intravenous bolus of TXA significantly reduces EBL, as well as total and intraoperative transfusion rates compared with no TXA. TXA does not affect surgical duration or the risk of complications. These findings support the use of TXA for hemostasis in this high-bleeding-risk pediatric orthopedic procedure. Future studies should further refine the study design through large-scale, multicenter, prospective randomized controlled trials to explore the optimal TXA administration protocol, with the goal of offering safer and more effective treatment options for pediatric orthopedic surgery patients.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261429003 – Supplemental material for Tranexamic acid reduces blood loss and transfusion in single-stage bilateral combined surgery for developmental dysplasia of the hip: A retrospective study
Supplemental material, sj-pdf-1-cho-10.1177_18632521261429003 for Tranexamic acid reduces blood loss and transfusion in single-stage bilateral combined surgery for developmental dysplasia of the hip: A retrospective study by Shiwei Li, Xueyang Tang and Xiaodong Yang in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
We express our gratitude to statistical expert Ting Wang from the Clinical Research Management Department of West China Hospital, Sichuan University, for providing us with professional statistical advice.
Author contributions
Shiwei Li: Data curation, formal analysis, Investigation, and writing-original draft; Xueyang Tang: Data curation, formal analysis and Investigation; Xiaodong Yang: Conceptualization, investigation, methodology, and supervision, writing—review & editing.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.*
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Clinical Research Incubation Project of West China Hospital of Sichuan University(2020HXFH017).
Ethical considerations
This study was approved by the Institutional Review Board of West China Hospital, Sichuan University (approval No. IRB 21-588). Due to its retrospective nature and the use of anonymized data, the requirement for informed consent was waived.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.