
Abstract
Objective
This study aimed to characterize health literacy among adults with brachial plexus birth injury (BPBI) and identify challenges and opportunities to improve BPBI care for affected adults.
Methods
A prior multiphase, mixed methods outcomes study of adults with BPBI identified health literacy as salient factor needing further analysis. The current convergent mixed methods secondary analysis thus combined relevant quantitative and qualitative data from this prior study specifically to analyze health literacy in this population. Quantitative data included five scales of the Health Literacy Questionnaire (HLQ) (n = 147). Qualitative data included open-ended survey responses (n = 183) and individual interviews (n = 12). The qualitative data from the surveys and interviews were combined and coded. Then qualitative data and quantitative data were merged in joint displays, utilizing the qualitative data to expand on the quantitative findings.
Results
Mean HLQ scores were midrange with wide standard deviations. Corresponding qualitative data tended to cluster at the negative and positive extremes. Negative health literacy experiences revealed opportunities for improving care for affected adults, while positive experiences provided examples to guide such improvement.
Conclusion
Health literacy varies among adults with BPBI. In this variability lie opportunities for improving overall care for affected individuals throughout the lifespan.
Introduction
Brachial plexus birth injury (BPBI) is an injury to the nerves of the brachial plexus during birth, leaving affected individuals with temporary or permanent paralysis of one or both arms. This injury occurs in approximately one to three live births per 1000. 1 Spontaneous recovery is possible within the first several months of life; yet 20 to 30% of children experience some degree of permanent limitation in arm mobility and/or sensation.2,3 In cases without spontaneous resolution, additional musculoskeletal sequelae occur, including contractures, joint deformity/dislocation, and altered arm growth.3,4 A variety of therapeutic and surgical interventions are used to address these sequelae, but none are curative, leaving many children with permanent neuromusculoskeletal consequences of BPBI. 5 Among adolescents with BPBI, pain and negative coping strategies have been identified as risk factors for mental health concerns. 6 Furthermore, participation restrictions and distress with body image can negatively impact health related quality of life (HRQoL) in affected adolescents. 7
Despite knowledge of negative HRQoL impacts of BPBI among affected adolescents and the permanent nature of BPBI sequelae, relatively little attention has been paid historically to the impact of BPBI into adulthood. To fill this knowledge gap, a recent international, multi-phase mixed methods study (
Addressing this mismatch requires investigating relationships between affected individuals and healthcare resources. An appropriate theoretical framework in which to do so is the concept of health literacy, defined as an individual's ability to access health information and act to improve their health. 11 Health literacy is broader in scope than medical literacy, which refers to an individual's ability to read and understand written medical information. 12 The health literacy of adults in the United States was identified as a problem impacting the quality and cost of healthcare two decades ago. 13 Because health literacy is perceived to empower patients toward improving their quality of life, scholars have declared that health literacy should be a shared responsibility of patients as well as healthcare professionals to the point of being a social norm.12,14,15
The development of tools for health literacy research has accompanied the heightened focus on the importance of health literacy in recent years. In 2008, an international consortium of scholars at the 36th Annual North American Primacy Care Research Group developed an agenda for health literacy which included the need for 1) tools to measure health literacy, and 2) research to be grounded in common theory and conceptual frameworks of health literacy to facilitate international comparison studies. 16 The development of the Health Literacy Questionnaire (HLQ) followed. Patients with chronic medical conditions participated in developing the conceptual framework for the HLQ by describing their experiences and concerns with accessing and applying medical information and services. 17 The psychometrics of the HLQ were then established 18 and the tool has been applied to investigate health literacy among adults with a variety of chronic medical conditions.19–22
Five HLQ scales were among the PROMs identified as relevant in the LEAP study, underscoring the saliency of health literacy in this population. The current secondary data analysis was performed to characterize health literacy among adults with BPBI using qualitative and quantitative data from the LEAP study in a convergent mixed methods approach. 23 The purpose of the current analysis was to identify challenges and opportunities to improve BPBI care for adults with the condition.
Methods
This convergent mixed methods analysis combined health literacy information from three LEAP study phases: (1) survey, (2) interview, and (3) PROMs (Figure 1). For the current secondary data analysis, the qualitative healthcare experience data included two LEAP sources: (1) open-ended survey responses and (2) interview data. The quantitative HLQ data included scores for the five HLQ scales administered in the PROMs phase. Following the logic of a convergent mixed methods approach, 23 the qualitative healthcare experience data and the quantitative HLQ data were analyzed independently of one another and with equal priority. Then the datasets and results were merged by the dimensions of health literacy for joint interpretation so that the qualitative results could expand on the quantitative findings. 24 Through the mixed methods analysis, a complete picture of health literacy among adults with BPBI was sought by applying the complementary qualitative results to extend the breadth of the interpretations beyond the quantitative HLQ mean scores.25,26
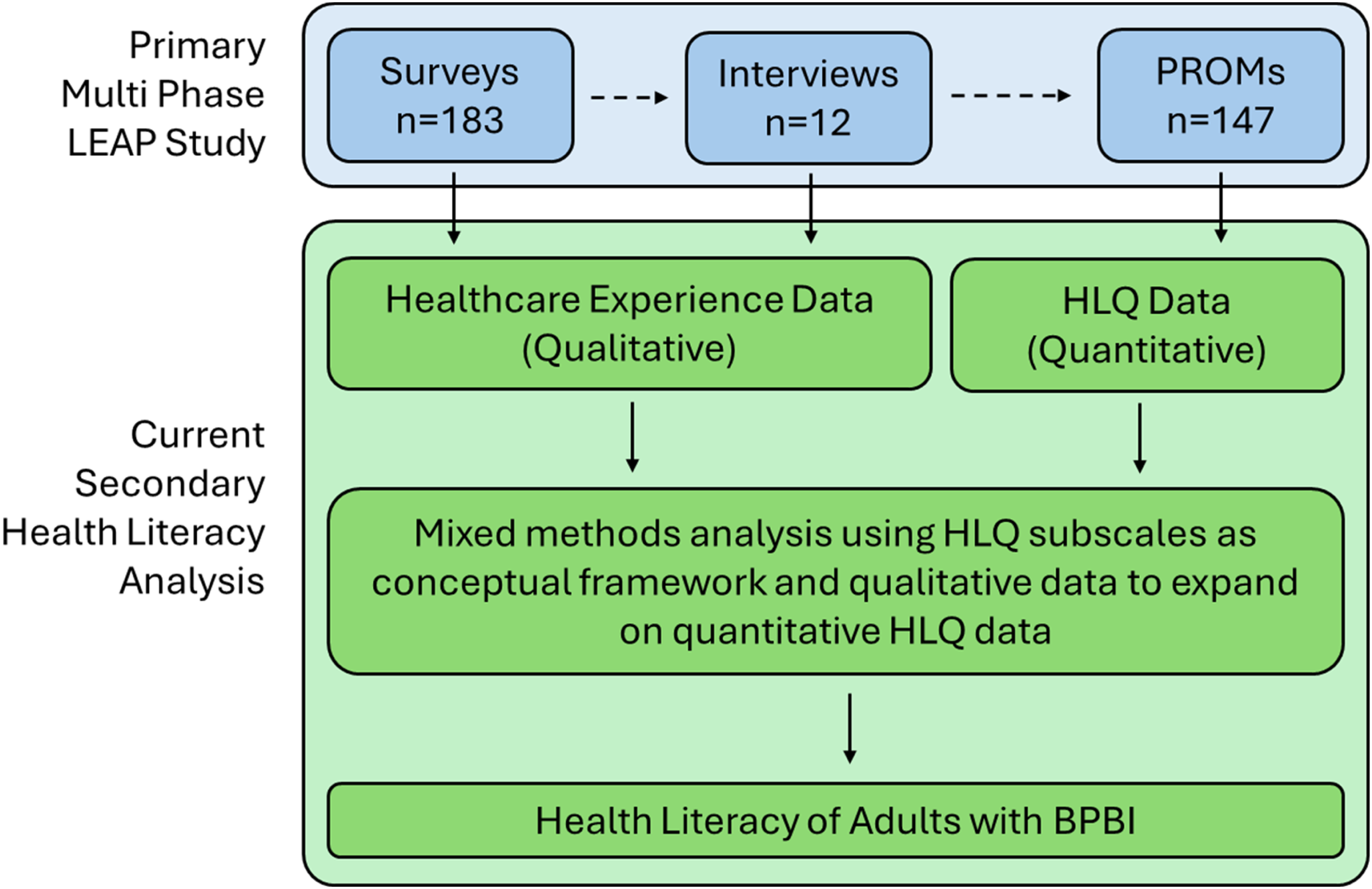
Convergent mixed methods health literacy analysis design.
Population
The Institutional Review Board of a pediatric academic medical center approved the primary multi-phase LEAP study. Participants were recruited from two international online BPBI support groups and were screened to ensure only inclusion of individuals 18 years old and older, who were fluent in English, with a brachial plexus injury acquired during birth.
Data sources
Data for the current analysis were retrieved from the qualitative and quantitative datasets generated in the three LEAP study phases (Figure 1). Two sources of qualitative data were generated in the initial two phases. First, in the survey phase, an electronic survey (N = 183) of open- and close-ended questions was posted on two social media pages of BPBI-affected adults to gather broad information regarding participants’ HRQoL and healthcare experiences (survey data). 9 Second, in the interview phase, a maximum variation sampling strategy was applied to derive a sample of 12 participants from the survey respondents who engaged in individual semi-structured interviews (see Dorich et al. 2024 for the detailed strategy). 8 The interviews were conducted to gain deeper perspective about participants’ HRQoL and healthcare experiences (interview data). 8 The combined LEAP survey and interview data comprise the qualitative healthcare experience data examined in the current analysis.
The quantitative HLQ data were generated in the final phase of the LEAP study. The PROMs phase involved administering PROMs to BPBI-affected adults (N = 147) to quantify the population's HRQoL outcomes. To identify which PROMs to use, qualitative survey and interview data were converted to International Classification of Functioning, Disability and Health (ICF) codes using ICF linking (i.e., matching alphanumeric codes in the ICF to qualitative data).27–30 Two researchers with experience in ICF linking coded the qualitative survey and interview data into meaningful concepts and linked these meaningful concepts to ICF alphanumeric codes. These ICF codes were weighted by the number of times each corresponding meaningful concept appeared in the qualitative data. Because the survey data set had a larger number of meaningful concept instances than the interview data due to its larger sample size, frequency distributions of the weighted ICF codes were performed separately for each dataset. Then, to combine the two datasets, the frequencies of each ICF code were averaged between the two datasets to determine the final frequency distribution for the pooled qualitative data. The most frequently occurring ICF codes of the combined data were then utilized to determine the most relevant PROMs to use for the third phase of the LEAP study by matching the high frequency ICF codes to the published ICF linking of candidate PROMs. 31 Relevant to healthcare experience, the combined survey and interview data linked to five of the nine HLQ scales (Table 1). In the PROMs phase of the LEAP study, these five HLQ scales along with the other PROMs identified through ICF linking were then administered through an electronic link posted on the same two social media groups of BPBI-affected adults (HLQ data).
Health literacy questionnaire scales used for the LEAP PROMs phase.
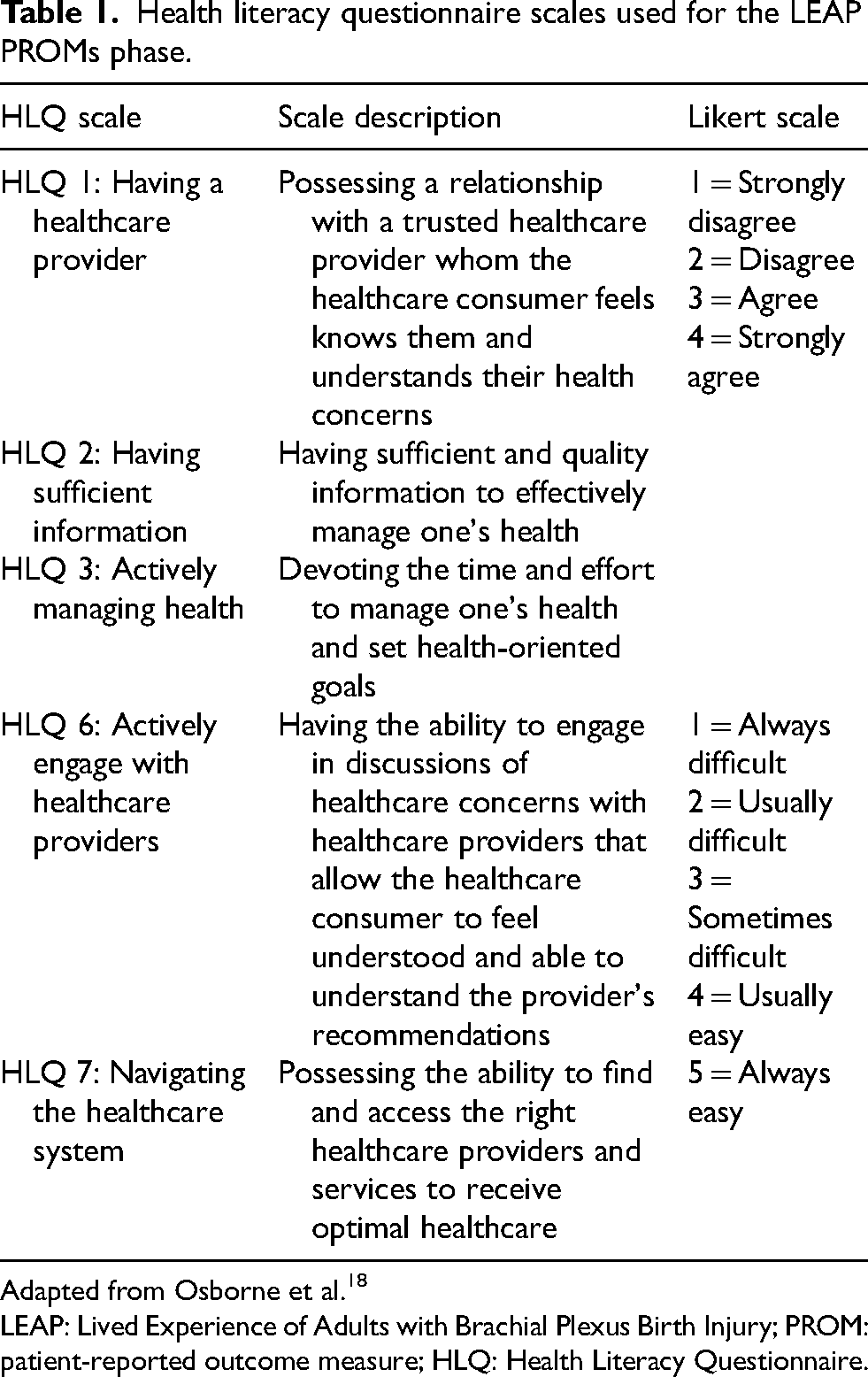
Adapted from Osborne et al. 18
LEAP: Lived Experience of Adults with Brachial Plexus Birth Injury; PROM: patient-reported outcome measure; HLQ: Health Literacy Questionnaire.
HLQ
The HLQ has nine subscales for measuring various aspects of health literacy. 18 Subscales 1–5 have a four-point response scale, ranging from 1 = strongly disagree to 4 = strongly agree. Subscales 6–9 have a five-point response scale, ranging from 1 = cannot do or always difficult to 5 = always easy. Normative scores are not available for the HLQ. In the LEAP study PROMs phase, the HLQ subscales which matched the data from the survey and interview phases were used. Thus, the current analysis includes HLQ scores for subscales 1–3 and 5–6 (Table 1).
Data analysis
The current analysis applied the World Health Organization's definition of health literacy, i.e., an individual's ability to access health information and act to improve their health, as a theoretical framework for data analysis. 11 Qualitative and quantitative data pertaining to the population's healthcare experiences from the three phases of the LEAP study were used to assess the health literacy of adults with BPBI in the current secondary data analysis. Qualitative survey and interview data were combined (i.e., healthcare experience data) and imported into MaxQDA 2020 (VERBI Software, 2019) 32 for analysis of all qualitative data pertaining to the population's health literacy. 23 Two researchers (JW and JD) derived a qualitative coding scheme aligned with the five HLQ scales used for data collection in the PROMs phase of the LEAP study and independently coded the healthcare experience data. Then they met to bring consensus to the coding with a third researcher (RC) serving as an arbitrator to resolve differences in consensus building. Coded data were then reviewed by the three researchers (JW, JD and RC) to identify main concepts associated with the five HLQ scales and relevant participant quotes.
For the quantitative analysis, mean scores, standard deviations (SDs), and confidence intervals were calculated for the five HLQ scales assessed in the PROMs phase. The results from the qualitative healthcare experience data and quantitative HLQ data were integrated and compared side-by-side for each of the five health literacy dimensions in two joint displays so that qualitative results could be used to expand on quantitative findings. 33 The full research team analyzed the joint displays in multiple meetings to derive the mixed methods interpretation of the integrated data.33,34
Results
Participant demographics for the three phases of the primary LEAP study are summarized in Table 2. A wide age range of BPBI-affected adults participated in all three rounds of data collection. Respondents were predominately female for the two electronic surveys, while a more equal distribution of male and female participants participated in the interview phase as a result of the maximum variation sampling technique for participant recruitment in the interview phase of the LEAP study.
Participant demographics for each phase of the LEAP study.
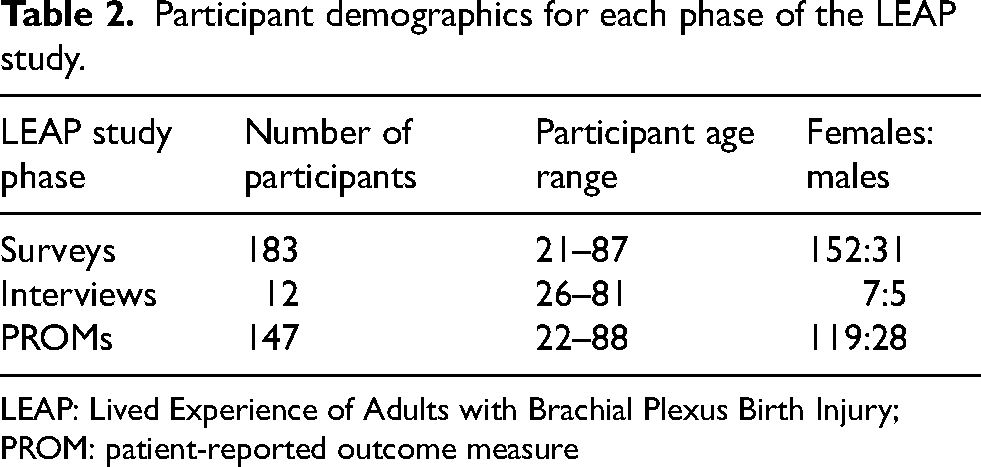
LEAP: Lived Experience of Adults with Brachial Plexus Birth Injury; PROM: patient-reported outcome measure
Table 3 is a mixed methods results joint display, organized by the five HLQ scales used in this analysis. It includes the quantitative HLQ data and the main concepts derived from the qualitative health experience data arranged side-by-side for data comparison. The research team's analysis of the integrated data is in the Mixed Methods Interpretation column. Overall, the mean scores for all HLQ scales were mid-range with notable variation as evidenced by the large SDs and confidence intervals. Analysis of the distributions revealed unimodal distributions about the means rather than a bimodal distribution of the data. The qualitative findings provide a more nuanced illustration of the range of experiences among the study sample for each health literacy domain. The qualitative findings either clustered as positive or negative experiences (HLQ 1, 2 and 6) or spanned a broad spectrum of experiences (HLQ 3 and 7) depending on the HLQ subscale.
Joint display of HLQ scores and healthcare experience data.
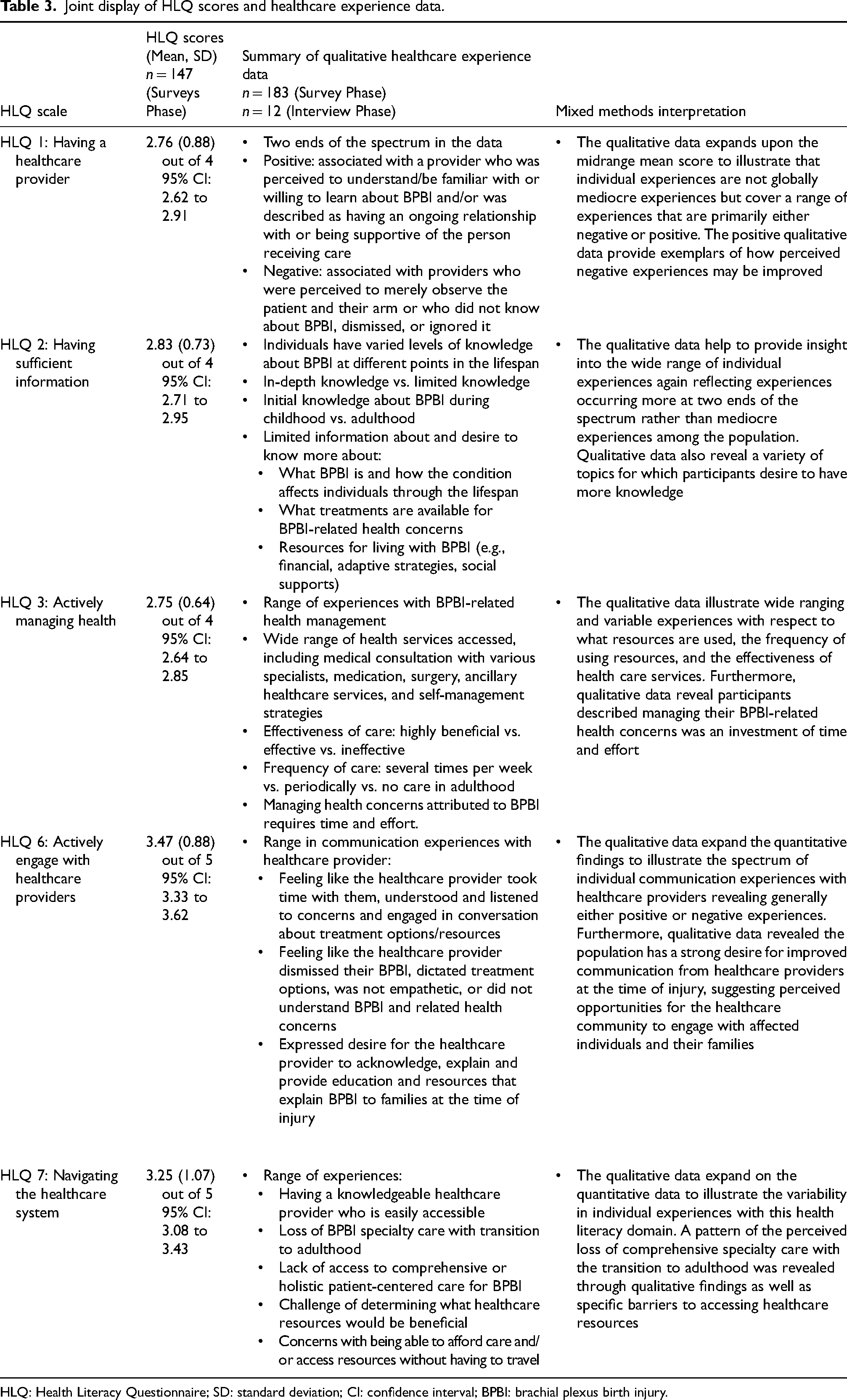
HLQ: Health Literacy Questionnaire; SD: standard deviation; CI: confidence interval; BPBI: brachial plexus birth injury.
Figure 2 further illustrates how the qualitative data expand on the quantitative data to provide a more complete picture of the study sample's health literacy experience. In Figure 2, color coding is applied such that the quantitative and qualitative data for a particular scale are depicted in the same color. The population's mean HLQ scores +/- one SD are plotted on the corresponding Likert scale placed beside individual participant quotes from the qualitative healthcare experience data that reflect the extremes of the positive or negative experiences discovered in the qualitative results. The range in variability of participant's BPBI health literacy is evident in the combined quantitative and qualitative data.
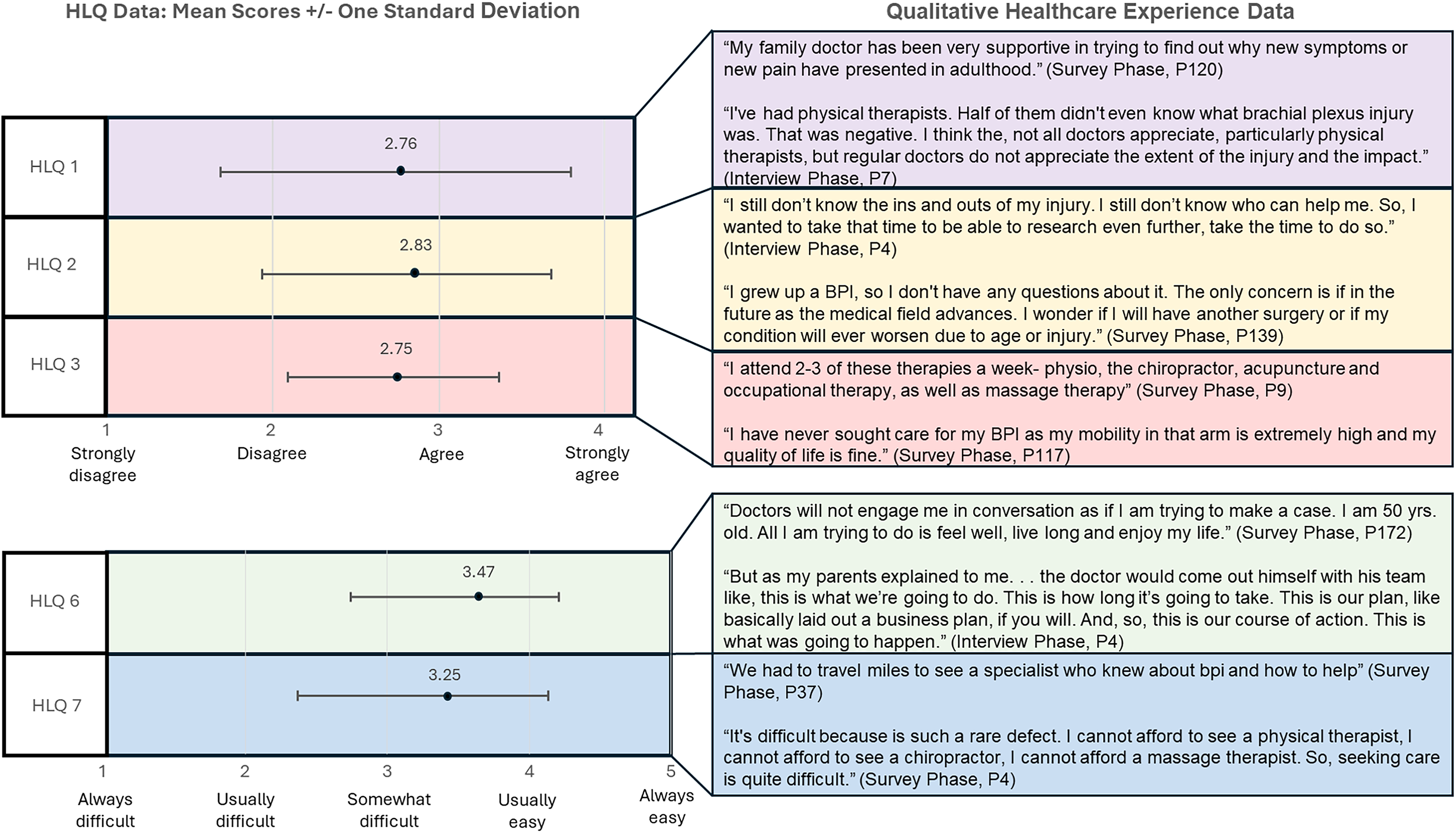
Quantitative and qualitative range of health literacy across HLQ scales.
Expanding on the mixed methods analysis of study findings, the findings for each HLQ scale are summarized. HLQ 1 Having a healthcare provider pertains to feeling that a healthcare provider relates to the healthcare consumer and their healthcare concerns. While the mean HLQ 1 score (2.76; SD 0.88) fell in a range on a four-point Likert scale that did not align with agreement or disagreement, qualitative data expand to illustrate experiences which were either positive or negative. Attributes of healthcare providers who fostered positive experiences include the healthcare consumer perceiving their healthcare provider demonstrates one or more of the following: (1) familiarity with BPBI, (2) willingness to learn about the condition, and/or (3) partnership with the healthcare consumer to know and understand their healthcare concerns and act to address them. Conversely, many respondents noted the experience of healthcare providers seeming dismissive of or unfamiliar with the healthcare consumer's BPBI and the associated sequelae and HRQoL impacts.
Similarly, the mean score for HLQ 2 Having sufficient information (2.83; SD 0.73) was in a range consistent with neither strong agreement nor disagreement. Questions on this scale pertain to the healthcare consumer's ability to obtain adequate information to effectively manage their healthcare needs. The qualitative data for this construct show that experience is varied regarding participant knowledge of BPBI, with participants indicating knowledge about their condition being either extensive or limited. Participants’ experiences with the timing of gaining this knowledge ranged from early childhood to still having limited knowledge in adulthood. The qualitative data reveal opportunities for enhancing access to information about a variety of aspects of BPBI, including disease progression through the lifespan and treatment options and resources for affected adults to address their HRQoL and associated concerns.
HLQ 3 Actively managing health reflects the experience of allotting resources to managing the healthcare consumer's health. While the HLQ 3 mean score is near the midpoint of the Likert response scale (2.75; SD 0.64), the qualitative data illustrate a broad range of experiences. The continuum spans from not having to devote any resources to managing BPBI-related HRQoL concerns in adulthood to utilizing a myriad of resources to address health-related concerns attributed to BPBI. The quantitative mean suggests participants generally dedicated time and energy into managing their health, which also is supported by the qualitative findings.
Additionally, the qualitative findings provide a more complete description of what is involved when BPBI-affected individuals manage their health related to the utilization, perceived effectiveness and frequency of accessing healthcare services. The range of healthcare resources accessed included family doctor, orthopedic surgeon, sports medicine doctor, neurologist, pain medicine doctor, and specialized brachial plexus clinics. Participants reported utilization of the following types of medical management: pain medication, cortisone shots, medical marijuana, medication for depression and anxiety, botulinum toxin injections, and muscle relaxers. Additionally, ancillary healthcare resources used included acupuncture, chiropractic care, physical therapy, occupational therapy, massage therapy, psychotherapy (to address the desire to hide the affected arm; emotions associated with having BPBI), and aquatic therapy. Participants reported having a variety of surgical procedures performed which included shoulder replacement (unaffected side), rotator cuff repair (unaffected side), thumb carpometacarpal joint surgery (unaffected side), radiculopathy, carpal tunnel release, cervical surgery, supraspinatus repair, cervical fusion, shoulder fusion, and various surgeries in childhood. Finally, participants described modalities they used to help manage their health concerns, including various forms of exercises and stretching, slings/orthoses, electrical stimulation, and heating pads.
The perceived effectiveness of utilized medical interventions was broad. Some participants described the care they received as effective, or even highly effective, while others expressed the medical intervention they received was ineffective. The frequency of healthcare utilization ranged from no care, to periodic care, to accessing healthcare intervention multiple times a week.
The mean score for HLQ 6 Actively engage with healthcare providers (3.47; SD 0.88) fell between “sometimes difficult” and “usually easy” on the five-point Likert scale. This scale has questions about the ease of communicating with healthcare providers. For this scale, the qualitative findings again more completely depict the range of communication experiences. Some participants described experiences with healthcare providers being unwilling to engage in conversations about their BPBI-related health concerns. Other participants described positive communication experiences with healthcare providers; however, it is notable that the positive accounts pertained to experiences during adolescence or childhood when participants described participating in routine specialty care. Participants also expressed a need for increased communication from healthcare providers with the family at the time of injury to facilitate understanding of the condition and available resources for managing BPBI.
HLQ 7 Navigating the healthcare system pertains to the ability to find the healthcare resources desired for optimal management of a medical condition. Like the other scales, the mean score (3.25; SD 1.07) fell midrange with a unimodal distribution reflecting neither ease nor difficulty as the average experience. Here again, the qualitative data elaborate on the experience of accessing services reflecting a range of experiences and providing insight into barriers. While some respondents did describe having an easily accessible healthcare provider knowledgeable of BPBI, many challenges were reported. Some respondents expressed an inability to find healthcare resources for adults with BPBI, and others reported difficulty determining which healthcare resources may be beneficial. A lack of patient-centered and holistic care was described by some respondents. Some described an experience of having routine healthcare resources to address their BPBI in childhood and a loss of those resources with the transition to adulthood. Challenges with affording healthcare resources and accessing healthcare resources without having to travel were also reported barriers to navigating healthcare resources for BPBI in adulthood.
Discussion
In order to identify challenges and opportunities for improving care for BPBI, this convergent mixed methods secondary data analysis was undertaken to provide a comprehensive depiction of the health literacy of adults with BPBI. The findings of mean HLQ scores that fell in the midrange of the five scales used in the current analysis are similar to that of other studies examining the health literacy of adults with chronic medical conditions.21,22,35 While the quantitative findings had unimodal distributions clustering around the midrange mean scores, the qualitative findings depict participant experiences that seemed to cluster at the extremes of either positive or negative experiences with respect to the examined health literacy factors. This was especially clear in the qualitative data for HLQ 1 Having a healthcare provider, HLQ 2 Having sufficient information, and HLQ 6 Actively engage with healthcare providers, whereas, for HLQ 3 Actively managing health and HLQ 7 Navigating the healthcare system, the variation in the qualitative data was broad, but more evenly distributed, representing a wide range of experiences.
In prior work, the HRQoL outcomes of adults with BPBI were found to be variable with respect to many factors including affected adults’ hand and arm function, general health, activity participation, life roles, emotional health and relationships. 9 The drivers of this variability may include factors beyond the affected arm's function. For instance, de Heer et al. found that pain has a greater association with daily functioning in young adults with BPBI rather than their affected arm's function. 36 Similarly, Yau et al. found that a history of BPBI surgery, employment status, disability benefits status and having a life partner were all factors that impacted the affected adults’ overall ratings of their HRQoL. 37 Thus, it is possible that the wide range of experiences of living with BPBI in adulthood accounts for variation in health literacy among the population revealed within the current study's qualitative findings. Yet, this is likely an inadequate explanation since prior studies have found differing relationships between HRQoL outcomes and measures of health literacy in other populations.22,38–40 Prior research has found an association between low health literacy scores and low HRQoL scores,22,40 whereas no correlation was found between measures of health literacy and HRQoL in other studies.38,39 Other authors have examined health literacy in adults with chronic medical conditions with respect to specific demographic variables and found that higher health literacy scores are associated with higher income and education levels.21,35 Yet, these studies were in convenience samples of single-country populations rather than findings of international populations. Thus, it is plausible that the diversity in experiences living with a chronic medical condition and the multidimensional factors related to health literacy are so complex that even the application of mixed methods research is not able to fully distill the health literacy of a population into a neat picture. 41 Nonetheless, the current analysis provides insights that can inform healthcare delivery for adults with BPBI.
HLQ 1 Having a healthcare provider and HLQ 6 Actively engage with healthcare providers are both HLQ scales that measure the healthcare consumer/provider interface. The current analysis suggests opportunities for improvement in this interface for adults with BPBI and their healthcare providers. Qualitative data revealed participant experiences in which adults with BPBI felt their healthcare provider did not listen or was even dismissive of their expressed concerns. Furthermore, experiences of healthcare providers not acknowledging or being unknowledgeable of BPBI seemed to undermine trust in the healthcare consumer/provider relationship.
Challenges regarding the patient-provider interface may also be in part driven by the healthcare setting. In a population of adults with chronic kidney disease, HLQ 1 Having a healthcare provider had the lowest mean score of all HLQ scales. The context of receiving care was described as lacking consistency in medical providers across the healthcare consumers’ medical appointments. The authors postulated this experience of inconsistent healthcare providers may explain this finding. 35 Conversely, in a study examining health literacy among participants in a cardiac rehabilitation program, the highest HLQ scores were for HLQ 1 Having a healthcare provider, with HLQ 6 Actively engage with healthcare providers falling within the range of positive scores. 19 This healthcare delivery context was a defined program with consistent healthcare providers and programmatic features designed to enhance participants’ health literacy and self-efficacy. Therefore, it is possible that consistency in healthcare providers who assist with managing the healthcare consumer's medical condition and related HRQoL concerns may contribute to the overall rating of the healthcare provider/consumer interface health literacy variables. Further research is warranted to explore this interface for adults with BPBI, as participants articulated an expressed desire to have healthcare providers who were knowledgeable about BPBI across the lifespan, including at the time of injury.
In the current analysis, findings for HLQ 2 Having sufficient information revealed inconsistent experiences with accessing sufficient information about BPBI. This may be related to the multigenerational study population and changes in medicine over time. For example, regional BPBI centers with multidisciplinary healthcare experts are presently found in pediatric medical institutions internationally. These condition-specific specialty clinics have emerged along with increased recognition of BPBI among medical professionals globally and with an expansion of research to guide clinical practice. For younger study participants, the opportunity to have specialty care was more readily available than for participants who were in their 70 s and 80 s at the time of the primary LEAP study. Nonetheless, participants desired information about BPBI to be more readily available for the general public, and for the medical community to have more knowledge of BPBI as well. Additionally, study participants expressed that information about how BPBI affects individuals through the lifespan is limited. Opportunities to create resources for affected individuals to access comprehensive information about BPBI, intervention options, and other resources to manage their HRQoL concerns are needed.
Varied experiences with healthcare utilization are consistent with the populations’ variation in HRQoL outcomes in adulthood. 9 Importantly, the current analysis revealed that adults with BPBI continue to have HRQoL concerns they attribute to the condition, as well as related health literacy needs, across the lifespan. In fact, the current analysis revealed the population has a desire for information about BPBI outcomes across the lifespan, available treatments for BPBI-related health concerns in adulthood, and wide-ranging resources for affected individuals. Qualitative data revealed that some participants expressed a lack of comprehensive holistic patient-centered care for BPBI, especially in adulthood; some participants reported positive experiences with BPBI specialty care in childhood that was lost with the transition to adulthood. These findings underscore opportunities for improving health literacy in terms of access to BPBI resources and healthcare providers with expertise in BPBI. The need for children with BPBI to have a transition of disease-specific healthcare resources in adulthood aligns with this recognized need for other condition-specific populations. 42
It is noteworthy that participants desired access to BPBI-specific healthcare resources for affected adults that are both affordable and available without requiring travel. Thus, while having BPBI specialty centers that provide care for affected adults may be a possible area of service growth, making the resources in those regional centers readily available must be considered. Services such as telehealth and electronic health resources may provide solutions.43,44 Additionally, the current analysis revealed that some participants described difficulty determining which healthcare resources would be beneficial for addressing their BPBI-related HRQoL concerns. In the previously cited study evaluating health literacy in adults attending cardiac rehabilitation, the authors found that participants could be clustered according to their HLQ scores. 19 Profiles ranged from participants with high health literacy scores described as confident healthcare consumers who felt supported with their healthcare needs to participants with low health literacy scores who experienced barriers to meeting their healthcare needs. 19 Drawing upon these findings, it is possible that this range of health literacy profiles exists across populations of adults with various chronic medical conditions, including BPBI. Thus, healthcare providers should routinely assess patients’ health literacy to determine the need for health literacy supports for empowering individuals in the self-management of their BPBI-related HRQoL concerns. 14
Limitations
This study has several limitations, despite employing a robust convergent mixed methods analysis with a relatively large patient sample. The first limitations pertain to the study sample. The use of an e-survey link posted on social media sites may not be inclusive of those with limited access to technology. This recruitment methodology, together with a focus on ensuring anonymity, also limits the ability to verify the diagnosis or obtain clinical information related to injury severity, recovery, and treatment. Furthermore, in keeping with uneven gender distributions among members of online support groups, 45 the sample was predominantly female, especially among older participants, which is not representative of the roughly equal distribution of BPBI across genders. 1 In addition, the sample included participants across a 67-year age range, with care having changed substantially in that span. Because of this potential confounder, comparison of variables across ages was not attempted. Nonetheless, despite the potential biases inherent in this study population, the current study contributes perspective on affected adults that has not previously been available.
A second limitation of the current analysis is the exclusion of personal factors, such as income, education level, and participant geographic location, limiting the ability to analyze the social determinants of health among the participants with respect to health literacy scores. Prior studies have discovered that such personal factors correlated with healthcare consumer health literacy scores in other disease populations.21,35 Therefore, knowledge of whether such a relationship between personal factors and HLQ scores among adults with BPBI could be helpful in enhancing health literacy for the population. Third, the current analysis did not include data from all nine HLQ scales, since only five of nine HLQ scales were measured in the primary LEAP study. However, in an effort to limit response burden, the LEAP study applied qualitative data from the survey and interview phases to identify which PROMs matched to the population's expressed HRQoL and healthcare concerns. As such, only a subset of HLQ scales were found relevant for administration in the primary LEAP study. It is possible that a more complete picture of health literacy would be discovered with administration of all HLQ scales, so future studies of health literacy in the population could include the complete battery of HLQ scales. However, given the finding of midrange unimodal HLQ mean scores, yet health literacy experiences that clustered to be positive or negative on a majority of the scales, caution should be taken in interpreting only mean HLQ scores without qualitative data. Finally, in coding the qualitative healthcare experience data, some data seemed to align with two similar codes, such as HLQ 1 Having a healthcare provider and HLQ 6 Actively engage with healthcare providers. Consensus meetings among researchers were required to code the qualitative data consistently among similar HLQ scales. However, while there seems to be some conceptual overlap in a few of the HLQ scales, the primary qualitative findings were consistent across the scales, so the findings and conclusions are not likely to be affected by the specific grouping of qualitative data into specific HLQ scales. Overall, despite its limitations, this analysis provides the first picture of the health literacy experience of BPBI-affected adults and reveals opportunities for improving healthcare resources for this population.
Future directions
While these study findings reveal that opportunities exist for improving healthcare services to enhance health literacy for adults with BPBI, further research would be instrumental in identifying how to effectively adapt the healthcare system to better serve adults with BPBI. Furthermore, health literacy is impacted by both the healthcare system and the individual healthcare consumers. 46 Therefore, further research should address individual factors that may offer opportunities for improving health literacy among adults with BPBI. In other populations of adults with chronic health conditions, personal factors were found to impact the HLQ scores of adults with other chronic medical conditions.21,35 Therefore, future studies should consider an analysis of health literacy in relationship to social determinants of health for adults with BPBI. Identification of personal factors which are associated with lower health literacy scores would help to identify individuals in the population who may be in greater need of health literacy support.
Conclusion
The current mixed methods secondary data analysis revealed that health literacy experiences of adults with BPBI vary from negative to positive across multiple health literacy domains. Healthcare system factors that pose a challenge to health literacy include a lack of general awareness about BPBI, scarce resources for adults with BPBI-related concerns, and limited knowledge of BPBI among adult-oriented healthcare providers. Opportunities for improvement are particularly pertinent at the transition from childhood care to adult healthcare settings.
Footnotes
Acknowledgements
The authors have gratitude for the LEAP study participants for sharing their stories. We appreciate the United Brachial Plexus Network (UBPN) and the Adults with Brachial Plexus Birth Injury Facebook Groups and their membership for supporting this study. We thank Sierra Richardson for her contributions with study figures.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Cincinnati Children's Hospital Medical Center, (grant number Place Outcomes Research Award).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.