
Abstract
Background
Dystonic cerebral palsy is a severely disabling condition that poses significant management challenges, compounded by multiple associated comorbidities and the limited availability of effective treatment options.
Objective
This study aimed to study the clinical characteristics, functional impact and caregivers’ priorities among children with dystonic cerebral palsy.
Methods
This was a cross-sectional observational study (n = 50) among children with dystonic cerebral palsy aged four to 18 years. The Hypertonia Assessment Tool and Barry-Albright Dystonia Scale were used to identify and measure the severity of dystonia. The Dyskinetic Cerebral Palsy Functional Impact Scale was used to assess the daily impact of dystonia and caregivers’ priorities.
Results
Fifty children (70% male, mean age 8.6 years old) with majority functional status from level III to V across all functional classification systems were included. Significant correlation was observed between functional impact with dystonia severity scores (p = 0.003). The caregivers’ priorities were beyond gross motor and mobility concerns.
Conclusions
Understanding the clinical characteristics, comorbidities, functional profiles and caregivers’ priorities is imperative in tailoring interventions to those most relevant and important for children with dystonic cerebral palsy and their families.
Introduction
Cerebral palsy is a common cause of neurodisability in childhood, with a higher prevalence in lower income countries. 1 Dyskinetic cerebral palsy is classified into two major movement disorder patterns, dystonia and choreoathetosis, and is one of the most disabling forms of cerebral palsy. 2 Dystonic cerebral palsy is the most common presentation of dystonia in children, with leading aetiology due to hypoxic-ischemic injury during the prenatal, perinatal, or infantile period.3,4
Dystonia in childhood may be under-recognised by paediatricians and allied health professionals, particularly in cerebral palsy, as it may coexist with spasticity.4,5 Although dystonia is essentially a clinical diagnosis, reliable measurement is crucial for the characterisation of clinical patterns and evaluation of the effects of targeted management. 6 Previous studies of children with cerebral palsy have shown an increased severity of dystonia across gross motor, manual ability and communication functional levels.6,7
Treatment for most children with dystonia is primarily symptomatic, with aims to improve daily activity and quality of life by improving movement and posture and relieving any associated disability, pain, and discomfort. 8 Management must be tailored to the individual child based on motor and functional goals. Understanding the clinical characteristics, comorbidities, functional profiles and caregivers’ priorities is imperative in providing optimal, family-centred care to meet the needs and expectations of children with dystonic cerebral palsy and their families.
The primary objective of this study was to determine the clinical characteristics, functional impact and caregivers’ priorities among children with dystonic cerebral palsy.
Despite growing recognition of the burden of dystonic cerebral palsy, few studies have quantified the daily functional impact and caregivers’ priorities using validated measures. This study addresses this gap within a middle-income context, providing region-specific evidence.
Methods
Study design and patients
This was a prospective, cross-sectional observational study conducted among children with dystonic cerebral palsy aged four to 18 years. The study was undertaken in Hospital Tunku Azizah, the main tertiary centre for children with neurological disorders in Malaysia, from 1st September 2022 until 30th September 2023.
A universal sampling method was used, in which all eligible patients attending the outpatient neurology clinics during the study period were invited to participate. Participants aged 4–18 years with a clinical diagnosis of dystonic cerebral palsy were included. Patients with dystonia secondary to neurodegenerative, neurogenetic, or metabolic conditions were excluded. Written informed consent for participation and publication was obtained from patients or their caregivers.
Based on a previous study, 50 patients were enrolled to meet the minimum sample size required to determine correlation between Dyskinetic Cerebral Palsy Functional Impact Scale (D-FIS) total scores and the Barry–Albright Dystonia Scale (BADS). 6
Data collection and assessment tools
Clinical data were obtained using a structured data collection form. The Hypertonia Assessment Tool (HAT) is a seven-item clinical instrument designed to differentiate subtypes of paediatric hypertonia – namely, spasticity, dystonia, and rigidity – and has demonstrated high internal consistency for identifying dystonia. 9 BADS is a five-point ordinal severity scale for secondary dystonia which has shown high internal consistency.10,11 Both HAT and BADS were administered by experienced clinicians trained in their use during routine clinical assessments. D-FIS is an 18-item caregiver-reported measure assessing the impact of dyskinesia on 16 daily activities and two additional constructs (pain and fatigue), with items rated on five-point Impact and four-point Priority Scales. The D-FIS has demonstrated good construct validity and high internal consistency. 6 The D-FIS was translated into Malay following the developer's guidelines and validated as part of this study, yielding good reliability (Cronbach's α = 0.86).
Data analysis
All data obtained were analysed using IBM SPSS Statistics 23.0. Descriptive statistics included frequencies and percentages for categorical variables, and means with standard deviations for numerical variables. Median and interquartile range were used for numerical variables as appropriate. Kruskal-Wallis H and Mann-Whitney U tests were used to identify significant differences between severity of dystonia and clinical characteristics. Spearman rank correlation was used to determine significant association between functional impact with dystonia severity scores and levels, while the Kruskal-Wallis H test was used to determine significant differences in functional impact score according to levels of functional profiles.
This study protocol has been registered on the National Medical Research Register. Results are reported according to the Strengthening the Reporting of Cohort, Cross-Sectional and Case-Control Studies (STROCCS) 2021 guidelines. 12
Results
Demographic and clinical characteristics
Demographic and clinical characteristics of patients are depicted in Table 1. Fifty patients were included, with a mean age of 8.6 years old, predominantly male (70%) and Malay ethnicity (84%). The most common cause of cerebral palsy was prematurity (defined as birth before 37 completed weeks gestation) with complications (30%), followed by perinatal asphyxia (22%), and several other causes that each represent less than 7% of the patients. The topographical distribution was bilateral in all but one patient. Overall, 98% of the patients were level III to V on the Gross Motor Function Classification System (GMFCS), 86% on the Manual Ability Classification System (MACS), 84% on the Communication Function Classification System (CFCS), and 56% on the Eating and Drinking Ability Classification System (EDACS). More than 30% of participants had one or more of the following comorbidities: hip displacement, epilepsy, low weight, chronic constipation, learning disability/global developmental delay, or contractures. The most common comorbidities were hip displacement (52%) followed by epilepsy (50%) and low weight (44%). Patients almost always received at least one anti-dystonic medication (94% cumulatively), with baclofen and trihexyphenidyl prescribed to more than half of the patients. Only two patients had history of status dystonicus.
Demographic and clinical characteristics of patients.
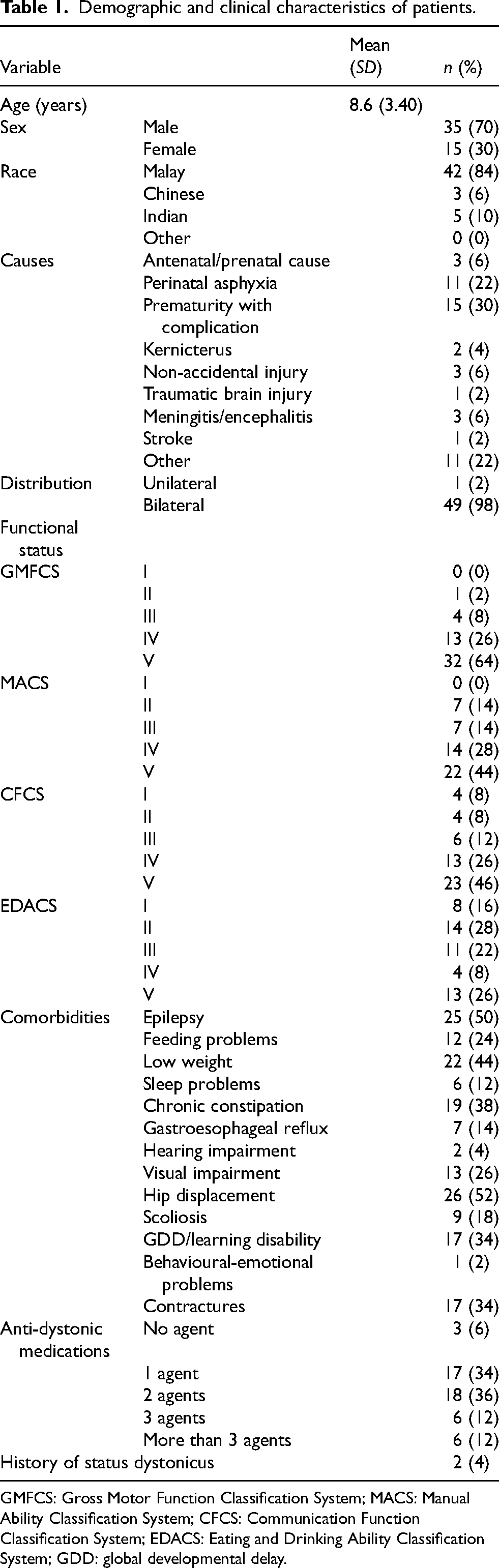
GMFCS: Gross Motor Function Classification System; MACS: Manual Ability Classification System; CFCS: Communication Function Classification System; EDACS: Eating and Drinking Ability Classification System; GDD: global developmental delay.
Dystonia severity, functional impact and caregivers’ priorities
In the study cohort, the median severity of dystonia as measured by BADS was 15.5 with an interquartile range of 8.25. The distribution of dystonia severity scores according to functional profiles is shown in Figure 1. Dystonia severity scores ranged higher in GMFCS IV and V as compared to lower levels. There were also more variations of dystonia severity scores in MACS and CFCS levels I to III, whilst scores across levels IV and V remained more consistent. Functional profiles on EDACS showed less variation across all levels, with higher levels showing higher medians. The Kruskal–Wallis H tests revealed no statistically significant differences in dystonia severity according to the underlying cause of cerebral palsy, the number of pharmacological agents used, or the number of comorbidities (p > 0.05; Supplementary Material).
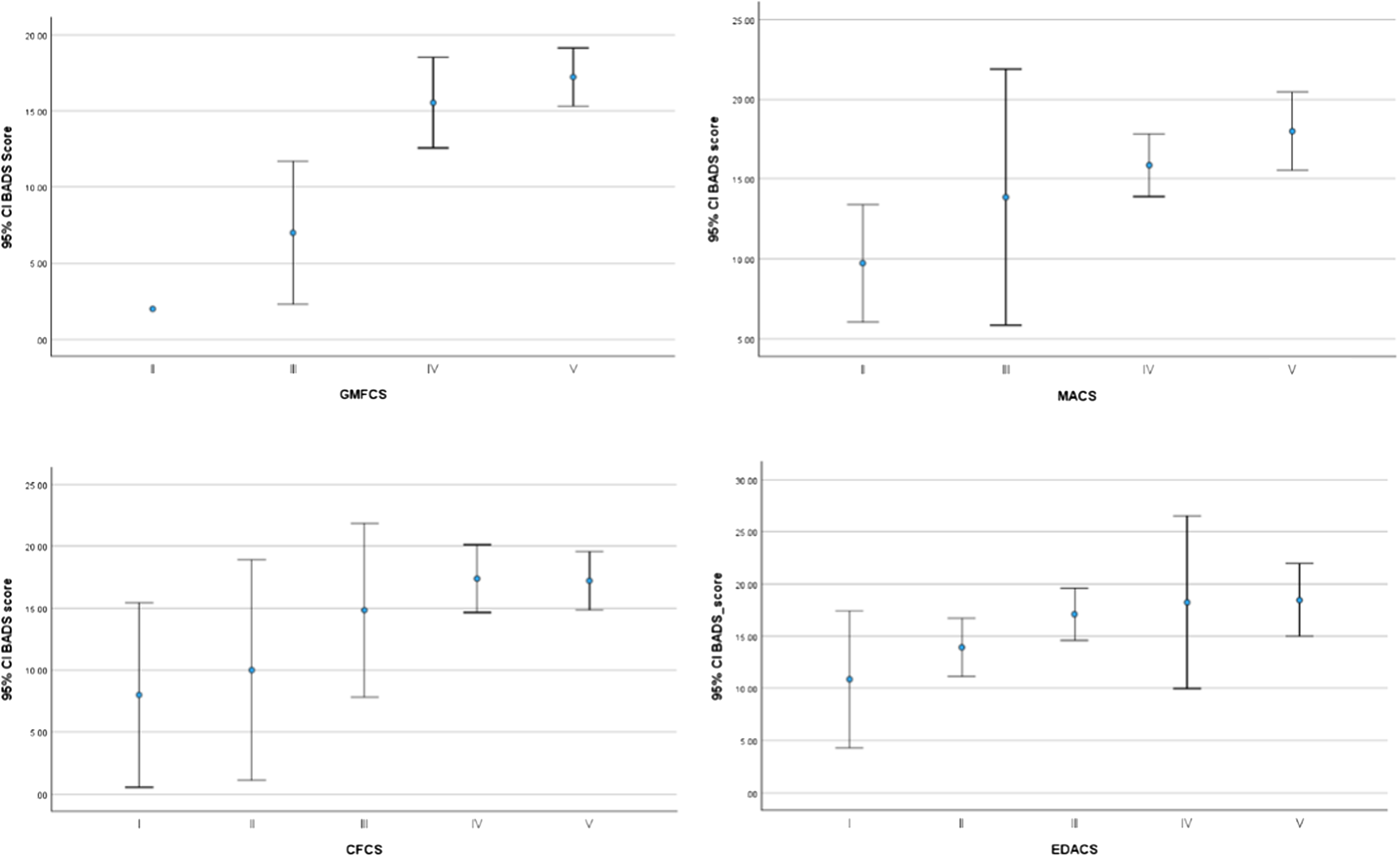
Barry-Albright Dystonia Scale (BADS) score plot according to functional profiles.
The median functional impact score was 28.0 with an interquartile range of 16.25, representing a large variation of functional impact scores among the patients (Table 2). The highest impact scores were in fine motor, followed by sitting, reaching and technology. Sitting, positioning, transfers, hygiene, upper and lower body dressing, feeding, speech, leisure, and sleep were rated as highest priorities. The discrepancy between functional impact of dystonia on the child and caregiver's priorities was most obvious for sitting, positioning, transfers, reaching, hygiene, upper dressing, lower dressing, feeding, speech, leisure, and sleep. In this cohort, priorities were often rated highly by the caregivers despite their child having mild to moderate functional impact ratings. Fine motor and reaching, specifically, were reported as having moderate or severe functional impact and were rated as highest priorities. There were no significant differences in functional impact scores according to levels of GMFCS, MACS, CFCS, or EDACS functional profiles (p > 0.05) as shown in Table 3. Further analysis using the Spearman rank correlation was used to determine significant association between functional impact with dystonia severity scores (rspearman = 0.417, p = 0.003). Dystonia severity scores showed positive moderate correlation with functional impact scores, with higher dystonia severity scores corresponding to higher functional impact scores (Supplementary 1). Priority scores were plotted for descriptive comparison across GMFCS levels (Figure 2). The highest priorities across all GMFCS groups were for sitting, positioning, transfers, fine motor activities, reaching, hygiene, upper and lower dressing, feeding, speech, sleep, and leisure. Patients with GMFCS levels I–III tended to score activities such as standing, walking, and using technology as higher priorities.

Priorities according to gross motor function classification system (GMFCS) level.
Functional impact scores and priorities.
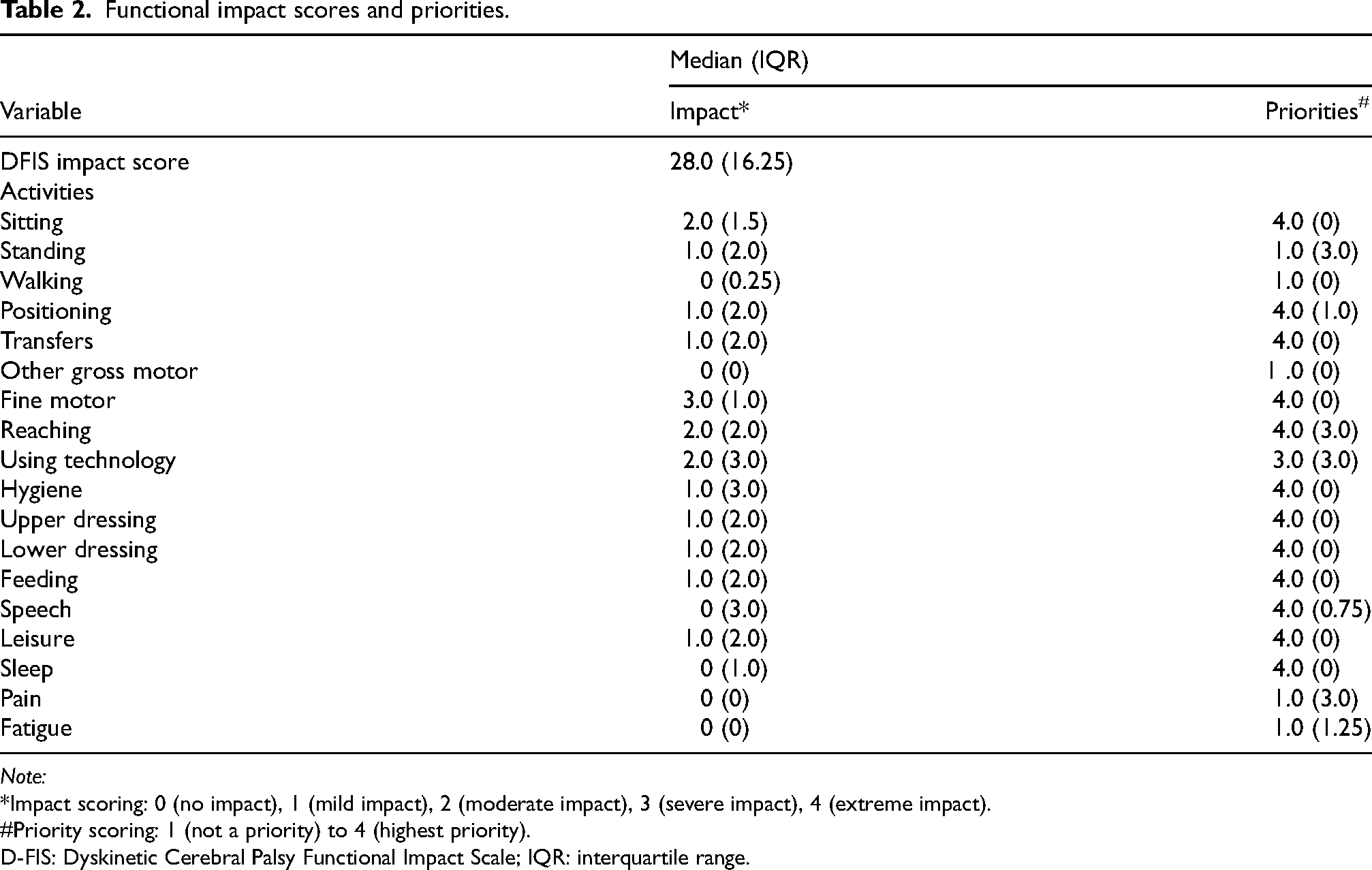
Note:
*Impact scoring: 0 (no impact), 1 (mild impact), 2 (moderate impact), 3 (severe impact), 4 (extreme impact).
Priority scoring: 1 (not a priority) to 4 (highest priority).
D-FIS: Dyskinetic Cerebral Palsy Functional Impact Scale; IQR: interquartile range.
Functional impact scores according to functional profiles.

IQR: interquartile range; GMFCS: Gross Motor Function Classification System; MACS: Manual Ability Classification System; CFCS: Communication Function Classification System; EDACS: Eating and Drinking Ability Classification System.
Discussion
This hospital-based study highlights important aspects of clinical characteristics, functional classifications, and impact among children with dystonic cerebral palsy. The main findings include the combined quantification of functional impact and caregivers’ priorities using a validated tool, D-FIS, use of which has shown to be practical even in a busy outpatient clinic setting.
This was the first study in this region to investigate functional impact and caregivers’ priorities in children with dystonic cerebral palsy. The majority of participants demonstrated functional status within levels III to V across all classification systems. As the study centre serves as a tertiary neurology referral centre, most children with cerebral palsy are referred for intervention, particularly for management of tone abnormalities and associated comorbidities. Almost all of these patients have mixed-spastic dystonic phenotype, whereas frequent co-morbidities reported in other studies are epilepsy and cortical visual impairment. 13
In this study, dystonia severity scores ranged higher in GMFCS IV and V as compared to lower levels, findings that correspond to previous studies using both BADS and HAT.7,14 This indicates that greater levels of dystonia correspond with lower levels of motor function, which influences overall function further than previously recognised. 7 Using the reliable measurement kit D-FIS, higher dystonia severity scores were shown to be related to higher functional impact scores.
When the functional impact on a particular activity is coupled with the priority scale, an individualised management plan can be provided based on activities deemed important by patients or caregivers. For example, for a patient who reports having severe functional impact in fine motor domains, and for whom reaching is rated as the patient's or caregiver's highest priority, specific intervention targeting this treatment goal would be important. Aspects related to self-care and social participation such as hygiene, leisure, use of technology, and speech were rated as higher priorities compared with mobility-related domains, including gross motor activities, walking, and standing. This finding further underscores the importance of addressing functional concerns beyond mobility and gross motor function in children with dystonic cerebral palsy. 5
This study has several limitations. The single-centre design, with a predominance of patients with moderate to severe functional involvement, may limit the generalizability of findings to the wider cerebral palsy population. The modest sample size, which became smaller when stratified by functional level, further restricted subgroup comparisons. Reliance on caregiver-reported outcomes for the D-FIS introduced potential reporting bias, although this remains necessary for children with communication difficulties. Moreover, the cross-sectional design precluded assessment of changes over time or responsiveness to interventions. Future multicentre studies with larger, more heterogeneous cohorts are recommended to validate these findings, evaluate longitudinal trajectories, and include child self-report measures when feasible.
The findings of this study have important clinical implications and future directions, underscoring the need to integrate caregivers’ perspectives into the multidisciplinary management of children with dystonic cerebral palsy. Routine use of validated functional impact measures to capture caregiver-identified priorities can enhance family-centred and goal-directed care planning, ensuring that interventions target outcomes most meaningful to children and their families. Understanding functional impact and caregiver priorities enables clinicians to better tailor rehabilitation, pharmacological, and surgical strategies to individual needs.
In conclusion, recognising dystonia severity and embedding caregiver-reported functional impact and priorities into clinical practice and research offers a practical framework for delivering more responsive and holistic care to children with dystonic cerebral palsy and their families.
Supplemental Material
sj-docx-1-prm-10.1177_18758894261450013 - Supplemental material for Clinical characteristics, functional impact and caregivers’ priorities in Malaysian children with dystonic cerebral palsy
Supplemental material, sj-docx-1-prm-10.1177_18758894261450013 for Clinical characteristics, functional impact and caregivers’ priorities in Malaysian children with dystonic cerebral palsy by Husna Musa, Nor Hanim Mohamad Hanapi, Poorani Anandakrishnan, Suhaila Omar and Teik Beng Khoo in Journal of Pediatric Rehabilitation Medicine
Footnotes
Acknowledgements
The authors thank the patients and their parents and the Director General Health of Malaysia for granting permission to publish these research findings.
Ethical considerations
Ethical approval for the study was obtained from the Medical Research and Ethics Committee, Ministry of Health Malaysia (NMRR ID-22-01911-GWL (IIR)).
Patient consent statement
All respondents provided written informed consent.
Author contributions
HM drafted the manuscript with inputs from all other authors. HM, NHMH, PA, and SO collected data and clinical information. HM, NHMH, PA, SO and TBK reviewed the manuscript and finalised the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received a research grant from the Malaysian Paediatric Foundation (MPF) Sham Kasim Research Award.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.