
Abstract

1-Pre-Congress Courses
PCO1
University of Oxford, United Kingdom
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor symptoms resulting from the loss of dopaminergic neurons in the substantia nigra pars compacta, along with a wide range of non-motor manifestations such as olfactory, sleep, and autonomic disturbances. Neuropathologically, PD is defined by intraneuronal alpha-synuclein (aSyn) aggregates, Lewy bodies and Lewy neurites, as well as glial aSyn inclusions across selectively vulnerable brain regions. However, aSyn pathology is not confined to the brain; it extends to the spinal cord and peripheral nervous system, including the enteric nervous system (ENS), which innervates the gastrointestinal (GI) tract. This widespread distribution may underlie early non-motor symptoms, such as constipation, which often precedes the onset of motor deficits by several years. The emerging body-first versus brain-first hypothesis proposes that PD can originate either in the periphery, with aSyn pathology spreading to the brain via autonomic and vagal pathways, or centrally, with subsequent dissemination to peripheral organs. Distinct propagation routes and aSyn strain conformations may therefore contribute to the pronounced clinical and pathological heterogeneity observed among individuals with Parkinson’s.
This talk will present our recent work characterizing human aSyn aggregates derived from the ENS and comparing these with brain-derived aSyn aggregates from PD patients. Preliminary findings reveal clear biochemical and structural differences between ENS- and brain-derived aSyn. Using antibody binding profiles, aSyn seeding capacity, morphology, limited proteolysis, and mass spectrometry, we are identifying the molecular determinants of these distinct aggregate species.
By integrating aSyn seed amplification assays with high-resolution biophysical techniques and AI-assisted digital pathology (“pathomics”), we aim to define how aSyn strain polymorphism and conformational templating drive selective vulnerability and propagation along the gut–brain axis. These interdisciplinary approaches, coupled with spatial multi-omics, will reveal how region- and cell-type–specific environments influence aggregate structure and toxicity.
Defining pathological trajectories is key for early diagnosis, biomarker development, and precision therapies. Our work aims to uncover the molecular underpinnings of aSyn propagation to guide mechanism-based subtyping and targeted treatment in PD.
PCO2
Yale University, United States
Alpha-synuclein is genetically linked to Parkinson's disease (PD), with point mutations (PARK1) and gene multiplications (PARK4). Alpha-synuclein is also the defining protein component of Lewy bodies, the signature pathology of PD. It is now appreciated that alpha-synuclein pathology is seen in other neurodegenerative diseases, including Lewy Body Dementia and Multiple Systems Atrophy, which are collectively known as synucleinopathies. In this talk, I will summarize our current understanding of the physiological functions of alpha-synuclein in neurons and its pathological properties in synucleinopathies. I will also describe how our insights into alpha-synuclein biology is translating into biomarkers and new therapies.
PCO3
KU Leuven, Belgium
Animal models are essential to study the pathophysiology of Parkinson’s disease and to develop disease-modifying therapies. Technical advancements and new insights into α-synuclein pathology have led to a wide array of available rodent models that have greatly contributed to our understanding of different aspects of Parkinson’s disease. The identification of α-synuclein as a disease-associated gene and the discovery of this protein as one of the major constituents of Lewy bodies, have prompted the generation of animal models based on α-synuclein transgenesis or viral vector-mediated α-synuclein overexpression. Later, new insights on the “prion-like” properties of α-synuclein led to the development of transmission models based on intracerebral inoculation of α-synuclein preformed fibrils. In this talk, we will give a comprehensive overview of the different α-synuclein-based rodent models that have been developed, each with their own characteristics, advantages and limitations. The best choice of the animal model will be dependent on the specific question or scientific hypothesis to be tested.
PCO4
United States
The goal of managing of motor symptoms in Parkinson’s disease is to maximize mobility while minimizing side-effects of treatment which become disabling as the disease advances. Recent interventions that are designed to achieve this objective include oral carbidopa and levodopa extended-release capsules, and subcutaneous infusions of foscarbidopa and foslevodopa and apomorphine hydrochloride. In randomized controlled trials, the oral extended-release formulation of carbidopa-levodopa increased good on-time per dose by 1.55 hours compared to the immediate release formulation. Of the infusions, foscarbidopa and foslevodopa improved on time by 1.75 h compared to immediate-release carbidopa levodopa and apomorphine reduced off time by 1.89 h compared to placebo. Newer drugs awaiting FDA clearance that have shown promise to also improve on time without dyskinesias are tavapadon, a selective D1/D5 receptor partial agonist, and ND0612, a subcutaneous infusion of levodopa-carbidopa solution. Ongoing Phase 3 trials of Parkinson’s disease drugs designed to improve motor symptoms include CVNB424, a GPR6 receptor modulator, and P2B001, a combination of low doses of extended release rasagiline and pramipexole. While we await disease modifying therapies in Parkinson’s disease, pursuing scientific research of clinical treatments that minimize the impact of motor and non-motor symptoms on quality of life is imperative.
PCO5
Arizona State University, United States
Gait and balance remains an important challenge for people with Parkinson’s disease. However, recent advances have improved our ability to treat these symptoms. In particular, there are a number of treatments currently in the research pipeline showing promise for treatment of gait and balance, including physical and cognitive rehabilitation, attentional strategies, robotics, and surgical techniques. The current presentation will discuss recent clinical and scientific findings in this area, detailing current and future approaches to reduce the burden of this challenging symptom.
PCO6
Stanford University, United States
Current symptomatic therapies for cognition and mental health are limited for people with Parkinson's disease. We will discuss currently available treatments and discuss their benefit and limitations. In addition, we will discuss the pipeline for future advances in this field and discuss ways to enhance this line of research through biomarker and non-motor endpoint development.
PCO7
University of British Columbia, Canada
PET and SPECT are both forms of molecular imaging. While each has its advantages and disadvantages, both allow one to quantitate the distribution of chemical and metabolic changes in the brain. In Parkinson’s, where structural changes may be limited, particularly in early disease, this may be of particular value. The most widespread approach from a molecular imaging perspective is the assessment of striatal dopamine innervation, using a a variety of tracers for the membrane dopamine transporter (both SPECT and PET), fluorodopa PET (dopamine synthesis and storage) and vesicular monoamine transporter 2 (VMAT2) PET. While dopaminergic markers provide information on the neurotransmitter whose loss is a defining feature of PD, they are not specific for the diagnosis, as atypical forms of parkinsonism (AP) may result in similar abnormalities. Furthermore, the relationship between changes in dopaminergic imaging markers and clinical progression of PD is not straightforward, which means the findings in trials of disease modifying therapies must be interpreted with caution. From a molecular diagnostic perspective, glucose metabolic (FDG) PET may be more reliable to differentiate between PD and AP, and is also sensitive to the effects of both symptomatic and disease modifying therapies. Other molecular markers of interest include those that assess the impact of disease on other neurotransmitter systems (e.g. serotonin, norepinephrine, cholinergic) and those that assess mitochondrial function or neuroinflammation. These are largely at an experimental change, as are markers of abnormal protein deposition (tau or α-synuclein). The availability of a reliable tracer for abnormal α-synuclein deposition would be a major advance. While considerable progress has been made in the last few years, this is still at a developmental stage. It should be emphasized that no single imaging approach suits all purposes and the different approaches (including both molecular imaging and MRI) should be seen as complementary rather than competing.
PCO8
Paris Brain Institute, France
There are three main MRI-based biomarkers of degenerative changes in the substantia nigra (SN) in Parkinson’s disease: the so-called neuromelanin-sensitive MRI (NM-MRI), iron-sensitive MRI and diffusion-based markers. NM-MRI detects the loss of neuromelanin signal and volume changes of the SN. Changes are early (detected at the prodromal stage of Parkinson's disease), categorize patients from controls with high accuracy, correlate with markers of striatal dopaminergic function and with motor and cognitive changes, and aggravate with disease progression. Iron-sensitive MRI include T2* relaxometry and quantitative susceptibility mapping (QSM). These techniques detect iron accumulation in the SN. Changes are also detected early, increase with disease progression, and correlate with motor and cognitive impairment in some studies. Iron increase is also visible using high-resolution susceptibility-weighted images in the nigrosome-1 region, a Parkinson-vulnerable substructure. Loss of the “swallow tail sign” on susceptibility-weighted imaging indicates nigrosome-1 degeneration and is a key radiological signature of Parkinson's disease. Diffusion imaging measurements commonly include fractional anisotropy (FA) and mean diffusivity that have shown only modest interest in Parkinson's disease. More recently, another diffusion-derived metric, free water, has shown better performance than FA to detect changes in the SN in Parkinson's disease. Free water changes are also detected early at the prodromal stage, increase with disease progression, correlate with striatal dopaminergic function and predict clinical changes in some studies. NM, iron and free water changes in the SN are not specific for the diagnosis of Parkinson's disease, as atypical forms of parkinsonism present similar abnormalities. All three markers are potential candidates for trials of disease modifying therapies, but their usefulness remains to be validated. Lastly, the development of a multiparametric MRI approach including the three markers for the early and specific detection of Parkinson's disease could also be of interest.
PCO9
Clínica Universidad de Navarra, Spain
Multimodal neuroimaging has identified key biomarkers associated with cognitive decline and dementia conversion in Parkinson’s disease (PD). [18F]-FDG-PET studies reveal that hypometabolism in posterior cortical regions—particularly the parieto-temporo-occipital cortex—strongly predicts future dementia, outperforming anterior or focal deficits. This posterior cortical hypometabolism represents an early marker of functional network disruption and impending cognitive deterioration.
Dopaminergic dysfunction contributes to early cognitive changes. Dopamine loss in the associative and limbic striatum correlates with deficits in early PD. Selective involvement of the anterior putamen and caudate nucleus in drug-naïve patients increases dementia risk, and a reduced putamen-to-caudate uptake ratio on DAT-SPECT at onset predicts cognitive decline.
Cholinergic alterations further accelerate deterioration. Reduced volume of the nucleus basalis of Meynert (NBM) and microstructural abnormalities on diffusion tensor imaging precede gray matter loss and predict early impairment. Cortical cholinergic denervation, often coexisting with caudate dopaminergic depletion, represents a synergistic neurotransmitter failure driving progressive decline.
Structural MRI findings show that hippocampal atrophy strongly predicts both mild cognitive impairment and dementia, while white matter hyperintensities independently affect long-term cognitive outcomes, highlighting vascular and microstructural contributions.
Functional MRI demonstrates early disruption of the default mode network, particularly reduced connectivity in bilateral prefrontal cortices before clinical symptoms appear. As decline advances, widespread dysfunctions affect frontostriatal, limbic, thalamo-insular, frontoparietal, and attention networks, accompanied by degeneration of cholinergic and noradrenergic pathways.
Finally, coexisting β-amyloid pathology in cortical and striatal regions is linked to more severe cognitive impairment than cortical amyloid alone, suggesting an additive effect of diffuse β-amyloid burden.
Overall, cognitive decline in PD reflects interacting metabolic, dopaminergic, cholinergic, structural, and network-level abnormalities. Neuroimaging biomarkers—posterior cortical hypometabolism, striatal dopaminergic loss, NBM degeneration, and reduced default mode connectivity—offer powerful tools for early detection, risk stratification, and therapeutic targeting.
PCO10
Aarhus University, Denmark
During Parkinson’s disease (PD), α-synuclein oligomerizes and aggregates across multiple neuronal populations in both the central and peripheral nervous systems. This aggregation disrupts key cellular processes, neurotransmission, and neuronal function, ultimately leading to the characteristic motor and non-motor symptoms of the disease. These neurodegenerative changes occur in 2-Oral Sessionswith immune alterations. Innate immune cells respond to neuronal changes and α-synuclein aggregates, triggering inflammatory signaling cascades and activating the adaptive immune system. In addition, disturbances in crucial neuroimmune pathways, such as the gut–brain axis, further modulate systemic and local immune responses. The result is a complex interplay between innate and adaptive immunity that contributes to disease progression.
To mimic these events, diverse animal models have been developed to capture specific aspects of PD pathology and immune involvement. Toxin-induced, genetic models and α-synuclein based models have revealed that microglial activation, cytokine dysregulation, and T-cell infiltration are early and sustained features of disease development. These models have been invaluable in identifying immune mechanisms driving neurodegeneration and in testing immunomodulatory strategies. However, no single model fully reproduces the multifaceted neuronal and systemic immune interactions seen in humans.
In this talk, I will integrate findings from established and emerging animal models to highlight what we have learned about immune mechanisms in PD. I will discuss their translational potential and limitations, and reflect on how next-generation models might help to bridge the gap between experimental neuroimmunology and clinical intervention.
PCO11
Canada
Parkinson’s disease is characterized by a period of non-motor symptoms, including gastrointestinal dysfunction, preceding motor deficits by several years to decades. This long prodrome is suggestive of peripheral immunity involvement in the initiation of disease. We previously developed a model system in PINK1 KO mice displaying PD-like motor symptoms at late stages following intestinal infections. Herein, we map the initiating immune events at the site of infection in this model. Using single-cell RNAseq, we demonstrate that peripheral myeloid cells are the earliest highly dysregulated immune cell type followed by an aberrant T cell response shortly after. We also demonstrate an increased propensity for antigen presentation and that activated myeloid cells acquire a proinflammatory profile capable of inducing cytotoxic T cell responses. Together, our study provides the first evidence that PINK1 is a key regulator of immune functions in the gut underlying early PD-related disease mechanisms.
PCO12
California Institute of Technology, United States
Parkinson’s disease (PD) impacts over 10 million people worldwide and is the fastest growing neurological disease. While monogenic causes explain about 20% of PD, most cases likely arise from gene-environment interactions. The gut microbiome is a major environmental contributor to human health, influencing functions of the immune, metabolic, and nervous systems. Indeed, numerous studies report dramatic differences in microbiome profiles between individuals with PD and controls. Many PD patients have serious gastrointestinal (GI) issues such as constipation that often precede motor symptoms by many years and seriously impact quality of life. Accordingly, it is proposed that some forms of PD can originate in the gut, with pathology subsequently spreading to the brain, leading to neurodegeneration.
Aggregates of the neuronal protein α-synuclein (aSyn), a hallmark of PD, is prevalent in the intestines and brains of postmortem PD samples. We previously revealed that a gut bacterial amyloid named curli (encoded by the csgA gene) promotes aSyn aggregation in the colons and brains of mice, leading to motor symptoms. Since our discovery, clinical research has uncovered that the csgA gene is elevated in the microbiomes of many PD patients in numerous cohorts. Based on this work, we propose that the CsgA protein may represent a target for novel PD treatment.
We therefore developed a novel small molecule compound that inhibits CsgA aggregation. Remarkably, oral administration of AX-5006 potently reverses existing motor symptoms in multiple behavioral tests in a PD mouse model and also clears aSyn aggregates from the brains of mice. Built on innovative concept and basic research studies, our long-term goal is to unravel the pathophysiology of PD and develop breakthrough interventions that target the gut, rather than the more challenging prospect of delivering therapeutics to the brain.
PCO13
Radboudumc, Netherlands
In this presentation we will discuss thr unique challenges persons with young onset Parkinson's disease face in there daily live. We will address epidemiology, clinical presentation and therapy choices special to the young Parkinson's disease persons. Fuurthermore we will show the special approach we developed in the Netherlands which we co-created together with persons living with young onset Parkinson's disease. The voice of the persons living with young onset Parkinson's disease will be addressed throughout the presentation.
PCO14
Rush University Medical Center, United States
Early Onset Parkinson’s Disease (EOPD), defined by symptom onset before age 50, presents unique and profound psychosocial challenges distinct from late-onset PD. This presentation explores the multifaceted impact of EOPD through clinical vignettes and a synthesis of current literature, highlighting the biographical disruption and evolving identity experienced by individuals navigating diagnosis, treatment, and life with this condition.
Key psychosocial domains affected include:
Mental Health: Individuals with EOPD face significantly higher rates of depression, anxiety, substance use, and psychiatric hospitalization. The diagnostic journey is often prolonged and traumatic, with symptoms frequently misattributed to psychological causes. Social and Occupational Roles: EOPD often coincides with peak career and caregiving years, leading to early retirement, unemployment, and economic strain. Disclosure fears and stigma further complicate workplace accommodations and interpersonal relationships. Sexual and Reproductive Health: Sexual dysfunction, diminished intimacy, and relationship dissatisfaction are prevalent. Family planning and pregnancy in PD remain under-researched, though emerging guidelines support safe management with levodopa and DBS during pregnancy. Social Cognition: Alterations in empathy, theory of mind, and facial emotion recognition may impair interpersonal dynamics, contributing to marital strain and isolation.
Despite these challenges, EOPD can serve as a positive inflection point. Opportunities for growth include increased advocacy, research participation, career pivots, and deeper social connections. Resources tailored to individuals with EOPD and their care partners are expanding, offering support across domains. This session aims to equip participants with insights and tools to better recognize and address the psychosocial needs of individuals with EOPD, fostering holistic, person-centered care.
PCO15
Parkinson's Europe, Germany
In this short talk I will share my experience from having attended 3 WPCs. How to get the most out of the WPC depends what you are here to do. If it's your first time, you might be looking for information on how better to manage your disease. Repeat attendees will be aiming for a mixture of information and networking. Leave this session with ideas on how best to manage your time here.
PCO16
Icahn School of Medicine at Mount Sinai, United States
There are a myriad of reasons why genetics is important in Parkinson’s, and especially young-onset Parkinson’s (YOPD): Genetic causes are more likely to be identified in YOPD, therapies are being developed to target the genetic changes or the effects of the genes, with some trials already on-going, and there are other ramifications.
Parkinson’s disease (PD) is a complex genetic disorder. This means that even when people have gene changes (called variants) that are closely associated with developing PD (so-called “highly penetrant” genes, or major genes), not all people who have these gene variants will develop PD. Regardless of penetrance, environmental factors and other individual differences also play a role in PD. Further, it is not only the gene that matters but the specific variant. For example some variants in the GBA1 gene, called “severe” variants are much more likely to cause Parkinson’s than “risk” (and more common) variants in the same gene.
When variants are identified, most people have inherited these from one or both parents.
Major genes where a person with PD has to inherit a variant from both the mother AND the father (autosomal recessive inheritance) include PRKN, DJ-1 and PINK1. People with YOPD are more likely have autosomal recessive genes, esp PKRN. While children of people with autosomal recessive PD always inherit one copy of the variant from the parent with 2 recessive copies, they are unlikely to develop PD, as they do not usually inherit the variant from the other parent.
Examples of major genes where a variant only needs to be inherited from one parent, either the mother OR the father, (autosomal dominant inheritance) include LRRK2 and GBA1 and the less common SNCA and VPS35 genes. The children of a person with PD who has a variant in one of these autosomal dominant genes, have a 50% chance of inheriting the gene variant. However, even if a child inherits the variant, because of incomplete penetrance, the child has a risk of PD, but will not necessarily develop PD, and this depends on which gene and variant are identified.
Exciting therapies are being developed that target the genetic changes, or the effects of the genes on the proteins they encode, and some are already in trials (see clinicaltrials.gov). Genetic testing is usually performed for trial entry. Genetic counselors can aid in considering implication of genetic testing and interpreting results, and in connecting people with genetic testing resources.
2-Oral Sessions
O1
Radboud University Medical center, Netherlands
In clinical practice, a diagnosis of Parkinson’s Disease or Dementia with Lewy Bodies is based on the presence of overt motor or cognitive features. However, the underlying pathological processes begin many years before these core features become clinically overt. Indeed, over 60% of dopaminergic nigrostriatal neurons have already been lost when the cardinal motor features of Parkinson’s Disease finally emerge, and – similarly – the state of neurodegeneration is already advanced when dementia and core clinical features of Dementia with Lewy Bodies become manifest. This advanced stage of pathology hinders the potential efficacy of disease-modifying interventions.
Recently, two biological frameworks have been developed which aim to redefine Parkinson’s Disease and Dementia with Lewy Bodies based on biological criteria: SynNeurGe and NSD-ISS. The purpose of these frameworks overlaps: both are classification systems that define disease subtypes, including the earliest phases that predate overt parkinsonism or dementia. The NSD-ISS additionally proposes a staging system that rates the putative extent or severity of the disease in an individual. Both frameworks are based, in part, on the weighted sum of genetic risks, presence of pathological alpha-synuclein and loss of dopaminergic neurons, but there are differences in how the frameworks are operationalized.
Although still tentative and in need of robust validation, these frameworks pave the way for new research into disease modification in Parkinson's Disease, Dementia with Lewy Bodies and – to varying extents – related disorders. This presentation highlights exciting opportunities introduced by these frameworks, as well as remaining challenges in the definition, classification and staging of disease, which will be the focus of further studies over the next years.
O2
University of Toronto, Canada
Over the past decade, the landscape of biomarkers for α-synucleinopathies has been transformed by the advent of seed amplification assays (SAAs), which provide a direct, ultrasensitive readout of the underlying protein misfolding process in Parkinson’s disease, multiple system atrophy, and dementia with Lewy bodies. These assays now achieve diagnostic accuracies exceeding 90%, representing one of the most significant advances in biomarker development for neurodegenerative diseases.
In 2026, the field is moving beyond proof-of-concept toward quantitative and biologically informative SAA applications. Novel kinetic analyses, digital platforms, and endpoint quantification strategies are enabling the estimation of seeding burden and potency, offering new opportunities to track disease progression, stratify patients, and assess target engagement in therapeutic trials. This evolution marks a shift from binary detection to quantitative pathology-based biomarkers, bridging molecular pathology with clinical phenotypes.
Importantly, the reach of α-syn SAAs is now extending beyond classical synucleinopathies. Positive seeding activity has been reported in a subset of Alzheimer’s disease, progressive supranuclear palsy, and normal pressure hydrocephalus cases, underscoring the prevalence of α-syn co-pathology and its potential contribution to disease heterogeneity. These findings highlight the emerging role of α-syn SAAs as a window into the broader spectrum of neurodegenerative proteinopathies, redefining how we conceptualize and classify overlapping pathologies.
The lecture will address the current state and future directions of α-synuclein biomarkers, emphasizing assay standardization, multicentre validation efforts, and advances in quantitative and high-throughput SAA technologies. Finally, it will discuss how the integration of clinical, omics, and imaging biomarkers with α-syn, tau, and TDP-43 SAAs provides a powerful framework for precision diagnosis, biological staging, and trial readiness across parkinsonian and related neurodegenerative disorders.
O3
Stanford University, United States
Recently proposed frameworks for a biological definition of Parkinson’s Disease (PD) have been developed to address critical areas of unmet need , i.e. to enhance diagnostic precision in people presenting with parkinsonian symptoms, to enable early diagnosis independent of the presence of clinical symptoms and to develop objective measures for disease staging . These current frameworks have already sparked intense scientific discussion and multiple research efforts to test their validity, which will address the current uncertainty that need to be resolved before these concepts are ready to become implemented in the clinical arena to benefit people with PD or those at risk for disease.
These include assays that go beyond simply detecting and quantifying alpha-synuclein pathology as a central diagnostic anchor, opportunities to improve the scalability and reliability of the current assays for widespread use of alpha-synuclein seed amplification assays (SAA’S) in clinical routine, and ultimately development of more accessible tests, such as blood-based tests. Another area that needs better underunderstood is that, much like final pathology, a positive alpha-synuclein SAA biomarker can be present in individuals who meet clinical criteria for other disorders, including Alzheimer’s disease or PSP. In addition, there is limited, but growing, information regarding the future risk for clinical symptoms in asymptomatic individuals. For instance, it is unknown the rate and timeline of developing clinical symptoms for the 5-10% of older asymptomatic adults who have positive tests. Finally, the predictivity for clinical symptoms also needs to be defined in prospective long-term studies of individuals with traditional PD-risk factors.
Before clinical usage it is critical we understand how a biological framework anchored on biomarker evidence for alpha-synuclein pathology could be used in 2-Oral Sessionswith traditional clinical definitions, as certain subgroups of people with classical clinical PD would not be evaluable under a biological framework due to absence of such laboratory evidence. Lastly, a biological staging system of disease severity, that is based on objective and quantifiable biomarkers and anchored around clinically meaningful function impairment, needs better developed and ultimately validated in prospective cohorts.
O4
Tidewater Physicians Multispecialty Group, United States
For people living with PD, the shift from clinical staging to biological staging enables earlier detection, guides personalized interventions, improves disease monitoring, expands eligibility for biomarker-driven clinical trials, and ultimately fuels the hope of disease-modifying or preventive therapies. In short, biologic definition and staging can transform the patient–physician relationship from one based on symptom management that may be less understood by the patient into a transparent, collaborative partnership rooted in science, honesty, and shared goals.
Why it Matters?
Earlier detection and diagnosis – Provides the opportunity to educate individuals about their risk for neurodegenerative disease before movement symptoms appear. Adherence to healthy lifestyle factors is higher with personalized education. Biologic definition may help facilitate eligibility for research studies, creating more opportunities to enroll patients based on biological markers and for patients to benefit from emerging gene therapies. Better Planning for Future Needs - If you know that you have a pre-clinical biomarker for Parkinson’s, Lewy Bodies or another Parkinsonism, it should and can influence life and financial planning. Movement toward Precision Medicine - Biologic staging for PD may help stratify patients into subgroups for more effective, targeted treatments and personalized treatment based on a person’s unique genetic makeup. Better Tracking of Progression of Disease – biological staging may help give patients a clearer picture of the individualized progression of disease and can better prepare them emotionally, practically, financially, and medically for the future. Strengthen Patient – Physician Relationship - Biologic definitions give patients a clearer explanation of what is happening in their body. Instead of staging based on symptoms, the dialogue changes to a discussion of measures based on what is happening inside the body. This new framework of communication encourages a relationship where the patient and physician are better able to talk honestly about what to expect next, without overwhelming patients with uncertainty. Promotes earlier Access to Care and New Research Entrants into the Field – A biologic definition could lead to earlier diagnosis and therefore earlier access to care. Biologic definition should also encourage more research and by extension encourages more people to enter this research area earlier in their careers.
O5
Radboud University Medical Center, Netherlands
Wearable sensors can be used to monitor motor and non-motor signs in daily life, offering opportunities to improve clinical trials and support personalized care. In particular, clinical trials focusing on disease-modifying therapies are expected to benefit from more sensitive digital biomarkers to capture disease progression in early-stage or even prodromal Parkinson’s disease (PD). Passive (i.e., continuous) monitoring is a promising approach to capture everyday functioning in an unobtrusive fashion, yet little is known about its ability to capture long-term progression.
In this talk, I will present recent insights from the Personalized Parkinson Project, a longitudinal study following 623 individuals with early-stage PD. For two to three years, participants were monitored nearly continuously —on average 21 hours per day— using a wrist sensor that captured raw movement and heart rate data. From this, we derived digital biomarkers for tremor, reduced arm swing during gait and altered heart rate regulation. All algorithms were made available to the community in the form of an open-source toolbox (ParaDigMa). I will share insights into the digital biomarkers’ ability to measure disease progression, and place the findings in the context of earlier studies. In addition, I will discuss challenges and opportunities of using continuous, real-life data, and conclude with future perspectives on the place of digital biomarkers in the growing landscape of measurements for PD.
O6
Oregon Health & Science University, United States
Gait is a fundamental aspect of mobility and a sensitive marker of health and disease. Changes in gait patterns often precede clinical symptoms in many conditions, particularly for neurodegenerative diseases, such as Parkinson’s disease (PD). However, traditional gait assessments conducted in clinical or laboratory settings capture only brief snapshots of walking, limiting their ability to reflect day-to-day variability and functional mobility. Advancements in digital technologies, such as wearable inertial sensors, smartphones, and home-based systems, enable continuous, unobtrusive monitoring of gait in real-world environments. These tools provide objective, high-frequency data on key gait parameters, including stride length, gait speed, cadence, variability, and asymmetry. Capturing this information in daily life offers valuable insights that are often missed during episodic clinical visits.
This presentation will focus on monitoring and improving real-world gait in PD with an emphasis on sensitive markers of early disease, progression, and fall risk prediction. Longitudinal data indicate that changes in gait and turning behavior observed in daily life can emerge before alterations detected by traditional clinical scales (e.g., MDS-UPDRS) or laboratory-based assessments. Moreover, increased variability in gait and turning are among the strongest predictors of falls in individuals with PD. Early detection of these markers through digital monitoring enables timely interventions, such as physiotherapy, assistive devices, or home modifications, to reduce fall risk and improve safety. Real-world data can reveal subtle functional decline before it becomes apparent in clinical evaluations, supporting earlier diagnosis and better tracking of treatment effects over time. Despite challenges related to standardization, data interpretation, and integration into clinical workflows, the potential benefits for patient outcomes and healthcare systems are substantial.
O7
Purdue University, United States
Speech and swallowing impairments are highly common in Parkinson’s disease (PD), with over 90% of individuals experiencing dysarthria (speech problems) and dysphagia (swallowing issues) during the disease course. These problems greatly affect health and quality of life and are linked to increased risks such as malnutrition, respiratory infections, and social isolation. Traditional in-person assessments and treatments for speech and swallowing are limited by accessibility, cost, and the intermittent nature of clinical visits, highlighting the urgent need for reliable and valid remote management solutions. Recent advancements in digital health technologies and wearable devices offer promising avenues for capturing key features of speech and swallowing in real-world settings and providing remote management opportunities. The state of the science includes the development of smartphone-based acoustic analysis, improvements in speech recognition algorithms, sensor-equipped wearable patches (e.g., accelerometers, surface electromyography), and AI-driven algorithms capable of detecting early signs of dysfunction or improving biofeedback strategies. Several pilot studies have demonstrated feasibility, moderate-to-strong correlations with clinical gold standards, and promise for long-term monitoring. However, large-scale validation, regulatory approval, and integration into clinical practice are ongoing challenges. Continued innovation and interdisciplinary research are essential to enable proactive, personalized speech and swallowing care for individuals with PD and other neurogenerative diseases. This presentation will end by highlighting upcoming developments in this area that could revolutionize speech and swallowing management for patients with PD.
O8
University Hospital Erlangen / FAU Erlangen-Nürnberg, Germany
Parkinson’s disease (PD) pathology is driven by lysosomal dysfunction, which impairs clearance of α-synuclein (SNCA) aggregates. Our work integrates insights into lysosomal cathepsins (CTSB, CTSL, CTSD) and GBA1-encoded β-glucocerebrosidase (GCase) function as well as their potential as therapeutic targets. The autophagy-lysosomal pathway is crucial for maintaining neuronal homeostasis, and defects in this system are increasingly recognized as central to PD and other neurodegenerative diseases. Lysosomal cathepsins, including CTSB, CTSL, and CTSD, are key proteases involved in the degradation of disease-associated proteins. Their role in SNCA clearance, however, is only beginning to be fully understood.
Using dopaminergic neurons derived from PD patient iPSCs and transgenic mouse models, we demonstrate that lysosomal dysfunction is a hallmark of synucleinopathy. We show that recombinant human procathepsins (rHsCTSB, rHsCTSL, rHsCTSD) are efficiently endocytosed by neurons, correctly trafficked to lysosomes, and matured into active enzymes. Treatment with these proteases leads to a significant reduction of insoluble SNCA in both neurons and brain slices. Notably, this treatment not only reduced pathological SNCA conformers but also restored endo-lysosomal and autophagy function, highlighting the critical role of lysosomal cathepsins in SNCA clearance.
2-Oral Sessionsinvestigations into GBA1 variants (E326K, N370S, L444P), which represent some of the highest genetic risk factors for PD, reveal that lysosomal GCase activity can be partially rescued by overexpressing its transporter, LIMP-2. Structural cryo-EM analysis identified helices 5 and 7 of LIMP-2 as essential for binding GCase via a hydrophobic interface and a key salt bridge. Furthermore, a LIMP-2-derived peptide was shown to enhance lysosomal GCase activity in PD patient fibroblasts, underscoring its therapeutic potential. GCase deficiency, which leads to glucosylceramide accumulation and promotes SNCA aggregation, can be mitigated by activating and/or stabilizing the GCase enzyme.
Collectively, these findings converge on lysosomal trafficking and protease activity as dual pillars for SNCA clearance in PD. Enzyme replacement strategies—including procathepsins and GCase chaperones—as well as LIMP-2-derived peptides, emerge as promising approaches to counteract proteostatic failure in PD, offering new hope for disease-modifying therapies in PD and related synucleinopathies.
O9
Walter and Eliza Hall Institute of Medical Research, Australia
Mutations in the PINK1 protein cause early onset Parkinson’s disease. PINK1 is a ubiquitin kinase that accumulates on the outer membrane of damaged mitochondria. Upon accumulation, PINK1 becomes activated and phosphorylates ubiquitin, generating a unique phospho-ubiquitin signal that triggers mitophagy, the process of removing damaged mitochondria. Enhancing PINK1 activation is a promising strategy for boosting mitochondrial turnover in Parkinson's patients. Using Cryo-EM, we recently visualised human PINK1 for the first time, docked on the surface of mitochondria. In this talk, I will present our structure of human PINK1 and explain how we are using our structural platform to study mechanisms of PINK1 activation. These findings open up new therapeutic possibilities for using PINK1 to promote the turnover of damaged mitochondria in Parkinson’s patients.
O10
Weill Cornell Medicine, United States
α-Synuclein exists in an equilibrium between a membrane-bound pool on synaptic vesicles and a cytosolic pool. Physiologically, through its synaptic vesicle-bound pool, α-synuclein is enriched at nerve terminals, clusters synaptic vesicles, and chaperones SNARE-complex assembly to maintain neuronal communication. In contrast, aggregated α-synuclein is the major component of Lewy bodies in various neurodegenerative disorders including Parkinson’s disease and Lewy body dementia. α-Synuclein pathology is proposed to originate from a toxic-gain-of-function of aggregating α-synuclein, and approaches to eliminate α-synuclein in the brain represent an active area of research for treating synucleinopathies. Yet, α-synuclein aggregation may also endanger neurons by removing it from synaptic vesicles and thereby diminishing its function in a loss-of-function event. This loss-of-function is predicted to aggravate with accelerated aggregation of α-synuclein, such as in patients with α-synuclein gene multiplications and mutations. It is also controversial if aggregation of α-synuclein initiates from its lipid-bound α-helical form or from its unstructured cytosolic state: membranes have been reported to both accelerate and inhibit α-synuclein fibril formation. Strikingly, all familial Parkinson’s disease mutations are located within the lipid binding domain of α-synuclein. This suggests that changes in membrane binding affect both α-synuclein physiology and pathology. Yet, factors that determine membrane association and dissociation of α-synuclein remain poorly understood. Using in vitro, in cellulo, and in vivo readouts, we have identified multiple factors affecting the membrane binding of α-synuclein, offering new diagnostic and therapeutic strategies for synucleinopathies.
O11
University of British Columbia, Canada
Parkinson’s disease (PD) is characterized by profound clinical and biological heterogeneity, motivating decades of research to identify meaningful disease subtypes. Early attempts at subtyping relied on single factors such as age at onset or motor phenotype, distinguishing tremor-dominant from postural instability–gait difficulty (PIGD) forms. While these classifications provided initial insights into differential progression and therapeutic response, they proved unstable over time and insufficient to capture the full spectrum of PD variability. More recent data-driven approaches, leveraging multivariate analyses and large longitudinal cohorts, have advanced the field by integrating both motor and non-motor domains. These analyses have consistently revealed reproducible patterns, including a mild motor-predominant subtype and a more diffuse form characterized by a complex constellation of non-motor features—cognitive, autonomic, and sleep-related symptoms—often associated with a faster rate of progression. The scope of subtyping has since expanded to include the prodromal phase of PD and patient-reported experiences, recognizing that meaningful stratification must begin before motor onset and incorporate symptoms most relevant to individuals with PD. Using patient-reported outcomes from large digital cohorts such as Fox Insight, novel subtyping models have emerged that cluster individuals based on self-identified, bothersome symptoms, offering a complementary perspective grounded in lived experience. Biomarker research has further strengthened the biological foundation of PD subtypes. Analyses of dopaminergic imaging, structural MRI, and cerebrospinal fluid markers have revealed significant differences among subtypes, demonstrating that these clinical distinctions reflect true pathophysiological diversity rather than purely descriptive groupings.
O12
Luxembourg Institute of Health; University of Luxembourg; Centre Hospitalier de Luxembourg, Luxembourg
Rejko Krueger, MD (1,2,3)
Luxembourg Institute of Health, Luxembourg Luxembourg Centre for Systems Biomedicine, University of Luxembourg, Luxembourg Centre Hospitalier de Luxembourg, Luxembourg
Parkinson’s disease (PD) is increasingly recognized as a heterogenous neurodegenerative movement disorder. Traditional clinical subtypes (e.g., tremor-dominant vs. akinetic-rigid) fail to capture the underlying molecular diversity driving disease onset, progression, and treatment response. Recent advances across genetics and biomarker research have led to the proposal of biologically defined PD subtypes that reflect distinct pathogenic mechanisms.
In this context some genetically defined forms of PD can be considered as prototypes for different disease mechanisms and provided a first shift toward a biologically grounded PD classification. In this context converging evidence supports different mechanistic axes: (1) pathological protein aggregation based on mutation in the α-synuclein gene causing either conformational changes or increasing the overall expression of the protein (2) mitochondrial and bioenergetic impairment due to mutations in nuclear encoded mitochondrial genes, (3) lysosomal dysfunction related to GBA-associated PD (lysosomal dysfunction and accelerated cognitive decline) and neuroinflammation based on dysregulation of the innate or adaptive immune system observed in LRRK2-associated PD. All these pathways have been reproduced in the common sporadic, idiopathic form of PD using proteomic and transcriptomic datasets to establish specific signatures and recently polygenic risk score for mitochondrial dysfunction was functionally validated in neuronal cells derived from sporadic PD patients. Recognizing PD as a spectrum of different biological subtypes has major implications for translational research. Mechanism-matched enrichment - such as targeting lysosomal signatures or GBA carriers for disease modifying therapies - may increase trial efficiency and therapeutic precision. In summary, converging evidence from genetics and molecular assays like alpha-synuclein seed aggregation (SAA) supports a biologically based taxonomy of PD. The field is now transitioning towards a mechanism-driven framework for stratification of PD into different subtypes that allows for intelligent clinical trial designs and lay the foundation for precision medicine in PD.
Keywords: Parkinson’s disease, stratification, α-synuclein, genetics, precision medicine
O13
Stanford University, United States
Two recently proposed frameworks for a biological definition of Parkinson’s Disease (PD) – grouped under a new umbrella term of neuronal synuclein disease (NSD) in one of them - have used 3 types of biomarkers to define the presence of disease independent form clinical symptoms: evidence for the presence of alpha-synuclein pathology in, seed amplification assays (SAA), imaging findings of dopaminergic denervation and carrier status of PD associated genetic mutations. These proposed frameworks differ in a number of aspects – including a disease staging component in one but not the other - but a key similarity is that they both are currently considered only Research frameworks. Before such diagnostic and staging concepts are ready to be implemented in clinical care there are several key developments that need addressed. Some of the most important include the following:
Alpha-synuclein SAA’s need to become standardised and reliably available worldwide and, ideally, blood-based or other peripheral tests are ideal for widespread use in clinical routine. The former also applies to other matrices to detect alpha-synuclein like skin biopsies.
The predictive value of abnormal test results in neurologically asymptomatic individuals and those with minimal symptoms needs to be studied in prospective observational cohorts.
There needs to be research to understand the different biomarker profiles that can occur in people with a PD clinical symptom, in particular how to understand synuclein-assay negative clinical PD.
Quantitative biomarkers to stage disease severity must be developed and validated – including novel imaging modalities like alpha-synuclein PET.
Resources for physician training on when to order and how to interpret biomarker findings and for proper counseling of both people with PD as well as those at risk or simply concerned must be made available.
These and other issues will be discussed with participants.
O14
University of Toronto, Canada
The development of alpha-synuclein (α-syn) biomarkers has revolutionized our ability to detect and study Parkinson’s disease (PD), multiple system atrophy (MSA), and dementia with Lewy bodies (DLB) at the molecular level. Seed amplification assays (SAAs) now allow researchers to detect minute amounts of misfolded α-synuclein aggregates with extraordinary sensitivity and specificity, transforming these disorders from clinicopathological to molecularly defined diseases.
This 2-Oral Sessions will provide an informal, in-depth discussion on the current state and future directions of α-synuclein biomarkers. After a brief overview of key concepts—ranging from assay principles and validation challenges to interpretation of SAA kinetics—participants will be encouraged to explore practical questions such as:
How can SAAs be implemented in clinical and research settings?
What do quantitative SAAs tell us about disease burden and progression?
How do α-syn assays relate to other biomarkers such as NfL, tau, and imaging measures?
What are the challenges of translating laboratory findings into clinical tools?
O15
Radboud University Medical center, Netherlands
In clinical practice, a diagnosis of Parkinson’s Disease is based on the presence of overt “motor” signs, such as slowness of movement, tremor and rigidity. However, the underlying disease processes are already advanced when motor signs of Parkinson’s finally become overt in an affected individual. This advanced disease stage is likely a reason why it has proven so difficult in clinical trials to effectively slow Parkinson’s.
Recently, two new frameworks (SynNeuGe and NSD-ISS) have been developed which aim to redefine Parkinson’s based on biological criteria. The purpose of these frameworks is to classify disease subtypes, including the earliest phases before motor signs become overt in an affected individual. The NSD-ISS additionally aims to rate the severity of the disease in an affected individual. Both frameworks are based in part on genetic risk, the presence of pathological alpha-synuclein and loss of dopaminergic neurons, but there are differences in how the frameworks are operationalized.
Although still tentative and in need of robust validation, these frameworks pave the way for new research into disease modification in Parkinson's Disease and related disorders. This 2-Oral Sessions session will highlight exciting research opportunities introduced by these frameworks. This session will also highlight remaining challenges in the classification and staging of Parkinson’s, including potential implications of the new biological frameworks for individuals who are classified as having early-stage Parkinson’s despite the absence of overt motor signs.
O16
Radboud UMC Nijmegen the Netherlands, Netherlands
Dr. Annelien Oosterbaan will lead this session on pregnancy and Parkinson's disease (PD). Although this combination is rare, it is becoming more common due to the global increase in Parkinson's disease, the fastest growing brain disorder, and the rising age of mothers.
Annelien was trained as a gynecologist and is the founder of the research project on women and PD at Radboudumc Nijmegen. She started this project after her own experiences revealed the enormous research gap regarding the hormonal influence on Parkinson's disease in women, as she herself was diagnosed with PD in 2016.
She became aware of a cyclical pattern in her PD symptoms and, as she prepared for her fourth pregnancy, she discovered that little research had been done in this area. The decision to become pregnant without a proper management protocol available and without any idea of what to expect made her feel uncertain at times, but she was convinced she had made the right decision. In hindsight, the experience of two recent pregnancies confirmed her belief that Parkinson's and pregnancy go well together and that having children does not have to be ruled out for women with YOPD.
Annelien and her team, in collaboration with an international, multidisciplinary team of experts in the fields of neurology and gynecology, designed the online international registry for pregnancy and Parkinson's disease: www.pregspark.com. Through this online registry, they collect information from women around the world who have been diagnosed with Parkinson's disease and are pregnant. They collect data on the course of the pregnancy and on the health of both mother and child after birth. By combining all this information, they hope to provide better guidance and more accurate information to women with Parkinson's who are pregnant in the future.
Annelien will share the lessons she has learned so far from research and her own experience.

O17
United States
The goal of managing of motor symptoms in Parkinson’s disease is to maximize mobility while minimizing side-effects of treatment which become disabling as the disease advances. Recent interventions that are designed to achieve this objective include oral carbidopa and levodopa extended-release capsules, and subcutaneous infusions of foscarbidopa and foslevodopa and apomorphine hydrochloride. In randomized controlled trials, the oral extended-release formulation of carbidopa-levodopa increased good on-time per dose by 1.55 hours compared to the immediate release formulation. Of the infusions, foscarbidopa and foslevodopa improved on time by 1.75 h compared to immediate-release carbidopa levodopa and apomorphine reduced off time by 1.89 h compared to placebo. Newer drugs awaiting FDA clearance that have shown promise to also improve on time without dyskinesias are tavapadon, a selective D1/D5 receptor partial agonist, and ND0612, a subcutaneous infusion of levodopa-carbidopa solution. Ongoing Phase 3 trials of Parkinson’s disease drugs designed to improve motor symptoms include CVNB424, a GPR6 receptor modulator, and P2B001, a combination of low doses of extended release rasagiline and pramipexole. While we await disease modifying therapies in Parkinson’s disease, pursuing scientific research of clinical treatments that minimize the impact of motor and non-motor symptoms on quality of life is imperative.
O18
Arizona State University, United States
There are a number of approaches currently in the research pipeline showing promise for treatment of gait and balance, including physical and cognitive rehabilitation, attentional strategies, robotics, and surgical techniques. This 2-Oral Sessions will provide an opportunity to discuss the current state of gait and balance treatments for people with PD, as well as new advances and treatments currently being assessed for effectiveness and deployabiliy.
O19
University of British Columbia, Canada
PET and SPECT are both forms of molecular imaging. While each has its advantages and disadvantages, both allow one to quantitate the distribution of chemical and metabolic changes in the brain. In Parkinson’s, where structural changes may be limited, particularly in early disease, this may be of particular value. The most widespread approach from a molecular imaging perspective is the assessment of striatal dopamine innervation, using a a variety of tracers for the membrane dopamine transporter (both SPECT and PET), fluorodopa PET (dopamine synthesis and storage) and vesicular monoamine transporter 2 (VMAT2) PET. While dopaminergic markers provide information on the neurotransmitter whose loss is a defining feature of PD, they are not specific for the diagnosis, as atypical forms of parkinsonism (AP) may result in similar abnormalities. Furthermore, the relationship between changes in dopaminergic imaging markers and clinical progression of PD is not straightforward, which means the findings in trials of disease modifying therapies must be interpreted with caution. From a molecular diagnostic perspective, glucose metabolic (FDG) PET may be more reliable to differentiate between PD and AP, and is also sensitive to the effects of both symptomatic and disease modifying therapies. Other molecular markers of interest include those that assess the impact of disease on other neurotransmitter systems (e.g. serotonin, norepinephrine, cholinergic) and those that assess mitochondrial function or neuroinflammation. These are largely at an experimental change, as are markers of abnormal protein deposition (tau or α-synuclein). The availability of a reliable tracer for abnormal α-synuclein deposition would be a major advance. While considerable progress has been made in the last few years, this is still at a developmental stage. It should be emphasized that no single imaging approach suits all purposes and the different approaches (including both molecular imaging and MRI) should be seen as complementary rather than competing.
O20
University of Malaya, Malaysia
In recent years, there has been growing interest in the close relationship between gut health and the brain. This connection, often referred to as the “gut–brain axis,” has been particularly relevant to Parkinson’s disease (PD), where gastrointestinal symptoms such as constipation and bloating are common and may appear years before movement symptoms. At the same time, research has shown that the trillions of microorganisms living in the gut—the gut microbiome—play important roles in digestion, immunity, metabolism, and even how drugs are absorbed by the body. Laboratory and clinical studies have suggested that changes in the gut microbiome and its chemical products (metabolites) may influence inflammation and other biological pathways linked to PD. These findings have sparked interest in whether improving gut health could positively impact PD symptoms or slow disease progression.
Several approaches are currently being explored. Dietary strategies aim to support beneficial gut bacteria through increased intake of fibre, plants, and fermented foods. Prebiotics (nutrients that feed gut bacteria) and probiotics (live bacterial supplements) have been tested for various symptoms in PD, with some early studies reporting improvements such as better bowel function. Other emerging strategies include targeted antibiotics, microbial metabolites, and fecal microbiota transplantation (FMT), although these remain experimental and are not yet widely used in clinical practice. A major challenge in developing gut-based therapies is that PD is highly variable from person to person, and the microbiome also differs widely based on age, diet, geography, lifestyle, and medications. For these reasons, it is unlikely that a single “one-size-fits-all” approach will work for every person.
In this rountable, a summary of the latest scientific evidence supporting dietary and probiotic therapies for PD will be presented, with an interactive discussion on what we know so far, and what remains under investigation. This session will also cover the frequently asked questions regarding diet and probiotic regiment for people living with Parkinson.
O21
JPG Enterprises LLC, Barrow Neurological Institute, United States
Many people believe that Parkinson’s disease (PD) solely affects movement; however, cognitive changes are also an important aspect of PD, often misunderstood or overlooked. Moreover, misperceptions can lead to delays in diagnosis, inappropriate interventions, or unnecessary anxiety for patients and their families. This session will address the common myths and misconceptions of cognitive changes in PD, including the assumption that cognitive decline only occurs in later stage PD, that PD-related dementia is identical to Alzheimer’s disease, and that the trajectory of cognitive decline is inevitable. Up-to-date research explaining the spectrum of cognitive changes in PD, emphasizing that cognitive impairment varies widely among individuals, will be covered. In addition, the session will address confusion about the timing and progression of cognitive symptoms in PD and diagnoses of Lewy body dementia (PD dementia and dementia with Lewy bodies). The role of medication and non-pharmacological strategies, along with intersections with mood and sleep in cognitive health, and lifestyle factors will be discussed. The session will conclude with tips on how to communicate effectively about cognition in PD, debunking myths compassionately while empowering patients and caregivers, and providing educational and support resources to challenge misconceptions and promote better outcomes for those affected by PD.
O22
University of Cambridge & Cambridge University Hospitals NHS Trust, United Kingdom
There is now a wealth of evidence from studies in both animal models and people with Parkinson’s to support the theory that immune activation contributes to progression of the disease. This has provided a strong rationale for testing immune-suppressing drugs in PD, and we have recently completed a clinical trial to evaluate whether this approach might be beneficial. The AZA-PD trial repurposed a drug called azathioprine, an immunosuppressant therapy which is already used to treat a variety of autoimmune and inflammatory conditions. 66 people were recruited and randomly allocated to receive either azathioprine or placebo for 12 months, and both participants and assessors were blinded to treatment group. There was no positive effect of azathioprine on the main clinical outcome measure (a measure based on examination of posture, walking and balance). However, people who received azathioprine reported an improvement in movement symptoms. This improvement was greatest in women. A subgroup of participants with higher progression risk also experienced an improvement in memory and thinking scores. Azathioprine reduced immune cells in the blood and cerebrospinal fluid and appeared to slow progression of inflammation in the brain. The results also showed that the drug was generally well tolerated in people with PD. Overall, the study has provided encouraging data to support further trials of immune-suppressing therapies for PD. Several other trials of drugs which modulate inflammation and immune responses are now underway. However the immune system is highly complex, and there is considerable variability in immune activation between different people with Parkinson’s. Our future goal is to implement immune-based treatments for PD which are targeted to the right immune pathways, in the right people with Parkinson’s, at the right time in their disease course.
O23
University of Malaya, Malaysia
The discussions for this (very large and interesting!) topic will cover: the increasing choices of medications besides levodopa that are useful to treat Parkinson’s motor symptoms (these include other dopamine replacement therapies [DRT] such as dopamine agonists, and related medications such as COMT inhibitors and MAO-B inhibitors); non-dopaminergic therapies (e.g., amantadine and clozapine); medication treatments for a variety of non-motor symptoms (in the domains of cognitive-behavioural [e.g., psychosis, depression, anxiety, cognitive impairment], sleep [e.g., insomnia, REM sleep behaviour disorder], autonomic [e.g., constipation, urinary urgency/frequency, low blood pressure], and sensory aspects [e.g., pain]); their roles in the context of early, middle, and later stages of PD; issues of efficacy and potential side effects, as well as practical aspects on optimizing delivery/effect.
O24
Barrow Neurological Institute, United States
This 2-Oral Sessions will stimulate discussion concerning changes in cognition or thinking in Parkinson’s disease (PD). Current definitions of mild cognitive impairment (PD-MCI) and dementia will be reviewed and some recent arguments for an update of diagnostic criteria will be discussed. Various types of cognitive changes affecting attention, executive functions, language, visual perception and memory will be highlighted, as will risk factors for cognitive decline in PD. Participants will be encouraged to discuss strategies they find helpful to ameliorate cognitive changes and minimize their impact on daily function and quality of life. Brief discussion will also be entertained regarding effects of treatments on cognition, especially medication and neuromodulation.
O26
Northwestern University Feinberg School of Medicine, United States
Parkinson disease (PD) is a neurodegenerative disorder marked by the preferential dysfunction and death of dopaminergic neurons in the substantia nigra. A question critical to understanding PD is which affected processes are central to the preferential vulnerability of dopaminergic neurons in the substantia nigra. Pinpointing the most relevant subcellular processes is challenging, in part because there are multiple distinct pathways that contribute to the vulnerability of these neuronal populations, and in part because the various cellular dysfunctions of PD probably reciprocally influence each other. To identify the most high-yield targets for therapeutic intervention, it is important to consider the core cellular compartments and functional pathways upon which such varied forms of pathogenic dysfunction may converge. We hypothesized that a large number of PD-linked causative and risk genes converge on recurring subcellular pathologies, suggesting potential functional nodes that may be central to selective vulnerability. To test this hypothesis, we have studied several PD genes, focusing on the mechanisms of their potential convergence in disease pathogenesis. These genes and corresponding pathogenic pathways primarily localize to a subset of subcellular compartments, including mitochondria, lysosomes and synapses. We discuss how these pathogenic mechanisms that originate in different cellular compartments may coordinately lead to cellular dysfunction and degeneration of nigral dopaminergic neurons in PD. We will also highlight recent development of targeted therapies that were informed by the identifications of such converging mechanistic pathways in Parkinson’s disease.
O27
Biomedical Research Foundation, Academy of Athens, Greece
The protein kinase LRRK2, linked both genetically and functionally to the pathogenesis and progression of Parkinson’s disease (PD), plays a critical role in many cellular processes; including vesicular trafficking (e.g. lysosomal function), immune cell response (e.g. phagocytosis, cytokine release), and cell death signaling. Each of these signaling “systems” contribute to PD, at different stages of the disease and in different cell types. In this talk, I will highlight some of the recent findings in the field, and from our own work, characterizing some of these links between LRRK2 function (and hyperactivity) and lysosomal (e.g. GCase activity), and immune cell function, both in terms of disease pathogenesis as well as propagation. Despite its complicated role in PD pathogenesis, the regulatory function of LRRK2 in these critical systems opens multiple points of potential therapeutic intervention, employing more selective and precision-designed tools.
O28
Denali Therapeutics, United States
Variants in LRRK2 and GBA1 represent two of the most common genetic contributors to Parkinson’s disease (PD), yet the molecular interplay between these genes and their shared effects on endolysosomal dysfunction remain poorly understood. Our work has revealed that LRRK2 kinase activity regulates the function of the lysosomal enzyme encoded by GBA1, glucocerebrosidase (GCase), and that LRRK2-dependent modulation of GCase activity drives compensatory changes in bis(monoacylglycerol)phosphate (BMP) levels in select cell types, including iPSC-derived microglia. We have found that LRRK2 inhibition reduces GCase substrate accumulation in preclinical models and in cerebrospinal fluid (CSF) from LRRK2-PD patients, supporting both the relevance of LRRK2-mediated regulation of GCase and the potential use of GCase substrates as CSF biomarkers of LRRK2 activity. With respect to GBA1, we have discovered that the E326K risk variant alters LRRK2 activity and contributes to a convergent lysosomal dysfunction. We show the E326K variant reduces lysosomal GCase activity by impairing its delivery to lysosomes via altered interactions with its receptor, LIMP2. Functionally, this variant produces more pronounced deficits in PD-relevant pathways than severe GCase loss-of-function mutations linked to Gaucher disease, effects that are recapitulated in CNS cell models and in human E326K carriers. Together, these findings uncover a mechanistic basis for E326K-associated GCase dysfunction and highlight a bidirectional interplay between LRRK2 and GCase that contributes to lysosomal dysfunction in PD.
O29
Stanford University School of Medicine & Nexus NeuroTech, United States
Over recent years, increasing computing power, availability of large and ever-increasing amounts of data, and improved algorithms have converged to enable exciting opportunities to apply artificial intelligence (AI) to characterize the transition from health to disease, measure disease burden, and track disease progression/regression–all useful aspects of clinical care. Particularly when coupling data from various sensors on the body or in the environment with clinically validated algorithms, there is an opportunity to enable continuous, data-driven monitoring. For disorders of the brain like Parkinson’s disease, these new capabilities are urgently needed, since the diagnosis and monitoring of these conditions still largely relies on relatively crude and subjective methods, such as the clinical exam, subjective patient reports, and symptom scales. As the use of AI in healthcare becomes more pervasive, its application in the clinical care for those with Parkinson’s disease presents exciting opportunities to improve the timeliness and accuracy of diagnosis and to optimize treatment.
A number of other conditions can mimic Parkinson’s disease, and arriving at an accurate diagnosis as soon as possible allows implementation of the most appropriate treatment plan. The application of AI to various data types has shown the utility in improving the accuracy of the diagnosis of Parkinson’s disease. Rather than relying on a single data type, applying AI to multimodal data, may allow the diagnosis of Parkinson’s disease with even greater accuracy and at earlier stages. Methods employing AI to interrogate multimodal data sets are also emerging as a means of identifying patient subgroups that each have a similar symptom profile, disease course, and/or expected treatment response. This will likely help in counseling individual patients about their expected clinical course and in efficiently personalizing treatment, overcoming some of the challenges that the heterogeneity of Parkinson’s disease presents. The use of AI-powered approaches for symptom and severity assessment, progression monitoring, and treatment management is also now becoming real.
Perhaps more than many other brain disorders, Parkinson's disease lends itself to the creation of rich data from which AI can surface actionable insights that hold the potential to revolutionize care in a personalized manner.
O30
University of Pennsylvania, United States
Big data is transforming how we study and care for people with Parkinson’s disease. This talk will examine how integrating large-scale clinical, biomarker, and digital datasets can enhance research and lead to more personalized care. Dr. Vizcarra will discuss how artificial intelligence and bioinformatics are being used to identify meaningful disease patterns, refine patient stratification, and support data-driven clinical trial design. By bridging research and real-world data, big data offers a pathway toward more precise, efficient, and patient-centered approaches to Parkinson’s care.
O31
Tel Aviv University, Israel
The integration of digital technologies into Parkinson's disease (PD) clinical trials represents a paradigm shift in how we capture, quantify, and interpret disease progression and response to medication. Traditional clinical endpoints, relying on infrequent in-clinic assessments and subjective rating scales, often failing to capture the complex, fluctuating nature of PD symptoms that patients experience in their daily lives. Digital health technologies—including wearable sensors, smartphone applications, and remote monitoring devices—offer unprecedented opportunities to collect continuous, objective, real-world data on motor and non-motor symptoms reflecting not only pathological symptoms but also disease burden.
This lecture will examine the current landscape of digital endpoints in PD clinical research. Examples will be provided on the use of accelerometers and gyroscopes to quantify tremor, bradykinesia, and gait disturbances; the use of smartwatches for monitoring medication response and wearing-off phenomena and the utility of smartphone-based tests for evaluating cognition, speech, and finger tapping. The presentation will discuss the technical and clinical validation status of these tools and the regulatory perspectives from the FDA and EMA regarding their qualification as primary or secondary endpoints.
We will conclude by assessing whether digital endpoints have truly "arrived" or whether significant technological, regulatory, and clinical barriers still separate promise from practice. Key challenges for widespread implementation will be highlighted including data quality and standardization across platforms, managing the computational burden of analyzing massive datasets, and demonstrating meaningful clinical relevance beyond statistical sensitivity. However, things are shifting. Recent successful incorporations of digital measures in phase II and III trials signal upcoming change in the field.
O32
Australia
Exercise and physical activity levels are low in people with Parkinson’s disease, despite evidence showing benefits to physical function, disease progression and quality of life. Sticking to exercise is difficult for most people. It can be more challenging with age. Many people with Parkinson’s disease have additional barriers that can make it difficult to adopt and stick with an exercise or physical activity plan as a part of a healthy lifestyle. These can include factors associated with motor symptoms, such as poor balance or slowed movement, but also importantly, non-motor symptoms such as fatigue, sleepiness, mood changes. Common factors that make it difficult for people with Parkinson’s disease to adopt and adhere to exercise and physical activity will be discussed. Strategies for people with Parkinson’s disease and their carers to assist them with the capability, opportunity and motivation to get going and keep going with exercise and physical activity will be presented.
O33
University of Auckland, New Zealand, New Zealand
Patients, caregivers, clinicians and researchers are moving towards non-pharmacological approaches such as diet and exercise in the management of Parkinson’s disease (PD). Much is now known about exercise, yet the role of diet requires further investigation. Not only that but adhering to dietary habits requires attention.
Research suggests that there are a number of barriers that people face when trying to modify their dietary habits. These include financial cost, the lack of prior exposure to a food, and uncertainty about how to prepare the food. Cultural norms and taste preferences are important considerations. The social context of sharing and eating food together within a family or household is a critical aspect of many cultures. As such, the adoption of a specific dietary habit may be more sustainable if all household members engage, if appropriate. Education, health literacy, family and social support and the food environment all play a role.
The aim of this presentation is to review the science around sustaining evidence-based eating habits in PD. It will conclude with future perspectives which hold promise.
O35
Paris Brain Institute, France
In this 2-Oral Sessions discussion, we will discuss magnetic resonance imaging (MRI) biomarkers in clinical practice, their ability to predict motor conversion in the prodromal phase of Parkinson's disease, and their potential role in clinical trials. We will address their diagnostic, prognostic, and disease progression monitoring roles. We will discuss longitudinal data linking imaging abnormalities to phenoconversion and disease progression stage. We will evaluate existing data on tissue changes and the pathophysiology associated with Parkinson's disease. We will examine technical reproducibility, standardization, availability, and prior use in clinical settings and clinical trials. We will discuss their relevance to biostaging models.
O36
Special Interest Group - Black Diaspora/PD Movers, United States
Background: Currently, Black inclusion and participation rates in Parkinson’s Disease clinical research are well below their census in the United States and in most PD research studies miniscule to nonexistent. Special Interest Group – Black Diaspora and our collaborators wanted to learn WHY from listening to our Black PD community’s view.
Methods: In the absence of spaces where our Black PD community felt comfortable or empowered to address PD health knowledge and treatment gaps and to address barriers to clinical study participation, we routinely brought together large gatherings of the Black PD Community including not just impacted members, but also health care providers. We then empower this cohort to prioritize the challenges they need addressed. Leadership Teams provided culturally diverse data, and leveraged models created through effective community engagement to support, awareness, resources and research. We promote the theme: YOU ARE NOT ALONE!
We naturally looked at the gaps and unmet needs of our community to determine pragmatic solutions. These groups range from the Alliance for Black Support Group Leaders to social networking groups (support group alternatives).
Results: In these groups, the prime focus is on building community first. In each of these groups, attendees are exposed to opportunities to be empowered, e.g. participate in research, talk to researchers, go to the community and tell their stories, be an author (books, videos) collaboration with other groups, opportunities to speak, opportunities to share their talents, and to share their stories. A strong cohort of PD advocates and activity participants is emerging.
Culturally sensitive best practice guides and educational articles and outreach materials are in development.
Discussion and Conclusion: The next steps are to continue to collaborate with Health Care Professionals, Medical Schools, Pharmaceuticals, Parkinsons organizations, patient voice organizations to provide more, models, tools, communications and research that will be culturally diverse within ALL PD communities.
O37
Clínica Universidad de Navarra, Spain
Multimodal neuroimaging has identified biomarkers associated with cognitive decline and dementia conversion in Parkinson’s disease (PD). Among these, [18F]-FDG-PET studies have demonstrated the highest sensitivity and specificity to date. They show that hypometabolism in posterior cortical regions—particularly within the parieto-temporo-occipital cortex—strongly predicts future dementia, outperforming anterior or focal metabolic deficits. This posterior cortical hypometabolism represents an early marker of functional network disruption and impending cognitive deterioration.
Other functional biomarkers play a less prominent role in predicting cognitive decline in PD. DAT-SPECT and F-dopa PET examinations assessing dopaminergic dysfunction have shown that involvement of the anterior putamen and caudate nucleus in drug-naïve patients increases the risk of dementia. Moreover, a reduced putamen-to-caudate uptake ratio at disease onset predicts subsequent cognitive decline. Cholinergic alterations are also known to accelerate deterioration, as reflected by reductions in the volume of the nucleus basalis of Meynert (NBM) and cortical cholinergic denervation detected by PET.
Hippocampal atrophy and vascular abnormalities observed on structural MRI likewise influence long-term cognitive outcomes. Functional MRI demonstrates widespread network dysfunctions associated with cognitive decline.
β-amyloid pathology, as assessed by PET in cortical and striatal regions, correlates with greater cognitive impairment but is not a reliable predictor of cognitive decline.
Overall, cognitive decline in PD reflects the interplay of metabolic, dopaminergic, cholinergic, structural, and network-level abnormalities. However, for most of these, no biomarker currently achieves sufficient sensitivity and specificity to predict dementia in early-stage PD. Posterior cortical hypometabolism remains the most promising marker identified so far.
O39
Aarhus University, Denmark
Over the past twenty years, studies using animal models have greatly helped us understand how the immune system and the brain interact in Parkinson’s disease (PD). Research has shown that early changes in immune activity — including inflammation in the brain and signals from the body’s immune cells — play an important role in how the disease develops and progresses. These models have also helped us explore how changes in the immune system might contribute to neuronal damage and the symptoms of PD. However, no animal model can fully reproduce what happens in people with Parkinson’s. This makes it challenging to translate experimental findings into treatments for patients, especially when testing therapies that aim to target the immune system. In this round table, we will discuss what animal models have taught us about the role of immunity in PD, what their limits are, and how new models might better reflect the human condition to guide future therapies.
O42
California Institute of Technology, United States
Parkinson’s disease (PD) impacts over 10 million people worldwide and is the fastest growing neurological disease. While monogenic causes explain about 20% of PD, most cases likely arise from gene-environment interactions. The gut microbiome is a major environmental contributor to human health, influencing functions of the immune, metabolic, and nervous systems. Indeed, numerous studies report dramatic differences in microbiome profiles between individuals with PD and controls. Many PD patients have serious gastrointestinal (GI) issues such as constipation that often precede motor symptoms by many years and seriously impact quality of life. Accordingly, it is proposed that some forms of PD can originate in the gut, with pathology subsequently spreading to the brain, leading to neurodegeneration.
Aggregates of the neuronal protein α-synuclein (aSyn), a hallmark of PD, is prevalent in the intestines and brains of postmortem PD samples. We previously revealed that a gut bacterial amyloid named curli (encoded by the csgA gene) promotes aSyn aggregation in the colons and brains of mice, leading to motor symptoms. Since our discovery, clinical research has uncovered that the csgA gene is elevated in the microbiomes of many PD patients in numerous cohorts. Based on this work, we propose that the CsgA protein may represent a target for novel PD treatment.
We therefore developed a novel small molecule compound that inhibits CsgA aggregation. Remarkably, oral administration of AX-5006 potently reverses existing motor symptoms in multiple behavioral tests in a PD mouse model and also clears aSyn aggregates from the brains of mice. Built on innovative concept and basic research studies, our long-term goal is to unravel the pathophysiology of PD and develop breakthrough interventions that target the gut, rather than the more challenging prospect of delivering therapeutics to the brain.
O43
University of Wisconsin-Madison, United States
In Parkinson’s disease (PD), cognitive impairment frequently intersects with motor speech (dysarthria), swallowing (dysphagia), and gait deficits, contributing to reduced quality of life, social withdrawal, loss of independence, and heightened risks such as aspiration pneumonia and falls.
This talk will explore how cognitive domains—particularly attention, executive function, and working memory—support and constrain these functions. Evidence shows baseline cognitive deficits correlate with greater dysarthria severity (e.g., reduced intelligibility, prosodic impairment), increased dysphagia risk across oral and pharyngeal phases (e.g., premature spillage, residue, penetration/aspiration), and gait abnormalities (e.g., slower speed, shorter strides, variability, freezing). Dual-task paradigms reveal that dividing attention or raising cognitive load consistently worsens performance: speech becomes less clear and motor learning is impaired; swallowing safety and efficiency decline (with variable effects by cognitive severity); and gait deteriorates markedly, elevating fall risk due to competition for limited cognitive resources.
In PD, degraded motor automaticity increases reliance on cortical cognitive control, yet disease-related cognitive decline limits this compensation—creating a “double burden.” This interplay is often under-recognized in routine management of dysarthria, dysphagia, and gait.
The presentation will briefly discuss person-centered implications: incorporating cognitive screening into speech, swallowing, and gait evaluations; adapting therapies to individual cognitive profiles; and involving care partners. Early or prodromal cognitive support may build reserve and delay decline. Future directions include phenotype-specific approaches and deeper exploration of lived experiences across the cognitive continuum to advance holistic, synergistic care.
O44
University of Tasmania, Australia
Parkinson’s is the fastest-growing neurological condition worldwide, yet access to reliable, evidence-based information remains limited for many individuals and their support networks. In response, the University of Tasmania launched the Parkinson’s Massive Open Online Course (MOOC) in 2025, with support from the Parkinson’s Research Foundation.
This free, self-paced online course offers five comprehensive modules covering symptoms, pathology, treatment options, allied health therapies, and strategies for living with Parkinson’s. Designed for accessibility, the MOOC serves a diverse global audience—including people living with Parkinson’s, family, carers, health professionals, and advocates—by combining expert-led content with personal stories and strategies from those living with Parkinsons, as well as interactive learning tools.
The round table will explore the MOOC’s development, its approach, and its impact on knowledge, empowerment, and community building. Preliminary findings and feedback highlights increased understanding, reduced stigma, and enhanced confidence in managing Parkinson’s.
We would love to invite you to join us and contribute to a discussion on future directions, including topics, multilingual adaptations and integration with clinical and community care pathways.
By providing free access to high-quality education, the Parkinson’s MOOC exemplifies how digital tools can foster equity, inclusion, and hope in the global Parkinson’s community.
O45
Grenoble Alpes University, France
Recent advances in Deep Brain Stimulation for Parkinson’s disease
Since the mid-20th century, brain stimulation has played a role in Parkinson’s disease treatment. At first, it was mainly used to pinpoint where surgeons should perform permanent procedures. Over time, technology evolved, allowing for deep brain stimulation (DBS)—a method that is adjustable and reversible. Since the late 1980s, DBS has revolutionized how we treat advanced Parkinson’s. Today, it’s a recognized surgery for patients who experience motor issues and involuntary movements that medication can’t fully control. Studies confirm that it improves movement symptoms, though it doesn’t slow the disease itself. Over time, its effects may lessen—especially for symptoms like balance or speech. Not everyone qualifies, since patient selection is careful, and surgery plus follow-up programming require expertise. However, new technology is emerging. Personalizing DBS using brain signals, imaging, and smart software could improve long-term outcomes. New lead designs and combined techniques may also expand who can benefit, offering hope for even better, more inclusive care.
O47
Institute of Neurodegenerative Diseases-University of Bordeaux-CNRS UMR5293, France
Parkinson’s disease (PD) is a complex, progressive neurodegenerative disorder affecting millions worldwide. Developing effective therapies hinges on how accurately we model the disease in laboratory settings. Getting these models “right” is not merely a matter of scientific precision—it directly impacts the likelihood of discovering treatments that are both safe and effective for patients.
Traditional models of PD, including toxin-based animal models or genetic modifications, have provided invaluable insights into the disease's mechanisms. However, many of these models fail to fully replicate the multifaceted nature of human PD, particularly the progressive loss of dopaminergic neurons, non-motor symptoms, and individual variability. This disconnect has contributed to the high failure rate of clinical trials, where promising therapies in animal models often do not translate to humans.
Accurate disease modeling matters because it shapes how we understand disease onset, progression, and treatment response. Emerging technologies—such as patient-derived induced pluripotent stem cells (iPSCs), 3D organoids, and advanced computational models—offer more human-relevant systems. These models can reflect genetic diversity, age-related changes, and cellular environments more faithfully, allowing researchers to test drugs in conditions that closely mimic those in actual patients.
Furthermore, precision modeling can help identify disease subtypes, enabling personalized therapeutic approaches. Since PD manifests differently among individuals, a “one-size-fits-all” treatment is unlikely to succeed. Models that accurately represent various PD forms are crucial to discovering targeted interventions and to predicting which patients may benefit from which therapies.
Ultimately, getting PD modeling “right” is a moral and practical imperative. It reduces the cost and time of drug development, minimizes animal use, and improves patient outcomes by accelerating the path to truly effective treatments. As we push toward more nuanced and patient-centered research, refining our models will be central to transforming Parkinson’s disease from an incurable condition into a manageable one—and eventually, a preventable or reversible disorder.
O47
University of Piemonte Orientale, Italy
Peripheral immunity plays a crucial role in the pathogenesis and progression of Parkinson’s disease (PD), linking systemic inflammation to neurodegeneration in the central nervous system (CNS). Once considered a purely neurodegenerative disorder, PD is now recognized as a condition with significant immune dysregulation, where peripheral immune activation contributes to both the initiation and amplification of neuronal injury.
In the peripheral blood of PD patients, multiple immune abnormalities have been observed. Circulating monocytes, particularly the classical (CD14++CD16−) and intermediate (CD14++CD16+) subsets, show increased activation and elevated expression of major histocompatibility complex class II and Toll-like receptor 2. These changes indicate an enhanced capacity for antigen presentation and inflammatory cytokine release. Similarly, alterations in lymphocyte populations are common. CD4+ T cells exhibit a shift toward pro-inflammatory Th1 and Th17 phenotypes, secreting interferon-gamma and interleukin-17, while the proportion of regulatory T cells, which normally suppress immune activation, is reduced. CD8+ cytotoxic T cells also display heightened activity, with some recognizing α-synuclein-derived peptides, suggesting an autoimmune component directed against neuronal proteins.
The cytokine milieu in PD patients’ blood further reflects systemic inflammation. Increased levels of tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), interleukin-1β (IL-1β), and other pro-inflammatory mediators are consistently reported, often correlating with disease severity and progression. Elevated chemokines, such as CCL2 (MCP-1) and CXCL10 (IP-10), promote the recruitment of immune cells from the periphery to the CNS, potentially facilitating neuroinflammation.
Peripheral immune activation may also interact with the gut–brain axis. Chronic intestinal inflammation, barrier dysfunction, and altered gut microbiota can trigger systemic immune responses and provide α-syn antigens that prime peripheral immune cells. These activated cells and inflammatory mediators can cross a compromised blood–brain barrier, activating microglia and amplifying neuronal loss.
Overall, peripheral immunity in PD sustains a state of chronic, low-grade inflammation that bridges the gut, blood, and brain. This systemic immune dysregulation not only reflects the disease’s progression but also represents a potential therapeutic target for slowing or preventing neurodegeneration.
O48
Cure Parkinson's, United Kingdom
The goal of a "disease modifying therapy" (or DMT) is to alter the overall course of Parkinson's. That is: to slow, stop or reverse the progressive worsening of the symptoms. Researchers have attempted to do this using two basic approaches:
Testing neuroprotective interventions (agents that help to keep cells alive) Targeting the underlying disease-associated biology
There is a long history of the first approach, which has involved the clinical evaluation of different neuroprotective molecules that have demonstrated the ability to keep cells alive in preclinical models of neurodegeneration.
The second approach - targeting the underlying disease-associated biology - has arisen from research conducted over the last two decades that looks at the biological pathways associated with genetic risk factors. Parkinson's is not a genetic disease, but there are tiny variations in our DNA that can make us more vulnerable to developing the condition. By manipulating the biological pathways associated with those genetic variation, researchers hope to influence the progression of the disease. And the really exciting aspect of this research is that it has now developed to a point where we are in late-stage clinical testing of some experimental interventions that specifically target the biology believed to be influencing Parkinson's. In this presentation, you will be provided with an overview of the some of the biological pathways that are being therapeutically targeted.
O49
UCL Institute of Neurology, United Kingdom
The traditional approach of a using double-blind, placebo controlled, 2-Oral Sessionsgroup trial designs has not, to date, led to the discovery of any disease-modifying treatments for Parkinson's disease. There are multiple potential reasons underlying this which may in part relate to inadequate understanding of Parkinson's disease pathophysiology and therefore inappropriate treatment selection, as well as inability for the candidate drug to ultimately engage with its putative targets at the required dose. Beyond these critical issues which are relevant to the treatment of any medical condition, Parkinson's disease has some additional challenges that may be addressed by careful consideration of trial design. This includes the generally slow rate of disease progression necessitating long follow-up times to identify evidence of disease slowing, significant heterogeneity of the disease both in terms of motor and non-motor symptoms, lack of consensus regarding the optimal outcome measures that capture patient relevant disease progression, and lack of any consistent objective biomarker for disease progression. There are various approaches to try and improve the likelihood of success through addressing one or more of these issues. In this talk, I will discuss these issues and potential approaches that may help in the evolution of clinical trial design and thus ultimately provide a pathway to more successful identification disease-modifying treatments for Parkinson's disease.
O50
University of California, Irvine, United States
Despite the broad range of therapies in Parkinson’s disease, there remain critical unmet needs. Currently approved therapies provide substantial benefit for those with early and more advanced motor symptoms. However, none of these available therapies seek to restore what has been lost due to neurodegeneration. In the past two decades, enormous advances in technology have resulted in dramatically different approaches to treating Parkinson’s disease. Recent clinical trials in gene therapy and stem cell-based interventions have stimulated a reconsideration of how we might achieve a “regenerative” therapy in the near future. The focus of gene therapy has been upon delivering protective factors, notably glial cell-derived neurotrophic factor (GDNF) to the bilateral putamen of individuals with various stages of Parkinson’s disease. Cell therapies, on the other hand, have focused upon replacing the dopamine inputs to the putamen lost due to neurodegeneration, using surgical transplant protocols. In this “deep dive” into recent early phase trials, this presentation will take a critical look at progress to date, and future potential for “regenerative” therapy.
O51
Radboud UMC Nijmegen the Netherlands, Netherlands
Parkinson’s disease (PD) is a progressive neurodegenerative disorder that severely impacts quality of life. Since its complex biology is still not completely understood, the available treatments are mainly symptomatic and aimed at alleviating the advancing symptoms and challenges that us patients battle against on a daily basis. The development of potential disease-modifying therapies (DMTs) that can actually influence the disease process and slow, halt, or reverse disease progression, represents one of the most urgent unmet needs in PD research. From a patient-centered perspective, the promise of DMTs embody both scientific progress and hope for meaningful change.
Several DMTs are in development all over the world: therapies targeting alpha-synuclein aggregation, gene and stem cell therapies, mitochondrial enhancers, and immune-modulating interventions represent promising directions. For trials to succeed, patient participation is essential and it does not only take patient willingness to participate, but also the ability to take part in these clinical trials. Understanding what helps or hinders participation is therefore crucial.
For many, the hope of an effective treatment is a strong motivation to participate in research. It not only offers us a chance to contribute to the development of new therapies, but also the possibility of accessing innovative treatments that are not yet widely available. Altruism, trust in the medical team, and clear, honest communication are strong motivators. On the other hand, complex study designs, frequent hospital visits, travel costs, and uncertainty about placebo treatments often discourage participation. These days, technology can bridge part of this gap by providing virtual visits, wearable devices, and home-based assessments.
As someone living with Parkinson’s, looking ahead on the future of PD DMT trials, I believe that true patient-centered research means partnership: scientists bring their knowledge of disease mechanisms, while patients bring their experience of living with it. Together, we can shape the next generation of clinical trials. Decentralized and hybrid trial models, where participants can contribute data from home. Trials that are more personal, more flexible, and, hopefully, more inclusive. Trials that hopefully will bring us all closer to our main goal: ending Parkinson’s disease.
O52
ADEWUNMI DESALU PARKINSONS FOUNDATION (ADPF), Nigeria
My Story – Ufuoma Emore
My name is Ufuoma Andrew Emore, and I was born on July 3, 1976. I built my career as a lawyer and banker, working for over 15 years in law and finance. For much of my life, I focused on my profession and providing for my family.
In 2016, everything changed when I was diagnosed with Parkinson’s disease. At first, it was a difficult reality to accept. Parkinson’s is a condition that not only affects the body but can also challenge the spirit. Over time, I realized I had two choices: to let the diagnosis define me, or to use it as a platform to inspire and support others. I chose the latter.
Today, I am a Parkinson’s advocate. I share my story to raise awareness, fight the stigma around the condition, and encourage others who are living with Parkinson’s to know they are not alone. I believe in the power of community, open conversations, and building support systems that give hope and strength.
I am blessed with a loving wife and a child, who remain my greatest source of encouragement. They remind me every day that life, even with challenges, can still be lived with meaning, courage, and joy.
My journey continues, and I remain committed to using my voice and experience to make a difference in the Parkinson’s community and beyond.
thank
O53
Barrow Neurological Institute, United States
Changes in cognition or thinking frequently occur in Parkinson’s disease and very subtle declines may even start before the appearance of clinical motor symptoms. Persons may perceive trouble with different aspects of thinking near time of PD diagnosis. Indeed, it has been estimated that about a quarter of persons with Parkinson’s disease (PWP) have mild cognitive impairment (PD-MCI). Early cognitive changes most often affect attention, speed of thinking, and “executive” functions such as abstract thought, planning, and strategy generation and modification. It is thought that later changes occur in learning, remembering recent information and visual perception, and that these later changes are a risk factor or harbinger of dementia. This talk describes basics differences between MCI and dementia, risk factors for cognitive decline (both those one can and cannot change and recent biomarker work), and the cognitive mechanisms underlying changes in thinking. Although cognitive changes cannot yet be prevented, they can be detected early and lifestyle changes can be made that dampen cognitive decline.
O54
University of Wisconsin-Madison, United States
In Parkinson’s disease (PD), cognitive impairment frequently intersects with motor speech (dysarthria), swallowing (dysphagia), and gait deficits, contributing to reduced quality of life, social withdrawal, loss of independence, and heightened risks such as aspiration pneumonia and falls.
This talk will explore how cognitive domains—particularly attention, executive function, and working memory—support and constrain these functions. Evidence shows baseline cognitive deficits correlate with greater dysarthria severity (e.g., reduced intelligibility, prosodic impairment), increased dysphagia risk across oral and pharyngeal phases (e.g., premature spillage, residue, penetration/aspiration), and gait abnormalities (e.g., slower speed, shorter strides, variability, freezing). Dual-task paradigms reveal that dividing attention or raising cognitive load consistently worsens performance: speech becomes less clear and motor learning is impaired; swallowing safety and efficiency decline (with variable effects by cognitive severity); and gait deteriorates markedly, elevating fall risk due to competition for limited cognitive resources.
In PD, degraded motor automaticity increases reliance on cortical cognitive control, yet disease-related cognitive decline limits this compensation—creating a “double burden.” This interplay is often under-recognized in routine management of dysarthria, dysphagia, and gait.
The presentation will briefly discuss person-centered implications: incorporating cognitive screening into speech, swallowing, and gait evaluations; adapting therapies to individual cognitive profiles; and involving care partners. Early or prodromal cognitive support may build reserve and delay decline. Future directions include phenotype-specific approaches and deeper exploration of lived experiences across the cognitive continuum to advance holistic, synergistic care.
O55
Western University, Canada
Cognitive changes are a frequent and impactful aspect of Parkinson’s disease (PD), affecting domains such as attention, executive function, memory, and communication. These changes can influence independence, daily routines, and relationships, yet are often less visible than motor symptoms. This session will provide an evidence-informed overview of cognitive symptoms in PD and offer practical, real-world strategies to manage them.
Drawing on current clinical and research insights, we will discuss how cognitive changes relate to underlying neurobiological processes, medication effects, fatigue, and mood. Participants will learn how to recognize early cognitive changes and apply cognitive-compensatory and environmental strategies that support everyday functioning. Emphasis will be placed on maintaining engagement and autonomy through structured routines, external cueing, goal-setting, and communication strategies that enhance understanding and reduce frustration.
Care partners will gain guidance on supporting cognition, promoting shared problem-solving, and adapting communication to reduce stress and preserve partnership. Clinicians will also find practical takeaways for coaching patients and caregivers on implementing these approaches at home and in clinical contexts.
Participants will leave with an evidence-based and person-centred toolkit for coping with cognitive changes—aimed at optimizing participation, confidence, and quality of life for people living with PD and those who care for them.
O56
Amsterdam UMC, Vrije University Amsterdam, Netherlands
Background Alzheimer’s disease (AD) and vascular co-pathology are prevalent in Lewy body disease (LBD) and may contribute to disease severity and a faster progression rate. Here, we provide an overview of evidence from the Netherlands brainbank cohort for the contribution of AD and vascular co-pathology to the clinical and neuropathological severity in Parkinson’s disease (PD), Dementia with Lewy body dementia (DLB) and multiple system atrophy (MSA).
Methods We included neuropathologically defined PD(D), DLB and MSA cases with from the Netherlands Brain Bank (n = 502), including 212 cases with motor dominant disease, 119 with dementia dominant LBD and 70 MSA patients. Comprehensive pathological characterization included Braak alpha-synuclein (aSyn) staging, Thal amyloid-beta (Aβ), Braak AD staging, CAA type and severity, ARTAG, PART, LATE, microinfarcts and CERAD staging. Clinical information of the cohort was retrieved from the available clinical files. Regional and group differences were estimated using a linear mixed model analysis.
Results Limbic co-pathology loads were higher in mixed LBD than in mixed MSA cases. Mixed PDD and DLB cases had a higher alpha-synuclein load in the amygdala than in pure LBD cases (p = 0.03), while no differences were observed between MSA cases. In addition, aSyn load was strongly associated with higher Aβ and p-tau loads specifically in the amygdala for DLB (p < 0.001), but not for MSA cases. A shorter disease duration was observed in mixed LBD than in pure LBD donors (p = 0.02), which was not associated with AD or vascular co-pathology load or distribution. Cognitive impairment was associated mainly with Aβ and p-tau pathology burden in PD, DLB and MSA (p < 0.001), but not with presence of TDP-43 pathology. Concomitant pathology in MSA was mainly related to age-at-onset (68±9 in mixed vs. 59±9 years in pure MSA cases, p = 0.005), but not in DLB (69±8 in mixed vs. 67±8 years in pure DLB, p = 0.598). In addition, 90% of the mixed synucleinopathies were APOE-ε4-carriers, against 32% of the pure synucleinopathies (p < 0.001).
Conclusion Synergistic AD co-pathology in PD(D), DLB and MSA contributed to disease severity, but not to disease duration, while co-pathology in MSA was less frequent and mainly related to age-at-onset and APOE-ε4 genotype. The amygdala is most severely affected in mixed PD+AD and DLB+AD, but not in MSA. Our study highlights the differences in AD co-pathologies in the spectrum of synucleinopathies.
O57
United Kingdom
Intracellular protein aggregation is a feature of many late-onset neurodegenerative diseases, including Parkinson’s disease, tauopathies, and polyglutamine expansion diseases (like Huntington’s disease (HD)). Many of these mutant proteins, like alpha-synuclein in Parkinson's disease and huntingtin in HD, cause disease via toxic gain-of-funtion mechanisms and are autophagy substrates. In this talk, I will describe a core pathway that is dysregulated by alpha-synuclein that results in compromised autophagy and provide proof-of-concept for targeting it for therapeutic aims. We find that different alpha-synuclein disease-causing mutations (both the A53T point mutation and triplication) increase the activity of ATP citrate synthase (ACLY), a key enzyme that generates acetyl-CoA in the cytoplasm. This results in increased activity of the acetyltransferase p300 via two mechanisms which we have defined. First, ACLY activity increases acetyl-CoA levels which directly activates p300. Second, ACLY activation increases LKB1 acetylation, which inhibits AMPK, leading to increased cytoplasmic p300 and decreased levels of this acetyltransferase in the nucleus. The increased levels/activity of cytoplasmic p300 drive acetylation of cytoplasmic p300 substrates, like raptor, a component of the mTORC1 complex. This hyperactivates mTORC1 resulting in impaired autophagy. This would potentially cause a positive feedback loop in Parkinson’s disease as alpha-synuclein is degraded by autophagy. However, our findings reveal that ACLY is an attractive therapeutic target in this disease. ACLY inhibitors rescue pathological phenotypes in PD neurons, organoids, zebrafish and mouse models, suggesting that this pathway is a core feature of alpha-synuclein toxicity. As ACLY is druggable, our data provide the stimulus for further drug discovery in this domain.
O58
Grenoble Alpes University, France
Recent advances in Deep Brain Stimulation for Parkinson’s disease
Since the mid-20th century, brain stimulation has played a role in Parkinson’s disease treatment. At first, it was mainly used to pinpoint where surgeons should perform permanent procedures. Over time, technology evolved, allowing for deep brain stimulation (DBS)—a method that is adjustable and reversible. Since the late 1980s, DBS has revolutionized how we treat advanced Parkinson’s. Today, it’s a recognized surgery for patients who experience motor issues and involuntary movements that medication can’t fully control. Studies confirm that it improves movement symptoms, though it doesn’t slow the disease itself. Over time, its effects may lessen—especially for symptoms like balance or speech. Not everyone qualifies, since patient selection is careful, and surgery plus follow-up programming require expertise. However, new technology is emerging. Personalizing DBS using brain signals, imaging, and smart software could improve long-term outcomes. New lead designs and combined techniques may also expand who can benefit, offering hope for even better, more inclusive care.
O59
International HM Hospitales, Spain
Over the past ten years, MRI-guided Focused Ultrasound has emerged as a novel functional neurosurgical tool for the treatment of movement disorders. This technology can be applied in three main modalities: high-intensity focused ultrasound (HIFU) for therapeutic brain ablation, low-intensity focused ultrasound (LIFU) for blood–brain barrier (BBB) opening, and LIFU for neuromodulation. HIFU ablation has rapidly expanded as a symptomatic therapy aimed at improving motor manifestations in movement disorders, while the other two modalities remain experimental approaches for neurological and neurodegenerative diseases. HIFU has demonstrated strong efficacy in improving tremor and functional disability in essential tremor, both unilaterally and bilaterally. In the case of Parkinson’s disease, up to three randomized controlled trials have shown the efficacy of unilateral ablation in improving motor symptoms. Additionally, some uncontrolled reports have suggested the potential of bilateral treatment. However, the use of different brain targets - selected according to specific clinical profiles - and the intrinsic complexity of the disease, which involves more challenging post-treatment management, underscore the need for further evidence to fully realize the therapeutic potential and optimize patient selection.
Evidence for other indications, such as dystonia, pain, or psychiatric disorders, remains limited to small case series or isolated reports. This lecture will aim to summarize the most relevant evidence currently available for the treatment of Parkinson’s disease and other movement disorders, and to explore the potential for expanding its applications, both through HIFU ablation and the emerging prospects of LIFU neuromodulation and BBB opening.
O60
Denali Therapeutics, United States
This 2-Oral Sessions will focus on the interplay between GBA1 and LRRK2 and its therapeutic implications for PD. This discussion will explore what is known about shared and divergent consequences of PD-linked variants in LRRK2 and GBA1 on endolysosomal dysfunction and the genetic interplay of LRRK2 and GBA1 variants with respect to PD risk and manifestation. From a therapeutic perspective, we will explore how understanding this relationship can be translated into pathway biomarkers to assess benefits on lysosomal function in the clinic and into supporting patient selection and stratification for LRRK2 and GCase-focused therapies. We will discuss the gaps in our understanding and what we as a field can do to address them.
O61
Vall d'Hebron Research Institute (VHIR), Spain
Accumulation of misfolded and aggregated proteins is a hallmark of Parkinson’s disease (PD), related synucleinopathies, and other neurodegenerative disorders collectively known as proteinopathies. Increasing evidence indicates that failure of cellular protein-degradation systems including the autophagic pathways, the ubiquitin–proteasome system, and endosomal trafficking, plays a central role in the onset and progression of PD. These systems form a highly coordinated proteostasis network that ensures neuronal homeostasis by eliminating damaged or misfolded proteins, thereby preventing the neurotoxic accumulation of species such as α-synuclein.
This 2-Oral Sessions will review current knowledge of the molecular and cellular mechanisms underlying protein degradation in PD. Understanding these mechanisms not only refines our view of PD pathogenesis but also informs the development of disease-modifying strategies aimed at restoring neuronal proteostasis.
Altogether, these insights provide a framework for understanding how enhancing cellular clearance mechanisms may ultimately counteract proteotoxic stress and neuronal dysfunction in PD and related proteinopathies.
O62
Northwestern University Feinberg School of Medicine, United States
Parkinson disease (PD) is a neurodegenerative disorder marked by the preferential dysfunction and death of dopaminergic neurons in the substantia nigra. A question critical to understanding PD is which affected processes are central to the preferential vulnerability of dopaminergic neurons in the substantia nigra. Pinpointing the most relevant subcellular processes is challenging, in part because there are multiple distinct pathways that contribute to the vulnerability of these neuronal populations, and in part because the various cellular dysfunctions of PD probably reciprocally influence each other. To identify the most high-yield targets for therapeutic intervention, it is important to consider the core cellular compartments and functional pathways upon which such varied forms of pathogenic dysfunction may converge. We hypothesized that a large number of PD-linked causative and risk genes converge on recurring subcellular pathologies, suggesting potential functional nodes that may be central to selective vulnerability. To test this hypothesis, we have studied several PD genes, focusing on the mechanisms of their potential convergence in disease pathogenesis. These genes and corresponding pathogenic pathways primarily localize to a subset of subcellular compartments, including mitochondria, lysosomes and synapses. We discuss how these pathogenic mechanisms that originate in different cellular compartments may coordinately lead to cellular dysfunction and degeneration of nigral dopaminergic neurons in PD. We will also highlight recent development of targeted therapies that were informed by the identifications of such converging mechanistic pathways in Parkinson’s disease.
O63
Rush University Medical Center, United States
Peer mentoring has emerged as a promising intervention to support people living with Parkinson’s Disease (PD), their care partners, and healthcare professionals navigating the complexities of care. Approaches vary, yet all begin with the recognition that people with PD and their care partners hold immense wisdom and lived experience that can positively impact the lives of others on a similar journey. This interactive 2-Oral Sessions invites diverse participants—clinicians, researchers, individuals with PD, and care partners—to explore the growing body of evidence supporting peer mentoring and to collaboratively shape its future.
Drawing from early work in Alzheimer’s Disease and other chronic illnesses, through published and ongoing research on PD and Lewy Body Dementia care partner peer mentoring by Dr. Fleisher and colleagues, we will examine how structured peer mentor-led educational programs have demonstrated feasibility and potential benefits in reducing caregiver strain, anxiety, and depression. These interventions, include Share the Care and the ongoing PERSEVERE trial leverage the lived expertise of experienced care partners and individuals with PD to provide practical knowledge, emotional support, and a sense of community.
Participants will engage in facilitated discussions around key findings, such as the importance of mentor training, cultural and linguistic considerations, the role of virtual formats in expanding access, and mentoring as an addition or alternative to—rather than replacement of—traditional support groups. We will also explore future directions, including expanding peer mentoring to people with PD themselves and the key content and structures to provide maximal benefit.
This session invites attendees to share their own experiences, challenges, and ideas for enhancing peer mentoring. Whether you are a healthcare provider interested in implementing peer support, a person with PD seeking connection, or a caregiver with wisdom to share, your voice is essential. Together, we will identify opportunities to co-create research priorities and practical strategies that reflect the real-world needs of our community and build on the invaluable wisdom of everyone affected by PD.
O64
Tor Vergata University of Rome, Italy
Psychological dimensions play a pivotal yet often underrecognized role in Parkinson's (PD), where psycho-behavioral symptoms persist throughout the condition, influencing both prodromal stages and ongoing adaptation. The initial neuropsychological profile and individual reactions to the diagnosis critically shape the progression and future adjustments to the new life with PD. Beyond clinical symptoms, psychological and emotional factors fundamentally determine patients’ capacity to maintain meaningful relationships and support networks.
Mindfulness-based interventions have shown excellent results in enhancing self-awareness and stress regulation through meditative and breathing techniques; Compassion can boost insight and lasting psychological adaptation. Rooted in Paul Gilbert’s 2014 conceptualization of Compassion as a “particular sensitivity to one's own and others' suffering coupled with the motivation to alleviate it”, the integration of Compassion-based approaches could be a transformative framework for psycho-physiological well-being in people living with PD (PwPD). Compassion Focused Therapy (CFT) and its practices, encompassing meditation, visualization and psychoeducation, target both vagal regulation and cortical processes, enhancing autonomic balance and mentalization.
A pioneering pilot study by our team (Della Morte et al., 2014) demonstrated that a Compassion program effectively modulated vagal responses under psycho-emotional stress, as evidenced by improved heart rate variability (HRV) and increased Self-Compassion in PwPD, thereby mitigating stigma. These findings are encouraging for incorporating CFT into PD standard care protocols.
We must always remember that the diagnosis comes on a person, with his or her functioning and prior life experiences; caring for and understanding how a person has lived up to that point allows us to tailor therapies and more functionally direct the trajectory of care. It is time to scientifically explore and embrace holistic psychological support that addresses the real experience and challanges of PwPD, ensuring comprehensive and compassionate care for both patients and their loved ones.
O65
ZWAP Cycling Club, Norway
Psychological dimensions play a pivotal yet often underrecognized role in Parkinson’s (PD), where non-motor symptoms, especially psycho-behavioral ones, persist throughout the condition, influencing both prodromal stages and ongoing adaptation. The initial neuropsychological profile and individual reactions to the diagnosis critically shape the progression and future adjustments to the new life with PD. Beyond clinical symptoms, psychological and emotional factors fundamentally determine patients’ capacity to maintain meaningful relationships and mobilize effective support networks.
Mindfulness-based interventions have shown excellent results in enhancing self-awareness and stress regulation through meditative and breathing techniques. However, we could boost insight and lasting psychological adaptation using Compassion. Rooted in Paul Gilbert’s 2014 conceptualization of Compassion as a “particular sensitivity to one's own and others' suffering coupled with the motivation to alleviate it”, the integration of Compassion-based approaches could be a transformative framework for psycho-physiological well-being in people living with PD. Compassion Focused Therapy (CFT) and its practices, encompassing meditation, visualization, psychoeducation and psychological support, target both vagal regulation and cortical processes, enhancing autonomic balance and mentalization.
A pioneering pilot study by our team (Della Morte et al., 2014) demonstrated that a Compassion program effectively modulated vagal responses under psycho-emotional stress, as evidenced by improved heart rate variability (HRV) and increased Self-Compassion in people living with the condition (PwPD), thereby mitigating stigma. Despite the challenges posed by the COVID-19 pandemic during the study, findings are encouraging for incorporating CFT into PD standard care protocols.
Brain’s residual neuroplastic potential can be actively directed to compensate for neurodegeneration, but only if emotional and cognitive processes are consciously engaged and nurtured. Compassion-Based Practices foster adaptive thinking aligned with personal physiological responses and experience, enhancing resilience and quality of life (QoL).
It is time to scientifically explore and embrace holistic psychological support that addresses the real experience and challanges of PwPD, ensuring comprehensive and compassionate care for both patients and their loved ones.
O66
Ghent University Hospital, Belgium
The gut-brain axis is a complex communication network which allows the gut and the brain to influence eachother. Several clinical and biological factors emphasize the importance of the gastrointestinal tract in Parkinson’s disease. Moreover, therapies targeting the gut bacteria have shown beneficial effects in animal models of Parkinson’s disease. At this time, fecal microbiota transplantation (FMT) represents the most effective method for achieving comprehensive and long-lasting changes in gut microbiota composition. FMT is safely and successfully used for treating Clostridioides difficile infections, for which it is an approved indication. However, evidence supporting the use of FMT in patients with neurological disorders is limited. Our group and others have performed clinical trials investigating the effect of FMT in patients with Parkinson’s disease. We will discuss these results, extending to what this means for future clinical trials and potential other microbiota-targeting therapies.
O67
Belgium
Parkinson’s disease (PD) is a multisystem neurodegenerative disorder that affects the functioning of widespread brain networks. Cognitive symptoms in PD often emerge during complex activities—particularly when multiple tasks or several task components must be performed simultaneously. Neurorehabilitation for PD typically involves a combination of speech therapy, physical exercise, and motor learning. These interventions rely on specific task practice, the outcomes of which are encoded in motor memory, ultimately leading to consolidated motor gains.
In this round table, I will present scientific evidence on how both motor and cognitive capacities benefit from task training—whether performed as single- or dual-task activities—and how these processes influence learning and consolidation. I will also discuss the advantages and limitations of such combined approaches, as well as how non-motor factors may interact with learning mechanisms in PD.
O68
Western University, Canada
Cognitive and communication challenges in Parkinson’s disease (PD) often emerge gradually yet profoundly affect daily function and quality of life. Difficulties with attention, planning, and working memory can disrupt everyday routines—from remembering medication schedules and navigating mobility tasks to engaging in meaningful conversation. These cognitive changes often co-occur with speech, voice, and swallowing difficulties, further increasing communication effort, social withdrawal, and caregiver burden.
This session explores how Speech-Language Pathologists (SLPs) and Physical Therapists (PTs) can collaborate to address these interconnected non-motor symptoms. Using a person-centered, functional framework, we will examine how cognition influences communication, swallowing, and movement—and how therapy approaches can integrate across these domains to support participation in daily life. SLPs play a key role in assessing and treating cognitive-communication and swallowing changes—helping people with PD and their care partners recognize when attention, memory, or processing speed affect speech clarity, word retrieval, or safe swallowing. Evidence-based strategies such as external cueing, conversational pacing, partner communication training, and mindful swallowing techniques will be discussed, alongside approaches that reduce cognitive load and support dual-tasking. Working with PT contributes complementary expertise by addressing motor-cognitive integration. When SLP and PT interventions are coordinated, individuals can practice cognitive and communicative skills in real-world movement contexts—such as talking while walking, or planning complex tasks safely and efficiently.
The session will highlight interdisciplinary care models that empower PwPs and care partners to use shared routines, environmental supports, and self-cueing to maintain independence and safety. Participants will leave with an understanding of how SLP and PT strategies, when integrated, can mitigate the everyday impact of cognitive, communication, and swallowing challenges—helping people with PD stay active, socially connected, and confident in their daily lives.
O69
University of Cambridge, United Kingdom
The use of stem cells to treat many different conditions, including Parkinson's has expanded over the years not only in the form of academic pharma partnerships that lead to funded first in human trials but also in the private sector where clinics and companies offer such treatments for a price- so called stem cell tourism. This letter area of stem cell medicine is not without risk as many of these treatments have limited, if any, preclinical data in support of their use in patients and the evidence often supplied by these companies is through personal testimonies. As such people looking into such therapies for Parkinson's, should not have to pay for any such treatment as they are currently still at the experimental stage and unproven.
In the case of Parkinson's the most logical and best researched area is in the use of human pluripotent stem cells as a source for generating new dopamine cells to replace those lost to the disease process. These stem cells typically come from 2 sources- embryonic stem (ES) cells which come from spare embryos generated in IVF programmes and induced pluripotent stem (iPS) cells where the cells are derived through the reprogramming of adult cells such as skin fibroblasts or blood cells. This latter approach also offers the possibility of the patient being the donor of the cells for reprogramming and thus their own treatment- so called autologous grafting.
Stem cell therapies offer many advantages as a treatment in terms of:
being relatively easy to manipulate and engineer; enabling a ready supply of cells to be manufactured in the numbers needed to treat people with Parkinson's; being suitable for cryopreservation with standardised "doses" of cells that make trials easier to conduct; enabling the safety of the trialed product to be fully investigated prior to a trial.
As a result these cells have now moved to first in human clinical trials building on robust pre clinical work showing that these stem cell derived dopamine cells can survive, integrate into the host brain, release dopamine and restore the animals back to normal in terms of dopaminergic striatal innervation. These trials are now starting to be published and with this come the challenges for the next phase of development in terms of optimising the dose of cells needed, how best to deliver them and with what degree of immunosuppression in those not in receipt of autologous grafts. All of this will be discussed in this talk.
O70
VIB KU Leuven Center for Brain and Disease Research, Belgium and Amsterdam University Medical Center, the Netherlands, Netherlands
Introduction: How can cognitive health be maintained during human aging? To identify protective genetic and biomolecular factors that associate with the escape of cognitive decline we set up the 100-plus Study, a longitudinal cohort study of cognitively healthy centenarians. Currently the cohort includes >500 centenarians. We collect blood and faeces samples, and ∼30% of the centenarians agree to postmortem brain donation. This centenarian brain cohort offers a unique window into mechanisms underlying this neuroprotection.
Methods: Centenarians with high cognitive performance at baseline mostly maintain this until death. Neuropathological analysis indicate that these high performers resisted critical development of Aβ plaques, and tau abundance was low across all centenarians. Brain protein profiling indicated that across all centenarians, AD patients and healthy controls, only five proteins associated with Aβ abundance, revealing upregulation of HTRA1, LRP1 and NRXN1 as early AD-associated changes. Conversely, tau abundance associated with ∼20% of the quantified proteome, revealing GPRIN1 as the top tau-associated protein. While the majority of the centenarians resisted accumulation of amyloid, one third of centenarians had high Aβ abundance, often with wide tau-spreading (Braak stages IV/V), however, they diverged from AD cases and controls by maintaining an unexpectedly low local tau abundance. Furthermore, centenarians who maintained high cognitive performance until death had maintained proteostasis (low ubiquitin peptides, high proteasome components), high PCSK1 levels (prohormone maturation), high PFKFB2 levels(glycolysis regulation), high mitochondria-coupled lipid β oxidation and lower APOE levels.
Conclusions: Together, our findings suggest that, in a model where Aβ facilitates tau seeding, centenarians maintain brain health by actively buffering against tau accumulation.
O71
Department of Neurology and Neurorehabilitation, Klinikum Osnabrueck, Academic teaching hospital of the University Muenster, Germany
Parkinson's disease is heterogeneous in its clinical presentation and is characterized by the potential occurrence of numerous motor and non-motor symptoms. More than 20 different medical professions and care providers are involved in its management. There is therefore international consensus that establishing inter-professional regional network structures is essential for improving outcomes and providing the best possible care for people with Parkinson's disease. In Germany, under the guidance of the umbrella organisation Parkinson Netzwerke Deutschland (www.parkinsonnetzwerke.de, see Fig.) multiple regional treatment teams have joined forces in network structures in a bottom-up process in recent years and meet regularly during so-called multi-professional plenary meetings. Due to their diversity, which poses a particular challenge for multi-professional management, swallowing disorders and other gastrointestinal symptoms are particularly suitable as a model for illustrating the successful establishment of network structures with relevant effects in everyday clinical practice. The path to establishing such structures is the core topic of this session.
O72
Stanford University School of Medicine & Nexus NeuroTech, United States
Over recent years, increasing computing power, availability of large and ever-increasing amounts of data, and improved algorithms have converged to enable exciting opportunities to apply artificial intelligence (AI) to characterize the transition from health to disease, measure disease burden, and track disease progression/regression–all useful aspects of clinical care. Particularly when coupling data from various sensors on the body or in the environment with clinically validated algorithms, there is an opportunity to enable continuous, data-driven monitoring. For disorders of the brain like Parkinson’s disease, these new capabilities are urgently needed, since the diagnosis and monitoring of these conditions still largely relies on relatively crude and subjective methods, such as the clinical exam, subjective patient reports, and symptom scales. As the use of AI in healthcare becomes more pervasive, its application in the clinical care for those with Parkinson’s disease presents exciting opportunities to improve the timeliness and accuracy of diagnosis and to optimize treatment.
A number of other conditions can mimic Parkinson’s disease, and arriving at an accurate diagnosis as soon as possible allows implementation of the most appropriate treatment plan. The application of AI to various data types has shown the utility in improving the accuracy of the diagnosis of Parkinson’s disease. Rather than relying on a single data type, applying AI to multimodal data, may allow the diagnosis of Parkinson’s disease with even greater accuracy and at earlier stages. Methods employing AI to interrogate multimodal data sets are also emerging as a means of identifying patient subgroups that each have a similar symptom profile, disease course, and/or expected treatment response. This will likely help in counseling individual patients about their expected clinical course and in efficiently personalizing treatment, overcoming some of the challenges that the heterogeneity of Parkinson’s disease presents. The use of AI-powered approaches for symptom and severity assessment, progression monitoring, and treatment management is also now becoming real.
Perhaps more than many other brain disorders, Parkinson's disease lends itself to the creation of rich data from which AI can surface actionable insights that hold the potential to revolutionize care in a personalized manner.
O73
University of Cologne, Germany
The round table discussion “Current State of Biomarkers: The Limits and the Potential” brings together scientists, clinicians, people with lived experience and carers to explore how advances in biomarker research are transforming our understanding of PD while also acknowledging current limitations and real-world implications.
Biomarkers—whether derived from imaging, cerebrospinal fluid, blood, genetics, or digital sensors—are central to earlier diagnosis, improved disease stratification, and the development of targeted therapies. Yet, despite impressive scientific progress, few biomarkers have yet translated into routine clinical use. The discussion will address key questions: How close are we to identifying reliable diagnostic and progression markers? What do current biomarkers actually tell us about disease mechanisms? And how do we ensure that biomarker research remains relevant and beneficial to those living with PD?
Participants will share complementary perspectives. Researchers will outline recent breakthroughs in molecular imaging, fluid biomarkers and digital measures that capture motor and non-motor features in everyday life. Clinicians will reflect on how these tools could help tailor treatments and design more efficient clinical trials. Most importantly, people with lived experience and carers will speak about expectations, hopes, and concerns surrounding biomarker testing—from the emotional impact of “knowing early” to issues of privacy, accessibility, and the need for clear communication.
Ultimately, the session seeks to define what a responsible and person-centred biomarker roadmap could look like—one that integrates rigorous science, ethical reflection, and the everyday realities of people affected by Parkinson’s disease.
O74
University of Sydney, Australia
Astrocytes are the primary homeostatic cells of the CNS and are essential for neuronal survival and function. AI assessment of their role in Parkinson’s disease (PD) emphasises their dual role as both protective but also having detrimental actions, many of these similar to their role in other neurodegenerative diseases. The unique features identified are associated with processing α-synuclein and their concentration of proteins identified genetically in some families as causal for PD (PARK genes).1 Astrocytes normally accumulate α-synuclein in small aggregates mostly in processes, potentially sculpting synaptic plasticity.1 This process is increased substantially with increased amounts of α-synuclein. In patients with PD, more astrocytes than neurons contain α-synuclein aggregates with the α-synuclein non-fibrilised and uniquely post-translationally modified. PARK genes that concentrate in astrocytes and impact their mitochondrial (energy organelle) and lysosomal (degradation centre) functions are likely involved as astrocytes assist neurons by clearing damaged or transferring healthy mitochondria to neurons in addition to clearing synaptic α-synuclein. Recent gene trajectory analyses show a loss of protoplasmic and increase in fibrous astrocytes which become increasingly more reactive.2
Li W, Fu Y, Halliday G, Sue C. Front Cell Dev Biol 9, 612476 (2021)
Park J, Chung WS. Curr Opin Neurobiol 81, 102732 (2023)
Ma et al. Nat Comm 16, 7146 (20205)
O75
National and Kapodistrian University of Athens, Greece
Parkinson’s Disease (PD) is a progressive neurodegenerative disease characterized by loss of dopaminergic neurons and deposits of aggregated α-synuclein (a-syn), a small protein normally localized in the presynaptic nerve terminals. Besides neuronal loss, PD is now recognized as a multi-system disorder that involves notable neuroinflammation and immune dysfunction underlying many of the non-motor PD deficits which in most cases, preceded the onset of motor symptoms. The development of inflammation in the PD brain results from the activation of microglia and astrocytes leading to sustained astrogliosis. However, the exact trigger of glial reactivity and its contribution to disease progression remain unclear.
Using a transgenic mouse model of a-syn overexpression and human post-mortem PD brain tissue, we found that the presence of SDS-resistant hyper-phosphorylated a-syn oligomers, but not monomers, is correlated with sustained inflammatory responses, such as elevated levels of endogenous antibodies and cytokines and microglial activation. Detailed analysis revealed a decrease in phagocytic microglia and robust alterations in astrocyte number and morphology including process retraction. Using RNAseq and secretomic analyses combined with cell type-specific immunofluorescence, we have mapped the molecular pathways by which a-syn oligomers prolong neuroinflammation by sequentially activating specific signaling pathways in microglia and astrocytes. Our work revealed that astrocytes could function as novel neuroprotective mediators against neuroinflammation through the upregulation of functionally active T-type Cav3.2 Ca2+ channels which can mediate the secretion of the IGF-1 binding protein, IGFBPL1, an inducer of the beneficiary IGF signaling.
In sum, our data describe a neuroprotective mechanism upregulated in mouse brain to minimize a-syn-induced neurotoxicity and could possibly explain the higher tolerance of mouse neurons compared to human or primate neurons against a-syn-induced neuroinflammation. Since T-type channels and IGF1 have already been pharmacologically targeted for other disorders, our experimental evidence could provide the basis for ultimately repurposing such therapies for the benefit of patients suffering from synucleinopathies.
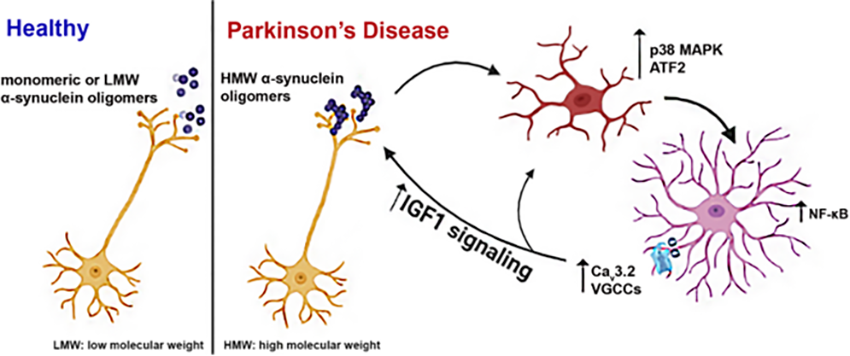
O76
Newcastle University, United Kingdom
Device-assisted therapies—such as deep brain stimulation (DBS), foslevodopa–foscarbidopa infusion, and continuous subcutaneous apomorphine infusion (CSAI)—can make a real difference for people living with Parkinson’s (PwP) when oral medication alone no longer provides good symptom control. Yet success with these therapies depends as much on how and when they’re introduced as on the therapies themselves.
Using foslevodopa-foscarbidopa infusion therapy as an example, this session will share practical, experience-based tips for clinicians and care teams involved in starting device-assisted therapies, and supporting PwP with their use. The session will consider how to recognise the right time to consider a DAT and how to prepare both patients and care partners for what to expect. Early education and clear communication about goals, potential benefits (motor and non-motor) and day-to-day management, together with multi-disciplinary support, can greatly improve satisfaction and outcomes.
O77
University Clinic Cologne, Germany
Not everyone with Parkinson’s disease experiences it the same way. Some people remain remarkably stable for years, while others face a faster decline after diagnosis. Scientists have been trying to understand these individual differences, which may stem from varying levels of resilience or reserve. These terms describe the brain’s ability to adapt and cope with damage, such as the loss of dopamine, to maintain function. Importantly, resilience and reserve seem to be shaped by lifelong experiences and habits.
In Alzheimer’s disease, the concept of cognitive reserve has been studied for more than two decades. Research shows, for instance, that higher levels of education can buffer the effects of brain damage on thinking and memory. Similar findings have emerged in Parkinson’s disease. More recently, researchers have begun exploring the idea of motor reserve, hence the ability to preserve movement and coordination even when the brain’s dopamine system is impaired. Brain imaging suggests that people with higher motor reserve have stronger connections between movement-related brain areas and even differences in brain chemistry that help them compensate for the disease’s effects.
It is still unclear exactly what builds motor reserve, but lifestyle seems to play a major role. People who stay physically active and mentally engaged, through exercise, work, learning, tend to have more flexible and resilient brain networks. For instance, education appears to make attention systems more robust, while lifelong physical activity supports movement networks. Together, these findings show how the brain’s systems for thinking and moving are deeply intertwined.
In my talk, I will discuss recent literature on resilience mechanisms in Parkinson’s disease and what we can learn from resilience research from other diseases, such as Alzheimer’s disease. I will highlight new research on how lifestyle and brain plasticity interact, and how this knowledge could guide the design of personalized therapies. Ultimately, understanding and strengthening resilience mechanisms may help people with Parkinson’s disease.
O78
Movement Disorders Clinic, Department of Neurology, School of Medicine of the University of São Paulo, Brazil
Parkinson’s Disease (PD) is a neurodegenerative condition, with clinical manifestations and disease progression varying significantly across individuals. The concept of brain resilience—underpinned by cognitive and motor reserve—provides a theoretical framework for understanding this clinical variability. Cognitive reserve (CR), built through factors like education and lifelong intellectual engagement, has been associated with reduced clinical impairment despite similar neuropathological burden. Patients with higher reserve exhibit better performance on motor activities and show preserved functional connectivity in prefrontal cortical regions and basal motor circuits. Structured cognitive training in PD patients has yielded improvements in executive function, working memory, and processing speed, effects associated with adaptive functional recruitment and synaptic reorganization.
Studies support the importance of physical therapy (PT) in PD management. The 2021 Clinical Practice Guideline issued by the American Physical Therapy Association (APTA) recommends (Grade A) gait training, balance exercises, muscular strengthening, aerobic conditioning, and dual-task interventions in PD. The guideline organizes approaches into key domains, suggesting the use of auditory, visual, and somatosensory cueing to enhance movement and postural reactivity. Early initiation of PT, combined with individualized monitored care plans, has been linked to reduced fall risk, improved gait, and maintained daily independence.
The combination of non-invasive brain stimulation (NIBS) and exercise has emerged as a promising intervention strategy. A systematic review and meta-analysis of 11 randomized controlled trials assessed the synergistic effects of NIBS particularly rTMS and tDCS alongside exercises. The findings demonstrated improvements in gait velocity, stride length, and cadence when compared to exercise alone or sham stimulation. Application of NIBS to specific motor cortical areas appears to enhance synaptic plasticity and facilitate motor relearning induced by exercise. The combined approach has shown to be a safe well-tolerated recommendation for PD with refractory motor symptoms unresponsive to conventional therapy.
In conclusion, integrated strategies combining motor training, cognitive stimulation, and social engagement should be considered essential in the design of therapeutic models focused on neuroplasticity, functional autonomy, and improved quality of life for PD.
O79
JPG Enterprises LLC, Barrow Neurological Institute, United States
Parkinson’s disease (PD) may include symptoms of cognitive decline including difficulties with attention, executive function, memory, and visuospatial skills, which are increasingly acknowledged as a significant aspect of the disease, affecting quality of life in patients and care partners. While medication interventions are limited in efficacy for some cognitive symptoms, non-pharmacological strategies such as cognitive training have shown promise and have grown in interest and recognition in PD. This session will explore the fundamentals, latest research, and clinical approaches for how cognitive training and cognitive rehabilitation may be applicable in PD management. An overview of cognitive impairment in PD, emphasizing how deficits can manifest even in early stages and progress over time, will be provided, with examples of how cognitive training and non-pharmacological strategies may play a role. The session will discuss different cognitive training modalities, ranging from computerized programs to therapist-led sessions and home-based exercises, and evidence from recent clinical trials and interpretation of study results. Identifying gaps in current research, such as the need for long-term studies to assess sustained benefits, the integration of cognitive training with other treatment modalities, whether medications or physical and occupational therapies, and the development of standardized protocols will be discussed. Key considerations include the importance of individualized approaches, motivational and other non-motor issues, and multidisciplinary collaboration. The session aims to provide a deeper understanding of both the challenges and the potential of cognitive training in PD, as well as practical strategies to apply in clinical practice.
O80
Cure Parkinson's, United Kingdom
At present, there are no "disease modifying therapies" approved for use in the treatment of Parkinson's. These are treatments that can slow, stop or reverse the progression of Parkinson's. A lot of research is being conducted in this area, however, and at this round table, we will discuss the current status of clinical trial programs focused on modifying the disease course of Parkinson's. We will also consider the previous 10 years of clinical trials addressing this goal and examine what could have been done differently. And finally, we will look to the future and where things might be heading.
O81
University of California, Irvine, United States
Regenerative therapy aims to repair, restore or replace damaged or lost cells, whether in the brain or other parts of the body. We know that in Parkinson’s disease, loss of dopamine leads to the vast majority of problems movement. More than that, loss of cell function or loss of the cells themselves is progressive, and spreads through broader networks in the brain. This leads to more problems, including thought processing, sleep disruption, and more. Despite the broad range of therapies available there is, as yet, no treatment available that would restore the cells that have been lost. Regenerative therapy, therefore, is an area of intense research, whether focused on stimulating the brain’s own healing mechanisms, or by introducing new cells.
There have been enormous recent advances in technology, particularly in gene therapy and cell therapy, that might now allow for a regenerative approach to Parkinson’s disease. Regenerative medicine is making its way into clinical trials. Gene therapy, for example, facilitates delivery of protective factors, for example glial cell-derived neurotrophic factor (GDNF). Cell therapies, delivered by surgical transplantation to the brain, aim to replace dopamine inputs that have been lost in Parkinson’s disease.
In this round table we will discuss current and pipeline efforts in regenerative therapy for Parkinson’s disease, take a look at the likely timeline, and examine what’s needed for success.
O82
UCL Institute of Neurology, United Kingdom
The traditional approach of a using double-blind, placebo controlled, 2-Oral Sessionsgroup trial designs has not, to date, led to the discovery of any disease-modifying treatments for Parkinson's disease. There are multiple potential reasons underlying this which may in part relate to inadequate understanding of Parkinson's disease pathophysiology and therefore inappropriate treatment selection, as well as inability for the candidate drug to ultimately engage with its putative targets at the required dose. Beyond these critical issues which are relevant to the treatment of any medical condition, Parkinson's disease has some additional challenges that may be addressed by careful consideration of trial design. This includes the generally slow rate of disease progression necessitating long follow-up times to identify evidence of disease slowing, significant heterogeneity of the disease both in terms of motor and non-motor symptoms, lack of consensus regarding the optimal outcome measures that capture patient relevant disease progression, and lack of any consistent objective biomarker for disease progression. There are various approaches to try and improve the likelihood of success through addressing one or more of these issues. In this talk, I will discuss these issues and potential approaches that may help in the evolution of clinical trial design and thus ultimately provide a pathway to more successful identification disease-modifying treatments for Parkinson's disease.
O83
Australia
This 2-Oral Sessions discussion will focus on the common barriers and evidence-based solutions to adopting and adhering to an exercise and physical activity plan for people with Parkinson’s disease and their carers. Multiple factors can make it uniquely challenging for people with Parkinson’s disease to get going and keep going with an exercise plan. A focus will be on using evidence-based approaches to change behaviour and self manage physical activity and get into and stick with an exercise routine. This 2-Oral Sessions will provide an opportunity to discuss practical strategies to enhance adherence to exercise, across the lifespan of the journey of a person with Parkinson’s disease and their carers.
O84
University of Pennsylvania School of Medicine, United States
Psychosis, including hallucinations and delusions, in Parkinson's disease is very common over the long-term, and can be quite problematic, requiring careful assessment and management. Determining the cause of the psychosis informs management strategies. Antipsychotics are used in Parkinson's disease, but the potential benefits and risks of their use need consideration.
O85
Thomas Jefferson University, United States
It is clear from both preclinical and clinical studies that exercise can lower the risk for developing Parkinson’s disease. Exercise, and particularly forms of aerobic exercise, has also become a front-line therapy in newly diagnosed individuals since it can also help to improve some of the symptoms of the disorder, with proven efficacy in issue related to balance, mobility and activities of daily living. Exercise has also been shown to improve some of the non-motor symptoms of PD, such as depression or constipation. For PD patients, another benefit of exercise, when done in sufficient amounts is that it can help to slow the progression of the motor symptoms of this disease. While the phenomenon of exercise-induced symptomatic relief is clear, the mechanisms underlying these benefits are just starting to be elucidated. In this 2-Oral Sessions discussion, we will discuss some of the key questions that we still need to be resolved. For example, what biochemical pathways are altered by neuroprotective levels of exercise? Are there any biomarkers that can be identified that indicate when sufficient levels of neuroprotective exercise have been reached? Do all patients benefit from exercise? Is there a time where it’s too late to get significant benefits from exercise? Are exercise’s beneficial effects different depending on the etiology (idiopathic vs familial) of the disease and perhaps most importantly, how long to the positive effects of exercise last?
O86
University of British Columbia, Canada
Parkinson’s disease (PD) is not a single disorder but a spectrum of clinical and biological entities that vary widely in symptoms, progression, and underlying mechanisms. Efforts to classify PD into subtypes have evolved over the past decades—from early clinical observations based on age at onset or purely motor phenotypes to more comprehensive, data-driven frameworks integrating both motor and variety of non-motor dimensions. These newer approaches have consistently identified reproducible patterns such as mild motor-predominant and diffuse subtypes, each with distinct trajectories and biomarker profiles. Emerging evidence from neuroimaging and biofluid analyses has revealed robust biological differences among subtypes, including variations in dopaminergic denervation, brain atrophy patterns, and cerebrospinal fluid markers. Such findings confirm that PD heterogeneity is rooted in divergent pathophysiological processes rather than clinical variability alone. Looking ahead, the next frontier in PD subtyping lies in the integration of machine learning and artificial intelligence to uncover deeper, multidimensional patterns across clinical, imaging, genetic, and molecular data. These advanced analytic techniques can refine existing subtype models, enhance reproducibility, and reveal mechanistic links that may define distinct biological pathways. Further exploration of the pathogenesis basis of PD heterogeneity will be essential to bridge clinical subtypes with underlying molecular signatures. Ultimately, the field is moving toward a personalized and precision-based framework in PD—where classification systems not only describe differences but guide individualized prognosis, biomarker-guided monitoring, and tailored therapeutic strategies.
O87
Luxembourg Institute of Health; University of Luxembourg; Centre Hospitalier de Luxembourg, Luxembourg
Parkinson’s disease (PD) is increasingly recognized as a heterogeneous neurodegenerative movement disorder encompassing both clinical and biological variability. Traditional clinical subtypes - such as tremor-dominant, akinetic-rigid, or postural instability/gait difficulty - have long served as practical tools to describe motor heterogeneity and predict certain aspects of the disease course. However, these phenotypes do not reflect the underlying molecular diversity that drives disease onset, progression, and treatment response. Recent advances in genetics, proteomics, and biomarker research have led to the proposal of biologically defined PD subtypes, that represent distinct pathogenic mechanisms. Some genetically defined forms of PD serve as prototypes for different disease mechanisms, marking a first shift toward a biologically grounded classification. Converging evidence supports several mechanistic axes: (1) pathological protein aggregation, where SNCA mutations induce α-synuclein misfolding or overexpression; (2) mitochondrial and bioenergetic impairment, driven by mutations in nuclear-encoded mitochondrial genes; (3) lysosomal dysfunction, typified by GBA-associated PD with characteristic cognitive vulnerability; and (4) neuroinflammatory dysregulation, as shown in LRRK2-related PD. Importantly, these pathways are not restricted to monogenic forms but are recapitulated in sporadic PD, as shown by proteomic and transcriptomic studies delineating distinct molecular signatures. Integrating clinical and biological dimensions represents the next frontier in PD subtyping. Emerging evidence suggests that molecular endotypes may underlie or even drive specific clinical trajectories, offering a path toward a unified clinico-biological taxonomy. Mechanism-matched enrichment, e.g. by targeting lysosomal dysfunction in GBA carriers holds promise to enhance trial efficiency and therapeutic precision. In summary, converging data from genetics, molecular assays such as α-synuclein seed amplification, and large-scale omics approaches support the evolution of PD classification from purely clinical to integrated clinical–biological subtypes. This transition will enable mechanism-based stratification, more intelligent clinical trial designs, and ultimately lay the foundation for precision medicine in Parkinson’s disease.
O88
University of Cambridge, United Kingdom
This 2-Oral Sessions discussion will start with the rationale for targeting the immune system in Parkinson’s disease, with a brief examination of the evidence from epidemiological and cohort studies. We will focus on the links between clinical phenotype, disease prognosis and immune profile, and therefore the potentially relevant targets when considering intervention. We will then cover the trials to date which have targeted the immune system in PD, including drugs aimed at reducing microglial activation and anti-inflammatory and peripheral immunosuppressants. The discussion will include learning points for future trial design, including the challenges faced when running trials of immune-acting medication, the importance of participant selection and the optimal use of biomarkers. We will finish with a discussion of future directions and drugs in development.
O89
Osaka Toneyama Medical Center, Japan
In considering fundamental treatments for Parkinson's disease, the creation of animal models is a critically important challenge. First, considering the symptoms, the disease is slowly progressive and involves both motor and non-motor symptoms. Ideally, it should respond effectively to L-dopa. Furthermore, regarding the cause, if we can confirm the presence of α-synuclein aggregates—currently the most reliable indicator—and observe the progression of this process, it would make for an even better model. Animal model development is currently underway worldwide toward this goal. However, Parkinson's disease symptoms vary significantly between individuals and are not uniform, which presents inherent limitations. We hope to discuss this aspect as well.
O90
Newcastle University, United Kingdom
In vivo Neuroimaging studies with Positron Emission Tomography (PET) and translocator protein (TSPO) ligands have enormously contributed to understand the role of neuroinflammation in Parkinson’s disease (PD) and other Parkinsonisms.
Ongoing neuroinflammation has been reported at different stages of PD and increased microglial activation in PD patients correlated with motor disability, cognitive performances, and non-motor symptoms.
PET studies have also identified increased level of neuroinflammation in patients at risk of developing Parkinsonism, including patients with isolated REM sleep behaviour disorder (iRBD) and carriers of gene mutations related to Parkinsonism. It is still debated if presence of neuroinflammation in these early stages is beneficial or detrimental. Recent evidence would suggest that neuroinflammation (microglia activation) in iRBD patients could have a detrimental rather than a protective role.
O91
Université Laval, CERVO Brain Research Center, Rempart Neurophysiologie Inc., Canada
Gut problems, particularly constipation, are an important feature of Parkinson’s disease. Many studies have suggested that gut health plays a role in how the disease progresses, and constipation is now considered a risk of factor for faster decline. This session will discuss the evidence on how gut health influences PD progression, what are the mechanisms that might be mediating this gut-brain interaction, as well as the modifiable risk factors that we should know and tackle.
O92
Helsinki University Hospital, Finland
Parkinson’s disease (PD) is increasingly understood as a condition that involves not only the brain but also the gastrointestinal system. Many people with PD experience constipation years before motor symptoms appear. This early involvement of the gut has led researchers to focus on the gut–brain axis—the two-way communication network linking intestinal function, the immune system, metabolism, and the central nervous system.
A key part of this axis is the gut microbiome, the community of microbes living in the digestive tract. Studies consistently show that people with PD have an altered microbiome (“dysbiosis”). These changes are not explained by aging alone. Several microbial groups involved in producing short-chain fatty acids, regulating inflammation, and supporting intestinal barrier integrity appear reduced in PD, while others associated with inflammation may be increased.
Disruptions in the gut can influence the brain through immune activation, microbial metabolites, and increased intestinal permeability. One hypothesis suggests that misfolded α-synuclein may originate in the gut and travel to the brain through the vagus nerve—although this mechanism remains under active investigation.
The gut–brain axis has opened new avenues for understanding PD progression and exploring disease-modifying strategies. Current research examines whether targeting the gut—through diet, bowel management, microbiota modulation, or specific microbial therapies—can influence symptoms or the course of the disease. Clinical studies, including trials of bowel cleansing, dietary interventions, and microbiota-based treatments, show that gut-focused approaches can improve gastrointestinal symptoms and may impact motor or non-motor outcomes, though robust evidence for disease modification is still emerging.
For people living with PD, this research highlights the biological importance of gut health and underscores that PD is a whole-body condition. For clinicians and scientists, the gut–brain axis provides a promising framework to develop new biomarkers and therapeutic strategies that address PD beyond dopamine replacement alone.
O93
Teachers College, Columbia University, United States
Airway protective disorders, including swallowing and cough disorders (dysphagia and dystussia, respectively), are a pervasive consequence of PD, with prevalence estimates ranging between 80-90%. These deficits result in decrements to quality of life, increased caregiver burden, and severe health consequences including malnutrition, dehydration, aspiration pneumonia, and ultimately, death. In fact, aspiration pneumonia is often the leading cause of death in individuals with PD. There are several treatments that have demonstrated efficacy to improve airway protective outcomes (swallowing and cough disorders) in PD. This 2-Oral Sessions will offer opportunities to discuss recent developments in swallowing and cough treatment in Parkinson's Disease.
O94
University of Pennsylvania School of Medicine, United States
Psychosis, including hallucinations and delusions, in Parkinson's disease is very common over the long-term, and can be quite problematic, requiring careful assessment and management. Determining the cause of the psychosis informs management strategies. Antipsychotics are used in Parkinson's disease, but the potential benefits and risks of their use need consideration.
O95
Thomas Jefferson University, United States
Over the past decade, preclinical research has built a consistent, mechanistic case that physical exercise is neuroprotective in models of Parkinson’s disease (PD). Across toxin-based (6-OHDA, MPTP, rotenone) and genetic (A53T, PFF-seeded) rodent models, both voluntary and forced aerobic paradigms—running wheels, treadmill, and structured aerobic training—have been shown to improve motor outcomes, preserve nigrostriatal dopamine markers, and reduce neuronal loss. These functional benefits are replicated in multiple labs and across model types.
Mechanistically, preclinical studies of positive exercise effects converge on several complementary pathways including contributions from neurotrophic factors, improvements in mitochondrial biogenesis and function, enhancement of autophagy/clearance pathways, and shifts in peripheral and central immune phenotypes toward less pro-inflammatory states. Additionally, it was found that neuroprotective levels of exercise induce hypoxia in the brain leading to the stabilization of the transcription factor HIF1α. HIF1α target genes promote angiogenesis as well as other metabolic and cell cycle processes. cKO of this gene in neurons, prevents exercise-indued neuroprotection.
While it is clear aerobic levels of exercise can protect against PD pathology in preclinical models, gaps remain. For example, most studies are short-to-medium term and focus on early or prevention paradigms; but few, if any address exercise begun after established pathology or how long the neuroprotective effects of exercise last.
The historical aspects of the role of exercise in neuroprotection will be reviewed in this talk. Discussion of some of the newer preclinical findings, including work from our own lab examining how exercise remodels the vasculature of the brain as well as how neuroprotective levels of exercise can alter the both the epigenome and genome will be covered. These processes may underlie some of the long-term effects of exercise related to PD onset and progression.
Finally, evidence will illustrate that animal data strongly support exercise as a multitarget intervention that mitigates symptoms and alters core disease biology in PD models. Our understanding of the underlying biology wil hopefully accelerate clinical translation.
O96
Northwestern University, United States
There has been a 40-year search for a pharmacological treatment that may be neuroprotective for Parkinson's disease (PD). All such clinical trials have failed. Between 2002 and 2014 Michael Zigmond published a series of articles demonstrating exercise can be either neurorestorative or neuroprotective for the basal ganglia. These studies, and others, have formed the preclinical background of 4 successful clinical trials evaluating the effects of high intensity aerobic exercise on people with PD. The first was published by Schenkman et al. in 2018 in JAMA Neurology. They demonstrated that when people with PD, who have not yet started medication, exercised on a treadmill at 80-85% of their peak heart rate for 6 months, they progressed by .3 points on the MDS-UPDRS part III. The wait list control group progressed by 4.1 points. van der Kolk et al. published the results of their study in Lancet Neurology and showed a difference of 4.2 points between 2 groups at 6 months when comparing an at home cycling intervention with a control group. In 2021, Mak et al. published their results in the Journal of Parkinson's disease and showed a 4.6-point difference at 6 months using a multimodal aerobic exercise intervention. Most recently, Alberts et al. presented the results of their clinical trial (CYCLE II) at the Movement Disorders Society conference in 2025. Their cycling group improved by 2.6 points and their usual care group progressed by 2.4 points. All 4 studies showed that the signs of PD progressed more slowly (about 4 points) in the high intensity aerobic exercise group when compared to the control group. Collectively these four studies provide every reason to think that exercising at a high heart rate slows down the rate at which Parkinson's disease progresses. Whether slowing disease progression is the same as neuroprotection or disease modification are great questions. Studies by Fisher et al. in the Archives of Physical Medicine and Rehabilitation (2008) and De Laat et al., in npj Parkinson's Disease (2024), both suggest high heart rate intensity aerobic exercise increases the binding potential of dopamine and this does hint at neuroprotection.
O97
Karolinska Institutet, Sweden
Parkinson’s disease (PD) is a multifaceted neurodegenerative disorder characterized by a broad range of motor symptoms—including bradykinesia, resting tremor, rigidity, and impairments in balance and gait. Non-motor symptoms such as executive dysfunction and depression further compromise daily functioning and quality of life, adding complexity to treatment strategies.
Exercise has emerged as one of the most promising interventions for individuals with PD, demonstrating beneficial effects across both motor and non-motor domains. It is widely regarded as safe and has become a cornerstone of PD rehabilitation. While numerous studies have confirmed the positive impact of exercise on clinical symptoms and functional outcomes, relatively few have successfully documented exercise-induced neuroplasticity, including structural and functional brain changes. However, various forms of exercise appear to influence markers of neuroplasticity, although the relationship between these neural changes and improvements in symptoms and functions such as gait and balance remains insufficiently documented.
This talk will explore findings from systematic reviews and clinical trials investigating structural and/or functional brain changes as well as functional outcomes following exercise in individuals with PD, with a particular focus on gait and balance training interventions. Neuroimaging techniques such as magnetic resonance imaging (MRI), functional MRI (fMRI) and functional near-infrared spectrometry (fNIRS) will be discussed in relation to their ability to detect exercise-induced changes in brain structure, connectivity, and activity. Furthermore, the talk will address methodological quality and designs, as well as exercise recommendations.
O98
Banner Sun Health Research Institute, United States
Despite recent encouraging progress in Parkinson’s disease (PD) research, patients still progressively deteriorate and there are no disease-modifying therapies. The roadblock(s) are unclear but could be at least partially due to the continued accumulation of comorbid pathologies, including those involving other aggregated proteins including Abeta, tau, and TDP-43, as well as cerebrovascular disease (see Figure). The frequency that two or more of these are concurrently present suggests a synergistic etiopathogenesis that we should be searching for. Recently developed methods such as single-cell and spatial transcriptomics should be applied. This will require an abundant supply of high-quality postmortem human brain tissue from both affected and unaffected individuals. Essential objectives required to achieve this goal include much more emphasis on rapid-response autopsy teams allowing uniformly short postmortem intervals, assessment of the quality of not only RNA but many other macromolecules and neurochemical entities, together with longitudinal comprehensive, standardized clinical research assessments, detailed neuropathological characterization and development of powerful databases for wide international sharing. Brain banks should have adequate tissue storage facilities as well as the capacity to serve a high volume of tissue and data requests. Dramatic increases in brain bank funding are needed and this will require creativity as governments have historically been unreliable in their support. Beach TG et al. Parkinson Disease Neuropathological Comorbidities: Prevalences from Younger-Old to Older-Old, With Comparison to Non-Demented, Non-Parkinsonian Subjects. medRxiv 2025 PMCID: PMC11759614.
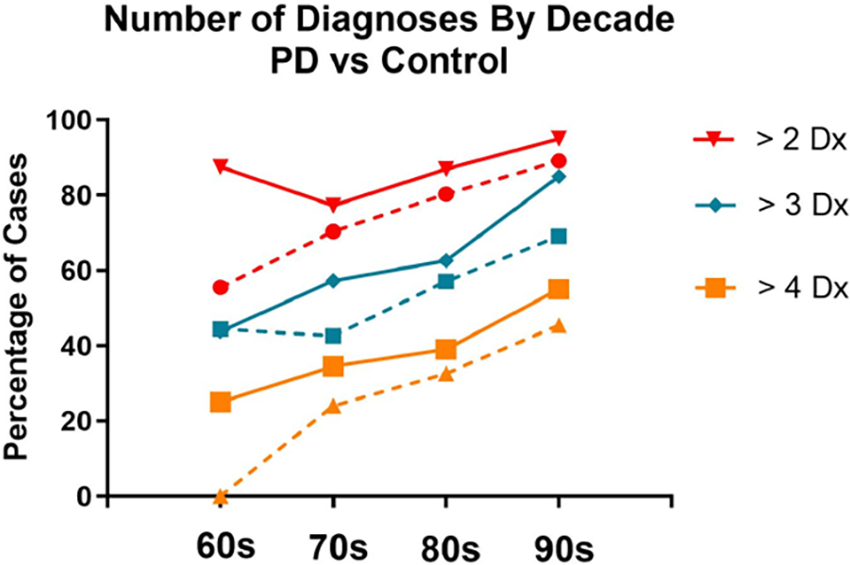
O99
Banner Sun Health Research Institute, United States
Brain and biospecimen banks have been instrumental in advancing our understanding of the molecular mechanisms underlying specific diseases and in guiding the development of targeted therapeutic interventions. Despite widespread recognition among scientists of their critical importance, the establishment and maintenance of comprehensive biobanks face numerous challenges. These challenges include difficulties in recruiting participants, often due to limited public awareness or misconceptions about donation. Additionally, participation can require a significant time commitment, especially when longitudinal clinical assessments are involved. Financial sustainability for the biobank is another major hurdle, as maintaining biobanks with high-quality characterized biological samples entails substantial costs for staffing and infrastructure.
The Brain and Body Donation Program (BBDP), part of the Arizona Study of Aging and Neurodegenerative Disorders and hosted at Banner Sun Health Research Institute, has addressed many of these challenges since its beginning in 1987. To date, the program has banked over 2,300 brains and received more than 970 whole-body donations.
Most participants are cognitively normal older adults residing in the retirement communities of metropolitan Phoenix, Arizona. The program also actively recruits individuals diagnosed with Alzheimer’s disease, Parkinson’s disease, cancer and other neurodegenerative disorders of aging. Enrolled participants undergo annual standardized assessments, including general medical, neurological, neuropsychological, and movement disorder evaluations. Many also contribute blood and cerebrospinal fluid samples and participate in ancillary imaging studies.
The program is built on a strong commitment to rapid autopsy, achieving a median postmortem interval of just 4.0 hours, ensuring the collection of high-quality, well-characterized biological samples, which have been shared with more than 850 investigators across 40 U.S. states and 29 countries, resulting in over 850 peer-reviewed publications in the past two decades.
The success of the BBDP is a testament to the dedication of its participants and the meticulous logistical and operational planning required to support it. This includes 24/7 availability of trained personnel, close coordination with families, hospices, and funeral homes, as well as sustained financial support from multiple national and state grants, as well as philanthropic contributions.
O100
Department of Neurology and Neurorehabilitation, Klinikum Osnabrueck, Academic teaching hospital of the University Muenster, Germany
Parkinson's disease and the gastrointestinal tract are linked in many ways. Pathophysiologically, the gastrointestinal tract is a gateway for alpha-synuclein pathology. Diagnostically, modern instrumental procedures allow increasingly precise imaging of movement disorders at all levels of the gastrointestinal tract, from the oral cavity to the rectum. In addition, specific phenotypes of gastrointestinal motility disorders can be used for the differential diagnosis of neurodegenerative Parkinsonian syndromes. Therapeutic options for gastrointestinal symptoms have increased significantly in recent years and serve to alleviate symptoms and improve the effectiveness of dopaminergic therapy. Due to the complexity of disorders throughout the gastrointestinal tract, modern management should be carried out in an interprofessional Parkinson's network. This lecture summarises current developments in this field and presents potential further developments.
O101
Ghent University Hospital, Belgium
The gut-brain axis is a complex communication network which allows the gut and the brain to influence eachother. Several clinical and biological factors emphasize the importance of the gastrointestinal tract in Parkinson’s disease. Moreover, therapies targeting the gut bacteria have shown beneficial effects in animal models of Parkinson’s disease. At this time, fecal microbiota transplantation (FMT) represents the most effective method for achieving comprehensive and long-lasting changes in gut microbiota composition. FMT is safely and successfully used for treating Clostridioides difficile infections, for which it is an approved indication. However, evidence supporting the use of FMT in patients with neurological disorders is limited. Our group and others have performed clinical trials investigating the effect of FMT in patients with Parkinson’s disease. We will discuss these results, extending to what this means for future clinical trials and potential other microbiota-targeting therapies.
O102
University of Malaya, Malaysia
In recent years, there has been growing interest in the close relationship between gut health and the brain. This connection, often referred to as the “gut–brain axis,” has been particularly relevant to Parkinson’s disease (PD), where gastrointestinal symptoms such as constipation and bloating are common and may appear years before movement symptoms. At the same time, research has shown that the trillions of microorganisms living in the gut—the gut microbiome—play important roles in digestion, immunity, metabolism, and even how drugs are absorbed by the body. Laboratory and clinical studies have suggested that changes in the gut microbiome and its chemical products (metabolites) may influence inflammation and other biological pathways linked to PD. These findings have sparked interest in whether improving gut health could positively impact PD symptoms or slow disease progression.
Several approaches are currently being explored. Dietary strategies aim to support beneficial gut bacteria through increased intake of fibre, plants, and fermented foods. Prebiotics (nutrients that feed gut bacteria) and probiotics (live bacterial supplements) have been tested for various symptoms in PD, with some early studies reporting improvements such as better bowel function. Other emerging strategies include targeted antibiotics, microbial metabolites, and fecal microbiota transplantation (FMT), although these remain experimental and are not yet widely used in clinical practice.
A major challenge in developing gut-based therapies is that PD is highly variable from person to person, and the microbiome also differs widely based on age, diet, geography, lifestyle, and medications. For these reasons, it is unlikely that a single “one-size-fits-all” approach will work for everyone with PD. Future treatment strategies may need to be personalized based on an individual’s biology, microbiome, and clinical profile.
This lecture will summarize the current scientific evidence supporting dietary and probiotic therapies for PD, highlight what we know so far, and discuss what remains under investigation. While there is genuine excitement about gut-directed interventions, well-designed clinical trials are essential to determine which approaches are effective, safe, and meaningful for people living with PD.
O103
VIB KU Leuven Center for Brain and Disease Research, Belgium and Amsterdam University Medical Center, the Netherlands, Netherlands
Introduction: How can cognitive health be maintained during human aging? To identify protective genetic and biomolecular factors that associate with the escape of cognitive decline we set up the 100-plus Study, a longitudinal cohort study of cognitively healthy centenarians. Currently the cohort includes >500 centenarians. We collect blood and faeces samples, and ∼30% of the centenarians agree to postmortem brain donation. This centenarian brain cohort offers a unique window into mechanisms underlying this neuroprotection.
Methods: Centenarians with high cognitive performance at baseline mostly maintain this until death. Neuropathological analysis indicate that these high performers resisted critical development of Aβ plaques, and tau abundance was low across all centenarians. Brain protein profiling indicated that across all centenarians, AD patients and healthy controls, only five proteins associated with Aβ abundance, revealing upregulation of HTRA1, LRP1 and NRXN1 as early AD-associated changes. Conversely, tau abundance associated with ∼20% of the quantified proteome, revealing GPRIN1 as the top tau-associated protein. While the majority of the centenarians resisted accumulation of amyloid, one third of centenarians had high Aβ abundance, often with wide tau-spreading (Braak stages IV/V), however, they diverged from AD cases and controls by maintaining an unexpectedly low local tau abundance. Furthermore, centenarians who maintained high cognitive performance until death had maintained proteostasis (low ubiquitin peptides, high proteasome components), high PCSK1 levels (prohormone maturation), high PFKFB2 levels(glycolysis regulation), high mitochondria-coupled lipid β oxidation and lower APOE levels.
Conclusions: Together, our findings suggest that, in a model where Aβ facilitates tau seeding, centenarians maintain brain health by actively buffering against tau accumulation.
O104
Buck Institute for Research on Aging, United States
Parkinson’s disease (PD) is a progressive neurological disorder which primarily affects motor movement but also causes a range of non-motor symptoms. Characteristic hallmarks include progressive loss of dopaminergic neurons in the substantia nigra pars compacta (SNpc) and the buildup of intracellular protein aggregates known as Lewy bodies containing the protein alpha-synuclein. While the etiology of PD is multifactorial, aging is widely recognized as the most significant risk factor for the disorder. Cellular senescence, a hallmark of aging, has in recent years emerged as a potential driver of pathology associated with PD. Senescent cells accumulate in the aging brain and exhibit a pro-inflammatory senescence associated secretory phenotype (SASP), contributing to disease pathogenesis through multiple mechanisms. This lecture will involve a discussion of the current evidence linking cellular senescence to PD, the potential underlying molecular and cellular mechanisms involved, and what is still needed to unlock the full therapeutic potential of targeting cellular senescence as a viable treatment for the disease.
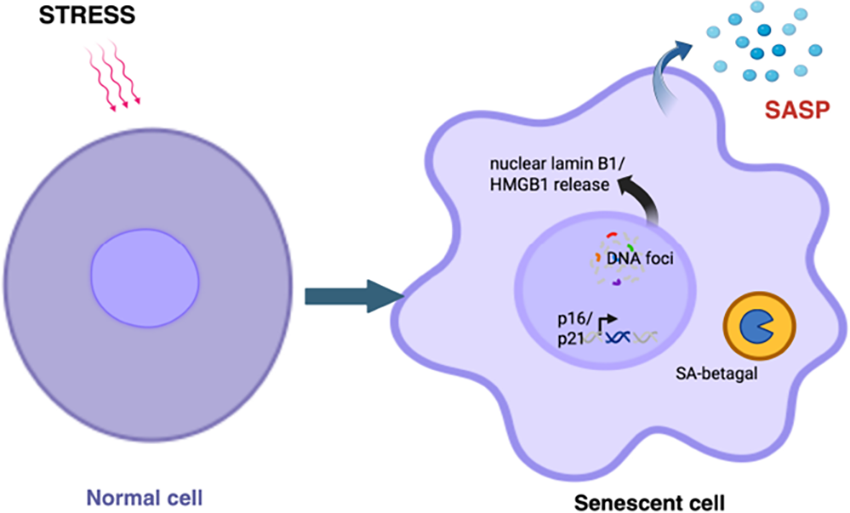
O105
University of Sydney, Australia
Astrocytes are the principal homeostatic cells of the central nervous system, playing a critical role in neuronal survival and function. In Parkinson’s disease (PD), their involvement is complex, both protective and detrimental, mirroring their dual role in other neurodegenerative disorders but with unique features. Notably, astrocytes contribute to α-synuclein processing and express proteins encoded by PARK genes, most of which are causative in familial PD 1.
Under physiological conditions, astrocytes clear extracellular α-synuclein, supporting synaptic plasticity 2. This clearance intensifies as α-synuclein levels rise. In PD, astrocytes accumulate more non-fibrillar, post-translationally modified α-synuclein aggregates than neurons. This suggests saturation of degradation pathways and the onset of astrocytic protein modifications. Dysfunctional PARK gene–encoded proteins further compromise mitochondrial and lysosomal integrity, diminishing astroglial capacity to clear synaptic α-synuclein and to transfer healthy mitochondria to neurons.
Recent gene trajectory analyses indicate a progressive shift toward fibrous, highly reactive astrocytes 3, reflecting phenotypic changes that may amplify disease pathology. These dynamics are further complicated by co-pathologies and regional α-synuclein burden 4, underscoring the need for comprehensive research to identify reliable astrocytic biomarkers and therapeutic targets.
Li W, Fu Y, Halliday G, Sue C. Front Cell Dev Biol 9, 612476 (2021).
Park J, Chung WS. Curr Opin Neurobiol 81, 102732 (2023)
Ma M, et al. Nat Comm 16, 7146 (2025)
Wang L, et al. Mov Disord doi: 10.1002/mds.70023 (2025)
O106
Purdue University, United States
This 2-Oral Sessions will examine how cutting-edge digital health technologies and wearable systems are transforming the management of speech and swallowing in Parkinson’s disease (PD). These disorders are highly prevalent in PD and, if left untreated, can lead to serious health complications and diminished quality of life. Emerging innovations are paving the way for earlier detection and more effective interventions. Participants will explore and discuss solutions such as smartphone-based applications, advanced speech recognition algorithms, sensor-integrated wearable patches, and AI-driven approaches currently in development and clinical deployment. The session will also address critical challenges, including large-scale validation, regulatory pathways, integration into clinical practice, and patient-centered considerations.
O107
Tel Aviv University, Israel
The integration of digital technologies into Parkinson's disease (PD) clinical trials represents a paradigm shift in how we capture, quantify, and interpret disease progression and response to medication. Traditional clinical endpoints, relying on infrequent in-clinic assessments and subjective rating scales, often failing to capture the complex, fluctuating nature of PD symptoms that patients experience in their daily lives. Digital health technologies—including wearable sensors, smartphone applications, and remote monitoring devices—offer unprecedented opportunities to collect continuous, objective, real-world data on motor and non-motor symptoms reflecting not only pathological symptoms but also disease burden.
In this round-table we will examine the current landscape of digital endpoints in PD clinical research including examples on the use of accelerometers and gyroscopes to quantify tremor, bradykinesia, mobility, gait and freezing of gait; the use of smartwatches for monitoring medication response and wearing-off phenomena and the utility of smartphone-based tests for evaluating cognition, speech, and finger tapping. During the 2-Oral Sessions, we will touch upon how these technologies are used, for which populations and under which conditions. We will explore their implementation in both research, care, and discuss the opportunities but also the challenges that arise from these technologies for widespread implementation.
O108
Cervo Brain Research Center, Université Laval, Canada
Neuroinflammation is a hallmark of Parkinson’s disease (PD), yet the initiating cellular events that sustain this chronic inflammatory state remain incompletely understood. Aging, the strongest risk factor for PD, is accompanied by the progressive accumulation of DNA damage and a decline in genome maintenance capacity. Such naturally occurring DNA lesions—arising from oxidative stress, mitochondrial dysfunction, and replication-independent breaks—can overwhelm repair systems, persistently activating DNA damage responses.
Mounting evidence suggests that cellular senescence may represent a key mechanistic link between age-related DNA damage and neuroinflammation in PD. Both neurons and glial cells exhibit molecular hallmarks of genomic instability, such as γH2AX foci and defective DNA repair pathways including non-homologous end joining and base excision repair. Persistent DNA lesions can trigger senescence-like responses even in post-mitotic neurons.
In the aging brain and PD models, senescent astrocytes and microglia release cytokines, chemokines, and matrix-remodeling enzymes collectively known as the senescence-associated secretory phenotype (SASP). This SASP amplifies neuroinflammation and can propagate senescence to neighboring cells, establishing a self-sustaining inflammatory loop. Dopaminergic neurons, particularly susceptible to oxidative stress, may thus become trapped in a feedback cycle where DNA damage induces senescence-like signaling, promoting SASP release, glial activation, and further neuronal injury.
Markers of senescence have been identified in post-mortem PD midbrain tissue and in alpha-synuclein–based models, reinforcing the contribution of senescence to disease progression. Interventions that target these pathways—such as senolytics, or DNA damage response modulators, show early preclinical promise in reducing inflammation and preserving dopaminergic neurons.
This 2-Oral Sessions will explore the hypothesis that age-related DNA damage–induced senescence drives neuroinflammation in PD. Discussions will examine the connections between genomic instability, cellular dysfunction, and markers of stressed or senescent cells. We will also consider how interconnected processes—including mitochondrial health, lysosomal function, and key signaling pathways—can influence neuronal vulnerability. By integrating these perspectives, we will discuss whether targeting multiple cellular pathways could offer new strategies to slow or modify PD progression.
O109
University Clinic Cologne, Germany
As part of the round table discussion, we will explore the emerging concepts of resilience and reserve in Parkinson’s disease and their growing importance for both research and clinical care. We will discuss how these mechanisms help explain why some individuals maintain motor and cognitive function for many years despite ongoing neurodegeneration, while others experience more rapid decline.
Drawing on recent clinical and neuroimaging studies, we will highlight evidence linking lifestyle factors, such as physical activity, cognitive engagement, and social participation, to measurable changes in brain structure and connectivity that support functional maintenance. These findings suggest that everyday behaviors may strengthen the brain’s ability to adapt and compensate, effectively building a buffer against disease progression.
Beyond understanding these mechanisms, we will also consider their practical implications. Resilience-based perspectives offer a new framework for developing personalized interventions that go beyond symptom management, targeting the underlying neural systems that promote adaptation and stability. Moreover, incorporating measures of resilience and reserve into clinical trials may enhance how we assess the true efficacy of novel therapies, helping to identify which treatments not only reduce symptoms but also strengthen the brain’s capacity to cope with Parkinson’s over time.
O110
United States
Biomarkers are transforming diagnosis and clinical monitoring across medicine. Biomarkers for Parkinson’s disease, such as dopamine transporter imaging, have been available for over a decade. New biomarkers that assess alpha-synuclein pathology, either by skin biopsy or spinal fluid sampling have recently become available. These new biomarkers have had a profound effect on research and are beginning to make their way into clinical practice. One major advantage of these biomarkers is that they can differentiate between Parkinson’s disease and some of the related conditions, such as Progressive Supranuclear Palsy, and possibly Multiple System Atrophy. Dopamine imaging does not have this ability. Disadvantages to alpha-synculein biomarkers include cost, need for invasive procedures to collect them and lack of clear impact on therapeutic decision making in the absense of disease modifying therapeutics. Finally, development of an alpha-synuclein PET tracer continues to be a major unmet biomarkers goal. Several research teams are making progress toward a successful PET ligand.
O111
Kyoto University Office of Research Acceleration, Japan
Parkinson’s disease (PD) is characterized by the progressive loss of nigral dopaminergic neurons, resulting in relentlessly advancing motor symptoms such as bradykinesia, resting tremor, and muscle rigidity. Non-motor symptoms, including autonomic dysfunction and cognitive decline—primarily attributable to the degeneration of non-dopaminergic systems—also represent key clinical features of PD.
Although L-dopa has remained the mainstay of symptomatic treatment for motor symptoms in PD for more than half a century, its long-term administration in advanced stages leads to troublesome motor complications, including wearing-off and dyskinesia. To restore dopaminergic function as an alternative therapeutic strategy, transplantation of fetal ventral midbrain (VM) tissue was initiated at Lund University, Sweden in the late 1980s. Subsequent open-label trials demonstrated marked improvement in motor—but not non-motor—symptoms, as well as reductions in dopaminergic medication use.
However, the applicability of this approach has been limited by the scarcity of electively aborted fetal tissue and substantial ethical concerns. Moreover, two randomized clinical trials conducted in the United States in the early 2000s failed to demonstrate superiority of fetal VM transplantation over sham surgery. A new adverse effect, graft-induced dyskinesia (GID), was also reported in a significant proportion of trial participants. Despite these unfavorable outcomes, sub-analyses suggested that patients aged ≤60 years and those with less advanced disease exhibited clinical benefit, rekindling interest in future trial design.
Stem cells, including embryonic stem (ES) cells and induced pluripotent stem (iPS) cells, have since attracted considerable attention as alternative sources of dopaminergic neurons. Recently, the Kyoto Trial—a first-in-human clinical study of iPS cell-derived dopaminergic progenitor transplantation—was completed. No serious adverse events or GIDs were observed, and four of the six recipients exhibited significant motor improvement two years after surgery.
In this round-table discussion, we will explore the current status and future prospects of stem cell-based transplantation therapy for PD, drawing on findings from the Kyoto Trial as well as recent ES cell-based clinical studies.
O112
International HM Hospitales, Spain
Over the past ten years, MRI-guided Focused Ultrasound has emerged as a novel functional neurosurgical tool for the treatment of movement disorders. This technology can be applied in three main modalities: high-intensity focused ultrasound (HIFU) for therapeutic brain ablation, low-intensity focused ultrasound (LIFU) for blood–brain barrier (BBB) opening, and LIFU for neuromodulation. HIFU ablation has rapidly expanded as a symptomatic therapy aimed at improving motor manifestations in movement disorders, while the other two modalities remain experimental approaches for neurological and neurodegenerative diseases. HIFU has demonstrated strong efficacy in improving tremor and functional disability in essential tremor, both unilaterally and bilaterally. In the case of Parkinson’s disease, up to three randomized controlled trials have shown the efficacy of unilateral ablation in improving motor symptoms. Additionally, some uncontrolled reports have suggested the potential of bilateral treatment. However, the use of different brain targets - selected according to specific clinical profiles - and the intrinsic complexity of the disease, which involves more challenging post-treatment management, underscore the need for further evidence to fully realize the therapeutic potential and optimize patient selection.
Evidence for other indications, such as dystonia, pain, or psychiatric disorders, remains limited to small case series or isolated reports. This lecture will aim to summarize the most relevant evidence currently available for the treatment of Parkinson’s disease and other movement disorders, and to explore the potential for expanding its applications, both through HIFU ablation and the emerging prospects of LIFU neuromodulation and BBB opening.
O113
DOMMO Clinic, Brazil
This 2-Oral Sessions explore recent advances in Deep Brain Stimulation (DBS), highlighting the rapid evolution of the field from traditional target-based approaches toward network-guided and personalized neuromodulation.
Panelists will discuss technological innovations including new directional leads, adaptive stimulation paradigms, and improved imaging integration, which are allowing more precise personalized modulation. The use of connectomic approaches and tractography was emphasized as an important tool for refining target selection and understanding variability in patient outcomes.
Clinical expansion of DBS indications was also addressed, with growing evidence supporting its application beyond movement disorders, including psychiatric conditions, chronic pain, and epilepsy. The panel reviewed current challenges such as patient selection, optimization of programming strategies, and long-term outcome monitoring.
Finally, the discussion underscored the importance of multidisciplinary collaboration, advanced imaging, and rigorous clinical research to further refine DBS therapies and translate emerging technologies into meaningful clinical benefit for patients.
O114
Karolinska Institutet, Sweden
Exercise has emerged as one of the most promising interventions for individuals with PD, demonstrating beneficial effects across both motor and non-motor domains. It is widely regarded as safe and has become a cornerstone of PD rehabilitation. While numerous studies have confirmed the positive impact of exercise on clinical symptoms and many functional outcomes, relatively few have successfully documented exercise-induced neuroplasticity. However, various forms of exercise appear to influence functional brain changes.
This round table will discuss findings of functional outcomes and changes in the brain following exercise in individuals with PD, with a particular focus on gait and balance training interventions. Different exercises and training interventions will be discussed as well as methodological quality and different designs and protocols. Neuroimaging techniques such as functional magnetic resonance imaging (fMRI) and functional near-infrared spectrometry (fNIRS) will be discussed in relation to their ability to detect exercise-induced changes in connectivity, and activity. Furthermore, exercise recommendations and how to implement them will be discussed.
O115
United Kingdom
The accumulation of alpha-synuclein is a pathological hallmark of Parkinson’s disease (PD) and is sufficient to cause neurodegeneration, as mutations in the alpha-synuclein gene that result in its increased expression cause autosomal dominant Parkinson’s disease. Understanding how alpha-synuclein causes pathology is clearly central to developing therapeutic strategies for PD. Likewise, since alpha-synuclein causes disease via gain-of-function mechanisms, it is important to understand how one can potentially ameliorate its toxicity by lowering its levels. We will discuss possible strategies that can be used to this end.
O116
Movement Disorders Clinic, Department of Neurology, School of Medicine of the University of São Paulo, Brazil
Recent evidence underscores the neurobiological and clinical efficacy of multimodal rehabilitation combining structured exercise, cognitive engagement, and non-invasive neuromodulation in Parkinson’s disease (PD). Sena et al. (2023) demonstrated through meta-analysis that high-intensity training significantly improves motor performance, aerobic fitness, and quality of life in PD. Rotondo et al. (2024) described the METEX-PD protocol, quantifying the dose–response effects of standardized aerobic exercise on neurotrophic biomarkers (BDNF, IGF-1, irisin) and brain connectivity, elucidating the molecular basis of exercise-induced plasticity. Zhao et al. (2024), in a network meta-analysis of 111 RCTs (n=5,358), identified Tai Chi, dance, and agility training as the most effective modalities for improving MDS-UPDRS-III, balance, and gait. Wong et al. (2023) reported that dual-task training significantly enhances gait and executive performance, supporting motor-cognitive integration. Finally, Leocadi et al. (2024) demonstrated that dual-task gait training combined with action observation and motor imagery reorganizes salience and default mode networks, correlating with improved executive accuracy. Collectively, these findings demonstrate that multimodal, high-dose exercise interventions promote neuroplasticity and functional gains in PD, supporting their inclusion as core components of neurorehabilitation frameworks.
References
Sena IG et al., 2023. PLoS One. Rotondo R et al., 2024. Front Neurol. Zhao H et al., 2024. Front Neurol. Wong P-L et al., 2023. Arch Phys Med Rehabil. Leocadi M et al., 2024. J Neurol.
O117
Washington University School of Medicine, United States
This 2-Oral Sessions will focus on the role of Occupational Therapy (OT) in supporting people with PD and their care partners across disease progression and clinical setting. Participants will share their experiences working with OT as well as tips and strategies to optimize the benefits of OT services.
O118
Radboud University Medical Center, Netherlands
The combination of monitoring technologies such as wearables and the emergence of artificial intelligence (AI) create exciting opportunities to better understand and manage Parkinson’s disease (PD). These tools enable objective and continuous measurement of PD in daily life, beyond what can be captured during brief in-clinic visits. This could help tailor care to individual needs, enable proactive and preventive interventions, support self-management, and provide more sensitive outcome measures for clinical trials.
However, their success depends on whether they measure aspects that matter to people living with PD, and produce actionable insights for patients, healthcare providers and researchers. This raises important questions: How do we ensure that digital biomarkers reflect meaningful aspects of PD? Which conditions need to be fulfilled to be able to trust these measurements? To what extend can we leave the interpretation of the large amounts of monitoring data up to AI? And how can we integrate these technologies into care and research without increasing the burden for those who use them?
In this session, we invite people with PD and their near ones, and all those involved in PD care, research, and technology development to share their experiences and ideas. Together, we will explore how monitoring technologies can shape the future of PD care and research, and identify key steps needed to get there.
O119
ShakingInMyBoots1, United States
This talk delves into the challenges faced by people with Parkinson's (PwPs) in managing their medication and the reasons they seek alternative treatments. I will highlight the limitations and side effects of prescribed medications, and how the unpredictability and mental burden of medication management often drive PwPs to explore other options, including natural sources of levodopa, alternative therapies, and other non-pharmaceutical approaches. By drawing from personal experience and conversations with other PwPs, primarily through my social media accounts, this talk aims to shed light on the reality of living with Parkinson's and the ongoing search for effective treatments beyond traditional healthcare offerings. I will also discuss the role that expectation, credible messengers, and misinformation on-line, often influence decision making and why education is needed to ensure expectations are realistic, people are not manipulated, and hope is not lost.
O120
University of Cambridge, United Kingdom
Stem cell therapies for Parkinson's come in many different forms but the one which is of greatest therapeutic potential is that which seeks to make replacement dopamine cells of the type lost in Parkinson's from human stem cell sources. In this approach, the strategy is to take a human stem cells line (either embryonic or taken from an adult- so called induced pluripotent stem cell lines) and generate dopamine precursor cells that can then be injected directly into the brain where they were differentiate and mature into a new population of nigral dopamine cells. By so doing, the expectation is that they will release dopamine and obviate the need for patients to take their dopamine drugs, which in turn will prevent them from developing the long term side effects from such agents (e.g. dyskinesias). At this stage this approach is still in early phase clinical trials so it is still not known whether this approach will work and even if it does whether this will be competitive against other advanced therapies being developed for Parkinson's as well as affordable. It is also important to understand that this approach will never be curative as the disease process underlying Parkinson's will continue but what it will do, if it works, is dramatically change how we treat the dopamine responsive elements of Parkinson's.
As with any new experimental therapy, all trials using these type of cells should be being done at no cost to the patient as they need to funded by those delivering the trial. In this regard, there are many therapies that are being advertised for Parkinson's that either expect the patient to pay for the treatment and/or it works in a way that is not related to dopamine cell replacement. In such cases it is important to better understand the basis for the trial and how it is proposed to work in Parkinson's and why one is having to pay for it, if it has not been proven and approved by national medicines agencies.
O121
University of Rochester Medical Center, United States
On the basis of both scientific progress and popular lore, there is growing optimism in the therapeutic potential of cannabis (marijuana) and cannabinoid-based chemicals for Parkinson's disease and other movement disorders. However, many also hold significant skepticism regarding the scientific basis for this therapeutic optimism and have additional concerns regarding the safety and regulation of cannabinoid products, particularly those available without prescription. In this session we will examine what the evidence supports and how people are approaching this in clinical practice when there is an absence of strong evidence. We will similarly look at what are the real and potential risks of these products.
The endocannabinoid system (the systems in the body that react to externally administered and internally created cannabinoids) is strongly tied to motor function and dysfunction, with basic research suggesting several promising therapeutic targets related to cannabinoids for movement disorders. Clinical research on cannabinoids for motor and nonmotor symptoms in Parkinson's disease, Huntington's disease, Tourette's syndrome, dystonia, and other movement disorders to date are promising at best and inconclusive or negative at worst. Research in other populations suggest efficacy for common symptoms like pain and sleep. While social campaigns against recreational cannabinoid use focus on cognitive changes in adolescents, the long-term sequelae of regulated medical use in older adults with movement disorders is unknown. The overall risks of cannabinoids may be similar to other commonly used medications and include falls and apathy.
Further research is greatly needed to better understand the actual clinical benefits and long-term side effects of medical cannabis products for movement disorders indications and populations.
O122
University of Auckland, New Zealand, New Zealand
Parkinson’s disease (PD) is the fastest-growing neurological condition, affecting more than 11 million people worldwide. The standard dopaminergic treatment for motor symptom control remains levodopa and despite many years of research, there have been no pharmacological innovations in disease-modifying therapies for PD. Whilst the search for disease-modifying and curative therapies for PD continues, the management of PD remains a major focus.
In recent years, there has been shift in interest by patients, caregivers, clinicians and researchers towards non-pharmacological approaches in PD such as the role of diet and exercise. Much is now known about exercise yet the role of diet requires further investigation.
The aim of this presentation is to review the scientific evidence which has examined the effect of dietary patterns, foods, beverages, dietary supplements including nutrients, bioactive compounds and biotics on outcomes in the management of PD. The presentation will conclude with future perspectives on the dietary approaches which hold promise in disease-modification in PD.
O123
University of Piemonte Orientale, Italy
Immune dysregulation in PD is both systemic and central. The main modifications detected so far include:
Peripheral blood immune changes Altered immune populations Monocytes Increased classical (CD14++CD16−) and intermediate (CD14++CD16+) monocytes, with enhanced expression of MHC-II and TLR2 (activated state) T cells Shift toward pro-inflammatory phenotypes Increased Th1 and Th17 CD4+ T cells Reduction in regulatory T cells, which normally suppress immune activation Cytotoxic CD8+ T cells with increased reactivity to α-syn peptides, suggesting antigen-specific adaptive immune activation B cells Overall reduced, with decreased antibody diversity and regulatory capacity Circulating cytokines and chemokines (sera/plasma) Pro-inflammatory cytokines are elevated: TNF-α, IL-1β, IL-2, IL-6, IFN-γ Chemokines CCL2 (MCP-1), CXCL10 (IP-10): recruit monocytes and T cells into the CNS Anti-inflammatory cytokines (IL-10) are often decreased/dysregulated Gut immune alterations Enteric glial cells and intestinal macrophages show increased inflammatory markers Gut barrier dysfunction allows bacterial products and immune signals to reach circulation α-syn pathology often begins in the enteric nervous system, possibly triggered by chronic mucosal inflammation Central (Brain/CNS) immune changes Microglial activation Postmortem studies show chronic activation of microglia in substantia nigra and striatum Activated microglia produce ROS, TNF-α, IL-1β, IL-6, and complement proteins, perpetuating neuronal injury Astrocyte reactivity Astrocytes shift to a pro-inflammatory phenotype under microglial signals, contributing to neuronal stress and α-synuclein aggregation Infiltrating peripheral immune cells T cells (CD4+ and CD8+) have been identified in the substantia nigra, cingulate cortex, and CSF of PD patients Peripheral adaptive immunity gains access to the brain, possibly through a compromised blood-brain barrier (BBB) Autoimmunity to α-synuclein Misfolded α-synuclein acts as a neoantigen, presented by MHC-II on microglia or peripheral APCs Specific α-synuclein-reactive T cells have been found in PD blood and brains
Further to reinforce the clinical relevance of immune dysregulation in PD, the degree of systemic inflammation correlates with disease severity and progression, and immune-modulators (e.g., TNF inhibitors, Treg-boosting strategies, α-synuclein vaccines) are currently under investigation as disease modifying treatments.
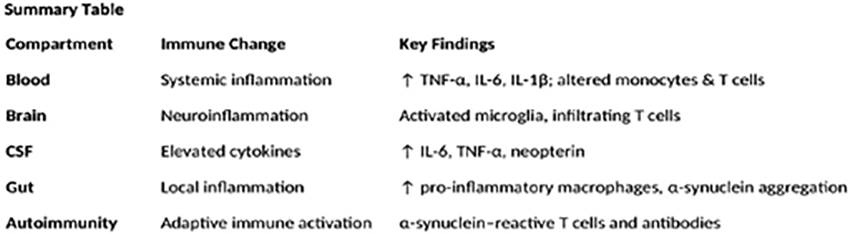
O124
Newcastle University, United Kingdom
Chronic neuroinflammation is thought to induce neuronal death and accelerate progression of neurodegenerative diseases by overproduction and secretion of pro-inflammatory cytokine.
Both post-mortem and in vivo imaging studies have reported presence of ongoing neuroinflammatory processes in Parkinson’s disease (PD) and other parkinsonisms. Evidence of activated microglia, the main immune defence in the CNS and the major cellular mediators of neuroinflammatory processes, has also been reported in patients at high risk of PD, suggesting a potential detrimental effect of neuroinflammation in the prodromal stage of the disease, although this is still debated.
Neuroimaging studies with Positron Emission Tomography (PET) and translocator protein (TSPO) ligands have enormously contributed to understand the role of neuroinflammation in PD and other neurodegenerative diseases, and this field is rapidly expanding. In fact, while drugs able to modulate neuroinflammation could play a significant role as disease-modifying agents, a better understanding of the time course, extension, and role of neuroinflammation in the different stages of the disease is still needed.
Technical advancements in the imaging field are also occurring to overcome the limitations of PET TSPO ligands, which, currently, are the most used for imaging brain inflammations. Non-TSPO ligands, including radiotracers targeting the cannabinoid receptor 2, cyclooxygenase-2, and P2X7 receptor are at this time being evaluated. Additionally, there is growing evidence that new Magnetic Resonance Imaging techniques could also play a significant role in characterising neuroinflammation in neurodegenerative diseases.
O125
University of Cambridge, United Kingdom
This talk will start with the rationale for targeting the immune system in Parkinson’s disease, with a brief examination of the evidence from epidemiological and cohort studies. This will focus on the links between clinical phenotype, disease prognosis and immune profile, and the potentially relevant immune targets when considering intervention. It will then cover the trials to date which have targeted the immune system in PD, including drugs aimed at reducing microglial activation and anti-inflammatory and peripheral immunosuppressants. The talk will cover learning points for future trial design, the challenges faced when running trials of immune-acting medication, the importance of participant selection and the optimal use of biomarkers. It will finish with a discussion of future directions and drugs in development.
O126
Luxembourg
Human brain organoids have matured from a conceptual curiosity to a robust, disease-relevant platform to evaluate disease-modifying therapies. We have established midbrain-specific organoids that reproducibly generate dopaminergic neuron populations and recapitulate core Parkinson’s disease (PD) features, including progressive dopaminergic vulnerability, α-synuclein pathology, oxidative stress, and neuromelanin-like granules. Patient-specific models carrying PD-associated variants (e.g., LRRK2 and GBA) display disease associated phenotypes, providing entry points for intervention. We have extended these systems into functional assembloids to model inter-regional circuitry and incorporated microglial components to capture neuron–immune crosstalk that modulates α-synuclein phosphorylation and spread.
Building on these advances, we deploy organoids as quantitative testbeds for candidate disease-modifying strategies. Standardized differentiation pipelines, lot-to-lot QC (cell composition, transcriptomic identity, electrophysiology), and imaging-based phenotypic endpoints enable reproducible pharmacology at scale. Using these readouts, we have demonstrated (i) mutation- and pathway-specific responses of LRRK2 and GBA backgrounds to modulators of kinase activity, mitochondrial stress, and lipid metabolism and (ii) target engagement linked to cellular rescue (e.g., restoration of TH+ neuron integrity, normalization of autophagic flux).
Key challenges remain, including maturation state, vascular and peripheral inputs, and inter-donor variability. However, these are increasingly tractable through protocol refinements and benchmarking to human datasets. The central message of this talk is rather pragmatic; by anchoring therapeutic hypotheses in human pathomechanisms observable in complex, patient-specific tissue models, organoids allow us to de-risk translation, and focus resources on interventions with a realistic chance to modify PD progression.
O127
Osaka Toneyama Medical Center, Japan
It is well established that early intervention is critical for the effective treatment of neurodegenerative diseases. The significance of this approach has increased with the advancement of nucleic acid-based therapies and antibody treatments, particularly those targeting protein aggregation and propagation. Consequently, the development of animal models that exhibit early symptoms is essential for advancing Parkinson’s disease research and therapeutic development. Demonstrating therapeutic efficacy in these models is a key step in halting disease progression.
Prodromal symptoms of Parkinson’s disease include olfactory dysfunction, REM sleep behavior disorder, sleep disturbances, gastrointestinal dysfunction, and mood or psychiatric symptoms. Various animal models—based on genetic modifications, α-synuclein overexpression, α-synuclein injection, or exposure to environmental toxins—have been developed to replicate these early features. In this context, we will introduce these models and provide detailed information on the mouse and monkey models we have developed.
O128
Barrow Neurological Institute, United States
There is a growing appreciation for the fact that Parkinson’s disease (PD) is not the result of the death of a single neuronal circuit, but rather, a multi-system failure of several circuits within the brain. It is likely that pathology, degeneration, and neuroplasticity alter connectivity across dopaminergic, noradrenergic, and serotonergic circuits, amongst others, to produce the composite of motor and non-motor symptoms that we recognize as PD. Along with this complexity comes the need for equally complex tools to model disease, either single symptoms or in congregate. Gene transfer tools such as viral vectors, often used in conjunction with specialized transgenic animals, have become an increasingly powerful tool to achieve this. For example, recombination-dependent vectors paired with the appropriate animal model allows for the precise manipulation of single or multiple circuits. Moreover, the combination of multiple recombination systems allows for the manipulation of specific neuronal projections. In addition, novel viral vectors have been engineered to facilitate improved retrograde transduction or trans-synaptic spread. To add, identification of non-coding sequences to direct genetic payloads to specific subcellular locations confers an added level of experimental precision. With this growing toolbox of gene transfer tools, researchers can 1) Readily interrogate the pre- and post-synaptic compartment using genetically encoded indicators such as GRAB-DA and calcium sensors. 2) Modulate neuronal activity using modalities such as DREADDs and channelrhodopsins. 3) Perform intricate mapping of single circuits, identify collaterals, and bilateral projections, and even map connectivity. 4) Direct the expression of pathology, such as that resulting from wildtype alpha-synuclein or its mutant forms, to specific cells and/or their afferents. Guided by the clinical picture of PD, many of these modalities can be combined to ask increasingly complex questions about the changing parkinsonian brain. In short, as our recognition of the complexity of the PD brain increases, so to should our ability to study such intricate disease mechanisms.
O131
National and Kapodistrian University of Athens, Greece
It is now well established that brain function arises from the concerted activity of a network comprising of neurons and glia. In neurodegenerative diseases, neuroinflammation and local immune system over-activation compromise this network ultimately leading to neuronal dysfunction and demise. In Parkinson’s Disease (PD), such immune dysfunction is believed to underlie many of the non-motor deficits such as sleep and gastrointestinal abnormalities, which in most cases, precede the onset of motor symptoms. In principle, neuroinflammation can act as a dynamic mechanism to eliminate the potential toxic insult; however, in pathological conditions, such as PD, the sustained inflammation becomes harmful and can ultimately aggravate neurodegeneration.
The main cells involved in neuroinflammation are microglia and astrocytes. As the resident macrophages of the CNS, microglia continuously survey neuronal tissue and are transformed into a pro-inflammatory activated state upon infection or injury. Astrocytes are responsible for preserving neuronal homeostasis by regulating synaptic transmission and providing structural, metabolic and nutrient support through the release of gliotransmitters. In addition, as part of the brain immune response, astrocytes can be activated by microglia by a process called reactive astrogliosis. Depending on the insult, reactive astrocytes can change their transcriptome, morphology and secretome to affect neuronal physiology beneficially or detrimentally.
Despite the intensive research on this field, the signaling pathways involved in microglia and astrocyte activation and the modulators (genes, miRNA, proteins, gliotransmitters, lipids) that regulate the communication between microglia, astrocytes and neurons under conditions of PD inflammation are just beginning to be elucidated at the cellular level. Transferring such knowledge to the circuit level will provide a solid understanding of the basic cellular mechanisms behind disease pathophysiology and facilitate the identification of potential therapeutic targets that (a) restore astrocyte-neuron communication and therefore facilitate the design of repair or compensatory strategies, (b) exacerbate inflammation and mediate neurotoxicity and could be selectively inhibited as a neuroprotective approach, and (c) facilitate the stratification of patients to allow personalized medical care.
O133
University of the Sunshine Coast, Australia
Parkinson’s Disease (PD) is a progressive neurological condition where the cumulative impact of complex motor and non-motor symptoms significantly impairs daily activities and quality of life. Traditional rehabilitation often addresses these symptoms in isolation—an impairment-focused approach that fails to manage their combined effect on an individual’s real-world functioning. A fundamental shift towards holistic, person-centred care is required. Research confirms that targeting client-specific goals yields superior outcomes, and people with PD consistently prioritise goals related to daily functioning in self-care, domestic tasks, and community life. Critically, studies reveal that the primary barriers to achieving these goals are often non-motor cognitive impairments, highlighting the profound impact of 'mental functions' on everyday performance.
To meet the complex needs of people with PD, interventions must move beyond symptom management to focus on participation and goal attainment. Occupation-based metacognitive strategy training (MST), including approaches like the Cognitive Orientation to Daily Occupational Performance (CO-OP) approach, offer a promising solution. CO-OP is a person-centred, problem-solving framework that empowers individuals to achieve their chosen functional goals. This individualised, home-based intervention has proven feasible and acceptable for people with PD, with preliminary evidence demonstrating improved goal performance, self-awareness, and management of daily life.
This round table discussion will explore how to translate these person-centred principles into clinical practice. We will debate the necessary shift in rehabilitation to prioritise client-identified goals and comprehensively address function-limiting non-motor symptoms like executive dysfunction, planning deficits, and apathy. Key topics include analysing the mechanisms of holistic interventions like CO-OP—particularly its ‘Goal-Plan-Do-Check’ strategy—in developing self-management skills. We will also examine practical implementation considerations, such as adapting therapy for the home environment, managing cognitive fatigue, determining optimal intervention intensity, and effectively involving care partners. Join us to discuss the future of person-centred rehabilitation for Parkinson's Disease.
O134
Indiana University School of Medicine, United States
Background Genetic testing is not considered standard of care for individuals with Parkinson’s Disease (PD); however, patient interest is growing. Earlier studies estimated that 5-10% of individuals have monogenic forms of PD; recent findings from large-scale research initiatives indicate that the prevalence of pathogenic variants among individuals with PD is closer to 13%. Individuals may pursue testing to gain insight into their condition, assess eligibility for clinical trials, and estimate PD risk for family members. Genetic counselors (GCs) play a key role in this process by helping individuals understand the medical, psychological and familial implications of genetic information.
Why involve a GC?
Ordering and interpreting genetic testing for PD is a complex process. Laboratories offer a range of testing options, and methodologies and reporting policies may vary. Interpretation of results adds another layer of complexity. Results can have personal and familial implications, affecting medical management as well as emotional, financial, and social aspects, which GCs are trained to address. Discussions with a GC empowers people to make thoughtful, informed decisions about their genetic testing.
How to access a GC?
Genetic counseling and testing for PD are available in clinical settings. GCs are often part of the multidisciplinary care team and provide both pre and post-test counseling. In addition to clinical care, GCs may also support research participants by facilitating the return of genetic results and helping them understand the implications of those findings. Individuals interested in meeting with a GC can consult the National Society of Genetic Counselors directory, which lists certified professionals across various specialties and service models, including in-person and telehealth options. However, certified GCs may not be available in all countries; in such cases, genetic counseling may be provided by other healthcare professionals with specialized genetics training.
Conclusion All individuals considering genetic testing should have the opportunity to make informed choices. This is particularly important because results may have implications not only for the patient but also for family members. GCs are uniquely equipped to interpret complex genetic information, provide context, and tailor education to each person’s needs, thereby making the testing process less daunting, and ultimately more meaningful.
O135
Northwestern University, United States
Proving that exercise protects the brain in Parkinson’s disease (PD) is difficult because animals do not naturally develop PD, so we lack a true preclinical model. This means we must rely on human studies to demonstrate neuroprotection.
PD symptoms appear when about 50–80% of dopamine-producing neurons in the substantia nigra pars compacta are lost. The goal of neuroprotective therapy is therefore to slow the death of these neurons and/or help the remaining ones maintain or increase dopamine production.
Current treatments, such as levodopa therapy or surgical interventions, improve symptoms by replacing dopamine or altering abnormal brain circuits. However, these treatments only work while they are being used. When treatment stops, the benefits disappear, and there is no evidence that they slow neuron loss or preserve dopamine production. Their effects are short-lived—lasting only hours.
To prove that an intervention, such as exercise, truly protects neurons or modifies disease progression, we need to show three things:
A consistent and clinically meaningful difference between an exercise group and a control group over a significant time period. Biological evidence of neuroprotection. A clear explanation of how exercise causes this protection.
For the first point, strong evidence now exists from four studies lasting six months or one year. These studies show that high-intensity aerobic exercise slows PD progression compared with controls, based on scores from the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (part III). I will discuss these four studies in detail at my presentation at the congress.
For the second point, biological measures that might indicate neuroprotection include a slower decline in the striatal specific binding ratio measured by DaTscan, other PET imaging markers, or fluid biomarkers such as Brain-Derived Neurotrophic Factor (BDNF). I will present 2 studies that have demonstrated changes in stratal specific binding potential that are consistent with neuroprotection.
The third point—explaining the mechanism of neuroprotection—is likely the most challenging. Options include increasing blood flow to the brain which declines as people age, as well changes to neurons within the basal ganglia.
O137
Canada
REM sleep behavior disorder (RBD) is caused by a loss of the system that normally keeps us paralyzed when we dream; as a result, persons with RBD can act out their dreams at night. RBD has a very strong link to Parkinson's disease, in two primary ways. First, in those who have PD already, it can mark a subtype of disease, generally characterized by a more 'diffuse' disease, with more non-motor features. Second, and of major future importance, it is the strongest known risk factor for Parkinson's. About 80% of those who have isolated/idiopathic RBD (that is, RBD without a diagnosis of Parkinson's disease or related disorders such as dementia with Lewy bodies) will eventually develop PD or DLB in the future, often a decade or more after the first symptoms of RBD develop. This has major implications for studying the earliest stages of Parkinson's, in order to understand how disease evolves. In the future, as neuroprotective therapies become available, it may also provide a way to intervene early, such that the full manifestations of Parkinson's could even be prevented completely. This round table will have an open discussion about the implications of RBD for people living with Parkinson's and for the future of Parkinson's disease therapeutics.
O138
Weill Cornell Medicine, United States
Parkinson's disease (PD) is the fastest growing neurodegenerative disorders affecting over 1 million people only in the US, and imposing an escalating social and economic burden as the population ages. Despite decades of research, one critical factor has been overlooked: how biological sex (whether related to genetics or hormonal factors) influences women lived experiences with PD diagnosis, treatment and quality of life. Emerging research and Dr. Marongiu’s own work point to reproductive hormones as powerful regulators of PD risk. Yet, the mechanisms linking sex, hormones, and disease progression remain poorly understood and are rarely considered in treatment development.
This 2-Oral Sessions will be an open conversation on most pressing topics such as: 1. Sex differences in PD motor and non-motor symptoms; 2. how genetic factors and reproductive hormones affect disease risk and progression, prevention and treatment strategies in women; 3. Possible role of the immune system; 4. Unmet needs of women with PD, etc…
O139
Ireland
In this Warring Table, we'll be reflecting on the Action Plan from the paper on Unmet Needs of Women Living with Parkinson's Disease: Gaps and Controversies https://pubmed.ncbi.nlm.nih.gov/35060180/ and what has been achieved and what has yet to happen. We look forward to input from people who are interested in this topic. Women with Parkinson’s are very much invited to take part in this discussion.

O140
Oregon Health & Science University, United States
How we walk, our “gait”, is a window into our overall health. In Parkinson’s disease (PD), small changes in walking often appear long before other symptoms become noticeable. Yet, traditional assessments done in clinics or laboratories only capture short snapshots of walking, which may not reflect how people move in their daily lives. Today, new digital tools such as wearable sensors, make it possible to measure walking continuously and naturally as people go about their day. These technologies can reveal subtle shifts in gait, turning and variability across the day or multiple days that might otherwise go unnoticed. Such subtle changes may improve early impairments in Parkinson’s, track how the condition progresses, and predict who might be at greater risk of falls.
This 2-Oral Sessions will discuss how real-world gait monitoring can improve care for people with Parkinson’s by bringing together clinicians, researchers, and technology experts. Together, we’ll explore how continuous movement data can support earlier diagnosis, more personalized treatment, and better safety at home, as well as the challenges of bringing these digital approaches into everyday healthcare.
3-Poster Presentations
BASIC SCIENCES: Etiology, genetics, epidemiology, and toxicants
P01.01
1 Royal Veterinary College, United Kingdom
Autosomal dominant mutations in LRRK2 are the most common genetic cause of Parkinson’s, however the LRRK2 gene is noteworthy for additional coding and non-coding risk associated with the disease risk. This includes the G2385R variant, found in East Asian populations, associated with an odds ratio of 2.69. In contrast to autosomal dominant mutations described to date, which reside exclusively within the enzymatic core of LRRK2, the G2385R variant is located in the carboxy terminus WD40 scaffolding domain. The precise biochemical mechanisms underlying the association of this variant with heightened disease risk are unclear. To assess the impact of the G2385R variant, we have carried out an exhaustive analysis of signalling pathways and cellular events linked to LRRK2 following expression of the G2385R variant in HEK293 cells. This has been achieved using phosphospecific immunoblot read outs for LRRK2 kinase activity, coupled with live cell imaging and validated LRRK2 stimulators including L-Leucyl-L-Leucine methyl ester (LLOME). Our results support a distinct mechanism of action for G2385R, with a reduced impact on enzymatic activity compared to mutations in the ROC-COR-Kinase core of LRRK2, and altered cellular localisation compared to other variants. The frequency of the G2385R variant, and distinct mechanism of action, highlight targeting the WD40 domain as an important unexploited opportunity for drug discovery modulating the activity of LRRK2. Further investigations into the structural basis for the association of G2385R with disease, coupled with
P01.02
1 Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije University Amsterdam, Amsterdam, The Netherlands., Netherlands
2 Department of Molecular and Cellular Neurobiology, Center for Neurogenomics and Cognitive Research, VU University Amsterdam, Amsterdam, The Netherlands., Netherlands
Objectives: The identification of disease mechanisms underlying Parkinson’s disease (PD) is complicated by the heterogeneous nature of the disease within brain tissue. Notably, both clinical and neuropathological descriptors, such as the alpha-synuclein (aSyn)-based Braak staging, poorly correlate with proteome changes in specific disease-affected regions. Quantifiable disease-associated molecular changes, such as aSyn accumulation and the loss of enzymatic activity of beta-glucocerebrosidase (GCase), are observed in the brains of patients. This study aims to identify proteome correlates of biochemically-quantified aSyn levels and total GCase activity in the human brain of GBA1-related and idiopathic PD patients.
Methods: We quantified serine129-phosphorylated (pSer129) aSyn, aa122-truncated aSyn (CTT122- aSyn), and Total aSyn using alphaLISA assays and measured total glucocerebrosidase activity in frozen human post-mortem brain samples from the gyrus temporalis medius (GTM, n=114) of patients with GBA1-related PD, idiopathic PD, incidental Lewy body disease (iLBD), and controls. In parallel, we conducted high-resolution shotgun proteomics (TIMS-TOF). Correlation analyses were performed between the quantified protein intensities and the biochemical measures of aSyn proteoforms and GCase activity.
Results: Initial analysis identified GTM proteomic alterations correlating with either an increase in Total and pSer129 aSyn proteoforms or with a decrease in GCase activity, or both. Proteomics alterations were involved in protein degradation and lipid metabolism pathways. Comparisons across PD, and iLBD samples showed progressive proteomic dysregulation and identified pathways linked to disease progression in the early stages of disease development.
Conclusions: These data provide new insights into the molecular underpinnings of PD, offering valuable information on the pathways involved in the early stages of disease progression and identifying new protein targets of interest associated with key molecular events in PD pathogenesis (aSyn accumulation and GCase dysfunction). This study empathizes the importance of biochemically-resolved proteomic analyses in understanding neurodegenerative mechanisms.
P01.03
1 McGill University, Canada
BACKGROUND Variants in the GBA1 gene, which cause Gaucher’s disease (GD) in biallelic forms, are also associated with increased Parkinson’s disease (PD) risk in heterozygous carriers. While carriers of GBA1 variants classified as severe or mild (causing GD type 1 or GD types 2 and 3, respectively) can enroll in clinical trials, carriers of variants classified as “unknown” are typically excluded.
OBJECTIVE We sought to evaluate the contribution of GBA1 variants with “unknown” GD classification to PD risk and to inform genetic stratification in clinical trials.
METHODS We systematically reviewed and meta-analyzed 34 published case–control studies, encompassing 24,060 PD patients and 14,465 controls, relying on the curated GBA1-PD Browser. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated from study-level data, with pooled estimates derived from random-effects models. Between-study heterogeneity was assessed by the I2 index. To refine interpretation, “unknown” variants were further stratified by the American College of Medical Genetics (ACMG) classification (pathogenic, likely pathogenic, variant of uncertain significance [VUS], likely benign, benign).
RESULTS Overall, 307 PD patients (1.28%) and 138 controls (0.95%) carried “unknown” variants. In aggregate, this group of 125 nonsynonymous variants was not significantly associated with PD (OR = 1.34, 95% CI: 0.93–1.93; I2 = 52.4%). However, stratification by ACMG revealed that variants categorized as VUS were significantly associated with PD (OR = 1.59, 95% CI: 1.25–2.02; I2 = 0%). When pathogenic, likely pathogenic, and VUS variants were pooled, the association persisted (OR = 1.63, 95% CI: 1.28–2.06; I2 = 0%).
CONCLUSIONS These results provide evidence-based guidance for expanding genetic eligibility criteria in GBA1-targeting trials, thereby improving recruitment and ensuring more representative inclusion of patients. GBA1 variants classified as “unknown” may be considered with caution for inclusion in PD clinical trials if they are also categorized by ACMG as VUS, likely pathogenic, or pathogenic.
P01.04
1 Clínica Santa María, Chile
Objective: To characterize the genetic architecture of Parkinson’s disease (PD) in a Chilean cohort.
Background The genetics of PD remains underexplored in South America, with only a few studies from Chile[1]. Limited resources reduce access to genetic testing and counseling, underscoring the need to characterize PD-associated genes to allow inclusion in precision medicine trials.
Methods We conducted a cross-sectional observational study at a referral center for movement disorders in Santiago, Chile. Patients meeting the UK Brain Bank criteria for PD were consecutively recruited. Demographic and clinical data were collected, and peripheral blood samples underwent DNA extraction. Genetic testing was performed using the NeuroBooster array[2] and/or next-generation sequencing. Patients were considered positive if they carried at least one pathogenic/likely pathogenic variant in autosomal dominant genes, or biallelic variants in autosomal recessive genes.
Results Among 461 patients (59.0% male; 30.0% early onset; 33.8% with family history), pathogenic or likely pathogenic variants were identified in 55 (11.93%). Positive family history was the only differentiating feature between positive and negative cases (50.9% vs. 31.5%, p = 0.007).The most frequent variant was LRRK2 p.G2019S, present in 6.29% of the cohort (52.7% of positive cases), followed by GBA1 variants in 4.99% (41.9% of positive cases), including p.N370S (34.8%), p.E326K (17.4%), p.L444P (13.0%), p.T369M (13.0%), p.R496H (13.0%), and one case with p.L(-11)Afs*18 and other with exon 10 deletion. One patient each carried variants in PRKN (homozygous deletion of exons 8-9), SNCA (duplication), and SQSTM1 (p.P308L), a gene linked to other neurodegenerative disorders but not typically associated with PD. No variants were identified in VPS35 or PINK1.
Conclusions This study represents the largest genetic characterization of PD in Chile. The very high prevalence of LRRK2 p.G2019S, the highest reported in South America, positions Chile as a compelling site for LRRK2–targeted clinical trials.
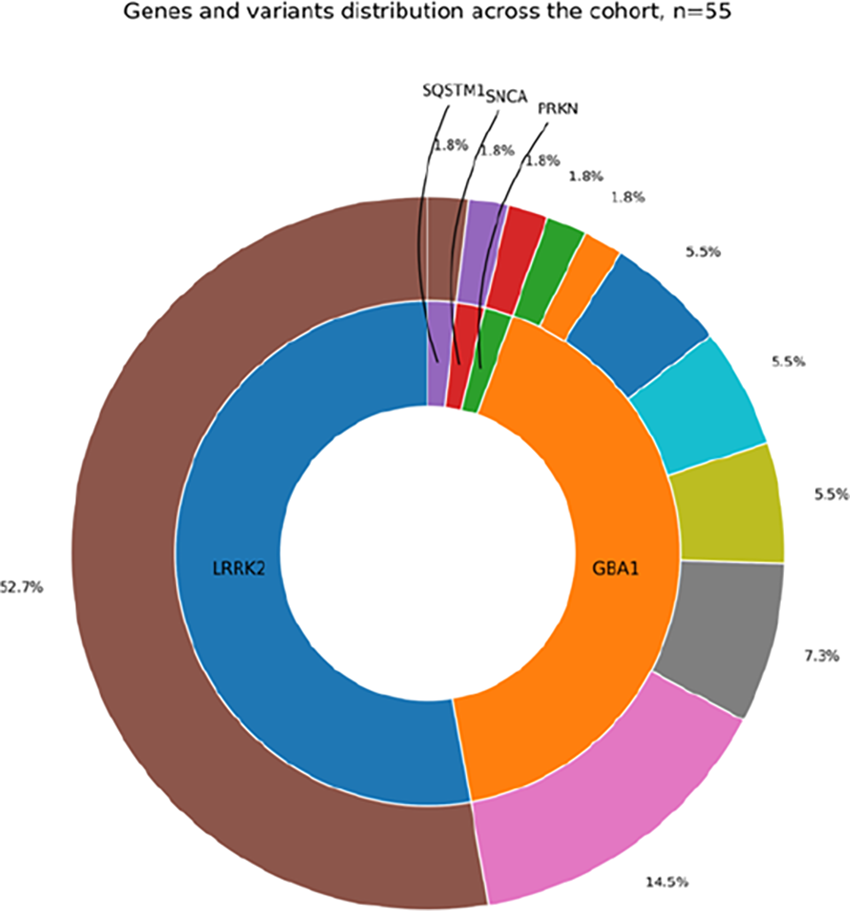
P01.05
1 Northeast Ohio Medical University, United States
Trichloroethylene (TCE) and related chlorinated solvents were widely used by the United States military for aircraft, equipment, and facility maintenance throughout the twentieth century. Decades of toxicologic and epidemiologic research link TCE exposure to mitochondrial dysfunction, oxidative stress, and selective dopaminergic neuron loss, the key pathological features of Parkinson’s disease (PD). Veterans constitute a uniquely exposed population because of solvent use in confined workspaces and persistent groundwater contamination surrounding many installations.
A narrative literature review (1980–2024) synthesized PubMed studies, Department of Defense environmental reports, and Freedom of Information Act (FOIA) data from confirmed contaminated sites such as Kelly Air Force Base. Search terms included Parkinson’s disease, trichloroethylene, solvents, veterans, and toxic exposure. Cohort and case control studies were evaluated for risk magnitude, latency, and policy relevance.
Epidemiologic analyses demonstrate up to a sixfold increase in PD risk among individuals with occupational or environmental TCE exposure (Goldman et al., Ann Neurol, 2022). The Department of Defense has documented solvent contamination at more than 1,300 facilities, with vapor intrusion and groundwater plumes persisting for decades after closure. Latency between exposure and symptom onset frequently exceeds 15 years, yet current Veterans Affairs (VA) policy restricts presumptive service connection for toxic exposures to a 10 year post discharge window. This policy fails to reflect the delayed neurodegenerative timeline observed in TCE associated PD.
TCE related PD is a preventable, service connected disease. Expanding the presumptive window, enhancing exposure mapping, and improving interagency coordination among the VA, DoD, and EPA are critical to identify and support affected veterans. Recognition of environmental PD within this population is both a scientific imperative and a moral obligation, ensuring that those who served are no longer harmed by invisible toxicants long after their active duty has ended.
P01.06
1 Icahn School of Medicine at Mount Sinai, United States
2 Radboud University Medical Center, Netherlands
Aim. α-Synucleinopathies, including Parkinson’s disease (PD) and dementia with Lewy bodies, are characterized by the selective loss of dopaminergic neurons in the substantia nigra (SN). We aimed to define disease-associated cell states across cell types in the SN and to assess their associations with PD polygenic risk.
Methods. We performed single-nucleus RNA-seq on 425,000 oligodendrocyte-depleted nuclei from 71 donors (40 with α-synucleinopathies and 31 controls; 81 samples across the SN, amygdala, and frontal cortex). Analysis then focused on the SN. Key findings were replicated in the publicly available AMP-PD snRNA-seq dataset (97 donors; 443 samples; five brain regions).
Results. Principal component analysis distinguished the SN from amygdala and frontal cortex, supporting SN-focused analyses. Within the SN, we resolved five neuronal, six astrocyte, eight microglial, five endothelial, and six pericyte clusters. Across cell types, we identified clusters enriched for proteostasis-related pathways, specifically the unfolded protein response (UPR) and autophagy, which showed increased abundance in PD. Differential gene expression and pathway enrichment analyses consistently identified UPR and autophagy as the top upregulated pathways across cell types, and these patterns were replicated in AMP-PD. Spectra factor analysis revealed multiple disease-associated gene programs. In astrocytes, factors enriched for glycolysis, lipid metabolism, and phagocytosis correlated with Braak Lewy body scores, while in microglia, mitochondrial UPR pathways were associated with Braak Lewy body stages. PD polygenic risk was enriched in dopaminergic neurons, microglia (heat shock protein/mitochondrial UPR subtypes), and astrocytes (Ca2+/junction subtypes).
Conclusions. We created a large atlas of oligodendrocyte-depleted nuclei from the substantia nigra in α-synucleinopathies. Analyses revealed convergent activation of proteostasis pathways across cell types, with astrocytes and microglia showing the strongest disease associations, while PD genetics highlighted cell-type–specific risk at both cluster and factor resolution.
P01.07
1 Université de Lille, INSERM, CHU Lille, U1172, Lille Neuroscience & Cognition (LilNCog), Lille, France, France
2 Service d'Anatomo-pathologie, Hôpital Saint Vincent de Paul, Lille, France, France
3 IMT Nord Europe, Institut Mines-Télécom, University Lille, Centre for Energy and Environment, Lille, France, France
Introduction: Parkinson’s disease (PD) arises from a complex etiology involving both genetic and environmental determinants. Increasing evidence highlights the contribution of the latter such as pesticides, air pollution and microplastics to PD risk. However, the underlying molecular mechanisms remain poorly understood. Among air pollutants, ultrafine particles (UFP; <0.1µm) represent a major concern due to their ability to cross the blood-brain barrier (BBB) and reach the brain. UFP exhibit a complex composition enriched in organic (e.g., metals) and inorganic chemicals (e.g., polycyclic aromatic hydrocarbons; PAH), making them potential inducers of ferroptosis and neurotoxicity. In this work, UFP biodistribution in the brain was investigated in vivo to further explore in vitro the molecular mechanisms involved in PD-related pathological processes.
Methods: Male Balb/cJRj mice (specific opportunistic pathogen free, 10 weeks, n=6/group) were exposed for 3 months by 2 intranasal instillations/week to 0, 10 or 30 μg of UFP/40 μl of sterile saline and sacrificed 24h after their last exposure. UFP biodistribution in the brain was assessed by transmission electron microscopy (TEM) and tissue metal profiling via inductively coupled plasma mass spectrometry, while the expression of genes involved in PAH metabolism (i.e., AhR, Cyp1a1, Cyp1b1) and metal homeostasis (i.e., Mt1–Mt4) was measured by RT-qPCR. Statistical differences were assessed using non-parametric Mann-Whitney U-test (p<0.05).
Results: TEM observations revealed small electron-dense particles within neuronal axons and cell bodies, confirming UFP penetration into the brain parenchyma. Accordingly, metal analysis showed elevated levels of Cu and Co in brain tissues, suggesting accumulation of UFP-associated metals despite the protection of BBB. Gene expression analysis showed strong AhR, Cyp1a1, Cyp1b1, Mt1, Mt3 and Mt4 upregulation, especially at the highest UFP dose, indicating activation of the AhR pathway and altered metal homeostasis.
Conclusion/perspectives: Overall, these results confirmed the presence of UFP and chemicals derived from them in exposed mice, suggesting that this exposure could contribute to neurotoxicity. In vitro experiments on differentiated human dopaminergic neurons (LUHMES) will now clarify the molecular mechanisms and type of cell death induced by UFP, which will enable the development of biomarkers and therapeutic strategies associated with prevention.
P01.08
1 Icahn School of Medicine at Mount Sinai, United States
Background. α-synucleinopathies, including Parkinson’s Disease (PD) and dementia with Lewy bodies (DLB), are characterized by α-synuclein-containing Lewy bodies and the selective loss of dopaminergic neurons in the substantia nigra. Using genotype information and single-cell transcriptomics we asked whether PD genetic variants modulate microglia states.
Methods. We sequenced 425,000 oligodendrocyte-depleted brain nuclei (53,000 myeloid nuclei) from 98 donors (109 samples; amygdala, substantia nigra, cortex) and an additional 134,000 fresh myeloid cells from 21 donors (36 samples; substantia nigra, cortex). For replication, we leveraged the AMP-PD dataset which contained 130,000 myeloid nuclei from 97 donors (443 samples; five brain regions).
Results. We identified eight distinct brain-resident myeloid cell states, including phagocytic and sensome (P2RY12-high), unfolded protein response (UPR; HSP90AA1-high), and perivascular (CD163-high). In α-synucleinopathy brains, P2RY12-high microglia were depleted (logFC ≈ -0.21), while HSP90AA1-high microglia expanded (logFC ≈ 0.57). These shifts were accentuated in Braak LB late-stage cases and consistently replicated across cohorts (in-house nuclei, in-house cells, AMP-PD). Pseudobulk differential gene expression analysis pinpointed that HSP90AA1-high microglia upregulate glycolytic and lipid metabolic pathways while downregulating lysosomal, endoplasmic reticulum homeostasis, and phagocytic functions. Next, we tested state- and pathway-level enrichment for polygenic disease risk. We found that HSP90AA1-high microglia and the mitochondrial UPR pathway were significantly associated with PD GWAS (GP2) risk gene expression. Our previous work identified that the microglia-specific eQTL rs3732765-A reduces P2RY12 expression and is protective against PD. Donors with rs3732765-A displayed an expansion of P2RY12-high (logFC ≈ 0.34) and depletion of HSP90AA1-high microglia (logFC ≈ -0.21), while UPR transcription was suppressed.
Conclusions. Our findings reveal genetic regulation of microglial state dynamics in α-synucleinopathy brains. PD polygenic risk is linked to microglial dysregulation while protective alleles constrain maladaptive reprogramming. These findings nominate microglial stress programs as genetically validated, disease-relevant therapeutic targets.
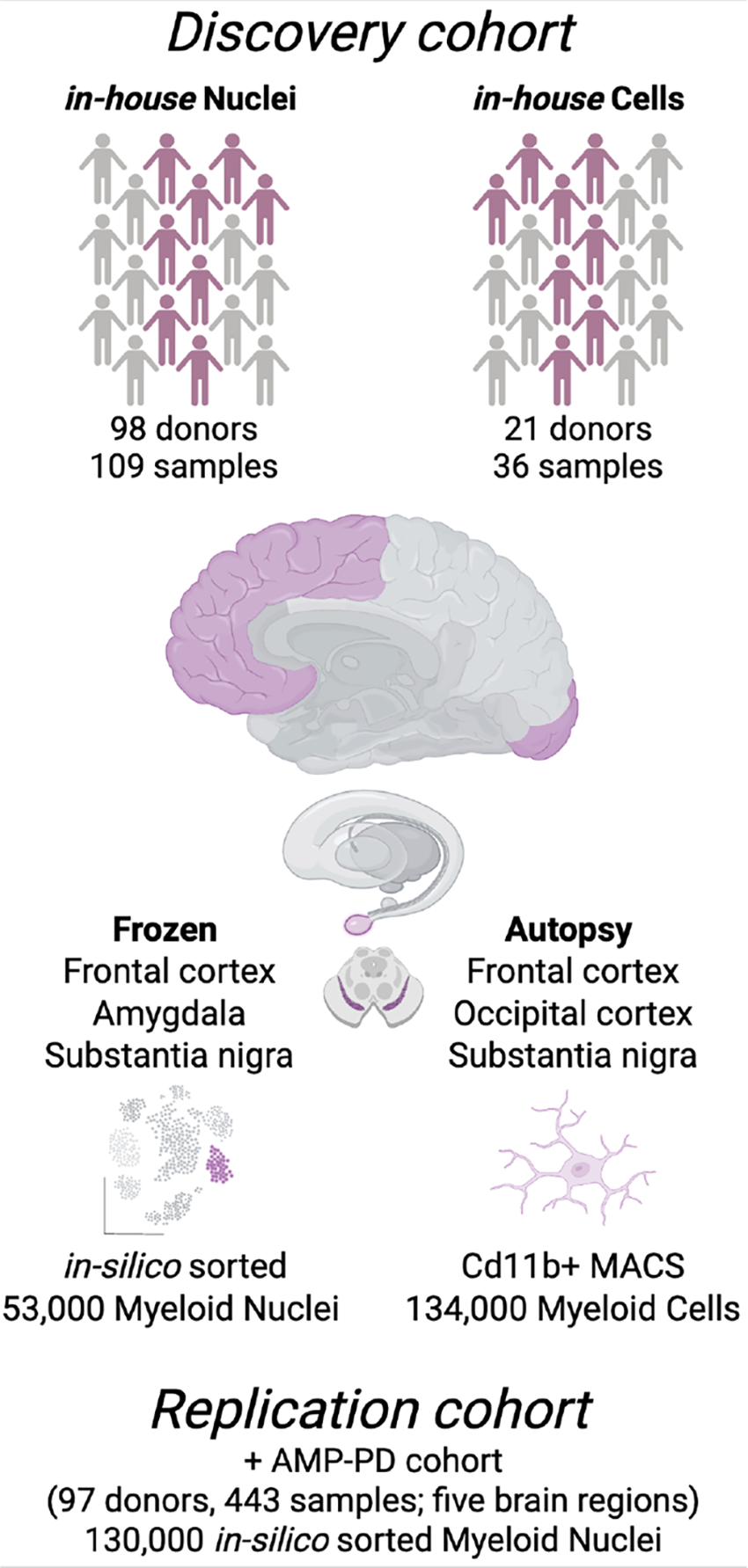
P01.09
1 Indiana University, United States
2 University of Florida, United States
3 Stanford University, United States
Introduction: Emerging evidence suggests that gut health and intestinal inflammation contribute to both the onset and progression of Parkinson’s disease (PD). Patients with inflammatory bowel disease (IBD) have an increased chance of developing PD, and treatment of IBD symptoms appears to be protective. Several genetic risk factors are also shared between IBD and PD, including variants in LRRK2. The LRRK2 R1441C mutation, one of the most common in familial PD, is associated with lysosomal dysfunction and chronic inflammation. Because peripheral inflammation can exacerbate neurodegeneration, particularly in the dopaminergic neurons of the substantia nigra, we sought to determine how intestinal inflammation interacts with LRRK2 genotype, aging, and sex to influence neurodegenerative outcomes.
Methods: Acute intestinal inflammation was induced using dextran sodium sulfate (DSS) in middle-aged and aged wild-type and LRRK2 R1441C mice. Flow cytometry and MSD to assess peripheral inflammation and characterize brain-associated immune cells. Dopaminergic neuron loss was evaluated by staining for TH+ cells in the substantia nigra. This design enables a systematic comparison of how age, sex, LRRK2 mutation, and intestinal inflammatory status influence neuroinflammatory and neurodegenerative processes. Additionally, we evaluated the therapeutic potential of a soluble TNFa inhibitor (xPro1595) in mitigating peripheral inflammation, with the goal of reducing neuroinflammation and neurodegeneration. xPro was administered during the DSS administration to reduce overall exposure to peripheral inflammation.
Results: Preliminary findings suggest that the LRRK2 R1441C mutation amplifies inflammatory responses in both the periphery and the brain. Treatment with xPro1595 reduced chronic inflammation and appeared to protect against select markers of neurodegeneration.
Conclusions: These studies highlight the interplay between genetic susceptibility, aging, and peripheral inflammation in modulating PD risk. They further support the potential of targeted anti-inflammatory interventions as neuroprotective strategies in genetically or immunologically high-risk populations.
P01.10
1 Queensland University of Technology, Australia
2 EpicentRx, United States
3 Stanford University, United States
Parkinson’s Disease (PD) is increasingly recognized as one of the most prevalent and disabling neurological conditions worldwide. Emerging evidence points to environmental and occupational exposure to neurotoxic agents, including pesticides such as paraquat and rotenone, as risk factors in PD development. Current treatments are symptomatic, leaving the underlying disease mechanisms unaltered, which highlights the pressing need for effective neuroprotective therapies. Our current study, supported by the grant funded by the Congressionally Directed Medical Research Programs (CDMRP) of the U.S. Department of Defense, focuses on evaluating the neuroprotective efficacy of RRx-001 (Nibrozetone). This small molecule exhibits dual functionality as an NLRP3 inflammasome inhibitor and NRF2 pathway activator, both of which are associated with enhanced cellular defense and reduced neuroinflammation. In in vitro models using dopaminergic N27 cells, LUHMES neurons, THP-1 macrophages, and microglial cultures, RRx-001 has demonstrated substantial protection against paraquat-induced neurotoxicity. Observed benefits include reduced neuronal death, improved mitochondrial function, and suppressed inflammasome activation, as measured by caspase-3/7 activity, MitoSOX fluorescence, IL-1β ELISA, and qPCR analysis of mitochondrial markers. We are now progressing to in vivo rodent studies to assess the compound’s ability to mitigate behavioural impairments and neuropathological features characteristic of paraquat-induced PD-like neurodegeneration. If validated through translational research, RRx-001 holds promise as a disease-modifying agent with both preventive and therapeutic potential for PD and other neurodegenerative diseases.
P01.11
1 Queensland University of Technology, Australia
2 EpicentRx, United States
3 Stanford University, United States
Parkinson’s Disease (PD) is one of the fastest-growing neurological disorders and a leading cause of disability worldwide. Increasing evidence implicates environmental and occupational chemical exposures—particularly metals such as manganese and vanadium as significant contributors to PD pathogenesis. Current therapies primarily target symptoms rather than underlying disease mechanisms, highlighting the urgent need for neuroprotective interventions. Funded by the Congressionally Directed Medical Research Programs (CDMRP) of the U.S. Department of Defense, our study investigates the neuroprotective potential of RRx-001 (Nibrozetone), a small molecule with dual activity as an NLRP3 inflammasome antagonist and NRF2 pathway activator. These mechanisms are known to promote cellular resilience and attenuate neuroinflammation. Current in vitro studies using dopaminergic neuronal N27 cells, LUHMES neurons, THP-1 macrophages, and microglial cultures, RRx-001 demonstrated significant protection against MnCl2-induced neurotoxicity, including neuronal loss, mitochondrial dysfunction, and inflammasome activation as measured by caspase-3/7 activity, MitoSOX fluorescence, IL-1β ELISA, and qPCR for mitochondrial markers. We are now extending this work to rodent models, assessing the efficacy of RRx-001 in mitigating behavioural and neuropathological phenotypes associated with manganese induced PD like neurodegeneration. If validated through translational research, RRx-001 could represent a disease-modifying therapeutic strategy with both prophylactic and interventional potential for PD and related neurodegenerative conditions.
P01.12
1 McGill university and Douglas Research Center, Canada
2 Douglas Research Center, Canada
3 Banner Sun Health Research Institute, United States
4 Mayo clinic, United States
5 Barrow Neurological Institute, United States
The amygdala is a particularly susceptible region that accumulates a-synuclein pathology in Parkinson’s disease (PD). It has an important role in the processing of emotion and have been related to the pathophysiology of depression and neuropsychiatric symptoms. It is closely connected to the olfactory bulb and involved in olfactory processing as well. We aimed assess gene expression changes, affected pathways and co-expression networks by transcriptomic profiling of the amygdala in subjects with and without clinicopathologically defined PD and associate these changes with measures of olfactory function, depression and neuropsychiatric burden.
We performed bulk RNA sequencing on frozen human amygdala of 20 PD and 20 controls without dementia or any other neurodegenerative disorder, from the Arizona Study of Aging and Neurodegenerative Disorders and it’s Brain and Body Donation Program.
Results from differential expression analysis, corrected for age, sex and post-mortem interval revealed 40 significantly differentially expressed genes (DEGs) in PD. Downregulated genes were mainly related to altered hemoglobin expression while upregulated genes included inflammatory markers and glutamine transporter. Significantly enriched pathways were involved in oxygen and carbon dioxide transport, cellular oxidant detoxification and regulation of glutamine secretion. Co-expression network analysis using Weighted correlation network analysis (WGCNA) subsequently identified significant modules associated with (1) olfactory dysfunction that were involved in neuroinflammation, neuronal death and lysosomal transport, with (2) depression that were involved in extracellular matrix organization and neuroinflammation and with (3) neuropsychiatric symptoms involved in mitochondrial dysfunction and calcium signaling pathways
In conclusion, these results suggest cellular alterations in the amygdala related to mitochondrial dysfunction, altered oxygen homeostasis, oxidative stress, inflammation as well as glutamatergic neurotransmitter dysfunction that may contribute to neurodegeneration in PD.
P01.13
1 France
Background: Parkinson’s disease (PD) is characterized by postural, autonomic, and cognitive disturbances. Previous research has demonstrated a significant cross-correlation between temporomandibular disorders (TMD) and PD, and has identified jaw deviation—defined as a discrepancy between centric relation and centric occlusion—as a major risk factor for TMD. Additionally, masticatory deficiency has been shown to impair cognitive function via hyperactivation of the hypothalamic–pituitary–adrenal (HPA) axis. A bidirectional relationship between jaw position and body posture has also been reported.
Objective: We hypothesize that a substantial proportion of Parkinsonism and PD cases may be associated with excessive mandibular deviation.
Methods: To test this hypothesis, we assessed jaw deviation at the dental occlusion level using 459 MRI scans obtained from the PPMI database (June 8, 2025), including 293 scans from PD patients and 166 from non-PD controls. Jaw deviation was quantified by comparing coronal and axial angular discrepancies between the maxilla and mandible, using a threshold calibrated from the first 36 samples.
Results: Twenty-two cases were excluded due to insufficient visibility of the maxilla or mandible. The diagnostic test yielded a sensitivity of 87.8% (95% CI: ±6.4%) and a specificity of 73.5% (95% CI: ±8.6%) for predicting PD based on jaw deviation.
Conclusion: These preliminary findings suggest that jaw deviation may represent a potential risk factor for chronic conditions such as Parkinson’s disease. Identifying occlusal and postural dysfunctions at early stages of Parkinson’s may facilitate targeted therapeutic strategies and improve patient outcomes. Splint therapy could be considered for PD patients presenting with significant jaw deviation.
Keywords: Parkinson’s disease, Parkinsonism, Jaw deviation, Dysautonomia, Cognitive decline, PPMI
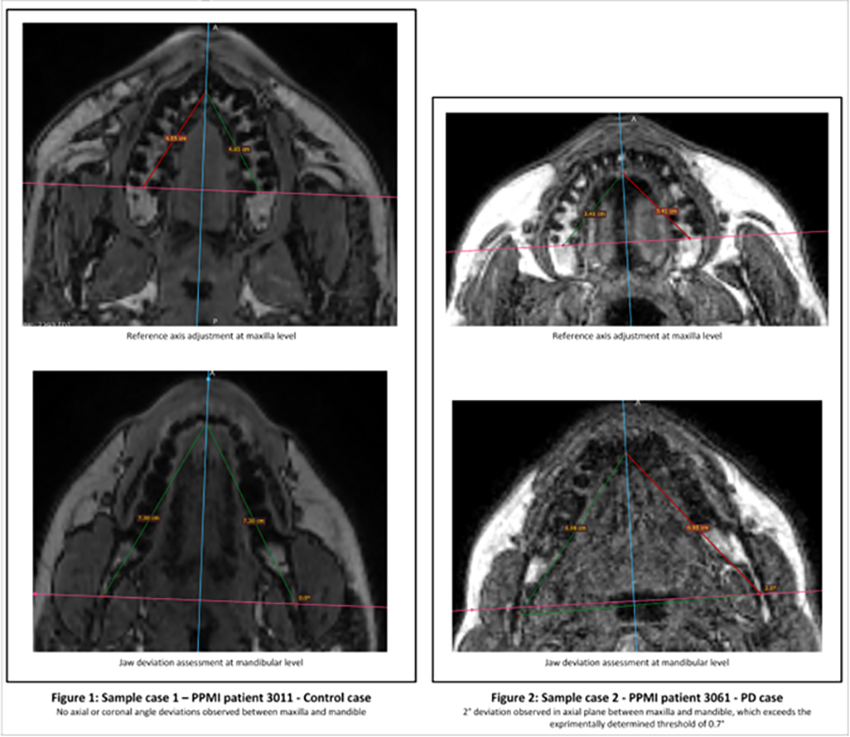
P01.14
1 Cooper University Hospital, United States
OBJECTIVE: To evaluate the bidirectional association between Graves’ disease (GD) and Parkinson’s disease (PD) using data from population-based studies. BACKGROUND: Emerging evidence suggests autoimmune thyroid disorders may influence neurodegenerative processes. Graves’ disease, characterized by hyperthyroidism and autoimmunity, could share pathogenic mechanisms with PD, including immune dysregulation and oxidative stress. However, the strength and direction of this association remain unclear. DESIGN/METHODS: A systematic review was conducted using PubMed to identify observational studies assessing the relationship between GD and PD. Studies reporting incidence or prevalence of GD in PD patients or PD in GD patients were included. Data were pooled using Mantel–Haenszel odds ratios (OR) under fixed and random-effects models. Heterogeneity was assessed with I2 and Cochran’s Q. Publication bias was evaluated using fail-safe N methods. RESULTS: Three studies met inclusion criteria (Rugbjerg et al., 2009; Li et al., 2012; Cho et al., 2022), encompassing 392,280 participants and 1,398 events. For PD→GD (two studies), the fixed-effect pooled OR was 2.51 (95% CI: 2.28–2.75; p < 0.0001), indicating a significantly increased risk of GD among PD patients. Random-effects analysis showed OR 3.38 (95% CI: –3.72 to 10.49; p = 0.35) with low heterogeneity (I2 = 1%). For GD→PD (one study), the OR was 1.37 (95% CI: 1.21–1.56; p < 0.0001). Fail-safe N analyses suggested robustness against publication bias.
CONCLUSIONS: Our findings support a bidirectional association between GD and PD, with PD patients exhibiting a higher risk of GD and GD patients showing a modestly increased risk of PD. Shared autoimmune and neuroinflammatory pathways may underlie this link. Further longitudinal studies are warranted to clarify causality and mechanisms.
P01.15
1 Cooper University Hospital, United States
OBJECTIVE: To evaluate whether systemic lupus erythematosus (SLE) is associated with an altered risk of Parkinson’s disease (PD) using evidence from population-based studies. BACKGROUND: Autoimmune mechanisms have been implicated in neurodegenerative disorders, but the relationship between SLE and PD remains unclear. Previous studies report conflicting results, warranting a systematic synthesis of available data. DESIGN/METHODS: A meta-analysis was conducted following PRISMA guidelines. PubMed was searched for observational studies assessing the bidirectional association between SLE and PD. Data extracted included events and sample sizes for exposed (SLE) and control groups. Odds ratios (ORs) were pooled using Mantel–Haenszel methods under fixed and random-effects models. Heterogeneity was assessed with I2 and Cochran’s Q. Publication bias was evaluated using Egger’s test and trim-and-fill analysis. RESULTS: Five studies met inclusion criteria. For SLE→PD, the fixed-effect model showed a significant association (OR = 0.78; 95% CI: 0.64–0.94; p = 0.01), suggesting a lower risk of PD among SLE patients. The random-effects model yielded a non-significant estimate (OR = 2.24; 95% CI: 0.71–6.99; p = 0.17) with low heterogeneity (I2 = 1%). For PD→SLE, the fixed-effect model did not show association (OR = 1.24; 95% CI: 0.79–1.93). Trim-and-fill analysis indicated potential publication bias, with two missing studies and a substantial change in effect size (>150%). Fail-safe N calculations suggested susceptibility to bias.
CONCLUSIONS: Current evidence does not support a robust association between SLE and PD. While fixed-effect analysis suggests a protective trend, random-effects and bias assessments highlight uncertainty. Larger, well-controlled studies are needed to clarify this relationship.
P01.16
1 Queen Mary University, United Kingdom
2 Northwestern University Chicago, United States
3 Universidad de Malaya, Malaysia
4 University of Malaya, Malaysia
5 UCL Institute of Neurology, United Kingdom
6 Baylor College of Medicine, United States
7 German Center for Neurodegenerative Diseases, Switzerland
8 German Center for Neurodegenerative Diseases, Germany
9 National Institute on Aging, United States
10 Global Parkinson's Genetics Program, United States
11 Institute of Neurogenetics Lübeck, Germany
12 Queen mary University, United Kingdom
13 Global Parkinson's Genetics Program, Spain
Objectives: Disruption of the lysosome-autophagy pathway and dysregulation of α-synuclein are recognised features of Parkinson’s disease (PD). EPG5 bi-allelic loss-of-function variants have been shown to cause Vici Syndrome, a congenital disorder of autophagy. Recent evidence suggests mutations in this gene could also cause adult movement disorders. Our aim was to investigate its role in PD aetiology.
Methods: Data was obtained from GP2 release 8, release 10 and UK Biobank. We used burden tests and linear regression models to test associations with PD compared to controls. Burden tests were run for different mean allele frequencies (MAFs) and variant types. Regression models only included variants with MAF ≤ 0.01 and were adjusted for age, sex and principal components. Variant extraction was performed to identify rare variants in homozygous or compound heterozygous (CH) cases. Individuals identified via variant extraction were further studied to classify the clinical presentation, patterns of inheritance and exclude alternative genetic risk factors.
Results: In 5,690 GP2 PD samples, we identified 8 potential CH cases carrying a total of 13 variants, of which 11 were missense and 2 were stop-gain. 3 of these individuals met the criteria of early onset PD (≤50yrs) without genetic evidence of autosomal dominant family history. Variant phase analysis confirmed compound heterozygosity in 2 of them. The phenotype was a rapidly progressive PD with dystonia. Our complex analysis did not yield any significant results.
Conclusion: We are currently screening the remaining individuals and conducting proof-of-concept studies in vitro using fibroblast cultures. Nonetheless, our preliminary findings confirm a link between EPG5 gene mutations and PD aetiology. Further classifications of the identified individuals are necessary to better characterise this association.
P01.17
1 Department of Neurology, Movement Disorders and Neuromodulation Center, Weill Institute for Neurosciences, University of California San Francisco, United States
2 Neuroscience Institute, The Queen’s Medical Center, and University of Hawaii at Manoa, John A Burns School of Medicine, Honolulu, HI, United States
3 Department of Neurology, Movement Disorders and Neuromodulation Center, Weill Institute for Neurosciences, University of California, San Francisco, United States
4 Department of Neurology, Movement Disorders & Neuromodulation Center, Weill Institute for Neurosciences, University of California San Francisco, United States
5 Division of Occupational and Environmental Medicine, University of California San Francisco, San Francisco Veterans Affairs Health Care System, United States
6 Pacific Health Research and Education Institute, VA Pacific Islands Health Care System, United States
Background Environmental exposures and lifestyle behaviors may be important contributors to risk or progression in people with PD. Interviewer-based methods for collecting this information exist, but these methods are resource intensive and limit scalability. A self-report method would increase efficiency and expand accessibility for collecting information about environmental exposures.
Methods The NINDS Common Data Elements recommend a number of lifestyle and environmental assessments for collection by interviewers (Grinnon et al., 2012). A short version, termed the Mini Environmental Risk Factor Questionnaire for Parkinson's Disease (MERQ-PD) was developed as part of the NINDS-supported Parkinson's Data Organizing Committee. Derived from these interviewer-based assessments, we have developed a modified short self-reported version (mMERQ-PD) that can serve as an initial screening tool for environmental exposures, providing a first-stage high-level assessment, to guide more detailed data collection when indicated.
Results Testing of a self-report version of this instrument is in progress. Initial populations will be English- and Spanish-speaking U.S. residents of various ethnicities, including Native Hawaiians. Expansion to other countries and development of culturally appropriate translations in multiple languages are planned. Formatting of responses will be standardized across versions to facilitate seamless data pooling across studies.
Conclusions Self-reported data collection is a valuable complement to more resource intensive interviewer based data collection. This approach has potential to increase participant access to clinical research and reduce burden in large-scale studies. Results of our ongoing work and recommendations for implementation will be presented.
References:
Grinnon ST, Miller K, Marler JR, Lu Y, Stout A, Odenkirchen J, Kunitz S. National Institute of Neurological Disorders and Stroke Common Data Element Project - approach and methods. Clin Trials. 2012 Jun;9(3):322-9. doi: 10.1177/1740774512438980. Epub 2012 Feb 27. PMID: 22371630; PMCID: PMC3513359.
P01.18
1 Indiana University School of Medicine, Indiana, USA, United States
2 Parkinson’s Foundation, Florida, USA, United States
3 Genomic Medicine Institute, Cleveland Clinic, Ohio, USA, United States
The PD GENEration (PDGENE) study provides CLIA-certified genetic testing and counseling to individuals living with Parkinson’s disease (PD). To enhance diversity in PD genetic research, the study expanded to Latin America through a collaboration with the Latin American Research Consortium on the GEnetics of Parkinson’s Disease (LARGE-PD). As part of the expansion, a study-specific training was developed to support providers in the genetic counseling process.
Providers participating in the training completed either a pre-recorded video or a live-mock session of a structured genetic counseling results disclosure. Some disclosed negative results while others disclosed a positive compound heterozygous PRKN variants with a heterozygous GBA1 variant. A structured checklist, outlining core competencies, key topics, and communication skills was provided in advance. Each participant was evaluated using the same framework and received written individualized feedback. Participants that failed were given the opportunity to send another video or to do a live session. Evaluations were thematically analyzed to identify recurring areas of strength and weakness.
A total of 46 completed evaluations, from two training cycles, were analyzed. Areas of weakness were seen across all competencies at least once. With weaknesses being seen in important genetic counseling concepts like understanding of genetics/genetic terminology, familial risks, session organization, and study protocol understanding. In contrast, areas of strength were seen in all competencies at least once. Participants demonstrated strengths in the following relevant areas like use of visual aids, PD-related information, pace of session/space for questions, and phenotype/genotype correlations. In total, 14 providers needed to do a remediation video, nine completed the remediation, seven did so successfully and two did not.
These findings highlight the important need of targeted genetic counseling training for providers that return genetic testing results. Providers that needed remediation of the first video, were more likely to succeed with a second video after detailed feedback, suggesting that structured, iterative training programs can be an effective means of standardizing and strengthening genetic counseling. Continued capacity-building efforts are essential to ensure equitable and high-quality return of genetic results in large-scale international studies.
P01.19
1 Weill Cornell Medical College, United States
2 Weill Cornell Medical College, Neurosurgery Department, New York, NY., United States
3 University of California San Diego, Department of Neuroscience and Pathology, San Diego, CA, United States
4 Weill Cornell Medical College, Neurosurgery Department, New York, NY; Weill Cornell Medical College, Genetic Medicine Department, New York, NY; Weill Cornell Medical College, Feil Family Brain and Mind Institute, New York, NY, United States
Introduction: Parkinson’s Disease (PD) exhibits sex differences in prevalence, clinical features, and disease progression, yet the mechanisms underlying these differences remain unclear.
Methods: Using longitudinal data from the Parkinson’s Progression Markers Initiative (PPMI), this study aims to further characterize sex differences in PD progression and to explore the immunologic and epigenetic factors that may drive them. Clinical symptoms and immune cell counts were trended from baseline to Year 3 for female and male individuals with and without PD. Sex differences in disease progression were evaluated using independent two-sample t-tests on changes in scores between baseline and Year 3 and pairwise comparison of slopes for the four cohorts from baseline to Year 3. Differentially methylated positions (DMPs) and genes (DMGs) from whole plasma samples were identified across four sex- and diagnosis-based comparisons. DMGs were further analyzed for pathway enrichment, chromosomal distribution, and overlap with genes previously reported as dysregulated in PD.
Results: Longitudinal analysis revealed dynamic sex-specific patterns across clinical, cognitive, and immune measures in PD. Early differences, such as higher UPDRS Part I scores in women (p = 0.03), resolved by Year 3, while new disparities emerged, including lower MoCA scores in men (p = 0.02). Immune profiles also shifted: sex differences in CD8+ T cells (p = 0.02, p = 0.01), B cells (p < 0.001, p < 0.001), and monocytes (p < 0.001, p = 0.002) persisted across time points, whereas an initial NK cell difference in PD (p < 0.001) resolved by Year 3. Pairwise comparison of slopes revealed significant sex differences in progression for fatigue and NK cell counts. A total of 304 genes and 634 positions showed significant epigenetic differences (adjusted p < 0.05) between men and women with PD.
Conclusion: These findings demonstrate that sex differences in PD clinical features are dynamic, underscoring the importance of incorporating longitudinal and sex-specific perspectives when studying the disease. They also suggest that immune factors and epigenetic changes may play a key role in driving these differences. Ongoing analysis will further investigate how methylation changes relate to clinical and immune trajectories in PD, and their potential use as biomarkers.
P01.20
1 Cooper University Hospital, United States
OBJECTIVE: To evaluate whether metformin use is associated with altered risk of Parkinson’s disease compared to other antidiabetic treatments. BACKGROUND: Emerging evidence suggests that type 2 diabetes mellitus may influence neurodegenerative processes, including Parkinson’s disease (PD). Metformin, a widely used antidiabetic drug, has been hypothesized to exert neuroprotective effects. However, comparative risk estimates across different glucose-lowering agents remain unclear. DESIGN/METHODS: A systematic review and meta-analysis was conducted using PubMed-indexed observational studies comparing PD incidence among patients treated with metformin versus alternative antidiabetic therapies. Six studies (2012–2025) were included, encompassing over 500,000 participants. Risk ratios (RR) were pooled using a random-effects model (DerSimonian-Laird) with Mantel-Haenszel weighting. Subgroup analyses were performed by comparator drug class. Heterogeneity was assessed using I2 and Cochran’s Q. Publication bias was evaluated via Egger’s test and trim-and-fill method. RESULTS: The overall pooled random-effects estimate showed no significant association between metformin use and PD risk (RR = −0.30; 95% CI: −1.08 to 0.47; p = 0.44), with substantial heterogeneity (Q = 284.07, p < 0.001). Subgroup analyses revealed reduced PD risk for metformin versus insulin (RR = −1.68; 95% CI: −2.32 to −1.05) and versus no-metformin (RR = −0.89; 95% CI: −1.18 to −0.59), but increased risk compared to SGLT2 inhibitors (RR = 1.17; 95% CI: 1.02 to 1.31). Trim-and-fill analysis suggested potential publication bias, with three missing studies and an adjusted effect estimate shifting toward null.
CONCLUSIONS: Metformin may confer differential PD risk depending on comparator therapy, with possible protective effects versus insulin and no-metformin, but higher risk compared to SGLT2 inhibitors. High heterogeneity and evidence of publication bias warrant cautious interpretation. Further prospective studies are needed to clarify metformin’s neuroprotective potential.
P01.21
1 Cleveland Clinic, United States
2 Hospital Sanatorio de la Trinidad Mitre, United States
3 Hospital Ophir Loyola, Brazil
4 Hospital e Maternidade Celso Pierro (HMCP) da Sociedade Campineira de Educação e Instrução, Brazil
5 Universidad Nacional de Colombia, Colombia
6 Fundacion Valle del Lili, Colombia
7 Centro de Transtornos del Movimiento (CETRAM), Chile
8 Universidad de Antioquia, Colombia
9 Universidad andres Bello, El Salvador
10 Hospital Interzonal General de Agudos San Martin de La Plata, Argentina
11 Hospital Universitário Walter Cantídio/Universidade Federal do Ceará, Brazil
12 Instituto Nacional de Neurología y Neurocirugía, Mexico
13 TECNOLOGICO DE MONTERREY TecSalud, Mexico
14 Hospital de Clínicas de Porto Alegre da Universidade Federal do Rio Grande do Sul, Brazil
15 Instituto Nacional de Ciencias Neurológicas, Peru
16 University of Puerto Rico, Puerto Rico
17 Hospital Ramos Mejia, Argentina
18 Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da USP *, Brazil
19 Universidad Federal de São Paulo - UNIFESP/EPM, Brazil
20 Hospital Angel C. Padilla, Argentina
21 Universidad de Chile, Chile
22 Universidad Nacional Autonoma de Mexico, Mexico
Background: Age at onset (AAO) of Parkinson’s Disease (PD) is a complex trait and the understanding of its genetic drivers remains limited. This gap is larger in underrepresented populations, where studies are constrained by sample size and genetic heterogeneity. We therefore performed a meta-analysis of ancestry-aware genome-wide association studies (GWAS) in Latino individuals with PD.
Methods: Our analysis accounted for the three-way admixture of Latinos using a previously described GWAS pipeline (Leal et al., 2025). A total of 3,138 patients from phase 1 and phase 2 of the Latin American Research consortium on the GEnetics of Parkinson’s Disease (LARGE-PD) were included. AAO was modeled as a function of imputed genotype dosages, sex and the first ten genetic principal components. Linear regression was implemented by SAIGE and TRACTOR to account for cryptic relatedness and local ancestry respectively. Random and fixed effects meta-analyses of phase 1 and phase 2 GWASs were performed with GWAMA. Post meta-GWAS analyses used FUMA.
Results: The SAIGE meta-analysis (n=3138) identified a genome-wide significant signal in chromosome 6. A well imputed (MAF=0.3%, INFO R2>0.98) intronic variant in PRKN was identified (rs537244270-T, β = −0.87 (SE = 0.15), P = 4.0×10−8; CADD-Phred = 6.24). Previous works found association of another intronic PRKN variant (rs9356013-A, MAF=7%), showing the relevance of this gene (Bandres-Ciga et al., 2019). Nonetheless, they are ∼272Kb away and completely independent from each other (r2=0). Conversely, TRACTOR meta-analysis (n=2922) split by African, European, and Native American ancestral backgrounds, did not reveal any significant variant associations. And only Multi-marker Analysis of GenoMic Annotation through FUMA yielded significant results for pathway enrichment in African ancestry.
Conclusions: We identify a novel candidate PRKN variant associated with AAO in Latino PD patients. This signal aligns with PRKN’s role in early-onset PD and provides genetic insights about the overall earlier mean AAO observed in LARGE-PD (54.5 ± 13.4 years). Follow-up studies are encouraged to gather further evidence in this regard. Finally, it is worth noting that AAO characterization is susceptible to recall bias and motor-onset definitions. Statistical power for localization of specific risk loci to partitioned ancestries is still limited; fostering an even representation of diverse ancestral backgrounds in upcoming research initiatives.
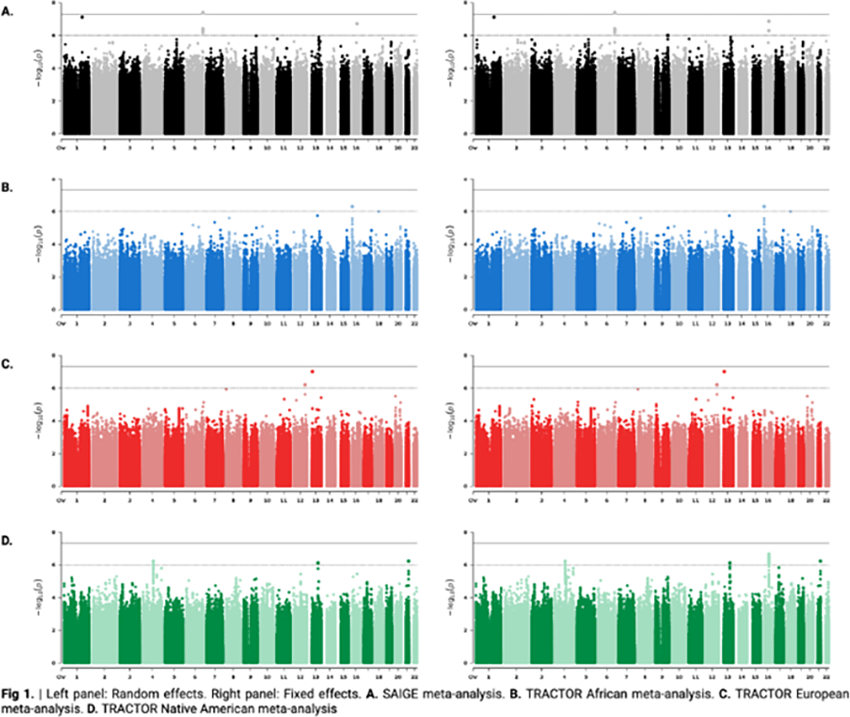
P01.22
1 David Geffen School of Medicine at UCLA, United States
Introduction: While genetic factors contribute to the development of Parkinson’s Disease (PD), environmental influences also play a significant role. Exposure to toxicants, such as pesticides and heavy metals, has been associated with increased risk for developing PD. Recently, copper (Cu)-containing pesticides, such as copper sulfate pentahydrate (CuSO4·5H2O), have been associated with incident PD and faster disease progression. Exposure to high levels of Cu has been associated with neuronal damage, but its mechanism of toxicity remains poorly understood. Here we investigated if exposure to Cu-based pesticides is associated with an increased risk of developing PD and if this association is causal using a zebrafish (ZF) model.
Methods: We investigated the potential association of Cu-containing pesticides to PD risk using data from the Parkinson's Environment and Gene study. Exposure was assessed in the Central Valley of California (n = 824 controls; n = 829 PD patients) using residential and occupational proximity to agricultural sites applying Cu-based pesticides over multi-decade periods. Pesticide application data was obtained from the California Pesticide Use Report, allowing estimation of individual exposures using geocoding. For the ZF studies, locomotion was assessed using the ZebraBox under light-dark cycling. The dopaminergic (DA) and non-DA sensory neuron numbers were determined using immunohistochemistry.
Results: Subjects exposed to 3 or more Cu-containing pesticides from 1974 until disease onset had an increased risk of developing PD with odds ratios of 1.83 for occupational and 1.46 for residential exposures. ZF larvae exposed to CuSO4·5H2O had significantly reduced motor activity at 7 days post fertilization in a dose-responsive manner. This reduced swimming activity coincided with a 28% DA neuron loss at an environmentally relevant concentration of 500 nM, while sensory neurons remained unaffected reflecting selective neurotoxicity.
Conclusions: Exposure to Cu-based pesticides is associated with an increased risk of developing PD. Preliminary studies in ZF suggest that this association appears to be causal since larvae exposed to environmentally relevant concentrations of CuSO4·5H2O recapitulated some aspects of PD that include impaired locomotion and selective DA neuron loss. Studies are underway investigating the mechanism of neurotoxicity which would add to the biological plausibility of Cu-based pesticides being a true PD risk factor.
P01.23
1 Shy, United States
Introduction: Cherry angiomas—also known as senile hemangiomas—are benign vascular lesions that can appear in clusters during episodes of inflammation, immune activation, or cutaneous irritation. Because people and pets share living environments, exposure to similar microbes or mites (e.g., Cheyletiella, Demodex) may influence skin and systemic inflammation, potentially linking dermatologic and neurological disease. In a 2024 cross-sectional study of 215 Parkinson’s disease (PD) patients, 45.1% had cherry angiomas, and 79.3% developed them before PD diagnosis, suggesting they may serve as visible, early indicators of disease processes. This project explores cherry angiomas as potential non-motor or environmental markers associated with Lewy body diseases (LBDs).
Methods: Photographic documentation and symptom logs were reviewed from a family reporting clusters of cherry angiomas, bullous eruptions, and sensations of biting after contact with household pets exhibiting dermatitis. Observations were compared with published evidence describing skin manifestations in PD—particularly seborrheic dermatitis, xerosis, rosacea, and cherry angiomas (PMCID: PMC11620005).
Results: Clusters of new cherry angiomas appeared on the trunk, neck, scalp, and retro-auricular regions after pet exposure. One family member later developed Lewy body dementia, while another relative by marriage developed Parkinson’s symptoms. Both individuals exhibited new-onset cherry angiomas and other cutaneous abnormalities preceding neurological decline.
Conclusion and Implications: Cherry angiomas may represent an underrecognized, non-motor biomarker of Lewy body diseases. Given their frequency, visibility, and potential to precede motor onset, routine dermatologic screening could complement neurological assessment in PD and LBD. Future research should (i) quantify angioma burden and temporal onset, (ii) include coordinated human–pet skin sampling with PCR-based mite and microbiome testing, and (iii) integrate skin α-synuclein assays (e.g., Syn-One). Clarifying whether cherry angiomas act as markers—or mediators—of inflammatory and vascular dysregulation may uncover new avenues for early detection and disease-modifying intervention.

BASIC SCIENCES: Neuroprotection, trophic factors and regenerative approaches
P02.01
1 School of Biomedical Sciences, Queensland University of Technology, Brisbane, QLD 4102, Australia
2 EpicentRx Inc, Torrey Pines, CA, 92307, United States
3 School of Biomedical Sciences, Queensland University of Technology, Brisbane, QLD 4102, Faculty of Medicine, The University of Queensland, Brisbane, QLD 4029, Translational Research Institute, Brisbane, QLD 4102, Australia
Environmental and occupational exposures to specific neurotoxicants such as pesticides, heavy metals, and organophosphates has been linked to increased risk and onset of Parkinson’s disease (PD). The growing evidence supporting chemical exposures and PD risk in occupational settings and military service highlights the urgent need to develop new disease modifying therapies and medical countermeasures to protect the central nervous system. In this study, funded by the US Department of Defense CDMRP Toxic Exposures Research Program (TERP), we used a combination of cell culture and mouse models of chemical exposures linked to central nervous system toxicity to evaluate RRx-001 as a prophylactic and neuroprotective medical countermeasure. RRx-001 is a small molecule dual NLRP3 inflammasome inhibitor and protective NRF2 activator that in currently in clinical stage studies (Phase 2) as chemoprotective and radioprotective agent. Using dopaminergic N27 and LUHMES cells, as well human monocytic (THP-1) and microglia cultures, we evaluated the effects of multiple PD-linked neurotoxicants (chlorpyrifos, DEET and vanadium) on neuronal death, mitochondrial dysfunction, and inflammasome activation. RRx-001 was evaluated for its ability to prevent and rescue these toxic effects. Caspase-3/7 activity, MitoSOX fluorescence, qPCR for mitochondrial markers, and IL-1β ELISA were used as key endpoints.
RRx-001 significantly attenuated neuronal death and mitochondrial dysfunction induced by toxicants in both N27 and LUHMES dopaminergic cells. In addition, to its neuroprotective properties in dopaminergic cells, RRx-001 also suppressed NLRP3 inflammasome activation in monocytes and microglia. Notably, RRx-001 reversed these toxicant’s induced neurotoxicity. Following testing of RRx-001 in cell culture models of PD and the validation of a minimal effective dose with nanomolar potency, our ongoing studies are evaluating RRx-001 in preclinical rodent models of neurotoxicity.
Our results confirm that nanomolar doses of RRx-001 can exert robust neuroprotective effects against a diverse chemical toxicant linked to occupational exposure and military service, as well as idiopathic PD. These findings highlight its potential for development as a medical countermeasure for chemical exposures in military and occupational settings.
P02.02
1 CERVO Brain Research Centre - Université Laval, Canada
2 The Neuro - Montreal Neurological Institute, Canada
3 St. Patrick Research Group in Basic Oncology, Oncology Division of CHU de Québec-Université Laval, Canada
4 Department of Molecular Biology, Medical Biochemistry, and Pathology, Faculty of Medicine, Université Laval, Canada
5 Department of Psychiatry and Neurosciences, Faculty of Medicine, Université Laval, Canada
Parkinson's disease (PD) is a chronic neurodegenerative disorder characterized by abnormal protein aggregates called Lewy bodies and the loss of dopaminergic neurons in the substantia nigra (SNC), which project into the striatum. Cell transplantation therapy for PD is challenged by toxic protein aggregates that hinder neuron survival and cause alpha-synuclein pathology, limiting the long-term efficacy of the grafts. Furthermore, current clinical trials face diAiculties in creating grafts that integrate properly, necessitating neuron transplantation directly into the striatum, which prevents the restoration of natural nigrostriatal pathways.
Our recent studies indicate that RIT2 protein influences autophagy-related processes and facilitates pathological alpha-synuclein clearance. RIT2 overexpression protects dopamine neurons and reduces motor dysfunctions in preclinical PD models. Additionally, our lab found that PLXNC1, an axon guidance receptor in neurons, mediates axon repulsion in response to SEMA7a, which is highly concentrated in the dorsal striatum. Modulating RIT2 and PLXNC1 expression in grafted neurons may therefore shield them from alpha-synuclein pathology and enhance striatum innervation.
We generated dopamine neurons from human embryonic stem cells (ESCs) overexpressing RIT2 or with reduced PLXNC1 expression. Using alpha-synuclein preformed fibrils as a PD model, we injected them into the SNC of adult immunocompromised mice. Subsequently, purified human ESC derived dopamine neurons were transplanted into the SNC. Neuropathology was evaluated for Lewy body markers, and neural projections to the dorsal striatum were quantified to assess the impact of RIT2 overexpression and PLXNC1 knockdown.
Preliminary results indicate that RIT2 protects against alpha-synuclein pathology and enhances the survival of dopamine neurons. Additionally, PLXNC1 knockdown improves the innervation of transplanted neurons in the dorsal striatum. These findings underscore the potential of modulating RIT2 and PLXNC1 as promising strategies to enhance the efficacy and long-term benefits of cell transplantation therapy for treating PD.
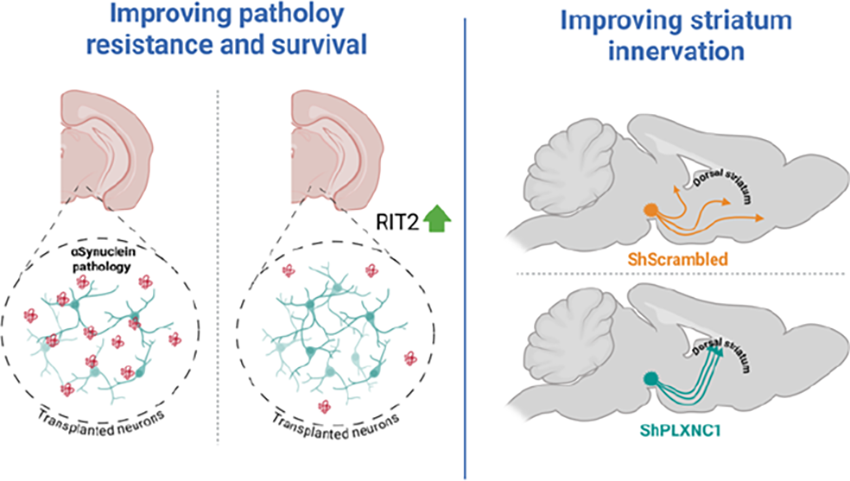
P02.03
1 Treefrog Therapeutics, France
2 Univ. Bordeaux, CNRS, Institut des Maladies Neurodégénératives, UMR 5293, France
With the rapid expansion of the field of 3D cultures and organoids, interest in their therapeutic use is growing. However, these innovative formats pose unique challenges for clinical translation as their physical and biological properties substantially differ from those of conventional single-cell-based products. Their handling imposes new constraints, such as much faster sedimentation, which must be addressed from the fill-and-finish stage to the final delivery procedure in the target region to ensure accurate dosing and precise cell placement. In this study, we present the development of a strategy to maintain homogeneity throughout the entire downstream process for the delivery of 3D neural microtissues as a cell therapy for Parkinson’s disease. This includes the development of a custom-made delivery solution. Various delivery methods were compared using in vitro tests. The final selected strategy was validated through in-use testing and led to successful engraftment in a non-human primate, with the presence of dopaminergic (DA) neurons observed 1 month after transplantation. While qualitative evidence of reinnervation was demonstrated in NHPs, quantitative evaluation was further carried out in the hemiparkinsonian rat model. The development approach described here holds potential for broader applications in other diseases and supports using next-generation cell therapies employing 3D formats.
P02.04
1 Cervo Brain Research Center, Université Laval, Canada
2 The Neuro's Early Drug Discovery Unit (EDDU), McGill University, Canada
3 UK Dementia Research Institute, Cambridge, United Kingdom
4 Tigem Napoli, Italy
Parkinson’s disease (PD) is the second most common neurodegenerative disorder, characterized by motor and non-motor symptoms in patients. One hallmark of the disease is the loss of dopaminergic neurons in the substantia nigra pars compacta (SNc), accompanied by Lewy bodies – proteinaceous inclusions mainly composed of alpha-synuclein (aSyn) - in surviving neurons. Mechanisms underlying the formation and clearance of these inclusions are still under intense investigation. The autophagy-lysosome pathway is dysregulated in PD and likely contributes to the defective clearance of aSyn. Current treatments are symptomatic, highlighting the urgent need to provide new therapeutic targets for further investigations. We performed a CRISPR-based, genome-wide screen to identify novel targets implicated in dopamine neuron survival. One of the hits, Flcn is implicated in the mTOR pathway and regulates lysosome biogenesis through MiT/TFE transcription factor modulation. When dopaminergic neurons are exposed to oxidative stress, Flcn knockout (KO) increases their viability in vitro. To validate the neuroprotective effect in vivo, we knocked-out Flcn in mouse dopaminergic neurons in the SNc. Four months after AAV-mediated expression of aSyn with or without Flcn KO, we assessed motor performance and brain pathology. Flcn KO ameliorates motor deficits induced by aSyn overexpression and rescues the loss of dopaminergic neurons in the midbrain and axon terminals in the striatum. Most importantly, Flcn KO also reduces the levels of phosphorylated aSyn in the midbrain. In parallel, we used iPSC-derived dopaminergic neurons, derived from PD patients carrying either the triplication of the SNCA gene or the A53T-aSyn mutation, and the respective isogenic controls. PD neurons display lysosomal and mitochondrial defects and an increase of aggregated forms of aSyn. FLCN KO decreases the levels of aggregated aSyn and increases the abundance of lysosomes. TFE3, a member of the MiT/TFE family, translocates to the nucleus and the mRNA levels of CLEAR target genes are increased when FLCN is depleted. Overall, our findings identify FLCN as a novel modulator of dopamine neuron function. Its depletion enhances degradative capacity, reduces aSyn accumulation, and protects neurons both in vitro and in vivo. Targeting FLCN may represent a promising strategy to boost lysosomal function and modify PD progression. Future work will explore transient FLCN downregulation as a therapeutic approach.
P02.05
1 Barrow Neurological Institute, United States
2 Michigan State University College of Human Medicine, United States
3 R&R Perez LLC, Drug Development, El Paso, TX, United States
4 Michigan State University Udall Center of Excellence, United States
5 Harvard Medical School/Brigham and Women's Hospital, United States
Alpha-synuclein (α-syn) aggregation is a defining pathological hallmark of Parkinson’s disease (PD). While its accumulation has traditionally been viewed as a toxic gain-of-function (GOF) process, the neurophysiological role of soluble α-syn remains poorly understood. Our previous work demonstrates that acute depletion of α-syn in mature nigral neurons in rodents and non-human primate induces progressive, dose-dependent neurodegeneration, preceded by inflammation and pathological markers, suggesting that loss of α-syn function may itself be deleterious. Here, we investigated whether preserving soluble, functional α-syn, in the adeno-associated virus (AAV)-α-syn model which results in α-syn aggregation and neurodegeneration, can mitigate α-syn–related neurotoxicity. To that end, we engineered an AAV expressing a non-aggregatable α-syn variant (α-syn-C6), in which six non-essential amino acid residues were replaced with cysteine residues, thereby disrupting its amyloidogenic propensity. Using an AAV-mediated co-expression paradigm in the rodent substantia nigra pars compacta, we tested whether low level α-syn-C6 expression could rescue the neurotoxicity induced by human α-syn (hα-syn) overexpression. Dopaminergic neuron integrity was assessed through unbiased stereological counts of tyrosine hydroxylase–positive (TH+) neurons, measurements of striatal TH enzymatic activity, and proteinase K resistance assays combined with serine-129–phosphorylated α-syn (pSer129) detection were performed to evaluate insoluble α-syn species. Co-expression of α-syn-C6 with hα-syn significantly attenuated TH+ neuronal loss observed in the hα-syn–only group, reduced somal shrinkage and dystrophic neurites and normalized the abnormal striatal TH enzymatic activity characteristic of this overexpression model. Importantly, α-syn-C6 did not interfere with the aggregation pattern of α-syn under co-expression conditions. Together, these findings support a model in which α-syn contributes to PD pathophysiology not only through toxic GOF mechanisms but also via toxic loss-of-function, whereby sequestration of soluble α-syn exacerbates neuronal vulnerability. Importantly, our results also demonstrate that α-syn aggregates are not directly toxic per se. The α-syn-C6 variant maintains physiological function while resisting aggregation, highlighting a novel therapeutic strategy in which preserving functional, aggregation-resistant α-syn may mitigate the neurodegeneration observed in PD.
P02.06
1 Southwest National Primate Research Center, United States
2 University of Texas Health San Antonio, Joe R. & Teresa Lozano Long School of Medicine, United States
3 NEONEURON LLC, United States
Parkinson’s disease (PD) is a relentlessly progressive neurodegenerative disease caused by the death of dopamine (DA) neurons in the substantia nigra pars compacta (SNpc). The loss of DA neurons in the SNpc results in a range of debilitating motor symptoms such as bradykinesia, tremor, rigidity and postural instability. Induced pluripotent stem cells (iPSCs) are specialized cells that can be differentiated from adult somatic cells genetically ‘reprogrammed’ to an embryonic stem cell state and serve as a valuable source for cell-based replacement therapies. Evidence indicates that stem cell derived dopaminergic neurons are a promising avenue in the search for a viable long-term treatment of PD. Here, we report the isolation of self-renewable neural stem cells (NSCs) from human iPSCs. The NSCs demonstrated the ability to proliferate in response to mitogenic growth factors. The isolated NSCs were further differentiated into neurons of dopaminergic lineage. The dopaminergic neurons co-expressed the tyrosine hydroxylase, β-tubulin and midbrain transcription factors (e.g.: FoxA2, Nurr1, Pitx3, Lmx1a, ALDH2, GIRK2). Differentiated neurons were transplanted into the putamen of MPTP-lesioned marmoset model of PD. The grafted animals were subjected to either a physical and cognitive training (PCT) or to sedentary conditions and monitored for a period of 6 months. This exercise paradigm engages cognitive and fine visuomotor coordination. Using Actigraphy, we observed that the grafted animals significantly improved their daily activity returning to normal baseline level and the PDRS improved by 88.23% compared to sedentary. The object retrieval task with barrier detour improved by approximately 63.95% and the success rate improved by 83.61% compared to pretreatment. The cognitive task (barrier reach) improved significantly by 77.58% compared. Morphological analysis demonstrated that the TH+ terminals of grafted DA neurons colocalize the pre- and postsynaptic puncta, synaptophysin and PSD-95, respectively suggesting synaptic formations with host cells in the PCT group. These synaptic structures were scarce in sedentary animals 6 months post-transplant. These data suggest that PCT enhances graft reinnervation of the striatum and restore optimal sensorimotor and cognitive functions.
P02.07
1 The University of Melbourne, Australia
2 Florey Institute of Neuroscience and Mental Health, Australia
3 Karolinska Instiitute, Sweden
Aim As an accessible outpouching of the brain, the retina affords a useful location to develop scalable biomarkers for Parkinson’s disease (PD) and response to treatment. Previous studies have shown that nicotinamide (NAM) is neuroprotective in another neurodegeneration, glaucoma. A53T mice recapitulate retinal biomarkers observed in people living with PD. This study aims to examine whether NAM treatment ameliorates A53T induced retinal biomarker changes and the underlying mechanisms.
Methods Alpha-synuclein transgenic mice (A53T) and wild type (WT) littermates were administered NAM (550 mg/kg/day) or vehicle in drinking water from 3 to 6 months old. At 6 months in vivo optical coherence tomography (OCT) and electroretinography (ERG) measures were used to assess retinal structure and function (n=8-18/group). Western blot (WB) and immunohistochemistry (IHC) were performed on retinal tissue and metabolomics on retina/brain tissue (n=4-11/group). Two-way ANOVA, with post-hoc Sidak’s multiple comparison was conducted.
Results A53T mice demonstrated thinning (OCT outer nuclear layer) and dysfunction (ERG a-wave) of photoreceptors compared with WT controls which was ameliorated with NAM (interaction effect, p<0.05). Supranormal ERG responses were also found in WT mice administered NAM (p<0.05). Metabolomics show that NAM metabolism is elevated in the retina and brain of mice treated with NAM compared to vehicle in both WT and A53T mice (1-methylnicotinamide, 6-hydroxynioctinamide elevated in retina, substantia nigra, CPU, frontal cortex (p<0.001), niacinamide elevated in retina (p<0.001). Western blot shows elevated inflammation (GFAP) with A53T which is partially ameliorated with NAM (p<0.05), elevated protective markers of oxidative stress in NAM treated mice (DJ1, p<0.01) and mitochondrial markers (TOM20, CytC, p<0.01). No significant changes were found in SOD1, DRP1, VDAC. Qualitative examination of IHC mirrored WB changes in GFAP and showed localization of DJ1, Tom20, CytC around photoreceptors and inner retinal layers.
Conclusions NAM ameliorates photoreceptor retinal thinning and dysfunction in the A53T mouse model. This parallels changes to inflammatory, mitochondrial and protective markers of oxidative stress in the retina as well as NAM metabolism in the retina and brain. This lays the foundation for NAM as a therapeutic intervention in PD and also demonstrates the utility of the eye as a PD detection and drug treatment biomarker.

P02.08
1 The Buck Institute, United States
2 Compass UOL, Brazil
3 Compass UOL, United States
4 Brown University, United States
5 Middlebury College, United States
To date, exercise is one of the only therapeutics shown to effectively ameliorate the progression of Parkinson’s disease (PD). One fascinating aspect of exercise is the rapid change which occurs to the physiological state of the gastrointestinal (GI) system where constriction of blood flow results in lower gut oxygen levels and changes in the organ’s metabolic demands. Such changes can ultimately alter the gut ‘microbiome’, the vast community of microorganisms that inhabit the digestive tract. Ingestion of beneficial microbiota in the form of pro-biotics has been shown to improve gut health, brain health, and exercise performance. Over the last decade or so, poor gut health has been established as an important prodromal symptom of Parkinson’s, manifesting as early as three decades before diagnosis. Given that exercise slows disease progression in those with PD, this begs the question as to whether administration of ‘exercise-probiotics’ might provide a targeted benefit. To answer these questions, we have performed bioinformatics analysis and AI-predictive modeling on data from 278 individuals enrolled in FoxInsight, an initiative from the Michael J. Fox Foundation (MJFF). Despite the high diversity of environmental conditions which can influence the microbiome, we have found significant differences in stool microbiomes based on exercise intensity (light, moderate, strenuous) and frequency (never, seldom, sometimes, often). Our results show that participation in strenuous exercise versus no-exercise has the greatest impact on bacterial Beta-diversity (R2=0.006, p=0.012) versus moderate and light exercise (R2=0.004, p=0.13 and R2=0.003, p=0.96, respectively.) Greater significance in Beta-diversity is observed upon comparison of individuals within the strenuous exercise group who exercise often versus sometimes (R2=0.014, p=0025), while alpha-diversity trends towards lower diversity in often-exercisers (Simpson Index, p=0.1), perhaps indicating a reduction in pathogenic bacteria. Using AI-predictive modeling, we were able to further establish substantial differences between bacterial composition based on exercise behavior. Here, we found four bacteria species which predict strenuous exercise, six which predict moderate exercise, and four which predict light exercise. Our current work is focusing on similar characterization of oral bacteria as well as models which examine correlations between bacteria and disease symptomatology.
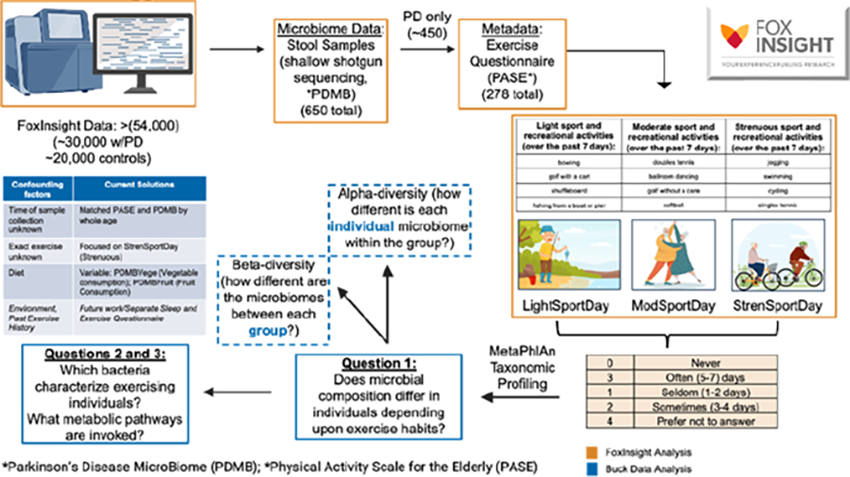
P02.09
1 University of Arizona, United States
2 The University of Arizona, United States
INTRODUCTION Mild cognitive impairment and Parkinson’s Disease (PD) Dementia are aspects that currently do not have satisfactory treatment options. We previously demonstrated that the glycosylated Ang(1-7) analog PNA5 improves cognition in male Thy-1αSyn (hαSyn) mice after 2-month treatment (1mg/kg) through reduction of microglia-mediated neuroinflammation. We now further explore PNA5 dose efficacy and mechanisms in males and females.
METHODS 20 males and females/group (WT-saline, hαSyn-saline, hαSyn-1mg/kg and hαSyn-0.5mg/kg PNA5). Behavioral testing at 4-months of age (baseline) and after 2-months treatment. Cognitive tasks: Novel Object Recognition, Y-maze, and 1-Trial, Object-Place Recognition. Motor tasks: Beam and Nestlet. Post hoc: immunohistochemistry to assess microglia and astrocytes, alpha synuclein load and synaptic markers (n=10/group), RNAseq analysis (n=10/group), and plasma analysis for biomarker identification.
RESULTS Overall, PNA5 treatment improved cognition (WT = 66.6% compared to hαSyn = 56.7%, 65.4% after treatment p = 0.034. In terms of sex differences, decreased alternation of male hαSyn animals relative to WT at 4 months (63.7% vs. 53.6%, p=0.0082) was seen in the Y-maze, indicating baseline cognitive deficits, whereas no deficits were seen in the females. After treatment, WT male mice show 4.7% change from baseline, while hαSyn animals show -8.7%, indicating further cognitive decline. PNA5-treated animals showed a 8.1% change from baseline, indicating a reversal of cognitive decline (p=0.0336). In the beam taest, a significant increase in the number of errors per step was seen at baseline in both sexes, (WT = 0.005 errors/step, hαSyn = 0.05 errors/step for females, p = 0.0074, and in males WT = 0.00 errors/step, hαSyn = 0.03 errors/step, p = 0.002). Analysis of the other behavioral tasks is currently underway. Additionally, we are also imaging and analyzing microglial and other pathological changes in the brain, and also conducting a transcriptional analysis of PNA5-mediated effects.
Conclusion Our analyses thus far further supports the ability of PNA5 to reverse cognitive decline. Ongoing studies will elucidate the molecular mechanisms underlying the PNA5-mediated cognitive enhancement and provide targets for biomarker development.
BASIC SCIENCES: Protein misfolding, aggregation and handling
P03.01
1 CEA, France
2 Institut Pasteur, France
3 CNRS, France
Objectives: The aim of this project was to create a tool to study the relationship between 3D structures of fibrils involving the protein alpha-synuclein (aSyn) reported as of today, through the pockets of interaction they form at their surface.
Methods: The rapid development of cryogenic electron microscopy (cryoEM) enabled the elucidation of various aSyn fibrillar structures, whether obtained from in vitro polymerization of recombinant protein or ex vivo filament extraction from brain tissue. Both of those methods have showne a high degree of polymorphism. As of today, very few exemples of classification and comparison of those structures have been reported. However, a better understanding of the structure-biology relationship is key to further tackle synucleinopathies outbrek and progession. By detecting pockets of interaction at the surface of each aSyn fibril polymorph and comparing the obtained results using a single metric entitled Pocket Similarity Index (PSI), we were able to design the pocketome as a tree map (TMAP) graph allowing the visualization of each pocket and addressing the biggest local similarities. The properties of each pocket can be obtained through various navigation and legend possibilities.
Results: We detected 227 pockets from 59 aSyn structures available on the PDB. This approach enabled us to show that aSyn polymorphs, whether they were obtained by in vitro protein aggregation or ex vivo filaments extraction from tissue, show a major diversity of potential pockets of interaction at their surfaces, with some features being shared, such as the importance of the Y39 fold for interaction. This approach was validated using the small number of existing cryoEM fibrillar structures with a small molecule, and pockets were successfully detected each time matching the hypothesized ligand binding mode. A DBSCAN algorithm has also been used to further cluster some pockets, yielding 10 groups of pockets, half of which are polymorph and sequence specific.
Conclusions: The obtained pocketome will hopefully guide future research on fibrillar structures of alpha-synuclein, and provide a tool to compare new polymorphs elucidated to the existing pool through the pockets of interaction they exhibit. It could be used to further understand the underlying mechanism of fibril formation and growth, and to guide ligand design of those aSyn fibrils to gain in both affinity and specificity.
P03.02
1 University of Pennsylvania, United States
In either the diagnostic setting or vascular setting, very high shearing and/or extensional forces can alter the structure and function of soluble proteins. For plasma-derived von Willebrand Factor (vWF), shear rates above ∼3000 s-1 drive coil-stretch transitions to create massive insoluble vWF fibers. In the seed amplification assay, hundreds of minutes or hours of vortexing with beads are required to drive amplification of synuclein aggregates. Although opportunities potentially exist for vWF and synuclein to interact in vivo, particularly where the blood brain barrier is disrupted, almost no information exists on this interaction. We developed an impingement-post microfluidic device that drives the formation of impingement-post deposits of massive vWF fibers from healthy human plasma. A buffer rinse and then perfusion of monomeric alpha synuclein (250 ug/mL) resulted in the accumulation of synuclein aggregates on the vWF fibers (using X-34 amyloid dye or MJFR-14-6-4-2 (Abcam) anti-aggregated synuclein Ab for epifluorescence detection). The synuclein aggregates formed on vWF fibers at 18,000 s-1, but not at 1800 s-1. This indicates that vWF fibers created at positions of pathologically high flow can facilitate and localize the formation of detectable alpha synuclein aggregates. Perfusion of healthy human plasma lacking exogeneous supplementation of monomeric alpha synuclein produced no deposits on vWF at either low or high shear rate. Pre-aggregated synuclein was found to readily bind to vWF-fibers, whether spiked into plasma prior to perfusion or added via buffer solution after vWF-fiber deposition. This work reports a previously unexplored link between pathological flow, vWF-fiber localization, and alpha synuclein aggregation processes.
P03.03
1 Department of Neurophysiology, National Institute of Neuroscience National Center of Neurology and Psychiatry, Tokyo / Department of NCNP Brain Physiology and Pathology, Graduate School of Medical and Dental Sciences, Institute of Science Tokyo, Tokyo, Japan
2 Department of Neurophysiology, National Institute of Neuroscience National Center of Neurology and Psychiatry, Tokyo, Japan
3 Department of Degenerative Neurological Diseases, National Institute of Neuroscience National Center of Neurology and Psychiatry, Tokyo, Japan
4 Department of Neurology, Kyoto University Graduate School of Medicine, Kyoto, Japan
The prodromal stage of Parkinson’s disease (PD), which can extend for more than a decade before motor onset, represents a critical period for early intervention. Insomnia is highly prevalent among older adults and patients with PD; frequent nocturnal awakenings leading to sleep fragmentation are the major complaint in patients with PD. Recent clinical studies suggest that chronic sleep fragmentation may exacerbate the progression of PD rather than being a consequence of PD progression, yet its causal role remains uncertain. Here, we investigated whether chronic sleep fragmentation accelerates the onset of prodromal symptoms and neuropathology in a mouse model of PD.
A53T SNCA bacterial artificial chromosome transgenic (Tg) mice, which reproduce non-motor symptoms and neuropathology characteristic of the prodromal stage, and wild-type (WT) mice were used. At 10–11 weeks of age, before the onset of detectable symptoms in Tg mice, mice were assigned to either of the following conditions: (1) Sleep Disturbance (SD) group housed in a running-wheel-based device (SD cage) that induces chronic sleep fragmentation resembling the sleep patterns of patients with PD, (2) Wheel Cage (WC) group housed in a regular cage with voluntary wheel running but no sleep disruption, or (3) Normal Cage (NC) group housed in a regular cage without a wheel. After 5 and 6 weeks, constipation and hyposmia was assessed, respectively. After 7 weeks, phosphorylated α-synuclein (p-syn) accumulation in the brain and colon and dopaminergic cell loss in the substantia nigra were assessed.
Tg mice exposed to chronic sleep fragmentation (SD group) exhibited both constipation and hyposmia, while WT mice in the SD group showed only mild constipation and no hyposmia. In Tg mice, proteinase K (PK) –resistant p-syn was significantly increased in the piriform cortex and showed a tendency to increase in the myenteric plexus of the colon in the SD group; PK-resistant p-syn accumulation in the piriform cortex positively correlated with hyposmia severity. Moreover, among the Tg mice, tyrosine hydroxylase-positive neurons in the substantia nigra were significantly reduced in the SD group. These findings demonstrate that chronic sleep fragmentation accelerates prodromal symptom onset and neuropathological progression in PD model mice. Chronic sleep fragmentation may thus serve as a modifiable risk factor and therapeutic target to delay PD progression during the prodromal stage to prevent motor onset.
P03.05
1 UNTHSC, United States
Introduction: Alpha-synuclein (aSyn) is highly implicated in Parkinson’s disease (PD) development, playing an important role in pre-synaptic neurotransmission through vesicular association. However, aSyn is intrinsically unstable and prone to misfolding into oligomers. As this oligomerization occurs during PD pathogenesis, we determined if the striatum may have inherently greater levels of oligomer compared to the substantia nigra (SN), given its vulnerability in PD. Using blot immunolabelling, we characterized the degree of monomer vs oligomeric forms between the striatum and SN. As a comparison DA pathway, the relative abundance of these forms was also evaluated in the mesoaccumbens pathway. We hypothesized that nigrostriatal neurons would show greater relative abundance of oligomeric forms of aSyn, reflecting their vulnerability in PD pathology.
Methods: Presence of total aSyn protein and relative monomer versus oligomer, using a qualified antibody that detects both forms of aSyn, were evaluated by western blot for striatum, SN, Nucleus accumbens (NAc), and ventral tegmental area (VTA) in intact brains of experimentally-naïve Sprague-Dawley rats. We evaluated total aSyn immunoreactivity and assessed percents of monomer vs oligomeric forms from 15 to 250 kDa across these 4 brain regions.
Results: In intact brains, there was greater total (monomer + oligomer) aSyn immunoreactivity in the SN vs striatum. However, the percent of monomeric forms of aSyn were greater in the SN vs striatum; this difference also held between VTA and NAc. We observed significantly greater presence of a 60 kDa oligomer in the Striatum compared to SN and NAc. Trends in the data observed included a higher percent of total oligomer in the striatum compared to SN and in NAc vs VTA.
Conclusions/Next steps: This data implies that even at baseline, aSyn oligomeric forms are predominantly in the striatum and establishes a baseline comparison against possible accumulation of oligomeric forms in toxin models. Thus, we predict toxin models may have greater amounts of oligomeric forms of aSyn in both the striatum and SN. This investigation into how aSyn morphology evolves upon lesioning and PD progression has the potential to outline aSyn’s potential role in the trajectory of DA neuron demise.
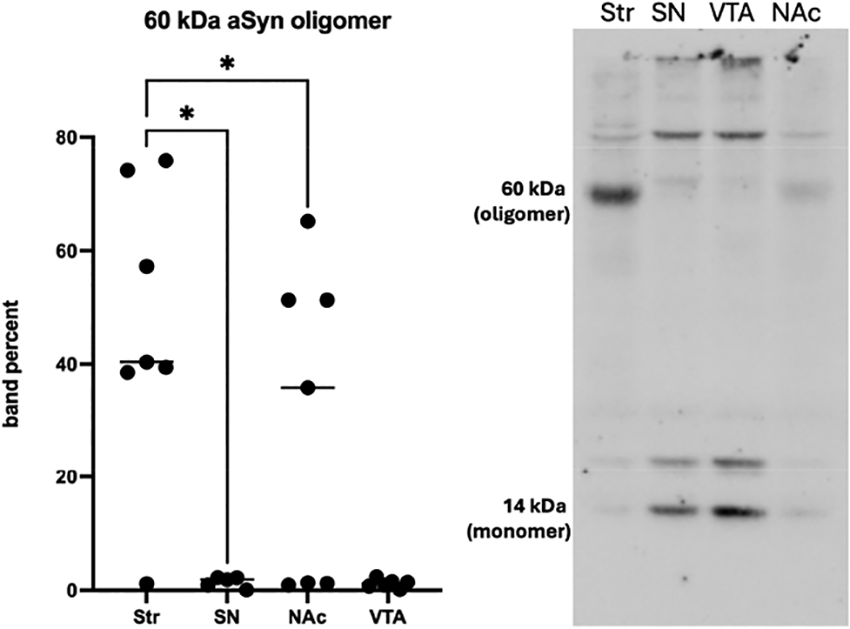
P03.06
1 Vall d'Hebron Research Institute (VHIR), Spain
2 Universitat Autònoma de Barcelona, Spain
3 Vall d’Hebron Hospital, Spain
4 Centro de Investigación Príncipe Felipe (CIPF), Spain
Our team has developed the NanoERT Platform, an innovative nanotechnological solution designed to improve enzyme replacement therapies (ERTs) by integrating advanced nanocarrier systems with customized conjugation strategies. This platform enhances protein stability, bioavailability, and targeted biodistribution.
As a proof of concept, our initial focus is on glucocerebrosidase (GBA), the lysosomal enzyme encoded by GBA1 gene, and deficient in Gaucher disease (GD) and Parkinson’s disease associated to GBA1 (PD-GBA1). We have generated a range of nanoGBA conjugates combining recombinant GBA with polypeptide-based nanocarriers optimized for diverse delivery strategies. These include systemic administration, CNS-targeted delivery via BBB-penetrating polymers, and brain-directed approaches based on validated intranasal CNS-penetrant technologies.
In in vitro models of PD-GBA1 and GD, nanoGBA conjugates efficiently enter neurons via endocytosis, localize to lysosomes, and release functional GBA, restoring enzymatic GCase activity, reducing sphingolipid accumulation, and lowering phosphorylated α-synuclein levels. In vivo, different nanoGBA formulations have shown enhanced biodistribution and superior efficacy compared to conventional ERTs, both systemically and in CNS-targeted applications.
The NanoERT platform offers a promising and versatile strategy for delivering therapeutic enzymes to key disease tissues and opens the door to disease-modifying treatments for GBA1-associated PD and neuropathic GD.
P03.07
1 BRFAA, Greece
2 University of Florida, United States
Introduction. Parkinson’s disease (PD) is the second most common neurodegenerative disorder, primarily known for its progressive motor symptoms. Mutations in leucine-rich repeat kinase 2 (LRRK2), a kinase/GTPase, drive PD by causing excessive kinase activity towards multiple substrates, and cellular dysfunction. Rab GTPases coordinate most membrane trafficking processes in eukaryotic cells and are well-characterized LRRK2 substrates that become aberrantly phosphorylated and dysregulated in disease. Select Rab GTPases can also reciprocally modulate LRRK2 kinase activity through mechanisms that remain incompletely characterized. In this study, we examined how Rab29 and the PD-linked S71R-Rab32 mutant are able to stimulate LRRK2 kinase activity, focusing on their effects on LRRK2 dimerization.
Methods. Using an overexpression system of different Rab GTPases along with two proximity biotinylation constructs of LRRK2 in HEK293T cells…
Results. We demonstrate that Rab29 enhances LRRK2 kinase activity without promoting its dimerization. In contrast, S71R-Rab32 activates LRRK2 by promoting dimerization, primarily via interactions with monomeric LRRK2. Our findings further reveal that disruption of the main dimerization interface of LRRK2 (COR-B) under S71R-Rab32 overexpression leads to partial reversal of its kinase-activating effects by reducing LRRK2 autophosphorylation but not downstream substrate phosphorylation. Further, we investigated the other protein interactors binding in this domain of LRRK2 (armadillo), namely the death adaptor FADD, and how its binding or absence affects LRRK2 interactions with Rab’s. Treatment with a peptide to displace the binding of FADD to the ARM domain, resulted in elevated phosphorylation of Rab10 in cells, but no change in LRRK2 auto-phosphorylation, indicating that intrinsic kinase activity was unchanged. We used this approach to also examine the physical interaction between LRRK2 and Rab’s via this domain. Finally, a variant in the ARM domain, L403, was found to prevent the induction of LRRK2 activity by mutant S71R-Rab32, as well as Rab29.
Conclusions. The N-terminal armadillo domain is a protein interactor “hot-spot”, and by modulating that interaction of specific proteins in this region, we can affect the binding and functional effects of other proteins such as the Rab GTPases. These studies will help open new avenues for therapeutic development targeting specific interacting proteins in this domain of LRRK2.
P03.08
1 BRFAA, Greece
2 VIB/VUB, Belgium
Introduction. Mutations in the LRRK2 gene, first reported in 2004, are the most common genetic cause of Parkinson’s disease. Most of the described pathogenic mutations lead to an increase in the kinase activity of LRRK2, however the mechanisms of this activation are not fully understood. Conformational changes, such as dimerization, can underlie regulation of kinase activity; and tools such as single-chain variable domain antibodies, known as nanobodies (Nb’s) are being deployed to unravel these mechanistic questions. We employed a small library of LRRK2 Nb clones to assess conformational changes between WT and mutant LRRK2, as well as baseline and activated LRRK2 in disease-relevant cellular models. Our earlier screens identified specific clones of Nb’s that show increased affinity for dimeric LRRK2, over monomeric. We focused on these dimer-specific clones to further explore conformational differences and changes under various conditions.
Methods. We employed multiple cellular models commonly used in PD to assess changes in LRRK2 conformation and activation in the context of specific stressors. We selectively labeled WT or mutant LRRK2 dimer complexes using biotin. We compared binding of each clone to the isolated dimers to determine if conformational changes can be detected using Nb’s. In RAW macrophages, we used an ELISA-based approach to compare the affinity of specific Nb clones to LRRK2 isolated from cells exposed to toxicants (e.g. oxidative stress).
Results. We identified multiple clones that exhibit altered binding between WT and mutant G2019S-LRRK2 dimers. Notably, one clone displayed significantly greater affinity to homo-dimers of G2019S-LRRK2, compared to WT dimers or WT/mutant hetero-dimers. Since we had previously shown that the homo-dimers of G2019S-LRRK2 exclusively exhibit increased LRRK2 activity, we next asked is this Nb clone could be used to monitor changes in WT LRRK2 at endogenous levels. Macrophages treated with LPS respond with increased LRRK2 activity; and measuring Nb-binding affinity, we showed that WT LRRK2 from cells exposed to stressors can assume a mutant-like conformation.
Conclusion. Using tools such as single-chain nanobodies we are beginning to understand the role of conformational changes and dimerization in the regulation of LRRK2 activity. This will enable the development of more precise tools to disrupt pathological LRRK2 signaling, and PD pathogenesis.
BASIC SCIENCES: Mitochondria, Oxidative Stress
P04.01
1 Laval University, Canada
In Canada, ∼38 people are diagnosed with Parkinson’s Disease (PD) every day, but there is still no viable treatment plan capable of slowing or reversing disease progression. Mitochondrial dysfunction is a central hallmark of PD, contributing to dopaminergic neuron degeneration in both sporadic and genetic cases of the disease. Here, we investigate whether enhancing mitochondrial function by overexpressing Nuclear Respiratory Factor 1 (NRF1), a key transcription factor for mitochondrial biogenesis and protein production, can mitigate PD-related pathology. Using human iPSC-derived dopaminergic neurons harbouring the 3xSNCA mutation and isogenic controls, we observed decreased mitochondrial membrane potential, increased reactive oxygen species levels, and reduced mitochondrial protein import in 3xSNCA neurons. NRF1 overexpression rescued all three deficits, increasing TMRM intensity, reducing oxidative stress, and restoring NDUFS3 import levels. Additionally, NRF1 increased the expression of TOM20, suggesting enhanced mitochondrial mass or import machinery, even in control neurons. Morphologically, NRF1 promoted increased neurite branching in both human neurons and primary mouse ventral midbrain cultures and has also been shown to increase neuronal firing synchronicity in multi-electrode array recordings. In vivo, AAV-mediated NRF1 delivery in a mouse α-synuclein injection model led to increased survival of tyrosine hydroxylase (TH)+ neurons and rescued behavioral deficits, including improved balance beam performance and forelimb grip strength. Together, these findings highlight NRF1 as a potent enhancer of mitochondrial function and neuronal resilience in both human and rodent PD models. Our study supports the potential of mitochondria-targeted gene therapy as a disease-modifying strategy for PD.
P04.02
1 Soonchunhyang University College of Medicine, South Korea
2 Gumi Hospital of Soonchunhyang University, South Korea
3 Faculty of Medicine, University of British Columbia, Canada
The purpose of this study is to understand the change of mitochondria morphology for some genes to cause young onset familial Parkinsońs diseases using drosophila.
We would study PINK1 knock-out (PINK1-/-) , Parkin knock-out (Parkin -/-) and dCHCHD2 knock-out (dCHCHD2 -/-) in normoxia or hypoxia condition. In cellular level, Parkinson's disease (PD) has prominent mitochondrial dysfunction. PINK1 and Parkin, which encode mitochondrial protein kinase and cytosolic ubiquitin (Ub) ligase, relatively, were identified as the genes responsible for the autosomal recessive form of juvenile Parkinson's disease. Parkin gene encodes an ubiquitin ligase (E3), as we know, induces mitophagy to control mitochondria quality. And loss of Parkin gene results in degradation of mitochondria. Parkin, PINK1 and DJ-1 are associated with mitophagy and mitochondria homeostasis.
The newly identified PD-related gene CHCHD2, which encodes a mitochondrial protein, was one of etiologies of PD. The loss of CHCHD2 in Drosophila causes abnormal matrix structures and impaired oxygen respiration in mitochondria, leading to oxidative stress.
P04.03
1 The American University in Cairo, Egypt
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by dopaminergic neuronal loss in the substantia nigra and the accumulation of misfolded α-synuclein. While most therapeutic approaches focus on symptomatic relief, limited progress has been made in slowing or reversing neuronal degeneration. Recent evidence suggests that mitochondrial dysfunction is a central contributor to PD pathogenesis. The goal of this research is to investigate the therapeutic potential of a novel synthetic mitochondrial-targeted peptide, MT-13, designed to stabilize mitochondrial membrane potential and reduce oxidative stress in early PD stages.
The effects of MT-13 on neuronal survival, oxidative markers, and mitochondrial respiration were evaluated using both in vitro dopaminergic neuron cultures and in vivo murine models of α-synuclein overexpression. The peptide was administered via nanoparticle delivery to ensure selective targeting of midbrain neurons. Mitochondrial activity was assessed using high-resolution respirometry, while oxidative damage and apoptosis were quantified through immunocytochemistry and Western blot analysis. Behavioral assessments, including rotarod and open-field tests, were conducted to evaluate functional recovery in treated mice.
The results showed that MT-13 treatment significantly restored mitochondrial complex I activity, reduced reactive oxygen species (ROS) accumulation by 42%, and increased dopaminergic neuronal survival by 38% compared to untreated PD models. Behavioral tests revealed marked improvement in motor coordination and spontaneous locomotion, indicating that mitochondrial stabilization translated to functional recovery. Moreover, no adverse systemic effects were observed following chronic administration of the peptide.
In conclusion, the constructed novel peptide was shown to have great potential in restoring cellular energy homeostasis rather than merely alleviating symptoms. The findings provide compelling preclinical evidence that targeted mitochondrial peptide modulation can mitigate neurodegeneration and motor deficits in Parkinson’s disease, paving the way for future translational studies on mitochondrial-based neuroprotection in PD.
P04.04
1 Eurac Research - Institute for Biomedicine, Italy
Background: Mitochondrial dysfunction and aggregation of α-synuclein are hallmarks of Parkinson’s disease (PD), and targeted interventions in these pathological pathways may mitigate disease onset and progression. Monogenic PD forms are closely linked to mitochondrial defects, and increasing evidence shows that GBA1-associated and many idiopathic PD cases also feature mitochondrial impairment. The mitochondrial signature lipid cardiolipin, central to membrane curvature and bioenergetics, interacts with α-synuclein, connecting membrane composition to early protein misfolding. Previous work has demonstrated that neural progenitor cells (NPCs) derived from patient-iPSCs display a neuronal-like mitochondrial metabolism and are an effective tool for phenotypic drug screening in neurological disorders associated with mitochondrial dysfunction. Here, we propose NPCs as a disease-relevant model to investigate mitochondrial phenotypes in PD mutations, with the aim to screen for potential therapeutic approaches focused on restoring mitochondrial function.
Methods: We derived NPCs from PD patients carrying 3xSNCA, A53T SNCA and L444P/WT GBA1 mutations and controls using small molecules. Cells were characterized for mitochondrial phenotypes with biochemical and imaging-based techniques.
Results: Biochemical characterization of patient-derived NPCs revealed that, regardless of the specific mutation, cells presented reduced OXPHOS-driven ATP content, indicating a more glycolytic profile. Moreover, Complex I enzymatic activity was reduced in all three mutations. The potentiometric probe TMRM was used to assess mitochondrial membrane potential (MMP) with a high content imaging (HCS) approach. Data indicate that the heterozygous L444P GBA1 NPCs present a constant MMP depolarization, consistent with decreased Complex I enzymatic activity. This represents a robust and easily quantifiable phenotypic trait for screening applications. Notably, in line with the reduced activity of the lysosomal enzyme GCase, α-synuclein accumulation and basal autophagy changes were detected in L444P GBA1 NPCs, which could further contribute to mitochondrial dysfunction.
Conclusions: NPCs represent an efficient, disease-relevant model for mitochondrial impairment in the context of PD, as they i) already present a shift towards OXPHOS metabolism, enabling the detection of mitochondrial phenotypes; and ii) are well suited for HCS approaches.
Supported by The Silverstein Fellowship Program 2025.
P04.05
1 Institut Pasteur, France
Parkinson’s disease (PD) is largely characterized by α-synuclein (α-syn) aggregates perturbing neuronal degradative pathways, damaging mitochondrial functions, and leading to neuroinflammation. Microglia aid -syn-burdened neurons through clearance, and our lab has shown that both α-syn and mitochondria can be transferred between these cells through tunneling nanotubes (TNTs) to ease the burden. CD4+ T cells also play a significant role in the initial inflammatory response to α-syn-laden neurons; however, this diminishes over time in PD patients along with functional properties. Here, we seek to elucidate the effects of α-syn on the neuronal-microglia-CD4+ T cell network, specifically on mitochondrial metabolism and inflammatory responses. We found that α-syn can be internalized and degraded by the Jurkat CD4+ T cell line. When re-exposed to α-syn and subsequently co-cultured with SH-SY5Y cells, Jurkat cells develop enlarged, circular mitochondria that localize more towards the immunological synapse. The cellular body also extends towards the neuronal cells and the TNT connections per cell increase; however, additional exposures to α-syn reduces these, suggesting possible exhaustion. With repeated exposures, Th1 lineage and exhaustion markers within Jurkat cells seem to increase, as has been previously shown in circulatory CD4+ T cells of PD patients. When naïve Jurkat cells are tri-cultured with α-syn-treated SH-SY5Y and HMC cells, they preferentially form TNTs with SH-SY5Y cells with some Jurkat/SH-SY5Y connections containing mitochondria, which is lost when HMC3 are absent and suggests an instigating role by HMC3 cells on Jurkat/SH-SY5Y cells. Moreover, Jurkat-derived mitochondria was found within SH-SY5Y and HMC3 cells, indicating their potential beneficial roles in the initial response to α-syn antigen. These data suggest that upon α-syn presentation, CD4+ T cells become activated, undergo mitochondrial reprogramming, and provide mitochondria to α-syn-laden neuronal cells, followed by a Th1/Treg and exhaustive phenotype with chronic α-syn exposure. The metabolic state compared to inflammatory/activation states of Jurkat cells re-exposed to α-syn in a tri-culture will be further investigated to determine factors driving CD4+ T cells towards exhaustion in PD. Altogether, we aim to explicate the exhausted fate of α-syn-chronically exposed CD4+ T cells by the intertwining metabolic and inflammatory relationship.
Parkinson’s disease (PD) is largely characterized by

P04.06
1 Institute for Biomedicine, Eurac Research, Bolzano, Italy
2 Department of Psychiatry and Neurosciences, Faculty of Medicine, Université Laval, CERVO Brain Research Centre, 2601 Chemin de la Canardiere, Quebec City, QC, Canada
3 Development, Aging and Regeneration Program, Sanford Burnham Prebys Medical Discovery Institute, La Jolla, CA, United States
4 Clinical Lipidomics Unit, Institute of Physiological Chemistry, University Medical Center, Mainz, Germany
5 5Department of Pediatrics, Faculty of Medicine, Université Laval, Centre de Recherche de l’Institut Universitaire de Cardiologie et Pneumologie de Québec City, QC, Canada
6 Department of Biology, University of Padova, Padova, Italy
7 Institute of Biomolecular Chemistry of CNR, Padova Unit, Padova, Italy
8 Institute for Biomedicine, Eurac Research, Bolzano, Italy, Italy
9 Department of Pediatrics, Faculty of Medicine, Université Laval, Centre de Recherche de l’Institut Universitaire de Cardiologie et Pneumologie de Québec City, QC, Canada
Background. The accumulation of misfolded α-synuclein (αSyn) in Lewy bodies is a hallmark of Parkinson’s disease (PD), primarily affecting dopaminergic neurons vulnerable to mitochondrial stress. Mitochondrial defects are central to αSyn toxicity, yet the molecular mechanisms linking altered organelle integrity and lipid dysregulation to αSyn pathology remain unclear. Stomatin-like protein 2 (SLP-2, encoded by STOML2) is a mitochondrial inner membrane scaffold that stabilizes respiratory chain supercomplexes and maintains cristae organization. Beyond its structural role, SLP-2 coordinates mitochondrial lipid homeostasis by organizing cardiolipin-rich microdomains and facilitating lipid exchange at mitochondria–ER contact sites. Perturbation of these lipid-regulatory functions may connect mitochondrial failure to αSyn pathology and neuronal vulnerability in PD.
Methods. We quantified SLP-2 levels in TH+ neurons from post-mortem PD brains and A53T αSyn transgenic mice to assess its association with pathology. Functional studies were performed in SH-SY5Y cells, hiPSC-derived dopaminergic neurons from PD patients with SNCA-mutations, and transgenic Drosophila and mouse models expressing human A53T αSyn. Mitochondrial function was evaluated by live-cell imaging and oxygen consumption rate measurements, while lipid profiles were analyzed using untargeted lipidomics. SLP-2 overexpression or knockdown was applied to determine its impact on αSyn toxicity, mitochondrial performance, lipid composition, and neurodegeneration.
Results. SLP-2 levels were significantly reduced in TH+ neurons of PD patient brains and in A53T αSyn mice. In the cellular models, SLP-2 upregulation restored mitochondrial morphology, rescued bioenergetic defects, and reduced phosphorylated αSyn (pS129) association with mitochondria. Lipidomics revealed alterations in several lipid classes, including glycosphingolipids (GSLs), which were partially normalized by mild SLP-2 overexpression. In vivo, SLP-2 overexpression preserved dopaminergic neurons, maintained mitochondrial function, and prevented motor deficits. Conversely, SLP-2 knockdown exacerbated αSyn-induced neurodegeneration and impaired motor performance. SLP-2 also reduced pS129-αSyn levels and aggregate formation in both Drosophila and patient-derived hiPSC neurons.
Conclusions. These findings suggest SLP-2 as a key regulator of mitochondrial resilience and a potential therapeutic target for PD and alpha-synucleinopathies.
P04.07
1 Eurac Research, Institute for Biomedicine, Italy
Background: Alterations in lipid metabolism have emerged as a critical feature of Parkinson’s disease (PD), influencing protein aggregation, mitochondrial integrity, and neuronal survival. Mitochondrial dysfunction, mainly driven by oxidative stress and protein misfolding, is a hallmark of PD. The lipid composition of mitochondrial membranes, including cardiolipin (CL), a mitochondria-specific phospholipid, plays a crucial role in maintaining mitochondrial integrity and function. Stomatin-like protein 2 (SLP-2) is an inner mitochondrial membrane-organizing protein that regulates mitochondrial proteases and facilitates CL synthesis. Recent genome-wide association studies have identified variants in lipid biosynthesis genes, including Serine Palmitoyltransferase Small Subunit B (SPTSSB), fatty acid synthase (FASN), and cardiolipin synthase 1 (CRLS1), that are linked to increased PD risk. These findings reinforce a lipid-centric model of PD pathogenesis, highlighting the interplay between mitochondrial lipid metabolism and neuronal vulnerability.
Results: In nematode models (C. elegans) exposed to paraquat, a mitochondrial stressor that activates the mitochondrial unfolded protein response (mtUPR), we observed reduced CL levels and altered mitochondrial phosphatidic acid (PA) composition. Oxidative stress disrupted the mitochondrial membrane distribution of stomatin-like protein STL-1, an ortholog of human SLP-2, linking lipid imbalance to proteostatic stress. In SH-SY5Y neuroblastoma cells, α-Synuclein overexpression led to changes in CL levels; SLP-2 knockdown impaired mtUPR activation, whereas its overexpression restored the expression of heat shock proteins HSP60 and GRP75, rescuing stress-induced phenotypes. Lipid-binding assays revealed that both C. elegans STL-1 and human SLP-2 directly interact with PA and CL, suggesting a lipid-sensing function.
Conclusion: Together, these findings identify an evolutionarily conserved mechanism of mitochondrial protection, in which SLP-2 orthologs detect changes in mitochondrial phospholipid composition to fine-tune mtUPR activation and promote cellular stress resilience. Targeting mitochondrial lipid alterations through genetic or small-molecule interventions (such as Elamipretide or Nobiletin) may offer promising therapeutic opportunities in PD.
BASIC SCIENCES: Pathology
P05.01
1 Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije University Amsterdam, Amsterdam, The Netherlands., Netherlands
2 Erasmus MC, University Medical Center Rotterdam, Department of Clinical Genetics, The Netherlands., Netherlands
3 Department of Neurology, Oslo University Hospital, Oslo, Norway, Norway
4 Roche Pharma Research and Early Development, F. Hoffmann-La Roche Ltd, Basel, Switzerland., Switzerland
Background: Parkinson’s disease (PD) features alpha-synuclein (aSyn) brain deposition and lysosomal dysfunction. Variants of the gene GBA1 reduce the activity of the lysosomal enzyme beta-glucocerebrosidase (GCase), increase PD risk and are linked to earlier disease onset. Prior reports suggest greater cortical αSyn in GBA-PD patients compared to idiopathic PD (IPD). Nonetheless, the relation between GCase deficit and αSyn remains unclear.
Methods: We sequenced GBA1 in 160 post-mortem cases (21 controls, 25 incidental Lewy body disease (iLBD), 114 PD) to identify carriers of risk variants. Frozen brain from locus coeruleus (LC, n=71), substantia nigra (SN, n=53), and gyrus temporalis medius (GTM, n=115) underwent sequential extraction into Soluble and Insoluble fractions. We developed alpha-LISA assays to quantify total, phosphorylated-Ser129 (pSer129), and C-terminally aa122 truncated (CTT122) αSyn. Similarly, total GCase activity and abundance were measured by enzymatic assay and ELISA.
Results: GBA1 risk variants were present in 21.9% of PD cases, including a novel variant. pSer129 and CTT122 αSyn accumulated markedly in iLBD and PD in Insoluble fractions, but not in Soluble fractions. The ratio of Insoluble pSer129 to Soluble total αSyn best predicted the presence of aSyn pathology. Cortical Insoluble αSyn did not differ between IPD and GBA-PD, nor across GBA1 variant severity. Similarly, Insoluble αSyn in SN and LC did not differ between IPD and GBA-PD. GCase activity was reduced in GBA-PD and IPD versus controls and correlated with Insoluble pSer129 levels. GCase activity and αSyn measures strongly correlated with Braak-αSyn stage.
Conclusions: Here we describe GCase impairment in both GBA-PD and IPD. GCase activity reduction correlates with increased Insoluble αSyn pathology in both IPD and GBA-PD. Importantly, we find no evidence for increased (cortical) αSyn burden in GBA-PD versus IPD. Moreover, the data underpins the importance of differential protein extraction for the detection of pathological αSyn load in post-mortem human brain.
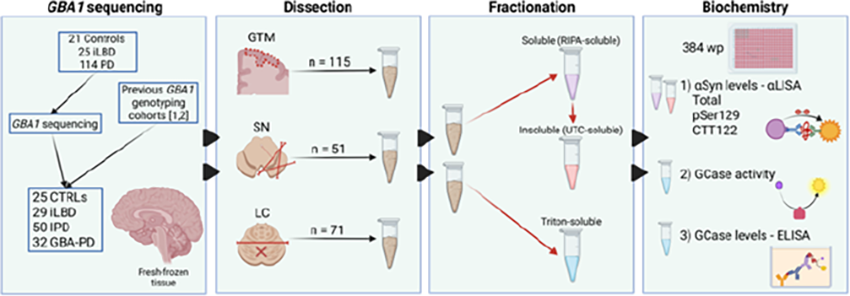
P05.02
1 Department of Environmental Health Sciences, Florida International University, Miami, FL, USA, United States
Background: Parkinson’s disease (PD) is characterized by α-synuclein (α-syn) aggregation and neuroinflammation, driving dopaminergic neurodegeneration. Dynamin-related protein 1 (DRP1), a key regulator of mitochondrial fission, has emerged as a potential mediator of these pathogenic processes by linking mitochondrial dysfunction, autophagy, and inflammatory signaling. Here, we investigated whether partial loss of DRP1 (Dnm1l+/−) confers neuroprotection against α-syn–induced pathology and neuroinflammation, including exosome-mediated propagation of neurotoxic factors.
Methods: Dnm1l+/- mice were crossed with transgenic mice overexpressing wild-type human α-synuclein (SNCA+/-). α-syn pathology (total α-syn, phospho-Ser129, and Syn303) was quantified in tyrosine hydroxylase (TH)–positive neurons and glia using immunostaining and Imaris 3D rendering. Inflammatory markers were assessed by qPCR and cell-type–specific laser microdissection. Brain-derived exosomes were purified by gradient ultracentrifugation and analyzed for α-syn and inflammatory cargo. Exosomes from SNCA+/− or Dnm1l+/−;SNCA+/− mice were intranasally administered to wild-type mice to assess behavioral and neuropathological outcomes.
Results: SNCA+/− mice exhibited α-syn aggregation and neuroinflammation at 6 and 12 months; however, such pathology was markedly attenuated by Dnm1l heterozygous deletion. DRP1 nuclear translocation was enhanced in microglia of SNCA+/− mice and correlated with NF-κB activation and elevated inflammatory mediators, particularly Lcn2 in glia. Notably, lipocalin-2 protein, but not mRNA, was elevated in TH-positive neurons, suggesting glia-to-neuron transfer. Supporting this notion, exosomes from SNCA+/− mice contained increased lipocalin-2, α-syn, and phospho-α-syn (pS129), which were less in exosomes from Dnm1l+/− mice. In stable dopaminergic cells with inducible α-syn, recombinant lipocalin-2 promoted accumulation of proteinase K–resistant α-syn. Intranasal administration of SNCA+/− exosomes induced ventral midbrain α-syn pathology, tremor, and motor deficits in wild-type mice, effects that were significantly reduced with Dnm1l+/− exosomes.
Conclusions: Our findings reveal that DRP1 promotes α-syn–driven neuroinflammation and exosome-mediated spread of pathology through an NF-κB–Lipocalin-2 signaling axis. Partial DRP1 loss mitigates these processes, positioning DRP1 as a central regulator of neuroimmune and proteostasis, and a promising therapeutic target for PD.
P05.03
1 Section Clinical Neuroanatomy and Biobanking, Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
2 Section Clinical Neuroanatomy and Biobanking, Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands., Netherlands
3 Department of Pathology, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
4 Department of Pathology, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands; Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
5 Tanz Centre for Research in Neurodegenerative Diseases, University of Toronto, Toronto, Ontario, Canada, Canada
6 Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam, The Netherlands, Netherlands
7 Department of Neurology, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
8 Netherlands Brain Bank, Netherlands Institute for Neuroscience, Amsterdam, The Netherlands; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
9 Section Clinical Neuroanatomy and Biobanking, Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands.; Amsterdam Neuroscience, Neurodegeneration program, Amsterdam UMC, Amsterdam, The Netherlands, Netherlands
Background Amygdala-predominant alpha-synuclein (aSyn) pathology is common in neurodegenerative diseases, including Alzheimer’s disease (AD), Parkinson’s disease (PD) and dementia with Lewy bodies (DLB). In these diseases, amygdala aSyn pathology has been associated with amygdala atrophy, cognitive decline, visual hallucinations and olfaction deficits. However, amygdala-predominant Lewy body disease (LBD) is still poorly understood. We investigated the clinical and neuropathological features of this subtype in a brain bank cohort.
Methods We included cases from the Netherlands Brain Bank (1998-2023) which had been neuropathologically characterized and classified as amygdala-predominant (Alafuzoff et al., 2009) (n=70; 5%) by expert neuropathologists. The burden of aSyn pathology was semi-quantified (scale 0-3) in immunostained (KM51 and 5G4) sections of the medulla oblongata (MO), substantia nigra (SN), amygdala (AMY), anterior cingulate gyrus (CG) and medial frontal gyrus (F2). Demographical and clinical data were retrieved from clinical records. Neuropathological features (e.g. Braak aSyn and NFT stages, Thal phase, age-related tau astrogliopathy (ARTAG) and cerebral amyloid angiopathy (CAA)) were retrieved from autopsy reports and diagnostic tissue sections stained for phosphorylated tau (p-tau) and amyloid-β (Aβ).
Results Demographical, clinical and pathological features of the cohort can be found in Figure 1. In short, 80% had dementia, 37% parkinsonism and 29% both. Hallucinations (41%), anxiety (34%) and depression (41%) were frequently reported. The most common neuropathological diagnosis was AD with Lewy bodies (AD-LB; 46%), mostly for clinical AD cases. While Braak NFT stage ranged from 0 to 6, Braak aSyn stage was 4-6 or atypical. Thal phase was 0-3 for PD(D) and DLB cases and 4-6 for AD(-LB) cases. ARTAG and CAA were found in 29% and 77% of the cases, respectively. Whereas AD-LB and PD(D) cases regularly showed moderate AMY aSyn pathology and mild or no aSyn pathology in other regions, some PD(D) cases displayed a high aSyn burden in the AMY and mild to moderate burden elsewhere. The AMY also often showed many (pre)tangles in the p-tau and diffuse plaques in the Aβ staining.
Conclusion These brain bank data show that severe psychiatric symptoms, dementia and parkinsonism are common in amygdala-predominant LBD. Moreover, the varying regional burden of aSyn pathology implies that the neuropathological diagnostic criteria should be reconsidered.

P05.04
1 University of Alabama at Birmingham, United States
The interstitial fluid (ISF) and protein aggregates move through the brain extracellular space towards the venous paravascular space, where they are drained out of the brain parenchyma into the cerebrospinal fluid (CSF). Notably, the ISF-CSF clearance (glymphatic clearance) is impaired in the brains of Parkinson’s disease patients, which could contribute to the brain accumulation of α-syn aggregates. The factors that control the ISF transport and CSF clearance of α-syn fibrils in Parkinson’s disease are poorly known. The speed and direction of the ISF diffusion are profoundly affected by the macromolecular obstacles in the brain extracellular matrix, including the negatively charged heparan sulfate (HS) proteoglycans. Here, we investigated the amount of the HSPGs contribution to interstitial flow kinetics and CSF clearance using radiolabeled mouse recombinant α-syn preformed fibrils (PFFs) and positron emission tomography/computed tomography (PET/CT). We found that radiolabeled PFFs diffuse to multiple brain areas, primarily the cortex and lateral ventricles, in the first hour post striatal injection. 25 hours post-injection, fibrils barely moved. Radioactivity in the spinal cord (consequence of glymphatic clearance of the PFFs) was only detected in mice after 72 hours. PET/CT imaging showed faster ISF diffusion and CSF clearance of radioactivity in mice expressing lower neuronal HS sulfation than in wild type littermates. Moreover, using a gamma counter we detected significantly lower levels of radioactivity in the brain and skull of HS mouse mutants as compared to wild type mice. Our studies provide the first in vivo evidence of HS as a host cofactor that controls the kinetics of ISF transport and CSF clearance of α-syn fibrils and suggest that manipulating HS composition in the brain EC matrix is an appealing strategy to slow Parkinson’s disease progression.
P05.05
1 Vall d'Hebron Research Institute (VHIR), Spain
2 University of Barcelona; Department of Biomedical Science, Spain
3 Vall d'Hebron Research Institute (VHIR) and Vall d'Hebron University Hospital, Spain
4 Vall d'Hebron Research Institute (VHIR); Aligning Science Across Parkinson’s (ASAP) Collaborative Research Network; Department of Biochemistry and Molecular Biology, Autonomous University of Barcelona; Catalan Institution for Research and Advanced Studies (ICREA)., Spain
5 University of Barcelona - Department of Biomedical Science, Spain
6 Vall d'Hebron Research Institute (VHIR) and Aligning Science Across Parkinson’s (ASAP) Collaborative Research Network, Spain
Parkinson’s disease (PD) is the second most common neurodegenerative disorder, characterized by progressive motor dysfunction and diverse non-motor symptoms. Mounting evidence supports a crucial contribution of the gut–brain axis to PD pathogenesis, as gastrointestinal alterations and microbial dysbiosis often precede motor onset by several years. Among the microbial components involved in this communication, bacterial extracellular vesicles (BEVs) have emerged as potent mediators of microbiota–host interaction. These nanosized particles transport proteins, lipids, nucleic acids, and metabolites across biological barriers, influencing systemic physiology and potentially contributing to neurodegeneration. Despite their biological significance, the role of BEVs in PD remains largely unexplored.
In this study, we investigated circulating BEVs in PD through an integrated clinical, molecular, and functional approach. BEVs were isolated from the plasma of people with Parkinson’s disease (PwPs) and matched healthy controls from the VHIP cohort using Size Exclusion Chromatography and Density Gradient Ultracentrifugation to ensure high purity. Characterization by flow cytometry, Western blotting, cryo-electron microscopy, and Nanoparticle Tracking Analysis confirmed their bacterial origin and defined morphological and biophysical features. Proteomic and transcriptomic profiling revealed distinct molecular signatures and pathways linked to inflammation, barrier dysfunction, and neuronal stress. Functional assays in epithelial (Caco-2), neuronal (SH-SY5Y), and immune (THP-1) models demonstrated that BEVs modulate cellular responses relevant to PD pathology, including epithelial integrity, immune activation, and α-synuclein–related mechanisms. In vivo administration of labeled BEVs in wild-type and neuromelanin-accumulating (tgNM) mice provided insights into their biodistribution and impact on PD-related molecular networks.
Altogether, this work identifies BEVs as novel players in the gut–brain axis and establishes a powerful translational framework to investigate their clinical potential. By elucidating how microbial vesicles contribute to early pathogenic processes, this study opens new avenues for biomarker discovery and early disease detection. Ultimately, understanding BEV-mediated communication paves the way for preventive and therapeutic disease-modifying strategies.
P05.06
1 University of Alabama at Birmingham, United States
2 University of California, San Diego, United States
Aggregated α-synuclein (α-syn) propagates between neurons and drives neurodegeneration in Parkinson’s disease and dementia with Lewy bodies. Extracellular α-syn contributes to disease progression, but the neuronal receptors mediating its internalization remain unclear. Heparan sulfate proteoglycans (HSPGs) act as receptors for α-syn pre-formed fibrils (PFFs) in immortalized cell lines, mouse primary hippocampal neurons, and, more recently, in iPSC-derived human microglia and dopaminergic neurons. However, the role of HSPGs in neuronal uptake and pathology in vivo remains unknown. We hypothesize that HSPGs interact with α-syn aggregates on the plasma membrane of neurons through the sulfate groups in their HS chains, mediating the neuronal internalization of these pathogenic aggregates. In vitro, primary cortical neurons from NdstSynCre+ mice, which exhibit 33% reduced HS sulfation due to a mutation in Ndst1, the enzyme required for N sulfation of HS chains, show dramatically reduced α-syn PFF uptake compared with NdstSynCre- (wild type) neurons with physiological sulfation. Treatment with heparinase enzymes, which degrade HS chains, or sodium chlorate, which inhibits HS sulfation, produces similar reductions in PFF internalization, indicating that sulfated HS chains are required for neuronal α-syn internalization. To explore the contribution of HS in α-syn pathology in vivo, we injected PFFs into the striatum of NdstSynCre+ and NdstSynCre- mice. At 17 weeks post-injection, NdstSynCre+ mice showed ∼49% less α-syn deposition in the substantia nigra pars compacta (SNpc), ∼60% less in the cortex, and ∼77% less in the hippocampus. NdstSynCre+ mice also displayed reduced motor and anxiety-like behavioral deficits. Importantly, HS sulfation reduction itself does not alter endogenous α-syn expression or behavior in uninjected or α-syn monomer-injected mice. These findings demonstrate that neuronal HSPGs act as functional receptors for α-syn internalization in vivo and identify HSPG biosynthesis as a potential therapeutic target for synucleinopathies.
P05.07
1 Amsterdam UMC, location Vrije Universiteit, Netherlands
Introduction: Lewy bodies (LBs) are neuronal inclusions containing accumulated proteins and lipids, representing the pathological hallmark of Parkinson’s disease (PD). A prominent component of LBs is alpha-synuclein (aSyn), which is an important target for disease-modifying therapies in PD. However, the mechanisms underlying aSyn accumulation in LBs remain unresolved. We have previously described abnormal cytoplasmic retention of TFEB – a key transcription factor for lysosomal clearance of proteins – in PD, particularly in neurons with aSyn pathology. As this potentially reflects a more widespread nucleocytoplasmic transport (NCT) deficit, here, we examine the relationship between various selected NCT markers and aSyn pathology.
Methods: We selected post-mortem substantia nigra tissues from 12 donors with advanced PD (Braak LB stage 5/6) and 11 age-matched controls, which were utilized for multiplex immunohistochemistry. Stained sections were analyzed using high- and super-resolution confocal and STED microscopy, to examine subcellular distribution patterns of NCT markers (e.g., Karyopherins, Ran and TDP-43) and markers for nuclear integrity (Lamin B, nucleoporins), respectively. Nuclear:cytoplasmic ratios for NCT markers were determined using quPath software and statistically analyzed using Mixed Models, comparing neurons with and without LBs. In parallel, we are establishing cell models to study the mechanistic interrelation between NCT disruption and aSyn inclusion formation.
Results: We found that antibodies against all analyzed NCT shuttling proteins showed immunoreactivity in the majority of aSyn inclusions (ranging from 55 to 80%). We found significant reductions in nuclear:cytoplasmic ratios for NCT proteins, including TDP43, in PD neurons with aSyn pathology. STED microscopy revealed that the nuclear integrity of PD neurons with aSyn inclusions was compromised, e.g., by increased nuclear invaginations, while mislocalization and/or decreased densities of Lamin and nucleoporin were particularly associated with mature inclusion morphologies.
Conclusion: We found evidence for compromised nuclear integrity and altered distribution of NCT shuttling proteins in nigral neurons in PD, which was strongly associated with LB pathology. Insights into the mechanistic relation between NCT deficits and aSyn inclusion formation may inspire new therapeutic approaches in PD, as targeting NCT pathways has shown promise in other neurodegenerative diseases such as ALS.
P05.08
1 Barrow Neurological Institute, United States
2 CMK Data, United States
Parkinson's Disease (PD) is a neurodegenerative disorder characterized by motor symptoms (tremors, rigidity, and bradykinesia) alongside non-motor symptoms (cognitive decline and mood disorders). The etiology of PD is multifactorial, encompassing genetic, environmental, and epigenetic factors. Research often relies on molecular biology “-omics” approaches, which enable a system analysis at multiple levels. Part of the power of these approaches is in the large amount of data generated; however, this can lead to hyperfocus in some areas with abandon of others, a loss of divergent method metadata, and confusion over extrapolation feasibility across studies. Succinctly, there is need to incorporate data into a functional shared knowledge space. To accomplish this, we made a hand-curated database that contains information on wet lab methodology, post-laboratory statistical analysis, and final results: PARK-Seq Literature Findings. The database houses results from 41 studies published 2014 through 2025 with transcriptomic (n = 34), proteomic (n = 14), or other (n = 6) data on gene and protein expression in subjects with PD (n =7802), Alzheimer's disease (n = 284), Lewy body disease (n = 13), multiple sclerosis (n = 21), multiple system atrophy (n = 22), progressive supranuclear palsy (n = 49), other neuropathology not specified (n = 85), or control subjects (n = 7418). The study/cohort age range was 0 to 102 years with an mean average of 68 years at death or time of sample extraction. Studies included samples from blood (n = 5), brain gray matter (n = 24), brain white matter (n = 2), CSF (n = 1), induced pluripotent stem cells (n = 4), midbrain (n = 16), subcortical structures (n = 6), and urine (n = 2). Each study had an average of 9 files including the main text, and making this database involved hand curation of 337 files, with a final inclusion of data from 179 figures and tables. Integrating data from -omics approaches fosters a systems biology perspective, revealing complex regulatory networks and potential therapeutic targets. By making this database freely available and open for anyone to use, it is our hope that researchers can find expanded information on genes of interest as well as discover new connections across genes and cohorts
BASIC SCIENCES: Animal models of Parkinson's and Parkinsonism
P06.01
1 Institut de Génomique Fonctionnelle (IGF), Université de Montpellier, CNRS UMR5203, INSERM U1191, Montpellier, France, France
Parkinson's disease (PD) is a neurological disorder caused by degeneration of the dopaminergic neurons of the substantia nigra pars compacta (SNc). Patients with PD have sensory abnormalities accompanied by chronic pain that often precede the onset of locomotor deficits, and that are resistant to motor symptom treatments. The early appearance of sensory deficits questions about the link between pain symptoms and SNc degeneration in PD. Unfortunately, early PD symptoms are difficult to study in humans asymptomatic for motor deficits, and pre-clinical models mostly recapitulate the late phase of the disease. Therefore, there is a need to develop a pre-clinical model adapted to the study of PD-related pain symptoms at the onset of dopaminergic neuron degeneration.
In PD, SNc dopaminergic neurons degenerate primarily through apoptosis following an increase in Caspase-3 activity. Therefore, temporally and locally manipulating Caspase-3 activity in SNc neurons would offer an avenue to study the progressive consequences of dopaminergic neuron apoptosis. To do so, we used local adeno-associated-virus (AAV) viral approach to express a Cre-inducible autocatalytic caspase-3 enzyme (taCasp3) in the SNc of Tyrosine hydroxylase (TH)-CreERt2 genetically modified mice to selectively target dopaminergic neurons. By gradually inducing the expression of taCasp3 expression with increasing tamoxifen doses, we aim to demonstrate the sequential effects of dopaminergic neuron ablation on the sensory and motor symptoms.
The first observations in male and female animals reveals that strong induction of taCasp3 leads to SNc degeneration, causes locomotor deficit, and induces mechanical sensory hypersensitivity. Next, the effects of a progressive targeted dopaminergic neuron ablation with increasing tamoxifen dosage lead to a sequential appearance of somatosensory deficits, including tactile allodynia, largely before the onset of motor symptoms. Pharmacological treatments shows that the use of a brain penetrant T-type calcium channel inhibitor is able to acutely reverse the tactile hypersensitivity in this model.
Potentially, this preclinical approach may offer a better way to recapitulate the course of clinical sensory and motor signs of PD and notably better asses the underlying pain pathophysiological mechanisms and potential new pharmacological treatments efficient for the distinct symptoms of PD.

P06.02
1 Institute of Functional Genomics, University of Montpellier, CNRS, INSERM, Montpellier, France
2 ANSES, University of Lyon, Lyon, France
3 MGX-Montpellier GenomiX, University of Montpellier, CNRS, INSERM, Montpellier, France
4 Toxalim (Research Center in Food Toxicology), INRAE, ENVT, INP-Purpan, UPS, Toulouse University, Toulouse, France
Introduction: Exposure to certain pesticides appears to be involved in metabolic disorders, such as type 2 diabetes (T2D), and Parkinson's disease (PD) onset. T2D and PD belong to the group of "protein misfolding diseases" and are reported to be epidemiologically associated. While the exact causes of this association and the mechanisms linking these diseases are not fully known, it seems important to assess the extent to which environmental factors such as pesticides could be involved. Very few studies have addressed the question of dietary exposure to low-doses of pesticide mixtures. The aim of our study was to evaluate the neuronal and metabolic consequences of chronic dietary exposure to a mixture of pesticides at levels below the Acceptable Daily Intake (ADI) in transgenic mice prone to develop motor disorders.
Methods: Male mice expressing mutated A53T human α-synuclein (M83) and wild-type (WT) mice were fed with a control diet or a diet enriched with 6 pesticides (captan/boscalid/chlorpyrifos/thiachloprid/thiophanate/ziram) for 50 wks. Motor function was assessed using open-field test, and neuropathology with different markers (number of dopaminergic neurons, neuronal inclusions of Ser129P α-synuclein, tyrosine hydroxylase, dopamine transporters levels). Glucose and insulin tolerance tests, plasma insulin assay and pancreas analysis (islet morphometry/transcriptomics) were performed.
Results: Despite no detectable signs of molecular neuropathology, pesticide exposure induced early motor deficits with a reduction in total distance travelled and average speed in M83 mice from 12 wks. Moreover, pesticide exposure led to body weight gain and insulin resistance in both WT and M83 mice, associated with a reduction in hepatic insulin receptor protein levels. While pesticide exposure promoted glucose intolerance in WT mice, M83 mice surprisingly showed improved glucose tolerance accompanied by an increase in pancreatic islet mass and function. Transcriptomic analysis revealed an abundant expression of α-synuclein in M83 islets associated with an enrichment of genes involved in amino acid metabolism.
Conclusion: Our study shows early motor deficits and insulin resistance in α-synucleinopathy mice exposed to pesticides, and points to an unexpected role of α-synuclein in pancreatic islet adaptation to pesticide-induced insulin resistance. It also highlights certain adaptive processes common to the onset of PD and T2D, such as an increase in amino acid metabolism.
P06.03
1 Aarhus University, Denmark
2 University Hospital of Cologne, Germany
3 Aarhus University Hospital, Denmark
4 Linköping University, Sweden
Background Lewy body disorders (LBDs) are characterized by pathological alpha-synuclein (asyn) propagation across the gut-brain axis. In Dementia with Lewy bodies (DLB), up to 85% of cases show amyloid plaques and tau tangles, suggesting DLB should be viewed as a mixed-pathology disorder rather than a pure synucleinopathy. Meta-analysis shows 76% of early DLB cases are misdiagnosed as Alzheimer's Disease (AD) due to shared dementia symptoms, though DLB distinctively features peripheral nervous system dysfunction, similar to body-first Parkinson’s disease (PD). We have previously shown the feasibility of gut-first PD using aged wild-type rodents, but peripheral-to-central propagation with AD co-pathology remains unexplored. Here, we aim to establish a novel “mixed-pathology multi-system” DLB.
Methods Six-month-old Alzheimer Fisher 344 rats (expressing mutant Swedish APP and Δ exon 9 PS1 genes) will receive injections of murine asyn preformed fibrils in the duodenum (60 μg or vehicle, Ngut-first=15, Ncontrol=12). Disease progression will be monitored at 1, 3, and 6 months post-injection. The following multi-disciplinary approach will be used for multi-system disease follow-up: (1) behavioral testing to assess cognitive (novel object recognition), motor (grip strength), hyposmia and autonomic dysfunction (gastroparesis, heart rate variability); (2) PET/MRI imaging using the tracers 18F-MFBG (cardiac innervation), 18F-FDG (cognitive function), 18F-PE2I (dopaminergic integrity), 18F-flortaucipir (tau tangle pathology); and (3) immunohistochemistry (IHC) for quantification of asyn, Aβ and tau pathology in the brain and peripheral tissues.
Results Data collection is ongoing. We anticipate that the AD phenotype in body-first models will exacerbate cognitive and autonomic dysfunction to what we previously observed in wild-type Fisher 344. Preliminary results from imaging studies, as well as initial IHC analysis in brain and peripheral organs at the early disease stage, will be presented at the conference.
Conclusion This model will provide insights into the synergistic role of asyn, Aβ and tau proteins in multi-system dysfunction, and may serve as a platform for developing combinatorial treatment approaches targeting multiple proteinopathies. This work may initiate a paradigm shift from viewing DLB as a ‘brain-centric synucleinopathy’ to a ‘multi-organ mixed proteinopathy,’ potentially enabling intervention at the pre-motor stage for body-first LBDs like DLB.
P06.04
1 Department of Neurology & Neurosurgery, Montréal Neurological Institute, McGill University, Montréal, Canada, Canada
2 Department of Pharmacology and Physiology, Faculty of Medicine, Université de Montréal, Canada, Canada
3 3Institut de Recherches Cliniques de Montréal, Canada, Canada
4 Department of Neurology & Neurosurgery, Montréal Neurological Institute, McGill University, Montréal,Canada, Canada
Background: Parkinson’s disease (PD) is a progressive neurodegenerative disorder defined by dopaminergic neuronal loss in the substantia nigra pars compacta (SNc). While PD is classically characterized by overt motor impairments, a prodromal phase spanning up to two decades is marked by non-motor symptoms such as depression, gastrointestinal dysfunction, and subtle activity and circadian level disturbances. Growing evidence implicates mitochondrial dysregulation and immune mechanisms as central drivers of PD pathophysiology. For example, adoptive transfer of 2C CD8+ T cells, engineered to recognize the mitochondrial antigen oxoglutarate dehydrogenase (OGDH), into PINK1 WT and KO mice, compared to OT-I CD8+ T cells recognizing ovalbumin as a control, induces L-DOPA-reversible dopaminergic neurodegeneration in the SNc, producing Parkinsonism in both genotypes. However, whether this neuroimmune model recapitulates prodromal features of PD remains unknown. Here, we investigated early behavioural alterations following 2C or OT-I CD8+ T cell transfer.
Methods: Male and female PINK1 WT and KO mice received adoptive transfer of 2C or control CD8+ T cell underwent a battery of assays, including automated home-cage locomotion tracking (DVC system), tail suspension tests, and fecal water content analysis to assess locomotor, depressive-like, and gastrointestinal phenotypes.
Results: This study revealed sex-specific outcomes: males showed hyperactivity during sleep onset and sleep phases without overt motor, depressive-like, or gastrointestinal symptoms, whereas females exhibited late-phase wake hypoactivity and mania-like behaviours, also without gastrointestinal changes.
Conclusion: These findings reveal prodromal, sex-specific behavioural phenotypes in a neuroimmune model of PD, providing insights into early disease mechanisms influenced by adaptive immunity that precede irreversible motor impairments.
P06.05
1 Boston University, United States
Glia play an essential role in healthy neural function(1-3), and glial dysfunction, specifically among astrocytes and microglia, is implicated in the exasperation of neuroinflammation in Parkinson’s Disease(4). Microglia, which function as the resident immune cells of the central nervous system and are responsible for regulation of inflammatory signaling and clearance of misfolded proteins(5), undergo distinct state changes under conditions of neuroinflammation(6). However, microglial molecular and morphological changes in the context of Parkinson’s disease are poorly understood both at disease onset and as it progresses. In this study, we evaluated how persistent accumulation of human alpha synuclein (aSyn) in the mouse striatum, achieved via AAV-based overexpression (AAV1/2 Human A53T aSyn), effects motor functions, neuronal death, and changes to local microglia over 12 weeks. Our data show that over three discrete time points of 4 weeks, 8 weeks, and 12 weeks post viral induction (PVI), microglia undergo a progressive morphological reprogramming to display bushy activated morphology as early as 4 weeks (Fig 1b), far earlier than any substantial neuronal loss, which only occurred at 12 weeks PVI. Additionally, microglia at sites of the aSyn accumulation show temporally dependent, increased expression of CD45 followed by CD13 indicative of distinct functional phenotypes (Fig 1c). Therefore, we establish a benchmark for microglial activation states over time in the human aSyn overexpression AAV disease model.
We also investigated the use of published RNA-seq datasets to identify surfaceome proteins that can be used to direct microglia specific targeting of therapeutics. We use an unsupervised screen to assemble a list of highly and uniquely expressed genes that were specific to microglia, astrocytes, and neurons, and one of the identified targets for microglia is Slc2a5, the gene coding for the cell surface fructose transporter Glut5. Thus, our continuing work is exploring the incorporation of fructose into drug vehicles for targeted delivery to microglia.
(1) Khakh, BS. Nat. Neurosci. 18, 942–952 (2015). (2) Salter, MW. Nat. Med. 23, 1018–1027 (2017). (3) Allen, N. Nat. Neurosci. 457, (2009). (4) Kam, T. Neurobiol. Dis. 144, 105028 (2020). (5) Hickman, S. Nat. Neurosci. 21, 1359–1369 (2018). (6) Burda, J.E. Nat. 606, 557–564 (2022).

P06.06
1 The University of Melbourne, Australia
Background: The eye is an extension of the brain and in people living with Parkinson’s disease changes in 3D retinal scans (optical coherence tomography, OCT) have been found. An alpha-synuclein overaccumulation model has been found to recapitulate these OCT changes but the underlying mechanisms driving these and the time course involved is not understood. This study aims to fill this gap by evaluating in vivo OCT over a range of ages and examine the time course of alpha-synuclein, mitochondrial dysfunction and oxidative stress markers in the mouse retina.
Methods: Human alpha-Syn transgenic mice (A53T) mice and wild-type littermates at 3, 5, 8 and 13 months old (n = 9 to 19 per group) underwent OCT imaging (Spectralis®) and western blot analysis of retinal tissue (n = 6/group). Markers of dopamine (Tyrosine hydroxylase,TH), alpha-synuclein (phosphorylated-129,P129) , mitochondrial dysfunction (VDAC), oxidative stress (DJ-1) and inflammation (GFAP) were examined. A two-way ANOVA with Sidak’s post hoc comparisons was conducted. Deming regression with Spearman correlation (rs) were conducted to correlate retinal layer thicknesses with western blot markers.
Results: A53T mice exhibited a thinner total retinal thickness (TRT), but thickening of ganglion cell-inner plexiform layer (GCIPL) and photoreceptor (PR) segments compared to their wild-type littermates (p<0.01 to 0.0001). A significant interaction was found for outer plexiform (OPL) and outer nuclear layer (ONL) thickness, driven by greater thinning with advancing age in A53T mice (p<0.01 to 0.05). Western blot analyses showed elevated levels of a-synand GFAP (p<0.001) in A53T mice compared to WT. An interaction effect was found with DJ1 (p<0.05) . P129 was significantly correlated TRT, OPL, ONL, GCIPL (p<0.05, rs= -0.38, -0.61, -0.53, 0.32), TH correlated with GCIPL (p<0.05, r = 0.30), VDAC with TRT, GCIPL (p<0.05, r = -0.42; -0.52), DJ-1 with PR (p<0.05, rs = -0.37) and GFAP with ONL, TRT (p<0.05 rs = -0.28, -0.39).
Conclusion: This study finds with alpha-synuclein overaccumulation, there is greater inflammation and mitochondrial alterations in the retina which are associated with thinning in OCT layers corresponding to photoreceptors and total thickness, as well as thickening of a ganglion cell layer. In the future, correlation with brain markers and intervention with therapeutics would further facilitate our understanding of the mechanistic drivers of OCT and inform their utility as biomarker for PD.
P06.07
1 Institute of Biomedical Research of Barcelona (IIBB-CSIC), IDIBAPS, CIBERSAM, Spain
2 Institute of Biomedical Research of Barcelona (IIBB-CSIC), IDIBAPS, CIBERSAM, UPV/EHU, Spain
3 Instituto de Biomedicina de Sevilla (IBiS), CSIC, Spain
4 IDIBAPS Experimental 7T MRI Unit, Spain
Background: Depression is a major non-motor symptom in Parkinson's disease (PD), often preceding motor symptoms and severely impacting quality of life. While α-synuclein (α-Syn) pathology is found in serotonergic (5-HT) raphe nuclei early in the disease, its contribution to brain circuit alterations remains unclear. This study investigated the role of the 5-HT system in synaptic plasticity, cellular activity, and functional connectivity in a PD-like mouse model with depressive phenotype.
Methods: A PD-like mouse model with depressive phenotype was induced by AAV-mediated overexpression of human α-Syn in raphe 5-HT neurons. At 8 weeks post-infusion, levels of pre- and post-synaptic markers (SV2A, SYP, VAMP2, PSD95, MAP-2) were assessed in the medial prefrontal cortex (mPFC), caudate-putamen (CPu), and hippocampus (HPC) using immunohistochemistry and Western Blot. For translational validation, these markers were evaluated in postmortem dorsolateral prefrontal cortex (dlPFC), caudate nucleus (CAU) and HPC tissue samples of PD patients at early (Braak 2-3) and late (Braak 5-6) stages. Whole-brain cellular activity was mapped using in situ hybridization for Egr1 mRNA and seed-based analysis of resting-state fMRI (rs-fMRI) was performed to evaluate the functional brain connectivity.
Results: Progressive α-Syn accumulation in the mouse 5-HT system led to regionally specific synaptic pathology and altered cellular activity. Levels of presynaptic SV2A, SYP, and VAMP2 proteins were increased in the mPFC and CPu, alongside a reduction of postsynaptic PSD95; however, these changes were not observed in the HPC. Crucially, the presynaptic alterations were mirrored in tissue from early-stage PD patients. This was accompanied by increased Egr1 mRNA expression in cortico-limbic areas, but a significant decrease in the raphe nuclei. Functionally, rs-fMRI analysis revealed widespread hypoconnectivity, with seed-based analysis showing reduced coupling of the mPFC, CPu, and HPC with their cortical and subcortical targets.
Conclusion: Our findings provide evidence linking 5-HT system-specific α-synucleinopathy to early synaptic pathology and a functional network disruption affecting key networks in emotional regulation. The validation of these synaptic changes in early-stage human PD highlights their translational potential as biomarkers for depression risk in PD patients and establishes our mouse model as a key tool for testing therapies targeting non-motor symptoms.
P06.08
1 University of Iowa, United States
2 University of Wisconsin-Madison, United States
Vagally mediated functions, such as gastrointestinal (GI) motility, swallowing, and vocal communication, are affected early in Parkinson disease (PD). These signs are highly prevalent, debilitating, and often emerge years before clinical diagnosis, substantially reducing quality of life. Despite their clinical significance, they are rarely identified or treated in early disease stages and do not respond to dopaminergic therapies, limiting current treatment efficacy. Moreover, sex-based differences in PD manifestation are well documented but understudied in translational models.
To address these gaps, we examined vagally and non-vagally mediated behaviors in the Pink1-/- rat, a validated genetic model of early-onset PD. At four months of age (reflecting the prodromal stage prior to dopaminergic depletion) male and female Pink1-/- and wild-type (WT) rats were assessed for vocal communication (ultrasonic vocalizations), swallowing and GI function (videofluoroscopy), and limb motor performance (tapered balance beam). We hypothesized that Pink1-/- rats would exhibit significant impairments in vagal functions relative to WT controls, with males showing more pronounced deficits, and that vagal behaviors would be more affected than limb motor function.
Results supported these hypotheses: Pink1-/- rats demonstrated significant deficits in GI motility and semi-solid swallowing (p<0.05), as well as some changes in vocal communication, while limb motor function remained largely preserved (p>0.05). Sex-specific differences were most evident in GI outcomes, with Pink1-/- males exhibiting the greatest impairments. Interestingly, sex differences in vocalizations observed in WT rats were absent in Pink1-/- rats.
These findings indicate that vagally mediated functions are disrupted early in PD pathogenesis, preceding hallmark motor signs. Recognition of genotype- and sex-specific patterns of prodromal dysfunction enhances understanding of disease progression and underscores the potential of vagal biomarkers for earlier diagnosis and targeted interventions.
P06.09
1 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark. Department of Pathology, Aarhus University Hospital, Aarhus, Denmark., Denmark
2 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark,. Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
3 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
4 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
5 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
6 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
7 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Denmark
8 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
9 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark. Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
10 Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
11 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark. Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
12 Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
13 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark. Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
Parkinson’s disease (PD) patients exhibit contradictory autonomic symptoms (hypotension/hypertension, constipation/dumping), suggesting differential involvement of parasympathetic and sympathetic nervous systems. Despite the emergence of novel theories such as the body-first and brain-first PD subtypes, the temporal patterns of parasympathetic vs. sympathetic involvement remain unclear among these subtypes. We investigated the spatiotemporal distribution of alpha-synuclein (asyn) pathology in animal models of both subtypes, correlating findings with cell-type-specific degeneration and functional deficit.
Fourteen-month-old Fisher 344 rats received injections of murine asyn preformed fibrils in the amygdala (10μg, nbrain-first=20) or duodenum (60μg, ngut-first=20). Control rats (nbrain-sham=8; ngut-sham=7) received vehicle injections. Animals were examined at 1 and 6 months post-injection (mpi) in heart and stomach using multiplex immunolabeling to (1) map distribution of phosphorylated asyn, (2) co-localize with cholinergic (ChAT+) vs. sympathetic (TH+) components, (3) correlate with measures of gastroparesis and awake blood pressure measurements.
At 1 mpi, brain-first rats showed pathology in vagal-dense fundic region only, while gut-first rodents displayed significant pathology across all stomach regions and heart. Asyn pathology was associated to enteric cholinergic denervation in both groups but noradrenergic cardiac deficit only in gut-first animals (6mpi). Notably, early sympathetic hyperinnervation was observed in GF at 1mpi and in BF at 6mpi. These distinct pathological patterns correlated with corresponding phenotypes: severe gastroparesis with early hypotension in gut-first rats, and moderate gastroparesis with early hypertension in brain-first animals.
Our findings reveal distinct autonomic involvement patterns between PD subtypes: brain-first models show top-down CNS propagation with pathology limited to vagal-dense forestomach, while gut-first models exhibit early involvement of both autonomic systems. We also observed remodeling and plasticity of the sympathetic nervous system preceding denervation, highlighting the unique role of the sympathetic nervous system in PD pathophysiology. Collectively, our data support the hypothesis that PD comprises distinct subtypes with different pathological origins and progression patterns, which may necessitate tailored therapeutic approaches targeting the specific autonomic pathways affected in each subtype.
P06.10
1 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark., Department of Pathology, Aarhus University Hospital, Aarhus, Denmark., Denmark
2 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
3 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark, Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
4 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark., Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
5 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark., Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
6 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
7 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark. Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
8 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark., Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
9 Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark., Denmark
10 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Biomedicine and DANDRITE-Danish Research Institute of Translational Neuroscience, Nordic-EMBL Partnership for Molecular Medicine, Aarhus University, Aarhus, Denmark., Denmark
11 Department of Clinical Medicine, Aarhus University, Aarhus, Denmark., Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
12 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark Department of Clinical Medicine, Aarhus University, Aarhus, Denmark Department of Nuclear Medicine and PET, Aarhus University Hospital, Aarhus, Denmark, Denmark
13 PACE - Lundbeck Foundation Parkinson's Disease Research Center, Aarhus University, Denmark., Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Core Center for Molecular Morphology, Department of Clinical Medicine, Aarhus University, Aarhus, Denmark, Denmark
Background Alpha-synuclein (asyn) pathology may originate in the peripheral nervous system or brain, leading to distinct clinical subtypes in Parkinson’s disease (PD). The Synuclein-Origin Connectome (SOC) model proposes that pathological asyn aggregates spread trans-synaptically along neuronal networks from initial seeding sites. The vagus nerve represents a critical bidirectional pathway connecting the peripheral and central nervous systems, potentially explaining different patterns of disease progression based on origin site.
Methods Aged wild-type Fisher 344 rats received injections of murine asyn preformed fibrils either in the amygdala (10 μg, “brain-first” model, n = 20) or duodenum (60 μg, “gut-first” model, n=20). Control rats (brain, n = 8; gut n = 7) received vehicle injections. Animals were sacrificed at 1, 2-3 and 6 months post-injection. Vagus nerves and brains were dissected for immunohistochemical analysis of Ser129 phosphorylated asyn pathology, with quantification of load, distribution and laterality of pathological deposits.
Results Gut-first rats displayed dense pathological deposits bilaterally in the vagus nerves with higher overall levels of pathology compared to brain-first rodents at equivalent timepoints. In contrast, brain-first rats showed deposits in both vagus nerves, but with one nerve consistently more affected, even at later time-points. This asymmetric pattern corresponds with the unilateral brainstem pathology that persists throughout disease progression in the brain-first model.
Conclusion Temporal analysis revealed distinct vagal propagation patterns depending on initial seeding location. The persistent asymmetry in brain-first models compared to bilateral involvement in gut-first models may explain clinical heterogeneity in PD, with more asymmetric motor phenotype and slower overall disease progression in brain-first PD due to predominant unilateral vagal involvement. In contrast, severe bilateral vagal involvement in gut-first PD may explain the less asymmetric motor phenotype and faster overall disease progression. Our findings provide the first mechanistic proof of the SOC model of asyn propagation and suggest that neuroanatomical connectivity patterns critically influence disease progression trajectories, with important implications for early diagnosis and prognosis.
P06.11
1 Weill Cornell Medicine, United States
Parkinson’s disease (PD) affects non-motor circuits involved in emotional processing and learning. The amygdala integrates emotional and sensory information, yet circuit-level changes remain poorly understood and may differ by sex in PD. We used the mouse model in which wild-type C57BL/6 mice received striatal injections of α-synuclein preformed fibrils (PFFs); controls received α-synuclein monomer. Mice were euthanized, and brains sectioned at 1 and 8 months post-injection. Multifluorescent immunolabeling was used to quantify synaptic markers in the amygdala. Markers included VGLUT1 and VGLUT2 (excitatory presynapses), HOMER1 (excitatory postsynapses), colocalized VGLUT1–HOMER1 (cortical–amygdala connectivity), colocalized VGLUT2–HOMER1 (thalamic–amygdala connectivity), and phosphorylated synuclein as a pathology marker. Sections were imaged using a fluorescent microscope and puncta quantified in QuPath/ImageJ/Synbot. Marker quantification showed time-dependent, sex-specific changes in amygdala synapses. Completion of this work is currently undergoing. . . Future work will also map phosphorylated synuclein to affected synapses, assess morphology alongside density, and integrate input-specific changes with behavior, with sex as a biological variable.
P06.12
1 U of A: Cowen Lab, United States
2 University of Arizona, United States
3 University of Arziona, United States
4 University of California San Diego, United States
5 University of Arzioan, United States
Introduction: The most visible motor symptoms of Parkinson’s disease (PD) include tremor, bradykinesia and rigidity. More subtly, patients with PD see deficits in fine motor control, sometimes manifesting as dysgraphia or smaller handwriting. While animal research in PD often focuses on gross motor movements, fine motor tasks are relatively understudied.
Methods: Here, we used a string-pulling paradigm, where male rats (n=8) pull a string for a food reward to measure fine motor changes after unilateral 6-hydroxydopamine (6-OHDA) lesion. Then, using fiber photometry , we looked at dopamine (DA) dynamics using GRAB-DA in the dorsolateral striatum (DLS) during string pulling and compared motor deficits induced by 6-OHDA lesion to differences in dopamine levels.
Results: We found that, after unilateral 6-OHDA lesion, rats pulled less total string in a 30 min session. Paw speed decreased in both the intact and lesioned paws; however, the ratio of lesioned paw speed to intact paw speed showed that the lesioned paw showed a greater decrease. We also found that the lesioned paw decreased its reach range, defined as the maximum Y position in a pull minus the minimum. One of the benefits of our novel string-pulling task is that we can extract detailed information about different phases of movement. String pulling can be segmented in reaching (release and upward reach) and withdrawal (grip and downward pull). We found that reaching speed was more impacted by 6-OHDA lesion than withdraw speed. We then measured DA dynamics in 3 intact rats during string pulling with fiber photometry in the DLS, known for controlling motor behaviors. We found that the onset of a string pulling was associated with an increase in DA levels, with larger DA changes leading to faster and stronger pulls. We also investigated whether DA had a greater role during reaching or withdrawal. We found that DA fluorescence was most intense during the withdrawal phase and relatively low during reaching. However, we found that the change in DA activity during withdrawal was negatively correlated with string tension, but positively correlated with subsequent reach distance, suggesting a ramping up of DA before reaching.
Conclusion: Taken together, these results indicate that DA is particularly correlated with pulling speed and reaching in this task, mirroring changes in movement seen during severe dopamine deficit induced by 6-OHDA lesion.
Funding: NIH R01 NS122805
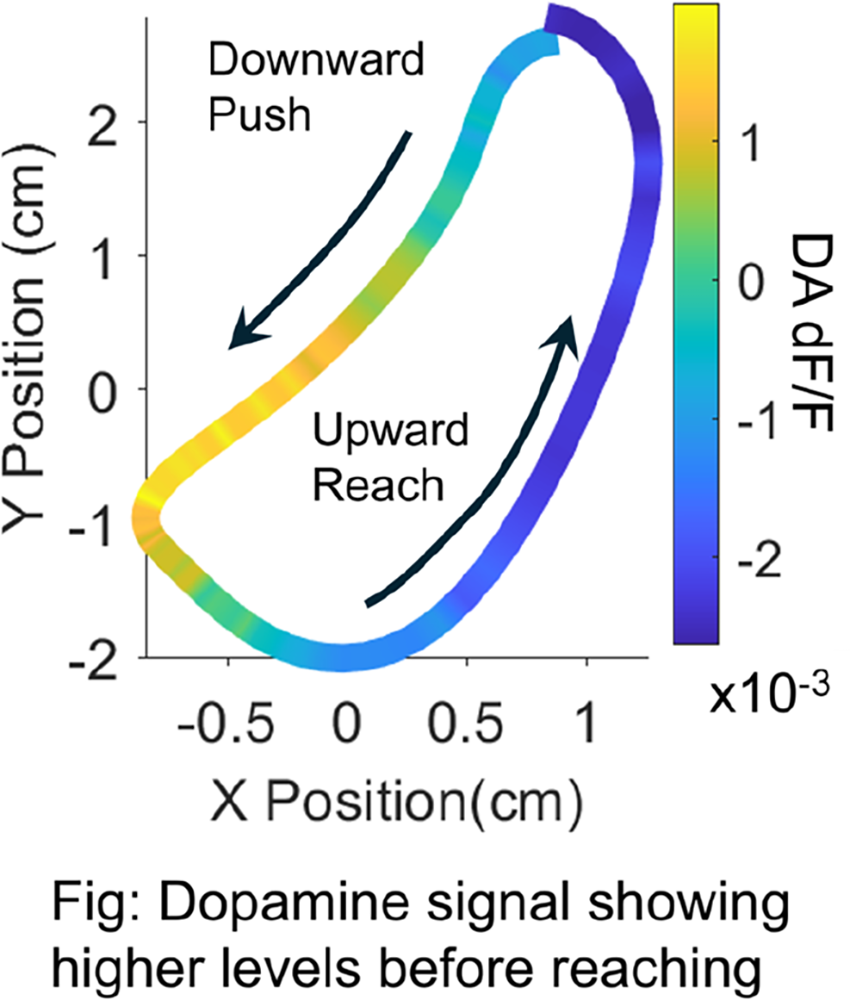
P06.13
1 University of Arizona, United States
2 University of California San Diego, United States
Parkinson’s Disease (PD), characterized by loss of dopaminergic neurons in the substantia nigra pars compacta, includes symptoms such as bradykinesia, rigidity, and tremors. These deficits are often treated with Levodopa (L-DOPA) as dopamine replacement therapy. Although gross motor deficits in PD are well identified, fine-motor deficits are less defined; and the extent to which L-DOPA restores dexterity and skilled movement is unclear. Clarifying PD’s effects on fine-motor control, and L-DOPA’s contribution to skill recovery, can assist targeted therapies. We utilized a toxin-based rat model of PD and a novel behavioral task to assess fine-motor function. We hypothesized that the PD condition would significantly impair fine-motor control and that these deficits could be partially recovered with L-DOPA.
Sprague Dawley rats (N=12 males) underwent 14 days of string-pulling training. After reaching proficiency, the rats were injected with 6-hydroxydopamine (6-OHDA) in the right medial forebrain bundle. Post-recovery, the rats were re-trained for 14 days. Video recordings were obtained 3 days before the lesion and on the last 3 days of the re-training period using a high-speed video camera. L-DOPA (6mg/kg) & Benserazide (15mg/kg) were then injected IP, and the rats were recorded for 4 more sessions. Recordings were processed using DeepLabCut and analyzed in MatLab. Distances pulled were acquired using SpikeGLX via a rotary encoder.
The 6-OHDA lesion severely disrupted paw trajectories, pulling speeds, and overall pulling performance, which were partially recovered with an acute L-DOPA injection. Total distance pulled decreased following the lesion and was subsequently increased following L-DOPA. The lesion reduced rats’ reaching distances in the y-axis with no effect on x-axis sway. Interestingly, when phases of pulling were separated into reach and withdraw periods, the reach period had separation of paw speeds, with the left paw decreasing in speed post 6-OHDA. The right paw additionally appeared to compensate for the left by pulling faster immediately into the bout. Post L-DOPA, paw speed appeared to match more closely in the reach phase, however, we are unsure if this is L-DOPA-induced or the rat’s adaptability to motor deficits.
We would like to assess motor deficits independent of motivation, in tasks such as the Rotarod or Treadmill tests. We would also like to incorporate an effort sensor into the pulling machinery and obtain a group of saline sham rats.
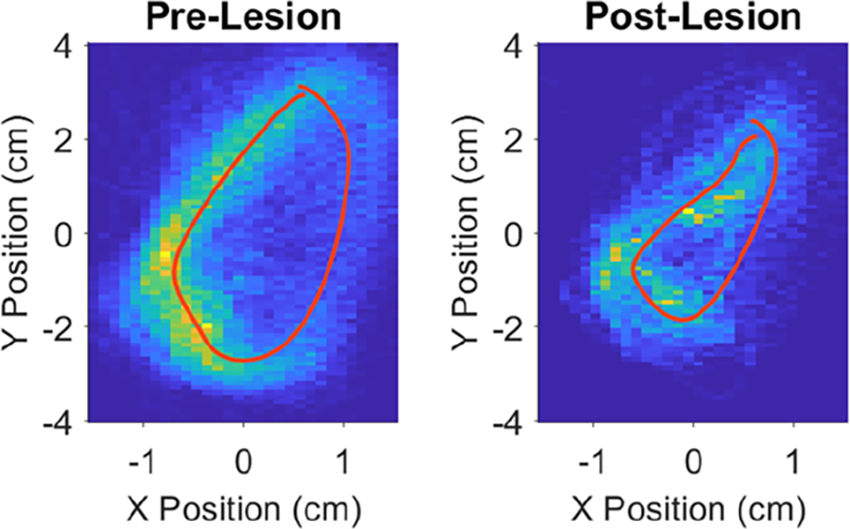
P06.14
1 VHIR Vall d'Hebron Institut de Investigación, Chile
2 VHIR Vall d'Hebron Institut de Investigación, Spain
Introduction: Parkinson’s disease (PD) involves alterations in both the central and peripheral nervous systems, including metabolic and intestinal dysfunction. However, available models fail to fully reproduce these dimensions of the pathology.
Methods: In this study, we characterized the peripheral phenotype of neuromelanin-producing transgenic mice (tgNM), a model that faithfully mirrors human PD pathophysiology by reproducing the progressive, age-dependent accumulation of neuromelanin in catecholaminergic neurons
Results: TgNM mice exhibited gastrointestinal dysfunction in the prodromal phase before the appearance of dopaminergic dysfunction. These functional alterations correlated with an altered composition of the fecal microbiome and metabolome, as well as increased fecal and intestinal inflammation markers. These changes intensified with age, reflecting the progressive nature of the Parkinsonian phenotype. Significantly, chronic exposure to a high-fat diet worsened metabolic, inflammatory, and neurodegenerative manifestations, demonstrating that metabolic stress plays a role in neuronal vulnerability and accelerates disease progression.
Conclusion: The tgNM model represents a robust preclinical tool that naturally replicates both the central and peripheral symptoms of PD, including its metabolic and intestinal aspects, offering a unique experimental platform to investigate early pathogenic mechanisms and to evaluate disease-modifying treatments. Our findings also emphasize the vital role of the gut–brain axis in PD progression and open new therapeutic avenues targeting metabolic and intestinal imbalances in Parkinson’s disease.
P06.15
1 University of Arizona, United States
2 Michigan State University, United States
Introduction: Parkinson’s disease (PD) is a progressive disorder that, in addition to its cardinal motor symptoms, often also presents with depression and pain. Levodopa (L-DOPA) effectively improves motor symptoms but not non-motor symptoms, and chronic use can lead to L-DOPA-induced dyskinesia (LID). We previously showed that sub-anesthetic ketamine treatment (20 mg/kg, 5 doses, 2-hrs apart over 10-hrs) reduced established LID in the standard rat model acutely, and long-term effects were seen for >50 days post-ketamine treatment. This was mirrored in our recent Phase 1 clinical trial (NCT06021756) with LID still significantly reduced from baseline at 3-month post sub-anesthetic ketamine infusion. Since long-term effects of ketamine can vary in the context of a brain-derived neurotrophic factor (BDNF) single nucleotide polymorphism in other disease models (e.g., the long-term antidepressive effect of ketamine is blocked), this study assessed whether ketamine reduces LID in rats expressing the BDNF Val/Met polymorphism.
Methods: To test ketamine’s effects on established LID, we used 13-month-old male Sprague-Dawley rs6265 knock-in rats with moderate unilateral 6-hydroxydopamine lesions. LID was induced by two weeks of daily 12 mg/kg L-DOPA injection (i.p.; with 14 mg/kg benserazide), followed by increasing doses, first to 50 mg/kg L-DOPA and then to 72 mg/kg L-DOPA (n = 9).
Results: Three L-DOPA baseline testing sessions 3-4 days apart showed stable abnormal involuntary movements (AIMs) with mean scores >30. Rats then received ketamine (20 mg/kg) over a 10-hr period (5 i.p. injections, 2-hrs apart), followed immediately by L-DOPA (72 mg/kg), and AIMs were scored. AIMs retesting with L-DOPA (72 mg/kg) was done every 3–4 days. We report here on a 11-day post-treatment period, and the study is still ongoing. The results show that ketamine effectively alleviated established LID acutely by more than 50%, and a sustained long-term reduction in LID was still observed in the following testing days. The effect size was slowly getting smaller, and at day 11 post-ketamine treatment a ∼20% reduction of AIMs was still present.
Conclusion: In summary, the acute and long-term anti-dyskinetic activities of ketamine are largely maintained, and the ongoing study will reveal if the timeline of long-term anti-LID effects is reduced compared to our prior work in wild type LID rats. This work further supports the repurposing of sub-anesthetic ketamine for individuals with LID.
P06.16
1 Department of Neurology, Kyoto University Graduate School of Medicine, Japan
2 Department of Neurology, Kyoto University Graduate School of Medicine, Department of Neurological Disease Control, Osaka Metropolitan University Graduate School of Medicine, Japan
3 Central Research Laboratory, Hamamatsu Photonics K.K., Japan
4 Sumitomo Pharma Co., Ltd., Japan
5 Kyoto University Institute for the Advanced Study of Human Biology, Department of Physiology and Neurobiology, Kyoto University Graduate School of Medicine, Japan
6 Department of Physiology and Neurobiology, Kyoto University Graduate School of Medicine, Japan
7 Department of Therapeutics for Multiple System Atrophy, Kyoto University Graduate School of Medicine, Japan
8 Kyoto University Research Administration Center (KURA), Japan
9 Human Brain Research Center, Kyoto University Graduate School of Medicine, Laboratory of Neuropsychopharmacology, Faculty of Pharmaceutical Science, Kobe Gakuin University, Japan
Background: The impairment of mitochondrial complex I (MC-I) is involved in the pathogenesis of Lewy body disease (LBD) including Parkinson’s disease and Dementia with Lewy bodies. Recently, we developed a non-human primate model of LBD by inoculating alpha-synuclein (αSyn) preformed fibrils (PFFs) into the olfactory bulb (OB), which exhibits the propagation of αSyn aggregates via the olfactory system and the widespread reductions in brain glucose utilization from 3 months after inoculation as detected by 18F-FDG-PET (Sawamura M et al., Mov Disord. 2022). In this study, we performed 18F-BCPP-EF-PET to measure MC-I activity and 18F-FDG-PET to assess reginal glucose utilization, in order to investigate their relationship with αSyn pathology.
Methods: We inoculated αSyn PFFs into the bilateral OBs of four adult marmosets, and 18F-BCPP-EF-PET and 18F-FDG-PET were performed before and 1, 3, 6, 9 and 12 months after αSyn inoculation. Immunohistochemical analysis for phosphorylated αSyn (p-αSyn) has been performed after the last PET imaging, and a regression analysis of PET images has been performed for temporal changes from pre-inoculation to 12 months post-inoculation. We analyzed the correlation between the severity of αSyn pathology in regions of interest (ROIs) based on the marmoset standard brain atlas and the rate of change of standard uptake value ratio (SUVR) using whole-brain activity as the reference at 12 months to the baseline in each PET scan.
Results: We observed abundant p-αSyn aggregates mainly in the olfactory pathway, with some of these aggregates colocalized with mitochondrial markers. PET image analysis showed time-dependent decline in MC-I activity in the prefrontal area, piriform cortex, and amygdala while glucose utilization decreased particularly in the occipital lobe. αSyn pathology was significantly negatively correlated with MC-I activity (rs = -0.35, p < 0.0001), but was not correlated with glucose utilization, which indicated that αSyn aggregation was associated with mitochondrial dysfunction.
Conclusions: We demonstrated that αSyn pathology is associated with MC-I dysfunction in a non-human primate model of LBD. 18F-BCPP-EF-PET is potentially an excellent biomarker of LBD correlated with disease-associated αSyn aggregates.
P06.18
1 Sanofi, United States
2 Sanofi, France
3 The University of Dundee, United Kingdom
Genetic variants in the LRRK2 gene, which encodes leucine-rich repeat kinase 2 (LRRK2), are associated with the onset of both familial and idiopathic Parkinson’s disease (PD). Pathogenic LRRK2 variants including the most prevalent G2019S mutant increase LRRK2 kinase activity. Recent observations of increased LRRK2 kinase activity in idiopathic PDs suggest LRRK2 kinase inhibition as a compelling therapeutic approach for both familial and sporadic PD. Here we described a highly brain penetrant small molecule LRRK2 kinase inhibitor showing potent inhibition of LRRK2 kinase activity in primary cells, rodents, and non-human primates (NHP). This inhibitor demonstrated functional rescue of lysosomal defects in cellular models. Interestingly, we observed an indirect pharmacokinetic-pharmacodynamic (PK-PD) relationship of this compound in NHP, but not in rat. Chronic dosing with the small molecule LRRK2 inhibitor caused LRRK2 protein depletion, resulting in sustained inhibition of LRRK2 activity in NHP even after clearance of the compound. We developed an in vitro PK-PD model using primary PBMC cultures which recapitulated these cross-species differences and demonstrated a congruous PK-PD relation between human and NHP. Finally, we defined the minimal active dose of this LRRK2 inhibitor in NHP with the inhibitory effect mostly driven by total LRRK2 depletion. Our work on LRRK2 inhibitor provides a roadmap for LRRK2 inhibition-based therapeutic programs.
Disclosures: This study was funded by Sanofi. Authors as Sanofi employees may hold shares and/or stock options in the company. All in vivo studies were conducted according to IACUC approved protocols in an accredited institution following institutional, local, state, and country requirements.
P06.19
1 Department of Otolaryngology - Head & Neck Surgery, University of Wisconsin-Madison, United States
2 Department of Communication Sciences & Disorders, University of Northern Colorado, United States
3 Perelman School of Medicine, University of Pennsylvania, United States
Introduction Dysphagia in Parkinson disease (PD) is caused by lingual dysfunction and is associated with increased mortality. Peripheral nervous system pathogenesis highlights the need to study muscle morphology, function, and exercise to preserve swallow function. The validated Pink1-/- rat model enables controlled translational investigations to address these gaps in knowledge. Our previous work showed early swallowing deficits (4-6mo) and increased tongue force with altered myofiber composition in extrinsic tongue muscles in Pink1-/- compared to wildtype (WT) controls. Here, we tested the hypotheses that (1) lingual neuromuscular junction (NMJ) morphology and muscle contractile properties are impaired in Pink1-/- rats compared to WT controls (10mo), (2) 8 weeks of tongue exercise mitigates this by improving NMJ integrity and muscle contractile properties in the genioglossus (GG) and styloglossus (SG) muscles.
Methods 21 Long-Evans male Pink1-/- rats were randomized to either 8 weeks of lingual exercise (n=13) or sham exercise (n=8) and compared with non-exercised WT (n=16). GG and SG were stimulated to measure protrusive/retrusive tongue contractile properties (twitch/tetanic forces (mN), contraction and decay times (ms)), then processed for immunofluorescent labeling (endplates, nerve terminals), and imaged for NMJ morphology (nerve terminal and endplate area (µm2) and volume (µm3), %-overlap, endplate dispersion). Dependent variables were tested via one-way ANOVAs (α=.05) across Pink1-/- exercise and control groups.
Results Pink1-/- sham rats showed greater retrusive twitch force (p<.02), longer contraction times (p<.02), and longer protrusive twitch decay time than WT (p=.04). Exercise did not affect contractile properties. GG NMJ morphology: Compared to WT, Pink1-/- sham rats displayed greater fragmentation (p<.01) and endplate dispersion (p<.05). Pink1-/- lingual exercise attenuated these differences with larger, more organized motor endplates (p<.02) and reduced NMJ disruption (p<.03) compared to no exercise.
Conclusion Pink1-/- rats showed altered GG NMJ morphology (smaller, fragmented, less overlapping motor endplates) at 10 months. Lingual exercise partially rescued these morphologic changes but did not change muscle contractile properties. Further research is needed to optimize exercise paradigms and to better understand the mechanisms underlying peripheral plasticity in PD models.
BASIC SCIENCES: Brain physiology, electrophysiology and circuitry
P07.01
1 University of South Dakota, United States
Gait dysfunction, particularly freezing of gait (FOG), is a debilitating symptom in Parkinson's disease (PD). Despite advances in pharmacological and surgical treatments, effective management of gait disturbances in PD remains a significant challenge. Recent studies have implicated the cerebellum in the pathophysiology of PD, particularly in relation to motor symptoms. Our study explored mid-cerebellar neural activity as a potential biomarker and therapeutic target for PD-related gait deficits. We examined theta-band oscillations (4-7 Hz) in the mid-cerebellum during walking tasks in three groups: PD patients with FOG (PDFOG+), PD patients without FOG (PDFOG–), and healthy age-matched controls. PDFOG+ subjects exhibited significantly reduced mid-cerebellar theta power during walking tasks compared to other groups. Furthermore, 5 Hz repetitive transcranial magnetic stimulation (rTMS) applied to the mid-cerebellum in PDFOG+ participants increased mid-cerebellar theta power and improved gait kinematics compared to sham rTMS. These results suggest a link between mid-cerebellar theta activity and gait disturbances in PD and indicate that rTMS may be a promising approach to enhance mid-cerebellar networks and improve gait dysfunction in PD patients.
P07.02
1 Ecole Normale Supérieure, France
Levodopa remains the gold-standard symptomatic treatment for Parkinson’s disease, but its prolonged use often leads to Levodopa-induced Dyskinesia (LID), a major source of disability. Despite its prevalence, effective therapies for LID are lacking. While research has largely focused on maladaptive plasticity within cortico-striatal networks, the contribution of the cerebellum, closely connected with forebrain motor circuits through thalamo-cortical and thalamo-striatal pathways, has been underexplored. Recent preclinical findings suggest that Purkinje cells, the sole output of the cerebellar cortex, theta-burst stimulation (TBS) may represent a promising anti-dyskinetic strategy. This specific TBS, has been shown to induce a robust and lasting reduction of LID. However, the underlying mechanisms and the cerebellar contribution to LID remain largely unknown.
We hypothesized that the therapeutic effect of cerebellar TBS is mediated by the propagation of theta rhythms through cerebello-forebrain circuits. To test this, we examined whether: (1) connectivity between Purkinje cells and deep cerebellar nuclei (DCN), the sole output of the cerebellum, is altered in LID; (2) cerebellar output to the motor cortex and striatum is disrupted; and (3) direct DCN stimulation is sufficient to reduce dyskinesia. Using a validated murine model of LID, we combined cerebellar optogenetic stimulation with in vivo electrophysiological recordings in freely moving animals, targeting the DCN, thalamus, striatum, and motor cortex to assess functional connectivity across these circuits.
We found that LID is associated with impaired intra-cerebellar connectivity and weakened cerebello-thalamo-striatal communication. The reduction in cerebello-thalamic connectivity shows a strong correlation with LID severity. Importantly, optogenetic TBS of the DCN markedly reduced dyskinesia without compromising the therapeutic benefit of Levodopa. These findings highlight a previously underestimated cerebellar contribution to LID, from both mechanistic and therapeutic perspectives. They demonstrate that cerebellar output TBS can effectively alleviate abnormal involuntary movements, pointing to a novel, clinically relevant strategy that may improve the quality of life of patients. Ongoing work is determining how cerebellar TBS modulates altered network connectivity.
P07.03
1 Institute of Neurodegenerative Diseases, France
Parkinson’s Disease (PD) is characterized by the progressive degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc), leading to both motor and non-motor symptoms, including pain disorders. The subthalamic nucleus (STN), a key structure within the basal ganglia, plays a crucial role in the circuit by influencing output structures of the system and also cortical areas, as its neurons project directly to the cortex. While the STN is known to be involved in both motor and nociceptive functions, the specific contribution of STN-cortical projections to these functions remained unexplored. The present study aimed to investigate the anatomo-functional organization of direct STN-M1 cortical pathways in both normal and parkinsonian conditions, using a combination of chemogenetic and optogenetic approaches alongside with behavioral studies and in vivo electrophysiology in the Vglut2-cre mice. The first results show that selective chemogenetic inhibition of STN glutamatergic neurons, as confirmed by in vivo extracellular electrophysiological recordings, significantly improved motor and nociceptive deficits in parkinsonian mice. This supports the hypothesis that the beneficial effect of therapies like the STN deep brain stimulation (DBS) proceed from an inhibitory action over this nucleus. More importantly, our research shows that specific inhibition of the STN-M1 pathway produced similar effects, correlating with a restoration of neuronal activity in the M1 cortical motor area. We also demonstrate that M1 cortical neurons are implicated in nociceptive processes, and the alteration of these processes correlates with a disruption in the response of these neurons. These results reveal for the first time the importance of the STN-M1 pathway in the pathophysiology of PD and its potential therapeutic implications, contributing to the development of more precise targeted treatments with reduced side effects.
P07.04
1 University of Arizona, United States
Introduction: Brain oscillations are thought to be markers for synchrony within and across brain regions. The phase of an oscillation can time individual neuron firing (phase-locking) and other oscillations (e.g. phase-amplitude coupling). In Levodopa-induced dyskinesias (LID), a debilitating side-effect of levodopa (L-DOPA) treatment for Parkinson’s disease (PD), a characteristic pathological synchrony is in the 70-90 Hz range, called fine-tuned gamma oscillations. Previous work has suggested a desynchronization of motor cortex activity during LID marked by low neuronal phase locking, reduced cross-frequency coupling, and reduced coupling to movement. Our goal was to understand the synchronous and asynchronous oscillatory activity during LID and how sub-anesthetic ketamine might work to alleviate LID symptoms. Recent studies in animal models indicate that low-dose ketamine reduces LID without interfering with the effectiveness of L-DOPA treatment. However, ketamine’s effects on oscillatory synchrony are unclear, with studies showing both oscillatory synchrony across brain regions and localized desynchrony in gamma band activity and neuronal firing. We predicted that ketamine would selectively increase phase-amplitude coupling to gamma frequencies in a dopamine depleted state to reverse decreased oscillatory coupling during LID. Methods: We implanted electrodes bilaterally in the motor cortex (AP:1.5, ML:+/-2.2mm) of 6-hydroxydopamine hemi-lesioned PD rats that were treated daily with L-DOPA (12mg/kg for ≥10 days) to induce LID. LID (n=5) and sham-lesioned (n=5) animals were administered L-DOPA (12mg/kg, i.p.) or saline followed by ketamine (20mg/kg, i.p.). Results: Preliminary data showed that during LID there was decreased neuronal phase locking to any frequency, and marginal reduction in theta and gamma phase-amplitude coupling in the dopamine depleted hemisphere, supporting the desynchronization hypothesis. We found that ketamine administration during LID significantly increased theta (5-11 Hz) and high gamma (74-140 Hz) phase-amplitude coupling in only the dopamine depleted hemisphere. This effect was not a result of overall increase in theta power but was correlated with ketamine’s ability to reduce behavioral symptoms of LID and LID-induced fine-tuned gamma oscillations. Thus, ketamine’s ability to selectively restore phase-amplitude coupling could be a mechanism for improving synchrony in the motor cortex and reducing abnormal movements during LID.
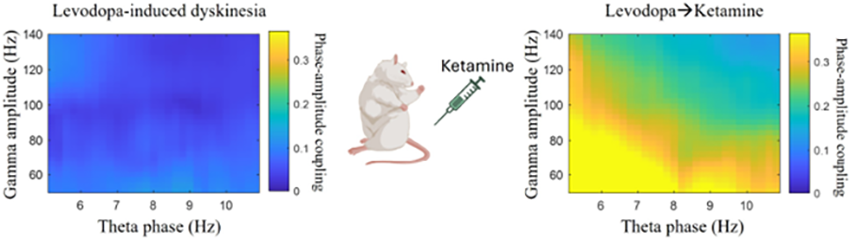
P07.05
1 Human Anatomy and Embryology Department, Faculty of Medicine, University of Valencia, Valencia, Spain / Institute of Biomedical Research of Barcelona (IIBB), Spanish National Research Council (CSIC), Barcelona, Spain / August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain / Biomedical Research Networking Center for Mental Health (CIBERSAM), ISCIII, Madrid, Spain, Spain
2 Institute of Biomedical Research of Barcelona (IIBB), Spanish National Research Council (CSIC), Barcelona, Spain / August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain / Biomedical Research Networking Center for Mental Health (CIBERSAM), ISCIII, Madrid, Spain, Spain
3 August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Barcelona, Spain, Spain
4 Human Anatomy and Embryology Department, Faculty of Medicine, University of Valencia, Valencia, Spain, Spain
Parkinson’s disease (PD) is a motor disorder, although it is now recognized that non-motor symptoms can precede the onset of motor manifestations and constitute a significant component throughout all stages of the disease. Among these, depression and anxiety are the most prevalent symptoms and cause a higher symptom burden in women than in men. Alterations in the serotonergic (5-HT) system are associated with mood disorders, and aggregates of α-synuclein (α-Syn) have been reported in the 5-HT raphe nuclei of patients with PD and depression. To elucidate the contribution of the ventromedial prefrontal cortex (vmPFC)–dorsal raphe nucleus (DR) circuit in depressive/anxiety-like disorders in PD, we employed a female mouse model of α-synucleinopathy within the 5-HT system, generated through AAV1/2-mediated overexpression of the A53T mutant human α-synuclein (h-α-Syn) in the raphe nuclei. The anxious/depressive phenotype was evaluated through a battery of behavioral tests. Neuronal activity in the infralimbic (IL) and prelimbic (PL) cortices of awake mice was recorded using single-unit and local field potential (LFP) measurements obtained with a multichannel probe in a virtual reality environment. Functional and structural connectivity between interconnected brain regions was assessed using functional magnetic resonance imaging (fMRI). In addition, synaptic and functional markers were analyzed by western blot and immunofluorescence. Female mice overexpressing h-α-Syn in 5-HT neurons developed an anxiety-like phenotype. In parallel, h-α-Syn overexpression in the 5-HT system altered the firing dynamics and functional organization of the vmPFC–DR circuit, changing the firing rates of pyramidal and GABAergic neurons (somatostatin and parvalbumin interneurons) in the PL and IL. This disruption shows a breakdown in normal firing-rate patterns and suggests that α-Syn pathology damages the specific electrical characteristics that maintain proper vmPFC circuit organization. These alterations were accompanied by disrupted brain connectivity and changes in synaptic markers (SV2A, PSD95, synaptophysin…) in PFC. Importantly, ketamine treatment partially reversed these neural and synaptic changes, along with the anxiety-like phenotype. Overall, this study suggests that overexpression of h-α-Syn in 5-HT neurons alters the functionality and connectivity of the vmPFC-DR circuit, resulting in an anxious phenotype in female mice.
P07.06
1 University of South Dakota, United States
Background: Parkinson’s disease (PD) is associated with deficits in both motor performance and cortical oscillatory activity, particularly within the midfrontal regions implicated in movement initiation and cognitive-motor control. While exercise interventions, including resistance training, have shown promise in improving motor outcomes, the neural mechanisms underlying these improvements remain poorly understood.
Objective: To investigate whether a 4-week resistance training program modulates midfrontal oscillatory activity during overground walking in individuals with PD and whether such changes correspond to improvements in gait performance.
Methods: Seven individuals with PD completed a twice-weekly resistance training regimen for four weeks. Electroencephalographic (EEG) data were collected during 2–3 minutes of overground walking both before and after the intervention. Power spectral analysis focused on midfrontal theta (4–7 Hz) and beta (13–30 Hz) frequency bands. Gait parameters, including walking speed and stride length (averaged across both legs), were derived from wearable motion sensors.
Results: Following the resistance training intervention, participants demonstrated a significant increase in midfrontal theta power and a reduction in beta power during walking compared to baseline. These neurophysiological changes were accompanied by improvements in gait outcomes, with mean walking speed and stride length showing positive percentage changes relative to pre-training measures.
Conclusion: This study provides preliminary evidence that resistance training can modulate cortical oscillatory activity associated with gait control in PD. The observed enhancement in midfrontal theta and suppression of beta power following training may reflect improved cortical engagement and reduced pathological synchronization. These neural adaptations were paralleled by measurable improvements in walking performance, supporting the potential of resistance training as a therapeutic strategy to enhance motor and neural function in PD.
P07.07
1 Emory University, United States
The objective of this study is to determine differences in brain activity between people with Parkinson’s disease (PD) with and without freezing gait (FoG) using a well-controlled probe of reactive balance.
FoG, a brief inability to start or continue walking, can lead to falls and reduce quality of life. FoG episodes are transient, unpredictable, and individual-specific, making it difficult to study its underlying neural mechanisms. Discrete balance perturbations similar to “getting the rug pulled under the feet” provide a tightly-controlled, reproducible method to study changes in brain activity that may underlie FoG. This paradigm elicits a reliable brain signal (N1) localized to the supplementary motor area (SMA), a brain region heavily involved in walking and balance control found to have altered activity in PD using functional neuroimaging. The N1 is also associated with individual differences in set-shifting, balance ability, and fall history. We hypothesize that SMA dysfunction will be greater in FoG which we predict will result in a smaller and less distinct N1 in FoG+ than FoG- individuals.
Preliminary data were collected from FoG+ (n=6) and FoG- (n=12) during on and off dopamine replacement medication states. We determined FoG status using a self-report FOG questionnaire or documentation in clinical records. Participants experienced discrete support-surface standing balance perturbations while we recorded brain activity using electroencephalography. We extracted the N1, defined as the largest most negative peak 100-300 ms post-perturbation from the Cz electrode (central midline) using standard processing pipelines. We then compared the N1 between FoG+ and FoG- individuals as well as during on and off medication states.
We found a clearly-defined N1 in FoG- (M=32.5 µV, Range=10.2-52.5 µV) that was less pronounced in FoG+ (M=12.43 µV, Range=4.3-20.9 µV), consistent with SMA dysfunction that is specific to FoG+. We did not find consistent differences in the N1 when comparing on and off medication states in either FoG+ or FoG-, which may indicate that the N1 may be responsive to medication status only in some individuals. N1 differences between FoG+ and FoG- and the significant variability across medication states may support the usage of the N1 as a neurophysiological biomarker that may detect FoG susceptibility without needing to trigger it and regardless of medication state.
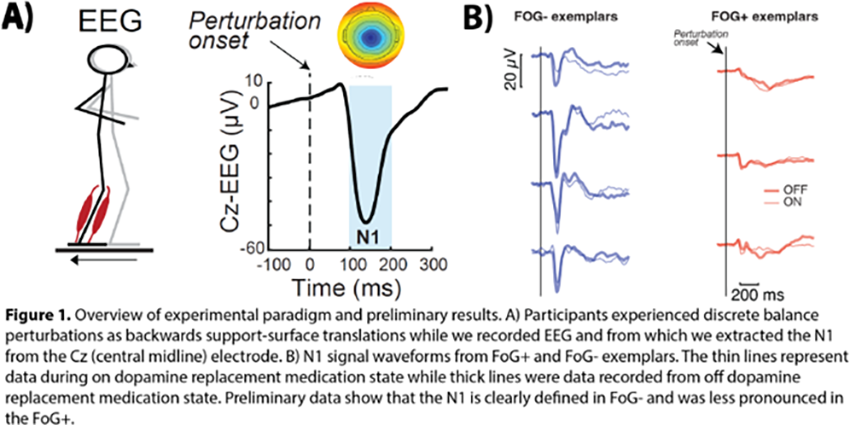
P07.08
1 Institut des Maladies Neurodégénératives, Université de Bordeaux, France
Changes in firing rates and synchronized oscillatory activity in basal ganglia (BG) are crucial for motor information coding in both normal and Parkinson’s disease (PD). Abnormal firing rates and increased neuronal synchronization have both been linked to movement inhibition in PD. However, the specific activities that cause movement issues such as akinesia and bradykinesia remain unknown. Understanding the individual contribution of these activities on the motor system is key to develop new PD treatments. In our project, we will utilize our lab’s advanced technology and expertise in manipulating firing rates and synchronization level of BG circuits using in vivo optogenetics. This approach allows us to independently control these neural modes with spatial and temporal precision. By combining these manipulations with behavioral analyses of skilled movement in rats and neuronal recordings in BG, we aim to quantify the disruptive effects of these activities on fine movement parameters. Our goal is to uncover the neuronal mechanisms causing action inhibition in PD, with the ambition to reverse-engineer the pathological changes in BG circuits and explore novel therapeutic mechanisms.

BASIC SCIENCES: Dopamine, receptors and other neurotransmitters
P08.01
1 INSERM, France
Introduction: Studies highlight a defect in endocytosis as a precursor and critical event in the neuronal loss associated with Parkinson’s disease (PD). On the one hand, mounting evidence suggests that Leucine-Rich Repeat Kinase 2 (LRRK2) is a master regulator of membrane trafficking events, particularly within the endolysosomal and autophagic pathways; and gain-of-function mutations of LRRK2 are associated with familial and sporadic PD. On the other hand, clathrin-mediated endocytosis, a major pathway for receptor internalization, is regulated by ubiquitously expressed cyclin-G-dependent kinase (GAK) and neuronal-specific protein auxilin 1. Both proteins have been identified as risk factors for PD in genome-wide association studies, and have been shown to interact with LRRK2.
Objective: Our aim is to elucidate the mechanisms underlying LRRK2-GAK and LRRK2-auxilin interactions and to determine their functional roles in endocytosis under both physiological and pathological conditions.
Methodology: Firstly, we will characterize the molecular mechanisms underlying the interaction using biochemical approaches, including co-immunoprecipitation (Co-IP) with truncated protein constructs and microscale thermophoresis to quantify binding affinities. Next, we will investigate the functional role of the complex in endocytosis through advanced microscopy techniques and assess the impact of pathogenic LRRK2 mutations on this process. Finally, we will develop pharmacological tools to modulate complex formation, thereby validating its involvement in endocytosis and the pathophysiology of PD.
Results: In preliminary experiments, combining in silico prediction using AlphaFold and cellular assay with Co-IP, we observe that ARM and ANK domains of LRRK2 are involved in the interaction with GAK. In addition, Co-IP experiments with LRRK2 clinical variants (protective: R1398H and pathogenic: N1437H; R1441C; Y1699C; G2019S and I2020T reveal that the pathogenic mutant N1437H enhances this interaction, whereas the protective variant R1398H exhibits reduced binding. These results strengthen our hypothesis that an imbalance in the LRRK2-GAK or LRRK2-Auxilin complex may contribute to the development of PD.
Conclusion: Our results suggest point to the interest of further exploring the role of LRRK2 in endocytosis, with the potential to better understand pathophysiological mechanisms of PD and open avenues for developing novel neuroprotective therapeutic strategies.
P08.02
1 Lehigh University, United States
Parkinson's disease (PD) disproportionately affects males, as females are less likely to develop PD, tend to manifest motor symptoms later in disease progression, and self-report less severe motor impairments. Despite these clear sex differences, the cause of increased susceptibility in males remains unknown. The fruit fly, Drosophila melanogaster, is an ideal model for studying sex differences in PD due to its short generation time, genetic tractability, cell autonomous sex determination, and conservation of many PD related genes. We found that expressing mutant α-synuclein A53T (αSyn A53T) in Drosophila dopamine (DA) neurons recapitulates the sex differences observed in human PD. Male flies developed motor symptoms earlier, exhibited greater motor impairment, and showed more severe DA neuron degeneration than females. Selective masculinization of female DA neurons via knockdown of the sex determination gene Transformer (Tra) eliminated the observed sex differences in locomotor ability and neurodegeneration by increasing the severity of motor deficits and degeneration in females. Previous studies have demonstrated that expression of the Vesicular Glutamate Transporter (VGLUT) is lower in male than in female DA neurons in both fruit flies and humans. Consistent with these results, knockdown of Tra in female DA neurons reduced total VGLUT staining in the brain. Furthermore, direct knockdown of VGLUT in female DA neurons expressing αSyn A53T exacerbated motor dysfunction, increased oxidative stress, altered mitochondrial morphology, intensified αSyn aggregation, and accelerated DA neuron degeneration. Conversely, VGLUT overexpression in male DA neurons rescued locomotor defects and DA neuron degeneration. Increasing cytosolic DA via knockdown of the Vesicular Monoamine Transporter (VMAT) or increasing total DA levels via L-DOPA treatment phenocopied VGLUT knockdown, suggesting that VGLUT protects DA neurons by reducing cytosolic DA. These results support a model in which lower VGLUT levels in males result in higher levels of cytosolic DA, which leads to increased αSyn aggregation, oxidative stress, and accelerated DA neuron degeneration.
BASIC SCIENCES: Neuropharmacology
P09.03
1 Unaffiliated, United Kingdom
Background Dopamine agonists are a commonly used therapy in Parkinson's disease but can cause impulse control problems. Previous studies have estimated the incidence of impulsive or obsessive behaviour when taking these drugs to be in the range 6-18% but, anecdotally, people with Parkinson’s seem to have issues more frequently than this.
Methods We conducted a survey of people in the UK who are currently taking, or had previously taken, either ropinirole, rotigotine or rotigotine to treat the symptoms of Parkinson’s disease. There were 54 respondents.
Results
24% of respondents reported issues with significant impact, 39% reported issues with moderate impact and 37% reported no issues Changes of behaviour related to shopping (20% of respondents), gambling (7%), sex (37%), binge eating (20%), online gaming (20%) and other obsessive behaviour (20%) 52% of respondents either did not report or played down the severity of impulse control issues when speaking with their medical team Men are more likely than women to experience issues with a significant impact, and men are more likely to experience sex related issues The incidence of issues across the three drugs is similar, but the severity varies with pramipexole more likely to lead to issues with a significant impact and rotigotine the least likely to lead to issues with significant impact 17% of respondents said the risks were not properly explained to them Of the respondents who had stopped taking an agonist, 50% reported a full reversal of impulse control issues
Conclusion Clinicians need to be aware that the incidence of impulse control issues with this class of drugs is likely much higher than previously thought due to the tendency for patients to under-report. They must give clearer warnings of the risks to patients, and more closely monitor for changes in behaviour.
P09.04
1 SK Biopharmaceuticals, South Korea
Variants in the GBA1 gene are among the strongest risk factors for Parkinson's disease (PD), primarily contributing to its pathology by reducing lysosomal β-glucocerebrosidase (GCase) activity. Yet no therapy has successfully and directly restored GCase function in the brain.
We report a novel small molecule GCase activator, SKPD, that directly and allosterically binds GCase to enhance catalytic efficiency without conformational stabilization effect on GCase. SKPD significantly increased GCase activity to clinically relevant levels in both the brain and peripheral blood mononuclear cell (PBMC) samples from wild-type mice. Notably, it restored the diminished GCase activity in GBA1 heterozygous mice and caused a significant dose dependent reduction in the GCase substrate glucosylceramide in whole brain tissue, confirming direct target engagement. To further substantiate the mechanism, in-depth structural analysis of SKPD and GCase interaction is ongoing using analytical ultra centrifugation (AUC), isothermal titration calorimetry (ITC), and X-ray crystallography.
In key models of Parkinson’s disease, SKPD effectively reduced α-synuclein aggregates across multiple cellular and animal models, including α-synuclein-overexpressing cells, GBA1 heterozygous mice, and α-synuclein pre-formed fibril (PFF)-injected mice via upregulated autophagy and lysosomal clearance function. SKPD also induced autophagic activation, suggesting the possible association between GCase activity to lysosomal function and the autophagic clearance as one of the main cellular pathways for α-synuclein degradation. Beyond these potential disease-modifying effects, SKPD also demonstrated symptomatic benefits by improving motor performances in both acute (MPTP) and chronic (α-Syn PFF-inoculation) models.
Taken together, SKPD represents a promising preclinical candidate targeting a fundamental pathological mechanism that is applicable to both GBA1 PD patients and idiopathic PD patients. IND-enabling studies are underway with the goal of submitting an IND application by the second half of 2026.
P09.05
1 Institut de Psychiatrie et Neuroscience de Paris, France
Parkinson’s disease (PD) is characterized by a selective loss of dopaminergic neurons in the Substantia Nigra pars compacta (SNpc) and the consequent reduction of dopamine (DA) in the striatum, which underlies the motor symptoms of the disease. The striatum is connected to multiple other regions of the brain, and the Parkinsonian state, both in terms of DA depletion and acute and chronic replenishment with L-DOPA, is poised to affect the brain as a whole. Changes in brain connectivity could underlie certain disease symptoms and could mediate side effects of medications, such as L-DOPA induced dyskinesia, which is characterized by drug-induced jerky involuntary movements. Here we propose to study functional connectivity (FC) changes in the Parkinsonian and dyskinetic brain using a novel imaging technique, functional ultrasound (fUS). Based on the principle of neurovascular coupling, fUS allows the imaging of brain connectivity in awake and moving mice, removing the bias of anesthesia that is often present with other imaging modalities. In the unilateral striatal 6-OHDA lesion model, along with reduced cortico-striatal and thalamo-cortical connections in the lesioned side, we observed a significant reduction of the interhemispheric connectivity of multiple components of the basal ganglia circuit, notably the striatum, the thalamus and the globus pallidus. Importantly, these alterations were completely normalized by two weeks of chronic L-DOPA administration, pointing towards a possible beneficial effect of L-DOPA. In contrast, cortex and hippocampus show increased bidirectional connectivity, which is even more pronounced upon chronic treatment. Of note is the fact that the changes are not limited to the lesioned side, but the unlesioned one seems affected as well, suggesting that in a bilateral lesion model and in PD patients, similar results may be expected. Taken together, these data will show for the first time a fingerprint of the PD brain, dopamine depleted and replenished, in freely moving mice, advancing our understanding of the pathology and contributing to identify disease and treatments’ mechanisms.
P09.06
1 Queensland University of Technology, Translational Research Institute, Brisbane, Australia, Australia
2 University of Queensland, Brisbane Australia, Australia
Parkinson’s Disease (PD) manifests as a spectrum of debilitating motor and non-motor deficits, with current treatments limited to dopamine replacement therapy for symptom management. Chronic immune and inflammasome activation, triggered by misfolded synuclein aggregates, is increasingly recognized as a key driver of PD neuropathology. Indeed, the NLRP3 inflammasome is currently one of the most attractive targets for disease modification in PD, with multiple therapeutic agents in clinical and preclinical development. Previous work from our team demonstrated extensive NLRP3 inflammasome activation in people with PD. We have also demonstrated that pharmacological inhibition of NLRP3 is neuroprotective in multiple disease models. Since kinases and phosphatases undertake the assembly and activation of inflammasome complexes, we sought to understand the specific kinases responsible for NLRP3 inflammasome activation in PD in our study. We identified that spleen tyrosine kinase (Syk) was highly activated in postmortem brain samples of PD patients and central and peripheral immune cells. In primary microglia, we found that activation loop phosphorylation of Syk at tyrosine 525 precedes inflammasome activation and IL-1β release triggered by synuclein aggregates. Using the orally active small molecule Syk inhibitor Entospletinib, we found that once-daily dosing could prevent striatal dopamine depletion and dopaminergic degeneration. We also found that Syk inhibition reduced synuclein pathology and spread in the striatum, motor cortex, and corpus callosum in a preformed fibril model of synuclein. Our results uncover Syk as a new druggable therapeutic target elevated in PD patients. Inhibition of Syk in the CNS could be a novel therapeutic strategy for disease modification in PD by targeting inflammasome driven neuropathology and dopaminergic degeneration.
P09.07
1 U1172, Lille Neuroscience & Cognition, France
2 Ambagon Therapeutics, Netherlands
3 University of Padova, Italy
4 Department of Cell Biochemistry, Groningen, Netherlands
Leucine-Rich Repeat Kinase 2 (LRRK2) is a large multi-domain protein with a functional GTPase and kinase domain. LRRK2 mutant forms found in familial and idiopathic Parkinson’s Disease (PD) display increased kinase activity and cellular abnormalities (e.g. lysosomal and mitochondrial dysfunctions, reduced neurite ramification…). To date, studies on LRRK2 targeting in preclinical models are promising for PD treatment and agents such as kinase or expression inhibitors are currently in clinical testing. LRRK2 protein forms a complex with 14-3-3 proteins that requires the phosphorylation of its Ser910 and Ser935 sites within a phospholoop of the LRR domain. Phosphorylation of these sites is decreased in PD-associated LRRK2 mutants and restored upon 14-3-3 overexpression. We recently showed that dephospho-mimicking LRRK2 mutant is hyperactivated compared to WT-LRRK2, suggesting that preserving LRRK2 phosphorylation by stabilizing the LRRK2:14-3-3 complex may be beneficial against PD. The aim of this project was to assess cellular activity of molecular glues of the LRRK2:14-3-3 complex. Candidate glues have been developed that show the stabilization of a LRRK2 pS910-pS935 spanning peptide with 14-3-3 protein via a Fluorescence Polarization assay. Two hits compounds that emerged from this in vitro assay were tested for their activity on the phosphorylation status of stable LRRK2 WT expression in HEK293T cells. Their potential to increase and/or maintain phosphorylation of the Ser935 was observed together with their ability to promote in cellulo LRRK2:14-3-3 interaction. In addition, immunocytochemistry revealed that glues prevent pathological condition associated discrete accumulations of LRRK2. Finally, this allosteric strategy of stabilizing LRRK2:14-3-3 interaction block LRRK2 pathomechanisms shows promise as an innovative approach for PD therapy.
BASIC SCIENCES: Neuroinflammation & Immune systems
P10.01
1 Johns Hopkins University School of Medicine, United States
2 Valted Seq Inc, Gaithersburg, Maryland, United States
Introduction: Parkinsonism, including Parkinson’s disease (PD) and Progressive Supranuclear Palsy (PSP), lacks reliable, non-invasive biomarkers for diagnosis and monitoring. Various brain cells—neurons, astrocytes, microglia—release exosomes, which carry molecules that influence recipient cells, making them promising biomarkers. This study longitudinally examined inflammatory and autophagic mediators in L1CAM- and TMEM119-enriched exosomal serum samples from patients with PD and PSP.
Methods: We collected serum from 30 PD patients, 20 PSP patients, and 30 healthy controls at baseline and after 1 year. Neuron- and microglia-derived extracellular vesicles were isolated by immunoprecipitating the neuronal marker L1CAM and microglial marker TMEM119. Exosomes were characterized by Nano Flow-cytometry and validated for canonical EV markers (TSG101, CD9, CD63, CD81). Crude serum samples were compared with exosomal lysates to confirm marker reliability. We assessed inflammatory markers (NLRP3, IL-1β, TLR2), autophagic mediators (pmTOR/mTOR, pNF-κB/NF-κB, ATP6AP2), and phospho alpha-Synuclein/total alpha-Synuclein. Kruskal-Wallis tests with multiple comparison corrections were applied.
Results: L1CAM and TMEM119-enriched exosomes from PD and PSP patients showed significantly elevated ATP6AP2, pmTOR/mTOR, and pNF-κB/NF-κB relative to controls (p < 0.01). Serum NLRP3 inflammasome and IL-1β levels increased significantly over 1 year in both PD and PSP groups (p < 0.05). Notably, pmTOR/mTOR, pNF-κB/NF-κB, and ATP6AP2 distinguished PD from PSP (p < 0.01). ROC analyses of NLRP3, IL-1β, and ATP6AP2 demonstrated diagnostic value differentiating Parkinsonism from controls, with AUCs of 0.78, 0.77, and 0.72 respectively (p < 0.05).
Conclusion: This study highlights the potential of L1CAM- and TMEM119-enriched exosomal inflammatory and autophagic mediators as biomarkers in PD and PSP. Associations of NLRP3 and IL-1β with disease progression support their role in monitoring. Autophagic markers pmTOR/mTOR, pNF-κB/NF-κB, and ATP6AP2 effectively differentiate PD from PSP, confirming disease specificity. Results indicate superior sensitivity and specificity of exosomal biomarkers versus crude serum markers. Larger prospective studies involving cell-type-specific markers and therapeutic interventions are needed to validate these biomarkers for parkinsonian syndromes.
P10.02
1 University of Cambridge, United Kingdom
Neuroinflammation provides novel avenues for development of new therapeutic strategies for Parkinson’s Disease (PD), with both peripheral and central inflammation having been associated with PD pathogenesis alongside Lewy body pathology. Multiple studies to date have reported changes in the adaptive immune system, however it is less clear how the innate immune response changes. In order to explore this, as well as address the need for more easily accessible immune biomarkers for therapeutic response monitoring and stratification of participants in immune-based clinical trials, this work aims to characterise the role of NK cells, monocytes and neutrophils in PD and determine the feasibility of measuring innate immune changes in nasal swab samples from people with PD across different disease stages and dementia risk groups. Matched nasal swab and blood samples from 20 people with PD and 6 healthy age and sex-matched controls were immunophenotyped using spectral flow cytometry with a panel of eighteen markers to characterise changes in the proportion and activation state of NK cells, monocytes and neutrophils. Pilot data has shown that immunophenotyping of nasal samples is feasible, with cell numbers sufficient to identify neutrophil, monocyte and NK cell subsets. Initial results from analysis of blood have indicated that there are more cytotoxic neutrophils, less NKG2A+ inhibitory NK cells and more NKG2D+ activated NK cells in PD versus controls. In nasal swabs, there was a trend towards more NK cells in PD versus controls, and an increase in the number of nasal NK cells and monocytes was associated with more severe hyposmia (OdofinTM Sniffin’ Sticks score). Nasal swabs represent easily accessible biosamples from an area highly relevant to PD pathology. Characterisation of innate immune changes within these samples is feasible and warrants further exploration for biomarker discovery in PD. Our pilot data suggests nasal innate immune activation is related to hyposmia.
P10.03
1 Acurex Biosciences, United States
2 University College London, United Kingdom
3 University of Pittsburgh, United States
OBJECTIVES Chronic microglia activation drives disease-associated microglia (DAM) phenotypes that worsen Parkinson's disease (PD) through dysregulated pro-inflammatory cytokine release, impaired phagocytosis of α-synuclein aggregates, and compromised neuronal survival. Because 15-lipoxygenase (15-LO) generates lipid hydroperoxides elevated in the PD brain and CSF, and its inhibition reduces DAM phenotypes, we investigated how 15-LO activity regulates PD-relevant DAM phenotypes.
METHODS We combined disease-relevant in vitro and in vivo systems: genetically modified human iPSC-derived microglia and the rat rotenone model of sporadic PD. Orthogonal imaging, histochemical, and biochemical assays quantified lipid peroxidation, inflammatory signaling, and microglial phenotypes within the context of 15-LO activity.
RESULTS Human iPSC-derived microglia harboring the A53T SNCA mutation showed heightened, time-dependent lipid peroxidation (C11-BODIPY) versus isogenic controls, with inhibition of 15-LO, using the small molecule inhibitor (CU-12991), preventing this increase. Given the reports that 15-LO activity drives LRRK2 kinase hyperactivation, we tested this pathway in microglia. Interferon-γ (IFNγ) elicited LRRK2-dependent IL-6 release; 15-LO inhibition blocked IFNγ-induced phospho-Rab10 levels and IL-6 secretion. In the rotenone rat model, 15-LO inhibition prevented rotenone-induced microglial phenotype changes within the substantia nigra.
CONCLUSIONS 15-LO inhibition coordinates lipid peroxidation and pro-inflammatory signaling that promote DAM phenotypes in PD. Inhibition of 15-LO normalizes these processes in human microglia and in vivo, supporting 15-LO inhibition as a therapeutic strategy to modulate microglia pathology in PD.
P10.04
1 Florida International University, United States
2 St. Jude Children's Research Hospital, United States
3 Arizona State University, United States
Introduction: Excess lipid droplet (LD) accumulation in microglia is a hallmark of aging and neurodegenerative diseases, including Parkinson’s disease (PD). These lipid-laden microglia exhibit a proinflammatory phenotype linked to altered lipid metabolism, suggesting that limiting LD buildup may offer therapeutic benefits. We previously showed that dynamin-related protein 1 (DRP1), a key regulator of mitochondrial dynamics, suppresses microglial activation by reducing NF-κB transcription. Here, we investigated whether DRP1 also contributes to LD accumulation and the underlying molecular mechanisms.
Methods: We analyzed publicly available RNA-Seq data (GSE139946) from flow-sorted microglia with high versus low LD content to assess DRP1–LD correlations. Dnm1l heterozygous knockout (Dnm1l+/−) and wild-type (Dnm1l+/+) mice were compared at young (3–4 months) and aged (18–24 months) stages. Metabolomic and lipidomic profiling were conducted on ventral midbrain tissues. LPS-induced neuroinflammation was modeled in vivo (1 mg/kg/day, 4 days) and in vitro using primary microglia treated with LPS (100 ng/mL) ± DRP1 inhibitor (P110) or NF-κB inhibitor (BAY 11-7082). LD accumulation, gene expression, and protein levels were assessed by immunofluorescence, qPCR, and immunoblotting, respectively.
Results: Aged Dnm1l+/+ mice exhibited significant enrichment of lipid metabolism pathways and elevated LD accumulation in ventral midbrain microglia and dopaminergic neurons compared to Dnm1l+/− mice (p<0.05). DRP1 mRNA levels positively correlated with LD content in microglia (p=0.007). Both DRP1 inhibition (P110) and Dnm1l haploinsufficiency significantly attenuated LPS-induced LD formation (p < 0.05) in vitro and in vivo. Mechanistically, DRP1 deficiency or inhibition suppressed the LPS-driven upregulation of Acsl1, a key LD biosynthetic enzyme transcriptionally regulated by NF-κB (p<0.005), and reduced expression of NF-κB (p65) and downstream cytokines (Tnfa, Il6, Il1b).
Conclusions: These results demonstrate that DRP1 plays a critical role in microglial metabolic reprogramming and LDs accumulation. As an upstream regulator of both LD accumulation and inflammation via the NF-κB-Acsl1 axis, DRP1 represents a good target for therapeutic development conditions involving lipid dysregulation.
P10.05
1 Queensland University of Technology- Translational Research Institute, Australia
2 Uinversity of Queensland, Australia
3 University of Queensland, Australia
4 University of Georgia, United States
Parkinson’s disease (PD) increasingly recognized as a multi-system disorder, multi-system disorder that extends beyond the central nervous system. Mounting evidence implicates the gut microbiome as a key player in its pathogenesis. Consistent reports of gut microbial dysbiosis across independent cohorts of people with Parkinson’s disease (PwPD) suggest that alterations in microbial communities may contribute to disease onset and progression. Notably, gastrointestinal disturbances often precede the development of motor symptoms by several years, underscoring the potential role of early, gut-derived metabolic changes in PD. Despite these associations, the mechanistic contribution of microbial metabolites to neurodegeneration in PD remains poorly defined. Using functional metagenomic profiling of faecal samples, we identified a significant upregulation of trimethylamine (TMA) production in PwPD (n=31) versus age-matched healthy controls (n=31). TMA, a neuroactive metabolite generated by microbial TMA lyase activity, and its oxidized derivative TMAO, have been implicated in neuroinflammation and cognitive decline. Our study found elevated TMA and TMAO in both plasma and urine of PwPD. We also detected increased formaldehyde (FA), a neurotoxic by-product of TMA metabolism, in this cohort. Importantly, we identified enrichment of TMA-producing bacterial taxa and metabolic pathways in PD faecal microbiomes. In humanized gnotobiotic mice colonized with healthy microbiota and fed a high-fat diet, plasma TMAO levels increased significantly. Pharmacological inhibition of TMA lyase using 3,3-dimethyl-1-butanol (DMB) and its analogues reduced circulating TMAO, providing proof-of-concept for microbiome-based intervention. This study provides the first functional metagenomic evidence linking TMA metabolism to PD, highlighting a novel, modifiable microbial pathway with therapeutic potential. Targeting TMA-producing bacteria and their enzymes may represent a promising strategy for slowing PD progression. Future work will involve the use of PD-derived microbiota in humanized mouse models to evaluate both pharmacologic (DMB) and microbial (engineered biotherapeutics) approaches for precision intervention. These findings pave the way for microbiome-informed therapeutics in neurodegenerative disease.
P10.06
1 University of Cambridge, United Kingdom
Introduction Neuroinflammation is increasingly recognised as a major contributor to Parkinson’s disease (PD) pathogenesis. However, its role in the atypical parkinsonian disorders progressive supranuclear palsy (PSP) and corticobasal degeneration (CBD) remains poorly defined. It is currently unclear whether these disorders share common inflammatory pathways with PD, or exhibit distinct, disease-specific profiles. This study aimed to systematically compare neuroinflammatory gene expression across PD, PSP and CBD to identify both shared and disease-specific inflammatory signatures which may provide insights into disease mechanisms and potential therapeutic targets.
Methods Using the NanoString nCounter platform, we profiled neuroinflammatory and glia-associated gene expression in post-mortem brain tissue from 10 pathologically confirmed cases each of PD (substantial nigra, putamen, amygdala and prefrontal cortex), PSP and CBD (putamen and prefrontal cortex), alongside age and sex-matched controls. Regions were selected to represent disease-vulnerable areas. All tissue was sourced from, and processed by, the Cambridge Brain Bank, with detailed clinical and neuropathological characterisation available for each case. Differential expression and pathway enrichment analyses were performed to identify overlapping and distinct inflammatory signatures across disease-region combinations.
Results Robust neuroinflammatory signatures were seen across all three diseases, with both shared and disease-specific transcriptomic profiles. Clustering analyses demonstrated that PD, PSP and CBD can be distinguished transcriptomically, by their inflammatory gene expression patterns. Notably, region-specific enrichment of microglial genes and pathways linked to innate immunity was observed, alongside the upregulation of cytokine and interleukin signalling.
Conclusion These findings indicate that neuroinflammation is a convergent yet heterogeneous hallmark of PD, PSP and CBD. The coexistence of common and distinct inflammatory pathways suggests overlapping mechanisms across Parkinson’s disease and atypical parkinsonian disorders, while also highlighting disease-specific immune profiles. Understanding these patterns may help identify novel therapeutics, either by targeting common immune pathways or by tailoring interventions to specific disease subtypes.
P10.07
1 Queensland University of Technology, Translational Research Institute, Brisbane, Australia, Australia
2 University of Queensland, Brisbane, Australia, Australia
3 University of Queensland, Brisbane Australia, Australia
4 Queensland University of Technology, Translational Research Institute, Brisbane, Australia and Princess Alexandra Hospital, Brisbane, Australia., Australia
NLRX1 is a mitochondria-associated NOD-like receptor that regulates innate immune and metabolic signalling. Emerging evidence suggests NLRX1 acts as a negative regulator of inflammasome activation in inflammatory diseases. In neurons, NLRX1 is hypothesised to support mitochondrial health, although its precise function remains unclear. This study aimed to define the mitochondrial role of NLRX1 in immune cells and dopaminergic neurons and determine whether pharmacological activation of NLRX1 can inhibit NLRP3 and resolve inflammation in Parkinson’s disease (PD) cellular models. Human THP-1 macrophages, primary microglia, and neuronal LUHMES and N27 cells were pretreated with either LABP-72 (CNS-penetrant, MPO 5.2) or NX-13 (gut-restricted, MPO 2.78) and subsequently exposed to paraquat (500 µM in THP-1; 100 µM in microglia), α-synuclein fibrils (5 µM in THP-1; 10 µM in microglia), or MPP+ (50 µM in LUHMES; 900 µM in N27). NLRX1 expression, cytokine release, and inflammasome activation were analysed by Western blot, ELISA, and qPCR. Caspase-3/7–dependent apoptosis and mitochondrial superoxide generation were assessed using live-cell imaging and confocal microscopy. NLRX1-interacting proteins were identified by immunoprecipitation coupled with DDA-mass spectrometry and analysed using Ingenuity Pathway Analysis (IPA). NLRX1 expression was reduced across immune and neuronal PD models. NX-13 did not prevent NLRX1 loss, whereas LABP-72 (150 nM) maintained NLRX1 expression, suppressed TNF-α release, and reduced NLRP3 inflammasome activation. In neurons, LABP-72 prevented caspase-3/7 activation, decreased mitochondrial superoxide production, and preserved elongated mitochondrial filaments under MPP+- and PQ-induced stress. Proteomic analysis revealed NLRX1 interactions with PRDX3, HSPD1, EIF2AK4, TRIM21, TUFM, and MRPS23, and IPA predicted these interactions to be involved in mitochondrial and immune signalling pathways. Collectively, these findings demonstrate that pharmacological activation of NLRX1 with LABP-72 maintains mitochondrial integrity and suppresses neuroinflammation in PD cellular models. NX-13 was less effective in vitro, likely due to lower agonist potency. Importantly, NLRX1 agonists are under clinical evaluation: NX-13 for IBD and LABP-66 for MS, highlighting the translational potential of targeting NLRX1. Future studies will test LABP-72 for its ability to halt PD progression, supporting its potential as a disease-modifying therapeutic target.
P10.08
1 Queensland University of Technology- Translational Research Institute, Australia
2 University of Queensland, Australia
3 University of Georgia, United States
4 Queensland University of Technology- Metro South Health, Australia
Parkinson’s disease (PD) is increasingly recognized as a multi-system disorder, with growing evidence implicating the gut microbiome in its pathogenesis. Alterations in gut microbial composition—termed dysbiosis—have been consistently reported across independent cohorts of people with Parkinson’s disease (PwPD). Gastrointestinal symptoms often precede motor features by decades, highlighting the relevance of early gut-derived metabolic changes. However, the mechanistic contribution of microbial metabolites to PD progression remains poorly understood. In this study we characterised the gut microbial composition in an Australian cohort of patients with Parkinson’s disease (n=50) and their age matched heathy controls (n=50) using high resolution functional faecal metagenomics. Microbial species were characterised using the taxprofiler pipeline. Taxonomic profiling revealed reduced microbial diversity in PD patients, with partial overlap in microbial community structures between groups. The gut microbiota in both cohorts was dominated by Firmicutes and Bacteroidetes, with Bacteroides and Blautia enriched in PD, and GGB9463 more prevalent in HC. At the species level, Akkermansia muciniphila was most abundant in PD, while Faecalibacterium prausnitzii dominated in HC. Several commensal species essential for intestinal homeostasis, including Clostridium disporicum and Streptococcus agalactiae, were significantly depleted in PD. Functional profiling identified significant alterations in amino acid, lipid, and carbohydrate metabolism in PD. Notably, pathways involved in amino acid and lipid metabolism were downregulated, whereas specific carbohydrate metabolic pathways were upregulated. Additionally, PD patients exhibited unique microbial enzymatic reactions and increased expression of pathways linked to nucleotide biosynthesis and DNA repair. These findings provide insights into microbial compositional and functional shifts in PD and lay the foundation for translational research using humanized gnotobiotic models to explore microbiome-targeted interventions.
P10.09
1 Institute of Biomedical Research of Barcelona (IIBB), Spanish National Research Council (CSIC), Spain
2 Departmet of Pharmacology, University of the Basque Country EH, Bizkaia, Spain
3 Departmet of Pharmacology, University of the Basque Country EHU, Bizkaia, Spain
Background: Parkinson's disease (PD) is a multisystem disorder frequently comorbid with non-motor symptoms like depressive disorder (DD) and gastrointestinal (GI) dysfunction. Chronic neuroinflammation and disruption of the gut-brain axis are implicated as shared pathological drivers, but the precise molecular mechanisms connecting these conditions remain unclear. We hypothesized that a shared miRNA-mediated inflammatory profile underlies this clinical triad, representing a point of pathological convergence.
Methods: We analyzed the expression of a panel of inflammatory bowel disease (IBD)-associated miRNAs, inflammatory markers, and glial response in postmortem brain tissue (dlPFC and CAU) from patients with PD, DD, and matched healthy controls. To investigate causality and gut-brain axis involvement, two mouse models were used: (i) PD-associated α-synucleinopathy was induced in dorsal raphe serotonin (5-HT) neurons; and (ii) DD-like based on corticosterone (CORT)-induced stress. Mice were assessed for depressive-like behaviors and GI dysmotility, and their brain (mPFC and CPu) and ileum tissues were analyzed for the same molecular markers.
Results: We identified a conserved miRNA pattern in the brains of both PD and DD patients, characterized by the significant downregulation of miR-199a-5p and miR-219a-5p and the upregulation of miR-200a-3p. This dysregulation was strongly associated with a pro-inflammatory state, as evidenced by increased expression of TNFα, IFN-γ, and NFκB1, as well as changes in the glial response. Mice with α-synucleinopathy in the 5-HT system exhibited a depression-like phenotype and reduced intestinal motility, accompanied by increased Iba1 and GFAP signal. Comparable effects were observed in mice subjected to CORT-induced stress. Notably, the same pattern of miRNAs and inflammatory cytokines observed in the human brain was replicated in the brain and ileum of DD-PD-like mice, providing direct evidence of a parallel pathological process spanning the gut-brain axis.
Conclusion: This study identified a specific miRNA-inflammatory axis as a common molecular mechanism connecting the pathophysiology of PD, DD, and gut dysfunction. This pattern represents a critical point of convergence that drives a shared, bidirectional inflammatory cascade along the gut-brain axis. Targeting this miRNA triad provides a new therapeutic approach for addressing the motor, psychiatric, and GI symptoms of these interconnected disorders simultaneously.
P10.10
1 University of Cambridge, United Kingdom
Approximately 50% of people with Parkinson’s disease (PD) develop PD dementia after 10 years, however we currently have no preventative treatments or validated biomarkers to predict its onset. Previous cross-sectional studies have associated a dysregulated immune response with cognitive decline, and worse disease severity in PD. Here we conduct a 5 year multi-modal study to determine which immune/inflammation markers are most associated with both cognitive and overall disease progression longitudinally, and whether longitudinal change in immune parameters could improve prediction of PD progression.
40 newly diagnosed PD cases were recruited. Blood, CSF and 11C-PK11195 PET/MRI were obtained at baseline and 3 year follow up. Immunophenotyping was performed using flow cytometry on PBMCs and CSF. Serum and CSF cytokines were measured using Mesoscale Discovery electrochemiluminescence assays. Neuroinflammation was measured using 11C-PK11195 PET. Clinical follow-up data was collected over 5 years (including ACE-III for cognition, and MDS-UPDRS).
Linear mixed-effects models demonstrate higher blood CD8+ T cell proportion, CD8+CD57+ counts in the CSF (CSF:blood ratio) and whole brain 11C-PK11195 non-displaceable binding potential (BPND) were the variables most strongly associated with cognitive decline longitudinally. Higher blood memory B cells, CD4+CD57+ CSF:blood ratio, CSF IL-17A, and 11C-PK11195 BPND in temporo-parieto-occipital regions were associated with MDS-UPDRS progression. ROC analysis suggests longitudinal immune changes (0-3 years) provide a more accurate prediction of cognitive outcome at 5 years than baseline immune markers.
Longitudinal measurement of immune parameters in PD could improve patient stratification for clinical studies and inform therapeutic targeting.
P10.11
1 Institut Imagine, France
2 Institut Imagine, INSERM UMR1163, France
3 Romane Lasmarrigues, France
4 Platform for Metabolic Analyses, SFR Necker, INSERM US24/CNRS UAR 3633, France
The gut–brain axis has emerged as a fundamental regulator of neurological health and disease, increasingly recognized as a critical contributor to the pathophysiology of Parkinson’s disease (PD). Mounting evidence links gut microbiota-derived metabolites, particularly short-chain fatty acids (SCFAs), to systemic and neuroinflammatory processes that may influence disease onset and progression. Alterations in microbial composition and SCFA levels have been observed in patients with PD, suggesting that changes in the intestinal environment can shape peripheral immune responses and impact brain homeostasis. However, despite significant progress, the precise role of SCFAs in regulating immune cell metabolism and function, and their contribution to PD pathogenesis, remains controversial.
To investigate this, we used induced pluripotent stem cell (iPSC)-derived microglia as a human model to assess how microbial metabolites influence innate immune responses. Our results revealed that exposure to SCFAs triggered a strong pro-inflammatory phenotype, marked by increased secretion of cytokines. In parallel, we observed a pronounced accumulation of lipid droplets (LDs) within microglia. Interestingly, these LDs often localized in close proximity to mitochondria, suggesting enhanced organelle crosstalk and pointing to a potential link between lipid storage, mitochondrial function, and inflammatory activation.
Proteomic profiling further supported this hypothesis, showing that SCFA exposure leads to extensive lipid remodelling and significant alterations in mitochondrial and energy metabolism pathways. Together, these findings indicate that microbial metabolites can reprogram microglial metabolism toward a lipid- and inflammation-associated state.
Ongoing analyses are aimed at determining how this SCFA-driven metabolic reprogramming affects microglial responses to α-synuclein pathology, with the goal of elucidating how gut-derived metabolic cues may contribute to neuroinflammation and neurodegeneration in PD. These insights may ultimately help define new mechanisms linking peripheral metabolic changes to central nervous system dysfunction.
P10.12
1 Nantes University, The Enteric Nervous System in Gut and Brain Disorders, U 1235 / UMR_S 1235, France
Recent observations, which showed that Parkinson’s disease (PD) and Crohn’s disease (CD) are genetically and epidemiologically linked, reinforce the assumption that the gastrointestinal tract could be critically involved in the development of Parkinson’s disease (PD). With regard to genetics, several studies identified the Leucine-rich repeat kinase 2 (LRRK2) gene, which is the gene most commonly associated with both familial and sporadic PD, as a major susceptibility gene for CD. These observations suggest that LRRK2 may sit at the crossroads of gastrointestinal inflammation, PD, and CD. Here, we examined the expression levels of LRRK2 mRNA in colon biopsies from subjects with overt PD (n=34) and prodromal PD (idiopathic REM-sleep behavior disorder, n=20) and compared them to samples from controls (n=20) and subjects with CD (n=18). We showed that LRRK2 expression was significantly increased in both inflammatory and non-inflammatory areas in CD samples when compared to controls. In sharp contrast, no difference in LRRK2 mRNA levels were observed between PD, iRBD and controls. The discrepancy observed in enteric LRRK2 expression between PD (either prodromal or overt) and CD suggests that these two disorders, despite their genetic links, differ mechanistically. Future research should be conducted to investigate the transcriptional regulation of LRRK2 and to elucidate its possible role in the gut in both PD and CD.
P10.13
1 Indiana University, United States
2 Indiana University, United Kingdom
3 Barrow Neurological Institute, United States
There is widespread evidence that cannabinoid type 2 receptor (CB2) is a regulatory driver of immune responses, which is consistent with its cellular distribution primarily on activated microglia and leukocytes. Brain expression of CB2 is increased in Parkinson’s disease (PD) patients and in animal models of proteinopathies, suggesting it’s functional relevance under disease conditions. We’ve previously found that pharmacological targeting of CB2 can reduce alpha-synuclein (α-syn) aggregation in a rat model of nigral synucleinopathy. However, it remains unclear whether this effect was mediated specifically by microglia since CB2 is found on peripheral immune cells and to a much lower degree neurons.
Therefore, mice with CB2 conditionally deleted from CX3CR1+ cells (CB2 cKO) and WT mice (n=4/group) were stereotaxically injected with AAV-human-WT-α-syn into the substantia nigra. The brains were collected after 2 months and immunostained for phosphorylated α-syn (pSer129) and proteinase-k resistant α-syn to evaluate α-syn aggregation, tyrosine hydroxylase to evaluate dopamine nigral neurons, and microglial markers (TMEM119, IBA1, MHCII, CD68) to identify microglia phenotypes. Preliminary in vivo findings reveal a trend toward reduced pSer129 pathology in CB2 cKO mice (p = 0.089), suggesting that CB2 in fractalkine receptor immune cells may influence early α-syn aggregation. Furthermore, nigral TH+ cell counts reveal an average of 24.7% loss in WT mice and 8.7% loss in CB2 cKO when compared to the uninjected nigra. Quantification of MHCII reveals no difference between groups, yet CD68-immunoreactivity was reduced in CB2 cKO mice compared to WT. Further analyses are underway to complete α-syn aggregation and microglia evaluation. Altogether, these data suggest that the removal of CB2 from microglia and other CX3CR1+ cells alters immune phenotypes which may in turn increase α-syn clearance resulting in the protection of nigral TH+ neurons. These studies will advance our understanding of the role of microglial CB2 in α-syn removal and potentially highlight CB2 as a therapeutic target against proteinopathies such as PD.
P10.14
1 Florida International University, United States
Background: Neuroinflammation is a key driver of neurodegeneration in disorders such as Parkinson’s disease (PD). Targeting this process offers a promising therapeutic avenue. Dynamin-related protein 1 (DRP1) is best known for regulating mitochondrial fission, but our recent study (PMID: 38504290) suggests broader cellular functions. Here, we uncover a previously unrecognized transcriptional role of DRP1 in regulating neuroinflammation.
Methods and Results: Neuroinflammation was modeled in vivo by exposing transgenic mice to lipopolysaccharide (LPS) (5 mg/kg for 6 hr, i.p.) and in vitro using primary microglia treated with LPS (100 ng/ml for 6 hr). Across in vitro and in vivo models, we found that DRP1 undergoes stimulus-dependent nuclear translocation following LPS exposure. Once in the nucleus, DRP1 binds directly to the promoter region of Rela (encoding NF-κB p65), enhancing NF-κB transcription and promoting downstream expression of proinflammatory cytokines, notably Lcn2 which encodes lipocalin 2 (LCN2). Among the NF-κB–regulated genes, Lcn2 was the most strongly induced and showed cell-type specificity–LPS significantly increased Lcn2 expression in laser micro-dissected microglia, astrocytes and DA neurons in mice, but not in GABA neurons. Elevated Lcn2 levels were also observed in the brains of α-synuclein–overexpressing transgenic mice and aged mice (18–24 months), underscoring the importance of this pathway in chronic neuroinflammation. In contrast, heterozygous DRP1-knockout markedly attenuated NF-κB activation, cytokine expression, and Lcn2 upregulation both in vivo and in vitro.
Conclusions: These findings reveal a novel function of DRP1 as a transcriptional regulator for the NF-κB–LCN2 inflammatory axis. Through such mechanism of DRP1, this study also provides potential therapeutic targets for PD and other conditions linked to inflammation.
P10.15
1 University of Alabama at Birmingham, United States
Parkinson’s disease (PD) is a neurodegenerative disease characterized by pathological accumulation of alpha-synuclein (α-syn) and the subsequent loss of dopaminergic neurons. While α-syn driven neuroinflammation has been shown to exacerbate neurodegeneration, the role of central nervous system (CNS) resident macrophages in this process remains unclear. Viral overexpression of α-syn in murine substantia nigra pars compacta recapitulates many of the features seen in human disease including microgliosis, T cell infiltration, and entry of peripheral monocytes occurring prior to neurodegeneration. Utilizing single cell RNA sequencing and BAM depletion strategies, our lab has demonstrated that BAMs adopt a disease-associated activation state (DaBAMs) that orchestrates immune cell recruitment, cytokine production, and neuronal damage primarily through antigen presentation to CD4 T cells.
However, how alpha-synuclein pathology promotes the appearance of disease associated BAM subsets remains unclear. BAMs, in addition to microglia, primarily derive from early erythro-myeloid progenitor cells in the fetal yolk sac. While these CNS resident cells are mostly thought to be self-renewing and yolk sac derived, various inflammatory states such as stroke, infection, or aging can induce peripheral monocyte infiltration and subsequent differentiation into inflammatory macrophages subsets that persist in the CNS. How alpha synuclein pathology influences the balance of peripheral and yolk-sac derived BAMs in the CNS, and whether shifts in this balance underlie immune-driven neurodegeneration remain incompletely understood. Utilizing transgenic fate mapping strategies with bone marrow chimeras and Ccr2eGFPCreER/+::R26tdTomato/+ mice, we show that monocytes readily infiltrate the CNS compartment after disease initiation, differentiate into MHCII+ BAMs along the border regions of the substantia nigra pars compacta, and persist as a pro-inflammatory BAM’s subset throughout our model.
P10.16
1 Indiana University, United States
Aims We have previously demonstrated that the PD-associated, R1441C-LRRK2 mutation, induces an age-acquired immune cell exhaustion (ICE) phenotype in myeloid cells from both knock-in (KI) mice and R1441C-PD patients. It is currently unknown the effects of this on the adaptive immune system. Here we aimed to test the hypothesis that innate-to-adaptive immune communication is altered due to innate immune exhaustion (ICE) in Lrrk2 mutant models of PD. Specifically, we examined how chronic inflammatory or proteostatic (α-syn PFF) stress in macrophages affects CD8+ T cell function, and whether LRRK2 kinase activity contributes to these effects.
Methods Peritoneal macrophages (pMacs) from 2-3 mo G2019S-, R1441C-Lrrk2 mice and B6 controls were exhausted via chronic ex vivo treatments with LPS (3000EU/mL) or α-syn PFFs (10 μg/mL) +/- Lrrk2 kinase inhibitor. CD8+ T cells from B6 mice were added to generate macrophage–T cell co-cultures and T cell function and ICE assessed after 2 hours, 6 hours or 5 days. ICE/T cell function was assessed via flow cytometry, multiplexed immunoassays and live cell imaging. PBMCs from healthy controls (aged 20 - 80 years), G2019S-PD and iPD patients were assessed for ICE and an ex vivo LPS assay was optimized to assess ICE induction dynamics in aged PBMCs.
Results Chronic LPS or PFF exposure reduced phagocytic activity in pMacs from Lrrk2 mutants, with effects ameliorated by Lrrk2 kinase inhibition. Co-culture with B6 CD8+ T cells elevated macrophage PDL1 expression even without stimulation, suggesting bidirectional immune stress. PFF-induced PDL1 expression in LRRK2 mutants correlated with elevated Annexin+ apoptotic CD8+ T cells and reduced Ki67 proliferation. In human G2019S-PD PBMCs, non-classical monocytes displayed increased PDL1, and CD8+ T cells exhibited elevated TIM3 and LAG3, confirming ICE phenotypes in patient immune cells.
Conclusions These findings indicate that chronic innate stimulation induces ICE in LRRK2 macrophages, disrupting innate–adaptive immune communication and impairing T cell survival and proliferation. ICE phenotypes are also present in peripheral immune cells from G2019S-PD patients. Together, these results support a model in which LRRK2-associated innate immune exhaustion contributes to maladaptive immune aging in PD and suggest that targeting LRRK2 kinase activity may restore immune resilience.
P10.17
1 1 Dept. of Biomedicine & Dandrite, Aarhus University, Denmark, 2 The Lundbeck Foundation Parkinson’s disease research center, PACE, Aarhus, Denmark, Denmark
2 1 Dept. of Biomedicine & Dandrite, Aarhus University, Denmark, Denmark
The vagus nerve represents a key communication route between the gut and brain, with epidemiological data suggesting a significant involvement in the risk and progression of Parkinson’s disease (PD). Vagus nerve holds significant immunomodulatory capacity in the so-called anti-inflammatory reflex, which is mediated mostly by cholinergic signalling. Despite growing evidence linking the vagus nerve, α-synuclein pathology, and neuroinflammation, their precise roles and combined impact on Parkinson’s disease progression remain poorly understood.
We used the intrastriatal preformed fibril (PFF) rat PD model to assess how disruption of vagal signalling and its immunomodulatory function influences disease progression. To simulate vagal dysfunction, adult rats underwent either bilateral sub-diaphragmatic vagotomy (VGT) or sham surgery (SHAM), followed by unilateral striatal injection of murine α-synuclein PFFs [8µg] or phosphate-buffered saline (PBS) as control. Motor behaviour (cylinder and corridor tests) and histopathology were assessed at 1.5- and 5-months post-injection. Brain immunostaining was used to evaluate α-synuclein pathology, microglial activation, and neuronal degeneration.
Vagotomy lead to significant decrease of the cholinergic neurons in the dorsal motor nucleus of the vagus. Early after PFF injections (1.5 months), VGT animals exhibited elevated α-synuclein aggregation (MJF14+) in the amygdala, striatum, and piriform cortex bilaterally, with increased propagation to the contralateral hemisphere compared to the SHAM-PFF. At 5 months, pathology remained higher in the amygdala and substantia nigra of VGT rats compared to SHAM. Microglial MHCII expression was higher in the amygdala of PFF-VGT animals (vs. PBS-VGT) after 1,5 months and significantly higher in the substantia nigra at 5 months post-PFF injection (SHAM vs. VGT). Tyrosine hydroxylase immunostaining showed that PFF-induced nigrostriatal loss without additional dopaminergic degeneration attributable to vagotomy.
Taken together our findings suggest that loss of vagal integrity promotes α-synuclein pathology and neuroinflammatory responses in vulnerable brain regions, supporting a modulatory role of the vagus nerve in disease progression. Ongoing analyses of peripheral tissues and immune profiling will further elucidate mechanisms linking vagal disruption to neuroinflammation and PD progression.
P10.18
1 Barrow Neurological Institute, United States
2 Arizona State University, United States
Parkinson’s disease (PD) is characterized by the progressive loss of dopaminergic neurons in the substantia nigra pars compacta, with growing evidence implicating astrocyte-mediated neuroinflammation in its pathogenesis. Chitinase-3-like protein 1 (CHI3L1/YKL-40), a non-enzymatic glycoprotein associated with astrocytic activation, has been linked to several neurodegenerative diseases, yet its role in PD remains unclear. We hypothesize that astrocytic CHI3L1 modulates neuroinflammatory signaling and may contribute to dopaminergic neurodegeneration. To investigate this, we examined CHI3L1 expression in both human post-mortem tissue and in a rat model of PD. Also, in order to study function, we developed a series of AAVs to manipulate CHI3L1 protein levels in vivo. Postmortem human PD substantia nigra exhibited significantly elevated CHI3L1 immunoreactivity compared to controls, supporting disease-associated upregulation. Similarly, increased CHI3L1 expression was detected in an AAV-humanα-syn mediated rat model of PD rats, suggesting a correlation between CHI3L1 upregulation and α-syn–induced neuroinflammation. To further explore functional roles, we engineered astrocyte-specific GFAP-driven rAAV-miRNA vectors to knock down CHI3L1 and a set of CBA-driven rAAVs for overexpression of constructs designed to express CHI3L1, including two isoforms, a mutant with a deleted secretion signal peptide, and a mutant with a substituted GDNF signal peptide to promote secretion. Vectors were delivered by stereotaxic surgery to the substantia nigra of rats, and brains were collected for histological analysis at three weeks post-surgery. Partial knockdown was achieved in astrocytes, confirmed by GFAP colocalization, while overexpression vectors induced increased CHI3L1 mRNA levels. Thus far, our findings suggest that CHI3L1 is upregulated in both human PD brain and by α-synuclein–induced pathology in rodents and may play a regulatory role in astrocyte-mediated neuroinflammation. Quantification to assess intra- versus extracellular CHI3L1 localization is ongoing. Work will continue aimed at determining the relationship between CHI3L1 upregulation, glial reactivity and dopaminergic neuron loss, as well as its potential as a therapeutic target in PD.
P10.19
1 Icahn School of Medicine at Mount Sinai, United States
2 Brigham and Woman's Hospital, United States
3 New York University Langone Health, United States
4 Mount Sinai Beth Israel, United States
Background: T-lymphocytes are important in Parkinson’s disease (PD), influencing the inflammatory response from the periphery to the brain. Genetic studies link human leukocyte antigen (HLA) class II alleles to PD risk. Our goal is to investigate the role of peripheral inflammation in PD by rigorously characterizing immune cell transcriptional profiles and T-cell receptor repertoires in patient blood.
Methods: We performed a large-scale, comprehensive single-cell RNA-seq analysis of human peripheral blood mononuclear cells (PBMC) from 172 donors. Our cohort includes controls (n=49), individuals with idiopathic PD (iPD; n=51), genetic PD with GBA or LRRK2 mutations (gPD; n=40), carriers of GBA or LRRK2 mutations (n=12) and prodromal patients with REM Sleep Behavior (RBD; n=20). We obtained gene expression, V(D)J immune receptor expression, genotypes and imputed HLA alleles. We performed standard single-cell data processing, differential cell type composition, differential gene expression and clonal expansion analysis. We are performing HLA expression quantitative trait loci (eQTL) association analysis to relate HLA alleles to gene expression differences in our cohort.
Results: We found changes in cell type composition driven by aging, sex, diagnosis and GBA/LRRK2 mutation status. As expected, naive T-cells decreased with aging (p<0.001) while effector T cell types such as Th1 and Th2 increased (p<0.05). Classical monocytes were higher in men (p<0.01). Parkinson’s patient's blood had more naive CD8+ T-cells (p<0.05) and showed lesser degree of clonal expansion compared to controls in clonal analyses. We also found that the relationship between sex and cytotoxic CD8+ T cells differs between diagnoses (p<0.01). While there are more cytotoxic cells in female than male PD blood, the opposite is true in control blood. Differential expression analysis shows more pronounced changes in the prodromal RBD group with relatively smaller changes seen when comparing controls to iPD or gPD. Furthermore, our analyses reveal that HLA genotype influences HLA gene expression in a cell type-specific manner
Conclusions: We present the largest collection to-date of neurodegenerative-focused paired single-cell transcriptomic and immune repertoire data from human PBMCs. Overall, these results further our understanding of the role of T-cells in PD and help determine the potential for targeted immune-based therapeutic interventions or biomarker capabilities.
P10.20
1 Arizona State University, United States
Type 2 diabetes mellitus (T2DM) and its prodromal state, prediabetes (Pre-DM), are increasingly recognized as systemic modifiers of immune responses and neurodegenerative development, particularly parkinsonian symptoms. Prior evidence suggests that inflammatory pathways contribute to insulin resistance and vascular degeneration. While variable lymphocyte activity, linked to impaired glucose utilization due to insulin receptor dysfunction, has been associated with volumetric changes in the substantia nigra (SN). Identifying biomarkers of glycemic control (HbA1c, glucose), dyslipidemia (LDL, HDL), and immune response (WBC, lymphocytes), alongside subcortical SN alterations measured via diffusion MRI free-water (FW) values, may help stratify risk for neurodegenerative diseases such as Parkinson’s disease (PD). This study tested the hypothesis that subcortical SN structural alterations co-vary with immune, metabolic, and cognitive markers across the glycemic spectrum in older adults. Through elucidation of these correlates, we aim to (i) advance pathophysiological understanding of nigrostriatal degeneration and its systemic drivers and (ii) provide proof of concept for AI-driven segmentation and risk stratification for high risk populations. De-identified data from the Health and Aging among Elders (HABLE) study included 474 participants (mean age = 62.52 ± 7.83 years): 103 with diabetes, 49 with prediabetes, and 321 controls. Blood biomarkers, cognitive markers, and MRI-derived anterior (ASN) and posterior substantia nigra (PSN) FW values were analyzed using IBM SPSS 30.0. Multivariate ANOVA and Spearman correlation analyses were performed across all diagnostic groups. Among controls, significant associations were observed between ASN and PSN FW and glucose levels (p = 0.024, power = 0.617; p = 0.026, power = 0.607, respectively), between PSN FW and HbA1c (p = 0.012, power = 0.709), and between PSN FW and WBC levels (p = 0.0919, power = 0.649). In the no-diabetes group, glucose correlated positively with right PSN FW (p = 0.025, ρ = 0.184). Although not statistically significant, the diabetes group displayed negative trends between PSN FW and HDL (r = −0.200, p = 0.054) and between ASN FW and LDL (r = −0.200, p = 0.054). These findings suggest that nigral microstructural alterations are linked to systemic glycemic and immune markers even in non-diabetic older adults, supporting multimodal, AI-based models for early neurodegenerative risk stratification.
P10.21
1 Indiana University, United States
Chronic systemic inflammation (CSI) has been identified as a key factor in the pathogenesis of many age-related diseases including neurodegenerative diseases (NDs) such as Parkinson’s disease (PD). Interestingly, sources of CSI, such as poor gut health due to lifestyle choices, physical inactivity, stress, sleep disturbances, exposure to industrial toxicants, pre-existing chronic inflammatory diseases (CIDs) (including rheumatoid arthritis (RA), inflammatory bowel dis-ease (IBD), irritable bowel syndrome (IBS), and psoriasis), genetics, and aging overlap significantly with risk factors for developing PD. This suggests that CSI may act as a common trigger in the development and progression of PD; however, the role of peripheral immune cell dysregulation in this process remains largely understudied. Previously, we have shown that 6 weeks of exposure to peripheral lipopolysaccharide (LPS)- induced CSI results in sex-specific dysregulated immune responses in the central nervous system (CNS) and the circulation of wild-type C57BL/6 mice. However, as CSI may persist for decades in humans, we therefore aimed to understand how longer exposures to CSI would impact immune cell populations and dynamics systemically and in the CNS. We hypothesize that increased durations of CSI will exaggerate dysregulated immune responses. To test this, we exposed wild-type B6 mice to either 6 or 12 weeks of biweekly intraperitoneal injections of 1X106EU/Kg of LPS or sterile saline and isolated immune cells in the blood and brains for flow cytometry. This work will help illuminate the impact of extended CSI on the central and peripheral immune systems, which will enable development of more translationally relevant CSI models, and advance our understanding of the role of early immunologic contributions to the development and progression of idiopathic PD.
P10.22
1 Indiana University School of Medicine, United States
Age is the greatest risk factor for Parkinson’s disease (PD). Immune dysregulation in both the central nervous system (CNS) and periphery has been observed in PD, yet the role of immune aging in PD remains underexplored. Chronic systemic inflammation (CSI) is a hallmark of PD pathology and may drive neurodegeneration. One consequence of CSI is immune cell exhaustion (ICE), a hyporesponsive state marked by impaired effector function and upregulation of inhibitor receptors. Recently, ICE has recently been implicated in PD, with PD-associated mutations inducing ICE in peripheral immune cells. Because ICE increases with age, PD may reflect accelerated immune aging. However, whether peripheral ICE contributes causally to degeneration in PD is unknown. We hypothesize that an aging immune system and CSI synergize to induce ICE, and that peripheral ICE is required for CSI-mediated dopaminergic neuronal loss in the midbrain.
Young (2–3 mo) and aged (18 mo) B6 female mice (N=6) were exposed to acute (5×106 EU/kg LPS, 24 h) or chronic (9×105 EU/kg LPS daily for 7 d + 72 h recovery) LPS or saline. Brains were fixed, stained, and assessed for TH and Pdl1 to evaluate dopaminergic neuron loss and ICE induction. To establish causality, young B6 females (N=6) received chronic LPS or saline with anti–Pdl1 or isotype control (5 mg/kg) every 3 days. Hemi-brains were analyzed for TH, Tmem119, Iba1, Pdl1, Pd1, and Tim3 to assess ICE in distinct cell types. Immune cells from remaining hemi-brains and PBMCs were analyzed for ICE via flow cytometry.
Chronic but not acute LPS caused a significant decrease in midbrain TH expression in both young and aged mice relative to saline controls, with greater loss in aged mice. Chronic LPS also induced a significant increase in expression of the inhibitory receptor PDL1 in the midbrain of aged mice relative to all other groups.
Anti-Pdl1 experiments are ongoing. It is anticipated that anti–PD-L1 treatment will block the induction of ICE in peripheral and CNS immune cells and prevent TH loss in the midbrain.
Our results suggest age and CSI may synergize to induce ICE which is associated with TH reduction in the midbrain. Ongoing anti-PDL1 experiments will provide data for us to conclude if this peripheral ICE is required for degeneration in the midbrain in this model. These results have direct translational application, highlighting peripheral ICE as a potential therapeutic target for slowing or preventing neuronal degeneration in PD.
BASIC SCIENCES: Prevention, neuroprotection and neuroplasticity
P11.01
1 Grenoble Institut Neurosciences, France
Parkinson’s Disease (PD) is a progressive and incurable neurodegenerative disease characterized by an irreversible loss of nigrostriatal dopaminergic neurons. Its symptomatology evolves over the years from a prodromal stage, including neuropsychiatric symptoms such as loss of motivation and anxiety, to a clinical stage with significant motor impairments. Today, the causes of PD pathogenesis are still poorly understood. In this context, we recently performed a large translational metabolomics study on serum and brain samples of both rat and non-human primate PD models and newly diagnosed PD patients, which revealed a decoupling between the glycolysis and the Krebs cycle. These metabolic perturbations strongly suggest that impairments of the Pyruvate Dehydrogenase (PDH), the key enzyme linking these two metabolic pathways, could be a major actor in the mechanisms underlying the pathogenesis of PD. Consistently, it have been shown that the congenital mutation of the PDH can leads to the development of a Leigh syndrome with neurodegeneration of the nigrostriatal pathway and that the PDH is downregulated in the nigrostriatal pathways of patients with idiopathic PD. Based on this, our work aimed to better decipher the role of this enzyme in PD pathophysiology. To this end, we first induced a local PDH downregulation in the nigrostriatal pathway of healthy rats by using a AAV-microRNA strategy and stereotaxic surgery. The results show that this strategy has induced a 40% nigrostriatal PDH downregulation, resulting in the development of a hypomotivated state with anxious behaviors but without motor impairments. These symptoms are reminiscent of a prodromal-like PD symptomatology, and are associated with the evidences of a parkinsonian-like metabolic profile in both blood and brain. In addition, in a preliminary study, we have shown that the overexpression of PDH in the nigrostriatal pathway of a well-known Parkinson’s disease rat model, the unilateral 6-OHDA model, partially prevented motor deficits. In particular, we have highlighted a significant rescue of motor function in the cylinder test, with 6-OHDA rats with nigrostriatal PDH overexpression exhibiting almost twice as many contralateral forelimb contacts compared to untreated 6-OHDA rats. Altogether, these results indicate that a PDH dysfunction is likely to be involved from the early stages of the PD pathophysiology and that PDH should therefore be considered as a new potential therapeutic target for PD.
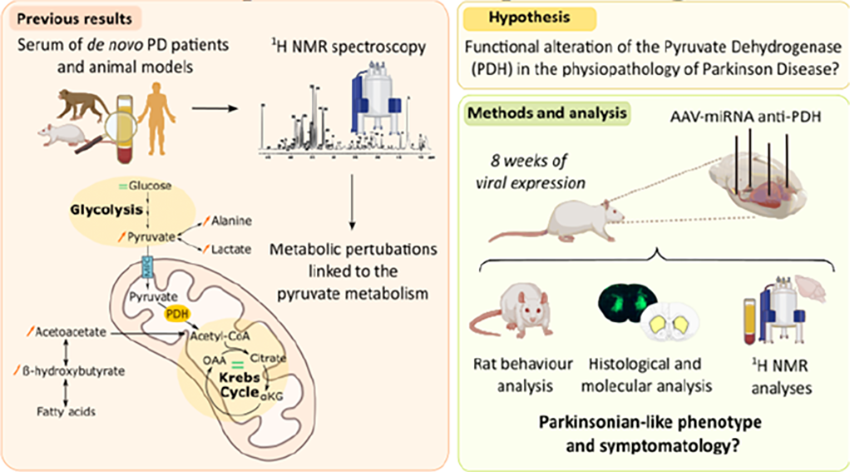
P11.02
1 Eurac Research, Italy
2 KU Leuven, Belgium
3 University of Piemonte Orientale, Italy
4 Istituto Italiano di Tecnologia (IIT), Italy
5 University of Verona, Italy
Parkinson's Disease (PD) is a progressive neurodegenerative disorder characterized by loss of Substantia Nigra dopamine neurons and the accumulation of phosphorylated α-Synuclein (pS129-αSyn) in surviving ones. The major unmet clinical need in PD remains the lack of disease-modifying treatments.
The small GTPase RIT2 has emerged as a potential modulator of PD pathology. Its genetic locus is associated with PD, and RIT2 mRNA levels are reduced in the brains of idiopathic PD patients and in experimental PD models. Our previous studies demonstrated that increasing RIT2 in cellular and murine PD models overexpressing G2019S-LRRK2 or A53T-αSyn reduces LRRK2 hyperactivity, ameliorates αSyn pathology and lysosomal dysfunction, and prevents neurodegeneration, supporting the therapeutic potential of restoring RIT2 levels in PD.
To pursue this strategy, we developed SINEUP molecules targeting RIT2. SINEUP – Short Interspersed Nuclear Element B2 UP regulation – is a class of long non-coding RNAs that specifically enhances endogenous translation of their target mRNA, providing a controlled and physiologically relevant increase in protein expression, attenuating the risk of toxicity associated with overexpression or ectopic gene delivery.
First, we designed five SINEUP-RIT2 molecules, tested into murine Neuro2A cells and identified two molecules increasing RIT2 protein without transcriptional changes. SINEUP-dependent elevation of RIT2 correlated with increased p38-MAPK phosphorylation, a downstream effector of RIT2, suggesting functional effects of SINEUP-driven translation.
The two most effective SINEUP-RIT2 molecules were then tested in G2019S-LRRK2 SH-SY5Y cells, a human cell model recapitulating key cellular features of LRRK2-associated PD, including aSyn pathology and increased LRRK2 kinase activity. Treatment with SINEUP-RIT2 reduces pS129-αSyn inclusions, decreases LRRK2 phosphorylation at S1292 – a proxy for kinase activity – and Rab10 phosphorylation at T73 – one of LRRK2 substrates, thus effectively mimicking the effect of RIT2 overexpression (see figure).
We are currently differentiating induced pluripotent stem cells (iPSCs) into cortical neurons from PD patients carrying the G2019S-LRRK2 mutation and healthy controls, to then assess the efficacy of SINEUP-RIT2 molecules in a disease-relevant human neuronal model.
Together, these findings suggest that SINEUP-mediated RIT2 upregulation represents a novel and promising therapeutic approach for PD.
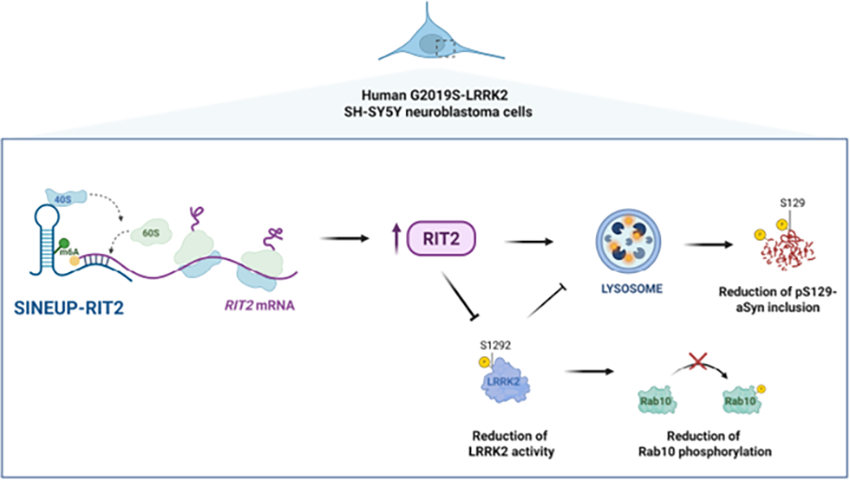
P11.03
1 Weill Cornell Medicine, United States
Anxiety is one of the most common and disabling non-motor symptoms of Parkinson’s disease (PD), affecting up to half of patients and reducing quality of life (Pontone et al., 2009, Martinez-Martin et al., 2010). Importantly, anxiety often emerges years before motor symptoms and occurs more frequently in women (Penninx et al., 2021, Carey et al., 2021). The amygdala, a central hub for emotional regulation, has been increasingly implicated in PD-related anxiety (Wang et al., 2023, Carey et al., 2020), yet the mechanisms driving sex differences in its dysfunction remain unclear.
To investigate this, we performed experiments in a progressive PD mouse model, induced by striatal injections of a-synuclein (asyn) preformed fibrils (PFFs) in wild type C57Bl6 male and female mice. We observed sex-dimorphic propagation of asyn pathology (immunolabelling for phosphorylated Ser129 asyn), paralleled by sex-specific changes in neuronal activity and cortico-amygdala connectivity over time (immunolabelling for cfos expression, dendritic spine density/morphology). These circuit-level alterations paralleled sex-specific behavioral differences in emotional and cognitive processing (open field and fear conditioning tests) in absence of neurodegeneration (immunolabelling for Nissl in the amygdala, and TH in the substantia nigra and striatum) (See Attached Figure).
Our findings reveal that asyn pathology induces early, sex-specific synaptic and network remodeling in the amygdala circuit in absence of neuronal loss. By identifying divergent circuit adaptations to asyn stress in males and females, this work underscores the importance of incorporating both sexes in PD studies to elucidate mechanisms underlying non-motor symptoms and to inform the development of more precise, individualized interventions.
Significance: Understanding how asyn pathology alters emotion-related circuits differently in males and females provides a critical framework for interpreting early, non-motor manifestations of PD. Anxiety often precedes motor symptoms by years, offering a potential window for early detection and targeted intervention. By linking sex-dependent neural circuit remodeling to behavioral outcomes, this work contributes to the growing recognition that biological sex is a key determinant of PD vulnerability and treatment response, highlighting opportunities for sex-informed therapeutic strategies aimed at improving quality of life in PD.

P11.04
1 Thomas Jefferson University, United States
2 Rutgers University, United States
Aerobic exercise is a disease-modifying intervention in Parkinson’s disease (PD), shown to attenuate UPDRS Part III motor progression and improve select non-motor symptoms. As a component of a healthy lifestyle, exercise enhances mobility, flexibility, balance, and coordination in PD patients. Epidemiological data indicate that early-life or sustained moderate activity through midlife significantly reduces PD risk later in life. In a preclinical model, running exercise protects against toxin-induced SNpc DA neuronal death; DA cell loss is reduced from 20% in sedentary mice to 5% in exercised mice. We previously demonstrated that exercise induces cellular hypoxia and stabilizes the transcription factor HIF1α in SNpc DA neurons. HIF1α target genes promote angiogenesis as well as other metabolic and cell cycle processes. Morphometric analysis of the microvascular network in the SNpc revealed a reduced neuron-to-vessel distance and an increase in branch points per vessel in exercised mice. This data suggests vascular remodeling contributes to neuroprotection, but the permanence of the changes beyond active exercise and acute hypoxia remains unknown. To assess the durability of exercise-induced neuroprotection, mice underwent 90 days of voluntary exercise followed by 60 days of sedentary housing (SH), maintaining full protection against MPTP-induced DA neuron loss; protection equivalent to that of MPTP administration immediately post-exercise. Longer duration exercise (150 days) also confers neuroprotection but induces a higher proportion of activated microglia, comparable to MPTP treated groups. To explore molecular mechanisms that are induced by exercise, we investigated signatures of methylation and hydroxymethalyion at CpG sequences within the SNpc. Epigenetic modifications link gene activity to environmental factors like exercise and can persist lifelong and transgenerationally. We find that exercised mice exhibit differential methylation of several genes, including those involved in synaptic structure, plasticity, dopamine signaling as well as angiogenesis, with sex-specific patterns observed. Ongoing studies are aimed at extending the sedentary duration following a 90-day bout of exercise and assessing whether vascular network remodelling and neurovascular responses of pericytes and microglia endure through this window. Further, we aim to identify stable epigenetic marks associated with continued neuroprotection.
P11.05
1 University of Arizona, United States
Neurodegeneration increases and neuroregeneration decreases with age, laying the foundation for diseases like PD. Examining neural stem and progenitor cell (NSPC) biology during aging is critical to understanding these basic phenomena. From this viewpoint, our lab has been studying NSPC aging and has identified a critical middle-age period (CP) of neurogenic decline, mediated by the reduced expression of Nrf2, a redox-sensitive transcription factor. NSPCs exist in different cellular states like active, quiescent, deeply quiescent or senescent states in the adult brain. While quiescence is favorable and reversible, senescence is the irreversible state of cell cycle arrest. This study examines how NRF2, and ovarian sex hormones (Estradiol, E2/ Progesterone, P4) influence NSPC cellular states during the CP.
Male (aged 9 & 14 months) and female (aged 6 & 10 months) WT and Nrf2 KO rats were used (n=7/group). Female rats were ovariectomized (OVX) or remained Intact. These chosen age-groups were focused upon to understand Nrf2 and E2/P4 effects related to the 13-15 mos male CP and 7-9 mos female hormone-loss associated CP’s, respectively. Immunohistochemical (IHC) and behavioral assays were applied to identify quiescent and senescent NSPCs, and assess NSPC function.
Behavioral analysis, showed significant reduction in fine and gross olfactory discrimination capacities at both ages and sexes in Nrf2-KO group. OVX worsened this phenotype in females. In the object-context pattern separation task, male Nrf2 KO rats trended towards worse performance than WT at both ages. With females, the OVX and KO groups performed worse at 10 mos when compared to the 6 mos old cohort. IHC analysis assessing quiescence (Ki67- and LaminB1+) and senescence (Ki67- and γH2AX+/p16+/LaminB1-) of type B, C and A NSPCs is underway. Preliminary data show a trend towards lower numbers of proliferating NSPCs and higher non-proliferating (quiescent or senescent) NSPCs with age and KO of Nrf2 in males. In the females, LaminB1 showed reduced expression at 14mos compared to 6mos.
In conclusion, this study determines the effects of Nrf2 and E2/P4 loss on the cellular state transitions of the NSPCs during CP’s of neurogenic decline in males and females. These data will provide the basic framework for the translational possibilities targeting reduction in the senescent NSPCs through senolytics, activation of Nrf2, or supplementing E2/P4, in the context of age-related neurodegenerative states such as PD.
P11.06
1 University of Padova, Italy
2 Department of Biology, University of Padova, Italy
3 iQure Pharma Inc., United States
Glutamate is the primary excitatory neurotransmitter in the brain and is essential for normal neuronal communication. However, excessive extracellular glutamate can lead to excitotoxicity and neurodegeneration. In Parkinson’s disease (PD), impaired function of the astrocytic glutamate transporter EAAT2 (also known as GLT-1) has been reported, suggesting that glutamate dysregulation contributes to disease progression. This research aims to evaluate i) the neuroprotective potential of iQ-007, a novel positive allosteric modulator of EAAT2, and ii) to elucidate its molecular and cellular mechanisms of action.
In the translational study, iQ-007 is being tested across complementary preclinical models of PD, including MPTP-treated mice, G2019S-LRRK2 knock-in mice, a GLT-1 downregulated mouse line, and MPTP-treated non-human primates. Both preventive and therapeutic treatment regimens will be assessed for their effects on motor and cognitive performance, glutamate homeostasis, and neuropathological outcomes.
In the mechanistic study, we are investigating iQ-007–mediated modulation of EAAT2 in human iPSC-derived astrocytes and examining its impact on EAAT2 protein stability in vivo. Furthermore, we are exploring the neuroprotective effects of iQ-007 on PD-relevant pathogenic pathways, including LRRK2-mediated regulation of EAAT2 trafficking and modulation of EAAT2 functionality by α-synuclein aggregates.
We hypothesize that restoring EAAT2 function with iQ-007 will normalize extracellular glutamate levels, protect against dopaminergic neuron loss and cognitive deficits, and mitigate levodopa-induced dyskinesias. Establishing a mechanistic link between glutamate regulation and PD progression could open a novel therapeutic avenue and support biomarker-based patient stratification in future clinical trials. Upon validation of efficacy and mechanism in preclinical models, iQ-007 will advance to early-phase clinical evaluation in PD patients.
BASIC SCIENCES: Genetic and other Cellular Models of Parkinson's, including iPSCs
P12.01
1 Asan Medical Center, South Korea
2 Myongji Hospital, Gyeonggi-do, South Korea
Objective: To identify single nucleotide variants (SNVs) associated with the development of Parkinson’s disease dementia (PDD) using a genome-wide survival study (GWSS) and to evaluate the impact of polygenic risk scores (PRS) related to Parkinson’s disease (PD), Alzheimer’s disease (AD), and amyloid-β (Aβ) deposition.
Background: Genome-wide association studies have revealed several genetic variants linked to PD. However, the genetic determinants of PDD remain insufficiently characterized.
Design/Methods: We recruited patients with PD between January 2009 and December 2016 and conducted genomic sequencing using a Korean genotyping array. GWSS was first performed to identify SNVs associated with PDD. PRS were then constructed based on variants from previous studies of PD, AD, and Aβ positivity. Associations between PRS and incident dementia were assessed using Cox proportional hazards models.
Results: Among 964 participants, 225 developed dementia during a median follow-up of 10 years. GWSS identified SNVs in HS1BP3, PTPRM, APOE, and TOMM40 as being associated with PDD. Both the Asian AD-PRS (PGS000779; HR 1.31, 95% CI 1.19–1.45, P < 0.001) and the European AD-PRS (PGS0002280; HR 1.89, 95% CI 1.23–2.91, P = 0.004) were significantly associated with increased risk of PDD. In addition, the Aβ-PRS was associated with dementia in PD (HR 2.07, 95% CI 1.17–3.65, P = 0.012). In contrast, the PD-PRS was not significantly associated with PDD.
Conclusions: Our findings demonstrate that AD-PRS and Aβ-PRS are significantly associated with the development of dementia in PD, whereas PD-PRS is not. These results provide important insights into the pathogenic mechanisms underlying PDD and may inform future strategies for risk stratification and therapeutic development.
P12.02
1 madhavan, United States
2 University of Arizona, United States
Understanding the mechanisms causing Parkinson’s disease (PD) remains a fundamental pursuit and a vital need in the development of early diagnostics and therapeutics. Patient induced pluripotent stem cell-based models represent a powerful human system to gain insights into the etiopathology of PD. From this perspective, we studied several iPSC-derived dopamine neuron (iPSC-DAN) lines, from individuals with idiopathic PD, which is the most common form of PD. Sporadic PD (n=10) and age- and sex-matched control (n=10) iPSC lines were differentiated into dopamine neurons (iPSC-DAN) for 50-55 days via a floor plate-based method using dual SMAD inhibition. An in-depth analysis of different bioenergetic pathways and cellular quality control mechanisms, and whole proteome analysis was performed. Wide ranging impairments in oxidative phosphorylation (OXPHOS), glycolysis and creatine kinase pathways were seen in the PD iPSC-DAN. Specifically, the PD neurons exhibited reduced oxygen consumption rates (OCR) at baseline and after challenges with mitochondrial inhibitors, as well as decreased glycolytic reserves (ECAR). This translated to lower OCR:ECAR ratios signifying more reliance on glycolysis vs OXPHOS in the PD cells. Moreover, a mislocalization of creatine kinase B to mitochondria was seen in the PD cells. These energetic changes synergized with the enhanced expression of mitochondrial fission proteins, disrupted mitophagy and oxidative stress. Additionally, the PD neurons contained more monomeric, phosphorylated and aggregated forms of alpha synuclein and displayed reduced viability. Ultrastructural examination through immuno-electron microscopy showed more alpha synuclein gold particles directly associated with mitochondria and packing autophagic vesicles. Moreover, whole proteome analysis identified significant downregulation of specific proteins in the PD neurons compared to controls. Some differences between the phenotypes of male and female lines were also seen in terms of these different readouts. In essence, these data capture a web of pathological changes in human iPSC-DAN from idiopathic PD subjects, providing a robust platform for further mechanistic assessment and identification of molecular pathways that could be therapeutically targeted.
P12.03
1 Brigham and Women's Hospital, United States
2 Brigham and Women's Hopital, United States
Mutations in the GBA1 gene encoding glucocerebrosidase (GCase) are the most common genetic risk factor for Parkinson’s disease (PD) and Dementia with Lewy Bodies (DLB). PD/DLB associated mutations in GBA1 result in reduced GCase enzymatic activity which leads to the accumulation of its lipid substrates glucosylceramide and glucosylsphingosine in the lysosome. Recent studies have suggested that GBA1 mutations can elicit cognitive behavioral deficits in a mouse model, however, the underlying mechanisms remain elusive. Therefore, we aimed to investigate the effects of GBA1 inhibition and PD-associated GBA1 mutations on synaptic transmission. We measured synaptic vesicle (SV) cycling as a read-out of neurotransmission. For this we used, a pHluorin based SV cycling assay in which a pH sensitive GFP is fused to the synaptic vesicle protein synaptophysin, creating a fluorescent “sensor” (SypHy). We found that GBA1 knockdown (KD) results in decreased vesicle exocytosis in both primary cortical and hippocampal neurons. To understand whether enzymatic activity of GCase plays a role in regulating neurotransmission we measured SV exocytosis in neurons treated with conduritol β-epoxide which is a specific inhibitor of GCase. We found a decreased SV release in hippocampal neurons and delayed exocytosis in cortical neurons. We also observed that aSyn protein levels were increased upon GBA1 KD. We then measured SV exocytosis in aSyn KO cortical neurons and found no differences between GBA1KD and vector control. This further confirms that GBA1 KD causes disruption in aSyn homeostasis which leads to impairment in SV release. We also compared SV cycling in PD-associated GBA1 mutations E326K and L444P in patient-derived induced neurons with their isogenic control. We found no significant changes in E326K, however SV cycling was reduced in both basal and stimulated conditions in L444P. Our study concludes that reduced GCase activity leads to enhanced levels of aSyn which causes impairment in synaptic transmission. The identification of the novel functions of GCase in regulating neurotransmission and synaptic plasticity will help shed light on the mechanisms underlying its pathological roles. Altogether, our study enhances our understanding of synaptic regulation in PD which is a crucial step in our efforts to develop a disease-modifying treatment for PD.
P12.04
1 Icahn school of medicine at Mount Sinai, United States
Parkinson’s disease (PD) is marked by α-synuclein aggregation, dopaminergic neuron loss, and maladaptive microglial activation. A protective SNP, rs3732765-A, lies in a microglia-specific P2RY12 enhancer and lowers PD risk by reducingP2RY12 expression. P2RY12 regulates microglial chemotaxis and inflammation, but how genotype calibrates early microglial transitions, proteostasis, and crosstalk under α-syn stress is unknown.
The Multicellular Integrated Brain (miBrain) is a human iPSC-derived 3D neuroimmune system incorporating CRISPR-edited rs3732765-A (A/A) microglia and A53T SNCA-overexpressing neurons, enabling dissection of genotype-instructed programs during early α-syn aggregation.
Long-Term Goal: Define how rs3732765-A shapes microglial immune and proteostatic programs to confer resilience in synucleinopathies.
Objective: Identify P2RY12-dependent microglial signatures and contextualize their effects on multicellular responses.
Central Hypothesis: The rs3732765-A allele dampens over-activation and lysosomal hyperactivity, preventing astrocyte neurotoxicity and preserving neuronal health.
Aim1: Perform bulk RNA-seq of iMGL monocultures (G/G vs A/A) to identify genotype-dependent gene modules and pathways, compared with postmortem microglia.
Aim2: Use snRNA-seq of G/G and A/A miBrains to resolve cell states, quantify subtype composition, and map pathways and ligand–receptor networks.
Methods CRISPR-edited iPSC-derived microglia (G/G vs A/A) were embedded into MiBrains containing A53T α-synuclein–overexpressing neurons. Bulk RNA-seq identified baseline microglial signatures, while snRNA-seq resolved genotype-driven programs across microglia, astrocytes, and neurons. Analyses included differential expression, co-expression modules, pathway enrichment, and ligand–receptor inference, validated in genotype-stratified postmortem brains.
Results A/A microglia remained more homeostatic at baseline with dampened lysosomal activation. In MiBrains under α-syn stress, A/A microglia showed attenuated inflammatory responses, astrocytes biased toward neuroprotective modules, and neurons displayed preserved synaptic resilience.
Conclusions This work establishes the first cell-resolved atlas of miBrain responses to α-syn stress and shows that rs3732765-A calibrates microglial activation and proteostasis to support multicellular resilience, nominating early therapeutic targets.
P12.05
1 University of Rochester, United States
2 Parkinson's Foundation, United States
3 Tel Aviv Sourasky Medical Center and Columbia University, United States
Introduction: PD GENEration is an international genetic registry study that has provided genetic testing and counseling to >22,000 people with PD and identified PD-related genetic variants in ∼12%. The success of PD GENEration provides a unique opportunity to expand testing to family members of individuals with PD and PD-associated genetic variants and to inform understanding of family member interest in genetic testing. Here, we describe the design of the Parkinson’s Foundation PD GENEration Family Genetic Registry (PDGENE Family).
Methods: PDGENE Family will 1) provide genetic testing and counseling to family members of PD GENEration probands with autosomal dominant PD and 2) create a repository of genetic data and DNA samples for future research use. PDGENE Family will enroll individuals ≥ 40 years of age who are first-degree biological relatives of PD probands with a PD-associated genetic variant and interested in receiving PD-related genetic test results for the PD GENEration Primary Panel (GBA1, LRRK2, SNCA, VPS235, PRKN, PINK1, and PARK7) with optional return of Secondary PD and Non-PD related panels. PDGENE Family will initially focus on enrolling family members of probands with LRRK2 PD, with plans to expand to other autosomal dominant forms of PD. PD GENEration probands will be asked to consent to the sharing of their genetic test results with eligible family members and to provide contact information for potentially eligible family members. After enrolling either via a self-guided online process or at a study site, family member participants will complete a demographic and clinical survey, pre-test genetic counseling, sample collection, and post-test genetic counseling. Home-based self-collection of blood will be enabled by use of Tasso+ kits. De-identified samples and associated data will be shared with the Global Parkinson’s Genetics Program (GP2).
Results: PDGENE Family was approved by the Advarra Institutional Review Board in August 2025. We anticipate enrolling the first participant in October 2025.
Conclusion: By enabling the genetic testing and counseling of family members of individuals with autosomal dominant PD, PDGENE Family will inform understanding of interest in genetic testing, empower at-risk individuals, and create a pool of potential participants for future PD prevention trials.
This abstract has been accepted for presentation (without publication) at the Parkinson Study Group conference in December 2025.
P12.06
1 Eurac Research, Italy
2 Eurac Researcher, Italy
The generation of 2D neurons and 3D brain organoids is gaining exponential interest to investigate the causes of neurodegeneration, as these models permit to study human cells and tissue, and to reconstruct in vitro the pathophysiology of the human brain.
Given the neuropathology of Parkinson’s disease (PD), human modelling focuses on the use of patient iPSCs to derive midbrain and cortical neurons and organoids.
Our group has found the small GTPase Rit2 modulates lysosome function and validated its potential as therapeutic target for PD. In addition, we have implicated a Rit2-LRRK2-lysosome axis in PD pathogenesis.
To further advance the human relevance of this pathway, we employed 2D neurons and 3D organoids derived from induced pluripotent stem cells (iPSCs) from G2019S-LRRK2 PD patients and healthy controls, and engineered a control line via CRISPR-Cas9 to generate Rit2 KO cells.
Cortical neurons from G2019S-LRRK2 PD displayed reduction in Rit2 and Lamp1 immunosignals, consistent with Rit2 and lysosome depletion in familial and idiopathic PD. Since we observed altered lysosomal calcium release via TPC2 channel under Rit2 depletion, we explored lysosomal calcium and neuronal activity relation. Stimulation of TPC2 release increased neuronal firing, measured on Multi-Electrode Arrays, up to 30 min in control neurons, while activity in G2019S-LRRK2 quickly returned to basal levels. TPC2 protein levels were consistently reduced in G2019S-LRRK2 cortical neurons. To complement these results, we generated midbrain organoids and performed MEA recording. Stimulation of TPC2-mediated release increased neuron firing in control organoids, but it was less effective in G2019S-LRRK2 PD-derived organoids. Further, these models displayed reduced TH content and accumulation of phosphorylated Tau protein. Interestingly, long-term treatment with the LRRK2 kinase inhibitor PF-06447475 prevented the loss of TH. To further explore the role of Rit2 in this context, we generated midbrain organoids from Rit2 KO iPSCs, which displayed a decrease in the firing rate upon MEA recording. Consistently, Rit2 KO 2D midbrain neurons also showed reduced spontaneous action potential firing in whole-cell patch clamp experiments.
We are now generating forebrain organoids to investigate cortical processes. Indeed, forebrain organoids from G2019S-LRRK2 cells display defects in neural rosette formation, supporting a destructive effect of the mutation on brain physiology.
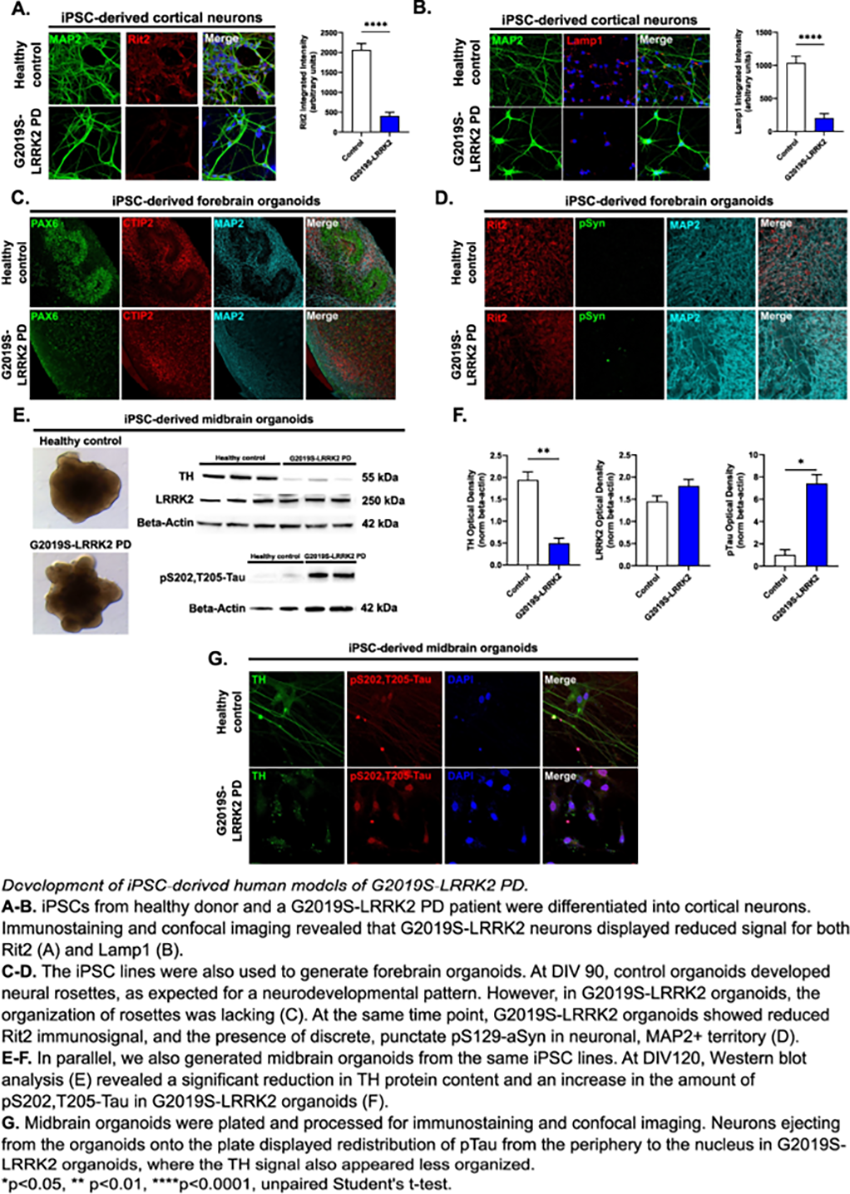
P12.07
1 Van Andel Institute, United States
2 AC Immune SA, Switzerland
Objectives: Parkinson's disease (PD) is the second most prevalent neurodegenerative disorder worldwide. It is characterized by the loss of dopaminergic neurons and the accumulation of pathological alpha-synuclein (αSyn), particularly in its phosphorylated form at serine 129 (pSer129). Although genetic evidence strongly supports a central role for αSyn in PD pathogenesis, the precise timing of its aggregation during neuronal maturation remains unclear.
Methods: Induced pluripotent stem cells (iPSCs) from six individuals carrying the SNCA p.A53T mutation and six healthy controls were differentiated into midbrain spheroids and matured for up to 150 days. Phosphorylation and aggregation of αSyn were monitored longitudinally using immunostainings, biochemical analyses, aggregation assays, and binding of a tracer specific for aggregated αSyn. Omics analyses were used to identify cellular pathways and network-level changes associated with αSyn pathology.
Results: iPSC-derived midbrain spheroids from SNCA p.A53T carriers spontaneously developed pSer129-positive αSyn aggregates during extended post-differentiation culture. These aggregates are insoluble, resistant to proteinase K digestion, amyloid-specific OC antibody-positive, and demonstrate seeding competence in protein misfolding cyclic amplification (PMCA) assays. In collaboration with AC Immune, we confirmed the presence of bona fide fibrillar αSyn species using a proprietary ACI-12589, a clinically validated tracer that selectively binds to αSyn fibrils, thereby independently confirming their fibrillar nature. Furthermore, transcriptomic profiling revealed disease-specific gene expression changes in PD spheroids compared with controls that correlated with the αSyn aggregation process.
Conclusions: Our integrative approach demonstrates that αSyn aggregation initiates during neuronal maturation in PD iPSC-derived midbrain spheroids and is associated with distinct transcriptional alterations. These findings indicate that PD spheroids capture early pathogenic events and exhibit disease-specific molecular signatures, supporting their utility for patient stratification. Moreover, the selective detection of αSyn with ACI-12589 underscores the translational potential of this model as a platform for testing and screening anti-aggregation compounds.
P12.08
1 Van Andel Institute, United States
2 Lund University, Sweden
3 Umeå University, Sweden
4 Van andel Institute, United States
5 Exeter University, United Kingdom
Aims Parkinson’s disease (PD) and multiple system atrophy (MSA) share overlapping pathological features, yet their molecular drivers remain incompletely understood. We aimed to delineate mechanisms of neurodegeneration by integrating proteomic, phosphoproteomic, and metabolomic analyses on patient-derived midbrain organoids.
Methods Induced pluripotent stem cells (iPSCs) from PD patients (familial and idiopathic), MSA patients, and healthy controls were differentiated into midbrain spheroids and aged to 100 days. Spheroids were analyzed using label-free shotgun proteomics, phosphoproteomics, and metabolomics (GC/LC-MS). Differential expression (limma eBayes), Weighted Gene Co-expression Network Analysis (WGCNA), and pathway enrichment identified dysregulated networks. Findings were verified in post-mortem brain tissue.
Results PD and MSA midbrain spheroids exhibited comparable cellular composition and, despite representing clinically distinct synucleinopathies, shared widespread proteomic alterations involving mitochondrial dysfunction, lysosomal-autophagy, ubiquitin-proteasome activity, and immune pathways. A central axis of metabolic disruption was identified, encompassing glucose, branched-chain amino acid (BCAA), and lipid metabolism. Metabolomics revealed impaired glycolytic flux, pyruvate accumulation, depletion of TCA intermediates, disrupted BCAA catabolism, and compensatory peroxisomal β-oxidation. Phosphoproteomics highlighted dysregulation of kinases regulating glycolysis, BCAA degradation, energy sensing (AMPK, AKT), mTOR, PKA, and PKC signaling, linking metabolic stress to membrane remodeling and inflammatory responses. These metabolic signatures were conserved in post-mortem PD and MSA brain tissue.
Conclusions Our integrative multi-omics approach identifies metabolism as a central hub of dysfunction in PD and MSA, connecting impaired energy production, protein homeostasis, and membrane remodeling. These findings position metabolic dysregulation as a unifying molecular hallmark across synucleinopathies and highlight potential therapeutic targets to restore metabolic balance.
P12.09
1 First Dept of Neurology, National and Kapodistrian University of Athens Medical School, Greece
2 Biomedical Research Foundation of the Academy of Athens, Greece
3 University Mental Health Research Institute, Greece
4 Institut Francois Jacob (MIRCen), CNRS, CEA and Laboratory of Neurodegenerative Diseases, Fontenay-aux-Roses, France
5 Alexander Fleming Biomedical Sciences Research Center, BSRC, Greece
6 University Mental Health Research Institute, UMHRI, Greece
Our main aim is to unravel the biochemical properties of the novel A30G α-synuclein (α-syn) mutant in a cellular context, deciphering the mechanisms governing aggregation and neurotoxicity, leading to a better understanding of Parkinson’s Disease pathogenesis. Hence, we constructed stable SH-SY5Y neuroblastoma cell lines overexpressing at comparable levels WT or A30G α-syn and assessed the proteomic profile, a-syn conformations, the α-syn-induced neurotoxicity and various related cell indices, as well as the seeding propensity of A30G α-syn compared to WT upon neuronal differentiation with retinoic acid. In the proteomic analysis, we observed differences regarding several metabolic pathways involved in neurodegenerative disease pathology, i.e. cellular cell response, membrane organization, lysosome and mitochondria homeostasis. We assessed A30G α-Syn-induced neurotoxicity by measuring ROS levels, mitochondrial transmembrane potential, caspase activity and cell viability. Neuronally differentiated A30G cells displayed an early pattern of oxidative and mitochondrial stress and decreased TH levels, accompanied by caspase 3 activation and increased cell death. Surprisingly, A30G cells displayed much lower levels of Triton-soluble and insoluble oligomeric and S129-phosphorylated asyn species relative to WT. This was accompanied by reduced membrane binding. Using WT and A30G α-syn recombinant fibrils (PFFs) in WT and A30G differentiated neuroblastoma cells, as well as in WT iPSC-derived dopaminergic neurons, we examined seeding and aggregation of endogenous α-syn, as well as the induced cell stress. Upon WT PFF addition, seeding and aggregation of endogenous α-syn occurred within 4 days of PFF incubation, resulting in the accumulation of insoluble α-syn species, that were further increased when A30G PFFs were used in both cell models. A30G PFFs induced ROS production in both neuroblastoma cell lines, while A30G cells exhibited increased oxidative stress regardless of the PFF strain. Our results highlight that the enhanced neurotoxicity of A30G α-syn is accompanied by its reduced oligomerization and phosphorylation in a cellular context, while in its fibrillar form it is more potent than WT in seeding endogenous a-syn, propagating pathology.
P12.10
1 Denali Therapeutics, United States
Parkinson’s Disease (PD) is characterized by progressive, debilitating motor and non-motor symptoms resulting from a combination of genetic and environmental factors. Variants in GBA1 are among the most common genetic risk factors for PD, as 5% to 20% of PD patients across populations carry GBA1 variants. GBA1 encodes the lysosomal hydrolase beta-glucocerebrosidase (GCase), and pathogenic GBA1 variants ultimately result in reduced lysosomal GCase activity associated with lysosomal dysfunction. However, only a subset of GBA1 pathogenic variant carriers develop PD, suggesting the presence of additional genetic modifiers that influence both GCase activity and penetrance of GBA1-PD mutations. Moreover, deficits in GCase activity have been demonstrated in sporadic PD (sPD) cases, suggesting a broader role for GCase in the pathogenesis of PD. To discover genetic regulators of GCase activity, we performed genome-wide, loss-of-function (LoF) CRISPR-Cas9 screens in cells expressing wild type GBA1 or E326K, the most common GBA1 variant associated with PD. Endolysosomal GCase activity was measured using a selective, fluorescence quenched GCase substrate, and knockouts with reduced or increased GCase activity were collected by fluorescence-activated cell sorting and identified by next-generation sequencing. The screen revealed 688 putative suppressors and enhancers of GCase activity. Using data from the latest PD GWAS study in Europeans, we found that half of the 134 known PD-associated loci contain at least one GCase activity screen hit and that PD heritability is significantly enriched in genomic regions defined by screen hits. Furthermore, gene burden analysis of rare, predicted LoF variants from 4 independent PD case-control whole exome sequencing datasets revealed dysregulated GCase activity as a major node of PD genetic risk. Taken together, our work uncovers genetic modulators of GCase activity, providing a framework to investigate how these genes may influence the penetrance of GBA1 mutations and contribute to genetically-driven reductions in GCase activity in sPD.
P12.11
1 Florida International University, United States
Background: Dysfunction of the autophagy–lysosome pathway is strongly implicated in Parkinson’s disease (PD) pathogenesis. Paraquat (PQ), a herbicide linked to increased PD risk, has been shown to disrupt autophagy; however, the underlying mechanisms remain unclear. We recently reported that manganese, which causes parkinsonism, impairs lysosomal acidification and autophagic flux through a mechanism prevented by DRP1 inhibition (PMID: 38504290). Here, we investigated how PQ affects lysosomal function and whether this effect is influenced by DRP1 activity.
Methods: Six-month-old heterozygous DRP1 knockout (Dnm1l+/−) and wild-type (Dnm1l+/+) mice were injected intraperitoneally with PQ (10mg/kg every other day for five doses) or saline. Rat dopaminergic N27 cells were treated with PQ (100μM, 24h) with or without the DRP1 inhibitor P110 (1 μM). TFEB phosphorylation (Ser142), cytosolic and nucleus TFEB, and autophagy markers (p62, LC3-II) were assessed using immunoblotting. v-ATPase subunit expression was quantified using qPCR. v-ATPase enzymatic activity was measured in lysosomes isolated by ultracentrifugation. Publicly available transcriptomic data (GSE89562) from PQ–Maneb-treated mouse nigrostriatal tissue were analyzed for genes regulating v-ATPase assembly.
Results: Immunoblotting showed increased p62, LC3-II, and TFEB-S142 levels in WT mice injected with PQ but significantly attenuated in Dnm1l +/- littermates. Consistent with these observations, rat dopaminergic neuronal N27 cells showed impaired TFEB translocation from the cytosol to nucleus by PQ. Furthermore, several TFEB downstream genes that encodes the proton Transporting V0 and V1 Subunits of vATPase, were also reduced. DRP1 inhibition improved TFEB, autophagy flux and vATPase activity against PQ-induced neurotoxicity. Our results are further supported by secondary data analysis showing reduced lysosome v-ATPase related transcription in animals exposed to PQ-Maneb.
Conclusions: Our findings identify DRP1 as a key mediator of PQ-induced lysosomal dysfunction. PQ impairs autophagy by inhibiting TFEB activation and reducing v-ATPase expression and activity, leading to compromised lysosomal acidification. Combined with our previous manganese study, targeting DRP1 may protect against environmental toxin–induced parkinsonism by preserving autophagy–lysosome function.
P12.12
1 Department of Molecular Neurology, University Hospital Erlangen, Friedrich-Alexander University, Erlangen-Nürnberg (FAU), Germany, Germany
2 Institute of Anatomy, Functional and Clinical anatomy, Friedrich-Alexander University, Erlangen-Nürnberg (FAU), Germany, Germany
Variants in GBA1, encoding the lysosomal enzyme β-glucocerebrosidase (GCase, gene name GBA1), are among the most common genetic risk factors for Parkinson’s disease (PD). The interaction between GCase and its lysosomal transporter, the lysosomal integral membrane protein 2 (LIMP-2), is essential for proper lysosomal trafficking and enzymatic activity. Previous work from our group demonstrated that co-expression with LIMP-2 enhances lysosomal localization and activity of GCase, including the common PD-associated variant p.E326K. Notably, a lysosome-targeting peptide derived from LIMP-2 significantly increased lysosomal GCase activity in patient-derived fibroblasts harboring the GBA1-E326K mutation (Dobert et al. 2024).
To further characterize lysosomal function and the role of LIMP-2 in a disease-relevant context, we generated dopaminergic neurons differentiated from induced pluripotent stem cells (iPSCs). These iPSCs were reprogrammed from PD patient-derived fibroblasts of two individuals (GBA1wt/E326K) identified at our outpatient clinic. We characterized these GBA-PD neurons to analyze GCase activities, LIMP-2 maturation, a-syn accumulation and lysosomal function, to gain insights into the molecular mechanisms of GBA-PD. These GBA-PD neurons exhibited decreased GCase activity, accumulation of pathological alpha-synuclein and differential LIMP-2 glycosylation and maturation patterns, relative to healthy control neurons. We are currently evaluating GCase-targeting therapies in these neurons to assess their potential to activate GCase enzymatic function, and reduce GluCer accumulation and α-synuclein pathology in these neurons. Taken together, our work establishes a patient-derived neuronal model to study GBA1 biology, GBA1-linked pathology and evaluate GBA1-targeted therapeutic strategies.
COMPREHENSIVE CARE: Caregiving, relationships, respite care, families
P13.01
1 University of Southampton, United Kingdom
2 Northumbria University, United Kingdom
3 Public contributor, United Kingdom
Introduction: Cognitive impairment is a well-recognised and common complication of Parkinson’s disease, associated with significant clinical impact and increased carer distress. Carers provide a vital role in helping maintain quality of life in people with Parkinson’s and cognitive impairment (PwP-CI). However, a lack of adequate carer support can lead to carer breakdown and avoidable health and social care costs. The iSupport-PD programme aims to adapt a globally available digital cognitive behavioural intervention for dementia carers (iSupport) to meet the specific needs of carers of PwP-CI. The current study aimed to explore the challenges faced by this group to inform the intervention adaptation.
Methods: Thirty-three semi-structured and think-aloud interviews were conducted with 31 carers of PwP-CI living in the United Kingdom. Participants were recruited through charities, support groups, social media, and via the networks of our Patient and Public Involvement group. Purposive sampling was used to recruit diverse carers. Interviews were recorded, transcribed and analysed using inductive reflexive thematic analysis.
Results: Carers shared how the complex, gradual, and fluctuating nature of cognitive impairment often led to a lengthy and frustrating diagnosis process for the PwP-CI. Carers experienced feelings of exhaustion, overwhelm, and anxiety in the face of unpredictable and challenging behaviours (e.g. aggression, changes in judgement) and in response to taking on more of the ‘cognitive load’ from the PwP-CI. Carers were often reluctant to ask for help from others, restricted by feelings of pride or duty, or worries about being a ‘burden’ to others. Changes to the PwP-CI’s personality and mood, evolving relationship dynamics, and restrictions to their social life left carers with a sense of loss that further exacerbated feelings of loneliness. Carers also shared strategies that helped them to cope with their role.
Conclusions: Support interventions should be tailored to the unique needs of carers of PwP-CI, supporting them to navigate complex and fluctuating symptoms, overcome barriers to seeking professional and social support, and develop coping strategies to minimise the impact of the caring role on their own physical and mental health. Findings were used to inform the creation of guiding principles, outlining how the needs and challenges of carers of PwP-CI were addressed in the digital intervention.
P13.02
1 Western University, Canada
2 Macquarie University, Australia
Introduction: Individuals living with Parkinson’s disease often depend on informal caregivers to support their daily activities. While existing literature highlights some positive aspects of caregiving, it largely underscores the significant burden caregivers may experience. This burden can manifest as stress, anxiety, depression, and physical exhaustion. Despite their critical role in reducing healthcare costs and improving patient outcomes, informal caregivers frequently lack access to resources that address their wellbeing and mitigate caregiver burden. If left unaddressed, this burden can lead to burnout and compromise their ability to continue providing care. Internet-based cognitive behavioural therapy is an emerging solution that offers several advantages over traditional in-person therapy, including greater accessibility, flexibility, and cost-effectiveness. The aim of this study is to adapt a previously developed internet-based cognitive behavioural therapy wellbeing program to better support the unique needs of caregivers of individuals with Parkinson’s disease.
Methods: A patient-oriented steering committee guided the adaptation of the program. The committee included eight caregivers of individuals with Parkinson’s disease, three representatives from Parkinson Society Southwestern Ontario, and three research team members. Participants independently reviewed the program’s content and presentation of materials, providing feedback on areas for refinement. This iterative process continued until at least 70% of participants agreed that the modules were suitable and appropriate for this caregiver population.
Results: Feedback and subsequent program modifications focused on four key areas: i) language and readability, ii) design and flow, iii) content relevance, and iv) development of ecologically valid case studies.
Conclusion: Caregivers of individuals with Parkinson’s disease face distinct physical, emotional, and cognitive challenges that are not adequately addressed by current support systems. This adapted program will offer caregivers a flexible and accessible resource to help them better manage the demands of caregiving. A second phase will involve conducting a pilot trial to assess the program’s feasibility, acceptability, usability, and practicality. Preliminary data will also be collected to evaluate its impact on caregiver wellbeing.
P13.03
1 Singapore General Hospital, Singapore
Background Caregivers are central to the long-term management of people with Parkinson’s disease (PwP). They enable PwP to remain in their communities, while reducing healthcare utilisation and economic burden on society. Despite their vital role, caregiving is associated with significant physical, emotional, and psychosocial strain. To ensure sustainability of care, it is essential to support caregivers and safeguard their health and quality of life.
Objective This study evaluated caregiver burden and health-related quality of life (HRQOL) among caregivers of PwP in Singapore, following participation in a two-year community-based care programme.
Methods Data from 146 caregivers were analysed. The programme involved home visits by community nurses and physiotherapists to support PwP and their caregivers. Caregiver strain was assessed using the Zarit Burden Interview (ZBI); HRQOL was assessed using the EuroQOL five dimensions (EQ-5D-5L); and health status using EuroQol Visual Analogue Scale (EQ5D-VAS). These outcomes were measured at baseline, 1 and 2 years. The Friedman’ s test was used to analyse changes in outcomes across time. Significance set at p < 0.05.
Results The majority of caregivers were cohabiting family members, most commonly spouses, children, and siblings. Caregivers were predominantly female (61%, n=89), and more than half were unemployed (53%, n=45). One-quarter had domestic helper support. (ZBI) increased over time (baseline median = 22; Year 1 = 32; Year 2 = 30), though the change did not reach statistical significance (χ2 = 5.26, p = 0.07). (EQ5D-VAS) significantly declined (baseline median = 80%; Year 1 = 75%; Year 2 = 70%; χ2 = 7.82, p = 0.02). EQ-5D-5L dimensions showed progressive worsening across domains, though without statistical significance.
Conclusion Despite implementation of a structured, community-based care programme, caregivers of PwP experienced a significant decline in self-reported health status over two years, accompanied by a non-significant increase in caregiver burden. These findings highlight that current support is insufficient to fully address the emotional and physical toll of caregiving. Care programmes for PwP should integrate targeted caregiver support, particularly in the areas of emotional resilience and coping strategies. Support groups, peer-sharing platforms, and structured caregiver education may provide critical avenues for sustaining caregiver well-being while ensuring optimal care for PwP.
P13.04
1 Kristianstad University, Sweden
2 Linköping University and hospital, Sweden
Introduction One way to support the care partners of persons with Parkinson’s disease could be to increase their knowledge of the disease including its symptoms and therapy and to provide them with self-care advice and strategies to increase their experience of well-being. To investigate what information care partners need in relation to caring for a person with Parkinson’s disease, the aim of this study was to explore care partners’ information needs when caring for a family member with Parkinson’s disease.
Methods A qualitative study was conducted where fifteen care partners to persons with Parkinsońs disease representing all stages of disease were interviewed in focus groups, individually or in pairs, using open-ended questions. Data was analysed using reflexive thematic analysis.
Results The analysis revealed four themes that describe care partners’ information needs: (1) to be prepared when symptoms limit daily life, (2) to preserve participation and social life, (3) to find reassurance together with others and (4) to cope with uncertainty.
Conclusion This study suggests that care partners need timely, relevant information – such as how to prepare for changes in everyday life, maintain social participation and cope with uncertainty – to feel supported in their caregiving role. The results demonstrate the need for person-centred information meeting the care partners’ physical, social, emotional and existential needs. This calls for holistic information-based interventions built on collaboration between healthcare professionals, the person with Parkinson’s disease and the care partner, aimed at promoting care partners’ well-being and helping them support their family member with Parkinson’s disease. The themes identified in this study can be used as a guide when planning to provide information-based interventions to care partners to persons with Parkinson’s disease.
P13.05
1 Parkinson Voice Project, United States
More than 80% of people with Parkinson’s disease develop dysphagia (Suttrup & Warnecke, 2015), and up to 95% experience voice and communication difficulties (El Sharkawi et al., 2002). These impairments significantly impact quality of life and lead to social withdrawal. Parkinson’s disrupts learned, automatic movements such as walking, talking, and swallowing due to dysfunction in the basal ganglia (Yin & Knowlton, 2006). Resulting speech deficits often include hypokinetic dysarthria—marked by reduced vocal intensity, limited articulatory movement, and diminished prosody (Duffy, 2005).
SPEAK OUT!® Therapy, developed in 2010, empowers people with Parkinson’s to regain and retain speech and swallowing by shifting speech from an automatic function to an intentional act. Building on the work of the late Dr. Daniel R. Boone, the program teaches individuals to activate the direct motor pathway, improving vocal volume, articulation, and intonation.
However, the success of SPEAK OUT! Therapy is not achieved alone. Care partners determine long-term success. As the primary communication partner, the care partner shapes the environment where speech is practiced and retained. Their involvement makes the difference between limited progress and meaningful gains. By attending therapy sessions, learning to cue with INTENT, and reinforcing strategies at home, care partners become active members of the therapy team and powerful agents of change. Consistent support strengthens carryover, builds confidence, and ensures generalization into daily life.
This presentation will include case studies and video samples from before and after SPEAK OUT! treatment, illustrating the power of collaborative care. Strategies for the care partner will be taught, including:
Attend SPEAK OUT! Therapy sessions Learn the most effective cue for the person with Parkinson’s Role play cueing with INTENT Use the SPEAK OUT! Therapy Flashcards and eLibrary for home practice Record speech with and without intent for comparison Use the “King’s X” card to reset communication
The SPEAK OUT! Therapy Program not only provides a structured pathway for speech and swallowing improvement It provides a shared mission. When care partners engage fully, they give their person with Parkinson’s voice, confidence, and hope for the journey ahead.
P13.06
1 Newcastle upon Tyne Hospital NHS Foundation Trust and Northumbria University, United Kingdom
2 Public contributor, United Kingdom
3 Northumbria University, United Kingdom
4 University of Southampton, United Kingdom
Introduction Changes in cognition are a well-recognised complication of Parkinson’s with significant clinical impact. As symptoms progress, people with Parkinson’s (PwP) require increasing support from an (unpaid) care partner to help maintain quality of life. Lack of adequate support can lead to carer breakdown and avoidable hospital and social care costs. Despite their important role, there is a scarcity of support for carers of PwP with cognitive impairment. We have developed SPARC, a digital intervention to prevent and/or decrease the mental and physical health problems associated with caring and improve the quality of life for carers of PwP and cognitive impairment. The aim of the study was to determine the feasibility and acceptability of SPARC.
Methods The iSupport-PD study was a parallel, two-arm, feasibility Randomised Control Trial (RCT) with an embedded pilot health economic analysis and mixed-methods process evaluation. Data on numbers of participants identified, recruited, commenced and finished was collected. Secondary outcomes included validated outcome measures, National Health Service (NHS) and social care resource use and health economic data long with participant demographics such as age, relationship to PwP, and gender. Consented participants were randomised using a 1:1 ratio to either the intervention or usual support (control group). Data were collected at baseline, 3, 6,12 months. As part of our process evaluation, SPARC usage data was collected to understand engagement. Semi-structured interviews were conducted with the intervention group to understand the acceptability and usability of SPARC.
Results.
We recruited 92 carers from across the UK, via Parkinson’s UK, social media, Parkinson’s support networks and Parkinson’s specialist NHS clinics. Preliminary follow-up rates are high at 3months (78% Intervention, 79% Control) and 6months (69% Intervention, 78% Control). 12month follow-up is ongoing. Usage data demonstrated good engagement with SPARC at 84%. In the interviews, carers reported that SPARC was easy to use, the information was clear, and the content was relevant and meaningful to them.
Conclusion We were able to successfully recruit to our feasibility RCT and demonstrated good trial retention, intervention engagement and acceptability. We now plan to secure a further funding to conduct a fully powered clinical effectiveness study and explore implementation plans to embed SPARC into health and care practise across the UK.
P13.07
1 University of Southampton, United Kingdom
2 Northumbria University, United Kingdom
3 Public contributor, United Kingdom
Introduction: Most care needs of people with Parkinson’s with cognitive impairment (PwPCI) are met by informal carers. Such carers report higher carer burden and poorer quality of life and physical and mental well-being, compared to carers of people with Parkinson’s without impairment and carers of those with other dementias. Despite the important role they provide, there is a lack of support for carers of PwPCI. The iSupport-PD programme aimed to adapt a globally available digital cognitive behavioural intervention for dementia carers (iSupport) to meet the specific needs of carers of people with PwPCI (SPARC).
Methods: The adaptation was guided by the Person-Based Approach to intervention development, informed by: (1) co-production with carers, people with Parkinson’s, health and social care professionals, and the Parkinson’s UK charity; (2) qualitative literature on Parkinson’s carer needs and experiences; and (3) qualitative semi-structured and think-aloud interviews with 31 carers of PwPCI. Guiding principles highlighted key intervention design objectives and features to address the needs of this target group to maximise user engagement.
Results: Adaptation work highlighted the need for additional intervention content addressing the unique complexities of cognitive impairment in Parkinson’s and improvements to user engagement. Such modifications included: (1) educational content about behavioural changes unique to cognitive impairment in Parkinson’s; (2) stories from diverse carers to normalise and provide encouragement to carers to seek support; and (3) use of empowering, destigmatising, and lay-friendly terminology. Carers in the think-aloud interviews found the intervention content relevant, helpful and easy to understand. They valued the stories and advice from other carers, practical advice on how to deal with challenging symptoms, and the focus on non-medical aspects of caring (e.g. communication, involving others). Negative feedback was used to further optimise SPARC.
Conclusions: A SPARC intervention prototype was developed using rigorous co-production methodology. Our guiding principles highlight key design objectives and features to consider when developing interventions for carers of PwPCI. Subsequent think aloud interviews helped optimise the intervention and demonstrated that SPARC is likely to be acceptable to this population. A randomised control trial is currently underway to assess intervention feasibility and acceptability.
P13.08
1 University of Rochester, United States
2 City of Hope, United States
3 University of Massachusetts, Dartmouth, United States
Objectives: Inadequate preparedness to meet the high caregiving needs of persons with Parkinson’s disease and Lewy-body dementia (PwP) puts both carers and patients at high risk for poor health outcomes. To improve holistic support for carers it is important to go beyond the construct of “caregiver burden” and understand carers’ perspectives on caregiving and what matters most to them. The purpose of this study was to use Perspective Mapping, a novel hybrid mixed method technique to understand (a) carers’ perceptions and experiences, and (b) what matters most to them.
Methods: We conducted video interviews with current carers of PwP in the United States of America (USA) using Perspective Mapping to elicit their perspectives and experiences. Prior to the interview, study participants received a document with nine caregiving domains (e.g., Caregiving Preparedness, Decision-Making, Spiritual, Social & Cultural, Emotional, and Preserving Self) and related key concepts. During the interview a visual of the map created with a mind-mapping software was presented and served as a framework for the discussion. Using their notes participants responded to questions to describe (a) the domains that mattered most and second most to them and (b) their experiences with the key concepts associated with the domains. Data were collected until there was evidence of saturation. The sum of the domain rankings (what mattered most and what mattered second most) was calculated.
Results: Participants (n=20) were predominantly female (75%) Caucasian spouses (95%). Carers reported that the perspective map helped them reflect, understand, and discuss their needs in a more meaningful way. They described the challenges related to caring for themselves, and feelings of gratitude for being able to provide care. The domains that mattered most and second most were Preserving Self (62%), Emotional (30%), Decision Making (29%), and Care Coordination (23%).
Conclusion: Our findings demonstrate that Preserving Self through the key concepts such as getting physical respite, maintaining own identity, guilt management, and being kind to self is important. These findings will inform the development of a peer-led intervention targeting what matters most to caregivers. Perspective mapping is a promising method to elicit what matters to carers.
This work was presented at International Neuropalliative Care Society Annual Meeting on September 11, 2025.
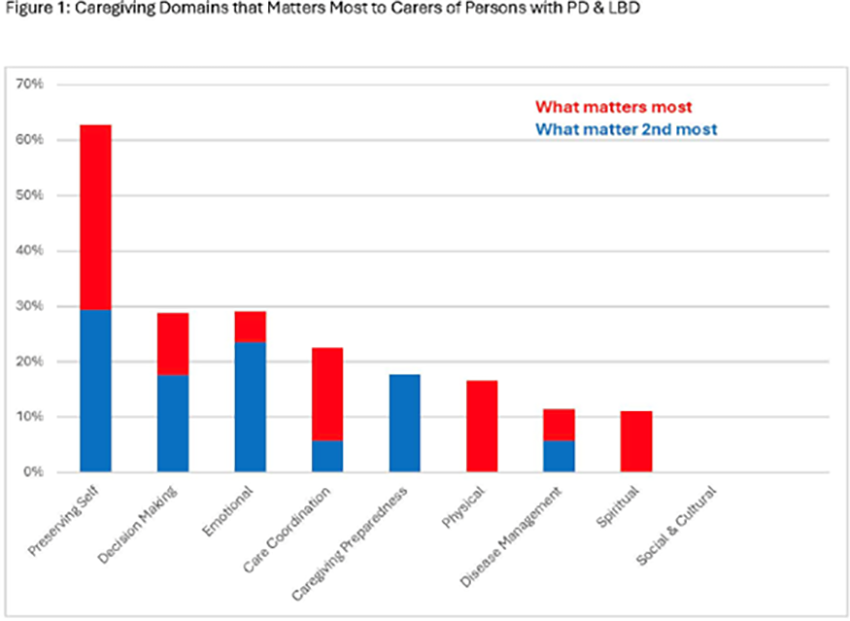
P13.09
1 Linköping University, Sweden
2 Linköping University, Linköping, Sweden
Swedish advanced-level nursing education in neurocare must address the complex needs of patients with Parkinson’s Disease (PD) as well as their care partners (CPs). Providing nursing interventions and support related to the management of PD, requires advanced clinical competencies and skills in collaborative care strategies.
Combining disease specific information with a model used in medical pedagogy, this study integrates clinical realities with educational design. The model of the didactic triangle is addressing the why (purpose), what (content), and how (pedagogy). The purpose, the why, pertains to the necessity for well-educated specialist neuro care nurses to provide high-quality care to patients with PD and CPs. This necessity leads to the identification of the content, the what, that is relating to disease specific knowledge and understanding of CP burden. By defining the specific content, nursing education can be refined to prepare future neuro care nurses for appropriately supporting patients with PD and CP in their professional role. The pedagogy, the how, refer to the educational interventions that can be employed in the advanced-level nursing programme to meet the nursing students learning objectives and ultimately fulfil the purpose. The aim of this study is to identify how practical skills and disease specific knowledge of PD can be integrated in Swedish advanced-level nursing education in neurocare.
The didactic triangle – defining why, what and how - will be used as a guiding framework to explore the needs and educational requirements of advanced-level nursing students in supporting both CPs and patients with PD. Group Concept Mapping will be utilised to define the educational needs for specialist nurses in the field of neurocare. By bringing together important stakeholders including patients living with PD, their CPs, clinical staff, organisational leaders, researchers and higher education teachers, the method explores and defines educational needs in a co-productive manner. The results will inform future educational design and the pedagogy to integrate this into the advanced- level neuro care nursing programme.
This study contributes to the refinement of the Swedish advanced-level nursing curricula in neurocare, bridging the gap between higher education and clinical practice, and promoting transformative learning that will ultimately improve PD care and patient and CPs outcomes in Sweden.
P13.10
1 Iowa State University, United States
Care partners (CPs) of those with Parkinson’s disease fulfill many roles and frequently report feelings of emotional isolation, lack of appreciation, and overwhelming fatigue. Moreover, CPs in rural areas often report a lack of resources. The Caregiver Buddy App was developed to offer a warm, gentle, and emotionally intelligent mobile environment designed to provide practical support, emotional validation, and subtle moments of connection and reflection, addressing the unique needs of CPs of those with PD. The purpose of these study was to obtain feedback on the initial design from key stakeholders.
Qualitative analysis of initial interviews with CPs provided the basis for the initial design of the app. A workshop was then held for CPs and key stakeholders to provide feedback on the initial design. Sixteen participants were first provided an overview of the app design and then divided into four focus groups. Groups discussed and presented their thoughts on what elements were missing and which design concepts were unclear. Groups then ranked the features of the app from “needs improvement”, to “strong interest”, to “must have”. Results revealed that 80% of the feedback collected was positive. Among the most well-received features were essential elements that safeguarded users’ privacy, supported emotional well-being, and provided autonomy in social interaction. Gamified elements such as badges and achievement-based tracking were largely met with resistance. Many CPs expressed discomfort with competitive reward systems, noting that caregiving is a deeply personal and emotionally complex experience. They preferred features that acknowledged progress quietly and meaningfully, rather than through public or gamified displays. Privacy was another key concern. CPs wanted complete control over what they shared and with whom. To address these needs, the design team has future plans to translate the user feedback into actionable refinements. Specifically, future research will be completed to better understand the use of gamified elements by CPs. It is hoped that this user-centered approach will not only reduce barriers to engagement but also affirm the dignity and humanity of the caregiving experience.
P13.11
1 Fondazione Pezzoli per la Malattia di Parkinson, Milan, Italy; Parkinson Institute, ASST Gaetano Pini-CTO, Milan, Italy, Italy
2 ASST Gaetano Pini-CTO, Milan, Italy, Italy
3 Fondazione Pezzoli per la Malattia di Parkinson, Milan, Italy; ASST Gaetano Pini-CTO, Milan, Italy, Italy
4 Fondazione Pezzoli per la Malattia di Parkinson, Milan, Italy, Italy
5 Parkinson Institute, ASST Gaetano Pini-CTO, Milan, Italy, Italy
Background: Parkinson’s Disease (PD) is characterized by a combination of motor and non-motor symptoms, significantly affecting patients’ and families’ quality of life (Martinez-Martin et al., 2011). Effective management requires an integrated approach also addressing non-motor challenges (Lidstone et al., 2020). Patients and caregivers often experience uncertainty and difficulties adapting to the chronic, progressive nature of PD.
Goals: To address these complex needs and provide comprehensive informational support, including disease education, self-management strategies, and guidance on healthcare and social services.
Methods: The Parkinson’s Disease and Parkinsonism Family Center, established at the Parkinson Institute, ASST Pini-CTO, Milan, promoted by the Pezzoli Foundation for Parkinson’s Disease and funded by ATS Milan grants, is now in its second year. It represents an innovative service within the Lombardy public healthcare system, bridging diagnostic and treatment centers with local healthcare, administrative and social services, and providing psychoeducational interventions for patients and families. Activities include individual and family psychoeducational sessions, informational support via the 'family care' service, newly introduced peer-support groups, and a family assistance desk providing welfare and administrative guidance. All services are free for patients. Users complete satisfaction questionnaires at the end of their participation.
Results: In its first year, 215 users (94 M, 121 F; mean age 64.6) contacted the service, and 182 (88 patients, 94 caregivers; mean age 64.3) completed the program. Thirty-five users were exclusively connected to local services, while 147 also attended psychoeducational sessions. Satisfaction questionnaires yielded a mean score of 4.33/5, with the greatest improvements in disease knowledge, management of patient-related challenges, interpersonal relationships, and awareness of local services.
Conclusions: Structured psychoeducational and informational services improved disease knowledge, interpersonal relationships, management of patient-related challenges, and awareness of local services. These outcomes suggest enhanced coping, psychological adaptation, and social support. Peer-support groups and the family assistance desk are expected to further reinforce these benefits. In the second year, we aim to consolidate results and provide a replicable, integrated, multidisciplinary model for comprehensive PD care.
P13.12
1 Bayer AG, Germany
2 Kielo Research, United Kingdom
3 Kielo Research, Switzerland
4 Parkinson & Movement Disorder (PMD) Alliance, United States
Introduction Advanced therapies for Parkinson’s disease (PD) may be considered when oral medications become inadequate. However, little is known of treatment preferences for advanced therapies among moderate-stage patients with PD (PwP) and their care partners (CP).
Methods We conducted qualitative interviews with 20 USA PwP-CP pairs (n=40) recruited via PMD Alliance. PwP had moderate-stage: minimum 4 years post-diagnosis, motor fluctuations or dyskinesia, use of oral PD medications, and no prior advanced PD therapies. Interview transcripts underwent content analysis.
Results Participant characteristics: Overall median (IQR) age was 63 (58-72) years and 88% White; 65% PwP and 50% CP were female. PwP had median PD diagnosis of 6 (5-10) years and 90% on levodopa regimen. CP provided median 7 (4-15) hours/week of care.
Perceived disease severity: 55% of PwP and 30% CP perceived PD severity as mild; 40% PwP and 65% CP as moderate. Consensus amongst participants that PD progression has remained steady slow (83%), with 65% anticipating future deterioration, and 78% expect treatment plans to change.
General factors for advanced PD treatment: Within the dyad, PwP remain the primary decision-maker. New treatment information came from other patients (80% PwP vs 50% CP), internet searches (60% vs 70%), advocacy groups (80% vs 50%), and healthcare practitioner (HCP) (65% vs 50%). Major treatment considerations were risks (70% vs 45%), benefits (45% both), efficacy (40% vs 35%), scientific evidence (30%), and HCP recommendation (10% vs 35%). Major barriers to treatment uptake were cost (30% vs 40%), risks (25% vs 20%), and administration mode (15%).
Determinants of uptake for new advanced PD treatments: Major willingness factors included disease/symptom progression (90%), daily levodopa impact (90% vs 75%), reduced dependence on others (80% vs 70%), and treatment benefits (70%). For disease progression, CP were more willing if progression/symptoms appear (80% vs 90%), while PwP were more motivated by losing ability to walk (10% vs 0%) or HCP discussion (5% vs 0%). For levodopa impact, PwP were more favorable if reduced frequency (80% vs 70%) and avoided side effects (20% vs 10%).
Conclusion This dyadic PwP-CP study is the first to examine factors influencing treatment decisions for advanced PD therapies. These results highlight key similarities and differences between PwP and CP decision process, as well as how expected disease progression impacts treatment acceptability.
P13.13
1 University of Wisconsin-Madison, United States
2 Denver University, United States
3 UW-Madison, United States
Critical support is provided by care partners (CPs) for people with Parkinson disease (PD). Latinos are more likely than white adults to be CPs, but there is limited information on the experiences of Latino CPs. To support CP health, it is vital to identify meaningful daily activities they can participate in to support their well-being, these activities are also referred to as occupations. The Canadian Occupational Performance Measure (COPM), a tool used by occupational therapists, has been used to collect individual’s self-identified occupation goals and has the potential to be used with CPs. The purpose of this descriptive qualitative study was to depict the impact of PD on daily activities and identify the occupational priorities among CPs in the Latino community. Participants completed a demographic questionnaire, semi-structured interview, and the COPM. NVIVO 15 was used to thematically analyze interviews. To participate, individuals had to be an adult providing unpaid care for a person with PD, be Latino or care for a Latino person with PD, able to communicate in English or Spanish, and live in the US. 29 individuals were identified via PD community organizations and electronic health records; 15 have completed the study to date(60+ 11.7 years old; 13 females, 2 male), with recruitment and data collection ongoing. Participants identified as Mexican (n=7), Puerto Rican (n=3), or another Latino origin (n=3); 2 participants did not identify as Latino, but their partner did. According to the COPM, the top occupational priorities were leisure (active recreation and socializing), and productivity (learning about caregiving, volunteering). CPs faced challenges negotiating their time in self-care, professional goals, and care tasks. The care experiences and occupational priorities of CPs within the Latino PD community provide information about what is meaningful and important to these essential individuals, and offers insights that can further inform future health interventions tailored to this population.
COMPREHENSIVE CARE: Exercise and Physical Activity
P14.01
1 Intermountain Health, United States
2 Menzies Institute for Medical Research, University of Tasmania, Australia
3 Wicking Dementia Research and Education Centre, University of Tasmania, Australia
4 Netherlands
5 Department of Neurology, University of Utah, United States
6 Department of Neurology, University of California San Francisco, United States
7 United States
8 Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine and McCormick School of Engineering, Northwestern University, United States
Exercise is an essential part of the treatment of Parkinson's disease. However, certain symptoms can make exercise difficult. In this poster, we describe an under recognized symptom called running-induced dystonia (RID), which can prevent people with Parkinson's from exercising in their preferred way. We summarize the existing literature and use three case studies to outline potential mechanisms, aggravating and relieving factors and both pharmacological and non-pharmacological therapies to get rid of RID. The three case reports are written by people with PD - all three of whom are co-authors on the poster, and two of whom have a health professional background (physician-scientist and physiotherapist).
P14.02
1 Parkinson's Foundation, United States
2 Shirely Ryan Ability Lab, United States
3 Northwestern University, United States
Objective: To align the 2021 Parkinson’s Exercise Guidelines with current evidence and stakeholder feedback.
Background: In 2021, the Parkinson’s Foundation, in partnership with the American College of Sports Medicine, created new Parkinson’s disease (PD) exercise recommendations to ensure that people with Parkinson’s are receiving safe and effective exercise programs and instruction. As is customary to review clinical guidelines every three years, we deemed it necessary to update our recommendations based on new research, stakeholder feedback, and other established guidelines.
Methods: We adapted the Delphi method to synthesize opinions and generate consensus. An internal committee of four subject-matter experts conducted a focused literature search to identify and correct gaps in the recommendations. The revised professional-facing guidelines were then examined by a panel of 11 international subject-matter experts and individuals with PD. The internal committee refined the guidelines based on the panelists’ feedback, after which a public comment period was initiated.
Results: There was a high degree of agreement among subject-matter experts on the importance of safety, with referral to a physical therapist and modifications based on the client’s ability, medication status, and stage of disease incorporated into the guidelines. The balance, agility, and multitasking (BAM) domain was expanded to more accurately describe this distinctive aspect of exercise prescription, and a narrative related to time management was added, encouraging exercise professionals to consider activities that combine domains to efficiently meet the recommendations. The current literature dictated changes to the time component of strength training, flexibility, and BAM, and the panelists provided valuable suggestions of PD-related considerations and examples of relevant activities across domains. In addition, formatting was improved for clarity and flow, and concepts were widely simplified, particularly related to the intensity of aerobic and strength training.
Conclusions: Subject-matter experts achieved a consensus on comprehensibility and alignment with the current evidence, providing exercise professionals with optimal guidance to design and lead exercise for people with Parkinson’s.
P14.03
1 JOY Explorations, United States
2 Pacific Northwest University of Health Sciences, United States
3 ProtoKinetics, United States
Introduction: Postural dysfunction such as forward lean and reduced arm swing are common debilitating features of Parkinson Disease (PD). Physical therapy can address these impairments with varied cuing, yet specific strategies are unclear. Pole walking is an emerging intervention that may improve gait mechanics, however evidence in people with PD is limited. This study aimed to evaluate the feasibility and effectiveness of an 8-week independent pole walking program on arm swing and postural gait characteristics.
Methods: This was a randomized controlled single blinded pilot. Arm swing and postural gait characteristics derived from a 3D Motion Capture System (Ultium-IMU, Noraxon USA Inc., Scottsdale, AZ) were analyzed prior to and following an 8-week independent walking program with or without (control) specialized walking poles. Bilateral wrist sensors calculated arm swing regularity, regularity of angular velocity, peak forward velocity, peak backward velocity, swing frequency, amplitude asymmetry, and peak velocity asymmetry. Postural gait characteristics included thoracic spine forward tilt, thoracic rotation, and shoulder flexion. Pre- and post-intervention data were analyzed using 2x2 mixed ANOVAs, alpha set to 0.05.
Results: There were 6 subjects in the intervention group and 5 matched controls all with PD. Inferential statistics failed to find significant differences in pre-and-post-intervention characteristics, however there were large effect sizes for “time” for peak velocity backward (ηp2 = 0.28), forward (ηp2 = 0.3), amplitude asymmetry (ηp2 = 0.29), and peak velocity asymmetry (ηp2 = 0.15). Descriptive statistics reveal greater improvements and increasing trends in extremity regularity, swing frequency, overall symmetry, and upright posture in the pole walking group versus controls.
Conclusion: While no significant differences were observed, the pole walking group demonstrated meaningful trends toward improved arm swing symmetry, frequency, and upright posture versus controls. These findings suggest an 8-week independent pole walking program may be a feasible and promising strategy to address postural and extremity gait deficits seen in individuals with PD. This pilot study supports the need for larger trials to further explore pole walking as a targeted, accessible, and potentially effective approach to improve functional gait characteristics in individuals with PD, especially in rural areas where patients have limited access to PT.
P14.04
1 University of Colorado Anschutz Medical Campus, United States
2 Parkinsons Pointe, United States
Background: Individuals with Parkinson’s Disease (PD) often reduce participation in exercise and community activities as symptoms progress. Community exercise programs may improve participation, but challenges remain with attendance/adherence and retention. This analysis aims to understand participant characteristics and their potential impact on participation in community exercise classes. Specifically, it sought to: 1) identify differences in demographics between class attendance groups; 2) determine the odds of class participation based on demographics and outcomes; and 3) explore the relationship among baseline demographics and outcomes.
Methods: Data were collected at a community exercise program (Parkinson’s Pointe) as part of a quality improvement project. At baseline, outcomes collected included: demographics, class attendance, functional mobility, loneliness, and self-efficacy. Outcomes were first analyzed as total scores and then categorized based on existing cut-offs. Class participation was categorized into two groups: no class attendance and class attendance (≥ 1 class). Loneliness was measured using the Loneliness Scale (1-9 scale) and categorized into lonely (>5) and not lonely (≤5). Fall risk was categorized into two fall risk groups based on the Timed Up and Go (TUG), with high fall risk (TUG time > 14 seconds) and low fall risk (TUG time ≤ 14 seconds). Self-efficacy was measured using the Chronic Disability Scale (0-30 scale) and categorized into low self-efficacy (≤15) and high self-efficacy (>15).
Results: Of the 191 participants, 88 attended at least one class, and 103 registered but did not attend any classes (no attendance). Age differed significantly across groups (p < 0.001). Those at a high fall risk had 76.2% lower odds of class attendance (OR: 0.238, 95% CI: 0.060 – 0.923, p = 0.036). Loneliness was significantly associated with total attendance (p = 0.031), TUG scores (p = 0.015), and self-efficacy (p < 0.001).
Discussion: Community exercise programs continually seek ways to increase class attendance and better meet the needs of people with Parkinson’s Disease. These results highlight the association between class participation and participants' baseline characteristics. Future research examining the impact of functional mobility, loneliness, and self-efficacy on class attendance may help to identify strategies to improve exercise adherence and sustainability within community exercise programs.
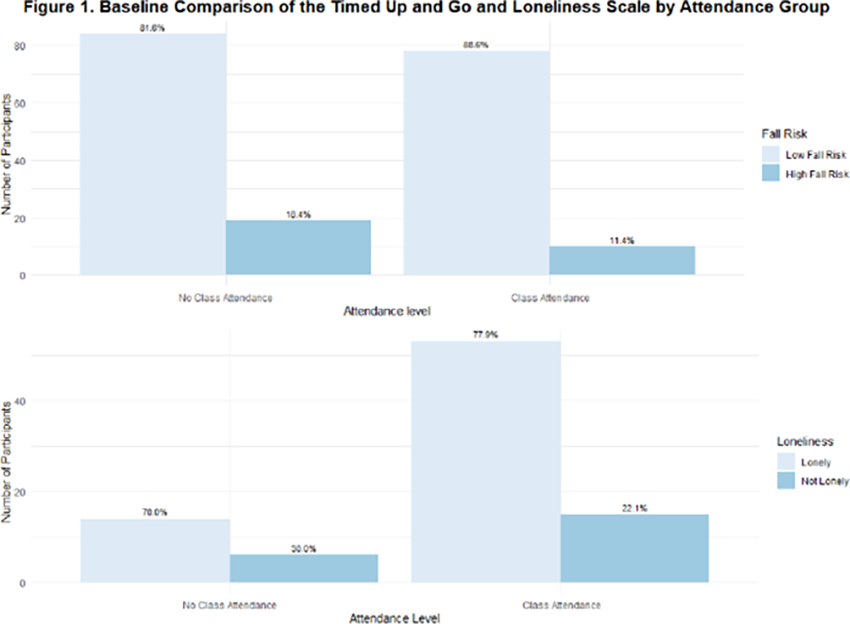
P14.05
1 Shirley Ryan Abilitylab, United States
Background: Exercise, a form of structured physical activity (PA), is a key component in healthy aging and can improve symptoms in people with Parkinson’s disease (PwPD) when performed at higher intensities. Many PwPD struggle to meet the recommended 150 weekly minutes of moderate-to-vigorous (M-to-V) intensity exercise, with some having low activity before diagnosis and others reducing it afterward due to uncertainty and fear. Clinicians have difficulty monitoring PA and exercise because most available tools are surveys limited by recall bias and time burden or costly research-grade wearables. The purpose of this study is to explore the pragmatic use of consumer-grade wearables in PD by examining relationships between self-reported exercise and PA and direct measures from these devices. Methods: Three self-report surveys were administered: 1) weekly frequency and duration of M-to-V exercise (Exercise Vital Sign), 2) confidence to exercise despite barriers (Self-Efficacy for Exercise Scale), and 3) readiness to start/maintain exercise (Exercise Stages of Change, ESOC). Wrist-worn heart rate-enabled activity trackers (Apple, Garmin, or Fitbit) were used to collect direct measures of 1) weekly minutes above moderate (moderate+) exercise, 2) weekly minutes of total exercise (all intensities), and 3) daily steps, based on personalized goals set by physical therapists. Trackers were worn at least four days per week, and four weeks of data were extracted. Spearman’s rank correlation coefficients were computed to assess the associations among these six measures. Results: Eighty-three participants (medians: age 68 yrs, disease duration 6 yrs) were part of the analysis. Weekly total exercise minutes had the highest correlations with all surveys (ρ=0.298–0.468, moderate for ESOC), while weekly moderate+ exercise minutes (ρ=0.284–0.368) and daily steps (ρ=0.131–0.226) showed weaker correlations with surveys. Discussion: Low correlations between self-reported and direct measures suggest that the two approaches capture related but distinct aspects of exercise and PA in PwPD. Self-reported weekly exercise minutes aligned more closely with total exercise minutes than with moderate+ exercise minutes, suggesting participants may include all activity intensities when reporting. Self-report surveys may capture general exercise engagement, but clinicians should interpret them cautiously and consider wearable-based monitoring to better assess moderate+ exercise participation.
P14.06
1 Rocky Mountain University, United States
Purpose: To determine the impact of participating in a Community-Based Group Exercise Class on self-initiated daily ambulation for people with Parkinson’s Disease.
Participants: Individuals with Parkinson’s Disease (PD).
Methods: Participants attended a 50-minute multi-modal high intensity exercise program twice per week for 10 weeks and performed pre- and post-program standardized testing and questioning. Participants also kept track of daily step counts for 7 days prior to the start of the class and for 7 days following the completion of the class.
Results: Participants of this study showed statistically significant improvements in gait speed (0.08 m/s; p=0.016), 3 Meter Backwards Walk Test (mean = 1.07 seconds, p=0.002), Timed Up and Go (mean = 1.93 seconds; p=0.002), Timed Up and Go Cognitive (mean =1.93 seconds; p=0.002) and the difference between TUG Cognitive/TUG (mean = .99 seconds; p=0.026). Participants did show a slight improvement in weekly step counts, measured to be 105.35 steps, however it was not considered to be statistically significant and there is no established reference to determine if this value is clinically significant.
Discussion: There has been much discussion in recent years related to the difference between changes in performance or ability versus changes in daily life utilization or participation. People with PD participating in a community exercise program demonstrated statistically significant improvements in functional mobility performance within the semester class. A small increase in spontaneous lifestyle walking, as measured by daily step counts, was observed, but did not reach significance. This supports the theory that objectively measured ability improvements may be related but not directly translated to lifestyle and participation gains. Both functional ability and lifestyle utilization habits are important measures to consider when working with a progressive disease process like PD. This exercise intervention showed some improvements in both, which may help facilitate improved functional mobility and reduce the expected decline in this patient population. Alternative measures of participation may reveal changes not captured by daily step counts.
P14.07
1 Drexel University, United States
2 Thomas Jefferson University, United States
Golf supports lifelong physical activity and social participation in older adults. Proficient golfers demonstrate mobility, power, and coordination reflected in greater clubhead velocity and reduced variability in distance and directional control. These attributes are often diminished in people with Parkinson’s disease (PwPD). This study examined the impact of Parkinson’s on golf performance, participation, and quality of life to inform targeted interventions. Nine PwPD participated in a golf-based program. After a brief warm-up, each participant hit five shots with a driver (1-wood) and five shots with a 7-iron. Performance metrics were collected using TrackMan, including club speed, ball speed, carry distance, and total distance. Participants also completed the Parkinson’s Disease Questionnaire (PDQ-39), PROMIS Global Health, and semi-structured interviews to assess golf participation, barriers and facilitators, and broader quality-of-life outcomes. Six participants (mean age 70.3 ± 9.8 years, 95% CI [60.1, 80.6]; mean age at diagnosis 64.0 ± 11.9 years, 95% CI [51.5, 76.5]) completed golf performance testing. For the driver, mean club speed was 67.1 ± 15.8 mph (95% CI [50.6, 83.7]), mean ball speed 88.8 ± 21.5 mph (95% CI [66.3, 111.4]), mean carry distance 90.4 ± 57.7 yds (95% CI [29.8, 151.0]), and mean total distance 125.7 ± 54.3 yds (95% CI [68.7, 182.7]). For the 7-iron, mean club speed was 60.2 ± 14.3 mph (95% CI [45.1, 75.2]), mean ball speed 71.9 ± 19.7 mph (95% CI [51.2, 92.6]), mean carry distance 71.5 ± 46.0 yds (95% CI [23.2, 119.9]), and mean total distance 99.8 ± 40.2 yds (95% CI [57.6, 142.0]). Compared with normative values, PwPD demonstrated reduced club speeds relative to age-matched controls. Seven participants (mean age 69.3 ± 12.6 years, 95% CI [58.1, 80.5]; mean age at diagnosis 62.7 ± 15.3 years, 95% CI [47.0, 78.4]) completed patient-reported outcome measures. PDQ-39 averaged 45.7 ± 22.4 (95% CI [21.5, 69.9]) and PROMIS averaged 31.3 ± 4.9 (95% CI [25.4, 37.1]). Interviews highlighted barriers, including stigma, fear of inconveniencing others, frustration, and fatigue. Benefits included reduced anxiety, diminished fear of falling, and enjoyment of golf in a climate-controlled simulator. PwPD demonstrate reduced club head speed compared to normative values, but participation in a supportive, simulator-based environment was feasible, enjoyable, and associated with perceived benefits for confidence and quality of life.
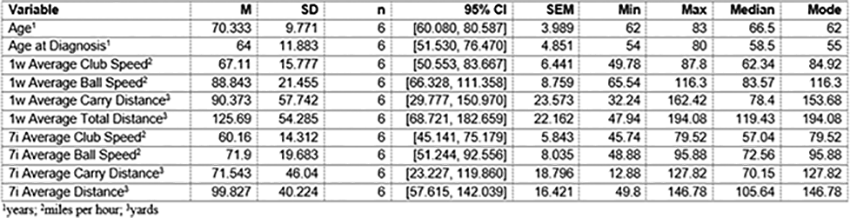
P14.08
1 Tianjin Huanhu Hospital, China
2 Tianjin medical university, China
3 Tianjin Chest Hospital, China
Background: Cardiopulmonary dysfunction is a critical non-motor feature that adversely affects prognosis and quality of life in Parkinson's disease (PD). While aerobic exercise is beneficial, long-term adherence remains challenging. This study aimed to investigate the effects of a short-term, supervised home-based aerobic cycling intervention on cardiopulmonary function in patients with mild-to-moderate PD.
Methods: A single-center, pre-post intervention study was conducted. Seventeen PD patients (Hoehn-Yahr stage 1-3) underwent a 4-week supervised home-based cycling program, exercising at 70-80% of heart rate reserve for 40 minutes per session, three times per week. Remote supervision was facilitated via a mobile application. Primary outcome was maximal power output (Watt). Secondary outcomes included anaerobic threshold (AT), peak oxygen uptake (VO2peak), heart rate parameters, and pulmonary function tests. Assessments were performed at baseline (T0) and after the intervention (T1) in the ON medication state.This study was approved by the Ethics Committee of Tianjin Huanhu Hospital(NO.2023-124) and registered with the Chinese Clinical Trial Registry(ChiCTR2300074453).
Results: Significant improvements were observed in key cardiopulmonary parameters after the 4-week intervention. Maximal power output increased from 40.71±27.53 W to 58.71±29.47 W (P<0.001). Peak oxygen uptake (VO2peak) improved from 14.39±2.79 ml/kg/min to 16.46±3.94 ml/kg/min (P=0.006). Anaerobic threshold power and related heart rate measures also showed significant enhancement (P<0.05). In contrast, most pulmonary function parameters did not change significantly, except for a slight improvement in peak expiratory flow (P=0.027).
Conclusion: A 4-week supervised home-based aerobic cycling program is a feasible and effective intervention, leading to significant improvements in aerobic capacity, metabolic efficiency, and cardiovascular response in patients with mild-to-moderate PD. This short-term, technology-assisted model offers a promising strategy to overcome barriers to exercise adherence and should be integrated into comprehensive PD management.
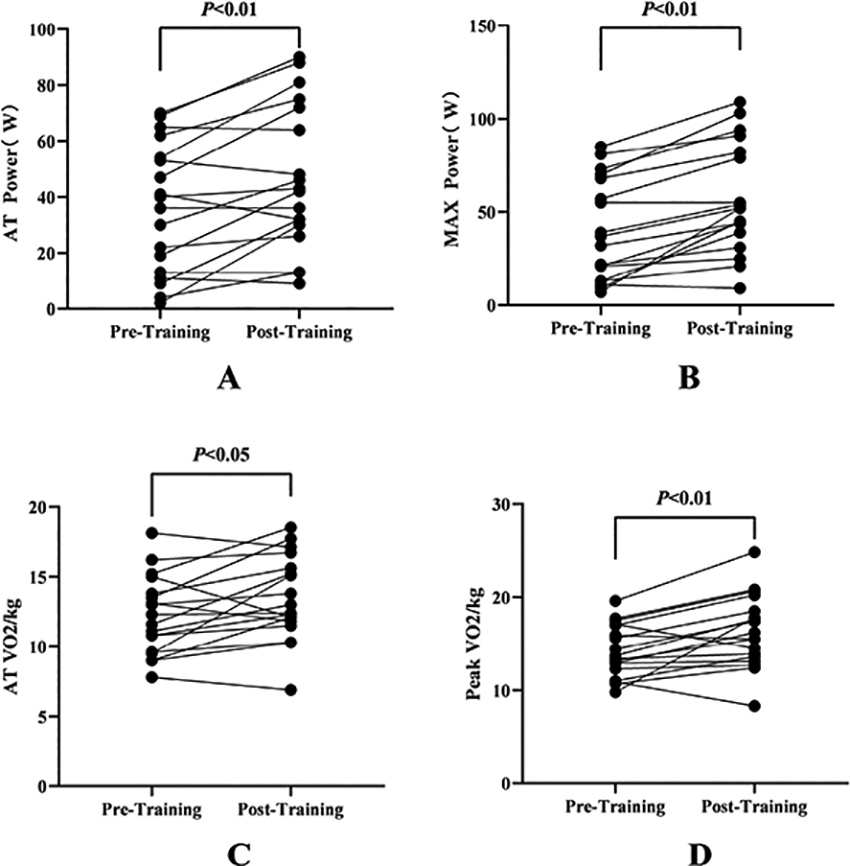
P14.09
1 University College London, United Kingdom
2 Robert Gordon University, United Kingdom
3 Neu Health, United Kingdom
4 University of Plymouth, United Kingdom
Introduction: PD is the fastest growing neurological disease in the world. Exercise is advocated for people with PD and is considered important for managing PD symptoms. Group exercise remains a popular method of supporting people with PD to exercise. Due to wider accessibility issues often experienced by people with PD, more people have utilised online exercise groups. Recent literature suggests online exercise groups are safe and feasible. They may reduce some of the known external barriers to participating in exercise including time, access, cost and transport whilst offering a more flexible approach to exercise around daily lives. With new evidence emerging on this novel approach to exercise a scoping review is needed to explore the extent, nature, and characteristics of the existing evidence on online group-based exercise interventions for people with Parkinson’s disease.
Aim: To map and clarify the existing evidence base, definitions, and conceptual understanding of online group-based exercise interventions for people with Parkinson’s disease.
Inclusion criteria: Eligible sources included participants with idiopathic PD who have participated in PD-specific online exercise groups. The interventions must have occurred as a live class and include an exercise/physical activity component. Studies were included where the intervention took place remotely using an online platform. All types of sources were included with no limit on date range.
Methods: The JBI methodology for scoping reviews was utilised. A three-step search strategy was used: (a) identify keywords from a preliminary search of MEDLINE, CINAHL and Embase databases, (b) refine the search strategy and use keywords in databases to search MEDLINE/PubMed, CINAHL, Web of Science, Embase, Emcare, Cochrane Library, PsychInfo and grey literature, and (c) review references from included studies to identify additional studies. 4 reviewers independently assessed titles and abstracts, then reviewed the full text of the selected articles, applying the inclusion criteria. Data pertaining to key study details will be extracted into a summary table as well as the Consensus on Exercise Reporting template. This will then be summarised narratively. This review is currently being undertaken and will be completed by March 2026.
The findings from this study will inform collective understanding of how online group exercise has been explored in literature and consider areas for future research.
P14.10
1 University of Alabama at Birmingham, United States
INTRODUCTION: Exercise is a cornerstone adjunct therapy for people with Parkinson’s Disease (PwP). However, exercise tolerance and capacity are often impaired by non-motor processes including decreased motivation, psychological arousal, and physical effort allocation. Self-selected music (SSM) has been repeatedly shown to improve motivation and arousal state in healthy individuals thereby leading to increases in exercise capacity. Whether these positive effects of SSM on exercise capacity translate to PwP is unclear. The purpose of this study was to measure the effects of SSM on psychophysiological responses and exercise capacity during a 6-minute walk test (6MWT) in PwP. METHODS: In a counterbalanced crossover manner, PwP (n=10; age= 65.8 yrs +/- 7.0; height= 173.5 cm +/- 6.6; body mass= 81.0 kg +/- 7.9; age of diagnosis= 55.6 yrs +/- 11.9) completed two 6MWT under different listening conditions: 1) Control (CON; White Noise) and 2) SSM. Participants were instructed to walk as far as possible in 6 minutes while listening to the corresponding condition and heart rate, metabolic equivalents (METs), steps, and distance were monitored with a medical grade smart watch. After the completion of each 6MWT, motivation, psychological arousal, enjoyment, and rating of perceived exertion (RPE) were assessed via subjective scales. Comparisons of means between conditions were calculated via paired samples t-test and effect size (Cohen’s d) was estimated for each outcome measure. RESULTS: SSM music resulted in significantly higher heart rate (+9.5%; p=0.004; d=1.1), METs (+25.8 %; p=0.013; d=0.9), and total steps (+6.3%; p=0.029; d=0.8) compared to CON. Non-significant moderate-sized increases in total distance were observed with SSM (+5.4%; p=0.072; d=0.6) compared to CON. Levels of arousal (+62.6%; p=0.001; d=1.6), motivation (+94.1%; p<0.001; d=1.4), and enjoyment (+139.7%; p<0.001; d=2.0) were higher with SSM compared to CON. No differences in RPE were seen with SSM versus CON (-19.0%; p=0.309; d=0.3). CONCLUSION: These data suggest SSM may aid in improving responses to exercise and potently modulates psychophysiological determinants of exercise capacity in PwP. Although larger sample sizes and more robust testing are warranted, SSM may be an effective ergogenic tool for PwP to improve exercise tolerance and capacity.
P14.11
1 Karolinska Institutet, Department of Neurobiology, Care sciences and Society, Division of Physiotherapy, Sweden
2 Faculty of Medicine and University Hospital Cologne, University of Cologne, Germany
3 Stockholm Sjukhem Foundation, Stockholm, Sweden, Sweden
Background: Parkinson’s disease (PD) is increasingly recognized as benefiting from secondary prevention strategies, particularly through physical activity and exercise. One common challenge in PD is dual-tasking—the ability to perform two tasks simultaneously—which tends to be impaired and contributes to a higher risk of falls. Targeted dual-task training (DTT) has been shown to enhance gait velocity in individuals with PD. Although current evidence supporting DTT primarily comes from clinical settings, research suggests that home-based DTT using digital technology is both safe and feasible. However, large-scale trials evaluating its efficacy in home environments are still lacking. The STEPS (Support for home Training using Ehealth in Parkinsons diseaSe) study was designed to investigate the effects of eHealth delivered DTT on walking capacity in people with PD. To further support improvements in walking capacity, the intervention also aimed to increase participants’ levels of physical activity.
Methods: Between September 2022 and June 2024, baseline and post-intervention assessments were conducted at a clinical site in Stockholm, Sweden. Participants were randomized to either an intervention or control group, each following a personalized exercise program three times per week for 10 weeks. The intervention group performed motor-cognitive home exercises supported by eHealth tools, targeting cardiovascular capacity, strength, flexibility, dual-tasking, and physical activity levels. The control group received a paper-based program focused on strength and flexibility. Linear mixed models will be used to evaluate the intervention's effects.
Results: Preliminary results describe the subject sample. A total of 138 participants were enrolled (mean age: 69.5 years; mean Hoehn & Yahr: 2.3), with 113 completing the 10-week intervention. Data analysis using linear mixed models will be finalized in early 2026. To assess changes in walking capacity, the 6-minute walk test was employed as the primary outcome. Secondary outcomes included the 2-minute walk test and Timed Up and Go under single and dual-task conditions, Mini-BESTest, Trail Making Test (conditions II & IV), accelerometer-measured physical activity, and questionnaires evaluating health-related quality of life and exercise self-efficacy.
Conclusion: The STEPS study was a double-blind efficacy trial and the data analysis is ongoing. These results will be presented in detail at WPC 2026.
P14.12
1 Independent Researcher, Austin, Texas; in collaboration with Power for Parkinson's, United States
2 University of Texas at Austin, United States
3 Independent Researcher, United States
Background: Exercise is a key non-pharmacological intervention for Parkinson’s disease (PD), with evidence supporting benefits for mobility, cognition, mood and quality of life. However, most evidence comes from structured research settings, while less is known about real-world, community-based programs that must balance accessibility, sustainability, and engagement. Power for Parkinson’s (PFP), a nonprofit in Austin, Texas, offers free symptom-focused exercise classes designed for people with PD and is open to their caregivers. Understanding participants' perspectives is critical for evaluating effectiveness and informing broader implementation of such programs, as conceptualized by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) framework.
Objective: To explore how people with PD and their caregivers describe the benefits, challenges, and factors that influence sustained engagement in a community-based exercise program.
Methods: This qualitative study invites members of the PFP community to participate through recruitment across in-person classes. Semi-structured interviews are conducted via Zoom, audio-recorded, and transcribed verbatim. Individuals with PD also complete standardized surveys (PASE, PHQ-9, PDQ-39). We plan to interview >=20 people with PD and >=10 caregivers, or until no new themes emerge, ensuring variation in class modality, frequency, and caregiver involvement. Thematic analysis follows an inductive, multi-coder process, with peer review to ensure rigor. Survey data are summarized and integrated with qualitative findings.
Results: Data collection is ongoing. Anticipated findings include perceived benefits across motor, emotional, cognitive, and social domains, with participation shaped by class accessibility, instructor quality, and social connectedness. Caregivers are expected to describe shared motivation, emotional support, personal well-being benefits, and improved understanding of PD-related challenges, as well as changes in communication, relationship quality, and caregiving roles that support sustained engagement.
Conclusions: This study will provide in-depth insights into the lived experiences of people with PD and their caregivers in a real-world community exercise program. Findings will inform RE-AIM-guided strategies to enhance accessibility, engagement, and sustainability of community-based exercise initiatives, helping expand equitable, community-driven options for people living with PD worldwide.
P14.13
1 Universidade da Região de Joinville, Brazil
2 Secretaria de Esportes da Prefeitura Municipal de Joinville - SC, Brazil
3 Secretaria de Esportes do Município de Joinville, Brazil
4 Secretaria de Esportes do Município de Joinville - SC, Brazil
5 Associação Viva Parkinson - Santa Catarina, Brazil
6 Associação Viva Parkinson -= Santa Catarina, Brazil
7 Universidade da Região de Joinville - Univille, Brazil
Introduction: In the second semester of 2023, we embraced a significant challenge: organizing the Parkinson’s Integration Games, an unprecedented and innovative initiative. Although we had never imagined engaging in such an endeavor, we recognized its relevance and committed ourselves wholeheartedly, driven by enthusiasm and a willingness to learn. To describe the actions carried out to organize and hold the Parkinson’s Integration Games and the results achieved. Methodology: The proposal initially raised doubts and apprehension about Parkinson’s Disease (PD) and how to design activities that were both inclusive and integrative. This uncertainty led us to conduct research and review studies that deepened our understanding of the relationship between physical activity and PD, confirming the feasibility of creating an event centered on participation, recreation, and sport. From this vision, the Parkinson’s Integration Games emerged. Results: We identified key characteristics of PD and the positive impacts of exercise, using these insights to guide planning. The Sports Department team in Joinville, SC, Brazil, structured the event with the collaboration of professors and students from the Physical Education program at Univille University. Committees were formed, and alignment and simulation meetings were held to refine logistics and ensure accessibility. The final design included participants with varying stages of PD, grouped by color and age categories. The program featured athletics, basketball, boccia, Nordic walking, ballroom dance, soccer, table games, matrogymnastics, racket games, and adapted volleyball. Upon arrival, participants received a Univille campus map, participation card, T-shirt, and identification ribbon. Guided by the map, they freely chose the order of their activities. After each task, they earned a sticker, with support available at all times. At the end, results were based on the total number of stickers collected. Conclusion: Participants engaged according to their abilities and interests, leading to highly positive outcomes. Expectations regarding inclusion, socialization, and healthy competition were fully achieved. Both organizers and participants surpassed their personal limits in a joyful and empowering environment, confirming the transformative role of sports, the value of shared challenges, and the deep human impact such experiences can create.
P14.14
1 University of Canberra, Australia
Introduction: Exercise is a vital aspect of the management of Parkinson’s disease and needs to be sustained. While the facilitators and barriers to exercise have been reported few studies have investigated what keeps people with Parkinson’s exercising over the long term. This study aimed to understand the experiences, attitudes and beliefs of people with Parkinson’s who have continually participated in an exercise class for longer than five years.
Method: A qualitative study with experiential epistemology. Semi-structured interviews were conducted with ten people who had mild to moderate Parkinson’s and had been attending a weekly student-led physiotherapy exercise class for an average of 8.3 years (range 5-11). Interviews were recorded, transcribed and analysed using inductive reflexive thematic analysis.
Results: Six interlinking themes were identified. “So far I’m lucky”, reflected people’s attitude that they were lucky to be able to exercise despite having Parkinson’s. “We give and we take”, encompassed that the class was more than just exercise. Being a student-led exercise class enabled participants the opportunity to educate future health professionals and provided a sense of purpose for the people with Parkinson’s. The optimistic attitude of participants was identified in the theme “I hope it will make a difference”, in delaying the progression of their Parkinson’s, giving them a sense of control over their disease and the ability to track their symptoms over time. “It’s good to be with other movers and shakers” highlighted the benefits of exercising with other people with Parkinson’s. “The program is designed to keep me exercising” acknowledges the importance of having Parkinson’s specific exercise classes where people feel both psychologically and physically safe. “It’s in the diary” showed that long-term attendees prioritised the exercise, making it part of their routine and committed to attending regularly.
Conclusion: People with Parkinson’s who sustained exercise for over five years displayed an optimistic attitude that they are lucky, a belief they were helping others which gave them sense of purpose and had a positive experience when exercising.
P14.15
1 University of Plymouth, United Kingdom
2 Newcastle University, United Kingdom
Introduction: Parkinson’s is the fastest-growing neurological condition in the world. It can affect mobility and independence. Worldwide research suggests physical activity can slow Parkinson's progression, yet people with Parkinson's are often less active than their peers. This study aims to find out if ENGAGE-PD, which provides personalised, therapist-led physical activity coaching support, could help people recently diagnosed with Parkinson's in UK NHS rehabilitation settings. ENGAGE-PD was developed in the USA with three main elements:
Physical activity coaching A physical activity workbook Physical activity monitoring
To develop a UK version of the ENGAGE-PD physical activity coaching intervention, we consulted with people with lived experience of Parkinson’s using ‘Group Concept Mapping’ (GCM). This consensus approach involves qualitative and quantitative methods in a structured process to organise the ideas of a group.
Methods: Parkinson’s UK supported recruitment of people with lived experience of Parkinson’s through their ‘Take Part Hub’. Using a secure online web application, participants were sent a focused prompt that had been pilot-tested with a Project Advisory Group (PAG) of four people with lived experience of Parkinson’s. Participants were asked to provide ideas to complete the statement: ‘Specific things to engage people newly diagnosed with Parkinson’s in physical activity are…’ The answers formed the basis of GCM ‘Brainstorming’. The next stages involve ‘Sorting’ the ideas into groups that make sense to the participants, then ‘Rating’ on a 4-point Likert scale for relative importance and feasibility. GCM uses multivariate analysis of information from the three stages to represent the ideas of the group in two-dimensional concept maps.
Results: Sixty-two participants (n = 32 male, n = 30 female) contributed to the Brainstorming stage of GCM. Fifty-nine were people with Parkinson’s, 45 within five years of diagnosis. Three participants were care partners. The sample were predominantly White British (n= 59) mainly identifying as Christian (n= 38). The sample were well educated and came from every region of the UK. The sample contributed 118 single idea statements to respond to the focus prompt.
Next steps: The ideas will be taken forward into sorting and rating phases with results anticipated by 2026. The resulting concept map will contribute to a UK version of ENGAGE-PD, co-designed with the PAG, to test in a future feasibility trial.
P14.16
1 John Carroll University, United States
2 InMotion, United States
Introduction: People living with Parkinson’s Disease (PLWPD) experience a myriad of motor symptoms including postural instability, impaired balance, and slow, shuffling gait. These symptoms increase the risk of falls in PLWPD, with fall risk nearly double that of age-matched older adults.
Purpose: The purpose of this study was to investigate the effects of a fall prevention-focused physical activity and education program on measures of physical function in PLWPD.
Methods: Eleven participants (54.5 % female, 74.7 ± 6.0 years old, 6.5 ± 3.1 years since diagnosis) enrolled in a free, community-based fall prevention-focused physical activity and education program completed baseline and 6-month physical function assessments. Eight participants had lower mobility (no assistive device but required exercise accommodations), while three had higher mobility (some exercise limitations but could get on and off the floor independently). Mean baseline Missouri Alliance for Home Care (MAHC-10) score was 4.4 ± 2.0 indicating increased risk of falling. Classes were offered twice weekly and included physical activities such as strength and mobility exercises, dynamic gait activities, progressive balance activities, and dual tasking, etc. Fall prevention education included key fall contributors, fall recovery skills, falling techniques, rising from the floor, etc. Assessments included the MAHC-10 and Falls Efficacy Scale-International (FES-I) questionnaires, 30 second sit to stand, four square step test, functional reach, Timed Up and Go (TUG), TUG with cognitive task, TUG with manual task, and a Two Minute Walk Test (2MWT). Data was analyzed using SPSS 31.0, checked for normality, and alpha level was set a priori at 0.05.
Results: Results from Related-Samples Wilcoxon Signed Rank Tests indicate that there were statistically significant improvements in TUG (W = 1.0, p = 0.007) and 2MWT (W = 58.0, p = 0.026) scores at the 6-month assessment.
Conclusion: Final assessments will be completed in December of 2025. Preliminary results indicate effectiveness of a fall-prevention course in improving walking speed and functional mobility, balance, coordination and fall risk as measured by the TUG test. Outcomes of this study suggest that community-based interventions are effective at improving mobility in PLWPD and can be used to inform future programing aimed at fall reduction by implementing a multi-faceted approach that includes both physical and educational components.
P14.17
1 Keep Moving for Parkinson's, United States
Background: Exercise is a well-established non-pharmaceutical therapy that can mitigate motor and nonmotor symptoms in people with Parkinson’s disease (PD). However, less than 40% of individuals with PD meet the recommended 150 minutes of weekly exercise.
Purpose: This community-based initiative explored the implementation and participant feedback on the impact of a seven-day multimodal exercise initiative, Keep Moving for PD: Exercise Week, on participants’ confidence, motivation, and perceived quality of life. The initiative aligns with current recommendations for exercise in the Parkinson’s population, ensuring participants meet the minimum requirements in each domain. By addressing these needs holistically, “Keep Moving for PD” fosters physical and mental resilience in participants.
Methods: Nineteen individuals with PD participated in a hybrid (in-person and virtual) weeklong program from February 24- March 2, 2025. Each day featured a unique evidence-based modality (boxing, yoga, Pilates, PD Warrior™, resistance training, and community walking). This project was conducted as a community engagement initiative and did not require IRB approval. It evaluated the impact of a seven-day multimodal exercise initiative, Keep Moving for PD: Exercise Week, on participants’ confidence, motivation, and perceived quality of life. Participants completed post-program surveys that combined quantitative ratings with open-ended qualitative feedback. Descriptive statistics and thematic analysis were used to evaluate outcomes.
Results: All participants rated the program as Excellent or Good. The most frequently cited benefits were the variety of exercises, a supportive community, and accessibility. Every participant reported increased confidence in incorporating daily movement. Thematic analysis revealed five dominant themes: (1) empowerment, (2) engagement through variety, (3) accessibility and flexibility, (4) community connection, and (5) challenge and growth.
Conclusion: The Keep Moving for PD initiative demonstrates that a structured, short-term, multimodal exercise program can enhance confidence, motivation, and engagement among people with PD. Integrating both quantitative outcomes and participant narratives highlights the effectiveness of community-based, hybrid exercise programs in improving both physical and psychosocial well-being, empowering individuals living with PD to achieve the recommended weekly activity limits.

P14.18
1 Cardiff University, United Kingdom
2 Reach Your Peak, United Kingdom
Background: Regular exercise can support people with Parkinson’s (PwP) to self-manage but can be difficult to achieve, evidenced by high inactivity levels in this population. Reach Your Peak (RYP) is an innovative digital exercise platform promoting supported home-based exercise. Recently transitioned to an app, it collects self-reported measures related to activity, function and quality of life. Individuals who have completed the 10-week introductory ‘Get Started’ programme on the platform report improvements in movement, fitness, health and wellbeing; however this has not been formally evaluated. The RYP developers and researchers at Cardiff University have conducted initial exploration of data collected via the app.
Aim: To establish baseline characteristics of ‘Get Started’ participants and explore initial data from patient reported outcome measures submitted via the app.
Methods: Ethical approvals were obtained to analyse participant data pre and post the of ‘Get Started’ intervention. Data collected included daily step count (recorded via personal devices e.g. smart phones/Fitbits), adherence, PDQ8 and the 30 second sit-to-stand test.
Results: Since moving to the app-based platform (March 2025), 27 individuals (13 female, 14 male; aged 49–83, mean 64.4 SD 13.4) completed the ‘Get Started’ programme. Primary motor symptoms were bradykinesia (40.7%), rigidity (25.6%) and tremor (33.3%); non-motor symptoms included fatigue (29.6%), depression/anxiety (22.2%) and constipation (18.5%). Falls within the previous six months were reported by 14.8% of participants, freezing of gait by 11.1%, and 55.6% had comorbidities. Fatigue and balance median scores were 3 (1 best; 5 worst). Mobility aid use was 29.6%. Mean 30 second sit-to-stand repetitions improved from 12.86 to 14.50 (SD 4.12). No clear patterns from preliminary step count data have been observed (n = 5). Compliance averaged 3.13–4.35 (out of 5) sessions weekly. After completing ‘Get Started’, 40.7% continued exercising on the platform (37% structured workouts and support, 3.7% workout only access), 18.5% restarted, and 37% discontinued.
Conclusion and next steps: Preliminary data outlines participant characteristics and initial functional improvements from the Reach Your Peak ‘Get Started’ platform. Ongoing data collection includes sit-to-stand, PDQ8 and step counts. Research funding to formally evaluate the programme was submitted in September 2025, with the outcome expected end-2025.
P14.19
1 Robert Gordon University, United Kingdom
2 Robert Gordon University, Canada
3 Robert Gordon University, United States
Background: Parkinson’s disease (PD) is the fastest-growing neurodegenerative condition worldwide, characterised by a wide range of motor and non-motor symptoms that significantly reduce quality of life. Although exercise is well evidenced to improve outcomes in PD, many people with Parkinson’s (PwP) remain sedentary. Walking football (WF) has successfully increased exercise participation in other neurological populations, yet little is known about its impact in PD. This study explored the perceptions and experiences of PwP to assess the potential value of implementing WF clubs more widely across the UK.
Methods: A qualitative descriptive design was adopted. Ten participants (nine males) attending a Parkinson’s-specific WF club in the Northwest of England were recruited. All had attended at least four sessions within a 12-week period. Semi-structured one-to-one interviews were conducted via Microsoft Teams and analysed using a framework approach.
Results: Three overarching themes were identified: (i) physical benefits, (ii) social and emotional benefits, and (iii) mental health and wellbeing. Participants perceived improvements in stamina, fluidity of movement, and confidence in relation to falls. Beyond physical gains, engagement fostered social connection, enhanced self-efficacy and self-confidence, and contributed to an improved sense of quality of life.
Conclusion: PwP highly valued the physical, social, and psychological benefits of WF participation. Findings suggest that expanding WF opportunities could support exercise uptake and wellbeing in this population. Further quantitative research is warranted to establish efficacy and inform wider implementation.
P14.20
1 Universidade da Região de Joinville, Brazil
2 Associação Viva Parkinson Santa Catarina - Brazil, Brazil
3 Universidade da Região de Joinville - Univille, Brazil
4 Secretaria de esportes - Prefeitura Municipal de Joinville - SC Brazil, Brazil
The Parkinson’s Integration Games are a pioneering Brazilian initiative that brings together athletes, families, and specialists in a collective movement celebrating life and confronting the challenges of Parkinson’s disease through sport and knowledge sharing. The event aimed to raise awareness of the crucial role of physical exercise in the prevention and treatment of Parkinson’s disease, foster the exchange of experiences among patients, caregivers, and health professionals, and demonstrate, in practice, the inclusive potential of sports. Its purpose was to describe actions related to sport, integration, and community participation during the Games, measured through a questionnaire applied to participants. Organized by the Viva Parkinson Association (Santa Catarina, Brazil), the event was held in partnership with the Municipality of Joinville through the Sports Department (SESPORTE), the University of the Region of Joinville (Univille), and the Orbenk Group. The Games gathered 175 athletes from eight Brazilian states and 35 cities. Adapted sports modalities included athletics, 3x3 basketball, and paralympic boccia, among others. In addition to competitions, there were spaces for family interaction and discussion circles with specialists. The event took place over a weekend on the Univille campus, and each participant could freely choose their preferred sports activities. The organizing team included SESPORTE professionals and professors and students from Univille’s Physical Education program. During the activities, participants reflected and answered a brief questionnaire on the importance of the Games and the impact of sports in their daily lives. Results showed that 100% of participants reported significant improvement in motor symptoms and overall quality of life related to physical activity. All athletes expressed satisfaction with the event, emphasizing belonging and shared joy. As one participant noted: “There was no room for tremors, rigidity, or slowness. Everyone, each in their own rhythm, gave their best. In the Games, I found more than sport—I found a community.” More than a sporting event, the Parkinson’s Integration Games became a replicable model of community intervention, combining health, quality of life, and social inclusion in an inspiring way. The initiative confirmed the power of exercise as a means of overcoming challenges and strengthening social bonds, establishing a transformative network of care and support.
P14.21
1 New York University, United States
INTRODUCTION High-intensity exercise has emerged as a promising intervention for Parkinson's disease (PD), with evidence supporting motor benefits and neuroprotection. However, the relationship between intensive exercise and gastrointestinal function in PD remains poorly understood. As a person with PD for 16 years who maintained 35-40 miles weekly of treadmill running, I experienced a paradox: running provided motor benefits and temporary constipation relief while potentially contributing to progressive upper GI dysfunction. This report examines the interplay between intensive exercise, PD, and gastric dysmotility.
METHODS This presentation synthesizes peer-reviewed literature on exercise-induced gastrointestinal syndrome, gastric emptying physiology, and PD-associated autonomic dysfunction with retrospective analysis of a 16-year case. The case includes progression from early dysautonomia through post-surgical paralytic ileus to severe gastric dysmotility requiring hospitalization. Clinical endpoints include bowel function, medication absorption, and acute complications.
RESULTS Research demonstrates exercise affects GI function intensity-dependently. While low-to-moderate exercise enhances gastric emptying and colonic motility, high-intensity exercise (≥60-70% VO2max for ≥1 hours) impairs upper GI function through splanchnic vasoconstriction and reduced gastric emptying, promoting gastroparesis. In PD, preexisting enteric dysfunction compounds these effects. This case illustrates the dichotomy: intensive running accelerated colonic transit, masking progressive gastroparesis, while exacerbating upper GI dysfunction culminating in medication malabsorption, weight loss, and complete GI paralysis requiring three-week hospitalization.
CONCLUSIONS Intensive endurance exercise presents a complex risk-benefit profile for people with PD and underlying GI dysfunction. While exercise remains first-line therapy for motor symptoms, this case highlights importance of monitoring for gastric dysmotility signs including medication absorption issues and weight loss. Mechanical stimulation during running may paradoxically mask deteriorating upper GI function. PD patients engaging in intensive exercise may require closer GI monitoring, earlier intervention, and modified exercise prescriptions balancing motor benefits against GI risks. Further research is needed to establish optimal exercise parameters for PD patients with autonomic dysfunction.
P14.22
1 Queen Mary University of London, United Kingdom
2 Radboud University Medical Centre, Netherlands
3 Norwich Medical School, University of East Anglia, United Kingdom
Introduction Parkinson’s disease (PD) is the fastest-growing neurological disorder, with no proven disease-modifying therapy. The prodromal phase offers a critical window for preventive intervention. Hyposmia, a reduced sense of smell, is among the most prevalent prodromal markers and is associated with nearly fourfold increased risk of PD. Exercise is safe, scalable, and supported by evidence for neuroprotective effects. Building on international collaborations, Slow-SPEED UK (Slowing Parkinson’s Early through Exercise Dosage) aims to test whether long-term, gamified physical activity supported by a Fitbit and motivational app can feasibly increase daily movement in people with hyposmia and provide a platform for future prevention trials.
Methods Slow-SPEED UK is a two-arm, double-blind randomized controlled trial embedded in Slow-SPEED International. Researchers will recruit 110 adults aged ≥40 years with University of Pennsylvania Smell Identification Test (UPSIT)-confirmed hyposmia (≤15th percentile). Following a 4-week run-in with wearable monitoring, participants with activity of <7,000 steps/day will be randomized 1:1 to full-dose intervention (+100% step target) or active control (+10% target). Both arms will use a smartphone app, Fitbit device, and gamified features. Assessments will be conducted at baseline (in-person), 9 months (remote), and 18 months (in-person). Optional blood and skin biopsy samples will support exploratory biomarker analyses. The primary outcome is change in average daily step count at 18 months. Secondary outcomes include feasibility of increasing moderate-to-vigorous physical activity, digital fitness markers, prodromal motor and non-motor features, and completeness of digital monitoring.
Results Recruitment is planned for December 2025, with outcomes including feasibility metrics (recruitment, adherence, retention), safety, and exploratory biomarker data. Participants' baseline characteristics will be presented at the Congress. Final results are expected in 2027.
Conclusion Slow-SPEED UK will deliver the first UK-based feasibility data on a long-term, fully remote, gamified exercise programme in individuals with prodromal PD defined by hyposmia. As part of the international Slow-SPEED consortium, findings will be pooled across UK, Dutch, and US cohorts, strengthening the evidence base for scalable, non-pharmacological strategies to delay or prevent clinical features of PD.

P14.23
1 Heartland Neurological Therapy and Wellness Center, United States
Purpose: As the fastest growing neurological disease across the globe, Parkinson’s Disease continues to have a widespread impact across physical, emotional, social, and economic domains. With growing bodies of information for management of Parkinson’s Disease and recent publication of Clinical Practice Guidelines, there is an increasing push for implementation of best practice in management of this progressive neurological disease. The purpose of this study is to evaluate the implementation and effectiveness of a Parkinson’s therapy, wellness, and resource center in a Midwest community.
Description: This study plans to analyze the results of at least twenty- five individuals who have participated in Parkinson’s-specific therapy and community wellness programs for a duration of three or more years. All participants also must have a primary caregiver able to report on caregiver outcomes. Outcomes measures were chosen based on International Classification of Functioning, Disability, and Health and PDEDGE recommendations from the Academy of Neurologic Physical Therapy and include the following: Unified Parkinson's Disease Rating Scale (UPDRS), Parkinson’s Disease Questionnaire (PDQ-39), Caregiver Burden Scale, 6 Minute Walk Test (6MWT), Timed Up and Go Dual Task (TUG-DT), 5 x STS, and self-reported weekly exercise participation.
Summary of Use: This study aims to gather information regarding the current implementation and effectiveness of practices in our clinic across a variety of domains. We plan to use the results of this study to further improve our clinic model and provide education to others in the Parkinson’s community for a comprehensive, interdisciplinary approach to Parkinson’s care.
Implications for Neurological Physical Therapy: There is a significant growth in both the prevalence of Parkinson’s Disease and the evidence of best-practice recommendations for care. This study aims to highlight findings from our clinic and serve as a model for others wishing to implement Parkinson’s-specific care.
P14.24
1 Tor Vergata University of Rome, Italy
2 2Department of Medicine and Aging Sciences "G. d'Annunzio" University of Chieti-Pescara, Italy
3 ParkinZone A.p.s association, Rome, Italy
4 Parkinson No Limits association, Fuerteventura, Spain
5 Department of Neurology, IRCCS INM Neuromed, Pozzilli, Italy
Introduction: Parkinson’s Disease (PD) is a complex neurodegenerative and neuropsychological disorder with diverse motor and NM symptoms, sometime inadequately managed by pharmacological treatments alone. Our team integrated Body-Mind activities, combining physical exercise and psychological counseling, into new standardized outdoor therapeutic programs for people living with PD (PwPD). These programs leverage the restorative effects of natural environments to enhance quality of life (QoL) and health status. Such initiatives are currently active in Italy (Sail4Parkinson) and Fuerteventura (Fuerte4Parkinson), where associations ParkinZone A.p.s and Parkinson No Limits organize therapeutic vacations for PwPD and caregivers.
Methods: We evaluated the feasibility and efficacy of 10 days outdoor therapeutic programs for PwPD, combining physical activities, both aquatic (surf, SUP, sailing) and non-aquatic (non-contact boxing, Pilates, yoga, Tai Chi), with integrated psychological sessions. Participants underwent physical and neuropsychological assessments before, after and during the programs.
Results: 16 PwPD (9M, 7F)(MA 60.67 yrs, sd 7.063)(MDD 9.38 yrs, sd 4.60) were included in this study. Preliminary analysis shows a tendency toward reduction of the daily levodopa intake (LEDD), althought not statistically significant (p=0.51). Significant correlations were found between the LEDD taken and the levels of sedentary behavior in participants, indicating that the more time spent sedentary, the higher the levodopa intake (p < 0.05). Conversely, light-to-moderate intensity of physical activity, both total and average, showed a significant negative correlation with LEDD (p < 0.05), highlighting that higher physical activity levels are associated with lower LEDD requirements. No significant changes emerged from the analysis of QoL questionnaires, except for a tendency toward reduction in the Physical Discomfort subscale of PDQ-39 (mean of 42.13 sd=23.65 at baseline to 40.10 sd=26.57 at follow-up) (p > 0.34). Qualitative feedback reported an extremely positive and pleasant perception of the experience.
Conclusion: Outdoor therapeutic programs are feasible and potentially beneficial for PwPD. Further research with larger sample sizes is needed to confirm their effectiveness
P14.25
1 Dancing With Parkinsons, Canada
2 Dance For PD, United States
3 School of Psychology, University College Dublin, Ireland
4 Division of Neurology, University of Toronto, Canada
5 Academic and Research Collaborative in Health, La Trobe University, Australia
Background Parkinson’s disease (PD) can profoundly affect an individual’s physical, emotional, and cognitive well-being.
Dance has been associated with enhanced motor performance and non-motor function in people with lived experience of PD. While the holistic experience of dance is essential, the key factors contributing to beneficial outcomes need to be identified to optimise the benefits and tailor dance programs.
Objective We demonstrate and describe some of the core aspects of the Dance for PD (DfPD)/Dancing with Parkinson’s (DWP) methods. By integrating perspectives of experts and individuals with lived experience, we report key choreographic and pedagogical elements that may be relevant for optimising movement, health and wellbeing.
Methods We conducted a demonstration of selected choreographic elements and movement sequences from the DfPD/DWP methods. Please see video here: https://drive.google.com/file/d/1QcQicuRLCpXQ_6eLG92QkLHJVeiKohpG/view?usp=sharing We gathered input from dance experts trained in the DfPD/DWP method, a person living with PD, a PD caregiver, a cognitive neuroscientist, a physiotherapist, and a movement disorders neurologist.
Results Core aspects of the DfPD/DWP methods were found to include: 1) imagery and storytelling, 2) improved movement control through rhythmic auditory cueing to music, entrainment to partner movements and choreography, 3) performance of controlled bilateral and midline-crossing movements, 4) fine motor activation through hand gestures, 5) social mirroring and facial expression and 6) partner-based movements. The integration of motor, cognitive, emotional, and social aspects suggest that the DfPD/DWP methods may activate multiple brain regions and circuits. The premotor, supplementary motor and primary motor cortices, basal ganglia, cerebellum, proprioceptive and limbic pathways play an important role in these elements of dance.
Conclusion We generated a framework of DfPD/DWP by integrating interdisciplinary perspectives and evidence to identify key elements of dance that may positively influence motor and non-motor aspects of PD. This provides a foundation for future research into the mechanisms and clinical applications of dance interventions in people living with Parkinson’s and related conditions.
P14.26
1 Movement Revolution, United States
Introduction: Group exercise classes have the capacity to impact mobility, and quality of life in individuals experiencing Parkinson’s disease at multiple stages. A community-based program, such as those provided through Movement Revolution, fosters consistent social interaction and targeted exercise programming. The purpose of this study was to determine the impact of a community-based group exercise program for individuals with mid-stage PD and YOPD over the span of 1 year.
Methods: Participants were recruited from Movement Revolution Rock Steady boxing classes for individuals with mid-stage Parkinson's (3X a week) and a high-intensity class for YOPD (1X a week). Both classes incorporate endurance, balance, and strength exercises. PDQ-39 and ABC questionnaires were administered at baseline and 1 year follow-up. Effect sizes via Hedges’ g were determined for pre and post measures for each group, along with average change scores. Between-group effect sizes were also found for mid-stage PD with age-matched controls.
Results: Of 121 participants, 7 completed initial and 1-year follow-up assessments. Effect sizes for the mid-stage exercise group included PDQ total scores (g=0.37), ADLs (g=0.24), EMO (g=1.09), SOCIAL (g=.17), and an average change score of 4.14 (CMD >4.22). Between-group differences included PDQ total (g=-0.89), ADLs (g=-0.59), emotional well-being (-0.50), and social well-being (-0.80). Within group ABC differences were indicated (g= -0.75), along with between group differences (g= 0.88), with an average % change of -3.97% (CMD>13%). For 4 preliminary YOPD participants, intervention effect sizes included PDQ total (g=1.68), ADL (g=0.75), emotional well-being (g=0.66), and social well-being (g=0.87), with an average change of 10.98. One-year follow-up of ABC differences was (g=-0.07), with a -0.31% average change.
Conclusion: From our preliminary data, the mid-stage PD group benefited from consistent group exercise relative to age-matched controls as reflected by total PDQ, social well-being scores, and ABC scores. Average change in PDQ scores and ABC %, indicated that participants did not experience disease progression as reflected by CMD. However, more data is needed to understand PDQ changes in the YOPD group. Our pilot data reflects the benefit of our group exercise intervention and its capacity to slow disease progression for mid-stage PD and YOPD. Future data will report the full cohort of the intervention program with motor outcomes.
P14.27
1 Parkinson Wellness Recovery | PWR!, United States
2 Kirk Gibson Center for Parkinson's Wellness, United States
3 University of Michigan - Flint, United States
Introduction: Our previous research established retrospective cutoff scores using common therapy assessments (including the original SPS transfer test), as part of a decision-making tool for stratifying persons with Parkinson disease (PwP) into multilevel exercise classes. We have since revised the scoring of the floor transfer to add qualitative aspects of motor performance into a new Total Combined score. The ability to transfer to and from the floor is an important skill to test and train because it deteriorates in PwP and interferes with participation in classes incorporating floor activities. Many exercise programs avoid floor activities due to difficulty rising without assistance, though studies show floor-based exercise is safe and can reduce fear of falling. In addition, whole body coordination and functional strength training opportunities are abundant on the floor! Despite its clinical importance, few validated measures assess floor transfer ability. There is also a critical need for exercise class instructors to have a practical screening tool to determine how best to assist individuals in safely getting to and from the floor.
Methods: The revised SPS Transfer Test was administered to 333 PwP at the Kirk Gibson Center for Parkinson’s Wellness as part of assessments used to assign participants to one of four functional levels for PD-specific exercise classes. Outcome measures used were based upon previously published cutoff scores and included: Montreal Cognitive Assessment (MoCA), Five Times Sit-to-Stand, Timed Up and Go (normal/cognitive), 3-Meter Backward Walk, Gait Speed (normal/fast), Six-Minute Walk Test, and the original SPS Transfer Test.
Results: Like our original floor transfer test using only a Total Time score, both the Total Time and the new Total Combined Score were statistically different for the revised floor transfer test across all class levels (p<.001). New pre/post floor transfer confidence ratings were improved and significantly different across all groups (p<.001). Other insights from adaptations, cueing, assist, most advanced position achieved, and movement deficits will be reported across groups.
Conclusions: The revised scoring for the SPS transfer test was sensitive to class level and the scoring process may empower participants and increase their willingness to participate in challenging floor exercise, while informing the instructor how to adapt, provide feedback, and design floor exercise activities.
P14.28
1 Egas Moniz School of Health & Science, Portugal. ; Inova Parkinson's and Movement Disorders Center, Alexandria, VA, USA, Portugal
2 Triad Health AI, Aurora, CO, United States; Inova Parkinson's and Movement Disorders Center, Alexandria, VA, USA, United States
3 Inova Parkinson's and Movement Disorders Center, Alexandria, VA, USA, United States
Background: There is limited guidance on how individuals can adjust their routines when facing new or changing health challenges in managing Parkinson's Disease (PD). This lack of direction may leave people vulnerable.
Objective: To explore how people with PD adapt their exercise routines following health setbacks, identify barriers and facilitators, and develop a practical guide to support adaptation.
Methods: A qualitative online survey was developed by rehabilitation specialists who were delivering an educational program. This survey was distributed in September 2025 to individuals living with Parkinson's disease (PD). It included multiple-choice questions and open-ended text responses, focusing on triggers for changing exercise routines, adaptations made, perceived impacts on motivation, and the resources needed for future challenges.
Results: Forty-one people with PD (mean age 75 years; 37% <5 years since diagnosis, 32% 5–10 years, 32% >10 years) and two care partners completed the survey. Of 43 respondents, 33 (77%) reported changing their exercise routine due to health issues. The most common reasons were new health diagnoses unrelated to PD (40%) and sudden PD-related events such as falls or injuries (35%). Strategies included changing exercise type (42%), seeking professional guidance (35%), temporarily stopping activity (28%), and reducing frequency or intensity (26%). Most decisions regarding these changes were made independently (26%), though some respondents received input from physiotherapists (12%) and neurologists (7%). The impact of these changes on confidence and motivation varied: 42% reported a positive impact, 30% experienced no change, and 24% reported a negative impact. Barriers to maintaining exercise included limited access to facilities (37%), fear of worsening symptoms (35%), and a lack of knowledge about safe alternatives (35%). Despite these challenges, most respondents felt at least somewhat confident in their ability to adapt their exercise routines, with 58% feeling somewhat confident and 26% feeling very confident.
Conclusion: This survey highlights a significant unmet need: individuals with PD require structured support when adapting their exercise routines after experiencing health setbacks. In response to these findings, we developed a practical exercise adaptation guide that outlines various adjustment strategies to help maintain safe, effective, and sustainable engagement in exercise (see Table 1).

P14.29
1 University of Connecticut, United States
Introduction: Parkinson disease (PD) affects approximately 12 million people globally, with the highest incidence amongst Latinx individuals. Although physical activity (PA) is a critical component of disease management, many older Latinx individuals face barriers to regular PA engagement. To address this gap, an 11-week, culturally tailored, peer-supported, remotely delivered PA intervention was examined. The purpose of this study was to qualitatively assess the feasibility of this novel intervention.
Methods: Participants who completed the interventional study were invited to participate in a virtual focus group. A semi-structured interview protocol guided the focus group, which was conducted in Spanish and English. The recorded session was translated, transcribed, and analyzed thematically following Braun and Clarke’s six-phase framework.
Results: All 10 participants who completed the intervention took part in the focus group. Four overarching themes were identified: 1. Building a sense of community and support; The peer-partner model fostered mutual encouragement, accountability, and belonging, creating a sense of community in those with a common language and culture 2. Self-efficacy for exercise; Engagement increased participants’ confidence and understanding of evidence-based exercise for the management of PD and how to exercise safely with PD. 3. Technology as a barrier and facilitator of exercise behavior; Participants appreciated the use of wearable technology enabling them to track their progress however, some faced difficulties navigating digital platforms and suggested refinements such as simplified technology. 4. Building flexibility into the intervention to enhance participation; Participants suggested expanding the intervention to have advanced and beginner levels and recommended increasing exercise class offerings and options, as symptom fluctuations and fatigue influenced participants’ ability to consistently engage with the intervention.
Conclusions: Thematic analysis highlighted that the intervention was feasible and acceptable for Latinx adults with PD. Participants valued the sense of community, peer support, and increased exercise knowledge and skill that the program provided. While managing symptom variability and technology was a challenge, the overall experience was positive. This emphasizes the importance of enhanced social connections and accessible technology to reduce health disparities in this underserved population.
P14.30
1 University of Michigan, United States
Objective: Comparing the effect on gait speed of a non-exercise physical activity intervention consisting of 12 sessions of 4 hours of standing versus standing combined with weight shifting/lateral stepping in People with Parkinson's Disease (PwPD).
Background: Axial motor dysfunctions in PD incline many patients towards a sedentary lifestyle. Physical exercise is strongly encouraged and backed by robust evidence. However, recent advances in physical (in)activity research increasingly recommend non-exercise physical activity (any bodily movement that is not part of physical exercise) approaches to promote healthy lifestyle modifications as well. We have developed a desk with a tabletop that oscillates in the horizontal plane, which cues users to make periodic mediolateral postural adjustments ("dynamic standing") while performing routine tabletop activities, thus providing a low barrier option for non-exercise physical activity to PwPD.
Methods: 20 participants completed 12 sessions of a 4-hour protocol, 10 behind a normal (static) standing desk (age 69.3±4.0, M/F 8/2, H&Y 2.3±0.5) and 10 behind the dynamic standing desk (age 64.2±6.8, M/F8/2, H&Y2.5±0.6). Gait speed was collected before and after the intervention. Additional control comparison data for 9 PwPD (sitting, no intervention) was also collected (age 66.3±4.0 M/F 8/1, H&Y 2.2±0.4).
Results: Mixed-model analyses (t-test, repeated measures ANOVA) to analyze gait speed before and after the intervention revealed that gait speed increased significantly in the dynamic desk group (p=0.04) but not in the static standing and control group.
Conclusions: Standing improves health by combating the negative effects of physical inactivity due to prolonged sitting. For PwPD, it may be an ideal form of low-intensity, non-exercise physical activity because of lower extremity muscle and postural activity that can be easily incorporated in many routines of daily living. These data suggest that promoting non-exercise physical activity in the form of standing, combined with mediolateral weight shifting and stepping improves anterior gait speed. This has important clinical implications for PwPD. First, this non-exercise physical activity could be a valuable additional intervention for gait training. Second, standing with periodic side stepping, which mostly trains the lateral hip mobilizers (strong predictor of fall risk), can increase forward gait speed, improve general mobility, and quality of life in PwPD.
P14.31
1 International Table Tennis Federation Foundation, Spain
2 Sense 4 Care SL, Spain
Introduction:Table tennis has been reported by many people with Parkinson’s disease (PwP) as a physical activity that alleviates motor symptoms and improves well-being. However, scientific evidence supporting these claims remains scarce. Monitoring the potential benefits often relies on subjective questionnaires and brief clinical assessments, that may not capture fluctuations in daily life. STAT-ON®1, a certified Class IIa wearable medical device, enables objective and continuous monitoring of motor symptoms in PwP in real-world conditions.
Methods:A pilot study was conducted during the Bornholm PwP Training Camp organised by Cure4Parkinson and the ITTF Foundation. Four patients with mild to moderate Parkinsońs disease (3 women, 1 man; mean age 54.8 years) wore STAT-ON® for one week. Following a dedicated 3-hour specialized table tennis training session during 6 consecutive days focused on simultaneous motor–cognitive skill development on hand–eye coordination, balance, focus, and memory, participants continued to wear the device for one additional day to assess immediate effects. Parameters analyzed included ON/OFF time, dyskinesia, inactivity, bradykinesia index, minutes walking, number of steps, falls, and freezing of gait (FoG).
Results:All participants showed a reduction in OFF time (–13.8% on average) and an increase in ON time (+22.8%). Among those with dyskinesia, mean dyskinesia time decreased (–6.0%). Bradykinesia index and inactivity also improved after training. Conversely, walking time and step count decreased, likely due to contextual differences between daily live and training camp conditions. FoG detection slightly increased, probably reflecting false positives from short step movements during play, without statistical relevance.
Conclusions:This pilot study suggests that specialised table tennis training for simultaneous motor–cognitive skill may produce measurable short-term improvements in PwP motor states, potentially enhancing quality of life. Despite promising results and good design of sessions, the small sample, and non-everyday setting limit generalizability. Larger, longer-term studies are warranted to validate the role of table tennis as a key therapeutic exercise in Parkinson’s disease management.
[1]Rodríguez-Martín D, Cabestany J, Pérez-López C, Pie M, Calvet J, Samà A, et al. A New Paradigm in Parkinson’s Disease Evaluation With Wearable Medical Devices:A Review of STAT-ONTM. Front Neurol. 2022;13. doi:10.3389/fneur.2022.912343

P14.32
1 University of Nevada, Las Vegas, Nevada., United States
2 Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais., Brazil
Introduction: People with Parkinson’s disease (PwPD) often experience reduced physical activity and social participation, affecting physical conditioning, mental health, and quality of life. However, community-based exercise interventions that integrate physical and social components remain scarce for PwPD. The 10,000 Steps Club (10KSC) addresses this need through a community-based Nordic walking program designed to enhance physical activity and social engagement for PwPD. This study assessed preliminary effectiveness and participant satisfaction of the 10KSC. Methods: In this pre-post cohort study, PwPD participated in a 6-month walking program consisting of weekly 60-minute community walks. Nordic walking poles were used to promote full-body movement and enhance safety during walks. Participants received activity-tracking watches to monitor daily activity and were encouraged to increase physical activity. Outcome measures assessed at baseline and 6 months included: gait capacity (6-Minute Walk Test), self-efficacy (Self-Efficacy for Managing Chronic Conditions), quality of life (Parkinson’s Disease Questionnaire-39), balance (Mini-BESTest), social isolation (Berkman Social Network Index), balance confidence (Activities-Specific Balance Confidence Scale), and program satisfaction. Results: To date, 21 participants have enrolled, with eight completing the 6-month intervention and post-assessment (7 males; mean age 69±5 years). Statistically significant improvements were observed in gait capacity (baseline=389.3±121.4 m, post=414.85±243.28 m; p=0.017) and social isolation (baseline 12.9±3.4, post 15.3±3.3; p=0.027). Balance confidence decreased significantly (baseline=83.3±15.3, post=76.8±21.1; p=0.028). Participant satisfaction was high: 75% reported overall program satisfaction, and 87.5% were willing to recommend it to other PwPD. Half of the participants (50%) reported feeling more or much more physically active, and 62.5% felt more socially engaged following the program. Conclusion: The 10KSC demonstrated promising effectiveness with improvements in gait capacity and social connectedness. The decrease in balance confidence warrants further investigation but may indicate heightened risk awareness rather than actual functional decline, particularly given participants' reported increases in physical activity. High participant satisfaction supports program acceptability. Final conclusions await study completion with the full sample.
P14.33
1 Interior Health, Canada
2 University of British Columbia Okanagan, Canada
Background Aerobic exercise improves gait, posture, and balance in Parkinson’s disease (PD). But traditional modalities such as treadmill or cycling can be difficult for individuals with balance or orthostatic impairments. Upper limb ergometer (ULE) training, or hand cycling, offers a safe, seated form of aerobic exercise. Benefits have been reported following ULE and lower limb ergometry, but data on short-term effects on hand dexterity are limited. Given evidence that a single aerobic session can increase dopamine release, examining immediate functional outcomes is warranted. The objective of our study was to determine the short-term effect of a single session of steady-state versus interval hand cycling.
Methods Participants with PD were recruited from the Movement Disorder Clinic in Kelowna, BC. Inclusion required diagnosis of PD, age ≥18 years and absence of unstable cardiovascular disease. Clinical data (MDS-UPDRS score, affected side, medication timing, and treatment history) were collected from medical charts. Baseline assessments included PDQ-39, CSEP Get Active Questionnaire, International Physical Activity Questionnaire, vitals, and anthropometrics. Other baseline measurements collected were hand function via 9-Hole Peg Test and finger tapping, and mood via the Positive-Activated Affect/Activation Scale.
Each participant completed two randomized five-minute ULE sessions (steady-state and interval) on a MONARK ergometer with Garmin Rally sensors. Steady-state sessions maintained 60 rpm; interval sessions alternated 45 seconds at 60 ± 5 rpm with 15 seconds of maximal effort. Heart rate (HR) was continuously monitored using an arm-worn photoplethysmograph. Vitals, hand function, and affect were reassessed post-exercise. Once heart rate returned within 10% of baseline, the second session was completed.
Results As of October 2025, our goal of ten participants completed the protocol. Data analysis is ongoing.
Conclusions This study will provide insight into the acute effects of ULE exercise on hand dexterity and mood in PD. Findings may inform safer, more enjoyable exercise prescriptions to enhance adherence. Future studies could include exploration of gamified exercise, variable cadence ULE interventions, and including comparisons between ON/OFF medication.
P14.34
1 Population Health Sciences Institute, Faculty of Medical Sciences, Newcastle University, Newcastle Upon Tyne, United Kingdom, United Kingdom
2 Translational and Clinical Research Institute, Faculty of Medical Sciences, Newcastle University, Newcastle Upon Tyne, United Kingdom, United Kingdom
3 Northumbria Healthcare NHS Foundation Trust, Newcastle upon Tyne, United Kingdom, United Kingdom
4 University of Ghana Medical School, Korle Bu Teaching Hospital, Accra, Ghana, Ghana
5 Department of Physiotherapy and Rehabilitation Sciences, University of Health and Allied Sciences, Ho, Ghana, Ghana
6 Richard Novati Catholic Hospital, Sogakope, Ghana, Ghana
Introduction: In low- and middle-income countries chronic disease burdens, limited healthcare resources, and shortages of healthcare professionals (HCPs) shape the experiences of people with Parkinson’s (PwP). Parkinson’s symptoms (e.g. bradykinesia, rigidity) profoundly affect physical mobility, particularly walking, which is central to physical, social, and emotional experiences. Prior research using wearable devices on the lower back for seven days found PwP in Ghana walk less with poorer gait quality than age-matched Ghanaian controls and British PwP, differences not fully explained by disease factors. Socioecological factors may offer further insight. This study explored the walking experience of PwP in Ghana.
Methods: Four workshops were conducted in urban and rural Ghana, two with PwP (n=7) and caregivers (n=7), and two with HCPs (n=13), with content informed by 23 interviews with PwP in Ghana. Creative participatory methods elicited in-depth discussions around experiences of physical mobility loss and how this is assessed and managed. Activities included mapping symptoms on a body diagram, card-sorting to rank impacts, and vignette discussions. Themes from the data were mapped onto the socioecological model using a framework analysis to provide a clear and actionable results.
Results: Physical mobility is consistently highlighted as a complex and multi-layered experience which is linked to profound impacts. While Parkinson’s symptoms are one aspect influencing physical mobility, this does not describe the whole picture (Figure 1). Intrapersonal factors (e.g. internalised stigma, accessibility of treatment), interpersonal factors (e.g. discrimination due to preconceptions, dependence on family support), environmental and institutional factors (e.g. lack of recreational spaces, education and awareness), and wider structural issues (e.g. fragmented healthcare systems, high healthcare costs, and sporadic insurance coverage) all play a role in influencing the quantity of a person’s walking. This leads to physical deconditioning and worsening walking quality, highlighting a vicious cycle that promotes further inactivity.
Conclusions: By integrating perspectives of PwP, caregivers, and HCPs, a holistic understanding of the walking experience has been developed. Further exploration is essential to inform policy and identify areas for wearable devices to support PwP in the clinical care received, potentially through diagnosis, monitoring, and prediction.

P14.35
1 São Paulo State University (UNESP), Brazil
Introduction: Postural control impairments are common in Parkinson’s disease (PD) and may vary according to the clinical subtype, such as Postural Instability and Gait Difficulty (PIGD) and Tremor Dominant (TD) subtypes. Understanding how different subtypes respond to external perturbations can help identify specific mechanisms related to postural instability and guide rehabilitation strategies. Aim: To investigate the effects of perturbation direction and PD subtype on temporal and spatial parameters of postural responses during unexpected platform displacements. Methods: Thirty-eight individuals with PD (22 PIGD, 16 TD) participated. Subtypes were classified based on the ratio between tremor and postural instability/gait difficulty scores from the MDS-UPDRS. Participants stood on a force platform mounted on a motorized perturbation system, feet at pelvic width and eyes fixated 1.5 m ahead. The platform translated 5 cm at 15 cm/s in forward and backward directions (three trials each). Center of pressure (CoP) data provided response time, recovery time, CoP amplitudes during reactive, response, and recovery phases, and peak CoP velocity. A two-way mixed ANOVA was conducted with direction (forward, backward) as the within-subjects factor and subtype (PIGD, TD) as the between-subjects factor. Results:Perturbation direction had a consistent and strong effect on all dependent variables (ηp2 = 0.17–0.64; p< .01), with larger amplitudes, velocities, and longer times observed in backward perturbations compared to forward ones. No significant main effects were found for subtype (p > .10), indicating similar postural responses between PIGD and TD groups. A significant interaction between direction and subtype was found only for recovery time (F(1,36)= 4.584, p= .039, ηp2= .113). Specifically, the TD group exhibited a marked increase in recovery time from forward to backward perturbations, while the PIGD group showed relatively stable values across directions, suggesting greater directional asymmetry in TD individuals. Conclusion: Postural responses were mainly influenced by perturbation direction, not by PD subtype. Backward perturbations elicited larger and slower responses, indicating greater challenge to recover stability. TD individuals showed higher asymmetry in recovery time, suggesting subtle differences in dynamic stability, while overall CoP magnitudes and velocities were similar across subtypes.
P14.36
1 Northern Arizona University, United States
Introduction: People with Parkinson’s (PwP) disease often have difficulty transferring therapeutic movement strategies learned in rehabilitation to daily life due to barriers such as apathy and lack of social support. This research seeks to understand the roles of daily apathy as a barrier and social support as a predictor for PwP application of Large Amplitude Movement Training (LAMT) to both exercise routines and functional mobility in everyday life. LAMT promotes high-effort, whole-body movement with increased amplitude that can be completed as exercise and applied to functional mobility with the goal of improving movement in PwP. However, the successful translation of LAMT from clinic to daily life may depend on PwP intrinsic motivation and/or supportive social environments. We hypothesize: (1) PwP will report less use of LAMT on days when apathy is higher than usual; (2) PwP will report more use of LAMT on days when social support is higher than usual; and (3) the daily relationship between higher apathy and less use of LAMT will be attenuated on days when PwP receive more social support.
Methods: This microlongitudinal study involves digital health daily diary methods to collect lived experiences of PwP using mobile devices over 14 days. To capture daily fluctuations in PwP application of LAMT to exercise and functional mobility, participants answer questions about daily apathy and social support (predictors) and LAMT exercise plus application to functional mobility (outcomes). We are recruiting 50 community-dwelling participants from Arizona who have been diagnosed with idiopathic PD, are over the age of 50, and have been exposed to LAMT during therapy to address PD symptoms.
Results: Data collection is ongoing with expected completion in early 2026. As of October 2025, 11 PwP have participated (Mean age=74.55 years, SD=4.71, Range=69-83; 36% women; 55% at Modified Hoehn and Yahr Stage 2.5). Results will inform whether daily apathy and social support are associated with LAMT-related exercise and functional mobility within PwP over time in their everyday life.
Implications: Findings will help clinicians target modifiable psychosocial factors in PwP everyday life to improve the maintenance of functional health outcomes post-discharge from LAMT therapy. Future work may build on this research by studying daily variability in other risk and protective factors impacting PwP mobility and participation in meaningful activities.
P14.37
1 JOY Explorations, United States
Background: Following a Parkinson Disease (PD) diagnosis, many people find their world becomes smaller – not just physically but in all facets of life. Daily movements feel different, doubt creeps in about what the body can accomplish, & anxiety prevails about keeping up with family & friends resulting in limited activity & reduced social engagement. Evidence shows integrating exercise, sleep, diet, mindfulness, & socialization improve PD symptoms & quality of life. Unfortunately, these elements are often taught in isolation, not as a connected, actionable lifestyle that helps PwPD thrive.
Objective: The retreat delivers an immersive, evidence-informed weekend of movement, lifestyle education, & restorative experiences designed to build confidence, enhance well-being, & provide practical strategies to support sustainable, life-improving habits for PwPD.
Methods: The four-day, three-night retreat at a lakeside resort surrounded by a wooded landscape harnesses the restorative benefits of nature. Program designed & led by a Doctor of Physical Therapy with specific PD certifications & experience. Additional therapy & fitness staff with extensive PD qualifications. A small cohort size (∼20) cultivates a support community. It also offers a 1:4 staff-to-participant ratio for safety, & to provide each participant with personalized attention & professional guidance. Participants experience evidence-based principles of high-intensity training, large-amplitude movement, balance, strength, coordination, dual-tasking, & flexibility—integrated into fun, functional activities such as hiking, basketball, yoga, tai chi, kayaking & biking. Classroom sessions complement these experiences with education on exercise, sleep, nutrition, & mindfulness, along with guided reflection & practical strategies for applying the principles to everyday life. Outcome measures collected at check in & check out: 1 minute Sit to Stand (1MSTS), Stand Prone Stand, 4 Square Step with & without Cognitive Task.
Results: 70% of participants from inaugural retreat returned the next year. In the four days, all participants improved in at least one of the outcome measures. 1MSTS results showed a significant difference (average improvement for PwPD 5.3 reps). All participants improved ability to get on/off ground.
Conclusion: An immersive, holistic retreat can significantly enhance function, confidence, & quality of life for PwPD – reflecting its effectiveness & lasting impact.

P14.38
1 Texas A&M University, United States
2 Robert Conte Foundation for Parkinson's Disease and Movement Disorders, United States
Background: Community-based exercise programs can enhance motor function and quality of life for individuals with Parkinson’s disease (PD) while offering experiential learning for future healthcare professionals. This study evaluated a service-learning initiative that integrated undergraduate kinesiology students into a PD exercise program and assessed outcomes for both participants and students.
Methods: Across eight academic semesters, 96 individuals with PD and 267 undergraduate students participated in a structured 10-week exercise program involving individualized motor training, functional testing, and guided reflection. Participants completed pre and post-assessments, including the Berg Balance Scale (BBS), Timed Up and Go (TUG), and 30-second Sit-to-Stand (30s STS). Reflections were analyzed using reflexive thematic analysis to identify patterns in learning and professional growth.
Results: Individuals with PD demonstrated consistent improvements in functional balance and mobility, with most showing meaningful gains across clinical assessments. Participants frequently described greater motivation, confidence, and enjoyment, reinforcing the social and emotional value of group-based exercise. Undergraduate students reported increased understanding of PD, enhanced empathy for participant challenges, and greater confidence in clinical and communication skills. Thematic analysis revealed four overarching areas of student growth: (1) knowledge of PD and motor assessment, (2) empathy and awareness of daily challenges, (3) interpersonal connection, and (4) personal and professional development.
Conclusions: This dual-benefit model demonstrates that community-based exercise programs can simultaneously improve mobility in individuals with PD and foster empathy-driven professional growth among future clinicians. The findings highlight a sustainable, evidence-informed approach to integrating education and rehabilitation within community settings.

P14.39
1 University of Connecticut, United States
2 UConn Health, United States
Introduction: Evidence for the effectiveness of exercise to slow disease progression and improve quality of life for people living with Parkinson’s disease (PD) is compelling. However, this powerful intervention does not reach all individuals living with the disease. Unfortunately, Latinx older adults with PD often do not believe that exercise is important in the management of the disease, participate in physical therapy and exercise at lower levels than non-Latinx individuals, and experience lower quality of life and higher burden of disease earlier in the disease course.
Purpose: Examine the feasibility of a digital intervention using peer support to increase physical activity in older Latinx/Hispanic adults living with PD
Methods: This study was a prospective feasibility trial using a single-group, pre-posttest design to assess the primary outcomes of feasibility, acceptability, and appropriateness of a remote, peer-supported, exercise intervention for Latinx individuals living with PD. It was approved by the UConn Health’s IRB and registered with clinicaltrials.gov (NCT06170866; 23-117S-2)
Intervention: This 11-week, peer-supported, remotely delivered, physical activity intervention was tailored to common Latinx cultural values. It included peer training and synchronous and asynchronous components for improving social support and physical activity.
Main Measures: Feasibility, acceptability, and appropriateness were assessed quantitatively (recruitment, attendance, retention rates and safety) and by participant-reported outcome measures (Acceptability of Intervention Measure (AIM), Intervention Appropriateness Measure (IAM), and Feasibility of Intervention Measure (FIM)). Secondary outcomes assessed knowledge, motivation, depression, apathy, social support, physical activity, and quality of life.
Results: Ten individuals were recruited and retained for the study duration without any significant adverse events. Primary outcomes all exceeded the criterion levels (AIM, IAM, and FIM (criterion 75%; 93%, 89%, and 87% of agreement, respectively), attendance (criterion 70%; 82.73%), retention (criterion 90%; 100%). Secondary outcomes demonstrated improvement at the individual and group level.
Conclusions: The peer-supported intervention demonstrated high feasibility and yielded measurable improvements in health-related outcomes, providing preliminary evidence for testing this intervention in a larger, controlled trial among older Latinx individuals with PD.
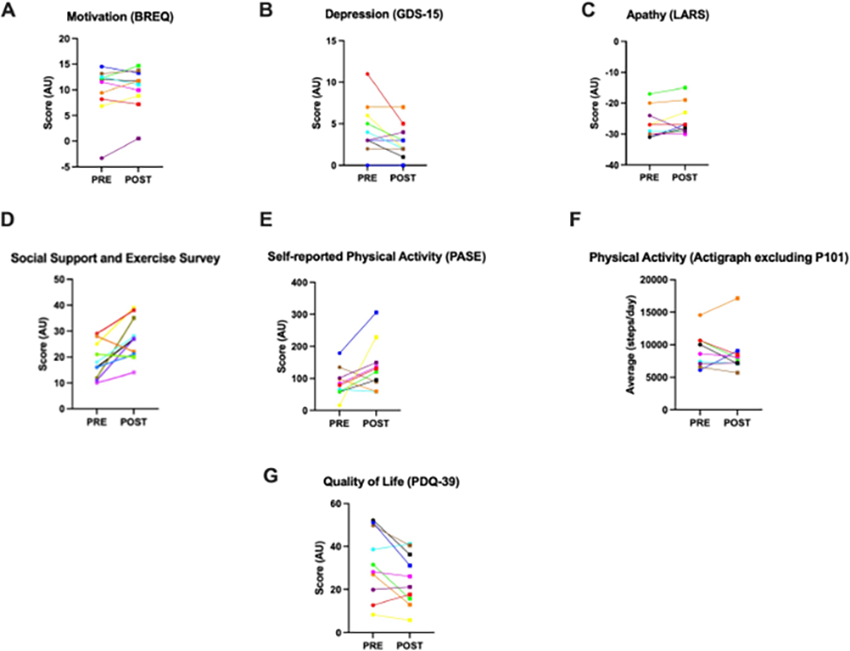
P14.40
1 Teachers College, Columbia Univeristy, United States
2 Parkinson's Body and Mind, United States
3 Teachers College, Columbia Univeristy; Marist University, United States
4 Teachers College, United States
Aerobic exercise is widely recognized as the most effective intervention to slow the progression of Parkinson’s Disease (PD) and manage its symptoms. Exercise guidelines for people with Parkinson’s (PwP) recommend 150 minutes per week of exercise that incorporates aerobic, strength, flexibility, and balance components. Research suggests activities that blend these elements, such as dance, boxing, yoga, and ping pong, may have functional benefits. Group classes also offer psychosocial benefits through social engagement. Thus, community-based exercise programs tailored for PwP are growing. However, instructors often lack specialized training, and few educational resources exist. To address this gap, our team developed an asynchronous, online certificate program for movement professionals working with PwP.
The program was created through collaboration with academic researchers, physical therapists, and Parkinson’s Body and Mind, a patient-facing, nonprofit organization. The team met virtually to identify knowledge gaps among community-based fitness instructors, including understanding PD symptoms, the role of exercise in slowing progression, and movement modifications for specific symptoms. Experts developed modules aligned with their specialties. Lecture videos, recorded at Teachers College, Columbia University, combined slides and demonstrations—featuring PwP and fitness instructors—to illustrate dance, boxing, and yoga adaptations.
The final course includes four modules: Parkinson’s Disease: An Overview for the Exercise Professional; The Role of Exercise and Parkinson’s Disease; Exercise Variations for PwP; and Exercise Types for PwP. The course is designed for professionals across disciplines, including therapists, trainers, coaches, and instructors in dance, boxing, yoga, and Pilates. Learning objectives include applying movement science to creative, practical programming; developing skills to safely serve PwP; and empowering PwP by extending functional independence through targeted exercise. The course costs $350 and provides a certificate upon completion.
As community-based exercise options for PwP expand, there is a critical need to educate instructors. Our interdisciplinary team developed a comprehensive course to equip movement professionals with knowledge and empower them with confidence to deliver safe, effective, and engaging programs for PwP. This resource supports the growth of inclusive, evidence-based exercise opportunities in the community.
P14.41
1 University College Dublin, Ireland
2 Augusta University, United States
3 Emory University, United States
Background People with Parkinson’s (PwP) have limited modulation of spatiotemporal features of forward stepping. Spatiotemporal Activity Modification (STEAM) is a recently developed treatment and assessment tool that uses a library of movement patterns to elicit altered spatial (e.g., joint coordination), temporal (e.g., stepping rhythms), or combined spatiotemporal movement features. A randomized controlled trial was conducted to examine the feasibility, acceptability, and potential outcomes of STEAM training for PwP with mild to moderate symptoms.
Methods PwP were randomly assigned to STEAM treatment administered in either isolated (ISO) or coupled (COU) classes. In ISO classes, spatial and temporal instructions were taught separately, and in COU classes, spatiotemporal instructions were combined. Assessments were completed before and after a 3-week intervention period consisting of 10 x 1.5-hour ISO or COU classes. Feasibility was assessed in terms of recruitment, enrollment, retention, and outcome measure completeness. Acceptability was assessed by a satisfaction questionnaire completed at the end of the intervention.
Results Recruitment and enrollment: Of 292 PwP initially contacted, 68 were eligible, and 42 agreed to participate and provided informed consent. Three did not complete baseline assessments. Using blocked randomization, stratified by sex and disease stage, 22 PwP were allocated to ISO classes and 17 PwP to COU classes (age = 71.80 ± 7.2 years; sex = female 33.3%, male 66.7%; Hoehn & Yahr stage 1 = 16, 2 = 20, 3 = 2, 4 = 1).
Retention: Of 39 randomized participants, 34 completed 10 classes (ISO = 20, COU = 14), 3 completed at least 8 classes, and 2 attended fewer than 5 classes. Seven instructors were trained to use a manualized syllabus and deliver classes with high fidelity. A total of 375 classes were completed (214 ISO, 161 COU).
Outcome measures: Completion rate of clinical outcome measures was high (approx. 0–2.5% missing across key assessments). All participants provided complete motion capture data.
Acceptability: Satisfaction questionnaire data (n = 32) indicated high levels of enjoyment across groups (93.75%). Average positive feedback was similar in the COU (76.19%) and ISO (71.43%) intervention groups.
Conclusions Results indicate that the STEAM intervention is feasible and acceptable for PwP with mild to moderate symptoms. Further analysis will provide preliminary effectiveness data on motor, cognitive, and psychosocial outcomes.
P14.42
1 Arizona State University, United States
2 The Excelling Edge, United States
Older adults often recruit additional neural resources to maintain task performance, a compensatory process that may paradoxically limit neuroplastic capacity and responsiveness to training. Recent evidence, however, indicates that targeted sensorimotor interventions may enhance neuroadaptive potential even in the presence of age- or disease-related decline. In this longitudinal study, we examined visual-motor and cognitive performance in aging adults and individuals with Parkinson’s disease (PD) following a customized sensorimotor training program. Seven participants (ages 54–78 years; 57% female), including two with confirmed PD, completed comprehensive Senaptec-based assessments across nine domains—visual clarity, contrast sensitivity, near-far quickness, target capture speed, perception span, multiple object tracking, eye-hand coordination, and reaction time. Participants engaged in eight weeks of individualized, multimodal training combining home-based and supervised 45-minute sessions, with pre- and post-assessments and one-year follow-up for PD participants. Group-level analysis showed an 86% success rate in Near-Far Quickness training, with substantial perception span gains among older adults (+50% to +100%). Longitudinal PD analyses revealed heterogeneous yet domain-specific improvements: one patient demonstrated cognitive resilience across Near-Far Quickness (+70%), Perception Span (+43%), and Multiple Object Tracking (+42%), while the other showed marked Perception Span gains (+60%). Both exhibited increased near-far accommodation reaction times. Attention-based domains showed consistent responsiveness across all participants, irrespective of age or diagnosis. These findings demonstrate preserved neuroplastic capacity in cognitive-attentional systems despite motor decline, supporting a shift toward individualized, sensorimotor-based intervention strategies that account for inter-individual variability in training responsiveness.
P14.43
1 University of Wisconsin - Madison, United States
2 Wisconsin Chapter of the American Parkinson Disease Association, United States
Decreased access to community-based programming and physical activity (PA) is particularly impactful for people with Parkinson disease (PD). In response, the Wisconsin Chapter of the American Parkinson Disease Association (APDA) partnered with the UW-Madison Sensory Motor Integration Lab research team to create the original Active-At-Home Initiative (AHI) Kit. The Kit includes various PA, adaptive, and informational tools and was designed to promote engagement in meaningful occupations and accessibility of exercise in the home. Community collaborator feedback was gathered from rural dwelling individuals with PD to inform the refinement of the AHI Kit for use in a subsequent telehealth intervention.
Methods: Prototype AHI kits were sent to 30 rural-dwelling individuals with PD who were identified by the APDA. Of this group, 13 community collaborators volunteered to provide feedback and work with the research team to inform development. Semi-structured virtual demonstration calls were scheduled with individual collaborators and qualitative data were gathered, synthesized and extracted into broad themes.
Results: 5 primary themes were identified: some items required demonstration, PD progression informed/will inform use, general appreciation for inclusion, utility of items for caregivers, and varied item usefulness. As informed by community collaborators, the finalized AHI Kit will consist of 5 PA aids, 6 adaptive equipment items, and 14 educational resources.
Discussion: Occupational therapists are uniquely qualified to address the motor and non-motor impacts of PD on everyday life; however, only through collaboration with rural individuals with PD can meaningful and impactful programming address the needs of this community. The results of this development project will inform a telehealth program for rural individuals with PD, and family caregivers, focused on use of the Active at Home Kit. Including rural community collaborators with PD in the development of the resources included in the finalized kit will allow for effective and relevant occupational therapy interventions that promote participation in meaningful activities in the home.
Conclusion: Collaborating virtually with rural individuals with PD was a feasible and accessible mode for gathering feedback and informing resource and program development. Partnering with community collaborators to produce PD-specific resources is a necessary step in developing programming for those in rural areas.
COMPREHENSIVE CARE: Alternative & complementary therapies/ Creativity
P15.02
1 Lucerne University of Applied Sciences and Arts, Switzerland
2 Lucerne University of Apllied Sciences and Arts, Switzerland
3 University of Lille, France
4 University of Hertfordshire, United Kingdom
5 The Music Workshop Company, United Kingdom
6 Switch2Move, Netherlands
7 Conservatorio della Svizzera italiana, Switzerland
8 Leiden University, Netherlands
9 University of Western Ontario, Canada
10 University of Manchester, United Kingdom
11 Western Sydney University, Australia
12 Luzerner Kantonsspital (Lucerne Regional Hospital), Switzerland
13 University of Bern, Switzerland
14 University of Lucerne, Switzerland
15 Ente Ospedaliero Cantonale (Lugano Regional Hospital), Switzerland
16 Clinica Hildebrand, Switzerland
17 Clinica Hildebrand, Ente Ospedaliero Cantonale (Lugano Regional Hospital), Switzerland
18 Brunel University of London, United Kingdom
Introduction Research suggests interventions combining music and movement can positively influence both motor and non-motor symptoms for people with Parkinson's (PwP). Taking a multidisciplinary approach (including PwP, practitioners, medical professionals and researchers), we co-developed a 12-week group intervention titled Songlines for Parkinson’s that provides a toolbox of music-based strategies to improve symptoms for PwP.
Methods Using a mixed methods convergent parallel design, three trials were conducted in the UK and Switzerland (N=42). Functional mobility was assessed using motion capture, gait was evaluated using a pressure-sensitive mat, and symptom severity and quality of life were measured using gold-standard clinical scales (e.g., MDS-UPDRS), and standardized questionnaires (e.g., PDQ-39). Additional questionnaires and bespoke items assessed apathy, imagery use and ability, and music/dance sophistication. Qualitative methods included content and thematic analysis of brief interviews conducted pre, during and post intervention, alongside evaluation of the protocol using field notes and video footage.
Results A statistically significant and clinically meaningful reduction in motor symptom severity (MDS-UPDRS) was found post-intervention F(2,82)=5.51, p=.006, η2G=.02. Significant improvements in gait included increased stride length/velocity (p<.001), foot height (p=.013) and reduced double support time (p=.007). Similarly, improvement in sit-to-stand, stand-to-sit, and decreased yaw angles of head, trunk and pelvis (all p<.01) emerged post-intervention. None of the standardized questionnaires showed significant change, yet the bespoke items indicated a significant (p<.001) increase in the use of motor and music imagery post intervention. Qualitative findings indicated participants experienced a heightened sense of social support, reconnection with their musical identity, and a greater sense of agency over symptom management.
Conclusion The inclusive nature of the development process and method of continuous feedback enabled protocol refinement, contributing to the acceptability, efficacy and enjoyment of the intervention. International trials yielded meta-inferences through integrated methods demonstrating statistically significant, clinically meaningful, and subjective experience of symptom reduction. The intervention is currently being tested in clinics to build on this evidence and enhance accessibility to this non-pharmacological intervention.
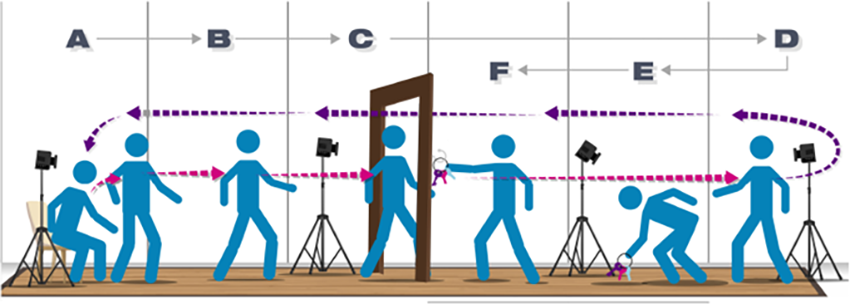
P15.03
1 Radboud University Medical Center, Netherlands
2 University of Vienna, Austria
Background: Artistic professions have been linked to a reduced risk of developing Parkinson’s disease (PD). Separately, diverse arts engagement programs are associated with better mental health in clinical and aging populations. It is unclear whether past artistic occupation or a current creative lifestyle is more relevant for mental health after PD diagnosis.
Methods: Cross-sectional survey study of people with PD (N=360, PRIME-NL sub-cohort). Occupational history was RIASEC-coded (vocational framework classifying professions based on “Realistic”, “Investigative”, “Artistic”, “Social”, “Enterprising”, or “Conventional” qualities); current creativity change (decrease −5 to +5 increase) reflected the past 3 months at timepoint of survey. Outcomes: BDI (depression), SHAPS (anhedonia), STAI (state/trait/total anxiety), PAM-13 (patient activation), PDQ-39 (PD-related quality of life).
Analyses: Wilcoxon rank-sum (artistic vs non-artistic occupation), Kruskal–Wallis with Dunn–Bonferroni (Business/People-oriented/Technical occupational groups), and Spearman correlations (creativity change vs outcomes) with bias-corrected 95% CIs and Holm correction.
Results: Past artistic occupation showed no significant associations with current creativity change or any mental-health outcome. In contrast, higher current creative lifestyle was consistently associated with lower depression (ρ=−0.22), lower anhedonia (ρ=−0.19), lower state/trait anxiety (ρ≈−0.23/−0.20), higher patient activation (ρ=+0.18), and better PD-related quality of life (lower PDQ-39; ρ=−0.22); all Holm-adjusted p ≤ 0.001.
Conclusions: After PD diagnosis, what people do now matters: our findings show that a current creative lifestyle aligns with better mental-health profiles, whereas past artistic occupation does not. These observations are compatible with reports that up to 41% of people with PD experience changes in creative engagement. Clinically, results support signposting to arts engagement programs as part of person-centred care. They also align with recent neuropsychological accounts that supportive creative activity should be distinguished from maladaptive behaviours (e.g., hobbyism, impulse-control disorders, punding). Prospective and randomized studies should test mechanisms and quantify benefits to guide care.
P15.05
1 Centre for Trials Research, Cardiff University, United Kingdom
2 Cardiff University, United Kingdom
3 Sparky Samba, United Kingdom
Background: Music-based interventions are increasingly recognised for their potential to support motor, cognitive, and psychosocial wellbeing in people with Parkinson’s Disease (PD). However, few are systematically described or tailored to the needs of this population. Sparky Samba is a novel group-based percussion intervention designed to promote rhythmic engagement, social connection and movement in PD. Prior to evaluation as a therapeutic intervention, it is necessary to understand how such initiatives may function as health interventions.
Objective: To describe and refine the Sparky Samba intervention using the Template for Intervention Description and Replication (TIDieR) framework, ensuring clarity, adaptability and replicability.
Methods: A qualitative study was conducted using ethnographic observations and semi-structured interviews with participants, band leaders and volunteers. Data were analysed thematically to identify core components, mechanisms of change, and contextual factors influencing delivery. Coded data were systematically mapped onto differing theoretical models as part of a behavioural mapping exercise aimed at identifying the framework that most closely aligns with the mechanisms and outcomes of the Sparky Samba intervention.
Results: Key aspects of Sparky Samba identified included including musical structure, facilitation style, group dynamics and accessibility adaptations. Self-Determination Theory was successfully mapped against the data, aiding identification of mechanisms that may influence engagement and therapeutic outcomes. A logic model was developed to articulate the intervention’s theoretical underpinnings and pathways to impact.
Conclusion: Sparky Samba is a promising, adaptable intervention for PD with clearly defined mechanisms of change. The use of the TIDieR framework enhances its potential implementation, evaluation, and scaling in diverse settings.
P15.06
1 Tor Vergata University of Rome, Italy
2 ParkinZone A.p.s association, Rome, Italy
3 Parkinson No Limits association, Fuerteventura, Spain
4 Department of Neurology, IRCCS INM Neuromed, Pozzilli, Italy
5 Neurosciences and Cell Biology Institute, City St George's University of London, London, United Kingdom
Introduction: Parkinson’s disease (PD) is a complex neuropsychiatric and neurodegenerative disorder characterized by a broad spectrum of motor and non-motor symptoms, substantially impairing quality of life (QoL). Women have long been underrepresented in scientific research, despite the current growing evidence highlighting the unique challenges they face due to differences in physiology and psychosocial factors. Although recent studies are starting to address the real impact of PD in women, targeted therapeutic interventions for their psychological well-being remain scarce.
Objective: This pilot study aims to test the feasibility and outcomes of the innovative outdoor therapeutic program for women with PD, called “Be Woman”, harnessing the restorative power of nature and movement
Methods: Through Parkinson No Limits association in Fuerteventura (Canary Islands, Spain), an all-female team of professionals led a week-long outdoor therapeutic program on the island. Participants engaged in tailored art therapy, adaptive sports, bio-dance and counseling, addressing psychological challenges of women with PD and fostering a new life-project. Neuropsychological assessments were conducted two weeks before and after the retreat.
Results: 10 women with PD were succesfully tested (MA 61.4 ds 6.68)(MDD11.8 ds 4.26)(MoCA≥24)(UPDRS III 25.88 ds 10.99) and completed the week-long outdoor therapeutic program. Preliminary results indicate a significant improvement in QoL as measured by the PDQ-39 questionnaire, including the total score (p = .014) and the subscales of Mobility (p = .034), Activities of Daily Living (p = .028), and Physical Discomfort (p = .049). A significant improvement was also observed in the A subscale of the Parkinson Anxiety Scale (PAS), reflecting a reduction in Persistent Anxiety (p = .030). No significant changes were detected in total Levodopa equivalent daily dose (LEDD) before and after treatment. Further analyses are ongoing.
Conclusion: The Be Woman project is an innovative outdoor therapeutic program feasible for women with PD and effective in enhancing QoL features and psychological well-being. This pilot study lays the groundwork for integrating such initiatives into standardized care for women with PD, addressing their specific needs and promoting tailored rehabilitation.
P15.07
1 Cornwall partnership NHS FT, United Kingdom
2 Independent Dance Artist, United Kingdom
Dance for people with Parkinson’s (PwP) has achieved largescale global growth over the past decade, alongside a strong evidence base across the Arts and Health sectors. Studies show improvements in both motor and non-motor symptoms, including balance, gait, upper limb function, fatigue, and mood as well as enhanced social connection, cognitive function, and overall quality of life.
Parkinson’s Dance Science (PDS) combines this evidence with clinical physiotherapy specialism and artistic experience of dance to help manage Parkinson’s symptoms. Its aim is to offer a personal, social, artistic and creative dance experience with a theoretical, evidenced and therapeutic underpinning.
Method: PDS is a 9 component model - ‘Postural alignment, Fun seated warm up, Dynamic striding, Plies and Sways, Feet and Legs, Vocal creative, Routine/Creative exploration, Cool down and Thanks’.
Each section has a therapeutic underpinning, specifically targeting motor and non-motor symptoms.
A longitudinal, pragmatic, observational evaluation using questionnaires of quality of life (PDQ39), mobility and freezing status at baseline and 3 monthly follow-ups through to 2 years was completed in the naturalistic setting.
Results: The PDS model has successful delivered dance classes for PwP for 12 years making it one of the longest running models worldwide. There are 8 classes delivered across the southwest of England with an average 120 PwP dancing weekly.
46 PwP completed baseline questionnaires with 220 questionnaires returned over the 2-year follow-up period.
Trends for improved scores on all categories of the PDQ39 were noted across the 2 years, as well as significant improvements between baseline and 6 months in ‘improvements in wellbeing’ (P=0.014), ‘stigma’ (P=0.032) and ‘bodily discomfort’ (P=0.039). The majority of participants (63%) retained the same mobility and freezing status over the two-year period.
Conclusions: As designed, this evaluation suggests PDS has a positive long-term effect on both the motor and non-motor symptoms of Parkinson’s, in addition to a possible condition stabilisation against an expected decline.
Importantly, this appears to be in the areas where traditional medical models of care achieve less impact, demonstrating the holistic, sustainable, cost-effective and enjoyable long-term potential for Parkinson’s management from this dance practice.
Further, larger studies are required to demonstrate efficacy and a diversity of impact.
P15.08
1 NeuX Technologies, United States
2 PdLIFE, United States
3 Nova Southeastern University, United States
Introduction Pain is one of the most common and disabling symptoms of Parkinson’s disease (PD), significantly reducing quality of life. Low back pain (LBP) is the most frequent musculoskeletal complaint, affecting 43–74% of people with PD. Compared to the general population, those with PD experience more intense, longer-lasting pain episodes. Contributing factors include altered posture, such as thoracic kyphosis, and PD-related rigidity and dystonia that heighten stress on spinal structures. This case study aims to highlight a non-pharmacological alternative therapy to manage LBP in people with PD.
Methods Interactive Neuromuscular Stimulation (iNMS) is an advanced electrical therapy combining direct current (DC) with alternating current (AC). The NXPro device delivers high-frequency AC (10,000 Hz) with lower-frequency DC (up to 250 Hz) to optimize sensory and motor effects. The AC signal provides a regional nerve block-like effect, relaxing the nervous system, while DC influences motor neurons to reduce rigidity and spasms. Unlike traditional stimulation, iNMS uses active movement during application, promoting neuromuscular re-education. The AC provides an analgesic effect; the DC component supports longer-term neural adaptation and pain reduction.
A 69-year-old male with PD, diagnosed three years earlier, presented with chronic LBP unrelieved by injections, acupuncture, or physical therapy. He declined surgery due to concerns about postoperative inactivity. The patient’s pain level was tracked at each session and pain level effects on exercise participation. Treatment involved iNMS twice weekly for six weeks using the NXPro device. Stimulation at 250 Hz targeted the lumbar region with a flexion-preference protocol, followed by pad placements for hip mobility, posterior chain activation, and spinal mobility.
Results Preliminary outcomes showed decreased pain and increased participation in PD exercise program. Baseline pain averaged 8/10. After iNMS, pain decreased to 3/10, with relief lasting up to two days. Patient had fewer days of extreme pain with overall less pain and increased exercise attendance and participation. Reduced pain enabled greater participation in PD exercise classes, enhancing mobility and quality of life.
Conclusion This case suggests iNMS may be an effective, non-pharmacological option for managing musculoskeletal pain in PD. Improved pain control enhanced exercise participation and mobility. Further controlled studies are warranted.
P15.09
1 Interdisciplinary Laboratory for Research, Education and Disability Support – IREDS Lab, Department of Physiotherapy, University of West Attica, Athens, Greece, Greece
2 Department of Hygiene, Epidemiology and Medical Statistics, Medical School, National and Kapodistrian University of Athens, Athens, Greece, Greece
3 Department of Health Data Processing, Digital Governance Service, Greek Ministry of Health, Greece
4 Department of Physiotherapy, University of West Attica, Athens, Greece, Greece
5 1st Department of Neurology, Eginition Hospital, Medical School, National and Kapodistrian University of Athens, Athens, Greece, Greece
Dance for Parkinson’s Disease (DfPD®) is a dance program specially designed for people with PD. We aim to investigate the effect on quality of life (QoL), as well as the safety, feasibility, and patient satisfaction of a DfPD® program delivered both in-person and online to Greek early-to-mid-stage PD patients. Pre- and post-interventional assessments of balance, cognitive functions, motor and non-motor PD symptoms and signs (using MDS-UPDRS), depression, anxiety, fatigue, sarcopenia, frailty and body mass index (BMI) were performed. The Upbeating GReek Application of DancE in Parkinson’s Disease (UPGRADE-PD) (ClinicalTrials.gov NCT06220084) is a 3-arm crossover and open-label randomized controlled trial (in-person DfPD®, online DfPD®, control). It consists of a total of sixteen 60-minute dance classes twice a week for each interventional group, a 2-month non-interventional control group, and two 2-month washout periods in-between. Forty patients (35% men, aged 67±9) participated to the program.
A multivariable linear mixed-effects model with random participant intercepts was applied to account for the crossover design. In-person treatment was a strong, independent predictor of QoL (PDQ-8) improvement post-treatment, compared to the online arm (β=−3.96, p=0.007), with the control group exhibiting a comparable effect (β=−3.31, p=0.029). Marginal associations confirmed that the in-person treatment produces the strongest and most significant gains in QoL post-treatment (β=−2.79, p=0.030) than both online and control approaches. The findings were adjusted for age, levodopa equivalent daily dose (LEDD), and disease severity (H&Y). No evidence of carryover effects was observed. A record of a) no adverse events, b) high adherence (80,3% vs 79,86% for in-person vs online) and low attrition (5% for both) rates, and c) a preference to continue the in-person versus the online intervention (76% vs 63%, p=0,022) was noted. Overall, significant benefits on QoL were noted with the in-person versus the online intervention, while further analysis of secondary outcomes is ongoing.
P15.10
1 Iowa State University, United States
Introduction/Background: Research in neuroimaging has revealed that listening to preferred music stimulates the ventral tegmental area (VTA) and nucleus accumbens (NA), suggesting that music may engage the same dopaminergic networks that are involved in reinforcement learning and reward (Menon, 2005). Furthermore, previous work in animal models has demonstrated that stimulation of the VTA through optogenetics is associated with an increase in slow wave Delta band (1-4 Hz) oscillations in the prefrontal cortex (Kim et al., 2017). This study aims to determine if preferred music listening will modulate delta cortical oscillations in the VTA and NA via measurement of their upstream projections in the PFC in persons with Parkinson’s disease (PD).
Methods: Data from healthy young adults (HYAs), healthy older adults (HOAs), and persons with PD were collected. Participants completed 3 different listening conditions: rest, white noise, and preferred music. Each condition lasted 3 minutes. The preferred music condition consisted of a participant-selected song that was self-rated as an 8 or above on the Likert scale, was non-lyrical, and had a tempo between 120-150 bpm. During the collections, the participants wore a MUSE EEG headband consisting of four wireless electroencephalographic electrodes (TP9, AF7, AF8, and TP10) to measure activity over the PFC.
Results: Percent change scores of cortical oscillations from participants were assessed within preferred music listening and white noise conditions. A repeated measures
ANOVA was conducted to compare the effect of music condition on delta oscillation scores. Preliminary results show no significant differences between electrode placement or music condition, t(7)=1.11, p>0.14, but a moderately strong effect size (d=0.72), associated with electrode AF8 between music and white noise conditions in HYAs. Data analysis in HOAs and those with PD is ongoing.
Conclusions: Preliminary results suggest that there is no significant difference between music and white noise conditions. Results from this research will be extended to explore if these neural mechanisms are similar in HOAs and persons with PD.
P15.11
1 The Queen’s Medical Center, United States
2 The Queen's Medical Center, United States
3 University of Hawai'i-John A. Burns School of Medicine, United States
4 Pacific Health Research and Education Institute, United States
Introduction: Evidence-based dance programs have demonstrated improvements in physical and emotional outcomes for people with Parkinson’s disease (PD). The indigenous Hawaiian dance form, hula, has shown promise in enhancing quality of life among people with cardiovascular risk, yet its feasibility for PD remains unexplored. This study evaluated the practicality, acceptability, and potential benefits of a hula intervention for people with PD.
Methods: The program was developed with guidance from people with PD, care partners, Hawaiian cultural practitioners, and professionals from Dance for PD®. Individuals with mild to moderate PD were recruited through The Queen’s Medical Center Parkinson’s and Movement Disorders Center and community outreach efforts. Weekly one-hour hula classes, led by an experienced hula instructor and supervised by a movement disorder specialist, were held from January to April 2025. The primary outcome was feasibility, assessed through retention, safety, and resource needs. Secondary outcomes included motor and non-motor function measured by the Unified Parkinson’s Disease Rating Scale-Part III (UPDRS-III) and the Parkinson’s Disease Questionnaire-39 (PDQ-39), administered pre-and post-intervention. Qualitative interviews following the program were thematically analyzed to capture participant experiences.
Results: Of 18 enrollees, 14 completed the program and 2 were excluded from data analysis due to diagnosis changes. The average attendance rate of 11 participants (7 females, 4 males; Asian American=6, White=3, Native Hawaiian=2) was 69% (9 out of 13 classes). The only adverse event was a fall, unrelated to class activities and without significant complication. Mean UPDRS-III scores decreased by 4.18 points, though changes in PDQ-39 were not statistically significant. Qualitative data indicated perceived improvements in mood, motivation, confidence, social connection, and self-efficacy. Participants described hula’s integration of Hawaiian language, music, and storytelling as more cognitively engaging than conventional movement therapies.
Conclusion: The hula program was feasible, safe, and well-received by people with PD. While not powered to detect significant score changes, positive trends warrant larger studies. Findings suggest that hula may serve as a holistic, culturally grounded intervention that fosters physical, emotional, and cultural well-being while supporting the preservation of Hawaiian language and traditions.
P15.12
1 International Table Tennis Federation Foundation, Spain
Introduction: This work introduces an innovative therapeutic framework that combines table tennis with simultaneous motor–cognitive actions specifically designed for people with Parkinson’s disease (PwP). Rather than focusing on table tennis alone, the approach centres on performing physical and cognitive tasks at the same time, promoting the interaction between mind and muscle. The framework aims to strengthen coordination, balance, focus, and memory through structured and engaging activities that challenge both body and cognition concurrently.
Methods: Four training modules were developed: (1) hand–eye coordination, combining table tennis movements with simultaneous independent hand actions to enhance bilateral control and neuroplasticity; (2) postural balance, linking stroke execution with controlled stance and centre-of-gravity adjustments to improve proprioception and whole-body awareness; (3) attentional focus, integrating visual stimuli and decision-making tasks that demand concentration and problem-solving while maintaining technical precision; and (4) memory stimulation, coupling table tennis exercises with short- and long-term recall activities that activate working and procedural memory through structured interaction and repetition.
Results: The simultaneous execution of motor and cognitive tasks encourages continuous mind–body engagement and stimulates neuroplastic mechanisms through dual activation of cognitive and motor pathways. This combined practice enhances coordination, stability, attention, and recall more effectively than isolated table tennis or single-domain training, producing a broader functional response and greater participant motivation.
Conclusions: By focusing on specifically designed simultaneous motor–cognitive exercises rather than isolated performance measures, this integrated, multi-domain approach positions table tennis as an effective and enjoyable therapeutic model for Parkinson’s disease. Supported by pilot evidence (Ortega-Montes & Rodríguez-Martín, STAT-ON®, 2026), it represents an innovative, replicable, and engaging pathway for improving functional performance and reducing symptoms in PwP to a greater extent than table tennis alone. Future studies could further investigate whether simultaneous motor–cognitive training produces greater symptom reduction and quality-of-life improvement than table tennis alone.
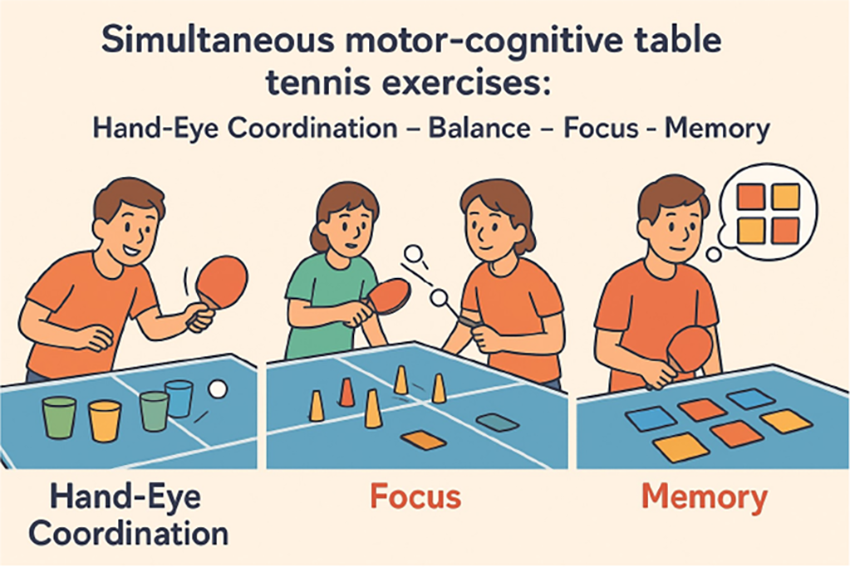
P15.13
1 Universidade Federal do Rio Grande do Sul, Brazil
Introduction: PD is a neurological disease characterized by the impairment of dopaminergic cells. PwP live daily with motor and non-motor symptoms that negatively impacting their quality of life. Given the absence of a cure, treatment is multidisciplinary, creating opportunities for dance to be integrated into health promotion and rehabilitation. Research indicates that the constant changes experienced by dancers in improvisational contexts challenge balance, agility, attention, choice, and decision-making, along with other physical and cognitive skills (Batson, 2016). Methods: This proposal implemented an one-hour improvisational dance workshop for seven PwP in celebration of World Parkinson’s Disease Awareness Day (April 11th). It was designed to stimulate participants’ creativity through dance improvisation and a reflection moment to write about the their relationship to PD and to dance. Results: During the workshop, it became clear that dancers explores movement paths, using their bodies as a form of language. Stereotypes and preconceptions were set aside, leaving only bodies, experiences, and individual narratives. Improvisations were guided by the rhythm, beat, and lyrics of the music, and dancers often transformed observed movements creatively, reinforcing a sense of community and belonging. Written reflections from the participants included statements such as: “Having Parkinson’s isn’t very good, but having dance is wonderful”; and “Thanks to Parkinson’s, my life has changed radically in every way. I am a transformed human being. I am grateful and touched by everything the teachers teach us.” These examples highlight the therapeutic potential of dance, even within an one-hour workshop. Conclusion: Improvisation involves engaging creativity, accessing personal repertoires, memories, and stories, activating the imagination. It also requires surrender and enjoyment. This was the invitation extended to PwP on their dedicated day. A day to acknowledge those who face and overcome daily challenges imposed by the disease and by a society often unaware of their reality. Through dance and spontaneous personal composition, participants created a shared space of strength and companionship, allowing them to experience moments of joy, laughter, and fun.
References: BATSON, Glenna et al. Verbal Auditory Cueing of Improvisational Dance: a proposed method for training agency in parkinson’s disease. Frontiers In Neurology, [S.L.], v. 7, p. 1-10, 17 fev. 2016.

P15.14
1 Saltmarche Health .& Assoicates, Canada
2 Gaitway Neurophysio, Canada
3 Brain and Mind Centre, University of Sydney, Australia
4 Sydney Adventist Hospital, Australia
5 Veterans Affairs Boston Healthcare System,, United States
6 School of Pharmacy, University of Mississippi, United States
7 NHMRC Clinical Trials Centre, University of Sydney, Australia
8 College of Health and Medicine, Australian National University, Australia
Objective: To evaluate the effects of extended photobiomodulation therapy (PBMt) combined with exercise on health-related quality of life (HRQoL), plus motor and non-motor outcomes in people with Parkinson’s disease (PD).
Methods: In this three-stage, randomized, sham-controlled trial, participants received active or sham PBMt - e.g., transcranial, cervical, and abdominal light-emitting diode (LED)/laser therapy three times a week for the first eight weeks, alongside at least three hours per week of vigorous exercise (e.g., Rock Steady Boxing). Stage 1 provided active PBMt (n=32) vs. sham PBMt (n=31); Stage 2 provided all participants with active PBMt; Stage 3 followed “continuers,” i.e., those who chose to continue PBMt home treatment (n=17) versus “non-continuers” (n=26), for up to 48 weeks. Content and thematic analyses provided a quantitative overview of quality of life data, as well as a deeper qualitative understanding of the meaning behind the narratives of participants and families.
Results: The therapy was safe, well-tolerated, and easy to use at home, with no reported side effects. The thematic analysis revealed substantial improvements in HRQoL, with participants and families reporting benefits such as improved sleep, cognition, and social engagement: “Everyone has noticed the improvement—it is really remarkable,” “I have my grandpa back”, and “Gives us hope, taking action against Parkinson’s.” Participants found PBMt easy to use at home and to integrate into daily routines, resulting in consistent treatment.
Conclusions: The results complement the quantitative motor and non-motor outcome measures, that indicated improvements in the primary outcome measure (timed up-and-go), components of the Movement Disorder Society-Unified Parkinson’s Disorder Rating Scale (MDS-UPDRS), and anxiety. Extended PBMt combined with exercise led to many qualitative improvements in quality of life, recognized by the Parkinson’s participants, their caregivers and family, that were not seen in those participants who participated in exercise alone. These findings support PBMt as a promising adjunctive therapy for Parkinson’s disease and warrant further large-scale, long-term trials.
P15.15
1 Saltmarche Health .& Assoicates, Canada
2 Gaitway Neurophysio, Canada
3 Brain and Mind Centre, University of Sydney, Australia
4 Sydney Adventist Hospital, Sydney, Australia
5 Veterans Affairs Boston Healthcare System, Department of Neurology, Boston University School of Medicine, United States
6 School of Pharmacy, University of Mississippi, United States
7 College of Health and Medicine, Australian National University, Australia
Background: Facial masking (hypomimia) and speech changes, such as a soft, monotone, or hoarse voice (hypophonia), are common in Parkinson’s disease (PD). These symptoms, caused by impaired motor control of facial, oral, and throat muscles, reduce emotional expressiveness and hinder communication. Misinterpretation of emotions often leads to frustration, social withdrawal, and reduced quality of life (QoL) for people with PD and their families.
Objective: To evaluate the effects of extended photobiomodulation therapy (PBMt) combined with exercise on facial expression, voice, health-related QoL, plus motor/non-motor outcomes in PD.
Methods: In a three-stage randomised controlled, sham-controlled trial, real-world trial, participants received active or sham PBMt, e.g., transcranial, neck, and abdominal light emitting diodes (LED) and laser therapy, three times weekly for eight weeks plus ≥3 hours per week of vigorous exercise monitored weekly (e.g., Rock Steady Boxing). Stage 1 provided active (n = 32) vs sham (n = 31); Stage 2 provided all participants with active PBMt; Stage 3: “continuers” i.e., those who continue PBMt home treatment (n = 17) vs “non-continuers” (n = 26) for up to 48 weeks. Computer vision and deep-learning analysis of participant videos quantified facial expressivity and voice. Participants and family members reported perceived changes in communication and QoL.
Results: Deep-learning analysis revealed measurable gains in facial expressivity and vocal intensity. Participants and caregivers reported enhanced communication, increased social engagement, and improved overall quality of life. PBMt devices were easy to use and safely integrated into home routines.
Conclusions: Extended PBMt plus exercise produced sustained improvements in facial expression, communication, mobility, and anxiety versus exercise alone. These results reinforce the previously reported improvements in both motor and non-motor symptoms observed in this clinical trial. PBMt was safe and simple to use at-home therapy. These findings support PBMt as an adjunct to comprehensive, multidisciplinary PD management. Further research is warranted.
COMPREHENSIVE CARE: Lay/professional health literacy & Public thought
P16.01
1 University of North Dakota School of Medicine and Health Sciences, United States
Introduction: Patients with Parkinson Disease (PD) are at considerable risk of hospitalization due to baseline disturbances in balance, gait, and swallowing dysfunction. Many PD patients have strict regimens for dopamine-replacing agents, and disruption to these schedules can lead to uncontrolled symptom management, as well as other medical and psychiatric adverse events. During hospitalization, patients may face multiple challenges in getting their carbidopa-levodopa (CL) medications on time. This project aims to evaluate how often CL was not given on schedule across our hospital system.
Methods: We reviewed 101 patients with a diagnosis of PD admitted to our hospital system between 2021 and 2025. Patients not on any form of CL were excluded from this study. Home medication lists were reviewed for each patient and compared to the inpatient Medication Administration Record (MAR), including the dosage, formulation, and scheduled frequency. Administration time of each CL dose was logged. Doses of CL not given within 15 minutes of a patient’s prescribed home schedule were considered improperly timed.
Results: All patients reviewed had the correct dosage, formulation, and frequency of their CL ordered while hospitalized. However, adherence to home dosing schedules varied widely. A total of 947 CL doses were reviewed, with 590, or 62.3%, of doses found to be incorrectly timed.
Conclusions and Implications: Our analysis found that the majority of CL doses were not administered to hospitalized CL patients within a timely manner. Coordinating accurate and timely CL administration for hospitalized PD patients can be understandingly difficult for providers and staff less familiar with these regimens. This project aims to provide awareness and underscore the importance of adhering to proper PD medication times. Multidisciplinary coordination among clinicians, pharmacy, and nursing staff is essential to optimize inpatient care for individuals with PD.
P16.02
1 University of Connecticut, United States
2 Parkinson's Foundation, United States
Introduction. Many people with Parkinson’s disease (PD) report having unasked or unanswered questions and a desire for more information on disease progression and daily life. Limited understanding of symptoms, treatments, and disease management leaves patients seeking reliable information beyond clinical encounters. As a result, individuals are turning to social media communities such as Reddit to ask questions, share experiences, and connect with others. These online discussions provide a valuable, real-time window into the priorities and lived experiences of people with PD. We analyzed posts from the Parkinson’s Reddit community to identify key themes in patient discussions.
Methods. Posts from the r/Parkinson’s subreddit between January 1, 2024, and March 1, 2025, were extracted using Python and analyzed using Braun and Clarke’s reflexive thematic analysis. Of 984 posts by 672 users, 318 (from 207 users) were identified as being written by a person with PD or someone questioning a diagnosis. These were coded independently by two coders (agreement = 94%), with conflicts resolved by a third reviewer, yielding full consensus. Findings were confirmed by a patient researcher. This study was deemed not human subjects research by the University of Connecticut IRB.
Results. Four themes emerged: (1) the everyday reality of PD, including changing relationships, challenges of daily living, financial concerns, and navigating healthcare; (2) navigating diagnosis and risk factors, reflected in posts about symptoms, diagnosis experiences, test interpretations, and possible causes; (3) medical management of PD, encompassing symptom sharing, medication use, lifestyle changes, alternative therapies, and medical procedures such as hospitalization and DBS; and (4) finding support and solidarity, focused on emotional experiences, shared resources, and community connections. Because of the nature of Reddit, demographics are unavailable; however, 75 users self-reported their age (M = 47.8, SD = 13.6).
Conclusion. Online discussions reveal that people with PD seek answers, guidance, and community support on a wide range of issues. The themes identified in this study highlight critical gaps in information, care, and connection that affect how individuals understand and manage their condition. Insights from these conversations can guide more responsive clinical practice, patient-centered education, and future research that better addresses the lived realities of people with PD.
P16.03
1 American Parkinson Disease Association, Florida Chapter, United States
Background: The Florida Chapter of the American Parkinson Disease Association (APDA) partners with Mayo Clinic–Jacksonville, one of nine APDA Centers for Advanced Research (CAR), to advance scientific discovery while ensuring that people with Parkinson’s disease understand and benefit from these developments. The Mayo Clinic–Jacksonville CAR conducts studies on gene mutations, gait and balance in advanced PD, and the role of Lewy bodies in the gut. Each year, the team cares for approximately 1,500 patients and performs 75–100 deep brain stimulation procedures. To bridge the gap between cutting-edge research and the lived experience of Floridians with PD, the APDA Florida Chapter collaborates with the research team and community partners to promote engagement, education, and dialogue. Objective: To highlight the Florida Chapter’s efforts to connect the Mayo Clinic–Jacksonville CAR with the local Parkinson’s community through educational programming and to summarize participant feedback from the 2025 research-focused event. Methods: In March 2025, the APDA Florida Chapter hosted a research-focused community event in Ponte Vedra featuring presentations from Mayo Clinic–Jacksonville investigators. Researchers explained their projects in clear, accessible language, describing why their work matters and how findings may impact people with PD. The program concluded with a panel discussion and Q&A session led by APDA staff, offering participants the opportunity to engage with experts. Attendees completed post-event surveys assessing clarity, accessibility, and engagement. Results: Surveys showed high satisfaction and strong community interest. Seventy percent of participants rated the research presentations as “Excellent,” while 74% gave the same rating to the panel discussion and Q&A. Content relevance was the main reason for attendance (82%), and all respondents (100%) expressed interest in future programs. Many attendees indicated new interest in research participation, citing comments such as “I’d like to sign up for a study,” and “I plan to donate to research in my dad’s honor.” Conclusion: The Florida Chapter’s collaboration with the Mayo Clinic–Jacksonville CAR demonstrates that research–community partnerships can successfully connect patients, caregivers, and scientists in shared learning. Building on this success, APDA Florida and Mayo Clinic plan to expand this approach into an annual Research Conference to deepen engagement and extend impact statewide.
P16.04
1 Methodist College, United States
Prevalence rates for Parkinson's disease (PD) are increasing. The increased prevalence is associated with growing interest from the news media. Recently, a dozen articles on PD have appeared across various sources of the mainstream press. PD is chronic, progressive, and varies greatly across people. Research suggests that increased preparation of nurses can lead to significant improvement in well-being for those impacted by PD. To this end, the Edmond J. Safra Foundation has worked toward training nurse educators to enhance knowledge, skills and abilities of nursing students related to PD. We report on the inclusion of Parkinson's disease as a broad theme for an established campus/community film group (ongoing for 7 years) at a small midwestern nursing/health sciences college and a local Osher Lifelong Learning Institute. Initially, the film group was designed to provide a forum for students to interact with older adults in non-healthcare environments to help disabuse stereotypes about older people and to help relieve isolation and loneliness for older adults. The course used for the film group is an introductory psychology course with course content divided into three sections (biological, social and clinical psychology) with films matched to each subject matter. Integrating a prevalent chronic disease as an overarching theme for the films allowed us to attract the interest of others from the community (e.g., existing Parkinson disease support groups) to provide other perspectives on this disease. Twenty-three people were involved in the film group. Students served the role of film facilitators for two films following the lead provided by the course instructor who reviewed the first film. As an experiential learning project, students also prepared reflections related to participating in the group. Initial qualitative analyses showed these themes: enhanced knowledge about PD; authenticity of each type of movie (independent, box-office and documentary) in allowing audience to see/hear about lived experiences with PD; positive experience of sharing stories with family members of people with PD and learning miscues about PD from professionals early in their careers; development of skills related to patient advocacy; and appreciation for communicating/listening skills development when involved in campus/community project such as this one.
COMPREHENSIVE CARE: Disability and quality of life
P17.01
1 Cardiff University, United Kingdom
2 World Health Organisation, United Kingdom
Background: Loneliness and social isolation remain major challenges for people living with progressive neurological conditions (PNC), including Parkinson’s disease (PD). Social participation is closely linked to quality of life, yet opportunities are constrained by accessibility barriers, stigma, and inconsistent service provision. Despite directives, evidence to guide sustainable interventions remains limited.
Objective: This mixed-methods PhD, guided by patient involvement, investigates current approaches to supporting social participation, examines barriers and facilitators, and synthesises evidence to inform the development of actionable recommendations and a framework for future interventions.
Methods: Four interlinked workstreams were undertaken:
Scoping review of interventions promoting social participation among people with PNC.
Survey of individuals with PNC, health and social care professionals, and activity organisers.
Qualitative interviews with people affected by PNC and health/social care professionals, plus focus groups with activity organisers.
Workshops to co-produce a logic model and intervention framework.
Results: The scoping review included 37 studies and identified a range of interventions, from physical activity programmes to digital initiatives, yet many failed to overcome barriers to accessibility and inclusion. The survey included responses from people with PNC, including PD (n = 40), multiple sclerosis (n = 11), ataxia (n = 6), motor neuron disease (n = 1), and multiple system atrophy (n = 1), alongside health and social care professionals (n = 16) and activity organisers (n = 10). Interviews (n = 21) and focus groups (n = 3; n = 4) highlighted stigma, transport, and financial constraints as barriers. Person-centred approaches, clear communication, and trust in providers were marked as essential, while seeing peers with similar conditions take part was a powerful motivator. Service providers stressed funding constraints and fragmented links between services, limiting sustainability and reach. Cross-cutting themes included digital accessibility, equity of provision, and the influence of societal attitudes.
Conclusion: By integrating multiple perspectives, this research highlights systemic barriers while also identifying practical levers for change. The emerging logic model and recommendations will provide a framework for developing effective interventions to enable people with PD and other PNC to remain connected, active, and socially engaged.
P17.02
1 University of Canberra, Australia
Introduction: This study aims to explore the psychosocial impacts and access to community health services for young women diagnosed with Young Onset Parkinson’s Disease (YOPD). Parkinson’s Disease (PD) is typically diagnosed in individuals over the age of 50, but YOPD affects those under 50, leading to unique challenges and unmet needs. The study focuses on the Australian context, acknowledging the global burden of PD and the lack of targeted research on YOPD, particularly among women and ethnic minority groups.
Methods: The research employs a mixed-methods approach, combining quantitative data on the incidence and prevalence of YOPD with qualitative interviews and surveys to understand the psychosocial impacts on young women. The study also reviews existing literature to identify gaps in research and treatment plans for YOPD patients. The research design includes Memory Work, focus groups, and participatory research methods, where participants act as co-researchers. This multi-phase approach ensures a comprehensive understanding of the participants' experiences.
Results: The findings indicate that young women with YOPD face significant psychosocial challenges, including increased medical costs, prolonged uncertainty, and higher incidences of anxiety and depression. The delay in diagnosis and treatment exacerbates these issues, leading to a lower quality of life (QoL) and unmet psychosocial needs. The study also highlights the lack of specific guidelines and resources for women and other minority groups with YOPD. Common coping strategies were identified, emphasising the need for gender-sensitive healthcare and individualised treatment plans to improve their QoL.
Conclusion: The study underscores the need for a more targeted, multidisciplinary approach to improve the QoL for young women diagnosed with YOPD. Future research should focus on developing individualized treatment plans and improving access to community health services. The proposed project, "Young Women Improving their Wellbeing Together Post-Diagnosis of Parkinson’s Disease," aims to address these gaps by providing tailored support and resources to enhance the wellbeing of young women with YOPD. The findings will inform healthcare recommendations and advocate for policy changes to better support these women, with a focus on enhancing mental health support, improving workplace and health policies, and promoting social connections.
P17.03
1 University of the Sunshine Coast, Australia
2 Person with Parkinsons and consumer researcher, Australia
Background Stigma is a common and damaging experience for people with Parkinson's disease (PwPD), strongly linked to poorer quality of life, psychological distress, and social isolation. Visible symptoms (e.g., tremor, rigidity) and non-motor symptoms (e.g., cognitive impairment) can both contribute to stigmatising encounters, often due to misinterpretation. Traditional standardised measures used to study stigma are limited by recall bias, failing to capture the subjective and dynamic nature of these real-world experiences. This study aimed to overcome these limitations by using Ecological Momentary Assessment (EMA)—a real-time data capture method—to explore the lived experience of stigma.
Purpose To explore the real-world experiences of stigma among PwPD using EMA to increase understanding about its contextual features, specific triggers, and impact on daily life. This includes identifying the situations of stigma, exploring how PD symptoms contribute to these experiences, and describing the coping strategies PwPD employ.
Methods This study used an exploratory mixed-methods design with 20 adults diagnosed with PD. After a baseline assessment using validated tools to measure symptoms, quality of life, and stigma, participants began a seven-day EMA period. Using a smartphone app, they responded to four brief, randomised survey prompts per day and could also self-initiate a survey immediately following a stigmatising event. These momentary surveys gathered real-time data on the context, nature of the stigma, symptom status, and coping responses. Following the EMA period, focus groups were conducted to provide qualitative depth and aid in interpreting the quantitative data.
Results and Conclusion This methodology successfully yielded rich datasets detailing subjective daily experiences. Preliminary analysis confirms that stigma is a highly contextual and dynamic phenomenon, with significant variability in the frequency, source, and type of experiences across different environments and social interactions. By providing an accurate, real-world portrayal of stigma, this study identifies specific situational triggers and coping strategies. These findings will supply crucial evidence for creating targeted stigma-reduction initiatives designed to enhance support, promote social inclusion, and ultimately improve the quality of life for the entire Parkinson's disease community.
P17.04
1 Laboratoire Ergonomie et Sciences Cognitives pour les Transports, LESCOT, Université Gustave Eiffel, Univ Lyon, Lyon, France, France
2 Service de Médecine Physique et de Réadaptation Neurologique, Hôpital Henry-Gabrielle, Hospices Civils de Lyon, Lyon, France / Université de Lyon, Université Claude Bernard Lyon 1, Lyon, France, France
3 Service de Médecine Physique et de Réadaptation Neurologique, Hôpital Henry-Gabrielle, Hospices Civils de Lyon, Lyon, France, France
Background: Parkinson’s disease (PD) is associated with reduced mobility, social withdrawal, and decreased quality of life. Physical activity is now well known to reduce the manifestations of the disease, by slowing its progression and reducing the motor symptoms. An intensive, multidisciplinary rehabilitation program was developed to address daily life difficulties in PD. Group of 6 patients join a 5-weeks rehabilitation program including up to 5 daily activities (physical therapy, speech therapy, occupational therapy and adapted physical activity sessions). Our previous findings on 14 patients showed an improvement in walking performance and cortical activity. Indeed, immediately after the intensive training, decreased stride time and increased stride length were observed. These behavioral changes were accompanied by a reduced cortical activation in the prefrontal cortex, suggesting a decreased cognitive demand during motor task following the program. Yet the perceived impact of the program on daily life remains unclear.
Aim: An ongoing study aims to compare two groups of 30 patients: one receiving the intensive program and the other under conventional care to measure que impact of the intensive rehabiliation program perceived by patients on their daily life.
Methods: Three standardized questionnaires are administered at baseline (T0) and six months later (T1): the Parkinson’s Disease Questionnaire (PDQ-39) for quality of life, the French version of the Life Space Assessment (LSA-F) for mobility, and the Community Integration Questionnaire for social participation.
Expected Results: We hypothesize that at T1 patients in the experimental group will report sustained improvements in quality of life, mobility, and social participation compared with both their baseline assessment and the control group. Preliminary results will be presented during the congress.
Conclusion: If confirmed, these results will contribute valuable evidence for the mid-term benefits of the intensive multidisciplinary rehabilitation program in PD and support the implementation of more patient-centered therapeutic interventions.
P17.05
1 Raimunda Moura Program for Parkinson’s Disease-SMS/Atibaia/Brazil., Brazil
2 Raimunda Moura Program for Parkinson's Patients, Brazil
Introduction: Parkinson's disease is a degenerative disorder of the central nervous system that primarily affects the motor system.(Nitrini and Bacheschi, 1991; Gamboa et al., 2001).
Due to the conditions inherent to Parkinson's disease (rigidity and bradykinesia), changes in the areas of voice, speech, and swallowing are common. These changes compromise patients'communicationandeating.
Instituted by municipal law number 4464 of October 11, 2016, the Raimunda Moura Program for Parkinson's Patients objective to treat and care for patients by improving their functional capacity, flexibility, balance, muscle strength, and, consequently, their ability to perform activities of daily living and achieve independence. This program is located in the city of Atibaia, in the interior of SP.
Objectives: to evaluate speech-language disorders in the elderly population with Parkinson's disease, with a mean age of 68.8 years and in stages I, II and III of the disease according to the HY scale.In speech-language pathology, 25 patients are assessed using validated protocols such as PADAF and PARD and receive treatment for speech, voice, and swallowing.
Result: Among the 25 patients in the study, 15 had mild dysarthria (10 in stage 1 of the disease and 5 in stage 2); however, 6 patients had moderate dysarthria (2 in stage 1 of the disease and 4 in stage 2). Relevant to this, 4 patients had severe dysarthria (2 in stage 2 of the disease and 2 in stage 3). Of the 25 patients in the study, 17 had mild dysphagia (9 in stage 1 of the disease and 8 in stage 2); 7 patients with moderate dysphagia (4 in stage 2 of the disease, 2 in stage 1 and 1 in stage 3) and 1 patient with severe dysphagia who was in stage 2. Among the 25 patients in the study, the majority 17 men and 8 women. The mean age of the participants was 68.8 years.
Conclusion: Early speech-language pathology intervention in Parkinson's disease is crucial to slow the progression of symptoms, prevent serious complications, and preserve the patient's quality of life. Initial intervention focuses on preventive and rehabilitative aspects, helping to maintain independence and social participation.
P17.06
1 Tor Vergata University of Rome, Italy
2 ParkinZone A.p.s association, Rome, Italy
3 Parkinson No Limits association, Fuerteventura, Spain
4 Department of Neurology, IRCCS INM Neuromed, Pozzilli, Italy
5 Neurosciences and Cell Biology Institute, City St George's University of London, London, United Kingdom
Introduction: Parkinson’s disease (PD) is a neuropsychiatric neurodegenerative disorder that profoundly impacts all aspects of daily life, from independence to functionality in everyday activities, including clothing choices and self-perception. The worsening of motor and non-motor symptoms combined can lead to a dysfunctional relationship with the body, which also influences people with PD (PwPD) in their clothing and fashion choices. Scientific evidence on these specific topics and challenges are still limited.
Objective: This international online survey aimed to assess daily clothing challenges for PwPD, also exploring their self-image perception and raise awareness of possible gender differences and disparities.
Methods: The survey was sent to participants via Google Forms questionnaire during 2024 and 2025. It included Likert scales, open-ended, and multiple-choice questions.
Results: 225 PwPD participated in this international online survey (M=88, F=137)(118 from Italy, 99 from Spain and 8 from England)(MA 61.9yrs ds 1.5)(MDD 10.9yrs ds 1.38). Although general interest in fashion was high (84%), 54.2% of PwPD reported changes in clothing choices due to disease progression (65.6% in women). The survey identified back zips, high heels, buttons, and shoelaces as the most problematic items. Further patient-reported analysis highlighted additional problematic clothing types, ranked as underwear, tight-fitting garments, and heavy outerwear (e.g., thick jackets/coats). Women experienced greater discomfort with gender-specific clothing: 46.4% of men reported difficulty with neckties, while 72.5% and 87% of women reported difficulties with brassieres and high heels, respectively. Regarding body image, only 11% described their current self-image as "Great," 22% as "Good/Fine," while 36% perceived it as "Worsened," 21.5% as "Awful," and 9.5% reported dispreception or non-recognition when seeing themselves in the mirror (73.7% among women).
Conclusion: These findings effectively identify the most challenging clothing items for PwPD, emphasizing the impact of body self-perception and a possible gender predominance in experiencing dispreception phenomena. This international survey calls on the scientific community and the fashion industry to recognize and address the dressing and clothing challenges faced by PwPD, with the goal of improving everyday quality of life and reducing gender differences and disparities.
P17.07
1 Shirley Ryan AbilityLab, United States
2 Shirley Ryan AbilityLab; Northwestern University, Feinberg School of Medicine, United States
Background: Quality of life is central in Parkinson’s disease (PD) care and is often measured with self-reported questionnaires such as PDQ-39 and its short form, PDQ-8. While well established, PDQ-39 is lengthy and burdensome for clinical use, and PDQ-8 is less comprehensive than PDQoL7 in capturing the impact of both motor and non-motor symptoms. PDQoL7 is a recent alternative that has been validated in Greek but has not been evaluated in English. This study explores whether the English translation of PDQoL7 correlates with PDQ-39 and PDQ-8 to assess suitability for clinical use. Methods: A total of 116 participants with PD (age: 67.4±8.3 yrs; disease duration: 7.2±5.5 yrs; 48.3% female) completed PDQoL7 (7 items) and PDQ-39 (39 items, 8 domains) in English. For each measure, a summary index (SI) and subscores were computed, with PDQ-8 derived from one PDQ-39 item per domain. Item nonresponse was allowed, and no imputation was performed for missing scores. Spearman’s rank coefficients (ρ) were used to evaluate the correlations between (1) PDQ-39/8 indexes and PDQoL7 SI, (2) PDQ-39/8 subscores and PDQoL7 SI, and (3) PDQ-39/8 indexes and PDQoL7 subscores. Results: PDQoL7 SI was strongly correlated with both PDQ-39 SI (ρ=0.869, n=97, p<0.001) and PDQ-8 SI (ρ=0.856, n=113, p<0.001). Each PDQ-39 subscore (ρ=0.487-0.719, n≥110, p<0.001) and each PDQ-8 subscore (ρ=0.420-0.655, n≥115, p<0.001) showed moderate to strong correlations with PDQoL7 SI, with generally higher coefficients for PDQ-39 subscores. Each PDQoL7 subscore showed mostly strong correlations with PDQ-39 SI (ρ=0.601-0.704, n≥97, p<0.001) and PDQ-8 SI (ρ=0.607-0.706, n≥113, p<0.001), with the sleep subscore being the weakest for both (ρ=0.381 and 0.388, n=97 and 113, respectively, p<0.001). Discussion: Despite its brevity, PDQoL7 showed strong correspondence with established English quality of life measures, and its stronger alignment with PDQ-39 subscores than PDQ-8 suggests that it preserves a broader quality of life scope. Uniformly positive, mostly strong PDQoL7 subscore-to-index associations support translation adequacy. Weak sleep associations reflect gaps in PDQ-39 and PDQ-8, emphasizing PDQoL7’s added coverage of non-motor aspects. Given these findings, the English version of PDQoL7 offers a concise, clinically feasible tool that appears to be a valid measure of Parkinson’s quality of life, particularly for non-motor symptoms.
P17.08
1 Queen's University Belfast, United Kingdom
Background: Parkinson’s disease (PD) is a progressive neurological condition affecting over ten million people globally. Many individuals with PD reside in care homes where institutional routines and documentation shape daily experiences. This study used Institutional Ethnography (IE) to explore how residents with PD and staff in Northern Ireland understand and support “living well,” and how their experiences are organised through institutional practices and culture.
Methods: Guided by IE, the inquiry began from the standpoint of residents with PD and traced how everyday activities were coordinated by institutional relations. Data were generated through semi-structured interviews with residents (n=15) and four focus groups (n=8 per group) with nurses, care assistants, activity coordinators and managers. Field notes captured daily routines, staff–resident interactions, and the physical and social environment. Documentary audits of care plans, medication charts and policies examined how residents’ lives were represented textually. Interviews and focus groups were audio-recorded, transcribed and analysed thematically using Braun and Clarke’s reflexive approach, guided by IE principles to connect individual experiences with institutional processes. This study took place between January 2025-October 2025.
Results: Residents described living well as maintaining identity, humour and social connection within institutional constraints. Many experienced tension between safety and autonomy, where organisational priorities limited personal choice. Staff identified three main processes shaping care: navigating clinical and emotional complexity, creating moments of personhood through individualised interactions, and managing systemic constraints such as limited PD-specific training and fragmented multidisciplinary input. Care records and audits showed that documentation primarily reflected medical and functional perspectives, with limited attention to personal preferences or emotional wellbeing.
Conclusion: Institutional Ethnography demonstrated how organisational routines and documentation structure the experiences of residents with PD in care homes. Living well was supported through relational and person-centred practices but constrained by institutional priorities for safety and efficiency. Enhancing PD-specific education, reflective documentation and relational care can strengthen organisational capacity to support living well in long-term care.
P17.09
1 Veterans Administration- PADRECC, United States
2 Veteran, United States
3 Richmond VA PADRECC, United States
The motor symptoms of Parkinson’s disease (PD) and other movement disorders can impact balance, mobility, and fine motor skills which can lead to the loss of leisure activities. Mental health symptoms are widely reported in PD and can contribute to isolation, loneliness, and decline in quality of life. Additionally, Veterans face unique challenges with PD accompanied with post-traumatic stress disorder, mental health struggles and/or toxic exposures. Many Veterans in clinic were reporting loss of leisure activities, as they were no longer able to woodwork or tinker in their garage due to their PD. The Richmond Veteran’s Administration (VA) Parkinson’s Research Education and Clinical Center (PADRECC) piloted a virtual Lego group in Jan 2024 with 10 Veterans. Initial pilot survey results revealed that the group had positive benefits to quality of life. This group has continued, doubling in size and popularity. Sets are picked out or mailed, to be completed at home in their spare time. Virtual group sessions (every 3 weeks) serve as show-and-tell. An anonymous, virtual survey was sent out to current and former group members to assess preferred building sets, self-perceived benefits of group, and comment boxes to share what they love/dislike about group. Since starting the Lego group in 2024, there have been 34 virtual group sessions. Three off-site field trips, 3 on-site in-person group builds and 1 on-site group showcase was also organized. Since initiation, our Veterans have completed 311 sets. 11 Veterans completed the online survey. The types of sets most enjoyed were larger sets, technic sets, military sets and buildings/architectures sets. Slider bar questions asked which areas of their life were most affected since participating in this group. Highest rated responses to this included: mental health (85), overall happiness (82) and isolation/loneliness (81). 82% of them were interested in participating in future research. Written-in comments were overly positive with 10 out of 11 Veterans (91%) commenting on enjoying the social aspect of the group. There were no negative comments shared. This group was created with the intention of bringing fun and leisure back to Veterans, but has instead been transformative in creating community and belonging, impacting mental health and improving quality of life for these Veterans. Future direction will include expansion to other PADRECC sites, with Richmond members serving to help facilitate these groups.
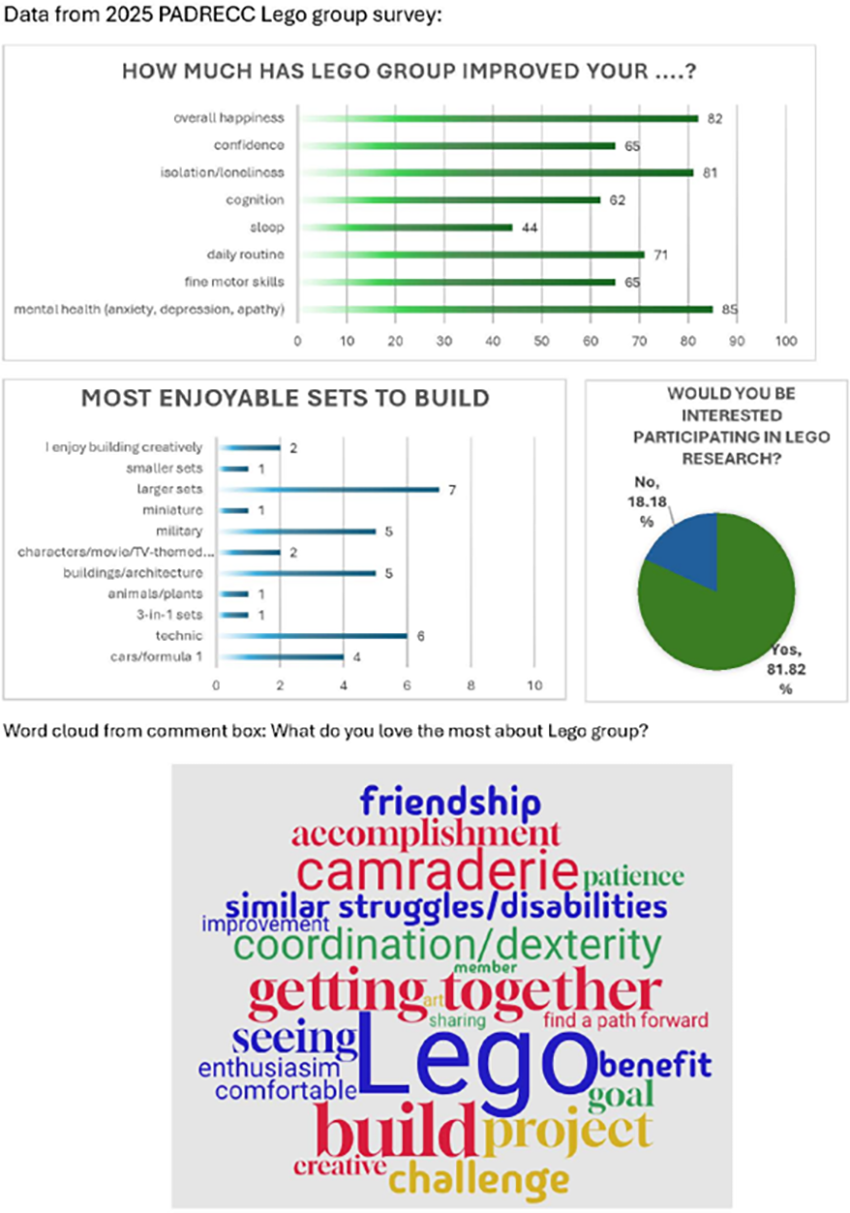
COMPREHENSIVE CARE: Shared Decision Making: PwP - Clinician partnership
P18.01
1 Retired Paediatric Pulmonologist and patient, steering committee member Oslo and Akershus Parkinson's Association., Norway
2 Professor of Paediatric Epidemiology, Institute of Social and Preventive Medicine (ISPM), University of Bern., Switzerland
3 Porfessor of Neurology and Neurogenetics, Haukeland University Hospital, Bergen., Norway
Background: Parkinson's disease (PD) is the fastest-growing neurodegenerative disorder. Norwegian prevalence data have confirmed increases in all age groups in both sexes, especially among the elderly. The number of people living with PD (PwPD) in Norway is expected to increase from the current estimate of 13 000 to 22 000 by 2050, further compromising access to diagnostic and treatment services provided by neurologists and to multidisciplinary assessment and follow-up, and rehabilitation. Norwegian 2024 registry data showed that 41% of PwPD were satisfied or very satisfied with their care. A recent survey conducted by the Norwegian Parkinson’s Association (NPA) revealed heterogeneity in how a PD diagnosis is delivered including by text message, letter, or scan report without the opportunity for the PwPD to ask questions or receive information about their diagnosis.
Aims: To identify, quantify and describe factors affecting the experience of getting a PD diagnosis from the point of symptom onset and of accessing multidisciplinary treatment. With this information, in conjunction with patients and healthcare professionals, we will document the patient journey with signposting as a tool to improve recognition of PD symptoms, provide information, improve the engagement of health professionals with PwPD and reduce patient anxiety.
Methods: This is a quantitative and qualitative study in the form of an anonymous questionnaire (REDCap platform) comprising 49 questions relating to current health status, symptoms prediagnosis, the diagnostic process and engagement with the health service postdiagnosis. Inclusion criteria: PwPD who are NPA members and have an email address. People without PD are excluded. Invitation to participate will be sent via email and PwPD or their caregivers can complete it online. Data will be stored in the Secure Access to Research Data and E-infrastructure system at Bergen University (UiB) and analysed using STATA. The decision to answer the questionnaire implies consent. UiB Ethics Committee approval 933568.
Results: The questionnaire was piloted on 11 PwPD and 1 carer and modified iteratively in 3 online meetings. The final version was approved by the steering committee and launched by NPA in October. Results will be available at the conference.
Conclusion: Given the projected increase in numbers of PwPD and the perceived service shortfalls, there is a need for a comprehensive map of the patient journey including patient defined outcomes.
P18.02
1 Parkinson's Centre for Integrated Therapy, School of Psychology, University of Kent, United Kingdom
Given the diverse nature of Parkinsonian symptoms, it is essential to adopt a patient-centred approach to ensure that clinical care reflects individual needs. However, many people with Parkinson’s (PwPs) and carers experience unmet needs and dissatisfaction with their clinical consultations due to short appointment times, long follow-up intervals, and a lack of holistic support. Furthermore, non-motor symptoms such as anxiety, depression, hallucinations, and impulse control disorders are often underreported in clinical consultations due to a lack of awareness, stigma, and communication difficulties.
The Patient Concerns Inventory (PCI) is a condition-specific prompt list originally developed for head and neck cancer to improve patient–clinician communication. Following its successful adaptation for several other conditions, the present study aimed to develop a Patient Concerns Inventory for Parkinson’s disease (PCI-PD) to help PwPs and carers communicate their concerns more effectively during consultations; this was carried out in three stages. The first stage involved a literature review of common concerns in PD, after which a draft PCI-PD was generated. This draft was then reviewed by multidisciplinary clinicians (N=11) working with PwPs. Two focus groups were then conducted with PwPs and carers (N=10; one in-person (n=5), one online (n=5)) to review the PCI-PD draft. The data received through the feedback was analysed using content analysis and thematic analysis, which identified themes relating to support during initial appointments, coping strategies, and suggestions to the PCI-PD. The PCI-PD includes 65 items grouped into six domains: physical functioning (e.g., tremor, balance), emotional and psychological wellbeing (e.g., anxiety, hallucinations), activities of daily living (e.g., dressing, eating), social care and wellbeing(e.g., avoiding going out), treatment-related queries (e.g., medication management), and signposting to multidisciplinary care. Thematic analysis generated three overarching themes- Coping with Parkinson’s disease, Navigating Appointments, and Support and Resources, along with subthemes that reflect distinct but interconnected elements within the participant’s experiences. This study highlights the potential of the PCI-PD to bridge the gap between patient and clinician priorities, empower PwPs and carers to voice their concerns, and facilitate more person-centred collaborative consultations.
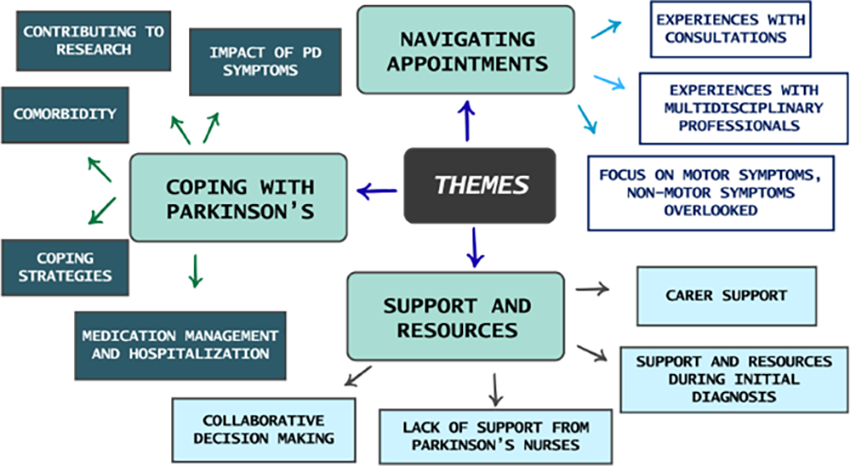
P18.03
1 Duke University School of Nursing, United States
Background Parkinson’s disease (PD) is a complex, progressive neurodegenerative disorder characterized by a wide range of motor and non-motor symptoms. As the disease advances, individuals often experience an increasing treatment burden and healthcare decisions that may not reflect their personal values and goals. While clinicians are proficient in evidence-based management of PD, there remains an opportunity in aligning care with what matters most to patients, especially with multimorbidity and functional or cognitive decline.
Conceptual Framework The Patient Priorities Care (PPC) approach offers a structured, person-centered framework designed to identify and act on patients’ health priorities. Originally developed for older adults with multiple chronic conditions, PPC emphasizes eliciting patients’ values, health outcome goals, and care preferences, and aligning clinical decisions accordingly. This approach shifts the focus from disease-specific guidelines to individualized care that supports what matters most to the patient.
This presentation will outline the PPC framework and demonstrate its application through clinical case examples.
Application to Parkinson’s Disease Integrating PPC into PD care involves clinical conversations to explore patients’ desired outcomes and acceptable trade-offs. For instance, a patient may prioritize maintaining independence over aggressive symptom control or prefer a simplified medication regimen to minimize side effects. PPC provides a structured method for these nuanced discussions and tailor care plans accordingly.
Goal-aligned care has the potential to reduce treatment burden, enhance patient and care partner satisfaction, and foster interprofessional collaboration by uniting the care team around clearly defined patient priorities.
Time constraints, limited clinician familiarity with the PPC process, and challenges in reconciling patient priorities with disease-based guidelines may slow down the use of PPC approach. However, through clinician training, team-based workflows, and documentation strategies we can integrate PPC into routine practice.
Conclusion The PPC approach offers a practical, scalable method to align PD care with what matters most to patients. By integrating this framework into clinical practice, clinicians can deliver more meaningful, goal-concordant care that honors the lived experience of individuals with Parkinson’s disease and their care partners.
P18.04
1 University of Bristol, United Kingdom
2 Parkinson's UK, United Kingdom
3 University of Aberdeen, United Kingdom
4 Caithness Support Group, Parkinson's UK, United Kingdom
5 North Bristol NHS Trust, United Kingdom
6 Fife Support Group, Parkinson's UK, United Kingdom
Parkinson’s is a highly variable condition with over 40 associated symptoms that may present in different combinations, at different points in the disease course, and may change at different rates. Historically, this variability has made it difficult to accurately predict how a person’s Parkinson’s will progress (i.e., to provide a prognosis). However, research data now allows us to identify groups of people with Parkinson’s (PwP) who are more or less likely to develop certain symptoms or outcomes. Prognostic models are also being refined which will be able to give more personalised prognoses. However our understanding of how and when such information should be used and the impact on PwP has not kept pace with these developments Giving people information about how their disease is likely to affect them in the future is an important part of patient-centred care and care planning, which support effective use of individuals’ and healthcare resources. However, we know that PwP, their supporters and clinicians often find it difficult to discuss prognoses and engage in shared decision making about care.
This research aims to explore the views of PwP, supporters and clinicians regarding impact and appropriate use of personalised prognostication. We will then develop a toolkit of resources for PwP, supporters and clinicians to support the appropriate use of personalised prognostic information and subsequent care planning.
Guided by Intervention Mapping and the Person-Based Approach to intervention development, we will conduct focus groups and interviews with PwP, supporters and clinicians to identify preferences, needs, barriers and enablers regarding prognostic information and care planning. The findings from this qualitative work will be used to set guiding principles for the development of resources to support prognostic discussions between PwP, supporters and clinicians. Resources will be iteratively refined using think aloud interviews with PwP, supporters and clinicians. The outcome will be a toolkit of resources ready for PwP, supporters and clinicians to use in practice.
PwP and supporters helped us design this research and will be involved throughout the project both as members of the project team and in Patient and Public Involvement meetings.
P18.05
1 Koios Care BV, Belgium
2 Koios Care, Belgium
3 The IMPACT research group, Department of Medicine, Huddinge, Karolinska Institute, Stockholm, Sweden, Sweden
4 MoVeRe group, GIGA-neuroscience, University of Liège, Belgium & Department of Neurology, CHU Liège, Belgium, Belgium
Objectives: Routine assessment of Parkinson’s disease symptom fluctuations between outpatient visits is limited by memory bias and failures in capturing objective daily variations in symptom severity and timing. In this work, as a proof of concept in one patient, we tested whether this unmet need could be adequately addressed by continuous passive digital recordings of real-world behaviors such as eating.
Methods: In a recent validation study, we used commercial smartwatches and smartphones to passively collect real-world data in 88 people with PD over a 20-week period. Outcome measures from AI-driven analyses showed high within-subject reliability (Intraclass Correlation Coefficient, ICC) and sensitivity to longitudinal change (Cohen’s d). In one of the participants, affected with significant dopa-induced motor fluctuations, we compared the time spent with bradykinesia 30 days before and 30 days after an outpatient visit with the treating neurologist who was presented with a visual summary of daily variations in motor symptoms obtained from the AI-driven system.
Results: Before the outpatient visit, the patient's data showed 3.03 hours of daily symptomatic time, primarily bradykinesia. A data-informed therapeutic adjustment resulted in a reduction of symptomatic time to 1.33 hours, resulting in a 57% decrease in detected bradykinesia. This was in good agreement with the patient's global clinical impression; a reduction of the UPDRS Part II score from five to two.
Conclusions: Objectively visualizing a 57% reduction in bradykinesia provides clear, data-driven proof of a treatment plan’s efficacy. Although preliminary, these results show the high potential of this approach in both clinical settings and research trials.
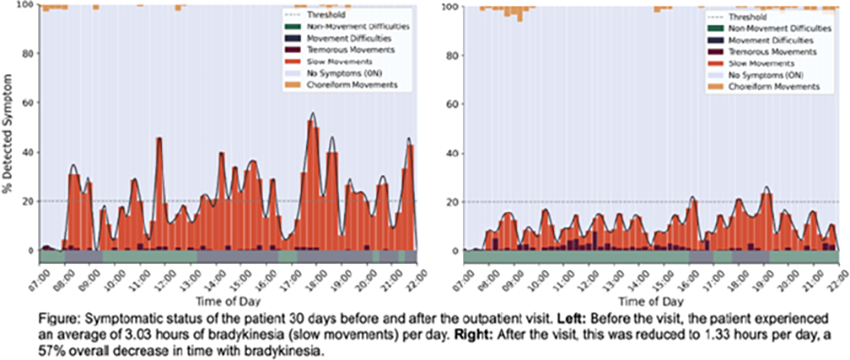
COMPREHENSIVE CARE: Palliative Care/ Advanced Planning/ End of Life Care
P19.01
1 1. France Développement Electronique (FDE), Monswiller, France - 2. CIC 1414, CHU de Rennes – Université de Rennes, Rennes, France, France
2 Association France Parkinson, France
Introduction EoL care for PD in France remains suboptimal. Building on the APO PALLIA and SPARK initiatives supported by FP, this work was informed by two complementary studies conducted in 2024: (i) a nationwide FP survey of healthcare professionals and care partners, which identified deficits in training, medication management and care coordination; (ii) research exploring patients’ perspectives on EoL needs. Concurrently, an initiative within a private nursing home group, LNA Santé, where facilities with PD expertise expressed specific needs for EoL support, underscored the pressing demand from frontline services.
Methods FP and SFAP convened a multidisciplinary working group comprising FP staff, palliative care specialists, neurologists, pharmacists, nurses, and nursing home representatives. A consensus-based, practice-oriented methodology was applied: (1) review of international literature; (2) integration of French survey findings and frontline feedback ; (3) iterative drafting with peer review; (4) feasibility assessments across hospitals, home care and nursing homes.
Results The guide was published in February 2025 and addresses key domains of PD EoL care, including safe medication management, PD-adapted pain assessment; red flags and terminal phase; oral adaptations and non-oral option; DBS management at EoL; advance care planning; nursing home specifics; and practical annexes. Beyond the guide, this project also created a new modus operandi for FP, developing a replicable model for co-producing field guides in collaboration with healthcare professionals. Early reception suggests strong uptake (5k print runs). SFAP ensured national dissemination by sending the digital guide to all palliative care units and mobile palliative care teams in France. A follow-up survey of early readers is currently underway to assess the guide’s perceived usefulness, its impact on professional practice, and remaining gaps.
Conclusion This first-of-its-kind, co-produced guide shows that addressing PD-specific EoL issues is feasible and valuable at national scale. Building on this method, FP is preparing a second version co-designed with patients and care partners, and a dedicated guide for nursing homes incorporating tailored recommendations. Next steps include releasing the guide under Creative Commons, expanding European collaboration, and direct involvement of patients in the review process.
P19.02
1 University of Bristol, United Kingdom
2 Parkinson’s UK, United Kingdom
3 University of Aberdeen, United Kingdom
4 Parkinson's UK, United Kingdom
5 Caithness Parkinson’s Support Group, United Kingdom
6 North Bristol NHS Trust, United Kingdom
7 Dundee Research Interest Group, United Kingdom
Introduction People with Parkinson’s (PWP) often report that their clinicians do not provide enough prognostic information, despite many PWP wanting and expecting this information from clinicians. For the majority of PWP, who would like more information about their prognosis than that provided by clinicians, the lack of clinician-provided information creates a gap which PWP may choose to fill with information sought through online resources.
We aimed to understand and describe how prognostic information is presented in publicly accessible online information resources relating to Parkinson’s, and to identify ways to support the development of appropriate person-centred prognostic resources.
Methods We conducted a qualitative document analysis of online resources collected through a series of keyword searches using the Google search engine conducted over a two-week period. We included documents which discussed prognostic information about Parkinson’s which appeared on the first page of each Google search. Data will be analysed using critical discourse analysis. We will draw on Susteric et al’s (2016) framework for evaluating information resources, and on features of prognosis described by Moons et al (2009) and Bloom et al (2022). PWP and supporters helped us design this research, including the selection of keywords, and will be involved throughout the project as members of the project team and in Patient and Public Involvement meetings.
Results 172 documents were returned, with 56 documents included for analysis after deduplication and screening. Documents included text-based webpages, AI overviews, podcasts, videos and academic articles.
Conclusions Through understanding the context of how prognosis for Parkinson’s is currently presented in available online resources, the findings of this research will be used to support the development of a toolkit of resources for PwP, supporters and clinicians to support the appropriate use of personalised prognostic information and subsequent care planning.
P19.03
1 HUS, Helsinki University Hospital, Neurocenter, Finland
Background The prevalence of Parkinsońs disease is increasing as the population ages. It is predicted that the number of device-assisted treatments will also increase. Currently there are two infusion treatment routes in use: One through the abdominal wall via a Peg/J tube and another subcutaneous infusion therapy, which has been introduced in Finland in 2024. Peg/J-tube problems caused congestion in the endoscopy and neurology units. Costs increased as both ward and an anesthesia team had to be reserved. Due to complications of subcutaneous infusion therapy (local skin infections and contact dermatitis), the neurology unit has received repeated patient contacts.
Material and method
The job description of a Movement Disorder Nurse (MDN) was created and three neuroscience nurses (NSN) were trained. The training included a lecture on the techniques, reviewing the reasons and clarifying possible contraindications. It also included practical training and demonstrating the changes to the doctor in the endoscopy unit. The MDN job description includes passive changes to the Peg/J inner tube and tubing connectors, also checking for possible problems with the infusion pump. This job description has evolved. New tasks include checking for possible skin problems, guiding patient´s and the unit’s staff after the start of treatment.
Conclusions In Finland, the role of NSN working in specialized care is to act as experts in their own field. The MDN job description is based on in-depth knowledge of their own field of specialization and individual training. MDN work is a task transfer from a physician to an NSN. Before MDN patients were contacted by the neurology unit, the doctor either made a referral to the endoscopy unit for the insertion of a new Peg/J-tube or the patient came to the unit for skin problems. Both neurology - and endoscopy units have benefited from the MDN procedure. Patients can access treatments more quickly and are spared from sedation, laboratory tests, and X-ray procedures. This brings cost savings to both units.
Advanced nursing in Parkinson Disease improves patient access to treatment, increases patient satisfaction and produces high-quality treatment outcomes. Patients have experienced an improved quality of life with the MDN procedure. Working independently and having expertise in neuroscience nursing increases MDN commitment and job satisfaction.
P19.04
1 Parkinson Patients Support Organization -EThiopia, Ethiopia
Objective: To evaluate the effectiveness of a home-based care program in improving the physical, functional, and emotional wellbeing of bedridden Parkinson's Disease (PD) patients.
Background: From November 2023 to September 2025, the Parkinson’s Patients Support Organization – Ethiopia (PPSO-E) delivered home-based care to 80 bedridden PD patients. Interventions included PD medication (levodopa-carbidopa), sanitary materials, assistive devices, speech/physiotherapy, and health education for patients and caregivers, aiming to enhance quality of life.
Methods: A pre-post mixed-methods cross-sectional study design was employed involving qualitative and quantitative data collection and analysis methods. Validated tools and locally adapted questionnaires was used to measure changes in the quality of life the PD patients. Quantitative data was analyzed descriptively using IBM SPSS v25 software and the qualitative data was analyzed using thematic analysis approach. Finally, triangulation by data sources and methods were used under predefined and emergent themes.
Results: Pre-intervention, only 34% met hygiene and wellbeing criteria, rising to 68% post-intervention (100% relative increase). Secondary infections fell from 54% to 28%. Functional independence improved from 42% to 61%. High symptom burden declined from 72% to 64.5%, with more predictable patterns aiding planning. Mobility issues decreased from 54% to 30.8% (69.2% improvement). Communication clarity rose from 47% to 56% through speech therapy. Depression and sleep disruptions dropped from 38% to 24%, boosting alertness and resilience.
Conclusions: The project significantly improved PD patients' quality of life by addressing symptoms through home-based medication, therapy, and education. Scaling this model could promote equitable neurological care across Ethiopia.
COMPREHENSIVE CARE: Health accessibility/ Underserved populations
P20.01
1 Central Michigan University, United States
2 Detroit Medical Center Rehabilitation Institute of Michigan, United States
3 Level Eleven Physical Therapy - A Rehab Without Walls Clinic, United States
Purpose: Successful management of Parkinson’s disease (PD) at the national level depends on reaching underserved rural populations. The Parkinson’s Report Card Program (PRCP) aimed to improve disease self-management through triannual symptom tracking, education, and follow-up support in three rural Michigan communities. Through interviews completed at the conclusion of the program, investigators hoped to explore the perceptions of people with Parkinson’s disease (PwPD) and their caregivers regarding the implementation of the PRCP in rural settings following completion of the program.
Methods: Twenty-eight individuals with PD completed outcome measures at three timepoints over one year, including balance, gait, strength, balance confidence, self-efficacy, and non-motor symptoms. Participants received individualized performance summaries (“report cards”) and targeted recommendations based on their results, followed by check-in phone calls between testing sessions. Semi-structured interviews were conducted at the program conclusion and qualitatively analyzed via inductive axial coding to identify perceptions of their experience and influence the program had on management of their PD. Caregivers, if present, were also invited to participate in the interviews along with PRCP participants.
Findings: Participants and caregivers perceived changes in self-efficacy and disease management confidence. Qualitative analysis revealed three major themes: (1) Benchmarking for Long-Term Consistency, (2) The Trustworthy Source: Importance of an Embedded Specialist, and (3) Accessing Specialized Care: A Balancing Act. Themes highlight barriers participants in rural communities face when managing PD, and the positive impact specialized disease management services can have on individuals, their family, and their community. Even in the absence of significant objective or perceived improvements in participant self-efficacy, across all three themes caregivers described how the PRCP provided support and improved their confidence in assisting or managing their loved one’s PD at times when they otherwise felt isolated.
Conclusions: The PRCP supported and empowered PwPD and their caregivers in rural areas, though systemic barriers to specialty care persist. Findings underscore the need for scalable, community-based interventions. Consistent feedback and trustworthy care relationships can enhance self-efficacy and engagement in chronic disease management for PwPD in rural communities.
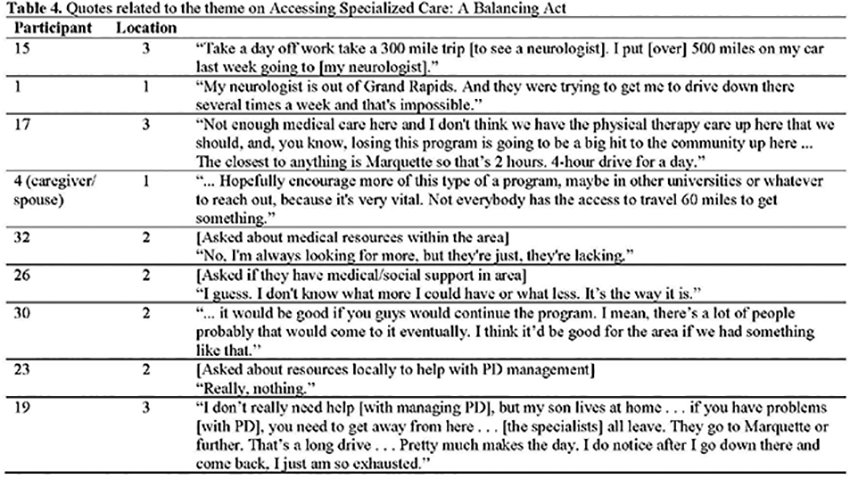
P20.02
1 Boston University School of Medicine, United States
2 Boston University Chobanian & Avedisian School of Medicine/ Boston Medical Center, United States
3 Boston University Chobanian & Avedisian School of Medicine, United States
BACKGROUND: Telehealth visits for Persons with Parkinson Disease (PwP)) have become a more accepted way of providing care that may otherwise not occur in the context of a patient’s increasing disability over time.
OBJECTIVE: To understand the characteristics of those using Telehealth (TH) vs In Person (IP) visits, and how it can improve access to essential care by movement disorder specialists. Additionally, to determine if Physical Therapy (PT) referrals were taking place at the same frequency at TH and IP visits. Given Telehealth challenges including user proficiency and limited neurologic examinations, we hypothesized there would be less referrals to PT at TH visits than at IP visits.
METHODS: Random sampling of PD outpatient visits from EPIC medical records, seen by movement disorders neurologists at Boston Medical Center in 2023, as approved by Boston University Medical Campus IRB. Analyzed with R 4.4.1 Studio and Python 3.11.
RESULTS: Reviewed 135 patients age 53 - 95 yrs, mean 73.7 yrs, Males 55.6%, Females 44.4%, White 70%, Hispanic/Latin 21%, Black 7%, Asian 2%. ANOVA and Chi Square tests revealed IP and TH visits did not significantly impact referrals to Physical Therapy. Variables of Sex, race, age, distance to site, disease duration, DBS, stage of PD, PT offered, and ongoing PT did not significantly impact PT referrals. This showed no clinician bias toward a particular group. Secondary analyses found it was more likely for someone to complete an IP visit when they were non-Caucasian of Hispanic/Latin ethnic origin. Caucasian English speakers were more likely to complete TH visits compared to other groups. Those living farther away and older tended to rely more on TH than IP visits.
CONCLUSION: While longer disease duration was associated with more TH visits, it was not statistically significant. This study provides an opportunity to better understand TH in care referrals to PT for PwP. This shows Telehealth is a viable option for those as they age, reside further from specialists, and seek to manage this progressive neurodegenerative condition. This study highlights how certain groups adapted to using telehealth, while also demonstrating how telehealth can provide better access to important care and specialists when distance and advanced disease state create bigger barriers over the course of PD.
P20.03
1 Groupement Hospitalier Eaubonne Montmorency, France
In France, when it comes to setting up continuous subcutaneous devices, the neurologist manages the prescription, but the nurse plays a key role in coordinating and implementing the treatment.
For two decades, apomorphine has been an alternative treatment for patients with Parkinson's disease, positioned in the therapeutic regimen for people who have had the disease for some time and whose treatment progression is described as advanced. Belonging to the family of dopamine agonists, its side effects and implementation have long been the subject of expertise in specialized centers. It was not until the Covid period that the development and deployment of this therapy accelerated. A private healthcare offering called “healthcare provider” developed around it.
It was not until 2024 that a new subcutaneous therapy appeared, challenging the established order of this mode of therapeutic administration: subcutaneous foslevodopa/cardidopa has many theoretical advantages, being related to the L-DOPA family, which is thought to have fewer side effects than dopamine agonists.
To understand the impact of the arrival of this therapy, a questionnaire was distributed to gauge the feelings and perceptions of the nurses who manage the coordination and implementation of these two treatments.
Following this distribution, twenty-one nurses answered twelve questions comparing apomorphine and foslevodopa-carbidopa in terms of the mode of administration (outpatient, full hospitalization, weekday hospitalization, day hospital), three items (logistics, availability, support), a summary description (defects and qualities), as well as a projection of the ideal method of administration, a perception of subcutaneous treatments as a whole, and a rating of the quality of support for a subcutaneous device.
The results show:
An overall rating difference of 1.53/5 in favor of apomorphine The home is the best place to initiate subcutaneous treatment Nurses believe they are better supported when patients are using subcutaneous devices A rating of 7/10 for the quality of support
P20.04
1 Queen Mary University of London, United Kingdom
Background The East London Parkinson Disease (ELPD) project investigates the symptoms, manifestations, and determinants of Parkinson’s disease (PD) among people from diverse ethnic backgrounds. Launched in 2019, the project aims to understand how PD is experienced by diverse communities to address health inequalities. Patient and Public Involvement and Engagement (PPIE) is important to ensure research is relevant and meaningful to those affected by PD. However, implementing PPIE effectively and ensuring that involvement is impactful can be challenging.
Objective To describe our approach to embedding PPIE within ELPD and share practical learnings.
Methods A key PPIE contributor was recruited to join the study team and shape decision-making throughout the research process. Over 75 people with PD and care partners have contributed through our PPIE working group, providing input on study design, prioritising research questions, reviewing participant-facing materials, interpreting study results, and guiding dissemination strategies. Activities and impacts are regularly logged to reflect on learnings, outcomes, and impacts.
Results Cultural inclusivity and accessibility were central to successful PPIE. This included translating study materials and PPIE newsletters into English and Bengali, having bilingual researchers available to PPIE members, and ensuring cultural sensitivity at events (e.g., providing space for prayer, considering dietary needs). Practical measures, such as hosting events in accessible community venues and reimbursing travel expenses facilitated engagement. Recognising and communicating how PPIE had informed the research process through timely updates and sharing concrete examples (e.g., versions of materials pre-post feedback) helped maintain engagement. Interactive activities that created opportunities to connect with others affected by PD and engage in two-way dialogues with researchers were valued. Embedding robust and meaningful involvement required significant time and resources.
Conclusions We show how we tailored our PPIE approach to meet the needs of diverse communities affected by PD. PPIE input helped identify and address barriers to participation in ELPD and enhanced the relevance of our research. These insights can now inform future PD research aiming to promote inclusion and engagement of underrepresented groups.
P20.05
1 CND Life Sciences, United States
2 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
3 Norton Neuroscience Institute, Louisville, KY, United States
Introduction: Skin biopsy detection of P-SYN is a recent addition to the diagnostic pathway in patients with suspected neurodegenerative synucleinopathies. However, the economic impact of skin biopsy detection of P-SYN in clinical care has not been fully elucidated. The primary objective of this study was to evaluate the health economic impact of skin biopsy detection of phosphorylated alpha-synuclein (P-SYN) in patients with suspected synucleinopathies.
Methods: A retrospective review was done on the costs associated with clinical care in 100 patients with suspected synucleinopathy in a private practice that completed cutaneous P-SYN testing between January 2022 and December 2024. Records were reviewed to determine the number of neurologic diagnostic procedures, tests, treatments, and referrals before and after P-SYN testing to determine the costs of care. Average costs in Louisville, KY, were used to determine the total financial burden. The final estimated costs were normalized on an annual basis (at current pricing) to account for differences in duration of treatment and follow-up.
Results: 50 males and 50 females (73±8 years) were included in this study. Length of evaluation before P-SYN testing was 26.1±10.3 months, and length of follow-up after P-SYN testing was 14.6±6.8 months. A total of 599 tests were ordered for the cohort, with 69% (413/599) ordered before the Syn-One test. Significant annual reductions in all test categories were noted after Syn-One testing (P<0.01, all groups). 89 MRIs and 20 DaTscans were ordered before P-SYN testing; 23 MRIs and 6 DaTscans were ordered after. Neurological health care costs for the cohort was $587,000 annually. The cohort spent $172,000 more before the cutaneous P-SYN testing. Healthcare expenditure after cutaneous P-SYN testing decreased by $100,521 annually. At a practice level, 135 DaTScans were ordered annually before the introduction of P-SYN testing, and 33 DaTScan’s were ordered annually after the introduction of P-SYN testing.
Conclusions: The economic burden for suspected synucleinopathies for neurological care is significantly reduced after cutaneous P-SYN testing. Reductions in neuroimaging, laboratory studies, and physician referrals drove cost savings.
P20.06
1 University Medical Center Göttingen, Department of General Practice and Family Medicine, Humboldtallee 38, 37073 Göttingen, Germany
2 University of Applied Sciences and Arts Hildesheim/Holzminden/Göttingen, Faculty of Social Work and Health, Goschentor 1, 31134 Hildesheim, Germany
3 University of Applied Sciences and Arts Hildesheim/Holzminden/Göttingen, Faculty of Engineering and Health, Health Campus Göttingen, Annastraße 25, 37075 Göttingen, Germany
Introduction: Most of Germany’s regional Parkinson networks (PN) emerged through individual initiatives without systematic consideration of stakeholder perspectives. To incorporate perspectives of patients with Parkinson's disease (PwPD), their relatives, and health workers into a PN concept, the project "ParkNetz" (Sector-independent networking in healthcare for people with Parkinson's disease in Southern Lower Saxony) comprises subprojects with a participatory approach and a comprehensive survey with health workers.
Objective: The survey aims to capture health workers' views on regional care and support for PwPD, their relatives and their PN-related needs, to inform the ongoing co-creation-based PN development.
Method: From April to June 2025, an anonymous cross-sectional paper-pencil survey was distributed to 1,801 health workers in outpatient (n=1,717) and inpatient (n=84) settings, including professionals from medicine, therapy, psychosocial care, nursing, medical supply stores, and pharmacies. Quality and accessibility of healthcare services for PwPD, waiting time, information exchange with other professionals and importance of various PN services for PwPD and health workers as well as tasks related to research and structures of the health system, were rated on 5-point scales. Data were analyzed exploratorily in R.
Results: The response rate was 14% (29.37% male, 68.25% female). Healthcare quality (M=3.02, SD=0.85) and accessibility (M=2.66, SD=0.85) for PwPD were rated low, with even lower ratings for psychotherapy access (M=2.43, SD=1.12) and corresponding waiting time (M=2.18, SD=0.98). Information about PwPD from other workers was seldom received (M=2.51, SD=1.02). 81.59% did not include technology-based services (e.g., wearables) for treatment of PwPD. Regarding a future PN, highest ratings were given to services directed at PwPD and their relatives: a database with easy-to-understand information on Parkinson's disease/healthcare (M=4.36, SD=0.79), followed by psychosocial support services (M=4.35, SD=0.66) and an overview of Parkinson's experts in the region and their services (M=4.31, SD=0.80).
Conclusion: Findings reveal typical challenges in fragmented healthcare systems and emphasize the importance to focus on the needs of PwPD and their relatives when refining the regional PN in Southern Lower Saxony, extending beyond the conventional focus on interprofessional coordination.
P20.07
1 American Parkinson's Disease Association, United States
Background: Mandarin-speaking families affected by Parkinson’s disease (PD) often face barriers to care and reliable information. Limited English proficiency can make it difficult to understand diagnoses, treatment options, and medical terminology. Families may struggle to navigate the U.S. healthcare system. Caregiver strain, low digital literacy, and social isolation further compound these challenges. Culturally responsive resources and partnerships can help these families navigate PD.
Objective: To describe APDA’s engagement with Mandarin-speaking communities and share lessons from outreach efforts combining translated resources, community partnerships, and qualitative research to inform future culturally tailored programs.
Methods: Beginning in 2022, APDA addressed language and cultural barriers through the translation of materials - The Parkinson’s Disease Handbook and Be Active & Beyond: A Guide to Exercise and Wellness, into Simplified Chinese. Since 2023, APDA has partnered with Chinese community organizations in California and New York to deliver Mandarin PD education sessions and to create additional Simplified Chinese resources, including factsheets on constipation, fatigue, and nutrition, and a children’s storybook, Something’s Different About Grandpa. Mandarin-language videos on PD basics and APDA-funded research were produced, along with in-person and virtual Dance for PD and Connecting Through Art classes. APDA also collaborated with ThinkNow Research to conduct eight patient interviews and two caregiver focus groups, and expanded the National Financial Hardship Fund to accept Simplified Chinese applications.
Results: Mandarin videos received over 800 views in FY24, and translated materials were downloaded 400 times and ordered 1,100 hard copies. Focus-group participants often misinterpreted early PD symptoms as normal aging, relied heavily on Chinese-language social platforms, and reported stigma that discouraged disclosure. Caregivers valued visual, narrative-based materials but requested stage-specific, mobile-friendly tools and a Mandarin hotline for real-time support.
Conclusion: Effective outreach to Mandarin-speaking families requires more than translation—it demands cultural adaptation, attention to caregiver roles, respect for traditional health beliefs, and use of preferred communication platforms. These lessons can guide future PD outreach strategies to ensure equitable access to care and support across language and cultural boundaries.
P20.08
1 American Parkinson's Disease Association, United States
Background: The American Parkinson Disease Association (APDA) identified two major gaps in Parkinson’s disease (PD) research and developed funding mechanisms to address them: (1) the psychosocial challenges that shape daily life with PD, such as caregiver burden, stigma, and mental health, and (2) the need to understand PD in communities traditionally excluded from research (Gilbert & Standaert, 2020).
Objective: To highlight APDA’s efforts to address these research gaps through two complementary grant programs: the Social Science Research Grant and the Diversity in Parkinson’s Disease Research Grant.
Methods: The Social Science Research Grant, launched in 2024, supports areas of study include coping mechanisms, resilience, and emotional well-being, as well as the influence of stigma, family dynamics, and caregiver stress. Projects may evaluate interventions, programs, or community resources that improve quality of life for people with PD and caregivers.
The Diversity in Parkinson’s Disease Research Grant, inaugurated in 2021, funds work aimed at reducing inequities in diagnosis, care quality, and research participation among underrepresented populations. Since its launch, the program has supported projects such as investigating barriers to deep brain stimulation among minoritized populations, characterizing PD in African American and Latino communities to understand diagnostic and treatment disparities, improving access to advance-care planning for Hispanic patients, examining gender differences in shared decision-making, and developing machine-learning models to predict dyskinesia risk in diverse populations.
Results: The Social Science Research Grant was awarded for the first time in 2025, funding research on recreational therapy as a fall-prevention strategy in small-city communities. Since 2021, nine Diversity in PD Research Grants have been awarded, supporting ten investigators, generating eight peer-reviewed publications, and producing 158 citations to date (Oct, 25). A virtual Diversity in PD Research Roundtable held in November 2023 showcased grantee findings and fostered cross-collaboration.
Conclusion: Together, these initiatives expand the PD research landscape beyond the biomedical domain. By advancing psychosocial inquiry and promoting inclusion of historically underrepresented groups, APDA’s grant programs build a more complete understanding of Parkinson’s disease and how best to support every community affected by it.
P20.09
1 Indiana University School of Medicine, United States
2 Parkinson's Foundation, United States
3 Genomic Medicine Institute, United States
To describe the creation, implementation, and outcomes of a structured genetic counseling training initiative designed for providers within the Latin American Research Consortium on the GEnetics of Parkinson’s Disease (LARGE-PD), aimed at preparing them to deliver genetic results as part of the PD GENEration (PDGENE) study.
In 2019, PDGENE started providing CLIA-certified genetic testing and counseling free of charge to individuals diagnosed with Parkinson’s disease (PD). In 2024, a strategic partnership with LARGE-PD was established to increase Hispanic/Latino participation in PD genetic research. Since the return of results in PDGENE is conducted through formal genetic counseling sessions, a tailored training framework was designed to equip LARGE-PD providers with the competencies necessary to perform this role effectively.
Six asynchronous training modules were developed, encompassing foundational genetics, Parkinson’s disease genetics, genetic counseling principles, and result interpretation. To inform this training, a needs-based assessment (NBA) was distributed to LARGE-PD providers to identify knowledge gaps and prioritize additional content. In addition, the NBA guided the development of supplementary modules focused on pre-test counseling and additional findings.
The study-specific certification training program was made available to all LARGE-PD members, and so far two training cycles have been completed. In the initial training cycle, 33 providers expressed interest, 26 completed the training, and 16 achieved certification. The second cycle yielded similar outcomes, 34 providers expressed interest, 26 completed the training, and 16 were certified. Overall, 32 providers across 13 participating countries have been certified, ensuring that every LARGE-PD site has at least one trained provider capable of delivering results through a formal genetic counseling session. To date, 899 participant results are available, with 351 genetic counseling sessions successfully completed.
Since the expansion into Latin America, the PDGENE–LARGE-PD collaboration has implemented and refined a study-specific training framework to support genetic counseling capacity. This model demonstrates the feasibility of building local expertise to support the return of genetic results in regions where specialized training and resources are limited, contributing to greater equity, access, and representation in PD genetic research.
P20.10
1 University of São Paulo, Department of Neurology, Movement Disorders Center, São Paulo, Brazil, Brazil
2 Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Neurology, Centre of Expertise for Parkinson & Movement Disorders, Nijmegen, the Netherlands, Netherlands
Introduction: Walking difficulties are common in people with Parkinson’s Disease (PD). Compensation strategies are a key element of gait rehabilitation, ideally requiring involvement of specialized therapists. However, access to healthcare is not universally guaranteed, and a lack of equitable access poses a significant challenge in providing optimal care for vulnerable populations. Here, we aimed to explore the safety and efficacy of using an online platform dedicated to compensation strategies for gait impairment to support rehabilitation in persons with PD living in rural areas, where access to healthcare services is scarce.
Methods: In this prospective cohort study, we evaluated the safety and efficacy of an online platform to deliver compensation strategies for gait in 25 underserved individuals with idiopathic PD in rural Brazil, who had never received physical therapy to improve their gait. Those who lacked internet access and those with cognitive impairment were excluded. This platform contains background information about gait impairment in PD in plain language and focuses on the framework of seven distinct categories of 59 compensation strategies to overcome these gait impairments. Participants were instructed to test the different compensation strategies they came across for a period of three-weeks in their own home environment. To assess the impact of using the online platform, a pre- and post-intervention at-home assessment was performed by a trained research assistant.
Results: After three weeks of use, the primary outcome, the median patient-reported impact of gait impairment on daily activities[rated on a visual analog scale, 0–10], decreased from 7 to 4 (p<0.001). Among the 18 participants with FOG, the secondary outcome, self-reported impact of freezing episodes, also significantly decreased following the intervention (from 6 to 3, p=0.022). No falls or other adverse events were reported during the study period.
Conclusion: This open-label, uncontrolled study suggests that the platform is a safe and possibly effective tool for supporting gait rehabilitation in underserved communities with limited access to healthcare services. The efficacy and long-term effects require further evaluation in controlled studies. A continued global effort is warranted to provide innovative solutions to ameliorate access to healthcare services in vulnerable PD communities and to facilitate optimal care for every person living with PD worldwide.
P20.11
1 Davis Phinney Foundation, United States
2 Parkinson's Foundation, United States
3 Parkinson's and Movement Disorders Alliance, United States
4 LARGE PD, United States
5 Muhammad Ali Parkinson Center, United States
6 Michael J Fox Foundation, United States
7 Power for Parkinson's, United States
8 American Parkinson's Disease Association, United States
9 Fundación Degén, Spain
10 Promotores Embajadores de Parkinson, United States
Objective: To maximize resources and improve the experience of Spanish-speaking individuals and families affected by Parkinson’s through collaboration, awareness building, and knowledge sharing among organizations serving the Hispanic community.
Background: Before 2023, Parkinson’s organizations offering Spanish-language educational materials and programs often worked in isolation, resulting in overlapping events, duplicated resources, and missed opportunities for joint impact. The COVID-19 pandemic dramatically expanded digital engagement among Hispanic Parkinson’s communities, connecting individuals across the U.S., Latin America, and Spain and creating new potential—and need—for organizational collaboration.
Methods: The Davis Phinney Foundation launched HOPE PALS (Hispanic Organizational Partners Engaged in Parkinson’s Awareness and Leadership Solutions) to unite leaders from national and international Parkinson’s organizations. Beginning in early 2023, monthly virtual meetings and a shared calendar were established to share events, improve communication and foster partnerships. Coalition members include the American Parkinson’s Disease Association, Davis Phinney Foundation, LARGE-PD, The Michael J. Fox Foundation, Muhammad Ali Parkinson Center, Parkinson’s Foundation, PMD Alliance, Promotores Embajadores de Parkinson and Power for Parkinson’s, later joined by the Federación Española de Parkinson and Fundación Degén in Spain.
Results: Through regular monthly meetings, organizations have reduced scheduling conflicts, expanded cross-promotion of resources, and inspired new collaborative projects—like Parkinson Positivos, an illustrated educational book created through a partnership among the American Parkinson’s Disease Association, Columbia University, and the Davis Phinney Foundation (DPF). Twice-yearly (April and September), the DPF’s Espacio Parkinson webinar invites coalition members to showcase materials and events, strengthening visibility and access for the Spanish-speaking Parkinson’s community.
Conclusion: HOPE PALS demonstrates the power of cross-organizational collaboration to amplify education and support for underserved Parkinson’s communities. By leveraging digital connections and shared leadership, this coalition has elevated collective impact, enhanced community trust, and expanded culturally relevant resources for the international Spanish-speaking Parkinson’s community.
P20.12
1 Bastyr University, United States
2 Parkinson Center for Pragmatic Research, Colombia
3 Parkinson Center for Pragmatic Research, Poland
Financial well-being is an under-explored determinant of health in Parkinson’s disease (PD). This study examined the associations between financial status, financial behaviors, and health outcomes using patient-reported data from Modifiable Variables in Parkinsonism study. 1,509 individuals with PD completed survey questions related to financial health, symptom severity, and quality of life. Higher income consistently predicted better outcomes across all domains: lower baseline PRO-PD scores (p < 0.001), higher PROMIS physical (β = 0.22, p < 0.001) and mental (β = 0.42, p < 0.001) scores, and higher satisfaction. Individuals with greater income and credit scores exhibited lower PRO-PD symptom severity, and difficulties affording food predicted higher severity across nearly all symptoms. In contrast, having a financial plan or spending less were paradoxically associated with lower mental health scores, suggesting that declining health or caregiver involvement may prompt financial conservatism. Financial health and behaviors are strongly linked to physical, mental, and functional well-being in PD. Income and credit stability appear protective, while food insecurity is associated with greater symptom burden. Financial planning behaviors may also reflect compensatory responses to deteriorating health. Integrating financial assessments and support into PD care and research could illuminate socioeconomic contributors to disease progression and improve quality of life outcomes.
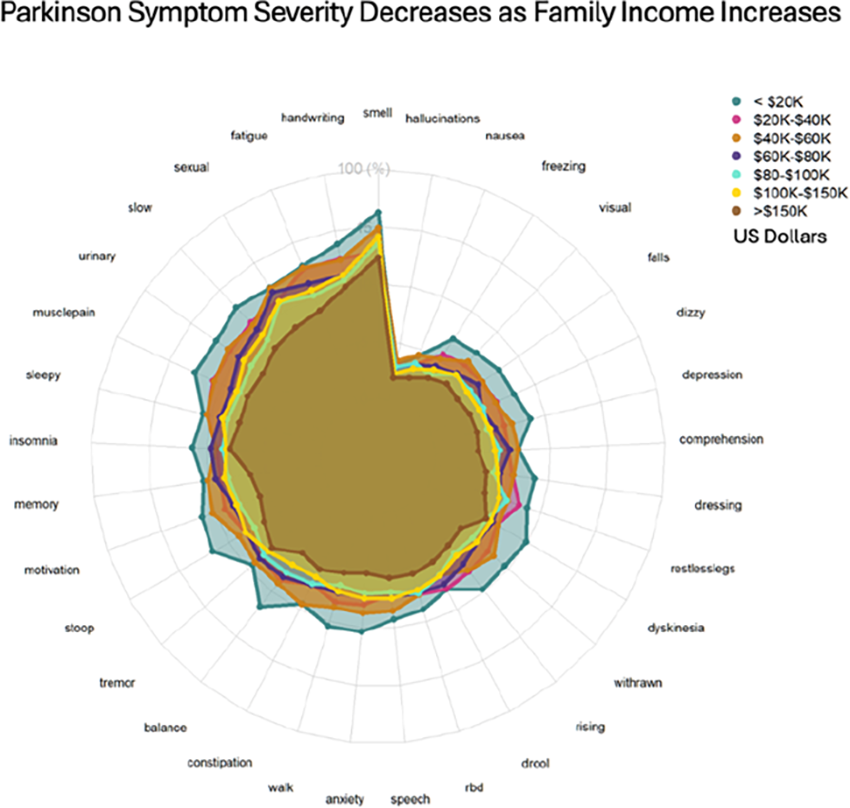
COMPREHENSIVE CARE: Sexuality & Intimacy
P21.01
1 Eastern Health, Australia
2 Melbourne University, Australia
3 Monash University, Australia
Background: There are changes in sexual function, intimacy and relationships after a diagnosis with Parkinson’s Disease (PD). Intimacy and sexual expression are critical for healthy relationships and contribute to quality of life.
Aims: To explore the beliefs and attitudes of individuals with Parkinson’s Disease (PD) and partners regarding discussions about sexual function, intimacy and relationships. Secondary objectives include exploring opinions on existing consumer handouts available.
Methods: Semi-structured interviews of both people with PD and partners of someone with PD (non-dyadic) were completed. Data from the semi-structured interviews underwent inductive thematic analysis.
Results: 20 participants (10 PD, 10 partners) were interviewed. Average age was 67 years and mean interview length was 38 minutes. Main themes identified were: 1) Sexual dysfunction is diverse in presentation and its impact on relationships. 2) Grief and loss are experienced as an individual and within the couple unit. 3) Role changes in the couple unit resulted in a fluid state between acceptance and resentment. 4) Adaptation to these changes was impacted by the strength of the pre-existing relationship between partners. 5) Health systems are blind to the couple as treating health professionals do not initiate conversations on these topics. No participants had seen online or written content, and when shown found them unsatisfactory.
Conclusion: People with PD (and partners) identify changes in many aspects of their sexual function, intimacy and relationships and want to talk about these topics with their treating health professionals but felt a lack in opportunity or confidence. Participants were unaware and unsatisfied with resources available.
P21.02
1 American Parkinson's Disease Association, United States
Background: Living with Parkinson’s disease (PD) can place both physical and emotional strain on couples. Symptoms such as tremors, stiffness, fatigue, and mood changes may make intimacy more challenging, and these concerns are often overlooked in medical visits. Yet, closeness and connection remain essential to maintaining quality of life and emotional well-being.
Objective: To describe the creation and early evaluation of ParkinSex, an intimacy guide and kit developed by the American Parkinson Disease Association (APDA) in collaboration with Havas Lynx New York, with input from the PD community and a clinical sexologist. The resource was designed to help people with PD and their partners enhance intimacy and communication. A survey was implemented to gather user feedback and insight.
Methods: Each kit contains an illustrated booklet explaining how PD can affect intimacy, with practical tips for physical and emotional connection. The kit also includes a feather, massage oil, scented candle, touch stones, blindfold, and bath bomb, each paired with suggestions for use. The booklet is available for download and as a narrated video. To assess the impact, APDA launched a survey asking users what was helpful, what was not, and how the resource could be improved.
Results: During the 2023 soft launch, all available kits were claimed within 24 hours. To date, ParkinSex has been distributed to more than 780 kits to individuals and couples, with thousands of online views and downloads, demonstrating strong demand for resources addressing intimacy in PD. Preliminary feedback reflects appreciation for its candid yet supportive tone. Users reported that the kit “opened a door for conversations we were avoiding” and that “it made something awkward feel hopeful again.” Full survey data are being collected through March 2026. The program has received widespread recognition, earning three MM+M Awards (Titanium “Best in Show,” Gold for Best Use of Customer Experience, and Gold for Best Use of Film or Video) and two Reggie Awards (Gold for Multicultural or Lifestyle Segment Marketing and Bronze for Purpose, Cause, or Charity Marketing).
Conclusion: ParkinSex represents a critical step toward breaking the silence around intimacy and PD. By combining education, creativity, and empathy, it provides couples with a supportive, evidence-informed guide to reconnect physically and emotionally reminding the community that intimacy is central to a full and meaningful life.
P21.03
1 University of Sao Paulo, Brazil
2 Universidade de São Paulo, Brazil
Introduction: Sexual health impairment is a frequent and neglected non-motor symptom of Parkinson’s disease (PD), particularly in women, leading to reduced quality of life, emotional distress, and relationship dissatisfaction. This multifactorial condition involves complex interactions between biological, motor, and psychosocial factors. Despite its relevance, there is a lack of structured interventions with standardized content, fidelity, and outcome assessment specifically targeting sexual health in women with PD. Remote synchronous interventions hold great potential to expand access to specialized care, minimize mobility and geographic barriers, and preserve privacy in this sensitive domain, thus supporting equity in health access and clinical implementation. Objective: To investigate the effects of a remote multidimensional intervention on the sexual health of women with PD. Methods: A randomized, parallel-group, assessor-blinded clinical trial will be conducted with 72 women diagnosed with idiopathic PD, Hoehn & Yahr stages I–III, aged 21–75 years, heterosexual, with a stable sexual partner, and internet access. Exclusion criteria include other neurological diseases, dementia, major depression, uncorrected sensory deficits, or recent pelvic surgery. Participants will be randomized (1:1) to intervention or control groups. The intervention group will receive 12 weekly synchronous sessions (3 months), including psychosocial activities (20 min), motor exercises (20 min), pelvic floor muscle training (15 min), and closing guidance (5 min). The control group will attend one 60-minute remote lecture about factors affecting sexual health in PD and receive a digital booklet. Assessments will occur at baseline, seven days, and 35 days post-intervention by blinded evaluators. The primary outcome will be the Female Sexual Function Index (FSFI). Secondary outcomes include self-esteem (Rosenberg Self-Esteem Scale), depressive symptoms (Beck Depression Inventory), and relationship quality (Dyadic Adjustment Scale). Expected Results: The multidimensional intervention is expected to result in greater improvements in sexual function, self-esteem, mood, and dyadic adjustment compared to the control condition, contributing to scalable, evidence-based strategies for women with PD. Funding: FAPESP #2013/07699-0, #2025/14403-7, #2025/02885-7. Ethics approval: CAAE 92292725.0.0000.0378.
P21.04
1 University of Sao Paulo, Brazil
2 Universidade de São Paulo, Brazil
Background: Sexual dysfunction is frequent in Parkinson’s disease (PD) and negatively affects quality of life, self-esteem, and couple relationships. Its multifactorial nature—combining motor, non-motor, and psychosocial factors—suggests that men and women may experience distinct determinants of sexual health. Understanding these differences is essential for developing individualized, interdisciplinary rehabilitation strategies. Objective: To identify and compare the factors that most strongly influence sexual health in men and women with PD. Methods: A cross-sectional study included 180 participants (100 women, mean age 54.4 ± 8.3; 80 men, 53.5 ± 10.8) in Hoehn and Yahr stages 1–3, all reporting an active sexual life in the past six months. Assessments comprised demographic and clinical data, cognition (MoCA), fatigue, depressive symptoms, sleep quality, self-esteem, relationship quality (CRQ), and motor/non-motor experiences (MDS-UPDRS I & II). Sexual health was assessed using the Female Sexual Function Index (FSFI) and the International Index of Erectile Function (IIEF). Separate multiple regression models were conducted for men and women including variables with moderate correlations (r > 0.30) with FSFI or IIEF total scores. Results: Distinct predictors emerged between sexes. In women, relationship and sleep quality were the strongest predictors of sexual function (adjusted R2 = 0.36, F (3,80) = 16.57, p < 0.000001), emphasizing psychosocial and sleep-related mechanisms. In men, motor disability alone predicted sexual health (adjusted R2 = 0.36, F (1,78) = 44.67, p < 0.00001), highlighting the physical component of sexual performance. Age, disease duration, and medication dose were not significant in either group. Conclusion: Sexual health in PD is shaped by distinct gender-specific mechanisms. While men’s function is primarily linked to motor impairment, women’s sexual well-being depends more on relational and sleep-related factors. These findings underscore the need for early, interdisciplinary, and gender-sensitive rehabilitation approaches integrating physiotherapy, psychology, and sexual counseling to promote holistic care and improve quality of life in PD. Funding:FAPESP #2013/07699-0, #2025/14403-7, and #2025/02885-7. Ethics approval: CAAE 39971420.0.0000.0003.
P21.05
1 Bastyr University, United States
Sexual health is an essential component of overall well-being and quality of life, yet little research on the topic exists in individuals with Parkinson’s disease (PD). The nuances of what contributes to sexual interest has received little interest to date. The goal of this study was to describe the relationship between PD symptoms and sexual interest in men and women with PD. The PROMIS Sexual Health Scale (SexFS) was added to the ongoing internet-based natural history study, Modifiable Variables in Parkinsonism (MVP) Study, in 2023. Descriptive statistics were used to explore the relationships between symptoms and sexual interest. The PROMIS Sexual Health Scale (SexFS) was used to evaluate sexual health and the Patient-Reported Outcomes in PD (PRO-PD) was used to describe symptom severity. PD symptom severity was compared to responses on the SexFS questionnaire regarding sexual interest to identify symptoms most strongly associated with interest in sex. Among the 844 individuals with self-reported PD that completed the scales, reduced sexual interest was linked to several non-motor symptoms. Women reported their level of sexual interest “not at all” more frequently than men (32.82% vs 9.06%, respectively.) In women, total PRO-PD scores were associated with overall sexual interest (p=0.0353), and loss of desire was particularly associated with daytime sleepiness, fatigue, walking difficulties, withdrawn, apathy, depression, loss of motivation. Men’s overall sexual health was most severely impacted by erectile dysfunction and recent satisfying experiences, whereas interest and desire were leading drivers in women’s sexual health. These findings suggest that PD symptoms affect sexual interest in both men and women, with men experiencing a broader range of symptoms influencing their sexual interest, while women are affected by a more limited set of symptoms. Clinically, this underscores the importance of considering both motor and non-motor symptoms when addressing reduced sexual interest in individuals with PD. This is a large dataset using validated outcome measures. The survey-based nature of the study does not allow for any objective verification of PD status, and the cross-sectional design does not allow any inference into causation. Future research should focus on developing targeted, gender-specific interventions aimed at improving sexual health and quality of life for patients with PD.

COMPREHENSIVE CARE: Daily life activities including working & driving
P22.01
1 Teachers College, Columbia University, United States
BACKGROUND: People with Parkinson’s disease (PwP) often experience rigidity, or increased resistance to passive movement across joints, contributing to gait disturbances and falls. While prior studies have explored the relationships between trunk ROM and functional task performance, most focused narrowly on trunk rotation.
PURPOSE: To compare active trunk ROM (flexion, extension, lateral flexion and rotation) and trunk mobility during functional tasks between PwP and age-matched peers (AMPs), and to evaluate relationships between trunk ROM, trunk mobility and functional task performance.
METHODS: Trunk ROM was measured using a hand-held goniometer. Total trunk ROM was calculated as the sum across all planes. Trunk mobility was assessed using wearable inertial measurement units (APDM Opal sensors) during the Stand and Walk (SAW) and Timed Up and Go (TUG) tests, which include walking, sit-to-stand (STS) and turning. Descriptive statistics, mean differences (MD) and 95% confidence intervals (CI) were reported. T- test and Pearson correlations were used to analyze group comparisons and relationships, respectively.
RESULTS: 19 PwP (H&Y: I-II, mean age (SD): 68.5 (6.3)) and 18 AMPs (mean age (SD): 62.1 (8.8)). PwP showed significantly lower total trunk ROM compared to AMPs (PwP: 318.7° ± 67.0°, AMPs: 371.2° ± 50.3°), p = .011, MD = 52.5°, 95% CI [12.8, 92.3]. Trunk mobility during SAW test was also reduced in PwP (PwP: 17.28 ± 3.62°, AMPs: 21.41 ± 7.25°) p= .017, MD = 4.13°, 95% CI [0.31, 7.95]. Greater trunk mobility was associated with faster functional task performance (STS; r = -.527, p = .020). Total trunk ROM was associated with faster turn duration (r = -.595, p = .007) and shorter STS duration (r = -.511, p = .025).
CONCLUSION: In summary, people with early-stage Parkinson’s disease demonstrate significant reductions in trunk range of motion and mobility compared to age-matched peers, which are closely linked to slower performance of functional tasks. These findings highlight the importance of assessing trunk movement across multiple planes to better understand and address mobility limitations in this population.
COMPREHENSIVE CARE: Self-management, empowerment, coping strategies
P23.01
1 Kristianstad University, Sweden
2 Linköpings University, Sweden
Parkinson’s disease (PD) affects 1–2% of people over 65 and require long-term management. While care appointments in outpatient settings are scheduled once or twice a year, persons with PD (PwPD) spend the majority of time in self-care. Effective information is essential for enabling self-management, yet research shows gaps in how and when such support is provided. This study explored PwPD’s needs and experiences of information across different stages of the disease trajectory in Sweden.
We conducted a descriptive qualitative study using semi-structured interviews, individually and in focus groups, with 19 PwPD recruited from three neurology clinics. Participants represented early, middle, and advanced stages of PD. Data were collected between October and December 2023 and analyzed using reflexive thematic analysis.
The analysis identified an overarching theme: Individually adapted and easily accessible information enables self-management in everyday life. Three main themes described PwPD’s perspectives:
Easily available and trustable information – PwPD obtained knowledge from health professionals, peers, the internet, and patient organizations. While online resources were valuable, many emphasized the importance of trustworthy professionals and peer exchange. Timely information to fit personal needs and stage of disease – Information needs varied by disease stage, personal preferences, and life situation. Key moments included time of diagnosis, onset of new symptoms, and treatment changes. Stepwise, repeated provision was preferred over one-time information sessions. Disease specific content and self-management strategies – PwPD needed both medical knowledge (symptoms, prognosis, medications, side-effects) and practical strategies for daily life and emotional coping. Beyond biomedical facts, support for psychosocial adaptation and self-efficacy was essential.
PwPD in Sweden emphasize the need for timely, tailored, and accessible information to support their self-management. Educational interventions should integrate medical and practical aspects, include peer perspectives, and be delivered continuously throughout the disease trajectory. A person-centered, flexible approach can empower PwPD, enhance self-efficacy, and improve quality of life while reducing strain on healthcare systems. We propose exploring co-created educational resources integrating professional and lived expertise and assessing their impact on patient outcomes.
P23.02
1 Central Michigan University, Department of Physical Therapy, United States
2 University of Michigan Health-Sparrow, United States
3 Mary Free Bed Rehabilitation Center, United States
Introduction: People with Parkinson’s disease (PwPD) in rural communities face delayed diagnosis and limited access to specialized care, and lower self-efficacy for disease management. A physical therapist designed the Parkinson’s Report Card Program (PRCP) to provide improved access to symptom monitoring, feedback, education, and follow-up support every six months for one year, aiming to enhance disease management when access to specialized care is challenging. This study evaluated the impact of the Report Card Program on non-motor symptoms, physical function, care-seeking behaviors, and self-efficacy. Methods: Twenty-eight participants from three rural communities completed assessments at baseline, 6 months, and 1 year. Measures: Chronic Disease Self-Efficacy Scale, Non-Motor Symptom Questionnaire, Activities-Specific Balance Confidence Scale, 10 Meter Walk Test, 3 Meter Backward Walk Test, Brief Balance Evaluation Systems Test, and 30 Second Sit-to-Stand Test. At each visit, participants received personalized report cards with feedback/recommendations to address each area. Repeated-measures ANOVA and mixed models were used to examine changes and associations among outcomes. Results: After one year, the use of movement disorder specialists increased by 50%, and 67% of subjects received referrals to physical therapy to address impairments noted during testing. Of the 15 subjects who previously reported exercising less than 2 days per week, 93% adopted regular exercise at least twice weekly. Significant improvements were observed in comfortable walking speed (p=.023), backward walking speed (p=.002), and leg strength (p=.011), which were maintained at one year. Higher self-efficacy was associated with greater balance confidence, fewer non-motor symptoms, and faster walking, although mean self-efficacy scores did not change significantly. Conclusion/Impact: The Parkinson’s Report Card Program improved measures related to fall risk, exercise frequency, and use of movement disorder specialists to manage care in PwPD living in rural communities. Correlations between self-efficacy, non-motor symptoms, balance confidence, and walking abilities underscore the importance of early diagnosis, exercise, and specialist consultation for optimal management of the disease. Bi-yearly, in-person, on-site screening and continuous monitoring assistance within rural communities can lead to improved symptom management and help address the care gap that rural communities face.
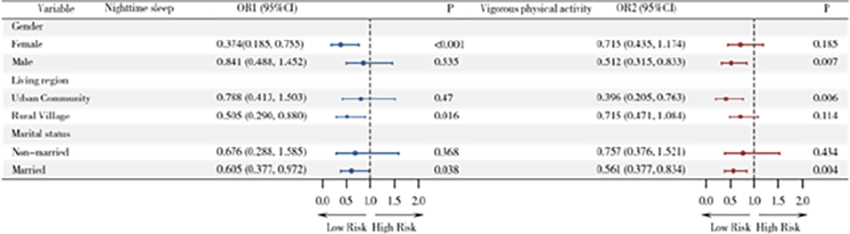
P23.03
1 Duke University School of Medicine, United States
2 Duke University School of Medicine, Parkinson’s Foundation, United States
Introduction: Posttraumatic growth (PTG), a common experience of people with neurodegenerative disorders, encompasses positive changes like creativity and adaptability rather than the negative aspects of deterioration and decline that most patient-reported outcomes are designed to evaluate. In this study, we examined PTG in people with Parkinson’s (PwP), including self-reflection on hope and strength..
Methods: In summer 2025, PwP seen in Duke Neurology’s interprofessional Parkinson’s Disease (PD) Clinic were invited to complete a PD Hope Survey. The survey began with asking PwP to list three things they were hopeful for. They then completed several patient-reported outcome measures: the Satisfaction with Life Scale (SWLS) and the State Hope Scale (SHS), which have been previously validated in PwP, and the Turbocharged Living Tool (TLT), a new scale developed by Jim Plews-Ogan, MD, a physician diagnosed with amyotrophic lateral sclerosis in his 60s, as a tool to evaluate PTG in patients with neurodegenerative disorders. TLT scores range from -12 (low PTG) to 36 (high PTG). The survey concluded by asking PwP to rate their experience. Demographic and disease data, including the Clinical Impression of Severity for Parkinson’s Disease (CISI-PD) and Hoehn & Yahr stage, were determined through review of the medical record.
Results: Thirty-nine PwP (18 female, mean age 69.6 years, mean disease duration 5 years, mean Hoehn & Yahr stage 2.1) completed the survey. Themes in what patients were hopeful for included information about their disease, improved symptoms and independence, activities (“walking”), and feelings (“remain positive”). PwP reported overall high levels of PTG (mean TLT 15.7, standard deviation 9.19), hope (mean SHS 36.8, standard deviation 8.27), and satisfaction with life (mean SWLS 24.0, standard deviation 7.66). There was a moderate negative association between CISI-PD and SHS (R^2 = 0.4) and between CISI-PD and SWLS (R^2 = 0.3). Fourteen PwP reported being asked about their strengths as someone with PD before the visit, and 14 PwP reported that the survey provided insight on the skills gained as someone with PD.
Conclusion: PwP can experience posttraumatic growth as they adapt to living with a neurodegenerative condition. Encouraging self-reflection on PTG may provide PwP with valuable insight and potential therapeutic benefit. Further research will adapt and refine the TLT for the experiences of PwP.
P23.04
1 Radboud University Medical Center, Netherlands
2 Patient research council, Dutch Parkinson Association, Netherlands
3 Radboud University Medical Center / Maastricht University Medical Center, Netherlands
4 University Medical Center Groningen, Netherlands
Background: Lifestyle interventions have the potential to support people with Parkinson disease (PD) in managing their disease and improving quality of life. There is growing evidence for positive effects of lifestyle interventions in single domains, such as physical activity, stress and nutrition. However, despite potential additive and synergetic effects, research on the effects of a combination of lifestyle interventions is limited. Furthermore, lifestyle interventions are only scarcely part of standard medical care, and there are significant challenges related to changing lifestyle behaviour and adherence to such interventions. In this study, we evaluate the (cost-)effectiveness of an integrated, personalized and stepped care lifestyle approach for people with PD.
Methods: We perform a 12-month randomized controlled trial in 256 people with PD, equally randomized between two groups. Both groups receive a clinical assessment with a lifestyle coach and can partake in usual care. The intervention group receives an additional lifestyle intervention, the SENSS approach, consisting of guidance and interventions on different lifestyle domains: stress, exercise, nutrition, sleep and self-management (SENSS). The intervention is performed remotely according to a stepped-care model to personalize the intervention to the participants’ needs and abilities. The primary endpoint of this study is the between-group difference in quality of life over 12 months measured with the Parkinson’s Disease Questionnaire-39. Secondary endpoints include between-group differences in PD symptoms, health-related outcomes, self-management and personal goals measured through questionnaires. They also include physical activity and sleep quality, monitored with a wrist-worn sensor for one week at baseline and after 12 months. In addition, cost-effectiveness of the intervention will be analysed, and the experiences of participants and healthcare professionals are explored through a qualitative study.
Preliminary results: Inclusion for the SENSS study started November 2024 and is expected to be complete by the end of 2025. At the congress, we will present the baseline characteristics of the included participants.
Discussion: We expect this intervention to improve quality of life and self-management of people with PD, without increasing healthcare costs. In addition, we expect this trial to offer valuable insights into how such intervention can be integrated into current care for people with PD.
P23.05
1 University of Canberra, Australia
2 The University of Sydney, Australia
3 Calvary Health Care Kogarah, Australia
Introduction: The benefits of exercise for people with Parkinson’s disease are well known. Despite these benefits, starting and maintain exercise over the long term is challenging. Developing exercise self-management skills and exercise self-efficacy is key for people with Parkinson’s to engage in and continue with exercise. The aim of this project was to co-design an online exercise self-management program, incorporating behaviour change techniques, to increase exercise uptake and promote an exercise habit in people with Parkinson’s.
Method: A series of four focus groups and three individual interviews were conducted to develop an online exercise self-management program, EnhanceLife-PD. The Theoretical Domains Framework and the Capability, Opportunity, Motivation, Behaviour model of behaviour change were used to determine the facilitators and barriers to exercise which informed the content and design of the program.
Results: The EnhanceLife-PD website was developed consisting of five modules. 1. Exercise – what is it and why is it important?, 2. Getting started, 3. Maintaining and sustaining exercise, 4. Factoring in your falls risk and 5. Exercise health professionals. Modules 1 to 4 are designed for people with Parkinson’s disease to use under the guidance of an exercise health professional, alongside prescribed exercise. Module 5 is designed for exercise health professionals to assist them in supporting people with Parkinson’s who are completing the EnhanceLife-PD program.
Conclusion: The EnhanceLife-PD program is a freely available online exercise self-management specific to the needs to people with Parkinson’s. EnhanceLife-PD has the potential to assist people with Parkinson’s to exercise over the long term.
P23.06
1 Radboudumc, Netherlands
Introduction Young onset Parkinson disease (YOPD) has a big impact on the individual during an active phase of life. This can affect their partner, and sometimes their children who are also in a stage of development. However, insights into the needs of this family system is lacking.
Methods We investigated the needs of persons with YOPD, their partners and their children through thematic analysis of 48 semi-structured interviews. We also analyzed the consumption of allied and mental healthcare in the first eight years after diagnosis in a YOPD population (n=808). The results from both analyses were combined to contextualize the findings.
Results There was both substantial overlap and unique needs between persons with YOPD, their partners and their children. Overlapping needs included being able to positively influence the disease, being supported and being able to understand the situation through appropriate information. Persons with YOPD and their children often expressed a need for control. Partners and children expressed a need to support the person with YOPD, while at the same time they wanted to have some time or activities for themselves. Only persons with YOPD disclosed a need for a sense of meaning in life.
Healthcare consumption was moderate to low. In the first 8 years of the disease, physiotherapy was used most often (44.1% in the first year after diagnosis, 26.6% in years 2 to 8), but mental healthcare, occupational therapy and speech and language therapy were all used by a minority (ranging from 1.5-10.5% and ranging from 1.7-13.2% in years 2-8).
The interview data revealed many reasons for the limited consumption of allied and mental healthcare, e.g., dissatisfaction with therapy methods, lack of knowledge about existing therapies and a dismissive or avoidant coping strategy.
Discussion This study highlights the varied needs of persons with YOPD, which go beyond drug- or therapy related needs. Furthermore, it highlights the needs of their family system and provides examples of needs for partners and children. However, despite existing therapies, healthcare consumption is low in this population. Addressing these needs, signposting whenever appropriate, and improving self-efficacy and understanding of the disease can prove essential for decreasing overall disease burden.
P23.07
1 PMD Alliance, United States
2 CND Lifesciences, United States
3 CND LifeSciences, United States
Objective: Advances in research now enable earlier identification of neurodegenerative disease risk due to genetics, family history, alpha-synuclein biomarkers, or prodromal symptoms (iRBD, anosmia, constipation, mood disorders). Individuals in the “space between” risk and formal diagnosis often miss opportunities to adopt neuroprotective lifestyle changes. The Proactive Brain Health Alliance (PBHA) aims to understand the experiences and needs of those at risk or in preclinical/prodromal stages of disease, offering credible health education, evidence-based interventions, and peer connection. Prior research (Schaeffer et al., 2020) underscores the importance of follow-up education, psychosocial support, and self-advocacy resources.
Method: PBHA provides expert-led education on risk factors, early symptoms, neuroprotective lifestyle strategies, and research participation. Interactive discussions enable participants to engage directly with neurologists, receive emotional support, reduce stigma, and build self-efficacy. An ongoing survey assesses participants’ experiences with risk identification, current knowledge, and support needs, complemented by post-program feedback polls.
Results Among survey respondents (n=28), 75% desire information on lifestyle modification, and 75% expressed interest in clinical trials. 45% reported their healthcare provider explained their risk status, and 45% received actionable next steps. 42% cited mental health impacts, and all respondents emphasized the importance of a supportive community. Post-program polls (n=122) showed 97.5% felt their knowledge improved and 91% planned to make lifestyle or behavioral changes.
Conclusion Early identification of neurodegenerative risk creates both opportunities and challenges—enabling prevention through lifestyle change but revealing gaps in education and psychosocial support. PBHA findings highlight that at-risk individuals want credible information, empowerment in risk management, and greater access to resources to mitigate the burden of early risk identification.
P23.08
1 Western University, Canada
2 Lucerne University of Applied Arts and Sciences, Switzerland
Background: External auditory cueing with music improves gait in people with Parkinson’s Disease (PwP). Internally generated cues may provide similar benefits, but without the technological limitations of delivering external cues and greater practicality for everyday use. However, little is known about which internalized cues might work best (e.g., familiar music or specially devised novel stimuli). In addition, assessing spontaneous (non-instructed) synchronization of gait may help illuminate the mechanisms and index reception to internal cueing.
Objective: We compared the effects of imagining a familiar (self-selected) tune versus a novel ‘ditty’ on spatiotemporal gait parameters (variability and mean difference from baseline). We also explored styles of spontaneous synchronization between the imagined internal cues and footsteps.
Methods: We recruited PwP (n = 13, Mage = 70yrs, Modified H&Y 1-4) and two control groups: younger adults (n = 15, Mage = 22yrs), and older adults (n = 14, Mage = 70yrs). Baseline gait was measured (no cueing), followed by two internal cueing conditions: Familiar vs Novel. No instructions were given to synchronize steps with the cues. To qualitatively assess spontaneous synchronization, the conditions were repeated and audio-recorded while participants sang the cues out loud. Participants also completed cognitive tasks (e.g., digit span), music-related tasks (e.g., beat processing, experience with music and dance), and a measure of imagery ability (BAIS).
Results: Across groups, neither type of internal cueing significantly changed gait variability (stride length, stride velocity, cadence). However, we were able to identify three styles of spontaneous synchronization: on the beat, syncopated, and dissociated (no synchronization). PwP synchronized more with the novel ditty than their familiar tune, but also showed wider strides, suggesting greater cognitive load. Control groups synchronized similarly to familiar and novel conditions. Across all groups, vividness of imagery was associated with synchronization style for the familiar but not the novel condition.
Discussion: Here we show that it is possible to teach internalized cueing using novel musical stimuli and that PwP often naturally synchronize their steps to such material. Future research should explore individual differences that may help to better tailor internal cueing strategies for everyday support for PwP.
LOVE: February 2025 Neuromusic: To be presented November 2025
P23.09
1 Queen's University Belfast, United Kingdom
Background Parkinson’s medication regimens are complex, yet timely adherence is essential for maintaining symptom control and quality of life. To design interventions that support self-management, empowerment and coping - and to identify where behaviour change is needed - it is necessary to understand how people with Parkinson’s (PwP) and carers sustain adherence and where it breaks down.
Methods A UK-wide survey of PwP (n=509) examined whether demographic factors or levels of medication self-efficacy (PROMIS®) were associated with adherence (MARS-10). Qualitative interviews (n=20; PwP=12, carers=8) explored how functional ability affects adherence, what influences self-efficacy, and what strategies are used to overcome challenges. The COM-B model was applied to identify capability, opportunity and motivation factors shaping adherence.
Results Adherence difficulties were almost universal (95%; n=485), and 15% (n=78) reported significant challenges. Self-efficacy showed a statistically significant but weak association with adherence (r=.32, r2=.10, p<.001) indicating that self-efficacy alone is insufficient to explain adherence. Medication-taking was shaped by fluctuations in function, cognitive and psychological changes, perceived benefit and the desire to preserve independence. Self-efficacy emerged as a dynamic, co-constructed process built through adaptation, trust and support. COM-B analysis identified reflective motivation and psychological capability as core behavioural drivers, with physical opportunity (e.g. carer input, reminders, access) acting as the main facilitator when capability or motivation weakened. Participants called for tailored, practical and clinically trustworthy supports to strengthen coping, self-management and empowerment.
Conclusion Medication self-management in Parkinson’s is a fragile but actively maintained system. PwP engage in reflective and cognitive work, while carers and environments provide compensatory scaffolding when capability or motivation falters. Interventions should target this adaptive balance rather than assume stable behaviour. The next phase will integrate quantitative estimates of difficulty with qualitative insights on lived strategies and behavioural drivers to inform the co-design of a digital educational tool to empower medication self-management in everyday life.
P23.10
1 Australia
2 UCLA, United States
Introduction: This study looked at how stigma — the negative attitudes or judgment people face — makes it harder for people with Parkinson’s disease (PWP) in Latin America to get healthcare. It found that stigma affects not just medical access but also how people see themselves, how they join in social life, and how they accept their condition. The goal of this research is to understand these experiences better and find ways to reduce stigma so people can receive fair and respectful healthcare.
Method: Four online discussion groups were held with 25 people living with Parkinson’s (and 4 carers) from ten Spanish-speaking Latin American countries. Participants were invited through the Alianza Iberoamericana de Parkinson. A Spanish-speaking psychologist led the sessions. Everyone gave consent and was protected under an ethics-approved process. The group discussions were recorded in Spanish, translated into English, and analysed to find common themes and experiences.
Results: People shared many examples of stigma in everyday life and healthcare. They talked about feeling judged, afraid to get diagnosed, and being embarrassed by their symptoms. Limited access to treatment made symptoms harder to hide and more embarrassing. Misunderstandings about Parkinson’s led to unfair treatment at work, in social situations, and even in health services.
To cope, some people avoided others or denied their condition, which often caused loneliness, sadness, and less engagement with care. Still, some participants described how they found strength to not let stigma bother them which shows that stigma can be challenged.
Conclusion: Stigma is a big reason why many people with Parkinson’s in Latin America delay getting help or hide their disease. Feelings of shame and fear stop people from seeking care or joining activities. However, learning more about the disease and connecting with others can reduce these barriers.
This study shows the importance of training healthcare professionals to recognise and address stigma, and of community programs that build understanding and inclusion. Reducing stigma at all levels — personal, social, and institutional — is essential for better, fairer care for people with Parkinson’s across the region.
(This abstract has been written in consumer/ patient friendly language for the WPC).
P23.11
1 Department of Nursing, Juntendo University Hospital, Japan
2 Department of Neurology, Juntendo University School of Medicine, Japan
Introduction: Foslevodopa-foscarbidopa continuous subcutaneous infusion (LDP/CDP) therapy has been developed to achieve continuous dopaminergic stimulation and reduce motor fluctuations in patients with Parkinson’s disease (PD). Although some patients are obliged to initiate LDP/CDP therapy as outpatients because of their employment or family circumstances, outpatient initiation may present distinct challenges. This report presents the nursing approaches and outcomes observed in patients who initiated the therapy in an outpatient setting.
Methods: Eight participants (6 men, 2 women), who were diagnosed with clinically established PD according to MDS clinical criteria, initiated LDP/CDP therapy as outpatients between June and September 2025. Prior to therapy, the nurses provided individualized education on device operation, medication management, and infusion site care. We retrospectively reviewed nurse-led telephone and e-mail consultations after LDP/CDP initiation to assess patient progress and characterize the nursing support provided.
Results: The mean age of participants was 57.9 ± 11.7 years, mean disease duration 11.5 ± 4.0 years, and mean oral levodopa dose before initiation 664.3 ± 3.3 mg/day. A total of 30 consultations were recorded: 20 (66.6%) were related to PD symptoms, four (13.3%) to skin complications, and four (13.3%) to device handling. Skin complications included panniculitis in three cases and local infection in two patients, with one patient requiring temporary discontinuation of therapy. The remaining seven patients (87.5%) continued therapy for more than one month. Nearly half of all consultations (n=14, 46.6%) occurred within the first week after initiation. With continued nursing support, the number of consultations decreased to two after one month.
Conclusion: During outpatient initiation of LDP/CDP therapy, frequent nursing support was crucial in the early phase to manage fluctuations in PD symptoms and address skin complications. The continuous involvement of nurses enhanced patient confidence, self-efficacy, and self-care abilities. Such nursing engagement may expand access to LDP/CDP for patients who encounter barriers to initiation on an inpatient basis.
P23.12
1 Cornwall partnership NHS FT, United Kingdom
2 CORNWALL PARTNERSHIP NHS FOUNDATION TRUST, United Kingdom
3 Active Cornwall - Cornwall Council, United Kingdom
Introduction: Exercise and physical activity are essential for people with Parkinson’s (PwP), yet most do not achieve recommended frequency, intensity, or duration for neuroprotection and long-term benefit. Evidence for behaviour change and lifelong self-management is limited. Partnership across health, social care, and charitable organisations offers a feasible, sustainable approach to long-term self-management.
This project aimed to empower PwP with knowledge, skills, and resources to manage their condition through access to high-quality physical activity, clinical evidence, best practice guidelines, UK standards, and government policy.
Methods: Over 7 years, a mixed-method, pragmatic approach designed, delivered, and evaluated a four-phase physical self-management pathway across a county population (≈ n1500) in England. (See Figure 1).
Partnerships across sectors enabled integrated long-term management, Parkinson’s-specific training, network development, and capacity building of activity providers.
Results: 325 PwP participated in Park-Way. In a sub-sample (n47), Self-efficacy for Exercise (SEE) scores increased by a mean of 3.41 (SD 1.28). Key reasons for effectiveness: 1. Motivation, 2. Confidence/Information, 3. Knowing where to get help. Most participants reported it was extremely or very helpful and changed their view on exercise. All intended to increase activity after participation.
64 community exercise/activity providers received Parkinson’s-specific training. Six Connect and Conquer events engaged 246 PwP and 92 providers.
Conclusion: Internal evaluation indicates Park-Way positively impacts short-term intention to be highly active, though long-term effects, cost savings, and disease modification remain unknown. Partnership across health, social care, and charitable sectors has established a high-quality, evidence-based, sustainable approach to person-centred physical self-management. It has raised awareness of Parkinson’s and the importance of activity while providing PwP with choice, opportunity, and access to diverse, enjoyable activities to self-manage their condition.
P23.13
1 Yoshimoto Registered Management Consultant Office, Japan
2 Nutrition Support Association, Japan
Background: For people living with Parkinson’s disease (PD), medication remains the cornerstone of treatment, yet it is not sufficient to maintain quality of life (QOL). Comprehensive self-management that integrates medication, exercise, and nutrition is essential. Among these factors, nutrition serves as a central pillar influencing medication effectiveness, physical strength, and overall well-being. This approach uniquely combines the perspectives of a person living with PD and a registered dietitian, offering an innovative patient-led model of empowerment and multidisciplinary collaboration.
Objective: This study aims to clarify how self-management practices—particularly nutritional management—can empower individuals with PD to maintain physical and psychological stability and to extend that empowerment to others.
Methods: A qualitative case-based approach was used, focusing on the experiences of a registered dietitian living with PD who has implemented self-management strategies since her diagnosis in 2015. Data included long-term records of body composition, nutritional balance, and physical fitness test results, combined with testimonies from peers in a PD boxing program (Rock Steady Boxing (RSB) Tokyo).
Results: Following the initiation of structured self-management in 2020, noticeable increases in muscle mass and BMI were observed, accompanied by improved physical stability and daily functioning. Nutritional balance—particularly moderate protein, calcium, and fiber intake—was associated with better physical strength and QOL. These quantitative improvements were mirrored by qualitative changes—patients reported renewed motivation, confidence, and hope, illustrating the empowering effect of holistic self-management.
Conclusion: Self-management integrating nutrition and exercise may help stabilize physical condition and improve QOL in people with PD. Among these, nutritional management provides a sustainable foundation for both physical stability and effective medication response. Furthermore, this patient-professional partnership model may serve as a blueprint for scalable empowerment programs for people with PD worldwide.
P23.14
1 University of Plymouth, United Kingdom
2 University of Plymouth; University Hospitals Plymouth NHS Trust, United Kingdom
3 Translational and Clinical Research Institute, Newcastle University; National Institute for Health and Care Research (NIHR) Newcastle Biomedical Research Centre, Newcastle University., United Kingdom
Introduction Current healthcare pathways inadequately meet the needs of people with Parkinson’s (PwP). An innovative PD care pathway has been developed within University Hospitals Plymouth (UHP), UK, providing supported self-management, remote monitoring and timely reviews. Embedded in the pathway is annual review by questionnaire (quantitative and free-text) of PwP care experience, including contact with professionals, PD understanding and self-management confidence. Initial evaluation demonstrated benefits compared with standard care, (Kehagia et al. 2024). The objective of this study is to determine how PwP experiences changed with time, both in relation to time on the care pathway, and in subsequent cohorts.
Method Questionnaire responses from the initial cohort (C1) of 108 enrolled PwP (from Oct 2019) will be evaluated over the subsequent 4 years, with questionnaire response categories being analysed descriptively across domains, supplemented by content analysis of free text responses. A 2nd cohort of PwP (C2) ( from May 2021) will be similarly evaluated. Extraction of organisational factors contemporaneous with the evaluation periods will allow an understanding of how contextual factors may impact experience of care.
Results In preliminary analysis, the proportion of PwP feeling ‘listened to’ and ‘’treated as an individual’ remained broadly stable for 4 years’ follow-up duration (mean 79% and 84% respectively for C1, and 71% and 77% respectively for C2). The mean proportion of C1 PwP reporting good understanding of PD was higher at months 36-48 compared with months 6-12, in terms of recognising how PD affects them (85% increasing to 100%), how to request help (71% increasing to 87%) and confidence to self manage (71% increasing to 86%). In C2 PwP, the mean proportion reporting good understanding was similar to C1 PwP in all domains at 6-12 months (81%, 73%, 72% respectively), with less improvement by months 30-36 (88%, 55%, 73% respectively); the variability may be explained by the lower number of responses at later time points. Additional analyses will explore experience related to healthcare professional contact, as well as relationship to contextual factors.
Conclusion This evaluation will enable understanding of PwP longitudinal experience of a supported self-management pathway, and how this may relate to underpinning infrastructure. Findings will inform recommendations to improve pathway delivery for future patient benefit.
COMPREHENSIVE CARE: Multidisciplinary/Interdisciplinary teams
P24.01
1 Parkinson's Foundation, United States
2 Yale School of Medicine, United States
3 Johns Hopkins University School of Medicine, United States
Objective: This study aimed to identify the instructional preferences and barriers to continuing education (CE) participation and completion among healthcare professionals caring for people with Parkinson’s disease (PD).
Background: CE is a requirement for many licensed healthcare professionals working with individuals with PD and movement disorders, yet there is limited research on their preferred learning methods that influence their decisions to participate in online CE activities.
Methods: A 16-question online survey was developed by a team of Parkinson’s Foundation staff and healthcare professionals and then distributed to inpatient and community-based healthcare providers via convenience sampling over three weeks. Descriptive statistics and regression analyses (simple and multivariable) were used to characterize the sample and examine interactions between learner demographics and preferences. The study and its methods were approved by John Hopkins University Institutional Review Board (IRB) IRB00373495.
Results: A total of 4,947 healthcare professionals, primarily from the US, completed the survey and were included in our analyses. Most were between 31–40 years old (46%), and 55.7% identified as women. Most identified as White (65.6%); Black (21.5 %); Hispanic/Latino (45.7%). Live webinars were the most preferred online CE format (62%), followed by recorded webinars (54%) and journal articles (53%). Half favored 1–2 hours for course length (50.5%). Relevance to practice was a primary indicator of CE selection (61%). Institutional funding support was reported by 46%; 37.5% paid out of pocket. Nearly half (48.2%) preferred CE courses priced between $100–$500. Interactive simulations (37.5%) and case studies (36.1%) were preferred formats. Most (55.3%) use the Movement Disorder Society as a source for online CE. Time (40.1%) and financial constraints (34.5%) were the largest barriers. Course workload (28.5%) and toggle speed of audio/video (20.2%) were the largest barriers to starting, but not completing, CE.
Conclusions: Clinically relevant, synchronous, interactive, and applied learning experiences are preferred instructional methods. Time and financial constraints are barriers. Course workload and media playback speed affect completion rates. These findings will inform future online CE development for healthcare professionals.
P24.02
1 Rocky Mountain University, United States
Purpose: To examine the effects of participating in a 10-week transdisciplinary, multimodal community exercise class on motor, cognitive, and speech abilities of individuals with Parkinson’s Disease (PD).
Participants: Individuals with PD Methods: Participants attended a 50-minute multi-modal high intensity exercise program twice per week for 10 weeks, that was led by both physical therapy and speech language pathology students. Participants performed standardized testing and questioning pre-and-post participation. An 8-week gap between exercise series following with repetition of the testing to start the next semester.
Results: For the 4 semesters that this program has incorporated both PT and SLP, the participants showed statistically significant improvements within the semester for gait speed (mean = 0.07 m/s; p=0.014), 3 Meter Backwards Walk Test (mean = 0.67 seconds; p=0.011) and the Timed Up and Go (TUG) (0.85 seconds; p=0.001). Participants showed no change in performance of the 30 Second Sit to Stand Test, TUG-cognitive or the difference between the TUG-cognitive/TUG. One semester of SLP data has been collected, and participants showed maintenance of performance for the Brief Cognitive Status Examination (BCSE), the Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V) loudness and Maximal Phonation Time (MPT), despite the progressive nature of PD.
Discussion: PD is a progressive neurological disease in which we expect gradual decline in mobility, independence, speech quality, swallowing and cognition. A program that maintains function in this population is considered successful; if improvements can be shown over a 3–5-month period, that program is achieving remarkable impacts. This program demonstrated maintenance of cognitive and vocal functions and improvements in mobility constructs. This suggests that providing a trans-disciplinary approach to an exercise program can help improve functional outcomes for individuals with PD and help provide greater independence and potentially slow down the progression of the disease process. Further research to investigate the maintenance or continued improvement over longer periods is warranted.
P24.03
1 HAWK University of Aplied Sciences and Arts Hildesheim, Holzminden, Goettingen; Faculty of Social Work and Health, Germany
2 University of Cologne, Faculty of Medicine and University Hospital Cologne, Medical Psychology | Neuropsychology and Gender Studies, Centre for Neuropsychological Diagnostics and Intervention (CeNDI), Germany
3 Brandenburg University of Technology Cottbus - Senftenberg, Faculty for Human Sciences, Department of Physiotherapy, Germany
Background: People with Parkinson’s Disease (PwP) need individually tailored, continuous and coordinated care provided by an interprofessional team – as integrated care networks (ICN) aim to facilitate [1, 2]. The literature describes relevant components of ICN [1,3,4], but so far, there is no agreement regarding the core components. Furthermore, it is mostly unclear to what extent these ICN take into account the perspectives of PwP and their relatives (R). Therefore, this scoping review aims at providing a comprehensive overview of their perspectives on what is important in Parkinson’s Disease related healthcare.
Methods: The protocol for this scoping review was developed with PwP, R and healthcare providers and published at Open Science Framework (osf.io/mgdkx). We searched Medline, CINAHL, PubPsych, LIVIVO and grey literature for relevant publications. Inclusion criteria were: a focus on experiences, needs, expectations and wishes of PwP and R regarding their healthcare, publication in English or German between Jan 2005 and Mar 2025. Title-abstract and full text screening was conducted by three independent reviewers. Data extraction will be performed by one and verified by a second reviewer. Any disagreements will be discussed und solved by consensus or by decision of a third reviewer.
Results: The analysis has not been completed at the time of abstract submission. After title-abstract screening, 251 records were included in full text screening. Completion of data extraction and analysis of included full texts will be finished by the time of the presentation.
Conclusion: Our findings will contribute towards shaping ICN in a more person-centred approach, ultimately improving quality of life of PwP/ R and the quality of healthcare.
References
Vester L. B., Haahr A., Nielsen T. L., Bartolomeu S. & Portillo M. C. (2023). doi: 10.1016/j.pec.2023.107931 Rajan R., Brennan L., Bloem B. R., Dahodwala N., Gardner J., Goldman J. G., Grimes D. A. et al. (2020). doi: 10.1002/mds.28097 Bloem B. R., Henderson E. J., Dorsey E. R., Okun M. S., Okubadejo N., Chan, P., Andrejack J. et al. (2020). doi: 10.1016/S1474-4422(20)30064-8 van de Warrenburg B. P., Tiemessen M., Munneke M. & Bloem B. R. (2021). doi: 10.3389/fneur.2021.638853
P24.04
1 University of Miami Miller School of Medicine, United States
2 The University of Miami, United States
Objective: To analyze differences in baseline characteristics of patients with idiopathic Parkinson’s disease (PD) versus patients with atypical Parkinsonism (including progressive supranuclear palsy, corticobasal degeneration, multiple system atrophy, dementia with Lewy bodies, and undifferentiated atypical parkinsonian syndromes) at an academic Parkinsonism interdisciplinary clinic (PIDC).
Background: Atypical parkinsonism is characterized by a more aggressive course and rapid progression to dependency and mortality than PD, necessitating timely, comprehensive care. The PIDC at the University of Miami (UM) evaluates patients with Parkinson's Disease and atypical parkinsonism in a single visit through interdisciplinary assessments by neurology, neuropsychology, physical and occupational therapy, speech-language pathology, nutrition, and social work.
Methods: A retrospective chart review was conducted for all patients evaluated at the UM PIDC from January 1, 2022, to July 31, 2025. Patient demographics and diagnoses were compared against various functional status measures obtained during IDC visits. Statistical analysis included Chi-square, 2-sample 2-tailed independent t-tests, and correlations. Statistical significance was set at p=0.05.
Results: During the period studied, 49 out of 201 PIDC patients had atypical parkinsonism. These patients had greater functional impairment at PIDC presentation (higher HY stage [mean of 3.24 vs. 2.26, p<0.001], higher MDS-UPDRS III score [47.1 vs. 29.8, p<0.001], and lower score on the Schwab & England scale [53.2% vs. 76.1%, p<0.001]), worse physical therapy measures (increased 5x sit-to-stand [29.9 vs. 18.9 seconds, p<0.001] and timed up and go [31.2 vs. 18.3 seconds, p=0.04]) and greater impairment of swallowing function (decreased Functional Oral Intake Scale [5.9 vs. 6.7, p<0.001] and more likely to fail the Yale Swallow Protocol [p<0.001]) than PD patients.
Conclusions: Although patients with atypical parkinsonism have similar interdisciplinary referral needs as those with Parkinson's Disease, they presented to our PIDC with more advanced symptoms. Reasons likely include diagnostic delays and more rapid disease progression. Earlier IDC referrals may help mitigate complications and morbidity in the atypical parkinsonism population.
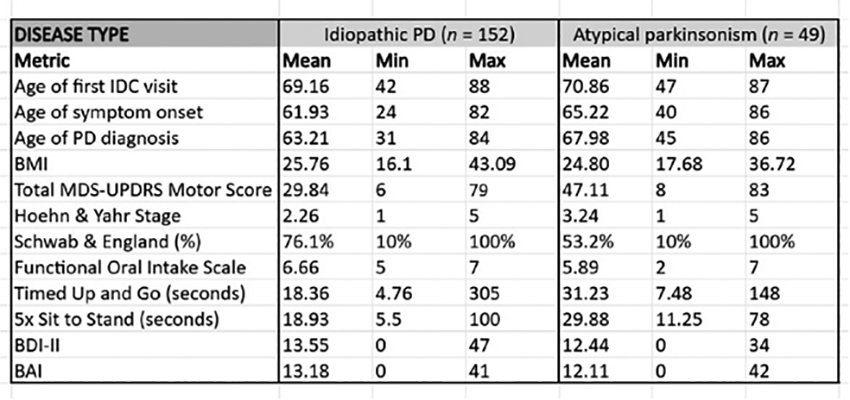
P24.05
1 Parkinson's Foundation, United States
2 Parkinson's, United States
Background Community Partners in Parkinson’s Care is designed to educate and prepare staff in senior living communities and home care agencies to provide better care for people with Parkinson’s across the United States. This program originated in the regional Upper Midwest of the United States in 2012 and was acquired by the Parkinson’s Foundation in January 2023. Currently the program serves 86 partners in 122 locations within 24 US states. To date, this program has trained over 26,000 direct care providers.
This poster shares outcomes of a recent survey of current site champions at Community Partner sites. Site champions serve as the primary resource for each partner site. These individuals ensure ongoing required staff training, collect program outcomes on a semi-annual basis, and maintain communication and collaboration with Community Partners program staff.
Methods Surveys were conducted using the EthosCE webform functionality with all current site champions within the Community Partners Program.
Survey questions focused on:
Role as a site champion PD care improvements at each partner site Current challenges impacting program success
Survey results were compiled and analyzed in Tableau to review and consider future program modifications and updates.
Results - Overall, site champions understood their role and felt that their individual care of people with Parkinson’s improved.
- There was reported improvement in interprofessional communication and care planning for clients with Parkinson’s.
- Program challenges included frequent staff turnover necessitating ongoing training
Conclusions Community Partners in Parkinson’s Care conducted a successful survey to monitor site champion impressions of the program which will be used for future program modifications and updates.
P24.06
1 Eastern Health, Australia
2 Healthscope, Australia
Background: Non-pharmacological and non-surgical interventions from nursing and allied health professionals play an important role in management of Parkinson’s disease, but there is no clear source of evidence-based recommendations to guide these therapies.
Objective: To critically appraise the content and quality of recommendations regarding non-pharmacological and non-surgical interventions from high-quality PD clinical practice guidelines (CPGs).
Methods: CPGs were identified through database searches (inception to September 2025) and hand searching. Quality was assessed using validated tools (AGREE-II and AGREE-REX), and recommendations from higher-quality CPGs were mapped to the International Classification of Functioning, Disability and Health (ICF). Confidence in these recommendations was assessed using the Grading of Recommendations Assessment, Development and Evaluation Confidence in Evidence from Reviews of Qualitative Research (GRADE-CERQual) assessment.
Results: Of 29 guidelines identified, 9 met the threshold for high quality and contained 114 recommendations. From the included guidelines included, 40 GRADE-CERQual summary statements were developed: one with “high confidence”, 16 with “moderate confidence”, 22 with “low confidence” and one with “very low confidence”. The high confidence recommendation was related to use of augmentative technology in speech pathology, and moderate confidence in interventions related to a range of clinical domains including bladder and bowel management, nutrition, movement strategies, exercise, handwriting, dysphagia and dysphonia management.
Conclusion: This breadth of high to moderate confidence recommendations in high quality clinical practice guidelines highlights the importance of the multidisciplinary allied health team in managing symptoms of people with PD to improve function, reduce symptom burden and improve quality of life.
P24.07
1 Parkinson's Foundation, United States
Introduction The U.S. faces a crisis in Parkinson’s disease (PD) care. The prevalence of PD is increasing, there’s a growing shortage of PD specialists, and the national economic burden of PD is rising. As the U.S. population continues to age, these challenges will only be amplified. The National Parkinson’s Project was signed into law into 2024 with the purpose of designing a plan to prevent, diagnose, treat and cure PD. The Parkinson’s Foundation convened the National Roundtable on Parkinson’s Care and Innovation on September 4, 2025 to lay the groundwork for this national agenda.
Methods The Roundtable identified 20 key stakeholders to participate, bringing together people living with PD, care partners, physicians, health care providers, health system leaders, policy experts, and innovators across disciplines and industries—inside and outside of the PD space. Participants first completed a survey to identify major challenges and the highest impact, most feasible levers for addressing those challenges. The Foundation then interviewed each participant to discuss their survey responses and to better understand their expert perspective. Finally, participants came together in Washington, DC for a day-long convening beginning with a discussion of eight challenges and potential solutions, followed by a prioritization exercise.
Results Participants emphasized the critical importance of upskilling community clinicians (e.g., general neurologists, primary care providers, including nurse practitioners and physician assistants), ensuring people with PD have access to integrated care including care navigation support, using better data to drive better care, and supporting technology innovation in the PD space. The Roundtable discussion will be synthesized into a proceedings report set for release in late 2025. At the participants’ encouragement, the report will include a set of short- and long-term action steps to ensure that the momentum to build a national agenda is maintained.
Conclusion The Parkinson’s Foundation is a national leader in improving care for people with PD, with the aim that every person with PD receives the highest quality care possible, regardless of setting. The PD community is at a pivotal moment for transforming care, with new approaches and tools emerging across technology, care delivery, and policy. The National Roundtable represents a key input towards establishing a shared national vision and facilitating coordinated action across sectors.
P24.08
1 CHU Toulouse, France
Background: ParkinsonNet is a nationwide network of more than 4000 health care professionals specialized in PD spread across 70 regional networks in The Netherlands, aiming to improve the quality of PD care.
Objectives: to establish a coordinated care network in the Haute-Garonne (France), inspired by the ParkinsonNet model. Action-PD has been funded by a European grant in September 2024 over 24 months. It seeks to strengthen collaboration among healthcare professionals (HCPs) for PD patients, provide specialized training for physiotherapists (PT), occupational therapists (OT), and speech therapists (ST), and build an interdisciplinary network. It also intends to develop and disseminate tailored resources for healthcare providers, individuals living with PD, and their caregivers.
Methods: a multidisciplinary team in Toulouse (PT, OT, ST and a research assistance) trained by the Dutch ParkinsonNet team to educate HCPs in the Haute-Garonne in PD and to create a local network of specifically trained HCPs. Key partners include the THCS, the French Ministry of Health, Toulouse University Hospital (CHU Toulouse), the Parkinson Expert Center (CHU Toulouse) and ParkinsonNet.
Results: From September 2024 the Toulouse team have done: a) an analysis of the local healthcare system, stakeholder engagement, and development of documentation incorporating information from patient and professional associations, healthcare institutions, and networks; b) HCPs training initiatives covering care delivery, patient management, and follow-up of practitioners already involved PD care; c) Team training by ParkinsonNet International in the Netherlands (June 2025); d) Creation of the “PluriPark” network, including its logo and communication materials, to foster local collaboration; e) A webinar, titled “Multidisciplinary Management of Parkinson’s Disease,” which gathered over 120 HCPs; f) Preparation of a 2026 professional training program, “Rehabilitation in Parkinson’s Disease: Specific and Collaborative Approaches”, a two-day, free course with an accompanying e-learning module (two sessions planned for January and February 2026); g) Development of professional resources, including mapping of regional care structures, identification of tools facilitating communication and access to information for people with PD in Haute-Garonne.
Conclusion: The Action-PD project paves the way for high-quality patient-centered care for people with PD in France.
P24.09
1 ParkinsonNet, Netherlands
2 Radboudumc, Netherlands
Background: ParkinsonNet is a Dutch, innovative, cost-effective, evidence-based, integrated and patient-centred model of network care for people with Parkinson's disease (PwPD). Its mission is to improve the lives and guarantee the best possible care for PwPD worldwide. In the Netherlands, ParkinsonNet has improved PD expertise for health care professionals, interdisciplinary collaboration and patient education.
The ACTION-PD project, funded by THCS, will accelerate the implementation of this model in four regions in Europe; Katowich, Rome, Padua and Toulouse and initiate an implementation model for further scaling.
Methods:We anticipate three mechanisms that will improve efficiency: A centralized train-the-trainer concept, so that these national health care professionals can train their national colleagues in their own language and subsequently supervise the network in their own country. Importantly, these trained trainers then have the tools and expertise that is required for further nationwide scaling in the respective countries; Implementation in four regions in three countries simultaneously instead of one after the other; The implementation teams will learn from each other, creating a community for lifelong learning and further continuous healthcare improvement.
The Dutch team will support the regional teams consisting of an Occupation therapist, Physiotherapist, Speech therapist and Project lead.
From the start in September 2024 till now the regions have done a feasibility study about the current delivery of care in their region and stakeholder analysis followed by a 3 day training of the regional teams. There was a focus on coordinating an evidence-based approach in treating PwPD and a train-the-trainer program for the allied health care professionals. After the training the new trainers started a monthly coaching meeting with the Dutch experts to learn from and with each other's implementation process. The Dutch experts coaching and guide them with all the knowledge and expertise on forming the network and implementing the model during these sessions. This will take up until September 2026.
Conclusion:The ACTION-PD project is successfully ensuring that regions can learn from each other during implementation. They have also gained a better understanding of how healthcare is currently organized and can respond to areas where improvements can be made. Lastly trained health care professionals feel more competent in treating people with parkinson.
P24.10
1 Parkinson's Foundation, United States
Objective The Parkinson’s Foundation (PF) Hospital Care Initiative (HCI) aims to eliminate preventable harm and promote higher reliability in care for people with Parkinson’s disease (PWP) in the hospital.
Background Annually, 1 in 6 PWP will experience avoidable complications in the hospital, often related to issues with medication management, mobility and dysphagia. The PF Hospital Care Recommendations are the foundation of the HCI and outline five Standards of Care to address these challenges.
Methods PF employs a multi-faceted strategy, bolstering our commitment to community advocacy and clinical education, broadening our reach through awareness raising and coalition building, and expanding our impact through our learning collaborative and research consortium.
Results Community Advocacy: Since 2011, PF has distributed over 200,000 hospital safety resources to members of the Parkinson’s disease (PD) community.
Clinical Education: Through PF’s ‘Learning Lab’- an online education platform, we accredit courses focused on improving hospital care for Physicians, Nurses, Advanced Practice Providers, Pharmacists, Psychologists, and Social Workers.
Raising Awareness: In 2025, PF raised awareness through: (1) Publication in high profile journals, (2) A patient safety awareness campaign, and (3) Presentations at national conferences.
Coalition Building: Expanding our reach beyond PD experts, PF is building relationships with leading healthcare and quality organizations including the Institute for Healthcare Improvement, the Geriatric Emergency Department Collaborative, and more.
Learning Collaborative: Launched in 2023, PF currently partners with nearly 40 health systems and their clinical teams, working to implement PD quality improvement projects aligned with PF’s Recommendations.
Research Consortium: PF is funding, partnering, and leading projects to strengthen the evidence-base demonstrating the negative health outcomes that PWP experience while hospitalized as well as creating and measuring the impact of solutions designed to improve inpatient care for PWP.
Conclusions PF invites hospital and health systems to join our work to improve hospital care for PWP.
P24.11
1 Shirley Ryan AbilityLab, United States
Introduction and Program Goals: There is a growing need for tailored, interdisciplinary rehabilitation approaches for people with Parkinson’s Disease (PD), particularly in Hoehn and Yahr (H&Y) stages 2–3. In response, an intensive, cohort-based “PD Boot Camp” model was created within DayRehab(TM) . The program emphasizes group-based therapy with a focus on dual-task training, education, connection with community resources, and peer support.
Program Methods: 3-8 participants per cohort attend sessions 2-3 days a week over 6–8 weeks. Comprehensive physical therapy (PT), occupational therapy (OT) and speech therapy (ST) with access to social work and psychology services are provided. Participants completed surveys pre, post program, and 6 months post on demographics and quality of life outcomes including the Parkinson’s Disease Questionnaire – 39 (PDQ-39) and satisfaction surveys. Functional outcomes were completed pre and post program. These included Functional Gait Assessment (FGA), 10-meter walk test (10MWT), 9-hole peg test, 3 word recall (3WR), average vocal intensity (AVI), NeuroQOL (NQ), and maximum sustained phonation duration (MSPD).
Program Results: In the first 5 cohorts, 27 participants were between the ages of 58-87 years old with 33% female. 22% had never had PT, while 56% and 41% never had OT or ST respectively.
Based on preliminary results, PDQ-39 summary index scores were unchanged at post and 6 months. Trends of improvement in the mobility, cognition and bodily discomfort dimensions may be confirmed with additional participants.
Clinician and patient satisfaction surveys show agreement with feasibility, accessibility, and appropriateness of the program.
For those completing outcomes at pre and post, minimal detectable change was exceeded on FGA (n=11, p=0.004), 10MWT (n=13, p=0.094), and right and left 9-hole peg test (R n=11, p=0.037; L n=12, p= 0.40). Performance was maintained across all ST measures (3WR, AVI, MSPD, NQ, p = (0.095-0.84).
Conclusion: Starting PD Boot Camp was aimed at improving interdisciplinary, coordinated care for people with PD. Early outcomes from the program have been positive, including both functional outcomes and patient satisfaction. We aim to continue to spread to other sites across our organization.
P24.12
1 University of Bristol, United Kingdom
2 North Bristol NHS Trust, United Kingdom
The North Bristol NHS Trust’s Parkinson’s Hub aims to provide expert, holistic assessment for patients with rapidly deteriorating Parkinson’s and related disorders at risk of admission or with unmet palliative care needs. The Hub was initiated in response to several factors: i) waiting times for routine reviews have increased and hospital admissions for PwP could be avoided if they could access a specialist at the first signs of deterioration in their condition; ii) as people reach the advanced stages of Parkinson’s they have particularly complex needs requiring input from multiple services; iii) palliative care for PwP is known to improve quality of life yet access is poor.
This ethnographic study describes the various elements of the multidisciplinary Parkinson’s Hub (see Figure) and explores the experiences of patients, carers and healthcare practitioners involved in the Hub. We conducted 106 hours of observations of Hub clinics and multidisciplinary team meetings, and completed 33 interviews with patients, carers and practitioners.
The core Hub team comprises specialist Parkinson’s practitioners (SPPs) based in the community and movement disorder specialist geriatricians, a specialist pharmacist, dementia practitioners and an administrator based in secondary care. Additional specialists (e.g., palliative, psychiatry) are brought in as needed. Patients are mainly identified and referred to the Hub by SPPs; other referrals come from care home, general practice and Emergency Department teams. Patients may be offered an appointment at the weekly out-patient Hub clinic. Weekly multidisciplinary team meetings are held online to discuss new referrals and agree treatment plans for all patients, which can then be implemented immediately. Patients are reviewed after 4 weeks or as needed.
The Hub is valued by PwP and carers for providing rapid access to a specialist at a time of need. Multidisciplinary input and longer consultations provided in the Hub clinic better enabled holistic assessment of patients’ complex needs and primary palliative care. Practitioners working with the Hub also value it for the support and learning opportunities it provides, which better enable them to meet their patients’ needs. The Hub model provides a potential means of integrating services to deliver timely, comprehensive care that overcomes pervasive problems in current Parkinson’s care and aligns with the UK health service priority of shifting from “hospital to community” care.
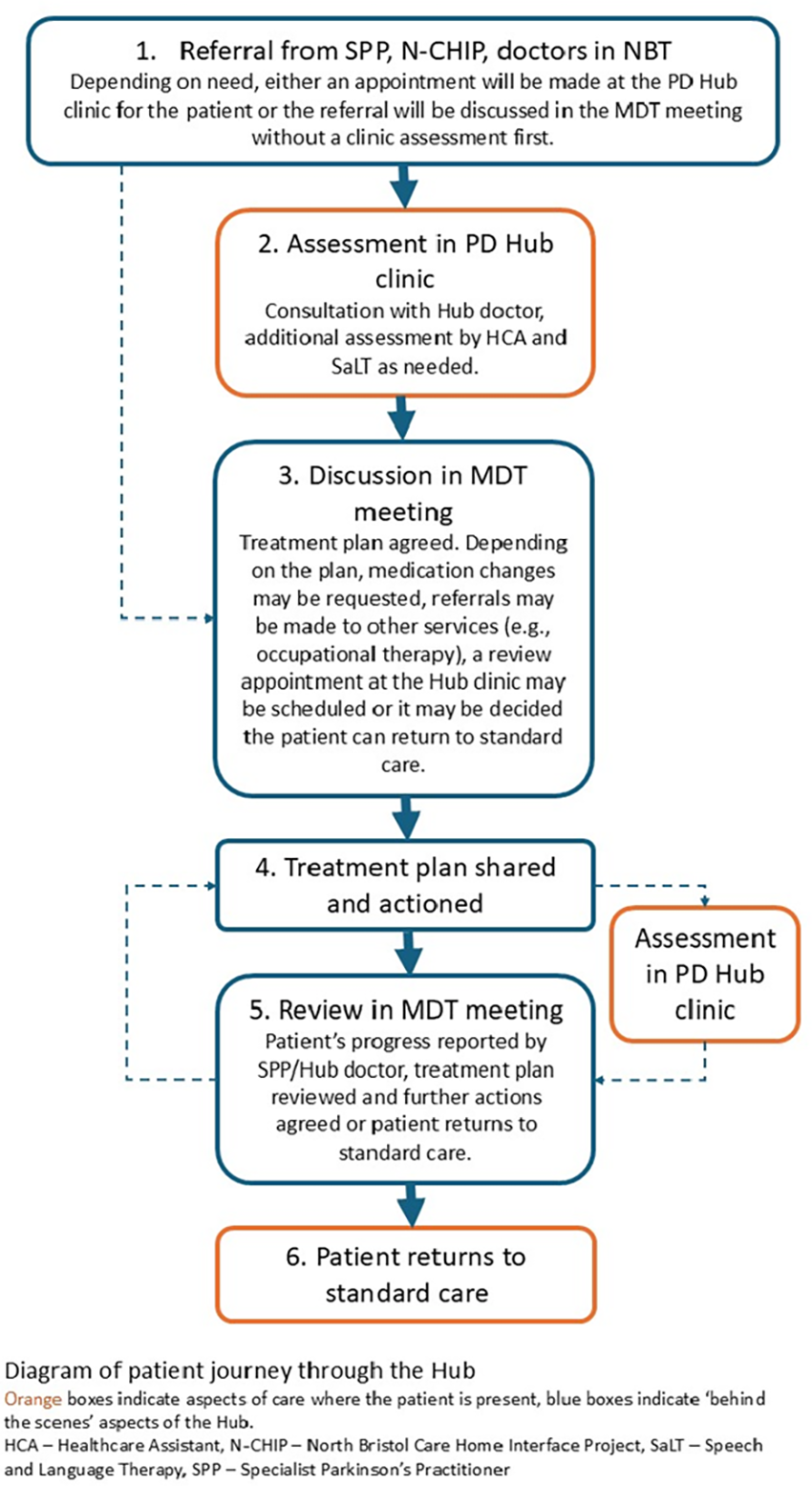
P24.13
1 Shirley Ryan AbilityLab and Northwestern University Feinberg School of Medicine, United States
2 Florida State University College of Medicine, United States
3 Shirley Ryan AbilityLab, United States
4 Shirley Ryan AbilityLab Northwestern University Feinberg School of Medicine, United States
Introduction:
The Parkinson's disease questionnaire (PDQ-39) is used to measure the impact of Parkinson's disease on patient's quality of life. We have used the PDQ-39 in our interdisciplinary rehabilitation Parkinson's disease and movement disorder clinic since 2009, but challenges with completion, clinical utility and follow up use exist. We hypothesized that completing the survey digitally (in advance or in office) rather than on paper may improve completion which could better enable clinical decision-making using the PDQ-39.
Methods: From 2021-2023, patients received the PDQ- 39 in paper forms at the time of the interdisciplinary clinic visit. Paper forms were scanned as pdf files into our electronic medical record. For 11 months in 2025, patients in the interdisciplinary clinic received emails in advance of their visit to complete the PDQ-39 digitally in the research electronic data capture (REDCap). If not completed prior to their visit, the patient received a tablet to complete the form, while waiting for the appointment.
On later review, all paper records were noted if completed, partially completed with skipped questions or scanning errors, or not completed. Digital records were reviewed if completed or not.
Results: From January 1, 2021, to December 31, 2023, paper extraction showed 33% (438 of 1314) of encounters with PDQ-39 scans. 267 (20%) were fully completed, with an average summary index score of 22.0±16.7. 141 (11%) were partially completed, 30 (2%) were blank scans. From January 21, 2025 to November 18th, 2025, 131 (46%) digital surveys were completed out of 285 administrations, with an average summary score of 20.6±15.7. Six (2%) were started but not completed and 148 (52%) were missing. Regardless of format, clinicians (physiatrists, physical, occupational, and speech therapists) reported rarely using the surveys to guide care.
Conclusion: In our clinical setting, use of the PDQ-39 may be valuable to track patient’s perceptions of their quality-of-life following rehabilitation interventions; however clinical utility is limited by low completion rates and redundancy with other screening performed. Digital forms had a higher completion rate and are easier for clinicians to view/track in the medical record but remain seldom used to guide clinical decisions. Further research will evaluate shorter screening tools and work with an advisory board to inform improving completion and utilization of patient-reported outcome measures.
P25.04
1 Robert Gordon University, Aberdeen, United Kingdom
Introduction: Seeing a Parkinson’s specialist Physiotherapist is recommended from diagnosis, yet no clear consensus defines this role—limiting clarity and training pathways. This study used a consensus-based approach to define the role and identify the knowledge, skills, and training required for Parkinson’s specialist Physiotherapists.
Methods: A modified Delphi study was conducted in two phases. Phase one recruited people living with Parkinson’s (PwP) and registered Physiotherapists to complete an online survey, which informed Phase two. Phase two was an international modified online Delphi study involving three expert groups (PwP, Clinical Physiotherapists, Academic Physiotherapists). The Delphi consisted of three rounds: rounds one and two collected quantitative data with consensus set at 75% a priori; round three involved focus groups to agree a role definition and explore items not reaching consensus earlier.
Results: Phase one: 132 participants (29 Physiotherapists, 103 PwP) completed the survey exploring perceptions of specialist Parkinson’s Physiotherapy and its core competencies. 97% of Physiotherapists and 88% of PwP agreed PwP should see a Parkinson’s specialist Physiotherapist. Additionally, 93% of PwP and 84% of Physiotherapists supported a standardised training pathway. Findings highlighted the need for a clear role definition.
Phase two: 23 participants (9 PwP, 7 Clinical, 7 Academic Physiotherapists) completed all Delphi rounds. Round one achieved consensus on 43/69 statements across three domains (Knowledge, Skills, Attributes); round two achieved consensus on 4/23 remaining statements. Items not reaching consensus were discussed in round three. Data from rounds one and two informed a role definition and scope of practice. Round three achieved 92% consensus on the proposed role definition and explored barriers to role standardisation.
Conclusions: This study, using a consensus-based approach, identified four core pillars that define the role of a Parkinson’s specialist physiotherapist: clinical practice, leadership and management, research and, education. Future research should develop a training pathway to support the consistent, effective delivery of care for this complex condition.
COMPREHENSIVE CARE: Rehabilitation sciences (PT, OT, SLP)
P25.02
1 Curtin School of Allied Health, Curtin University, P.O. Box U1987, Perth, WA 6845, Australia, Australia
Background: People with Parkinson's experience a range of communication difficulties impacting their conversations and quality of life. As conversations are a two or more-way interaction, communication partners play an important role in conversational success. Recent studies including collaborative design research, highlighted the value of their lived experiences in shaping therapeutic approaches.
Aims: To 1) capture the lived experience of people with Parkinson’s and their partners regarding barriers faced and strategies used to support conversations; 2) develop a therapy program supporting their conversations incorporating the principles of co-design; and 3) trial and evaluate this program using a repeated measures experimental design, mixed-methods approach.
Methods: During phase 1, data were collected from 45 participants (25 people with Parkinson's and 20 partners) across five focus groups and analysed using qualitative content analysis. During phase 2, a series of six co-design groups were conducted to develop a conversation therapy program with three people with Parkinson's and their partners. During phase 3, this co-designed program was trialled in two groups with people with Parkinson's and their partners. The feasibility and effectiveness of the program was statistically evaluated. Its acceptability, clinical, and social validity were explored using qualitative methods.
Results: During phase 1) participants discussed five categories of barriers to conversation relating to the person with Parkinson's, partner, conversation dynamic, background noise, and limited information and services. Participants described six categories of strategies including those used to prepare for conversations, during conversations, for phone use, acceptance and awareness, services and information, and engagement in activities.
During phase 2) participants co-designed a program which would comprise of four weekly group sessions with a speech pathologist and four/five dyads. This program was unique in that each dyad would be working on specific individual goals to improve their conversations. Preliminary findings indicate promising trends regarding its feasibility, acceptability, and potential effectiveness.
Conclusion: People with Parkinson's face unique challenges in conversation and through their lived experience of Parkinson's they have developed strategies that support conversational success. A group therapy approach to practice such strategies has potential for success.
P25.03
1 NeuroFit Networks dba Parkinson Wellness Recovery, United States
Freezing of Gait (FOG) affects nearly 40% of people with Parkinson disease (PD), with increasing prevalence as the disease progresses. This disabling motor symptom disrupts forward movement despite the intent to walk, significantly impairing mobility and quality of life. Pharmacological and surgical treatments remain inconclusive, and physical therapy is often the recommended intervention. However, individuals with FOG may have reduced ability to retain therapy benefits compared to those without FOG. This case study explores the potential benefits of a high-frequency physical therapy model—three to five consecutive sessions per week on a recurring monthly basis. The goal is to assess whether this approach may lead to greater improvements in functional mobility and support longer-term retention of gains within our challenging health care model.
Four individuals with PD and FOG participated in this case study.
All patients completed physical therapy intensives as described above for at least four months. Interventions were individualized but focused on reducing gait interference, modulating arousal, applying compensation strategies, and increasing gait thresholds.
All four patients completed the Freezing of Gait Assessment. Patients demonstrated improvements in scores ranging from 3-9 points and were able to maintain improvements in mobility and reduce falls over the four months.
FOG remains a complex symptom to manage in PD due to its unpredictability and limited response to conventional care. Individuals with FOG may have greater difficulty retaining the benefits of physical therapy, highlighting the need for innovative delivery models. This case series suggests that periodic, high-frequency physical therapy intensives may be effective at improving FOG and sustaining therapeutic gains. Further research comparing this model to traditional frequencies is warranted to guide best practices in dosing and delivery.

P25.05
1 University of the Pacific, United States
Parkinson's disease (PD) is a progressive neurological condition with about 90,000 new cases in the USA each year. Approximately 5% of those diagnosed with PD are women under 40 years of age (Parkinson's Foundation, n.d.), placing them in the menstruating age group. These women must navigate the symptoms of Young Onset Parkinson's Disease (YOPD), taking care of children and family, and managing their careers. Although PD symptom fluctuations are well documented, those associated with hormonal changes, and their specific impact on occupations are not well-researched. Many women report worsening of motor symptoms, pain, stiffness, fatigue, and other mental health challenges during menstruation (Tolson, Fleming, & Schartau, 2022). These are likely to have an impact on many occupations such as personal care, work, leisure participation, sexuality, and sexual expressions.
This qualitative case series focuses on the lived experiences of menstruating women with PD, from occupational therapy perspective. Emphasis is placed on participation in meaningful occupations during premenstrual and menstrual phases, challenges related to the use of menstrual care products, pain, fatigue, sleep, and the extent of perceived support from healthcare professionals for the challenges specifically related to menstruation. The second part of the study will explore further the impact of PD on sexual expression, and the ability experience pleasure from intimate activities. The study is currently underway and is in the initial phase of data collection. The outcomes of the study will inform the healthcare professionals at large about the PD symptom profile during the menstruation, and how PD impacts the PwP's sense of sexual self, sexual expression, and ability to engage in sexual activity in a meaningful and satisfactory manner.
P25.06
1 ohsu-portland, United States
2 Oregon Health & Science University, United States
Introduction: Cueing, which involves using external temporal or spatial stimuli such as auditory, visual, or tactile cues, improves gait in Parkinson’s disease (PD). Our previous work demonstrated that personalized, tactile cueing delivered to the wrist improved gait stability and the quality of turning in individuals with PD. However, the effects of personalized cueing in the real world remain unknown for this specific cueing modality. This is an exploratory analysis of an ongoing randomized clinical trial (RCT) where we test the hypothesis that personalized (step-synchronized) but not fixed tactile cueing will improve the quality of turning and gait during daily life.
Objective: To evaluate the practicality and impact of a personalized cueing intervention on daily-life walking in people with PD.
Methods. The ongoing double-blinded, RCT (NCT05818189) was designed to assess the effects of personalized versus fixed cueing on gait automaticity in people with PD. This trial will enroll 60 eligible people with mild-to-moderate PD who will be randomized into receiving personalized (n=30) and fixed cueing (n=30) at home for at least 30 minutes per day for one week when they feel in their ON-medication state. Participants will wear two instrumented socks (one per foot) and a lumbar Opal sensor for 3 weeks to measure gait and turning at home, with the first and third weeks without cueing and the second week with personalized or fixed cueing. Here, we have compared the effects of no cueing (first week) vs. cueing (second week) on daily-life mobility.
Results. We have enrolled 14 people with PD who were randomized to personalized (n=6) and fixed (n=8) cueing at home, respectively. Both types of cueing were feasible, enjoyable, without adverse events, and reached similar doses at home (average: 340 minutes for fixed and 246 minutes for personalized, p=0.101). Personalized cueing, but not fixed, increases the daily-life stride length (effect size=0.40) and decreases the daily-life stride length variability (effect size=-0.35) and daily-life turn peak velocity variability (effect size=-0.39) compared to no cueing.
Conclusion. Our preliminary data suggest that personalized tactile cueing, delivered to the wrist, is feasible for people with mild-to-moderate PD and may potentially have an impact on their daily-life walking. Future steps will be to test if cueing dosage may be associated with improvements in daily-life walking.

P25.07
1 Hawaii Parkinson Association, United States
2 Speech, Swallowing, & Voice Specialists of Hawaii, United States
3 Neurology Associates, United States
4 PHREI- researcher, United States
Over 89% of people with Parkinson's experience difficulties with speech as the disease progresses. Patients may struggle with a weak voice, slurring, mumbling and managing their saliva. Communication challenges are a significant influence of lower quality of life. They are associated with decreased communication participation, social withdrawal, and increased risks for social isolation and stigmatization in persons with Parkinson’s disease. There are evidenced based programs to assist in improving and maintaining speech including LSVT Loud and Speak Out programs as well as standard speech therapy. The challenge for many is how to maintain these capabilities when no longer in active therapy. Breath control, volume, pitch and articulation are also the key factors taught in playing harmonica. We believe that by learning and playing harmonica, people with PD can maintain / improve speech and saliva management as well as garner other benefits including social interaction from being in a group and learning to play a musical instrument. The goal of our pilot study was to look at the feasibility of using a recreational group harmonica program as adjunct to speech therapy in maintaining and/or improving speech. The study enrolled 22 participants with PD and speech problems randomized to the treatment group of 12 people who received harmonica instruction/group class 2 x a week for 3 months and a control group of nearly equal size (10) who received a standard home speech therapy program. Pre and post testing of speech characteristics and movement disorder symptoms were performed by speech therapists and movement disorder neurologists. The treatment (Harmonica) group showed an improvement in all 8 speech tests, UPDRS and PDQ-39 over the control group which did not change significantly; however, the small sample size limit definitive conclusions regarding efficacy. Our conclusions are that teaching harmonica to people with PD and speech problems is feasible and safe. Findings further suggest that harmonica playing as an adjunct to speech therapy can aid in maintaining and/or improve speech factors in individuals with Parkinson’s Disease. More research on the benefits for playing harmonica for improved speech in PD is needed. This study was funded by Parkinson Foundation Community Grant and Hawaii Parkinson Association Community Outreach Grant.

P25.08
1 University of Texas Health Science Center, San Ant, United States
2 University of Texas Health Science Center at San Antonio, United States
Introduction: Over 80% of persons with PD will experience dysphagia during their disease. Currently, behavioral rehabilitation is the standard of care for swallowing intervention. Unfortunately, while dysphagia is present early in PD, it is under-recognized, and intervention is often delayed until obvious issues arise. This study evaluated a novel preventative intervention for swallowing decline in PD.
Methods: A pre-post study evaluated 20 patients with Parkinson’s disease (Hoehn & Yahr score x̅ = 2.8) treated biweekly for 6 weeks with a sensorimotor swallow exercise program and followed to 1-month post-treatment. Swallowing was evaluated across four domains: Perceptual: Swallowing fear (SWKS), Eat-10, Sydney Swallow Questionnaire (SSQ), Symptomology: Drooling, Functional: Functional oral intake score (FOIS), Mann Assessment of Swallowing (MASA,) Physiologic: Modified Barium Swallow Impairment scale (MBSImp), Penetration-Aspiration score (PAS), Lingual strength, Spontaneous swallowing frequency (SSF)
Results: Subjects exhibited deconditioned swallowing at baseline (FOIS </= 5, drooling, food/fluid avoidance). At baseline, self-reported swallowing impairment (EAT-10) was x̅=7.8 (SD:4.3), and the MASA score was x̅=173.3 (SD:11.6), with 68% of subjects below the cut-off for dysphagia (<178). The PAS score was x̅ = 2.37 (SD: 1.78), but only one instance of PAS > 5 was noted. Following treatment, the MASA score [nonparametric ANOVA, Q=8.6, p<.01], MBSImp score [Q=8.3, p<.01], swallowing frequency rate [Q=14.8, p<.001], SSQ [Q=9.9, p<.01], EAT-10 score [Q=8.7, p<.01], and swallowing fear [Q=6.2, p<.04] all improved, demonstrating significant change with maintenance to 1 month. Effect sizes (Cohen’s d) achieved across measures ranged from d= 0.59 to 1.67. The reliable change index (RCI), the amount of change in function not due to measurement error, was RCI MASA = 14.4 and SSF = 0.18. RCI (MASA) was achieved by 38.5% post-treatment and 54% at 1-month post. RCI (SSF) was 61% post-treatment and 69.23% at 1-month post. The minimal detectable change (MDC) indicating absolute reliability and measurement responsiveness was achieved by 46% [MASA] post-treatment and by 61.5% [SSF] post-treatment.
Conclusion: These data suggest a program of intense swallow motor exercise applied proactively is safe and specific to swallowing, intrinsically motivating, and works both musculoskeletal and sensorimotor timing substrates. These results offer compelling evidence for trialing this approach in larger PD populations
P25.09
1 Istanbul Health and Technology University, Faculty of Health Sciences, Department of Physiotehrapy and Rehabilitation, Turkiye
2 Istanbul Health and Technology University, Faculty of Health Sciences, Department of Physiotherapy and Rehabilitation, Turkiye
Background and aim: Motor imagery is the process of mentally simulating a movement without physically performing it. It is known that during an imagined movement, brain regions similar to those activated during actual movement are engaged. This highlights the importance of motor imagery in terms of neuroplasticity and rehabilitation. This relevance is particularly important in Parkinson’s disease, where impairments are observed not only in overt motor execution but also in the internal representation of movement. The present study therefore aims to comparatively examine the relationship between motor imagery capacity, walking, and cognitive functions in patients with Parkinson’s disease and age- and sex-matched healthy individuals.
Methods: The study included 12 patients with Parkinson’s disease (6 women, 6 men) in Hoehn and Yahr stages 1–3 with Mini Mental Test scores above 24, and 12 age- and sex-matched healthy individuals. The mean age of participants was 67.01 ± 7.06. Functional capacities were evaluated using the Timed Up and Go (TUG) and 10-Meter Walk Test (10MWT). The same tests were also mentally imagined by the participants, and both actual and imagined durations were recorded to calculate motor imagery accuracy. Cognitive functions were assessed using the Trail Making Test. The data were analyzed through group comparisons and correlation analyses.
Results: Functional performance in the TUG and 10MWT tests differed significantly between the Parkinson and control groups (p=0.008; p=0.002). The motor imagery accuracy for the same tests was significantly lower in the Parkinson group (TUG: 38.0 ± 22.03%; 10MWT: 55.0 ± 27.81%) (p=0.017; p=0.028). Significant group differences were also found in the Trail Making Test parts A and B (p=0.035; 0.002). Additionally, strong positive correlations were found between Trail Making Test scores and TUG/10MWT durations, while strong negative correlations were observed with motor imagery accuracy.
Conclusion: The results of this preliminary study suggest that motor imagery capacity is reduced in patients with Parkinson’s disease and this reduction may be associated with both functional and cognitive performance. Motor imagery-based therapies are considered to have the potential to support rehabilitation by improving motor learning and stimulating neuroplasticity, but larger randomized controlled trials are required to verify these possible benefits.
P25.10
1 University of Missouri–Kansas City (UMKC), United States
Introduction: Up to 90% of individuals with Parkinson’s disease (PD) experience voice and speech difficulties that affect communication, reducing quality of life. Over 30% identify voice deficits as among the most challenging aspects of PD, highlighting the need for comprehensive treatment strategies. Therapeutic group singing (TGS) has shown promise for voice improvement, while semi-occluded vocal tract exercises (SOVTs) are widely used in voice rehabilitation. However, few studies have examined combining TGS and SOVTs (TGS+SOVTs) as an integrated approach. This study examines whether TGS+SOVTs lead to greater improvements in both acoustic and self-reported voice outcomes compared to TGS alone. Method: We employed a 10-week, two-sequence randomized crossover design (AB/BA) with Tremble Clefs, a therapeutic singing group for individuals with PD in Arizona and Iowa (N = 44; Group A = 25; Group B = 19). Participants were randomly assigned to one of two intervention orders: Group A (TGS+SOVTs → TGS only) or Group B (TGS-only → TGS+SOVTs). Each group completed two 4-week interventions separated by a 2-week washout. Voice recordings were collected as pre- and posttests (weeks 1, 4, 7, and 10) and analyzed using the Acoustic Voice Quality Index (AVQI). Participants also completed the Visual Analogue Subjective Voice Rating Scale (VASVRS) before and after each weekly session to rate subjective voice quality, loudness, and vocal fatigue. Results: A linear mixed-effects model (LMM) revealed both TGS-only and TGS+SOVTs were similarly effective in improving acoustic and self-perceived voice outcomes. No significant group, period, or interaction effects were observed in AVQI scores, supporting the crossover design and absence of carryover effects. However, subjective voice quality ratings revealed a significant Group x Period interaction (p = .037), with decreased voice quality in Group B during TGS+SOVT (Period 2), compared to Group A in Period 1. Vocal fatigue ratings showed a significant period effect (p = .027), with lower fatigue reported in Period 2 regardless of intervention. Baseline scores were the strongest predictors across all models (p < .001), indicating individual variability. Conclusion: Singing-based interventions may address voice and speech difficulties, supporting long-term communication improvements in individuals with PD. Findings suggest TGS and TGS+SOVTs hold therapeutic potential as augmentative intervention for voice rehabilitation.

P25.11
1 Teachers College, Columbia University, United States
It is estimated that close to 40% of individuals with Parkinsońs disease (PD) present with mild cognitive impairment (MCI; Baiano et al., 2020). MCI may involve difficulties in executive dysfunction, attentional control, episodic memory, working memory capacity, and visuospatial skills. These interfere with planning, daily functioning, and autonomy, ultimately lowering health-related quality of life and heightening care partners stress (Baylor et al., 2024). Cognitive-linguistic deficits also impact patients’ social connectedness (Moya-Galé et al., 2025), which is crucial in reducing social isolation in this population.
We developed our first cognitive-linguistic group during the spring semester of 2025, with an average number of five participants attending the group in person once a week for eight weeks. So far, 13 participants have benefited from this experience. Prior to the start of our groups, our graduate students at Teachers College, Columbia University, complete screenings and a thorough cognitive-linguistic assessment with participants. Each cognitive-linguistic group session lasts two hours and begins with greetings and a collaborative review of the session’s schedule, which encourages student and participant engagement. Our targeted strategies include word retrieval (e.g., semantic feature analysis and verb network strengthening treatment) embedded in conversational, procedural, and narrative discourse; planning skills (e.g., calendars, goal–plan–do strategies); problem solving (e.g., SWAPS strategies); visuospatial processing; and memory skills (working memory, procedural memory, and compensatory strategies). Activities are intentionally functional, such as practicing with Google Maps or using Siri, and tailored to the participants’ individual needs (for instance, practicing with real-life locations from their neighborhoods). Because home practice is considered essential for skill generalization, a homework review has been built into every weekly schedule.
Our program has been shown to be sustainable over time. University clinics represent an ideal context for improving service delivery by embedding cognitive-linguistic group programs that are evidence-based, functionally oriented, and socially supportive. By leveraging these training environments, we can both expand access to services for individuals with PD and ensure that future clinicians are prepared to deliver holistic, person-centered care.
P25.12
1 Parkinson Voice Project, United States
More than 80% of people with Parkinson’s develop dysphagia (Suttrup & Warnecke, 2015), and up to 95% develop a voice disorder and struggle to communicate (El Sharkawi et al., 2002). These impairments lead to social isolation and reduced quality of life. Parkinson’s interferes with the production of learned, automatic movements, such as walking, talking, and swallowing, due to impaired pathways in the basal ganglia (Yin & Knowlton, 2006). Resulting speech deficits include hypokinetic dysarthria, characterized by decreased intensity, articulatory range of motion, and decreased prosody (Duffy, 2005).
SPEAK OUT!® Therapy, developed in 2010, helps people with Parkinson’s regain and retain speech by converting it from an automatic function to an intentional act. Thanks to the contributions of the late Dr. Daniel R. Boone, individuals with Parkinson’s increase their volume and improve their articulation and prosody by activating the direct (intentional) motor pathway instead of relying on the indirect (automatic) motor pathway. Case studies with videos of speech samples from pre-treatment and post-treatment will be presented.
Research supports to effectiveness of the SPEAK OUT! Therapy Program. Statistically significant improvements were achieved in the acoustic measures of intensity, prosody, voice quality, and patient self-perception of voice (Behrman et al., 2020). Boutsen et al. (2018) found that SPEAK OUT! Therapy significantly improved speech intensity, reading intelligibility, and vocal quality for people with Parkinson’s. Levitt and Walker-Batson (2018) also reported that SPEAK OUT! Therapy improved the patient’s perception of quality of life. Notably, Candea & Franklin (2025) found perceived leadership qualities in patients after SPEAK OUT! Therapy treatment. The leadership qualities improved were confidence, competence, communication, trustworthiness, and leadership inclination. These compelling findings underscore the effectiveness of SPEAK OUT!® Therapy and highlight the need for continued research.
This presentation will demonstrate how the SPEAK OUT! Therapy Program provides effective, evidence-based treatment by converting speech from an automatic function to an intentional act. The SPEAK OUT! Therapy Program offers voice and hope for individuals living with Parkinson’s disease.
P25.13
1 Associação Brasil Parkinson, Brazil
2 University of Sao Paulo, Brazil
3 Brazil Parkinson Association, Brazil
Background: Physiotherapy (PT) offers well-established short-term benefits for people with Parkinson’s disease (PwPD), improving mobility, balance, and quality of life through gait training, strength exercises, and cognitive-motor rehabilitation. However, while immediate functional gains are well documented, evidence regarding long-term neuroprotective effects or the potential of PT to slow disease progression remains limited. Objective: To investigate whether weekly group physiotherapy can reduce the progression of motor symptom severity in PwPD. Methods: A longitudinal, prospective, non-randomized controlled trial was conducted with 56 PwPD (Hoehn & Yahr stages I–III). Participants were allocated to an experimental group (EG; n=29) or control group (CG; n=27) based on their availability. Inclusion criteria included a confirmed idiopathic PD diagnosis, dopaminergic medication use, and ability to perform exercises and attend weekly in-person sessions. The EG participated in weekly 1-hour group PT sessions (≤10 participants) focusing on mobility, balance, and gait, with individualized corrections provided by the physiotherapist. Evaluations occurred at baseline (EV1) and after 12 months (EV2), conducted by a blinded assessor. The primary outcome was motor symptom severity (UPDRS III); secondary outcomes included cognitive function (MoCA) and quality of life (M-PDQ-8). Results: Repeated-measures ANOVA showed a significant group × time interaction (F(1,48)=5.47, p=0.02, effect size=0.07). Post hoc Tukey tests revealed that only the control group exhibited a significant increase (worsening) in UPDRS III scores after 12 months (p=0.004), while the experimental group maintained stable scores. Conclusion: A structured weekly group PT program effectively prevented the worsening of motor symptoms in PwPD over a 12-month period. Clinical implications:These findings demonstrate the feasibility and efficacy of low-frequency, group-based physiotherapy as a long-term management strategy for PD. Even a modest PT dosage, when applied consistently, can help slow the progression of motor decline and support the maintenance of quality of life in individuals with Parkinson’s disease.

P25.14
1 Parkinson Voice Project, United States
Therapeutic home exercise programs (HEP) are essential to implementing and sustaining skills. Adherence combines therapist recommendations and patient implementation (Zweben & Zuckoff, 2002). Barriers include cognitive-communication deficits, apathy, and limited care partner involvement. Addressing these improves quality of life for people with Parkinson’s.
The patient’s executive functioning determine how much support is needed. People with Parkinson’s disease often have secondary diagnoses of mild cognitive impairment, impacting attention, decision-making, organization, time management, and delayed gratification. These skills are needed to schedule the HEP, create a habit, and attend to the task. Strategies provide the necessary structure for success.
Active patient and care partner involvement increases implementation success. Collaborative goal-setting acknowledges the autonomy of the individual, increasing participation (Womack, 2012). Dopamine loss in Parkinson’s results in apathy or loss of motivation. Person-centered goals engage the patient and care partner to improve motivation (Rose et al., 2017).
Due to apathy and limited insight, habit formation requires therapist and care partner support. Initially, the patient may implement the HEP independently but lapse as the disease progresses. Care partner involvement from the beginning of therapy increases carry-over and long-term adherence.
An effective HEP for speech therapy is the SPEAK OUT!® Therapy Program. The treatment protocol includes daily home practice using a structured workbook and online practice sessions. The Certified SPEAK OUT! Provider educates the patient and care partner to regain and retain speech and swallowing. Case studies with videos will be presented.
Evidence-based strategies for effective and meaningful HEP will be presented. These include:
Establish regular practice times (Gardner et al., 2012), use calendars and alarms, and set up a consistent practice station (Wood & Neal, 2016). Eliminate distractions by turning off the TV, silencing cell phones, or going to an isolated area (Mason-Baughman & Lander, 2012). Reference videos of the exercises to increase independence, motivation, and adherence (Bartlett, Carpenter, & Chapman, 2022). Incorporate meaningful and motivating activities (Womack, 2012). Focus on tasks tied to personal interests or daily routines. Involve friends in setting up accountability systems, which can help relieve the burden on the care partner.
P25.15
1 Shirley Ryan AbilityLab, United States
Introduction: For those with Parkinson’s disease (PD), symptoms occur early in the disease process. However, historical utilization of allied health therapies is low in early PD. Early treatment demonstrates benefits in decreasing symptoms, delaying disease progression, and slowing quality of life deterioration. A proactive care delivery model’s goals are to provide early assessment, education, and treatment prescription to identify and address motor and non-motor symptoms to slow functional decline. This model provides an integrated, consultative approach to care.
Methods: This proactive program consists of a 90-minute evaluation, which includes discipline specific strategy training, Parkinson’s disease (PD) specific education, home exercise program development, and follow-up recommendations for additional care and community resources. It is recommended that the person with Parkinson’s (PwP) return every 6 months to 1 year for re-assessment. This re-assessment period allows allied health team members to screen for new functional concerns, to provide education and interventions to prevent decline in function and to manage any newly observed problems. The therapists providing this level of care receive specialized training to meet the needs of the PwP within a proactive care model. They also assist participants with scheduling return appointments at the 6-12 month period, with the initial visit being scheduled by a specialty trained administrative coordinator.
Results: The proactive program was implemented in 2016 for PT only with 28 patients. It expanded to OT and SLP in 2018 with 77 total patients seen across disciplines. The proactive model has since expanded from 1 to 3 outpatient clinics and increased the number of providers in the organization. Proactive PT has grown to over 550 cumulative PwP, or approximately 100 per year in recent years. Approximately 50% of PwP seen each year are return visits. Proactive OT and SLP programs grew, but continue to have lower utilization than Proactive PT. In 2025, there were 138 PwP referred to the proactive program, with 108 scheduled across disciplines.
Conclusion: Proactive care is an evidence-based approach that allows PwP to address potential symptoms and functional changes early after diagnosis. Proactive care can optimize quality of life and exercise participation. This care model is feasible in the outpatient setting with PT, OT, and SLP.
P25.16
1 Ulster University, United Kingdom
Evidence suggests that smart speakers, such as Alexa, encourage increased vocal effort, loudness, and clarity; goals aligned with Lee Silverman Voice Treatment. Some speech and language therapists (SaLT’s) have begun integrating smart speakers into therapy for individuals with dysarthria, with improvements in volume and intelligibility. Therefore, we sought to understand facilitators and barriers to using smart speakers from the perspectives of people with Parkinson’s, carers and speech and language therapists and co-produce solutions to support the therapeutic use of smart speakers for speech and voice difficulties.
Focus groups (n=6) and interviews (n=2) were conducted with people with Parkinson’s, carers and SaLT’s who were already using smart speakers with a speech and voice difficulty and analysed using framework analysis. Results informed six problem statements, which were considered across online co-design workshops, with people living with Parkinson’s, carers, SaLT’s, charity representatives and technology and design experts.
Focus groups yielded a range of facilitators and barriers. Key themes encompassing included smart speakers as a potential driver of positive speech therapy outcomes, concerns about privacy and confidentiality, usability challenges, support needs in knowledge and education and developing an Alexa Skill for speech therapy. Two prototypes were developed in response to solving barriers identified in focus groups: education and guidance addressing privacy, troubleshooting, delivery considerations, and therapeutic usage guides for people with Parkinson’s and SaLTs with catalogues of standard features which can be adapted for therapy, and speech therapy specific smart speaker features including creating an Alexa skill that supports Lee Silverman Voice Treatment, AI integration for conversation, increased feedback and improved privacy. Collaborators reported feeling valued and appreciated the balance of perspectives.
This study generates smart speaker intervention prototypes to aid its integration into speech and language therapy practice. Future work is required to clinically test the impact of using smart speakers to improve volume and intelligibility for people with Parkinson’s in a large-scale study.
P25.17
1 University Hospitals of Derby and Burton NHS Foundation Trust, United Kingdom
2 Derbyshire Community Health Services NHS Foundation Trust, United Kingdom
3 Beautiful Voice Limited, United Kingdom
Background Approximately 10 million people worldwide are living with Parkinson’s. Over 90% of people with Parkinson’s (PwP) experience speech and language difficulties during the course of their illness. These challenges often include reduced vocal loudness and monotone voice, slurred or imprecise articulation, altered speech rate, and difficulties with working memory and word retrieval. Such impairments are closely linked to increased care costs, reduced confidence and independence, and diminished wellbeing.
Research demonstrates that high-intensity, high-frequency speech and language therapy leads to both short- and long-term improvements in communication for PwP. However, the global shortage of Speech and Language therapists (SLTs) severely restricts access to therapy, resulting in long waiting lists and suboptimal outcomes.
Developing a digital therapy platform offers an opportunity to increase therapy dosage, accessibility, and SLT efficiency. This project engaged PwPs and clinicians to explore the opportunities and challenges associated with using digital technology to support speech and language therapy.
Research questions
Can SLTs use a digital platform to deliver speech and language therapy? What effects does digital speech and language therapy have on clinicians, PwP and the NHS?
Methods In phase 1, PwP and caregivers were recruited for co-design workshops, where user feedback and feature mock-ups were discussed. This was followed by a pilot evaluation, where SLTs from the NHS services used a digital platform to provide therapy to PwPs. SLTs prescribed personalised exercises for self-practice at home via the platform, which also captured PwP adherence and voice metrics during the practice. Oromotor and Voice Handicap Index assessments were conducted at the beginning and end of the therapy period.
Findings Preliminary results from 25 sessions indicate strong support from clinicians and PwPs for using the platform to enhance therapy access. Participants highlighted the platform’s potential to increase therapy dosage, promote self-management and knowledge sharing, and enable remote monitoring and feedback to clinicians. Key requirements, benefits, challenges and proposed clinical pathway are being summarised to be presented at the conference.
Discussion Based on user feedback, the platform will be further improved and undergo a randomised controlled trial to investigate its effectiveness in improving voice and speech symptoms and cost saving for the NHS.

P25.18
1 The University of Texas at San Antonio, Health Science Center, United States
2 Northwestern University, United States
Introduction: Postural instability is a hallmark motor symptom in Parkinson’s disease (PD) and a major contributor to falls. Non-motor symptoms such as cognitive impairment are associated with postural instability and an increased risk of fall. Aerobic exercise training is an intervention that can increase cardiovascular fitness and improve motor symptoms and cognition in individuals with PD. When aerobic exercise is combined with targeted cognitive-motor rehabilitation such as virtual reality (VR)-based training, it could produce additive effects and potentially reduce the risk of falls. This pilot study investigated the effects of exercise training followed by VR games on balance and cognition in PD.
Methods: Individuals with PD were randomized to high-intensity interval training (HIIT) and VR games (HIIT-VR, n=8) or stretching and VR games (St-VR, n=7). The HIIT-VR group performed 30 minutes of exercise (intervals at >80% heart rate maximum) on a recumbent stepper before 30 minutes of VR games thrice per week for 8 weeks. The dose-matched St-VR group performed whole-body stretches prior to VR games. Outcomes were obtained at baseline, post-intervention, and 6-week follow-up. The primary outcome was the mini-Balance Evaluation Systems Test (miniBESTest). Secondary outcomes included 6-minute walk distance (6MWD), postural sway, PD-cognition rating scale, spatiotemporal measures of gait during single and dual task conditions and quality of life.
Results: Fifteen individuals [mean ± SD age: 68.1 ± 10.5 years, Hoehn and Yahr stages 2-3] participated in this study. Significant group-by-time interactions were observed for the miniBESTest [F(1.3, 16.9) = 5.36, p = 0.02] and 6MWD [F(2, 26) = 5.7, p = 0.009]. The HIIT-VR group showed greater change in the miniBESTest (6.3 points, 95% CI 0.6, 12) and 6MWD (141.3 m, 95% CI 7.5, 275) compared to the St-VR group at post assessment. There were no differences between groups in measures of postural sway, cognition, gait, and quality of life.
Conclusion: Our findings show that combining HIIT with VR-based training appears to elicit meaningful gains in balance and endurance, suggesting that it may facilitate motor learning and improve rehabilitative outcomes in PD. It is plausible that increased cardiorespiratory fitness in the HIIT-VR group facilitated neuromotor control, improving balance. Larger controlled studies are needed to evaluate long-term effects and identify the underlying neurobiological mechanisms.
P25.19
1 University Leuven (KU Leuven), Belgium
2 KU Leuven, Department of Rehabilitation Sciences, Belgium
3 Department of Neurology, University Hospitals Leuven, Belgium
Turning in place (TIP) is the most common trigger for freezing of gait (FOG) in people with Parkinson's disease (pwPD) due to high demands on gait adaptation and dynamic balance. Although split-belt treadmill (SBT) training improves gait adaptation in pwPD, these benefits have not transferred to overground turning nor been related to improved FOG at home. This double-blind RCT investigates whether SBT combined with overground gait adaptation exercises (SBT+) can reduce FOG during TIP at home compared to SBT with seated upper limb training (SBT-).
28 pwPD with daily FOG were randomly assigned to SBT+ or SBT-. Training occurred twice weekly for 1 h over four weeks. Assessments included a standardized home-based protocol with TIP under single- (ST) and dual-task (DT) conditions, performed ON medication at three time points: pre-, post-intervention, and retention (6 weeks). All sessions were video-recorded, and FOG severity was quantified via gold-standard annotation. As the trial is ongoing, results are reported for within-group changes over time in the pooled groups (N = 12). Primary and secondary outcomes were % time frozen (%TF) and #FOG, with tertiary outcomes UPDRS III, Mini-BESTest, and NFOGQ. Changes across time points were assessed with Friedman tests. Post-hoc analyses used Wilcoxon signed-rank tests with Bonferroni correction; effect sizes (ES) were calculated using Cohen’s d.
Figure 1a showed a small pre- to post-intervention improvement in %TF during ST, which was not maintained at retention (Friedman p=0.51, ES<0.2). #FOG showed a trend toward reduction in both ST and DT from pre to post-intervention (ES=0.23), without reaching significance (Friedman p=0.12 for ST, p=0.35 for DT). Self-reported FOG showed a modest, non-significant improvement (NFOGQ: Friedman p=0.15, ES=0.33). No change was observed in UPDRS III (Friedman p=0.9, ES=0.1). Mini-BESTest scores improved over time (Friedman p=0.04), with post-hoc gains from pre- to post-intervention (p=0.022, ES=0.84) and at retention (p=0.024; ES=0.80), indicating meaningful balance improvements.
Regardless of training type, SBT appears to enhance balance in pwPD with FOG and may reduce self-reported FOG in some. While the final analysis will include all participants, the limited interim sample warrants cautious interpretation. Nonetheless, these preliminary findings suggest SBT may yield meaningful improvements in FOG and balance, helping people with FOG better manage daily mobility.
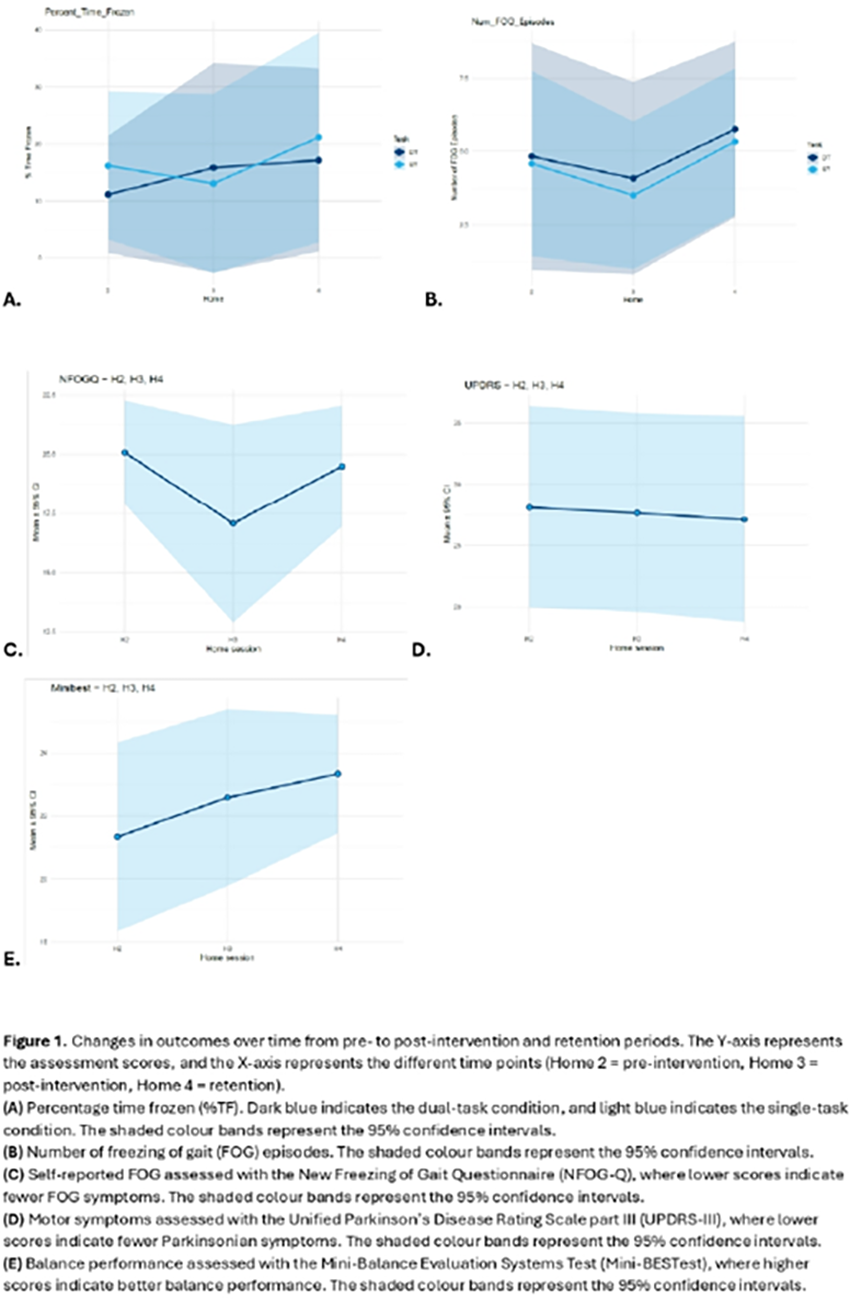
P25.20
1 Robert Gordon University, United Kingdom
2 Augusta University, United States
Background: Clinical guidelines recommend referral to Occupational Therapy (OT) for people with Parkinson’s (PwP). While the potential role of OT in Parkinson’s care has been described, there is limited evidence on the specific treatment and management approaches adopted in practice, and little is known about the availability of OTs with expertise in Parkinson’s. Understanding current practice and workforce demands is essential to inform undergraduate and postgraduate education, ensuring equitable, high-quality care for PwP regardless of geographical location.
Aim: To investigate current OT management of PwP, confidence in delivering Parkinson’s-specific interventions, and the geographic availability of OTs across two international contexts.
Methods: A cross-sectional survey was conducted of OT practicing in Scotland and Georgia, USA. The survey included closed and open-ended questions exploring the range and type of interventions and outcome measures used with PwP, and OT’s confidence in managing PwP.
Results: All analyses and reporting will be completed by December 2025 and will be presented in full at the World Parkinson Congress. Preliminary analysis suggests variation in the type of OT interventions that are delivered between OTP’s practicing in Scotland and Georgia, including frequency and intensity OT services. Within Georgia, OTPs deliver more hands-on based forms of rehabilitation, whereas self-management and education were more utilized among OTPs from Scotland. Similarities also arise, such as a focus on a holistic view of the person and needs.
Conclusions: This study provides new insight into current OT service provision for PwP, highlighting both between and within country differences and similaries in the delivery of OT. Findings demonstrate gaps in practice and serve to inform opportunities for shared learning between Scotland and Georgia, and clarify OTPs’ confidence in managing PwP. The results will inform curriculum development in Scotland and Georgia and may be applicable to other geographical contexts supporting improvements in the quality of care delivered to the Parkinson’s community.
P25.21
1 Parkinson Caracas Civil Association, Venezuela
2 Valencian International University, Spain
3 BonMed Clinic, Chile
4 Santo Tomás University, Chile
5 Valparaiso University, Chile
Background: The symptomatology of Parkinson's Disease (PD) includes hypophonia, dysprosody, and significant limitations in expression, which negatively affect the caregiver's comprehension of messages, particularly in face-to-face conversation with People with Parkinson’s (PwP). There is a notable absence of data collection instruments specifically designed to ascertain how voice, speech, and language alterations, collectively referred to as Communication Disorders (CDs), impact their caregivers' burden. Therefore, it is essential to develop and validate a questionnaire to measure this specific type of impact.
Objective: To design and validate a questionnaire aimed at evaluating the negative impact or effect of CDs caused by PD on the quality of communication between PwP and their Informal Caregivers (ICs). Furthermore, the study seeks to analyze the burden experienced by ICs and the potential risk of CDs in PwP generating caregiver overload in ICs.
Methods: The development and validation of the Caregiver Impact of Communication Disorders in Parkinson's Questionnaire was conducted in Spain. The questionnaire's development involved four versions, the final of which comprised 20 items divided into three dimensions: Identification of CDs in PwP; Impact of CDs on PwP's Communication Quality; and Impact of CDs on Caregiver Burden. The questionnaire was evaluated by a nine-specialist expert panel and was applied to 30 informal caregivers along with the Zarit Burden Interview as a reference instrument for assessing caregiver overload. This evaluation confirmed content validity, construct validity, and the verification of internal consistency.
Results: The questionnaire demonstrated a high level of agreement among the expert panel, as well as adequate internal consistency and reliability (α=0.8). The provisional results from its application to the sample of informal caregivers suggest robust construct validity and appear to support its content validity. This is evidenced by significant correlations with the reference instrument, which increases confidence for further validation.
Conclusion: The questionnaire appears to be a scientifically rigorous instrument and a practical, accessible tool suitable for assessing the impact of CDs on PwP and their caregivers. A satisfactory validation outcome would position it as a valuable resource for healthcare professionals and researchers aiming to accurately evaluate the impact of CDs and caregiver overload in PD caregivers.
P25.22
1 UF Health Rehab Center - Norman Fixel Institute for Neurological Diseases, United States
Introduction: Interdisciplinary care is the gold standard for treatment of people with Parkinson’s disease (PwP) throughout the disease progression, including PT, OT and SLP. Appointments with neuro-rehab specialists are more widely recommended at onset of diagnosis, prior to functional limitations, for the purposes of education and functional maintenance programs. Deep brain stimulation (DBS) is a surgical procedure used more frequently for PwP at varying points in disease progression. PwP seek DBS for management of tremors, rigidity, bradykinesia, dystonia, dyskinesia and motor fluctuations. DBS can improve motor symptoms, but has the potential to have surgical and stimulation-induced side effects. Given the potential for surgical risks and benefits, identifying individuals who present as “good candidates” is multifactorial and includes consideration of social support cognition, balance, swallowing capabilities and more. Standard of care consists of neurology, neurosurgery, and in some cases neuropsychology, appointments pre- and post-DBS. However, consultation by PT, OT and SLP adds increased education, use of objective assessments pre- and post-DBS, increased interdisciplinary care communication and, ultimately, the potential to improve patient outcomes. Currently, there is limited information on the benefits of incorporating rehabilitation into a surgical process. Organizing the layout of a well-established program will assist other medical centers to incorporate rehabilitation into the DBS process for candidacy consideration. Receiving feedback from established neurologists and neurosurgeons will illustrate the pros and cons of incorporating rehabilitation during the DBS consideration.
Methods: Identify important outcome measures performed by PT, OT and SLP to establish baselines and assess for change pre- and post-DBS. Case examples of individuals’ scores will be incorporated to demonstrate the impact rehab can have pre- and post- DBS. Gather information from neurologists, neurosurgeons, PwP and rehabilitation staff on the pros and cons of an interdisciplinary model for all people undergoing DBS surgery. Illustrate the time frame that has demonstrated success with incorporating rehabilitation appointments alongside neurology appointments pre- and post- DBS.
Goals for the program: Create a multidisciplinary clinic framework for other medical centers to replicate to promote improved patient outcomes and expectations for DBS programs.
P25.23
1 Universidade Federal de Minas Gerais, Brazil
2 University of Nevada, United States
Introduction: Although canes are commonly used by individuals with Parkinson's disease (PD), the effects of assistive devices on gait in this population remain poorly understood. Previous studies have primarily focused on the immediate effects of device use, without considering the need for repetitive practice for motor learning. Moreover, these studies have emphasized gait-related variables measured in clinical tests, overlooking patient-centered outcomes. Finally, methodological limitations, such as the lack of randomization and insufficient reporting of clinical characteristics, compromise the internal and external validity of the results. The objective of this study was to investigate the effect of cane training and use on gait speed (primary outcome), cadence, step length, gait confidence and fear of falls (secondary outcomes) in individuals with PD. Methods: These data come from an ongoing randomized clinical trial (NCT06950255/CAAE: 75158123.2.0000.5149). Individuals with PD were randomly divided into two groups: (1)experimental group (EG) – cane training and use; and (2)control group (CG) – stretching and health education. The intervention consisted of four, 40-minute sessions delivered over 15 to 22 days. Individuals were evaluated at baseline and after training sessions. Data were analyzed using repeated-measures ANOVA with an intention-to-treat approach. Results: A total of 26 individuals were included, 13 in each group. A significant group × time interaction was observed for gait speed (EG: pre 0.70 ± 0.32 m/s, post 1.00 ± 0.37 m/s; CG:pre 0.61 ± 0.19 m/s, post 0.70 ± 0.23 m/s; p = 0.017) and cadence (EG: pre 1.43 ± 0.32 steps/s, post 1.71 ± 0.36 steps/s; CG: pre 1.33 ± 0.26 steps/s, post 1.38 ± 0.25 steps/s; p = 0.015) indicating greater improvement in the EG . No significant differences were found between groups for the remaining outcomes, including, step length (EG: pre 0.47 ± 0.15 m, post 0.56±0.15 m; CG: pre 0.44 ± 0.10 m, post 0.49 ± 0.11 m; p = 0.152), gait confidence (EG: pre 61.69 ± 24.25, post 68.15 ± 20.89; CG: pre 66.30 ± 15.81, post 63.23 ± 15.54), and fear of falling (EG: pre 36.76 ± 15.83, post 32.00 ± 11.25; CG: pre 30.74, post 31.23 ± 10.00). Conclusions and implications: Cane training and use provided significant improvements in gait speed and cadence, indicating that structured practice enhances device-assisted mobility in individuals with PD. These findings should be interpreted with caution until the study is completed.
P25.24
1 Universidade Federal de Minas Gerais, Brazil
2 University of Nevada, United States
Introduction: Prescribing canes is commonly used to enhance mobility in persons with Parkinson’s disease (PwPD). However, few studies have examined the effects of cane use on mobility, and evidence is limited by methodological issues. To our knowledge, no previous studies that explored patients’ perceptions have been published, despite the importance of patient-centered care. Furthermore, individuals with varying functional levels may respond differently to assistive devices. The objective of this study was to investigate the immediate effects and perceptions of cane use on mobility outcomes in PwPD according to gait speed subgroup (G1: gait speed ≤1.1 m/s and G2: gait speed >1.1 m/s). Methods: Secondary data from an ongoing clinical trial were analyzed. PwPD, naive to assistive devices, ≥40 years of age, stable on medication, able to walk independently, and able to use a single-point cane were included. Participants received five minutes of cane instruction and were assessed under randomized conditions (with and without a cane) using the 10-meter walk test (10MWT) and Timed Up and Go (TUG) test. Participants reported perceived changes and need for the device. Results: A total of 50 PwPD were included, 25 in each group (64 ± 9 years, 34 males, 16 females). A significant condition × group interaction was observed for gait speed (p=0.049). Bonferroni-adjusted post hoc analyses showed that cane use significantly reduced gait speed in G2 (without cane: 1.30±0.16; with cane: 0.97±0.31; p≤0.001), while it had no significant effect in G1 (without cane: 0.93±0.18, with cane: 0.77±0.26, p=0.019,). Cane use worsened TUG performance in both groups (p≤0.001), with no significant condition × group interaction (p=0.101). After testing, participants reported perceived benefits, including improved gait (G1: 40%; G2: 24%) and reduced fear of falling (G1: 36%; G2: 28%), with no significant differences between groups (p=0.148 and p=0.839). In G1, perceived need to use a cane increased from 16% pre-testing to 36% post-testing, showing a trend toward a greater change (p=0.059), while in G2, perceived need did not change (24% to 28%, p=0.564). Conclusions and implications: Participants with slower gait speeds reported more positive perceptions and showed no significant gait speed declines with immediate cane use, suggesting that this subgroup may be particularly likely to benefit from cane prescription following adequate training.
P25.25
1 Arizona State University, United States
Introduction: Falls are a major cause of injuries, economic burden, and reduced quality of life among people with Parkinson’s disease (PD). People with PD often exhibit impaired balance control, which substantially increases their fall risk. One effective way to prevent falls is to utilize compensatory stepping responses to regain stability after a balance loss. While most previous studies have focused on anterior or posterior balance perturbations, such as slips or trips, stepping response during lateral balance loss remains relatively understudied. The present study aimed to characterize stepping strategies during lateral perturbations in people with PD and to examine how these strategies change following an 8-week balance training program.
Methods: Thirty-one individuals with PD completed four experimental sessions: two baseline assessments (B1 & B2) prior to and two post-training assessments (P1 & P2) after an 8-week balance training program. During each session, participants experienced six lateral balance perturbations (three per side) on a treadmill while secured in a safety harness. Step strategies were classified as no-cross, front-cross, or back-cross, depending on whether and how the stepping foot crossed the stance leg. A fall was defined when the force applied to the harness exceeded 10% of the participant’s body weight. Stepping strategy frequency and fall rate were compared between specific sessions using the Wilcoxon signed-rank tests to examine the effects of exposure to a perturbation (B1 vs. B2) and balance training (B2 vs. P1), and retention of training effects (B2 vs. P2).
Results: Stepping strategy frequencies did not significantly differ between sessions. However, fall rate was significantly decreased following balance training. Specifically, people with PD showed a significantly lower fall rate in P1 and P2 compared to B2 (p = 0.04 and 0.03). No significant differences were found between other pairs of sessions.
Conclusions: Although people with PD chose consistent stepping strategies across sessions, they demonstrated fewer falls after training, and this improvement was retained. These findings suggest that balance training enhances stability in people with PD without altering their stepping patterns.

P25.26
1 Northern Arizona University, United States
2 Idaho State University, United States
Background: Cognitive-motor interference during gait is a hallmark of Parkinson’s disease (PD) and contributes to falls. Traditional single-task gait measures may underestimate mobility limitations in complex environments.
Objectives: To determine whether a visual Stroop task with the 10-Meter Walk Test (10MWT) detects dual-task deficits in PD and to evaluate its reliability and validity against established measures.
Methods: Twenty persons with PD (PwP), 19 healthy older adults, and 21 young adults completed the 10MWT, Standing Stroop, Stroop-enhanced 10MWT, and Timed Up and Go with cognitive task (TUG-cog). Completion times, Stroop errors, and dual-task costs were analyzed. Reliability was assessed using Cronbach’s alpha and intraclass correlation coefficients (ICC).
Results: Groups did not differ on single-task 10MWT or Standing Stroop. However, PwP were significantly slower and committed more Stroop errors than older adults on the Stroop-enhanced 10MWT (p = .036 and p = .009, respectively). Within PwP, Stroop-10MWT performance was worse than TUG-cog (p = .041). Dual-task costs were greater for gait than for cognition (p < .001). The Stroop-10MWT showed high internal consistency (α = .982) and excellent test–retest reliability (ICC = .953).
Conclusions: The Stroop-enhanced 10MWT exposes dual-task gait impairments in PwP not evident on single-task or simpler dual-task measures. Its strong psychometric properties support its use as a reliable tool for detecting cognitive-motor interference and informing rehabilitation strategies in PD.
P25.27
1 University of São Paulo, Brazil
Background: Gait impairment is one of the most disabling symptoms of Parkinson’s disease (PD), contributing directly to falls, loss of independence, and reduced quality of life. A key factor behind these problems is the decline in gait automaticity, the ability to walk with minimal attentional control. When automaticity deteriorates, patients must consciously focus on walking, increasing dual-task interference and fall risk. Identifying clinical predictors of this decline is crucial for early intervention and rehabilitation planning. The Montreal Cognitive Assessment (MoCA) is widely used for global cognition screening, but its ability to predict gait automaticity loss remains unclear. Objective: To examine whether MoCA scores predict gait performance during dual-task (DT) conditions in people with PD. Methods: This cross-sectional study followed STROBE guidelines. Thirty-seven participants with idiopathic PD (17 women, 20 men; mean age 59.9 ± 8.4 years; H&Y 1–3) were recruited via the Rede AMPARO network (amparo.numec.prp.usp.br). Cognitive performance was assessed with the MoCA, and gait parameters were recorded using the GAITRite® walkway. Participants completed 10 randomized trials under three conditions: (1) single motor (walking), (2) single cognitive (verbal fluency), and (3) DT (walking + verbal fluency). Linear regression and ROC analyses tested the predictive power of MoCA scores. This study was approved by the research ethics committee under protocol number CAEE 67388816.2.0000.0065 and was produced as part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by grant #2025/02885-7, #2025/14403-7. #2024/16868-4. Results: Total MoCA scores showed moderate correlations with step length (r = 0.41, p = 0.012) and stance time (r = −0.36, p = 0.024), but none remained significant after Bonferroni correction (adjusted p > 0.05). ROC analysis revealed poor predictive accuracy (AUC = 0.61, 95% CI = 0.47–0.73, p = 0.19). No MoCA subdomain correlated with DT gait cost. Conclusion: MoCA did not predict gait performance under DT conditions in PD. This finding highlights that global cognitive screening alone cannot identify patients at risk for reduced automaticity and falls. More sensitive, domain-specific cognitive–motor tools are needed to detect early functional decline and guide preventive, individualized rehabilitation strategies in PD.
P25.28
1 University of São Paulo, Brazil
2 State University of Southwest Bahia, Brazil
3 University of São Paulo, Ribeirão Preto, Brazil
4 Federal University of Bahia, Brazil
Background: Postural instability is classically described as a mid- to late-stage symptom of Parkinson’s disease (PD), typically marking the transition from Hoehn & Yahr (H&Y) stage II to III. However, subtle changes in balance control may occur earlier, increasing fall risk and functional dependence before they become clinically apparent. Identifying these early alterations is crucial for preventing falls and preserving quality of life through timely intervention.Objective: To determine whether postural control deficits can be detected from the earliest stages of PD, even when clinical balance tests still fail to differentiate between stages I and II. Methods: Fifty-five individuals with idiopathic PD (37 men; H&Y I = 11, II = 23, III = 21) were recruited through the Rede AMPARO network. Participants completed standard clinical balance tests—the Timed Up and Go (TUG), Balance Evaluation Systems Test (BESTest), and MDS-UPDRS pull test—and a 30-second quiet-stance task analyzed by a bidimensional kinematic method to compute a Postural Instability Index (PII). Group differences were analyzed using one-way ANOVA and Kruskal–Wallis tests with post-hoc comparisons (p < 0.05). Results: While clinical tests detected balance deterioration only from stage II to III (p < 0.01), the kinematic analysis identified significant differences already between stages I and II (p = 0.006), and progressively across all three stages (I vs III, p < 0.0001; II vs III, p = 0.02). These findings demonstrate that subtle postural control alterations are present even when traditional clinical measures still indicate preserved balance. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, CAPES, Brazil #88882.377008/2019-01), National Council of Technological and Scientific Development, CNPq, Brazil (Grants: 307828/2018-2/ 303359/2022-6) and was produced as part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by FAPESP grant #2025/02885-7 and #2025/14403-7.Conclusion: Postural instability in PD begins earlier than traditionally recognized, emerging between the first and second stages of the disease. The detection of these early balance changes underscores the need for sensitive and accessible assessment tools in clinical practice to guide preventive and individualized rehabilitation strategies from the onset of PD, reducing fall risk and maintaining independence.
P25.29
1 Teachers College, Columbia University, United States
2 Purdue University, United States
3 Columbia University Irving Medical Center, United States
Introduction: Expiratory Muscle Strength Training (EMST) and Cough Skill Training (CST) have been shown to improve swallowing safety and cough effectiveness in Parkinson’s disease (PD). However, detraining occurs once treatment is discontinued. Maintenance programs designed to sustain this function remain largely unexamined. This interim analysis from an ongoing clinical trial assessed the feasibility of a 12-month maintenance treatment protocol (EMST + CST) in PD.
Methods: Participants completed four weeks of intensive EMST and CST followed by a 12-month maintenance protocol, which included monthly visits and home practice. Feasibility was defined by 1) dropout, 2) attendance, and 3) rescheduling rates. Descriptive statistics were used to summarize data.
Results: Fifty participants with PD (23 female; age in years: M = 71, SD = 7.98) completed at least 6 months of maintenance therapy. Of these, 20 participants completed the full 12-month protocol, 9 completed 6-11 months, and 21 withdrew from maintenance therapy prior to six months. Mean disease duration was 6.1 years (SD = 4.33), and disease severity ranged from H&Y stages 1-5, with a mean UPDRS Motor score of 30.26.
Among those who completed the 12-month protocol (n =20; mean MDS-UPDRS = 29.25), attendance rate averaged 93%, with 11 attending all visits and 9 missing 1-6 visits due to medical (n=4) or personal (n=5) reasons. The mean rescheduling rate was 67% (range: 25-92%).
For those who completed 6-11 months (n=9; mean MDS-UPDRS = 30.78), attendance rate averaged 92%, with 5 attending all visits and 4 missing 1-2 visits due to medical (n=1) or personal reasons (n=3). The mean rescheduling rate was 75% (range: 17-100%).
The drop-out rate was 42% (n=21; mean MDS-UPDRS = 31.0) with withdrawals occurring throughout the maintenance phase: nine during months 1-3, three during months 4-6, four at the completion of the 6-month assessment, four during months 7-9, and one during months 10-12. Withdrawals were due to medical reasons (n =7), personal events (n=11) and study funding freezes (n=3).
Conclusions: These findings align with prior reports of variable long-term exercise adherence in PD. While this maintenance treatment was achievable across a range of disease severities (predominantly mild), long-term adherence was a barrier for some and was impeded by personal and disease-related events. Future analyses will explore factors influencing engagement, adherence, and outcomes with maintenance treatment.
P25.30
1 University of São Paulo, Brazil
BACKGROUND: Dual-task (DT) interference - simultaneous motor and cognitive task performance - disrupts gait automaticity and increases fall risk in Parkinson’s disease (PD). Understanding these effects across disease stages is essential for early rehabilitation strategies. PURPOSE: To investigate the impact of DT conditions on gait and cognitive performance across different stages of PD. METHODS: A cross-sectional study was conducted with 49 individuals with idiopathic PD (mean age = 61.1 ± 9.7 years; H&Y stages 1–3). Participants had a mean education of 17.5 ± 6.2 years, MoCA total score of 23.8 ± 3.5, depression score of 6.3 ± 3.7, and UPDRS-III mean score of 28.1 ± 14.8. Inclusion criteria: idiopathic PD (confirmed by a neurologist), use of dopaminergic medication, ability to walk short distances without assistive devices, and no diagnosis of dementia. Exclusion criteria: other neurological, cardiovascular/respiratory or orthopedic conditions, uncorrected visual or auditory impairments, and inability to perform verbal fluency tasks. Gait was assessed using the GAITRite® system under two randomized conditions: single-task (ST, walking only) and dual-task (DT, walking + verbal fluency task). Spatiotemporal gait parameters and the number of words produced were analyzed using two-way repeated-measures ANOVA (condition×stage), followed by Tukey post-hoc tests (α=0.05). (Ethical approval CAAE 67388816.2.0000.0065). This study was part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by grant #2025/02885-7, #2025/14403-7, #2024/16868-4. RESULTS: No interaction between condition and stage was found (p > 0.05), but significant main effects were observed for both factors. Compared with ST, DT produced reduced gait velocity, shorter step and stride length, longer double-support time, and shorter single-support time (p < 0.001). Participants in stages 2 and 3 showed overall slower and less stable gait than those in stage 1 (p < 0.05). The cognitive task performance (number of words generated) remained unchanged across conditions and stages (p > 0.05). CONCLUSION: DT conditions impair gait from early PD stages, indicating early loss of automaticity despite preserved cognition. Findings support incorporating DT gait training to enhance motor performance and reduce fall risk in daily life.
P25.31
1 Northwell Health, United States
Objective: To demonstrate the ability to improve vocal volume and improve perceived disability and quality of life in Parkinson’s disease (PD) patients at the unstructured conversational level during a 2-week in-patient multimodal intensive neurorehabilitation and care (i-MINC) stay.
Background: SPEAK OUT!® Therapy Program is a 12-week vocal intensity training program with maintenance via group treatment to improve vocal volume and intelligibility consisting of 40-minute sessions, 3 times weekly with home practice twice daily required. This was modified for use during a 2-week acute rehabilitative stay. Expiratory muscle strength training (EMST) has been shown to significantly improve vocal volume in people with PD over a 5-week period.
Methods: 323 moderately advanced PD patients who were able to complete Voice Handicap Index (VHI) scale and participate in the protocol were included in this study. SPEAK OUT!® program was modified for use during a 2-week i-MINC stay and performed once daily during 60-minute therapy session. EMST performed daily per protocol recommended by manufacturer during therapy session. Vocal volume was monitored for 330 patients during all tasks and during unstructured conversation utilizing a sound level meter. Both VHI and Vocal volume were evaluated on admission and discharge from the i-MINC program, and scores were analyzed using a T-test.
Results: The mean admission vocal volume was 51.98dB and increased to 58.0dB at discharge.
The mean VHI scores upon admission were 49.0 and decreased to 42.4. Both changes were extremely statistically significant (<0.001) for improvement utilizing the protocols during i-MINC.
Conclusion: This study highlights the effectiveness of utilizing EMST along with a modified and condensed SPEAK OUT!® program during an abbreviated i-MINC admission. The parallel improvement in Vocal Volume and VHI scores suggest that the protocols in place during i-MINC are effective in improving patient’s volume of voice as well as perception of disability and quality of life in a shortened time period. Future studies may focus on the efficacy of modification of current PD protocols to adapt for use during i-MINC.
References:
QR code
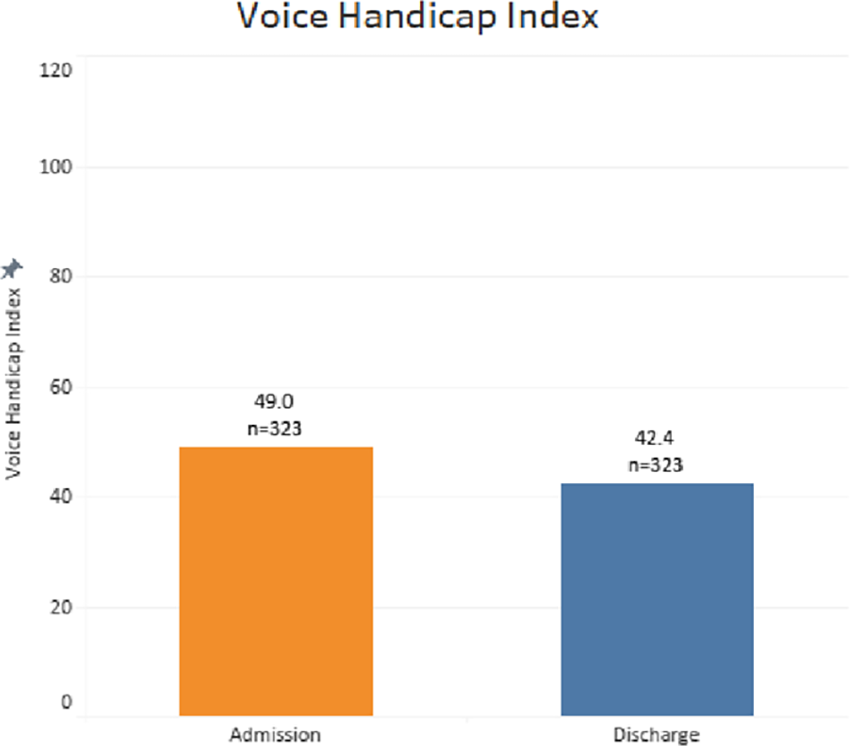
P25.32
1 School of Medicine of University of Sâo Paulo, Brazil
2 University of São Paulo, Brazil
Background: Gait impairments are among the main contributors to falls, reduced independence, and loss of autonomy in Parkinson’s disease (PD). While healthy older adults can adapt their walking pattern under cognitive load through compensatory strategies - such as increasing step time or adjusting stride length - people with PD may lose this adaptive capacity early in the disease course. Understanding these deficits is essential to prevent instability and functional decline before major mobility limitations occur. Objective: To compare gait performance under dual-task (DT) conditions between people with PD (PwPD) and healthy older adults (HOA) matched for age, cognition, and balance, highlighting how early loss of automatic control contributes to increased risk of falls and loss of independence. Methods: Thirty-six PwPD (H&Y stages 1–3) and 37 HOA, matched for demographic and cognitive variables, performed single-task walking, verbal fluency, and DT walking on a GAITRite® walkway. A 2×2 repeated-measures ANOVA (group × condition) analyzed spatial and temporal gait parameters (α = 0.05). This study was approved by the research ethics committee under protocol number CAEE 67388816.2.0000.0065. The study will be produced as part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by grants #2024/16868-4, #2025/14403-7 and #2025/02885-7. Results: Groups were similar in cognition and balance, yet significant group × condition interactions emerged for step time (F(1,55) = 4.84, p = 0.032), single support time (F(1,55) = 4.17, p = 0.046), and stride length (F(1,55) = 37.91, p < 0.001). During DT, HOA adopted adaptive strategies—slower and longer steps with shorter single support—to maintain stability. In contrast, PwPD failed to adjust gait parameters, indicating impaired automaticity and inability to compensate under cognitive stress. Conclusion: People with PD exhibit an early loss of gait automaticity, limiting their ability to use protective compensatory strategies when attention is divided. These deficits increase the risk of falls and threaten independence and autonomy in daily life. Early detection and targeted physiotherapy focused on restoring automaticity and adaptive motor control are crucial to prevent disability and preserve quality of life in PD.
P25.33
1 Teachers College, Columbia University, United States
2 Lang Lab, Program in Physical Therapy, Washington University School of Medicine, St Louis, MO, United States
3 Laboratory for the Study of Upper Airway Dysfunction, Teachers College, Columbia University, New York, NY, United States
4 Department of Neurology, Columbia University Irving Medical Center, New York, NY, United States
5 Neurorehabilitation Research Laboratory, Teachers College, Columbia University, New York, NY, United States
Purpose: Aspiration pneumonia and falls are primary causes of mortality and reduced quality of life in people with Parkinson’s disease (PwPD). These outcomes are driven by highly prevalent axial symptoms; airway protective deficits affect over 80%, while balance or mobility dysfunction contributes to falls in approximately 50% of PwPD. However, the interaction between these underlying axial symptoms is unclear, and understanding this relationship is crucial for developing integrated and proactive approaches to care. Therefore, this study aimed to determine if self-reported physical activity, fall risk, or balance confidence was associated with objective cough and swallowing deficits in PwPD.
Methods: PwPD completed objective airway protection assessments, including a videofluoroscopic swallowing study (VFSS) and cough testing. Primary outcomes were swallowing safety, measured by the Penetration-Aspiration Scale (PAS) across thin liquid trials (5, 10, 20, and 90mL), and cough strength, measured by peak expiratory flow rate (PEFR) for voluntary and reflex coughs. Participants also completed self-reported outcomes: the International Physical Activity Questionnaire, a 6-month fall history, and the Activities-specific Balance Confidence scale. Mixed-effects models evaluated predictors of cough strength and airway invasion, accounting for multiple trials and key covariates (e.g., disease severity). Alpha was set to .05.
Results: Participants (n=20, 7F, mean age 69.9y, mean UPDRS-III 30.6) showed only balance confidence was significantly associated with cough strength (β = 0.19, 95% CI: 0.05 – 0.32, p = .026) after controlling for all predictors and covariates. Physical activity (β = -0.37, p = .581), fall risk (β = 0.48, p = .581), and balance confidence (β = -0.25, p = .236) were not significantly associated with PAS scores.
Conclusions: This is the first study linking self-reported balance confidence with an objective measure of airway protection in PD. This finding suggests a linked trajectory of decline for axial functions, given that postural control and airway protection rely on common neural and motor systems disrupted by the disease. These results may encourage proactive interdisciplinary collaboration between dysphagia and mobility specialists. Future work should explore this relationship using objective balance measures and a larger, more diverse sample.
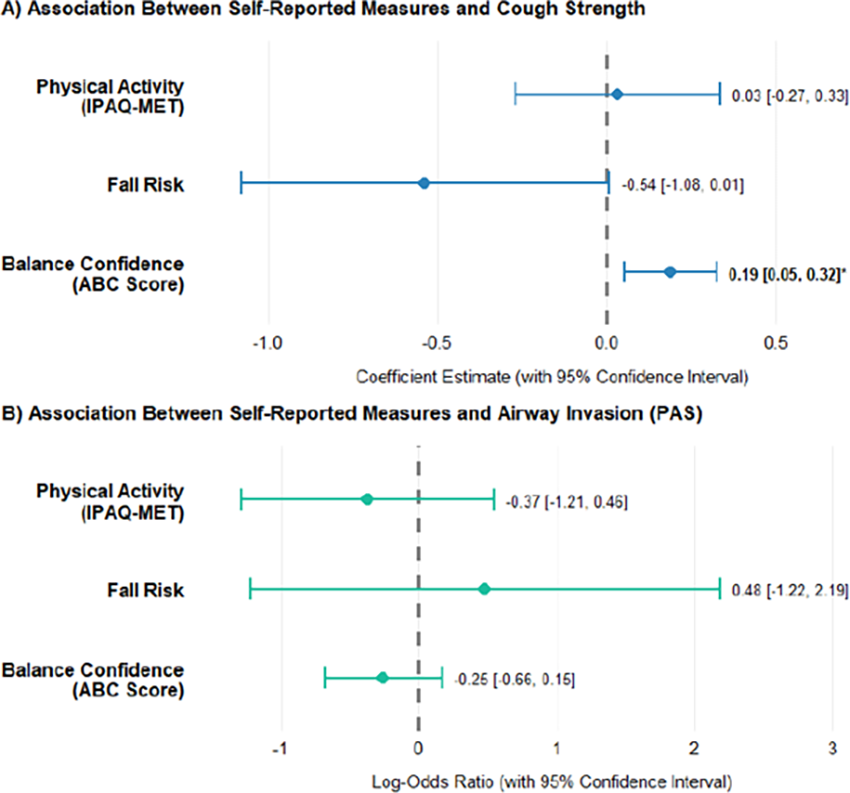
P25.34
1 Shirley Ryan AbilityLab, United States
2 Parkinson's Foundation, United States
3 ., United States
Introduction to the Program: In Fall 2023 we initiated phase 2 of the Parkinson’s Foundation Rehabilitation Medicine Initiative -- to facilitate the implementation of the consensus statement for delivering multidisciplinary rehabilitation care across the Parkinson’s Foundation Centers of Excellence through the development of written and electronic resources.
Methods: Four heterogeneous Parkinson’s Foundation Centers of Excellence were identified by the Foundation to voluntarily contribute to the Initiative: Northwestern University/Shirley Ryan AbilityLab, University of Utah, University of Michigan, University of Southern California. In March 2024, initial needs assessments were conducted with each site to understand barriers and facilitators to implementing the consensus statement and improve excellence of Parkinson’s care at their facility. All sites were then brought together in a learning collaborative to share identified program strengths and opportunities. Common needs across the Centers were identified, including better language and understanding of rehabilitation care pathways, and provision of rehab in acute care. We prioritized the implementation strategy of training and education through development of healthcare professional and patient-facing resources.
Results: There were eleven multisite subgroup meetings over twelve months for content development, review, and refinement. The finalized healthcare professional resources are: (1) rehabilitation care pathway overview, (2) proactive care pathway, (3) restorative care pathway, (4) supportive care pathway, and (5) rehabilitation while in the hospital. A final patient-facing resource outlines the different disciplines. Finalized resources were first disseminated at the Parkinson’s Disease Clinical Conference in September 2025. These resources are available for download on the Parkinson’s Foundation Rehabilitation Medicine Initiative webpage. Up to date download data will be shared.
Conclusion: A clinical learning collaborative can develop shared language and resources to align multidisciplinary rehabilitation care across the Parkinson’s Foundation Centers of Excellence and to health systems outside of the network. Future research can evaluate the effectiveness of this education-based dissemination strategy.
P25.35
1 Eastern Washington University, United States
Although 89% of patients with Parkinson’s experience speech and swallowing difficulties, only 3–4% receive speech therapy (Fullard, et al., 2017). Because people with Parkinson’s Disease (PwPD) face reduced mobility, motivation, transportation, and access to care, telehealth may increase therapy participation. Telepractice eliminates travel barriers, reduces caregiver burden, and enables family and friends to join sessions and home practice remotely.
The SPEAK OUT!® Therapy Program, developed by Parkinson Voice Project (PVP), helps people with Parkinson’s and related disorders regain and retain speech and swallowing. The program provides all therapy materials on the PVP website, allowing clinicians and patients to use them during therapy and homework. Its format lends itself well to telepractice.
This study surveyed SPEAK OUT!-trained Speech-Language Pathologists’ (SLPs) perceptions and use of telepractice for SPEAK OUT! service delivery to PwPD. The survey examined: 1) how many used telepractice; 2) SLPs’ confidence providing assessment and intervention remotely; and 3) whether telepractice was perceived as effective as in-person service.
Participants were recruited from PVP’s list of certified providers. The survey, hosted on SurveyMonkey.com and based on Swales et al. (2020), included 20 multiple-choice, sliding scale, yes/no, and 5-point Likert questions. Invitations were distributed via email, the PVP newsletter, and Facebook group. The survey was open for six weeks.
Ninety-two percent of respondents use telepractice. Ninety-four percent have provided SPEAK OUT! via telepractice for one to five years. Twenty-seven percent felt extremely confident and 39% very confident conducting assessments, while 42% felt extremely confident and 33% very confident providing intervention. Thirty-one percent strongly agreed, 28% agreed, and 25% disagreed that SPEAK OUT! via telepractice was as effective as in-person.
Results are promising: most clinicians felt confident and found telepractice effective. Because telepractice reduces barriers such as transportation, mobility, and provider access, more PwPD can receive needed therapy. Reducing access barriers and educating providers about telepractice can improve speech outcomes for this population.
P25.36
1 Washington University in St. Louis - School of Medicine, United States
2 Saint Louis University, United States
3 University of Nevada Las Vegas, United States
Background: More than half of people with Parkinson disease (PD) live with pain. Despite its high prevalence, little is known about pain-related fear and also how pain interferes with daily life activities in people with PD. The purpose of this study was three-fold: 1) to describe pain-related fear in PD, 2) to characterize the extent to which pain interferes with daily life in PD, and 3) to assess relationships between pain-related fear and pain interference in PD.
Methods: One-hundred fifty-one people with PD (mean age: 65.5 ± 11.3; 52.3% female; 91% Caucasian) completed the Survey of Treatment, Exercise, Participation, and Symptoms in PD (STEPS-PD). To assess pain-related fear, participants were asked to quantify the extent to which fear of pain and fear of pain from movement limited their ability to do the things they enjoyed with 0 being “not limiting” and 100 being “very limiting”. To assess pain interference, participants completed the PROMIS Pain Interference Short Form. To assess relationships between pain-related fear and pain interference, we conducted Spearman correlational analyses (α=0.05).
Results: Participants rated their average pain intensity over the last week (0 being no pain, 10 being the worst possible pain) at 5.1 ± 2.0. On average, fear of pain (general) was rated to be 37.3% ± 30.0% limiting. Fear of pain from movement was rated to be 35.8% ± 28.6% limiting to performing preferred activities. With respect to pain interference, 57.7% of respondents noted that pain at least somewhat interfered with their enjoyment of life. 76.3% of respondents noted that pain at least somewhat interfered with enjoyment of recreational activities. Also of note, 39.1% of respondents noted that pain at least “sometimes” kept them from socializing with others. General fear of pain was moderately to strongly related to pain interference as indicated by correlation coefficients between fear of pain and all PROMIS Pain Interference items ranging from 0.55 to 0.66 (all p<0.001).
Conclusions: People with PD experience fear of pain, which may impact their performance of preferred activities. Furthermore, pain appears to interfere with performance of recreational activities, socialization, and life enjoyment. Clinically, it is imperative that clinicians screen for and address pain and its associated fear in people with PD in an attempt to minimize pain interference in daily life.
P25.37
1 Univeristy at Buffalo, United States
2 Purdue University, United States
3 University of Arizona, United States
4 Medical University of South Carolina, United States
5 State University of New York at Cortland, United States
Background: Devices that elicit the Lombard Effect, like the SpeechVive device, have been found to be an effective treatment for increasing vocal intensity in persons with Parkinson Disease (PD). However, the long-term effectiveness of this device, and its impact on the respiratory mechanisms used for speech production have not been studied.
Objective: Assess the longitudinal impact of device use on vocal intensity and respiratory patterns supporting speech following device use in persons with PD.
Methods: 12 people with PD completed a two-week baseline period. Participants were instructed to wear the device 2-8 hours per day. Post-treatment data were collected one week after 8-weeks of device use. The device was withdrawn for 1 month to assess detraining effects. The participants then wore the device for 6 additional months. Respiratory inductance plethysmography captured ribcage and abdominal movements which were calibrated to estimate lung volume. A calibrated microphone signal was used to estimate mean sound pressure level (SPL). Data were collected during a monologue task, first with the device off and then with the device on. Linear mixed effects models were used to assess change over time and with device status (off/on) with alpha level set to p<0.05.
Results: SPL increased from pre (M=80.85 SD=4.87) to post (M=81.45 SD=8.49 p<0.001), decreased during detraining (M=79.82 SD=6.77 p<0.001), and increased six months later (M=83.01 SD=8.24 p<0.001). SPL was significantly higher with the device on than off at all time points (p<0.001). Lung volume initiation (LVI) and termination (LVT) decreased from pre (LVI: M=18.18 SD=16.34; LVT: M=0.37 SD=16.56) to post (LVI: M=15.76 SD=20.14 p=0.036; LVT: M=-2.86 SD=19.57 p=0.02), increased during the detraining month (LVI: M=21.69 SD=18.12 p<0.001; LVT: M=1.33 SD=18.08 p=0.06), and decreased six months later (LVI: M=19.32 SD=17.62 p=0.02; LVT: M=0.71 SD=17.90 p=0.08). Lung volume excursion (LVE) did not change significantly during the study. LVI, LVT, and LVE were not significantly different in the device off and on conditions.
Conclusion: The SpeechVive device is an effective long-term treatment approach in persons with PD. Data show a training effect of increased SPL at the end of 9 months. Respiratory patterns are close to baseline after 9 months; changes to patterns at 8 weeks are not maintained. This may be beneficial since using higher lung volume would be more efficient for speech production.
P25.38
1 ohsu-portland, United States
2 Oregon Health & Science University, United States
3 Oregon Health & Science Universit, United States
Introduction: Telerehabilitation is a viable option for people with Parkinson’s disease (PD). An increasingly common approach in rehabilitation is to incorporate dual-task (DT) training into physical therapy that involves gradually increasing the difficulty of simultaneous motor and cognitive tasks to improve mobility and cognition. It is unknown whether a person’s cognition plays a role in this approach for telerehabilitation. The hypothesis is that people with PD who have non-mild cognitive impairments (MCI) will undergo more DT training in telerehabilitation, resulting in greater improvements in DT mobility outcomes compared to those with MCI.
Objective: To evaluate the impact of cognitive status on the amount of DT exercises performed in the adapted Agility Boot Camp (ABC) for telerehabilitation (Tele-ABC) in people with PD.
Methods. This study is part of a larger randomized controlled trial called TelePD (NCT05680597). Preliminary data were analyzed from participants in the Tele-ABC program who underwent 12 sessions (60 min) of supervised ABC via videoconferencing (Tele-ABC). Exercises were progressed to add motor or cognitive DT to increase difficulty based on safety and quality of movement. People with (<26 score) and without (>25 score) MCI based on the Montreal Cognitive Assessment were assessed before and after the Tele-ABC intervention, with clinical mobility (Timed Up and Go (TUG) test) and objective mobility (e.g., gait speed) with Opal sensors with DT conditions. The amount of exercises performed with DT in each session throughout Tele-ABC was averaged for each group.
Results. Eight people with MCI and 21 without MCI with mild-to-moderate PD were analyzed. The non-MCI group performed significantly more DT progressions throughout 12 sessions than the MCI group (P=0.001). Clinical and objective mobility outcomes, such as DT-TUG (effect size=0.81) and DT-gait speed (effect size=0.72), showed significant and moderate-to-large effect sizes only for the non-MCI group. The MCI group showed non-significant and small effect sizes (effect size<0.25) for the outcome measures.
Conclusion. The preliminary data show that people with MCI perform less DT training, which may be one of the factors limiting their response to telerehabilitation on mobility measures. More studies should investigate whether more appropriate types of DT training could be used in telerehabilitation for people with PD and MCI.

P25.39
1 University of the Pacific, United States
PURPOSE: To evaluate recent literature to determine whether virtual reality (VR)-based physical therapy is more effective than conventional physical therapy in improving gait and balance in patients with Parkinson’s Disease (PD).
DESCRIPTION: This report critically appraises four randomized controlled trials investigating the use of VR in PD rehabilitation. All studies assessed functional outcomes such as the Berg Balance Scale (BBS), Dynamic Gait Index (DGI), and other mobility assessments. A study by Pazzaglia et al., 2020 reported significant improvements in BBS (VR group mean difference: 3.6 (1.3 to 5.9); conventional group mean difference: 0.8 (−1.3 to 2.9), p=0.003) and DGI scores (VR group mean difference: 1.6 (0.6 to 2.5); conventional group mean difference: −0.2 (−1.3 to 0.9), p=0.003) following VR-based therapy. Another study by Kashif et al., 2024 compared VR with motor imagery (MI) techniques, finding that VR—alone or combined with MI—led to better outcomes in BBS scores than MI or routine therapy alone (VR+RPT mean ±SD at 12 weeks: 50.10 ± 4.897; MI+RPT mean ± SD at 12 weeks: 47.45 ± 5.510; RPT alone mean ± SD at 12 weeks: 45.50 ± 4.559, p<0.001). Similarly, an earlier study by Kashif et al.,2022 showed improvements in BBS scores using VR technology (experimental group mean ± SD at 12 weeks: 51.36±2.83; control group mean ± SD at 12 weeks: 45.77±4.52, p<0.001). A study by Feng et al., 2019 showed that VR therapy significantly improved BBS (experimental group mean ±SD difference: 6.07±0.35; control group mean ±SD difference: 1.93±0.70, p<0.05) and other functional mobility scores compared to conventional therapy. The combined evidence indicates that VR-based therapy is more effective in improving gait and balance than conventional physical therapy.
SUMMARY OF USE: The findings across four recent studies support the use of VR as one intervention for improving balance and gait in persons with PD. VR therapy demonstrated statistically significant improvements in clinical measures, suggesting it as a valuable addition to traditional rehabilitation programs.
IMPORTANCE TO REHABILITATION PROFESSIONALS AND PEOPLE LIVING WITH PD: Clinicians may consider incorporating VR as its engaging format may enhance motivation and adherence, particularly those with travel limitations or reduced engagement with traditional therapies. Incorporating VR into clinical practice could expand therapeutic options and improve patient outcomes in neurorehabilitation.
P25.40
1 University of Keele, United Kingdom
Introduction Appropriate foot action is essential for balance and gait. In Parkinson’s, foot dystonia, an understudied phenomenon associated with young onset Parkinson’s but also reported more widely, can disrupt this. Understanding foot impairments is essential to physiotherapy management; however, physiotherapists’ knowledge and treatment of foot dystonia in Parkinson’s is unknown. Therefore, this study explored physiotherapists’ awareness of foot dystonia in Parkinson’s and current treatment strategies.
Methods Following ethical approval, members of a physiotherapy special interest group, who regularly treat Parkinson’s, were invited to complete an online questionnaire. Objectives: to ascertain physiotherapists’ awareness of foot dystonia in Parkinson’s, its’ impact on gait and identify related treatment strategies. Results were analysed using descriptive statistics and thematic analysis. Purposive sampling was used to select respondents with experience of treating foot dystonia in Parkinson’s. Semi-structured interviews explored their knowledge and treatment of foot dystonia in Parkinson’s in depth. Reflexive thematic analysis (two independent researchers) was used to analyse the interview transcripts.
Results The questionnaire had 57 respondents, with 37 (64.1%) aware of foot dystonia in Parkinson’s. Eleven related problems were identified: toe clawing; pain in the foot, calf or ankle; reduced ankle range of movement; ankle inversion; abnormal great toe; foot drop; reduced balance; increased muscle tone; foot stiffness; and gait abnormalities. Treatments included stretching, referral for botulinum toxin injection, ankle strengthening, and gait re-education. Interviews (n=7) identified four themes: knowledge of foot dystonia; impaired gait due to altered foot posture; foot dystonia assessment and treatment strategies. Foot dystonia was detected based on physiotherapists’ observation and assessment. Treatments included stretching, improving proprioceptive awareness, mobilisation of the foot, referral to podiatry, and use of orthotics and botulinum toxin. Participants highlighted a lack of literature and research on this topic.
Conclusion Approximately two thirds of experienced physiotherapists working with people living with Parkinson’s possessed some knowledge of foot dystonia, its’ presentation and impact on gait and balance. Physiotherapy treatments are used to address the problem, but their effectiveness needs to be studied further.
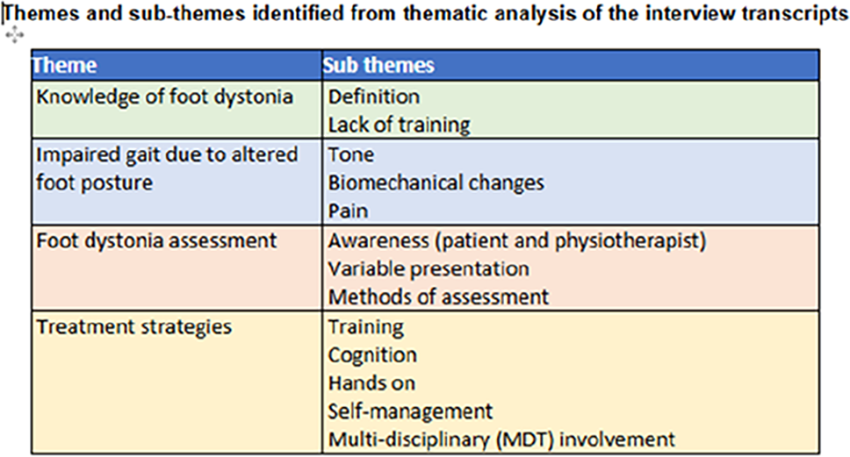
P25.41
1 Unión Parkison Bío Bïo, Chile
2 Universidad de Chile, Chile
Background Balance control relies on a distributed neural network within the central nervous system, which becomes compromised from the early stages of Parkinson’s disease (PD), affecting functional mobility. Physical exercise has been proposed as an effective intervention to improve balance in this population, although its underlying mechanisms remain unclear. This study compares the effects of a boxing-based balance and agility training (EBA-B), which simultaneously challenges multiple domains of postural control, with an active control (AC) of mobility and education, composed of simple movements that partially recruit the balance control network. It was hypothesized that a challenging, multidomain physical training would produce global improvements in balance compared to less demanding exercise programs.
Methods A randomized, crossover, controlled clinical trial was conducted with 22 individuals with PD. Participants were randomly assigned to the EF group (EBA-B first) or the EDU group (AC first), receiving both interventions for eight weeks each, separated by a three-week washout period. Assessments were performed in the ON medication state at the beginning and end of each intervention. A linear mixed-effects model was used to analyze the primary variables (MiniBESTest and FGA) and secondary variables (MDS-UPDRS III, PDQ-39, ABC, and mobility metrics obtained through inertial sensors).
Results EBA-B significantly improved balance (MiniBESTest, p < 0.001) and gait (FGA, p < 0.001), particularly in the domains of anticipatory postural adjustments (APA) and dynamic balance. It also reduced the severity of motor symptoms (MDS-UPDRS III, p < 0.001). The AC condition showed maintenance effects and specific improvements in dynamic balance during gait (p = 0.037).
Conclusions EBA-B produced global improvements in balance and motor symptoms, whereas AC impacted only specific domains of balance control. However, the effects of both interventions appear complementary, achieving better outcomes when combined and supporting the hypothesis that simultaneously challenging the distributed neural network of balance may offer greater functional benefits in PD.

P25.42
1 University of Nevada, Las Vegas, Nevada., United States
2 Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais., Brazil
3 Saint Louis University, St. Louis, Missouri., United States
4 Washington University in St. Louis, St. Louis, Missouri., United States
Introduction: Gait and balance treatment effectiveness in Parkinson’s disease (PD) is typically assessed through objective clinical measures. Yet, these treatments continue to be recommended without adequately considering how people with Parkinson’s disease (PwPD) perceive their effectiveness. Although various PD interventions have been studied, patients' perceptions of treatment effectiveness, particularly among those with and without a history of falls, remain unexplored. This study explores how PwPD perceive the effectiveness of different gait and balance treatments based on their fall history. Methods: This cross-sectional study assessed perceptions of treatment effectiveness for gait and balance interventions, based on fall history, recurrent falls, and injurious falls, through an online survey. The data were analyzed using descriptive statistics, the Mann-Whitney U tests, and the Chi-square tests. Results: Among 211 participants (mean age 67±9.5 years; 50.2% males), 53.6% reported at least one fall in the past year. Assistive devices had the highest overall perceived treatment effectiveness (78%), followed by community exercise programs (75%) and home exercise programs (68.5%). Significant differences in perceived treatment effectiveness were found between fallers (64%) and non-fallers (77%) for home exercise programs (p=0.013). Recurrent fallers (56%) rated home exercise programs lower than non-recurrent fallers (75%) (p<0.001). Injured fallers (50%) reported lower effectiveness for community exercise programs than non-injured fallers (72%) (p=0.026). A significant association was observed between injurious fall status and engagement in Physical Therapy (PT) intervention (p=0.037), indicating that individuals who experienced injurious falls were more likely to seek PT treatment. Conclusion and Implications: Fall history and recurrent falls negatively impacted perceived effectiveness of home exercise programs, whereas injured falls affected perceptions of community exercise program effectiveness. These perceptions can significantly impact patient adherence to intervention and should influence clinical decision-making. Our findings underscore the importance of patient-centered practices that incorporate patients' lived experiences with intervention effectiveness.
P25.43
1 George Fox University - Oregon Health and Science University, United States
2 Oregon Health & Science University, United States
3 George Fox University, United States
Introduction: Among chronic diseases, Parkinson’s Disease (PD) results in the most falls. Abnormal postural sway during standing is affected by PD. Lower limb control, especially the ankle, is crucial for maintaining balance and stabilizing gait, and it is significantly affected in PD. Research indicates that people with PD struggle with sensing and controlling the amplitude, timing, and coordination of agonist-antagonist muscles. These difficulties highlight motor and sensory challenges in achieving precise joint control over movement angles and forces. To date, no studies have investigated the precise control of the ankle in people with PD, and its effects on balance.
Objective: Investigate whether people with PD have difficulties learning to control precise ankle angles and forces, and to explore the effects of this ankle training on balance control.
Methods. Nine people with PD (Age=69±8, H&Y=2-3, MDS-UPDRSIII=34±12) and 7 Healthy controls (HC, Age=69±6), age-matched, have been recruited. Before and after the ankle training, we assessed balance using the Mobility Lab V2 system (APDM, Clario), in three conditions: 1) One foot, Eyes Open, Firm Surface, Trained side; 2) One foot, Eyes Open, Firm Surface, Untrained side; and 3) Feet together, Eyes Closed, Foam Surface. All the participants trained the foot with a larger sway area during the one-foot stance (from APDM). A custom-made device to control angle and force with the ankle was built, using an angle sensor (IMU mbientlab MMS) and one force sensor (load cell DYMH-103).Half of the trials show the participant’s performance, or knowledge of performance (KP), and the other half does not show the visual feedback (no KP). The participants were instructed to follow a sinusoid pattern continuously using the same inputs (angles and forces) and conditions (KP & noKP).
Results. People with PD had higher performance improvements controlling angles than HC with or without KP (p-values in Figure 1). Neither the PD nor the HC groups learned to control forces (KP or noKP). The ankle training increases the one-foot time with the trained side and the time in the feet together condition.
Conclusion. Our preliminary data suggest that people with PD can improve ankle motor learning (controlling angles) and that the ankle training improves the one-foot and feet-together standing balance control. Our plan is to increase the sample size, the number of training days, and to incorporate more objective gait and balance measures.
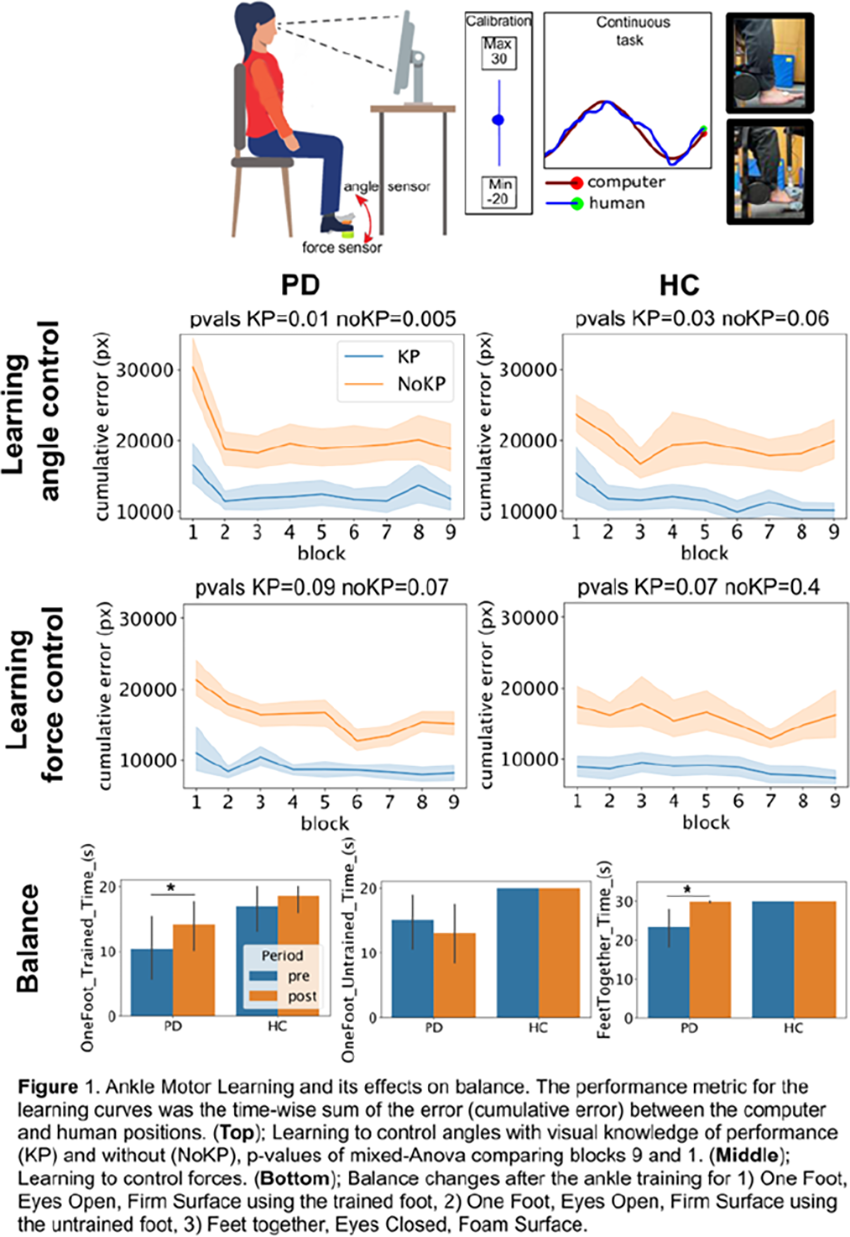
P25.44
1 Dartmouth Hitchcock Medical Center, United States
Introduction: Physical therapy (PT) services are recommended to help patients with Parkinson disease (PD) to best utilize evidence related to exercise as a disease management strategy. Experts advocate for referral to physical therapy at the time of diagnosis. The Parkinson’s Foundation reported in an analysis of 5,020 participants with PD 35.3% were referred to therapy; of these 25.1% received a multi-disciplinary referral. Similarly, there is a mismatch between patients with PD cared for at Dartmouth Hitchcock Medical Center by neurologists and PTs. When considering patients within 30 miles (July 2022-June 2023) 61% were referred to PT and 33.8% were seen by a PT.
To address this mismatch a quality improvement project was conducted with two main goals: increase referrals from 4 to 8 per month and increase percent scheduled with PT to 80% consistently.
Methods: A team was assembled that consisted of a PT, neurologist, social worker, scheduler and Lean Six Sigma (LSS) Blackbelt coach. The project moved through the Define, Measure, Analyze, Improve, Control stages of the LSS approach. With voice of customer data was collected via provider, staff, patient surveys, the team identified and validated root causes as to why patients are not receiving PT services. The team chose one Plan, Do, Study, Act (PDSA) cycle to test a new brochure for neurologists to provide to patients referring to PT. The number of referrals and patients scheduled with PT was collected for 6 months during the PDSA cycle and compared to data prior to determine next steps.
Results: The data showed an increase in referrals during the PDSA cycle from a median of 4 to 5.5 per month. This change was close to but not statistically significant. The percent of referrals scheduled went from a median of 75% to 87.5% per month. This did not reach significance as it was highly variable.
Conclusion: This project highlighted that beyond just the referral, other barriers exist to patients accessing PT services. Specifically, patient education about the benefits of PT for tracking progression and utilizing exercise to mitigate disease burden was found to be lacking despite the neurologists’ best attempt to share this information. In addition, schedulers’ knowledge about the importance and benefit of PT was also identified as a factor. We have implemented patient education with some improvement. Additional improvement in our metrics is expected with the planned implementation of scheduler education.
P25.45
1 NeuroFit Networks dba Parkinson Wellness Recovery, United States
2 Magnes AG, Switzerland
Freezing of gait (FOG) severely impairs mobility in advanced Parkinson's disease (PD), often worsening under cognitive load. Wearable biofeedback devices that analyze gait in real-time and deliver targeted vibrotactile corrections may enhance motor control by addressing asymmetries and hesitations. This single-patient case study evaluated the short-term impact of NUSHU smart shoes—which monitor movement via sensors and provide adaptive vibrotactile feedback to guide corrections—within a 4-day gait training program for a PD patient with major FOG.
A 76-year-old female with 3-year idiopathic PD (Hoehn-Yahr stage 3; participated in four 60-minute sessions (March 10–13, 2025) targeting freezing of gait training. Sessions 1 and 4 were performed with activated NUSHU shoes for real-time gait analysis and vibrotactile feedback; sessions 2 and 3 followed the same protocol without vibrotactile feedback. Pre- and post-session evaluations comprised: Freezing of Gait Assessment (FOG-A; completion time and 0–3 severity score for initiation, turns, doorway); cognitive FOG-A (with serial 3s subtraction); Timed Up and Go (TUG; time) and cognitive TUG (TUG-Cog). Lower times/scores denote better performance.
Overall, FOG-A times decreased (pre-mean 57.5 ± 10.3 s to post 56.2 ± 10.1 s), with scores holding steady or improving on feedback days (Day 1: 69 s/2 → 65 s/2; Day 4: 57 s/3 → 47 s/0) compared to variable non-feedback results (Day 2: 60 s/0 → 65 s/0; Day 3: 44 s/1 → 48 s/2). Cognitive FOG-A gains were pronounced with feedback (pre-mean 78.8 ± 34.4 s to post 73.5 ± 16.8 s; scores 3.0 ± 3.2 → 1.3 ± 1.5), e.g., Day 4: 61 s/1 → 55 s/0. TUG durations shortened (pre 36.0 ± 12.9 s → post 31.0 ± 5.5 s), reducing all festination/FOG events post-sessions. TUG-Cog times remained stable (pre 38.0 ± 4.8 s → post 41.0 ± 6 s). The patient noted significant improved gait awareness during feedback sessions.
Adaptive vibrotactile feedback from NUSHU shoes reinforced training effects on FOG, especially in dual-task scenarios, by providing movement-specific corrections that likely reinforced sensorimotor integration. This case suggests promise for smart wearables in PD rehabilitation, though limited by its single-subject nature. Future randomized studies with increased sample size should be studied.
P25.46
1 Teachers College, Columbia University, United States
2 Department of Biobehavioral Sciences, Teachers College, Columbia University, United States
Purpose/Hypothesis: Sitting and rising from the floor (floor-SR) is a complex task that requires coordination, muscle strength, balance, and flexibility, which are often impaired in People with Parkinson’s Disease (PwP). PwP are often slower and may have difficulty performing floor-SR independently. The Sitting-Rising Test (SRT) is a standardized measure that evaluates the ability to perform floor-SR by quantifying the number of supports used (e.g., hand, elbow) and loss of balance. The SRT is a simple test that requires minimal clinician training and equipment and assesses disease-specific deficits, e,g., incoordination. However, the reliability of SRT in PwP has not been investigated. We, therefore, aimed to assess the inter-rater and intra-rater reliability of SRT in PwP.
Number of subjects: 10 PwP (8 males), age (mean ± SD) = 68.1 ± 6.98 yrs, H&Y = I-II, tested during on-medication state.
Materials and methods: The analysis included 27 SRT trials, 1-3 per participant. Performance was videotaped using an iPad positioned at a 45-degree angle towards the person performing the task. Four raters, 2 clinicians (1 Physical Therapist, 1 Chiropractor), and 2 research assistants (RA), independently scored videos played once at normal speed. The scoring was performed in two sessions, spaced five days apart. The first session was used to assess inter-rater reliability, and both sessions were used to assess intra-rater reliability. SRT has a baseline score of five points for each component (sitting and rising) of Floor-SR. The total SRT score ranges from 0 to 10, representing the sum of two components. A point is subtracted for each support used, and a half point for perceived imbalance. All assessors received the same training, which included a 30-minute guided session on demonstrations of a standardized scoring procedure.
Results: In PwP, the mean ± SD SRT score was 4.68 ± 3.81. The inter-rater reliability among clinicians was (ICC[2,1] = 0.90, 95% CI [0.78–0.95], p < .001) and among non-clinicians was (ICC[2,1] = 0.96, 95% CI [0.92–0.98], p < .0001). Intra-rater reliability for the clinicians was (ICC[3,1] = 0.93, 95% CI [0.85–0.97], p < .0001), and for non-clinicians was (ICC[3,1] = 0.98, 95% CI [0.95–0.99], p< .0001).
Conclusions: We found excellent inter- and intra-rater reliability for the SRT in PwP. This provides support for SRT test reliability among PwP and for its applicability to be used by clinicians and non-clinicians.
P25.47
1 Universidade Federal de Minas Gerais, Brazil
2 University of Nevada, United States
3 Universidade Federal de Minas, Brazil
4 Saint Louis University, United States
5 Washington University, United States
Introduction: Assistive devices (AD) are frequently utilized by people with Parkinson’s disease (PwPD) to compensate for mobility deficits, although their use may be influenced by various factors. Understanding the determinants of device use in different contexts is essential to optimizing their use as low-cost therapeutic strategies. This study aimed to investigate the determinants of assistive device use at home and in the community among PwPD. Methods: A cross-sectional study including PwPD aged ≥50 years was conducted. Participants with other forms of parkinsonism or conditions that could require assistive device use were excluded. Data were collected via the Survey of Treatments, Exercise, Participation, and Symptoms in Parkinson’s disease (STEPS-PD) project. The dependent variables were: (1) AD use at home and (2) AD use in the community. Independent variables included sex, age, disease duration, falls in the past month (non-recurrent/recurrent), falls in the past year (non-recurrent/recurrent), injury from falls in the past year (non-injured/injured), perceived severity of problems with balance, falling, fear of falling (FOF), gait, freezing, and FOF avoidance behavior (Modified Fear of Falling Avoidance Behavior Questionnaire-mFFABQ). Logistic regression was performed for each context. Results: A total of 186 PwPD were included (age 69±10 years; 101 males). For home AD use, older age (OR=1.103, p=0.017), recurrent falls in the past month (OR=0.051, p≤0.001), higher perception of gait problems (OR=1.026, p=0.024), and greater FOF avoidance behavior (OR=1.126, p=0.01) were determinants (Nagelkerke R2=0.61). For community AD use, older age (OR=1.077, p=0.032), recurrent falls in the past month (OR=0.244, p=0.027), higher perception of FOF (OR=1.024, p=0.048), and greater FOF avoidance behavior (OR=1.095, p=0.004) were determinants (Nagelkerke R2=0.60). Conclusions and implications: Age, recurrent falls in the past month and FOF avoidance behavior were significant determinants of device use in both contexts. Individuals' perception of gait problems was a determinant of home AD use, while a perception of FOF was a determinant of community AD use, suggesting that motivations for device use may vary by context. These findings highlight the importance of routine fall history screening and individualized, patient-centered assessment to inform safe and appropriate device prescription in PwPD.
P25.48
1 New York Institute of Technology, United States
Background: Fatigue affects half of people with Parkinson's disease, but pharmacological treatment options remain limited. Physical and occupational therapy plays an important role in Parkinson’s symptoms management, but interventions primarily focus on addressing motor symptoms, and fatigue management is lacking. Physical exercise and sleep hygiene education have shown effective in Parkinson’s fatigue management, but self-efficacy and routine establishment may have been the barriers of these practices.
Purpose: This project aims to develop an evidence-based treatment protocol for Parkinson’s disease fatigue management utilized by allied health practitioners with multidisciplinary approach, with focus on improving self-efficacy and routine establishment in performing moderate to high intensity physical exercise three times a week and developing proper sleep hygiene habits.
Method: Community-dwelling individuals with Parkinson’s fatigue (N=16) participated in six weekly group meetings with education on moderate to high intensity exercise (Rock Steady Boxing, stationary bike, treadmill, brisk walking with hand weights) and safety, and sleep hygiene education. Gradual decrease in exercise supervision and sleep hygiene practice follow up occurred over a 12-week period. Stress management and social support are included. Protocol development was guided by the problem-solving component of cognitive behavioral theory and occupational-based approach.
Result: In the 12-week period, 75% of participants reported improvement in Self-Efficacy for Exercise (SEE) Scale with medium effect size, and 56% of participants reported improvement in Sleep Hygiene Index (SHI) that exceeds minimal detectable change (MDC). Qualitative data in self-efficacy reported the positive influence in motivation, exercising with peers, the instructions in exercising properly and safely, exercise alternatives, pre-bedtime routine, lifestyle change such as eliminating caffeine and sweet in the evening, and social support.
Conclusion: This 12-week program focuses on establishment of moderate to high intensity physical exercise routine 3 times a week and proper sleep hygiene habits. A gradual decrease in direct intervention approach is utilized to encourage independence in problem-solving, self-efficacy and routine establishment. This protocol contributes to knowledge of PD fatigue management utilized by occupational, physical and other allied health practitioners.
P25.49
1 Parkinson Wellness Recovery | PWR!, United States
2 The Kirk Gibson Center for Parkinson Wellness, United States
Background: Freezing of gait (FOG) in Parkinson disease (PD) has a complex pathophysiology that begins with episodic shortages of dorsal striatal dopamine and over inhibition of brainstem locomotor regions. Over time, compensatory networks breakdown, aberrant limbic inputs further strain processing, and FOG worsens. FOG can occur in 26% of persons with denovo PD to as much as 80% in advanced PD. Improved clinical detection tools and the identification of at-risk predictors has increased the ability to screen for FOG onset, assess FOG severity, and to capture the benefits of behavioral interventions.
A systematic review that included “freezers only,” showed that a broad range of physical therapy and exercise interventions aimed at: 1) allocating more attention to gait, and 2) targeting the motor / nonmotor correlates of FOG, reduced subjective FOG severity, while general exercise interventions did not, and retention was short-lived. High intensity aerobic studies in PD “non-freezers,” have shown attenuation of motor symptoms and increased functional connectivity of the “spared” striatal circuits. We suggest these studies support regular screenings for FOG onset, starting early (even in at-risk “non-freezers”), targeting high-intensity aerobic exercise and the training of motor / nonmotor correlates to increase resilience of motor and cognitive reserve, incorporating compensatory strategies, and addressing FOG-focused sustained practice.
Theoretical Framework: To design personalized interventions, we propose that clinicians start with an understanding of the pathophysiological mechanisms that characterize the episodic nature of FOG, based upon expert reviews and updates of the evidence since 1966. With those insights, combined with a clients’ personal factors, clinical characteristics, triggers, and preferred compensations, therapists can use clinical reasoning to choose from existing evidenced-based training interventions, or create novel interventions that address each person’s theoretical underpinnings.
Illustration of Methodology: We will summarize rehab considerations, and five theoretical models: Interference, Sensori-Perceptual Processing, Threshold, Decoupling, and Cognitive Dysfunction. For each model, supportive observations will be provided to justify clinical decision-making, and video examples of representative interventions in “freezers” or at-risk “non-freezers” will be available for viewing using a “barcode” to link to a video library.
P25.50
1 USP, Brazil
Parkinson’s disease (PD) is among the neurological conditions with the greatest global impact, affecting 11.8 million people in 2021, a 270% increase since 1990. In Brazil, prevalence among adults ≥50 years is 0.84%, corresponding to ∼536,000 individuals in 2024, projected to exceed 1.25 million by 2060. This growing burden challenges the public health system, which faces long wait times and limited access to specialized neurological rehabilitation. Despite advances in PD management, current assessment tools are often lengthy, complex, and insufficiently sensitive to subtle motor and functional changes, limiting precise clinical follow-up and individualized interventions. This study aimed to identify a brief, validated battery capable of predicting disability in activities of daily living (ADLs), optimizing physiotherapy care. A retrospective analysis included 238 participants with idiopathic PD. Validated assessments: UPDRS II/III, GDS-15, MoCA, TC6, Mini BESTest, STDP 5X, and 9HPT were reviewed. Spearman correlations identified associations with UPDRS II. Non-parametric regression models (Random Forest, K-Nearest Neighbors, Support Vector Regression, Decision Tree) were compared; Random Forest was selected as the final model. Variable importance, cross-validation, and discriminative ability were evaluated using ROC curves and AUC.
The 10 most relevant variables maintained predictive performance (accuracy=0.71 vs 0.74 for 22-variable model). Selected variables included motor items from UPDRS (arising from chair, speech, bradykinesia) and functional tests (TUG, 9HPT). A reduced battery of 10 validated tests allows rapid estimation of motor disability in ADLs for people with PD. This brief tool facilitates efficient clinical assessment, supports early, targeted interventions, and enables physiotherapy treatments tailored to disability level.
P25.51
1 University of Utah, Department of Physical Therapy and Athletic Training, United States
2 University of Utah, Division of Epidemiology, United States
3 Cleveland Clinic, Department of Biomedical Engineering,, United States
4 Cleveland Clinic, Department of Biomedical Engineering, United States
5 Cleveland Clinic, Dept. of Quantitative Health Sciences, Cleveland Clinic, Mellen Center for Multiple Sclerosis Treatment and Research, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, United States
6 University of Utah, Department of Physcial Therapy and Athletic Training, United States
Objective: The primary aim of this analysis was to examine whether longer turn duration predicts recurrent falls in people with Parkinson’s disease, and to evaluate whether this measure can inform a practical fall risk scoring tool.
Background: Turning is biomechanically more complex than straight line walking because it requires coordination between gait, postural control and dynamic adjustments of the center of mass. Turning roughly accounts for 25-25% of daily steps. In individuals with PD, turning deficits appear early in the disease, even when straight-line gait remains relatively preserved. Typical turning impairments in people with PD include axial rigidity, increased step count, shorter step length, narrower base of support and prolonged turn duration. Despite these features most clinical fall risk models rely on straight line walking metrics. The primary aim of this analysis was to develop a simple clinical risk score to predict recurrent falls (defined as ≥2 falls) in individuals with Parkinson’s disease.
Methods: Recurrent falls (≥2 in 12 months) served as the primary outcome. Predictors were turn duration (≤2 , 2–3, ≥3 seconds), age (<60, 60–69, ≥70 years), and years since diagnosis (<4, 4.5–6.5, ≥7). Multivariable logistic regression estimated odds ratios (ORs) and 95% confidence intervals (CIs). Model discrimination using the area under the receiver operating characteristic curve (AUC). Regression coefficients were transformed into a point-based risk score.
Results Among 249 participants, 34% reported two or more falls in12 months. In the multivariable model, longer turn duration, older age, and longer disease duration were independently associated with recurrent falls. Turn duration ≥3 s was associated with over four times the odds of recurrent falls (OR 4.61, 95% CI 1.54–13.85). Age ≥70 years (OR 2.80, 95% CI 1.25–6.29) and disease duration ≥7 years (OR 4.96, 95% CI 2.47–9.97) were also significant predictors. The final model demonstrated good discrimination (AUC 0.75, 95% CI 0.69–0.81).
Conclusion Incorporating quantitative turn measures into clinical assessment may improve identification of individuals at greatest risk for recurrent falls.
P25.52
1 Saltmarche Health .& Assoicates, Canada
2 Gaitway Neurophysio, Canada
3 Brain and Mind Centre, University of Sydney, Australia
4 Sydney Adventist Hospital, Sydney, Australia
5 College of Health and Medicine, Australian National University, Australia
6 Veterans Affairs Boston Healthcare System; Department of Neurology, Boston University School of Medicine, United States
Objective: To determine if photobiomodulation therapy for up to one year was able to improve micrographia in people with Parkinson’s disease (PwP)
Background: Parkinson’s disease (PD) as a progressive neurodegenerative condition has an array of motor and non-motor symptoms that progressively worsen over time. Micrographia is a clinical motor sign of PD where there is an overall decrease in writing speed and size of the letters that may be progressive. This symptom may occur in up to 70% of PwP. Micrographia might be reverse with dopamine replacement therapy in some cases and there are some tools that may help with writing and some modifications to writing that may help, such as using paper with grids lines and using block letters. Photobiomodulation (PBM) is the use of non-thermal light of various wavelengths (most commonly red and near infrared) to improve cellular function. We have previously reported the success of PBM treatment to improve a number of motor and non-motor symptoms in PD. This study was part of a larger PBM PD study. We report here on the changes in micrographia in that cohort of participants where micrographia was part of the original PD symptom mix.
Methods: Participants were asked to write a sentence three times. The area and perimeter of selected letters was determined using FIJI software.
Results: Results show improvement in micrographia in a number of the participants of the study who continued to use PBM therapy for up to 1 year.
Conclusion: These results indicate that PBM has the potential to improve specific symptoms of PD such as micrographia and confirms the results of previous studies of the treatment of PD with PBM. PBM is a safe, easy to use treatment that should be considered as a part of a comprehensive, multidisciplinary approach to treating Parkinson’s symptoms. Further research is warranted.
P25.53
1 Texas A&M University -- College Station, TX, United States
2 ROCK, United States
3 Texas A&M University -- University College Station, United States
4 Texas A&M University -- College Station, TX, Uzbekistan
Background: Physical Therapy (PT) incorporating equine movement provides multisensory stimulation and rhythmic movement that may enhance balance and postural control in individuals with Parkinson’s disease (PD). This study examined the acute and short-term effects of such therapy on postural stability and functional mobility.
Methods: Eighteen participants with mild-to-moderate PD were assigned to a group that received PT utilizing equine movement or a control group. Balance and mobility were assessed pre-intervention, post-intervention, and at one-week follow-up using the Berg Balance Scale (BBS), Timed Up and Go (TUG), Five Times Sit-to-Stand Test (5xSTS), and force-plate measures of center-of-pressure (CoP) under four sensory conditions (eyes open/closed, with/without foam). Data were analyzed using (1) a repeated-measures model assessing within-subject effects across time and sensory condition, and (2) a mixed 2×2 model comparing groups across time. Correlation analyses examined relationships between improvements in postural stability and clinical outcomes.
Results: Preliminary analyses revealed reductions in CoP ellipse area and significant improvements in BBS and TUG scores following PT including equine movement. Participants demonstrating greater stabilization also exhibited larger functional gains. No adverse events were observed.
Conclusions: Mechanistic links between postural control metrics and clinical outcomes will be discussed. Our results support PT treatments that integrate equine movement into evidence-based rehabilitation programs may enhance balance and mobility in PD.

P25.54
1 KU Leuven, Belgium
2 UZ Leuven / KU Leuven, Belgium
Background: Touchscreen use is compromised in Parkinson’s disease (PD) and motor learning may mitigate these deficits. As daily life touchscreen use often involves cognitive distractions, dual task (DT) training may better support skill retention by facilitating attentional networks.
Objective: To investigate the behavioural and neural effects of single task (ST) versus DT touchscreen training in PD and healthy controls (HC).
Methods: Thirty-seven people with PD (OFF-medication) and 37 HC trained the Swipe-Slide Pattern (SSP) task in either ST or DT condition (depending on randomization) during two task-based fMRI sessions and four days home-based practice. Linear mixed models examined the change in SSP movement time (pre-, post-training, and after two days follow-up) and in task-based functional within- and between-network connectivity (pre-training, follow-up). Correlations between behavior and brain connectivity at follow-up were assessed, and partial correlations explored the influence of clinical factors (i.e., age, cognitive capacity, device proficiency) on behavioral gains, controlling for Training (ST-DT) and Group (PD-HC).
Results: Both training modalities improved SSP performance, with gains retained at follow-up in PD and HC. Notably, in PD, immediate improvements were retained following DT training (p=0.453) but declined after ST training (p=0.026). We found disparate learning effects of training (DT>ST) in motor (F(1,69)=6, p=0.018) and frontoparietal-subcortical (F(1,68)=5, p=0.041) connections, with stronger connections relating to better SSP-performance at retention. For HC, we found stronger learning-related connectivity in attentional (F(1,67)=5, p=0.033) and motor-cerebellar (F(1,67)=6, p=0.031) networks than in PD. While controlling for Group and Training, older participants (r-partial=0.3, 95%CI [0.1 0.6]) with poorer cognition (r-partial=-0.3, 95%CI [-0.5 -0.02]) and reduced mobile device proficiency (r-partial=-0.4, 95%CI [-0.7 -0.2]) demonstrated greater improvements.
Conclusion: Both ST and DT training enhanced touchscreen skill learning in PD and HC, with DT training showing superior retention in PD. Stronger DT-related connectivity was linked to better retention, suggesting that incorporating distractions to training may enhance task engagement and retention. Notably, training was especially beneficial for older participants and those with poorer cognition and lower mobile device proficiency.
COMPREHENSIVE CARE: Nutrition and gastrointestinal issues
P26.01
1 University of Calcutta, India
2 Biochemistry and molecular pharmacology, University of Calcutta, India
Introduction: Parkinson’s disease is a prevalent neurodegenerative disorder with limited therapeutic options. Environmental factors and dietary habits are recognized risk components in various diseases, including neurodegenerative disorders. Emerging evidence suggests that diet during early life and living environment may influence the incidence of PD later in life. However, epidemiologic data on this topic, particularly from India, remain sparse. This large-scale case-control study, employing network pharmacology and molecular docking, aimed to identify dietary and environmental risk factors associated with Parkinson’s disease (PD).
Methods: We recruited 200 patients with PD, 150 with Alzheimer’s disease (AD), and 200 healthy age-matched controls. Dietary intake and environmental exposures were assessed using a validated Food-Frequency Questionnaire and Environmental Hazard Questionnaire. Cox regression models evaluated associations between dietary/environmental factors and mortality risk. Subsequently, network pharmacology approaches, including protein-protein interaction (PPI) networks and enrichment analyses, alongside molecular docking, were employed to identify potential dietary and environmental molecular targets in PD.
Results: Patients with PD exhibited significantly higher intake of carbohydrates and fats, and significantly lower intake of dietary fiber and fruits, compared to AD patients and healthy controls. Notably, meat and milk consumption were significantly associated with increased mortality risk in both PD and AD groups (p < 0.01). Conversely, rural living and regular exercise were linked with decreased mortality risk in PD patients (p < 0.001). Network pharmacology and molecular docking analyses identified key molecular targets and pathways implicated in neurodegeneration relevant to PD and AD.
Conclusion: This pioneering large-scale study identifies specific dietary patterns and environmental factors associated with mortality risk in PD and AD in an Indian population. These findings highlight potential preventive strategies focusing on modifiable diet and environment-related factors that could be clinically valuable in managing PD.
P26.02
1 Radboud university medical center, Netherlands
2 University Medical Center Groningen, Netherlands
3 Parkinson Verenging, Netherlands
The rising prevalence of Parkinson's disease (PD) may be impacted by environmental and lifestyle factors. Therefore, increasing attention is being paid to non-pharmacological approaches in the treatment of PD. Dietary interventions can have a direct symptomatic effect by improving gastrointestinal functioning and constipation. This can in turn improve the efficacy of levodopa and thus have an enormous impact on clinical functioning. Moreover, current pharmacological treatments only alleviate symptoms, but do not alter disease progression. Recent research indicates the potential pivotal role of gut microbiome dysbiosis in PD pathogenesis through inflammation. Dietary interventions, particularly plant-based diets, have been shown to effectively manage chronic inflammatory diseases, and may potentially also modify disease progression in PD.
We are now evaluating the effects of a plant-based diet on daily life functioning in people with PD, as well as its effects on the clinical and biological effects of the diet. The study is an RCT in 260 people with PD in all disease stages, randomized into a control and an intervention group. The intervention group follows a 12-month whole-foods plant-based diet and receives consultation by a registered dietician. The plant-based diet includes supplementation of vitamins B12, D3 and omega-3. The control group only receives the supplements without additional dietary advice. Assessments at baseline, 6 and 12 months evaluate motor and non-motor symptoms. Primary outcome is the difference in motor experiences of daily living, measured with the MDS-UPDRS part II at 12 months follow-up. In addition, we explore the biological effects of the intervention using analyses of microbiome composition, intestinal permeability, and systemic inflammation. At baseline and 12 months, participants wear a study watch for one week. Between visits, participants complete records of their dietary intake to measure dietary adherence. People with PD are members of the research team. We will present preliminary baseline participant characteristics and current dietary intake.
With this trial, we will gain insights into the potential of plant-based diets for managing and modifying PD as well as in the support that is needed to successfully execute the lifestyle change that is required to switch to a fully plant-based diet. If proven to be effective, the steps towards implementation in health care will be explored both nationally and internationally.
P26.03
1 SMG-SNU Boramae Medical Center, South Korea
2 Kangnam Sacred Heart Hospital, South Korea
Background and Objective: Although muscle mass loss is an emerging public health concern, its prevalence, associated factors, and clinical significance in Parkinson’s disease (PD) remain unclear. This study aimed to investigate the prevalence of low muscle mass (LMM) in patients with PD in comparison to the general population and to examine its association with orthostatic hypotension (OH) and orthostatic symptoms.
Methods: We prospectively recruited patients with PD with a Hoehn and Yahr scale of 3 or lower. For comparisons, PD patients were matched with individuals from the general population in a 1:5 ratio by age, sex, and height using data from the Korea National Health and Nutrition Examination Survey. All participants underwent dual-energy X-ray absorptiometry to measure appendicular skeletal muscle mass. In PD patients, blood pressure (BP) was measured in the supine position and at 30 seconds, 1 minute, 3 minutes, and 5 minutes after standing during head-up tilt tests. Orthostatic symptoms were assessed using items 14 to 16 of the Scales for Outcomes in Parkinson’s Disease–Autonomic Dysfunction questionnaire.
Results: 409 PD patients (mean age, 71.1±9.5 years; 52.3% men) and 2045 matched population-based controls were included. The prevalence of LMM was significantly higher in the PD patients compared to the controls (35.0% vs. 24.8%; P<0.001), and this difference was pronounced in men and individuals aged ≥70 years. In the PD group, no significant differences were observed in the prevalence of OH between the LMM and normal muscle mass (NMM) groups (46.8% vs. 38.6%; P=0.412). When orthostatic BP changes were analyzed as continuous variables, the LMM group showed significantly greater drops in systolic BP (P=0.036) and diastolic BP (P=0.009) during 5 minutes after standing compared to the NMM group. When individual time points were examined separately, a significant difference was observed only at 30 seconds after standing in both systolic BP (P=0.020) and diastolic BP (P=0.012). There were no significant differences in the frequency or severity of orthostatic symptoms between the groups.
Discussion: Patients with mild to moderate PD showed an elevated risk of muscle mass loss, especially among males and older individuals. Although muscle mass loss was associated with greater BP reductions particularly in the initial period after standing, it did not appear sufficient to trigger OH or associated symptoms.
P26.04
1 My Moves Matter, Ireland
2 Beaumont Hospital, Ireland
3 University College Cork, Ireland
Background: Parkinsons Disease (PD) is a chronic neurological condition with significant nutritional implications that can be optimised through dietetic input. However, approximately 90% of PD patients lack access to dietetic services.
Aim & Objectives: This study aims to evaluate PD-related nutrition knowledge amongst Irish dietitians, assess current practices, identify existing knowledge gaps and explore barriers to the delivery of care.
Research Design: An online cross-sectional survey was distributed to CORU registered dietitians in Ireland via Qualtrics, running for 2- 3 weeks in May 2024.
Results: A total of 85 responses were collected, with 39.5% (n=32) from basic grade dietitians and 42% (n=34) from senior dietitians. Majority of dietitians (n=57) are aware of the importance of diet in management of PD. Dietitians who see PD patients are more confident in provision of dietary advice (p=<.001) and more familiar with nutritional challenges associated with the condition (p=<.001) compared to those who do not see PD patients. Regarding access and referrals, 78.4% (n=58) reported inadequate access to dietitians amongst PD patients and 55.9% (n=33) reported they do not receive necessary referrals for PD patients. 87.7% (n=50) felt that both undergraduate and postgraduate programmes insufficiently covered the links between diet and PD. Key barriers to PD-related care included lack of referrals, inadequate dietetic training and limited dietitian involvement in the multidisciplinary team.
Conclusion: This study highlights gaps in PD-related knowledge and training amongst dietitians as well as barriers to care. Addressing these gaps through targeted education and increased integration of dietitians within multidisciplinary teams could enhance overall patient outcomes.
P26.05
1 Neurodegenerative Diseases Research Group, Vall d’Hebron Research Institute (VHIR) - Network Center for Biomedical Research in Neurodegenerative Diseases (CIBERNED), 08035 Barcelona, Spain., Spain
2 Neurodegenerative Diseases Research Group, Vall d’Hebron Research Institute (VHIR) - Network Center for Biomedical Research in Neurodegenerative Diseases (CIBERNED), 08035 Barcelona, Spain - Aligning Science Across Parkinson’s (ASAP) Collaborative Research Network, Chevy Chase, MD 20815, USA - Department of Biochemistry and Molecular Biology, Autonomous University of Barcelona, 08193 Barcelona, Spain - Catalan Institution for Research and Advanced Studies (ICREA), 08010 Barcelona, Spain., Spain
3 Neurodegenerative Diseases Research Group, Vall d’Hebron Research Institute (VHIR) - Network Center for Biomedical Research in Neurodegenerative Diseases (CIBERNED), 08035 Barcelona, Spain - Aligning Science Across Parkinson’s (ASAP) Collaborative Research Network, Chevy Chase, MD 20815, USA., Spain
Introduction: Parkinson’s disease (PD) is the second most common neurodegenerative disorder. Non-motor symptoms, particularly gastrointestinal dysfunction, often precede motor symptoms and are considered prodromal features of the disease. Our group has developed a novel transgenic mouse model of PD (tgNM) that shows neuromelanin accumulation and neurodegeneration in dopaminergic, noradrenergic, and cholinergic systems, resulting in both motor and non-motor symptoms that emerge progressively across preclinical (3 months), prodromal (12 months), and early (20 months) PD stages (Laguna et al, Nat Comm, 2024). TgNM mice display gut dysbiosis, increased intestinal permeability and systemic inflammation that enhance neurodegeneration (Lorente et al, in preparation). Ketogenic interventions have recently emerged as promising non-pharmacological and non-invasive approaches for neurodegenerative diseases due to their reported properties to improve gut health, enhance energy metabolism, and modulate inflammation.
Aim/Methods: We aimed to test whether a ketogenic diet (KD) could ameliorate the parkinsonian phenotype in tgNM mice. We evaluated sex-specific effects of a KD (90% lipids—20% MCTs, 10% protein, 0% carbohydrates) administered for 4 months to 8-month-old tgNM mice.
Results: Male tgNM mice fed with a KD achieved a deep state of nutritional ketosis, while female mice reached only mild ketosis. KD improved glucose regulation in males, whereas the opposite effect was observed in females. They also presented different patterns of feeding regulation (water, food and calorie intake) being females more susceptible to weight gain. Dietary adaptation led to hepatic hypertrophy in males and pancreatic hypertrophy in females. TgNM males fed with KD accumulate brown fat while tgNM females, white fat. KD reduced intestinal permeability and improved metabolic and cytokine profiles in TgNM mice. Behaviorally, KD reduced depression-like behavior, improved long-term memory, and partially restored the loss of vocalizations observed in tgNM mice, although anxiety levels increased. Notably, all beneficial effects were more evident in males.
Conclusions: Male tgNM mice exhibited a better overall response to the KD across metabolic, gastrointestinal, and behavioral domains. These findings underscore the importance of considering biological sex when evaluating nutritional interventions for neurodegenerative diseases such as Parkinson’s disease.
P26.06
1 Clínica de Parkinson y Trastornos del Movimiento, Hospital Universitario “Dr. José E. González”, Mexico
2 Clínica y Consulta de Nutrición, Hospital Universitario “Dr. José E. González”, Mexico
3 Laboratorio y Unidad de Monitoreo de Epilepsia y Sueño, Hospital Universitario “Dr. José E. González”, Mexico
Introduction: The relationship between diet and Parkinson’s has gained interest in recent years, as dietary patterns are being considered potential protective or risk factors for disease progression, which may be explained by deficiencies or excess intake of macro- and micronutrients [1].
Objective: To identify macronutrient and micronutrient deficiencies in a population with Parkinson’s in Northeastern Mexico.
Methods: A cross-sectional study was conducted in October 2024. Dietary assessment was performed using a 24-hour dietary recall, along with the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) and the Montreal Cognitive Assessment (MoCA). Macro- and micronutrient intake was analyzed using the Nutrimind software.
Reference values for daily recommended intake were obtained from the National Institutes of Health (NIH) compendium “Nutrient Recommendations and Databases” [2].
Results: Seven patients were included, of whom 4 (57.1%) were male and 3 (42.9%) female. Deficient intake was observed for vitamin B6 (0.71 mg), vitamin D (3.86 µg), vitamin E (2.29 mg), magnesium (206.43 mg), potassium (2072.86 mg), and water (671.86 mL).
Additionally, carbohydrate, lipid, total caloric intake, vitamin B9, vitamin B12, iron, and zinc levels were below recommended values. Detailed macronutrient and micronutrient data are presented in Table 1.
Among the participants, 5 (71.4%) had deficient total energy intake, 1 (14.3%) adequate, and 1 (14.3%) excessive. Percentages of lipid and protein intake were within normal ranges; however, 3 (42.9%) had carbohydrate deficiency. All 7 (100%) patients showed deficient intake of vitamin E and water, and 6 (85.7%) of vitamin D. Frequencies are described in detail in Table 2.
Conclusion: The studied population showed deficient intake of vitamins B6, D, and E, as well as magnesium and potassium. Such dietary patterns may contribute to disease worsening and cognitive decline [1]. The only patient with adequate caloric (1,978 kcal) and vitamin D (12 µg) intake showed better MoCA performance (26) and lower MDS-UPDRS scores (38) at Hoehn and Yahr stage 3. This may indicate the favorable impact of adequate daily dietary recommendations and the importance of promoting them. Increasing the sample size is necessary to strengthen the validity of these findings.

P26.07
1 Illinois Institute of Technology, United States
2 Sorridi Therapeutics, United States
Emerging evidence links gut dysbiosis and intestinal inflammation to the pathophysiology of Parkinson’s disease (PD). Altered microbial metabolism, characterized by reduced short-chain fatty acids (SCFAs) and elevated fecal calprotectin, may compromise gut barrier integrity and promote systemic inflammation. Dietary strategies that restore microbial balance and SCFA production could therefore offer a nonpharmacological approach for improving gastrointestinal and metabolic health in individuals with PD. We developed a prebiotic fiber blend, NeuroFiber, designed to selectively enrich SCFA-producing taxa and mitigate intestinal inflammation in individuals with PD. In this 4-week pilot study (NCT07127120), 18 individuals with PD consumed one NeuroFiber bar daily. Stool and blood samples were collected at baseline and week 4 for SCFA, bile acid (BA), calprotectin, and lipid profiling. Questionnaires assessed tolerability, gastrointestinal symptoms, and PD-related motor and non-motor features. The results of this study showed that NeuroFiber was well tolerated with no adverse events. Total fecal SCFA concentrations modestly increased, while fecal calprotectin significantly decreased (p=0.021), indicating reduced intestinal inflammation. Select primary (cholic acid) and secondary (lithocholic and nor-deoxycholic) BA concentrations decreased, suggesting shifts in microbial metabolism. Most participants (78%) reported improved gastrointestinal comfort, relief from constipation and reduced laxative use. Motor and non-motor symptom scores also improved over the 4 weeks. Significant reductions in total and LDL cholesterol (p=0.0063 and 0.0002, respectively) further suggest systemic metabolic benefits. These findings highlight the therapeutic potential of targeted prebiotic supplementation in individuals with PD to improve markers associated with gut and metabolic health. Larger controlled trials are underway to confirm these effects and explore whether sustained modulation of microbial metabolites influences neurodegenerative outcomes.
P26.08
1 University of Auckland, New Zealand, New Zealand
2 University of Auckland, New Zealand
3 My Moves Matter, Ireland
4 Auckland City Hospital, New Zealand
5 University of Bristol, United Kingdom
Background: There is an increasing need for people with Parkinson’s disease (PD) and relevant stakeholders to engage as partners with researchers to identify health research priorities. The aim of this study was to utilise World Cafés, a participatory method, to identify research priorities in the area of nutrition and PD.
Methods: People with PD, caregivers, healthcare professionals and other stakeholders were invited to attend a series of in-person and online World Café focus groups in New Zealand. Participants were asked how their/others’ PD impacts eating and drinking and where nutrition research should be focussed in the future. Written records were made of the discussions and from these, key topics were identified.
Results: Four World Café focus groups were held. One was online and 3 took place in the community, 2 of which were part of PD support group meetings. Thirty-eight participants took part which included people with PD, caregivers, family members, dietitians and nurses. Key issues and research priorities raised were related to gastrointestinal health, dietary supplements, drug-nutrient interactions and dietary strategies for symptom management.
Discussion: World Cafés were successfully used to understand key issues and research priorities of nutrition and PD. The discussions at the World Café focus groups provided a rich insight into issues in relation to nutrition and PD and identified research priorities that can be further developed in research co-design activities in the future.
CLINICAL SCIENCES: Symptoms, signs, features & non-motor manifestations
P27.01
1 Department of Geriatrics, Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń, Poland, Poland
2 York College of Pennsylvania, United States
3 Department of Neurological and Neurosurgical Nursing, Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Toruń, Poland, Poland
Abstract Background: Parkinson’s disease (PD) is widely recognized for its motor symptoms, such as tremor, rigidity, and bradykinesia. However, non-motor symptoms are equally important and can significantly impact a patient’s quality of life. Among these, sleep disturbances are particularly common and often appear early in the disease course. Typical issues include insomnia, nocturia, restless legs syndrome, REM sleep behavior disorder, fragmented sleep, and excessive daytime sleepiness. Despite their prevalence, these symptoms are frequently underrecognized and insufficiently addressed in clinical practice. Aim: This poster presents the Parkinson’s Disease Sleep Scale - 2 (PDSS-2), a validated, patient-reported tool designed to assess the severity of sleep disturbances in individuals with PD. The objective is to highlight its clinical relevance, describe its structure, and promote broader application, especially in the United States and Poland, where its use remains limited. Tool Description: The PDSS-2 is an updated version of the original PDSS, incorporating a broader range of nocturnal symptoms. It includes 15 items, each scored from 0 to 4, and assesses three key domains: (1) motor symptoms during the night (e.g., tremor, cramps), (2) disturbed sleep (e.g., difficulty falling or staying asleep, vivid dreams, nightmares), and (3) daytime sleepiness. The total score ranges from 0 to 60, with higher scores indicating more severe disturbance. The questionnaire is completed by patients and takes under 10 minutes, making it practical for both clinical and research use. Discussion: The PDSS-2 enables clinicians to identify sleep-related issues that may be missed during routine evaluations focused on motor symptoms. It facilitates patient-centered discussions and helps guide personalized interventions, such as medication adjustments, behavioral changes, or specialist referrals. It also supports monitoring of symptom progression and treatment outcomes. Despite its proven utility and widespread use in international settings, the scale is not routinely used in many clinical practices.
Conclusion: The PDSS-2 is a brief, reliable, and easy-to-use tool that provides valuable insight into sleep disturbances in PD. Its implementation in clinical practice can improve recognition and management of non-motor symptoms, contributing to more holistic care. Increasing awareness and use of this tool could significantly benefit people living with Parkinson’s disease.
P27.02
1 Medical University of South Carolina, United States
2 University at Buffalo, United States
Background: Parkinson disease (PD) disrupts respiratory function, impacting speech volume, clarity, and voice quality. Thoraco-abdominal asynchrony (TAA), characterized by out-of-phase movement of the ribcage (RC) and abdomen (AB), may underlie these impairments and increase effort, but has not been systematically evaluated in PD.
Objectives: (1) Determine whether PD alters TAA compared to healthy older adults; (2) Evaluate the effects of two evidence-based voice interventions, LSVT LOUD® and SpeechVive™, on TAA in PD.
Methods: Secondary data analysis includes 24 individuals with PD, 10 PD controls, and 24 healthy older controls. Twenty-four participants with PD were randomly assigned to LSVT LOUD (n=12) or SpeechVive (n=12). Control participants did not receive intervention. PD data were collected at baseline and one-week post-treatment; healthy controls were evaluated once. Respiratory inductance plethysmography captured RC and AB movements during monologue and reading tasks. Chest wall kinematics will be analyzed to quantify TAA. Data for 14 participants are presented; full dataset processing will be completed by February 2026.
Results: Objective 1: Preliminary analyses showed no group difference in the moving correlation between RC and AB (PD: M=0.84, SD=0.26; Controls: M=0.90, SD=0.04), though variability was markedly higher in PD [Coefficient of variation (CoV)]=31%) than controls (CoV=5%). Percent paradoxing was comparable between groups at baseline (PD: M=24%, SD=12%; Controls: M=26%, SD=10%), but variability was greater in PD (CoV=52% vs. 37%). Objective 2: No significant pre-to-post changes were observed in moving correlation for either intervention. Visual inspection suggests differing trends: SpeechVive users (n=7) showed improved coordination posttreatment (pre=0.859, post=0.920), while LSVT LOUD users (n=7) remained fairly stable (pre=0.934, post=0.944). Percent paradoxing did not change significantly, but variability decreased post-treatment in SpeechVive users (CoV pre=38%, post=25%) and increased in LSVT LOUD participants (CoV pre=40%, post=47%). Analyses of full group and session effects, including inspiratory and expiratory phases, are underway.
Conclusion: Persons with PD have reduced RC-AB coordination, but treatment-related changes remain inconclusive pending full data analysis. Findings have potential to refine therapeutic approaches and inform mechanisms of treatment response.
P27.03
1 Clínica Universidad de Navarra, Spain
2 Czech Technical University in Prague, Czechia
Introduction: Magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy is an effective and incisionless treatment for medication-refractory tremor in both essential tremor (ET) and Parkinson’s disease (PD). However, the potential impact of MRgFUS on speech remains unclear. Objective, quantifiable speech measures may help monitor post-procedure outcomes. This study aimed to assess speech performance in ET and PD patients following unilateral MRgFUS thalamotomy.
Methods: Sixteen ET and nine PD patients who underwent unilateral ventral intermediate nucleus (VIM) MRgFUS thalamotomy were included. Speech recordings were obtained using an external microphone and computer-based analysis both pre-treatment and at six months post-intervention. Four types of tasks were analyzed: phonation, diadochokinetic (DDK), text reading, and spontaneous monologue. Linear mixed models were used to evaluate longitudinal changes, with age, severity and disease duration as a covariate. Significance was set at p<0.05.
Results: Phonation tasks: In PD, the harmonic-to-noise ratio worsened significantly (p=0.042), indicating increased hoarseness. ET patients showed improvements in pitch variability and pitch tremor (p=0.031).
DDK tasks: PD patients exhibited longer voice onset times (p=0.017), suggesting impaired laryngeal–oral coordination. ET patients improved in DDK irregularity (p=0.029), indicating enhanced motor sequencing.
Text reading: PD patients showed significant reductions in pitch variability (p=0.002) consistent with monopitch. ET patients present significant monoloudness (p=0.004). ET patients remained stable or slightly improved.
Spontaneous monologue: ET patients showed significant improvements in voice quality, with increased cepstral peak prominence (p=0.007) and mean spectral energy (p=0.03). Median duration of pauses remained stable in both groups.
Conclusion: Patients with ET showed stable or improved speech measures, while PD patients demonstrated mild deterioration in several parameters. These results suggest that MRgFUS thalamotomy is speech-safe in ET, while in PD patients shows worsening in some variables. A control group is needed to decipher if these belongs to the neurodegenerative process of the disease. Longitudinal monitoring using objective acoustic metrics could enhance post-HIFU follow-up and individualized rehabilitation strategies.
P27.04
1 University of North Texas Health at Fort Worth, United States
2 University of North Texas Health of Fort Worth; The Parkinson Discovery Institute, United States
3 Texas Christian University, United States
4 Acclaim Health, JPS Health Network Physician Group, United States
5 University of Michigan Medical School, United States
6 University of Texas at Arlington, College of Nursing and Health Innovation, United States
7 University of North Texas in Denton, United States
Objectives: (1) Conduct a cross-species translational (CSTs) study using peripheral blood and brain tissue to illustrate the neuropathology and pathophysiological similarities between a 6-OHDA rat model of Parkinson disease (PD) and human subjects with early-stage idiopathic PD. (2) Use our CSTs to quantify the effectiveness of moderate intensity aerobic exercise (mAE) as a disease modifying therapy to improve PD-related motor and cognitive function using serum (human & rat) and rat brain tissue.
Background: 60 million people are projected to have PD by 2037 as the fastest growing neurodegenerative disease in the United States with Texas residents expected to grow at a higher rate than the national statistics.1,2 Presently, there is no cure for PD. Dopamine (DA) replacement therapy is the standard PD treatment although it is a 50-year-old drug where efficacy depends on patients undergoing a complex dosing regimen often plagued with extended ‘Off’ periods of instability and adverse side-effects impacting both motor and cognitive function. Moderate aerobic exercise (mAE) is known to improve some aspects of motor and cognitive function;3,4 however, the neurobiological mechanisms underlying mAE efficacy warrant further investigation with CSTs.5
Methods: A proof-of-concept, matched-control CSTs identified neurobiological mechanisms of effective mAE in early-stage idiopathic PD subjects and in 6-OHDA-lesioned rats [Figures 1, 2]. PD subjects were age and IQ-matched to non-PD healthy controls (NPHC) grouped as mAE vs. exercise naïve (EN). 18-mos rats (human PD onset ∼60-yrs-old) randomized to 3-mos of mAE vs. EN post-lesion vs. sham. Blood collection followed human CLIA, IRB, and rat IACUC standards. Multivariate general linear modeling with post-hoc comparisons, Pearson correlation, and receiver operating characteristics were used (95% CI, p<.05).
Results: mAE resulted in better motor and cognitive test performance as measured with neural and astrocytic serum biomarkers in humans [Table 1,2] that aligned with serum and brain tissue in rats [Figures 3,4,5].
Conclusion: Here, we have elucidated the core neurobiological mechanisms of mAE efficacy using cross-species-aligned motor and cognitive function tests, serum from patients with early-stage idiopathic PD and aged 6-OHDA lesion rats and rat brain tissue compared to healthy human and rat control subjects.

P27.05
1 Robert Gordon University, United Kingdom
2 Northumbria University, United Kingdom
3 University of Syndney, Australia
4 Newcastle University, United Kingdom
5 Teeside University, United Kingdom
6 Teeside university, United Kingdom
7 Sheffield Hallam University, United Kingdom
8 University Hospitals of Derby & Burton NHS Foundation Trust, United Kingdom
9 Department of Neurology, Manchester University, Manchester Centre for Clinical Neurosciences, Northern Care Alliance NHS Foundation Trust, Salford, UK, United Kingdom
Background: Pain is one of the most prevalent and distressing non-motor symptoms of Parkinson’s disease (PD), yet remains under-recognised and inadequately managed. Limited evidence exists on non-pharmacological interventions that specifically target pain in people with Parkinson’s (PwP). Empowering people to self-manage their pain can enhance autonomy and quality of life. Identifying and evaluating existing interventions and resources is critical to inform clinical practice and shape future research to improve pain self-management for PwP.
Objective: To map and critically appraise existing evidence on pain management in PD, focusing on behavioural interventions, educational, and professional resources, and strategies supporting self-management.
Methods: A scoping review of published and grey literature (2010–2025) was undertaken. Searches were conducted across PubMed, SCOPUS, CINAHL, MEDLINE, Web of Science, APA PsycINFO, and ASSIA. Two reviewers independently screened records. Data were extracted, thematically analysed and mapped to the Theoretical Domains Framework and COM-B components
Results: Twenty-one studies were included: 12 intervention trials, five systematic reviews, one observational, two mixed-methods, and one qualitative study. Ten intervention trials investigated exercise, primarily targeting posture; six aimed to reduce pain, and only one specifically recruited PwP with pain. Two trials used psychological approaches, but none delivered a tailored biopsychosocial intervention. Most reported numerical pain scales, with variable effects and pain was often a secondary outcome, measured using mixed PD-specific and generic tools. Barriers to pain self-management, mapped to COM-B components, included insufficient knowledge, limited professional support, and psychological challenges such as fear and depression. Facilitators were a sense of control and acceptance. Sixty-nine grey literature sources were reviewed; many advocated physical activity and biopsychosocial approaches, though detailed, actionable guidance was lacking.
Conclusion: This review highlights limitations in the evidence-base for pain management in PwP. Few interventions specifically target pain or adopt a biopsychosocial approach. Identified behavioural strategies and supports for pain self-management are limited, and pain is often a secondary focus. There is a need for evidence-based, tailored resources that address the complexity of pain and empower PwP to manage it effectively.
P27.06
1 Newcastle University, United Kingdom
2 Northumbria University, United Kingdom
3 University of Oxford, United Kingdom
4 University of Glasgow, United Kingdom
5 Imperial College London, United Kingdom
6 Kings College Hospital London, Dubai, UAE PDNMG, Kings College Hospital, London, UK Dementech Clinical Neuroscience Centre, London, UK, United Kingdom
7 Northumbria University. The Newcastle Upon Tyne Hospitals NHS Foundation Trust., United Kingdom
8 Northumbria Healthcare NHS Foundation Trust, United Kingdom
9 Salford Royal NHS Foundation Trust, United Kingdom
10 Newcastle University, UK., United Kingdom
Introduction: Pain is common in Parkinson’s. Whilst pain in Parkinson’s has been explored at one point in time, little has been done following the same cohort over time to comprehensively assess and evaluate pain and understand its trajectory.
Methods: Participants in the ‘Parkinson’s Pain Study’ were invited for follow up assessments (mean of 8.7±0.7 years) to explore how pain in Parkinson’s changes over time. Pain was assessed using The King’s Parkinson’s Pain Scale (KPPS) and Short Form McGill Pain Questionnaire (SFMPQ). Demographics, Parkinson’s symptom severity, experiences of daily living and motor symptoms (Movement Disorders Society Unified Disease Rating Scale; MDS-UPDRS) and quality of life (EQ5D) were assessed at baseline and close to follow up; anxiety and depression (Leeds Anxiety and Depression Scales) were assessed at baseline. Linear mixed effects modelling controlling for baseline covariates was used to assess change in pain over time.
Results: We recruited 111 people with Parkinson’s (PwP) with longitudinal follow up data. Overall pain burden significantly increased over time (KPPS and SFMPQ total), SFMPQ sensory and affective pain scores also significantly increased over time (p<0.05 for both). Increased pain (KPPS) was associated with increased non-motor symptoms severity (MDS-UPDRS I), higher baseline depression and higher baseline anxiety over time (p<0.05 for all), but not activities of daily living, motor symptoms, motor complications (MDS-UPDRS I, III, IV) or quality of life (EQ5D). Higher cross-sectional non motor symptoms scores were associated with increasing pain (SFMPQ total, sensory and affective scores, p<0.05 for all) but change over time was not (p>0.05 for all). Higher baseline anxiety was associated with higher cross-sectional pain severity in the SFMPQ total and affective scores (p<0.05 for both), but not with change in pain over time.
Conclusions: The severity of pain in Parkinson’s increases over time, however this is not explained by motor symptoms or complications. How PwP describe their pain is important to consider, with those showing a stronger emotional response to pain reporting higher anxiety. Pain in Parkinson’s increases over time and is closely linked with affective and non-motor symptom burden rather than motor progression. These findings highlight the need for routine pain monitoring and integrated management strategies to improve overall wellbeing in PwP.
P27.07
1 University College Cork, Ireland
2 My Moves Matter, Ireland
INTRODUCTION: Non-motor symptoms (NMS) such as mood, autonomic, and cognitive changes are common in Parkinson’s disease (PD) and strongly influence wellbeing. Women with PD (WwPD) experience greater non-motor burden and psychosocial vulnerability than men, yet female-focused research remains is limited. Understanding these symptom patterns and intervention use is critical to advancing gender-responsive care for PD.
OBJECTIVE: To describe self-reported non-motor symptom burden and psychosocial experiences among WwPD.
METHODS: WwPD aged >18 years were recruited to complete surveys capturing self-reported demographic and clinical characteristics, motor and non-motor symptoms, and current interventions accessed. n=502 participants completed an anonymised initial online survey and n=42 completed a follow-up survey. The 30-item Non-Motor Symptoms Questionnaire (NMSQuest; Chaudhuri et al 2006) was used to calculate total scores and to grade NMS burden (Chaudhuri et al 2015). At baseline, 520 WwPD completed the survey, of these 42 completed both Time 1 and Time 2 surveys (mean interval 247 days, SD=97; range 36–410). Paired-samples t-tests examined change in total NMSQuest scores.
RESULTS: At baseline, mean estimated (midpoint) age was 57.2 (SD=10.7). NMS were highly prevalent, with fatigue (72.3%), sleep disturbance (64.8%), constipation (53.5%), and anxiety/depression (49.6%) most frequently reported.
Mean NMSQuest score (M=8.12, SD=4.81) indicated moderate burden; 36.4% reported severe or very severe burden levels. In the paired cohort (N=42; midpoint age 54.63 (SD=8.99)), NMSQuest totals were stable between Time 1 (6.67±3.25) and Time 2 (6.86±4.08), t(41) = –0.43, p=.67, d=–0.07. Mild/moderate burden remained consistent (≈78%), while very severe burden rose slightly (n=0→4). Engagement in supportive interventions at baseline was limited. Fewer than half reported attending physiotherapy (47.5%), and participation in speech, occupational, or nutrition therapy were individually <16%. No participants listed mental-health interventions under “Other,” despite frequent reporting of anxiety and depression.
CONCLUSIONS: Non-motor symptom burden reported by WwPD was high and consistent over time. The absence of reported mental-health interventions, despite prominent mood symptoms, indicates substantial unmet psychosocial need. Findings underscore the necessity of integrating psychological and multidisciplinary support within gender-responsive Parkinson’s care.
P27.08
1 University of California San Francisco, Weill Institute for Neurosciences, United States
2 University of California San Francisco, Division of Geriatrics, United States
3 Rush University Medical Center, Department of Neurological Sciences, United States
Introduction: Parkinson’s disease (PD) develops over an extended period before diagnosis, during which people may experience subtle motor and non-motor changes. This early phase represents a critical window for recognizing PD before the disease is fully manifest. Understanding the earliest changes and when they are noticed relative to diagnosis may inform strategies for early detection, when future interventions may be most beneficial. This study aims to explore the types and timing of self-reported changes experienced by people with Parkinson’s disease (PwPD) prior to clinical diagnosis.
Methods: We invited PwPD participating in the Fox Insight study to complete a survey describing changes they experienced before their PD diagnosis. The survey was designed to capture the presence and onset of motor, autonomic, sleep, emotional, cognitive, and sensory changes.
Results: A total of 5,797 PwPD completed the survey. The mean age was 64.4 ± 8.9 years, 49.5% were male, and 96.7% identified as white. The mean age at diagnosis was 60.2 ± 9.8 years. Motor changes were most frequently endorsed (91%), followed by autonomic (70%), sleep (65%), emotional (51%), cognitive (47%), and smell/taste changes (45%). Among specific changes, shaking or tremor in arms or legs (50%), reduced ability to smell (42%), smaller handwriting (37%), getting up regularly at night to pass urine (37%), and difficulty staying asleep at night (36%) were reported most often. Sleep (54%), autonomic (52%), and emotional (36%) domains showed the highest proportions of PwPD endorsing changes ≥4 years before diagnosis and remained the most frequently reported domains >10 years before diagnosis (23%, 18%, and 12%, respectively). Among those endorsing each change, feeling sad most of the time (34%), feeling claustrophobic (32%), having frightening dreams (29%), constipation or needing to strain to pass a stool (29%), talking in your sleep (28%), feeling hopeless (26%), and feeling nervous or anxious (25%) were most frequently reported to have begun more than 10 years before diagnosis.
Conclusions: Sleep, autonomic, and emotional changes were among the earliest reported changes in PwPD, emerging more than a decade before motor features and clinical diagnosis. Characterizing the chronology of early PD changes may support efforts to refine PD screening and facilitate earlier detection and treatment.
P27.09
1 University of Michigan, United States
2 University of Michigan, Ann Arbor, MI, United States
Background: Sarcopenia can accompany Parkinson disease (PD) as an apparent peripheral muscular symptom that typically is attributed to increased sedentariness and aging. However, it is unclear whether central mechanisms may also play a role. The objective of the study is to examine the relationship between lower appendicular lean body mass and brain vesicular acetylcholine transporter (VAChT) PET binding in persons with Parkinson’s disease (PwPD) while controlling for the effect of age.
Methods: 37 PD patients (age=66.3±5.9 years, Hoehn and Yahr stage 2.4±0.6) underwent whole body tissue absorptiometry using a Hologic DEXA scanner and cholinergic brain PET imaging of the VAChT using the [18F]-FEOBV PET radioligand. Appendicular lean body mass (kg/m2) was calculated. [18F]-FEOBV PET was performed using delayed phase equilibrium imaging and a white matter reference region.
Results: Mean appendicular lean body mass was 7.73±1.61 kg/m2. Mean cortical 18F]FEOBV was 1.14±0.1. Lower appendicular lean body mass was associated with decreased cortical VAChT activity (R=0.38, P= 0.019).
Conclusions: Appendicular lean body mass (sarcopenia) correlates with cerebral cholinergic innervation in PD independent of age. This finding suggests a disease specific effect on frailty in Parkinson's disease. Further research is needed to determine whether cerebral cholinergic denervation is part of the so-called brain-muscle axis associated with parallel loss of spinal cord motor neuron cholinergic or neuromuscular junction frailty, leading to weakened peripheral muscular function that in turn may affect brain function in PwPD.
P27.10
1 SIBI, Ecuador
Abstract Introduction.
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by neuronal loss in specific brain regions, producing motor symptoms such as bradykinesia, tremor, rigidity, and postural instability, thereby increasing the risk of falls. Although levodopa therapy improves quality of life, fluctuations in motor response (“on” and “off”) reflect variations in treatment efficacy and central nervous system function, which emotionally affect patients who may experience anxiety, frustration, and psychological difficulties.
Methodology.
This study analyzed the relationship between motor fluctuations and emotional state in 50 patients with Parkinson’s disease, recruited from support groups.
Instruments and Procedures.
Symptom diaries, the Hamilton Anxiety Rating Scale (HAM-A), the Beck Depression Inventory-II (BDI-II), the Psychological Well-Being Scale (PWB), and semi-structured interviews were used to explore subjective experiences.
Data Analysis.
Quantitative analysis included descriptive and correlational statistics, while qualitative analysis was based on coding and thematic analysis to identify emotional and coping patterns.
Results.
The data showed that motor fluctuations are associated with greater emotional distress. An average of three “off” episodes per day was observed, lasting approximately 45 minutes each. Significant correlations were found between the frequency and duration of these episodes and higher levels of anxiety (r = 0.65) and depression (r = 0.70). Eighty-four percent of participants reported motor fluctuations, mostly occurring in the afternoon and evening. During “off” periods, negative emotional symptoms increased, affecting overall quality of life. Furthermore, longer disease duration and higher levodopa doses increased the likelihood of frequent fluctuations.
Conclusion.
Understanding the “on-off” dynamics in Parkinson’s disease requires an integral and interdisciplinary approach that combines medical care with psychological support. Prioritizing mental health helps reduce stress, anxiety, and depression, while improving treatment adherence and autonomy. Humanizing care involves listening to and understanding the patient, thereby strengthening their well-being, quality of life, and dignity in facing the challenges of Parkinson’s disease.
P27.11
1 University of Delaware, United States
Dual-tasking has been shown to impair gait in individuals with Parkinson’s disease (PD), underscoring the impact of divided attention on motor performance. While bimanual coordination is also understood to be impaired in PD, the effect of divided attention on upper limb motor control has yet to be explored. Understanding how attention demands affect bimanual coordination is crucial as many daily activities require both hands and divided attention simultaneously. This study aimed to examine the effect of a concurrent selective attention task on bimanual force production in older adults with and without PD. Participants (14 older adults [OA], 6 PD) completed a bimanual modified pinch-grip isometric sustained force production task at 15% and 30% of their maximum voluntary contraction. Force production was visually guided with real-time feedback projected as two bars to a screen in front of the participants. Participants were instructed to produce and maintain steady force to match a bottom participant-controlled bar the top target bar. Participants completed 10 trials at each force level in a block design once as a stand-alone motor task and once in conjunction with a selective attention task as a part of the dual-task condition. The dual task consisted of counting the number of letters in an audio clip while disregarding any numbers. Both groups exhibited increased standard deviation of normalized force at the higher force level, with the PD group experiencing greater variability. The PD group also demonstrated greater absolute error and coefficient of error than the OA group at the higher force level. These findings extend prior unimanual literature to demonstrate similar effects of dual-tasking on bimanual force control. At the lower force level, both groups showed greater absolute error in the dual-task condition compared to the single-task condition, highlighting the effect of divided attention in lower force demand conditions. Notably, the absolute error was greater in the PD group for the dual-task lower force condition. The initial results demonstrate that individuals with PD exhibit greater deficits in force variability and error in response to a dual-task condition than older adults at lower force levels. These findings suggest a potential interaction between the resources required for low-level motor tasks and selective attention tasks resulting in greater error for the motor task. However, these results remain to be confirmed in a larger cohort.
P27.12
1 Saint Louis University, United States
2 University of Nevada, Las Vegas, United States
3 Washington University in St. Louis, United States
Background: Although the prevalence of Parkinson’s disease (PD) symptoms has been a common topic of inquiry, patient perceptions regarding the most problematic PD symptoms are not well understood. Further, how their individual experiences related to the perceived extent of these symptoms could provide targets for interventions. The purpose of this study was two-fold: 1) to describe perceived symptom impact and 2) to determine the influence of fall history on perceived symptom impact among people with PD.
Methods: 292 people with PD (mean age: 66.7 ± 10.6; 50.6% female; mean PD duration: 7.8 years ± 7.0)) completed the Survey of Treatment, Exercise, Participation, and Symptoms in PD (STEPS-PD). Participants rated the extent to which specific PD symptoms were problems on a visual analog scale from 0 (not problematic) to 100 (very problematic). Additionally, falls over the prior year were reported and participants were subsequently classified as fallers or non-fallers. For aim 1, means, standard deviations and 95% confidence intervals across the entire sample were calculated. Additionally, a one-way ANOVA was conducted with Tukey post hoc tests to determine differences in degree symptoms were perceived as problematic. For aim 2, one-way ANOVAs were conducted between fallers and non-fallers.
Results: Participants rated fatigue as their most problematic symptom (μ= 50.4, ps<0.001). Additionally, poor balance (μ= 40.6), sleep disturbances (μ= 42.9), stiffness (μ= 41.3), and weakness (μ= 42.4) were rated as the next most problematic symptoms. Notably, sensory disturbances were the least problematic symptom reported. Among the sample, 157 reported at least one fall in the prior 12 months and were classified as fallers. Symptoms were nearly universally perceived as more problematic among fallers compared to non-fallers (excepting tremors). Among motor symptoms, balance (η2=0.179, p<0.001) and fear of falling (η2=0.169, p<0.001) were the most different between fallers and non-fallers. They also differed on non-motor symptoms, including speech (η2=0.120, p<0.001), swallowing (η2=0.111, p<0.001), and cognitive difficulties (η2=0.113, p<0.001).
Conclusions: These findings underscore the need to further explore the mechanisms contributing to heightened symptom perception among fallers. Future studies should examine whether interventions targeting fatigue, balance confidence, and fall-related fear can mitigate perceived symptom burden and improve participation.
P27.13
1 Grenoble Institut Neurosciences, France
2 Alan Edwards Center for research on pain, McGill University, Canada
3 Grenoble Institut des Neurosciences, France
Central neuropathic pain and chronic pain in Parkinson’s disease (PD) suggest potential dysfunction in the brain circuits involved in pain perception and processing. However, the precise pathophysiological mechanisms underlying these symptoms remain unclear. The literature suggests that these pain symptoms may be due to a dysfunction in the inhibitory pain control pathway originating in the Periaqueductal Gray nucleus (PAG). Despite this hypothesis, the functional state of the PAG has not been experimentally investigated in the context of PD.
Using both female and male PD mouse models, we first behaviorally assessed the activity of the descending inhibitory pain pathway using the Diffuse Noxious Inhibitory Control (DNIC) test. Subsequently, we recorded the firing rates and nociceptive responses of PAG neurons using in vivo extracellular electrophysiology in anesthetized mice.
Preliminary results from the DNIC test showed a decreased efficiency of the descending inhibitory pain pathway in female PD mice but not in male PD mice. Additionally, we found that the electrophysiological activity of neurons in the PAG was differentially affected in PD mice, varying by sub-region of the PAG and sex of the mice. The ventro-lateral part of the PAG, known to be at the origin of the descending pathway, exhibits exacerbated nociceptive responses, with shorter latencies, increased magnitudes and maximum amplitude of the nociceptive responses and increased firing rates. The other columns of the PAG are impacted differentially, with an effect of the sex, with longer latencies for the male mice in the lateral part. But also a lesion effect in the lateral PAG with an increased maximum amplitude of the nociceptive responses and firing rate. Other effects are to be confirmed with the addition of new results.
Those results will be completed with a more detailed analysis which will, for example, differentiate the neurons going to the descending pathway and the other neurons, but the preliminary results show that the abnormal nociceptive responses and firing rates are more pronounced in the neurons involved in the descending pathway.
These findings indicate that the PAG is indeed impacted in the context of PD, with exacerbated nociceptive responses, which may underlie some of the pain symptoms observed in PD patients.
P27.14
1 Transversal Translational Medicine, Luxembourg Institute of Health, Strassen, / Centre Hospitalier de Luxembourg, Luxembourg, Luxembourg
2 Independant Neurologist, Private Practice, Limpertsberg, Luxembourg
3 Luxembourg Center for Systems Biomedicine, University of Luxembourg, Belval, Luxembourg
4 Transversal Translational Medicine, Luxembourg Institute of Health, Strassen / Centre Hospitalier de Luxembourg, Luxembourg / Center for Systems Biomedicine, University of Luxembourg, Belval, Luxembourg
5 Centre Hospitalier de Luxembourg, Luxembourg, Luxembourg
Color discrimination and contrast sensitivity are impaired in Parkinson’s disease (PD) and at the early stage of the disease, they have best discriminative power among different non-motor symptoms. We investigated clinical visual performances (CVP) compared to optical coherence tomography (OCT) in PD patients versus controls, reporting here the CVP findings.
Within the Luxembourg Parkinson’s study, 71 PD patients and 90 healthy controls (age 68.3± 10.8 yrs, respectively 67.3 ± 10.3 yrs.) were recruited. PD duration was 13.5± 3.4 yrs. Patients with atypical Parkinsonism, Mild Cognitive Impairment (MCI) (Montreal Cognitive Assessment (MOCA) <26) or interfering ophthalmological conditions were excluded. We evaluated colour vision by the Farnsworth-Munsell 100 Hue Test (FM) and contrast discrimination (CD) by the Pelli-Robson Test(PR). Statistical analyses included univariate and multivariate logistic regression for PD diagnosis, and linear regression for associations with motor severity (MDS-UPDRS III), disease duration, levodopa equivalent daily dose (LEDD), and cognition (MoCA).
PD patients showed significantly worse performance in the FM total error score (76.42±70.93) versus controls (51.37±51.43)(p=0.014) and in 4/5 axes of the FM (p<0.05). PD patients also demonstrated reduced CD values across all three measures (CD Right eye: p<0.001; CD Binocular: p=0.020; CSF Left eye: p=0.041). We found that 7 out of 8 visual variables showed significant univariate associations with PD diagnosis, with 5 remaining significant after adjustment for age and sex (p<0.05). CD Right eye emerged as the most significant predictor (AUC=0.647, p=0.0005). The full multivariate model including all vision variables achieved an AUC of 71.1%. In PD patients, FM Axe 2, FM Total Score, CD Binocular correlated significantly with motor severity (UPDRS-III), FMAxe 2, FM Axe 3, FM Total Score, CD Right eye correlated with cognition (MoCA) and FM Axe 2, FM Axe 3 with disease duration, but not with LEDD.
Clinical visual testing reliably identifies PD patients and correlates with disease severity markers. Deficits in colour and contrast discrimination appear unaffected by the dopaminergic medication, and progress with disease duration. These easily performable, cost-efficient tests should be integrated into prodromal PD research protocols. Future validation as disease progression markers and comparison with OCT findings are warranted.
P27.15
1 Clínica Universidad de Navarra, Spain
2 Universidad Pública de Navarra, Spain
Introduction: High-Intensity Focused Ultrasound (HIFU) is a therapeutic option for patients with movement disorders, including Parkinson’s disease (PD) and essential tremor (ET). While its efficacy in tremor control has been demonstrated, objective assessments of gait changes after treatment remain limited. This study aimed to evaluate gait parameters in PD and ET patients at baseline and six months after HIFU treatment, identifying potential group-specific patterns and longitudinal changes.
Methods: Twenty-nine patients were included: 20 with ET (14 were treated with unilateral and 6 with bilateral thalamotomy) and 9 with PD who underwent unilateral thalamotomy. Baseline and at 6 months follow-up gait analysis were performed using accelerometric parameters (velocity, cadence, stride time and length, step/stride regularity, symmetry, smoothness, acceleration peaks, and energy). Longitudinal changes within groups (baseline vs. 6 months) were evaluated using Bland–Altman analysis and paired t-tests.
Results: At baseline, no significant differences were found between ET and PD groups across all gait parameters (p>0.05). In ET patients, acceleration peaks on the treated side significantly increased (p=0.01), whereas PD patients showed no significant changes. Subgroup analysis indicated decreased stride regularity in bilateral ET (p=0.04) and increased stride regularity in unilateral ET (p=0.05).
Conclusion: Six months after treatment, all patients with ET showed increased acceleration peaks, although those who underwent bilateral ET treatment demonstrated reduced stride regularity. Patients with Parkinson’s disease (PD) remained clinically stable. These findings should be interpreted with caution given the small sample size. Further studies with larger cohorts and longer follow-up are needed to clarify the functional significance of these gait changes.
P27.16
1 Neurologist, Luxembourg
2 2) Transversal Translational Medicine, Luxembourg Institute of Health, Strassen, Luxembourg, Luxembourg
3 4) Luxembourg Center for Systems Biomedicine, University of Luxembourg, Belval, Luxembourg, Luxembourg
4 5) Department of Neurology, Centre Hospitalier de Luxembourg, Luxembourg, Luxembourg, Luxembourg
Visual disturbances are prominent non-motor symptoms in Parkinson’s disease (PD) (1). Conclusive pathophysiological explanations are so far missing. Retinal detection of Lewy bodies (LB) suggests primary retinal involvement, whereas secondary trans-synaptic retrograde (Wallerian) degeneration, secondary to primary degeneration of neurons in the visual cortex has also to be discussed. Disentangling of these various etiologies may be facilitated by use of Optical coherence tomography (OCT) as allowing separate evaluation of the superimposed different retinal layers in short time and without specific patient preparation needed. It is broadly used in ophthalmology (age-related macular degeneration and glaucoma), but also finds its way into neurology (optic neuritis) and more specifically in neurodegenerative diseases like PD (2). We investigated OCT and clinical visual performances (CVP) in PD patients versus controls, reporting here the OCT findings.
Within the Luxembourg Parkinson’s study (3), 21 PD patients and 32 healthy controls (age 63.1± 9.1 yrs, respectively 70.4 ± 8.1 yrs.) were recruited. PD duration was 11.8± 4.5 yrs. Patients with atypical Parkinsonism, Mild Cognitive Impairment (MCI) (Montreal Cognitive Assessment (MoCA) <26) or interfering ophthalmological conditions were excluded. Around the macula we divided the dataset into 4 anatomically meaningful quadrants (superior, inferior, temporal and nasal) and analysed thickness and volume for the retinal nerve fibre layer (pRNFL) and the ganglion cell layer (GCL). Statistical analyses included univariate and multivariate logistic regression for PD diagnosis, and linear regression for associations with motor severity (MDS-UPDRS III), disease duration, levodopa equivalent daily dose (LEDD), and cognition (MoCA).
PD patients showed significant thinning in the superior macular RNFL (p=0.044 if adjusted for age and sex) and the nasal pRNFL (p=0.04 in the LASSO-Based multivariate model). The advanced machine learning analysis model SVM including all OCT variables achieved an AUC of 84.2% and macular parameters alone achieved 81.7% AUC. In PD patients, OCT findings reliably identify PD patients and correlate with disease severity markers. The deficits appear unaffected by the dopaminergic medication, and progress with disease duration. OCT could be integrated into prodromal PD research protocols. Future validation as disease progression markers and further comparison with CVP findings are warranted.
P27.17
1 Universidade Federal de Sao Paulo, Brazil
2 UNIFESP, Brazil
Background: Parkinson Disease has prevalent non-motor symptoms, including sensory and oral dysfunctions. Non-invasive biomarkers, such as salivary alpha-synuclein, are crucial, but their relationship with these symptoms is not yet fully established.
Objective: To identify profiles in PD according to salivary flow, alpha-synuclein, total protein and alpha-amylase levels, olfactory and gustatory sensitivities, and self-perception of swallowing disturbances and xerostomia.
Method: This case-control study included 65 PD participants (age range 44-88y; mean=68.4y) and 25 control ones (45-92y; mean=66.8y). Swallowing and xerostomia perception were assessed using the Eating Assessment Tool (EAT-10) and Xerostomia Inventory, respectively. Gustatory sensitivity was measured with the Three-Drop method, while isopropyl alcohol solutions detected the olfactory threshold. Salivary flow, alpha-synuclein, alpha-amylase and total protein concentrations were measured in saliva samples. Statistical analysis included Mann-Whitney test and K-means cluster analysis. Results: PD participants exhibited higher unstimulated salivary flow than controls (0.32±0.03 x 0.20±0.04 mL/min), although both showed normal ranges. EAT-10 scores, olfaction threshold, and gustatory sensitivity differed between groups (p<0.05). Alpha-synuclein levels and alpha- synuclein adjusted for salivary flow were lower in PD individuals (p<0.05). Salivary alpha-amylase, total protein and xerostomia complaints did not differ. Three clusters were identified: ‘Better sensory ability’ highlighting the relation between lower olfactory and gustatory thresholds and higher alpha-synuclein levels; ‘Lower gustatory sensitivity’, on the relation between lower alpha-amylase levels and lower gustatory sensitivity; and ‘Swallowing complaints’ with higher EAT-10 scores, lower olfactory sensitivity and lower alpha-synuclein concentrations. Conclusions: In PD, alpha-synuclein concentrations are consistently decreased, along with olfaction and taste. Moreover, clusters emphasized the relation between alpha-synuclein concentration, swallowing complaints, and lower olfactory and gustatory sensitivities.
Keywords: Parkinson Disease, Smell, Taste, Saliva, Alpha-Synuclein, Alpha-Amylase.
P27.18
1 USP, Brazil
Functionality is considered the third health indicator, complementing the traditional mortality and morbidity metrics. However, functionality is rarely assessed systematically in Parkinson’s disease (PD) clinical practice and research, where symptom-based scales predominate. Identifying declines across various dimensions of functionality in PD is essential for patient education, disease management, and guiding new intervention strategies. The World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0) is a comprehensive assessment tool developed by the World Health Organization (WHO) based on the International Classification of Functioning, Disability and Health (ICF) to standardize the measurement of functionality and disability impacts across diverse health conditions and cultural contexts. This study aimed to characterize functionality across PD severity stages using the WHODAS 2.0, independent of age, sex, socioeconomic status (SEC), and education. A total of 352 patients were divided into four clinically severity PD stage groups according to the Hoehn & Yahr (H&Y) scale. The age, sex, SEC and education levels were controlled to guarantee paired groups. All participants were evaluated remotely using the Telephone - Montreal Cognitive Assessment (T-MoCA), Beck Depression Inventory (BDI), Movement Disorder Society – Unified Parkinson's Disease Rating Scale, Part I (MDS-UPDRS I) and Part II (MDS-UPDRS II) and WHODAS 2.0. The most affected functionality dimensions were Mobility, Activities of Daily Life related to the Household, and Participation. The nonparametric Kruskal-Wallis test revealed a significant effect of the group for all functionality dimensions. Notably, Mobility, Activities of Daily Life related to the Household, and Self-Care showed a gradual decline starting from stage 1 of H&Y. In contrast, Cognition, Getting Along and Participation exhibited progressive impairment only from stage 2 of H&Y. This study is the first to describe functionality in PD using WHODAS 2.0 across severity stages controlling for key demographic factors. Findings highlight that WHODAS captures functional limitations not identified by symptom-focused scales such as MDS-UPDRS. Incorporating WHODAS into routine assessment may improve patient-centered care by informing interventions targeting functional limitations from early disease stages.
P27.19
1 University College Dublin, Ireland
2 University of Toronto, Canada
Background Individuals with Parkinson’s can exhibit alterations in sense of agency (SoA). In neurotypical participants, SoA is reflected in the perceived compression of time between a voluntary action and an associated perceptual event, a phenomenon known as intentional binding. Previous research has indicated potential links between SoA and internal representations of bodily signals (interoception) and movement (motor imagery). Because both interoception and motor imagery can also be affected in Parkinson’s, alterations in these internal representations may contribute to changes in SoA.
This study aims to provide preliminary data on the relationship between SoA, interoception, and motor imagery to better understand the integration of sensorimotor and cognitive processes in Parkinson’s.
Methods Participants with mild to moderate Parkinson’s (N = 10; 6 females; age M = 62.2 years; time since diagnosis M = 4.4 years) completed an intentional binding task in 4 blocked conditions. In baseline conditions, participants were required to judge the timing of a self-generated key press (baseline-key) or a presented auditory tone (baseline-tone). In operant conditions, participants made a key press which was followed by a tone, and estimated the timing of either the key press (operant-key) or the tone (operant-tone).
The intentional binding task provided an implicit measure of SoA (baseline vs. operant timing accuracy for the key or tone), as well as an explicit measure of SoA from subjective ratings of perceived control over actions. Participants also completed measures of interoception (Multidimensional Assessment of Interoceptive Awareness, MAIA-2), explicit motor imagery (Motor Imagery Questionnaire - MIQ-RS), and motor chronometry (difference in timing of executed vs. imagined aiming movements). Relationships between these measures were analyzed using non-parametric correlations.
Results Preliminary results showed a significant inverse correlation between tone-binding and interoceptive awareness, as well as trends suggesting an inverse relationship between subjective judgement of agency and accuracy of motor imagery timing (chronometry).
Conclusions These preliminary findings suggest that altered interoceptive and motor representations in Parkinson’s may disrupt the integration of predictive and reflective processes that support SoA. Further analysis of data from a larger sample is needed to clarify the nature of these relationships.
CLINICAL SCIENCES: Progression & Prognosis
P28.01
1 Brigham and Women's Hospital and Harvard Medical Achool, United States
2 Division of Movement disorders and American Parkinson’s Disease Association Center for Advanced Research, Brigham and Women’s Hospital and Harvard Medical School, United States
OBJECTIVE: To introduce the Harvard Biomarkers Study 2.0 (HBS 2.0), a large-scale, longitudinal, multi-modal resource designed to accelerate biomarker discovery, mechanistic understanding, and precision medicine in Parkinson’s disease (PD) and related synucleinopathies.
BACKGROUND: Accurate diagnosis and disease-tracking in PD remain limited by the absence of validated biomarkers. Building on two decades of the Harvard Biomarkers Study (HBS 1.0), HBS 2.0 expands this landmark natural-history cohort under new leadership to integrate comprehensive clinical, genetic, and biochemical data with cutting-edge analytical approaches.
DESIGN/METHODS: HBS 2.0 enrolls 2,500 participants (1,000 PD, 1,000 other neurodegenerative diseases, 500 controls) with baseline and seven annual follow-ups. Data include standardized motor, cognitive, autonomic, and olfactory assessments; blood, saliva, and optional CSF sampling; wearable sensor and telehealth modules; and linkage to other MGB-directed studies (MyTrial, CLIMB, Kneu Health). Integration of legacy HBS 1.0 datasets into a unified REDCap/i2b2 infrastructure enables harmonized querying and cross-study interoperability. Additionally, biochemical pipelines include optimization of quantitative α-synuclein seed amplification assays (SAA) in plasma and neuronal models. Lastly, genomic analyses leverage rare-variant association frameworks (SKAT-O, NERINE) to identify genetic determinants of progression.
RESULTS: Harmonization and database development have achieved full alignment of HBS 1.0 and HBS 2.0 variables. This allowed us to conduct slope analyses of UPDRS and MMSE trajectories, delineating fast versus slow progressors, and supporting downstream genotype–phenotype association testing. Biochemically, pilot SAA and immunoprecipitation methods demonstrate improved specificity for α-synuclein seed detection in plasma. Genomically, preliminary NERINE analyses highlight autophagy and vesicle-trafficking modules as enriched for PD-associated rare variants.
CONCLUSIONS: HBS 2.0 represents one of the world’s most comprehensive PD biorepositories, integrating longitudinal clinical, genetic, and biospecimen data. Its open-science infrastructure and methodological innovations establish a powerful platform for biomarker discovery, mechanistic insight, and future clinical-trial readiness in PD and related disorders.
P28.02
1 Institute of Neurobiology Universidad Nacional Autonoma de Mexico, Mexico
Background: Parkinson's disease (PD) is characterized by motor and non-motor heterogeneity, with phenotypes ranging from predominantly motor to predominantly cognitive. The factors driving this disparity remain poorly understood, and prognostic tools to differentiate these trajectories are lacking.
Objectives: To evaluate longitudinal cognitive trajectories in PD, prodromal, and healthy control cohorts, and to assess the impact of sex, chronological age, age at diagnosis, and years of education on cognitive decline.
Methods: We analyzed data from the Parkinson’s Progression Marker Initiative (PPMI), including PD patients (n=380), prodromal individuals (n=914), and healthy controls (n=179), assessed annually with the Montreal Cognitive Assessment (MoCA) from 2013 to 2024. Cognitive trajectories over a 10-year follow-up were analyzed using generalized linear mixed models. We also implemented a maintainable analysis pipeline for real-time model updates as new PPMI data is released.
Results: Later age at diagnosis (>50 years) was strongly correlated with a steeper rate of global cognitive decline. Male sex was identified as a significant predictor of lower MoCA scores over time, while a higher number of years of education was a protective factor against cognitive decline.
Conclusion: Our findings delineate a predictive profile for cognitive decline in PD, where late-onset disease and male sex are risk factors, and higher education is protective. This model aids in stratifying patients for prognostic accuracy and could inform the development of targeted therapeutic strategies. The dynamic analysis pipeline ensures these models remain current, enhancing their potential for clinical translation.
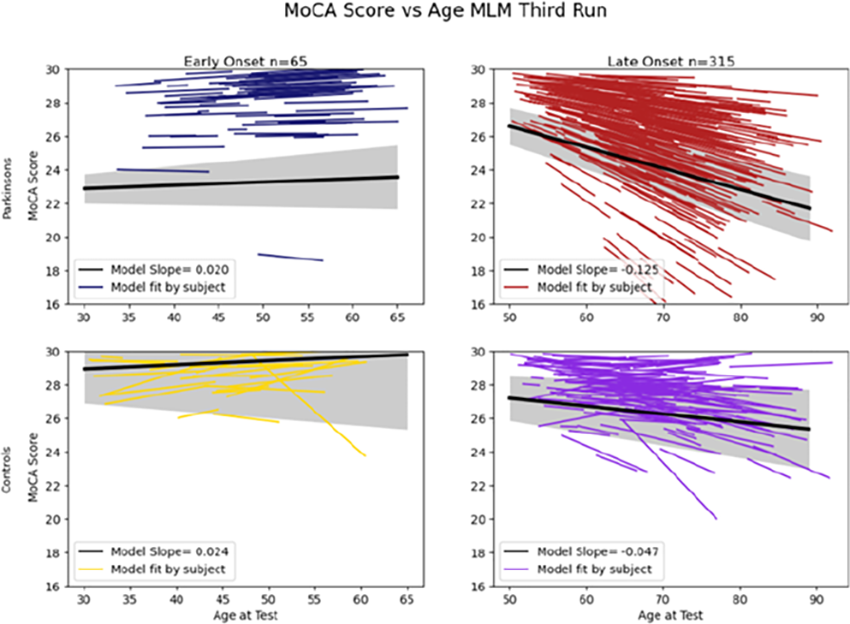
P28.03
1 University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Nuclear Medicine, Germany
2 University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Nuclear Medicine | Molecular Organization of the Brain, Institute for Neuroscience and Medicine II, Research Centre Juelich, Germany
3 University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Nuclear Medicine | Molecular Organization of the Brain, Institute for Neuroscience and Medicine II, Research Centre Juelich, Juelich, Germany | Life Molecular Imaging GmbH, Germany
4 Department of Medical Psychology | Neuropsychology and Gender Studies, Center for Neuropsychological Diagnostics and Intervention (CeNDI), Faculty of Medicine and University Hospital Cologne, Germany
5 Institute of Medical Statistics and Computational Biology (IMSB), Faculty of Medicine, University of Cologne, Germany, Germany
6 University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Nuclear Medicine | Molecular Organization of the Brain, Institute for Neuroscience and Medicine II, Research Centre Juelich | German Centre for Neurodegenerative Diseases, Germany
7 University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Nuclear Medicine | University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Neurology, Germany
Introduction: In Parkinson’s disease (PD), dopaminergic loss progresses asymmetrically across hemispheres—first affecting the putamen on one side before extending to the contralateral putamen, followed by both caudate nuclei. While putaminal dopamine deficits have been linked to motor symptoms, caudate degeneration is associated with cognitive dysfunction. The Dual Syndrome Hypothesis (DSH) attributes executive, attentional, and working-memory deficits to fronto-striatal dopaminergic dysfunction and memory and visuospatial deficits to posterior-cholinergic mechanisms. Yet, whether subregional dopamine loss drives motor and cognitive decline in PD remains unclear, as does the potential of dopamine transporter (DaT) imaging to serve as a monitoring biomarker. Accordingly, we tested whether lateralized DaT loss in the putamen and caudate nucleus is longitudinally associated with motor and fronto-striatal–dependent cognitive symptom progression, respectively.
Methods: We analysed five-year longitudinal data from early-stage PD patients (diagnosis<2 years) enrolled in the Parkinson’s Progression Markers Initiative. Motor symptoms were quantified using the MDS-UPDRS-III (off-medication), and nine neuropsychological tests captured cognitive performance. Based on the DSH and PD mild cognitive impairment criteria, five tests were classified as fronto-striatal–dependent and four as posterior-cholinergic–dependent. Using linear mixed-effects models we tested whether progressive DaT loss (time×DaT interaction), subdivided by striatal subregion and hemisphere, tracked longitudinal decline in motor and cognitive performance, controlling for demographic and clinical covariates.
Results: Among 783 participants (62±9 years; 62% male; MoCA=27±3) contributing 2148 observations, significant interactions (pone-sided<.05) were observed between dopamine loss in (1) the less affected putamen and motor symptom progression, and (2) the caudate nucleus and performance decline in four fronto-striatal–reliant and one posterior-cholinergic neuropsychological test.
Conclusion: Our findings not only largely align with the DSH but also provide strong evidence for a functional dissociation between striatal subregions in driving motor and cognitive symptom progression. The framework in Figure 1 integrates these results, suggesting that region- and hemisphere-specific DaT loss may define imaging-based anchor points for disease progression and support DaT imaging as monitoring biomarker in PD.

P28.04
1 University of Aberdeen, United Kingdom
2 Queen’s University Belfast, United Kingdom
3 Newcastle University, United Kingdom
4 Umeå University, Sweden
5 University of Cambridge, United Kingdom
6 Stavanger University Hospital, Norway
7 University of Bergen, Norway
Background Accurately predicting future outcomes has important benefits for people with Parkinson’s (PwP), including improved planning for the future and facilitating personalised treatment decisions. Standard prediction models combine individual characteristics measured at a single timepoint to predict the risk of future outcomes. Dynamic prediction models update risk predictions at different time points and can incorporate changes to patient characteristics that occur over time. We aimed to develop a dynamic prediction model to predict risk of dementia in PwP.
Methods We analysed pooled data from five prospective, population-based, incidence cohorts in Norway (ParkWest), Sweden (NYPUM), and the UK (CamPalGN, PICNICS, PINE). Dynamic prediction models were developed under a joint modelling framework with individual-participant-data meta-analysis. Together with baseline demographic/clinical variables, we used longitudinal measurements updated over time (MMSE and MDS-UPDRS part 3) to predict the 3-year risk of dementia, shifting forward the time of prediction yearly from baseline (near diagnosis) to 7 years post baseline. We assessed heterogeneity in discrimination and calibration performance between cohorts using internal-external cross-validation.
Results Among 900 PWP, 289 developed dementia over median follow-up of 7 years. We were unable to develop a single model which validated well across all cohorts due to heterogeneity between cohorts. We therefore developed and validated two models. The first model (developed in NYPUM and PINE) had reasonable discrimination (time-dependent AUC [tAUC] 0.59–0.81 in NYPUM; 0.69–0.81 in PINE), and variable calibration performance, with evidence of underprediction for some prediction time points. The second model was developed in ParkWest and externally validated in CamPaIGN and PICNICS. Discrimination was reasonable (CamPaIGN, tAUC=0.65–0.83; PICNICS, tAUC=0.56–0. 69) and calibration performance varied across prediction time points.
Conclusion Despite similar population-based recruitment, major heterogeneity between cohorts limited our ability to develop a generalisable unified model. Dynamic prediction models showed reasonable discrimination ability, but calibration was poor at some time points. This may partly be due to variable follow-up frequencies between cohorts, but further work should identify factors leading to heterogeneity and develop dynamic prediction models which perform well in different settings.
P28.05
1 Clínica Universidad de Navarra, Spain
Introduction: Essential tremor (ET) is the most common movement disorder, but many patients show mild parkinsonian features, such as resting tremor, rigidity, bradykinesia, or reduced arm swing, despite normal dopaminergic imaging. These overlapping phenotypes raise diagnostic and prognostic challenges. MR-guided focused ultrasound (MRgFUS) thalamotomy is an effective therapy for medication-refractory tremor, but it remains unclear whether subtle parkinsonian signs influence clinical outcomes. This study compared tremor improvement and adverse events between patients with classic ET and those with ET plus subtle parkinsonian features and preserved dopaminergic function.
Methods: A retrospective, single-center study was conducted at Clínica Universidad de Navarra including 69 patients, 43 ET and 26 ET with parkinsonian features and normal SPECT/PET imaging (ETp) treated with unilateral MRgFUS thalamotomy targeting the ventral intermediate nucleus (VIM). Tremor severity was assessed using the Clinical Rating Scale for Tremor (CRST) at baseline and 6 months. Primary outcomes were changes in CRST subscales (A: tremor characteristics in different body locations, B: motor tasks, C: functional disability). Adverse events (AEs) were recorded and classified by severity. Linear regression models adjusted for age, sex, severity and duration of the disease were used to explore predictors of outcome.
Results: Improvements in tremor severity after treatment were similar in both groups. Mean CRST A change was 4.12 ± 2.06 in ET and 4.46 ± 2.21 in ETp (p=0.514); CRST B, 10.16 ± 4.84 and 8.46 ± 4.83 (p=0.162); CRST A+B, 14.28 ± 5.88 and 12.92 ± 6.07 (p=0.362); CRST C (median [IQR]), 14.0 [5.0] and 14.0 [4.0] (p=0.742). Total CRST improvement was 28.74 ± 11.63 vs. 25.62 ± 12.73 (p=0.300). Adverse effects occurred in 53.5% of ET and 34.6% of ETp patients (p=0.144), most were mild and transient.
Conclusion: MRgFUS thalamotomy achieved comparable tremor control and safety profiles in ET and ETp groups. The presence of subtle parkinsonian features with normal dopaminergic imaging did not predict poorer outcomes, suggesting these signs may not represent distinct pathophysiology in the context of tremor response. Long-term follow-up will clarify whether these groups diverge in disease progression.
P28.06
1 University of São Paulo, Brazil
2 University of Texas Health Science Center at Houston, United States
3 Health, Clinical and Community Service, Fight Parkinsons, Australia
4 Department of Neurology, Silesian Center of Neurology, Poland
5 NeurologyFaculty of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
6 Department of Neurology, National Neuroscience Institute, Singapore
7 Department of Neurology, Mayoclinic, Rochester, United States
Context: Early-Onset Parkinson’s Disease (EOPD), defined by symptom onset before the age of 50, accounts for 5–15% of all Parkinson’s disease (PD) cases. Despite its prevalence, EOPD remains underrepresented in research and clinical guidelines. Individuals with EOPD face distinct challenges in genetics, psychosocial adaptation, and access to care that differ markedly from those with Late-Onset Parkinson’s Disease (LOPD). Understanding these gaps is essential for developing age-appropriate, integrated care models. Objective: To identify key knowledge gaps, controversies, and unmet needs in the management of EOPD, and to propose directions for clinical practice and research. Methods: A systematic review of the literature on the pathophysiology, epidemiology, and treatment of EOPD identified the specific challenges faced by this population and offered suggestions to improve their care. Results: A total of 146 articles were included. EOPD shows a stronger genetic contribution (notably GBA, PRKN, and LRRK2 variants) and complex gene–environment interactions, including associations with pesticide exposure and head trauma. Epidemiological data suggest increasing frequency in some regions, although underreporting persists in low- and middle-income countries. Individuals with EOPD exhibit slower motor progression but a higher burden of depression, anxiety, impulse control disorders, and sexual dysfunction, significantly affecting social roles, employment, and family life. Despite these unique needs, rehabilitation and multidisciplinary care models remain generalized, lacking dedicated programs for working-age adults. Access to counseling, reproductive health services, and tailored exercise programs is limited. Conclusion: EOPD represents a distinct subgroup that requires targeted strategies. Multidisciplinary clinics dedicated to EOPD should integrate genetic counseling, vocational and psychosocial support, and individualized rehabilitation. Future research should address genotype–phenotype correlations, the timing of advanced therapies, and interventions tailored to younger patients and their caregivers.
P28.07
1 Laboratory for Early Markers of Neurodegeneration, Center for the Study of Movement, Cognition and Mobility, Neurological Institute, Tel Aviv Medical Center, Tel Aviv, Israel., Israel
2 Insight Centre for Data Analytics, O'Brien Science Centre, University College Dublin, Dublin, Ireland, Ireland
3 National Institute for Health and Care Research (NIHR) Newcastle BRC, Newcastle University, Newcastle, UK, United Kingdom
4 Neurorehabilitation Research Group (eNRGy), Department of Rehabilitation Sciences, KU Leuven, Leuven, Vlaams-Brabant, Belgium, Belgium
5 Center for Neurology, University Hospital Tübingen and Hertie Institute for Clinical Brain Research, Tübingen, Germany, Germany
6 Department of Molecular Neurology, University Hospital Erlangen, Erlangen, Germany, Germany
7 Department of Neurology and Center for Health and Technology, University of Rochester, Rochester, NY, USA, United States
8 Gray Faculty of Medicine and Healthy Sciences and Sagol School of Neuroscience, Tel Aviv University, Tel Aviv, Israel., Israel
Introduction: Advances in digital technologies enable monitoring Parkinson’s disease (PD) symptoms. Yet, despite their potential, to date, digital metrics are not used as clinical outcomes in clinical trials or clinical-care. Small study samples, poor generalizability, variance in technologies, methods and algorithms and lack of clinical validation contribute to this gap. The Harmonization project aims to tackle these issues by merging data from several independently projects, in a wide-range of participants with PD to identify and standardize digital markers of daily-living, sensitive to disease severity and progression.
Methods: We incorporated daily-living data collected over 1-week using the Axivity Ax6 sensor in three different studies (Mobilise-D project, WATCH-PD and PPMI). Participants in all three studies wore the sensor on their lower back and data was combined and processed with the same algorithms. To explore difference across disease severity, we first explored turning and mobility. The modified MobGap pipeline was used to extract data on turns and compute digital mobility outcomes (DMOs) using MATLAB. Demographic and clinical data were gathered from each project and combined along with the DMOs into one database.
Results: Data from 886 participants were collated. Groups were similar in age but differed clinically from healthy controls, individuals in the pre-clinical and clinical stages of PD (Mobilise-D: PD: N=548, age: 68±10, MDS-UPDRSIII: 26±12, Females 36% and HC: N=205, age:66±8, Females 35%; PPMI: prodromal subjects: N:92, age=68±5, MDS-UPDRSIII:4±5, Females=55% and WATCH-PD: N=41, age:65±10, MDS-UPDRSIII: 24±9, Females=44%). Three turning DMOs (Fig. 1) show that in early stages, turning is roughly similar in PD and HC, but turning duration and variability increase with disease progression with significant group effect (p <0.01). PD significantly differed from HC and the prodromal group (p <0.01), with no difference between HC and prodromal (p >0.3).
Conclusion: These initial findings show the potential relationship of digital measures of daily living turns to disease severity. Importantly, we demonstrate how combining data from three projects can provide comparisons that were not possible by each project alone. Future work will include integrating additional clinical measures and DMOs to investigate their relationships with clinical outcomes, such as disease progression.
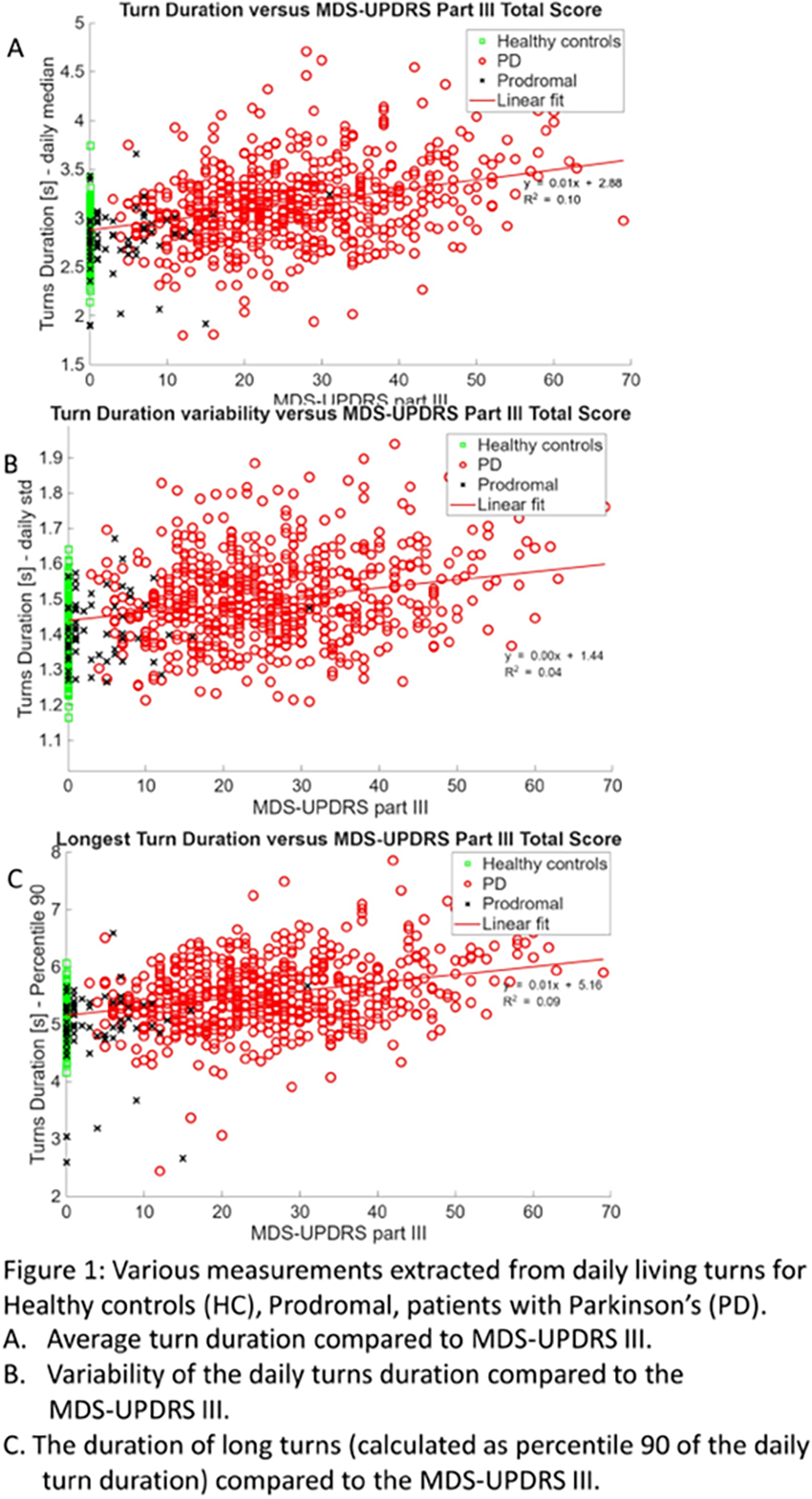
P28.08
1 Iowa State University, United States
Earlier and more accurate detection of Parkinson’s disease (PD) is vital, particularly through diagnostic methods that are rapid, easy, non-invasive, and cost-effective. Despite advances in disease-modifying treatments, no diagnostic chemical test currently exists to confirm the presence of PD. Identifying volatile organic compounds (VOCs) emitted through the skin offers a promising, non-invasive strategy for assessing disease-related metabolic changes. The development of highly selective and sensitive sensors capable of detecting the VOCs associated with PD offers a promising non-invasive approach to improve early diagnosis. In this study, laser-induced graphene (LIG) sensors were fabricated to enable targeted detection of PD-related VOCs: perillic aldehyde, eicosane, hippuric acid, and octadecanol. Data were collected from four participant groups: healthy young adults (HYA), healthy older adults (HOA), persons with PD on dopaminergic medication (PD-on), and de novo persons with PD (de novo). Each participant wore a sensor on the forehead for 30 minutes, during which VOC concentrations were measured at two-minute intervals. Preliminary results reveal there is a distinct difference in total gas emission capacitance between groups (HYA: 33.38 nF, HOA: 27.28 nF, de novo: 40.58 nF, and PD-on: 2.81 nF). While HYA, HOA, and de novo participants demonstrated intermediate levels of biomarker emission, PD-on participants exhibited a pronounced reduction. These results suggest that dopaminergic medication may alter cutaneous VOC expression. Overall, these findings support the feasibility of LIG-based biosensors as a rapid, non-invasive platform for detecting PD-associated biomarkers and highlight their potential role in advancing early diagnostic and disease-monitoring strategies in PD research.
CLINICAL SCIENCES: Epidemiology, genetics and risk factors
P29.01
1 department of Neurology, rz Tienen, Tienen, Vlaamse Parkinson Liga, Belgium
2 Vlaamse Parkinson Liga, Belgium
3 Klief, Oostende, Belgium
4 Department of Neurology, AZ St-Jan Bruges, Belgium
5 Department of Neurology Antwerp University Hospital, Edegem, Belgium
6 Department of Neurology, University Hospitals Leuven, Belgium
7 Department of Neurology, Ghent University Hospital, Ghent, Belgium
Background: Regional epidemiological data on parkinsonism and Parkinson’s disease (PD) are crucial for designing risk reduction and prevention strategies.
Objective: To provide consistent estimates of incidence and prevalence for Parkinson’s disease in Belgium over the past two decades using three complementary national data sources.
Methods: We analysed (1) the Intego primary care morbidity registry which records a diagnosis of parkinsonism (Flanders, 2000–2023), (2) six Sciensano national health interview surveys assessing the presence of Parkinson’s disease (1997–2018), and (3) the National Institute for Health and Disability Insurance (NIHDI) database of reimbursed dopaminergic medication prescriptions (2005–2023). Registry data was age-adjusted to the Belgian population.
Results: Through the Intego registry, we found that the parkinsonism prevalence in Belgium has risen steadily over the years, reaching approximately 50,000 patients by 2023. These results were corroborated independently by the Sciensano surveys and NIHDI database. The overall incidence rate exceeded 0.6 per 1,000 person-years since 2021, resulting in around 7,000 new diagnoses annually. Prevalence rate surpassed 4 per 1,000 people in 2023. The number of patients under 50 years old is estimated at 1,283. Population aging, especially the rise of life expectancy for men, compounded by overall population growth, appears to be the primary driver of these trends.
Conclusions: The findings highlight that Parkinson’s disease represents a sizeable and growing public health challenge in Belgium. The rise in incidence and prevalence underscores the need for targeted prevention, early diagnosis, and optimized care pathways, particularly in an aging population. However, current population registries are fragmented and incomplete, limiting the ability to monitor disease patterns accurately. The development of an inclusive, population-wide registry that integrates clinical, demographic, and prescription data would facilitate the capacity to detect unmet needs, guide healthcare resource allocation, evaluate interventions and ultimately improve outcomes for people living with Parkinson’s disease and other parkinsonisms.
Keywords: parkinsonism, Parkinson’s disease, incidence, prevalence, Belgium, epidemiology
P29.02
1 1 Lab Produtos Naturais, Universidade São Francisco, Bragança Paulista, Brazil 2 Programa de Pós-graduação em Ciências da Saúde, Universidade São Francisco, Bragança Paulista, Brazil, Brazil
2 Programa de Pós-graduação em Ciências da Saúde, Universidade São Francisco, Bragança Paulista, Brazil, Brazil
3 Lab Produtos Naturais, Universidade São Francisco, Bragança Paulista, Brazil, Brazil
Parkinson's disease (PD) is a progressive neurodegenerative disorder that mainly affects the elderly. It is marked by Lewy bodies, composed of aggregated α-synuclein, which disrupt proteostasis and lead to neuronal death, especially in the substantia nigra and motor-related brain regions. Genetic susceptibility involves mutations in PRKN and LRRK2 genes. This study investigated these mutations in PD patients and control individuals (CT) and explored correlations with lifestyle. Forty-four PD cases (sporadic and familial) and 42 CTs were recruited (Ethics Committee 74861423.2.0000.5514). Peripheral blood was collected for DNA extraction, integrity assessment via agarose gel electrophoresis, PCR amplification, and sequencing using a SeqStudio Genetic Analyzer. Data were analyzed with Seq A8 and SeqScape 4, aligned to reference sequences, and compared to ClinVar. Two LRRK2 variants were found: p.P1997= and the pathogenic p.G2019S in one PD patient (2.3%). No homozygous deletion of PRKN exon 4 was detected, but the p.Ser167Asn variant (uncertain significance) and a novel intronic mutation (CACTTC"Y") were observed (20.4%). Lifestyle analysis revealed significant differences between PD and CT groups in diet, physical activity, and intellectual engagement. PD patients reported inflammatory diets, no exercise, and low cognitive stimulation during their lifetime, while CTs showed healthier profiles for years. Among mutation carriers, CTs had higher supplement intake and activity levels, both physical and intellectual, different from PD. These findings confirm known and novel PD-related mutations and suggest lifestyle may influence disease development, even in genetically predisposed individuals for PD.
P29.03
1 Queen Mary University of London, United Kingdom
2 King's College London, United Kingdom
3 University College London, United Kingdom
Introduction: Exploration of the Parkinson’s disease (PD) prodrome has been limited by missing data, lack of longitudinal follow-up, and absence of PD-specific assessments. We previously validated an algorithm to predict phenoconversion to PD (PREDICT-PD algorithm). Here, we present the large PREDICT-PD cohort (n=12,138) and evaluate the performance of prodromal algorithms (such as PREDICT-PD) and simple screening tools.
Methods: Since 2011, 12,138 participants aged 50-80 have been recruited to PREDICT-PD. They completed a website-based battery of questionnaires and assessments at baseline, and were recontacted longitudinally for further submissions. We also carried out ‘passive follow-up’ through linkage to NHS records from inpatient, outpatient, mental health, and mortality datasets. We present the baseline characteristics of the cohort and used Cox regression models to compute hazard ratios (HR) for risk of phenoconverting to incident PD using the PREDICT-PD risk algorithm, the MDS prodromal criteria, baseline olfaction (five-item smell tests), and objective motor assessment (keyboard tapping). We used linear mixed effects models to study how scores change in the years prior to phenoconverting.
Results: All measures were significantly associated with increased risk of phenoconversion: MDS prodromal criteria (HR 1.82/10-fold increase, 95% CI 1.58–2.10, p<2e-16), PREDICT-PD algorithm (HR 2.19/10-fold increase, 95% CI 1.84–2.61, p<2e-16), smell test (HR 1.86/10-fold increase, 95% CI 1.32–2.63, p=0.0004), and keyboard tapping (HR 2.41/10-fold increase, 95% CI 1.71–3.39, p=4.3e-07). PREDICT-PD scores and keyboard tapping performance worsened in the years prior to diagnosis. The MDS prodromal criteria had high specificity but low sensitivity (80% threshold: sensitivity 1.7%, specificity 100%).
Conclusions: Current risk algorithms enrich populations for future PD. The PREDICT-PD algorithm, entirely web-based and cost-effective, offers strong performance compared with the MDS prodromal criteria. Longitudinal assessments can track risk trajectories. The low sensitivity of the MDS algorithm may reflect exclusion of high-likelihood-ratio risk factors in remote settings. The PREDICT-PD algorithm has strong real-world practical utility.
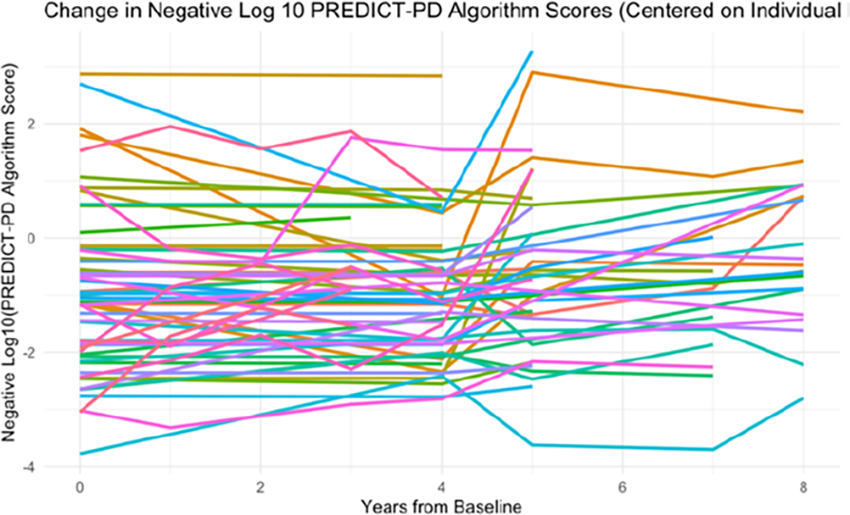
P29.04
1 McGill University, Canada
Introduction: Genetic regulation of messenger RNA stability is often overlooked in the literature, even though RNA stability jointly determines steady-state mRNA abundance alongside transcriptional regulation. Recently, Huang et al. systematically characterized allele-specific RNA stability (asRS) variants across human cell lines, demonstrating the influence of genetic variation on mRNA stability regulation. Building on these findings, we investigated the overlap of asRS variants with Parkinson’s disease (PD) GWAS loci, integrated brain eQTL data, and performed Mendelian randomization to assess possible causal stability-mediated effects in PD.
Methods: Huang et al. identified asRS variants using a metabolic labeling method which tracks newly synthesized mRNA and its decay over time to distinguish allele specific stability differences. Subsequently, using the latest PD GWAS summary statistics, we identified overlapping asRS variants with significant and suggestive loci, integrated brain tissue eQTL data from GTEx to the corresponding asRS genes. Finally, we performed Mendelian randomization and single-SNP MR analyses using the TwoSampleMR package in R, including the Steiger test to evaluate whether the assumption that the exposure likely causes the outcome is valid.
Results: For the overlap of asRS variants and significant GWAS loci, we found variants that are in LD with seven independent lead GWAS loci. For example, asRS variant chr12:45927731:A:T (GWAS p-value 3.53e-9) in the SCAF11 gene, which is in LD with lead GWAS variant chr12:46022785:T:C. Following table shows MR results of three of the ten different brain areas we analyzed (Bonferroni threshold for MR is 0.0029): Conclusion: We identified asRS variants in LD with lead GWAS variants, for instance in the SCAF11 gene which is annotated to be involved in apoptosis. We also found variants of suggestive GWAS significance and eQTL genome-wide significance that reached statistical significance in the MR analysis, for example the mitochondrial gene FAHD1, supporting their potential causal role through RNA stability mechanism.
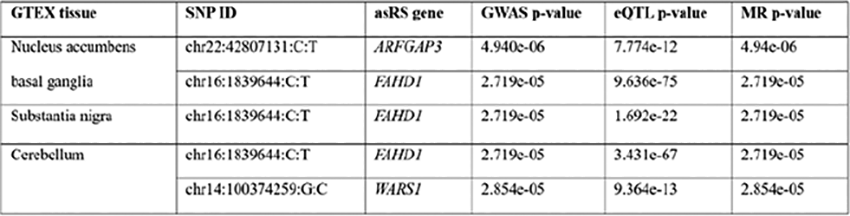
P29.05
1 Raimunda Moura Program for Parkinson’s Disease-SMS/Atibaia/Brazil., Brazil
2 Virtual University of the State of São Paulo, Brazil
MOURA, Marcos1,2; LOUSADA, Kátia2; NUNES, Luiz2; CAMPOS, Edevaldo3; MARTINO, Lucila2; AGUIAR, Marcos2; BERCHOL, Rose2; Rosa, Hans2.
Health Science Program, São Francisco University, Bragança Paulista, São Paulo, Brazil.
Raimunda Moura Program for Parkinsońs Patients, Atibaia, São Paulo, Brazil.
Virtual University of the State of São Paulo, Brazil.
Parkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder marked by heterogeneous trajectories and variable survival outcomes. The Hoehn & Yahr (H&Y) scale provides a standardized framework for staging disease severity and supporting prognostic evaluation. This study aimed to estimate overall survival and assess differences by baseline H&Y stage in a small longitudinal PD cohort initiated in 2015, explicitly addressing analytical challenges imposed by limited sample size and sparse event data. A time-to-event survival analysis was conducted using patient records aggregated to one observation per participant (entry = earliest record; exit = latest record; event = death; otherwise right-censored). Survival was estimated with Kaplan–Meier (KM) methods overall and stratified by baseline H&Y stage, combining Stages 2 and 3 to optimize group sizes. Numbers at risk were reported, and survival curves compared using the log-rank test. Univariable Cox proportional hazards regression was attempted; when unstable, crude incidence rates and rate ratios were calculated from total patient-years at risk. Sixteen patients were analyzed, with 9 deaths and 7 censored observations (Ethical Research Committee of São Francisco University number 5.791.053). Median overall KM survival was 10.0 years (95% CI not estimable). Baseline distribution: Stage 1 = 6; Stage 2 and 3 = 10. KM curves indicated shorter survival for Stage 2 and 3, although the log-rank test did not reach significance (χ2 = 2.226; p = 0.136). Cox estimates were unstable. Crude incidence rates were 0.0345 events/year for Stage 1 and 0.0805 for Stage 2 and 3(rate ratio 2.33; 95% CI 0.49–11.23). Patients with higher baseline H&Y stages exhibited numerically poorer survival, though differences were not statistically significant. The small cohort and limited event count constrained model precision. These findings reinforce both the feasibility and limitations of time-dependent survival analyses in PD and emphasize the need for larger, prospectively followed cohorts to generate robust hazard estimates and integrate additional clinical predictors.
P29.06
1 Queen Mary University of London, United Kingdom
2 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, London, United Kingdom, United Kingdom
3 Data Tecnica International, Glen Echo, MD, USA, United States
4 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, London, United Kingdom, United States
5 Department of Biomedical Science, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia, Malaysia
6 Institute of Neurogenetics, University of Luebeck, Luebeck, Germany, Germany
7 Department of Genetics, Ecology and Evolution, Biological Sciences Institute, Universidade Federal de Minas Gerais, Belo Horizonte, Brazil, Brazil
8 Hospital Regional de Concepción, Universidad de Concepción, Concepción, Biobío, Chile, Chile
9 Department of Biomedical Sciences, Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa, South Africa
10 Department of Neurology, University Medical Centre Ljubljana, Ljubljana, Slovenia, Slovenia
11 Neurology Department, Dr Benbadis University Hospital, Constantine, Algeria, Algeria
12 School of Biomedical Sciences, Faculty of Health, Medicine and Behavioural Sciences, The University of Queensland, Brisbane, QLD 4072, Australia, Australia
13 Laboratorio Internacional de Investigación sobre el Genoma Humano, Universidad Nacional Autónoma de México, Campus Juriquilla, Blvd. Juriquilla 3001, 76230, Santiago de Querétaro, México, Mexico
Goals The Global Parkinson’s Genetics Program (GP2; www.gp2.org) is an international collaborative effort committed to advancing our understanding of the genetic basis of Parkinson’s disease (PD). The Training and Networking group supports global and local capacity building in PD by providing resources and expertise to meet the training needs of GP2 and its collaborators.
Methods The Training and Networking group takes an integrated approach to building research capacity and fostering global collaboration within GP2. We have developed a free online learning platform (https://training.gp2.org/) offering courses in genetics, data science, and research methods to strengthen foundational skills in PD research. We also provide regional training opportunities tailored to local priorities, fostering equitable access and sustainable research capacity in underrepresented populations (URP). To facilitate networking and collaboration, we actively promote communication through the GP2 Trainee Network Slack channel and hold monthly meetings connecting trainees worldwide.
Results The GP2 Trainee Network has engaged 402 members since its launch, with 125+ currently active trainees guided by eight regional trainee representatives. Fifteen bioinformatics workshops have been held in URP countries, most recently in Ghana, Romania, Mexico, and Chile, with several GP2 trainees progressing to co-lead them under the “Train The Trainer” model. To bridge gaps in research opportunities, we have also supported a regional training initiative in Kyrgyzstan and hosted three hackathons. Nineteen PhD and eleven master’s fellowships have been awarded globally, along with 25 Sabbatical and 7 Visiting Scientist placements. Eleven online courses are available on the GP2 Learning Platform, accessed by 1,400+ learners. A new course on Return of Genetic Results was recently launched, with another on Whole Genome Sequencing data analysis in development. Since introducing the Micro e-Learning Program on the ASAP YouTube channel, the videos have accumulated 800 views within seven months. Collectively, these efforts have resulted in 22 completed and 28 ongoing projects, reflecting the growing momentum of trainee-led research across GP2.
Conclusion As GP2 evolves, the Training and Networking group is dedicated to empowering local research capacity and sustaining a growing community of trainees and researchers globally. These initiatives play a critical role in advancing our knowledge of PD genetics.
P29.07
1 Garvan Institute of Medical Research, Australia
2 University of Edinburgh, United Kingdom
3 C4X Discovery, United Kingdom
4 University of New South Wales, Australia
5 Northwestern University, United States
6 C4X discovery, United Kingdom
7 Cure Parkinson's UK, United Kingdom
8 C4X Dscovery, United Kingdom
INTRODUCTION: The cause of Parkinson's disease (PD) is unknown for ∼ 90% of people with the condition (idiopathic PD). PD likely comprises differing disease mechanisms which may contribute to the wide range of symptoms and progression rates. Viewing PD from a single mechanism perspective has hindered progress in finding treatments to slow progression. A Bayesian approach was used to identify genetic subgroups of idiopathic Parkinson’s patients that may reflect distinct disease mechanisms.
RESULTS: A unique genetic signal was identified that stratified PwP into 3 distinct subgroups A/B/C. Multiple novel subgroup-specific risk variants/SNPs were identified, strongly suggesting differing disease mechanisms between the subgroups. To test this hypothesis, we analysed two Phase III trials that targeted different proposed disease mechanisms but had not found efficacy: (i) STEADY-PD3, testing the calcium channel blocker isradipine; (ii) SURE-PD3, testing increased serum urate levels.
Subgroup C participants receiving isradipine displayed significantly slowed clinical progression, relative to subgroup C participants receiving placebo. However, isradipine did not slow progression in participants from subgroup A and B.
In contrast, elevated serum urate levels slowed disease progression in subgroup A participants but not participants from subgroup B or C. Subgroup-specific treatment responses to different targets supported our hypothesis that the three genetic subgroups represent distinct disease mechanisms.
We also analysed an independent PD longitudinal cohort - genetically stratified into subgroups A/B/C- and identified significant differences in clinical features and progression rates between the subgroups, further supporting the relevance of the three genetically defined groups to Parkinson’s disease.
CONCLUSIONS
People with idiopathic Parkinson’s can be divided into three genetic subgroups (A, B, and C). Each subgroup has unique genetic risk variants (SNPs). The subgroups show different clinical responses to disease-modifying treatments (DMTs). The findings support the hypothesis that each subgroup has a different disease mechanism. The findings support re-testing of isradipine in Subgroup C PwP and inosine/urate in Subgroup A PwP The subgroups have distinct patterns of symptom progression. Causal genes have been identified for each subgroup, providing insight into disease mechanisms and potential treatment targets.
P29.08
1 NHS, United Kingdom
2 Queen Mary University of London, United Kingdom
3 Lund University, Sweden
4 Oxford University, United Kingdom
5 Glasgow University, United Kingdom
6 Bristol University, United Kingdom
7 Royal London Hospital, United Kingdom
8 University of Lübeck, United Kingdom
9 University of Lübeck, Germany
Objective: To investigate the impact of type 2 diabetes mellitus (T2DM) on Parkinson’s disease (PD) symptom severity and progression.
Background: Previous evidence has suggested PD patients with T2DM (PD+T2DM) have more severe symptoms and a faster progression compared to PD without T2DM (PD-T2DM).
Methods: A meta-analysis of data from six observational studies* was undertaken. Differences in motor and cognitive symptom severity scores between PD+T2DM and PD-T2DM were cross-sectionally compared at baseline and also longitudinally. The difference in the rate of PD symptom progression (disease trajectory) between PD+T2DM and PD-T2DM was measured by analysing the combined effect of T2DM and time on longitudinal PD severity markers.
Results: In total, 5095 participants were included in the study. Of these, 468 (9.2%) were PD+T2DM. On average, PD+T2DM were older at symptom onset (mean age difference [MAD] = 3.64, p = <0.001) and at diagnosis (MAD = 3.50, p = <0.001). PD+T2DM had worse baseline H&Y stage (mean difference [MD] = 0.12, p = 0.02) and UPDRS-III scores (MD = 2.32, p = 0.03) compared to PD-T2DM. Baseline MoCA scores were non-significantly lower in PD+T2DM compared with PD-T2DM (MD = -0.57, p = 0.06). Longitudinally, PD+T2DM had worse H&Y stages (MD = 0.13, p = 0.03), UPDRS-III scores (MD = 2.55, p = <0.001), and MoCA scores (MD = -0.67, p = 0.02) compared with PD-T2DM. However, the rate of progression was not different between PD+T2DM and PD-T2DM.
Conclusion: Dysregulated metabolic pathways are common to PD and T2DM. Our findings demonstrate worse motor and cognitive symptoms in PD+T2DM compared with PD-T2DM, but no difference in the rate of progression between the groups.
P29.09
1 Ruijin Hospital affiliated to Shanghai Jiao Tong University School of Medicine, China
2 Shanghai Rising Stars of Medical Talents Youth Development Program, China
Objective: This study aims to investigate the causal relationship between disruptions in sleep circadian rhythms and the risk of seven brain disorders.
Background: Disruptions in sleep circadian rhythms have been linked to an increased risk of dementia and mental health issues. However, the genetic-related causal evidence and underlying mechanisms connecting these disruptions to brain disorders remain unclear. Utilizing data from the UK Biobank, this study employs multivariate Cox-proportional hazards regression models, Mendelian randomization, and polygenic risk score (PRS) analysis to elucidate these relationships and identify potential intervention strategies.
Methods: Sleep circadian rhythms, including shift work and sleep quality, were assessed using data from the UK Biobank. Multivariate Cox-proportional hazards regression models and Mendelian randomization were used to analyze the causal effects of disrupted circadian rhythms on seven brain disorders and their impact on brain structure. Sleep-related PRS was calculated to explore underlying mechanisms. Interactive analyses were conducted to identify at-risk populations and potential intervention points, such as physical frailty, physical activity, and CRP levels.
Results: Poor sleep quality was found to have a detrimental effect on brain disorders from both prospective and genetic perspectives. Shift work was specifically associated with an increased risk of stroke, dementia, and MDD. Brain regions, particularly the frontal lobe, were identified as being connected to sleep circadian rhythms. Interactive analyses revealed that physically frail individuals are at higher risk, with physical activity and CRP levels emerging as potential intervention points. PRS-based exploratory analyses suggested mediating effects of physical frailty and CRP in the associations between sleep quality and brain disorders.
Conclusion: This study provides evidence that disrupted sleep circadian rhythms negatively impact brain health and identifies potential mechanisms, at-risk populations, and intervention strategies. The findings highlight the importance of addressing sleep quality and shift work to mitigate the risk of brain disorders, offering new insights for preventive and therapeutic approaches.
P29.10
1 Ruijin Hospital affiliated to Shanghai Jiao Tong University School of Medicine, China
Olfactory dysfunction, a common early symptom in Parkinson's disease (PD), is linked to cognitive decline, but the underlying mechanisms remain unclear. This study aimed to investigate the relationship between olfactory dysfunction and cognitive decline, and the underlying mechanisms from the genetics and imaging prospects. Data from 406 patients with PD in the PPMI cohort and 172 patients in the Ruijin (RJ) cohort were analyzed using the Kaplan-Meier method to assess cognitive decline across different olfactory levels. We applied PD-related SNPs and neuroimaging, including voxel-based morphometry on MRI data and dopamine transporter SPECT imaging, to explore the underlying mechanisms using structural equation modeling. Our findings showed that olfactory dysfunction was associated with an increased risk of cognitive decline in both cohorts, with patients exhibiting olfactory dysfunction demonstrating a significantly higher likelihood of cognitive impairment at follow-up (PPMI: P = 0.00012; RJ: P = 0.017). Genetic analysis identified a significant association between olfactory dysfunction and the rs8005172 of GALC. Neuroimaging showed atrophy in the right superior temporal pole (STP) among GALC variant carriers. Exploratory analysis indicated that the GALC genotype directly influenced olfactory function (path coefficient = -0.2, P < 0.01) and indirectly affected cognitive performance through changes in brain structure. This study offers preliminary insights into the role of the GALC rs8005172 variant and right STP atrophy in the mechanism of cognitive decline associated with olfactory dysfunction in PD. These findings warrant further validation in larger and more diverse cohorts.
P29.11
1 Icahn School of Medicine/Mount Sinai Beth Israel, Department of Neurology, Puerto Rico
2 Albert Einstein College of Medicine, Department of Epidemiology & Population Health (Biostatistics), Department of Neurology, United States
3 University of California, Davis, Department of Pathology and Laboratory Medicine, United States
4 Icahn School of Medicine/Mount Sinai Beth Israel, Department of Neurology, United States
Background: Vitamin B12 (B12) plays a critical role in neurologic function and B12 deficiency has been implicated in cognitive and motor decline in Parkinson’s Disease. An association with LRRK2 has been postulated from pre-clinical studies.
Methods: Retrospective analysis to determine the association between B12 status and cognitive and motor outcomes in in PD as well as in LRRK2 G2019S and GBA1 variant carriers with PD, and to assess levels in gene carriers without motor features (non-manifesting carriers, NMC). B12, methylmalonic acid (MMA), homocysteine (tHcy) levels, and Montreal Cognitive Assessment (MoCA) and MDS-UPDRS III were assessed.
Results: Among 87 PwP (idiopathic PD, IPD), 42 LRRK2-PD, 59 GBA1 variant PD, 25 GBA1 NMC, 20 LRRK2 NMC, and 43 controls, tHcy was elevated in PD vs. controls (mean±SD 11.2±5.0µmol vs. 9.4±3.6µmol, p = 0.009), but B12 and MMA did not differ. Among PD: LRRK2-PD had higher B12 levels (809±475pg/mL) than GBA-PD (667±451pg/mL) and IPD (621±344pg/mL, p = 0.033), but other analytes were not different. In combined models, tHcy was independently associated with cognitive performance, with higher levels predicting lower MoCA scores (β=-0.18, p=0.001), accounting for LRRK2 or GBA1 status, as was GBA1 (β=-1.6, p=0.006). tHcy was associated with worse UPDRS-III total scores (β=0.35, p=0.034), but not with other B12 analytes. Among Genetic Subgroups: Homocysteine was higher in both LRRK2-PD (11.2±5.1µmol vs. NMC 9.1±3.8, p=0.043) and GBA-PD (11.4±6 vs. 8.6±2.5 µmol, p=0.004) compared to their NMCs. B12 levels were also found to be elevated among LRRK2-PD vs. NMCs (809.3±475 vs. 583±325 pg/mL, p=0.034).
Discussion: While the association between elevated tHcy and low cognition seen in LRRK2 and GBA1 was expected based on prior data, the higher level of B12 in LRRK2-PD in the setting of elevated MMA and tHcy raises the question of possible functional B12 impairment in LRRK2-PD. An effect of B12 on LRRK2 penetrance was not observed as might be anticipated from pre-clinical studies. Limitations include underreported and some unknown B12 supplementation status for which it couldn’t be controlled for and small genetic subgroup sizes. Nonetheless, these findings suggest a potential modifiable pathway involving B12 in PD, warranting further study with prospective data collection and better control of supplementation history. Analysis of an expanded cohort is underway and will be presented.
P29.12
1 Cleveland Clinic, United States
2 Hospital Sanatorio de la Trinidad Mitre, Argentina
3 Hospital Interzonal General de Agudos San Martin de La Plata, Argentina
4 Hospital Ramos Mejia, Argentina
5 Hospital Angel C. Padilla, Argentina
6 Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da USP, Brazil
7 Hospital de Clínicas de Porto Alegre da Universidade Federal do Rio Grande do Sul, Brazil
8 Hospital Ophir Loyola, Brazil
9 Universidad Federal de São Paulo - UNIFESP/EPM, Brazil
10 Hospital Universitário Walter Cantídio/Universidade Federal do Ceará, Brazil
11 Hospital e Maternidade Celso Pierro (HMCP) da Sociedade Campineira de Educação e Instrução, Brazil
12 Instituto de Ensino e Pesquisa Hospital Sírio-Libanes, Sao Paulo Clínica Integrada de Nerociencias, Brazil
13 Centro de Transtornos del Movimiento (CETRAM), Chile
14 Universidad de Chile, Chile
15 Universidad de Concepcion, Chile
16 Universidad de Antioquia, Colombia
17 Universidad Nacional de Colombia, Colombia
18 Fundacion Valle del Lili, Colombia
19 University of Costa Rica, Costa Rica
20 Universidad Andres Bello, El Salvador
21 Hospital San Felipe, Honduras
22 TECNOLOGICO DE MONTERREY TecSalud, Mexico
23 Instituto Nacional de Neurología y Neurocirugía, Mexico
24 Universidad Nacional Autonoma de Mexico, Mexico
25 Instituto Nacional de Ciencias Neurológicas, Peru
26 University of Puerto Rico, United States
27 University of Miami, United States
Introduction Studies show that males have ∼50% higher odds of developing Parkinson's Disease (PD) than females. Some studies suggest the magnitude of this discrepancy may vary by population. Despite this difference, sex chromosomes are typically excluded from genome-wide association studies. This exclusion is due to several factors, including biological, methodological, and statistical complexities analyzing these chromosomes.
In this work we conducted an X-chromosome-wide association study (XWAS) on the Latin American Research Consortium on the Genetics of Parkinson’s Disease (LARGE-PD) Phase 2 to investigate potential risk loci for PD in the X-chromosome (X-chr), both sex-dependent and independent.
Methods The LARGE-PD Phase 2 dataset comprises individuals (n=5315) from 11 countries across the Americas, genotyped using the NeuroBooster array and imputed with TOPMed. After quality control, the dataset contains 2219 males and 2419 females.
We performed an XWAS using methods from Leal et al., 2023, modifying the outlier removal step to rely on projected principal component analysis, avoiding removing outlier samples for non-ancestry-related reasons. Associations were run with PLINK2.0 for females only, males only, and jointly. Variants were considered statistically significant if p-values were lower than those described in Leal et al., 2023 (female: 1.33E-04, male: 6.65E-05, joint: 8.43E-05). Post-XWAS analyses were performed with FUMA.
Results We identified variants passing significance in or near the ASS1P4, WWC3, PTCHD1-AS, PCYT1B, and RBMX genes for the joint association; IL1RAPL1, DMD, UBA1, BCORL1, and IGSF1 in male only; and CLCN4, EGFL6, and RTL4 in female only. We also replicated a variant near the RPL10 gene associated with PD from previous XWAS (rs28602900) with the same effect direction in both the joint and the female only analyses. Gene-set analysis identified membrane trafficking and vesicle mediated transport gene sets, which both include the PD-associated gene RAB32, as significant for the male only analysis.
Conclusions We identified potential X-chr risk loci, emphasizing the need for its inclusion in genetic studies, especially in relation to phenotypes with sex biases, like PD. We further highlight the importance of including underrepresented ancestries in PD studies. The next steps for this study are performing replication in the LARGE-PD Phase 1 dataset and further investigating implications of the identified genes in PD-related pathways.
P29.13
1 Clínica de Parkinson y Trastornos del Movimiento, Hospital Universitario “Dr. José E. González”, Mexico
2 Laboratorio y Unidad de Monitoreo de Epilepsia y Sueño, Hospital Universitario “Dr. José E. González”, Mexico
Introduction: Environmental exposure to pyrethroids and organophosphates has been a topic of study for over a decade due to its association with the incidence of Parkinson’s, as well as its potential to worsen both motor and non-motor symptoms [1].
Objective: To describe the clinical profile of a population with Parkinson’s from Northeastern Mexico according to their history of environmental exposure to pyrethroids and organophosphates.
Methods: A cross-sectional study was conducted from June 2022 to September 2025. Participants underwent a neurological and environmental exposure interview, the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), and the Montreal Cognitive Assessment (MoCA).
Patients were categorized into four groups based on occupational exposure type to pyrethroids and organophosphates: no exposure, home exposure, occupational exposure, and combined exposure. Descriptive statistics were applied to analyze clinical and sociodemographic variables across groups.
Results: A total of 174 patients were evaluated, of whom 109 (62.6%) reported no exposure, 44 (25.3%) home exposure, 14 (8.0%) occupational exposure, and 7 (4.0%) combined exposure.
Patients with occupational exposure exhibited the most unfavorable clinical profile compared to other groups, showing the highest mean MDS-UPDRS score 72.93 (38.35) and the lowest MoCA mean score 19.50 (5.21). Detailed clinical and sociodemographic characteristics for each group are presented in Table 1 and Table 2.
Conclusion: The findings of this study support previous evidence linking exposure to pyrethroids and organophosphates with increased severity of motor and cognitive symptoms in Parkinson’s, particularly in the context of occupational exposure [2]. These results highlight the need to implement neuroprotective strategies for exposed workers and screening programs for populations at environmental risk due to proximity. Future research should focus on identifying specific agents and critical exposure thresholds to improve risk characterization in the Mexican population.
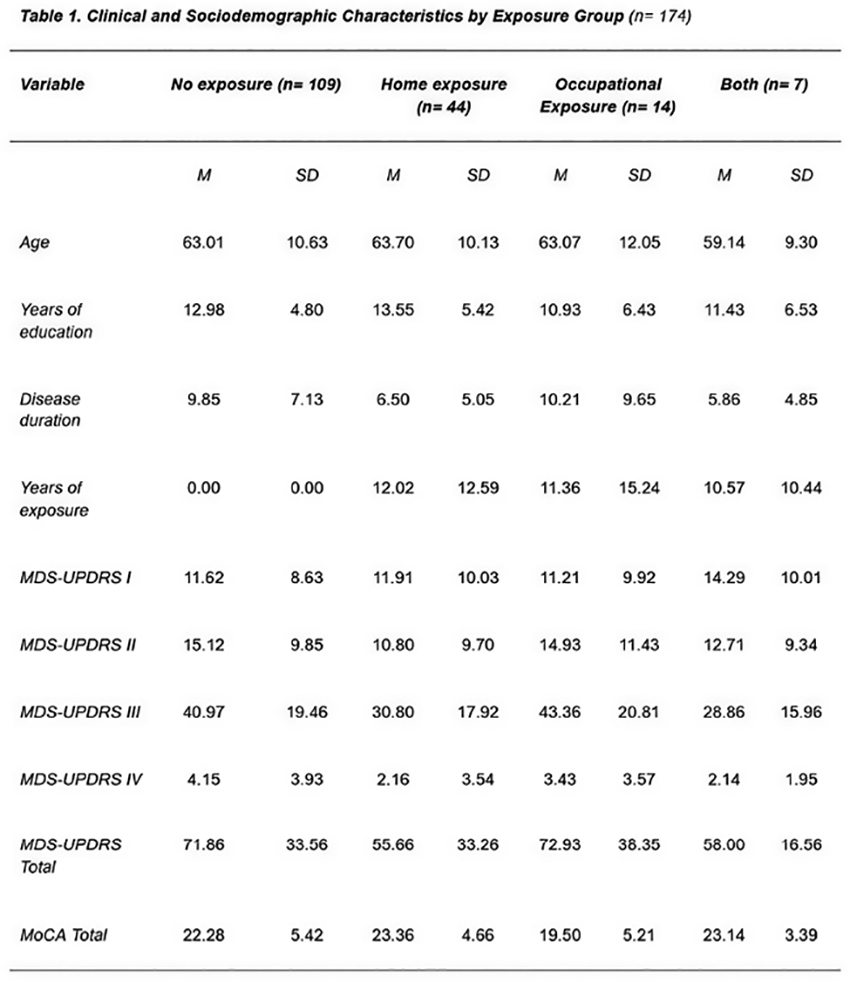
P29.14
1 Cleveland Clinic, United States
Background: The Latin American Research consortium on the GEnetics of Parkinson’s Disease (LARGE-PD) was established in 2006 to address the underrepresentation of Latin American populations in Parkinson’s disease (PD) research. At the time, most genetic studies focused on individuals of European ancestry, leaving these populations largely unstudied.
Objectives: This work aims to describe the achievements of LARGE-PD over the past 19 years, highlighting its contributions to PD research, regional capacity building, and integration into global genomics efforts.
Methods: LARGE-PD was implemented in two phases. In the first phase (2006–2018), participants were enrolled from six Latin American countries (Argentina, Colombia, Chile, Ecuador, Peru, and Uruguay), collecting DNA and clinical/environmental data initially in paper and Excel/Access formats. A harmonized clinical database and centralized biobank were developed with standardized protocols for phenotyping, DNA collection, and data management. In the second phase (2018–present), recruitment expanded to over 60 sites across 15 countries in Latin America and the Caribbean, including a regional biobank in Peru (2019), and REDCap was implemented for data management.
Results: LARGE-PD has enrolled over 13K participants (cases and controls), enabling comprehensive analyses of genetic risk and disease presentation across diverse Latino populations. The consortium has strengthened research infrastructure, trained clinicians and investigators, and produced over 20 scientific publications. In 2019, LARGE-PD joined the Global Parkinson’s Genetics Program (GP2), contributing Latino representation to international PD genomics efforts and being an example of a successful consortium in an underrepresented region. More recently, the PDGENEration initiative within LARGE-PD began returning CLIA-certified genetic results to participants with a clinical PD diagnosis.
Conclusion: LARGE-PD addresses the knowledge gap in Parkinson’s disease among Latin American populations by generating critical data, building regional capacity, and fostering international collaborations. Through PDGENEration, it translates genetic discoveries into clinical care with CLIA-certified results. Future efforts aim to expand ancestral diversity, integrate genomic and biomarker data, and ensure equitable application of findings, illustrating how sustained regional collaboration can advance global science and reduce health disparities.
CLINICAL SCIENCES: Cognition/ Mood/ Behavioral Disorders
P30.01
1 Université Laval, Canada
2 University of Toronto, Canada
Parkinson's disease (PD) is a neurodegenerative disease characterized by dopaminergic degeneration in the substantia nigra. Men have a higher risk of developing PD, while women show greater depression comorbidity, yet the mechanisms driving these psychiatric symptoms remain understood. The blood-brain barrier (BBB), comprising endothelial cells, astrocytes, and pericytes, maintains brain homeostasis and regulates α-synuclein (αSyn) processing, yet its involvement in PD pathology is unclear. We used a mouse model of PD in which αSyn preformed fibrils (PFF) were stereotaxically injected into the dorsal striatum. Behavioral analyses revealed sex-specific depressive-like behaviors, aligning with clinical observations. Transcriptomic profiling focused on the prefrontal cortex (PFC), a brain region implicated in mood regulation, uncovering region- and sex-specific neurovascular alterations: females exhibited BBB disruption, with reduced expression of endothelial markers, whereas males showed pronounced astrocyte reactivity. To model environmental risk factors for depression, mice were exposed to chronic social stress, the main environmental contributor to depressive symptoms. The chronic social defeat stress (CSDS) paradigm is well established to induce depressive-like behaviors in mice and, in our study, worsened both BBB alterations in mood-related brain areas and behavioral deficits. Interestingly, only stress-susceptible mice injected with PFF showed BBB leakage, as measured by mIgG extravasation (∼25 kDa), suggesting a combined effect of αSyn pathology and stress on BBB integrity. Future studies will evaluate the therapeutic potential of systemic and intracerebral anti-αSyn antibody administration to reduce αSyn aggregation, restore BBB integrity, and ameliorate depressive-like behaviors in a sex-dependent manner. Complementary in vivo magnetic resonance imaging (MRI) and functional MRI are ongoing to map how BBB hyperpermeability and cell-type-specific vascular responses modulate functional activity in mood-related circuits. Our findings indicate that sex-specific neurovascular dysfunction contributes to vulnerability to psychiatric manifestations in PD, and we hypothesize that targeted αSyn antibody therapies may protect BBB function and mitigate mood-related symptoms. This work provides a mechanistic neurovascular-targeted interventions, highlighting the interplay between αSyn pathology, stress, and neurovascular integrity.
P30.02
1 University of California, San Francisco, United States
2 University of California, San Diego, United States
INTRODUCTION Deep brain stimulation (DBS) is an FDA-approved therapy for people with Parkinson's disease (pwP). Approximately 40% of pwP develop psychosis, especially in later stages of disease. PwP who experience psychosis are typically not considered good DBS candidates. Thus, data are lacking regarding their postoperative course. This study examined the 1-year postoperative course of psychosis in pwP treated with DBS.
METHODS IRB approval was obtained. A retrospective chart review of 120 pwP treated with DBS and seen by the Psychiatry team at an academic center was conducted. Preoperative psychosis (i.e., auditory or visual hallucinations or delusions) was classified as: current (noted at most recent visit before surgery) and past (any time in the past). Postoperative (within 1 year of surgery) psychosis was noted. Other variables included age, sex, disease length, preop MoCA score, medications (dopamine agonists), substance use, mild/major neurocognitive disorder, timing of psychosis, and surgical target (STN, GPi). We examined the association between the patients’ preoperative (current, past) and postoperative psychosis using unadjusted logistic regression models. Each predictor was analyzed separately, with postoperative psychosis (yes/no) as the binary outcome. Given sparse cell counts, Firth’s penalized likelihood was used to reduce small-sample bias and to obtain stable estimates. Odds ratios (ORs) and 95% confidence intervals (CIs) were derived from the penalized likelihood estimates.
RESULTS Of the 120 pwP included, 27 (22.5%) had preoperative psychosis: 7 (5.8%) current, 26 (21.7%) past. 21 (17.5%) experienced continued psychosis, while 2 (1.7%) developed new-onset psychosis after DBS surgery. Unadjusted logistic regression using Firth’s penalized likelihood indicated a strong positive association between pre- and postoperative psychosis. Patients with past preoperative psychosis had markedly higher odds of postoperative psychosis than those without (OR = 30.3, 95% CI [8.1, 113.7], p < 0.001). The association was even stronger for current preoperative psychosis (OR = 38.6, 95% CI [5.3, 283.8], p < 0.001). Analysis regarding other variables is in progress.
CONCLUSION Preoperative psychosis, especially closer to surgery time, may increase risk for postoperative psychosis. This finding has important implications for clinicians and should be considered when educating pwP and families prior to DBS surgery. Further research in larger samples is necessary.
P30.03
1 SPAR Physical Therapy, PLLC, United States
2 Gateway Community College, United States
3 Tufts University, United States
4 Banner University Medical Center, United States
5 Sante of North Scottsdale, United States
6 Banner Physical Therapy, United States
7 Banner University Sleep Center, United States
Background: More than 50% of individuals with Parkinson’s disease (PD) conceal their diagnosis, mask symptoms, or avoid social situations due to stigma. Stigma—negative attitudes and misconceptions surrounding PD—can lead to isolation, depression, and anxiety. These psychosocial effects are often compounded by physical challenges such as impaired mobility, disrupted sleep, and cognitive decline, all of which reduce overall quality of life. Addressing these multidimensional factors is essential for comprehensive PD management. Supportive social environments and public education have been shown to reduce stigma, while emerging evidence suggests that vagus nerve stimulation (VNS) may further enhance well-being by improving parasympathetic regulation, reducing stress, and supporting neural connectivity linked to cognition, sleep, and mood. Methods: Five adults with PD (aged 64–77 years; mean disease duration 66 months) received auricular branch VNS twice weekly for eight weeks (16 sessions, 20 minutes each). Participants were in a relaxed, reclined position during stimulation. Assessments were administered at baseline, 10 weeks, post-intervention, and three weeks post-intervention, including the Parkinson’s Disease Sleep Scale (PDSS), Epworth Sleepiness Scale (ESS), Hamilton Depression Scale, and Parkinson’s Disease Questionnaire-39 (PDQ-39). Results: All participants reported reduced stigma during the intervention, with 4 maintaining improvement three weeks after treatment ended. Cognitive scores improved in 4 participants during treatment and in all 5 from baseline to post-intervention. Sleep quality improved across all participants, and 4 demonstrated enhanced mobility during treatment, though this effect decreased once treatment ceased. Three participants showed reduced depression scores from baseline to study completion. Conclusion: Vagus nerve stimulation was associated with improvements in stigma, cognition, sleep, and mobility among individuals with PD, with continued gains in cognition and reduced stigma following treatment. These findings support prior evidence linking VNS to improved neural connectivity and stress regulation. Additionally, group sessions may have fostered social interaction, further reducing stigma. VNS may represent a promising adjunct approach to enhance quality of life and psychosocial well-being in individuals with Parkinson’s disease.

P30.04
1 Univ. Lille, CNRS, UMR 9193—SCALab—Sciences Cognitives et Sciences Affectives, Lille, France
2 Univ. Tours, CNRS, UMR 7270 – LLL –Laboratoire Ligérien de Linguistique, F-37000 Tours, France
3 Univ. Lille, Inserm, CHU Lille, U1172 TREAT Team—LilNCog—Lille Neuroscience & Cognition, Lille, France
Background: Parkinson’s disease (PD) impacts speech production, with prosody among the most frequently reported altered dimensions. For instance, people with PD (PwPD) tend to produce monotonous speech and show rhythmic disruptions, even when overt speech impairment is mild. Although rhythm-based interventions are effective for gait and other motor behaviors, the link between rhythm perception and speech production remains underexplored in PD. Interestingly, an increasing body of work suggests that prior exposure to auditory rhythmic stimuli, known as rhythmic priming, can influence subsequent speech processing. In the current study, we aimed to determine whether rhythmic priming can improve speech production in PwPD.
Methods: Twenty-four PwPD and 20 age-matched controls read 12-syllable sentences after a Regular (R), Irregular (IR), or Silence (S) prime. R and IR each comprised 12 beats; only R formed regular three-beat groups with the final beat accented, mirroring the sentence prosodic structure.
Results: Speech initiation time was significantly shorter after R than S in both PwPD and controls. Participant-level contrasts showed that most individuals benefited from R compared to IR and S. Accuracy (proportion of sentences read correctly) and speech rate showed no significant condition effects. Relative to S, R did not measurably alter timing stability of vowels and consonant intervals, whereas IR increased consonant-timing variability in PwPD.
Conclusion: A brief regular auditory stimulus reflecting sentence rhythm before speaking facilitates speech initiation in PwPD while maintaining baseline-level rate and timing stability. Regular rhythmic priming could be a promising tool to support speech production in clinical settings and everyday life. To better understand the impact of rhythmic primes on speech production, further analyses are needed to investigate prosodic prominence and determine which type of rhythmic prime (e.g., long versus short or musical versus linguistic) provides the greatest benefit for PwPD.
P30.05
1 Universidad de Valparaíso, Chile
2 Institut de Recerca, Hospital Sant Joan de Déu, Spain
3 Faculty of Psychology and Neuroscience, Department of Neuropsychology & Psychopharmacology, Maastricht University, Netherlands
4 Faculty of Health, University of Santo Tomás and speech therapist at Clínica Dávila, kinesiotherapy department, Chile
5 Department of Otolaryngology, Faculty of Medicine, Pontificia Universidad Católica de Chile, Chile
6 Escuela de Fonoaudiologia, Facultad de Odontologia y Ciencis de la Rehabilitacion, Universidad San Sebastian, Chile
7 Department of Cognition, Development and Educational Psychology, University of Barcelona, Spain
8 Faculty of Psychology and Neuroscience, Department of Neuropsychology & Psychopharmacology, Netherlands
Introduction: Parkinson’s disease (PD) is frequently associated with reduced vocal loudness. This impairment in individuals with PD (IwPD) has been linked to abnormal processing of sensory feedback and potential dysfunction of feedforward control mechanisms. Furthermore, IwPD often underrecognize their vocal difficulties, limiting the clinical value of self-assessment tools. Electrophysiological research using Motor-Induced Suppression (MIS) and event-related potentials (ERPs; N1 and P2) has reported alterations associated with impaired mechanisms for voice loudness regulation in IwPD (Emmendorfer et al., 2021; Abur et al., 2018; Li et al., 2021).
Two Methods: Study 1: Self-perception of voice function were assessed using PROMs in 27 IwPD (61–79 years), 25 individuals with general voice disorders (GVD, 57–83 years), and 28 healthy controls (HC, 60–80 years). Group differences were examined using univariate and multivariate analyses.
Study 2: Sensory feedback mechanisms were assessed using ERPs (N1 and P2) during a Button Press Paradigm with three conditions: (a) Auditory-Motor Condition (AMC) with vocalizations at +15 dB while tapping, (b) Auditory-Only Condition (AOC) with passive listening to +15 dB voice playback, and (c) Motor-Only Condition (MOC) with tapping only. Each condition included 100 trials.
Results: Study 1: IwPD showed significantly reduced self-perception and awareness of vocal problems compared to GVD and HC groups, despite slightly higher PROM scores than HCs. Principal Component Analysis further confirmed distinct group differences in perceived vocal loudness and total scores.
Study 2: IwPD demonstrated altered auditory processing of their own voice, evidenced by differences in the N1 response to unexpected loudness increases, especially in the AOC condition, suggesting impaired efference copy and compromised suppression mechanisms.
Conclusions: IwPD underreport their vocal symptoms and exhibit altered auditory-sensory feedback processing for vocal loudness control. These findings highlight the need for targeted clinical assessment and therapeutic strategies that account for both reduced self-awareness and impaired neurophysiological mechanisms in PD.
P30.06
Abigail Baird1, Hannah Combs2, Celeste Harris3, Kathleen Crist3, Michele York2
1 Johnson Neuropsychology, United States
2 Baylor College of Medicine, United States
3 Houston Area Parkinson's Society, United States
Background: Cognitive rehabilitation has shown promise for individuals with Parkinson’s disease (PD). PD-CoRE is a structured seven-session cognitive rehabilitation intervention that teaches personalized compensatory strategies to improve executive functioning in individuals with PD. The present study evaluated the utility of PD-CoRE and examined the equivalence of a modified alternate form of the Test of Practical Judgment (TOP-J) for repeated program assessments.
Methods: 37 participants with PD were administered the Montreal Cognitive Assessment (MoCA) along with measures of practical judgment (TOP-J), life satisfaction, depressive symptoms, and self-efficacy before and after the PD-CoRE intervention. Paired-samples t-tests assessed pre–post change on outcome measures, and repeated measures ANOVAs tested moderating effects of age, education, years since diagnosis, and intervention round. Alternate form equivalence of the TOP-J was evaluated using independent samples t-tests and repeated measures ANOVA.
Results: Results indicated significant improvements on MoCA score (p = .001, d = 806), practical judgment (p = .001, d = 596), self-efficacy (p = .019, d = 365), and depressive symptoms (p = .019, d = .417) after PD-CoRE. Improvements on MoCA were moderated by age, with younger participants showing greater improvement. Education predicted changes in both judgment and self-efficacy. Analyses indicated equivalence between TOP-J forms, supporting its use for repeated assessments.
Conclusions: Findings support the utility of PD-CoRE in enhancing aspects of cognition and well-being in PD and highlight the importance of individual characteristics in treatment response. The validated alternate TOP-J form offers a reliable tool for longitudinal evaluation in clinical and research settings.
P30.15
1 Queen Mary University of London, United Kingdom
Introduction Motor fluctuations and dyskinesia affect about half of people with Parkinson’s disease (PD), with major impact on quality of life (QoL). These complications are not fully explained by disease severity or treatment, suggesting psychosocial factors may contribute. Negative illness perceptions and maladaptive beliefs are important in other chronic conditions but underexplored in PD.
Objectives To examine associations between illness perceptions, cognitive beliefs, and motor complications in PD, and their links with QoL, mood, sleep, fatigue, and balance confidence.
Methods Fifty-eight people with idiopathic PD (mean age 67, 55% male, mean disease duration 5.7 years) on stable dopaminergic therapy (>3 months) completed the Illness Perception Questionnaire-Revised and Cognitive Behavioral Symptom Questionnaire. Motor complications were assessed with the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) Part IV. A subgroup (n=47) wore the Parkinson’s KinetiGraph wearable (watch) for 7 days to capture dyskinesia, immobility, and step count. Additional measures included the Parkinson’s Disease Questionnaire-39 (PDQ-39), Hospital Anxiety and Depression Scale, Pittsburgh Sleep Quality Index, Fatigue Severity Scale, and Activities-specific Balance Confidence scale.
Results Greater motor complications were linked with more negative beliefs: symptom focusing (ρ=0.57, p<0.001) and catastrophizing (ρ=0.47, p<0.001) correlated with MDS-UPDRS IV. Embarrassment avoidance correlated with dyskinesia (ρ=0.38, p=0.016). All-or-nothing behavior predicted fewer daily steps (ρ=-0.42, p=0.005). QoL correlated strongly with maladaptive beliefs: PDQ-39 Summary Index with catastrophizing (ρ=0.62, p<0.001) and embarrassment avoidance (ρ=0.68, p<0.001). Regression confirmed QoL, anxiety, fatigue, and motor complications independently predicted illness perceptions and negative beliefs, explaining up to 53% of variance (adjusted R2=0.53).
Conclusions In PD, maladaptive beliefs and negative perceptions are strongly linked to motor complications, reduced activity, and poorer QoL, suggesting a self-reinforcing cycle between motor and psychological burden. Interventions targeting these beliefs may reduce dyskinesia, enhance coping, and improve mood, sleep, and fatigue. Despite small sample and cross-sectional design, these findings highlight the potential for cognitive interventions alongside wearable-derived metrics to advance holistic care in PD.
CLINICAL SCIENCES: Sleep Disorders
P31.01
1 Tianjin Huanhu Hospital, China
2 Tianjin medical university, China
Background: Sleep disturbances are among the most common non-motor symptoms of Parkinson’s disease (PD), but the role of sleep duration and quality in PD risk remains unclear, especially in large community-based populations.
Methods We analyzed data from 8,650 participants in the 2018 wave of the China Health and Retirement Longitudinal Study (CHARLS). Logistic regression models were used to evaluate the associations between nighttime sleep duration, daytime napping, sleep quality, and physical activity (PA) with the risk of PD.,Models were adjusted for demographic, lifestyle, and socioeconomic factors.
Results: Sleeping 6–8 hours per night was significantly associated with a lower risk of PD (adjusted OR = 0.621, 95% CI: 0.411–0.940, P = 0.024), whereas sleeping ≥8 hours showed no significant association. Poor sleep quality increased PD risk (adjusted OR = 1.772, 95% CI: 1.271–2.471, P < 0.001). Vigorous PA, but not moderate PA, was protective against PD (adjusted OR = 0.603, 95% CI: 0.426–0.852, P = 0.004). Daytime napping showed no significant associations with PD risk.
Conclusion Using data from the CHARLS, our analysis revealed that optimal nighttime sleep duration (6–8 hours), good sleep quality, and vigorous physical activity are protective factors against PD in older Chinese adults. .These findings highlight the importance of lifestyle interventions targeting sleep and exercise in PD prevention.

P31.02
1 CND Life Sciences, United States
2 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
Introduction: iRBD is a prodromal neurodegenerative disease characterized by dream reenactment and REM sleep atonia. IRBD is characterized pathologically by the deposition of P-SYN within the central and peripheral nervous systems. iRBD has a high risk of phenoconversion to a clinically apparent synucleinopathy (Parkinson’s disease (PD), multiple system atrophy (MSA), or dementia with Lewy bodies (DLB)), with >73% of patients converting over 12 years. The goals of this study are to 1) Determine rates of phosphorylated alpha-synuclein (P-SYN) deposition in idiopathic REM sleep behavior disorder (iRBD) and quantify changes in P-SYN deposition over time. 2) Determine if patterns of P-SYN deposition predict phenoconversion.
Methods: Patients with a confirmed diagnosis of iRBD (by polysomnography or validated questionnaire and history) were included in this multicenter study. Detailed examinations, orthostatic vital signs, and questionnaires were completed. Medical history, ancillary testing, and polysomnograms (PSG) were reviewed, if applicable. Skin biopsies at the distal leg, distal thigh, and posterior cervical sites were collected. Dual immunohistochemical immunostaining for nerve fibers (protein gene product 9.5) and P-SYN were completed.
Results: 80 subjects (31% female) were enrolled. The mean age of the subjects was 67.8±8.7 years. P-SYN was detected in 75% (60/80) of subjects. In a preliminary analysis of the first 33 patients to complete follow-up, there was a significant increase in P-SYN between baseline and 12 months (p=0.04). The average P-SYN composite score at baseline was 4.09±4.99, and at the 12-month follow-up was 5.63±5.87. No complications were noted in the biopsy procedure.
Conclusion: Final longitudinal reassessment of these subjects is in progress to determine if P-SYN can serve as a biomarker of disease progression and predict phenoconversion in iRBD patients. Preliminary analysis shows a significant increase in measured cutaneous P-SYN levels between baseline and 12 months.
P31.03
1 Acadia Pharmaceuticals, Inc, United States
2 University of California - San Francisco, Departments of Psychiatry and Neurology, United States
Objective: To evaluate the impact of baseline sleep disturbances on antipsychotic response to pimavanserin vs placebo in patients with Parkinson’s disease psychosis (PDP).
Background: Sleep-related disturbances are commonly associated with PDP. Pimavanserin is approved in the US for hallucinations and delusions associated with PDP, but the impact of sleep disturbances on pimavanserin response is unclear.
Methods: To identify patients with sleep-related disturbances, data from the pivotal phase 3 trial (NCT01174004) were stratified by baseline Scales for Outcomes in Parkinson’s Disease-nighttime sleep (SCOPA-NS) scores (≥7 or <7) and SCOPA-daytime sleepiness (SCOPA-DS) scores (≥5 or <5). The impact of baseline sleep disturbances was assessed using a mixed model for repeated measures including treatment, visit, SCOPA subgroup, and their interactions. The primary endpoint was the least squares mean (LSM) change from baseline in Scale for the Assessment of Positive Symptoms-Parkinson's Disease (SAPS-PD) score at week 6. Treatment differences (LSMD) vs placebo were estimated within each SCOPA subgroup, and an interaction test was conducted (not powered to detect differences; all nominal P values).
Results: Overall, pimavanserin improved psychosis symptoms vs placebo at week 6: SAPS-PD LSMD (95% CI), −3.02 (−4.89, −1.14); P=0.0018. For baseline SCOPA-DS<5, SAPS-PD LSMD (95% CI) was −5.27 (−8.41, −2.12); P=0.0015; for SCOPA-DS≥5, −1.97 (−4.24, 0.29); P=0.0872 (interaction test P=0.1429). For baseline SCOPA-NS<7, SAPS-PD LSMD (95% CI) was −3.35 (−5.79, −0.92); P=0.0074; for baseline SCOPA-NS≥7, −2.56 (−5.53, 0.40); P=0.0893 (interaction test P=0.6716). Notably, patients with nighttime sleep disturbances (baseline SCOPA-NS≥7) experienced sleep improvement with pimavanserin vs placebo: SCOPA-NS LSMD (95% CI), −2.54 (−4.14, −0.93); P=0.0025.
Conclusions: Pimavanserin demonstrated consistent antipsychotic efficacy vs placebo in patients with PDP regardless of baseline sleep-disturbance status. Additionally, patients with baseline impairment in nighttime sleep experienced improved nighttime sleep with pimavanserin. These findings support the consistent efficacy of pimavanserin in the presence or absence of daytime or nighttime sleep disturbance.
This abstract will have been previously presented at the American Academy of Neurology (AAN) 2026 Annual Meeting, April 18-22, 2026; Chicago, Illinois.
P31.04
1 Department of Neurology, Icahn School of Medicine at Mount Sinai and Mount Sinai Beth Israel New York, NY, United States
2 Light and Health Research Center, Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai New York, NY, United States
3 Department of Neurology, Icahn School of Medicine at Mount Sinai and Mount Sinai Beth Israel New York, NY,, United States
Objective: To determine whether a tailored lighting intervention (TLI) improves subjective measures of sleep and fatigue as well as objective sleep measures. Introduction: Sleep dysfunction is one of the most prevalent non-motor challenges in PD with significant negative impact on quality of life and motor and non-motor domains. Medications to address sleep disturbance in PD can have adverse side effects. Fatigue is especially complex to manage with limited evidence-based recommendations. We previously reported a pilot study on objective and subjective measures of sleep quality and fatigue before and after a passive TLI in a pilot cohort, which we now expand from 20 to 45 participants. Methods: In our single-arm within-subjects intervention study, light was delivered to participants at eye-level using table/floor lamps and glasses designed to maximally engage the circadian system for two hours every morning for four weeks. Light exposure data were collected with a daysimeter pendant (calibrated personal light measuring device). Sleep measures were recorded with wrist-worn actigraphy and pre-and post-intervention outcomes were evaluated using questionnaires. Results: Forty-five individuals (22 [49%] women) with PD completed the lighting intervention. Participants had a mean age of 71.2 (SD 9.2) years and mean PD duration of 10.1 (SD 5.6) years. Pre-to-post-intervention, mean sleep duration measured by actigraphy increased by 20.3 minutes (p=0.029). Fatigue as assessed by the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale improved by 3.4 points (mean baseline score 31.7±12.5 to post-TLI 34.2±10.9, p<0.001). Results showing the additional 25 participants, separate from the combined cohort, will also be presented. Conclusions: TLI demonstrated promising, albeit small, improvements in both subjective measure of fatigue and in sleep duration. While we had previously seen benefit in sleep duration in the smaller cohort, the new finding with an effect on fatigue in a larger cohort bolsters the support for light to improve this symptom that is difficult to treat in PD. Strengths of our study include the ability of participants to receive light without the need for strict positioning of a light box, production of less glare from our TLI compared to a traditional light box, and assessment of compliance with the daysimeter pendant.
CLINICAL SCIENCES: Diagnosis (differential, accuracy)
P32.01
1 University of Tasmania, Australia
2 Wicking Dementia Research and Education Centre, University of Tasmania, Australia, Australia
3 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, United Kingdom, United Kingdom
4 Sleep Disorders Centre, Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom, United Kingdom
5 School of Psychology, Brain and Mind Centre, University of Sydney, Australia, Australia
Introduction: Isolated rapid eye movement (REM) sleep behaviour disorder (iRBD) is a sleep disorder characterised by dream enactment behaviours during REM sleep - typically involving limb movements and vocalisations related to vivid dreams. It is often an early symptom of Parkinson’s and other related neurodegenerative diseases (NDDs), with over 80% of people developing an NDD within 14 years. However, there is an average delay in iRBD diagnosis of 9 years from the onset of symptoms, showing that we need easier methods of detection to improve access to specialist care and potential disease modifying clinical trials. We designed a multi-step approach to detect iRBD in a community of older adults (≥50 years) in Tasmania, Australia using home-based video-polysomnography (vPSG; sleep study).
Methods: The Tasmania-London (TASLON) protocol for iRBD detection comprised 3 key steps: participants completed an online iRBD screening question; those who screened positive were invited to undertake the TASLON iRBD Screening Interview by telephone; a sample then completed a home-based vPSG based on iRBD screening risk level. A sample of participants also completed a usability questionnaire and provided qualitative feedback regarding their home-based vPSG experience
Results: A total of 2891 participants (mean [SD] age 64 [7.7] years; 74% female) without any known NDD were recruited from throughout Tasmania. 267 (9%; age 63[7.7] years; 55% female) were identified as having ‘probable’ RBD through positive online screening; 87 (33%) agreed to complete the clinical screening interview; 47 (55%) underwent home-based vPSG; and 21 (45%; age 68[7] years; 52% female) were found to have iRBD. 24 participants completed the usability questionnaire, which showed that 100% of participants felt comfortable explaining their sleep symptoms to the researcher; 91% agreed they would prefer to have a home-based sleep study rather than a hospital-based sleep study; and 77% agreed that they gained insights about their sleep by participating in this research project.
Conclusion: The TASLON protocol is a feasible and acceptable method of improving timely access to iRBD diagnoses and early Parkinson’s detection in the community. It streamlines the path to vPSG by identifying those at highest risk of iRBD, thus improving access to diagnostic testing and clinical trial opportunities for people who otherwise may not have been identified.
P32.02
1 Grenoble Institut Neurosciences, France
2 CHU Grenoble Alpes, France
3 TIMC, France
4 Bruker BioSpin GmbH & Co. KG, Germany
Currently, the diagnosis of Parkinson’s disease (PD) remains delayed and insufficiently accurate, mainly due to the overlap of its clinical features with atypical parkinsonian syndromes—such as the multiple system atrophy (MSA) and the progressive supranuclear palsy (PSP) —, and the absence of reliable, validated biomarkers. To meet the urgent need for specific, cost-effective, and non-invasive diagnostic tools, molecular biofluid biomarkers are being increasingly investigated. In this context, we conducted a large translational metabolomics study both on serum and brain samples from three PD animal models, as well as on serum from de novo PD patients, i.e. newly diagnosed individuals not yet exposed to dopaminergic treatments. This study led to the identification of a novel serum-based metabolic biomarker (6M-BB, patent FR2011817), composed of a specific combination of six metabolites—acetoacetate, betaine, β-hydroxybutyrate (BHB), creatine, pyruvate, and valine—which demonstrated a robust ability to discriminate de novo PD patients from healthy controls with 83% accuracy. In this regard, the objective of this work was to evaluate the performances of this biomarker for the differential diagnosis of PD. To this end, serum samples from de novo PD (n=30), MSA (n=30), PSP, (n=30) and Alzheimer’s disease patients (AD, n=33), as well as healthy individuals (n=29), were analyzed by nuclear magnetic resonance (NMR) spectroscopy and classified using the 6M-BB. The resulting accuracy exceeded 87% for distinguishing PD patients from healthy individuals, and almost 83%, including all cases. We also successfully transferred it to the fully automated and standardized Bruker Avance IVDr NMR platform, designed for routine clinical metabolomics, and enhanced its performance by the addition of one lipoprotein and one other metabolite, reaching nearly 95% accuracy for PD identification against healthy individuals and 85% when including PSP and MSA. In conclusion, we confirmed the robustness and performances of our original 6M-BB for detecting PD at the de novo stage, as well as its relevance for differential diagnosis against atypical parkinsonian syndromes, namely PSP and MSA, which could help to bridge the gap between research and clinics through its implementation on an NMR system specifically designed for clinical application.
P32.03
1 Ottawa Hospital Research Institute, Canada
2 Élisabeth Bruyère Hospital, Canada
Background: Timely access to diagnosis, specialists and treatment is a major challenge in many healthcare systems, thereby negatively impacting adults with Parkinson disease (PD). We recently developed a simple-to-use prediction toolkit to calculate PD risk. Our goal is to empower family doctors to confidently establish a working diagnosis of PD and to initiate treatment ahead of a neurologist’s assessment. The PREDIGT-PD toolkit includes three components and is self-administered at home without the supervisory need of a medical professional: a short questionnaire, a simplified smell test, and a web-based app. Using the app, test-takers enter their responses to the questionnaire and the smell test on their own. The app then automatically calculates scores to generate a report of ‘high/intermediate/low risk for PD’ with recommended next steps. This toolkit has been developed and optimized using several case-control cohorts including a pilot study in Ottawa (‘The Ottawa Trial’).
Methods: The Ottawa Trial cohort represents a cross-sectional, observational study to pilot the PREDIGT-PD toolkit. Between 2023 and 2024, study participants were recruited at two outpatient neurology clinics, and all study assessments were completed by probands at-home.
Results: In the Ottawa Trial cohort with 49 participants diagnosed with PD [or dementia with Lewy bodies (DLB)], 21 subjects with other neurological diseases (OND), and 93 age-matched, neurologically healthy controls (HC), each component of the PREDIGT-PD toolkit showed high discriminative performance (Figure 1). AUC values of the 12-item questionnaire for PD/DLB vs. HC and PD/DLB vs. OND were 0.96 (95% CI 0.93-0.98) and 0.8 (0.67-0.92), respectively. The 8-scent simplified smell test showed similar discriminative performance of PD/DLB vs. HC [0.94 (0.9-0.98)] and PD/DLB vs. OND [0.74 (0.59-0.89)], as the 40-scent UPSIT test; and the diagnostic performance of the model was further improved by combining the questionnaire and the smell test, with AUC values for PD/DLB vs. HC and PD/DLB vs. OND at 0.97 (0.95-0.99) and 0.81 (0.68-0.94), respectively.
Conclusions: The results of our pilot study reveal robust performances by PREDIGT-PD in separating individuals with typical PD from those with other neurological conditions and healthy controls. We posit that the home-based, simple-to-complete toolkit could evolve into an effective screening tool to identify subjects with PD before their first assessment by a neurologist.

P32.04
1 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
2 CND Life Sciences, United States
Background: Multiple system atrophy (MSA) and Parkinson’s disease (PD) have overlapping clinical phenotypes that create diagnostic dilemmas, particularly early in the disease course. Quantitative assessment of phosphorylated alpha-synuclein (P-SYN) using skin biopsies can facilitate early distinction of disease courses. This study aimed to create a clinical-pathological algorithm to distinguish MSA from PD with diagnostic certainty.
Methods: After consent, patients with MSA and PD completed neurologic examinations, medical history review, cognitive evaluation, orthostatic vital signs and neurodegenerative disease questionnaires. Skin biopsies at the distal leg, distal thigh and posterior cervical sites were performed on all participants with quantitation of P-SYN by location, amount and nerve fiber subtype involvement. Clinical, demographic and pathological data were combined using unbiased weighted cluster analysis into an algorithm to differentiate the two disease states based on a training data set, with blinded prospective testing in a validation cohort.
Results: The training data set included 25 patients each with MSA and PD. The validation cohort included an independent group of 30 patients each with MSA and PD. Patients with MSA tended to be younger (67±6.8 vs 71±7.3, P<0.05), with greater synuclein deposition (8.6±4.1 vs 4.5±2.8, P<0.01). The training set identified demographic, clinical and pathological data that could be integrated into a predictive algorithm for diagnosis. The algorithm correctly identified 24/25 PD and MSA in the training set. In the validation data set, 33/35 PD and 32/35 MSA cases were correctly identified providing 92.8% accuracy in diagnosing MSA and PD.
Conclusion: Differentiation between neurodegenerative diseases, such as MSA and PD, remains challenging. The overlapping phenotypes lead to high rates of misdiagnosis in the absence of accurate diagnostic tools. These results, using a clinical-pathological scoring system, suggest that it is possible to differentiate between major synucleinopathy subtypes with high diagnostic accuracy.
P32.05
1 CND Life Sciences, United States
2 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
3 Norton Neuroscience Institute, Louisville, KY, United States
Introduction: The diagnosis of neurodegenerative synucleinopathies in clinical practice has been enhanced by diagnostic guidelines in recent years. However, these guidelines acknowledge that there is an inherent diagnostic uncertainty. The primary aim of this study was to evaluate the clinical impact of skin biopsy detection of phosphorylated alpha-synuclein (P-SYN) in the clinical care of patients with suspected synucleinopathies in a private practice neurology specialty clinic.
Methods: This is a retrospective chart review of patients seen in an outpatient private practice setting to define the clinical utility of skin biopsy detection of P-SYN in the evaluation of patients with suspected synucleinopathy. This data was collected between January 2022 and December 2024. Patients underwent skin biopsy by their treating neurologist when a possible synucleinopathy was suspected. Only patients with at least 12 months of clinical evaluation before skin biopsy and at least 6 months of clinical follow-up post skin biopsy were included in this study. Data extracted by chart review included demographic information, clinical history, physical examination findings, skin biopsy results, medications, referrals, treatment decisions, and changes to medications and diagnosis.
Results: One hundred patients with suspected neurodegenerative disease were included, 47 with tremor, 18 with gait dysfunction, 11 with rigidity/bradykinesia, and 24 with cognitive dysfunction. After skin biopsy testing for P-SYN, 60% had a change in diagnosis, and 91% had a change to their treatment plan.
Conclusion: In patients with suspected neurodegenerative disease, skin biopsy detection of P-SYN altered the diagnosis and management of the majority of patients. These findings indicate that cutaneous P-SYN detection offers significant clinical utility in the outpatient management of patients with suspected neurodegenerative synucleinopathy.
P32.06
1 University of Arizona College of Medicine-Phoenix, United States
2 Movement Disorders Center of Arizona, United States
Objective: To describe the results of skin biopsy for phosphorylated alpha-synuclein (P-SYN) and dopamine transporter (DAT) imaging in patients previously diagnosed with psychogenic parkinsonism (PP), and to evaluate the diagnostic utility of P-SYN biopsy in identifying underlying organic disease.
Background: Psychogenic or functional parkinsonism remains poorly characterized due to its clinical overlap with idiopathic Parkinson’s disease (PD) and the frequent coexistence of both in up to 30% of cases. Even with advanced diagnostic modalities such as surface EMG polygraphy, functional imaging and DAT imaging, differentiation remains challenging. The commercially available Syn-One test detects P-SYN through skin biopsy, and helps identify symptomatic or prodromal synucleinopathies, including PD, multiple system atrophy, dementia with Lewy bodies, pure autonomic failure, and REM sleep behavior disorder. DAT imaging is often used to help differentiate between PD and PP, though has pitfalls including false negatives, inaccurate results due to intake of psychiatric medications and subjective visual interpretation. To our knowledge, there are no published studies investigating results of cutaneous P-SYN in patients with PP.
Design/Methods: We retrospectively reviewed charts of patients diagnosed with PP who underwent DAT imaging, and P-SYN skin biopsy from 2019–2025 at our facility.
Results: Eight patients with PP were identified (6 men, 2 women; mean age 57 ± 16.22 years). DAT imaging was abnormal in 2/8 (25%) and normal in 6/8 (75%). P-SYN biopsy was (+) in 4/8 (50%). P-SYN positivity localized to the posterior cervical region in 3/4 (75%) and the distal leg in 1/4 (25%). Of the 6 patients with normal DAT scans, 3/6 (50%) were P-SYN(+). Of the 2 patients with abnormal DAT scans, 1/2 (50%) was P-SYN(+).
Limitations: Small sample size and referral bias limit generalizability. Additional barriers such as procedural discomfort, travel constraints, and testing costs may have influenced performance of skin biopsy.
Conclusions: P-SYN skin biopsy may identify underlying synucleinopathy in patients initially diagnosed as PP, particularly when DAT imaging is normal. Incorporation of P-SYN biopsy into standard evaluation protocols may improve diagnostic accuracy of PP, and help identify those with concurrent synucleinopathy and guide appropriate management.
P32.07
1 Preview Health, Australia
Parkinson’s disease (PD) is a highly heterogeneous disease where patients can exhibit vastly different symptoms and responses to interventions. By improving our understanding of the biological drivers of PD, we can target interventions more effectively and evaluate its efficacy over time. Here, we report a metabolomics-based assay that utilises machine learning to accurately detect PD and reveal PD-driving metabolites from blood plasma. In less than 20 minutes, this assay predicted PD with > 92% precision and elucidated individual molecular profiles corresponding to different Parkinson’s disease phenotypes. By better identifying different PD subtypes on a molecular level, it is anticipated that this blood test can be used to significantly improve PD care pathway and disease management.
CLINICAL SCIENCES: Co-morbidities
P33.01
1 Arizona State University, United States
2 Mayo Clinic, United States
Introduction: Erectile Dysfunction (ED) is becoming increasingly recognized as a potential marker of chronic medical conditions. Recent research has examined the association between ED and Parkinson’s Disease (PD). In fact, recent findings indicate that men with ED have upwards of a four fold higher risk of developing PD compared to those without a diagnosis of ED.
Objective: Our research investigates associations between self-reported ED severity and neurobiological factors, including measures of cognitive function and neuroimaging of dopaminergic integrity.
Methods: We performed a retrospective analysis of 731 participants (mean age: 65.08±9.53 years, 372 PD patients, 208 prodromal cases, and 108 healthy controls). Patients received cognitive testing through the MoCA and categorized into cognitive impairment levels. Neuroimaging of the bilateral caudate and putamen was measured through dopamine transporter SPECT imaging (DaTScan) binding ratios. Erectile dysfunction was self-reported using a modified International Index of Erectile Function scale (SCOPA-AUT), with possible scores ranging from 0 (no ED) to 4 (severe ED).
Results: Participants with ED showed significantly lower MoCA scores (26±3) compared to those without ED (27±2.15). ED severity negatively correlated with MoCA scores (r=-0.284, p<0.001. In our healthy controls, striatal DaTScan showed a significant, mild association between ED severity and both right caudate dopamine binding ratios (r = 0.236, p=0.0242) and the putamen dopamine binding ratios (r = 0.262, p = 0.0121). However, associations between ED severity and both left caudate (r = 0.150, p = 155) and right putamen (r = 0.143, p = 0.176) dopamine binding ratios did not reach statistical significance.
Conclusions: These data demonstrate that erectile dysfunction represents a multifaceted condition with distinct patterns across neurological health spectrums. ED severity was correlated with cognition in the PD and prodromal cohorts, whereas no correlation was found for the HC. Greater ED severity was significantly associated with increased striatal dopaminergic binding in health controls. This positive, age-adjusted association may reflect a compensatory dopaminergic response similar to that seen in the early stages of Parkinson’s disease. Overall, our findings suggest that ED could serve as a potential marker of central dopaminergic and autonomic alterations, even in the absence of clinically evident neurological disease.
CLINICAL SCIENCES: Fluid and tissue Biomarkers
P34.01
1 Qatar Biomedical Research Institute, Qatar
2 Lundbeck Foundation Parkinson’s Disease Research Center (PACE), Denmark
The body-first vs. brain-first hypothesis of Parkinson's disease (PD) proposes distinct etiological origins, yet its molecular basis remains undefined. To address this, we conducted an exploratory proteomic study using Proximity Extension Assay (PEA) technology (Olink) to measure 552 proteins in 44 body-first and 44 brain-first PD patients, rigorously characterized by imaging and polysomnography. Pathway enrichment analysis (KEGG, GO) revealed a striking molecular divergence. We identified 21 dysregulated proteins (unadjusted p < 0.05) that stratified into two biologically coherent patterns. The body-first subtype was characterized by elevated proteins implicating systemic thromboinflammation and cardiovascular stress, including VWF (coagulation), MBL2 (innate immunity), and NT-proBNP (cardiac dysfunction), which was further supported by enrichment of the complement and coagulation cascades pathway. Conversely, the brain-first subtype showed elevated proteins involved in neuro-immune communication and neural repair, including CXCL1 (neutrophil recruitment), PPP3R1 (T-cell signaling), and FES, with corresponding enrichment in TNF signaling and axon guidance pathways. Our findings provide the first plasma-based molecular evidence that body-first and brain-first PD may be driven by distinct biological processes, involving divergent systemic inflammatory and neuro-immune mechanisms. The strong coherence of these signatures provides a robust rationale for our ongoing work to validate these biomarkers in a larger cohort. These results hold significant promise for developing subtype-specific biomarkers and personalized therapeutic strategies for PD patients.
P34.02
1 Foundation for the National Institute of Health, United States
2 National Institute of Health | National Institute of Neurological Disorders and Stroke, United States
3 Denali Therapeutics, United States
4 Michael J Fox Foundation, United States
The Accelerating Medicines Partnership Parkinson’s Disease and related disorders (AMP® PDRD), launched in 2024, is a precompetitive public-private partnership between the National Institutes of Health (NIH), U.S. Food and Drug Administration (FDA), industry partners, and non-profit organizations. Managed by the Foundation for the National Institutes of Health (FNIH), this collaboration builds upon the first phase, the AMP in Parkinson’s Disease (AMP® PD), leveraging data-driven, precision medicine to identify and validate biomarkers that differentiate PD from related synucleinopathies, such as Dementia with Lewy Bodies (DLB), Multiple System Atrophy (MSA) and other atypical Parkinsonisms.
AMP® PD developed a cloud-native data portal accessible via the Terra platform and generated 11,000 participant clinical assessment and WGS sequencing data, 3,400 participant transcriptomics data, 1,000 participant proteomics data, and 100 postmortem single cell RNA sequencing data amongst 8 different clinical Parkinson’s Disease cohorts. The portal enables data access, utilization of analysis tools, and collaboration with over 1,500 registered users worldwide.
The AMP® PDRD research plan employs deep molecular characterization and longitudinal clinical profiling of harmonized patient data and biosamples to identify and validate diagnostic, prognostic and/or disease progression biomarkers for PD. The program emphasizes open data sharing of harmonized molecular (e.g., whole genome sequencing, transcriptomics, proteomics, single nucleus post-mortem sequencing) and clinical data to facilitate discoveries of new targets, disease subtypes, and predictive markers. AMP PDRD has thus far focused on further exploring Dopa Decarboxylase (DDC), Amyloid Beta, and phospho-tau as potential biomarkers within selected prodromal Parkinson’s disease and other atypical parkinsonism clinical cohorts. Initial fluid biomarker data is anticipated to be shared with the research community by Q3 2026.
AMP® PDRD leverages precision medicine to identify and validate biomarkers differentiating PD from related synucleinopathies and other Parkinsonism’s. New AMP® PDRD cohorts will undergo multi-omic profiling to uncover molecular signatures, support biological characterizations, and integrate new tools in the Knowledge Platform for a multi-scale analysis framework. This ecosystem advances PD and related disorders research, improves clinical trial design, and identifies potential new therapeutic targets.

P34.03
1 Departments of Neuroscience and Neurology, Yale School of Medicine; Interdepartmental Neuroscience Program, Yale University, United States
2 Departments of Pathology and Neuroscience, Yale School of Medicine, United States
3 Center for Neurodegenerative Disease Brain Bank, University of Pennsylvania Perelman School of Medicine, United States
4 Departments of Neuroscience and Neurology, Yale School of Medicine, United States
Parkinson's Disease (PD) is the most common of the synucleinopathies, a group of diseases with alpha-synuclein pathology and neurodegeneration that also includes Multiple System Atrophy (MSA) and Lewy Body Dementia. Their cellular and molecular underpinnings are incompletely understood, hampering disease-specific diagnostics and drug development. More specifically, rates of misdiagnosis between PD and MSA are high due to overlapping symptomatology, resulting in inaccurate prognoses, suboptimal treatment plans for patients, and skewed clinical trials. Recent work has highlighted the structure of alpha-synuclein fibrils in situ as a key difference between MSA and PD, which may be influenced by post-translational modifications such as phosphorylation. Indeed, a novel alpha-synuclein phosphorylation site at Threonine 81 (pT81) was enriched in proteomics analysis of MSA patient brains, but not in PD patient brains. Therefore, we aim to explore pT81 alpha-synuclein as a potential biomarker to differentiate between PD and MSA. We designed and validated the first known tool to assess pT81 alpha-synuclein localization: a polyclonal, phospho-specific antibody for pT81 alpha-synuclein. This antibody shows knockout-level specificity in Western Blot and phospho-specificity in ELISA assay. We then performed staining for pT81 and phospho-Serine 129 (pS129) alpha-synuclein in parallel on MSA, PD, and control post-mortem tissue. Preliminary data showed enriched pT81 alpha-synuclein in a subset of MSA patient midbrains, and none in PD or control midbrains, consistent with proteomic results showing enrichment in a subset of MSA patients. The lack of pT81 alpha-synuclein enrichment was not due to lack of pathology, as we observed pS129 pathology in all MSA and PD patients, specifically in glial cytoplasmic inclusions (GCIs) in MSA and Lewy Bodies and Neurites in PD. Interestingly, we observed enrichment of pT81 alpha-synuclein in neuronal soma as well as GCIs, even though pS129 alpha-synuclein was present almost entirely in GCIs in MSA brains. We are now expanding our dataset of MSA and PD brains to further explore cell-type and brain-area specific distribution of pT81 alpha-synuclein, as well as testing CSF from PD and MSA patients to assess pT81 alpha-synuclein levels via ELISA assay. We predict that pT81 positivity will serve as a crucial exclusion criterion for PD diagnosis, improving enrollment for PD clinical trials and accuracy of PD diagnostics in clinic.
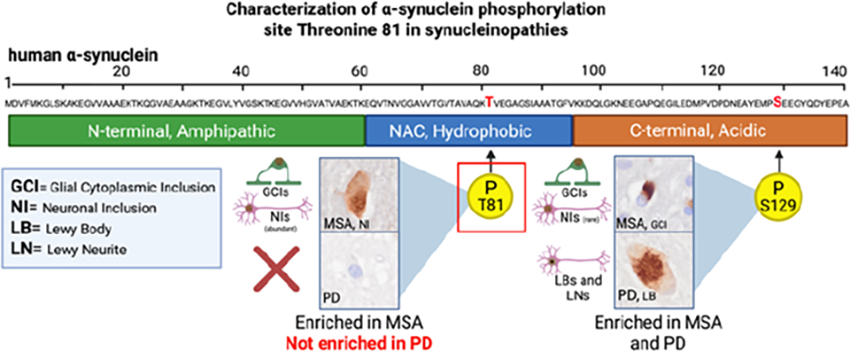
P34.04
1 School of Biomedical Sciences, Queensland University of Technology, Brisbane, QLD 4102, Australia
2 CWD Evolution LLC, Fort Collins, CO 80524, United States
3 School of Biomedical Sciences, Queensland University of Technology, Brisbane, QLD 4102, Faculty of Medicine, The University of Queensland, Brisbane, QLD 4029, Translational Research Institute, Brisbane, QLD 4102, Australia
Alpha-synuclein (α-syn) aggregation is a hallmark of Parkinson’s disease (PD) pathology, contributing to neurodegeneration and motor dysfunction. Traditionally, detection of pathological α-syn has relied on invasive procedures or postmortem analysis. Recent efforts have focused on identifying peripheral biomarkers that reflect central nervous system pathology, with fecal samples emerging as a promising, non-invasive source. The real-time quaking-induced conversion (RT-QuIC) assay has shown high sensitivity in detecting misfolded proteins, making it a valuable tool for α-syn biomarker development. However, detection of synuclein seeds in complex biological matrices such as blood or skin remains technically challenging.
We sought to develop a novel and proprietary fecal sample processing workflow to enable RT-QuIC based detection of gut α-Syn seeding activity in rodent models of PD followed by validation in human patient studies. Protocol development was performed using fecal samples from A53T α-synuclein transgenic (Tg) mice expressing human A53T α-syn and matched wild-type (WT) control littermates. Protocol validation studies were performed in human subjects diagnosed with PD and age-matched healthy controls. RT-QuIC assays were performed to quantify α-syn seeding activity. Thioflavin T (Th-T) fluorescence was monitored to assess aggregation kinetics, including lag phase duration and fluorescence intensity. Aggregation rates were quantified between groups. RT-QuIC analysis revealed significantly elevated Thioflavin T (Th-T) fluorescence and shortened lag phases in fecal samples from A53T α-synuclein Tg mice compared to wild-type controls, indicating robust α-syn seeding activity. Similarly, fecal samples from PD patients showed markedly increased Th-T fluorescence and aggregation kinetics relative to matched healthy controls. Quantitative metrics demonstrated a clear separation between PD and control groups, with aggregation rates significantly higher in A53T α-synuclein Tg mice than WT mice and higher in PD than healthy controls.
Fecal RT-QuIC is a sensitive and non-invasive assay capable of detecting pathological α-synuclein in PD. Its diagnostic potential spans both animal models and human patients, offering potential for early detection, disease monitoring, and may also assist in patient stratification for therapeutic interventions. However, further validation in larger and more diverse cohorts is essential for its robustness and reproducibility.
P34.05
1 Centre for Movement Disorders, Stavanger University Hospital, Norway
2 Stavanger University Hospital, Norway
Biobanks are crucial resources for understanding disease mechanisms and developing better treatments. However, participation can be difficult for people living with Parkinson’s disease and related conditions, particularly for those with limited mobility or living outside major cities.
To overcome these barriers, we have established a new biobank linked to the Norwegian Parkinson Registry that makes use of home-sampling kits. These kits are designed to be safe and user-friendly, allowing participants to collect and send biological samples from their own homes. In the first phase, we tested kits for the collection of dried blood spots, dried plasma spots, faecal samples, and saliva. These samples can be used to study genetic variation, protein biomarkers, and the gut microbiome.
We will present the development and rollout of the kits, share feedback from users, and discuss the opportunities created by linking samples with centralised, national registry data. This model offers a scalable, inclusive approach to biobanking that strengthens Parkinson’s research and can be extended to other neurological conditions. By reducing barriers to participation, this approach will empower more people, regardless of where they live or their health status, to contribute to research.
P34.06
1 Section Clinical Neuroanatomy and Biobanking, Department of Anatomy and Neurosciences, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands, Netherlands
2 Neurochemistry Laboratory, Department of Laboratory Medicine, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands, Netherlands
3 Department of Neurology, Amsterdam UMC, Vrije Universiteit Amsterdam, The Netherlands, Netherlands
4 ProPark, Netherlands
Background Parkinson’s disease (PD) is a clinically and biologically heterogeneous neurodegenerative disorder. Distinct molecular subtypes, driven by lysosomal and mitochondrial dysfunction, may underlie its clinical variability. This study explores blood-based lysosomal and mitochondrial pathway-specific expression profiles as measures of disease severity in PD.
Methods We analyzed 504 baseline plasma samples using a customized SomaScan aptamer-based assay targeting 394 lysosomal and 504 mitochondrial proteins. Samples were derived from a discovery cohort (ProPARK; PP: 145 PD, 73 non-neurological controls) and a validation cohort (ADRC: 104 PD, 182 controls) (Rutledge et al., 2024). Pathway-specific expression scores were derived using LASSO regression. Associations with motor severity (UPDRS-III, Hoehn&Yahr (HY)), cognition (MoCA), levodopa equivalent daily dose (LEDD), and disease duration (available only in PP) were assessed. Analyses were FDR-adjusted.
Results Lysosomal LASSO regression identified 8 proteins that best distinguished PD from controls (AUC: PP train 0.83, test 0.75; ADRC 0.80). Lysosomal score correlated with disease duration in PP (r=0.37, p<0.001), LEDD in both cohorts (PP: r=0.33, p=0.004; ADRC: r=0.41, p=0.004), and HY in ADRC (r=0.24, p=0.046). PD patients showed greater lysosomal score variability (PP SD: controls 0.52 vs PD 0.80; ADRC: controls 0.29 vs PD 1.34). Mitochondrial LASSO identified PARK7 and SDSL (AUC: PP train 0.66, test 0.65; ADRC 0.58). Though less discriminative, mitochondrial scores correlated with disease duration (r=0.27, p=0.004) and LEDD change per year in PP (r=0.30, p=0.004), but not in ADRC. Volcano analysis identified SUMF1 and ARRDC3 as elevated in PP PD vs controls (FC=0.50 and 0.44), replicated in ADRC (FC=0.78 and 0.44). Combined AUC: 0.81 (PP), 0.79 (ADRC). In PP, SUMF1 (r=0.36, p<0.001) and ARRDC3 (r=0.34, p<0.001) correlated with disease duration; SUMF1 also with LEDD (r=0.40, p<0.001). In ADRC, SUMF1 (r=0.32, p=0.045) and ARRDC3 (r=0.47, p<0.001) associated with LEDD; ARRDC3 also with HY (r=0.26, p=0.025).
Conclusion Lysosomal expression scores robustly distinguished PD from controls and were associated with disease severity in both cohorts. SUMF1 and ARRDC3 emerged as promising blood-based biomarkers. Mitochondrial markers showed limited diagnostic value but may reflect disease progression. These findings underscore PD’s biological heterogeneity and support pathway-specific biomarkers for stratification.
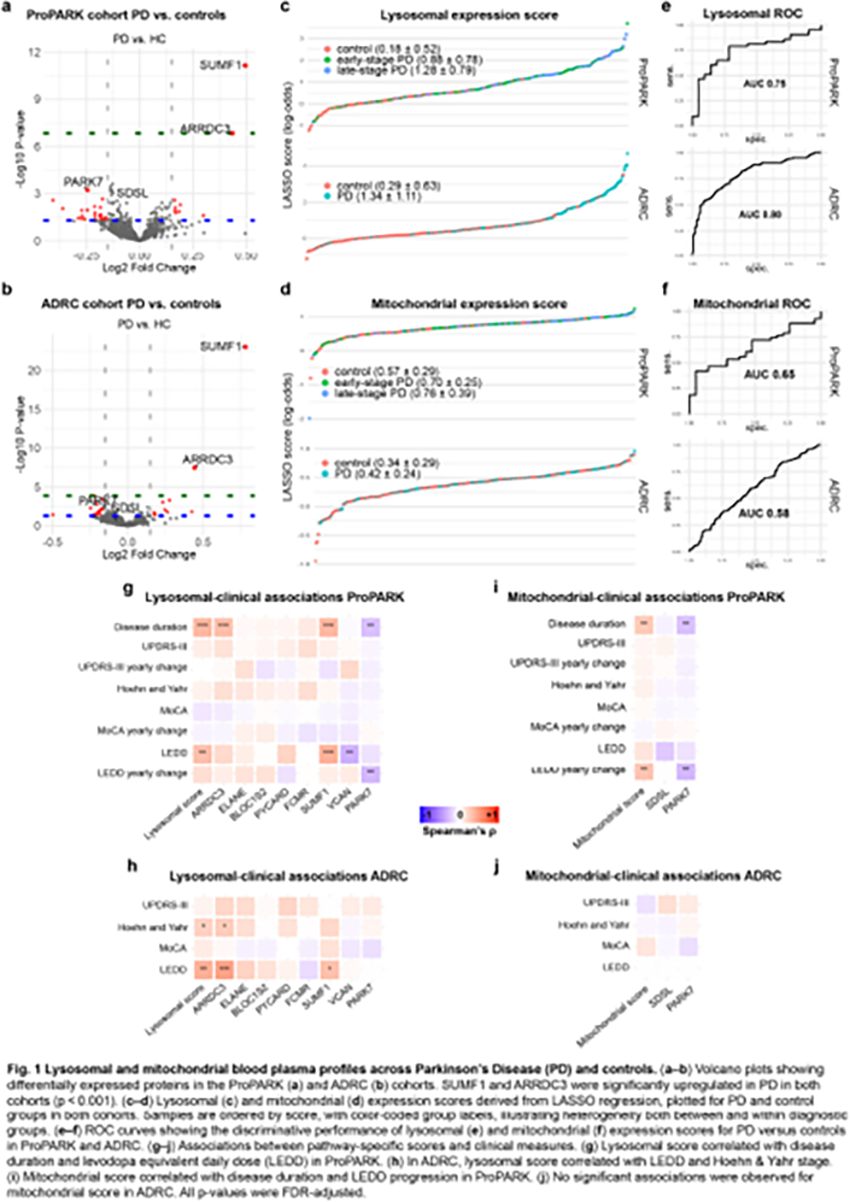
P34.07
1 CND Life Sciences, United States
2 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
Introduction: DLB is a neurodegenerative disease characterized by progressive accumulation of P-SYN within the central and peripheral nervous systems. Quantitative assessment of P-SYN using skin biopsies can facilitate the diagnosis of complex neurological disorders and serve as a potential therapeutic biomarker in clinical trials. We sought to validate a simple, reproducible marker of synuclein pathology in patients with MCI with the DLB phenotype (MCI-DLB) and MCI AD phenotype (MCI-AD) by quantification of the deposition of cutaneous phosphorylated alpha-synuclein (P-SYN).
Methods: After consent, participants with MCI-AD and MCI-DLB completed neurological examinations, medical history screening, and motor assessments. An expert panel blinded to pathology reviewed clinical assessments to confirm diagnoses. Distal leg, distal thigh, and posterior cervical skin biopsies were performed with quantitation of P-SYN.
Results: 103 MCI patients were enrolled, with 98 confirmed by expert panel to meet inclusion criteria. Of these, 44 were MCI-DLB (73.3±8.3 years, 11 female), 35 were MCI-AD (73.0±5.1, 18 female), and 19 were MCI-indeterminate (MCI-ind; 67.8 ± 10.0, 8 female). Groups did not differ in demographics or baseline Clinical Dementia Rating (CDR 0.5 for all groups). At time of abstract submission, follow-up data were available for 71 patients (33 MCI-DLB, 26 MCI-AD, and 12 MCI-ind). At follow-up, P-SYN was detected in 85% of MCI-DLB and 41% of MCI-AD patients. A continuous measure of total P-SYN increased in 69.7% of MCI-DLB, 15.3% of MCI-AD, and 25% of MCI-ind. Across groups, there was a statistically significant increase in P-SYN over 12 months (p<0.001), which was greater for MCI-DLB compared to MCI-AD (p<0.001) and significantly predicted increases in CDR sum of boxes (p=0.008).
Conclusion: Cutaneous P-SYN is detected in most patients with MCI-DLB. The prevalence in MCI-AD is consistent with autopsy reports of co-pathology. P-SYN deposition correlates with declines in cognitive function observed in MCI. Rate of cutaneous P-SYN increases may distinguish between dementia subtype trajectories.
P34.08
1 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
2 CND Life Sciences, United States
Introduction: Parkinson’s disease (PD) is characterized by progressive pathological alpha-synuclein (P-SYN) deposition in the central and peripheral nervous system. Skin biopsy has demonstrated high sensitivity and specificity for the detection of peripheral P-SYN in patients with PD. Recent technological advances now allow for quantitation of peripheral P-SYN, although longitudinal studies in PD have not been conducted. The primary aim of this study was to define changes in cutaneous P-SYN quantification over 18 months in patients with Parkinson’s disease (PD) and idiopathic REM sleep behavior disorder (iRBD).
Methods: After consent, participants with PD of Hoehn and Yahr stages 1, 2, 3 and iRBD completed neurological examinations, medical history, cognitive evaluation, motor assessments, olfactory testing (BSIT), orthostatic vitals, and neurodegenerative disease questionnaires. Skin biopsies taken from the distal leg, distal thigh, and posterior cervical sites were performed on all participants with blinded quantitation of P-SYN. Participants will return for follow-up visits at 6-month intervals following the baseline visit.
Results: At the time of abstract submission, 80 patients completed baseline testing (PD stage I: n=18, 63.3±6.1 years, 10 female; PD stage II: n=25, 67.7±8.7 years, 12 female; PD stage III: n=22, 72.8±9.7 years, 10 female; RBD: n=15, 65.7±9.4 years, 5 female). Baseline P-SYN results were available in 72 patients and 63 (87.5%) were P-SYN positive. Analysis by disease severity revealed 10/11 (90.9%) iRBD patients were P-SYN positive, 15/18 (83.3%) in PD Stage I, 23/25 (92%) in PD Stage II, and 15/18 (83.3%) in Stage III patients were P-SYN positive. P-SYN quantitative assessment correlated with greater motor impairment, indicated by the UPDRS Pt. 3 (r=0.26, p=0.026).
Conclusions: Cutaneous P-SYN was present in skin samples from patients with iRBD and in PD across Hoehn and Yahr stages 1-3. Preliminary data suggests a correlation between quantitative measures of P-SYN and disease severity. Longitudinal follow-up data collection is ongoing and will be reported at the 2026 WPC Meeting.
P34.09
1 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
2 CND Life Sciences, United States
3 IRCCS Institute of Neurological Sciences of Bologna, Italy
Introduction: Both skin and spinal fluid assays can detect pathological alpha-synuclein, but few studies have direct head-to-head comparisons of the results. The objective of this study is to compare the performance characteristics of two established current biomarkers, skin biopsy immunofluorescent and spinal fluid seed amplification assays, in the detection of pathological alpha-synuclein (P-SYN) in patients and controls from all head-to-head publications.
Methods: This is a meta-analysis of published data comparing skin immunofluorescent and spinal fluid seed amplification assays for the detection of P-SYN in patients with clinically established synucleinopathies and non-synucleinopathies disease controls using ancillary testing for confirmation (other than skin immunofluorescence or SAA). Publications using accepted methodologies, obtained at the same time point, were reviewed from the literature, with data extracted by individual patients for direct comparison.
Results: Two publications reporting simultaneous measurement of skin biopsy immunofluorescent and spinal fluid SAA (Donadio 2021, Liguori 2023) met criteria for the analysis. 108 patients were studied, 47 with synucleinopathy (isolated REM sleep behavior disorder [RBD-39], Lewy body disease [4] and multiple system atrophy [2]), and 61 with non-synuclein disease (narcolepsy [22], neuropathy [16], amyotrophic lateral sclerosis [3], depression [2], cerebrovascular disease [4], sleep apnea [3], Alzheimer’s [4], and other [9]). Using clinically established diagnoses supplemented by ancillary testing (DaTScan, cardiac MIBG, Polysomnography), skin biopsy was 88% sensitive and 100% specific for P-SYN detection, while SAA was 75% sensitive and 83% specific for the detection of P-SYN in established synucleinopathies. In patients with RBD, skin biopsy was 77% sensitive and 100% specific for P-SYN detection, while SAA was 67% sensitive and 83% specific for the detection of P-SYN. The overall accuracy of skin immunofluorescence was 91%, while SAA was 77% (across established synucleinopathy and RBD groups combined).
Conclusion: In patients with suspected neurodegenerative disease, skin biopsy immunofluorescence outperforms spinal fluid SAA in this meta-analysis of patients with neurodegenerative disease. The results of this analysis emphasize the need for well-conducted scientific studies of synuclein biomarkers across disease stages.
P34.10
1 Octave Bioscience, United States
Introduction: Multiple research groups have explored the potential for early detection of Parkinson’s Disease (PD) from blood protein levels; however, comparatively little work has been done to assess the specificity of candidate protein biomarkers for PD. Progressive supranuclear palsy (PSP) is a rare neurodegenerative disease that can mimic symptoms of Parkinson’s but responds only modestly to pharmacologic intervention. Yet, the extent of shared biomarker signal across atypical parkinsonisms such as PSP and PD is not known for most PD biomarkers.
Methods: 43 PSP participants enrolled before or after diagnosis, 591 PD participants enrolled no more than 10 years prior to diagnosis, and 9,903 age- and sex-matched neurologically healthy controls (NHCs) with proteomic profiling were ascertained in the UK Biobank. Protein abundances were standardized to z-scores relative to NHCs accounting for age, sex, and mean protein abundance assayed on the Olink Explore platform. We performed Mann-Whitney U tests to distinguish PSP vs NHCs and PD vs NHCs. LASSO logistic regression models were trained and evaluated using a 5-fold cross-validation procedure with the combined set of PD and PSP discovered biomarkers.
Results: PSP cases exhibited higher Neurofilament light polypeptide (NfL) and lower N-terminal Pro-Brain Natriuretic Peptide (NT-proBNP) levels than PD cases. 4 of the remaining top 10 proteins have been linked to genetic encephalopathies. All of the discovered PSP markers were selected across all folds. The full models (∼25 proteins) attained an average AUC of 0.733 (95% CI 0.646 - 0.819).
Conclusion: Consistent with reports in other cohorts, neurodegeneration as measured by NfL is higher in PSP cases relative to PD cases using clinical diagnoses. In contrast, autonomic dysfunction as measured by NT-proBNP was greater in PD cases. Our results suggest that atypical parkinsonisms have promising and distinct biomarkers that could aid assessment of abnormal movements. Furthermore, autonomic nervous system PD biomarkers may distinguish PD from other movement disorders better than CNS biomarkers. Characterization of the specificity of biomarkers across movement disorders is warranted prior to evaluating cases with uncertain clinical diagnosis.
P34.11
1 The University of Sydney, Australia
Parkinson’s disease is a progressive neurodegenerative movement disorder of which there is no medication to stop or slow disease progression. The lack of disease modifying therapies and biomarkers for Parkinson’s disease can be attributed to poor understanding of the disease pathobiology, in particular the early or initiating events. Compellingly, several Parkinson’s disease risk genes with a lipid-related function have recently been identified, including GBA1, GALC, SMPD1, SREBF1, ELOVL7, DGKQ, ASAH1 and PLA2G6. Recently, the serum lipid signatures of Parkinson’s disease subjects were found to be significantly distinguishable from controls with lipids involved in sphingolipid, phospholipid and glycerolipid metabolism, as well as insulin/glucose signalling particularly affected. However, it is recognised that subjects with a clinical diagnosis of Parkinson’s disease have actually sustained the disease for at least 10 years prior to clinical symptoms manifesting. This study therefore investigated if lipid dysfunction can be detected earlier, in the prodromal phase of Parkinson’s disease. To address this, a set of plasma samples from subjects with a sleep disturbance known as REM sleep behaviour disorder was attained. These subjects have a high chance of transitioning to a diagnosis of Parkinson’s disease within 10 years and provide a unique opportunity to study the prodromal phase of Parkinson’s disease. Results from LC-MS/MS presented include a comparison of 300 plasma lipid markers between those at a high risk of Parkinson’s disease (REM sleep behaviour disorder patients) compared to controls, and correlations of plasma lipid levels to clinical severity scales to assess biomarker potential.
P34.12
1 Queensland University of Technology (QUT), Australia
2 Princess Alexandra Hospital (PAH), Australia
3 The University of Queensland (UQ), Australia
Background: The gut–brain axis is increasingly recognized as a key driver of Parkinson’s disease (PD) pathogenesis. Gastrointestinal dysfunction often precedes motor onset by decades, and multi-omic studies consistently reveal gut dysbiosis—marked by depletion of short-chain fatty acid (SCFA)-producing taxa, enrichment of pro-inflammatory species, and altered microbial neurotransmitter metabolism. These disturbances contribute to gut barrier dysfunction, systemic inflammation, and α-synuclein aggregation. Translation into actionable biomarkers and therapies remains constrained by the absence of large, harmonized biobanks integrating clinical, microbial, and metabolic data.
Methods: The Parkinson’s Microbiome Biobank—a collaboration between QUT, TRI, Princess Alexandra Hospital, and UQ—is Australia’s first PD-specific multi-omic repository linking standardized clinical phenotyping with biospecimen collection. The target cohort (n=614; 335 PwPD, 279 matched controls) is recruited through specialist-led and remote pathways. To date, 269 participants (175 PwPD, 94 controls) have been enrolled under harmonized protocols incorporating Movement Disorder Society rating scales and PPMI-aligned questionnaires. Stool, blood, urine, and skin samples undergo shotgun metagenomics, metabolomics, immune profiling, and α-synuclein seeding quantification (RT-QuIC) to establish an integrated microbiome–immune–metabolic atlas of PD.
Results: Preliminary analyses reveal a distinct PD-associated microbial–metabolic signature. Metagenomics showed reduced alpha diversity and loss of Faecalibacterium prausnitzii, with enrichment of Blautia, Bacteroides, and Akkermansia—species linked to mucin degradation, barrier dysfunction, and pro-inflammatory signaling. Urinary metabolomics showed perturbations in aromatic amino acid, fatty acid oxidation, cholesterol and bile acid pathways, and polyamine and xanthine turnover—domains associated with oxidative stress and neuroinflammation. These findings suggest dysregulated microbial and host metabolic networks with impaired lipid and bile acid homeostasis, oxidative–inflammatory stress, and immune activation, supporting a mechanistic gut–brain axis in PD.
Conclusions: The Parkinson’s Microbiome Biobank provides a transformative platform for decoding microbial, metabolic, and immune mechanisms in PD, enabling biomarker discovery, longitudinal validation, and translational modeling to advance microbiome-informed precision neurology.
P34.13
1 Université Laval, CERVO Brain Research Center, Rempart Neurophysiologie Inc., Canada
2 Université Laval, CERVO Brain Research Center, Canada
3 Université Laval, Centre de recherche Nutrition, Santé et Société (NUTRISS), Institute of Nutrition and Functional Foods (INAF), Canada
4 CERVO Brain Research Center, Canada
5 Université Laval, CHU de Québec-Université Laval, Canada
6 Université Laval, Centre de recherche Nutrition, Santé et Société (NUTRISS), Institute of Nutrition and Functional Foods (INAF), Canada Research Excellence Chair in the Microbiome-Endocannabinoidome Axis in Metabolic Health (CERC-MEND), Canada
Parkinson’s disease (PD) is often diagnosed only after substantial neurodegeneration, long after non-motor changes have emerged. This delayed detection limits opportunities for timely intervention and underscores the urgent need for diagnostic biomarkers that can identify PD before symptoms appear. Our work addresses this gap by combining two complementary, non-invasive approaches to reveal disease signatures prior to overt clinical manifestation.
First, electroretinography (ERG) assessed retinal function in homozygous M83 mice overexpressing human A53T α-synuclein (N = 10 males, 11 females) and in patients with idiopathic PD (mean age 63.4 ± 7.7 years; disease duration 4.2 ± 2.1 years; N = 12 males, 8 females) alongside age-matched controls (mean age 61.7 ± 8.4 years; N = 9 males, 11 females). ERG detected functional deficits in bipolar, amacrine, and ganglion cells, establishing the retina as a sensitive window into PD progression.
Second, oral microbiota profiling using 16S rRNA sequencing revealed shifts in bacterial families—including Selenomonadaceae, Microbacteriaceae, Porphyromonadaceae and P5D1.392—that correlated with disease severity metrics such as H&Y score, symptom duration, and time since diagnosis. Sex-specific differences emerged in both mice and humans, uncovering previously unrecognized layers of disease heterogeneity.
Integrating retinal and microbiota features, we are developing predictive models to classify PD risk and progression based on these signatures. Concordant patterns across preclinical and clinical cohorts demonstrate the translational potential of these non-invasive tools. This multi-modal framework provides a path toward biological-based diagnosis well before traditional clinical detection, offering opportunities for timely intervention, personalized therapeutics, and a fundamental shift in how PD is understood and managed.
P34.14
Virgilio Gerald Evidente1, Rebecca Johnson1, Danielle Drake1, Danica Evidente1
1 Movement Disorders Center of Arizona, United States
OBJECTIVE: To compare results of skin biopsy alpha-synuclein immunofluorescence (αS-IF) assay with CSF alpha-synuclein (AS) seed amplification (SAA) assay in patients with parkinsonism or REM behavior disorder (RBD).
BACKGROUND: There are currently 2 FDA-approved tests for identifying synucleinopathies like Parkinson’s disease (PD), Multiple System Atrophy (MSA), Dementia with Lewy Bodies (DLB) and Pure Autonomic Failure (PAF). RBD is a nonmotor symptom that commonly precedes clinical symptoms in synucleinopathies, In Arizona, the Syn-One test for cutaneous AS has been commercially available since late 2019, whereas the SAAmplify (aka SYNTap) test for CSF AS became commercially available only in early 2025. There is a dearth of studies that compare results of cutaneous AS-IF with CSF AS-SAA. In a study of 41 RBD patients, cutaneous AS-IF showed 89% diagnostic accuracy compared to 69% for CSF AS-SAA. In another study of 90 patients fulfilling diagnostic criteria for synucleinopathies and non-synucleinopathies, both IF and RT-QuIC (a form of SAA) of skin and CSF showed high sensitivity and specificity in discriminating synucleinopathies from non-synucleinopathies.
DESIGN / METHODS: We retrospectively reviewed charts of all patients who have undergone both skin biopsy and CSF assay of AS from 2019-2025 in one movement disorders center.
RESULTS: We identified 36 patients who have undergone both cutaneous AS-IF and CSF AS-SAA for either parkinsonism or RBD. 11 were female, 25 were male. For all 36, skin biopsy preceded CSF tap by a mean of 28 months (SD=22.76). Results were concordant for 17/36 (47%) and discordant for 19/26 (53%). Of the 17 concordant cases, 4/17 (24%) were AS(+) for both skin and CSF, whereas 13/17 (76%) were AS(-) for both. Of the 19 discordant cases, 16/19 (84%) were AS(+) in skin but AS(-) in CSF, whereas 3/19 (15%) were AS(-) in skin but AS(+) in CSF. In 15/36 (42%) of patients, the diagnosis was altered after CSF AS-SAA.
CONCLUSIONS: The diagnostic accuracy may be increased by comparing cutaneous AS-IF with CSF AS-SAA in patients with suspected synucleinopathy where the diagnosis remains unclear. Combining the 2 tests may best identify patients with isolated peripheral synucleinopathy (like PAF or RBD with no central pathology) versus those with both peripheral and central synucleinopathy (like PD, MSA, DLB or RBD with central pathology). Combining the 2 tests may also help clarify false(+) or false(-) skin biopsy results.
P34.15
Danielle Drake1, Danica Evidente1, Sam Webster1, Virgilio Gerald Evidente1
1 Movement Disorders Center of Arizona, United States
OBJECTIVES: To determine if patients (pts) with REM behavior disorder (RBD) with skin biopsy (Bx) evidence of phosphorylated alpha-synuclein (P-SYN) with no movement disorder present with subtle abnormalities in kinematic gait analysis.
BACKGROUND: The synucleinopathies, which include Parkinson’s disease, Multiple System Atrophy, Dementia with Lewy Bodies and Pure Autonomic Failure, are often associated with RBD even in the premotor or prodromal stage. A Mayo Clinic study comparing 42 probable RBD pts with 492 controls showed that RBD pts had subtle gait changes on automated gait analysis including decreased velocity and cadence, along with increased double limb support, stride time and greater swing time compared to controls. To our knowledge, there are no studies analyzing gait in RBD pts with biological confirmation of pathological alpha-synuclein.
DESIGN/METHODS: We retrospectively reviewed charts of all pts seen in our center from 2019-2025 with RBD with no movement disorder, who underwent skin biopsy for P-SYN and kinematic gait analysis (KGA) utilizing the Zeno walkway. We examined velocity, cadence, walk ratio, step length, stride length, stride width, step time, stride time, stance time, stance %, swing %, single support % and double support %.
RESULTS: We identified 22 RBD pts, 17 men & 5 women, of which 19/22 (86%) were Bx(+) and 3/22 (14%) were Bx(-). Mean ages at time of Bx were 66.58 ± 9.59 for Bx(+) pts and 58.33 ± .7.50 for Bx(-) pts. KGA was normal in 16/22 (73%) and abnormal in 6/22 (27%). All 3 Bx(-) pts had abnormal KGA, whereas 13/19 (68%) of Bx(+) pts had abnormal KGA. DAT scan was performed in 16/19 Bx(+) pts, of which 3/16 (19%) were abnormal. UPSIT smell testing done on 11/19 Bx(+) pts was abnormal in 8/11 (73%). UPSIT done on 2/3 of Bx(-) pts was abnormal in 1/2 (50%). Statistically significant differences were noted between Bx(+) and Bx(-) pts for cadence (p=0.04), stride width (p=0.03), stride time (p=0.04) and stance time (p=0.002). In comparing Bx(+) pts with historical age-matched controls, statistically significant differences were noted for velocity (p=0.017), cadence (p=0.006), step length (p=0.012), stride width (p=0.0006), stance % (p=0.04), swing % (p=0.00001), single support % (p=0.000006) and double support % (p=0.000004).
CONCLUSIONS: Kinematic gait analysis may be combined with smell testing and DAT scan in helping identify asymptomatic RBD patients with prodromal synucleinopathy. Larger studies are required.
CLINICAL SCIENCES: Pharmacological therapy
P35.01
1 Department of Neurology, University of Florida, Fixel Institute for Neurological Diseases, United States
2 Selkirk Neurology & Inland Northwest Research, PLLC, United States
3 Department of Neurology, Movement Disorder Clinic, University Hospital of Bispebjerg, Denmark
4 Department of Clinical Neuroscience, University of Gothenburg, Sweden
5 Unidad de Trastornos del Movimiento, Servicio de Neurología y Neurofisiología Clínica, Instituto de Biomedicina de Sevilla, Hospital Universitario Virgen del Rocío/CSIC/Universidad de Sevilla; Centro de Investigación Biomédica en Red sobre Enfermedades Neurodegenerativas (CIBERNED), Instituto de Salud Carlos III; Departamento de Medicina, Facultad de Medicina, Universidad de Sevilla, Spain
6 Department of Neurology, Victor Babes University of Medicine and Pharmacy, Romania
7 AbbVie Inc., United States
8 Parkinson-Klinik Ortenau, Germany
Introduction: Foslevodopa/foscarbidopa (LDp/CDp) is a prodrug of carbidopa/levodopa approved for treatment of motor fluctuations in adults with advanced Parkinson’s disease (aPD) and is delivered via a 24-hour/day continuous subcutaneous infusion (CSCI) [1,2]. We evaluated satisfaction with LDp/CDp treatment in people with aPD in real-world settings.
Methods: The ROSSINI (Real-world Outcomes with continuouS Subcutaneous levodopa INfusIon) prospective, observational, multicountry study (NCT06107426) included adults with levodopa-responsive aPD who started LDp/CDp per local prescribing label (LDp/CDp naive) [1,2]. Questionnaire data were collected in a prespecified interim analysis 6 months after LDp/CDp treatment initiation, evaluating different aspects of treatment satisfaction. Satisfaction with a patient support program with nurses was assessed by people with aPD and healthcare providers (HCP) at month 6. Data are descriptive with no imputation of missing data.
Results: At month 6, 105 people were enrolled in the ROSSINI study (Canada, Israel, and Europe); of these, 51–52 answered questions about satisfaction with LDp/CDp. Regarding
satisfaction with nursing support, 68 people with aPD and 74 HCPs shared responses. The majority of people with aPD (76.9%) reported being “satisfied” or “very satisfied” with treatment, whereas 2 (3.8%) were “dissatisfied” or “very dissatisfied.” Similarly, the majority of people with aPD agreed that they wished they had started LDp/CDp treatment sooner, were likely to continue LDp/CDp treatment, would recommend LDp/CDp treatment to others, and were comfortable with the CSCI device; less than 10% of people with aPD reported a negative impression in any of these areas (Table). Six months after starting LDp/CDp, satisfaction with nursing support was also rated positively by the majority of people with aPD (Table).
Conclusion: People with aPD reported favorable satisfaction with LDp/CDp treatment received in real-world settings. Patient satisfaction can be an important factor in clinical decision-making and adherence to treatment.
Vyalev (foscarbidopa/foslevodopa). Prescribing information. AbbVie Inc.; 2024. Accessed Aug 2025. https://www.rxabbvie.com/pdf/vyalev_pi.pdf.
Produodopa (foslevodopa/foscarbidopa). Summary of product characteristics. AbbVie Ltd.; 2024. Accessed Aug 2025. https://www.medicines.org.uk/emc/product/15213/smpc.

P35.02
1 University of Texas Health Science Center at San Antonio, San Antonio, TX, USA, United States
2 Institute of Psychiatry, Psychology & Neuroscience, King’s College London, London, and Parkinson Foundation Centre of Excellence, Kings College Hospital, London, United Kingdom
3 University of South Florida, Tampa, FL, United States
4 AbbVie, United States
5 University of Lund, Lund, Sweden
Introduction: Sleep disturbances are prevalent in people with advanced Parkinson’s disease (aPD). Foslevodopa/foscarbidopa (LDp/CDp) 24-hour/day continuous subcutaneous infusion is approved for treating motor fluctuations in adults with aPD, and prior studies show that LDp/CDp is associated with improvements in sleep disturbances. The impact of changes in sleep disturbances on daytime motor symptoms has not been previously evaluated.
Methods: This post hoc analysis examined LDp/CDp-treated people with aPD with clinically relevant sleep disturbances at baseline (Parkinson’s Disease Sleep Scale-2 [PDSS-2] scores ≥ 18), from two phase 3 studies: a 12-week(W), randomized controlled trial (RCT), and a 52W open-label trial (OLT). Only participants with non-missing PDSS-2 scores at their respective final visit (W12 or W52) were included. Outcomes included changes from baseline (CFB, as mean[SD]) in PDSS-2 scores, “on” time without troublesome dyskinesia and “off” time (PD diaries), and activities of daily living (ADLs, MDS-UPDRS Part II). P-values were determined using 2-sided paired t-tests comparing change at final visit versus baseline.
Results: Overall, 56% (n/N=14/25) RCT participants with sleep disturbances at baseline who completed the study had improved to PDSS-2 <18 at the W12 visit, with a mean (SD) decrease of 17.4 (9.2) points (p≤.001). These participants showed concurrent significant improvements in "on" time without troublesome dyskinesia (CFB= 4.9[4.0] h, p≤.001), “off" time (-5.1[4.4] h, p≤.001), and MDS-UPDRS part II (-6.8[6.5], p=.002). In the OLT, 69.2% (n/N=54/78) of participants with sleep disturbances at baseline had PDSS-2 <18 at W52 (PDSS-2 CFB=-15.4 [8.8], p≤.001), along with significant improvements from baseline in “on” time without troublesome dyskinesia (4.6 [3.1] h, p≤.001), “off” time (-4.4 [3.2] h, p≤.001), and MDS-UPDRS part II (-4.9 [6.7], p≤.001).
Conclusion: Participants with PDSS-2 scores ≥18 at baseline, who experienced a reduction to <18 after LDp/CDp treatment, also showed significant improvements in motor symptoms and ADLs. These findings suggest that improvement of sleep disturbances is associated with greater daytime motor benefits, and that restoring better nights may potentially contribute to better days in aPD.
P35.03
1 Merz Therapeutics, Germany
2 Merz Therapeutics GmbH, Germany
Introduction The standard of care for the management of motor symptoms in people with Parkinson disease (PwP) is orally administered levodopa; however, PwP often experience a progressive decline of clinical effect over time and development of motor response fluctuations (OFF episodes) within 5 years of starting treatment. CVT-301 is an orally inhaled formulation of levodopa developed for the treatment of episodic OFF periods. This study assessed the efficacy and safety of CVT-301 in PwP stratified by time from first OFF episode to study treatment initiation.
Methods This post hoc analysis assessed the efficacy and safety of CVT-301 (84 mg) in PwP experiencing OFF episodes. Data were pooled from three phase III trials (CVT-301-004, CVT-301-004e [limited to roll-over from control arms in 004/005], and CVT-301-005). Analyses were conducted on subgroups based on the time between first OFF episode and the start of study treatment, defined as <2 years (early treatment initiation) and ≥2 years (late treatment initiation). Efficacy was assessed by change in Unified Parkinson’s Disease Rating Scale Part III (UPDRS-III) score from pre-dose to 30 minutes post-dose at Week 12. Safety endpoints included treatment-related treatment emergent adverse events (TEAEs) of cough or throat irritation.
Results A total of 437 PwP were pooled. The mean age (range) was 63.5 (37–82) years; 64.3% were male, and 96.3% were White. The mean (standard deviation [SD]) time since diagnosis was 8.7 (4.50) years and the mean (SD) time since first OFF episode was 3.8 (3.07) years. Most PwP experienced their first OFF episode ≥2 years before study treatment initiation (n = 337, 77.1%). The mean (SD) change in UPDRS-III score from pre-dose to 30 minutes post-dose at Week 12 was −14.6 (11.95) among PwP in the early-treatment-initiation group (n = 100) and −14.7 (10.12) for late-treatment-initiation group (n = 337), showing consistent effects. Cough TEAEs occurred in 22 (22.0%) PwP in the early- and 53 (15.7%) in the late-treatment-initiation groups. Throat irritation TEAEs occurred in 6 (6.0%) PwP in the early- and 7 (2.1%) in the late-treatment-initiation groups. Most TEAEs were mild across both early- and late-treatment-initiation groups (Table).
Conclusion These findings support the use of CVT-301 in PwP as a consistently effective and well-tolerated treatment in both early- and late-treatment-initiation groups.

P35.04
1 Merz Therapeutics, Germany
2 Merz Therapeutics GmbH, Germany
Introduction For people with Parkinson disease (PwP), orally administered levodopa is the first-line standard of care for the management of motor symptoms. The clinical effect, however, can decline over time and many PwP develop motor response fluctuations (OFF episodes) within 5 years of initiating oral treatment. CVT-301 has been developed as an orally inhaled formulation of levodopa for the treatment of episodic OFF periods. This analysis assessed the safety of CVT-301 in PwP, focusing on treatment-related treatment-emergent adverse events (TEAEs) of cough and throat irritation.
Methods Pooled data from three phase 3 trials (CVT-301-004, CVT-301-004e [limited to roll-over from control arms in 004/005], and CVT-301-005) were used for post hoc subgroup analysis to assess the safety of CVT-301 (84 mg) in PwP experiencing OFF episodes. Safety endpoints included incidence, onset, duration, and severity of cough or throat irritation TEAEs assessed as treatment related.
Results A total of 437 PwP were pooled. The mean age (range) was 63.5 (37–82) years; 64.3% were male, and 96.3% were White. The mean (standard deviation [SD]) time since diagnosis was 8.7 (4.54) years and since first OFF episode was 3.8 (3.07) years. Most PwP experienced their first OFF episode ≥2 years before study treatment initiation (n = 337, 77.1%). Cough was experienced by 75 (17.2%) PwP and throat irritation by 13 (3.0%). The median (interquartile range [IQR]) time to onset after study treatment initiation was 0.14 (0.14–3.86) weeks for cough and 1.14 (0.14–4.71) weeks for throat irritation. The probability to remain free of treatment-related cough was 90.1% at Week 1 and 84.7% at Week 60. The median (IQR) duration of cough was 4.0 (0.14–14.14) weeks and throat irritation 5.14 (0.43–43.43) weeks. Most TEAEs were mild across all dosing groups, with no dose-dependent increase in severity (Table).
Conclusion These findings support the use of CVT-301 as a well-tolerated treatment for use in PwP, with predominantly mild cough and throat irritation TEAEs across all groups, and no dose-dependent increase in incidence and severity. The probability of remaining free of treatment-related cough in long-term treatment was 84.7%. It is worth noting that during the study, participants were accompanied by healthcare professionals to practice treatment inhalation, which may have resulted in low numbers of TEAEs. It is recognized that PwP may require practice to use CVT-301 in a real-world setting.
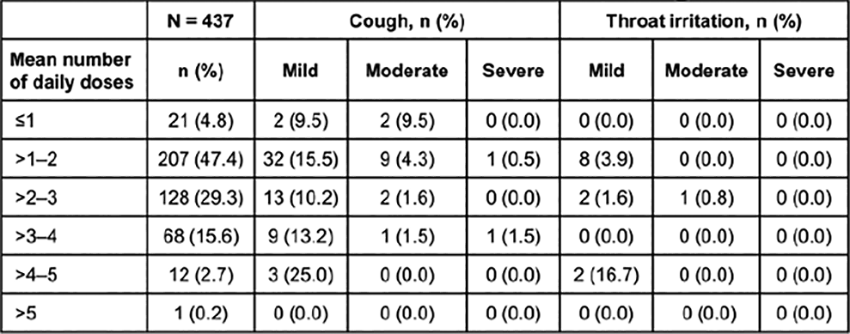
P35.05
1 CHU Toulouse, France
2 CHU University Hospital, France
Background: Up to 50% of Parkinson’s disease (PD) patients develop mild motor fluctuations (OFF-time) within 2 years of starting levodopa, increasing to 70% after 9 years. In 2017, the FDA approved two amantadine extended-release (ER) formulations (ADS-5012 and OS-320) for dyskinesia. Post-hoc analyses of ADS-5012 trials in 2021 showed significant OFF-time reduction (≈1 h vs. placebo), leading to FDA approval of amantadine ER as add-on therapy for motor fluctuations—though it remains unavailable in many European countries. No randomized clinical trial has yet evaluated amantadine immediate-release (IR) for motor fluctuations. We hypothesize that the dual mechanism of amantadine IR may improve motor fluctuations without worsening dyskinesia.
Methods: Amantadine-naïve PD patients with ≥2 h/day of motor fluctuations and no device-aided therapies will be enrolled. After 3–4 weeks of titration, participants will receive stable doses of amantadine IR (up to 300 mg/day) or placebo for 12 weeks (Figure 1). The primary endpoint is the change from baseline to 3 months in OFF-time (Hauser diaries, 3-day average). Secondary outcomes include dyskinesia, freezing of gait, fatigue, and quality of life.
This French multicenter, double-blind, placebo-controlled, phase 2 trial will include 132 PD patients across 18 expert centers. Analyses will be conducted on the modified intention-to-treat (mITT), modified full analysis set (mFAS), and per-protocol (PP) populations. The mITT includes all randomized patients with ≥1 dose of treatment; mFAS includes those with baseline and endpoint data; PP includes patients completing the study per protocol. Participants with major protocol deviations or antiparkinsonian treatment changes will be excluded from PP analysis.
Patient inclusion began in October 2025, with recruitment completion expected by August 2027 (ClinicalTrials.gov: NCT06817200).
Expected benefit: This study may offer a new, low-cost oral treatment for PD motor fluctuations—an area of unmet need despite optimized therapy. Motor fluctuations often impair quality of life more than dyskinesia. If effective, amantadine IR could uniquely improve both OFF-time and good ON-time (without troublesome dyskinesia), unlike current levodopa add-on options that reduce OFF-time at the cost of increased dyskinesia.

P35.06
1 Department of Environmental Health Sciences, Florida International University, Miami, FL, USA, United States
2 College of Health Solutions, Arizona State University, Tempe, AZ, USA, United States
3 The Herbert Wertheim UF Scripps Institute for Biomedical Innovation and Technology 130 Scripps Way Jupiter, FL, USA, United States
Background: Current pharmacological treatments for Parkinson’s disease (PD) primarily provide symptomatic relief without altering disease progression. Our recent data show that Dynamin-related protein 1 (DRP1), a key mediator of mitochondrial fission, has emerged as a regulator of neuroinflammation and α-synuclein pathology. To accelerate therapeutic discovery, we developed a high-throughput screening (HTS) platform to identify FDA-approved molecules that inhibit DRP1 activity.
Methods: Using an automated 1,536-well robotic system, we screened 3,208 FDA-approved compounds for inhibition of recombinant human DRP1 GTPase activity using a colorimetric assay. Lead compounds were validated through EC50 determination, and cytotoxicity assay (Alamar blue). Primary microglia from heterozygous DRP1-KO mice and their WT littermates were treated with lipopolysaccharide (LPS) and analyzed for inflammation using qPCR, soluble and insoluble α-synuclein using immunoblotting, and immunofluorescent detection of phosphorylated α-syn (pS129). Brain concentrations of oxytetracycline (OxyT) were determined at 0.1, 0.5, 3, 6, and 24hrs post administration using LC-MS/MS. C57Bl mice received OxyT (20 or 40 mg/kg every 3hrs for five doses) with or without LPS (5 mg/kg). Ventral midbrains were microdissected for multiplex ELISA quantification of neuroinflammatory markers.
Results: Five tetracycline derivatives: oxytetracycline, meclocycline, methacycline, tigecycline, and minocycline, were identified as DRP1 inhibitors. OxyT emerged as the lead candidate (EC₅₀=3.757μM) with no detectable cytotoxicity up to 100μM. Peak brain concentrations of OxyT were 0.1hrs post administration at 0.425ng/mg with an estimated half-life of 2.85hrs. OxyT suppressed LPS-induced inflammatory gene expression in primary microglia and dose-dependently reduced soluble, insoluble, and pS129 α-syn levels in PFF-treated microglia, astrocytes, and LUHMES neurons. OxyT significantly attenuated LPS-induced neuroinflammation in the ventral midbrain of C57Bl mice. Such protective effects of OxyT were also observed in vitro and in vivo models with heterozygous DRP1-KO.
Conclusions: We established a robust HTS platform for identifying small-molecule DRP1 inhibitors and uncovered OxyT with dual anti-inflammatory and anti-α-synuclein properties. Given OxyT’s antibiotic profile, further optimization and screening efforts are underway to identify additional DRP1 inhibitors with improved safety and chronic use potential.
P35.07
1 Britannia Pharmaceuticals Ltd, United Kingdom
Introduction: APO-go® infusion (continuous subcutaneous apomorphine hydrochloride) has a 30-year heritage of clinical use in the management of Parkinson’s disease, with clinical trial evidence supporting its efficacy and tolerability.1-4 Effective delivery of subcutaneous apomorphine is achieved using an ambulatory mini-pump (the CRONO® infusion pump) which delivers apomorphine subcutaneously via an infusion line. The infusion system is intended to be used during the patient’s waking day, so is set up by them each morning and then removed in the evening.
Innovation to meet patients’ needs: Set-up and use APO-go® infusion is not complex but does require a degree of careful preparation dexterity from the user. Over the past decade, the procedure for delivery of subcutaneous APO-go® has undergone continuous improvement and every development has been made based on practical feedback, patient advocacy to meet the evolving needs of people with Parkinson’s and their families. These improvements aim to simplify the set-up procedure, reduce the number of steps (from 12 steps to 8) and overall set-up time, and make the whole process more convenient for patients. Apomorphine medication was previously contained in prefilled syringes (PFS) which required liquid transfer and were therefore associated with a risk of spillage. The innovative APO-go® POD system, which attaches directly to the CRONO® PAR4 20 pump and has fewer components, was introduced in the UK in 2023, and streamlines that set-up process with a stepwise ‘prepare, attach, infuse’ procedure (Figure 1).
Conclusions: Historically, drug delivery innovation has been driven by technological advancements but in recent years, as in the case of APO-go®, the focus had shifted to improvements that address specific patient needs. If the treatment experience is simple and straightforward, this is likely to encourage treatment compliance and patient empowerment, giving them a feeling of control over their own health.
References
Stibe CM, et al. Lancet. 1988;1(8582):403-6. Jenner P, Katzenschlager R. Parkinsonism Relat Disord. 2016;33 Suppl 1:S13-S21. Katzenschlager R, et al. Lancet Neurol. 2018;17(9):749-59. Katzenschlager R, et al. Parkinsonism Relat Disord. 2021;83:79-85
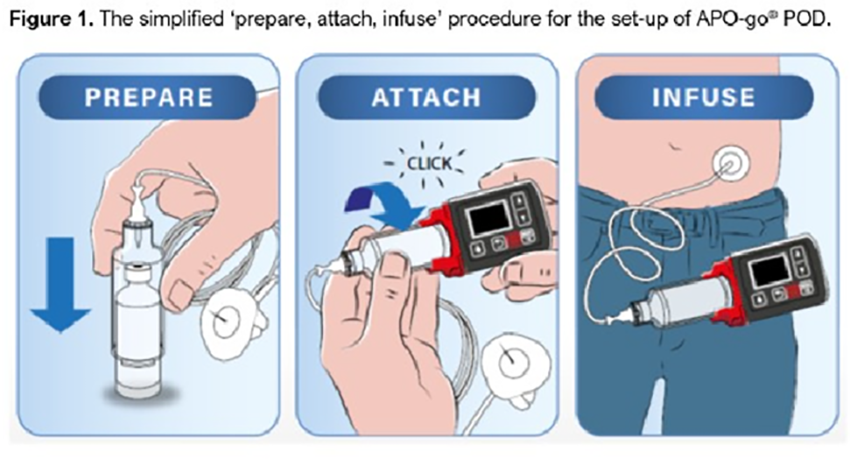
P35.08
1 USF Parkinson's Disease and Movement Disorders Center, United States
2 Parkinson's Disease and Movement Disorders Center of Boca Raton, United States
3 Icahn School of Medicine at Mount Sinai, United States
4 Texas Movement Disorder Specialists, United States
5 Amneal Pharmaceuticals, United States
OBJECTIVE: Evaluate interim outcomes from the real-world study of CREXONT, assessing its impact to extend “Good On” time and reduce “Off” time in PD patients after switching from other levodopa-based therapies.
BACKGROUND:
CREXONT, a novel extended-release carbidopa-levodopa formulation containing a mucoadhesive polymer, is designed to improve levodopa delivery and absorption, enhancing therapeutic benefit. ELEVATE-PD evaluates its safety and efficacy under real-world conditions.
DESIGN/METHODS: ELEVATE-PD is an ongoing multicenter, open-label phase 4 trial. After screening, patients are converted from their current therapy (IR CD-LD, IR + COMT inhibitors, or Rytary) to CREXONT and undergo a 5-week dose-optimization period (Visit 1–Day 35), followed by a 1-week stable dosing period (Day 35–42) and a 12-month follow-up. Eligible participants are required to have ≥2.5 hours of daily “Off” time. The primary endpoint is change in daily “Good On” time from baseline (Visit 1) to Day 42/Visit 4, assessed by the PD diary; the secondary endpoint is the change in daily “Off” time. This interim analysis includes the first 55 patients completing Week 6 (Day 42/Visit 4).
RESULTS: Fifty-five patients (mean age 66.4±8.95 years) were analyzed. At baseline, mean daily “Good On” time was 9.58±2.36 hours, “Off” time was 5.94±2.02 hours:
CREXONT treatment increased daily “Good On” time: +3.13 hours for patients switching from IR CD-LD (n=36), +2.31 hours from IR CD-LD+COMT inhibitor (n=6), +1.80 hours from Rytary (n=11). Corresponding reductions in “Off” time were –2.82, –2.36, –2.47 hours, respectively. CREXONT increased “Good On” time per dose by 1.81, 0.77, 0.78 hours, respectively. CREXONT also improved MDS-UPDRS total scores: –14.1, –4.2, –10.8 points, respectively. TEAEs were mild to moderate; most common (≥3%) were nausea (5.5%), falls (3.6%), dizziness (3.6%), urinary tract infection (3.6%).
CONCLUSIONS: CREXONT substantially increased “Good On” time, reduced “Off” time, and improved motor function in PD patients across all therapy groups, confirming that switching patients from other levodopa-based therapies to CREXONT offers meaningful improvements in symptom control through the day.
P35.09
1 UT Health San Antonio, United States
2 Amneal Pharmaceuticals, United States
3 USF Parkinson's Disease and Movement Disorders Center, United States
Objective: To assess the potential benefits of CREXONT® (IPX203) on sleep quality and nighttime motor states in Parkinson’s disease (PD) patients with sleep disturbances.
Background: Sleep disturbances affect up to 80% of individuals with PD and are among the most disabling non-motor symptoms. CREXONT is a novel extended-release CD-LD formulation. In RISE-PD, CREXONT significantly increased “Good On” time per day and per dose vs IR CD-LD.
Method: RISE-PD was a 20-week phase 3 study with a 3-week open-label IR CD-LD dose-optimization period, 4-week open-label dose-conversion to CREXONT, and a 13-week randomized, double-blind maintenance phase with two arms: IR CD-LD and CREXONT. The current analysis included patients with clinically relevant sleep disturbances at study entry (PDSS-2 total score ≥18). Outcome measures were changes in PDSS-2 total and subscale scores, and nighttime and early morning ‘Off’ per Hauser diary data.
Results: In the prespecified subgroup of patients with clinically relevant sleep disturbances (n=199), total PDSS-2 scores significantly improved during the open-label period (mean change = –6.99, p<0.001). Domain-specific analyses showed significant improvements: Disturbed Sleep Score improved from 11.94 ± 0.23 to 9.06 ± 0.28 (–2.88, p<0.001); Motor Symptoms at Night Score from 7.73 ± 0.24 to 5.56 ± 0.25 (–2.17, p<0.001); and PD Symptoms at Night Score from 6.62 ± 0.24 to 4.69 ± 0.22 (–1.93, p<0.001). Compared with study entry (V1), CREXONT treatment reduced nighttime “Off”: 2.5% reported none at V1, 4.5% at V2, and 18.6% by the end of CREXONT dose conversion. Early morning motor function also improved: 6.5% reported never experiencing early morning “Off” at V1, rising to 8% at V2 and 20.1% after CREXONT conversion.
Conclusion: These findings suggest that in PD patients with clinically relevant sleep disturbances, IR CD-LD optimization followed by conversion to CREXONT improves patient-reported sleep quality. CREXONT may also enhance nighttime and early morning motor control.
P35.10
1 Loma Linda University School of Medicine, Department of Neurology, United States
2 University of Cincinnati Gardner Neuroscience Institute, Gardner Family Center for Parkinson’s Disease and Movement Disorders, Department of Neurology, United States
3 Acadia Pharmaceuticals, Inc, United States
Objective: To examine the different response trajectories of patients with Parkinson’s disease psychosis (PDP) treated with pimavanserin who share similar patient profiles in baseline characteristics.
Background: Patients with PDP exhibit great variability in clinical presentation and treatment response, complicating treatment strategies. Understanding this heterogeneity and evaluating response patterns may help to individualize and personalize patient care.
Methods: Pooled data from 2 phase 3, randomized controlled trials in North America of pimavanserin in PDP underwent input-cluster analysis based on sex, age group, race, Mini-Mental State Examination (MMSE) category, duration of psychosis, and tremor presence. Outcome variables at week 6 included categorized responses on the Clinical Global Impression–Improvement (CGI-I; 1=very much improved, 7=very much worse) and the Scale for the Assessment of Positive Symptoms in Parkinson’s Disease (SAPS-PD; ≥30% reduction=responder, ≥10% to <30%=minimal response, ≥0% to <10%=no change, ≥−30% to <0%=worsening, and <−30%=relapse).
Results: Among 148 patients in the safety population, 134 had CGI-I data and 134 had SAPS-PD data at week 6. The 5 most commonly identified clusters based on 6 major input variables, including tremor status, ranged from 6 to 23 patients. Of these, the largest group (age 65-75 years, White, male, MMSE ≥25, disease duration ≥12 months, and tremor present) contained 23 (17.16%) patients distributed across 6 of the 7 outcome clusters for CGI-I and all 5 possible outcome clusters for SAPS-PD. Categorized responses “very much improved” and “much improved” on the CGI-I and “responder” on the SAPS-PD were dispersed across nearly all cluster inputs.
Conclusions: Although many patients from each of the 5 most common input clusters appeared in the improvement/response output clusters, overall, individual clinical outcome trajectories varied. Patients with similar baseline profiles may follow very different response trajectories, further highlighting the heterogeneity in PDP and underscoring the need for more personalized, patient-centered care.
This abstract will have been previously presented at the American Academy of Neurology (AAN) 2026 Annual Meeting, April 18-22, 2026; Chicago, Illinois.
P35.11
1 Southwest National Primate Research Center, United States
2 NEONEURON LLC, United States
Parkinson’s disease (PD) is a complex multisystem, chronic and so far incurable disease with significant unmet medical needs. Since its discovery in the 1961 levodopa remains the gold standard pharmacotherapy for PD. However, the progressive nature of the neurodegenerative process in and beyond the nigrostriatal system causes a multitude of side effects, including levodopa-induced dyskinesia (LID) within 5 years of therapy. The goal of this study is to screen a novel series of anti-dyskinetic compounds highly selective for the dopamine D3 receptor (D3R). We initially conducted a docking simulation to identify highly selective compounds for the D3R. Selected compounds were tested in the in vitro competitive D3R and D2R radioligand binding assays, in microsomes stability assay, in vitro ADME/T and in vivo pharmacokinetic. The in vivo pharmacology was evaluated in the marmoset model of PD expressing LIDs. We have identified a novel D3 receptor ligand that fully treated motor symptoms and reduced dyskinesias by 80% in the nonhuman NHP model of Parkinson’s disease exhibiting LIDs in response to levodopa treatment. The lead compound PD13R is G protein-biased partial agonist highly selective to D3R over the other dopamine receptors (D1R, D2R, D4R and D5R), orally active with desirable drug-like properties, including potency, selectivity and bioavailability. This study suggests that D3R is a promising target for treating dyskinesias and that the arylpiperazine class of pharmacophore is a favorable class of antidyskinetic ligands. Future studies are aimed at developing this lead compound for treating PD patients with dyskinesia.
P35.12
1 University of Texas Health Science Center at Houston, United States
2 University of Texas Health Science Center at Houston, United Arab Emirates
Background: Mesenchymal stem cells (MSCs) have neuroprotective and immunomodulatory properties, offering potential therapeutic benefit in Parkinson’s disease (PD). Clinical and immunological safety data of intravenous (IV) allogeneic bone marrow-derived mesenchymal stem cells (allo-hMSCs) are limited. We evaluated adverse event (AE) profiles and HLA sensitization outcomes following IV allo-hMSCs administration in phase I and phase II clinical trials.
Methods: Patients with mild to moderate PD, aged 45-79, OFF-state Hoehn and Yahr stage <4, and 4-10 year disease duration were enrolled. Phase I (n=20) tested single escalating IV infusions of 1, 3, 6, or 10 x 106 MSCs/kg. Phase II (n = 30) administered either 3 infusions of 10 x 106 MSCs/kg or 1 placebo, then 2 MSC infusions every 18 weeks. No pre-treatment was used. AEs, HLA profiles, and calculated panel reactive antibody (cPRA) were recorded at specified intervals. Mean Fluorescent Intensity threshold was set at 1000, and sensitization values (cPRA) was categorized as low (< 20%), moderate (20-79%) or high (>80%).
Results: Across both trials, 50 patients received allo-hMSCs, and 215 AEs were reported. Ten (4.7%) were treatment-related, with 8 being mild (80%), 1 moderate (10%), and 1 severe (10%). Common AEs included dyskinesia (30%), nausea (20%) and lymphocytic changes (20%). The severe AE was a new diagnosis of chronic lymphocytic leukemia in a patient with preexisting stable lymphocytosis, with counts remaining stable thereafter. AE profiles were consistent across trials, and infusions were well tolerated.
At 1-year post-infusion, 28 patients (56%) had stable or reduced cPRA values. Transient increases occurred in 8 (16%), and sustained increases with new HLA specificities in 6 (12%), all in phase II. One patient developed new high sensitization, and 8 (16%) developed new HLA specificities without cPRA change. Sensitization patterns showed a nonsignificant trend towards more sustained increases in Phase II vs. Phase I (p = 0.09). No donor specific antibodies were detected, and most patients stayed in the low category.
Conclusion: Single and repeated IV MSC infusions were safe and well tolerated in PD. Repeated dosing was associated with higher rates of sustained sensitization, yet most patients maintained low cPRA levels, suggesting minimal risk of clinically significant alloimmunity. Larger, longer-term trials are needed to fully determine the safety profile and immunologic impact of MSCs in PD.
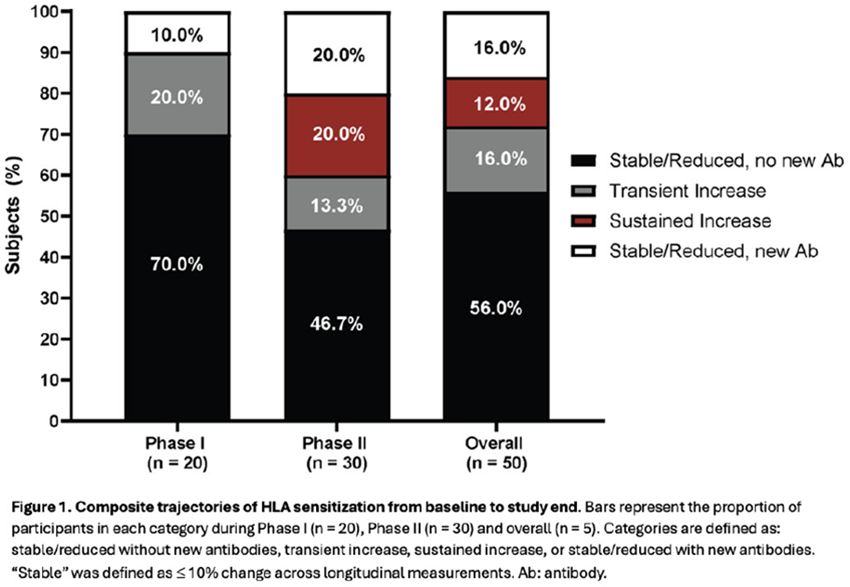
P35.13
1 Britannia Pharmaceuticals Ltd, United Kingdom
2 Centrafarm, Breda, Netherlands
3 Eurocept Homecare, Houten, Netherlands
4 Parkinson's Europe, United Kingdom
Introduction: For over 30 years, subcutaneously administered apomorphine has been used to treat motor fluctuations in people with Parkinson’s disease (PD), particularly when oral medications have failed to provide adequate relief of PD motor symptoms. APO-go® infusion has traditionally been administered using a portable pump system with the apomorphine solution provided in prefilled syringes (PFS). Until late 2024, PFS remained the only option to use with the Crono APO III pump. While effective, this system required significant preparation time and effort for the patient, comprised multiple components, and produced considerable medical waste. Recognising these challenges, a new delivery system, APO-go® POD, was developed which has pre-filled cartridges to simplify the set-up process and improve the user experience.
Methods: To evaluate the transition from PFS to POD in clinical practice, a survey was conducted in The Netherlands among 108 patients and caregivers enrolled in the APO-go® patient support programme. Participants were contacted in January 2025 or 1 month after switching to the POD system and 42 respondents provided feedback anonymously.
Results: Survey respondents highlighted significant improvements with the POD system versus PFS (Figure 1). Users reported reduced preparation time and effort, as well as fewer components needed for setup, making the process more straightforward. These changes were particularly important for older patients and long-term users, given the cohort’s demographic profile: most participants were >70 years of age had been living with PD for >10–15 years. They had used APO-go® for over two years, with some having over a decade of experience with the therapy. Respondents also noted the environmental benefits of reduced medical waste with the pre-filled cartridges. Almost unanimously, users expressed satisfaction with the new POD delivery system, indicating a significant improvement over the PFS method.
Conclusions: The results of this survey reinforce the importance of patient-centric innovation in PD and demonstrate the value of improving therapies in order to reduce treatment complexity, improve convenience, and align with the needs of people with Parkinson’s. The transition represents a successful example of how real-world patient insights can guide meaningful advancements in healthcare and enhance the quality of life for people living with chronic diseases, such as PD.
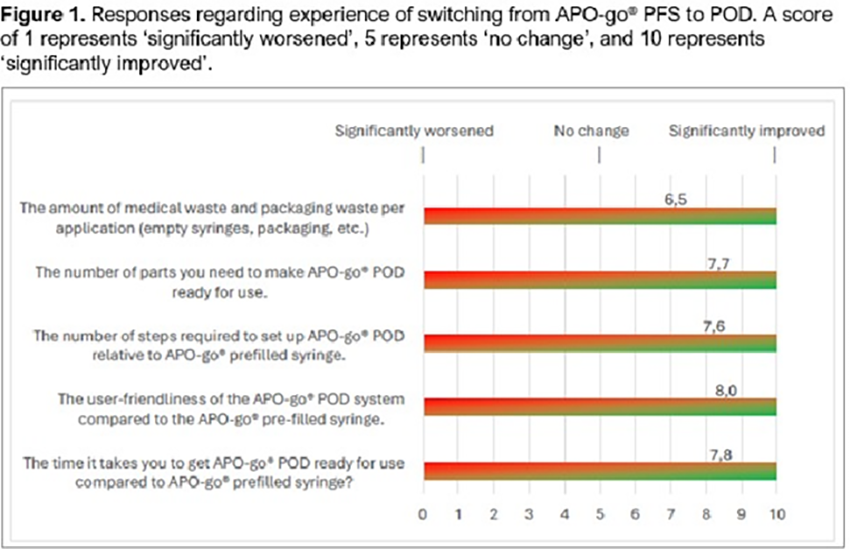
P35.14
1 Britannia Pharmaceuticals, United Kingdom
2 Britannia Pharmaceuticals Ltd, United Kingdom
Introduction: The availability of LECIG infusion since 2018 has expanded the options for device-aided therapy for people with advanced Parkinson’s disease (PD). As the formulation incorporates entacapone within the infusion, a lower levodopa dose in a smaller volume to be given while still maintaining therapeutically effective plasma levels (1). This has practical advantages as the medication can be delivered via small, lightweight pump. When determining the health impact of a treatment, the patient’s perspective may sometimes be overlooked in favour of the clinician’s expert perspective. Here we report data regarding both clinicians’ and patients’ views of the level of improvement in PD achieved following up to one year of treatment with LECIG by analysis of the interim dataset from the ELEGANCE study (NCT05043103). The aim was to determine the patients’ experience of treatment effect and evaluate if this correlated with that of the clinicians.
Methods: ELEGANCE study participants are advanced PD patients with severe motor fluctuations and hyperkinesia or dyskinesia despite optimised PD therapy who have been prescribed LECIG as part of routine clinical care. This interim analysis evaluated data for 167 patients with at least one post-baseline effectiveness observation. Clinical Global Impression of Improvement was rated separately by clinicians (CGI-I) and patients (PCI-I) from visit (V) 2 (3–6 months of treatment) onwards on a seven-point scale: ‘Compared to the patient's condition at baseline (prior to medication initiation), their condition is: 1=very much improved to 7=very much worse’. A score of 4.0 indicates no change.
Results: Taken separately, both CGI-I and PGI-I showed significant improvement at V2 (3–6 months of treatment) and V3 (6–12 months of treatment); p<0.0001 in each case for Wilcoxon’s signed rank test against a median score of 4. Taken together, CGI-I and PGI-I were significantly correlated. At V2, the Spearman Correlation Coefficient was 0.730 (p<0.0001) and at V3 was 0.628; p <0.0001 (Figure 1).
Conclusions: Reports from both clinicians and PD patients showed a significant correlation a with sustained favourable improvements in the patients’ disease following treatment with LECIG for up to one year compared with their baseline condition.
Reference 1. Senek M, et al. Mov Disord. 2017;32(2):283-6.
Disclosures: The ELEGANCE study is sponsored by Britannia Pharmaceuticals Ltd. VCG and BA are employees of Britannia Pharmaceuticals Ltd.
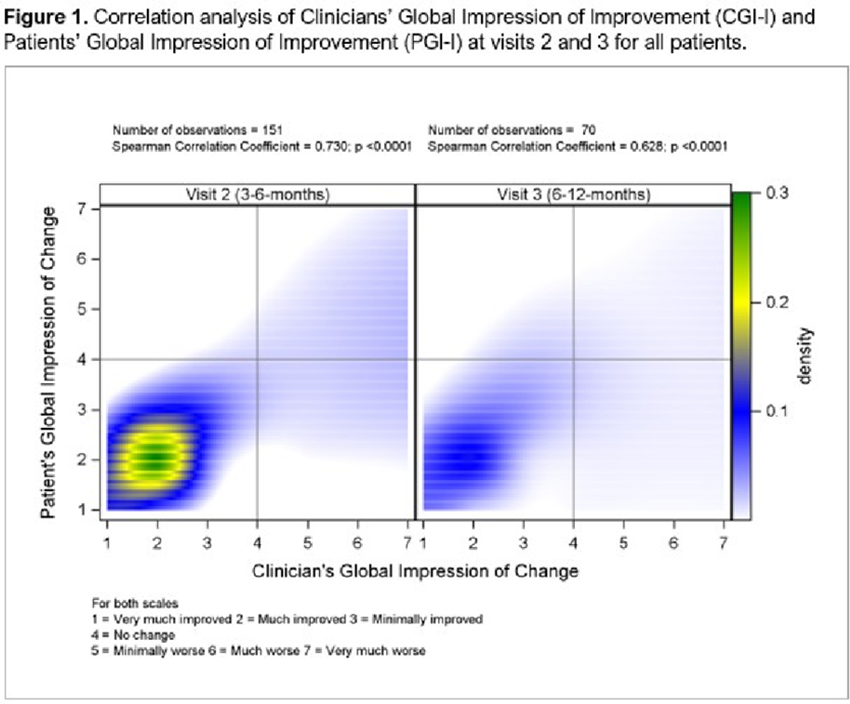
P35.15
1 Britannia Pharmaceuticals, United Kingdom
2 Britannia Pharmaceuticals Ltd, United Kingdom
3 Hospital Clínico San Carlos, Madrid, Spain
Introduction: For people with advanced Parkinson’s (PwAP), transitioning from their previous oral medication regimen, albeit generally requiring multiple drug doses daily, to a more invasive and technical device-aided therapy (DAT) option can be daunting with worries about the impact on their daily life. Levodopa–entacapone–carbidopa intestinal gel (LECIGON®, LECIG) was introduced in 2018 in Europe as a DAT option for PwAP and has been specifically designed with features that aim to improve their overall treatment experience.
Patient case history: Our case example is a 49-year-old woman, an economist by profession, with no relevant family history. She lives with her husband, has no children, and reports good social and family support. She was diagnosed with Parkinson’s several years earlier. In 2015, she started treatment with levodopa–carbidopa intestinal gel (LCIG) infusion after declining deep brain stimulation. Apomorphine infusion was not initiated due to the presence of an impulse control disorder.
Treatment outcomes: In December 2023, due to the development of severe dyskinesias and marked evening motor symptom worsening, the patient was switched from LCIG to LECIG. Previously, LCIG treatment had been administered for 16 h/day, with a morning dose of 10 ml, continuous doses of 3 ml/h on one pump and 2.7 ml/h on a second pump, and an extra dose of 2.8 ml as needed. After switching to LECIG, the regimen included a morning dose of 10 ml, a continuous dose of 1.9 ml/h, and an extra dose of 1.2 ml. After 6 months, the LECIG regimen was adjusted to a morning dose of 5.5 ml, continuous doses of 1.8 ml/h (flow rate [F]1), 1.7 ml/h (F2), and 1.6 ml/h (F3), with an extra dose of 1.2 ml.
Impact on daily activities: The patient uses three different flow rates on the Crono LECIG pump device according to her daily activities and needs. She reports that this flexibility has greatly improved her functional independence and adaptability throughout the day. Morning dystonia has resolved (after 15 hours of infusion), suggesting a longer effect of levodopa. She reports having experienced fewer dyskinesias, greater motor stability, and an overall improvement in her quality of life. Being a highly active person – she plays competitive table tennis and padel and also skis — she particularly values the smaller size and portability of the Crono LECIG pump, which has significantly enhanced her comfort and confidence.
P35.16
1 Britannia Pharmaceuticals, United Kingdom
2 Britannia Pharmaceuticals Ltd, United Kingdom
Introduction: The ELEGANCE study (NCT05043103) is an international, 24-month, non-interventional study that is capturing efficacy, safety and patient-reported outcomes data from advanced Parkinson’s disease (PD) patients treated with levodopa–entacapone–carbidopa intestinal gel (LECIG). Compared with standard levodopa–carbidopa intestinal gel (LCIG) infusion, LECIG infusion is delivered via a smaller, lighter pump and the presence of entacapone increases the bioavailability of levodopa such that lower doses can be given while still achieving the same effective plasma levodopa levels (1).
Methods: ELEGANCE study subjects are patients prescribed LECIG as part of their routine clinical care. Patients have a baseline assessment visit (V1) prior to starting LECIG treatment. From visit 2 (V2; after 3–6 months of treatment) onwards, patient-reported satisfaction with the treatment device is recorded: overall device satisfaction, handling, weight, size and noise, scored on a visual analogue scale of 1 = absolutely dissatisfied to 10 = absolutely satisfied, as well as a total score for all five parameters (possible total score: 50).
Results: As of September 2024, 312 patients have been recruited to the study. This planned interim analysis includes 167 patients who have effectiveness data from at least one post-baseline visit. Patient-reported satisfaction with the LECIG infusion pump was high with mean (± SD) total scores of 41.85 ± 6.71 (n=156) at V2 and 43.00 ± 7.52 (n=11) at V5. Patients also showed high satisfaction scores for all individual attributes of the pump from V2 to V5 (Figure 1). Mean scores were >7/10 for each attribute with particularly high score for noise (means >9.5/10 at each timepoint).
Conclusions: Patient satisfaction with PD therapy is an important factor that may contribute to treatment continuation. This analysis demonstrated patients were satisfied with the small, quiet and lightweight LECIG pump, and high satisfaction scores were sustained for up to two years.
Reference 1. Senek M, et al. Mov Disord. 2017;32(2):283-6.
Disclosures: The ELEGANCE study is sponsored by Britannia Pharmaceuticals Ltd. VCG and BA are employees of Britannia Pharmaceuticals Ltd. Data presented previously at the 30th World Congress of the International Association Parkinson’s Disease and Related Disorders (IAPRD), New York, USA, 07–10 May 2025.
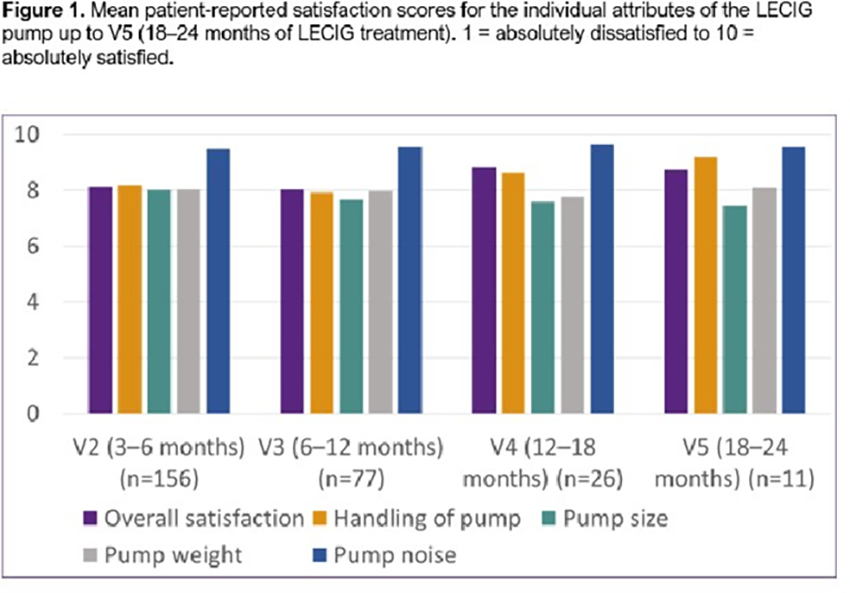
P35.17
1 Britannia Pharmaceuticals, United Kingdom
2 Britannia Pharmaceuticals Ltd, United Kingdom
Introduction: Levodopa and other oral therapies can effectively control the motor symptoms of Parkinson’s initially, but once it has progressed to the advanced stage, device-aided therapies (DATs) that allow continuous administration of medication are generally needed to maintain a good quality of life. For people with advanced Parkinson’s (PwAP), a range of continuous infusion options are available delivering medication subcutaneously or directly to the site of absorption in the intestine. Levodopa–entacapone–carbidopa intestinal gel (LECIGON®, d0dLECIG) was introduced in 2018 in Europe as a DAT option and was designed specifically to address feedback from PwAP and clinicians to improve convenience and usability. Previously, the only intrajejunal DAT available was levodopa–carbidopa intestinal gel (LCIG) which is delivered via a larger, heavier pump.
The rationale for LECIG: LECIG has been developed as a trigel comprising levodopa, carbidopa and entacapone in a single formulation. The inclusion of entacapone in the formulation extends the clinical benefits seen with LCIG allowing the administration of a reduced levodopa dose to achieve the same levodopa exposure, while also reducing levels of potentially harmful levodopa metabolites. This lower levodopa can be delivered using a smaller pump (the Crono® LECIG pump: weight with full cartridge/syringe: 227 g versus 550 g for the LCIG pump; size: 150 × 55 mm versus 197 × 100 mm for the LCIG pump) (Figure 1). This is also quieter than the LCIG pump, and reported to be preferred by users. The pump has three programmable flow rates that can be personalised to meet individual patient needs. LECIG treatment can therefore help simplify the treatment regimen, eliminating the need to take oral entacapone tablets. In addition, the simple set-up process requires no liquid transfer making it easier for PwAP and their carers.
Benefits for PwAP: In addition to providing effective control of motor symptoms,2 LECIG offers a flexible and straightforward DAT option for PwAP, that can be adapted based on their individual lifestyle. Using a reduced levodopa dose delivered with a smaller pump is designed to optimise the convenience, compliance and safety of the user. It enables PwAP to maintain an active and independent lifestyle, especially benefiting those who are frail, have limited strength, or low body weight. The pump is designed to be quiet and discreet, so is easy to wear in social situations and for daily activities.
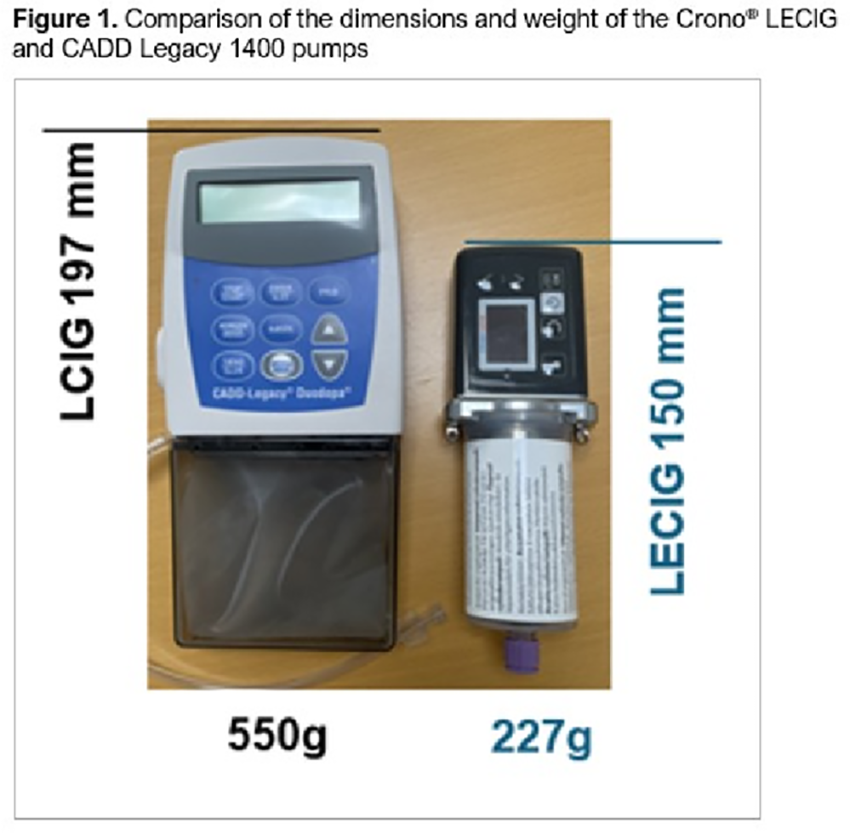
P35.18
1 Britannia Pharmaceuticals, United Kingdom
2 Britannia Pharmaceuticals Ltd, United Kingdom
3 Nordic Infucare AB, Bromma, Sweden
4 Movement Disorder and Pain Research Center, Neurological Department, Rigshospitalet, Copenhagen, Denmark
Introduction: Levodopa–entacapone–carbidopa intestinal gel infusion (LECIGON®; LECIG) is a device-aided therapy that has been shown to be effective and well tolerated for the management of advanced Parkinson’s disease (PD) (1,2). LECIG gel is infused into the duodenum – the site of absorption of levodopa – via a PEG-J system comprising percutaneous endoscopic gastrostomy (PEG; gastric port) and a jejunal intestinal tube (J) using a portable Crono® LECIG pump (Figure 1a).
Development of the Klem ring: The PEG-J system requires regular maintenance by the user who should disconnect it from the pump and flush it with cooled, boiled drinking water each evening to clean it. However, there have been reports that flushing too hard may cause disconnection the internal jejunal intestinal tube from the click adaptor; the intestinal tube then passes through the gastrointestinal system and out of the patient and has to be refitted in hospital. This also means that, without the jejunal tube in place, LECIG medication will be delivered into the stomach rather than into the jejunum which may impact absorption and clinical efficacy. Based on feedback from clinicians and patients, the PEG-J system has been improved to replace the original ‘soft’ Klem ring system (white cylinder in Figure 1b) with a harder silicone Klem ring that requires a much higher release force resulting in better attachment to the click adapter. Patients are also provided with a ‘white tightener help tool’ to make sure the attachment is secure. Experience from Sweden and Denmark of people with Parkinson’s treated with LECIG who have transitioned to using the new Klem ring have been positive with no occlusion issues.
Conclusions: By listening to clinician and patient feedback and making small design changes to components of the PEG-J system the overall treatment experience for LECIG-treated PD patients has improved. The inconvenience and additional time in hospital due to jejunal tube dislocations has reduced.
References: (1) Weiss D, et al. Mov Disord Clin Pract. 2025;12(8):1075-1085; (2) Poplawska-Domaszewicz K, et al. Expert Rev Med Devices. 2025;22(6):533-544.
Disclosures: VCG and BA are employees of Britannia Pharmaceuticals Ltd. DL is an employee of Nordic Infucare.
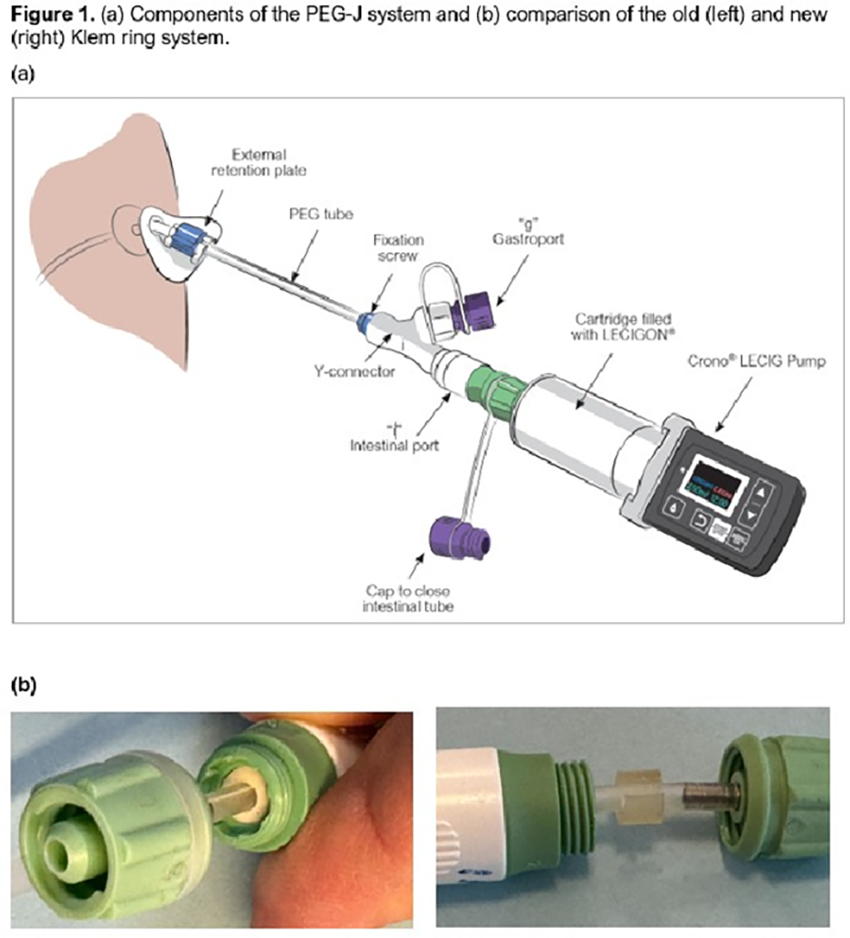
P35.19
1 Iowa State University, United States
Background: Gait impairment is a prominent and debilitating motor symptom of Parkinson’s disease (PD). Gait symptoms manifest as changes in stride length, cadence, arm swing, turning, and the duration of gate cycle phases. Persons with PD also tend to exhibit greater stride-to-stride variability. The common drug combination carbidopa-levodopa does not fully ameliorate all gait symptoms. Gait can be evaluated using wearable inertial measurement unit (IMU) sensors, which are reliable, sensitive, and user-friendly. IMUs are valid in extended overground walking tests, including the six-minute walk test (6MWT). This study aimed to evaluate the effects of carbidopa-levodopa on gait and variability by comparing gait performance in healthy older adults (HOAs) and persons with PD ON and OFF medication.
Methods: Eight HOAs and 15 participants with PD completed the 6MWT while instrumented with five IMUs. Participants were instructed to walk as far as possible in six minutes, using a 15 m walkway. Participants with PD completed the paradigm twice—once after 12-hour withdrawal from antiparkinsonian medication and again after taking 1.5 times their normal dose of carbidopa-levodopa only. Gait and variability outcome measures were computed from IMUs and separate linear mixed models were run for each outcome measure to compare differences across groups and medication status. An Index of Normalization (IN) was used to quantify the extent to which medication normalized outcome measures toward HOA values.
Results: The IN varied considerably across gait outcome measures. Arm swing, turning, and gait speed tended to be most normalized by medication. Contrast tests revealed significant differences between ON and OFF medication states for gait speed, stride length, and arm swing range of motion on the more effected side (α <.05). Cadence and duration of gait cycle phases were least normalized. Gait variability outcome measures normalized modestly but did not reach significance. Cadence variability and double support duration variability became further from that of HOAs following medication administration.
Conclusions: The normalizing effects of carbidopa-levodopa varied across gait outcome measures during an extended overground walking test. Additional investigation and intervention are warranted to identify and mitigate the mechanisms of gait impairment in PD.

P35.20
1 Cellestial Health Ltd; University of Cambridge, United Kingdom
2 University of Cambridge, United Kingdom
3 University of Cambridge; ALBORADA Drug Discovery Institute, United Kingdom
4 University of Cambridge; Eindhoven University of Technology, United Kingdom
5 University of Manchester, United Kingdom
6 Sciomics GmbH, Germany
7 Atuka Inc, Canada
Existing drug treatments of Parkinson’s disease (PD) mask motor symptoms caused by dopaminergic neurone loss but do not stop its progression as the molecular and cellular causes of PD are not fully understood. This calls for a deeper investigation of PD aetiologies. In particular, research into cell types beyond dopaminergic neurones is gaining prominence.
Astrocytes represent around 25-70% of brain cells, depending on the brain region, which control essential brain functions relevant to PD symptoms. Our research showed that astrocytic networks can transmit signals independently of neurones and that these networks become disrupted in human PD.
Connexin 43 (Cx43) is the main protein linking astrocytes in networks via channels called gap junctions (GJs). In PD, GJs close and decline, and Cx43 becomes re-directed to a “toxic” conformation called hemichannels (HCs) which abnormally open to the extracellular space.
Our work focussed on idiopathic PD which represents the largest unmet need (80%+ of cases). Aggregation of alpha-synuclein (a-syn) and inflammation are its prominent hallmarks. We utilised a number of models relevant to idiopathic PD to test whether the GJ deficit can be reversed with safe small molecule drugs.
We observed that Cx43 modulation that results in GJ protection and HC closure preserves astrocytic coupling, normalises calcium signalling, reduces astrocytic reactivity, and slows down a-syn aggregation in cell models of PD. Further, protective effects can be seen both in rodent and human cells, suggesting plausible clinical translatability. These effects are associated with changes in phosphorylation and acetylation of Cx43.
Next, we showed that a GJ-protecting drug can be delivered into the brain in rats where it exerts protective effects on GJs. This treatment reduces markers of inflammation in the brain and cerebrospinal fluid which correlates with the protection of the nigrostriatal system after a peripheral lipopolysaccharide challenge. Further, this treatment can reduce motor symptoms and a-syn aggregation in a rat PD model induced by a-syn-A53T overexpression.
Finally, we demonstrate that new GJ-protecting compounds can be generated for enhanced brain permeability and therefore more suitable for PD treatment.
In conclusion, our new results build on our previous work validating Cx43 as a disease-modifying target in PD and demonstrate feasibility of safely drugging this target using small molecule therapeutics with translational potential.
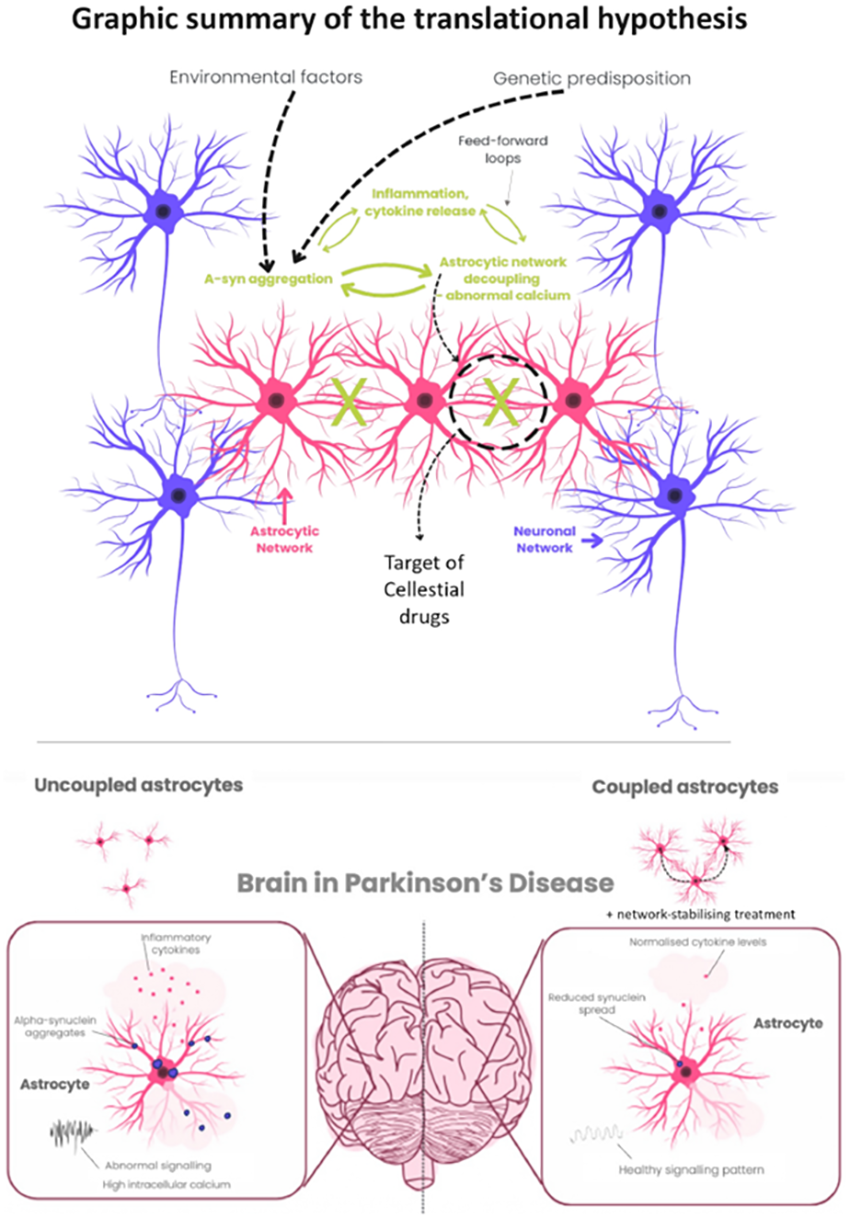
P35.21
1 MUSC, United States
Introduction Continuous subcutaneous infusion of foslevodopa–foscarbidopa (Fosl/Fosc) is a newly approved treatment for advanced Parkinson’s disease (PD). While Phase 3 trials have demonstrated its efficacy in reducing motor fluctuations, real-world data remain limited. This study presents early clinical experience with Fosl/Fosc during its first year of use at a university-based movement disorders center.
Methods We conducted a single-center retrospective chart review of PD patients evaluated for Fosl/Fosc therapy. Data collected included demographic characteristics, PD history, Hoehn & Yahr (H&Y) stage, MDS-UPDRS scores, concomitant PD medications, and clinical outcomes. Outcomes of interest were treatment initiation versus refusal, adherence and satisfaction among Fosl/Fosc users, changes in motor fluctuations, dyskinesias, gait instability, orthostatic symptoms, hallucinations, cognition, sleep, and infusion-site reactions.
Results Twenty-three patients met eligibility criteria for infusion therapy based on ≥3 hours of refractory “off” time per day. Of these, 18 initiated Fosl/Fosc and 5 declined. Among treated patients, 12 (66.7%) remained on therapy, and 6 (33.3%) discontinued. The mean age at initiation was 66 years, with an average disease duration of 8.5 years and mean H&Y stage of 2.3. All had baseline dyskinesias prior to initiation. Active users reported marked reductions in dyskinesia intensity, gait instability, and “off” time compared with those remaining on oral therapy. Improvements in mobility, hallucinations, sleep quality, and cognition were also more commonly reported among active users. Patients declining therapy typically had milder baseline symptoms or preferred oral treatment, whereas discontinuations were primarily related to device fatigue or infusion-site reactions (burning and nodule formation).
Conclusions Early real-world experience with subcutaneous Fosl/Fosc infusion demonstrates clinically meaningful reductions in “off” time and dyskinesia severity among moderate-stage PD patients initiating therapy. Those who opted for infusion generally had more advanced disease than those remaining on oral regimens. Beyond motor benefits, users experienced multidomain improvements in nonmotor symptoms, supporting Fosl/Fosc as a well-tolerated and effective option for continuous dopaminergic delivery in PD. Strategies to minimize infusion-site reactions may further enhance long-term adherence and treatment satisfaction.
P35.22
1 Vanda Pharmaceuticals Inc., United States
2 Laboratory of Cellular and Molecular Neurobiology, Hellenic Pasteur Institute, Greece
First delineated by Dr. Polymeropoulos et al. (1997), the p.A53T mutation in SNCA has been identified as a significant risk factor for early-onset Parkinson’s disease (PD). We propose an antisense oligonucleotide (ASO)-based allele-specific strategy to target the mutant p.A53T allele, without downregulating the wild-type (WT) allele. This allele-specificity ensures that healthy levels of α-synuclein are maintained by the WT allele.
We designed an ASO that selectively targets the mutant SNCA A53T allele. This ASO was designed to have a higher affinity for the mutant allele predicted in silico. HEL cells were incubated for 72-hours with the A53T-specific ASO using gymnotic uptake for qPCR and RNA-seq.
hiPSCs derived from patients harboring the SNCA A53T allele underwent directed differentiation to create a mixed neuronal model that displays PD-relevant phenotypes, including defective synaptic connectivity and α-synuclein aggregation. ASOs were dosed at 0.2-1 µM for two weeks.
ASO treatment resulted in a 40% reduction of SNCA expression in HEL cell lines. This knockdown with qPCR is consistent with RNA-seq data. Limited off-target effects were demonstrated in silico.
ASO treatment in the hiPSC-derived neuronal model revealed a notable effect on neuronal outgrowth, restoring the neuronal network and improving viability 5 days after administration. Levels of phosphorylated α-synuclein also diminished following ASO treatment. Network metrics analysis demonstrated that ASO treatment significantly improved neurite branching to comparable levels of healthy neuronal controls (p<0.0001). Additionally, measurements of synaptic connectivity show significantly increased connectivity of neurons (p=0.006).
It has been demonstrated that using CRISPR-Cas9 to delete the A53T SNCA mutation improved PD-related conditions, including α-syn overproduction, dopaminergic neurodegeneration, and motor symptoms. Achieving a ratio in favor of mutant allele downregulation is desirable as it preserves the WT allele while targeting the aberrant gain-of-function allele, a phenomenon that is not possible with other lines of treatment.
We present a novel ASO that achieves this goal in vitro, with promising results of synaptic function and neuronal health restoration. Given the high prevalence of PD, a treatment that works by directly targeting an underlying molecular cause of PD holds significant potential to significantly improve PD patients’ disease manifestation and quality of life.
P35.23
1 Vanqua Bio, United States
2 Centre for Human Drug Research (CHDR), Netherlands
3 University of British Columbia, Canada
Objective: To evaluate the safety, pharmacokinetics (PK), and pharmacodynamics of VQ-101 in patients with Parkinson’s disease (PD) with and without a GBA1 mutation.
Background: Reduced lysosomal glucocerebrosidase (GCase) activity caused by mutations in the GBA1 gene is a major risk factor for the development of PD. Reduced GCase activity results in an increase in plasma levels of the sphingolipid glucosylsphingosine. VQ-101 is a fully CNS-penetrant allosteric activator of lysosomal GCase under investigation for the treatment of PD. Preclinically, in GBA PD-patient-derived dopaminergic neurons, >50% activation of GCase by VQ-101 was shown to significantly block misfolded alpha synuclein accumulation.
Methods: VQ-101 was evaluated in a 28-day, double blind, placebo-controlled trial, followed by 2 months of open label at doses of 150 mg and 300 mg in patients with PD with and without a GBA1 mutation. GCase activation by VQ-101 was assessed using an analytically validated lysosomal GCase activity assay at the start of dosing and at several time points during the study. Plasma and CSF samples were collected for exploratory analyses, including analysis of glucosylsphingosine.
Results: VQ-101 demonstrated a favorable safety profile, full CNS penetrance, and a PK profile supporting once daily dosing in patients with PD. A significant increase in lysosomal GCase activity was observed, with sustained activation greater than 70% at both 150 and 300 mg doses. Sustained activation of GCase by VQ-101 led to a significant reduction in plasma glucosylsphingosine levels highlighting robust pathway engagement for this molecule. Additional analyses of pathway engagement are ongoing.
Conclusions: In patients with PD with and without a GBA1 mutation, VQ-101 demonstrated favorable tolerability, full CNS penetrance, sustained target engagement, and significant pathway engagement. This is the first demonstration of combined target and pathway engagement for a GCase-targeted therapeutic in patients with PD.
CLINICAL SCIENCES: Surgical therapy, including cell and gene therapy
P36.01
1 Asan Medical Center, South Korea
Objective: To investigate the impact of deep brain stimulation (DBS) on quality of life (QoL), depressive symptoms, and lived experiences among women with Parkinson’s disease (PD) following DBS surgery.
Background: DBS is an established therapy for advanced PD. However, little is known about its effects on QoL and psychosocial outcomes specifically in female patients with PD.
Methods: This mixed-methods case study included 12 women with PD who underwent DBS between December 2019 and April 2020. Clinical outcomes were assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS), Beck Depression Inventory (BDI), and the 39-item Parkinson’s Disease Questionnaire (PDQ-39). In-depth interviews were analyzed to capture patient-reported experiences.
Results: Motor function significantly improved after DBS, as reflected by reduced UPDRS Part III scores (39.3 ± 10.4 vs. 25.0 ± 16.8; p = 0.038). However, BDI and PDQ-39 scores showed no significant changes postoperatively (0.45 < p < 0.70). Qualitative analysis revealed sources of dissatisfaction, including stress from perceived external changes, pain at the implantation site, waning stimulation effects, financial burden of battery replacement, and anxiety related to device malfunction.
Conclusions: While DBS improved motor symptoms, its impact on QoL and mood was limited in this cohort of women with PD. These findings highlight unique challenges and concerns faced by female patients, underscoring the need for tailored clinical care and psychosocial support to address gender-specific issues in DBS treatment.
P36.02
1 St. George's University of London, United Kingdom
2 Julius-Maximilians University Hospital Wuerzburg, Germany
3 Radboud University Medical Center, Netherlands
4 Academic Medical Centre (Amsterdam UMC), Netherlands
5 Uniklinik Koln, Germany
6 University Hospital Tubingen, Denmark
7 University Medical Center Freiburg, Germany
8 University of Oxford, United Kingdom
9 University Hospital Giessen and Marburg, Germany
10 Charite University Medicine, Germany
11 Boston Scientific, United States
Overview: This study explored how a new deep brain stimulation (DBS) system might improve movement and overall quality of life for people living with Parkinson’s disease. Unlike older systems, this one uses advanced leads with 16 tiny contact points that deliver stimulation to the brain. These extra contact points give doctors more control over where and how the stimulation is applied, which may help reduce side effects and improve symptom relief.
Why It Matters: Traditional DBS systems have helped many people with Parkinson’s, but they can sometimes cause unwanted effects or lose effectiveness over time. The new system is designed to be more precise and flexible, allowing doctors to fine-tune the stimulation to match each person’s unique needs. This could lead to better results and fewer complications.
What Was Done: So far, 49 people with Parkinson’s across 10 medical centers in Europe have received this new DBS system, called Vercise Genus, developed by Boston Scientific. After surgery, the system was activated and adjusted to help manage symptoms. Researchers then monitored changes in movement, medication use, and overall well-being over time.
What Was Found: After 12 weeks, participants showed a 41% improvement in movement symptoms. These improvements continued through the first and second year after treatment. Use of Parkinson’s medications dropped by 37% after six months and stayed lower through year two. People also reported feeling better in areas such as walking, daily activities, physical discomfort, and how they felt about their condition. Importantly, no unexpected safety issues were reported during the study.
Relevance to Parkinson’s Treatment: For patients considering DBS, this new system may offer better control of symptoms with fewer side effects and less dependence on medication. Because it allows for more personalized adjustments, it may provide more consistent relief and a better quality of life. Although the research is still ongoing, early results are encouraging and suggest that this technology could be a valuable option for people with Parkinson’s.
Next Steps: Researchers will continue to follow participants and share updates as more data becomes available.
P36.03
1 Selkirk Neurology, United States
2 University of Miami, United States
3 University of Florida Norman Fixel Institute for Neurological Diseases, United States
4 The University of Tennessee Medical Center, United States
5 Boston Scientific, United States
Study Overview: This study looked at a new tool designed to help quickly and accurately adjust deep brain stimulation (DBS) settings in Parkinson’s disease patients. DBS is a treatment that uses electrical signals to improve movement symptoms, but finding optimal settings can take time and may involve trial and error. The newly developed tool, called automated image-guided programming (alGP), uses brain images to tailor stimulation settings to the anatomy of each patient. These suggestions are generated within seconds and aim to target the right areas while avoiding unwanted side effects.
Why It Matters: Traditionally, DBS programming requires multiple clinic visits and careful adjustments by a specialist. This process can be tiring and frustrating for patients. The alGP tool is designed to make this easier by using advanced imaging and computer modeling to guide the programming process. It helps doctors position the stimulation field more precisely, which may lead to better symptom control and fewer side effects.
What Was Done: Fifteen people with Parkinson’s disease so far have participated in this study across multiple medical centers. Each person had Boston Scientific designed DBS systems implanted in both sides of the brain and was tested under two types of programming: the standard method and the new image-guided approach. Researchers looked at how well each method improved movement symptoms and tracked daily experiences using motor diaries.
What Was Found: The results showed that the alGP tool improved movement scores by 39% when patients were off medication and by 54% when they were on medication, compared to when DBS was turned off. These improvements were similar to those achieved with traditional programming. Over time, patients using the alGP-guided settings experienced about 25 more minutes of good movement (“ON” time) each day and about 58 fewer minutes of troublesome movements (“ON with dyskinesias”), although these differences weren’t statistically significant. Doctors made very few changes to the settings suggested by the tool, indicating that the recommendations were already close to optimal.
What It Means: This new technology may help doctors program DBS more efficiently and with greater precision. It could reduce the time and effort needed to find the best settings, making the experience smoother for patients and potentially improving outcomes.
Next Steps: Further data will be shared as the study continues.
P36.04
1 University of Florida Norman Fixel Institute for Neurological Diseases, United States
2 University of South Florida, United States
3 University of Texas, San Antonio, United States
4 Providence Spokane Inland Neurosurgery & Spine Center, United States
5 Selkirk Neurology, United States
6 University of North Carolina, Chapel Hill, United States
7 Ohio State University, United States
8 University of Miami School of Medicine, United States
9 Albany Medical Center, United States
10 University of Arizona School of Medicine, United States
11 Northwestern University School of Medicine, United States
12 Rush University Medical Center, United States
13 University of Colorado Anschutz Medical Campus, United States
14 Northwell Health, United States
15 Nassau University Medical Center, United States
16 Texas Institute for Neurological Disorders, United States
17 St. Luke's Regional Medical Center, United States
18 Wake Forest University, United States
19 Boston Scientific, United States
Study Overview: This study examined the experiences and outcomes of people with Parkinson’s disease who received a newer type of deep brain stimulation (DBS) system in everyday medical settings across the United States. These systems use directional leads and a technology called Multiple Independent Current Control (MICC), which allows for the fine-tuning of stimulation more precisely. The goal is to better target the areas of the brain that control movement while avoiding unwanted side effects.
Why It Matters: DBS has long been used to help reduce movement problems in Parkinson’s, and its benefits can last for many years. The newer directional systems offer more flexibility in programming, which may lead to better symptom control and fewer complications. By collecting data from everyday clinical practice this study helps show how these systems work for real patients in real settings.
What Was Done: So far, 196 people have joined the study, and 163 have had their DBS systems (Boston Scientific manufactured devices only) activated. The average age of participants is about 65, and most have lived with Parkinson’s for around nine years.
What Was Found: After six months of using the DBS system, patients showed a 51% improvement in movement symptoms, and these improvements continued at one and two years. People also reported feeling better in many areas of daily life, including walking, doing everyday tasks, physical comfort, emotional well-being, and how they felt about their condition. More than 90% of both patients and their doctors said the benefits were still noticeable after two years. Importantly, no unexpected safety issues were reported. The most serious complication was infection at the implant site, which occurred in about 1% of cases.
What It Means: This U.S.-based research shows that advanced DBS systems with directional control and MICC can lead to lasting improvements in movement and quality of life for people with Parkinson’s disease. These results match findings from similar studies in Europe and support the use of these technologies in everyday medical care.
Next Steps: Researchers are continuing to collect and analyze data as more people join the study.
P36.05
1 Boston Scientific Neuromodulation, United States
2 Boston Scientific, United States
Study Overview: This study explored how long rechargeable deep brain stimulation (DBS) devices can last between charges and over their full lifespan. These devices, known as implantable pulse generators (IPGs), are used to help manage movement symptoms in people with Parkinson’s disease. The latest models include a technology called Multiple Independent Current Control (MICC), which allows doctors to fine-tune stimulation more precisely. These systems are designed to last more than 15 years and may require fewer recharges over time.
Why It Matters: To better understand how long these devices can operate before needing a recharge or replacement, researchers tested two types of rechargeable IPGs (Vercise Genus R16 and R32, made by Boston Scientific) under controlled lab conditions. The devices were placed in a warm saline bath to mimic the environment inside the body and were paired with DBS leads, just as they would be in a patient. Each device was fully charged before testing, and researchers simulated weekly patient check-ins using remote controls.
What Was Done: Five different stimulation settings were tested, ranging from low to high intensity, including directional stimulation and settings used by other DBS systems. The goal was to see how long each device could deliver therapy before entering “hibernation,” which means the battery was fully depleted and therapy was paused.
What Was Found: Early results indicate that the latest rechargeable IPGs with MICC (Multiple Independent Current Control) technology last more than 50% longer than older models. This means you may enjoy longer periods between recharging, giving you more freedom to travel or go on vacation without needing to carry your charger. These findings are encouraging for those who use DBS to help manage their symptoms, as they suggest greater convenience and simplicity in your everyday life.
What It Means: In summary, this research helps provide a clearer picture of how long rechargeable DBS devices can last in real-world use. The improved battery performance seen in newer MICC-enabled systems may offer meaningful benefits for patients, including less frequent charging and longer-lasting therapy.
Next Steps: More data will be shared as the study continues.
P36.06
1 Department of Neurology, The Icahn School of Medicine at Mount Sinai, New York, NY, USA, United States
2 Department of Neurology, Weill Cornell Medicine, New York, NY, USA, United States
3 Department of Neurology, University of California, Irvine, CA, USA, United States
4 Division of Neurosurgery, University of Toronto, Toronto, Ontario, Canada; Krembil Brain Institute, Toronto, Ontario, Canada, Canada
5 Krembil Brain Institute, Toronto, Ontario, Canada; Division of Neurology, University of Toronto, Toronto, Ontario, Canada; Edmond J Safra Program in Parkinson’s Disease, Morton and Gloria Shulman Movement Disorders Clinic, Toronto Western Hospital, UHN, Toronto, Ontario, Canada, Canada
6 Department of Neurosurgery and Center for Stem Cell Biology, Memorial Sloan Kettering Cancer Center, New York, NY, USA, United States
7 BlueRock Therapeutics LP, Cambridge, MA, USA, United States
Introduction: Bemdaneprocel is an investigational cell therapy composed of human embryonic stem cell-derived midbrain dopaminergic neuron progenitors under development for the potential treatment of Parkinson’s disease (PD). In the Phase 1, open-label, exPDite study (NCT04802733), 12 participants received low-dose (n=5; 0.9 million cells/putamen) or high-dose (n=7; 2.7 million cells/putamen) bemdaneprocel bilaterally in the postcommissural putamen with 1-year immunosuppression. All participants enrolled in a continued-evaluation study for assessment through 5 years (NCT05897957). Across both cohorts through 3 years, most of the 112 treatment-emergent adverse were mild or moderate in severity; none of the 8 treatment-emergent serious adverse events were related to transplanted cells or immunosuppression. In the high-dose cohort, changes from baseline in patient-reported ON times without troublesome dyskinesia and OFF times, as well as MDS-UPDRS Part III ON and OFF scores, demonstrated maintained motor improvement through 3 years (Table). These results support further development of bemdaneprocel.
Methods: exPDite-2—a Phase 3, multicenter, randomized, sham surgery–controlled, double-blind trial (NCT06944522)—will evaluate the efficacy of bemdaneprocel on motor symptoms in participants with PD. Approximately 102 eligible participants with clinically established PD, ≥45 to ≤75 years of age, ≥4 and <12 years from PD diagnosis with ≥2.5 hours daily OFF time will be randomized to bemdaneprocel (3 million cells/putamen) or sham surgery followed by 12 months of immunosuppression (bemdaneprocel group) or placebo (sham group).
Results: The primary endpoint in exPDite-2 is change from baseline at Week 78 in adjusted PD diary ON time without troublesome dyskinesia. Secondary and exploratory endpoints include motor, non-motor, activities of daily living, quality of life, and safety outcomes. The first participant was randomized and underwent surgery in 2025.
Conclusion: The favorable safety profile overall and maintained motor improvements observed in the high-dose cohort through 3 years in exPDite support the continued development of bemdaneprocel; however, further studies are needed. exPDite-2 is the first large-scale, potentially registrational trial of stem cell–derived midbrain dopaminergic neuron progenitors for PD.

P36.07
1 Department of Neurosurgery, University of Colorado Anschutz Medical Campus, United States
2 Department of Neuroscience, University of Kentucky College of Medicine, United States
3 Department of Neuroscience, University of Kentucky College of Medicine; Department of Neurosurgery, University of Kentucky College of Medicine, United States
The brain has a limited regenerative capacity, which distinguishes it from the peripheral nervous system. Injury to a peripheral nerve triggers a repair response mediated by Schwann cells and other supportive cells dedicated to promoting nerve regrowth. Among the Schwann cell-mediated effects are the release of neurotrophic factors and recruitment of additional cell types to assist in the nerve repair.
To lend the regenerative capacity of the peripheral nervous system to the brain, an investigational approach has been introduced where peripheral nerve fascicles are transplanted from the participant’s own sural nerve (located on the lower leg) to the most affected side of the substantia nigra (SN) and combined with bilateral deep brain stimulation (DBS) surgery. An open-label Phase 1 clinical trial has demonstrated the safety and feasibility of this investigational intervention, which has been termed DBS-Plus.
In a current exploratory study, the morphology, gene expression and protein expression of the nerve fascicle grafts and the ipsi- and contralateral SN are being examined by analyzing tissue samples from participants who underwent the DBS-Plus intervention and who later died from unrelated causes. By combining microscopic morphological assessment, immunohistochemical analyses, three-dimensional visualization and transcriptomics, our aim is to determine the localization, survival and cellular composition of the grafts and their interaction with the surrounding brain tissue.
Our preliminary findings demonstrate graft survival within the SN, as well as vascularization and innervation of the graft by the surrounding brain parenchyma. Ongoing analyses will determine the detailed characteristics of the graft vascularization, the cellular composition of and potential immune reaction to the grafts, and the potential presence of neurotrophic factors expressed by the grafts. The long-term goal is to determine how these parameters affect the dopaminergic neurons of the SN, and thus the potential efficacy of this intervention paradigm.
This work was supported by the Ann Hanley Neuroscience Fund, the NIA (1R01AG081356), Pro's Players Fore Parkinson's, and the Tegger Foundation.
P36.08
1 Neurology Department, Melhem International Hospital, Baku, Azerbaijan, Azerbaijan
2 Functional Neurosurgery Unit, Melhem International Hospital, Baku, Azerbaijan, Azerbaijan
3 Isık University, Natural Sciences & Engineering Faculty, Biomedical Engineering Department Istanbul, Turkey, Turkiye
Deep Brain Stimulation (DBS) is a well-established therapeutic option for advanced Parkinson’s disease (PD). However, regional experience and outcome data from developing centers remain limited. This study presents the first Azerbaijani series of 50 PD patients implanted with directional, rechargeable DBS systems, documenting surgical performance, safety, and comparative results between subthalamic nucleus (STN) and globus pallidus internus (GPi) targets.
Methods: Between March 2023 and September 2025, 50 idiopathic PD patients underwent bilateral DBS implantation at Melhem International Hospital. All surgeries were performed using Elekta stereotactic frames with BrainLab Element software for image-guided trajectory planning.
· Targets: The first 12 patients received STN DBS, and the subsequent 38 patients underwent GPi DBS following multidisciplinary reassessment.
· System: All implants utilized the Boston Scientific GENUS RC™ (Valencia, CA, USA) rechargeable pulse generator and directional 8-contact 45 cm leads. Clinical outcomes included changes in MDS-UPDRS Part III and L-Dopa equivalent daily doses (LEDD) at 6-month follow-up.
Results: The mean improvement in MDS-UPDRS III scores was 51%, accompanied by a 62% reduction in the L-Dopa equivalent daily dose (LEDD). One patient developed transient anterior STN stimulation-related side effects, and another required four days of postoperative ICU care for complications; both recovered fully. GPi-targeted patients demonstrated comparable efficacy with fewer stimulation-related adverse effects. No infections or hardware-related complications occurred during the follow-up period.
Conclusions: The introduction of directional, rechargeable DBS technology integrated with precise stereotactic and software-guided planning achieved significant clinical improvements and high safety in Azerbaijan’s first large PD DBS series. The transition from STN to GPi targeting yielded better tolerability while maintaining therapeutic benefit. These findings support continued expansion of advanced neuromodulation programs in emerging healthcare regions
P36.09
1 Insightec, United States
2 Insightec, Italy
3 Insightec, Netherlands
4 Insightec, Israel
Introduction: Parkinson’s disease (PD) is a fast-growing neurological disorder, with incidence rising over 50% from 2012 to 2020. As PD progresses, motor fluctuations and dyskinesia disrupt daily life, yet fewer than 2% of eligible people with PD undergo advanced therapies—often due to access disparities, perceived invasiveness, or treatment-related burden. MR-guided focused ultrasound (MRgFUS) is an incisionless, outpatient procedure that enables precise targeting with real-time thermometry and clinical feedback. It is now the most widely used advanced therapy for essential tremor and is increasingly adopted for PD. FDA has approved unilateral thalamotomy (2018), pallidotomy (2021), and staged, bilateral pallidothalamic tractotomy (2025), with CE Mark for unilateral PD across multiple targets (2022). Clinical trial and real-world data on MRgFUS outcomes in PD are reviewed.
Methods: Efficacy and safety data across clinical trials in PD, including thalamotomy (PD-T), pallidotomy (PD-P), subthalamotomy (PD-STN), and staged, bilateral pallidothalamic tractotomy (PD-PTT1 & PD-PTT2). Real-world data sources include published literature and post-market surveillance (PMS).
Results: Thalamotomy showed a 62% improvement in tremor (CRST A+B). Pallidotomy, subthalamotomy, and pallidothalamic tractotomy improved motor features and complications: PD-P improved 26.4% in MDS-UPDRS Part III OFF and 46.1% in Part IV; PD-STN by 34.2% (Part III) and 40% (Part IV); PD-PTT by 32% (Part III) and 68% (Part IV). Most adverse events (AEs) were mild (72% PD-T; 75% PD-P; 67% PD-STN; 87% PD-PTT1; 70% PD-PTT2), with severe events being rare. Common AEs included paresthesias and gait disturbance in PD-T; dysarthria, gait disturbance, and loss of taste in PD-P; dyskinesias, speech disturbance and gait disturbance in PD-STN, and fatigue (PTT1), and dysarthria (PTT2) in PD-PTT. Most resolved within 6 months, with no new or worsening AEs at long-term follow-up. Literature review showed similar safety, with mostly mild and transient events. Recent PMS data indicate AEs were reported in 0.6% of 2244 commercial PD procedures.
Conclusions: Unilateral and staged, bilateral MRgFUS provides significant and sustained improvement in motor outcomes with an acceptable safety profile. Its incisionless nature and expanding regulatory approvals position MRgFUS as a promising treatment option for people with PD, especially those underserved by existing therapies.
P36.10
1 Michigan State University College of Human Medicine, United States
2 ASU-Banner Neurodegenerative Disease Research Center (NDRC), United States
3 Parkinson’s Disease Research Unit Barrow Neurological Institute, United States
We have demonstrated that MRI-guided putaminal delivery of adeno associated virus (AAV)-CaV1.3-short hairpin (sh)RNA bilaterally to aged parkinsonian macaques decreases expression of dysfunctional CaV1.3 channels, reverses long-standing motor deficits ‘OFF’ medication, enhances motor response to levodopa, and prevents levodopa-induced dyskinesias (PMID:40437755). Studies exploring possible mechanisms underlying these unprecedented therapeutic benefits suggest that our RNA-interference therapeutic may provide neuroREgenerative efficacy to injured nigrostriatal dopamine (DA) neurons. In our model, monkeys first receive the neurotoxin MPTP into the right common carotid artery to induce rapid, extensive, primarily unilateral death of DA neurons in the RIGHT substantia nigra (SN). Two weeks later they receive intravenous MPTP (0.15-0.6 mg/kg) which results in bilateral parkinsonian motor signs (2-6 months). However, DA neurons in the LEFT SN subjected to systemic dosing show less rapid/less complete cell death, often demonstrating downregulation of the DA synthetic enzyme tyrosine hydroxylase (TH) in the absence of/prior to cell death. AAV is well-known for retrograde transduction and we have confirmed AAV-CaV1.3-shRNA retrograde transport from putamen to SN that appears to provide restoration of DA-phenotype (i.e., TH-immunoreactivity (ir)) in subpopulations of presumably quiescent DA neurons in left SN, those with lost TH-phenotype but not overtly killed by MPTP. Interestingly, despite similarities in TH-fiber denervation in left putamen, especially post-commissural, AAV-CaV1.3-shRNA recipient monkeys have significantly more TH-ir neurons in their left SN compared to right SN, and compared to left and right SN in AAV-SCR-shRNA controls. Further, recent evidence suggests that left SN DA neurons have restored DA function indicated by elevated/normalized DA transporter (DAT) levels in the left putamen despite continued sparsity of putaminal TH. The potential benefit of AAV-CaV1.3-shRNA in SN DA neurons derives from the fact that these neurons have autonomous pacemaking properties mediated by CaV1.3 Ca2+ channels resulting in excessively high metabolic demands implicated in their vulnerability to neurodegeneration in PD. It is reasonable to suggest that retrograde transduction of SN DA neurons with our potent CaV1.3 RNAi-based vector restores physiological balance, promotes restoration of the DA phenotype and leads to restoration of motor function. (NIH NS110398)
CLINICAL SCIENCES: Clinical trials: design, outcomes, recruiting etc.
P37.01
1 University of Delaware, United States
2 NeuroThera, United States
Parkinson's Disease (PD) is a progressive neurodegenerative disease largely attributed to dysfunction of the basal ganglia, a set of deep-brain nuclei critical for movement regulation via dopamine. Such dysregulation contributes to the motor and non-motor symptoms of PD, including slowness of movement, rest tremor, rigidity, postural instability, and cognitive decline. While current pharmacologic treatments can help ease symptoms, their effectiveness often declines as the disease progresses. Surgical treatment options such as deep brain stimulation have proven to be effective but are invasive and often not suitable for everyone, highlighting the need for alternative or complementary interventions. Our study explores the potential of transcranial photobiomodulation (tPBM), a non-invasive brain stimulation technique that sends low-level infrared light to cortical brain regions, and has been shown to increase cerebral blood flow and cellular metabolism. Given the frontal cortex’s role in executive function and its connection to the basal ganglia, we investigated whether tPBM delivered to the frontal cortex can improve motor and cognitive symptoms in PD. tPBM was delivered 3 times a week for six weeks (810nm wavelength, 12 min per session) with pre-post assessments of cognitive and motor function performed in the off-medication state (∼12 h washout). Outcome measures included validated tools, such as the motor section of the MDS-Unified Parkinson's Disease rating Scale (MDS-UPDRS-III) and the kinesiaOne wearable motion sensor. To date, 8 participants (age: 68.25 ± 7.95, gender: 2F, 6M) have completed the intervention, with 4 receiving active treatment and 4 receiving sham treatment. Preliminary results suggest that the active treatment group showed greater improvements (lower scores) compared to the sham for both measures. For KinesiaOne, the average total and upper extremity scores improved by 4 points for the active group and only by 1 point for the sham. Total MDS-UPDRS-III scores for the active group also showed greater reductions in motor impairment when compared to the sham. The intervention remains ongoing to solidify these preliminary findings. If proven effective, tPBM could serve as a powerful adjunct tool for the treatment of PD, with the potential to alleviate symptoms and enhance quality of life
P37.02
1 Rush University Medical Center, United States
2 Parkinson's Foundation, United States
3 Lewy Body Dementia Association, United States
4 University of Rochester Medical Center, United States
5 New York University Grossman School of Medicine, United States
Objective: Lewy Body Dementia (LBD) includes both people with Parkinson’s Disease Dementia (PDD, affecting up to 80% of people with PD over time) and people with Dementia with Lewy Bodies (DLB). LBD is often a missed or delayed diagnosis and LBD family care partners face high strain and adverse health outcomes without effective interventions. PD and LBD caregiver studies often face under-enrollment and homogeneous cohorts, with male, non-Caucasian, and rural-dwelling care partners underrepresented. Here, we describe a multipronged, community-engaged strategy to recruit >680 participants into a national, virtual, randomized controlled trial of an LBD caregiver intervention (PERSEVERE, NCT06389032).
Methods: We designed a three-tiered approach to recruit 682 LBD family caregivers over two years. Partnering with the Parkinson’s Foundation and Lewy Body Dementia Association, we sought to reach a broad PD and LBD audience through mass emails, helpline referrals, social media posts, and presence at community events. We shared information directly with neurologists and allied health professionals through direct outreach, staff presentations, and academic webinars. Through our LBD caregiver advisors, we identified support groups, social networks, and community organizations throughout the US. We created PD and LBD presentations and recruitment materials featuring diverse families to share with interested organizations and communities. Care partner advisors recommended social media to build awareness, leading to Facebook, Instagram, and TikTok feeds. Foundation partners and care partner advisors review all materials for representative and applicable content. Participant demographics and referral source are collected upon enrollment (ongoing).
Results: Over 16 months, we have screened 1,267 and enrolled 604 participants. Referral sources: national organizations (56.4%); support groups (21.6%); word-of-mouth (8.4%); referring provider (8.7%); and clinical trial websites (2.7%). Among enrolled participants, 13.7% are male, 9.6% non-Caucasian, and 8.1% rural-dwelling.
Conclusion: A national, community-engaged approach to care partner recruitment with early and sustained partnership with advocacy organizations and experienced care partners has yielded brisk trial enrollment from numerous sources, particularly from support groups and peer referrals. Community-engaged recruitment facilitates both study enrollment and generalizability of findings.

P37.03
1 University College London, United Kingdom
2 Newcastle University, United Kingdom
3 University of Sheffield, United Kingdom
4 University of Cambridge, United Kingdom
5 Medical Research Council Clinical Trials Unit, United Kingdom
6 Cure Parkinson's, United Kingdom
7 Expert by Experience, United Kingdom
Introduction: The Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) multi-arm, multi-stage trial will efficiently assess potential disease-modifying therapies (DMTs) in a representative UK sample of people with PD. Multi-arm, multi-stage (MAMS) designs enable simultaneous testing of multiple therapies against a shared placebo arm; early identification of ineffective therapies for discontinuation; and incorporation of new interventions within the established trial infrastructure.
Methods: >90 key stakeholders, including people with PD (PwP), carers /partners, and diverse community members, collaborated to design the trial via the EJS ACT-PD Initiative. Robust, iterative processes were developed and implemented to prioritise promising therapies and identify meaningful outcome measures. Trial-funded staff and a site selection model based on experience, capabilities and location will support efficient and diverse participant recruitment across more than 40 UK sites.
Results: The EJS ACT-PD trial is an inclusive phase 3, double-blind, MAMS trial for PwP on dopaminergic medication without dementia, severe disability or advanced PD treatments. The trial will launch with two active treatments arms (telmisartan and terazosin) against a shared placebo. A third active treatment arm (ursodeoxycholic acid) will open after 1 year. Participants will be randomised across all recruiting arms to take trial medication for up to 3 years. A hybrid delivery model will allow participants to complete their 6-monthly study visits either in-person or remotely, with trial medication being posted directly to participants’ homes. Early-stage analyses will use the MDS-UPDRS parts 1, 2 and remote 3 to inform discontinuation of ineffective treatments. The primary outcome is a 30% reduction in disease progression as assessed by parts 1 and 2 of the MDS-UPDRS. Trial sub-studies include use of a digital device to passively monitor progression and collection of additional blood and cerebrospinal fluid samples for biomarker analysis. Stage 2 of the EJS ACT-PD Initiative will focus on future treatment, emerging innovations and long-term sustainability of the trial.
Conclusion: Recruitment launched in September 2025 with sites gradually opening over the next 6-9 months. The trial will provide ongoing research opportunity for PwP, strengthen UK PD trials infrastructure, and provide replicable processes for future research initiatives.
P37.04
1 University College London, United Kingdom
2 Newcastle University, United Kingdom
3 University of Sheffield, United Kingdom
4 University of Cambridge, United Kingdom
5 Medical Research Council Clinical Trials Unit, United Kingdom
6 Cure Parkinson's, United Kingdom
7 Expert by Experience, United Kingdom
Introduction: The Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) Trial will be the UK’s largest PD trial and the first to use a multi-arm, multi-stage (MAMS) design. The trial’s scale, sustainability, adaptive methodology, and inclusive approach create a unique platform to address key gaps in PD research. To maximise this potential, a series of innovative sub-studies have been embedded to generate enriched datasets for wider impact on disease-modifying approaches.
Methods: Expert subgroups, including people with Parkinson’s (PwP), were convened within the EJS ACT-PD Initiative to consider methods for capturing digital data, biosamples, genetic samples, and partner/care partner impact. The digital measures subgroup prioritised concepts of interest and developed a selection framework informed by literature review, regulatory guidance, validation criteria, deployment feasibility, and data management. The biosamples subgroup reviewed available biomarkers, assessing their validity, reliability and reproducibility as an analysis, and acceptability to PwP. The Patient and Public Involvement and Engagement (PPIE) group advised on the inclusion of data collection from partners.
Results: A digital measures sub-study will utilise the Mobilise-D digital mobility outcome (DMO) using the AX6 Axivity lumbar sensor in all trial participants, to objectively capture indices reflective of real-world mobility performance. A biosamples sub-study includes several additional blood samples to confirm peripheral target engagement of trial treatments. Cerebrospinal fluid will be collected in a subset of participants to assess drug levels and target engagement at single timepoints as well as sustained engagement across several timepoints (baselined, 12 months, 36 months). With participants’ consent, their partners will be invited to take part in the partner sub-study and complete quality of life assessments at the same timepoints as participants. In collaboration with the PD Frontline study, all participants will be offered genetic testing for the GBA and LRRK2 genes.
Conclusion: The trial sub-studies will integrate digital mobility outcomes, gene scores, molecular biomarkers, and partner perspectives, for a multidimensional view of disease progression. This approach will enhance sensitivity to detect disease modification not captured by current methods (e.g., clinical scales).
P37.05
1 UCB, Brussels, Belgium
2 UCB, Braine-l'Alleud, Belgium
3 UCB, Monheim am Rhein, Germany
4 UCB (contracted by UCB), Slough, United Kingdom
Introduction: ATLANTIS (NCT06055985), a Phase IIa study, evaluated the D1 receptor positive allosteric modulator, glovadalen, in people living with advanced Parkinson’s. It was designed with direct and continuous involvement of people with Parkinson’s (PwP). A Patient Council comprising PwP, care partners and patient organizations in the UK and USA contributed to protocol development and co-creation of study materials for participants.
Methods: To ensure participants were well-informed and to optimize the study experience, materials such as a study brochure, visit guide and website were developed to manage participant/caregiver expectations. Text from these materials and the informed consent form was shared with a portion of the Patient Council for review. Feedback was collected via an online survey with predetermined questions addressing understandability, expectation management, document length, language, gaps and overall assessment. This was reviewed and implemented across all study materials as appropriate. Updates regarding implementation of Patient Council feedback were shared with participants. A separate survey was conducted by the Contract Research Organization following the recruitment period to obtain information about use of the materials by study sites. A summary leaflet of study-related topics was also shared with study sites to support understanding of participant/care partner priorities. At the end of ATLANTIS, interviews with participants were conducted.
Results: Six members of the Patient Council participated in the review of study materials. Feedback mostly indicated that materials were relevant, understandable and supported study participants, while some participants noted there was too much information/detail. Overall, 91 of 207 participants completed the exit interviews; responses suggested participants felt valued for their contribution and would recommend study participation to others. Fifteen participants (7.2%) discontinued ATLANTIS (adverse event, withdrawal by subject, other).
Conclusion: This work demonstrates the value of embedding participant perspectives throughout the clinical study lifecycle, from protocol development to post-study reflection. Key learnings from ATLANTIS have informed the expansion of this study design approach to other UCB trials across broader indications.
This abstract builds on the ATLANTIS poster presented at Alzheimer's & Parkinson's Diseases Conference (AD/PD) in April 2025 (Biagioni et al.).
P37.06
1 Biohaven Pharmaceuticals, New Haven, CT, United States
2 Clintrex, Sarasota, FL, United States
3 Northwestern University, Chicago, IL, United States
Objective: To describe the rationale and design of BHV8000-301, a Phase 2/3 trial of BHV-8000 in early Parkinson’s disease (PD).
Background: PD is a progressive neurodegenerative condition without approved disease-modifying therapies. BHV-8000 is a first-in-clinic, brain-penetrant, selective TYK2/JAK1 inhibitor, being developed to treat neuroinflammatory conditions including early-stage PD. Genetic, epidemiological, preclinical, and emerging clinical data demonstrate the role of immune dysregulation in early PD pathophysiology. Targeted inhibition of TYK2/JAK1 has been shown to block inflammatory pathways in the periphery, (e.g., inflammatory T-cells including Th17) and the CNS (e.g., glial cells), that can contribute to neuronal loss and functional decline in PD. BHV-8000 targets TYK2 and JAK1, avoiding safety liabilities of JAK2/JAK3 inhibition. The objective of BHV8000-301 is to test the safety and efficacy of BHV-8000 in participants with early PD.
Design/Methods: BHV8000-301 is a randomized, double-blind, placebo-controlled phase 2/3 study (NCT06976268). Approximately 550 adults aged 40-85 years, with early PD not treated with dopaminergic therapy, will be enrolled across 195 sites globally. Eligible participants will be randomized 1:1:1 to receive oral BHV-8000 10mg, 20mg, or placebo once-daily for 48 weeks. The primary endpoint is time to qualifying worsening event, defined as a confirmed ≥2-point worsening on the Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) Part II. Secondary endpoints include change from baseline to Week 48 on MDS-UPDRS Part III, Clinician Global Impression of Severity, DaT-SPECT, and Biohaven-developed, Parkinson’s Disease Composite Score (PARCOMS-Function). The Michael J. Fox Foundation’s Parkinson's Progression Markers Initiative (PPMI) and the Critical Path for Parkinson’s (CPP) database were utilized in the design of key efficacy endpoints.
Results: Enrollment began 5/2025 and is ongoing.
Conclusions: BHV-8000 is a novel, potent, brain-penetrant, selective TYK2/JAK1 inhibitor targeting central and peripheral immune dysregulation and inflammation underlying PD pathogenesis. The study utilizes an innovative endpoint and seamless Phase 2/3 design. Further information available at www.biohavenclinicaltrials.com/clinical-studies/parkinsons-disease/.
P37.07
1 Movement Disorders Unit, Dept of Neurology, Tel Aviv Sourasky Medical Center | Ono Academic College, Faculty of Health Professions, Communication Sciences and Disorders Department, Kiryat Ono, Israel
2 Department of Otolaryngology, Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel | Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
3 Movement Disorders Unit, Dept of Neurology, Tel Aviv Sourasky Medical Center, Israel
4 Department of Otolaryngology, Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel | Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
5 Department of Otolaryngology, Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Tel-Aviv, Israel
6 Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
7 Department of Otolaryngology-Head and Neck Surgery, University of California Davis, Sacramento, CA, United States
8 Movement Disorders Unit, Dept of Neurology, Tel Aviv Sourasky Medical Center | Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
9 Movement Disorders Unit, Dept of Neurology, Tel Aviv Sourasky Medical Center | Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Introduction Swallowing disorders is a common complication (up to 100%) in patients with Parkinson's disease (PWP) and is documented in all phases of swallowing. Reduced swallow safety may be related to decreased elevation and excursion of the hyolaryngeal complex. Increased submental muscle force generation has been associated with expiratory muscle strength training and subsequent increases in hyolaryngeal complex movement, provide a strong rationale for its use as a swallowing therapy tool.
Objective To evaluate the impact of the elevation training mask (ETM) on swallowing dysfunction in patients with Parkinson's disease (PWP) when used as a respiratory muscle strengthening tool.
Materials and Methods Thirteen PWP underwent Fiberoptic Endoscopic Evaluation of Swallowing (FEES) and spirometry assessments both before and after a 4-week ETM use, which included incrementally increasing resistance each week. Measurements taken included EAT10, swallowing disturbances questionnaire (SDQ), Penetration Aspiration Score (PAS), Yale score, Peak Expiratory Flow (PEF) and United Parkinson’s Disease Rating Scale (UPDRS). The study was approved by the institutional review board.
Results Out of the 13 male participants recruited for the study, mean (±SD) age was 70 ± 10 years, with a mean disease severity of 33 ± 11 according to the UPDRS. Pre-treatment EAT10 score was 11.5 ± 10, which slightly improved to 9.8 ± 7 post-treatment (p>0.05); Pre – treatment SDQ score was 15.4±7.2, which slightly improved to 13.6 ± 6.5 post treatment (p>0.04). FEES demonstrated a significant improvement in vallecular residue during swallowing of International Dysphagia Diet Standardization (IDDSI) 4 and 7 textures (p < 0.05). PAS for liquids of 2.5 ± 1.9 pre-treatment, which decreased to 1.3 ± 0.5 post-treatment (p>0.05). There was a non-significant improvement in the Penetration Aspiration Scale (PAS) across all textures, as well as in the residue score of the pyriform sinus (p > 0.05). PEF rates slightly increased from 4.8 ± 2.8 pre-treatment to 4.99 ± 2.5 post-treatment (p>0.05).
Conclusion A 4-week use of ETM, serving as a form of respiratory muscle strengthening, may improve swallowing function as observed by decrease vallecular residue in PWP with dysphagia. A larger study cohort is needed for a more comprehensive evaluation of ETM's role in swallowing rehabilitation.
P37.08
1 Individual researcher & advocate, France
Background: As a young-onset Parkinson's Disease (PD) patient diagnosed in July 2023, I discovered that lifestyle modifications significantly impact my cognitive and motor symptoms. This experience revealed a gap in PD research: while traditional RCTs provide population-level evidence, they may miss interventions that work dramatically for specific patient phenotypes due to disease heterogeneity, slow progression timelines, and the dismissal of documented individual successes as ""merely anecdotal.""
Objective: To implement a rigorous N-of-1 trial protocol testing multiple lifestyle interventions, demonstrating how systematic individual experiments can identify promising treatments for specific PD subtypes while complementing traditional research approaches.
Methods: This 15-month single-patient trial employs randomized 2-week intervention blocks with 1-week washout periods, testing: walking protocols (10-60 minutes), light exposure (retinal/skin), breathing practices and Non-Sleep Deep Rest protocols. Daily measurements include objective gait/tremor assessments via devices and subjective symptom scales. Confounding variables (sleep, stress, weather, medication timing) are systematically tracked. The protocol incorporates established methodological principles including randomization, washout periods, and systematic outcome measurement to ensure scientific rigor.
Innovation: This patient-driven approach addresses known limitations in PD research. By treating each patient as their own control, we can: identify responder subtypes faster and more economically than large trials, validate ""anecdotal"" improvements through rigorous methodology, and test multiple interventions for a fraction of the cost of a single traditional study. This methodology respects PD's likely nature as multiple conditions with different mechanisms rather than a single disease.
Expected Impact: Beyond personal optimization, this work could transform how we approach heterogeneous conditions. While RCTs remain essential for regulatory approval, N-of-1 trials could identify which patients respond to which interventions, potentially accelerating personalized medicine by years and at a fraction of the cost.
Conclusion: Rigorous patient-driven research offers a complementary paradigm that could unlock treatments we're currently missing.
INSTITUTION/AFFILIATION: Independent Researcher in partnership with France Parkinson (France) N-of-1 Hub (Australia)
P37.09
1 Centre for Trials Research, Cardiff University, United Kingdom
2 Cardiff University, United Kingdom
3 Sparky Samba, United Kingdom
4 Patient representative, United Kingdom
5 cardiff University, United Kingdom
6 Cardiff and Vale University Health Board, United Kingdom
Background: Interventions that include physical activity (exercise, physiotherapy, dancing) or repetitive beats to music have been shown to help with Parkinson’s disease (PD) symptoms. Providing such interventions in the community, rather than in clinical settings, may help people with PD stay engaged with the intervention to achieve sustainable potential health benefit. SParky Samba is a community-based Samba percussion group, developed by people with PD for people with PD. SParky Samba is popular with the people that take part, and they feel a number of benefits from being part of the group. We have worked together with the community group to investigate SParky Samba in a small clinical trial, which is the first step towards evaluating SParky Samba as a health intervention for people with PD.
Trial Design: We are conducting a randomised controlled feasibility trial in 60 people with PD. Trial design and delivery has been led by members of the original SParky Samba group. After completing baseline assessments, participants are randomly allocated to take part in a weekly local SParky Samba group or continue their usual activities for 12 weeks. After 12 weeks participants complete the same assessments and are then invited to answer an additional questionnaire and/or complete and interview to share their views on SParky Samba. Participants allocated to the activity as usual group can then take part in SParky Samba if they wish. The primary outcome is feasibility, determined by success against pre-defined criteria relating to recruitment, retention, data completion and intervention adherence. Secondary outcomes prioritised by people with PD include measures relating to motor function, well-being, cognition and physical activity engagement.
Analysis and Dissemination: Feasibility outcomes will be assessed according to the pre-defined criteria. Secondary outcomes will be summarised descriptively. Interviews and free-text responses in the end of trial questionnaire will be analysed qualitatively to understand the acceptability of SParky Samba and contextual mechanisms around its delivery.
Trial Status: The SParky Samba trial opened to recruitment at all three sites in South Wales, UK in July 2025. Recruitment will continue until May 2026. As of 1st October 2025, 25% of the target sample has been recruited.
Trial Registration: ISRCTN11861663
P37.10
1 Center for Neurodegeneration and Experimental Therapeutics, University of Alabama at Birmingham, United States
2 Selkirk Neurology & Inland Northwest Research, PLLC, United States
3 Inova Parkinson's & Movement Disorders Center, United States
4 Edmond J Safra Program in Parkinson’s Disease and Morton and Gloria Shulman Movement Disorders Clinic, Toronto Western Hospital and Division of Neurology, UHN, Division of Neurology, University of Toronto; Krembil Research Institute, Canada
5 AbbVie Inc., United States
6 Oregon Health and Science University School of Medicine, United States
Introduction: In a 12-week, phase 3 study, foslevodopa/foscarbidopa (LDp/CDp) improved motor symptoms, quality of life (QoL), and sleep disturbances vs oral therapy. This analysis evaluated the long-term benefits of LDp/CDp vs oral therapy.
Methods: US adults aged ≥30 years with advanced Parkinson’s disease (aPD) and ≥2.5 hours of “Off” time were included. An unadjusted indirect comparison of patients treated with LDp/CDp in a 52-week, single-arm, open-label trial (NCT03781167) and its ongoing 96-week open-label extension (NCT04379050) vs those receiving oral therapy in the 24-month real-world PROSPECT (PRospective Observational Study to evaluate the disease Progression and burdEn of disease of Parkinson’s disease patients inadequately Controlled by conventional Therapy) study was conducted. Outcomes included “Off” and “On” times (PD diary), QoL (39-item Parkinson’s Disease Questionnaire), motor experiences of daily living (m-EDL; Movement Disorders Society Unified Parkinson’s Disease Questionnaire Part II), and sleep disturbances (Parkinson’s Disease Sleep Scale-2). Mean differences in change from baseline and achievement of minimal clinically important difference (MCID) were descriptively compared at P<.05.
Results: Baseline characteristics were generally balanced (LDp/CDp [n=45]; oral therapy [n=58]). As early as 6 months, treatment with LDp/CDp vs oral therapy resulted in significant improvements in “Off” time (mean [95% CI] treatment difference for LDp/CDp vs oral therapy: −2.3 [−3.4, −1.3] hours), “good On” time (2.6 [1.5, 3.8] hours), QoL (−8.3 [−12.4, −4.2]), m-EDL (−4.8 [−7.1, −2.4]), and sleep disturbances (−7.2 [−10.5, −4.0]; Figure); which were sustained through 24 months for “Off” (−2.3 [−3.7, −1.0] hours) and “good On” times (3.3 [1.9, 4.8] hours), and through 12 months (last measurement) for sleep disturbances (−6.3 [−9.7, −2.8]). Treatment with LDp/CDp vs oral therapy up to 24 months resulted in significantly greater proportions of patients achieving the MCID in “Off” time (43.8% vs 13.5%), “good On” time (50.0% vs 8.1%), QoL (35.9% vs 11.9%), m-EDL (41.0% vs 15.2%), and sleep disturbances (12 months; 65.1% vs 37.0%).
Conclusion: Although limited by an indirect comparison, treatment with LDp/CDp led to significant and sustained (to 24 months) improvements in “Off” time, “good On” time, QoL, m-EDL, and sleep disturbances vs oral therapy in people with aPD. Timely initiation of LDp/CDp can provide optimal symptom control.
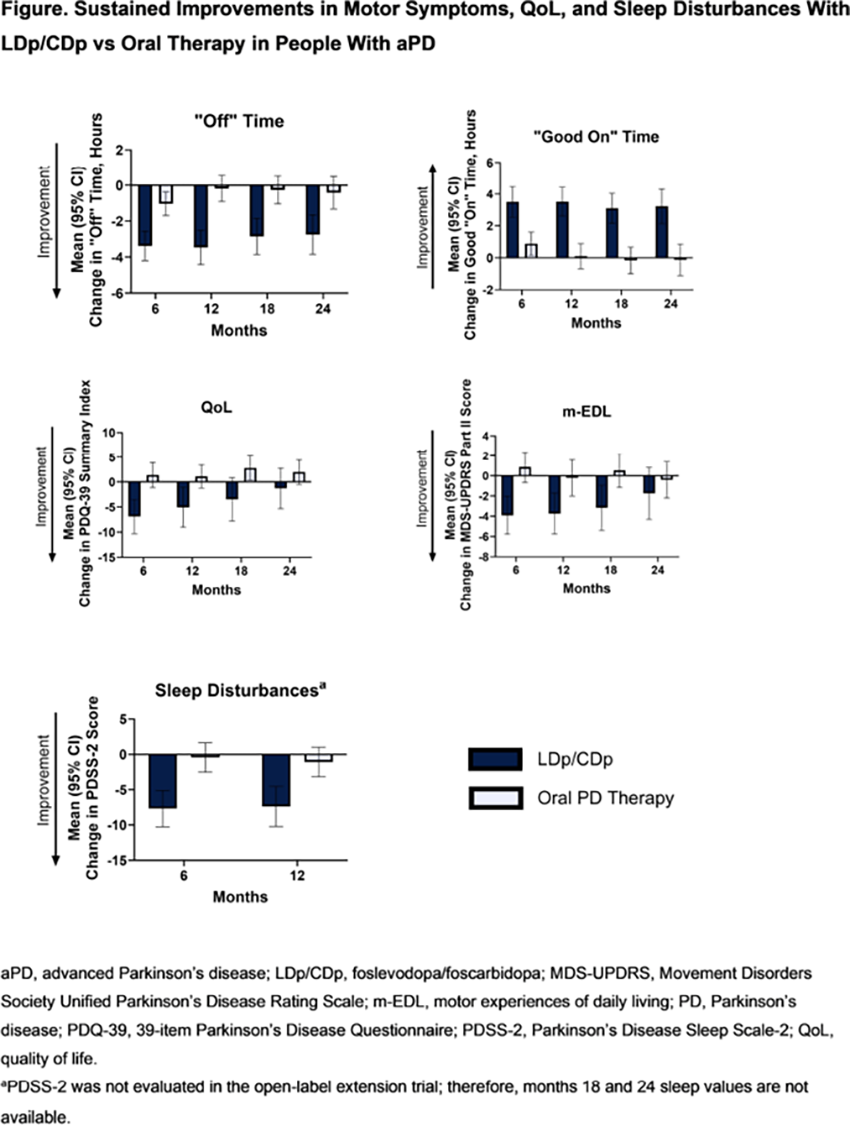
P37.11
1 PD research advocate, United States
2 Cure Parkinson's, United Kingdom
3 PD research advocate, United Kingdom
4 Michael J. Fox Foundation for Parkinson's Research, United States
Objective: To provide a longitudinal overview of the clinical trial pipeline in Parkinson’s disease (PD), focusing on drug therapies being tested in Phase 1-3 trials between 2015 and 2024. This review summarises research efforts worldwide and identifies gaps and opportunities for future studies and funding in order to support collaboration between the patient community, researchers, and funders.
Methods: A dataset of clinical trials for drug therapies in PD was obtained from the ClinicalTrials.gov online registry, identifying Phase 1-3 interventional trials registered between January 1st, 2015 and December 31st, 2024. Trials were filtered to exclude non-drug interventions. Each trial agent was categorised as a symptomatic therapy (ST) or disease-modifying therapy (DMT) and was assigned to a therapeutic category based on its target and/or mechanism of action. Each agent was also classified as novel, repurposed, reformulated, or new claim.
Results: 444 PD drug trials were identified, of which 282 (64%) targeted symptomatic relief and 162 (36%) investigated disease modification. Phase 2 represented the largest portion (46%), followed by Phase 1 (42%) and Phase 3 (12%). Symptomatic therapies were dominated by dopaminergic (43%) and non-dopaminergic neurotransmitter (44%) approaches, with reformulations and repurposed drugs accounting for more than half of ST trials. Among DMT trials, the most frequently investigated categories were agents targeting alpha-synuclein (17%), cell therapies (10%), energy and mitochondria (9%), and therapies addressing genetic risk factors (GBA1/LRRK2) (11% combined). Only nine DMTs were in Phase 3, accounting for 6% of DMT trials. Across all phases, target enrollment was over 39,000 participants, indicating strong patient engagement in the clinical trial pipeline.
Conclusion: This 10-year review illustrates both progress and challenges in PD drug development. While many agents have entered early- and mid-stage testing, the majority of trials have focused on symptomatic relief, with limited advancement of DMTs into late-phase studies. The significant proportion of reformulated and repurposed agents demonstrates a practical approach to drug development. Future progress will require continued innovation, improved trial design, and sustained collaboration among researchers, funders, and the patient community in order to improve symptomatic treatments and bring the first disease-modifying therapy to regulatory approval.
P37.12
1 Roche Pharma Research and Early Development (pRED), Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland
2 Product Development, F. Hoffmann-La Roche Ltd, Basel, Switzerland
3 Roche Products Ltd, Welwyn Garden City, United Kingdom
4 Genentech, Inc., South San Francisco, CA, United States
5 Special Interest Group (SIG) Black Diaspora, Morgan Hill, CA, United States
Introduction: Clinical trials for Parkinson’s disease (PD) have historically lacked diverse representation, with limited racial, ethnic, and geographic inclusion. These disparities may reflect varied diagnosis and treatment journeys, resulting in unequal opportunities to participate and reducing the generalizability of findings. This work aimed to explore the lack of diversity in early-stage PD (Hoehn and Yahr stage <3) clinical trials and to identify actionable gaps and strategies to improve inclusive representation.
Methods: A narrative review was conducted, drawing from recent clinical trial data in early-stage PD, relevant literature, and insights from patient and community stakeholders. The review encompassed interventional Phase 2 and 3 clinical trials listed on ClinicalTrials.gov, initiated from 2015 onward, with published demographics. Patterns in participant racial, ethnic and geographical distribution were analyzed and compared against global and US-specific PD incidence data. Key barriers to inclusion were identified and mapped to potential solutions.
Results: The review confirmed that early-stage PD trials remain predominantly white and centered in high-income regions, demonstrating a lack of representation compared to the demographic and geographic distribution of PD patients based on scarce, limited-granularity epidemiological data. Underrepresentation of populations may be reinforced by disparities in diagnosis, limited healthcare access, mistrust in the research process, burdensome study designs, language barriers and inconsistent reporting of participant demographics. Several emerging strategies—such as diversifying trial sites, implementing culturally tailored outreach, and adopting more participant-centric study models—show potential for enhancing inclusion when applied deliberately.
Conclusions: Overcoming disparities in PD clinical trials requires moving beyond passive diversity statements toward active, sustained community engagement and systemic change. Broader representation is not only an issue of equity—it is essential for generating scientifically robust and clinically relevant evidence that benefits all individuals living with PD.
Abstract has been submitted for consideration to the 2026 Alzheimer's & Parkinson's Diseases Conference (AD/PD).
P37.13
1 HAWK University of Applied Sciences and Arts Hildesheim/Holzminden/Göttingen, Germany
2 University Medical Center Göttingen, Germany
Introduction: The current research project ParkNetz is addressing the challenge of fragmented healthcare for people with Parkinson's disease (PwPD) in Southern Lower Saxony, Germany, in order to establish a Parkinson network. The participatory research approach Photovoice is employed to ensure that the future network meets the needs of those affected. In Photovoice, participants become co-researchers and document their healthcare experiences by taking pictures and discussing them in a group. Then, they planned the dissemination of the photographic and textual outcomes. This poster reports on (1) the experiences of PwPD using Photovoice, and (2) recommendations for using Photovoice with this population.
Methods: To understand the perspectives towards Photovoice, nine PwPD and four relatives were interviewed. The semi-structured interview guide was developed collaboratively by an academic researcher and two co-researchers with PD who were not part of the Photovoice project. Interviewees with PD were aged 51 to 80 years, with disease duration ranging from less than one year to 16 years. Relative-interviewees were aged 65 to 73 years, and the time since PD diagnosis of their partner ranged from 2 to 32 years. Interviews were transcribed verbatim and analysed using qualitative content analysis according to Kuckartz and Rädiker (2024).
Results: The co-researchers were initially unfamiliar with the Photovoice methodology. All PwPD found the approach effective for documenting their PD-related healthcare experiences. The photographs facilitated an in-depth exchange among the group. From their point of view, physical symptoms did not interfere with taking photographs; however, PD symptoms, such as on-off fluctuations hindered workshop participation. Participation also led to personal benefits, e.g. positive influence on well-being, changed perspective on one’s personal responsibility and getting to know acquaintances in an intense way. Overarching key success factors for participation included clear signage for rooms, catering during the workshops, technical support as well as limiting group size to five to seven co-researchers.
Conclusion: Photovoice was perceived as a feasible research method for implementation with PwPD. The study identified key factors essential for successful application of Photovoice with this population.
P37.14
1 Radboud University Medical Center, Netherlands
2 Parkinson Vereniging, Netherlands
3 Spierziekten Nederland, Netherlands
4 Radboud University, Netherlands
Work participation is increasingly compromised in persons with Parkinson’s disease (PD). Meeting physical and/or psychosocial work demands becomes more challenging, disrupting work-life balance. Consequently, persons with PD are faced with high unemployment rates and early retirement compared to the general population, impacting their well-being and quality of life. With PD prevalence rising and an aging population, supporting persons with progressive conditions in maintaining work is urgently needed. Yet, such support is rarely offered to persons with PD.
Within the EQuAL study (Enhancement of Quality of work And Life), we are now evaluating the (cost-)effectiveness of a preventive workplace intervention aimed at enhancing sustainable work participation in persons with slowly progressive neurological and neuromuscular disorders. This 18-month RCT with parallel process evaluation includes 124 participants - over half of whom have PD - randomized to either a control or intervention group. Both groups continue to receive usual care; only the intervention group additionally receives the “preventive participatory workplace intervention” (PPWI). The PPWI is a personalized approach facilitated by an independent process facilitator guiding participants and their managers at the workplace to jointly identify and address work-related challenges, aiming for a better fit between the employee’s capacity and workload. The PPWI is delivered by 13 occupational therapists across the Netherlands, all specialized in neurological conditions and trained as process facilitators. Remote assessments are performed at baseline, 6, 12, and 18 months. The primary outcome is the difference from baseline to 18-month follow-up in need for recovery after work – a subjective indicator of incomplete recovery after exposure to (high) work demands - measured using the QEEW2.0. Secondary outcomes include indicators of well-being, self-efficacy at work, health-related quality of life, productivity, and societal costs. We will present participant characteristics and preliminary findings on between-group differences after 12 months.
This trial will provide insight into the PPWI’s potential to enhance sustainable work participation, with a lower need for recovery as its short-term indicator. If (cost-)effective, identified barriers and facilitators to implementation will be translated into practical recommendations for feasible and scalable implementation.
P37.15
1 University of Sao Paulo, Brazil
Background: Freezing of gait (FOG) is a disabling symptom of Parkinson’s disease (PD) that increases the risk of falls and loss of independence. While conventional in-person rehabilitation is effective, accessibility remains limited. Remote delivery of physiotherapy could provide a safe and scalable alternative, yet evidence supporting its effectiveness for FOG remains scarce. Purpose: To evaluate the safety, feasibility, and clinical effects of a remote gait-training intervention on FOG severity and mobility in people with PD. Methods: A single-blind randomized controlled trial was conducted with 53 individuals with idiopathic PD (H&Y 1-3) who reported at least one daily FOG episode. Participants were randomized into an experimental (EG) or control (CG) group. Both groups completed 10 supervised online sessions (45-60 min, twice weekly) of gait training with identical intensity and progression; the EG integrated cognitive-motor strategies, while the CG performed equivalent physical training plus stretching. Assessments were performed at baseline, post-intervention, and 30 days later. Primary outcomes were FOG severity (New FOG Questionnaire, NFOG-Q) and freezing duration during the Rapid Turn Test (%FOG). Secondary outcomes included MDS-UPDRS II, PDQ-39 Mobility, and Telephone-MoCA. Repeated-measures ANOVA (permutation-based) was applied. Ethical approval was obtained under protocol number CAAE 50006321.1.0000.0068. The study was produced as part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by grant #2025/14403-7 and grant #2025/02885-7. Results: Forty-four participants completed the trial (EG = 18; CG = 26). Significant group x time effects were observed for FOG severity (p < 0.005), %FOG (p < 0.001), and UPDRS-II (p = 0.046). Improvements were maintained at follow-up for the EG, whereas the CG showed partial regression. No adverse events or falls were reported, and adherence exceeded 90%. Conclusion: Remote, therapist-supervised gait training is a safe, feasible, and effective approach for reducing FOG severity and improving motor performance in people with PD. High adherence and absence of adverse effects demonstrate the potential of tele-rehabilitation to expand access to evidence-based FOG management and support continuity of care beyond the clinic.
P37.16
1 University of Sao Paulo, Brazil
Background: Freezing of gait (FOG) is a disabling and complex symptom of Parkinson’s disease (PD), strongly associated with loss of gait automaticity and increased fall risk. Evidence suggests that individuals with FOG rely on compensatory cortical mechanisms, particularly involving the prefrontal cortex (PFC), to sustain gait under attention-demanding conditions. Notably, these same cortical regions are activated during mental practice (MP), indicating overlapping neural pathways that may be harnessed for rehabilitation. Investigating changes in PFC activity after targeted interventions may provide valuable insights into the neural mechanisms of gait improvement in PD. Purpose: To analyze changes in prefrontal cortical activation patterns before and after a remote intervention combining mental and physical practice (PM+PF) designed to reduce FOG in people with PD. Methods: This single-blind, randomized controlled clinical trial will include individuals with idiopathic PD and FOG confirmed by a neurologist. Participants will be randomly assigned to one of two groups: an experimental group (PM+PF) or a control group (PF with stretching). Both interventions will comprise 10 standardized remote sessions (40–60 minutes each). Cortical activation will be measured using functional near-infrared spectroscopy (fNIRS) during single-task (ST) and dual-task (DT) gait. Primary outcome: changes in PFC activation patterns during gait in ST and DT conditions. Secondary outcomes: spatiotemporal gait parameters (GAITRite), FOG severity (NFOG-Q), freezing duration (%FOG), MDS-UPDRS-II, PDQ-39, and MoCA. All evaluations will be conducted in person at four time points: baseline, post-intervention, and 30 and 60-day follow-ups. Data will be analyzed with repeated-measures ANOVA (p < 0.05). Ethical approval was obtained under protocol number CAAE 50006321.1.0000.0068. The study will be produced as part of the activities of FAPESP Research, Innovation and Dissemination Center for Neuromathematics #2013/07699-0, and supported by grant #2025/14403-7 and grant #2025/02885-7. Expected results: The combined PM+PF intervention is expected to reduce PFC hyperactivation during gait, reflecting improved neural efficiency and motor automaticity, along with reduced FOG severity and enhanced gait performance. These findings may advance understanding of compensatory cortical mechanisms and support the integration of remote cognitive-motor training into PD rehabilitation programs.
P37.17
1 Center for Neurodegeneration and Experimental Therapeutics, University of Alabama at Birmingham, United States
2 Department of Clinical Neurosciences and Hotchkiss Brain Institute, Cumming School of Medicine, University of Calgary, Canada
3 Department of Neurology, University Hospital of Toulouse, France
4 Departments of Neurology and Neurosurgery, University of Colorado School of Medicine, United States
5 Movement Disorders Unit, Department of Neurology, Vall d’Hebron University Hospital; Neurodegenerative Diseases Group, Autonomous University of Barcelona, Spain
6 Lille Neurosciences and Cognition, Movement Disorders Department, CHU Lille, Lille University, France
7 Research Center and Department of Neurology, Utano National Hospital, National Hospital Organization, Japan
8 Oregon Health and Science University School of Medicine, United States
9 AbbVie Inc., United States
10 Westmead Hospital; Sydney Medical School, University of Sydney, Australia
Introduction: Foslevodopa/foscarbidopa (LDp/CDp) is a 24-hour continuous infusion of levodopa/carbidopa prodrugs, indicated for the treatment of motor fluctuations in people with advanced Parkison’s Disease (PD). This analysis assessed improvements in early morning motor symptoms and motor stability with LDp/CDp vs real-world standard of care oral therapies over 24 months.
Methods: Data from 129 participants treated with LDp/CDp for 12 months in a single-arm, open-label, phase 3 trial (NCT03781167) and up to 12 months in its open-label extension study (NCT04379050) were indirectly compared with data from 185 participants treated with oral PD therapy in the 24-month real-world PROSPECT study. PD diaries were used to measure time spent in the “Off” and “On” states. Motor states upon waking were evaluated from the first non-sleep diary entry between 12:00 AM and 12:00 PM after ≥ 2 consecutive hours of sleep. Motor stability during a 16-hour waking day was assessed by the number of daily fluctuations between 3 motor states: “Off”, “good On” (“On” without troublesome dyskinesia [TSD]), and “On” with TSD. Measures were compared using a regression model adjusted for baseline characteristics and outcomes.
Results: A significantly higher proportion (approximately 80% vs 35%; P < .0001 for all time points) of participants treated with LDp/CDp vs oral therapy achieved “good On” time after waking through 24 months (Figure). Those treated with LDp/CDp had the greatest gains from baseline in hours of “good On” time within the first 4 hours of waking. The gain in “good On” time in the morning with LDp/CDp was significantly greater than that achieved by participants receiving oral therapy and was sustained throughout the day and maintained through 24 months (all P < .05; Figure). The proportion of participants receiving LDp/CDp with >9 daily motor-state fluctuations decreased nearly 5-fold from baseline to month 6 (34.3% to 6.7%), while the proportion with 0–3 fluctuations increased nearly 5-fold (11.4% to 58.1%); improvements were maintained through 24 months.
Conclusion: Participants on LDp/CDp vs oral therapy had significant improvement in symptom control in the early morning which persisted throughout the waking day, and had reduced daily motor fluctuations; improvements were sustained through 24 months of treatment. This suggests the 24-hour infusion may allow people with PD to wake up in the “On” state and experience less switching between motor states.

P37.18
1 National Institute for Health and Care Research (NIHR) Newcastle Biomedical Research Centre, Newcastle University, United Kingdom
2 MRC-Biostatistics Unit, University of Cambridge, United Kingdom
3 University College Dublin, Ireland
4 University College London, United Kingdom
5 Queen Mary University of London, United Kingdom
6 Expert through Experience, United Kingdom
7 University of Oxford, United Kingdom
8 University of Surrey, United Kingdom
Introduction Patient-relevant, objective outcome measures that sensitively measure changes in Parkinson’s disease (PD) progression are needed to allow the identification of new disease-modifying treatments. Real-world assessment of gait and mobility in PD through digital mobility outcomes (DMOs) was found to be feasible, valid and acceptable in the Mobilise-D study. Prior to pursuing regulatory approval of these DMOs, further evidence through proof of concept in a clinical trial, with identification of clinically meaningful change for use as electronic Clinical Outcome Assessments (eCOAs) is required. Furthermore, an understanding of whether and how the use of DMOs lead to participation biases and missing data in trials is needed to inform appropriate handling of these missing data in analyses.
Methods A body-worn lumbar device will be deployed within the Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) multi-arm multi-stage (MAMS) trial for disease modification. 1600 participants will be invited to wear the device for seven continuous days every six months for up to three years. DMOs such as gait speed, stride length, and number of walking bouts will be extracted using the validated Mobilise-D pipeline. Qualitative data on participant perceptions, clinically meaningful change and missing data will be collected.
Results A qualitative sub-study will be embedded with the EJS ACT-PD Digital Measures Sub-study to explore clinical meaningful thresholds for use in disease modification trials using anchor- and distribution-based methods. Monitoring of data completeness and demographic comparisons between those who consent to the digital measures study and the main trial cohort will identify any participation biases. A second qualitative study will further explore factors contributing to data loss related to non-consent, adherence and withdrawal, to inform handling of missing data within the analysis pipeline. This will include assessment of potential temporal variations in these factors and their relationship to disease progression.
Conclusions This work will support the development and validation of DMOs as eCOAs for trials that seek to evaluate disease-modifying therapies. Objective outcome measures are needed to speed up the evaluation of therapies and ultimately improve outcomes for people with PD.
P37.19
1 F. Hoffman-La Roche, Basel, Switzerland
2 F. Hoffmann-La Roche, Basel, Switzerland
3 University Feinberg School of Medicine, Chicago, IL, United States
4 Department of Neurology, McGill University, and Montreal Neurological Institute, Montreal, Canada
5 Clinical Ageing Research Unit, Newcastle University, Newcastle upon Tyne, United Kingdom
6 University San Raffaele Roma and the Institute for Research and Medical Care, IRCCS San Raffaele Pisana, Rome, Italy
7 Department of Neurodegeneration, Hertie-Institute for Clinical Brain Research, Tuebingen, Germany
8 Institute for Neurodegenerative Disorders, New Haven, CT, United States
Introduction: The Phase II trial of Anti-alpha-Synuclein Antibody in Early Parkinson’s Disease (PASADENA) is an ongoing double-blind, placebo-controlled trial evaluating the safety and efficacy of prasinezumab in early-stage Parkinson’s disease (PD). The main objective of these analyses is to evaluate the change in severity of motor progression from baseline to Year 5 in the PASADENA open-label extension cohort versus the external comparator population arm derived from the Parkinson’s Progression Markers Initiative (PPMI) observational study.
Methods: To ensure comparability, we selected the PPMI cohort using PASADENA inclusion/exclusion criteria. We then applied weighting, using a well-established propensity score method to balance the trial and comparator groups using baseline characteristics. The validity of this approach was confirmed by similar baseline characteristics and progression over 52 weeks between the PASADENA Part 1 placebo cohort and the weighted PPMI cohort.
Results: At Year 5, the combined PASADENA arm (delayed- and early-start groups) showed less disease progression compared to the PPMI cohort (Figure). This lower progression was observed across multiple measures (all reported as mean difference in points with 80% confidence interval [CI]):
For MDS-UPDRS Part III (OFF state), there was a –41% relative difference, with a mean difference of –4.75 (–6.12, –3.37). For MDS-UPDRS Part III (ON state), there was a –95% relative difference, with a mean difference of –3.65 (–4.92, –2.38). For MDS-UPDRS Part II (patient-reported), there was a –30% relative difference, with a mean difference of –1.59 (–2.25, –0.93). The use of most symptomatic medications was higher in PPMI, with L-Dopa combination therapy as an exception. The average LEDD remained approximately 100 mg higher in PPMI up to Year 5.
Conclusions: The effect of prasinezumab on slowing down motor progression in PD as measured by clinicians and study participants is sustained for up to 5 years relative to an external comparator.
Abstract has been submitted for consideration to the 2026 Alzheimer's & Parkinson's Diseases Conference (AD/PD).
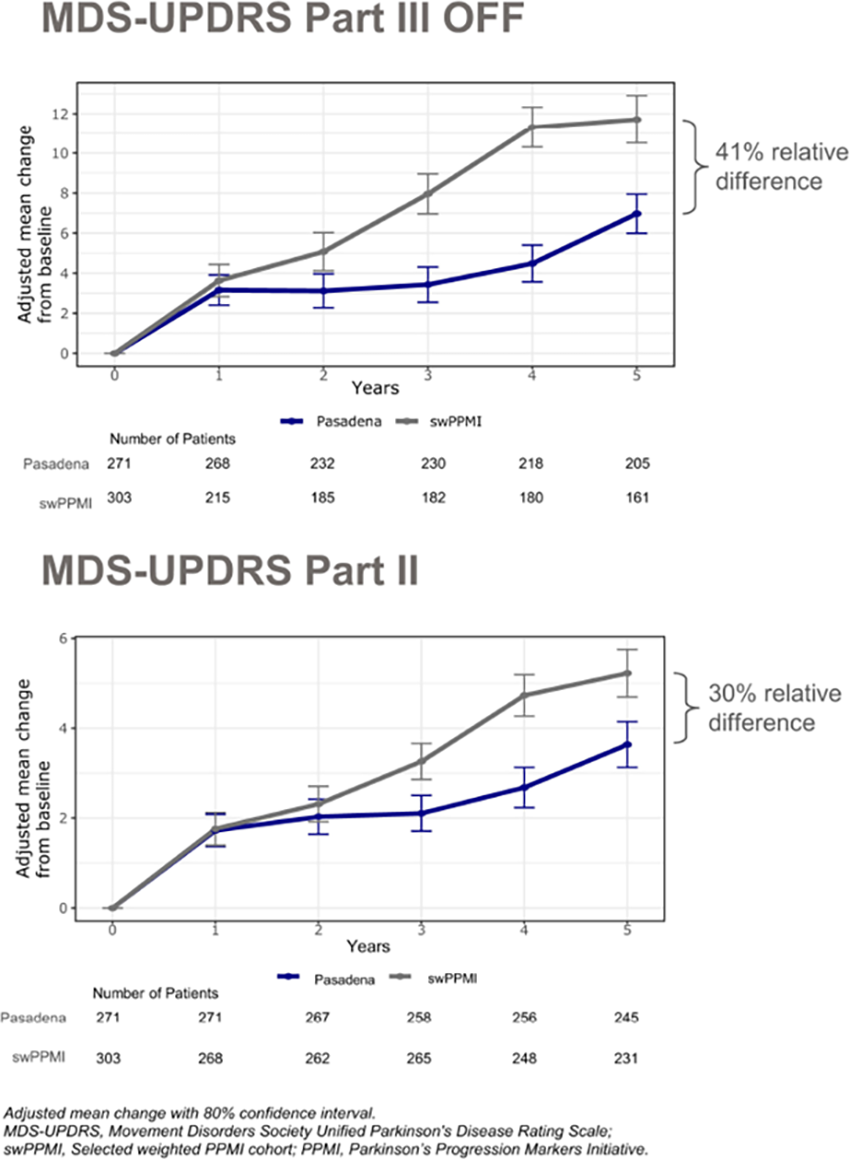
P37.20
1 Product Development Neurology, F. Hoffmann-La Roche Ltd, Basel, Switzerland
2 Roche Pharma Research and Early Development (pRED), Neuroscience and Rare Diseases Discovery and Translational Area, Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland; University of Exeter Medical School, London, United Kingdom
3 Roche Products Ltd, Welwyn Garden City, United Kingdom
4 Department of Neurology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States
5 Institute for Neurodegenerative Disorders, New Haven, CT, United States
6 Clinical Ageing Research Unit, Newcastle University, Newcastle upon Tyne, United Kingdom
7 Department of Neurology, Medical University Innsbruck, Innsbruck, Austria
8 Department of Neurology, University San Raffaele Roma and the Institute for Research and Medical Care, IRCCS San Raffaele Pisana, Rome, Italy
9 Department of Neurology, McGill University and Montreal Neurological Institute, Montreal, Canada
10 Product Development Data Science, F. Hoffmann-La Roche Ltd, Basel, Switzerland
11 Roche Pharma Research and Early Development (pRED), Neuroscience and Rare Diseases Discovery and Translational Area, Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland
Introduction: To evaluate the effect of prasinezumab on slowing down disease progression in participants with early-stage Parkinson’s disease (PD) on stable symptomatic medication.
Methods: PADOVA (NCT04777331) evaluated the efficacy and safety/tolerability of prasinezumab in participants with early-stage PD on stable monoamine oxidase type B inhibitor (MAO-Bi) or levodopa monotherapy. Primary endpoint was time to confirmed motor progression (≥5-points increase from baseline on MDS-UPDRS Part III in OFF-medication state). Secondary and exploratory efficacy assessments included continuous and time-to-event measures of disease progression, and participant- and clinician-rated global measures of change. Exploratory subgroup analyses based on baseline demographic and clinical characteristics were performed. Six months of additional open-label extension (OLE) data were used to assess prasinezumab’s effects after 2 and 2.5 years of follow-up.
Results: 586 participants were enrolled (74.2% receiving levodopa; 25.8% MAO-Bi). Primary endpoint did not reach statistical significance (p=0.0657), but there was a trend for prasinezumab’s potential clinical efficacy (HR [95% CI]=0.84 [0.69–1.01]), with a more pronounced effect in the levodopa population (HR=0.79 [0.63–0.99]). Pre-specified covariate-adjusted analyses showed a nominally significant effect on the primary endpoint (HR=0.81 [0.67–0.98]) and in the levodopa population (HR=0.76 [0.61–0.95]). Consistent positive trends across secondary and exploratory endpoints were also observed. Prasinezumab was well tolerated with no new safety signals observed. Subgroup analyses and an additional 6 months of OLE data will be presented.
Conclusions: Although the primary endpoint of PADOVA was missed, the totality of evidence suggests a possible clinical benefit of prasinezumab in slowing down disease progression in early-stage PD on top of symptomatic medication. Effects observed during double-blind treatment appear to be sustained over an additional 6 months of open-label treatment. These results warrant further exploration in Phase III.
Abstract has been submitted for consideration to the 2026 Alzheimer's & Parkinson's Diseases Conference (AD/PD).
P37.21
1 Patient Partners in Research, Working Group 7 in the NS-PARK MASTER Trial, France
2 Sorbonne University, Institut du Cerveau (Paris Brain Institute, ICM), Inserm, CNRS, Assistance Publique Hôpitaux de Paris, Paris, France
3 Medical Pharmacology department, Expert Center of Parkinson’s Disease, University Hospital of Lille, NS-Park/F-CRIN network, Lille Neuroscience & Cognition Research Center, Lille, France
4 Univ. Bordeaux, CHU Bordeaux, Service de Neurologie des Maladies Neurodégénératives, Parkinson Expert Center, NS-Park/FCRIN Network, CNRS, IMN, UMR5293, Bordeaux, France
5 Université Paris Cité, Université Sorbonne Paris Nord, INSERM, INRAE, Centre for Research in Epidemiology and StatisticS (CRESS), Centre d’Épidémiologie Clinique, Assistance Publique-Hôpitaux de Paris, Hôtel-Dieu, Paris, France
6 Department of Clinical Pharmacology and Neurosciences, Toulouse Parkinson Expert Centre, Toulouse NeuroToul Center of Excellence in Neurodegeneration (COEN), French NS-Park/F-CRIN Network, University of Toulouse 3, CHU of Toulouse, INSERM, Toulouse, France
7 Assistance Publique Hôpitaux de Paris, Department of Neurology, CIC Neurosciences, Hôpital Pitié-Salpêtrière, French NS-PARK/F-CRIN Network, Sorbonne Université, Institut du Cerveau - Paris Brain Institute - ICM, Inserm, CNRS, Paris, France
8 Association France Parkinson, Paris, France
Background: Patient and Public Involvement and Engagement (PPIE) has become a key element in clinical research, ensuring studies are relevant, feasible, and patient-centered. In France, the NS-PARK MASTER Trial, a national platform trial on Parkinson’s disease, has integrated a dedicated group of Patient Partners in Research (PPR) who contribute across all phases of the trial’s development and implementation.
Methods: The PPR group is composed of people living with Parkinson’s disease who are trained to act as patient experts in research. Their mission includes:
Identifying research priorities and contributing to trial protocol design Reviewing and co-developing patient-related materials (informed consent, information leaflets…) Advising on recruitment and retention strategies Participating in all working groups of the MASTER Trial (drug selection, trial design, infrastructure, outcome selection…)
A structured training program (5–7 online modules with interactive assessments and follow-up discussions) will equip participants with essential knowledge on research processes and clinical trials.
Results: The active involvement of PPR has strengthened the MASTER Trial by ensuring that patient perspectives are embedded in decision-making across scientific, ethical, and operational dimensions. Their contributions improve the clarity of communication tools, enhance recruitment feasibility, and increase the acceptability of study procedures.
Conclusion: The integration of trained Patient Partners in Research within the MASTER Trial represents an innovative model for patient engagement in Parkinson’s disease research. By placing patients at the heart of trial governance, the initiative not only improves trial quality and relevance but also fosters a culture of partnership that can inspire future clinical research in neurodegenerative diseases.
P37.22
1 Roche, Switzerland
Introduction Digital Health Technologies (DHTs) enable the remote, frequent and ecologically valid assessment of motor signs in people living with Parkinson’s Disease (PwPD). Here we report patient satisfaction with long-term daily DHT monitoring and its relationship with long-term adherence.
Methods A total of 586 individuals with early-stage PD in the PADOVA Phase IIb study (NCT04777331) performed remote assessments over ∼1.5–3 years with the Roche PD Mobile Application v3, 71% (n=417) of whom completed a DHT satisfaction questionnaire towards the end of the study. The DHT included eleven active tests (AT), surveys and passive monitoring (PM) via smartphone. The questionnaire included five 5-point Likert items on the acceptability of different DHT elements (1=very negative, 5=very positive), a yes/no item on factors reducing the willingness to carry the smartphone (free-text if yes) and open feedback. Global satisfaction was defined as the mean Likert score. DHT adherence was defined per participant as the average number of days/week with complete remote AT data and hours/day of PM with the smartphone.
Results Global satisfaction with the DHT in PADOVA was 3.9/5 (±0.7), corresponding to “positive”. Average satisfaction was positive for all DHT aspects: daily length of AT (4.3±1.0), information on how to wear the devices and complete the tests (4.2±1.0), confidence using smartphones (4.0±1.0), daily active testing (3.9±1.2) and the study app (3.4±1.0). Areas for future improvement included technical and device issues, repetitiveness of ATs and surveys, and practicability, comfort and usability of the provisioned devices. Global satisfaction correlated with adherence (AT: ρ=.22; PM smartphone: ρ=.16; both p<.001).
Conclusions Satisfaction with daily remote digital monitoring over ∼1.5–3 years was positive and associated with adherence, in line with previous findings from the PASADENA Phase IIa trial in an earlier-stage population of PwPD [1]. Participant feedback suggests that improvements in usability and the variety of tests may further increase satisfaction and adherence. Systematically incorporating PwPD feedback could reduce burden and improve adherence, thereby strengthening the robustness of continuous digital endpoints to track disease progression.
[1] Fehlmann B, et al. Mov Disord. 2022;37(Suppl 2).
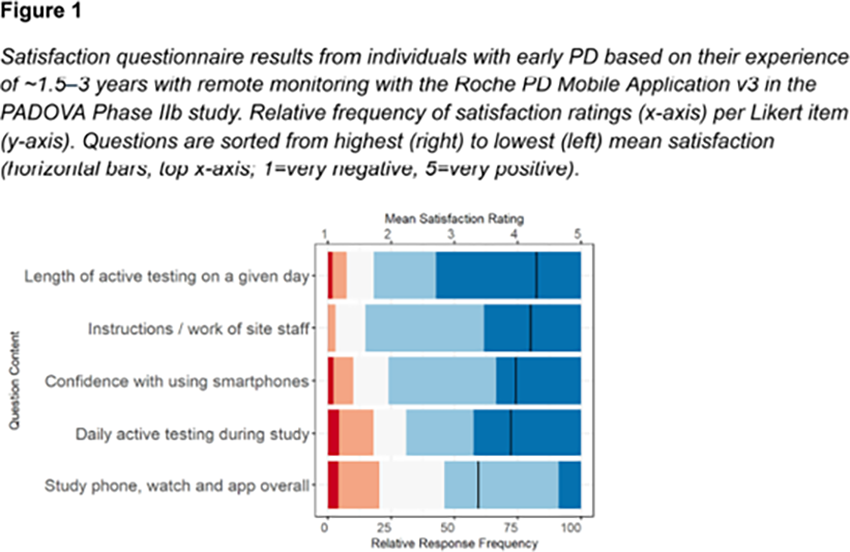
P37.23
1 Parkinson's Foundation, United States
2 Parkinson's Foundation, Canada
3 Aligning Science Across Parkinson’s, United States
4 Global Parkinson's Genetics Program, United States
5 Tel Aviv Sourasky Medical Center, Israel
Objective: To supplement genetics data collected in PD GENEration by providing new clinical research opportunities to PD GENEration participants through surveys, whole genome sequencing (WGS) and genetic counseling of family members, and collection of additional phenotypic data.
Background: The PD GENEration study (NCT04994015), sponsored by the Parkinson's Foundation in partnership with the Global Parkinson’s Genetics Program (GP2), offers WGS with genetic counseling and return of results to broad populations of people living with Parkinson’s disease (PD), reaching over 30,000 participants to date. Historically, data collection occurred only in people with PD (PwP) and was limited to a baseline survey collected at time of consent. Responding to the urgency to better understand genetic forms of PD, new sub-studies were added to PD GENEration to enhance participant engagement and facilitate the collection of additional data.
Design/Methods: PD GENEration expanded operationally with the creation of 3 sub-studies: 1) PDGENE Surveys, which deploys surveys to the entire cohort, 2) PDGENE Family, which invites family members of participants to receive genetic testing and counseling, and 3) PDGENE Insights, which collects additional phenotypic and clinical data from prior PD GENEration or PDGENE Family participants. All 3 sub-studies use a decentralized clinical trial design and remote consenting process, allowing for increased participant accessibility.
Results: PDGENE Surveys was successfully launched in July 2025 with a survey to 17,995 participants and we received a response rate of 44%. PDGENE Family is anticipated to start enrolling by October 2025 with a pilot enrollment goal of 500 family members in the first year. PDGENE Insights is anticipated to start enrolling by April 2026 with a pilot enrollment goal of 100 participants in the first year.
Conclusions: PD GENEration acts as an accessible gateway for diverse communities of people with PD to enter into research. The incorporation of sub-studies into PD GENEration offers, for the first time, additional research opportunities to participants, further expanding participant engagement in research and ensuring the research community has even more data to further their work to find a cure for PD.
P37.24
1 Yale School of Medicine, United States
2 Yale Schoool of Public Health, United States
Objectives: To describe the rationale and data supporting the design of PRISMS, a multicenter clinical trial testing if immune system modulation using the anti-TNFα antibody adalimumab can prevent progression of motor and cognitive changes leading to diagnosis of Parkinson’s disease in persons with REM Sleep Behavior Disorder (RBD), a prodromal PD syndrome marked by dream enactment and loss of REM-related muscle atonia.
Background: PRISMS will enroll persons with RBD and hyposmia; abnormal DaT scans or SAA positivity will not be required. The primary outcome measure will be the Parkinson disease Related Pattern (PDRP) on FDG-PET imaging (Tang et al., Nat Commun. 2024); the key clinical outcome will assess the proportion of participants meeting progression criteria on either MDS-UPDRS or MoCA.
Methods: The design was informed by study of 34 participants in the Yale RBD+ cohort with polysomnographically-confirmed RBD who underwent comprehensive clinical and biomarker assessments. We explored differences in clinical and biomarker measures along three non-exclusive biomarker-based axes (olfactory function, Synuclein aggregating (SAA) positivity and (DaT) binding) and two clinical outcome-based axes (MDS-Prodromal PD probability score and phenoconversion).
Results: We previously reported mild CSF pleocytosis with an increase in microglia-like macrophages and activation of TNF and other inflammatory pathways (Zhang et al., BioRxiv 2025) in RBD vs. controls. Hyposmia was associated with greater reductions in striatal DaT binding, a higher proportion of CSF α-syn SAA positivity, greater increases in CSF MACs, a higher ratio of CSF CD8+ to CD4+ T cells, and activation of inflammatory pathways. CSF, but not plasma Dopa Decarboxylase (DDC) levels were increased. Plasma neurofilament light chain (NfL) was increased, and there was a trend towards an increase in glial fibrillary acidic protein (GFAP). Participants diagnosed with PD or DLB during 4 years of follow-up all met MDS research criteria for prodromal PD, and had lower average MoCA scores than non-converters.
Conclusions: Our preliminary data supports conduct of a clinical trial of an anti-TNFα antibody in hyposmic RBD subjects, with the outcomes focused on whole-brain metabolic activity measured by FDG-PET, a comprehensive clinical outcome measure that accounts for potential cognitive as well as motor progression in this population and a biomarker focus on synaptic and axonal degeneration and glial activation.
P37.25
1 University of Kansas Medical Center, United States
2 University of Arkansas for Medical Sciences, United States
3 Cleveland Clinic Lou Ruvo Center for Brain Health, United States
4 Baylor College of Medicine, United States
5 Outpatient Clinic for Parkinson, Movement Disorders, Neurology, and Psychiatry, Germany
6 Bain Capital Life Sciences Investors, United States
7 Merida Biosciences, United States
8 AbbVie, Inc., United States
Introduction: Tavapadon, an oral, once-daily, selective D1/D5 agonist, demonstrated improvements in Parkinson’s disease (PD) motor symptoms with a tolerable safety profile over 27 weeks of treatment in phase 3 studies of adults with early PD (<3 years’ duration; TEMPO-1 [NCT04201093], TEMPO-2 [NCT04223193]) and PD with motor fluctuations (≥2.5 hours of daily OFF time; TEMPO-3 [NCT04542499]). The TEMPO-4 trial (NCT04760769) evaluated the long-term safety and efficacy of tavapadon in adults with PD.
Methods: Participants who completed the TEMPO-1, TEMPO-2, or TEMPO-3 trial, as well as newly enrolled participants with PD (modified Hoehn and Yahr stage 1, 1.5, 2, 2.5, or 3) on a stable dose of levodopa were enrolled in the phase 3, open-label TEMPO-4 trial. Participants received tavapadon (5 to 15 mg once daily) for up to 58 weeks (85 total weeks of exposure for those who had previously received tavapadon in the TEMPO-1, -2, and -3 trials), followed by a 10-day safety/withdrawal assessment period and 20-day safety follow-up period.
Results: Of 992 enrolled participants, 468 had previously received tavapadon in the TEMPO-1, -2, and -3 trials; 524 were previously untreated (placebo rollover, n=471; newly enrolled, n=53). In this interim analysis, 484 (48.8%) participants completed the study, 223 (22.5%) were receiving treatment, and 285 (28.7%) discontinued treatment. Adverse events (AEs; n=136 [13.7%]) and withdrawal by subject (n=71 [7.2%]) were the most common reasons for treatment discontinuation. The safety profile was consistent with previous studies; most AEs were non-serious and mild-to-moderate in severity (Table 1). There were low rates of AEs of interest , including AEs associated with currently approved D2/D3 receptor agonists. No new safety concerns were identified, including vital signs, laboratory/electrocardiogram results, or Columbia-Suicide Severity Rating Scale scores. Participants who received tavapadon in the TEMPO-1, -2, and -3 trials had stable improvements in motor function with continued tavapadon treatment. Placebo rollover and de novo participants showed motor improvements, which remained stable with continued treatment over 58 weeks.
Conclusions: This interim analysis demonstrated that tavapadon has a favorable long-term safety profile and provides stable efficacy with continued treatment. Selective D1/D5 agonism may offer a differentiated safety profile compared with D2/D3 agonists, as supported by the low rates of AEs of interest.

P37.26
1 Houston Methodist Neurological Institute, United States
2 Texas Movement Disorder Specialists, United States
3 AbbVie, Inc., United States
4 University of Arkansas for Medical Sciences, United States
Introduction: Tavapadon, an oral, once-daily, selective D1/D5 agonist, demonstrated improvements in Parkinson’s disease (PD) motor symptoms with a tolerable safety profile over 27 weeks of treatment in phase 3 studies of adults with early PD (<3 years’ duration; TEMPO-1 [NCT04201093] and TEMPO-2 [NCT04223193]) and PD with uncontrolled motor fluctuations (TEMPO-3 [NCT0452499]). Tavapadon also provided sustained efficacy in TEMPO-4 (NCT04760769), a 58-week phase 3, open-label extension trial. Sustained control of PD symptoms with tavapadon may delay levodopa initiation or lessen the need for levodopa dose increases when used as monotherapy or adjunct therapy, respectively, and possibly lower the risk of motor complications associated with long-term use of oral levodopa. This study assessed changes in levodopa use among people with PD receiving tavapadon in the TEMPO-4 trial.
Methods: Levodopa-naïve participants from TEMPO-1 and TEMPO-2, participants on a stable dose of levodopa from TEMPO-3, and newly enrolled participants with PD receiving stable levodopa treatment were enrolled in the TEMPO-4 trial (85 total weeks of exposure for participants who had previously received tavapadon in the TEMPO-1, -2, and -3 trials). This post hoc analysis evaluated initiation of levodopa in participants enrolled from TEMPO-1 and TEMPO-2, and levodopa dose modifications in participants enrolled from TEMPO-3 and newly enrolled participants.
Results: Treatment with tavapadon was associated with a stable levodopa dose or decreased need for levodopa across the TEMPO trials. Most participants (86.4% to 94.0%) in the early PD cohorts (TEMPO-1 and TEMPO-2 extensions) did not initiate levodopa during the treatment period (previously treated, 85 weeks of treatment; previously untreated, 58 weeks of treatment). Participants who were already receiving tavapadon adjunctive to levodopa (TEMPO-3 extension or newly enrolled participants) rarely required dose modifications. Most participants (81.3% to 87.6%) maintained a stable levodopa dose. When adjustments were required, participants were twice as likely to lower their levodopa dose (∼10%) than to escalate the dose (∼5%); the mean daily levodopa doses remained below 1000 mg.
Conclusions: Approximately 90% of tavapadon-treated participants did not need levodopa initiation or dose increases after a total of 14-20 months of treatment.
P37.27
1 University of Kansas Medical Center, United States
2 Cleveland Clinic Nevada, United States
3 Houston Methodist Hospital, United States
4 AbbVie, Inc., United States
5 University of South Florida, United States
Introduction: In phase 3 studies, tavapadon, an oral, once-daily, selective D1/D5 agonist, improved Parkinson’s disease (PD) motor symptoms with an acceptable safety profile. Currently approved dopamine agonists have a higher risk of daytime sleepiness, partly due to activation of extrastriatal-D2/D3 receptors. Selective activation of D1/D5 receptors with tavapadon may avoid excessive daytime sleepiness; however, this hypothesis has not been evaluated. Here, daytime sleepiness was assessed in people with PD treated with tavapadon across three phase 3 studies (TEMPO-1, TEMPO-2, TEMPO-3).
Methods: In TEMPO-1 (NCT04201093) and TEMPO-2 (NCT04223193), people with early PD (<3 years’ duration) received monotherapy with fixed-dose (5 or 15 mg) or flexible-dose tavapadon (5 to 15 mg), respectively. In TEMPO-3 (NCT04542499), people with PD experiencing motor fluctuations (≥2.5 hours of daily OFF time) received flexible-dose tavapadon (5 to 15 mg) adjunctive to levodopa. Daytime sleepiness was assessed using the Epworth Sleepiness Scale (ESS), which measures the probability of falling asleep during common activities. Total scores range from 0 to 24; higher scores denote greater sleepiness.
Results: Mean ESS total scores were stable over time, with no difference between tavapadon (TEMPO-1: n=177 for both doses; TEMPO-2: n=151; TEMPO-3: n=251; Figure 1) and placebo (TEMPO-1: n=175; TEMPO-2: n=153; TEMPO-3: n=254). In TEMPO-1, least squares mean (LSM) changes from baseline to Week 27 in ESS total score were −0.4 point with placebo, −0.7 with 5-mg tavapadon, and −0.4 with 15-mg tavapadon (LSM difference from placebo [95% CI], −0.2 [−0.9, 0.4] for 5 mg [P=0.44] and 0.0 [−0.6, 0.7] for 15 mg [P=0.91]). In TEMPO-2, LSM change in ESS total score from baseline was -0.3 point with placebo and -0.3 with tavapadon (LSM difference from placebo [95% CI], 0.0 [−0.6, 0.6]; P=0.94). In TEMPO-3, LSM change in ESS total score from baseline was -0.7 point with placebo and -0.9 with tavapadon (LSM difference from placebo [95% CI], −0.2 [−0.8, 0.4]; P=0.53). Item-level scores related to sleepiness on the Movement Disorder Society-Unified Parkinson’s Disorder Rating Scale and Parkinson’s Disease Questionnaire-39 were similar in both groups.
Conclusions: In the phase 3 studies, tavapadon did not increase daytime sleepiness compared to placebo over 27 weeks. These findings suggest selectively targeting D1/D5 receptors may avoid excessive daytime sleepiness.
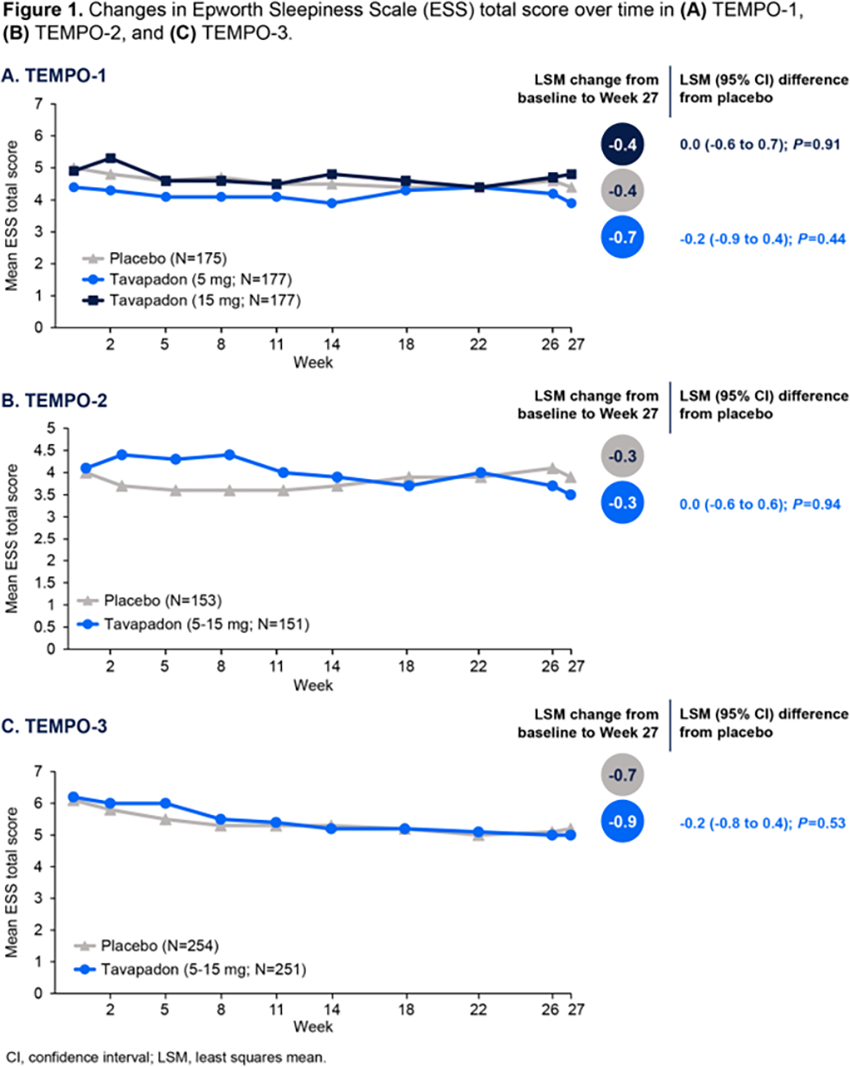
P37.28
1 Centre Hospitalier Universitaire of Grenoble, France
2 Booth Gardner Parkinson’s Care Center at Evergreen Health Medical Center, United States
3 AbbVie, Inc., United States
Introduction: In phase 3 studies, tavapadon, an oral, once-daily, selective D1/D5 agonist, provided significant improvements in Movement Disorder Society-Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Parts II/III scores, indicating experiences of daily living related to motor function and clinician-assessed motor function, respectively. This analysis assessed the effect of tavapadon on specific PD symptoms for which participants experienced impairments at baseline in people with early Parkinson’s disease (PD; TEMPO-1 [NCT04201093] and TEMPO-2 [NCT04223193]).
Methods: Participants with early PD (<3 years’ duration) received monotherapy with fixed-dose (5 or 15 mg, TEMPO-1) or flexible-dose tavapadon (5 to 15 mg, TEMPO-2) once daily for 27 weeks. This post hoc analysis assessed improvements in individual MDS-UPDRS item scores from baseline to Week 26. The proportion of participants with impairments at baseline (ie, score ≥1) who experienced either treatment response (≥1-point improvement) or symptom resolution (score of 0) was evaluated.
Results: Participants treated with tavapadon experienced greater improvements in MDS-UPDRS Parts II/III items for which participants reported baseline impairments versus placebo. For example, in TEMPO-2, tavapadon led to significantly greater improvements in body bradykinesia (the MDS-UPDRS item for which the largest number of participants reported baseline impairments) versus placebo (LSM [95% CI] difference from placebo, −0.5 [−0.6, −0.3]; P<0.0001). Additionally, a greater proportion of participants treated with tavapadon reported a ≥1-point improvement or resolution of symptoms at Week 26 compared to placebo-treated participants. For body bradykinesia, 30.4% of tavapadon-treated TEMPO-2 participants with impairments at baseline reported resolution of symptoms, and 46.7% reported a ≥1-point improvement, compared to 7.3% and 20.3% of placebo-treated participants, respectively. Tavapadon-treated participants in TEMPO-1 reported similar improvements in body bradykinesia (placebo, 20.3% response, 7.5% resolution; 5-mg tavapadon, 49.6% response, 23.1% resolution; 15-mg tavapadon, 52.4% response, 29.5% resolution).
Conclusions: Tavapadon-treated participants with baseline motor impairments experienced greater improvements in MDS-UPDRS Parts II/III scores or resolution of PD symptoms compared with placebo-treated participants.
P37.29
1 Baptist Health South Florida Miami Neuroscience Institute and Florida International University, United States
2 AbbVie, Inc., United States
3 Neuro Pain Medical Center, United States
Introduction: Tavapadon, an oral, once-daily, selective D1/D5 agonist, demonstrated improvements in Parkinson’s disease (PD) motor symptoms with a tolerable safety profile in two phase 3 studies in people with early PD (TEMPO-1 [NCT04201093] and TEMPO-2 [NCT04223193]). Tremor is among the most troublesome symptoms for people with early PD. This study assessed the impact of tavapadon on tremor in early PD using items on the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS).
Methods: Participants with early PD (<3 years’ disease duration) were randomized to receive tavapadon (TEMPO-1: fixed dose of 5 or 15 mg once daily; TEMPO-2: flexible dose of 5-15 mg once daily) or placebo for 27 weeks. This post hoc analysis assessed the impact of tavapadon on tremor, as evaluated by MDS-UPDRS Part II Item 10 (patient experiences of tremor) and Part III Items 15A-18 (clinician-assessed postural tremor, kinetic tremor, rest tremor amplitude, and rest tremor consistency).
Results: Treatment with tavapadon resulted in significant improvements in patient experiences of tremor (Part II) compared with placebo (Figure). In TEMPO-2 (N=304), improvements in tremor scores were greater with tavapadon at Week 26 (32%) versus placebo (6%; least squares mean [LSM] change from baseline: placebo, 0.0; 5-15 mg tavapadon, -0.4; LSM difference from placebo [95% CI], -0.3 [-0.5, -0.2]; P<0.0001). Of TEMPO-2 participants who experienced baseline tremor-related impairment (ie, score ≥1), a greater proportion of participants who received tavapadon reported ≥1-point improvement at Week 26 (45.2%) compared with placebo (23.3%). Additionally, more participants in the tavapadon group (26.2%) experienced resolution of symptoms (ie, score of 0) versus placebo (7.5%). Similar trends were reported in TEMPO-1 (N=529). Tavapadon treatment resulted in significant improvements in most clinician-assessed tremor items (Part III) compared with placebo (Figure; TEMPO-1: 5/10 items; TEMPO-2: 7/10 items); items that did not attain significance generally had low scores at baseline (ie, median score of 0 or 1).
Conclusions: Tavapadon demonstrated improvements in tremor in people with early PD, based on several tremor-related assessments measured with the MDS-UPDRS.
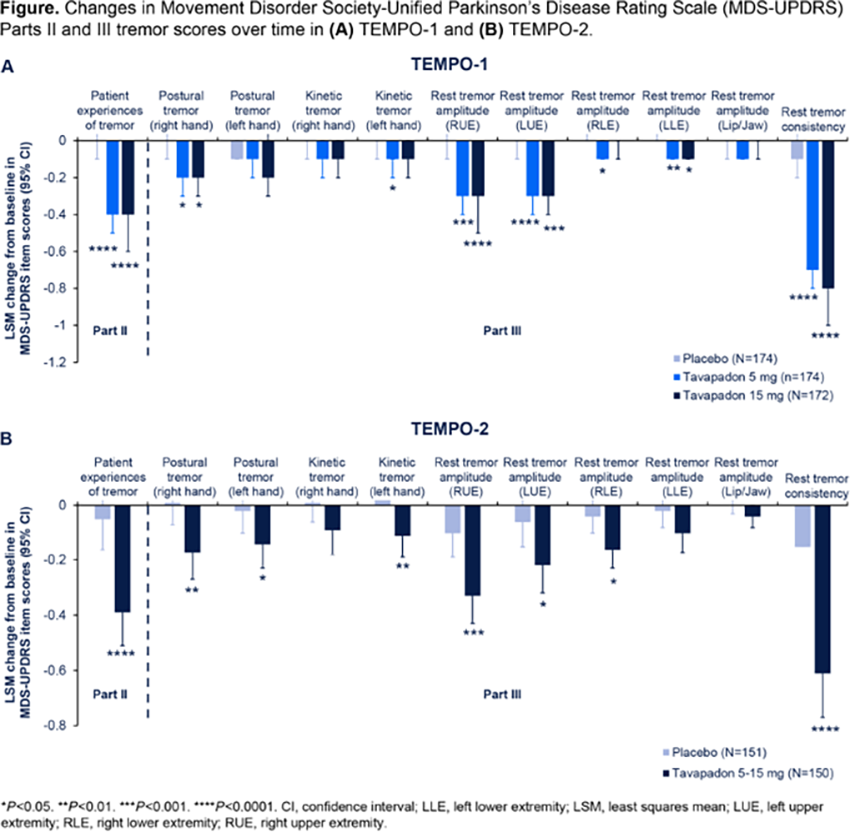
P37.30
1 Navitas Clinical Research, United States
The Parkinson’s Foundation (PF)’s mission is to improve care for people with Parkinson’s disease (PD) by advancing research towards a cure. PF leads an international, multi-site registry program called PD GENEration that offers genetic testing for several PD related genes and genetic counseling. The study operates as a de-centralized trial by allowing enrollment of participants by local clinical sites, or by participant self-referral through centralized supersites that coordinate sample collection and genetic counseling in a remote manner. PD GENEration has enrolled a total of 28,993 patients across the US, Canada, Israel, and Central and South America as of Oct 16, 2025. Navitas Clinical Research (NCR) is the Coordinating Center providing clinical operation and data management support to PF. Given the large number of sites, high enrollment, and the hybrid nature of this unique registry trial, NCR applies a risk-based quality management (RB-QM) approach for PD GENEration to achieve high quality for critical data. Key considerations for NCR’s RB-QM approach include identifying critical data elements that require targeted review for quality, leveraging centralized monitoring and trend analysis to gain insights to site performance, and developing a site communication plan tailored to address key performance indicators. High loss to follow-up (LTFU) rates in the study impact performance milestones and diversity initiatives. Using RB-QM strategies, PF and NCR can identify sites that require increased support to address LTFU participants and implement mitigation strategies. As part of a protocol amendment in March 2024, sample analysis using whole genome sequencing (WGS) was initiated. On Feb 3, 2025, 1,876 total participants were enrolled to the WGS protocol with an overall 6% LTFU rate across all sites enrolling under the WGS protocol. Nine sites had a LTFU rate greater than 10%. The majority of LTFU participants were assigned to have genetic counseling done remotely. On Aug 4, 2025, 5,454 participants were enrolled to the WGS protocol, and the overall LTFU rate decreased to 3.6%. The LTFU rate for 5 of the 9 sites was less than 10%. NCR utilized tailored data summary reports to identify sites with high LTFU rates and provided participant-level guidance to sites as a mitigation strategy in conjunction with the PF research coordinator team. Use of RB-QM procedures was instrumental in identifying key action steps to reduce LTFU in this large genetic registry.
P37.31
1 Insightec, United States
2 Insightec, Spain
3 Insightec, Netherlands
Introduction: As Parkinson’s disease (PD) progresses, dyskinesia and motor fluctuations emerge and further develop despite optimized medical therapy, leading to reduced quality of life. Magnetic resonance-guided focused ultrasound (MRgFUS) is an incisionless technique that enables precise targeting of the pallidothalamic tract at the H1/Field of Forel, offering a novel alternative for PD patients with motor complications. This study investigates the safety and efficacy of staged, bilateral MRgFUS pallidothalamic tractotomy (PTT) in patients with PD experiencing motor complications in a multicenter, phase III trial. This study led to recent FDA approval as a treatment in advanced Parkinson’s disease.
Methods: This prospective, open-label, single-arm trial (NCT04728295) enrolled 84 subjects across nine international centers. Eligible participants (≥30 years old) with PD and motor complications underwent unilateral MRgFUS PTT, followed by staged bilateral treatment at least 6 months later, if eligible. Primary efficacy was assessed by change in MDS-UPDRS Part III OFF (upper and lower extremity score) 3 months after staged, bilateral treatment. Secondary outcomes included MDS-UPDRS Part IV and total Part III OFF scores. Safety was evaluated through treatment-emergent adverse events.
Results: Fifty-four received unilateral treatment; 40 proceeded to bilateral. At 3 months post-unilateral treatment, Part III OFF (treated side) improved by 50% (20.9 ± 5.3 to 10.0 ± 5.4), and Part IV by 56.3% (10.5 ± 3.5 to 4.6 ± 3.7). Following bilateral treatment, bilateral extremity scores improved by 34%, total Part III OFF by 32% (51.3 ± 12.4 to 33.4 ± 11.4), and Part IV by 68% (10.7 ± 3.2 to 3.6 ± 2.9), all statistically significant (p < 0.0001). Improvements were sustained through 12 months’ post bilateral procedure. Adverse events were mostly mild or moderate. After unilateral treatment, 30 related events occurred in 21 subjects (87% mild); after bilateral treatment, 43 events occurred in 22 subjects (70% mild, 2% severe). Common events included imbalance, dysarthria, and fatigue.
Conclusions: Trial results show significant reductions in MDS UPDRS Part III OFF medication as well as in MDS UPDRS Part IV ON medication. These results may help guide clinicians and patients as to selection and expectation for those who choose this procedure. Overall, staged, bilateral PTT MRgFUS is a safe and efficacious option for advanced PD patients with motor complications.
P37.32
1 Critical Path Institute, United States
2 University of Rochester, United States
3 Parkinson's UK, United Kingdom
4 Parkinson's Research Advocate, United States
5 University of Arizona, United States
6 University of Tubingen, Germany
7 Patient Researcher Advocate, United States
8 Qairmel, France
9 My Moves Matter, Ireland
10 JPG Enterprises, United States
11 University College London, United Kingdom
12 University of Oxford, United Kingdom
13 Parkinson's Researcher Advocate, United Kingdom
14 Michael J Fox Foundation, United States
15 Parkinson's Researcher Advocate & Public Health Consultant, United Kingdom
16 UnshakableMD, Canada
17 Cure Parkinson's, United Kingdom
18 Northwestern University, United States
19 UCLA, United States
20 University of California San Francisco, United States
21 Patient Researcher Advocate and advisor, United States
Background: The lived experience of women with Parkinson’s Disease (PD) is different from men with emerging scientific research demonstrating true biological differences based on sex/gender. Studies have shown that women tend to have poorer health-related quality of life, more psychological distress and disability. Development of effective therapies for Parkinson’s has not been focused on the underlying symptoms and unique needs of women.
Worldwide collaborative initiatives are needed to advance new tools to inform drug development decision-making as well as to meet the needs of all affected by PD. The Critical Path for Parkinson’s (CPP) consortium, a public private partnership sponsored by Critical Path Institute consists of global nonprofit organizations, academic experts, patient advocates and industry with the goal of advancing innovative new tools to optimize clinical trials.
Objectives: To present Critical Path Institute’s recently launched Global Evidence in Medicine (GEM-PD), a pre-competitive worldwide network and describe how all stakeholders are working together to advance the unique needs of women with PD.
Methods: The strategy includes near term focus on the following goals (1) interrogating diverse datasets to uncover sex-specific insights in ; (2) modeling disease progression; and (3) evaluating digital health technology platforms and analyzing real-world data sources to capture outcomes meaningful to women with PD.
Results: The GEM-PD initiative was launched in 2025 in the spring in affiliation with ADPD2025 and in the fall at the C-Path global summit. In both forums, women with PD shared their personal experiences with diagnosis, symptoms and impacts, and healthcare, grounding the initiative in lived experience perspectives. Attendees at the EU launch emphasized urgent gaps and outlined a renewed call to action (Subramanian et al., Movement Disorders, Vol. 37 (3), 444, 2022), including the need to identify additional data sources beyond CPP’s Integrated Parkinson’s Database of more than 15,000 patient-level records to ensure the analysis of comprehensive biological information.
Conclusions: The information gathered from GEM-PD will apply five core competencies of C-Path In data and regulatory science, quantitative modeling, patient focused drug development, and digital health technologies to advance the inclusion of women in clinical trials and define novel innovative strategies to meet their needs.
P37.33
1 University of Rochester, United States
2 University of Rochester Medical Center, United States
3 Michael J. Fox Foundation, United States
4 Northwestern University, United States
5 Massachusetts General Hospital, United States
6 University of Pennsylvania, United States
7 University of Rochester Medical Center; Eli Lilly, United States
8 Harvard T.H. Chan School of Public Health, United States
9 University of Cincinnati Medical Center, United States
10 University of California, San Francisco, United States
11 Parkinson's Foundation, United States
12 Sage Bionetworks, United States
13 Atria Research and Global Health Institute; University of Rochester Medical Center, United States
INTRODUCTION: Remote, decentralized research studies are ideal for the study of mid-stage Parkinson’s disease (PD) as they enable collection of data from the home environment and at a stage when advancing disease may limit in-person research participation.
METHODS: Assessing Tele-Health Outcomes in Multiyear Extensions of Parkinson Disease Trials–2 (AT-HOME PD2) is a decentralized observational study of mid-stage PD designed to evaluate whether digital health technologies can improve prediction of falls and cognitive impairment. AT-HOME PD2 participants were recruited from AT-HOME PD, an observational study of participants from two phase III clinical trials (STEADY-PD III and SURE-PD3), and from PD GENEration, an on-going genetic registry study. Participants complete bi-annual video visits, quarterly smartphone-based motor assessments (mPower 2.0 or Koneksa Health apps), quarterly online surveys (Fox Insight), monthly wear of two accelerometers (ActiGraph CentrePoint® Insight Watch and Fitbit Charge 5), and weekly reporting of falls for up to 36 months. Here, we report recruitment metrics, baseline characteristics, and initial adherence with wearables.
RESULTS: The study enrolled 200 participants between October 2023 and April 2025. Breakdown of the “feeder” cohorts was as follows: AT-HOME PD (111, 56%), PD GENEration (72, 36%), STEADY-PD III only (9, 4.5%), and SURE-PD3 only (8, 4%). Participants reside in 35 US states, one US federal district, and one Canadian province. Baseline characteristics were 113 (57%) male, 194 (97%) White, mean (SD) age 69.0 ± 8.5 years, PD duration 8.9 ± 1.5 years, modified MDS-UPDRS Part 3 25.6 ± 9.7, and Montreal Cognitive Assessment 27.3 ± 2.5. Fifty-one (26%) participants reported ≥ one fall in the month prior to enrollment. At the first follow-up visit (n=182), 51% reported always and 45% sometimes complying with Fitbit wear, and 44% always and 53% sometimes complying with ActiGraph wear.
CONCLUSIONS: AT-HOME PD2 is a fully decentralized study. The fully enrolled cohort represents a mid-stage PD population, which has not been assessed with multi-modal digital measures in a structured, longitudinal way previously. Early adherence with monthly wear of wrist-worn accelerometers has been excellent. Upon completion of follow-up, the cohort will have undergone up to three years of comprehensive clinical and digital phenotyping, enabling examination of important mid-stage PD clinical milestones and their precedents.
P37.34
1 ASU College of Health Solutions, United States
2 NYU Grossman Long Island School of Medicine, United States
Background: Automaticity of gait is negatively affected in people with Parkinson’s disease (PwPD), increasing fall-risk and reducing overall mobility. Performing a secondary task during gait requires additional attentional demands, further compromising gait and increasing fall-risk for PwPD. Previous reports have shown that gait is related to global cognition. However, the specific cognitive domains associated with dual-task (DT) gait speed are unclear. Identifying cognitive domains that relate to DT gait can improve our understanding of why DT gait is impacted and guide interventions to improve mobility and reduce falls. Thus the purpose of this analysis is to determine the relationship between specific cognitive domains and DT gait speed in PwPD.
Methods: 74 PwPD completed cognitive assessments that measured global cognition, as well as 7 sub-domains (measured via the NeuroTrax cognitive battery): executive function, attention, visual spatial processing, verbal function, information processing, memory and motor skills. Gait was assessed under DT conditions involving serial subtraction (by 3’s and 7’s) and verbal fluency (animal naming) while walking at a comfortable pace. The primary gait outcomes were single-task (ST) gait speed and DT gait speed. A general linear model controlling for age and disease severity (Hoehn & Yahr Stage) assessed the associations among cognitive domains and ST and DT gait speed.
Results: Consistent with previous work, global cognition was positively correlated to DT gait speed (t = 2.15; p < 0.03). Regarding relationships with cognitive sub-domains; visual spatial processing was positively associated with ST gait speed (t = 2.32; p < 002) and DT gait speed (t = 2.83; p < 0.01), accounting for age and disease severity.
Discussion: Our findings confirm previous work that showed global cognition is related to gait speed. Specifically, when accounting for age and disease severity, global cognition and DT gait speed were significantly related. We then extended previous findings by looking at how specific cognitive subdomains relate to gait, observing that the visual spatial processing cognitive subdomain was most closely related to gait in PwPD. These findings suggest that visual spatial processing contributes to gait in PwPD, but that DT gait relies on the integration of multiple cognitive systems. Further investigation into this relationship may inform fall risk screenings and future fall prevention interventions for PwPD.
P37.35
1 São Paulo State University, Brazil
Individuals with Parkinson’s disease (PD) present impairments in postural control, often characterized by increased body sway. These impairments result from cortical and subcortical dysfunctions involved in postural regulation. As task complexity increases (e.g., standing on an unstable surface), greater recruitment of cortical regions occurs, including the prefrontal cortex (PFC) and the primary motor cortex (M1). To improve postural control, complementary therapies such as transcranial direct current stimulation (tDCS), motor exercises, and their combination have been explored. Despite promising results, the effects of this combination on postural control remain unclear. This randomized clinical trial aimed to analyze the effects of multiple sessions of multi-target tDCS combined with motor exercises on postural control on firm and foam surfaces in individuals with PD. Participants with mild to moderate PD were allocated into two groups: experimental (EG: n=7; 62.22±23.15 yrs) and control (CG: n=6; 64.53±15.37 yrs). The intervention protocol consisted of 10 sessions, conducted twice a week on non-consecutive days, involving exercises focused on balance and locomotion combined with tDCS. Each session lasted 30 minutes: 5 minutes of warm-up, 20 minutes of main exercises with tDCS, and 5 minutes of cool-down. The EG received active tDCS (2 mA, 20 minutes), while the CG received sham tDCS (30 seconds). Stimulation was applied simultaneously over M1 and PFC. Postural control was assessed using inertial sensors (Opal, APDM) and Mobility Lab™ software in bipedal stance on firm and foam surfaces. Three 30-second trials were performed for each condition. Body sway variables included mean velocity, root mean square in the anteroposterior direction, and sway area. Assessments were conducted before, 24h after the last session, and one-month post-intervention. Two-way ANOVAs with repeated measures revealed a main effect of moment for sway area (F2,22=5.549; p=0.011) during the firm-surface condition, indicating reduced sway area at post compared with pre-test (p=0.016) in both groups. These preliminary findings suggest improvements in postural control, reflected by a decrease in postural sway in individuals with PD after motor exercise, regardless of tDCS. Data collection is ongoing to expand the sample and reassess the effects of the intervention. This study was supported by the São Paulo Research Foundation (FAPESP #2025/00789-0; #2023/12924-4).
P37.36
1 São Paulo State University (Unesp), School of Technology and Sciences, Presidente Prudente., Brazil
2 São Paulo State University (Unesp), School of Technology and Sciences, Presidente Prudente, Brazil
People with Parkinson’s disease (PwPD) exhibit impairments in gait parameters, especially in challenging situations such as walking at a fast speed. Transcranial direct current stimulation (tDCS) appears to enhance the effects of physical exercise on locomotion in PwPD. However, the characteristics of tDCS (e.g., electrode placement and stimulation site) may influence this synergistic effect. Therefore, clinical trials combining motor exercises with tDCS applied simultaneously to cortical areas involved in locomotor control (e.g., primary motor cortex – M1 and prefrontal cortex – PFC) are needed to establish specific protocols that optimize its benefits. This study aimed to analyze the effects of combining multi-target tDCS with motor exercises on gait parameters during fast walking in PwPD. Preliminary data from this randomized clinical trial include 13 participants with mild to moderate disease severity, distributed into two groups: experimental (EG) and control (CG). Each group completed 10 sessions (twice weekly, 30 min) involving balance and locomotion exercises combined with tDCS over M1 and PFC. The EG received active stimulation (2 mA, during the central 20 minutes of the exercise protocol), while the CG received sham stimulation (2 mA, 30 seconds). Gait assessment was performed before (pre-test), immediately after the intervention (post-test), and at ∼1-month follow-up. Participants walked for thirty seconds at a fast speed back and forth along a 14-meter path, completing 180° turns at each end. Three trials were conducted. Gait parameters were measured using inertial sensors (Opal, APDM) and Mobility Lab™ software. Results from two-way repeated-measures ANOVA revealed a main effect of time for walking cadence (F2,22 = 5.241, p = 0.014) and step duration (F2,22 = 4.841, p = 0.018). Regardless of the tDCS condition, PwPD showed increased cadence at post-test (p = 0.030) and follow-up (p = 0.030) compared to pre-test, and decreased step duration at post-test (p = 0.033) and follow-up (p = 0.044). These preliminary findings suggest improvements in gait parameters during fast walking, regardless of tDCS. Thus, multi-target tDCS did not enhance the effects of motor exercise on gait in PwPD. However, data collection is ongoing to expand the sample. This study was supported by the São Paulo Research Foundation (FAPESP #2023/12924-4).
P37.37
1 Remepy Health Ltd., United States
2 Remepy Health Ltd., Israel
3 Reichman University, Israel
Objective: We aimed to evaluate the efficacy of DopApp, a mobile digital therapeutic used alongside levodopa, as a hybrid intervention across Parkinson’s disease (PD) stages.
Background: Despite available pharmacological treatments, PD patients face persistent challenges in symptom control, safety, and treatment duration. Notably, in more advanced PD, adjunctive treatments to levodopa often improve ON/OFF states without significantly affecting MDS-UPDRS scores.
Methods: Forty-two PD patients treated with levodopa participated in a prospective, double-blind, randomized, placebo-controlled trial. The 3-week digital treatment (DopApp) included a proprietary daily protocol of brief interactive interventions, including multisensory motor, psychological, and cognitive training. Patients were assessed pre- and post-treatment using clinical and psychological scales. The primary endpoint was the change in total MDS-UPDRS (sections 1+2+3). Subgroup analyses stratified patients by age, baseline MDS-UPDRS (high vs. low), PD duration, and daily levodopa dose, assessing MDS-UPDRS change.
Results: DopApp led to both significant and clinically meaningful improvements in MDS-UPDRS score compared to placebo (inter-group difference of 7.8 points, p=0.0005). Subgroup analyses showed that the treatment led to meaningful improvements in MDS-UPDRS scores across all baseline subgroups, indicating consistent effects across various stages of the disease. Notably, the treatment resulted in substantial reductions in symptom severity among patients with more advanced PD, including those with higher baseline MDS-UPDRS scores, longer disease duration, and greater medication dosage. Importantly, despite a mean age of 67 and the presence of motor impairments, adherence to the intervention was high (95.5±5.2% completion of treatment protocol), and participants reported a positive and engaging experience with DopApp.
Conclusion: Hybrid treatment with DopApp and levodopa improved both motor and psychiatric domains in PD. Critically, benefits were consistent across disease stages, including in more advanced patients, where previous adjunctive drug studies failed to impact MDS-UPDRS scores. High adherence rates suggest that neither digital literacy nor physical limitations posed substantial barriers in this population.
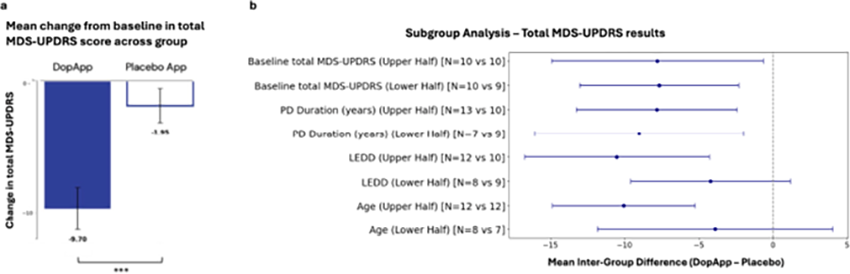
P37.38
1 Cooper University Hospital, United States
OBJECTIVE: To evaluate the efficacy of probiotics in alleviating gastrointestinal symptoms and motor outcomes in patients with Parkinson’s disease (PD). BACKGROUND: Constipation and gut dysbiosis are prevalent non-motor symptoms in PD, contributing to reduced quality of life and possibly influencing disease progression. Probiotics have been proposed as a therapeutic strategy to restore gut microbiota balance and improve bowel function, yet evidence remains fragmented. DESIGN/METHODS: We conducted a systematic review and meta-analysis of placebo-controlled randomized trials indexed in PubMed. Eligible studies compared probiotics to placebo in PD patients. Outcomes included complete bowel movements (CBM) per week, Bristol Stool Scale (BSS), Patient Assessment of Constipation Quality of Life (PAC-QOL), and Unified Parkinson’s Disease Rating Scale part III (UPDRS-III). Random-effects models were applied to calculate pooled mean differences (MD) with 95% confidence intervals (CI). RESULTS: Five trials met inclusion criteria. Probiotics significantly increased CBM/week (MD = 1.34, 95% CI [1.04, 1.64], p < 0.001) and improved stool consistency (BSS score: MD = 0.59, 95% CI [0.36, 0.81], p < 0.001). Quality of life related to constipation improved markedly (PAC-QOL: MD = –14.19, 95% CI [–19.16, –9.22], p < 0.001). No significant effect was observed on motor function (UPDRS-III: MD = –1.50, 95% CI [–4.27, 1.27], p = 0.29). Heterogeneity was low across analyses, and publication bias was minimal.
CONCLUSIONS: Probiotics are effective in improving gastrointestinal symptoms and constipation-related quality of life in PD, with no clear impact on motor outcomes. These findings support probiotics as a safe adjunctive therapy for non-motor symptoms in PD.
P37.39
1 Queensland University of Technology (QUT), Australia
2 UTHealth Houston (The University of Texas Health Science Center at Houston), United States
3 CUNY, The City University of New York, United States
Objective: To investigate the immunomodulatory effects of repeated intravenous (IV) infusions of allogeneic bone marrow-derived mesenchymal stem cells (allo-hMSCs) on peripheral inflammatory markers (IL-6, MCP-1, VEGF) in people with Parkinson’s disease (PD).
Background: Chronic neuroinflammation is a hallmark of PD1 and contributes to dopaminergic neuronal loss and disease progression. Elevated circulating cytokines—particularly IL-62 and MCP-13—along with increased cerebrospinal VEGF, have been consistently reported in PD, reflecting both systemic and central immune activation. Mesenchymal stem cells (MSCs) exert potent immunoregulatory effectsin PD5, however their systemic immunologic effects following repeated IV administration in PD remain incompletely characterized.
Methods: This double-blind, placebo-controlled phase 2 trial enrolled 45 individuals with mild-to-moderate PD (ages 50–79, Hoehn & Yahr stages 1–3). Participants received either: (1) three allo-hMSC infusions (n=16), (2) one placebo followed by two allo-hMSC infusions (n=14), or (3) three placebo infusions (n=15) at 18-week intervals. Serum IL-6, MCP-1, and VEGF levels were quantified at baseline and week 49. Bayesian modeling estimated standardized mean differences (SMD) and posterior probabilities (PP) relative to placebo.
Results: Forty-two participants completed 49 weeks of follow-up. Compared with placebo, three allo-hMSC infusions were associated with reductions in IL-6 (SMD = -0.55, CrI: -3.9 to 2.0, PP = 69.8%), MCP-1 (SMD = -0.99, CrI: -3.7 to 1.7, PP = 77.6%), and VEGF (SMD = -1.02, CrI: -3.9 to 1.6, PP = 78.6%). Two allo-hMSC infusions produced comparable decreases in IL-6 (SMD = -1.0, PP = 80.2%) and MCP-1 (SMD = -0.84, PP = 71.3%), though VEGF levels remained unchanged.
Conclusions: Repeated intravenous allo-hMSC infusions were associated with a systemic shift toward a less pro-inflammatory profile in Parkinson’s disease, consistent with their proposed immunomodulatory mechanism of action. These preliminary findings suggest that allo-hMSCs may mitigate peripheral inflammation—an upstream contributor to neurodegeneration—and underscore the importance of integrating longitudinal cytokine, cellular, and clinical assessments to clarify dose–response relationships and the durability of therapeutic effects.
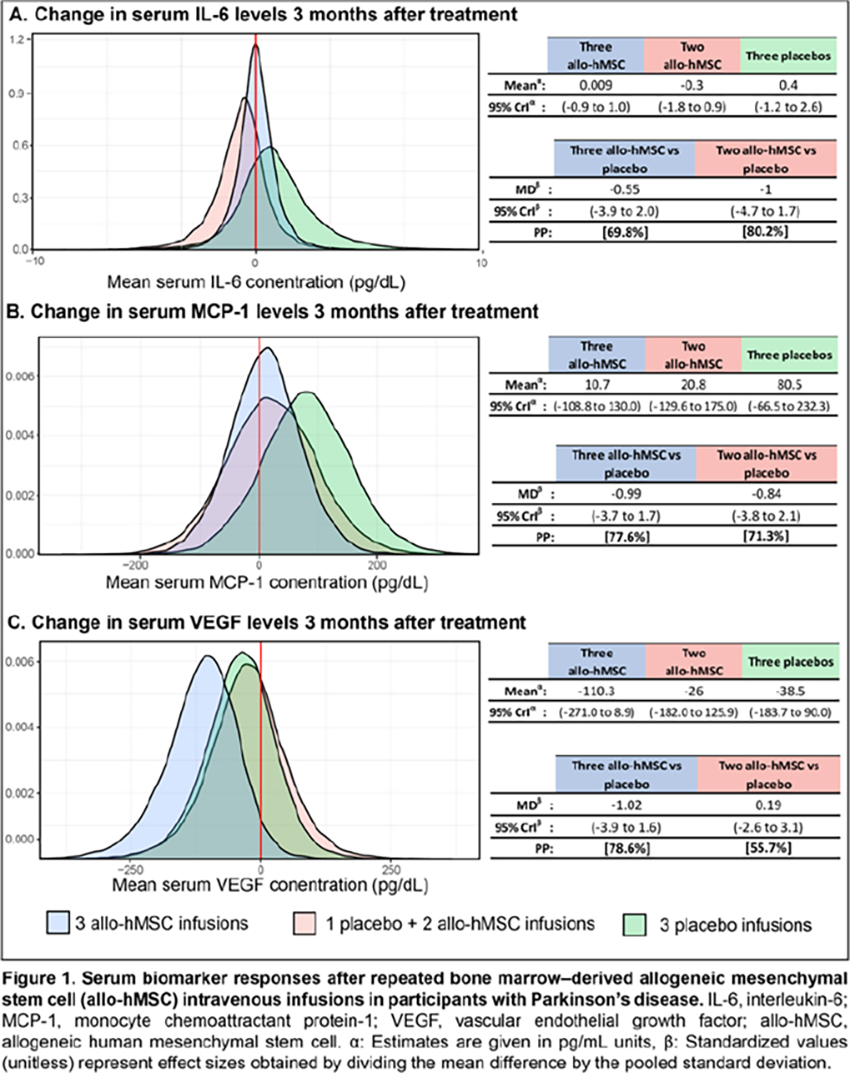
P37.40
1 Newcastle University, United Kingdom
2 Newcastle upon Tyne Hospitals NHS Foundation Trust, United Kingdom
3 Expert by Experience, United Kingdom
4 University College London, United Kingdom
5 MRC Clinical Trials Unit at UCL, United Kingdom
6 County Durham and Darlington NHS Foundation Trust, United Kingdom
Introduction: Identification of participants represents a significant delivery challenge for trials with many studies failing to reach their recruitment targets in time, leading to delays.
For patients, there are often barriers to engaging with research opportunities, due to limited access to research centres and because traditional in-clinic recruitment restricts effective self-referral pathways. The Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) trial sought to improve equitable access and support efficient recruitment through implementation of innovative systems.
Methods: The trial will recruit at >40 centres across the United Kingdom, geographically spread to facilitate access. We created a 2-step web-based system to facilitate potential participant identification and management at study sites: 1) An online self-referral registration of interest (ROI) portal managed through a PD research registry (Join Parkinson's Research registry (JPR@Research+Me)): People with Parkinsons’ (PwP) self-screen key eligibility criteria and select preferred trial sites; demographic data (including age, sex, ethnicity, education, deprivation) are collected. 2) A Recruitment Management System (RMS): Potentially eligible PwP are contacted by their preferred site; site staff can see demographic data to support inclusive recruitment, plan and log telephone pre-screening outcomes and invite potential participants to an in-person screening visit.
Automated ROI and RMS data dashboards facilitate live monitoring of the recruitment pipeline and allow the tracking of impact of targeted trial promotion activities through unique urls to the ROI.
Results: Launch and initial promotion of the ROI through charity mailing lists has led to self-referral of 1039 PwP to the EJS ACT-PD trial within the first week (data cut of 23/10/2025) 992 of which self-screened as potentially eligible representing 62% of the 1600 participant recruitment target.
Conclusion: The EJS ACT-PD web-based recruitment systems represent an important step in facilitating rapid participant identification with inbuilt mechanisms that promote inclusivity. In future, monitoring impact of targeted recruitment strategies and mechanisms in under-served communities will facilitate a shift in focus towards inclusive and representative recruitment.
P37.41
1 Newcastle University, United Kingdom
2 Expert by Experience, United Kingdom
3 University College London, United Kingdom
4 Westborough, United States
5 University of Plymouth, United Kingdom
Introduction: Patient and public involvement and engagement (PPIE) helps develop patient centred, deliverable and accessible research. Evidence is lacking on how PPIE co-design can be best supported in practice. The Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease initiative (EJS ACT-PD) involved over 90 interdisciplinary members, including 13 PPIE contributors, across six working groups (WG) to design a trial of disease modifying therapies in Parkinson’s. An extensive PPIE programme was embedded to support PPIE co-design and evaluate its impact. Here we explore consortium members’ perceptions of PPIE contributions to identify strategies to better support meaningful input.
Methods: Consortium members were sent the Patient Engagement in Research Scale-22 (PEIRS-22) at 12 months following project initiation. PPIE representatives and professional members willing to take part were purposively sampled to reflect a range of PEIRS-22 scores. Topic guides based on the Patient Focused Medicines Development framework and PEIRS-22 domains explored members’ overall PPIE experience and potential areas for improvement. Transcripts were thematically analysed. The PPIE WG extracted, prioritised and discussed actionable results, and developed implementable recommendations for programme improvement.
Results: Nine PPIE representatives and ten professionals participated in interviews. Resulting themes and implementable recommendations included: 1) Enabling contributions - an induction process that introduces the project and clarifies roles, alongside ongoing educational support to build confidence; understanding of representatives’ backgrounds and motivations to enable deployment where it adds value; skilled chairing inviting contribution and checking mutual understanding to support meaningful participation 2) Workload management - transparency about project workload and representatives’ capacity to help planning and task distribution. 3) Feeling valued - transparent communication of decision-making and PPIE impact, with mutual respect and accommodating representatives’ health status to foster feeling valued.
Conclusion: Our PPIE programme evaluation identified simple measures to enhance meaningful contributions that can be applied to future initiatives.
P37.42
1 Newcastle University, United Kingdom
2 Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle, United Kingdom
3 University of Plymouth, United Kingdom
4 Expert by Experience, United Kingdom
5 University College London, Department of Clinical and Movement Neurosciences, London, United Kingdom
6 MRC Clinical Trials Unit at UCL, London, United Kingdom
7 County Durham and Darlington NHS Foundation Trust, Durham, United Kingdom
8 Newcastle University, Translational and Clinical Research Institute, Newcastle, UK; National Institute for Health and Care Research (NIHR) Newcastle Biomedical Research Centre, UK, United Kingdom
Introduction Digital recruitment pathways have potential to support timely trial delivery and improve accessibility to diverse groups of people with Parkinson’s (PwP). The Edmond J. Safra Accelerating Clinical Trials in Parkinson’s disease (EJS ACT-PD) trial is a large platform trial of potentially disease-modifying therapies. To support recruitment, we developed: 1) A web-based Registration of Interest (ROI) portal for PwP that checks potential eligibility; 2) a Recruitment Management System (RMS) that refers potentially eligible PwP to sites and supports site staff telephone pre-screening activities. Exploring and optimising end-user experiences of digital solutions is important to maximise engagement and prevent digital exclusion. Here we share the development of a protocol to optimise the usability of the EJS ACT-PD recruitment systems.
Methods A literature search was conducted to identify frameworks, methodologies and questionnaires for assessing usability of web-based systems and recruitment tools. Methods were reviewed by stakeholder groups (PwP, care partners and trial delivery staff).
Results A mixed methods approach incorporating quantitative and qualitative components was selected to allow for representative feedback and further probing of identified issues. For an evaluation period of up to 3 months, all users (PwP and site staff) of the recruitment portal will be invited to participate in the usability evaluation and complete the modified System Usability Scale (SUS). PwP will additionally answer questions about their registration journey (e.g. data handling, automated messaging). Site staff will complete the Health Information Technology Usability Evaluation Scale (Health- ITUES). Demographic data and a digital literacy assessment will assess participant selection bias. A purposively sampled subset of participants will be invited to semi-structured interviews to explore usability in relation to ageing and disease-related barriers (MOLD-US). Up to three iterative testing cycles will be conducted followed by system optimisation (5-10 users per group) until no significant usability issues remain.
Conclusions This protocol provides a structured framework for evaluating usability of digital recruitment tools. The evaluation will ensure EJS ACT-PD recruitment systems are efficient and accessible. Insights will enhance functionality and user experience for PwP and staff and guide future recruitment system development managed through JPR@Research+Me.
P37.43
1 University of Plymouth, United Kingdom
2 Newcastle University, United Kingdom
3 University of Southampton, National Institute for Health Research, United Kingdom
4 University Hospital Southampton NHS Trust, United Kingdom
5 University of Southampton, NIHR Applied Research Collaborations Wessex, United Kingdom
6 UK Expert by Experience, United Kingdom
7 National Institute for Health Research, Clinical Research Network Wessex, United Kingdom
8 National Institute for Health Research, Clinical Research Network Thames Valley and South Midlands, United Kingdom
9 UK Parkinson’s Clinical Studies Group, United Kingdom
10 Cure Parkinson’s, United Kingdom
11 University College London, United Kingdom
12 University Hospitals Plymouth NHS Trust, United Kingdom
13 Newcastle University, University of Plymouth, United Kingdom
Introduction Few people with Parkinson’s disease (PD) take part in clinical trials due to limited research participation opportunities. This is a particular issue in under-served populations such as coastal and rural communities. The Edmond J Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) trial aims to deliver an inclusive multi-arm multi-stage disease modification trial in PD. We mapped national PD research capability to inform inclusive trial delivery strategies.
Methods We disseminated a survey to UK National Health Service (NHS) hospitals to assess their PD trial experience and capabilities. Sites were categorised into 3 tiers, with tier 1 having the least PD-research capability or experience, and tier 3 being experienced specialist centres. Tiers were mapped to PD prevalence, social deprivation and ethnic diversity to identify infrastructure gaps and trial delivery strategies developed.
Results Tier 3 sites were mostly located in urban centres with higher diversity and social deprivation. A greater proportion of tier 1 and 2 sites were located in areas of higher PD prevalence mostly within rural centres. Challenges identified included a lack of available staff to support trial delivery; less experience with PD-specific and in-person digital outcome measures; very little capacity for overnight accommodation for research participants; a lack of specialist imaging equipment and biomarker capability in tier 1 and 2 sites. Our mitigation strategies therefore included initial trial set-up at tier 3 sites to enable rapid and ethnically diverse recruitment, and core funded staff within strategic sites to develop regional solutions for inclusive trial participation. To enable research opportunity provision in areas where currently very little exists, and to promote retention over the three year study period, a hybrid delivery model of in-person and remote study visits will ensure maximal acceptability and deliverability.
Conclusion By mapping current national PD research delivery capability and experience we were able to identify delivery challenges and mitigate against these by developing a trial delivery strategy that will broaden the provision of research participation opportunity to under-served groups.
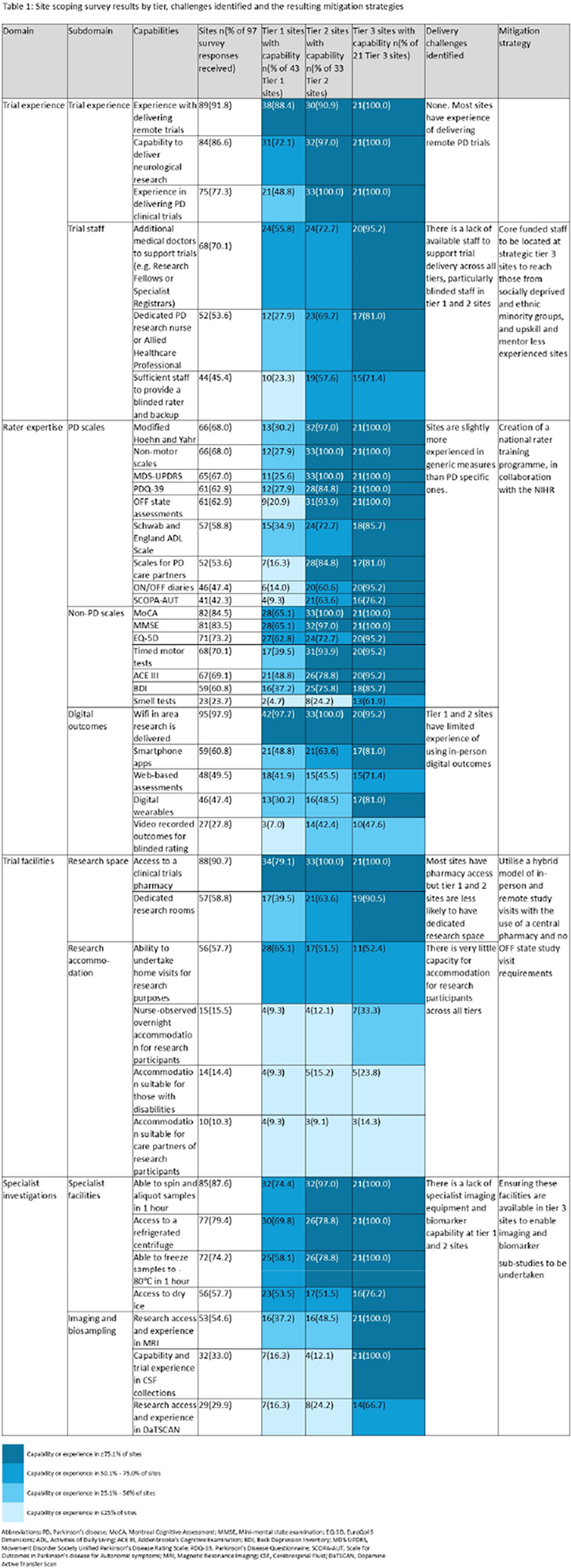
P37.44
1 Oregon Healthy and Science University, Brazil
2 Oregon Healthy and Science University, United States
3 Oregon Healthy and Science University and George Fox University, United States
Introduction. People with Parkinson’s disease (PD) exhibit reduced gait automaticity, which worsens during dual-task (DT) conditions (e.g., walking while performing a cognitive or a motor task). Gait variability measures (i.e., gait cycle, foot strike angle, stride length, etc.), typically higher in people with PD compared to healthy controls, have been used to infer gait automaticity. However, gait variability measures do not capture cortical contributions, such as increased prefrontal cortex (PFC) during walking. In contrast, the DT cost (DTC) of walking, whether for PFC or gait variability, accounts for this and serves as a representative measure of automaticity. Nonetheless, the effects of levodopa on DTC of walking in motor or cognitive DT, remain unclear. We hypothesize that levodopa intake may lead to a greater reduction in DTC of walking.
Objective. To evaluate the effects of Levodopa on DTC of walking using both PFC activity and gait variability in PD.
Methods. Twenty participants with mild-to-moderate PD were tested in their “Off” (after 12 hours of medication washout) and “On” (1 hour after their last dose of medication) conditions on different days. The PFC activity was measured by wireless fNIRS, and gait variability (in single and DT) by wearable sensors. The DTCs, for both PFC activity and gait variability, were calculated as: (dual task−single task)/single task*100. Cohen’s d effect sizes (ES) and confidence intervals (IC 95%) were calculated. The cognitive DT was a modified Continuous Performance Test (attention and vigilance), and the motor DT involved the same-arm–same-leg walking.
Results. Overall, the DTC on PFC was similar for motor and cognitive DT. However, for the cognitive DT, people with PD show a moderate ES towards reducing the DTC on PFC in the On vs Off medication (ES = 0.79), (Figure 1). The DTC of gait variability was overall higher in the motor DT compared to cognitive DT. However, within each DT, no changes in DTC on gait variability were found between the On and Off medication states (ES < 0.26).
Conclusion. Our preliminary data suggest that Levodopa tends to decrease the DTC on PFC activity, but no changes for DTC on gait variability, in cognitive DT. We plan to increase sample size and also look at single walking tasks alone in addition to DTC.
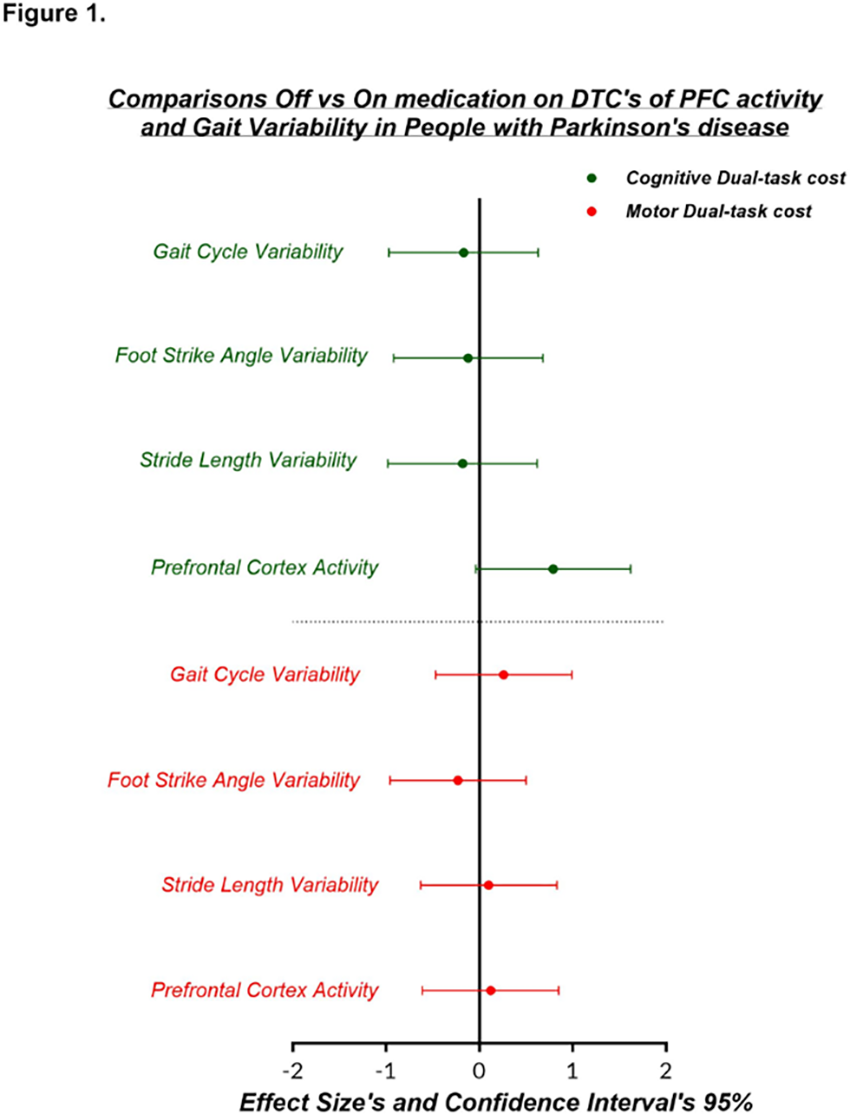
P37.45
1 Remepy Health Ltd., United States
2 Reichman University, Israel
3 Remepy Health Ltd., Israel
4 Rambam Medical Center, Israel
Objective: We aimed to evaluate the effects of an in-house developed digital sensorimotor spatial memory task combining multisensory integration with a visual masking paradigm, on thalamocortical connectivity in both monotherapy and hybrid drug therapy studies.
Background: Parkinson’s disease (PD) is characterized by the hallmark motor symptoms of bradykinesia, rigidity, tremor and postural instability, along with a wide range of non-motor symptoms such as cognitive decline and mood disorders, which are characterized by reduced basal ganglia- thalamocortical functional connectivity.
Methods: Two sequential studies evaluated the intervention’s effects on basal ganglia–thalamocortical connectivity. The first was a two-week, open-label trial with 17 healthy older adults (aged 55–60) with subjective cognitive decline (SCD), who completed a mobile-based training protocol combining sensorimotor integration tasks and psychological exercises. The second study extended this approach to PD in a three-week, double-blind, randomized, placebo-controlled trial involving 42 patients on stable levodopa therapy, who received a similar digital intervention. Resting-state fMRI (rsfMRI) assessed brain connectivity changes before and after the intervention.
Results: In the healthy cohort, increased bilateral connectivity was observed between the ventral thalamus and primary motor cortex, as well as between globus pallidus seeds and supplementary motor, putamen and insular cortices. In the PD trial, participants in the active intervention group demonstrated significantly increased connectivity in similar brain areas compared to the placebo-app group (pFDR<0.05). These connectivity changes correlated with improved motor performance as measured by MDS-UPDRS-III scores, indicating functional benefits beyond neural plasticity.
Conclusions: The digital intervention consistently improved connectivity in motor coordination circuits, supporting its neural impact. When combined with levodopa, it produced greater improvements in motor symptoms than levodopa alone, highlighting the potential of a digital-drug hybrid approach for enhancing treatment outcomes in PD.
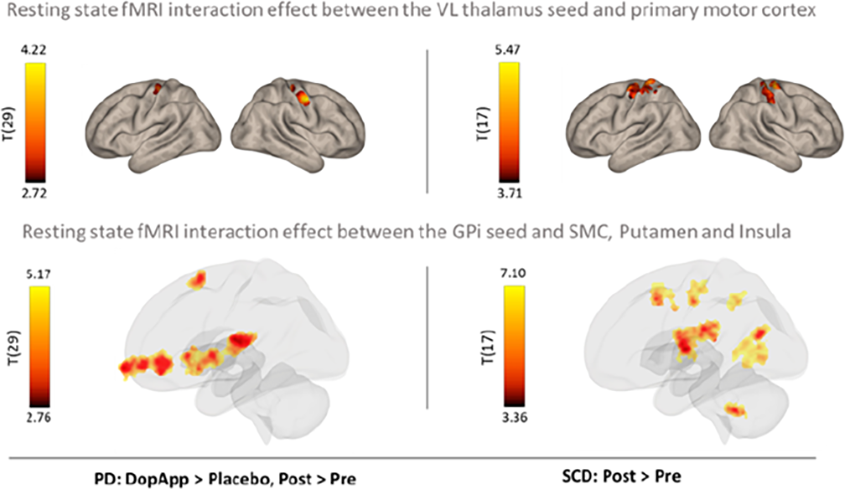
P37.47
1 University of California - San Francisco, United States
2 University of Pennsylvania, United States
3 Multiple institutions participating in the TOPAZ Study, United States
4 University of Rochester Medical Center, United States
5 Sutter Institute for Medical Research, United States
6 Veracity Neuroscience, United States
7 The Queen’s Medical Center, and University of Hawaii at Manoa, United States
8 Wake Forest School of Medicine, United States
9 Rush University Medical Center, United States
10 California Pacific Medical Center Research Institute, United States
11 University of Cincinnati, United States
12 Duke University School of Medicine, United States
13 Massachusetts General Hospital, United States
14 University of California ,San Francisco, United States
15 Morehouse School of Medicine, United States
16 University of California, San Francisco, United States
17 Stanford University Medicine, United States
18 University of California San Francisco, United States
Objective: To evaluate the feasibility, reach, and participant engagement of a fully remote telemedicine model for conducting research as part of the Trial Of Parkinson’s And Zoledronic acid (TOPAZ), a nation-wide home-based U.S. clinical trial.
Background: The TOPAZ study integrated telemedicine visits to expand access and reduce participation barriers to research participation for people with neurodegenerative parkinsonism. Telemedicine was introduced to confirm eligibility for this home-based study, overcoming mobility, transportation, and geographic barriers to participations while maintaining engagement and adherence to study protocols. If Parkinson’s disease (PD) or another neurodegenerative parkinsonism diagnosis and cognitive status were confirmed by a neurologist based on information available in medical records, a telemedicine screening was not required.
Methods: A standardized telemedicine workflow included five phases: (1) Initial Contact: coordinators contacted participants to review the telemedicine process; (2) Video Preparation: participants’ technology readiness assessed with guidance on Zoom and device use; (3) Scheduling: visits were coordinated across multiple time zones, with consideration of care partner availability; (4) Telemedicine Assessment: movement disorders specialist assessors conducted visits via secure Zoom video platform with live electronic Case Report Form (eCRF) data entry; and (5) Post-Visit Activities: recordings were uploaded to a secure server, reviewed for completeness, and finalized.
Results: Between study launch and analysis, 6,823 individuals visited the study website and expressed interest in study participation. Of these, 5,084 consented and 4,374 were deemed eligible to continue screening. Among them, diagnosis was not confirmed by neurologist record review in 885, who completed telemedicine visits. 860/885 were confirmed eligible. Telemedicine broadened reach nationwide, improved accessibility for those with mobility limitations, and increased participant and care partner comfort, reducing stress and logistical burden.
Conclusion: The TOPAZ telemedicine model successfully enrolled participants without requiring referral from a PD expert, demonstrating feasibility of a nationwide, fully remote research model. This approach expanded access, maintained data quality through live eCRF entry, and provided a scalable framework for decentralized clinical studies for people with neurodegenerative parkinsonism.
P37.48
1 University of Arizona, United States
2 University of arizona, United States
INTRODUCTION:
Allopregnanolone (Allo) is an endogenous pregnane neurosteroid and the first regenerative therapeutic that has been extensively investigated in animal models and more recently in humans for its capacity to promote regeneration in the central and peripheral nervous system.
Preclinical studies demonstrated that weekly allopregnanolone restored dopaminergic neurons and increased neurogenesis in MPTP-lesioned mice. A phase 1b/2a clinical trial of allopregnanolone in Alzheimer’s disease established safety, tolerability, maximally tolerated dose, pharmacokinetics and efficacy signals in brain imaging-based biomarkers.
This is the first clinical trial of allopregnanolone in Parkinson’s disease (PD). The main objective is to evaluate the feasibility of a large-scale trial of allopregnanolone in patients with PD, with assessment of safety, tolerability, and exploratory imaging and clinical outcomes.
METHODS: Ten participants (ages 53–78) with idiopathic or prodromal PD were enrolled in this open-label clinical trial (NCT06263010). Participants received 4 mg allopregnanolone via 30-minute intravenous infusion once weekly for 12 weeks. Primary outcomes were feasibility, safety, and tolerability. Exploratory outcome measures included neuroimaging (DaTscan, MRI) and functional/clinical assessments.
Results: All 10 participants completed treatment. Infusions were well-tolerated and without complications. The most frequent treatment-emergent adverse event was sleepiness reported by 3 participants. No serious adverse events related to study drug were reported. Outcomes of DaT-SPECT imaging indicated increased striatal dopamine transporter uptake in 9 participants. Brain MRI outcomes indicated increased neuromelanin volume in the substantia nigra pars compacta in 9 participants and greater fractional anisotropy in multiple white-matter tracts in all participants. Clinical outcomes indicated significant improvement in the Hoehn & Yahr stage and positive trends in the MDS-UPDRS Part III, PDQ-39, Montreal Cognitive Assessment, Ham depression rating scale, and CANTAB-Motor Screening Task.
CONCLUSION: Allopregnanolone treatment was feasible, safe and well-tolerated over 12 weeks in participants with PD or prodromal PD. Exploratory neuroimaging and clinical outcomes indicated preliminary signals of efficacy. These findings support progression to a phase 2 efficacy trial to further evaluate the regenerative potential of allopregnanolone in Parkinson’s disease.
P46.19
1 Special Interest Group - Black Diaspora/PD Movers, United States
Objective: To provide valuable insights for researchers and medical educators to increase Black PD Community participation in clinical research studies. To focused on utilizing a culturally sensitive engagement model, customized for the Black communities of the USA around Parkinson’s Disease Clinical Research Study participation.
Background: Currently, Black inclusion and participation rates in Parkinson’s Disease clinical research are well below their census in the US and in most PD research studies, is miniscule to nonexistent. Special Interest Group – Black Diaspora and our collaborators wanted to learn WHY by listening to our Black PD community’s experiences.
Methods: Utilizing safe spaces for Black PD Community dialogue, we facilitate discussions (n=143) leading to assembling a cohort of members (n=21) willing to share their personal clinical trial stories and then present them in educational spaces for researchers and hesitant community members. We arranged to train members (n=11) of the PD Movers (Black people with Parkinsons and their care partners), in the use of video editing software. Then we asked them: “Please tell us your stories of clinical research participation: motivations, benefits, challenges, and barriers.” The contributors own their stories and they are unmodified.
Results:
A cohort of Black PD Community first-hand storytellers capable of leading academic and community forums has been created to educate researchers and PD community leaders. A catalogue of current day community voiced challenges and barriers to clinical trial participation has been documented in video documentary (“Credible Messenger”) and a book (PD Movers – We Participate in Research). Topical education guides have been developed to facilitate researchers, educators, and PD community leaders to work on increasing participation of under-engaged communities in clinical studies. Focus groups, discussion round tables and on-going awareness events have been launched to collect study data, to activate measures from our learnings, and to publish our findings.
Discussion and Conclusion: If we, as a society, want to realize the benefits of diverse clinical research trial participation, we must include the voices of patients and care partners from diverse communities in the planning and design of clinical research trials, we must intentionally address the specific barriers identified, and we must embrace the novelty of solutions that inherently results from this inclusion.

P46.21
1 Special Interest Group - Black Diaspora/PD Movers, United States
2 Columbia University Irving Medical Center, United States
3 Saint Luke A.M.E. Church-Harlem, United States
4 Micheal J Fox Foundation, United States
5 Brian Grant Foundation, United States
6 Columbia Teachers, Columbia University, United States
Objective: To provide valuable insights for researchers and medical educators to increase Black PD Community participation in clinical research studies. To identify and document the challenges of developing research sponsor/PD healthcare provider/PD community partnerships aimed at increasing under-engaged PD community participation in PD clinical trials initially focusing on the Black PD community in the US. To develop and publish a model of effective collaboration between the interest holders of this endpoint.
Background: The challenges and barriers to increasing Black PD Community participation in clinic research and especially PD clinical trials are significant and at times complex. Many siloed efforts have been tried or are underway; the results have been less than sufficient. Most research and healthcare organizations lack the breath of in house expertise and lack the community relationships to produce scalable solutions. The issue demands an interdisciplinary approach and a strategic coordination of resources plus inclusion of the under engaged PD communities in solution design and review of desirable end points.
Methods: An interdisciplinary team of thought leaders in the Parkinson’s Disease space was assembled without regards to their work affiliations with several critical attributes. They had demonstrated a history of listening and responding compassionately to impacted PD communities, they had access to resources which might be needed to develop pragmatic solutions, they possessed a bias towards wholistic and patient/care partner centric approaches to helping the PD community members live better, and they possess a strong understanding of the research community challenges and/or the flexibility to discover what they did not know or understand that impacts barrier to participation.
Results:
A framework to bring in under engaged PD community members to contribute to the development of needed culturally sensitive educational resources has been developed and activated. A framework to elicit on demand researcher input requirements has been developed and activated. A cohort of Black PD Community first-hand storytellers capable of leading academic and community forums has been created. A documentary on this model of collaboration and how it has been deployed is developed.
Discussion and Conclusion: If we, as a society, want to realize the benefits of diverse clinical research trial participation, we must utilize greater interdisciplinary collaborations.
CLINICAL SCIENCES: Rating Scales and outcome measures
P38.01
1 University of the Sunshine Coast, Australia
Background: Parkinson’s Disease (PD) is a complex degenerative condition affecting movement and psychosocial wellbeing which ultimately impacts self-efficacy and daily life. Specialised scales measuring self-efficacy in cognition, falls, and exercise have been developed; however, there are no daily living self-efficacy scales validated in PD. Given the known impacts of PD on performance in activities of daily living (ADLs), validating a daily life self-efficacy scale is essential to help clinicians identify low daily living self-efficacy so it may be addressed therapeutically.
Purpose: To test the validity and reliability of the Daily Living Self-Efficacy Scale (DLSES) for people with PD (PwPD) living in the community.
Methods: A cross-sectional quantitative survey of 95 participants was completed. Construct validity, convergent validity, and internal consistency reliability were examined on the Daily Living Self-Efficacy Scale (DLSES).
Results: Cronbach’s α for the DLSES was 0.956 indicating excellent internal consistency. The DLSES was strongly positively correlated with measures of general self-efficacy, health-related quality of life (HRQoL), PD symptoms, and disability (p=≤0.001). It was moderately positively correlated with Parkinson’s stage (p=≤0.001) and cognition (p=≤0.01). These results indicate adequate convergent validity with measures of related constructs. The Principal Component Analysis (PCA) revealed a single component with an eigenvalue exceeding Kaiser's criterion of 1.0. This component’s eigenvalue was 8.16 and explained 68.0% of the total variance, supporting the unidimensionality of the scale. A secondary analysis investigating the relationship between DLSES scores and cognition was conducted, with findings indicating that individuals with and without MCI answered the DLSES similarly. This suggests the DLSES remains valid irrespective of MCI, supporting clinical utility of the DLSES
Conclusion: Findings indicate the DLSES is a valid and reliable tool for this sample of PwPD. This may offer new avenues for clinicians wanting to measure this construct in their clinical practice.
P38.02
1 Prime Access, Knutsford, United Kingdom
2 H. Lundbeck A/S, Denmark
Background Clinical progression in multiple system atrophy (MSA) is commonly assessed using the Unified Multiple System Atrophy Rating Scale (UMSARS). Treatment effects on UMSARS have been reported as absolute changes from baseline at a fixed time point. However, there is growing interest in evaluating trial outcomes as percentage changes over the entire treatment duration – particularly in the context of therapies with potential to slow clinical progression. Expressing clinical progression in the treatment arm relative to the placebo arm as a percentage change offers several advantages. It accommodates non-linear disease trajectories, enhancing the generalizability of findings. Moreover, it has been suggested that percentage-based outcomes are easier for patients and families to interpret. To explore this further, we aimed to establish consensus on the appropriateness and clinical relevance of expressing trial results as a percentage slowing of progression, and to identify the threshold at which such differences become clinically meaningful.
Methods International clinical experts in MSA (n=12 from Austria, France Germany, Hungary, Japan, Italy, Serbia, Spain, United Kingdom, and United States) participated in a Delphi panel (two virtual rounds) to evaluate consensus (defined as ≥70% agreement) on two key points: (1) the suitability of expressing treatment effects as percentage slowing in the Unified Multiple System Atrophy Rating Scale (UMSARS) to interpret clinical progression in MSA, and (2) the percentage change threshold in UMSARS considered clinically meaningful for individuals in the early stages of the disease.
Results The majority of the panel (83%, which met the threshold for consensus) agreed with the first statement in Round 1, “It is appropriate to express treatment effect (versus placebo) as a percentage-wise slowing in UMSARS for the interpretation of clinical progression in MSA.” One (8%) panelist disagreed with this statement, and one neither agreed nor disagreed. Consensus was reached (75% in Round 1 and 83% in Round 2) that percentage-wise slowing at 21% and above would be clinically meaningful. Over 50% agreed the lower range of 16–20% would be clinically meaningful, however, consensus was not met in either round.
Conclusion An international panel of MSA experts reached consensus that expressing treatment effects as percentage slowing in UMSARS scores is appropriate, identifying a threshold of 21% or greater as clinically meaningful.
P38.03
1 CHU de Québec - Université Laval, Canada
2 CIMA Universidad de Navarra, Spain
3 Clinica Universidad de Navarra, Spain
Introduction The MDS-UPDRS III scale remains the gold standard for assessing motor signs in Parkinson’s disease (PD) and evaluating treatment outcomes, including MR-guided Focused Ultrasound (MRgFUS). However, it is limited by examiner subjectivity. Accelerometry offers an objective and quantitative alternative. No studies to date have evaluated tremor changes following subthalamic nucleus (STN) ablation by MRgFUS using accelerometric analysis.
Methods Prospective, open-label study including 19 PD patients who underwent unilateral STN ablation by MRgFUS at Clinica Universidad de Navarra (2020–2023). Accelerometric recordings were performed off-medication at baseline and 3 months post-treatment. Custom-built devices with triaxial analog accelerometers (ADXL337) were placed on the shoulder, elbow, and wrist to record resting, proximal postural, distal postural, and action tremor. Power spectral density (PSD) was estimated using Welch’s method, and the main tremor peak was modeled with a Gaussian kernel to extract frequency and amplitude (area under the curve, AUC).
Results Of 19 patients, 15 provided analyzable data (13 males; mean age 61.3 years; mean disease duration 6.3 years). Tremor frequency showed no significant post-treatment changes across joints or tremor types. Tremor magnitude significantly decreased in all modalities (p<0.05), with the greatest reductions in resting (98%) and proximal postural (89%) tremor, particularly at the wrist. MDS-UPDRS III scores improved markedly: resting tremor from 3±1 to 0.47±0.74, postural from 1.93±0.96 to 0.07±0.26, and action from 0.67±0.72 to 0. Accelerometric magnitude at the wrist correlated strongly with MDS-UPDRS III for resting (r=0.58; p=0.0009) and postural tremor (r=0.70; p<0.001). There was a significant association between accelerometric magnitude and clinical scores (p=0.0004), especially between scores 0 vs. 2 and 0 vs. 3.
Conclusions This is the first study to objectively evaluate tremor response using accelerometry after MRgFUS STN ablation in PD. Accelerometry is a reliable and accessible tool for quantifying tremor changes, correlating strongly with clinical scales while detecting subtle variations missed by subjective assessment. Its integration into clinical practice could improve treatment monitoring and outcome evaluation.
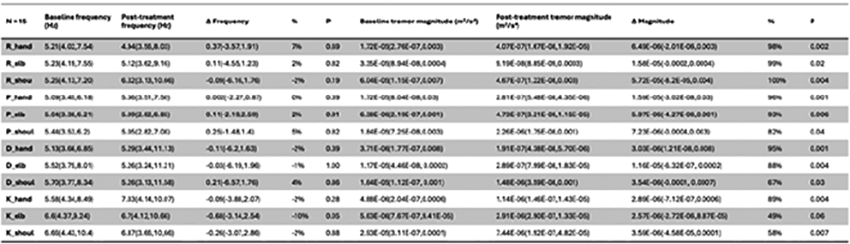
P38.04
1 b. University of São Paulo, Department of Neurology, Movement Disorders Center, São Paulo, Brazil, Brazil
2 University of São Paulo, Department of Neurology, Movement Disorders Center, São Paulo, Brazil, Brazil
3 Faculty of Medicine, Federal University of Juiz de Fora, Juiz de Fora, Minas Gerais, Brazil., Brazil
4 Faculty of Medicine, State University of Maranhão, Caxias, Maranhão, Brazil;, Brazil
Introduction: The assessment of upper limb functional capacity (ULFC) in Parkinson’s disease (PD) remains limited and underestimated despite its relevance for daily and occupational activities. A specifically designed instrument can serve as an outcome measure.This study aimed to construct and validate a comprehensive instrument for assessment of ULFC in individuals with PD.
Methods: A cross-sectional study including 100 individuals with idiopathic PD (H&Y 1-4) and 20 healthy controls. Participants were assessed by two physiotherapists specialized in PD. The instrument consists of a battery of 3 tests, specifically designed for this study, to measure the impact of motor symptoms on ULFC-related outcomes (bradykinesia, dysdiadochokinesia, and manual dexterity). The ULFC assessment battery was administered in two stages: the same evaluator performed the test twice (baseline (Assessment-1) and one week later (Assessment-2)) to assess test–retest reliability, while a second evaluator, blinded to the previous results, performed an independent assessment one week after baseline to assess inter-rater reliability (Assessment-3). The intraclass correlation coefficient (ICC) was calculated using a two-way random-effects model, agreement type, with the average-measures form [ICC(Assessment-2, Assessment-3)], reflecting the reliability of the combined evaluations and the reproducibility of the test across raters and over time. The receiver operating characteristic (ROC) curve was constructed to determine the optimal cutoff point (Youden index), and corresponding sensitivity, specificity, positive predictive value, and negative predictive value were calculated.
Results: The ULFC assessment battery showed excellent reliability (ICC=0.980; 95% CI: 0.972–0.985; p<0.001). The total score achieved an AUC of 0.932 (95% CI: 0.885–0.973), indicating outstanding discriminative accuracy between PD and controls. The optimal cutoff (69.3) yielded 71.0% sensitivity, 100.0% specificity, positive predictive value of 100.0%, and negative predictive value of 43.1%, confirming high diagnostic precision and stability of the measure.
Conclusion: The ULFC assessment battery demonstrated excellent test–retest and inter-rater reproducibility, as well as high discriminative power, supporting its use as a valid and reliable clinical tool for assessing functional upper limb performance in PD.
P38.05
1 Newcastle University, United Kingdom
2 University College London, United Kingdom
3 University of Twente, Netherlands
4 University of Plymouth, United Kingdom
5 University of Oxford, United Kingdom
Background Current dopaminergic treatments alleviate motor symptoms in Parkinson’s but do not alter disease progression. Exenatide, a glucagon-like peptide-1 agonist, showed potential disease-modifying effects in a phase 2 study, though these were not replicated in the phase 3 Exenatide-PD3 trial. However, conventional outcome measures such as the MDS-UPDRS may not fully capture meaningful, real-world aspects of function. We therefore explored the feasibility of integrating digital mobility outcomes (DMOs) as electronic Clinical Outcome Assessments (eCOAs) in the Exenatide-PD3 trial.
Methods Participants were randomised to receive weekly subcutaneous exenatide (2 mg) or placebo for 96 weeks. DMOs were collected using a lumbar wearable device (Axivity AX3) worn continuously for seven days at each assessment (baseline, 24, 48, 72, 96 weeks). Feasibility data were collected on data completeness, missingness and withdrawals. Raw data were processed using validated algorithms to derive 16 discrete gait (n=8) and walking activity (n=8) DMOs. Mixed-effects linear models examined whether DMOs had a significant response to exenatide treatment, adjusting for baseline, age, and sex.
Results Valid wearable data were obtained from 86 participants (n=39 exenatide, n=47 placebo). In terms of data completeness, 88% of exenatide and 90% of placebo assessments were included. Missing data were primarily due to unreported upload or setup errors, accounting for 22 assessments in total and were likely missing completely at random. Withdrawal due to device discomfort was minimal. Participants wore devices for an average of seven days (12 h/day). The treatment-by-time interaction indicated a signal of benefit for the exenatide group of borderline statistical significance, walking 22 minutes more per day on average (95% CI: 0.6–43.5, P = 0.047). No other significant effects were observed for activity or gait DMOs.
Discussion This study demonstrated the feasibility of incorporating DMOs into an interventional clinical trial. Consistent with primary trial findings, exenatide showed no significant effect on gait DMOs , although an improvement was observed in one measure of walking activity. Further work is required to establish clinically meaningful changes of DMOs alongside machine-learning and signal-based analyses, which may enhance detection of treatment responses. These findings inform trials integrating wearable-derived DMOs as eCOAs in future clinical research.
P38.06
1 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, United Kingdom
2 Sleep Disorders Centre, Guy's and St Thomas' NHS Foundation Trust, London & Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London., United Kingdom
3 Queen Square Institute of Neurology, University College London, United Kingdom
Background Hyposmia (smell loss) is a common prodromal characteristic of PD, detectable up to ten years before diagnosis. The University of Pennsylvania Smell Identification Test (UPSIT) is a validated 40-item smell test, but its length and cost are prohibitive to widespread testing. Shorter smell tests have been developed but their reliability over time remains uncertain. We sought to investigate the stability of the PREDICT-PD 6-item abbreviated UPSIT.
Methods PREDICT-PD is a longitudinal, UK-based cohort study of healthy and prodromal individuals aged 50-80. The PREDICT-PD abbreviated UPSIT includes ‘scratch and sniff’ panels for petrol/gasoline, soap, watermelon, lemon, cinnamon and gas. Following concerns about the stability of petrol, a manufacturing change occurred in February 2025. 1519 unique participants completed the test between October 2024 - April 2025. Individuals with PD, REM sleep behaviour disorder or pure autonomic failure were excluded. Multivariable binomial logistic regression (BLR) models assessed correct identification of each odour over time. Model 1 adjusted for sex, self-reported or ICD-10-coded hyposmia/anosmia, and the PREDICT-PD risk score. Model 2 adjusted for age, sex and hyposmia/anosmia only. Additional BLR models examined whether the petrol/gasoline odour stability improved following a manufacturing change in February 2025.
Results BLRs revealed that the proportion of individuals correctly identifying four of the six odours varied over time (Model 1: petrol/gasoline p=0.037; watermelon, lemon p<0.001; cinnamon p=0.042). The same odours demonstrated similar changes in Model 2 (petrol/gasoline, watermelon, lemon p<0.001; cinnamon p=0.034). The identification of soap and gas odours remained stable. A manufacturing change relating to the petrol/gasoline odour was not associated with improved correct identification.
Conclusion
After adjustment, four of the six items on the PREDICT-PD smell test changed significantly over time. These findings raise concerns over the reliability of abbreviated smell tests, highlighting the need to evaluate more robust smell tests for use in research and clinical settings.
P38.07
1 Northwell, United States
BACKGROUND The Timed Up and Go (TUG) test is a widely used measure of functional mobility. Its use is generally limited to patients able to walk independently. Modifications were made and further data was collected over 2 years to monitor its use over a longer period of time
OBJECTIVE To show the continued benefit of the Modified TUG as a marker for motor improvement in patients with Parkinson’s disease (PD) dependent on ambulatory assistance during a 2-week in-patient multimodal intensive neurorehabilitation and care (i-MINC) stay
METHODS 106 PD patients (H&Y stage ≥3) were included for 2024 and 2025. All required an assistive device and/or hands-on assistance on admission to i-MINC. They were assessed in their best ON state with a UPDRS examination and a modified TUG test which allowed for ambulatory assistance on admission and prior to discharge. A paired T-test was used to analyze changes in TUG time and UPDRS scores, and a Wilcoxon signed-rank test for changes in TUG level of assistance. The type of assistive device used during the test was recorded
RESULTS 97 out of 106 patients showed improvement in TUG completion time.106 patients improved in UPDRS total or motor scores. The average improvement in TUG completion time was 12.73 secs, paralleled by a 15.53-point improvement in UPDRS total score and 6.25-point improvement in UPDRS motor score. 75% of patients required a reduced level of assistance at discharge. Only 4 patients required a more restrictive assistive device and more hands-on assistance
CONCLUSIONS This study highlights the reliability of a modified TUG test as a marker for motor improvement in PD patients undergoing i-MINC. The joint reduction in TUG completion times, UPDRS total and motor scores strongly suggests that the modified test continues to be an effective, durable, and sensitive measure of motor function changes. With a larger number of patients included in this study, we are able to see the continued benefit of implementation over 2 years. Moreover, improvements in the level of assistance required during the test support the conclusion that i-MINC positively impacted functional mobility in the majority of patients. Adapting the TUG to accommodate patient’s functionality continues to support the idea of the TUG being utilized as a more inclusive assessment standard across the PD severity spectrum. Future studies may focus on continued reliability evaluation and application of the modified TUG test in other rehabilitation settings
P38.08
1 RACTHERA Co., Ltd, Japan
2 Kyoto University, Japan
INTRODUCTION: Recent years have seen active clinical trials of novel therapies for Parkinson’s disease (PD), particularly gene and cell therapies that target degenerating dopaminergic neurons. These therapies are expected to improve motor function over several years with a single administration. However, their long-term and future-oriented effects may appear as a gradual slowing of symptom progression, making it difficult for patients to perceive immediate benefits.
The MDS-UPDRS is a widely used, reliable, and sensitive tool for assessing PD symptoms. The MDS-UPDRS Part III, when assessed in the practically-defined OFF state, reflects the patient’s natural motor condition without medication and is considered suitable for evaluating gene/cell therapy effects. However, as it is scored by clinicians, it remains unclear how well it captures patients’ subjective experiences. Moreover, few large-scale studies have compared it with other motor function assessments.
This study aimed to clarify the characteristics of MDS-UPDRS Part III by comparing it with various PD assessment tools—including subjective motor evaluations, ADL, and QOL measures—using the Parkinson’s Progression Markers Initiative (PPMI) dataset (https://www.ppmi-info.org.), which contains extensive longitudinal clinical data.
METHODS: We extracted data from PD patients in the PPMI dataset, focusing on time points with MDS-UPDRS Part III (OFF state) scores. We also collected scores from other clinical indices (MDS-UPDRS Part II, S&E ADL scale, OFF time, and motor function questionnaire) recorded at the same time and analyzed their relationships. Additionally, we examined disease duration, age, and score fluctuations to evaluate each index’s sensitivity, ability to detect symptom changes, and reflection of patient subjectivity.
RESULTS: MDS-UPDRS Part III showed moderate correlation with subjective motor assessments, consistent across disease durations. Score fluctuation patterns were also aligned across indices. Objective measures tended to assess disease severity earlier than subjective ones and were more sensitive in detecting motor symptom changes.
CONCLUSION and IMPLICATIONS: Our findings suggest that MDS-UPDRS Part III, though objectively scored, reflects patient-perceived motor function to a certain extent. Characterizing motor assessment tools using large-scale clinical data may enhance diagnostic accuracy and support the selection of appropriate evaluation indices in future PD clinical trials.
P38.09
1 Oregon Health and Science University, United States
Background: Balance, gait, and cognitive changes are apparent since diagnosis in people with Parkinson’s disease (PD). However, the specific balance domains affected, and their relationship to cognitive impairments in newly diagnosed PD remain unclear. The Mini-Balance Evaluation Systems Test (Mini-BEST) is a validated clinical balance test to assess multiple systems (anticipatory, reactive postural control, sensory orientation, and dynamic gait). In PD, cognitive domains most often impaired are executive function, attention, visuospatial skills and memory. We hypothesized that early executive impairments in newly diagnosed PD relate to domain-specific balance impairments, reflecting early disruption of cognitive-motor integration.
Methods: 49 de novo PD without antiparkinson medication, and 31 healthy controls (HC) participants completed the MiniBEST and a cognitive battery including Montreal Cognitive Assessment for global cognition, Hopkins Verbal Learning Test for verbal memory, Benton Line Judgment Test for visuospatial ability, Letter-Number Sequencing for working memory, and the Trail Making Test (TMT) Part B&A for executive flexibility and set-shifting. Group differences were assessed using Mann-Whitney U tests with Bonferroni correction. Spearman’s rank correlations (ρ) with 95 % confidence intervals (CIs) examined relationships between TMT B-A and MiniBEST domains.
Results: People with PD showed lower MiniBEST total scores (p = 0.004) compared to HC, driven by dynamic gait deficits (p < 0.001) and trend toward poorer sensory orientation (p = 0.056). Anticipatory control (p = 0.13) and reactive control were similar between groups (p = 0.41). TMT B-A time was longer in PD (p = 0.016), while other cognitive domains were comparable. Balance-cognition associations differed: in HC, lower flexibility correlated with poorer Reactive (ρ = -0.38, [-0.65, -0.03]) and dynamic gait (ρ = -0.35, [-0.63, 0.01]) control, whereas in PD, it correlated most strongly with sensory orientation (ρ = -0.32, [-0.57, -0.03]) (all p < 0.05).
Conclusions: In de novo, untreated PD, dynamic gait impairment and slower executive flexibility are already present, while global cognition remains intact. These preliminary findings reveal distinct cognitive-motor correlation patterns at diagnosis: reactive and dynamic gait control in HC versus sensory orientation in PD. These differences may suggest early reorganization of balance control networks in PD.

P38.10
1 Marian University, United States
2 Community Health Network, Indianapolis, United States
3 Shirley Ryan Ability Lab, Chicago, United States
4 Indiana University Health, United States
Purpose: Rock Steady Boxing (RSB) is the largest community-based exercise program in the world for people with Parkinson’s disease (PwP). RSB’s rapid expansion has raised concerns about consistency and adherence of the RSB method across its 800+ affiliate programs. Using the principles of implementation science, we created the Fidelity, Implementation, and Safety Tool (FISTool) to assess potential variations in implementation. The purposes of the study were to evaluate the validity of the FISTool in the RSB environment, including content validity and known groups validity.
Methods: RSB classes across 19 affiliate sites in the Midwest were enrolled, purposively sampling for different environments (Parkinson's gyms, community centers, senior living centers, and hospital and university settings). At least two research team members observed each class and scored the FISTool. After class, FISTool responses were collected from boxers [PwP who box at RSB; n=192, mean age=72.6(6.8), median RSB classes/month=8.0(4.0)] and RSB coaches [n= 38, mean age=49.9(15.7), median RSB classes/month=9.5(7.0)] who participated in the RSB affiliate for at least the past month. Higher FISTool scores indicate stronger fidelity of RSB exercise and social components, and consistent implementation and safety with RSB methods in the past month.
Results: All RSB classes observed included boxers at different stages of Parkinson’s and varied in length of affiliation (range=1-11+ yrs.) and class duration (45-90 minutes). Researchers scored the fidelity exercise component section significantly lower than boxers (p=.000) and coaches (p=.000), mainly due to differences in application of cardio warm-up, core workout, and cool-down static stretching. Researchers scored the safety section significantly lower than boxers (p=.007) and coaches (p=.006), primarily due to lack of floor training during the session observed. There were no significant differences in scoring across groups for the social components, or between boxers and coaches for any section.
Conclusions: Some FISTool scoring inconsistencies may be due to only one class being observed by the research team. Improving definitions and examples of exercise components on the FISTool and enhancing coach training through establishing consistent language and ongoing knowledge and skill checks are recommended. With further refinement, the FISTool may enhance the fidelity, implementation, and safety across RSB global affiliates.
P38.11
1 University of Delaware, United States
Clinical research in Parkinson’s disease (PD) needs objective, easy-to-implement measures to quantify the underlying pathophysiology and progression of motor symptoms. Rapid isometric contractions provide several reliable candidate measures that distinguish people with PD (PwPD) from healthy adults. For example, rate of force development (RFD) and motor segmentation (segmentation). Segmentation, measured as excess zero crossings in the second derivative of force, quantifies transient reductions in neuromuscular excitation which disrupt force production. Aim 1 was to determine whether levodopa improves RFD, segmentation, and clinical bradykinesia measures. Aim 2 was to determine whether changes in bradykinesia relate to changes in force measures with levodopa intake. Ten PwPD (levodopa equivalent daily dose=859.9±695.7 mg, diagnosed 8.5±5.5 years, total Movement Disorder Society-Unified Parkinson Disease Rating Scale part III score off medication=44.5±14.2) participated in two visits in counterbalanced order, including one visit ≥12 hours off PD medication, and one visit 45 minutes post-levodopa intake. During both visits, PwPD performed rapid isometric index finger abduction contractions to 40% of their maximal voluntary contraction force. Kinesia ONE was used to quantify speed, amplitude and rhythm ratings for upper extremity tasks from the Unified Parkinson’s Disease Rating Scale part III. Dependent force measures included median peak RFD and median segmentation. Dependent clinical measures included the sum of speed, amplitude and rhythm ratings across tasks. Wilcoxon signed rank tests were used to test for differences in all measures on and off levodopa. Spearman and Kendall-Tau correlations were used to quantify relationships between force and clinical measures. Levodopa improved peak RFD (z=2.70, p=0.007 r=0.85) and segmentation (z=2.23, p=0.026 r=0.71) but not bradykinesia measures (all z≤0.82, all p≥0.413, all r≤0.26). Improvements in RFD with levodopa intake related to changes in bradykinesia speed ratings (ρ=-0.78, p=0.008) but not amplitude (ρ=-0.41, p=0.244) or rhythm (ρ=-0.40, p=0.257). Decreased segmentation with levodopa intake related to changes in bradykinesia speed (τb=0.66, p=0.014) and amplitude ratings (τb=0.53, p=0.047), but not rhythm (τb=0.31, p=0.253). These findings indicate that RFD and segmentation provide outcome measures for PD research that are more sensitive to levodopa intake than clinical bradykinesia measures.
P38.12
1 Teachers College, Columbia University, United States
Background/Aims: People with Parkinson disease (PwP) often present with spinal abnormalities, such as progressive thoracic kyphosis and camptocormia, which impair function and daily activities. Early detection and monitoring are important for early intervention and delaying postural deformity progression in PwP. However, gold-standard methods (e.g., radiography, motion capture) are costly and less accessible, and tools like inclinometers fail to capture the full thoracic contour. Inclinometer is a widely used clinical alternative but is limited to two angular measures between two points. Flexicurve, a simple, low-cost tool captures the full spinal curvature and has shown reliability in adults without impairments. This study aimed to (1) examine the Flexicurve’s convergent validity against the inclinometer and (2) assess its intra- and inter-rater reliability in PwP.
Participants: 19 PwP (11 males), age (M±SD): 68.52 ± 6.33 yrs, H&Y: I-II, tested during on-medication state.
Methods: In this cross-sectional study, the Flexicurve was molded along the thoracic spine (C7–T12) in a natural standing posture and traced on paper. Thoracic angle was calculated via a trigonometric formula. Two trained raters collected three trials per participant. For convergent validity, inclinometer angles were measured directly from the two readings from C7 and T12 in the same posture. Correlation analyses and intraclass correlation coefficients (ICC) were calculated to evaluate relationships and reliability between the two tools.
Results: Flexicurve and inclinometer angles correlated moderately (ρ = 0.52, p = 0.02, 95% CI [0.053, 0.829]). The Flexicurve demonstrated good to excellent inter-rater (ICC [2,1] = 0.89, 95% CI [0.75, 0.96]) and intra-rater reliability (Rater A: ICC [3,1] = 0.99, 95% CI [0.992, 0.999]; Rater B: ICC [3,1] = 0.99, 95% CI [0.991, 0.998]).
Conclusion: This study supports the Flexicurve’s reliability for assessing the thoracic angle in PwP. As the Flexicurve demonstrated moderate convergent validity with the inclinometer and likely measures distinct aspects of kyphosis, both tools should not be used interchangeably without caution. Flexicurve is an easy-to-use, low-cost, highly reliable tool that can be used clinically to assess the contour of the whole thoracic spine. Further research is needed to establish the construct validity of the tool in this population.
P38.13
1 KU Leuven, Belgium
Introduction: Axial rigidity is a hallmark feature of Parkinson’s Disease (PD) that hampers trunk rotation in a dissociated manner1. It negatively influences everyday tasks, including walking, turning1,2, bed mobility3, transfers, and traffic situations, for example when looking over one’s shoulder4. Surprisingly, despite its crucial role, no clinically rated scale exists to evaluate axial rotation impairments in PD. We therefore developed the Axial Rotation Scale (ARS) inspired by the MDS-UPDRS5. The ARS evaluates range of motion (ROM), dissociation- and quality of movement, and the presence of pain during rotatory movements of the spine. The ARS is being embedded in a larger test battery to chart cycling skills in PD (the MAESTRO-PD study). By doing so, we aim to identify its feasibility and psychometric properties to evaluate axial rotation in PD. Methods: The ARS includes passive movements that can be compared with subsequent active ROM. Implementation of a slow and fast condition evaluates the influence of speed. The scale consists of 28 items, with a maximum total score of 88 which represents maximal deficit. To measure feasibility, participants reported adverse reactions. For validity, we set out to investigate the scale’s discriminative ability (PD vs. HOA) and its association with head turning performance during cycling, and its ability to predict cycling falls. Results: As the Maestro-PD study is ongoing, interim results from 9 HOA’s and 2 PD’s are presented. Both patients and 4 HOA’s reported a prior cycling fall in the previous 5 years. The scale appears feasible as no adverse reactions were reported. Table 1 shows that the ARS scores appear consistently higher in the PD than in HOA, with a trend towards a group difference for the passive sub-score. Importantly, there was one positive correlation between the ARS total score and the number of errors made during the shoulder check when cycling in both groups (r=0.637, p=0.035). The ARS total score appears predictive of biking falls (AUC: 0.90, odds ratio: 1.87, 95%CI: 0.94-3.74, p=0.076). Conclusion: The ARS is developed to quantify the clinical assessment of axial rotation impairment in PD. Interim results indicate that the ARS seems feasible and has discriminative and construct validity, though verification in a larger cohort and with other disease-related outcomes as well as internal consistency is pending. A more comprehensive overview of the result will be presented at the WPC 2026.

P38.14
1 Bastyr University, United States
2 Parkinson Center for Pragmatic Research, Poland
The Patient-Reported Outcomes in Parkinson’s Disease (PRO-PD) scale is a 35-item visual analog measure of symptom severity, designed to quantify disease burden across motor and non-motor domains. This study aimed to evaluate the psychometric properties of the PRO-PD across two independent datasets, including assessment of reliability, validity, factor structure, and minimal clinically important difference (MCID). A cross-sectional sample (n = 46) with 34 items (excluding restless legs) was used to assess convergent validity with established instruments (Hoehn & Yahr, MoCA, PDQ-39, UPDRS, and PROMIS). A longitudinal cohort (n = 2,612; 35 items) was used for internal consistency, test-retest reliability, factor analyses, and known-groups validity. A subsample (n = 390) with 6-month follow-up and anchor ratings (“Improved,” “Stable,” “Worsened”) was analyzed to determine MCID thresholds using non-parametric tests, multinomial regression, and ROC curves. PRO-PD correlated strongly with established clinical measures, confirming convergent validity. Internal consistency was excellent (Cronbach’s α = 0.93–0.95). Test-retest reliability was good (ICC = 0.78 overall; 0.89 at 6 months). Confirmatory factor analysis of the Swedish 8-factor model showed suboptimal fit (CFI = 0.81, TLI = 0.78, RMSEA = 0.083), leading to an exploratory 4-factor model explaining 47.6% of variance, representing Cognitive Function, Autonomic, Motor, and Psycho-Emotional domains. PRO-PD scores increased significantly with longer disease duration and greater H&Y stage. The MCID for worsening was +53.5 and for improvement –78.5 points, with classification accuracy of 64% (AUC = 0.63–0.71). A subset of “stable” participants showed large score changes, suggesting recall bias or response shift in self-reported anchors. Across these data, the PRO-PD demonstrated excellent internal consistency, temporal stability, and strong construct validity. Factor analysis supported a concise, interpretable 4-domain structure consistent with Parkinson’s pathophysiology. The established MCID thresholds provide benchmarks for detecting meaningful clinical change in longitudinal and interventional studies. Findings confirm that PRO-PD is a reliable, patient-centered, remote monitory tool for quantifying symptom severity, worsening, and improvement.
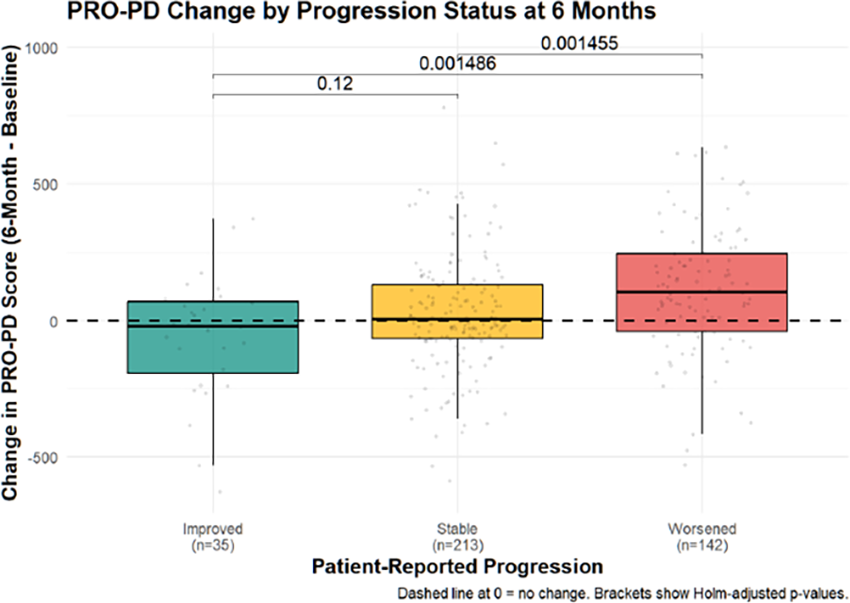
CLINICAL SCIENCES: Digital health, E-health and technology
P39.01
1 University of Florida, United States
Background: Bradykinesia is a core motor symptom of Parkinson’s disease (PD) and central to diagnosis and monitoring. Current clinical evaluations, such as the Movement Disorder Society-sponsored Unified Parkinson’s Disease Rating Scale (MDS-UPDRS), rely on subjective clinician ratings that are limited by variability and low sensitivity to subtle change. Digital health technologies provide objective alternatives, but most rely on wearable sensors, which face barriers to scalability. Video-based systems are more accessible but have not been evaluated for their ability to track longitudinal progression.
Objective: We investigated whether VisionMD, an open-source software platform for semi-automated video-based kinematic analysis, could detect longitudinal changes in bradykinesia over two years and whether progression patterns varied by baseline severity.
Methods: Twenty individuals with PD (disease duration ≤ 5 years, Hoehn & Yahr ≤ 2) were evaluated at baseline (T0) and two-year follow-up (T1). Each completed the finger tapping (FT) task (MDS-UPDRS item 3.4), yielding 80 videos. Clinical FT scores were derived by consensus of three certified raters. Videos were analyzed with VisionMD to extract seven digital measures of movement speed and variability. Longitudinal changes were assessed with Wilcoxon signed-rank tests (clinical scores) and linear mixed-effects models (digital measures), with false discovery rate correction.
Results: Clinical FT scores showed no significant group-level change (median difference = 0, p = 0.110). In contrast, digital measures revealed significant declines in Mean Speed (−13%, p-adjusted = 0.019), Mean Opening Speed (−15%, p-adjusted = 0.021), and Mean RMS Velocity (−13%, p-adjusted = 0.021). Stratified analyses showed that participants with baseline score 0 (PD0) exhibited worsening clinical scores and pronounced declines in speed and variability, while PD1 remained stable, and PD2 showed reduced variability without speed decline.
Conclusions: Video-based digital measures sensitively captured longitudinal progression of bradykinesia when clinical scores did not. VisionMD offers a scalable, objective method for monitoring PD progression. Future studies should validate VisionMD in larger cohorts and home-based settings.
P39.02
1 Srinakharinwirot University, Thailand
Introduction: Micrographia is one of motor symptoms in Parkinson’s disease (PD). This study investigates a handwriting-based screening approach tailored to the Thai language, incorporating tasks such as Archimedean spiral drawing, line tracing in multiple orientations, isolated character writing, and sentence composition. The aim of the study is to create digital platform for detecting micrographia and confirm diagnosis of PD.
Methods: A total of 94 participants included 44 individuals diagnosed with Parkinson’s disease and 50 age-matched healthy controls. Five handwriting templates were designed using Canva Pro and embedded within the application to serve as visual guides during data entry. These include: (1) an Archimedean spiral, (2) vertical lines, (3) horizontal lines, (4) Thai characters “ลอปร,” and (5) a complete Thai sentence "กนกชวนดวงกมลดมดอกขจร.” Each template was displayed on its corresponding task screen, prompting participants to trace or write directly over the visual cue.
Results: The Thai sentence task yielded the highest performance, with a sensitivity of 93.2% (95% CI: 81.3–98.6), specificity of 76.0% (95% CI: 61.8–87.0), and accuracy of 84.0% (95% CI: 75.5–90.6). Predictive values were also high (PPV: 77.4%, 95% CI: 63.8–88.0; NPV: 92.7%, 95% CI: 80.1–98.5), with likelihood ratios supporting strong discriminatory ability (LR+ = 3.88, LR– = 0.09). The Archimedean spiral and Thai letters tasks demonstrated comparable performance, each with an overall accuracy of 81.9% (95% CI: 72.9–89.0). The Archimedean spiral achieved higher sensitivity (90.9%, 95% CI: 78.3–97.5) but lower specificity (72.0%, 95% CI: 57.5–83.8), while the Thai letters task yielded a more balanced profile (sensitivity: 88.6%, 95% CI: 75.4–96.2; specificity: 74.0%, 95% CI: 59.7–85.4). In contrast, the vertical and horizontal line tasks produced lower overall accuracy (75.5% and 76.6%, respectively). Although sensitivity was acceptable (≥84%), specificity was reduced (66.0% for vertical lines; 70.0% for horizontal lines). Both tasks yielded lower PPV values (69.1% and 71.2%, respectively), consistent with modest LR+ values (2.54 and 2.80).
Conclusion: The Thai sentence, Thai letters, and Archimedean spiral provided superior discriminative power compared with simple line-drawing tasks. Further studies should focus to create sentences/letters that will provide high sensitivity and specificity for micrographia detection.

P39.03
1 UCLA David Geffen School of Medicine, United States
2 UCLA, United States
Background: Parkinson’s Disease (PD) is the second most common neurodegenerative disorder in the United States, affecting nearly one million individuals (Parkinson’s Foundation, 2023). Characterized by progressive motor impairment, cognitive decline, and loss of functional independence, PD requires consistent, specialized care. However, underserved populations in Los Angeles County—including racial/ethnic minorities, immigrant and non-English-speaking individuals, older adults on fixed incomes, and residents of low-income neighborhoods—encounter substantial barriers that delay diagnosis and reduce treatment access. Contributing factors include high out-of-pocket medication costs, limited transportation, low awareness of PD resources, cultural and linguistic mismatches, and the digital divide among older adults.
Methods: To better understand these inequities, we conducted a community survey of 110 individuals living with PD across Los Angeles County. Participants were recruited through local support groups, health fairs, and community centers. The survey assessed perceived barriers to care, cultural and linguistic accessibility, and interest in digital health solutions.
Results: Survey findings highlight significant unmet needs. Sixty-two percent of respondents reported medication costs as a major obstacle, while 72% identified transportation challenges in accessing specialty clinics. More than half (57%) indicated PD information was culturally inappropriate or available only in English. Importantly, 70% of respondents expressed strong interest in a mobile platform offering patient education, cost transparency, and accessible navigation features.
Innovation: In response, we developed Project P.A.T.H. (Parkinson’s Access to Technology & Health), a community-driven initiative designed to reduce disparities in PD care. Project P.A.T.H. leverages a digital platform to centralize essential PD tools, provide culturally relevant education, and promote cost transparency. Implementation will be paired with hands-on community outreach to build trust and overcome digital literacy barriers. By integrating multilingual resources, culturally tailored education, and patient-centered outreach, this initiative aims to improve equitable access to diagnosis, treatment, and supportive services for underserved PD populations in Los Angeles County and beyond.
P39.04
1 Seoul National University Hospital, South Korea
2 emocog, South Korea
Background Timely identification of Parkinson’s disease (PD) is hindered by heterogeneous clinical presentations, low public awareness, and limited access to movement disorder specialists. Digital biomarkers offer promise for scalable screening, yet most prior studies have relied on unimodal assessments with modest accuracy.
Methods We created and tested a smartphone application that combines simple motor tasks, a color-matching test, a short speech exercise, and a 25-item questionnaire to distinguish PD from healthy controls (HC). A total of 368 participants (233 PD, 135 HC) were enrolled for the initial version and 296 (204 PD, 92 HC) for the optimized version. Low-performing tasks were removed, others redesigned, and key features were selected using artificial intelligence methods. The final model was evaluated on an independent group of 98 participants.
Results Among individual tasks, the questionnaire achieved the highest AUROC (0.84), followed by finger tapping and vertical swipe. The integrated multimodal model reached an AUROC of 0.86, while a reduced model combining spiral drawing, finger tapping, and the questionnaire achieved the best performance (AUROC 0.91). Feature-level analyses revealed PD-specific dependencies between touch speed, balloon acceleration, and spiral path length, confirmed by Hotelling’s T-squared tests.
Conclusion A compact set of smartphone-based tasks, when combined with questionnaire data, enables accurate and scalable differentiation of PD from HC. This standardized, portable design highlights the feasibility of digital tools for early detection and community-level PD screening.
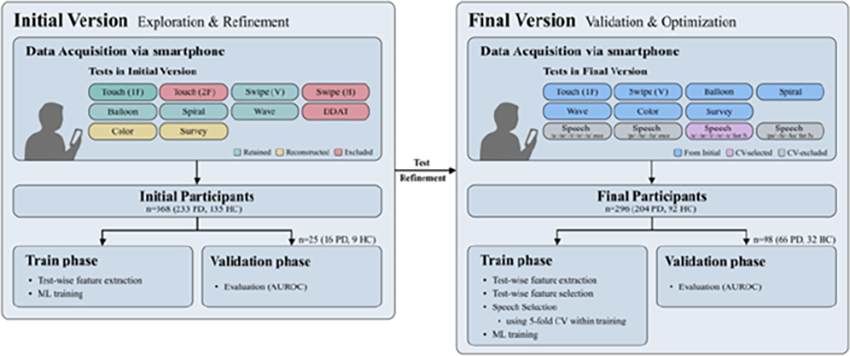
P39.05
1 Oregon Health and Science University, United States
2 Oregon Health and Science University, APDM Wearable Technologies, a Clario Company, United States
Background and Aim People with Parkinson's disease (PD) rely on executive control to maintain walking stability, reflected by increased prefrontal cortex (PFC) activity during simple walking. However, when task demands increase under dual-task conditions, their ability to further recruit the PFC is compromised, especially in those experiencing freezing of gait (FOG). It is unclear if exercises with mobility and cognitive challenges can change PFC activity during walking and whether such changes accompany gait improvements. This exploratory study investigated whether a novel intervention (TURN-IT) targeting mobility and cognition reduces executive reliance and improves gait and turning performance in people with PD, with and without FOG.
Methods Forty-six participants with PD were randomized to either a control group (n = 25, 15 FOG; mean age = 70.6 ± 6.7 years; MDS-UPDRS Part III = 39 ± 8.9) or the TURN-IT group (n = 21, 13 FOG; mean age = 70.1 ± 5.5 years; MDS-UPDRS Total = 38.9 ± 14.2). Participants completed two-minute single- and dual-task (ST, DT) walking tests at baseline and after six weeks (on medication). During DT trials, they recited individualized digit spans. The TURN-IT group completed six weeks of supervised turning and balance exercises targeting dynamic stability during gait transitions, while controls received no intervention. PFC activity was recorded using functional near-infrared spectroscopy (fNIRS), and gait metrics via wearable sensors. Post-intervention changes were compared between groups using ANCOVA controlling for baseline values, stratified by FOG status.
Results No overall group differences were observed in PFC activation during ST (p = 0.381) or DT walking (p = 0.060). Among participants with FOG, the TURN-IT group showed increased PFC activity during DT walking versus controls (p = 0.026). TURN-IT improved upper-limb control, increasing arm range of motion and reducing asymmetry variability under both conditions (all p < 0.04). Participants with FOG demonstrated greater improvements in arm-ROM variability, asymmetry, and turning metrics during DT walking (p ≈ 0.03–0.04).
Conclusions TURN-IT training enhanced gait control, particularly arm swing symmetry and turning performance, under both ST and DT conditions. In people with FOG, increased PFC activity during DT walking suggests strengthened cognitive–motor integration following rehabilitation, indicating differential neural adaptations in FOG versus non-FOG participants.
P39.06
1 University of Tasmania, Australia
2 Australia
3 Queen Mary University of London, United Kingdom
AIM: International guidelines recommend people with Parkinson’s should have access to information to help them self-manage, as well as a knowledgeable multidisciplinary team. The aims of this project were to co-produce a 5-week free Parkinson’s massive open online course (MOOC) for the Parkinson’s community, and to evaluate its uptake, reach and impact on knowledge.
METHOD: The course was co-led by a physiotherapist living with Parkinson’s and a Parkinson’s neurologist. There were five modules providing an overview of Parkinson’s, signs and symptoms, risk factors and biology, medical management, the multidisciplinary team and Parkinson’s wellbeing. Modules included animations, quizzes, interactive activities and >80 interviews with people with Parkinson’s, care partners, clinicians and researchers from six continents. The MOOC was advertised globally via social media and was open for four months. Participants were asked to complete a pre- and post-knowledge questionnaire.
RESULTS: 21,708 participants (n=162 countries) started and 9028 (41.6%) completed the course. Of these, 11,422 (mean age 51 years, 81% female) consented to research, and 7390 completed questionnaires (mean age 53, 81% female): 7% had Parkinson’s, 32% family members, 25% health professionals and 36% classified as other. Class Central ratings were 4.9/5, placing the course 4th globally amongst 12,000 Health and Medicine courses. Reviews portrayed the MOOC as an exceptionally well-crafted educational resource that informs, inspires, and supports a global audience interested in understanding and managing Parkinson’s. Knowledge scores improved for all groups (all p<0.05).
CONCLUSION: A free Parkinson’s online course was made with people with Parkinson’s for the Parkinson’s community. There is great interest in Parkinson’s education, as evidenced by wide uptake and positive global ratings. The MOOC has the capacity to influence and improve knowledge on Parkinson’s-specific content, as shown in pre- and post-survey outcomes and number of participant completions.
Key practice points:
MOOCs can improve knowledge about Parkinson’s MOOCs can meet the needs of people living with Parkinson’s, family members, health professionals and the general community all around the world
P39.07
1 Independent Researcher, Austin, Texas; in collaboration with Power for Parkinson's, United States
2 University of Texas at Austin, United States
3 Independent Researcher, United States
4 Power for Parkinson's, United States
Background: Regular exercise is a key non-pharmacological intervention for managing Parkinson’s disease (PD), improving mobility, mood, and quality of life. Yet, many people with PD face barriers to in-person programs, including lack of local classes, cost, transportation, and symptom fluctuations. While prior studies have examined structured, clinician-led virtual interventions, few have evaluated freely available, community-developed programs that people with PD can access independently. Power for Parkinson’s (PFP), a nonprofit in Austin, Texas, addresses these barriers by offering free, symptom-directed fitness classes on YouTube, accessible worldwide. Understanding who engages with these classes and how viewers perceive their value is essential for evaluating digital accessibility, reach, and perceived effectiveness of virtual exercise programs.
Objective: To assess the reach, user characteristics, perceived benefits, and usability of PFP’s online exercise videos for people with PD, and to identify implementation factors that enhance accessibility and engagement.
Methods: A mixed-methods, cross-sectional study will be conducted using three data sources: 1) an anonymous online survey of adults with PD who self-identify as PFP video users, 2) thematic analysis of viewer comments from publicly available videos, and 3) YouTube analytics summarizing audience geography and engagement metrics. The survey includes questions on viewing frequency, barriers overcome, perceived benefits, usability, and intent to continue. Quantitative data will be summarized descriptively. Qualitative data from open-ended responses and YouTube comments will undergo inductive coding to identify themes related to access, impact, and suggested improvements.
Results: Data collection is ongoing. Anticipated findings include broad geographic reach and high engagement among individuals with limited access to in-person exercise options. Viewers are expected to report perceived improvements in mobility, mood, and social connection, with digital usability and instructor clarity emerging as key facilitators of engagement.
Conclusion: This study will provide insights into how freely available online classes can extend reach and perceived effectiveness of PD-specific exercise beyond traditional settings. Findings will inform strategies for digital implementation, accessibility, and sustained engagement, supporting scalable, community-based approaches to exercise for people living with PD worldwide.
P39.08
1 Newcastle University, United Kingdom
Background / Rationale
Non-motor symptoms (NMS) of Parkinson’s disease, such as fatigue, sleep disturbance, anxiety, and cognitive decline, are among the most disabling yet least systematically monitored symptoms. They are subtler than motor symptoms, fluctuate daily, and the data tend to be lost between clinic visits. While traditional questionnaires capture snapshots, they rely on recall, which can be a challenge given cognitive impairments. Smartphone-based interventions offer an accessible way to regular symptom monitoring and self-management, but most existing interventions focus only on motor symptoms, making their impact limited.
Aim / Objectives
This study aims to investigate the impact of an artificial intelligence (AI)-enabled mobile app on NMS self-monitoring and management for people with Parkinson's and their care partners. Its objectives are to:
Evaluate usability and engagement patterns over six months; Assess the system's feasibility, acceptability, and usability and identify barriers to use; Explore whether users communicate issues to clinicians earlier; Assess preliminary signals of impact on users' confidence in managing their symptoms, symptom burden, and quality of life.
Methods This poster will present a mixed-methods feasibility study in which people with Parkinson’s and their informal carers use a smartphone app for 6 months. The app was co-designed with people with Parkinson's and their care partners and has features such as symptom monitoring, educational resources, goal setting, medication reminders, and a generative AI agent. The evaluation adopts validated questionnaires to evaluate the potential impact of the system, quantitative app use and study data to understand engagement and feasibility, and semi-structured interviews to explore acceptability and contextualise the engagement data.
Expected Outcomes / Impact
The system is expected to have a positive impact on users’ quality of life, as well as their confidence in managing symptoms. The findings will contribute valuable insights into the development of next-generation digital health pathways that move beyond basic symptom monitoring towards intelligent digital assistants in chronic disease management.
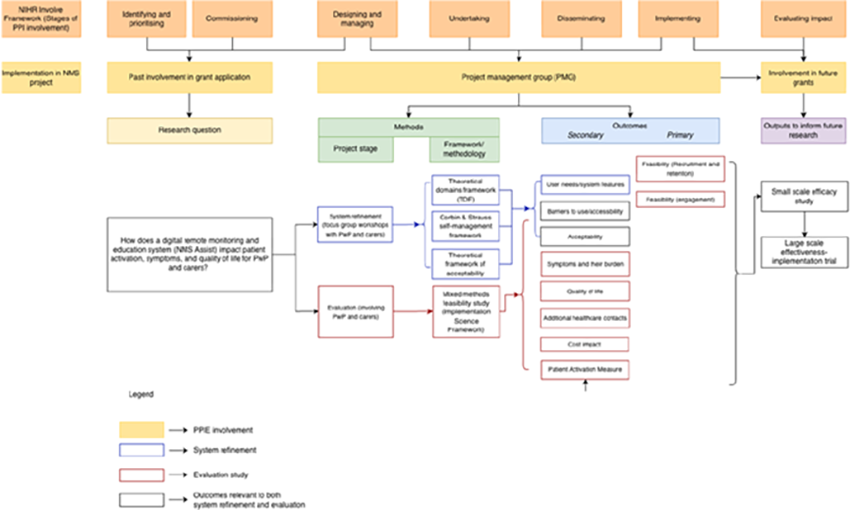
P39.09
1 Queen Mary University of London, United Kingdom
2 Royal London Hospital NHS Trust, United Kingdom
3 Homerton Healthcare NHS Foundation Trust, United Kingdom
Introduction Parkinson’s disease (PD) often leads to persistent motor disability and non-motor symptoms despite dopaminergic therapy and deep brain stimulation. Gait impairment, bradykinesia, sleep disturbance, and reduced quality of life (QoL) remain inadequately addressed. Vibrotactile stimulation may engage compensatory motor networks, but robust randomized evidence is limited. This study evaluated the usability, safety, and tolerability of a sternum-worn, non-invasive vibrotactile stimulation device (CUE1+; Figure 1), and explored its effects on motor and non-motor outcomes compared with a sham device.
Methods In this multicenter, double-blind, sham-controlled pilot trial, 50 adults with idiopathic PD were randomized 1:1 to active or sham stimulation for 12 weeks (≥8 hours/day). Assessments were performed at baseline and week 13 on stable antiparkinsonian medication. Primary outcomes were usability and safety. Exploratory outcomes included Movement Disorder Society-Unified Parkinson’s Disease Rating Scale, Part III (Motor Examination; MDS-UPDRS Part III), Functional Gait Assessment (FGA), Timed Up and Go, Bradykinesia Akinesia Incoordination tap test (upper limb dexterity measure; BRAIN), Pittsburgh Sleep Quality Index (PSQI), Parkinson’s Disease Questionnaire-39 (PDQ-39), and patient-reported global impression of change. Analyses were intention-to-treat using Analysis of Variance (ANCOVA) adjusting for baseline motor severity values. Confidence Intervals (CI) are reported.
Results Fifty participants (median age 69 years; 54% male) were randomized (25 active, 25 sham). Compliance exceeded 95% in both groups. Four participants discontinued. Mild skin irritation occurred in two participants. At week 13, MDS-UPDRS Part III improved by -15.6 points in the active group versus -4.5 in sham, yielding an adjusted between-group difference of -10.2 (95% CI -17.9 to -2.5; p=0.009). Active stimulation improved bradykinesia, gait (FGA difference: +3.0 vs +1.2), upper limb dexterity (BRAIN: +3.0, p=0.007), sleep quality (PSQI: -2.0 vs -0.7), and QoL (PDQ-39: -7.6; p=0.003). Patient-reported outcomes also favored active treatment.
Conclusion CUE1+ was safe, usable, and well tolerated. Exploratory results demonstrated clinically meaningful improvements in motor severity, gait, dexterity, sleep, and QoL compared with sham stimulation. These findings support larger multicenter trials to confirm its efficacy and cost-effectiveness as a non-invasive adjunct to standard PD care.
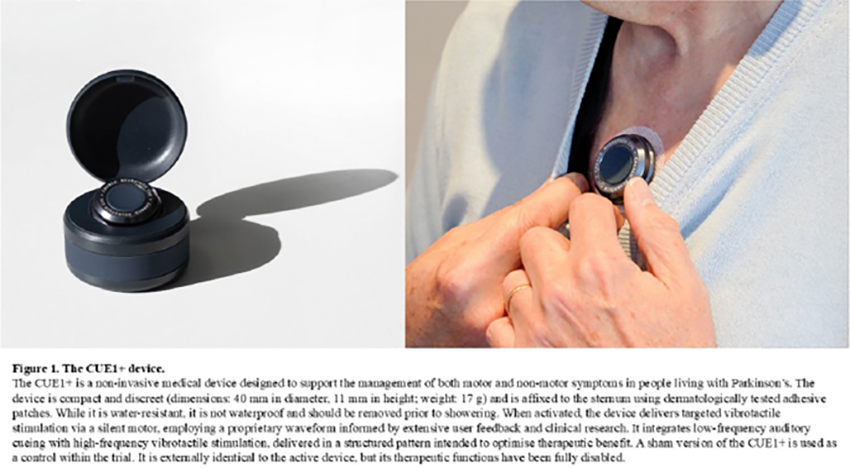
P39.10
1 Biogen Inc., United States
2 Indivi AG, Switzerland
3 Denali Therapeutics Inc., United States
Objective: To evaluate the sensitivity of routine smartphone-based performance assessments in the free-living environment as part of a randomized clinical trial in early Parkinson’s disease (PD).
Background: LUMA (NCT05348785) is a Phase 2b, multicenter, randomized, double-blind, placebo-controlled study to determine safety and efficacy of BIIB122 tablets in individuals aged 30 to 80 years with early-stage PD. The primary endpoint is time to confirmed worsening in MDS-UPDRS parts II and III combined score over the treatment period. An exploratory outcome is the effects of BIIB122 on the longitudinal progression of motor symptoms as measured by objective performance assessments administered through the Konectom smartphone application. Digital endpoints from Konectom assessments collected weekly may be more sensitive to subtle changes in disease disability compared to clinical rating scales.
Methods: Participants perform the Konectom assessments at specified clinic visits (twice at baseline, then once each at the week 24, 48, 72, and 96 visits) and on a weekly basis at home. Tests of walking, standing postural sway, pronation-supination, finger drawing, keystroke typing, finger tapping, speech production, and symbol-digit substitution are deployed through the smartphone application.
Results: The tests are being deployed at 91 sites across 11 countries and in 12 different languages. Critical steps in selecting digital endpoints with the strongest validity as indicators of worsening PD include analysis of test-retest reliability and sensitivity to longitudinal change. Reliability will be assessed using the test-retest design at the baseline clinic visit and, for unsupervised conditions, the first few weeks of remote assessments. Sensitivity to longitudinal progression relative to clinical anchors will be determined using a blinded subset of study subjects.
Conclusions: The protocol for Konectom assessments allows for a good compromise between feasibility and burden to the patients and enables the selection of digital endpoints based on test-retest reliability, relationship to established anchor measures of PD severity, and sensitivity to longitudinal progression. The digital data will allow for a comparison of performance in the clinic setting versus the free-living environment, provide insight into week-by-week variability in motor function, and may provide real-world, objective evidence of treatment efficacy in early-stage PD.
Previously presented at MDS 2025.
P39.11
1 Universidad Rey Juan Carlos (King Juan Carlos University), Spain
Introduction: Reactive sensory training has shown promise in improving motor performance in individuals with Parkinson’s disease (PD) by targeting movement initiation and response speed. Non-invasive brain stimulation techniques such as transcranial direct current stimulation (tDCS) have been proposed as adjuvant interventions to enhance neuroplasticity and motor outcomes. This study investigated whether applying anodal tDCS over the primary motor cortex (M1) simultaneously with reactive sensory training leads to superior improvements in motor function compared to training alone in people with PD.
Methods: In this double-blind randomized controlled trial, 60 participants with idiopathic PD were allocated to one of four groups: (1) reactive training + anodal M1 tDCS (RT+tDCS), (2) reactive training + sham tDCS (RT+sham), (3) reactive training only (RT), or (4) control. Reactive training was delivered through mimo.fit, an interactive home-based digital system that provides real-time visual and auditory stimuli requiring rapid motor responses from the upper and lower limbs. Participants in the intervention groups completed 24 sessions over 8 weeks in their own homes. Outcome measures, assessed pre- and post-intervention, included gait speed, Timed Up and Go (TUG), stepping choice reaction time, and arm choice reaction time. Data were analyzed using mixed-model ANOVAs with time (pre vs. post) as the within-subject factor and group as the between-subject factor.
Results: Significant time × group interactions were observed for all outcome measures (p < 0.01). Post-hoc analyses indicated significant pre–post improvements in all intervention groups, with no significant differences between the RT+tDCS, RT+sham, and RT groups. No significant changes were observed in the control group.
Conclusion: Home-based reactive sensory training using mimo.fit produced significant improvements in gait, functional mobility, and reaction times in patients with PD. However, the concurrent application of anodal M1 tDCS did not enhance these benefits compared to training alone. These findings suggest that mimo.fit reactive training is effective in improving motor function in PD, but adding tDCS does not provide additional advantages. Future studies should explore alternative stimulation parameters or targets to potentiate training-induced gains.
P39.12
1 Newcastle University, United Kingdom
2 Plymouth University, United Kingdom
Introduction Parkinson’s disease is a complex and variable condition, and current care pathways often fail to meet the needs of People with Parkinson’s (PwP). To address this, we developed Home-Based Care (HBC) , a new pathway that combines digital tools and remote monitoring to enhance patient autonomy, support self-management, and improve clinical decision-making. However, the scalability of HBC is limited by the manual effort required for data interpretation. Clinical Decision Support Systems (CDSS) can address this challenge by automating evidence-based data interpretation and generating recommendations at the point of care. Here, we describe the creation of SMaRT-PD, a CDSS designed to integrate multimodal data used in HBC including patient-reported outcomes, wearable data, and routinely collected clinical records to provide tailored insights for both patients and clinicians.
Methods SMaRT-PD was developed using a rule-based clinical decision-support architecture that models decision pathways for symptom management in Parkinson’s disease. A total of (58) rule-based decision tree wireframes were created. Clinical requirements were prioritised using the MoSCoW framework, informed by a survey of (80) Parkinson’s clinicians. To assess feasibility, a subset of (7) prioritised decision trees was implemented within an Azure Function App, drawing data from a temporary Excel-based repository in Azure Blob Storage. Ongoing evaluation and identification of limitations informed iterations and adaptation of the digital architecture.
Results The pilot system, though functional, relied on complex rule sets, duplicated code, and file-based data storage, which hindered scalability and data quality control. In response, the system was redesigned using a modern, modular architecture to improve maintainability, reliability, and scalability. A central PostgreSQL database replaced flat files, enhancing data validation, accuracy, and version control. This architecture enables integration of all decision trees, streamlines updates, and supports evolving clinical guidelines.
Conclusion This work demonstrates the progressive development of SMaRT-PD from a static rule-based model to a scalable, modular, and explainable CDSS architecture. It offers a replicable framework for digital health systems that balance clinical interpretability with computational robustness, an essential step toward integrating explainable, data-driven decision support into routine Parkinson’s care.
P39.13
1 Arizona State University, United States
Introduction: Postural instability in people with Parkinson’s disease (PwPD) contributes to falls, leading to injury and reduced quality of life. This instability is influenced by visual input, ground conditions, and divided attention. However, it remains unclear which factor should be prioritized in therapy. This study examined how visual input, ground compliance, and different levels of cognitive load affect postural stability in PwPD.
Methods: Ten PwPD maintained balance on a dual-axis robotic platform for 45 s under each condition. The platform generated rigid or compliant (500 Nm/rad) ground conditions. Participants performed a single task (ST) and a dual task with three different levels (DT1–DT3). The dual task involved continuously tracking a moving target displayed on a screen using a joystick, where higher levels increased target speed and movement randomness. Eye condition (open or closed) was applied only during ST. Postural stability was assessed using three balance metrics: virtual time-to-contact (VTC), sway area (SA), and path length (PL) of the center of pressure. Data were analyzed using linear mixed-effects models with Tukey’s HSD post-hoc tests.
Results: Ground compliance and task difficulty significantly affected all three balance metrics (p < .001) with no interaction. Compliant ground reduced postural stability, and post-hoc tests showed ST yielded higher stability than all DT levels (p < .05), while no significant differences were found among DT levels. In the ST analysis, both eye and ground conditions significantly affected stability without interaction. Compliant ground reduced balance for all metrics (p < .001). Eye closure reduced stability for VTC (p = .001) and PL (p < .001), but not for SA (p = .1354).
Conclusion: Visual, ground, and cognitive loads independently decreased postural stability in PwPD. The effect of cognitive load was most pronounced when transitioning from ST to DT, but increasing DT difficulty caused no further decline. These findings suggest that postural control in PwPD is independently influenced by sensory and cognitive challenges. In the ST analysis, SA did not show significant differences in response to eye condition, whereas VTC and PL demonstrated significant changes. This may suggest that SA is less sensitive than other metrics in evaluating balance. Future work should identify the neural mechanisms underlying these effects to guide targeted rehabilitation strategies.
P39.14
1 College of Health and Rehabilitation Sciences: Sargent College, Boston University, Boston, MA, United States
2 John A. Paulson School of Engineering and Applied Sciences, Harvard University, Boston, MA, United States
3 Department of Neurology, Parkinson’s Disease and Movement Disorders Center, Boston University, Boston, MA, United States
Purpose/Hypothesis: Freezing of gait (FOG) is a debilitating gait disturbance in Parkinson Disease (PD) that severely restricts daily mobility. Episodes of FOG are substantially elicited by individualized and person-specific contexts — referred to as ‘personalized hotspots’ — that could hinder daily mobility. Our team has pioneered a robotic apparel designed to prevent FOG, demonstrating initial successes during straight-ahead walking tasks. The next logical step in advancing this technology is to examine its effects under more complex and challenging conditions. This study evaluated the impact of our robotic apparel in preventing FOG at these personalized hotspots in people with PD (PwPD).
Subjects: 6 PwPD - age [Mean (SD)]: 70.8 (7.5) with mild-to-moderate PD (Hoehn & Yahr 2-3; Unified Parkinson’s Disease Rating Scale – Motor: 39.7 (14.3).
Methods: Our robotic apparel provided cable-driven mechanical assistance to each hip augmenting flexion during late stance and swing phase to assist with limb advancement during walking. Participants were asked to walk under personalized hotspot conditions, identified and tested in the home (1 visit) and re-created in the lab (3 visits). Percent time freezing (%TF) was obtained through video annotation by a physical therapist, complemented by wearable sensors and pressure insoles. To examine the effects of robotic apparel, we compared %TF during Assist-On and Assist-Off modes. Descriptive statistics were used to characterize effects of robotic apparel on FOG.
Results: At baseline, participants exhibited substantial FOG, averaging 41.99 (22.66) %TF without assistance. With robotic apparel assistance, freeze severity decreased for all participants to 18.19 (12.44) %TF. Despite wide baseline variability (range: 7.34 – 65.72 %TF without assistance) reflecting heterogeneity in FOG presentations, every participant showed improvement with robotic apparel, with the greatest benefits observed in those with more severe FOG at baseline.
Conclusions: Assistance provided by soft robotic apparel during walking in real world contexts is an innovative approach to reduce FOG in people with PD in personalized hotspots, which are highly provocative for FOG. This emerging approach represents a clinically relevant strategy to reduce FOG in contexts that are personalized to the individual, including complex home environments.

P39.15
1 College of Health and Rehabilitation Sciences: Sargent College, Boston University, Boston, MA, United States
2 John A. Paulson School of Engineering and Applied Sciences, Harvard University, Boston, MA., United States
3 Department of Neurology, Parkinson’s Disease and Movement Disorders Center, Boston University, Boston, MA, United States
Purpose/ Hypothesis: Freezing of gait (FOG) is a disruptive gait disturbance in persons with Parkinson Disease (PwPD), characterized by a sudden marked reduction of forward movement of feet despite the intention to walk. The variability of FOG triggers across individuals makes assessment challenging. Recent studies have introduced “personalized hotspots” – participant-identified, context-specific triggers – to better elicit FOG that may not be captured by standardized protocols. However, the usefulness of these hotspots in provoking FOG remains unclear. This study examined the ability to elicit FOG within personalized hotspots within home and laboratory environments.
Number of subjects: 7 PwPD age [Mean(SD)]: 69.3(7.9) with mild-to-moderate PD (Hoehn & Yahr 2-3; Unified Parkinson’s Disease Rating Scale – Motor: 40.3(13.2).
Materials and methods: Participants worked with a physical therapist in their home to identify 3 personalized hotspots. The hotspots were replicated in the laboratory incorporating key task and environmental features known to elicit FOG. One hotspot was repeated across 3 laboratory visits. A follow-up home visit was conducted with reassessment of all 3 hotspots. Freeze severity, defined as the percent time spent freezing during each task (%TF), was measured through video annotation. Non-parametric statistics (Wilcoxon Signed Rank Test and Friedman’s ANOVA) were used to compare %TF across days, and Spearman’s rho was used to examine correlations across visits.
Results: Hotspots elicited substantial freezing in the initial home visit, 31(27) %TF, with comparable %TF observed during the follow-up home visit, 24(22) %TF; p = .398. Time spent freezing did not differ significantly across three laboratory visits (p = .180). In addition, there were no differences between %TF in the initial home visit compared to the average of laboratory visits (36 (21) %TF; p = .499). No correlations were observed across visits in either home or laboratory environments, suggesting large individual variability.
Conclusions: Personalized hotspots elicited substantial FOG in PwPD, with lab-based recreations producing comparable freeze severity to home environments. High variability and weak correlations across testing days highlight the heterogeneity of FOG in PD, underscoring the need for repeated measurements. Personalized hotspots may serve as a valuable procedure for visualizing, understanding, and developing treatment strategies for FOG in clinical practice.
P39.16
1 Tel Aviv Medical Center, Israel
Introduction: Parkinson's disease (PD) is marked by progressive motor decline, with subtle motor alterations preceding clinical diagnosis by years. Wearable sensors objectively monitor daily movement, providing potential early PD risk stratification. We aimed to identify mobility-derived digital features that reflect PD risk and track progression.
Methods: Non-diagnosed participants from the BeaT PD Project with prodromal or genetic PD risk were included based on MDS-Prodromal Research Criteria likelihood ratios (Berg et al., 2015). Scores >70 indicated high risk. Accelerometry data came from a 3-axis Axivity AX6 worn for 7 days (100 Hz). After outlier removal (Tukey’s rule), 124 cases remained. 244 features were extracted and reduced to six via recursive feature elimination with logistic regression reflecting diurnal mobility - transition jerk (TJ), sedentary bout time (SBT), percent of walking at night (PWN), average active bout duration (AABD), standing time, and transitions from rest to active (TRA). Min–max scaled features were split into training (70%) and test (30%) sets, stratified by target (LR≥70). A logistic-regression classifier was trained and evaluated using accuracy, F1-score, and AUC-ROC. Group differences were tested using Welch's t-test or Mann–Whitney U with log1p-transformed data. Motor change over 4–5 years was assessed using Jonckheere–Terpstra test.
Results: The cohort included 170 participants (high risk; n=30; 54.5yrs+/-10.2, 26%F and low risk; n=140; 65.7yrs+/-10.2, 64%F). The six-feature model discriminated between groups with AUC=0.84, accuracy=0.94, and F1-score=0.93. Maximal SBT was shorter in high-risk subjects (−22.6%; p=0.001), and TJ was lower (−7.8%; p=0.01). High-risk participants had walked at night more frequent (33.6% vs. 66.7%; p=0.001) and higher PWN compared to low-risk (+10.2%; p=0.003). Progressors had more SBT (p=0.006) with longer yet less variable bout lengths and more of them walked at night (p=0.004). AABD declined over progression (p=0.006).
Conclusions: Digital mobility measures can identify individuals at high risk for PD prior to diagnosis. High-risk individuals were more sedentary, had more defragmented nights observed by more walking, and showed more rigid transitions than people with low risk for PD. Mobility features derived from a 7-day recording of lower-back accelerometry become more pronounced with progression to higher risk scores, reflecting the utility of digital monitoring in the preclinical stage.
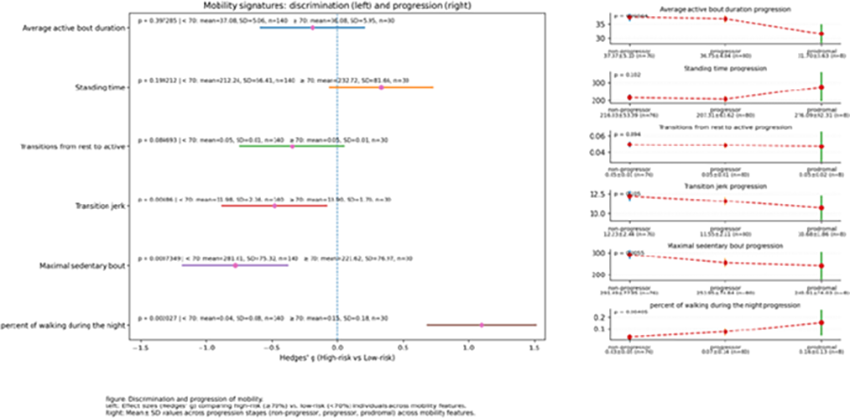
P39.17
1 National Institute for Health and Care Research (NIHR) Newcastle Biomedical Research Centre, Newcastle University, United Kingdom
2 Newcastle University, United Kingdom
3 University College London, United Kingdom
4 University Hospital Erlangen, Germany
Background Multiple system atrophy (MSA) is a rare progressive neurodegenerative disorder characterised by autonomic failure, parkinsonism, and/or cerebellar dysfunction. Early in the disease course, MSA may resemble Parkinson’s disease (PD), but subsequently progresses more rapidly. Accurate differentiation is crucial for timely intervention with potential disease-modifying therapies. Digital mobility outcomes (DMOs), captured using body-worn devices, may provide an objective means of distinguishing MSA from PD, by quantifying gait and mobility in real-world settings.
Methods This cross-sectional analysis utilised baseline data from the exenatide-MSA trial, an open-label 48-week phase 2 study at University College London. Age- and sex-matched PD participants (n=39) from the Mobilise-D Clinical Validation Study (Newcastle site) were included as comparators. MSA clinical severity was assessed with the Unified MSA Rating Scale (UMSARS); PD motor severity was evaluated with the Movement Disorder Society Unified Parkinson’s Disease Rating Scale Part III (MDS-UPDRS III). Real-world mobility was measured using a single lower-back worn wearable device for seven days (McRoberts MM+ or Axivity AX6). Wearable data were processed using the validated Mobilise-D pipeline to derive 24 DMOs quantifying walking activity and discrete gait characteristics. DMOs were compared between cohorts using generalised linear models adjusted for sex and age. Analyses were performed in R (v4.02).
Results MSA participants (n=39; mean age=63 years; mean UMSARS total score=44; disease duration=1.1 years) demonstrated significantly more impaired mobility compared to PD (n=39; mean age=64; MDS-UPDRS III=32.2; disease duration=9.8 years) with fewer steps (2218 vs 8265 per day), reduced walking time (0.3 vs 1.5 h/day), and fewer walking bouts (10 vs 20 per day) (all p < 0.001). People with MSA walked with significantly slower walking speed and shorter stride lengths across both short and long walking bouts.
Discussion Mobility performance was significantly reduced in MSA compared to PD, with lower levels of walking activity and more impaired gait. Remote monitoring in the home setting can yield valuable complementary insights beyond standard clinical assessments, and may provide ecologically valid measures to enhance diagnosis, monitoring and treatment targets.
P39.18
1 SPAR Physical Therapy, United States
2 Northern Arizona University, United States
3 Walk With Path, United Kingdom
4 Body Central Physical Therapy, United States
5 Arizona State University, United States
Background: Sixty percent of persons with Parkinson’s disease (PD) will fall at least once each year. While clinical tests can assess mobility and fall-risk, in-home monitoring of gait and balance may improve the ability to track and treat fall-prone individuals and reduce the risk of injury. Instrumented insoles are a novel, promising technology that can provide real-time, daily-life balance and gait tracking. The purpose of this report is to 1) provide validation of the remote therapeutic monitoring insole, and 2) evaluate views of health care providers and individuals on the use of this tool as a clinical utility for persons with PD. Methods: Forty-two participants (> 50 y.o.) completed a single data collection in which they walked on a computerized gait mat at normal pace (three trials) while wearing instrumented insoles. Insole data was collected via App and stored in cloud base system. Stride velocity, stride duration, stride length, and step length were extracted from both systems. In addition, focus groups including 33 adults over 50 years and 8 clinicians were conducted virtually to determine feasibility of the insoles as a remote therapeutic monitoring (RTM) device to assist in mitigating falls. Results: Eight hundred and twenty-seven steps across 42 individuals were compared across systems (insole to gold standard computerized walkway). The insole system was over 90% accurate in all parameters (stride velocity: 93%, stride duration: 98%, stride length: 92%, step length: 91%). A majority of the focus group members stated they are comfortable with technology; noting they already have a wearable device. Caregivers emphasized the value of identifying pre-fall events such as freezing. Approximately 30% stated they do not want to know if they are at risk of a fall if no solutions are provided, but changed their mind after explaining that measures to reduce fall risk could be provided via a health care professional such as a PT or OT. Others commented ‘we don’t want insurance to know we are at risk for a fall’. Conclusion: Smart insoles provide accurate and reliable data (in a structured environment) for gait outcomes related to falls in older adults. Further, the delivery of information via the App of gait deviations may be positively received by the user if an intervention is provided to help mitigate falls. Smart insoles are a promising tool for RTM to identify specific gait deviations suggestive of fall risk in order to provide early intervention.

P39.19
1 Reiwa Health Sciences University, Fukuoka, Japan, Japan
2 Graduate School of Media and Governance, Keio University, Kanagawa, Japan, Japan
3 (1) Graduate School of Media and Governance, Keio University, Kanagawa, Japan (2) ORPHE Inc., Tokyo, Japan (3) Research Center for Music Science, Keio University Global Research Institute, Tokyo, Japan, Japan
Auditory cues are known to be effective in reducing freezing of gait (FOG) in people with Parkinson’s disease. However, frequent turning and speed changes during daily walking limit the applicability of fixed-tempo cueing. This study evaluated a step-triggered auditory feedback system that provided real-time feedback synchronized with each step and assessed the effectiveness in a patient with severe FOG. This case report involved a woman in her 70s with a 2-year history of Parkinson’s disease who was diagnosed 18 months after symptom onset. The presenting symptom was gait difficulty. She was taking L-dopa (300 mg/day). The Movement Disorder Society–Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) total score was 48 (Parts I–IV: 6, 8, 34, and 0, respectively). The New Freezing of Gait Questionnaire (NFOG-Q) score was 24. Two walking tasks were assessed: a 10-meter walk, and a figure-of-eight walk test(F8WT) with two cones placed 1.5 feet apart. The completion time, total FOG duration, and FOG ratio were calculated after FOG episodes were identified by an experienced physical therapist from recorded videos. The FOG ratio was defined as the percentage of total FOG duration divided by the total completion time. Foot contact timing was detected using motion sensors (ORPHE CORE 3.0; ORPHE Inc., Tokyo, Japan) embedded under the insole, and a web application that was developed by ORPHE Inc. and Keio University generated a drum-kick sound at each foot contact. The participant performed one loop of the F8WT under three conditions: step-triggered feedback; fixed-tempo cueing matched to her natural cadence; and no sound. No FOG episodes were observed during the 10-meter walk. The F8WT completion time, total FOG duration, and FOG ratio were 72 s, 67 s, and 93% in the no-sound condition, 27 s, 20 s, and 74% in the fixed-tempo condition, and 12 s, 4 s, and 33% in the step-triggered feedback condition. The step-triggered auditory feedback system markedly reduced freezing episodes, suggesting potential benefit for real-world walking in people with Parkinson’s disease. Step-triggered feedback may outperform fixed rhythmic stimulation during complex walking tasks. This approach could help reduce FOG in daily environments. Corollary studies with larger samples are warranted.
P39.20
1 F Hoffman-La Roche Ltd, Switzerland
Introduction: Digital health technology tools (DHTs) enable remote and frequent measurement of motor signs in people with Parkinson’s disease (PwPD). Here we report findings from the Roche PD Mobile Application DHT in the PADOVA (NCT04777331) study of prasinezumab in early-stage PwPD on stable monoamine oxidase type B inhibitor (MAO-Bi) or L-dopa monotherapy.
Methods: 586 participants (74% L-dopa; 26% MAO-Bi) received monthly doses of prasinezumab (n = 293) or placebo (n = 293) until ≥ 248 primary events occurred and all participants completed ≥ 76 weeks (Nikolcheva et al, 2025). Participants were instructed to perform active motor tasks on provisioned study smartphones daily at home, and to input when they took their last medication. Predefined ‘features’ were extracted from each task and median aggregated over fixed time intervals. Summary measures were calculated for bradykinesia, speech, and the entire motor battery (‘Simple Sum’; Taylor et al., 2025). Prespecified analyses examined individual and summary bradykinesia/speech measures in the entire cohort. Since PwPD typically take L-dopa several times daily, all data were a priori assumed to be collected in a practically-defined ON state (i.e., 1-10h post intake); unexpectedly, PwPD collected 40% of at-home data in practically defined OFF L-dopa state. Therefore, post-hoc analyses examined all features/scores in the L-dopa population, split by practically-defined ON/OFF states. Generalized additive mixed models or mixed models for repeated measures tested for the effect of prasinezumab on changes from baseline to 72 and 104 weeks.
Results: The prespecified analyses showed no robust treatment group differences (all p>0.05). Post-hoc analyses of L-dopa population data collected ON (60% of data) showed no consistent trends, whereas consistent trends favoring prasinezumab were observed in data collected OFF (40%): Simple Sum score (72w: p=0.02; 104w: p=0.03); rest tremor (72w: p=0.015; 104w: p=0.007); postural tremor (72w:p=0.059; 104w: p=0.11); summary bradykinesia score (72w: p=0.1; 104w: p=.13).
Conclusions: The prespecified analyses of remote digital data in PADOVA showed no robust group differences, likely due to mixed ON/OFF L-dopa state data. Post-hoc analyses showed consistent trends favoring prasinezumab in digital data collected in practically defined OFF, but not ON, state. These exploratory results replicate the PASADENA ph2a Simple Sum digital finding and align with the clinical PADOVA readout.
P39.21
1 University College Cork, Ireland
2 My Moves Matter, Ireland
INTRODUCTION: The sex of a person with Parkinson's disease (PD) impacts their experiences of motor and non-motor symptoms, yet women with PD (WwPD) remain underrepresented in research. Hormones, particularly estrogen, are thought to affect how WwPD experience PD symptoms. However, understanding of menstrual-related fluctuations in PD symptoms and of effects of hormone replacement therapy (HRT) on PD risk are limited. In this study, self-reported PD symptoms and medication patterns were compared between menstruating and postmenopausal women.
METHODS: WwPD aged >18 years were recruited to complete surveys capturing demographics, symptoms and medication use. Of n=493 participants who completed an online survey, n=131 used a mobile application designed for WwPD to track symptoms, medications and menstrual cycles.
RESULTS: Survey analysis found significant differences between the symptoms reported by menstruating (n=125) and postmenopausal (n=283) women. For motor symptoms, rigidity was higher (p<0.001) and postural instability was lower (p=0.007), in menstruating women. For non-motor symptoms, depression/anxiety (p=0.026), pain (p=0.016), and mood swings (p<0.001) were higher, whilst hyposmia (p=0.003) and constipation (p=0.042) were lower, in menstruating women. No difference in self-reported medication usage was found between groups. HRT users aged 50-54 years reported lower tremor prevalence (p=0.006) than non-users. Analysis of data from the mobile app found that more dyskinesia (p=0.045) was reported by menstruating (n=45) than postmenopausal women (n=72), as were several premenstrual syndrome-related non-motor symptoms, ie. irritability (p=0.003), crying spells (p=0.014), hot flushes (p=0.007), pelvic cramps (p=0.001), mood swings (p=0.043), increased appetite (p=0.026), and excessive daytime sleepiness (p=0.026). N=131 participants used the mobile app, n=36 reporting menstrual cycle events and n=17 providing sufficient data to allow statistical analysis of symptoms across phases of the menstrual cycle.
CONCLUSIONS: Differences in both motor and non-motor symptoms were reported between menstruating and postmenopausal WwPD. Future optimisation of this novel app, the first of its kind aimed at tracking of symptoms and medication use in WwPD, should improve engagement. Overall, hormonal status appears to impact symptom patterns in WwPD, highlighting a need for further hormone-focused research and for tailored management approaches according to hormonal stage.
P39.22
1 Critical Path Institute, United States
Background Digital health technologies (DHTs) such as smartwatches and wearable sensors can transform Parkinson’s disease (PD) research and care by enabling continuous and objective data collection in real-world settings. By revealing sex-specific patterns of disease expression and treatment response, DHTs may help address historical underrepresentation of women in PD research. This work analyzes digital measures collected during the Wearable Assessments in the Clinic and Home in PD (WATCH-PD) study by identifying sex differences in baseline, progression, and treatment effects.
Methods WATCH-PD is a 12-month, multicenter observational study measuring features of early PD in 82 (36 female) individuals with early PD and 50 (32 female) age-matched controls using smartphones, smartwatches, and research-grade sensors (Clario, Inc.). Digital features were extracted using Mobility Lab software from the in-clinic 2-minute walk task. These measures were assessed for significance in differentiating: 1) baseline sex differences in both people with PD and healthy controls; 2) sex differences in total change over the course of the study; and 3) effects of sex and medication use during the study in participants with PD. Comparisons were performed in R using a generalized linear model controlling for height with alpha = 0.05.
Results
1) Baseline assessments of PD vs healthy controls demonstrated that women with PD exhibited significantly higher variability than men across a variety of lower limb gait features (e.g.: gait speed, stride length) and higher trunk range of motion. 2) No consistent sex differences in disease progression of the selected digital measures were found over the twelve-month follow-up. 3 Medication effects were evaluated by comparing total change over the study between participants who initiated dopaminergic treatment and those who remain unmedicated. Differences emerged in arm swing velocity, range of motion, turn duration, and foot strike angle were observed between groups, with a small sex-specific interaction in turn duration limited by small sample size.
Conclusion DHTs can provide objective measures of disease state, progression, and treatment effect. To maximize their impact, further work is needed to determine sex differences and assess the relevance of digital measures to the lived experience of women with PD. These findings underscore the importance of developing and validating DHTs that account for the needs and experiences of women.
P39.23
1 Roche Polska Sp. z o.o., Warsaw, Poland
2 F. Hoffmann-La Roche Ltd, Roche Information Solutions (RIS), Data, Analytics & Research, Roche Diagnostics, Basel, Switzerland
3 Roche Diagnostics, Clinical Validation, Sant Cugat Del Vallès, Spain
Introduction: Freezing of Gait (FoG) is typically characterised by a halt in forward movement; however, patients with Parkinson's disease (pwPD) often exhibit subtle step-like movements or shuffling during FoG episodes. This study used a novel step detection algorithm to identify these steps during FoG episodes. Our primary aims were to validate the algorithm's ability to measure these attempts and to determine if patients experiencing FoG show different turning behaviour compared to a matched non-FoG control group.
Methods: Data from a lower back-mounted wearable sensor were analysed from the WearGaitPD dataset. The cohort included five pwPD who experienced twenty confirmed FoG episodes and a control group of twenty-two non-FoG pwPD matched for age and disease stage. A previously validated step detection algorithm was used to identify and characterise steps during FoG episodes. To evaluate how FoG could influence turning behaviour, we first performed a comparison of signal amplitude-based features calculated during FoG turns against non-FoG turns within the same group of patients experiencing FoG. Second, we compared these features during turns between the FoG patient group and the matched non-FoG control group.
Results: Our step detection algorithm successfully identified steps during confirmed FoG episodes, which mainly occurred during turns, a well-known trigger. During FoG, step attempts were characterised by reduced signal amplitude, indicating feet were barely lifted off the ground. Furthermore, in contrast to the non-FoG group, pwPD experiencing FoG showed a generalised difficulty in executing turns and exhibited decreased signal amplitude even during non-FoG turns.
Conclusion: PwPD experiencing FoG exhibit a distinct, quantifiable impairment in their turning mechanics, even when not actively freezing. This finding provides a valuable, objective tool for clinicians to quantify the impact of FoG on the daily life of pwPD.
P39.24
1 Boston University, United States
2 MedRhythms, Inc., United States
3 Boston University Chobanian & Avedisian School of Medicine, United States
Introduction: Routine walking at higher intensities can slow gait decline in people with Parkinson disease (PwPD). Understanding who best responds to such interventions is vital for advancing personalized gait rehabilitation in PD. This study examined differences in baseline motor characteristics of higher- and lower-responders to an efficacious community-based walking intervention delivering closed-loop music-based rhythmic auditory stimulation (RAS). We hypothesized that higher-responders – i.e. those with greatest gains in daily step counts and moderate intensity walking — would have greater motor impairments, lower walking capacity, and worse balance at baseline.
Participants: 21 PwPD (66.95 ± 8.8 years of age; Hoehn & Yahr 2-3).
Materials/ Methods: We conducted a secondary analysis of experimental arm data from a completed randomized controlled trial (NCT05421624) evaluating real-world walking activity outcomes following a 6-week intervention. Baseline motor characteristics included motor severity (Unified Parkinson’s Disease Rating Scale–3; UPDRS3), walking capacity (6-Minute Walk Test; 6MWT), and balance (Mini-BESTest). As most participants improved following the intervention, participants were classified as higher-/ lower-responders based on: (1) changes in daily minutes of moderate intensity walking using a median split (23.8 minutes), and (2) changes in daily steps using published minimum detectable change (1,366 steps). Kruskal-Wallis Tests compared baseline motor characteristics, reported as medians ± interquartile ranges.
Results: Higher-responders based on moderate intensity minutes (n=11/21) had significantly lower baseline 6MWT distances (450 ± 127 vs 580 ± 145 m; p=.035) than lower-responders. Similarly, higher-responders based on daily steps (n=14/21) tended to have greater (worse) baseline total UPDRS3 scores (23 ± 10.5 vs 15.5 ± 14.75; p=0.063), and greater (worse) bradykinesia subscores (12.5 ± 7.5 vs 9.5 ± 7.25; p=.098) than lower-responders. No group differences in Mini-BESTest scores were observed.
Conclusions/ implications: PwPD with lower baseline walking capacities and potentially greater motor impairment exhibited stronger responses to the RAS gait intervention, which likely reflects the intervention’s observed training specificity in those with greater walking impairment. Closed-loop music-based RAS is a promising approach to boost routine walking intensities and volumes, especially for those with limited walking capacities.
P39.25
1 Roche Polska Sp. z o.o., Warsaw, Poland
2 F. Hoffmann-La Roche Ltd, Roche Information Solutions (RIS), Data, Analytics & Research, Roche Diagnostics, Basel, Switzerland
3 Roche Diagnostics, Clinical Validation, Sant Cugat Del Vallès, Spain
Introduction: Parkinson's Disease (PD) often leads to impaired postural stability, a condition linked to deficits in the complex sensorimotor control systems necessary to maintain an upright stance. The key measure of this stability is the sway path (i.e., the total length of sway movement), which can be monitored using an Inertial Measurement Unit (IMU), often integrated into smartphones. However, the accuracy of the sway path derived from IMUs must be validated against a well-established gold-standard reference before it can be implemented in a clinical trial. Therefore, this analysis compared the sway path computed from the IMU accelerometer data with the reference value obtained from the centre of pressure (COP) measured using a pressure-sensing walkway mat.
Methods: Publicly available data from the WearGaitPD study, which included 61 individuals with PD, were used for this analysis. Participants' static balance was assessed using a pressure-sensing walkway mat and synchronised body-worn IMUs while they performed a protocol consisting of six 10-second tasks. Task difficulty was progressively increased by altering stance width (feet together vs. apart) and visual condition (eyes open vs. closed). Accelerometer data from the IMUs placed on the xiphoid, L4/L5 of the lower back, the right and left lateral thighs were utilised. The xiphoid was included to provide a reliable measure of upper trunk sway. The remaining locations were specifically selected because they correspond to positions where people are likely to carry their smartphones. The sway path calculated from the COP time series was compared to the same feature calculated from the IMU accelerometer data.
Results: Strong correlations between the sway path from the reference COP data and multiple IMU locations were measured. All correlations across all four IMU locations and six subtasks were statistically significant (p<0.001), with correlation coefficients ranging from 0.721 to 0.906.
Conclusion: The strong correlation between the sway path derived from the IMU acceleration data and the COP supports the analytical validity of this feature across various subtasks and multiple common smartphone-carrying locations. This indicates that smartphone technology is a reliable tool for evaluating postural instability in individuals with PD.
P39.26
1 Roche Polska Sp. z o.o., Warsaw, Poland
2 F. Hoffmann-La Roche Ltd, Roche Information Solutions (RIS), Data, Analytics & Research, Roche Diagnostics, Basel, Switzerland
3 Roche Diagnostics, Clinical Validation, Sant Cugat Del Vallès, Spain
Introduction: A major challenge for wearable-based gait assessments is ensuring accurate and reliable gait measurements in populations with movement disorders, such as patients with Parkinson's disease (pwPD), regardless of the device's placement on the body. This study aimed to validate the gait pipeline available in the Roche Digital Biomarker Solution by demonstrating its ability to consistently and accurately measure gait, irrespective of the device's location, thereby offering a robust and user-friendly tool for clinical trials and care.
Methods: The Roche Gait pipeline was validated using the open-access WearGaitPD dataset, which involved 58 pwPD. Gait measures (e.g., number of steps, median step length, and median step velocity) from four inertial measurement units, located at the lower back, sternum, and thighs, were compared with measures from a gold-standard sensor-equipped walkway. The analysis involved both self-paced and fast-paced walking tests.
Results: The step detection algorithm demonstrated excellent performance, achieving sensitivity and precision rates above 98% in detecting steps. Concordance plots showed a high level of agreement and minimal systematic bias between the digital measures from the gait pipeline and the gold-standard measures from the walkway. These findings were consistent across all four sensor locations and both walking speeds.
Conclusions: Based on these findings, the Roche Digital Biomarker Solution is a technically and analytically valid tool for gait assessments in pwPD. This solution removes a significant barrier to real-world data collection by allowing users to carry their smartphones as they prefer. This validation increases confidence in the use of wearable-based gait assessments and supports the broader integration of digital biomarkers into clinical trials and standard healthcare practice.
P39.27
1 NeuroRPM Inc., United States
2 Davis Phinney Foundation for Parkinson’s Disease, United States
Aim: Evaluating the effectiveness of Parkinson's disease (PD) therapies remains challenging due to infrequent clinical visits and subjective patient reporting. Current methods do not capture dynamic motor symptom fluctuations during the day and across treatment modifications. We developed NeuroRPM, a FDA 510(k) cleared continuous remote patient monitoring platform that objectively measures motor symptoms in real-world settings. This enables precise evaluation of medication adjustments, deep brain stimulation (DBS) programming changes, and lifestyle interventions.
Methods: NeuroRPM uses Apple Watch to continuously monitor three cardinal motor symptoms: tremor (shaking), bradykinesia (slowness of movement), and dyskinesia (involuntary movements), along with ON/OFF states (periods when medication is working or not). NeuroRPM uses clinically validated algorithms to quantify symptom severity and prevalence across different time periods. We implemented comparative analysis evaluating changes to treatment such as medication and deep brain stimulation (DBS) programming.
Outcomes: Three representative cases demonstrate clinical utility:
Case 1 (Adaptive DBS): Patient showed noticeable improvements in symptom fluctuations using adaptive DBS. Continuous monitoring revealed reduced symptom variability and optimized ON State and ON State with dyskinesia (DK), validating programming refinements.
Case 2 (New DBS): Patient started DBS therapy in June 2025 which resulted in dramatic improvement in symptom control. Comparative analysis showed significant reductions in tremor and bradykinesia.
Case 3 (Medication Optimization): Patient with troublesome dyskinesia reduced medication. Monitoring showed substantial reduction in dyskinesia while maintaining acceptable bradykinesia and tremor control, confirming successful dose optimization. NeuroRPM detected statistically significant changes that were not apparent through standard clinical assessments, enabling data-driven optimization.
Conclusion: Continuous objective monitoring using NeuroRPM enables precise, evidence-based evaluation of PD therapies. NeuroRPM transforms real-world symptom data into actionable clinical insights, supporting personalized treatment optimization across pharmacological, surgical, and lifestyle interventions. This technology bridges the gap between infrequent clinical visits and continuous disease monitoring, improving outcomes through responsive, data-driven care adjustments.
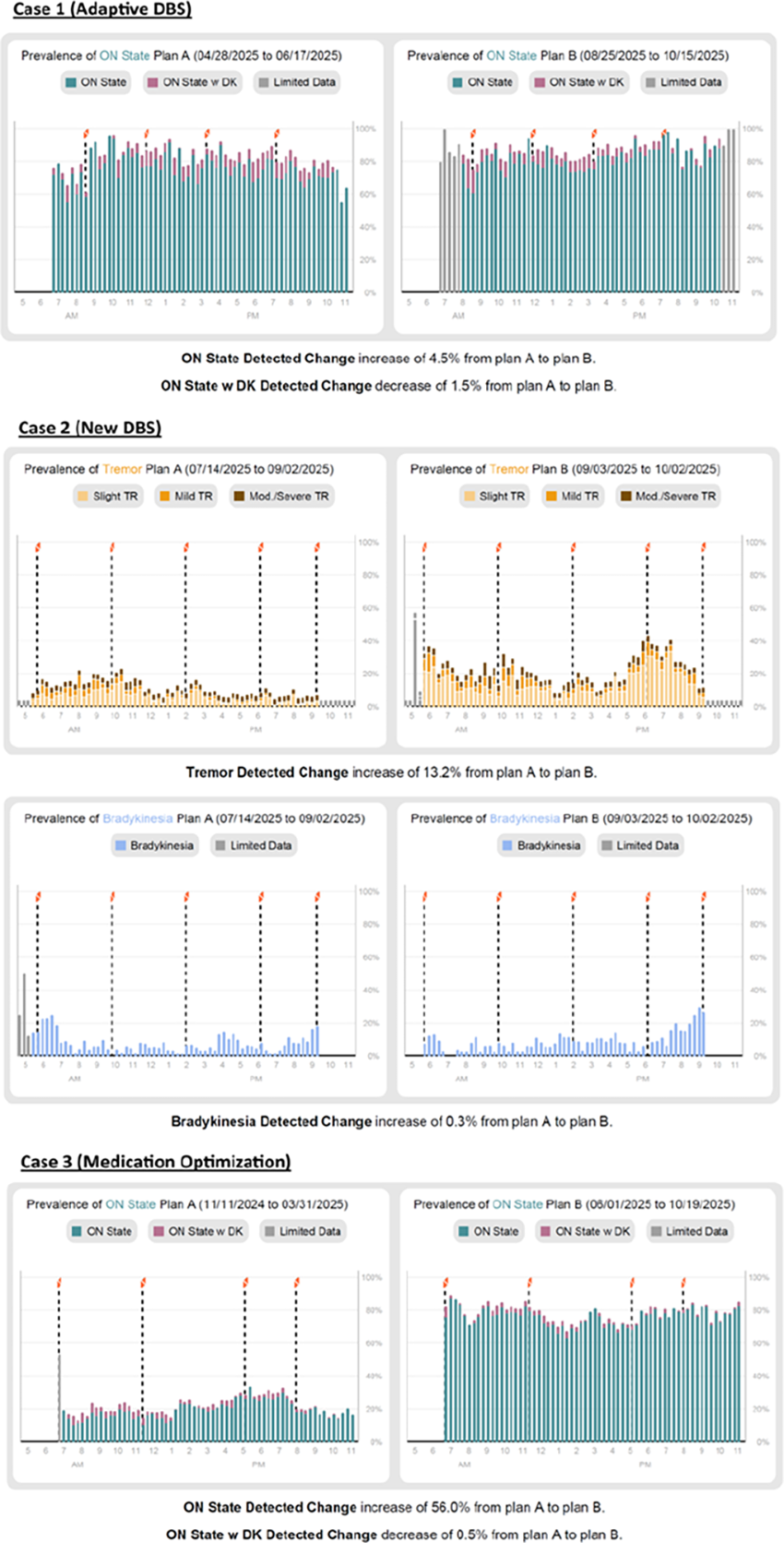
P39.28
1 Graduate School of Media and Governance, Keio University, Kanagawa, Japan, Japan
2 (1) Graduate School of Media and Governance, Keio University, Kanagawa, Japan (2) ORPHE Inc., Tokyo, Japan (3) Research Center for Music Science, Keio University Global Research Institute, Tokyo, Japan, Japan
3 Reiwa Health Sciences University, Fukuoka, Japan, Japan
4 Artificial Intelligence Research Center, National Institute of Advanced Industrial Science and Technology (AIST), Tokyo, Japan, Japan
5 Keio Research Institute at SFC, Kanagawa, Japan, Japan
6 (1) Research Center for Music Science, Keio University Global Research Institute, Tokyo, Japan (2) Faculty of Environment and Information Studies, Keio University, Kanagawa, Japan, Japan
People with Parkinson’s disease (PwP) frequently experience gait disorders, exhibiting reduced stride length and increased anxiety about walking. Rhythmic auditory stimulation (RAS), primarily based on fixed-tempo auditory cues, has been reported to alleviate such gait disorders. However, in daily life, because walking often involves turning in interaction with diverse environments, maintaining a fixed-tempo gait is not feasible. Recently, an auditory feedback system that provides a sound at each foot strike has been reported to significantly increase the distance walked in the 6-Minute Walk Test in PwP. A step-triggered auditory feedback system may improve gait quality, such as stride length and strike angle, even in turning, where walking tempo naturally varies. Therefore, we developed a motion-sensor-based step-triggered auditory feedback system (ORPHE DRumner) and examined whether it increases stride length and strike angle in PwP during turning gait, compared with fixed-tempo and no-sound conditions. Twenty-one PwP (69.3 ± 5.8 years old; mean ± SD) participated in this study. They wore shoes equipped with motion sensors mounted on the shoe instep to measure gait features. The participants completed three laps of the figure-of-eight walk test (F8WT) under each of the following three conditions: 1) step-triggered (ORPHE DRumner), 2) fixed-tempo, and 3) no-sound. Acceleration and angular velocity data were recorded at 200 Hz from the sensors during F8WT. The mean stride length and strike angle were calculated from these data using gait-analysis software (ORPHE Inc.). Two linear mixed-effects models were constructed, with the mean stride length and the mean strike angle as the response variables, respectively. In both models, condition was included as a fixed effect, and participant ID was included as a random effect. As a result, the mean stride length was significantly larger in the step-triggered feedback condition than in the fixed-tempo (β = 0.027, p = 0.003) and no-sound (β = 0.02, p = 0.03) conditions. Similarly, the mean strike angle was significantly larger in the step-triggered feedback condition than in the fixed-tempo (β = 1.09, p < 0.001) and no-sound (β = 0.83, p < 0.001) conditions. We demonstrated the effectiveness of a step-triggered auditory feedback system in improving gait quality during turning in PwP. These results suggest that ORPHE DRumner may be more effective than RAS in supporting daily-life walking in PwP.
P39.29
1 My Moves Matter, Ireland
2 My Moves Matter, Switzerland
Introduction Access to registered dietitians for people with Parkinson’s (PwP) in the UK and Ireland is very limited—only 15% of 1,400 PwP in Ireland have access. My Moves Matter created MediPD, an online Mediterranean diet programme designed by dietitians and delivered by a British avatar, Kayla. The programme includes video modules supported by an ‘Ask the dietitian’ chat group and downloadable resources. A three-week market test pilot in the UK aimed to test (i) acceptability and usability of the content, avatar and platform (ii) adherence and change in knowledge and Mediterranean diet score (MDS) and (iii) willingness to pay among PwP.
Methods Recruitment targeted UK members of the My Moves Matter database. 146 PwP applied for the test pilot and 30 participants (PwP and care partners) were selected representing a range of demographics and disease stages. PwP consented to take part in the programme. Data collected included engagement tracking, pre- and post-programme nutrition quiz and MDS, an online survey and online semi-structured interviews. The MDS combined elements of the mediterranean diet score and the MIND diet score.
Results MediPD had a high engagement rate (60% completion, 18 participants), outperforming typical online course rates by 4–20 times. 89% were satisfied or very satisfied, and 89% would recommend the programme. Kayla, the avatar, was easy to understand for all users. The average Mediterranean diet score improved from 8.7/20 to 11.9/20, and nutrition quiz scores rose from 65% to 84%. Post-pilot surveys (n=19) and interviews (n=10) showed participants rated their likelihood of making dietary changes at 9.4/10, and all interviewees reported at least one positive change. Two reported better bowel motion frequency. Trust in MediPD was universal due to its dietitian-led design. Willingness to pay was strong (77% would pay; average price £100). 37% believed it should be funded by third parties like the NHS or Parkinson’s charities.
Conclusion The MediPD market test pilot shows that online nutrition education is acceptable, feasible, and effective for PwP, yielding improvements in diet and knowledge. The paid program has been launched and continues to evolve based on participant feedback. Future plans include clinical research, collaboration with organizations like Parkinson’s UK and the NHS and beyond to expand access and further development of a full generative AI Nutrition platform to meet the nutrition care gap for PwP.
P39.30
1 Department of Neurology, Hospital Universitario 12 de Octubre, Madrid, Spain., Spain
2 Ken and Ruth Davee Department of Neurology, Northwestern University, Feinberg School of Medicine, Chicago, IL, USA., United States
3 Department of Neurology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA 15213, USA., United States
4 Sydney School of Health Sciences, Faculty of Medicine and Health, The University of Sydney, NSW 2006, Australia., Australia
5 Davis Phinney Foundation ambassador, United States
6 Senior Wealth Advisor, Portfolio Manager Scotia Wealth Management ® | ScotiaMcLeod ® , a division of Scotia Capital Inc. The Morse Group 95 St. Clair Avenue West, Suite 1400, Toronto, Ontario, M4V 1N6 Canada., Canada
7 Department of Neurology, Faculty of Medicine, Pavol Jozef Šafárik University, 04001 Košice, Slovakia., Slovakia
8 Department of Neurological Sciences, Rush University Medical Center, Chicago, Illinois, USA., United States
9 Clinical Department, CHDI Management/CHDI Foundation, Princeton, New Jersey, USA., United States
10 Department of Neurology, Medical University of South Carolina, Charleston, South Carolina, USA., United States
11 Kilimanjaro Christian Medical Centre, Moshi, Kilimanjaro, Tanzania., Tanzania
12 Senior Medical Officer (Ret.), Division of Neurology 1, Office of Neuroscience, U.S. Food and Drug Administration, Silver Spring, MD, USA., United States
13 Division of Movement Disorders Department of Neurology Yale School of Medicine 300 George St, Floor 3 New Haven CT. 06511 USA., United States
14 Department of Neurology, University Medical Centre Schleswig-Holstein and Kiel University, Kiel, Germany., Germany
15 James J. and Joan A. Gardner Family Center for Parkinson's Disease and Movement Disorders, Department of Neurology, University of Cincinnati, Cincinnati, OH 45219, USA., United States
16 Center for Networked Biomedical Research in Neurodegenerative Diseases (CIBERNED), Carlos III Institute of Health, Madrid, Spain., Spain
17 Ottawa Hospital Research Institute, University of Ottawa Brain and Mind Research Institute, Ottawa, Ontario, Canada., Canada
INTRODUCTION Traditionally, diaries in Parkinson’s disease (PD) monitor motor fluctuations but often overlook other motor and non-motor features. To address this, the International Parkinson and Movement Disorder Society (MDS) is developing an e-Diary (PD Diary by MDS), a patient-centered digital tool to capture the impact of PD on daily life. Phase 1 (2023–2024) defined key specifications via a multi-stakeholder Delphi process with people with Parkinson’s disease (PwP), care partners, clinicians, industry, and regulators. Consensus emphasized the measurement of daily function and disease progression, alongside accessibility across platforms. The tool will have two complementary modes: a Personal mode, allowing tailored tracking of relevant symptoms and activities, and a Research mode, with a fixed set of validated items for research and clinical trials. We present ongoing Phase 2 results on development, cognitive pretesting, and usability.
METHODS Phase 2 involved 10 PwP and 5 care partners in iterative evaluations combining quantitative and qualitative feedback. Participants first completed cognitive pretesting of the symptoms and activities items, assessing comprehension, meaningfulness, and preferred response format (categorical vs. visual analog scales [VAS]). They then interacted with an early prototype, completing predefined critical tasks, and subsequently rated usability using the System Usability Scale (SUS). Finally, participants took part in individual interviews with project team members to provide qualitative feedback on prototype interaction.
RESULTS Categorical response options were generally preferred over VAS, which were visually cluttered and more difficult to interpret. Minor wording issues were identified and refined via free-text feedback. Activities items were better understood than symptoms items, and early-stage PwP showed higher comprehension than advanced-stage PwP and care partners. Common usability challenges included technical or clinical language, long item lists, and navigation difficulties–particularly for medication tracking. Participant feedback guided subsequent refinements of item wording, response formats, and interface design.
CONCLUSION Phase 2 identified key usability and comprehension issues, guiding early prototype refinement. Subsequent stages, including iterative usability refinement, reliability testing, and pilot validation with additional stakeholders, are ongoing.
P39.31
1 University College Dublin, Ireland
2 University of Toronto, Canada
Background Considerable evidence indicates that dance can improve motor outcomes for people with Parkinson’s. However, most studies to date have relied on standardized clinical measures to assess outcomes such as gait, balance, and functional mobility. Quantitative kinematic measures can provide more precise data on different aspects of movement that may be enhanced by dance, as well as upper-body movements that are not well captured by current assessment tools. Computer vision, an artificial intelligence (AI) approach, has recently been applied to simple hand movements in people with Parkinson’s, and has the potential to be used as a low-cost tool to assess disease progression and therapeutic outcomes.
Methods A computer vision-based pose estimation analysis pipeline was developed using Mediapipe, an open-source machine learning framework, with a custom Python script. Pilot data were collected using home webcams from two individuals with mild to moderate Parkinson’s (one female, one male, aged 63 and 66 years respectively). The participants practiced short, seated dance sequences that included unilateral and bilateral movements in two sessions approximately one week apart. This preliminary analysis focused on the shoulder, elbow, and wrist joints of left and right upper limbs. Metrics included velocity, path length, and range of motion.
Results The pipeline successfully extracted kinematic data from home webcam recordings. Analysis indicates that both participants showed a pattern of increased velocity and path length across joints between sessions. One participant also demonstrated increased range of motion.
Conclusions This study provides initial proof-of-concept that computer vision can be used to analyze kinematics of complex movements like dance in people with Parkinson’s. Future work will focus on identifying kinematic signatures of dance movement in Parkinson’s.
CLINICAL SCIENCES: Neuroimaging
P40.01
1 UNESP - Universidade Estadual de São Paulo, Brazil
2 UNESP, Brazil
3 UFABC, Brazil
Introduction: Turning requires significant postural and cognitive control, involving body reorientation and anticipatory adjustments for stability. Individuals with Parkinson's disease (PD) exhibit increased turning time, more steps, and reduced trunk and neck motion, explained by increased prefrontal cortex activity, indicating low movement automaticity. This is worse in patients with freezing of gait (FoG), for whom turns are known triggers. The neural correlate for this worse performance remains unclear. One hypothesis is that the dorsolateral prefrontal area, which is dysfunctional in FoG, is activated due to higher cognitive demand during turning. Aim: To investigate cortical activity during turning in people with PD with (FoG) and without FoG (nFoG) during a simple task (ST) and a dual cognitive task (DT). Materials and Methods: Eleven participants with idiopathic PD (6 FoG, 5 nFoG; H&Y I-III; age 55 years; CAAEE #55703722.9.0000.5594) in the ON medication state performed alternating 360° turns at a self-selected pace for 30s (4 series), interspersed with 30s rest. In the DT condition, participants turned while mentally counting a specific number presented by audio. “Turn/stop” commands were audio-patterned. Oxyhemoglobin in the dorsolateral prefrontal region (OxDorso) was measured by fNIRS. A repeated measures ANOVA was conducted with factors Group (FoG x nFoG) x Condition (ST x DT) x Turn (stop x turn), followed by Bonferroni post-hoc if necessary. Result: For OxDorso, a significant ConditionxTurn interaction was found (F=5.316, p=0.046, ƞp2=0.371). Post-hoc analysis revealed that for both groups, DT turning resulted in significantly higher OxDorso compared to ST turning. No significant differences were observed for Condition (F=1.587, p=0.239, ƞp2=0.149) or Turn (F=0.187, p=0.676, ƞp2=0.020). Conclusion: OxDorso analysis showed a significant increase in neural recruitment during DT turning, indicating that adding a cognitive task exacerbates cortical demand during turning, regardless of FoG/nFoG group.
Funding: CAPES financially supports this project with scholarships, and the Michael J Fox Foundation funds the researcher.
Keywords: turning, walking, freezing of gait, Parkinson’s disease
P40.02
1 Department of Neurology, College of Medicine, The Catholic University of Korea, Seoul, South Korea
2 USC Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Cognitive impairment is a prevalent non-motor symptom in Parkinson's disease (PD). PD is characterized by striatal dopamine depletion and deep gray matter atrophy, with early cognitive decline often attributed to dopaminergic system dysfunction. We aimed to explore disparities in cognition based on based on striatal dopamine availability and regional brain volume among PD patients. This study included 287 patients with newly diagnosed PD who had not yet started. They all underwent brain magnetic resonance imaging, positron emission tomography with 18F-N-(3-fluoropropyl)-2beta-carbon ethoxy-3beta-(4-iodophenyl) nortropane, and 123I-MIBG scintigraphy. Patients were classified as having normal cognition, mild cognitive impairment, or PD dementia based on Seoul Neuropsychological Screening Battery-II, which includes 31 subsets covering activities of daily living and 5 cognitive domains. Using the Subtype and Stage Inference (SuStaIn) machine-learning technique, we categorized PD patients into subtypes by analyzing their progression patterns in deep gray matter atrophy and dopamine availability, and evaluated differences in cognition among these subtypes. SuStaIn algorithm categorized them into four distinctive subtypes: subtype 1 (n = 181), subtype 2 (n = 36), subtype 3 (n = 27), and subtype 4 (n = 31). The mean age of subtype 2 was lower than other groups. Motor symptoms in subtype 2 was milder than other subtypes. Subtype 2 showed higher cognitive function and subtype 3 and 4 displayed larger proportion of dementia. Subtype 1 and 2 generally showed less decrease of brain atrophy and dopamine availability than subtype 3 and 4. Subtype 1 showed early dopamine availability decrease and late brain volume reduction, while in subtype 2, brain atrophy was decreased initially, followed by dopamine availability. Subtype 3 and 4 were mixed type, in which initial change was globus pallidus atrophy and dopamine availability and brain atrophy were reduced similarlily. Our finding underscores the association between decreased dopamine availability and volume with cognitive dysfunction in PD. The typical pattern of initial decrease of dopamine availability or deep gray matter volume was associated with mild cognitive dysfunction, while mixed decreased pattern of dopamine availability and deep gray matter volume was linked to severe cognitive dysfunction, highlighting the spatiotemporal association between dopaminergic and structural pathology in cognitive impairment in PD.
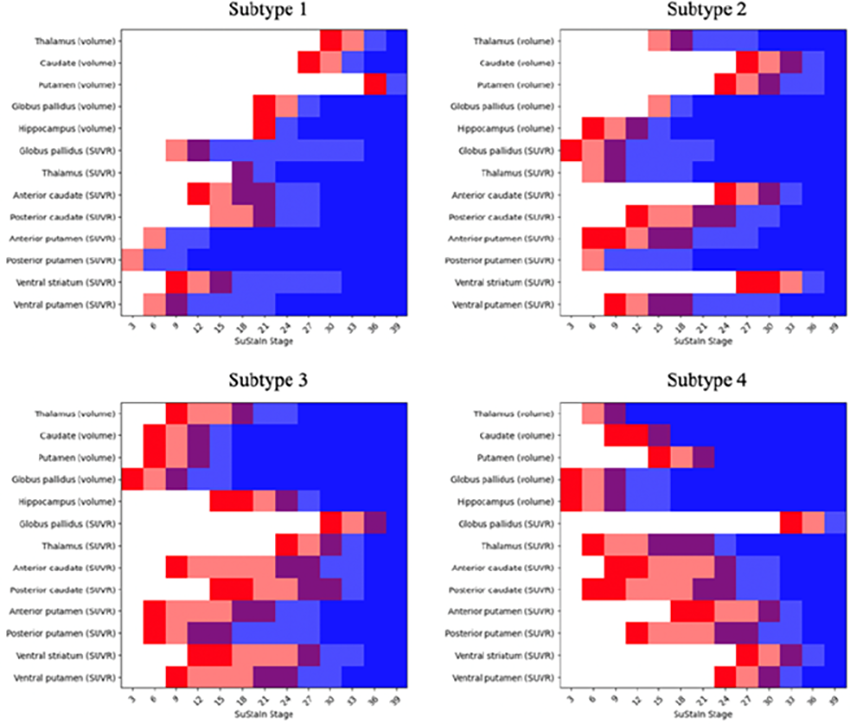
P40.03
1 Institute of Neurobiology, National Autonomous University of Mexico (UNAM), Queretaro, Mexico., Mexico
2 Faculty of Medicine, Autonomous University of Querétaro / Parkinson Care Clinic, Angeles Centro Sur Hospital, Queretaro, Mexico., Mexico
3 International Laboratory for Human Genome Research, National Autonomous University of Mexico (UNAM), Queretaro, Mexico., Mexico
4 Cognitive Neurogenomics Laboratory, Faculty of Psychology, National Autonomous University of Mexico (UNAM), Mexico City, Mexico., Mexico
5 Anahuac University, Mexico
6 School of Biomedical Sciences, Faculty of Health, Medicine, and Behavioural Sciences, The University of Queensland, Brisbane, QLD, Australia / Brain & Mental Health Program, QIMR Berghofer Medical Research Institute, Brisbane, QLD, Australia., Mexico
Introduction: Parkinson's disease is a neurodegenerative disease characterized by loss of dopaminergic neurons in the Substantia Nigra and the accumulation of alpha-synuclein in nerve cells. A wide range of symptoms may occur in Parkinson's disease. Cognitive impairment is a relatively common occurrence, the prevalence of cognitive impairment associated with Parkinson's disease is between 20 and 40 percent. However, the anatomical and functional brain bases of cognitive impairment in Parkinson's disease remains poorly understood.
Objectives: We aim to characterize brain phenotypes associated with cognitive performance in a cohort of Mexican Parkinson’s Disease patients.
Methods: Cognitive performance was assessed in a sample of 70 PD patients (42 males; 65.2 ± 10.8 years old) using the Montreal Cognitive Assessment (MoCA). Magnetic resonance imaging was acquired on a 3 T scanner, including high-resolution T1 and T2 weighted imaging, Resting-State functional MRI, neuromelanin-weighted imaging, and diffusion-weighted imaging. Brain volumes—comprising subcortical and cortical gray matter, white matter, cerebrospinal fluid, and 58 bilateral regions—were estimated using the AssemblyNet pipeline, a robust deep-learning–based tool for whole-brain MRI segmentation validated in diverse pathologies. To normalize for interindividual variation in overall brain size, volumes were expressed as a percentage of intracranial volume (%ICV). General linear models were utilized to predict MoCA scores from global and regional brain volumes, with age, sex, and years of education included as covariates.
Results: A significant positive association was identified for subcortical gray matter volume and cognitive performance (p < 0.001), thus, lower volumes are associated with lower MoCA scores. In contrast, cerebrospinal fluid (CSF) volume showed a negative association with cognitive performance in PD patients (p < 0.05). Furthermore, volumes of key subcortical structures—including the nucleus accumbens, thalamus, caudate, putamen, and hippocampus— also showed positive associations with MoCA scores, indicating that reductions in the volume correspond with poorer cognitive functioning.
Conclusion: Several subcortical structures shown to be associated with cognitive functioning in PD patients, including accumbens, caudate, putamen, thalamus and hippocampus, highlighting the role of these regions in cognitive function and cognitive impairment, a common non-motor symptom of Parkinson’s disease.
P40.04
1 UNAM, Mexico
2 Institute of Neurobiology, National Autonomous University of Mexico (UNAM), Queretaro, Mexico., Mexico
3 Faculty of Medicine, Autonomous University of Querétaro / Parkinson Care Clinic, Angeles Centro Sur Hospital, Queretaro, Mexico., Mexico
4 International Laboratory for Human Genome Research, National Autonomous University of Mexico (UNAM), Queretaro, Mexico., Mexico
5 Cognitive Neurogenomics Laboratory, Faculty of Psychology, National Autonomous University of Mexico (UNAM), Mexico City, Mexico., Mexico
6 Anahuac University, Mexico
7 School of Biomedical Sciences, Faculty of Health, Medicine, and Behavioural Sciences, The University of Queensland, Brisbane, QLD, Australia / Brain & Mental Health Program, QIMR Berghofer Medical Research Institute, Brisbane, QLD, Australia., Australia
Introduction: Parkinson's disease (PD) is a neurodegenerative disorder characterized by progressive loss of dopaminergic neurons in the basal ganglia, specifically in the substantia nigra. It is the most common neurodegenerative disease after Alzheimer's Disease. Bradykinesia, rigidity, and rest tremor constitute the cardinal motor features observed in PD patients. Concurrently, memory impairment represents one of the primary non-motor dysfunctions associated with the condition.
Objective: To investigate the association between white matter lesion and global cognitive function in a cohort of Mexican patients with PD.
Methods: A cohort study was conducted on 71 Mexican patients with PD (42 males; mean age 65.2 ± 10.8 years). Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA). Structural brain images were acquired on a 3 T Magnetic Resonance Imaging scanner (MRI), including T1 and T2-FLAIR weighted images. The T1w and FLAIR images were processed using the DeepLessionBrain tool, an automated deep-learning pipeline to identify and quantify the volume of white matter (WM) lesions. The Lesion Burden was quantified as the proportion of lesion volume relative to the volume of normal-appearing white matter. Finally, WM lesions volumes were entered as predictors of MoCA score in a General Linear Model adjusted for age, sex, and years of education.
Results: Periventricular lesions were the most frequent WM lesion subtype, observed in 78.9% of participants, compared to 15.5% with juxtacortical and 4.2% with deep white matter lesions. In the adjusted model, total WM lesion burden was a statistically significant negative predictor of MoCA (β = –1.867, p = 0.042). When decomposed by region, the periventricular lesion burden (PLB) specifically drove the association (β = -2.178, p = 0.024), indicating that a larger periventricular lesion volume is strongly associated with lower global cognitive scores.
Conclusion: The findings from this cohort demonstrate a negative association between the volume of lesions in the periventricular white matter and global cognitive function of patients with PD. These findings suggest that periventricular WM lesions may serve as an imaging biomarker of cognitive decline in PD.
P40.05
1 Roche Pharma and Early Development (pRED), Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland
2 Roche Pharma Research and Early Development (pRED), Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland
3 Roche Products Ltd, Welwyn Garden City, United Kingdom
4 Product Development Neurology, Roche Pharma Development, F. Hoffmann-La Roche Ltd, Basel, Switzerland
5 Product Development Data Science, F. Hoffmann-La Roche Ltd, Basel, Switzerland
6 Roche Pharma Research and Early Development (pRED), Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland; University of Exeter Medical School, London, United Kingdom
Introduction: To evaluate the effects of prasinezumab on neuroimaging biomarkers in individuals with early-stage Parkinson’s disease (PD) on stable symptomatic medication.
Methods: The PADOVA study (NCT04777331) evaluated the efficacy, safety and pharmacokinetics of prasinezumab in early-stage PD participants on stable monoamine oxidase type B inhibitor (MAO-Bi) or levodopa monotherapy. Biomarker endpoints included magnetic resonance imaging (MRI) of basal ganglia (putamen and caudate) and substantia nigra pars compacta (SNpc) using a T1-weighted neuromelanin (NM)-sensitive sequence as well as R2* relaxometry sensitive to iron deposition at baseline and week 76 at sites where the respective sequences were available.
Results: Of 586 enrolled participants, 194 provided longitudinal NM-MRI scans and 202 provided iron-sensitive MRI scans for analysis based on automated segmentation of regions of interest. In pre-specified analysis of covariance (ANCOVA) models, changes in SNpc NM intensity showed a trend towards an increase in the prasinezumab group (adjusted mean change [95% confidence interval]: 0.18 [-0.18, 0.55]), compared to a decline in the placebo group (-0.16 [-0.52, 0.20]; p=0.0792). Prasinezumab treatment was also associated with a decrease in SNpc iron, with concurrent progressive iron accumulation in the placebo group (-0.06 [-1.33, 0.27] vs. 0.47 [-0.26, 1.21], p=0.1903). This pattern was more pronounced in the putamen (-0.22 [-.62, 0.18] vs. 0.43 [0.05, 0.82], p=0.0025). Notably, further correlation analysis confirmed links between NM, iron, dopamine transporter-single-photon emission computed tomography (DaT-SPECT) and Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Part III.
Conclusions: Exploratory biomarker analysis of PADOVA suggests that prasinezumab is biologically active. This is supported by imaging biomarkers crucial to PD pathology, showing a slowing in the progressive loss of NM signal in SNpc and reduced iron accumulation in the putamen.
Abstract has been submitted for consideration to the 2026 Alzheimer's & Parkinson's Diseases Conference (AD/PD).
P40.06
1 Institut des Sciences Cognitives Marc Jeannerod, CNRS UMR 5229, Bron, France - Université Claude Bernard Lyon 1, Lyon, France., France
2 Institut des Sciences Cognitives Marc Jeannerod, CNRS UMR 5229, Bron, France - Université Claude Bernard Lyon 1, Lyon, France - Hôpital de Vienne, France, France
3 Hôpital des Charpennes, Hospices Civils de Lyon, Villeurbanne, France, France
4 Institut des Sciences Cognitives Marc Jeannerod, CNRS UMR 5229, Bron, France - Université Claude Bernard Lyon 1, Lyon, France - Hôpital de Vienne, France, France
5 Institut des Sciences Cognitives Marc Jeannerod, CNRS UMR 5229, Bron, France - Université Claude Bernard Lyon 1, Lyon, France - Hôpital des Charpennes, Hospices Civils de Lyon, Villeurbanne, France, France
6 CERMEP, Claude Bernard Université Lyon 1, Villeurbanne, France, France
Background: In Parkinson’s disease (PD), the pituitary gland—a central regulator of the hypothalamic–pituitary–adrenal (HPA) axis and broader endocrine function—remains largely unexplored. However, dysregulation of the HPA axis and serotonergic signaling via 5-HT₄ receptor subtypes may contribute to the non-motor symptoms of the disease. PD affects men approximately twice as often as women, suggesting that gender-related differences in neuroendocrine regulation could impact pituitary and serotonin function. Together, these observations suggest that the pituitary may represent a key, yet overlooked, contributor to PD pathophysiology.
Objectives: We investigated pituitary volume and 5-HT₄ receptor expression in early-stage PD patients compared with healthy controls, stratified by gender, to identify potential alterations.
Methods: Twenty PD patients (7 women; 13 men; disease duration 2–8 years) and 15 age- and sex-matched controls (including 6 women) underwent high-resolution MRI and PET with the 5-HT4 receptor ligand [11C]SB207145. The pituitary was manually segmented on each subject’s anatomical MRI to delineate its anterior and posterior lobes. MRI and PET volumes were coregistered, and parametric images were computed using SRTM model. Pituitary volumes were computed from the segmented masks. Group and gender effects were analyzed using t-tests, ANOVA, and ANCOVA, with correlations between volume and non-displaceable binding potential (BPND) assessed.
Results: PD patients exhibited smaller pituitary volumes than controls (anterior lobe: 402.5 ± 106.1 vs 471.9 ± 107.6 mm3, p = 0.042; total lobes: 519.6 ± 119.7 vs 604.7 ± 121.5 mm3, p = 0.033), with male PD patients showing marked atrophy (>30% reduction). No differences were observed in 5-HT₄ BPND between PD and controls, though females exhibited higher BPND than males (p = 0.027) in the anterior pituitary. The anterior pituitary volume correlated positively with anterior BPND (r = 0.37, p = 0.028) whatever the group considered (patients or controls). And age was associated with lower BPND independently of group effects.
Conclusions: Our preliminary results show that, at the onset of the disease, pituitary atrophy is detected specifically in men, while the binding potential of SB207145, which exhibits gender-related differences, is preserved.
Further analysis will determine whether these changes are associated with specific symptoms.
P40.07
1 Boston University, United States
Introduction: Walking difficulty in people with Parkinson disease (PwPD) arising from diminished gait automaticity is compensated by increased attention to walking through greater prefrontal cortex (PFC) activation. Rhythmic auditory stimulation (RAS) may improve gait, but its impact on the attentional demand of walking is unclear. Using functional near infrared spectroscopy (fNIRS) and wearable sensors, we examined PFC activation and gait during RAS-augmented walking compared to cognitive-motor dual-tasking. We hypothesized that RAS would improve gait and reduce PFC activation, while dual-task walking would impair gait and increase PFC activation.
Participants: 18 PwPD (age: 71.4 [5.70] yrs) with Hoehn & Yahr 2.
Methods: Participants walked under four conditions: single-task walking, dual-task walking (serial-3 subtractions), and walking with RAS at 100% (RAS-100) and 110% (RAS-110) of their usual cadence. Conditions were randomized, and each alternated with single-task walking. fNIRS (NIRSport2, NIRx) measured PFC activation as change in oxygenated hemoglobin (HbO2) relative to single-task walking. Data were processed using Homer3. Right and left PFC activations were calculated by averaging HbO2 in inferior, middle, and superior frontal regions per hemisphere. Wearable sensors captured changes in gait speed, cadence, and stride length relative to single-task walking. Repeated measures ANOVA with posthoc comparisons examined differences in PFC and gait outcomes across conditions.
Results: Relative to single-task walking, HbO2 decreased during RAS-walking (PFC deactivation) and increased during dual-task walking (PFC activation). For both right and left PFC, cortical activity differed across conditions (p<0.05), with RAS-110 significantly lower than dual-task walking. Similarly, gait speed, cadence, and stride length differed significantly across conditions (p<0.05), with greatest improvements during RAS-110, followed by RAS-100, relative to dual-task walking. While greater PFC deactivation occurred in RAS-110 than RAS-100, these differences were not significant.
Conclusion/ implications: RAS-walking in PwPD improved gait and reduced PFC activation compared to a known attention-demanding condition, suggesting improved gait automaticity (i.e., reduced attentional demand). Faster RAS tempos further reduced PFC activation, suggesting greater attentional benefit when walking faster. These results have implications for expanding RAS utilization in the community.
P40.08
1 Boston University, United States
Introduction: People with Parkinson disease (PwPD) lose gait automaticity and consequently increase their reliance on attentional resources in the prefrontal cortex (PFC) during walking. Rhythmic auditory stimulation (RAS) may improve walking automaticity, but how its effect might vary with cognitive ability is unknown. We hypothesized that PwPD with poorer cognition would preferentially benefit from RAS intervention, as evidenced by reduced PFC activity.
Methods: 21 PwPD (mean [sd] age: 71 [6.5]), Hoehn & Yahr = 2) participated in a walking study. Functional near-infrared spectroscopy (NIRx NIRSport2) measured PFC activation during usual and RAS-assisted walking at 100% and 110% of usual cadence (RAS100, RAS110). Changes in oxygenated hemoglobin (HbO2) during each condition, relative to usual walking, were analyzed in Homer3 with spline Savitzky-Golay motion correction and drift regression within the general linear model. Since responses were similar across hemispheres, changes in HbO2 were averaged across all PFC regions to calculate PFC activation. Global cognition was assessed using the Montreal Cognitive Assessment (MoCA) and executive function was assessed using the Stroop Test. The relationship between change in PFC HbO2 during RAS-assisted walking and each cognitive variable was examined using Spearman’s correlations. Differences in brain activation between PwPD with mild cognitive impairment (MCI, MoCA score < 26, n=9) and without MCI (n=12) were examined using Mann-Whitney U tests.
Results: PFC HbO2 generally decreased during both RAS conditions, indicating reduced cognitive load. Lower MoCA scores (poorer cognition) correlated with greater HbO2 decreases during RAS110 (rho=.57, p=.006). Lower Stroop scores (poorer executive function) correlated with greater HbO2 decreases during RAS100 (rho=.48, p=.027). Relative to the non-MCI group, the MCI group had greater HbO2 reductions during both RAS conditions, with a significant group difference in the RAS110 condition (effect size=.62, p=.004).
Conclusions: Reductions in PFC HbO2 during cued walking relative to usual walking suggested decreased attentional demands during RAS. Cognitively-impaired PwPD had a more robust response to RAS than those without cognitive impairment, indicating a larger benefit when walking with RAS. Given the limited treatment options for cognitively-impaired PwPD, it is critical to identify effective and viable interventions to improve gait in this population.
P40.09
1 Arizona State University, United States
2 Mayo Clinic - Phoenix, United States
Introduction: People with Parkinson’s Disease (PwPD) have impaired reactive stepping, defined as quick movements to regain balance after an unexpected step or trip, which increases their fall-risk. In PwPD, reactive balance can be trained through practice, however these improvements are often variable across subjects. Identifying neurological predictors and potential mechanisms of this variability can improve the efficiency of rehabilitation. This study investigated the association between improvements in reactive stepping performance through training and resting-state functional magnetic resonance imaging (rs-fMRI) in PwPD.
Methods: Participants (16 PwPD) underwent rs-fMRI and an eighteen-week multiple-baseline study, which included baseline assessments (B1 and B2 2-weeks apart), a 2-week training protocol, and post-training assessments immediately after protocol (P1) and a 2-month later (P2), in which we assessed margin of stability (MOS) at first foot contact. Functional connectivity was explored using a region of interest (ROI) analysis approach including the left (L) and right (R) caudate, L/R putamen, L/R thalamus, L/R amygdala, L/R hippocampus, L/R cerebellum, and L/R basal forebrain. ROI connections were correlated with immediate learning (P1-B2) and long-term learning (P2-B2) MOS covarying for age and MDS-UPDRS part III scores.
Results: Immediate Learning (P1-B2): We observed a positive correlation between MOS and functional connectivity in the R. thalamus-R. amygdala (pFDR’s<0.05). Long-Term Learning (P2-B2): We observed a positive correlation between MOS and functional connectivity in the L. caudate-L. hippocampus, L. thalamus-L. hippocampus, and R. thalamus-R. amygdala (pFDR’s<0.05). These findings suggest that stronger resting state connections are related to better stepping performance.
Conclusion: These findings highlight the importance of thalamo-limbic coupling in immediate motor and long-term motor learning in PD and could aid in identifying PwPD who would benefit most from balance rehabilitation.
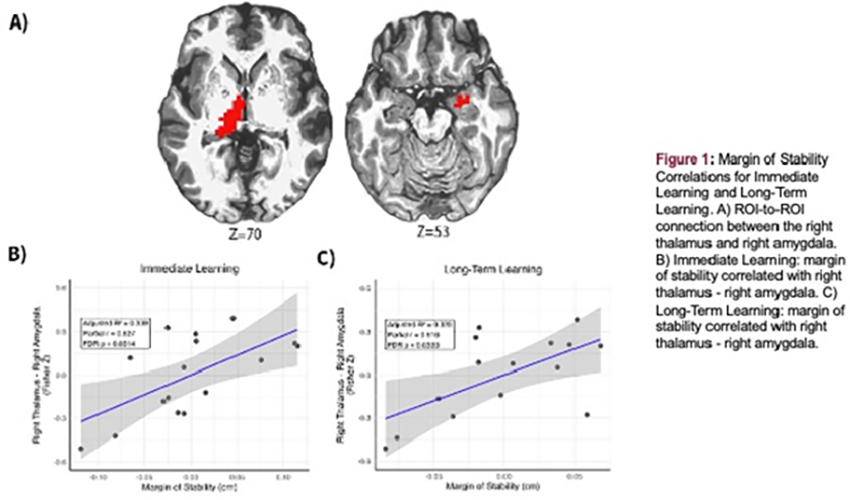
P40.10
1 Barrow Neuroimaging Innovation Center/Arizona State University, United States
2 Barrow Neurological Institute, United States
3 Arizona State University, United States
4 Binghamton University, Binghamton, United States
Brain connectivity changes have been observed in both Parkinson’s disease and the preclinical 6-hydroxydopamine (6-OHDA) model of Parkinson’s disease (PD) using functional magnetic resonance imaging (fMRI). The 6-OHDA model provides a controlled framework to investigate the effects of selective dopaminergic neurodegeneration on brain network organization. Identifying connectivity changes associated with dopamine loss can advance our understanding of PD pathophysiology and support the development of translational imaging biomarkers. To better capture the network-level effects of dopaminergic loss, we developed an integrated connectomic framework combining functional connectivity (FC), structural connectivity (SC), and FC–SC coupling metrics.
Adult male Fischer F344 rats (n=46; 23 6-OHDA, 23 sham) underwent unilateral 6-OHDA or saline injection into the medial forebrain bundle to induce dopaminergic denervation. MRI was performed on 7T (Bruker magnet) and included resting-state fMRI for FC and diffusion MRI for tractography-based SC. For each dataset, voxel-wise FC and SC matrices were calculated, as well as FC–SC coupling metrics. Group-level differences were assessed using a network-based statistic (|t| > 3.0) with days post-surgery included as a covariate, revealing 14 FC edges, 13 SC edges, and 5 coupling nodes that consistently differed between groups. These biologically constrained features were entered into a LASSO-regularized logistic regression model, which retained 12 non-zero features after regularization (7 FC, 4 SC, and 3 coupling) (Figure 1A). Under leave-one-out cross-validation (LOOCV), the model achieved excellent discrimination performance (AUC = 0.898, accuracy = 0.810, sensitivity = 0.818, specificity = 0.800) (Figure 1B–C). Bootstrap resampling (1000 iterations) confirmed model stability (Figure 1A). The most discriminative connections involved cortico-striatal, sensorimotor, and high-level integrative networks, reflecting both primary and compensatory circuit alterations in Parkinsonian models (Figure 1D).
This integrative connectomic framework demonstrates that combining FC, SC, and FC-SC coupling, together with network-based feature selection, enables robust detection of PD-related network alterations in the 6-OHDA model. Beyond accurate classification, this approach provides a biologically interpretable and translational platform that could be extended to monitor disease progression and evaluate therapeutic interventions in PD.
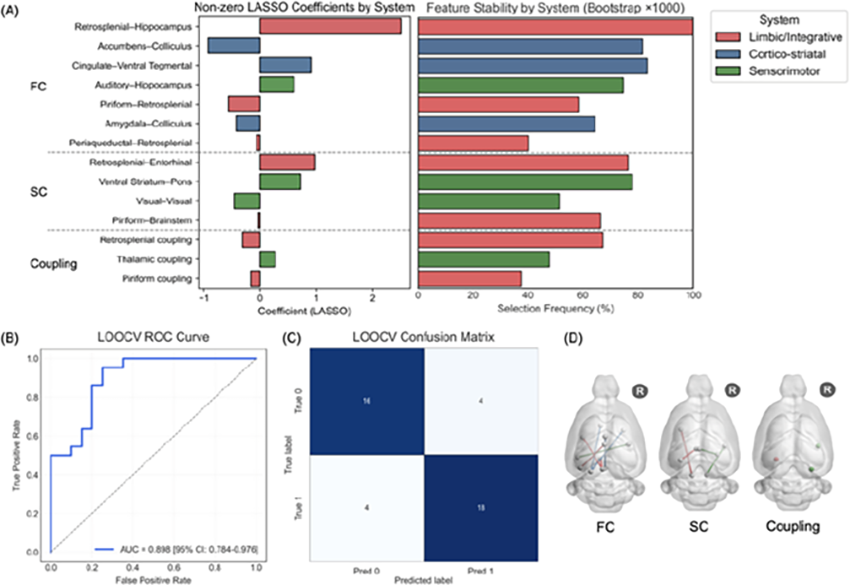
P40.11
1 USC Mark and Mary Stevens Neuroimaging and Informatics Institute, United States
Objective: Resting-state fMRI complexity (rsf-Cplx), an entropy-based measure of brain signal variability, reflects information processing capacity and declines with neurodegenerative progression. Given the role of dopamine in neural network regulation, we investigated rsf-Cplx as an early marker of dopaminergic dysfunction in Parkinson’s Disease (PD). We aimed to compare rsf-Cplx across healthy controls (HC), prodromal, and manifest PD, and to correlate it with dopamine transporter (DAT) availability, motor symptoms, and cognitive function.
Methods: We analyzed data from a small cohort (HC: n=19, Prodromal: n=20, PD: n=20, demographic info. in Fig. A) from the Parkinson's Progression Markers Initiative (PPMI) dataset. rs-fMRI was acquired with 2D EPI sequence with 3.5mm isotropic resolution, TR/TE 2500/30ms, FA 80 degree, for 240 volumes. rsf-Cplx was estimated using Multiscale Sample Entropy with pattern length of m=2 at sensitivity threshold r=0.3 across 10 scales (0.04-0.4Hz). We compared regional rsf-Cplx within PD-related regions of interest across the three groups using ANCOVA. Subsequently, we correlated between rsf-Cplx and DAT-SPECT-Standard Binding Ratio (SBR) in the striatum. Correlations with neuromotor and cognitive function (UPDRS-III, MoCA) were assessed. All statistical analyses were adjusted for age and sex.
Results: ANCOVA showed that rsf-Cplx significantly differed across groups in the postcentral gyrus (postCG, p < 0.05; Fig. B). Specifically, complexity was highest in HC, and lowest in manifest PD. Correlation analyses revealed: 1) trends of positive association between rsf-Cplx and DAT (e.g., postCG: r=0.26, p=0.052; precentral gyrus: r=0.22, p=0.099, Fig. C); 2) positive correlations between rsf-Cplx and MoCA scores (Superior and Inferior Frontal Gyri: r=0.29-0.32, p=0.015-0.026, Fig. D).
Conclusion: Our findings suggest that rsf-Cplx progressively declines from healthy aging to prodromal to manifest PD, reflecting the course of neurodegeneration. The positive correlations between rsf-Cplx in the motor cortex and DAT availability in the striatum support its potential as an early, non-invasive biomarker. These results suggest that dopaminergic neuronal degeneration leads to an imbalance between excitatory and inhibitory networks, consequently lowering rs-fMRI complexity. This novel metric warrants further investigation in larger longitudinal cohorts as a sensitive marker for early detection and monitoring of disease progression in PD.
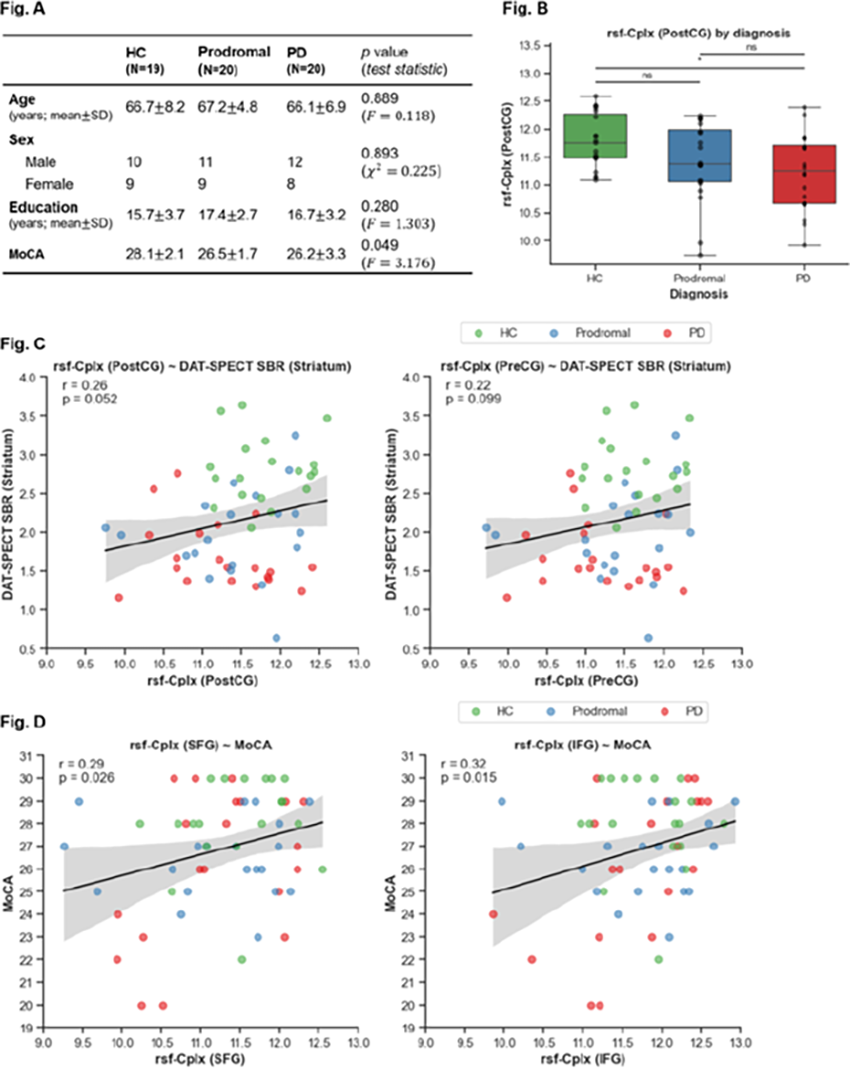
P40.12
1 Creighton University, United States
2 Barrow Neurological Institute, United States
Chronic manganese (Mn) exposure is linked to development of movement disorders including parkinsonism. Occupational inhalation of Mn-containing welding fumes results in toxicant deposition in the basal ganglia. T1-weighted MR imaging can be utilized to detect and quantify the deposition by extracting signal intensity indices. The present study examined longitudinal signal changes in the globus pallidus correlated with worsening motor control symptoms in occupationally exposed workers. Mn-exposed workers (n= 29; 81 visits) were recruited from multiple welding sites and completed at least two study visits. Each visit included T1-weighted MRI, occupational exposure assessment, and neurologic evaluation by a movement disorder specialist. Automatic segmentation of the MRI was performed using Freesurfer 6.0 software. A pallidal index (PI) was calculated as the ratio of T1 signal intensity in the globus pallidus to a predefined white matter reference region. Work history was used to calculate cumulative weighted welding exposure (mg Mn/m m3-years), and motor function was assessed using the Unified Parkinson’s Disease Rating Scale 3 (UPDRS3). Linear mixed effects models were employed to evaluate associations between Mn exposure, PI, and UPDRS3 scores, adjusting for scanner, age at baseline, and observation time. We found that PI increased with longer exposure duration (β = 2.814, p < 0.001), and greater intensity of Mn exposure (more exposure in a shorter amount of time) produced greater increases in PI (β = -0.033, p = 0.004). Additionally, greater PI values at baseline were associated with faster motor symptom progression (β = -0.005, p = 0.022). In summary, this study demonstrates an exposure and time-dependent increase in pallidal Mn deposition captured by PI, where greater exposure intensity corresponded to accelerated deposition, and higher PI was linked to acceleration of parkinsonian symptoms. These findings support the longitudinal reliability of PI as a biomarker for Mn exposure and its relevance in potential prediction of motor decline in exposed workers.
P40.13
1 Kimyo International University, Uzbekistan
2 Global Research & Scientific Collaborations Institute, China
3 Global Research & Scientific Collaborations Insitute, China
Background: Identifying neuroanatomical alterations in the prodromal phase of Parkinson’s disease (PD) is crucial for early diagnosis and intervention. Conventional volumetric tools often fail to capture subtle prediagnostic structural changes due to limited sensitivity and reproducibility. Deep learning-based volumetric analysis offers a robust and automated approach to detect small-scale regional variations across the brain.
Methods: This study included MRI scans from 25 prodromal PD and 25 age-matched control participants. Regional brain volumes were estimated using a weakly supervised confidence-integrated deep learning network and normalized to intracranial volume. Group differences were assessed across 109 brain regions for each subject using Welch’s t-tests with Benjamini–Hochberg FDR correction. Dimensionality reduction using principal component analysis (PCA) captured variance patterns, and machine learning classifiers (Random Forest and L1-regularized Logistic Regression) were applied to distinguish prodromal from control cases. Five-fold stratified cross-validation was used for model evaluation.
Results: Univariate analysis revealed significant regional volumetric differences across limbic, subcortical, and ventricular structures, most notably within the choroid plexus, nucleus accumbens, amygdala subnuclei, temporal pole, and third ventricle (q < 0.05). PCA showed that the first 10 components explained ∼75% of total variance, capturing distinct atrophy patterns in prodromal subjects. Machine learning classification achieved robust discrimination between groups, with Random Forest accuracy of 85% and ROC AUC of 0.90, while the sparse logistic model achieved 90% accuracy and AUC = 0.92. Feature importance analysis highlighted choroid plexus, accumbens, paracentral lobule, thalamic pulvinar, and optic chiasm volumes as key discriminative regions.
Conclusion: Deep learning volumetry with machine learning classification enables early detection of prodromal Parkinson’s disease using structural MRI. This framework identifies distinct atrophy patterns preceding motor onset and shows promise as a quantitative imaging biomarker for at-risk individuals.
P40.14
1 Kimyo International University, Uzbekistan
2 Global Research & Scientific Collaborations Institute, China
Background: Quantitative MRI volumetry provides sensitive markers of neurodegenerative progression in Parkinson’s disease (PD), but conventional segmentation tools are limited by variability and low reproducibility in small longitudinal datasets. Recent advances in deep learning offer robust and automated brain volumetry capable of detecting subtle structural changes over time.
Methods: This study investigated progressive brain atrophy in a PD longitudinal cohort using a deep learning based weakly supervised confidence-integrated network (CINet). MRI data from 20 participants were processed to extract cortical and subcortical regional volumes. Linear mixed-effects models with random intercepts were used to quantify temporal changes in normalized volume across follow-up years. Multiple comparisons were corrected using the Benjamini–Hochberg false discovery rate (FDR), and annualized percent volume change was computed relative to baseline means.
Results: Longitudinal analysis revealed region-specific volume reductions consistent with PD-related neurodegeneration. Significant progressive atrophy was observed in the right hippocampus (-1.2%/year), right caudate (-2.3%/year), thalamus (-1.1%/year), and frontal and temporal cortical regions (-1.5 and -2.0%/year) (FDR-adjusted q < 0.05). No regions demonstrated significant volume increase over time. These atrophic patterns align with the known fronto-striatal and limbic network vulnerability observed in early PD pathology.
Conclusions: Deep learning-based longitudinal MRI volumetry can sensitively detect subtle, region-specific progressive brain atrophy in Parkinson’s disease. The weakly supervised framework demonstrated robustness and high reproducibility in small longitudinal datasets, supporting its potential as a quantitative imaging biomarker for disease monitoring. Future work will integrate multimodal imaging, clinical metrics, and dopaminergic biomarkers to validate and generalize this approach to larger PD populations.
P40.15
1 University of Michigan, United States
2 University of Michigan, Ann Arbor, MI, United States
Background: Mobility disturbances, like freezing of gait and falls are among the most debilitating impairments in PD that become less responsive to dopaminergic treatment with advancing disease and impair quality of life. Most research on the dopaminergic system in PD continues to be dominated by the basal ganglia with only scarce information available on extra-striatal regions. The objective of this study is to examine the whole brain (striatal and extra-striatal) topography of dopamine transporters (DAT) in Parkinson's disease (PD) fallers and freezers using a highly sensitive and specific PE2I PET ligand.
Methods: Persons with PD (n=67; M48/F19, age: 68.20±6.34 yrs; Hoehn & Yahr stages: 1, 2, n=26, 2.5, n=20, 3 (n=10), 4 (n=3), and 5 (n=1), duration of motor disease: 6.08±4.40 yrs; Montreal Cognitive Assessment scale (MoCA: 25.26±3.50); underwent detailed clinical and motor assessments and [11C]-PE2I DAT brain PET-CT imaging. Direct clinical expert observation of freezing during a provocation protocol was used in the dopaminergic medication 'off' state. Fall status was defined by a 6-month fall diary. Statistical parametric mapping whole brain voxel-based group comparisons were performed between freezers vs. non-freezers and fallers vs. non-fallers.
Results: Freezers (n=13, M10/F3, age: 70.0±5.16 yrs; duration of motor disease: 7.4±3.4 yrs; MoCA scores: 26.8±2.6) had lower DAT binding in the anterior and more prominently in the mid cingulum, left peri-central and left premotor cortices compared to non-freezers (FDR corrected P<0.05). Fallers (n=26, M19/F79; age: 68.2±6.3 yrs; duration of disease: 6.1±4.4 yrs; MoCA: 25.3±3.5) had lower binding in the anterior and more prominently in the mid cingulum, right more than left operculum and anterior insulae, bilateral caudate nuclei and fornices, right more than left dorsomedial and anterior thalamus, left pulvinar and left globus pallidus, pars interna, compared to non-fallers (uncorrected, P<0.05).
Conclusion: Extra-striatal dopamine transporter binding losses, especially in paralimbic structures, were significantly lower in PD freezers and trended to be lower in fallers. The anterior cingulum and insula play a role in attentional processing whereas the mid cingulum plays a role in sensory processing, cognitive control, and execution of movements and may inform novel therapeutic approaches.

P40.16
1 Ruijin Hospital affiliated to Shanghai Jiao Tong University School of Medicine, China
2 Ruijin hospital, China
Background: Orthostatic hypotension (OH) is a prevalent non-motor symptom in Parkinson's disease (PD), associated with an increased risk of falls and cognitive decline. Despite its clinical significance, the mechanisms linking OH to cognitive impairment remain poorly understood. This study aims to investigate the relationship between OH and cognitive impairment in PD patients using gray matter volume (GMV) analysis.
Methods: Data were obtained from the Parkinson's Progression Markers Initiative (PPMI) database, comprising 351 PD patients categorized into OH (n=50) and non-OH (n=301) groups based on baseline assessments. All participants underwent comprehensive clinical evaluations, including the Montreal Cognitive Assessment (MoCA) for cognitive function (with a score <26 indicating impairment), and structural MRI scans using a 3.0T scanner. Demographic and clinical data, such as age, gender, disease duration, education, UPDRS scores, and non-motor symptom scales, were collected. GMV analysis was performed using voxel-based morphometry (VBM). Statistical analyses included independent t-tests, Mann-Whitney U tests, chi-square tests, Kaplan-Meier survival analysis, and Cox proportional hazards models to assess the association between OH and cognitive impairment.
Results: The median time to cognitive impairment onset was significantly shorter in the OH group (70.7 months) compared to the non-OH group (92.4 months; p=0.006). Cox regression analysis revealed that OH was a significant predictor of cognitive impairment (HR=2.11, p=0.008). At baseline, the OH group exhibited reduced GMV in the precentral gyrus and superior temporal gyrus. During follow-up, these patients showed further GMV reductions in the inferior frontal gyrus and inferior occipital gyrus, suggesting that OH may contribute to cognitive decline through structural changes in specific brain regions.
Conclusion: This study demonstrates that PD patients with OH are at a higher risk of developing cognitive impairment, potentially mediated by GMV reductions in key brain regions. The findings suggest that OH may influence cognitive function through mechanisms involving α-synuclein deposition, which affects both blood pressure regulation and cognitive-related brain areas. These insights provide a foundation for future research into targeted interventions aimed at delaying cognitive decline in PD patients with OH.
P40.17
1 Dongtan Sacred Heart Hospital, Hallym University College of Medicine, South Korea
2 Korea Institute of Radiological & Medical Sciences, South Korea
3 Busan Paik Hospital, Inje University College of Medicine, South Korea
4 Yonsei University Wonju College of Medicine, South Korea
Background: Isolated rapid eye movement behavior disorder (iRBD) is regarded as a very early stage of neurodegenerative disease, such as Parkinson’s disease (PD), dementia with Lewy bodies (DLB), and multiple system atrophy (MSA). RBD severity, relating to RBD pathogenesis, serves as a robust predictor of phenoconversion for these diseases.
Objectives: We aimed to determine which cortical areas are linked to RBD severity by examining structural and functional magnetic resonance imaging (MRI) measures.
Methods: Thirty patients with video-polysomnography-confirmed iRBD and 29 healthy controls underwent T1-weighted and resting-state functional MRI scans. Brain structure and function were assessed by surface-based morphometry (SBM) and fractional amplitude of low-frequency fluctuation (fALFF). We investigated areas showing correlations between RBD severity and these measurements.
Results: In the right superior parietal lobule, there was a correlation between increased cortical complexity (CC)and decreased fALFF as RBD severity increased (r = -0.4379, p = 0.0155). With advancing RBD severity, the CC of the right superior parietal lobule increased, and the fALFF of the left superior temporal gyrus decreased (r = -0.4775, p = 0.0076). In addition, higher RBD severity was correlated with both increased CC and fALFF in the left inferior parietal lobule(r = 0.4380, p = 0.0155).
Conclusions: Our findings suggest that cortical regions associated with the perceptual mechanism play an important role in the pathogenesis of RBD, and may represent a site of early pathological involvement.
P40.18
1 John van Geest Centre for Brain Repair, Department of Clinical Neurosciences, University of Cambridge, United Kingdom
2 Wolfson Brain Imaging Centre, University of Cambridge, United Kingdom
3 Department of Clinical Neurosciences, University of Cambridge, United Kingdom
4 Medical Research Council Biostatistics Unit, Cambridge Institute of Public Health, University of Cambridge, United Kingdom
5 Department of Psychiatry, University of Cambridge, United Kingdom
Aims: 50% of people with Parkinson’s Disease (PD) develop dementia within 10 years from diagnosis. However, the underlying neurobiological correlates of dementia risk remain poorly understood. 'NEuroinflammation and Tau accumulation in Parkinson's Disease Dementia' (NET-PDD) is an ongoing longitudinal study using PET neuroimaging to assess the contribution of neuroinflammation and tau aggregation to cognitive decline and dementia development.
Methods: People with newly-diagnosed PD and age-/sex-matched controls were recruited and assessed longitudinally with clinical and neuropsychological testing every 18 months for up to 5 years. Neuroinflammation and tau accumulation were assessed using PET-MR neuroimaging with [11C]-PK11195 and [18F]-AV1451 ligands at baseline and 3-year follow-up in 27 PD and 14 controls. Non-displaceable binding potential (BPND) was measured within across 43 bilateral regions of interest (ROIs) determined using the Hammers’ parcellation. Principal component analysis (PCA) was used to reduce the dimensionality of the data. Longitudinal changes in BPND in ROIs as well as PCA components were compared between groups.
Results: People with PD demonstrated significantly greater regional increases in [11C]-PK11195 BPND in the hippocampus, subcallosal area, and pons versus controls. In contrast, people with PD had smaller [18F]-AV1451 BPND changes over time across multiple brain regions compared to controls. Longitudinal changes in PCA component scores for [11C]-PK11195 and [18F]-AV1451 did not differ between PD and control groups, nor between PD cases who developed cognitive impairment and those who remained cognitively intact and did not relate to cognitive change (ACE-III) over time in a linear mixed-effect model (LMEM). However, whole brain [11C]-PK11195 BPND was associated with cognitive decline in a LMEM.
Conclusion: Our findings suggest limited regional change in neuroinflammation over time in early PD but an overall association at whole brain level with cognitive decline. Together with our previously published findings from this study (Kouli et al., 2024; Scott et al., 2025), our data indicate that baseline [11C]-PK11195 may be a more robust predictor of long-term cognitive outcomes than longitudinal [11C]-PK11195 change. We found no evidence that early tau accumulation is relevant to cognitive decline or outcomes in PD.
CLINICAL SCIENCES: E-health and technology
P41.02
1 Lifespark Technologies Private Limited, India
2 Lifespark Technologies, India
3 University of Leeds, United Kingdom
Background: Freezing of gait (FOG) remains one of the most disabling symptoms in Parkinson’s disease (PD), contributing substantially to falls, loss of independence, and reduced quality of life. Addressing FOG effectively is central to improving mobility and daily functioning in people with PD. We present findings from studies using a novel wearable neuromodulation device, WALK, which delivers vibration-based stimulation to the quadriceps and hamstrings. Previous work has demonstrated that WALK alleviates FOG in over 80% of users, providing meaningful, real-world benefits. In this retrospective analysis, we aimed to characterize clinical features that distinguish responders from non-responders, to inform more personalized and effective treatment approaches.
Methods: Data from 36 participants with PD and FOG were analyzed (20 responders, 16 non-responders). Responders were defined as those achieving a minimum clinically important difference (MCID) of >4.28 points in FOG severity scores. Participants were tested in the OFF-medication state under two conditions: without (Baseline) and with active WALK stimulation. FOG severity was assessed during a standardized mobility protocol including sit-to-stand, straight walking, turning, navigating narrow spaces, and doorway crossings, both with and without an arithmetic dual task. The primary outcome was the change in FOG severity score.
Results: Responders demonstrated an average improvement of 8.15 points, while non-responders improved by only 0.38 points. The greatest improvements were observed during turning and narrow-space walking tasks (p<0.001). In 7 of 12 activities, responders showed a shift from severe to mild FOG when using WALK. Non-responders showed no significant benefit. Clinically, non-responders more frequently exhibited greater rigidity, balance deficits, and pain—factors associated with reduced device responsiveness.
Conclusions: This analysis highlights key clinical factors—rigidity, balance impairment, and pain—that may limit the immediate benefit of vibration-based neuromodulation for FOG. Addressing these comorbid features through complementary physical or pain-management interventions could enhance the long-term efficacy of WALK. These insights contribute to a growing understanding of individualized, technology-assisted strategies to improve gait and independence in people living with Parkinson’s disease.

CLINICAL SCIENCES: Prodromal States
P42.01
1 Transversal Translational Medicine, Luxembourg Institute of Health, Strassen, Luxembourg
2 Transversal Translational Medicine, Luxembourg Institute of Health, Strassen; Parkinson’s Research Clinic, Centre Hospitalier de Luxembourg, Luxembourg
3 Department of Neurology, Medical University of Innsbruck, Austria
4 Paracelsus-Elena-Klinik Kassel, Germany
5 Parkinson's Disease and Movement Disorders Unit, Hospital Clinic de Barcelona, Spain
6 Luxembourg Centre for Systems Biomedicine, University of Luxembourg, Luxembourg
7 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, London, United Kingdom
8 Transversal Translational Medicine, Luxembourg Institute of Health, Strassen; Parkinson’s Research Clinic, Centre Hospitalier de Luxembourg; Luxembourg Centre for Systems Biomedicine, University of Luxembourg, Luxembourg
Background: Mild cognitive impairment (MCI) is a common non-motor feature of Parkinson’s disease (PD), affecting 20–40% of patients at diagnosis. Self-perceived difficulties in higher-order cognitive functioning (SPD-HOCF) may capture early vulnerability for MCI. While SPD-HOCF predict cognitive decline, the prevalence and relation to neuropsychological testing in prodromal PD stages remain unclear. We aimed to estimate SPD-HOCF prevalence in a population-based at risk cohort and assess concordance with objective cognitive testing.
Methods: Participants from the European multicentre Healthy Brain Ageing (HeBA) project completed an online survey including demographics, family history, and potential risk factors. MDS prodromal PD probability scores were calculated. SPD-HOCF was measured with the Penn’s Parkinson’s Daily Activities Questionnaire (PDAQ-15). Neuropsychological data from in-person visits at the Luxembourg site were compared with PDAQ-15.
Results: We included 26628 individuals (56.6% female mean age 63.0 ± 7.8 years) with complete PDAQ data across all HeBA sites. Overall, 2455 (9.2%) scored ≤49/60 cut-off (SPD-HOCF+). Compared to SPD-HOCF–, SPD-HOCF+ participants more often reported a family history of PD or Alzheimer’s disease (AD) (16.8% vs. 11.4%,p<0.001) and difficulties with remembering errands(p<0.001), new information(p<0.001), multitasking(p<0.001) and learning new gadgets(p<0.001). PDAQ total score correlated negatively with depressive symptoms(r = –0.477,p<0.001).
In-person visits in Luxembourg (n=303) showed that SPD-HOCF+ had lower MoCA scores (p=0.007), lower scores in the CERAD delayed word list recall (p=0.01), required more time for copying the complex Rey figure(ROCF, p=0.03) and for completing the Trail Making Test(TMT) A and B(p=0.003 and p=0.02). They also differed in Benton’s Judgment of Line Orientation(BJLO, p=0.004) as well as in the strategy to copy the ROCF (p=0.04) and had higher generalized anxiety(GAD-7) scores (p<0.001). After Bonferroni correction for multiple testing, BJLO, GAD-7 and TMT-A remained significant.
Conclusion: SPD-HOCF+ was associated with both higher PD risk and early difficulties in psychomotor speed and visuospatial functions as well as with significantly higher levels of generalized anxiety and depressive symptoms. Our results support the potential of assessing SPD-HOCF as an early marker of cognitive vulnerability. Future work will validate these findings across centers and in longitudinal follow-up.
P42.02
1 The Centre for Movement Disorders, Stavanger University Hospital, Norway
2 Stavanger University Hospital, Norway
The Pro-LBD study is a long-term research project following people who may be at higher or lower risk of developing a Lewy body disease (LBD). LBD include Parkinson’s disease, Parkinson’s disease dementia, and dementia with Lewy bodies.
Long before movement symptoms appear, many people experience changes such as sleep problems, mood changes, or issues with smell or digestion. Symptoms also associated with getting older. This early or "prodromal" phase can last many years. By studying it closely, we hope to recognize LBD earlier and open the door to better treatments and support.
The Pro-LBD study will follow 100 adults at the age of 50 or older for at least 10 years. Participants are grouped into “higher risk” or “lower risk” based on established criteria. Every 2.5 years, participants come in for an extensive set of assessments at the hospital. These include questionnaires, brain scans (MRI and DaTSCAN), sleep and brain activity tests, eye exams, and collection of samples such as blood, saliva, tears, and stool.
So far, nearly 500 people have been screened and 80 have joined the study. We are now carefully tracking their health and symptoms. Participants will stay in the study until they either develop LBD, withdraw or the study ends.
This is one of the first major efforts to track people before LBD becomes obvious using such a broad panel of examinations, combining clinical assessments, brain scans, sleep studies, eye exams, and a wide range of biological samples. Bringing these pieces together, we aim to uncover early warning signs, enable earlier and more precise diagnosis, guide new treatments, and improve the lives of patients and families affected by LBD.
P42.03
1 Transversal Translational Medicine, Luxembourg Institute of Health, Luxembourg / Centre Hospitalier de Luxembourg, Luxembourg
2 Transversal Translational Medicine, Luxembourg Institute of Health, Luxembourg
3 Centre Hospitalier de Luxembourg, Luxembourg
4 Luxembourg Institute of Science and Technology, Esch-sur-Alzette, Luxembourg
5 Transversal Translational Medicine, Luxembourg Institute of Health / Centre Hospitalier de Luxembourg / Luxembourg Center for Systems Biomedicine, University of Luxembourg, Esch-sur-Alzette, Luxembourg
REM Sleep Behavior Disorder (RBD) involves dream-enactment behaviors during REM sleep and often precedes neurodegenerative diseases like Parkinson's disease (PD) by several years. While non-motor symptoms such as mood and cognitive changes can appear early in RBD, the impact on facial emotion recognition—a crucial component of social cognition—remained unexplored.
This study examined whether participants with polysomnography (PSG) confirmed RBD show difficulties in recognizing facial emotions compared to control individuals, potentially revealing early social cognitive deficits.
We recruited 27 RBD participants from the Luxembourg National Sleep Study and 27 healthy controls from the Luxembourg Parkinson's Study, matched for age and sex. All participants completed a cognitive screening test (Montreal Cognitive Assessment; MoCA), questionnaires on depression (Beck Depression Inventory-I; BDI-I), apathy (Starkstein Apathy Scale (SAS), and facial emotion recognition testing (Ekman 60 Faces test including the six basic emotions such as anger, disgust, fear, happiness, sadness and surprise).
The RBD group (20 males, mean age 67.2 years± 6.5) and control group (19 males, mean age 66.9 years ± 6.3) showed similar education levels, depression scores, and overall facial emotion recognition performance (total score on Ekman test). However, RBD participants demonstrated lower cognitive scores (MoCA: 25.6 ± 2.4 vs 27.6 ± 1.9; p = 0.003) and higher apathy levels but without reaching the cut-off for presence of apathy (SAS: 12.9 ± 5.3 vs 9.9 ± 5.2; p = 0.02). Within the RBD group, increased apathy correlated with poorer anger recognition (r = –0.46, p = 0.02).
While general emotion recognition abilities remain largely intact in RBD participants, the relationship between apathy and difficulty recognizing anger suggests that specific social cognitive changes may begin during this pre-disease stage. This finding aligns with research showing that PD patients with apathy struggle particularly with recognizing negative emotions such as fear, disgust and anger, indicating that these selective deficits may emerge earlier in the disease process than previously thought. Further research will investigate whether variations in REM sleep quality are associated with emerging social cognitive changes.
LIVING WITH PARKINSON'S: Public Education or Awareness Programs
P43.01
1 National Parkinsons Institute, United States
The Parkinson’s Buddy Program is a partnership between the National Parkinson’s Institute (NPI) and the University of Louisville School of Medicine that connects future medical professionals with individuals living with Parkinson’s disease (PD). Created in response to the growing need for neurologists—particularly movement disorder specialists—and the importance of early, human-centered medical education, the program pairs first- and second-year medical students with Parkinson’s patients to foster lasting, mutually enriching relationships. The goals are to enhance empathy, communication, and understanding of chronic illness in future clinicians and to reduce isolation and build connection for people with PD.
Re-launched in 2021 after the COVID pandemic pause, the program was revived by NPI and dedicated second-year medical students. It begins with a structured orientation covering PD education, expectations, and communication guidelines. Pairs are matched by interest and availability and commit to meeting monthly—virtually or in person—for an academic year. Activities include casual conversations, community outings, and participation in NPI support groups and seminars. Coordinators collect qualitative data through surveys, focus groups, and check-ins to measure impact and inform improvements.
Since its creation in 2017, over 500 medical students have participated, with 95% reporting increased understanding of PD and greater confidence with neurologically complex patients. PD participants reported less isolation, greater purpose, and satisfaction mentoring future physicians. Anecdotal reports cite strong friendships, heightened interest in neurology, and empowered patient voices. The program also fostered interdisciplinary collaboration and expansion into allied health disciplines.
The Parkinson’s Buddy Program is a scalable, impactful model that connects academic institutions with nonprofits to enhance medical education and patient well-being. As the global PD population grows, it offers a humanistic approach to shaping the next generation of empathetic clinicians. Future plans include formalizing outcome measures, expanding to more universities, and evaluating long-term impacts on career paths and patient outcomes.

P43.02
1 Parkinson's Disease Community, Nepal, Parkinson's Nepal, Pokhara Academy of Health Sciences, Pokhara, Nepal, Nepal
Introduction: At the age of 42, while working as a Medical School Professor in Nepal, I began experiencing mild tremor and stiffness in my left hand. Despite of my medical background, I remained undiagnosed for over seven months. I visited multiple specialists, Orthopedists and General Physicians, before finally traveling to a neighboring country, India, for a DaT scan that confirmed my Young-Onset Parkinson’s Disease (YOPD). The years that followed after diagnosis were marked by internal struggle, professional pressure, psychological distress, and the weight of social stigma. I concealed my diagnosis until symptoms became visibly apparent, fearing it would jeopardize both my career and social identity.
Objective: I am now transitioning from academia to full-time advocacy and community engagement for Parkinson’s disease in Nepal. My goal is to increase awareness, promote early diagnosis, reduce stigma, and improve access to care in my country where neurological services are scarce and support systems are underdeveloped.
Insights: My dual perspective as both a healthcare educator and a person living with Parkinson’s has given me a unique lens to recognize the deep gaps in knowledge, support and empathy systems in low-resource settings. Now, I’ve learned that personal stories can spark collective changes
Conclusion: WPC 2026 represents an opportunity for me to grow by learning from international leaders and bring home practical, innovative approaches to Parkinson’s support and care. With the support and insights gained from WPC, I hope to lead efforts that give treatment visibility, voice, and dignity to people living with Parkinson’s in Nepal.
References:
Kieburtz K, Ravina B. Young-Onset Parkinson’s Disease: Clinical Perspective. Movement Disorders Clinical Practice. 2014;1(2):117–123. Basnyat B, et al. Health care in Nepal: a fractured system. The Lancet. 2017;389(10085):1361–1362. WPC 2023 Report. World Parkinson Coalition.
https://www.worldpdcoalition.org/
Seventh World Parkinson Congress (WPC 2026), May 24–27, 2026, Phoenix, Arizona, USA https://cdn.ymaws.com/www.worldpdcoalition.org/resource/resmgr/pdf-files/press_release_april23_2024.pdf
P43.03
1 PD Avengers, Canada
ABSTRACT | Cures Collective Perspective: Uncovering Shared Pathways Across Neurodegenerative Diseases
Neurodegenerative diseases—including Parkinson’s, ALS, Huntington’s, Multiple Sclerosis (MS), Progressive Supranuclear Palsy (PSP), and others—share a high degree of clinical, biological, and psychosocial overlap. While each condition is distinct, they frequently present with similar symptoms: motor dysfunction (tremor, rigidity, gait instability), muscle weakness, speech and swallowing difficulties, cognitive impairment, autonomic dysfunction, chronic fatigue, and sleep disturbances. These shared features can complicate diagnosis and contribute to care fragmentation.
At the molecular level, many of these diseases are driven by converging pathological mechanisms: chronic neuroinflammation, mitochondrial dysfunction, oxidative stress, and toxic protein aggregation (e.g., alpha-synuclein, beta-amyloid, tau, TDP-43, and huntingtn). These processes create overlapping cellular stress responses that accelerate neurodegeneration across diagnostic boundaries.
Equally significant are the shared lived experiences of people impacted by these diseases. Mental health challenges, identity shifts, financial strain, loss of independence, and caregiver burden are common threads. The need for integrated support services, accessible therapies, and public awareness is urgent.
In response to these commonalities, the Cures Collective was established in 2024 as a cross-disease collaborative movement. Bringing together advocates, researchers, clinicians, and people living with neurodegenerative conditions, the Collective fosters joint action in research, policy, and community engagement. Its mission is to break down disease-specific silos, identify shared priorities, and accelerate progress through collaboration. By focusing on what unites us rather than what divides us, the Cures Collective aims to build a more inclusive, efficient, and impactful approach to ending neurodegenerative diseases.
P43.04
1 Australian Public Sector, Australia
Background: Public understanding of Parkinson’s Disease (PD) is largely confined to visible motor symptoms in older adults. This narrow perception leaves Young-Onset Parkinson’s Disease (YOPD)—which affects people in the prime of their professional and family lives—widely misunderstood. As a result, those living with YOPD often experience stereotypes, stigma, and insufficient support from employers, peers, and healthcare systems. There is an urgent need to challenge these misconceptions through accessible, relatable education efforts that highlight the “invisible” aspects of the YOPD experience.
Objective: To design and deliver a first-person narrative–based public education program aimed at increasing understanding of YOPD in the general community, workplace, and healthcare environments. The objective is to reduce stigma, foster empathy, and build more supportive and inclusive spaces for individuals diagnosed at a younger age.
Methods: The presentation is centred on a personal story of being diagnosed with PD at the age of 37 and is structured into three key components:
Narrative Storytelling: A candid, first-hand account of the diagnosis, emotional impact, and the disruption of career, family, and identity during a peak period of life.
Thematic Exploration: Discussion of YOPD-specific challenges, including non-motor symptoms (anxiety, apathy, sleep disturbance), navigating professional responsibilities, parenting with a chronic illness, and maintaining self-confidence and relationships.
Interactive Dialogue: A Q&A component that enables audiences to ask questions, challenge assumptions, dispel myths, and explore practical ways to support colleagues, family members, and community members with YOPD.
The session is designed for adaptability and has been delivered in a range of settings, including corporate wellbeing programmes, healthcare forums, and community education workshops.
Conclusion: Storytelling is a powerful vehicle for raising public awareness of YOPD. By spotlighting the real-life experiences behind the diagnosis, this presentation promotes deeper empathy and shifts the conversation beyond tremors and age stereotypes.
P43.06
1 Composium.ai, United States
In a patient's ideal world, a medical professional would be available at all times to answer quesstions about PD and to provide professional, actionable guidance, all in the patient's own language. In the real world, PD-specialists are busy or expensive or unavailable, and the popular AI platforms are far from perfect. ParkiBot.com, a PD-focused AI with an understanding of patient vs researcher perspectives, was created by a PD patient and computer scientist to help every PD patient learn more about their disease through conversational interaction. This talk describes how ParkiBot avoided the challenges experienced by users of general purpose AI platforms such as ChatGPT, while retaining the friendly conversational style. Issues covered include: AI training, language and interpretation, use of nonviolent communication style, accessing comprehensive data about PD, mapping papers that describe laboratory results onto questions that are inherently clinical in nature, hallucination-avoidance, intention-alignment, and dealing with consequential questions such as hopelessness, self-harm, and family communications.
P43.07
1 University of California, Los Angeles (UCLA), United States
Each year, around 90,000 people are diagnosed with Parkinson's Disease (PD) in the United States, forming a community that generates millions of life-altering stories (Statistics | Parkinson’s Foundation, n.d.).
Public perception of PD was explored regarding awareness of the disease. Studies found that not only was the public unaware of non-motor symptoms, but also almost half of the participants had misconceptions about the treatment options (Jitkritsadakul et al., 2017). Some studies have found that people were fearful of patients with Parkinson’s, going as far as to avoid those who were diagnosed (Werner & Korczyn, 2010). Therefore, due to these social consequences, insightful patient stories are ignored.
It is crucial that the public can empathize with PD stories that are rich with hope for a cure. Virtual Reality (VR) can be that outlet. With no such simulation available, sharing these stories can engage a broader audience across age groups and levels of awareness, fostering empathy for the PD experience and shifting public perception.
In designing the simulation, Unity was utilized to plan the three-dimensional field with C# to code the movements and actions of the player. The simulation shows the slow progression of the disease through outlining different time points: day one displays the player's life without symptoms, with day three being at its worst. Motor symptoms are shown through controller vibrations and sound effects, while non-motor symptoms are conveyed through narration. A medication system is implemented as the player completes their daily tasks for the day. If the player ignores their symptoms and medication, tasks become increasingly difficult, and the player may have to restart.
The pilot simulation was created by a student at the University of California, Los Angeles, and has currently been implemented into a student organization called High-Tech Neurological Disorders (HAND). It has been presented at club events and has received feedback from club members and faculty. The project is currently being discussed with the Parkinson’s community of Los Angeles to introduce its message within the LA community.
Increasing awareness of PD starts with public perception. Through using VR, more conversation and passion can be devoted to researching for a cure. By continuing to talk to leading researchers and advocates in the Parkinson's community, a groundbreaking educational platform can be popularized in an increasingly virtual world.
P43.08
1 Fahr Beyond, United Kingdom
Fahr’s Disease (Primary Familial Brain Calcification) is a neurodegenerative disease and considered a parkinsonism, it involves Idiopathic Basal Ganglia Calcification without a secondary (non-genetic) cause (Tai & Batla, 2015). Fahr’s Disease is characterised by bilateral symmetrical calcifications of the basal ganglia (Manyam, 2005). Patients usually present with neurological and neuropsychiatric features including parkinsonism, tremor, loss of memory, urinary symptoms, cognitive dysfunction (Batla et al., 2017). The genes associated with Fahr’s Disease are: SCL20A2, PDGF-B, PDGFRB, XPR1, MYORG, JAM2, and NAA60 (Batla, et al., 2017; Chelban et al., 2020; Magrinelli et al., 2025). There remains a lack of population data about clinical presentation of patients, their needs and expectations of a clinical service.
This poster looks at the rapid development of research and support into Fahr’s. Specifically, the paper will draw light to the two new genes discovered in the last two years that also cause Fahr’s Disease. It will highlight how the world’s only dedicated national referral service (for the UK at National Hospital for Neurology and Neurosurgery, UCLH, London) has evolved and how the team have contributed to research advancement. Significantly, the poster will help educate people about two significant projects the Calcifade Study based at Utrcht University, Netherlands which is looking at the efficacy of a repurposed drug (etidronate) on calcification in the brain for SLC20A2 (US$470,000). The other study based at Southampton University, UK it is that of biochemistry sequencing and understanding of the genetic variants of Fahr’s (US$970,000).
Furthermore, the poster will show how Fahr Beyond has supported the community through convening educational engagement events between clinicians and patients internationally, to aid in the development of the world’s first diagnostic and management toolkit. Here, the purpose of the poster is to highlight this parkinsonism which is complex to diagnose but has very different management requirements compared to other parkinsonisms and Parkinson’s.
P43.09
1 Table Tennis For Life (www.tabletennisforlife.org), United States
Introduction: Parkinson’s disease (PD) is one of the fastest-growing neurological conditions worldwide, affecting over 10 million people, with cases projected to double by 2040 (Parkinson's Foundation, n.d.). Beyond tremors and motor dysfunction, PD impacts cognition, mood, and quality of life for patients and caregivers. While medications and surgeries provide symptomatic relief, there remains an urgent need for low-cost, accessible, community-based interventions. In 2024, Table Tennis for Life (tabletennisforlife.org) was launched by siblings Tanvi (14) and Aarav (12) Desai, U.S. National Team athletes, to harness table tennis to stimulate neuroplasticity, restore movement, and build social connection for people with PD and related conditions.
Methods: The program offers free weekly 90-minute sessions at local clubs, with rally-based activities targeting reflexes, coordination, rhythm, and decision-making. Outreach extended to support groups, senior centers, and care networks, engaging people with PD, individuals with autism, and caregivers. Outcomes were tracked qualitatively through observation, participant self-reports, and caregiver feedback across domains of motor skills, emotional engagement, and quality of life.
Results: Over 52 sessions in 15 months (each session is 90 mins long), the program engaged more than 500 participants (PD and their caregivers).
1) Motor improvement: Participants reported experiencing better hand–eye coordination and more rhythmic movements. We also observed improvements in ball return and other table-tennis–specific skills during the sessions.
Cognition & emotion: Participants described sharper reflexes, improved focus, and joy - some even noted “forgetting they had Parkinson’s” while rallying.
Caregiver outcomes: Families reported greater confidence, independence, and bonding through shared play.
Social connection: Reduced isolation and strengthened community ties.
Conclusion: This youth-led initiative shows that table tennis can serve as a scalable, non-pharmacological intervention to improve motor skills, cognition, and emotional well-being in PD. Its accessibility and adaptability make it suitable worldwide. The success of Table Tennis for Life highlights the value of integrating exercise-based neuroplasticity into PD care while underscoring youth leadership in innovation. Next steps include structured clinical collaborations, quantitative measures, and global expansion.

P43.10
1 The Resolve Band, United States
2020 was a difficult year.
Amidst the challenges we all shared during that first year of the pandemic, at age 66, I learned I had Parkinson’s disease. Some days, it wasn't easy to get up and get moving. My need for a simple reminder inspired me to create the Resolve Band. With INTENT on one side and Perseverance on the other, it became a daily anchor. Friends asked me about it, and I began sharing it.
The message was clear: You are not alone.
The idea spread quickly. Beth Israel Deaconess Medical Center featured it in its neurology newsletter (2,000+ readers). Clinicians at BIDMC gave bands to patients. Speech therapists at Northeast Rehab used them in voice-amplitude work. Parkinson Voice Project featured the Resolve Band in a daily online practice session, reaching thousands. I have shared hundreds more of the bands, passed directly between patients, clinicians, and advocates.
Each Resolve Band is presented in a ribboned box with definition and explanation cards. This curated packaging turns a wristband into an experience people remember. Spanish-language and Advocacy editions expanded reach, supporting inclusion and linking the band’s message to NIH research funding on Capitol Hill.
I was asked to lead New Hampshire’s delegation at the 2025 Parkinson’s Policy Forum, hosted by the Michael J. Fox Foundation and partner organizations. More than 250 advocates from 45 states came to D.C. for three days of advocacy training and congressional meetings. Since my diagnosis, I’ve participated in four research studies, including PD GENEration genetic testing, which gave me crucial answers about my family’s risk. That program exists because NIH appointed the Parkinson’s Foundation to analyze the data, connecting my results directly to federal research funding. I carried Resolve Bands with red ribbons and NIH funding messages into meetings with Senators Shaheen and Hassan and Congressman Chris Pappas. Seeing leaders wear the band showed how a personal symbol can also bridge policy conversations.
What began as one coping tool has grown into a working model:
A constant reminder for the newly diagnosed—you are not alone. A tool for clinicians in everyday care. A story that opens doors with elected officials.
It works because it’s simple, practical, and human; it spreads because people want to pass it on.
Outcome: A patient-led idea that turns private struggle into shared strength—supporting patients, helping care teams, and giving policymakers a reason to listen.

P43.11
1 Vibrar com Parkinson, Brazil
Introduction The project Vibrar com Parkinson (VCP) was launched as a university extension initiative at Universidade Federal do ABC (UFABC) under the leadership of biochemist Danielle Lanzer, diagnosed with Parkinson’s disease at 36. Its mission is to raise awareness, expand access to evidence-based information, and empower people with Parkinson’s in Brazil. In a country where reliable information and public resources are limited, VCP became a pioneering platform connecting science, patients, and society.
Methods The initiative combines digital outreach, scientific communication, and advocacy. Online activities included more than 100 live sessions on Instagram and Facebook, reaching over 16,000 followers and engaging patients, professionals, and researchers. Danielle delivered over 30 lectures and spoke at public hearings to advocate for policy changes and better treatment access. VCP also organized scientific events for the Parkinson’s community and students, with international experts on treatment and rehabilitation. Collaborations extended to documentaries and frequent appearances on national TV. All activities relied on volunteers and partnerships, without fundraising.
Results VCP’s multi-channel approach achieved tangible results. In 2018, advocacy supported a regulation expanding levodopa access for patients under 50. The project built a volunteer network of internationally recognized professionals contributing services. Cultural and media engagement broadened reach: documentaries linked to VCP were showcased at Cannes, one became a World Parkinson Congress finalist, and another won Gold and Silver Lions awards. Annual appearances on Brazilian TV further strengthened public awareness. Crucially, VCP was the first initiative in Brazil to make scientific, evidence-based information on Parkinson’s widely accessible to patients and families.
Conclusion VCP demonstrates how education, advocacy, and communication can transform public understanding of Parkinson’s and improve policies and quality of life. By combining academic expertise, social networks, and community engagement, it created lasting change—from influencing regulation to building a culture of scientific awareness in Brazil. Moving forward, VCP offers a model adaptable to other countries facing similar challenges, fostering collaboration and strengthening the global Parkinson’s community.
P43.12
1 nonprofit, United States
At its heart, The Bayou Bounce is an illustrated book that transforms medical complexity into something human, familiar, and deeply relatable — a story that bridges the distance between clinical precision and lived experience. Through the eyes of a child, it turns the often-isolating world of neurological illness into a story about love, learning, and cultural pride that is light, fun, and informative.
“It took years for Mom’s doctors to figure out what was wrong, but Mom never gave up… She found one who listened to her.”
This line captures more than a family’s perseverance — it captures what health equity truly means: being heard, being seen, and being understood. It speaks directly to the mission of modern medicine and resonates deeply with professionals committed to patient-centered care.
For hospitals, the story becomes an empathy tool — an accessible narrative to help neurology residents and patient educators understand the emotional landscape behind every diagnosis.
For medical schools, it offers a framework to teach cultural humility, communication, and trust-building across diverse communities.
For corporate foundations and CSR partners, it serves as a bridge — a tangible way to invest in brain health literacy and community resilience by distributing a resource that heals through storytelling.
Behind every diagnosis is a family learning how to dance again. Medicine treats the body. Storytelling heals the heart.
This book aims to remind clinicians why they chose to care — and families why they keep fighting.”
By centering humanity within science, The Bayou Bounce™ doesn’t just tell a story — it creates a movement. One that invites hospitals, educators, and philanthropists alike to join a global effort in turning diagnosis into a message of resilience.
P43.13
1 El Colegio de la Frontera Sur, Mexico
In this document, we would like to share the journey we have taken to set up a support group in Chiapas, Mexico, from the perspective of the founders.
There are no exact figures for Parkinson's cases in Mexico; however, the National Institute of Neurology and Neurosurgery estimates a prevalence of 50 new cases per 100,000 inhabitants per year (Reyes, 2023). This reality is exacerbated in Chiapas, where, in rural and indigenous populations, lack of knowledge about the disease delays diagnosis and treatment. The situation is further complicated by the double vulnerability faced by many patients, who also live in conditions of unemployment or lack access to essential medical services and medications (Hernandez, 2023).
Given this situation, in 2023, three people decided to form a support group in Chiapas with the aim of promoting the exchange of experiences and tools to improve the quality of life of people with Parkinson's.
Methods To integrate this learning community, key actions were implemented: contacting strategic individuals and entities, attending events to promote the group, developing promotional materials, and creating a WhatsApp group (as a viable and accessible medium). The community was consolidated with the creation of its identity (Parkinson Chiapas), the use of social media (Facebook and email), and the institutional support of ECOSUR, in addition to the active involvement of a student specializing in community health.
Results between April and October 2025, 31 people with Parkinson's and 7 caregivers were contacted, of whom 16 are actively participating. The members come from Tuxtla Gutiérrez, San Cristóbal de Las Casas, Tapachula, and other cities, demonstrating a state and regional reach. The ages of the participants range from 43 to 65, with a diagnosis time of 2 to 20 years. In the five meetings held in Tuxtla Gutiérrez, primary health-related needs were identified: exercise and physical therapy, alternative treatments, medication, and nutrition.
Conclusions: The group has succeeded in creating an enthusiastic community. However, it faces significant structural challenges: inconsistent attendance, lack of a permanent meeting space that is viable for everyone, and lack of funding to sustain the group. The main challenge lies in ensuring operational and financial sustainability in order to expand the group and offer a comprehensive and permanent support program for the benefit of people with Parkinson's in Chiapas.
P43.14
1 Asociación Uruguaya de Parkinson, Uruguay
Introduction In many countries, Parkinson's disease is diagnosed after a person has suffered from non-motor symptoms for several years that are not yet identifiable as the disease, due to the lack of awareness among many healthcare professionals and the vast majority of the population, causing disruptions to the patient's health and finances.
When a person receives the diagnosis, with minimal and stigmatized knowledge of the disease, they suffer anxiety and depression.
When searching for information, they find it in technical and unreliable language.
Methodology
The author, diagnosed with Parkinson's in 2021, implemented the following methodological strategy: He researched scientific information from conferences, discussions, and articles by specialized professionals, and summarized what was necessary and appropriate for the non-medical population.
He participated in support groups and group therapies.
He translated all the information and experiences into a language that was enjoyable, reliable, and accessible to all.
Results The main results are: On the one hand, the technical and scientific information on motor symptoms, endorsed by 39 specialists, compiled in verbatim and paraphrased quotes.
On the other hand, the extensive and detailed information on 40 non-motor symptoms with their corresponding pharmacological treatments, rehabilitation therapies, alternative treatments, social networks, and their impact on daily life, compiled by the same specialists and primarily from the experiences, testimonies, and needs of patients, their families, and caregivers.
Finally, the psychosocial aspects that do not always appear in the doctor-patient relationship, from diagnosis to the end.
All the information, needs, contributions, suggestions, problems, and solutions, from both the doctor and the patient, are intertwined and combined in simple, entertaining, friendly language, with humor and a great deal of emotion.
Conclusion The book turns knowledge into a tool for the main stakeholders: the physicians and healthcare professionals; the people receiving the diagnosis; their families and caregivers, and those who think they will never suffer from Parkinson's.
Destigmatizes the disease and promotes its acceptance.
Alleviates the emotional burden, providing comfort, motivation, and emotional support.
Accompanies and supports those who geographically have difficulty accessing healthcare.
Visualizes life with Parkinson's with dignity, resilience, and hope.
P43.15
1 Muhammad Ali Parkinson Center, Barrow Neurological Institute, United States
2 Barrow Neurological Institute, United States
Objective: To explore the Red Thread theory as a metaphor for Parkinson’s community interconnectedness and to create a participatory artistic project visually representing these unseen yet powerful connections
Background: The Red Thread theory posits an invisible thread connecting people destined to meet. This concept deeply resonates within the Parkinson’s community, where patients, caregivers, healthcare providers, and advocates form strong, meaningful connections. Despite the challenges of Parkinson’s, these interwoven threads of support, knowledge, and advocacy create a resilient global network
Methods: "Building on community-driven artistic initiatives like WPC 2023's “Pollinators of Change,” we propose a new participatory art project: 'The Tree of Connection.' This artwork will feature roots symbolizing foundational roles (patients, caregivers, researchers, supporters) that sustain the community, and leaves representing individual global Parkinson’s community members.
Each participant will be invited to color a leaf, adding personal touch and voice to the collective artwork. These individual leaves will be assembled into a large tree, brought to life by hundreds of unique contributions. A red thread will visually weave through the roots, trunk, and branches, linking the entire piece to represent strength of connection, unity, and shared purpose.
Results & Impact: The completed artwork, titled 'The Tree of Connection,' will be presented at the 7th World Parkinson Congress (WPC 2026) in Phoenix, Arizona, symbolizing inclusion, creativity, and global solidarity. An electronic version will be shared as an awareness tool with all participants. This project is anticipated to foster creative expression, cross-cultural unity, and shared identity. It reinforces the message that every individual (every 'leaf') matters, and that the Parkinson’s community strengthens through collective connection.
P43.16
1 Veterans Health Adminstration, United States
2 Veteran's Health Administration, United States
3 Veteran's Health Adminstration, United States
4 Parkinson's Foundation, United States
Background/Intro: An estimated 110,000 Veterans are living with Parkinson's disease (PD) in Unites States. In April 2020, the Parkinson’s Foundation (PF) entered into a formal partnership with the Veteran’s Health Administration (VHA) PADRECCs (Parkinson's disease Research, Education and Clinical Care Centers) with the goal of improving the health, well-being and quality of life of Veterans living with PD.
Methods: Recurring meetings and the establishment of a Memorandum of Agreement. Scholarships for VA providers offered by the Parkinson's Foundation for Parkinson’s-specific team training. PADRECC and PF have designated points of contact who meet biweekly to discuss, plan, and execute partnership goals. Additionally, bi-monthly meetings are held for all PADRECC leadership, education coordinators, PADRECC Associated Site directors, and the PF Strategic Partnership Team to provide partnership updates and discuss future goals. Highlighted partnership projects include: developing Veteran-specific outreach materials and webinars, providing PD-specific training opportunities for VA clinicians, offering VA-tailored training for PF Helpline Staff, and improving access to PF educational materials.
Results: Since the launch of the partnership, we have hosted 19 webinars with over 12,000 total registrations, created six educational print and digital resources specifically for Veterans and VA professionals including a series of detailed webpages on the PF website, over 130 VA professionals have participated in the PF Team Training program, and a total of 20,317 members of the veteran community have registered for an event, requested information or resources, or contacted the PF Helpline (since launch in 2020 as of May 31, 2025).
Conclusion: The partnership continues to thrive, evolve, and improve access to VHA care for Veterans with PD. Future projects are already under development for continued expansion. PADRECC staff have been able to address expressed needs and questions from PF Hotline calls specific to Veterans with PD for better access to care.
P43.17
1 The Davis Phinney Foundation, United States
Introduction The Davis Phinney Foundation’s Ambassador Leadership Program (ALP) was launched in 2015 to expand the Foundation’s mission to help people with Parkinson’s live well today. By empowering trusted local leaders, the program fosters meaningful connections, provides practical education, and amplifies community voices across the US and internationally. Now in its tenth year, the ALP has evolved into an innovative leadership model that blends lived experience, mentorship, education, and advocacy–creating sustainable community impact that traditional service models rarely achieve.
Methods The ALP recruits volunteer leaders who are living with Parkinson’s, caring for someone with Parkinson’s, or working professionally with the Parkinson’s community. Each Ambassador receives comprehensive training, professional development, and ongoing resources to serve their local communities. Ambassadors design their engagement based on five leadership strength areas–Mentorship, Advocacy, Innovation, Education, and Planning–to align with their personal strengths and local needs. The Foundation provides continuous support through orientations, monthly peer-networking and educational opportunities, one-on-one coaching, and access to educational materials and funding. In 2022, the program expanded to include Hispanic Ambassador Leaders, ensuring culturally relevant outreach and representation across diverse communities.
Results Over the past decade, the ALP has grown to a global network of community leaders embedded in 40 US states and 12 Countries, with ongoing efforts to reach all 50 states and expand Hispanic leadership. Ambassadors have hosted educational events, spoken at conferences, mentored peers, and advised on national Parkinson’s initiatives. Evaluation results show that the ALP has: Reduced social isolation by fostering deep peer-to-peer connections and purpose after diagnosis. Increased access to Foundation resources and education through localized outreach. Generated measurable impact through volunteer time and expertise valued at millions of dollars annually. And advanced systemic change through advocacy, awareness campaigns, and participation in policy discussions.
Conclusion The ALP demonstrates the power of grassroots leadership in chronic disease communities. By investing in people with lived experience, the Foundation’s created a scalable, sustainable model that transforms isolation into connection, challenges stigma, and drives collective empowerment.
P43.18
1 Parkinson's Foundation, United States
Background: Genetic clinical trials for Parkinson’s disease (PD) face significant challenges with enrollment beyond simply recruiting those with genetic forms of PD. Limited awareness and understanding of trial opportunities and processes by participants, in addition to concerns about risks and benefits are considerable barriers. To address these, the Parkinson’s Foundation created PD Trial Navigator to provide curated guidance for people living with PD about trial eligibility and to accelerate enrollment in genetic-focused trials.
Methods: Building off PD GENEration, an international genetic study which has enrolled over 28,000 participants since 2019, those identified as having a PD- associated genetic variant (n=2,674 as of 8/20/2025) will be invited to PD Trial Navigator. Interested participants can complete a brief survey and receive personalized information about PD, clinical research, and available gene-targeted trials all through a direct connection with our clinical trial team. Trial Navigators will use one-on-one virtual conversations, email, and/or phone as part of a multi-method approach. General education materials will include fact sheets, webinars, and podcasts. To inform the development of PD Trial Navigator, a focus group was held in August 2025 to assess understanding and awareness of personalized medicine, genetics and PD, and to collect initial feedback on the PD Trial Navigator program design.
Results: Focus group participants (n=9) demonstrated broad understanding of personalized medicine, but application within PD was more limited. Reflections on barriers to trial participation were discussed with many mentioning strict exclusion criteria, such as age, medications, comorbidities, causing frustrations and hopelessness. Participants described current approaches to learning about trial options as impersonal and expressed a need for personal connection and support. Tailored communication was noted as important. Individuals want to be able to choose the frequency and method of communication with the navigator.
Conclusions: PD Trial Navigator, launching in early 2026, will serve as a educate and empower people with Parkinson’s to make informed choices about enrolling in precision clinical trials. Engaging people with PD and care partners in the development of the program ensures the process and educational resources are relevant and reflective of the true needs of the PD community.
P43.19
1 Parkinson's Foundation, United States
Introduction For people with Parkinson’s disease (PD), healthcare appointments can feel overwhelming. There is a lot to cover in a short amount of time and there is no one-size-fits-all approach to PD care. People with PD and clinicians report frustration with the inability to efficiently identify appointment priorities and optimize their time together. However, healthcare appointments are critical opportunities to make a treatment change or get clarity on something that is affecting quality of life. The Parkinson’s Foundation set out to provide education, training and resources to empower people with Parkinson’s to make their healthcare visits more meaningful by becoming active partners in their PD care.
Methods To identify ways in which the Foundation could support people with PD in making the most of their care, the Foundation conducted a literature scan, formed a working group, hosted focus groups with community members and clinicians, and led a convening on quality care. After identifying “optimizing time spent with individuals with PD during their annual or semi-annual doctor visits” as a top priority, the Foundation conducted a landscape analysis and held recurring feedback sessions with clinicians (PD specialists and non-specialists), people with PD, care partners and health literacy experts.
Results The Optimizing Care Initiative uses the PD Appointment Cycle framework to educate and empower people with PD to take an active role in their PD care before, during and between visits. People with PD are encouraged to recognize their unique experience of living with Parkinson’s and to see themselves as active members of the care team. The approach to optimize care is broken out into simple, practical steps with an emphasis on self-reflection, self-education, and self-advocacy. Materials resources focus on the “how to” of optimizing and are available through a webpage, webinar and podcast episode, as well as a Steps to Prepare for a Parkinson’s Appointment worksheet that guides people with PD to select their top three appointment priorities based on what’s most impacting their daily life, what’s most time sensitive, and what matters to most to them.
Conclusion There are many challenges in managing and caring for PD. This shift to active partnership between a person with PD and their healthcare team represents an exciting innovation in PD care – one focused on reimagining the clinical relationship to empower and center the person with PD.
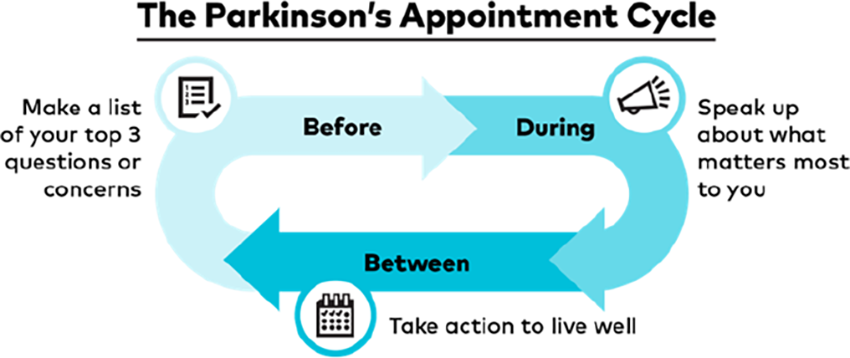
P43.20
1 Boston University, United States
2 American Parkinson Disease Association, United States
3 University of Connecticut, United States
4 DeAngelis Physical Therapy and Wellness, United States
5 Boston Medical Center, United States
6 US Department of Veteran's Affairs, United States
Background Exercise is increasingly recognized as a key component of standard care for managing Parkinson’s disease (PD). However, individuals with PD need clearer guidance on how to structure exercise programs for maximum benefit. Social media outlets offer an effective, broad-reaching and scalable means to disseminate critical information to help people with PD optimize mobility and engagement in exercise.
Methods Physical Therapists from the American Parkinson Disease Association’s (APDA) National Rehabilitation Resource Center (housed at Boston University), developed the “Let’s Keep Moving” Webinar series with professional production and promotion assistance provided by APDA . These webinars were streamed on YouTube, Facebook Live and LinkedIn. Webinars last approximately 30 minutes, with a 20-minute presentation followed by a 10–15-minute Q & A session. A Spanish language series, “Sigamos moviéndonos con la APDA” began in 2023. After the initial live event, the webinars remain posted on APDA social media outlets for access following the event.
Results As of September 30, 2025, a total of 37 Let’s Keep Moving episodes were developed. The series has been viewed a total of 76,369 times across all episodes. Under general exercise, 12 videos were developed with 21,052 views (mean views per episode 1,754). Under balance and postural control, 5 videos were developed with 16,801 views (mean views per episode 3,360). For freezing of gait, 2 videos were developed with 11,040 views (mean views per episode 5,520). Related to safe mobility and assistive devices, 6 videos were developed with 11,030 views (mean views per episode 1,839). For the emerging technology and research topic, 4 videos were developed with 8,562 views (mean views per episode 2,140). The Spanish language series consisted of 3 videos with a total of 1,463 views.
Conclusion The APDA Let’s Keep Moving Webinar series is a well-attended outreach program utilizing social media platforms to provide evidence-based recommendations on exercise and physical activity to the PD community. Videos on freezing of gait and balance had the highest average views per video suggesting high interest in these topics. Future development of the series would be aided by further outreach to the PD Community to identify topics of high interest related to exercise and mobility.
P43.21
1 Parkinson Society BC, Canada
2 PD Avengers, Canada
Introduction: Parkinson Ready is a program that raises awareness on common accessibility challenges faced by Persons living with Parkinson’s (PwP) and teaches service-facing industries how to best communicate and work with PwP to ensure inclusivity. The program is traditionally brought to host cities of the World Parkinson Congress (WPC) in preparation for an influx of PwP. 2024 was the first year Parkinson Ready was brought to a city without the WPC following and serves as a pilot to establish the feasibility of a stand-alone program addressing stigma, inclusivity, and equitable access to improve the lived experience of PwP in Vancouver. This was a collaborative project between World Parkinson Coalition, Parkinson Society BC, and PD Avengers, and was sponsored by AbbVie.
Methods: Parkinson Ready was carried out in 2024-2025 by a physiotherapist and a PwP. One-hour sessions were brought to service industries commonly used by PwP such as tourism, hospitality, public transport, police, fire, ambulance, and airport services. Goals of the program included: a) de-stigmatizing PD, b) removing accessibility barriers, c) promoting empathy and compassion and d) improving equitable community access. 11 training sessions were delivered with a total attendance of 400 participants. Pre-program and post-program surveys were conducted on the baseline knowledge of PD, the application of the knowledge in the workplace, and the usefulness in daily life when interacting with PwP.
Results: Before participating in the program, 36% of participants reported having adequate knowledge of PD and 22% reported confidence when interacting with PwP at their workplace and in their personal lives. After the program, 82% of participants reported having adequate knowledge of PD and 75% reported confidence when interacting with PwP at their workplace and in their personal lives. 93% found the program valuable at addressing community accessibility barriers.
Conclusions: The Parkinson Ready program offers a unique opportunity to address stigma, inclusivity and accessibility challenges faced by PwP in the community. By targeting commonly-used services, we hope to improve the lived experience of PwP in the community. The positive impact of the program shows the value of holding the Parkinson Ready program independently from the WPC, and could lead to replication in various cities around the globe.
P43.22
1 BIAL Portela Ca, Portugal
2 BIAL – Portela & Ca S.A., Coronado, Portugal, Portugal
3 Bial Pharma UK Ltd, Windsor, UK, United Kingdom
4 Parkinson’s Europe, Orpington, UK, United Kingdom
Background: Treatment adherence is a critical factor in the long-term management of Parkinson’s disease (PD), a chronic and progressive condition requiring complex medication regimens. Discontinuation or suboptimal adherence can significantly affect symptom control and quality of life. While multiple studies have examined clinical factors influencing adherence, fewer have explored the perspective of people living with PD on why, when, and how treatment routines are altered in real-world settings.
Objective: The aim of this study is to understand how people with PD experience and manage their treatment routines, and to identify factors influencing adherence, dose adjustments, and discontinuation.
Methods: This cross-sectional, observational survey was co-designed with Parkinson’s Europe. An anonymous online questionnaire will be available in multiple European languages (Portuguese, English, Spanish, Italian and German) for two months, to be completed by people living with PD under anti-PD medication. The survey will be anonymous, voluntary and non-participant identifiable. Sample size will be determined by uptake. A descriptive quantitative analysis will be conducted to identify key adherence patterns and drivers.
Results: The survey will include 30 questions and capture demographic data. All questions are grouped according to the five WHO domains of adherence: socioeconomic, healthcare system, condition-related, therapy-related, and patient-related factors. Findings are expected to highlight common barriers and facilitators of adherence, including regimen complexity, communication with clinicians, caregiver support, and external influences such as cost or media information.
Conclusion: By capturing real-world experiences, TRACK-PD study will shed light on the most relevant retention and adherence challenges faced by people living with PD today.
P43.23
1 Justeat Nutrition, Australia
Introduction: People with Parkinson’s disease (PD) often experience gut-related non-motor symptoms such as constipation, nausea and delayed gastric emptying, yet many are unaware of how diet can support gut–brain function. The MIND diet, a hybrid of the Mediterranean and DASH (Dietary Approaches to Stop Hypertension) diets, was originally developed for cognitive health and offers a practical framework that can be adapted to address nutritional challenges in PD. Nutrition education delivered in various formats can help translate emerging gut–brain science into realistic strategies for people with PD and their carers.
Methods: Education sessions were delivered through organisations including Fight Parkinson’s Victoria, Neurological Rehabilitation Group and Brighton Spine and Sports Clinic, via online presentations, podcasts and clinician interviews. Content focused on simplifying MIND diet principles, adapting them for constipation, poor appetite, early satiety and medication timing, and addressing common questions about coffee, dairy, alcohol and protein with levodopa. Practical tools such as sample meal plans, food swaps and meal-timing strategies were provided.
Results: Participants reported that complex scientific information was explained in a simple way that linked gut symptoms to brain function. They valued that the content was practical, with real meal ideas instead of theory alone. Many attendees requested slides and individual dietetic support, reflecting strong engagement and unmet need. Since these sessions, there has been an increase in people with PD independently seeking dietetic care rather than waiting for referral from their neurologist or GP, suggesting a shift towards proactive self-management. Feedback also highlighted the need for a PD-specific nutrition screening tool in routine care.
Conclusion: Translating MIND diet principles into PD-specific education has strong potential to improve non-motor symptom management and quality of life. There is a need to integrate gut-focused nutrition education incorporating MIND diet principles by a specialised dietitian much earlier in care. As no PD-specific nutrition screening tool currently exists, future work should focus on developing one tailored to this population. The long-term goal is for every newly diagnosed person with PD to be screened for nutrition risk and offered a dietetic referral as part of standard care.
P43.24
1 American Parkinson's Disease Association, United States
Background: Understanding the evolving needs and preferences of people with Parkinson’s disease (PD) and their care partners is essential for shaping education, outreach, and support programming. The American Parkinson Disease Association (APDA) conducts an annual Insight Survey to identify PD community priorities, preferred learning formats, and awareness of APDA resources across the United States. These data help guide how information is communicated, what topics matter most, and where service gaps persist.
Objective: To present key findings from the 2024 Insight Survey, compare trends with 2022 data, and preview forthcoming 2025 results that will be available by the time of the World Parkinson Congress (WPC).
Methods: The 2024 survey was conducted from July 29, 2024, to January 31, 2025, and offered in English and Spanish. A total of 681 respondents participated. Participants identified their top PD information needs, preferred delivery formats, and APDA resources they had heard of, used, and found helpful. Demographic questions were optional but completed by more than 80% of participants, providing a broad snapshot of APDA’s reach across age, gender, and regional groups. Data from the 2022 cycle (n = 1,120) were used for comparisons.
Results: Respondents most frequently prioritized information on new medications, PD progression, symptom management, cognitive changes, and exercise. Most (91%) said they were somewhat or very likely to continue using virtual or hybrid programs, and 54% selected webinars, online materials, and websites as their preferred learning formats. APDA webinars, online content, and printed educational materials were the most frequently recognized, utilized, and rated as helpful. Compared with 2022, 21% fewer respondents reported needing more PD information, suggesting improved baseline knowledge and expanded reach of educational tools. Several participants noted that virtual programming increased accessibility for those with mobility or transportation barriers.
Conclusion: The Insight Survey provides an ongoing, data-driven feedback loop that helps APDA adapt programming to the community’s evolving needs. Trends from 2022 to 2024 demonstrate a growing reliance on flexible, technology-enabled education and a more informed patient community. The 2025 survey will further enhance understanding of emerging topics, guiding national and international strategies for equitable patient engagement, education, and resource delivery.
P43.25
1 Egas Moniz School of Health & Science, Portugal., Portugal
2 Young Parkies Portugal, Portugal, Portugal
Introduction: Online exercise programs have become increasingly important for people with Parkinson’s (PwP), especially following the COVID-19 pandemic. Technological advances have improved access to specialized care, and combining exercise with cognitive training shows early promise in improving motor and cognitive outcomes. However, many current digital interventions may lack variation, gamification, and personalization.
Methods: MOVE ON UP is a European initiative aiming to address these challenges through the development and evaluation of an 8-week digital exercise program for 50 PwP. It also includes a 28-hour multidisciplinary training for 100 health professionals and caregivers. Guided by behavior change models, the program targets physical activity, motor symptoms, functional ability, and quality of life. The training component addresses barriers to digital adoption and aims to build digital health literacy. A mixed-methods approach will be used across five work packages, informed by the ADDIE instructional design model and the Be Healthy, Be Mobile framework. The project is funded by Erasmus+ Sport 2024 AND coordinated by the Egas Moniz School of Health and Science and includes partners from Portugal, Greece, Croatia, and Italy.
Results: The project was officially launched in January 2025. Key activities at the launch included discussions on overcoming barriers to digital transition and setting the framework for the upcoming program. All educational and exercise content has been developed and is scheduled for deployment on the platform in April 2026.
Conclusions: MOVE ON UP has the potential to enhance physical and cognitive health in PwP while supporting healthcare professionals in the digital transition. It aligns with key Sustainable Development Goals and supports the WHO Global Action Plan on Physical Activity 2018–2030.

P43.26
1 Kenya Parkinson's Care Network, Kenya
Background: Parkinson’s disease (PD) is not well understood in Kenya, especially in regions outside of the capital city (e.g., coastal Kenya), where access to neurologists and specialized care is scarce. Misunderstandings, stigma, and cultural beliefs can significantly delay both diagnosis and treatment. In these low-resource environments, it is crucial to engage patients and communities to enhance awareness, care, and advocacy, particularly in the absence of developed neurological care systems.
Objectives: We report here the experience and outcomes of the Kenya Parkinson’s Care Network – a non-governmental organization – in involving patients, caregivers and communities in Parkinson's advocacy across the Kenyan coast.
Methods: Kenya Parkinson's Care Network takes a multi-pronged grassroots, patient-centered approach to advocacy and awareness that includes: establishing support groups in Coastal Kenya; training community health volunteers to identify PD symptoms and offer basic support; organizing public awareness events, such as on World Parkinson's Day; engaging in radio discussions and social media campaigns to combat stigma; engaging persons with PD and caregivers in advocacy conversations with health authorities.
We collected qualitative feedback through group discussions and tracked quantitative data on participant numbers, training outreach and awareness initiatives.
Results: Kenya Parkinson’s Care Network began as a local support group in 2018 and now supports over 90 people with Parkinson’s across the coastal region. The network has trained over 20 community health volunteers to recognize PD, provide community support and refer to a neurology service. Our public forums, including radio programs, have reached an estimated audience of 100,000 people. The network was key in production of the award-winning documentary ‘Shaking hands with the devil’. Patients’ stories have encouraged local health facilities to refer PD patients to the support group. Participants have reported better understanding of PD, less stigma and stronger networks among caregivers.
Conclusion: In low-resource settings like Coastal Kenya, engaging patients and communities, and sharing their lived experiences can be a powerful driver for Parkinson’s advocacy and service enhancement. The Kenya Parkinson’s Care Network has shown that with the right local context and support, PD awareness and care can improve.
P43.27
1 Louisiana State University, United States
2 Mission for Movement, United States
3 Mission For Movement, United States
Introduction: In early 2020, the Parkinson’s population in Baton Rouge grew rapidly. Despite multiple programs, the community remained fragmented. Each group operated independently, leaving many people with Parkinson’s unaware of available resources. After a Saturday morning Dance for Parkinson’s class at the Neuromedical Center, two community advocates imagined how Baton Rouge’s programs could work together rather than compete. What began as a parking-lot conversation became the foundation for what would grow into Mission for Movement.
Goals: Our mission is to connect people with Parkinson’s and their care partners to equitable, accessible programs, education, and advocacy opportunities across Louisiana. We aim to unite existing resources under a collaborative umbrella for a “one-stop shop” and ensure every person living with Parkinson’s finds meaningful movement opportunities and community support.
Methods: To become the one-stop shop for people with Parkinson’s in Baton Rouge, we evolved from a single support group into a registered 501(c)(3) nonprofit advocacy organization. This transition created formal partnerships with universities, healthcare systems, community centers, national Parkinson’s organizations, and local YMCAs. Through collaboration, we unite community leaders, researchers, exercise instructors, healthcare professionals, faith organizations, and people living with Parkinson’s to identify needs and build lasting, inclusive programs across Louisiana.
Results: Within 18 months, Mission for Movement secured grants from the Davis Phinney Foundation and the Parkinson’s Foundation, organized successful fundraisers, and expanded programming throughout Baton Rouge and beyond. Collaborations launched Pedaling for Parkinson’s, Ping Pong for Parkinson’s, Dance for PD, and Tai Chi programs, as well as new support groups, including one in North Baton Rouge for underserved populations and a local healthcare screening. These efforts increased access to exercise, education, and resources while fostering stronger connections among Parkinson’s groups in Louisiana.
Conclusion: Mission for Movement demonstrates how a grassroots idea, starting from a Saturday morning conversation, transformed Parkinson’s care and community across Louisiana. By focusing on collaboration and inclusion, we’ve built a sustainable model that unites resources, fosters connection, and empowers people with Parkinson’s to live active, purposeful lives.
P43.28
1 Davis Phinney Foundation, United States
Introduction Since 2015, the Davis Phinney Foundation Ambassador Leadership Program (ALP) has empowered community leaders to further its mission of helping people with Parkinson’s Live Well Today. In 2022, guided by an advisory committee, the Hispanic Ambassador Leadership Program (HALP) was developed based on the principles of cultural relevance, inclusion, and accessibility. Centered on community-based work to ensure resources and approaches reflect international Spanish-speaking communities' values, needs, and lived experiences.
Methods As a sister program to the ALP, the HALP advances the Foundation’s commitment to inclusive, transnational leadership within the Hispanic community. Promoting cultural representation and capacity-building, HALP trains people with Parkinson’s, care partners, and health professionals as community connectors. Ambassadors receive world-class leadership training, individual coaching, access to global peer networks, virtual collaborations, and Spanish-language resources that enhance outreach and innovation. Through structured mentorship and interactive learning formats – including educational webinars, digital communication channels like WhatsApp, and 3en30, an exclusive space for bridging connections across the network cohorts– HALP fosters culturally responsive collaboration, expands access to Parkinson’s care, and strengthens sustainable community impact across borders.
Results HALP has grown into a global leadership network spanning eleven countries with diverse Hispanic communities. It promotes knowledge-sharing, peer support groups, community education, and care initiatives. Ambassadors have driven systemic change through advocacy, awareness campaigns, and participation in public policy discussions, strengthening the recognition of Parkinson’s as a public health and social well-being issue. The network includes 62 Ambassador Leaders (39 women and 23 men) representing over 20 communities and reaching over 7,500 people affected by Parkinson’s—reflecting the program’s cultural diversity.
Conclusion HALP demonstrates that investing in culturally relevant community leadership generates sustainable impact. By fostering cross-country collaboration and empowering local leaders, HALP shows that systemic barriers can be overcome through community-driven innovation – weaving international networks that enhance visibility, advocacy, education, and quality of life for Spanish-speaking people with Parkinson’s and its community.
P43.29
1 Columbia University, United States
2 American Parkinson Disease Association, United States
3 The Davis Phinney Foundation, United States
Objective: To create a culturally sensitive educational resource that (1) centers the voices of the Spanish-speaking community, (2) dispels misconceptions and breaks down barriers to resources, (3) showcases the community’s diversity, and (4) supports those receiving a PD diagnosis.
Background: The Spanish-speaking community living with PD face unique barriers that require a tailored approach to engagement.
Methods: The Davis Phinney Foundation, American Parkinson Disease Association, and Columbia University Irving Medical Center established a collaboration to create a storytelling educational resource featuring the voices of the Spanish-speaking Parkinson’s community. In 2023, at the WPC in Barcelona, 21 participants from 9 countries gathered to discuss the idea. Then, 8 focus groups with 49 Hispanics living with PD and caregivers from 10 countries were held over Zoom to identify themes to include. Individuals shared their testimonies via email, voice note, and photos of handwritten prose. Two writers, women living with PD, organized the stories. Two Hispanic editors then harmonized the material maintaining the conversational format and simple language of the focus groups. Dialogues start before the diagnosis and end with an invitation to personalize a Wellness Prescription. With final text, illustrations were developed by a Hispanic graphic design company, experienced with PD personally and professionally. Participants were kept abreast of progress.
Results: “Parkinson Positivos” [Figure 1, Book Cover] is a model of community engagement where the community’s voice, priorities, challenges and strengths are the centerpiece of the initiative. By ensuring the team members all had deep ties to the community, all elements of the book messaged the context, lived experience, and themes critical to this community. For example, the illustrations convey the emotional realities of those living with PD, and the colors, textiles and social interactions remind the reader of the Hispanic culture’s diversity and traditions.[Figure 2, example page].
Conclusions: “Parkinson Positivos” is a collaborative approach to weave the community’s voice with educational resources to provide hope and empowerment and increase awareness and knowledge of PD, so families can have a positive outlook and know they are not alone in their journey.

P43.30
1 Vall d'Hebron Research Institute, Spain
We describe here two projects developed at the Vall d’Hebron Research Institute and University Hospital in Barcelona (Spain) with the primary objective of stimulating citizen participation in science by fostering co-creation between the Vall d’Hebron scientific community, local Barcelona neighborhoods, particularly those near the hospital, and people living with Parkinson’s disease (PwP).
The PAIR (PArkinson Intergenerational caRe) project is an initiative that since 2024 connects Parkinson's patients with high school students from a disadvantaged neighborhood close to the Vall d’Hebron Campus. This project uses an Intergenerational Service and Learning methodology to combat loneliness and social isolation among patients while simultaneously promoting scientific learning and social engagement for the students. The core activities involve students and patients co-creating adapted games and artistic materials, with students also assisting researchers in designing and analyzing questionnaires to evaluate the program's impact on emotional well-being and disease outcomes. Ultimately, PAIR aims to be a transformative tool that reduces the stigma associated with neurodegenerative diseases and promotes community equity and inclusion.
The Weaving Research project is an initiative initiated in 2025 that established a Community of Practice (CoP) focused on Parkinson's disease bringing together PwP, families, professionals, and citizens to share knowledge and experiences. As a result of the collaborative work, the CoP reflected and defined priorities in health research and public health demands. This work led to the creation of an art exhibition to voice the needs and claims of those affected, advocating for a transformation in how the disease is managed and researched, demanding a more human-centered and holistic approach. Key themes emphasized by CoP members include moving beyond medical treatment to prioritize well-being through social, emotional, and physical support, and integrating diverse perspectives to overcome systemic and bureaucratic barriers that limit care. The collective work aims to humanize diagnosis and treatment, fostering a sense of community, mutual learning, and a non-judgmental approach to living with the unpredictability of Parkinson’s, ultimately seeking better research and assistance through shared vulnerability and acceptance.
P43.31
1 Richard Novati Catholic Hospital, Ghana
2 Newcastle University, United Kingdom
Introduction: Parkinson’s disease presents a great deal of challenge to both patients and relatives. These challenges are multifaceted and are beyond the usual treatment of clinical symptoms, which happens to be the focus of most practitioners. These challenges usually may not be attended to clinically. Deeply affecting these patients are their emotional, social and financial well-being. As part of the community engagement initiative under the project Transforming Parkinson’s Care in Africa (TraPCAf), sustained support to people with Parkinson’s disease and their caregivers alike was provided. Methods: Community durbars and interviews were used with purposeful sampling. Participants were 16 patients with PD and 11 caregivers. Data gathering was done through 12 support groups and 5 community engagements. Results: These interactions have led to peer interactions and shared learning for support. It has created a safe space for people with PD to share their experiences and reduce self-imposed isolation. Although several of these individuals have not been isolated by society, the feeling of shame has led to internalised stigma, and these community engagement activities have helped some of them come out of it. As one patient put it, “the day I got here and saw others shaking, I realised I was not alone”. Interviews conducted during this period revealed a recurrent theme of perceived burden on others, sadness and financial hardships imposed on them by the disease. Conclusion: Despite the challenges these individuals face, participants have reported increased emotional relief stemming from the various engagements. Optimism has been expressed with appreciation for the support of medication and finance provided to them. This CEI, spearheaded by TraPCAf, highlight the critical role of culturally grounded, community-based interventions in the provision of psychosocial outcomes for persons with Parkinson’s disease and their caregivers. The way forward is to sustain the gains made so far by continuing the support group meetings, awareness creation through community durbars, and hospital clinical meetings. Government and NGOs are expected to intervene in the treatment of PD due to the high cost of PD medications. Financial support should be extended to PD patients and their caregivers to mitigate their financial impact.
P43.32
1 Manamano, Spain
2 Manamano, Colombia
Background: Parkinson’s disease (PD) is the second most common neurodegenerative disorder. Yet its real magnitude in Colombia remains uncertain due to underdiagnosis and the absence of national registries. Beyond limited specialists or unstable medication access, the deepest barrier is informational: when science fails to reach people, imagination fills the gap. PD is often mistaken for “nerves,” “stress,” or even “divine punishment.” Patients are told to “pray more” or “be calmer to be cured.” These narratives reveal how a deficient information ecosystem turns disease into moral judgment and stigma, discouraging timely care and deepening isolation.
Methodology: Manamano emerged as a digital empowerment initiative treating communication as rehabilitation. Launched on World Parkinson’s Day 2025, it integrates health communication, visual semiotics, and social media strategy to translate medical knowledge into accessible, emotionally resonant narratives. Its symbol—the tulimán, a fusion of hand and tulip—embodies help, dignity, and hope: the hand, often seen as a sign of disability, is re-signified as solidarity and action, while the tulip evokes vitality and resilience. Manamano structures its content in four stages—Inform, Understand, Raise Awareness, and Empathize—across two pillars: Vivir (education and guidance) and Convivir (storytelling and emotional support).
Results: In its first year, Manamano built an organic community of nearly 700 members—88% from Colombia, most over 55—showing that older adults engage when communication is clear and respectful. Qualitative feedback is its strongest indicator of impact: caregivers express exhaustion and relief, patients seek guidance, and Manamano’s responses turn confusion into understanding. Exchanges around symptoms often begin with misinterpretation—such as attributing tremor to anxiety—but evolve into dialogue that clarifies neurological bases and fosters empathy. This shows how accurate, compassionate communication can replace stigma with awareness and isolation with community.
Conclusions: Manamano demonstrates that empathy and evidence can coexist in health communication. By merging science with storytelling, it reframes Parkinson’s not only as a medical condition but as a shared cultural experience. Ultimately, it rests on the belief that only a society empowered through understanding can demand from its institutions the structural change required to improve the lives of people living with Parkinson’s.

P43.33
1 Manamano, Spain
2 Manamano, Colombia
When I received my diagnosis of Parkinson’s disease (PD), I quickly realized that the greatest challenge was not the symptoms, but the way the world saw me—and sometimes, how I saw myself. In Colombia, PD is still perceived as a “disease of old age” or even a sign of instability. These misconceptions hurt because they erase who we truly are: people with dreams, resilience, and dignity.
After my diagnosis, I faced doubts about my professional capacity and emotional strength, yet I discovered that my body—with its tremors and pauses—remained a vessel of life and meaning. I realized that my story reflected a broader problem: across Latin America, people with PD face stigma, late diagnosis, and limited access to treatment. The greatest barrier is not always medical—it is social and cultural, born of silence and misunderstanding.
Determined to change that silence into connection, I decided to act. My purpose became to reshape how Parkinson’s is discussed—not from pity, but from empathy and truth. In 2024 I launched a communication project as a Parkinson’s ambassador and co-founded Manamano with my daughter, a physician. Together, we use digital platforms to create spaces of education, reflection, and visibility.
Through Instagram, YouTube, and community radio, I share daily reflections and testimonies that humanize PD. My goal is not admiration but connection—to speak to those afraid to tremble, reminding them that they are still themselves. These messages have built a community of over 20,000 people who share stories of fear, faith, and hope. Many express that seeing someone living openly with Parkinson’s helps them confront their diagnosis without shame. To reach those without internet access, I also collaborate with traditional media—radio, press, and television—to ensure that empathy and information reach everyone equally.
This work has opened dialogue with healthcare professionals and policymakers on improving access to medication, rehabilitation, and patient support. It has shown me that communication, when guided by empathy, can open doors that statistics alone cannot.
My vision is to continue building bridges between patients, caregivers, and society. I believe that empathy and visibility can transform how we understand illness. As I often tell my followers: “Do not condemn me, do not isolate me, do not exclude me. Walk with me, and you will see that the light still shines.”
P43.34
1 France Parkinson, France
The French Parkinson’s patient association has developed an educational board game designed to raise awareness and understanding of Parkinson’s disease. The game board represents the neural pathway from the substantia nigra to the striatum, illustrating the journey of dopamine within the brain. Magnetic playing pieces provide stability, ensuring accessibility for players with motor symptoms. By rolling a three-colored die, players answer questions in three categories—disease and symptoms, physical activity, and treatments and complications—progressively advancing their dopamine piece along the pathway. Co-created with individuals living with Parkinson’s disease, the game was carefully adapted to accommodate both motor and non-motor symptoms. This collaborative and interactive approach aims to promote learning, engagement, and empowerment for patients, caregivers, and the broader community.

LIVING WITH PARKINSON'S: Government Advocacy/Campaigns/ Public Policy
P44.01
1 Parkinson Argentina, Argentina
Introduction The quality of life of people living with Parkinson’s largely depends on the resources we can access. To sustain our vital functions, we need access to medications and other services that provide support for daily living. Universal access to these services and resources depends on the public policies of each country.
The aim of this abstract is to present certain indicators that reflect both the progress made and the pending challenges in Parkinson’s disease in Argentina.
Methods Five indicators were observed to assess the benefits and shortcomings that determine the quality of life of people living with Parkinson’s:
Results
Access to Clinical Research There is no systematized source of information where patients can consult and enroll in clinical trials. Participation in studies depends exclusively on prior contact with the service/study coordinator. If a pharmaceutical company contacts a physician or institution other than my own, I lose the opportunity to participate. Trials are delayed due to a lack of participants. Role of Patients There are no resources or projects that include patients in the management of funded projects. Access to Treatments Since 2004, the Mandatory Medical Program has been approved, covering 70% of commonly prescribed and chronic medications. Despite this, a high percentage of the population (percentage not known or published in Argentina) is unaware of this right. Access to Comprehensive Healthcare Supported by Public Policy Parkinson’s disease is not included in the national program for non-communicable diseases, nor in that of chronic diseases. There is no national Parkinson’s program or law. Access to Knowing Who We Are and How Many We Are There is no national patient registry, and no statistics are available on the disease.
Conclusions Although there have been advances, access to the resources necessary to live well with Parkinson’s remains inequitable. Many people are unaware that they have the right to free treatment. Greater dissemination is needed, starting with the creation of a national registry that would allow the design of better public policies, based on a clearer understanding of the phenomenon.
P44.02
1 Seattle University College Of Nursing & Health Sciences, United States
2 Chungnam National University, South Korea
Introduction Parkinson’s disease (PD), alongside dementia and stroke, is one of the most prevalent neurodegenerative diseases of aging, with its global burden accelerating due to aging. Both the United States and South Korea are experiencing rising clinical, social, and economic pressures from PD, yet their policy and advocacy landscapes diverge significantly. This project compared national approaches to PD prevalence, policy, public awareness, and advocacy in the two countries to identify lessons for strengthening global PD responses.
Methods A comparative policy analysis was conducted drawing on South Korea’s National Health Insurance Service Data and Korean Disease Control and Prevention Agency reports, as well as U.S. prevalence estimates, federal program reviews, and advocacy initiatives. Key areas of comparison included: (1) prevalence trends, (2) government support and financial protection, (3) advocacy and public awareness efforts, and (4) integration of PD into broader chronic disease and long-term care policy frameworks.
Results In South Korea, over 140,000 people have PD, with a prevalence at 165.9 per 100,000 among those 60+. Cases rise 13% annually. While PD is covered under the Medical Expense Support Program, aid is limited to medical costs. Support for caregiving, rehabilitation, or devices is minimal, and low public awareness delays diagnoses and adds to caregiver burden. By contrast, the U.S. has more than one million PD patients and a robust advocacy presence through organizations such as the Michael J. Fox Foundation. Advocacy has successfully influenced federal research funding and heightened public awareness. However, access to care is fragmented, especially in rural communities, and long-term care benefits remain vulnerable to shifting political priorities.
Conclusion Both countries face rising prevalence, mounting family and societal costs, and limited integration of PD into broader chronic disease frameworks. In South Korea, financial aid is restricted to severe disability cases, while research and policy remain underdeveloped. The U.S. invests in advocacy and research but struggles with inequitable access and policy instability. Strengthening PD policy globally requires greater awareness, expanded caregiver supports, and sustainable funding for research and care. This cross-national analysis, among the first to compare Asia and the U.S., highlights urgent gaps and opportunities for building equitable, resilient systems of care worldwide.
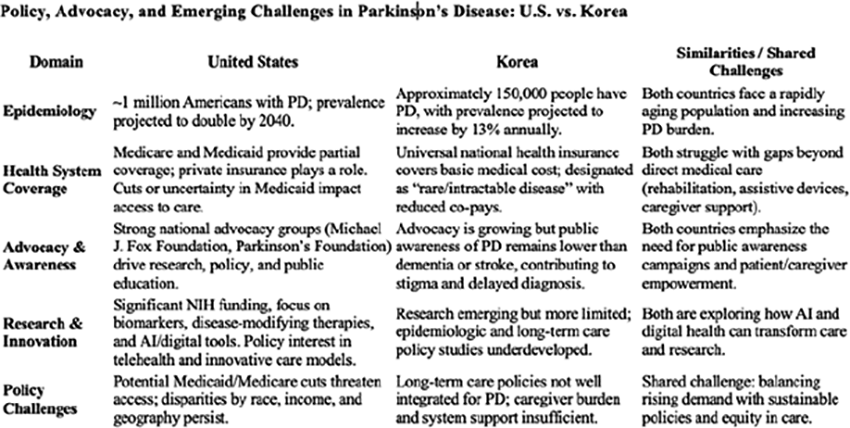
P44.03
1 Movers & Shakers, United Kingdom
You see before you some accidental activists. It all began when six friends met in a British pub and had two things in common: first, relatively high-profile careers, and secondly, we all had Parkinson’s. With a wry smile, we called ourselves the Movers and Shakers and decided to set up a podcast about what it was like living with the condition.We started every episode saying we’d gathered in the pub to have a bit of a laugh, a bit of a moan. People appreciated our light-hearted style, but people had much worse stories than we did — about delays, treatment generally, and the long waits before getting proper care. At first, we were concerned, then alarmed, finally angry. We had to do something — and that something was our five-point Parky Charter, setting out our demands to government. Those five points are: speedy specialists, instant information, the Parkinson’s passport, comprehensive care, and the quest for a cure. We were naïve about how to attract attention. We delivered a petition to Downing Street and made a silly film, using new words to “Gloria Gaynor’s I will survive”. We sang it outside Parliament. It wasn’t enough. We launched an official petition - if we reached 100,000 signatures, we’d get a debate in Parliament — and finally attract politicians’ attention. Again, such naivety. We thought it would simply happen — a few Instagram posts, a few appeals on the podcast. The petition would close on September 10th. If we’d failed by then, we’d failed for good. By June, we were desperate.Then Linda in Bexhill printed leaflets with QR codes and we went to Brighton to gather signatures along the wet seafront; Rory, put the QR code on T-shirts; we campaigned at Glastonbury, where the actress Tilda Swinton signed; then Stephen Fry made a special video for us. TikTok poet Liz Houghton made an emotional appeal about living with Parkinson’s. After that, the numbers rolled in. We got our 100,000 signatures by July. Now we need to attract the attention of MPs, making sure they take part in the debate on the plight of people with Parkinson’s. We’ve just won a Gold award for impact at the British Podcasting Awards. This for everyone who joined our campaign — all 100,000 people who signed.
LIVING WITH PARKINSON'S: Living Well with PD
P45.01
1 Anyone Can Dance, LLC, United States
2 Portland Therapy Center, Portland, OR, United States
Keywords: intimacy, sexuality, sensuality, communication, partnering, mood, apathy, hypersexuality
Objective: To assist and encourage carepartners and PWPs to openly address issues of closeness that may have been neglected after diagnosis, and offer innovative types of support to build confidence in discussing and addressing sensual and sexual issues.
Methods: Couples who have been living with PD may have been in a relationship for decades before diagnosis. Parkinson’s has often been called an intruder in the partnership. At a point where needs for functional assistance increase and the roles of each partner change unpredictably, it may be hard to reclaim intimacy between them.
Gay and lesbian couples may have additional concerns, because providers from the PD community may have little to no experience counseling them. Outreach to sexually marginalized groups with Parkinson’s will be an objective of this program.
In many partnerships, physical closeness, intimacy, and sex become more difficult as age advances. How can PWPs see and enjoy their lover again? How can carepartners enjoy a new form of closeness with their partner who has changed radically—physically, mentally and emotionally?
Open discussion, new methods of experimentation and play, and a re-casting of the sense of touch can create a pathway for stronger partnerships, and may lead to new approaches to communication, collaboration and intimacy in long-partnered couples. Thoughtful approaches to young-onset and newly diagnosed individuals about dating and expressing love are a major part of this program. Sharing of resources that facilitate ease of connection including props, attitudinal shifts, and realigning of unhelpful ways of thinking.
ACTIVITIES INCLUDE
Eye contact (and ways to encourage that) Conversations in movement and deliberate play (balloons, etc) Bed rolling together New forms of touching (non-functional) Blindfolded touch/feeding each other treats Body paints Writing love letters (expressing emotion) Separate bedrooms = creating “date nights”
Intentionally focusing on pleasure
Using all five senses to experience intimacy
Proposed Results: This program teaches partners to talk, look and act differently about their intimate needs and experiment with physical and emotional connection, which is often neglected in traditional Parkinson’s care.

P45.02
1 PD Avengers, Canada
Background: Parkinson’s disease (PD) is the fastest-growing neurological disorder globally, affecting over 11.8 million people. While daytime symptoms are widely acknowledged, nighttime symptoms—disrupted sleep, emotional distress, and physical challenges—are often hidden and undertreated. These burdens significantly affect care partners as well.
Objective: To assess the impact of nighttime PD symptoms on people with Parkinson’s (PwPs) and their care partners, and to inform care and advocacy strategies.
Methods: From March 15 to May 15, 2024, PD Avengers, in collaboration with AbbVie, conducted a multilingual online survey of 1,248 PwPs and 286 care partners across 27 countries and six languages. The survey explored sleep quality, symptom burden, healthcare engagement, and gender/regional differences.
Results:
96% of PwPs said PD affects their sleep, averaging 2.75 disruptions per night. 65% reported difficulty turning in bed, rising to 84% in advanced stages. 30% said healthcare providers never discussed sleep. Top symptoms: awakenings (53%), insomnia (50%), bradykinesia (41%), rigidity (38%), nocturia (38%). 88% of care partners reported sleep disruptions. Among them, 40% cited emotional strain, 34% lost sleep to assist, and 32% experienced chronic worry. 44% of PwPs said symptoms emotionally impacted their partners; 36% cited effects on partners’ physical health.
Call to Action: This joint SLEEP survey highlights the need to:
Tailor sleep-related interventions by region and severity. Support care partners in managing nighttime challenges. Encourage open dialogue between PwPs, care partners, and clinicians. Make sleep a standard part of PD care. Improve diagnosis of PD-related sleep issues, especially those overlapping with conditions like menopause.
Conclusion: Parkinson’s doesn’t sleep—and neither should our efforts to understand and address its 24-hour impact. Through global efforts like Spark the Night, which lit up 650 landmarks in 253 cities across 17 countries in 2025, PD Avengers shines a light on the hidden burden of PD after dark.
P45.03
1 Medical University of South Carolina, United States
Background: Exercise is critical in managing Parkinson’s disease (PD), offering benefits for both motor and non-motor symptoms as well as slowing disease progression. Despite this, only 27% of people with PD (PwPD) meet the recommended 150 minutes of weekly physical activity. While programs like Rock Steady Boxing are effective, additional accessible and engaging options are needed. Pickleball, the fastest-growing sport in the U.S., involves dynamic movement and social interaction, making it a promising exercise modality for PwPD.
Objective: The Pick it Up (PIU) program aims to introduce PwPD to pickleball by teaching techniques, movement strategies, and safety practices, helping participants incorporate the sport into their exercise routines.
Methods: PIU is an 8-week instructional program developed by exercise professionals and Movement Disorders specialists at MUSC. Led by a pickleball-certified coach with PD-specific training, classes meet twice weekly for 75 minutes. The curriculum includes warm-ups, specialized movement techniques, stroke mechanics, and game strategy. The final three weeks emphasize coached and supervised play.
Results: Two cohorts of PwPD have completed the PIU program at the MUSC Wellness Center and have successfully transitioned to recreational pickleball. Participant feedback highlights include increased confidence, improved agility and balance, strengthened social connections, and a strong desire to continue playing after the program. A Parkinson’s Foundation community grant has enabled the program to be offered free of charge at MUSC for the next year.
Conclusion: Community-based exercise programs that combine physical activity, education, and socialization are valuable for PwPD. Pickleball stands out due to its accessibility and popularity. The PIU program demonstrates that with proper instruction and support, pickleball can be a safe, enjoyable, and sustainable form of exercise for the PD community.
P45.04
1 Brooklyn Parkinson Group, United States
Introduction: The Brooklyn Parkinson’s Writing Circle (BPWC) came together In July 2024, as an offshoot of the Brooklyn Parkinson’s Group. The Group is based at the Mark Morris Dance Center (MMDC) in Brooklyn, NY, that developed and promoted its Dance for PD program and has sponsored other innovation in support of people living with PD, including the Movement Lab. The goal of the BPWC is to create an inclusive and collective work about its members’ personal experiences with Parkinson’s Disease (PD), to find what we have in common, and to write with honesty and realism. Participation in the BPWC improves the well-being of its members through greater awareness and acceptance of their situation. It offers a unique perspective to others from people with PD and explores new ways to engage in dialogue with families, caregivers, medical professionals and the broader public and to build understanding of what it means to live with PD.
Methods: The BPWC is self-organized by people with PD. Its main activity is writing by its members and mutual review. Each writer’s draft contribution is up to 500 words in any form and reflects personal experiences. Review comments emphasize the positive potential of each contribution and always with the intention of being constructive, with specific help to the writer, to improve the text. The Circle meets in person monthly in the MMDC. Meetings are open to new participants with PD. A series of interviews with and by its members will further deepen the content and provide feedback on how the writing activity improves the well-being of members. In addition, a board game has been developed as a tool for dialogue about PD and to build mutual understanding.
Results to Date: 8 participants remained active over a period of one year. Contributions include factual accounts, prose and poetry and a concept for a board game. Several submissions are accompanied by illustrations or photos. A public reading of texts for an audience of 60 people was held at a local Public Library in Brooklyn. A program printed for the event with texts was distributed, and the reading was video recorded.
Next Steps: Complete planned, written interviews, more public reading and dialogue engagements with structured quantitative and qualitative feedback, publication of a collection of writings and production of a board game.
P45.05
1 Banner Neuro Wellness, United States
2 Banner Neuro Wellness Center, United States
Abstract Parkinson’s disease (PD) is a progressive neurological disorder that affects both motor and non-motor functions, often compromising individuals’ independence, safety, and social engagement. While clinical treatment remains essential, community-based programs that integrate fitness, wellness, and social support may offer valuable complementary benefits. This study examines the perceived impact of the Banner Neuro Wellness program on individuals living with PD, with a focus on daily functioning, fall frequency, healthcare utilization, confidence, social participation, and overall quality of life, compared to individuals not enrolled in a similar program.
A cross-sectional survey was administered to current program participants and non-participants diagnosed with PD. The survey included both quantitative and qualitative items assessing self-reported changes in independence, confidence in daily activities, fall frequency, hospital visits, and social engagement. Descriptive statistics were used to analyze quantitative data, while thematic analysis was applied to qualitative responses.
Preliminary findings suggest that participants in the Banner Neuro Wellness program report increased confidence, fewer falls and hospital visits, and enhanced social connections—outcomes notably more positive than those reported by non-participants. Qualitative responses further underscore themes of empowerment, improved quality of life, and the value of peer support.
These results highlight the transformative potential of structured, community-based wellness programs as vital adjuncts to clinical care. By fostering independence, reducing fall risk, and promoting social engagement, such programs contribute meaningfully to the overall well-being of individuals with PD and support broader implementation of integrated wellness models.
P45.06
1 Chi Flow with Jo, Ireland
Chi Flow with Jo is a weekday-morning, live online Qi Gong community. People join from around the world to move, breathe, and connect together. Parkinson’s can disrupt identity and routine; daily, real-time practice with peers reduces isolation and restores structure and hope. Each session is led by Davy (lives with PD) and Jo (Qi Gong teacher), who guide, adapt, and support, reminding members that, although life has changed, with community support you can find your way.
Format: live 30-minute sessions every weekday morning (seated or standing), self-acupressure and breathwork embedded, with recordings emailed following Live class. Safety cues, gentle progressions, and repetition build confidence and adherence. Community mechanisms: real-time check-ins, encouragement in chat, and partner/caregiver welcome. Evaluation: pragmatic pre/post self-ratings (mobility, balance confidence, mood, sleep, bowel function, pain, connection), attendance/recording metrics, and short testimonials.
Feasibility is shown by sustained weekday attendance across time zones and consistent recording use. Participants commonly report improved ease of movement, steadier balance, calmer mood, better sleep and bowel regularity, and greater confidence. Typical comments include: “It brings structure to my mornings and injects joy and compassion into the day… I’m feeling fitter and healthier.” (Kerry Kilner) and “Best investment in my health… physical, emotional, spiritual. Feels like I have a friend walking with me daily.” (Carolyn O’Keefe). Reported changes align with published evidence that Tai Chi/Qi Gong improve balance, gait, and quality of life in PD, and that group-based exercise enhances engagement and well-being.
Conclusion & Implications A live, leader-led, community-first Qi Gong routine appears practical, low-risk, and scalable for people with Parkinson’s. Meeting together every weekday morning, recordings of class emailed, reduces loneliness, supports consistent practice, and helps people feel safer and more capable in daily life. Next steps include expanding cohort and data collection on balance, confidence and mood, and partnering with clinical services and PD organizations to compare community-based delivery with usual care across diverse settings.
Qigong significantly improved motor symptoms, walking ability, and balance in PD. https://pubmed.ncbi.nlm.nih.gov/32727214/
Qi Gong: Improved fine motor function and quality of life. https://pubmed.ncbi.nlm.nih.gov/39502276/
P45.07
1 ProParkinson SK, Slovakia
2 Neurology Clinic, Faculty of Medicine, Comenius University & University Hospital Bratislava, Slovakia
In Slovakia, more than 20,000 people live with Parkinson’s disease, but support, education, and awareness remain very limited. Many patients face isolation, stigma, and a lack of accessible resources. Younger people with Parkinson’s, in particular, often remain hidden, hesitant to join patient‘s groups, and unsure where to turn for reliable information. To address these challenges, I founded ProParkinson SK, a nonprofit patient-led organization that aims to inform, connect, and empower people across all generations.
My work combines community building, physical activity, and education. I organize regular gatherings where patients can meet, exercise together, and share their experiences in a safe and supportive environment. Outdoor activities, such as group walks and mountain trips, not only promote movement but also strengthen friendships and resilience. These events help people discover that Parkinson’s is not something to be ashamed of, but a condition that can be lived with actively and with dignity.
Education is another key part of my mission. I host seminars with neurologists, physiotherapists, and psychologists, offering practical advice and the latest information on treatment and management. I created our own website and Facebook page to make trustworthy resources accessible to people even in smaller towns. In addition, I launched a podcast on Spotify, where I interview neurologists, psychologists, physiotherapists, and other advocates. This platform has become an important tool for reaching people in their homes, giving them knowledge in their own language, and reducing feelings of isolation.
The impact is visible: patients are more willing to talk about their condition, caregivers feel better informed, and professionals increasingly see us as a valuable partner. For the first time, younger people with Parkinson’s in Slovakia are finding a space where they feel included and represented.
By attending the World Parkinson Congress 2026, I hope to connect with the global Parkinson’s community, learn new advocacy and educational strategies, and bring them back to Slovakia. I believe that the exchange of ideas and experiences will help me grow further and provide better support to thousands of people who still live in silence.

P45.09
1 Parkinson Mentors Arizona, United States
2 Midwestern University, United States
Purpose: This study explores how mentorship programs impact the overall quality of life for individuals with Parkinson’s Disease (PD). Mentorship programs pair people diagnosed with PD—one as a mentor and one as a mentee—to provide mutual support and encouragement. Few programs of this kind exist. Parkinson Mentors Arizona (PMAZ) is a program that is aiming to “provide peer support to people newly diagnosed with Parkinson’s Disease and individuals with established Parkinson’s so that each person feels supported and empowered” (PMAZ, n.d.). PMAZ was established in April 2024 with 11 mentors, the program has since expanded to 13 mentor-mentee pairs.
Objective: The study aims to examine how participation in the PMAZ mentorship program influences mentees’ quality of life, including physical, cognitive, emotional, and social well-being. Parkinson’s Disease often causes challenges with movement and motor skills, but it also affects communication, cognition, emotional health, and social participation. Understanding how peer mentorship can support these areas may guide future PD care initiatives.
Methods: Midwestern University’s Speech-Language Pathology Department partnered with PMAZ to conduct this research. Two graduate students helped develop and distribute a 15-item online survey (12 multiple-choice and 3 open-ended questions) to assess mentees’ perceived well-being. The survey was approved by the Institutional Review Board (IRB) on September 11, 2025, and distributed via email to 15 mentees on September 16, 2025. Responses are collected anonymously.
Results: As of September 29, 2025, six completed surveys have been received. Data collection will continue, with surveys administered at one month, three months, and five months after mentor pairing. Responses will help track changes in mentees’ quality of life over time and identify perceived benefits of mentorship. The findings will inform PMAZ leadership on program strengths, areas for improvement, and opportunities for future growth. Final results will be shared at the World Parkinson Congress (WPC) 2026. The survey will continue to be used to assess both short-term and long-term outcomes, focusing on comfort, confidence, self-care, and overall well-being among participants.
P45.10
1 University of Missouri–Kansas City (UMKC) & Tremble Clefs Arizona, United States
Introduction: Parkinson’s disease (PD) is among the fastest-growing neurological conditions, significantly impacting biological, psychological, and social aspects of life. While medications may alleviate motor symptoms, over 90% of individuals with PD report voice and speech difficulties, contributing to depression, anxiety, social withdrawal, and reduced quality of life (QOL). Therapeutic group singing (TGS) is an augmentative voice rehabilitation approach that addresses biopsychosocial symptoms through structured singing and social support. Program Description: Tremble Clefs (TC) is a therapeutic singing group for individuals with PD, their caregivers, and families. Founded in 1994 in Phoenix, Arizona, TC has become a model of evidence-based TGS that improves voice quality, emotional well-being, and community engagement. In 2018, Tremble Clefs Arizona (TCAZ) became a non-profit, offering weekly in-person sessions at four different locations and a telehealth group to reach broader communities. TC groups now exist across the U.S., sharing the same name, philosophy, and approach. Weekly sessions include warm-ups, group singing, socialization, and cool-downs designed to stimulate respiratory and phonatory systems while enhancing vocal function. The social component fosters community and support, strengthening adherence and outcomes. Significance: TC is the first therapeutic singing group for PD in the U.S. and has become a clinical model in PD care. Initiated by individuals with PD who recognized the therapeutic effects of singing in improving vocal volume, clarity, and intonation, TC expanded the therapeutic spectrum by integrating patient-identified needs into clinical practice and demonstrating efficacy. TC also holds public performances to raise awareness of PD and TGS as a holistic intervention. These performances reduce stigma and allow participants to showcase their progress to loved ones. Additionally, TC provides clinical training and research opportunities for music therapy students, clinicians, and researchers, advancing knowledge and refining TGS as a person-centered model. Conclusion: TC exemplifies the impact of TGS in enhancing biopsychosocial functioning for individuals with PD and demonstrates its value as a non-pharmaceutical approach to care. As one participant reflected: “A silver lining of PD is joining this choir, where my voice is heard in a supportive environment with friends who share the same challenges. I have a new family.”
P45.11
1 CogniBrain LTD, United Kingdom
Levodopa remains the most effective treatment for Parkinson’s disease (PD), but long-term reliance on synthetic formulations is often complicated by dyskinesia. Studies show that natural levodopa from Mucuna pruriens provides comparable motor benefit with a reduced dyskinesia risk (Katzenschlager et al., 2004; Cilia et al., 2017; Lieu et al., 2010). Used in traditional medicine for centuries, Mucuna pruriens is a non-inferior source of L-DOPA, and HPLC-standardisation ensures consistent, verifiable dosing (Singh et al., 2025).
The Continuum Method™ was designed to optimise HPLC-standardised Mucuna through a flexible, patient-centred dosing framework. It begins with baseline mapping, where patients record onset and duration of benefit after test doses to define their personal “ON window.” Transition usually starts by replacing a morning synthetic dose with Mucuna, then adjusting timing or quantity stepwise. Delayed-release forms may be added for night coverage, with “top-ups” introduced as needed to reduce OFF time and smooth fluctuations.
Observational feedback suggests that patients applying the Continuum Method achieve more stable ON states, fewer OFF gaps, and critically, fewer dyskinesias. Clinical crossover trials demonstrate that Mucuna pruriens matches or exceeds levodopa’s motor benefit with fewer or no additional dyskinesias, while primate studies confirm long-term anti-parkinsonian effects with reduced dyskinesia liability (Katzenschlager et al., 2004; Cilia et al., 2017; Lieu et al., 2010). This structured yet adaptable approach promotes autonomy and engagement while remaining compatible with clinician oversight.
In conclusion, the Continuum Method provides a novel framework for integrating HPLC-standardised Mucuna pruriens into PD care. By sustaining motor benefit with reduced dyskinesia risk, it offers a patient-driven strategy to extend the therapeutic value of levodopa in long-term management.
References
Katzenschlager R, Evans A, Manson A, et al. J Neurol Neurosurg Psychiatry. 2004;75(12):1672–1677.
Cilia R, Laguna J, Cassani E, et al. Phytother Res. 2017;31(9):1293–1299.
Singh S, Pal A, Tripathi M, et al. Explor Neuroprot Ther. 2025;5:101083.
Lieu CA, Kunselman AR, Manyam BV, Venkiteswaran K, Subramanian T. Parkinsonism Relat Disord. 2010;16(7):458–465.

P45.12
1 REACH Hand Therapy in Williston, VT, United States
Current rehabilitation programs for people with Parkinson’s disease (PwPD) focus primarily on motor symptom remediation. This project aimed to develop a client-centered social self-management (SocM) manual for PwPD that addressed biopsychosocial dimensions of health through involvement in valued daily activities. Manual development included literature review and analysis of de-identified data from the Social Self-Management (SocM) lab. Two rounds of the Delphi Method was utilized to determine manual helpfulness, relevance, and quality. After several revisions, the manual was disseminated via e-mail and printed flyers at the Tufts Dance for PD event. The manual, Motivate PD, has been evaluated and endorsed by interdisciplinary experts in the Parkinson’s community; it is ready to be piloted to determine its effectiveness in supporting people with PD and care partners over time.
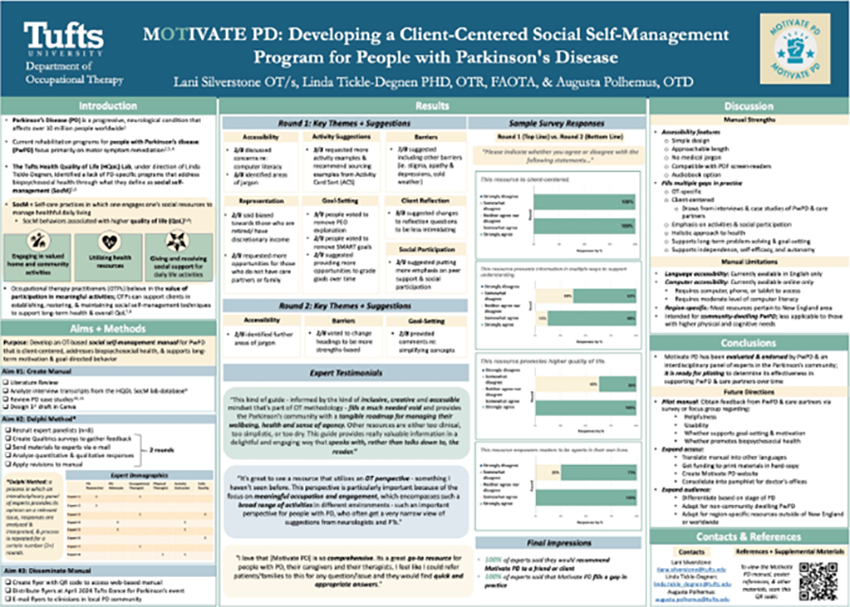
P45.13
1 Parkinsonlife Corporation, United States
2 Nova Southeastern University, United States
Background Parkinson’s disease (PD) symptoms such as tremor, bradykinesia, and facial masking often disrupt social roles, contributing to withdrawal and poorer quality of life.1˒2 People with PD frequently rely on outpatient therapy, community programs, and counseling.3 Engagement in group-based exercise and social activity improves mood, cognition, and mobility.4 The COVID-19 pandemic disrupted services in Tampa Bay, increasing isolation in an already vulnerable population. To address this gap, pdLIFE (Lifestyle, Information, Fitness, Empowerment) was founded in December 2020 with the mission to serve and unify the PD community through exercise, education, and social connection.
Methods Four processes guided formation: (1) creation of an LLC and IRS 501(c)(3) nonprofit application; (2) recruitment of board members including people with PD, care partners, healthcare providers, and advocates; (3) development of programs through rehabilitation and community fitness professionals; and (4) fundraising. A Facebook campaign funded initial outdoor classes during the pandemic. Legal and community support facilitated IRS approval, granted 18 months later, enabling growth through grants and private donations.
Results All programming is free of charge. pdLIFE has secured four Parkinson’s Foundation community grants, delivers eight weekly classes across three community sites, and offers multi-level exercise for general participants, care partners, and younger/early-stage PD. Monthly social lunches, caregiver and women’s retreats, healthcare provider seminars, and annual events such as the “pdLIFE Challenge” extend outreach. The organization’s listserv now connects more than 1,300 community members.
Conclusion Every six minutes someone in the U.S. is diagnosed with PD, with incidence 50% higher than previously estimated.5 Florida has the nation’s highest prevalence, with ∼80,000 individuals, including ∼11,300 in Tampa Bay.6 With a projected 20% increase by 2030,6 demand for community-based services will intensify. pdLIFE demonstrates that clinicians without business backgrounds can successfully establish sustainable nonprofit programs to support people with PD and their families.
P45.14
1 Northeast Ohio Medical University, United States
I explore how optimism and goal setting can shape the lived experience of Parkinson’s disease. Research on placebo and nocebo effects demonstrates that belief and expectation are not abstract ideas but biological forces that alter dopamine release, motor performance, and symptom severity. Neuroplasticity studies likewise show that effort and repetition can reshape the brain, even in the setting of neurodegeneration. Together, these findings suggest that the way Parkinson’s is presented at diagnosis can influence long term outcomes.
If Parkinson’s is framed as an inevitable decline, patients may disengage and retreat from active management. If instead it is framed as a condition that can be shaped through mindset, movement, and community, patients are more likely to act. Optimism, in this sense, is not naive. It is neurobiological.
One striking example of the power of mindset is Rhonda Foulds. Diagnosed in 1998, she states she went home and "waited to die." She gained over 100 pounds and required a wheelchair because she had become so unsteady on her feet. In 2005, after undergoing deep brain stimulation, her Marine son encouraged her to train for a 5K walk. As she began exercising and eating healthier foods, the weight came off and her life began to change. She began to set goals, and think of a future in which she could accomplish them. Running became her new identity. I met Rhonda at the 2024 Boston Marathon, where she finished her 125th marathon despite never having run one before her diagnosis. Meeting her, it is easy to see how mindset, humor, and an outrageous goal created a future and in her case helped reverse disability.
This case study illustrates what the research suggests: optimism and bold goals act as therapeutic tools. They engage biological pathways of resilience, sustain motivation, and promote behaviors known to slow disease progression.
At the point of diagnosis, clinicians have an opportunity not just to deliver a label but to plant the seeds of a mindset that transforms outcomes. By encouraging patients to pursue possibility, even through goals that seem impossible, we can help shift the trajectory of Parkinson’s disease from decline to resilience.
P45.15
1 New York Institute of Technology and Pass to Pass organization, United States
2 Pass to Pass Organization, United States
3 Pass To Pass Organization, United States
The International Classification of Functioning, Disability, and Health identifies Recreation and Leisure as essential components of well-being. Outdoor activities such as hiking offer physical and mental health benefits, yet individuals with Parkinson’s disease (PD) face barriers to participation due to PD symptoms. These barriers can contribute to social isolation and reduced quality of life. Pass to Pass (PtP) a benevolent organization, addresses these challenges by facilitating inclusive access to outdoor recreation for people living with PD.
Pass to Pass began as a grassroots initiative and has grown through the support of generous donors, a dedicated board of directors, and a team of volunteer hike leaders and support hikers. Many of whom have PD themselves. The program offers multi-day backpacking trips, with llamas carrying basic supplies for PD hikers. To accommodate a wide range of abilities and experience levels, the program has adapted its offerings over the years.
PtP now includes:
Lodge hikes: Hikers stay in a nearby lodge and do less remote day hikes. This is the least difficult option. Basecamp hikes: Hikers do day hikes of various lengths and difficulties from a basecamp location. Standard hikes: Hikes average 6 days over 30 miles, with varying degrees of difficulty. Advanced hikes: For PD hikers with backpacking experience and ability to carry their own gear. Hikes average 6 days and 30+ miles.
Pass to Pass has gained national recognition, including awards and media stories. Its sustainability is driven by community outreach and word-of-mouth referrals.
Now in its 10th year, PtP has hosted 59 trips with 283 PD hikers, 332 support hikers, and countless llamas, covering a cumulative total of 13,480 hiking miles. The program has expanded nationally, with hikers from 25 states and 3 Canadian provinces. There are now 7 local U.S. chapters in 6 states. Hiker testimonials highlight several positive outcomes, including increased confidence, reduced isolation, and a renewed sense of possibility.
Pass to Pass demonstrates that outdoor recreation is not only feasible but transformative for people living with PD. The program's success offers a replicable blueprint for others seeking to create inclusive, sustainable, and empowering recreational opportunities. By addressing barriers and fostering community, PtP helps individuals with Parkinson's live well—one trail at a time.

P45.16
1 Tango Therapy Project, United States
Introduction: Despite evidence of adapted tango’s benefits for people with Parkinson’s (PwP), there is a dearth of ongoing programming. The Tango Therapy Project (TTP) aims to share tango’s benefits more broadly by creating adapted tango programming for PwP, older adults, and those with other motor and neurologic conditions. In 2024, we hosted an Adapted Tango Fundamentals training and launched a nine-month pilot program for PwP and care partners.
Methods: TTP’s pilot program consisted of five 6-week adapted tango series, each open to 8 PwP and 8 care partners, led by 3 certified instructors, and supported by trained volunteers. Prior to each series, all PwP were invited to complete an optional 7-question QOL assessment adapted from the PDQ-39. At the first and final class, all PwP were invited to complete a TUG mobility test. Post-series, all PwP, care partners, and volunteers were invited to evaluate the program and opt into a qualitative interview.
Results: Results were overwhelmingly positive: 100% of evaluation respondents felt welcome and at ease; 89% of PwP would recommend TTP to other PwP, the majority improved on the TUG test, more than 75% showed QOL improvement, and many asked before each series concluded, “How can I keep dancing?.” Further results:
2 former dancers who now have PD enrolled, showing adapted dance programs enable disabled dancers to continue pursuing their art Care partners said our model put everyone “on equal footing” and created a space to witness other approaches to supporting a PwP 4 older adults without PD joined an under-enrolled series and integrated well Pilot year care partners have since trained to volunteer with TTP Volunteer interest is high and diverse (ages, race/ethnicity, gender, background: tango, dance, health, PT, caregivers, general public)
Conclusion: To expand and deepen our impact, we increased enrollment and series length and will broaden our audience to include people with other motor and neurological conditions, beginning with a post-stroke pilot. By developing ongoing programming, TTP can serve as a community site for investigating adapted tango’s impact, bridging clinical researchers and their intended beneficiaries. Such partnerships can advance awareness and funding for adapted tango—a joyful means of supporting QOL with age, alongside the technological advancements and scientific discoveries that have made our longer lives possible.
*PwP involved in program & design; not clinical research

P45.17
1 Parkinson Argentina, Argentina
Introduction Receiving a diagnosis of young-onset Parkinson’s disease has a profound impact. People cope with the new condition in different ways: some remain stuck in regret, living their lives sad or angry; others try to discover what can be learned from what happens to them and how to make meaning from it. When I was diagnosed at 33, I wish someone had shared with me some of the lessons that would help me navigate what was to come.
Objective To share, interact, and reflect on the experience of living with Parkinson’s for 15 years while being young.
Methods I used a qualitative methodology from anthropology known as autoethnography. Autoethnography seeks to systematically describe and analyze personal experience in order to understand cultural experience. In this approach, the researcher draws on their own experiences, reflections, and life events to explore and interpret broader social, cultural, and political phenomena.
Results As a sociologist, over the past 15 years I have spoken with hundreds of patients and healthcare professionals. I have also published articles, given presentations in diverse settings, interacted with specialists, worked at the National Ministry of Health, and contributed as a writer to the book Parkinson Positivos. Above all, I have lived through and accumulated experiences and challenges across different stages of my life. A synthesis of this journey can be expressed through 15 key reflections.
Conclusions Some of the main conclusions include: Parkinson’s is not everything in my life — it is just one quality among many. The diagnosis forces change, but it also offers an opportunity to redefine who you want to be. Parkinson’s in older adults is very different from Parkinson’s in younger people — not only in symptoms but especially in the social needs each person has. The diagnosis affects everyone around you, so it’s essential to build support networks.
It’s about focusing on the things I can do. The gaze of others can be uncomfortable, but the harshest judgment often comes from myself. Every person with Parkinson’s is unique. Trying to hide the disease only creates more stress. The effort must go elsewhere: toward learning to live with Parkinson’s and doing everything possible to live as well as I can.
Parkinson’s also gives you something we all should embrace: the ability to enjoy the present without waiting. Do today what you love, with the people you love.
P45.18
1 Tokyo Soteria NPO, Japan
At age 52, I was diagnosed with Parkinson’s disease. What unsettled me most was not the tremors, but the gradual erosion of speech — losing my voice felt like losing myself. As the words faded, so did my ability to maintain my professional role, social identity, and personal relationships.
I lead a community-based mental health organization in Japan. Ironically, while supporting others in expressing themselves and sustaining social inclusion, I was silently receding from these very structures. I began to withdraw — professionally, socially, emotionally.
To mask my impaired speech, I wore wireless earphones and pretended to have hearing issues. This allowed me to avoid speaking in public — an act of camouflaged communication that bought me time, dignity, and a sense of control over interactions. Yet it was also profoundly isolating.
Over time, I discovered adaptive tools. Delayed Auditory Feedback (DAF) technology, delivered through my earphones, enabled me to regain limited speech fluency. Similarly, Rhythmic Auditory Stimulation (RAS) via metronome apps improved my gait, helping me walk with more confidence. These tools not only enhanced function but also restored agency — rebuilding a fractured relationship between body and environment.
Losing verbal language led me toward alternative forms of expression — through short poems, gestures, and shared moments of silence. In unexpected encounters, I found renewed connection: instances where “not talking” still allowed for mutual understanding. These nonverbal exchanges, however brief or imperfect, reminded me that communication is more than speech.
This presentation offers an experiential perspective on the intersection of identity, loss, adaptation, and hope. It explores how people with Parkinson’s can reclaim connection — sometimes through speech, sometimes through silence, and sometimes through creative, embodied ways that transcend both.
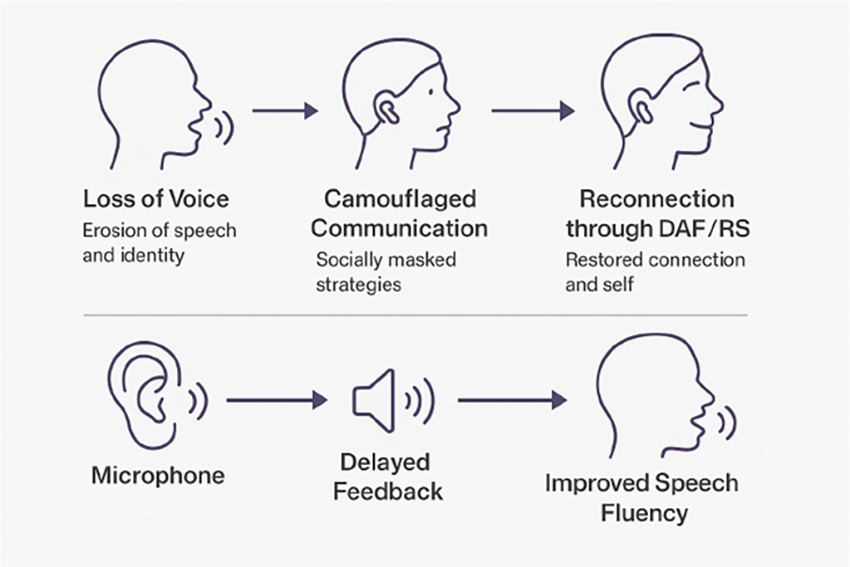
P45.20
1 Tokyo Soteria NPO, Japan
As the long-time care partner of a person living with Parkinson’s disease, I have witnessed how communication loss and emotional withdrawal gradually reshape identity — both for the individual and for those around them. My partner, diagnosed at 52, experienced a progressive loss of speech that affected not only the ability to express but also the sense of self.
This presentation is based on three years of longitudinal observation and reflective journaling, focusing on the psychosocial process of recovery rather than medical improvement. I observed how adaptation unfolded through a series of small, often invisible changes in daily life — moments of frustration, experimentation, and eventual rediscovery.
A key turning point came when my partner began using Delayed Auditory Feedback (DAF) and Rhythmic Auditory Stimulation (RAS). What began as coping tools for speech and gait evolved into instruments of self-regulation and emotional recovery. These simple auditory technologies did not merely enhance physical function; they reconnected my partner to others and to their own agency.
From a mental health perspective, recovery was not linear. There were alternating phases of withdrawal and re-engagement, silence and reconnection. Yet through creative expression — writing short poems, using gestures, sharing quiet moments — my partner gradually regained a sense of belonging. This process also transformed my own role: from trying to “fix” or “support” to co-existing with change and rediscovering meaning together.
Our experience suggests that recovery in Parkinson’s disease extends beyond clinical outcomes. It involves relational and emotional healing, supported by adaptive technologies, shared creativity, and mutual presence. For care partners, observing recovery becomes an act of participation — a reflective, reciprocal process that sustains hope for both.
P45.21
1 Vanderbilt University Medical Center, United States
BACKGROUND: Parkinson's Disease is much more than the hallmark motor symptoms. It is a disorder with a host of non-motor symptoms that impact each individual with Parkinson Disease with varying severity. These symptoms often predate motor symptoms and worsen with progression, but are often not as responsive to pharmacological and advanced therapies such as deep brain stimulation or focused ultrasound. Given the impact on the quality of life that these symptoms can have, it becomes important to utilize all the therapeutic interventions that might alleviate these symptoms. An integrative medicine approach can be beneficial here--incorporating mind-body medicine, Ayurveda and East Asian Medicine Modalities, and community building to formulate individualized treatment plans for individuals living with Parkinson Disease.
METHODS: Patients diagnosed with Parkinson's Disease are referred to a virtual group visit. Virtual group visits consist of 10 individuals with Parkinson Disease (+/- their care partner) and facilitated by movement disorders neurologists with integrative medicine expertise. The group visit will lasts 90 minutes with 30 minutes of didactics on a specific non-motor symptom and integrative therapeutic options for management and then 10 minute break out sessions with each patient to formulate a personal assessment and plan, while the remaining individuals meet and socialize. There will be a total of 7 visits. As a part of the visit, individuals will also fill out a survey regarding the visits and a QOL survey as well. They will continue seeing their primary movement disorders specialist as scheduled for medical management and advanced therapies.
RESULTS: Currently in Progress.
CONCLUSION: We are currently in the midst of the visits. The first visits were successful. This is a pilot project and so I am currently doing 3 group visits on the 2nd Friday of the month. Given the popularity, (170 patients requested a referral when it was announced) the goal is to offer these visits weekly on Friday mornings and afternoons. I hope there is an improvement in quality of life for individuals living with PD regarding management of the non-motor symptoms we address. I also hope there is less isolation and more connection since the groups will be together over the course of a couple of years and the hope is that relationships emerge that continue offline.
P45.22
1 watchyourstep, Australia
19/10/25 Abstract for poster – Self publishing
Goals and background.
How do we encourage those with Parkinson’s Disease (PD) to communicate better? Well, the author believes it is all about confidence and a little support goes a long way. Writing is a great way for those with PD to communicate better with their family, friends and the broader community. We with PD can achieve the goal of getting a personal story out; A published memoir or a novel that has been waiting for the right opportunity to emerge for half a life time. The author wants to assist as many as possible with PD to achieve this.
This poster explains how the author can help others with a desire to write to achieve a final product of a printed and/or e-book.
Methods The author has direct experience with a self-publishing project that took an autoethnographic approach privileging the lived context of participant/contributors,. As such, the project was designed with the individual contributors in mind. This is only one example of the infinite options available.
The author and collaborators have learnt through personal experience, the frustrations, revelations and sense of accomplishment that can be achieved by putting your thoughts on paper, telling the world about your journey. It involves putting yourself forward and involving those around you who you trust to support you in the substantial challenge of self - publishing.
The author discusses informed consent and many other legal and financial challenges associated with a quality project.
A book is always a personal venture and it may be a targeted audience, possibly for readers by invitation only, or something that is accessible to all. A personal understanding of what it is that one is wanting to achieve is the first of several questions that need to be asked and answered.
Results Many others may benefit from a self-published book as much as the author. Each author will regain confidence through achieving success and each publication is successful whether it sells 1000 copies or 10.
Conclusions The author now wants to encourage as many of my PD colleagues who have seriously considered this to take a leap of faith and roll the sleeves up and see it through to a final conclusion. You need to commit to allocating time, strategize financially along with a business plan as to how to market your book. Learn about several methods that the author has used to get the job done. Setting some basic goals and timelines will set you on the way.
Snowy Stinson
P45.23
1 NHS Health Professionals with Parkinson’s Support Group, United Kingdom
2 UK NHS Health Professionals with Parkinson's Support Group, United Kingdom
3 UK NHS Professionals with Parkinson's Support Group, United Kingdom
4 UK NHS Professionals with Parkinsons Support Group, United Kingdom
Background: Physical activity has established value in Parkinson’s disease both for improving current symptoms and possibly for disease modification. Amongst PwP, those with little previous experience of regular exercise may face challenges with motivation and adherence.
In 2024 the UK NHS Professionals with Parkinson’s Disease Support Group organised an exercise challenge for its members to help them adopt new, or maintain existing, exercise habits. This was intended to be a collaborative rather than competitive team effort and to accommodate all preferences and abilities. The challenge had a planned duration of one year to facilitate longer term adherence.
Methods: An invitation to sign up to a challenge devised by two members of the group (JA and RP) was sent out to the membership. This was entitled “The Great Wall of China Challenge” and represented a team effort to log cumulatively, over a year, a distance equivalent to the length of the Great Wall of China by means of running, walking, cycling, etc. Exercise modalities not usually denominated by distance such as martial arts and golf were counted by means of a formula awarding notional kilometres according to duration and intensity. Enrolment for the challenge was hosted on the Challenge Hound website which allowed participants to automatically upload their exercise data from a tracking device in addition to manual data entry. The Great Wall of China was chosen as an iconic and inspiring structure and its length (c. 21,000km) corresponded to what we had calculated might be an achievable distance for the group to “travel” in the course of a year.
Results: Out of 43 members of the group, 23 people signed up for the challenge which started on 1st April 2024. Distance“travelled” by each participant ranged from 31 – 3855km (mean 964, median 623). Total time spent on challenge-related exercise ranged from 10-382 hrs (mean 141; median 110.5) per participant. Mean number of exercise sessions per person participating over the period of the challenge was 172 (range 13 – 689; median 106.5).
Conclusions: Most participants fed back that they had found participation helpful for motivation and wanted to take part in a similar challenge the following year. Peer support seems to be a useful tool to support PwP in their efforts to engage with regular physical exercise.

P45.24
1 FuerteVida Parkinson No Limits, Spain
Introduction: Parkinson’s disease (PD) is a complex neurodegenerative disorder with motor and non-motor symptoms often inadequately managed by medication alone. Complementary therapies—physical exercise, artistic practices, and psychological support—are core elements of the Parkinson No Limits methodology, applied in both therapeutic holidays and daily rehabilitation.
Since 2019, Parkinson No Limits has implemented outdoor rehabilitation programs for people with PD (PwPD) and their families, in the Canary Islands and abroad. Disciplines include sports (surfing, kitesurfing, sailing, non-contact boxing, Nordic Walking, cycling, Pilates, Qi Gong), arts (theatre, dance, underwater painting, cooking), psychomotricity, Mindfulness, psychotherapy, hydrotherapy, music and speech therapy, physiotherapy, holistic nutrition, Shiatsu and much more.
In addition psycho- and neuroeducation promote self-awareness, understanding of psychophysical needs, and constructive communication with professionals and caregivers.
Method: Developed collaboratively by professionals, PwPD and families, the method integrates clinical, therapeutic, and social dimensions. Activities are conducted outdoors, benefiting from Fuerteventura’s mild climate and pristine natural environment, a UNESCO Biosphere Reserve.
Benefits: This holistic, transdisciplinary, person-centered approach, focused on individual resources and health potential, has significantly improved PwPDs’ quality of life, achieving national and international recognition. Outcomes are monitored through standardized tests, clinical evaluations, self-assessments, and ongoing research, part of which is presented at WPC2026.
Network and collaborations: FuerteVida Parkinson No Limits is a non-profit organization supported by the Canary Government and local institutions. It offers residents 5 weekly therapeutic activities (245 sessions per year) for free and accessible therapeutic holidays for non-residents.
The association collaborates with local and international Parkinson’s and neurological disorder organizations, educational institutions providing training and internships, and media for awareness campaigns.
Conclusions: The Parkinson No Limits method proves effective, innovative, and evolving. Its programs in the Canary Islands and personalized therapeutic holidays are internationally recognized as models of excellence. The growing volunteer and student training program has led to the creation of the Association’s training school.
P45.25
1 FuerteVida Parkinson No Limits, Spain
Introduction: Parkinson’s disease (PD) is a complex neurodegenerative and neuropsychological disorder with motor and non-motor symptoms often inadequately managed by pharmacological treatment alone. Complementary therapies such as physical exercise, artistic practices, and psychological support are integral components of the Parkinson No Limits methodology, also applied in therapeutic holiday programs.
Since 2019, Parkinson No Limits has been organizing personalized outdoor therapeutic holidays for people with PD (PwPD) and their families, both residents of the Canary Islands and international participants.
Methodology: Each therapeutic holiday is co-designed by the person with Parkinson’s, their family, and the multidisciplinary FuerteVida Parkinson No Limits team. A detailed assessment of health potential, residual resources, lifestyle, interests, and therapeutic needs leads to a customized program.
Activities include sports (surfing, paddle surfing, kitesurfing, swimming, sailing, non-contact boxing, archery, Nordic Walking, cycling, trekking, Pilates, Qi Gong), arts (theatre, dance, music, singing, underwater painting,painting), psychomotricity, mindfulness, bioenergetics, physiotherapy, hydrotherapy, music and speech therapy, shiatsu, craniosacral therapy, reiki, holistic nutrition and healthy cooking, horticultural therapy.
Nature and exploration of the local environment are key components. Therapeutic settings are outdoors, in areas chosen for optimal health conditions: stable climate, clean air, organic food, low stress, and strong connection with nature.
The process begins before arrival, continues during the stay, and is followed by individualized online support after return.
Method: The Parkinson No Limits method, developed by professionals and people with PD, integrates clinical, rehabilitative, and social aspects in outdoor practice, supported by Fuerteventura’s year-round mild climate and pristine environment, a UNESCO Biosphere Reserve.
Benefits: This holistic and transdisciplinary approach, centered on health potential and personalized care, has significantly improved the quality of life of PwPD and their families, earning national and international recognition. Short-, medium-, and long-term benefits have been evaluated through standardized tests, clinical monitoring, self-assessments, and ongoing studies, some presented at WPC2026.
P45.26
1 Patient Advocate, ParkinZone A.p.s (Rome), P.G.R. A.p.s (Rome), Parkinson No Limits (Fuerteventura), Italy
2 Clinical Psychologist, PhD Student in Neuroscience, Department of Systems Medicine, University of Rome Tor Vergata, Science Ambassador for World Parkinson Congress (WPC2026), Italy
Parkinson’s disease (PD) is widely recognized as a neurodegenerative condition with complex neuropsychological impact, affecting both physical and mental health and often disrupting family management and relationships, especially among people with young-onset PD. To address these challenges, multidisciplinary care should integrate peer support groups alongside other complementary interventions, aiming to reduce isolation and stigma while fostering well-being, good practices, and resilience.
A young-onset PD patient advocate launched two online peer support groups (Virtual Support Groups) to create an accessible online environment for active listening, sharing, and mutual support. The first one, “Tisana” (playing on words from Italian “Ti Sana” = Heal-Tea / CommuniTea), started in 2019 during the COVID-19 pandemic and was aimed primarily at people with PD over 60 years old. The second one, “Birretta” (literally “Little Beer,” conveying youthfulness and informality, similar in spirit to “Brew Crew”), targets younger participants. Both groups are still active today, meeting online once a week for about one hour.
The main goal of these initiatives is to improve the quality of life of people living with PD by providing a safe space for sharing experiences and promoting practical coping strategies and disease-related information. They also aim to reduce stigma and isolation, using technology to reach anyone in need.
Preliminary Results After more than five years of ongoing activity, during the last year Tisana held over 40 meetings with an average attendance of 14 participants per session, and Birretta held 21 meetings with an average of 11 participants per session. Consistent attendance and active engagement were observed, with subjective feedback highlighting enhanced emotional support, greater connection, and strengthened social bonds.
Both the Tisana and Birretta initiatives demonstrate that peer support groups can effectively complement traditional care, providing emotional, practical, and social resources for people living with PD. These experiences underline the value of participatory, peer-driven approaches in promoting resilience and counteracting isolation and stigma.
P45.27
1 School of Psychology, Faculty of Medical Sciences, University of Newcastle, United Kingdom
2 Department of Medicine, Aga Khan University, Kenya
3 Brain and Mind Institute, Aga Khan University, Kenya
4 Population Health Sciences Institute, Faculty of Medical Sciences, University of Newcastle, United Kingdom
Objective To explore how beliefs and attitudes towards Parkinson’s influence help seeking behaviours and experiences of stigma among people with Parkinson’s (PwP), caregivers and alternative healers in rural Kenya.
Background Despite the significant impact of Parkinson’s on quality of life (QoL) for PwP and their families, limited awareness, gaps in health literacy and culturally rooted understandings of illness can perpetuate stigma (Fothergill-Misbah, 2023). In Kenya, beliefs about health can result in practices of medical pluralism, with illness perceived as simultaneously physical and spiritual (Omonzejele, 2008). To optimise engagement with services, understanding these perspectives is essential to foster trust and deliver personalised, holistic care.
Methods Data collection took place in Kilifi, Kenya in December 2024. Semi-structured interviews were conducted with PwP (n=5), caregivers (n=2) and alternative healers (n=4). Interviews with PwP and carers sought to understand how they experience Parkinson’s within their cultural and social context, including the role of stigma in shaping disclosure and care seeking decisions. Interviews with alternative healers sought to explore how they understand and approach Parkinson’s.
Results Understanding was limited across groups with symptoms attributed to ageing, other diseases (hypertension, stroke or diabetes), or witchcraft. PwP described difficulties obtaining accurate diagnosis and treatment, with healers noting these challenges often led to their input being sought. Healers offered reflections on their role including barriers to collaboration, though some emphasised the value of working together. Differences in religious practices highlighted the intersectionality of cultural and spiritual beliefs in shaping care. Most PwP reported not discussing their condition or knowing others affected. Yet, a carer stated, “Now I know more, I wish this education about Parkinson’s could be spread more widely. The PwP are out there, we just need to find them. And those who know should not hide the condition from others.” Healers suggested ways community awareness could be increased through chiefs, intercessors and doctors.
Conclusion For PwP and their families, systemic change is needed to improve accessibility, acceptability and accountability. Improving QoL could be achieved through a commitment to understanding cultural beliefs and embedding a community driven, co-produced approach to Parkinson’s care.
P45.28
1 Parkinson Association of the Rockies, United States
2 Colorado State University, United States
3 Colorado State Univeristy, United States
4 University of Colorado Anschutz, United States
Introduction: People with Parkinson’s disease (PwPD) often experience loneliness, isolation, and reduced quality of life due to both physical and emotional symptoms. Social prescription offers one intervention which may reduce social isolation, improve mood, build confidence, and support management of long-term conditions. The goal of this project is to identify the barriers and supports involved in implementing an Occupational Therapy (OT) led social prescription program for PwPD from the perspectives of multiple stakeholders. Occupational Therapists are uniquely trained to understand how meaningful activities and engagement affect well-being across physical, mental, and social domains. The OT-led social prescription program included an activity analysis, co-designed social prescription in the community, and monthly follow-up to promote participation.
Methods: Focus groups were conducted with study participant completers (2 groups, n=7), CSU Extension specialists (1 group, n=5) and Parkinson's Association of the Rockies (PAR) staff (1 group, n=4) to learn about barriers, supports, and ideas for scalability of OT-led social prescription. Two research assistants independently reviewed and coded the data from the focus groups to identify common themes.
Results: Participants reported that their social prescriptions increased their social involvement, both in-person and virtually. Monthly check-ins with OTs supported motivation, accountability, and self-reflection, though some participants found them repetitive. CSU Extension and PAR staff identified barriers to expanding the program in rural areas, including limited activity options, transportation challenges, and the stigma surrounding loneliness. Participants also noted that caregivers and other older adults facing isolation could benefit from similar programs. Suggestions for study improvement included using less clinical language to reduce stigma and involving doctors’ offices to increase recruitment.
Conclusion and Implications: Findings from this study provide valuable insight into what helps or hinders the implementation of social prescription for people with PD. Future steps include refining the program based on feedback, updating language, addressing rural access challenges, and expanding outreach. Continued research and broader implementation will help raise awareness of social prescription as a tool occupational therapists can use to promote social connection and well-being.
P45.29
1 Parkinson Voice Project, United States
For people with Parkinson’s, speech and swallowing can be a daily battle. The SPEAK OUT!® Therapy Program, developed by Parkinson Voice Project®, helps people with Parkinson’s regain and retain their speech and swallowing. Besides individual and group speech therapy, we offer two singing groups to build stronger voices and hope. Our unique approach to singing combines the skills and talents of Speech-Language Pathologists (SLPs) and Music Directors.
Our in-person choir offers an opportunity for participants to strengthen their voices. However, many people with Parkinson’s have never sung in a choir or read music. Parkinson Voice Project has developed a unique method for writing song lyrics to teach our non-music-reading singers how to sing the music. We use specific color coding, highlighting, spacing, margins, and fonts to indicate to the singers when and what to sing. This group performs at concerts multiple times a year. Our lyric writing method helps the singers gain confidence.
We also developed an online Sing-Along program. Participants in this virtual group are encouraged to use INTENT with their voice, in a fun, relaxed setting. Each weekly Sing-Along session is thirty minutes. Simple, well-known songs are curated by themes, like Broadway Musicals, Old Time Rock and Roll, or Folk music. Lyrics are presented using a specific font, spacing, and highlighting to help singers clearly follow the music.
Our SLPs play a key role in the singing groups. For the in-person group, an SLP warms up their voices using the SPEAK OUT!® Therapy exercises. Throughout the rehearsal, singers are reminded to sing and smile with INTENT! An SLP hosts an online Read-Along weekly for the singers to practice reading with INTENT. The more familiar the singers are with the lyrics, the better they sing them. During the Sing-along, the SLPs remind the participants to sing with INTENT.
This combination of speech therapy and music direction creates a successful and fun way for the singers to sing with INTENT! Whether singing in our in-person choir or singing virtually from home, our singers use their voices with purpose…and find joy and connection in the process.
P45.30
1 Parkinson Voice Project, United States
A common misconception is that the internet is only for younger generations. False! Parkinson Voice Project®(PVP) squashes this stereotype. PVP opens the gateway to all things telehealth.
On a Thursday in March of 2020, due to COVID, our clinic had to close. Patients were unable to come to the clinic for their speech therapy sessions. This was a problem. The following day, Samantha Elandary, our Founder and CEO, led the first online SPEAK OUT!® Home Practice session on Facebook Live. In addition to their individual and group therapy sessions, patients need to practice their SPEAK OUT!® Therapy exercises every single day to retain their speech and swallowing. Thirty participants joined that day. We thought these practices would be temporary, but they became a game-changer for people with Parkinson’s.
We will celebrate six years of SPEAK OUT!® Home Practice sessions in March 2026. Approximately 5,000 people with Parkinson’s around the world practice with us weekly. What began as a temporary solution to help our local patients in Dallas has evolved into a phenomenal way to support people around the globe with Parkinson's disease.
We also transitioned our individual and group therapy sessions to Zoom. Now, we can help anyone in Texas regain and retain their speech and swallowing. Bad weather, “off” days, transportation problems, and mobility challenges no longer interfere. Our patients are mastering their goals in fewer sessions. Outcomes have improved.
We realized that there was now a way to make our program accessible to every American. Parkinson Voice Project is collaborating with university speech clinics to provide SPEAK OUT! Therapy without charge through telehealth. These SPEAK OUT! Therapy & Research Centers are also conducting efficacy research on speech and swallowing disorders in Parkinson’s.
Our Certified SPEAK OUT! Providers take the time to teach our patients the necessary steps to access Zoom and our abundant online resources. These skills enable them to attend other teletherapy appointments, connect with family members in another state through Zoom, and enhance their healthcare literacy. Society may put people with Parkinson’s in a tiny box. Parkinson Voice Project does not. No one is “too old” for teletherapy!
P45.31
1 Parkinson Voice Project, United States
Up to 90% of people with Parkinson's may develop a speech problem. Left untreated, it can become a swallowing problem, known as dysphagia. It does not typically appear as a sudden inability to swallow, but rather as subtle, progressive changes that disrupt the coordinated process of chewing and swallowing.
Swallowing is a complex, automatic movement that involves dozens of muscles working in perfect harmony. Dopamine is essential for planning and controlling these automatic muscle movements. As the dopamine-producing cells in the brain degenerate or become impaired in Parkinson's, this automatic coordination is disrupted, making the swallowing process challenging.
Initially, dysphagia may appear mildly with issues such as taking a longer time to eat a meal or coughing at mealtimes. However, it's vital to recognize that it can progress over time to become a critical symptom of Parkinson’s disease, which, left untreated, can be life-threatening.
Symptoms of a swallowing disorder may include:
Coughing While Eating or Drinking: This can be a significant warning sign that food or liquid might be entering the trachea instead of the esophagus. Wet or Gurgly Vocal Quality: This can suggest that food or liquid may have reached the vocal folds or is lingering in the throat. Managing mixed consistencies, such as cereal and milk or watermelon, which is 90% water, may be uncoordinated, resulting in some liquid falling back into the throat before the swallow is initiated. Feeling Like Food or Pills Are Getting Stuck in the Throat: This sensation can occur because the muscles aren't moving the bolus (chewed food or liquid) efficiently through the pharynx or esophagus. Unexplained Weight Loss: If a person struggles to swallow, they may begin to eat less, or their body might not be processing nutrients efficiently, leading to unintentional weight loss.
The SPEAK OUT!® Therapy Program, developed by Parkinson Voice Project®, helps people with Parkinson’s and related disorders regain and retain their speech and swallowing. Our therapy program teaches patients how to speak and swallow with INTENT. “INTENT” is doing something with conscious effort. People with Parkinson’s can keep their swallowing strong by going through the SPEAK OUT! Therapy Program, attending a weekly SPEAK OUT! Therapy Group, and by eating with INTENT. A swallowing disorder is not inevitable with a Parkinson’s diagnosis.
P45.32
1 Parkinson Voice Project, United States
Around 90% of people with Parkinson’s disease may have speech and swallowing disorders. Only 3-4% of people with Parkinson’s receive the speech therapy services they need. The numbers do not add up.
The SPEAK OUT!® Therapy Program, developed by Parkinson Voice Project®, helps people with Parkinson’s and related disorders regain and retain their speech and swallowing. Our therapy program teaches patients how to speak with INTENT. “INTENT” is doing something with conscious effort. The “Circle of INTENT” explains how our unique therapy program works. The Circle never ends, just like the SPEAK OUT! Therapy Program never ends. People with Parkinson’s need continual speech therapy services. The Circle of INTENT highlights the various therapy components and emphasizes that this program is lifelong.
The first step in our program is the SPEAK OUT! Therapy Evaluation. We take a video of our patients speaking with and without INTENT to see if they would be a good candidate for therapy.
For the second step, every patient receives a SPEAK OUT! Therapy Booklet at no cost. The Booklet contains exercises and lessons that the patient will practice to maintain their speech and swallowing strength. We also offer our eLibrary, which provides access to online materials at no cost.
The third step is the “What is Parkinson’s? Video.” This video explains Parkinson’s, the role of dopamine, and its impact on the voice. It is an informative video that patients and their families watch every 6 months.
The fourth and fifth steps in our program are the individual and group therapy sessions. Patients first attend individual therapy and then transition to group therapy. Patients first learn how to speak with INTENT and how to do the SPEAK OUT! Therapy exercises. In the SPEAK OUT! Therapy Groups, patients connect with others who are also speaking with INTENT.
The next part of our program is the Refreshers. We help our patients throughout their entire Parkinson’s journey. We re-evaluate patients every 6-12 months to ensure they are using INTENT and following their therapy protocol.
The last part of our program is the daily SPEAK OUT! Home Practice. Patients must continue to practice every single day by using their Booklet or the Home Practice Sessions online.
We are more than happy to help our patients for the long haul. It is a life-long commitment to keep the voice and swallowing strong. Voices do not have to be lost, and foods do not have to be avoided.
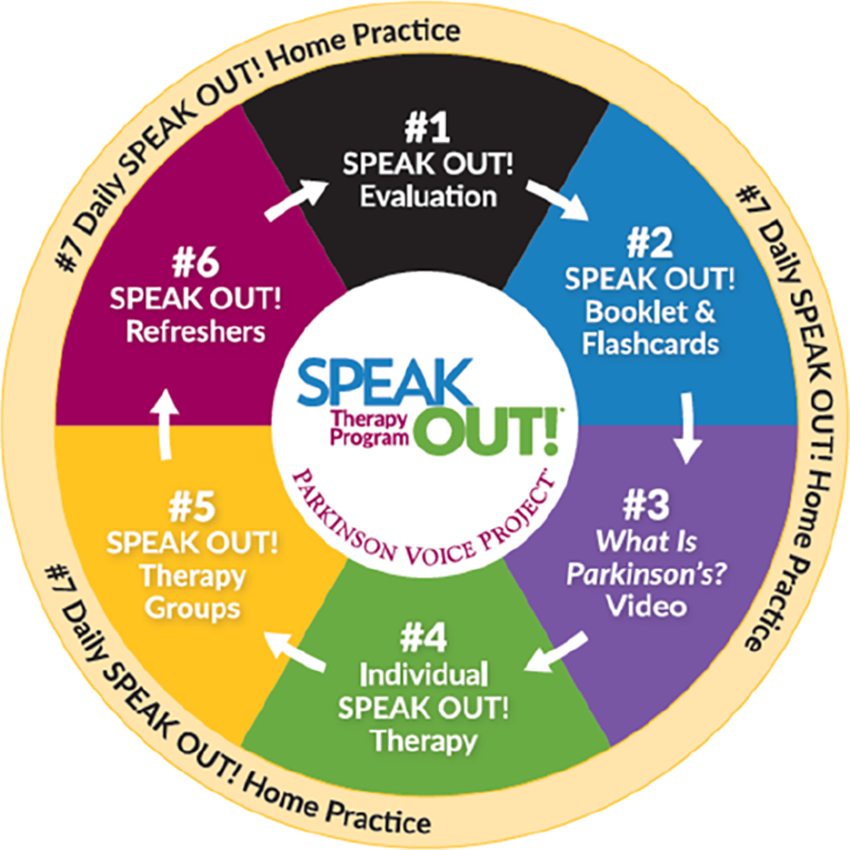
P45.33
1 American Parkinson Disease Association, United States
Background: People diagnosed with Young Onset Parkinson’s disease (YOPD) face unique challenges, including career and financial pressures, parenting responsibilities, and feeling alone in their diagnosis. Yet most PD programming is geared toward older populations, leaving YOPD needs unmet. To address this gap, the American Parkinson Disease Association Northwest Chapter launched YOPD-CON, a two-day conference designed by and for people with YOPD.
Objective: To reflect on insights from the inaugural 2023 YOPD-CON and to provide a preview of the expanded 2025 program, including planned evaluation and growth in reach.
Methods: The event was structured to (1) deliver practical, age-relevant education, (2) foster peer connection, and (3) elevate lived experience voices. The 2023 program included general sessions, breakout discussions, and networking. Post-event surveys captured satisfaction, learning, and suggestions for improvement. The 2025 event will incorporate pre- and post-event surveys to measure knowledge gained, confidence in self-management, sense of community, and intent to participate in future YOPD programming.
Results: In 2023, YOPD-CON hosted 94 attendees (67% people with PD, average age 53). Participants praised the event as “life-changing,” particularly the opportunity to meet YOPD peers for the first time. Feedback emphasized the need for greater accessibility, caregiver sessions, and a better balance of educational and social programming. Building on this, the 2025 conference (Oct 25–26) has already registered more than 210 participants, more than doubling the 2023 total.
Conclusion: YOPD-CON highlights the value of programming tailored to younger people with PD. By combining lessons learned from 2023 with expanded programming and evaluation in 2025, the event is evolving into a scalable model for addressing gaps, strengthening community, and improving quality of life for those navigating PD at a younger age.
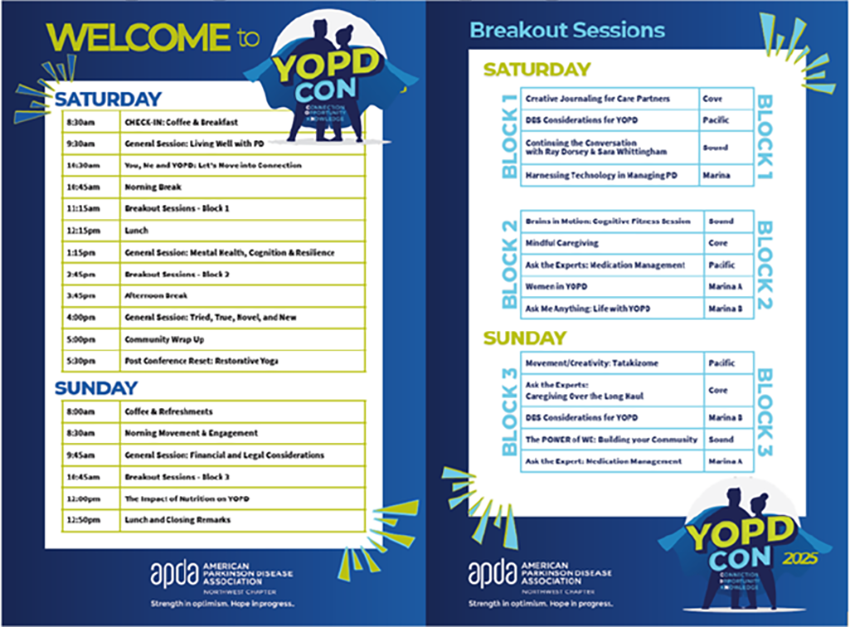
P45.34
1 Shirley Ryan AbilityLab, United States
2 Tellin' Tales Theatre, United States
3 Shirley Ryan AbilityLab; Northwestern University, United States
Introduction: People with Parkinson’s disease (PwP) and their care partners often voice challenges of acceptance, isolation, stigma, and limited psychosocial support opportunities. The Tellin’ Tales of Parkinson’s pilot program was designed to foster emotional expression, social connection, and empowerment by integrating storytelling and theatre-based practices that promote communication, cognitive engagement, and community building.
Methods: Eighteen participants completed the pilot program across three groups: two PwP groups (n = 7 and n = 6) and one care partner group (n = 5). Each group attended six virtual storytelling workshops, a dress rehearsal, and a final performance. The two-hour workshops introduced storytelling elements and incorporated theatre-based exercises to promote communication, collaboration, and emotional expression. Sessions included story sharing, peer feedback, and affirmations to foster resilience and optimism. Dress rehearsals focused on voice projection, movement, and transitions. Participants with geographic barriers pre-recorded their stories. The final performance, attended by loved ones and community members, gave participants a space to share their Parkinson’s stories and celebrate each other.
Results: Eighteen participants (13 PwP, 5 care partners) completed the 2024-2025 program. Among PwP, 9 were male and 4 female (ages 55-92, M = 70.5); for care partners, 2 were male and 3 female (ages 42-74, M = 61.4). Most identified as White (n = 15), with 1 Black, 1 Latino, and 1 Indian American. Participants represented multiple locations, including Chicago, nearby Illinois suburbs, North Carolina, Wisconsin, and Indiana. Year of PD diagnosis ranged from 2012-2024, with symptom onset from 2010-2024. Preliminary qualitative feedback indicated improved executive function, greater self-acceptance, and strengthened empathy and connection with peers and the Parkinson’s community. Many reported increased confidence and pride after the final performance, reinforcing community and contribution. One care partner shared, “Mom did an open mic last night. It’s the first time she’s read publicly in like 10 years.”
Conclusion: The Tellin’ Tales of Parkinson’s pilot program highlights storytelling as a powerful tool to support the emotional and social well-being of people with Parkinson’s and care partners. Preliminary findings suggest that integrating storytelling and theatre-based practices can foster connection, empowerment, and self-acceptance.
P45.35
1 Parkinson's Western Australia, Australia
Introduction In 2018 I was diagnosed with YOPD. This changed the direction of my life and career. As a neurologist and medical researcher I have the unusual position of experiencing PD as a PwP and a physician. My goal is to use this knowledge to enhance interactions between PwP and their medical attendants. I seek to advocate for improvements in the care for PwP and simultaneously attempt to assist my physician colleagues gain a greater understanding of living with PD, and what the needs of PwP are.
Methods I present my life story, focussing on the key events related to PD. This includes a long prodrome with an isolated exercised induced foot dystonia, two years of more obvious motor symptoms during which time I did not disclose my suspected diagnosis, then my reaction to the formal diagnosis, large scale public disclosure of the diagnosis, the exercise programs I developed using non-contact boxing and yoga, a period of stabilization or improvement, then the impact of several intercurrent illnesses and how these affected my PD. I conclude by discussing the idea that more positive framing of the diagnosis, along with early dopamine replacement to maximise the ability to exercise, along with other lifestyle changes, may alter the course of PD, by increasing “healthspan”.
Results For each of these key events I provide supportive data and references. This will include material on psychological issues related to adapting to and living with a chronic condition, doctor and PwP communication, specific issues relating to being a physician and a patient, the value of exercise (including my own work on boxing and yoga) and a section on peri-operative issues related to PD based on my experience of both elective and emergency surgeries, and the importance of diet and other lifestyle modifications.
Conclusions The goal of this is to integrate evidence based research into a narrative of living well with PD.
P45.36
1 Midwestern University, United States
2 Creighton University, United States
3 United States
Introduction and Background Parkinson disease (PD) is a progressive neurological disorder characterized by resting tremors, bradykinesia, rigidity, postural instability. This can cause a significant decrease in physical activity, social withdrawal, and quality of life. Several studies have reported positive effects of pickleball in the healthy adult population, including improved mental health, cognitive functions, physical capabilities, decreased pain, and improved quality of life. However, there are no known studies assessing the impact of pickleball on people with PD. This qualitative study aimed to examine the perspectives and experiences of individuals with PD who participated in a six-week pickleball program.
Methods Sixteen participants with idiopathic PD were enrolled in a 6-week, 2x/week pickleball program led by a certified pickleball coach. All sessions included a dynamic warm up, skills practice and scrimmages. Qualitative data was collected after completing the 6-week program via semi-structured small group interviews administered virtually. The interview guide consisted of seven open-ended questions focused on capturing the experiences and perspectives of participating in the pickleball program. Additional questions were included during the interviews based on the participants’ responses, to deepen the interactive discussion and enrich the data. The interviews were audio recorded, transcribed and reviewed independently by two researchers to identify codes and themes. The reviewers discussed and agreed upon the final themes.
Results: Sixteen participants were enrolled, with 15 (10 males, 5 females; mean year of diagnosis = 6.0 years; Hoehn and Yahr stages I-III) completing the entire study. One participant withdrew due to medical reasons unrelated to the study. Qualitative data revealed four themes: 1) Playing pickleball created positive social-emotional connections, 2) Pickleball allowed transcendence from their Parkinson identity, 3) Pickleball was thought to be a sustainable activity for people with PD, and 4) Participants felt that pickleball could address motor and non-motor symptoms of PD.
Conclusions The game of pickleball fostered social-emotional engagement among participants while also engaging in physical activity to address motor symptoms of PD. The participants alluded that playing pickleball, socializing, and learning a new skill allowed them to feel a sense of normalcy away from their identity as a person with a disease.

P45.37
1 Midwestern University, United States
2 Creighton University, United States
3 United States
Introduction and Background Parkinson disease (PD) is a neurodegenerative condition that presents with the cardinal signs of bradykinesia, resting tremors, rigidity, and postural instability. These symptoms can significantly impact motor and non-motor function. Pickleball is a fast-growing sport that has shown to improve mental health, cognition, physical function, and quality of life. To date, there are no known studies assessing the effects of pickleball on people with PD. The purpose of this study is to assess the effects of pickleball on motor and non-motor symptoms of people living with PD.
Methods A 6-week pickleball program was delivered in 12 classes of 1-hour duration twice weekly by an experienced pickleball coach with understanding of PD. All classes had warm-up, rules instruction, skills practice, game play, cool-down and debrief. Quality of life was assessed with the Parkinson Disease Questionnaire (PDQ-8), non-motor symptoms with the Non-Motor Symptom Questionnaire (NMSQ), global cognition with the Montreal Cognitive Assessment (MoCA), balance and gait with the Mini-BESTest, gait speed with the 10-meter walk test (10MWT), grip strength with handheld dynamometry (HHD) and upper limb function with the shirt buttoning test and 9-hole peg test (9HPT). Data collection occurred at pre-test, post-test, and one-month follow-up.
Results Sixteen participants were enrolled in the program, with one withdrawing due to unrelated medical issues. Therefore 15 participants (10 males, 5 females; mean year of diagnosis = 6.0 years; Hoehn and Yahr stages I – III) completed the entire program. Shirt buttoning across time (81.1s, 66.1s, 52.2s, p<.001, η2p = 0.6), HHD of the right hand (67.3lbs, 70.7lbs, 70.5lbs, p=.021, η2p = 0.26), and 9HPT of the left hand (32.4s, 30.8s, 28.8s, p=.003, η2p= 0.36) improved significantly over the duration of the study. Gait speed, Mini-BESTest, MoCA, 9HPT right, NMSS, PDQ8, and 10MWT scores were not statistically significant (all p>.14). However, there were trends of improvement in 9HPT left (p=.06, η2p =0.46).
Conclusions: The significant changes in the shirt buttoning task and handheld dynamometer grip test imply that a 6-week pickleball intervention may improve upper limb function to a greater degree than functional balance and gait speed in patients with PD.
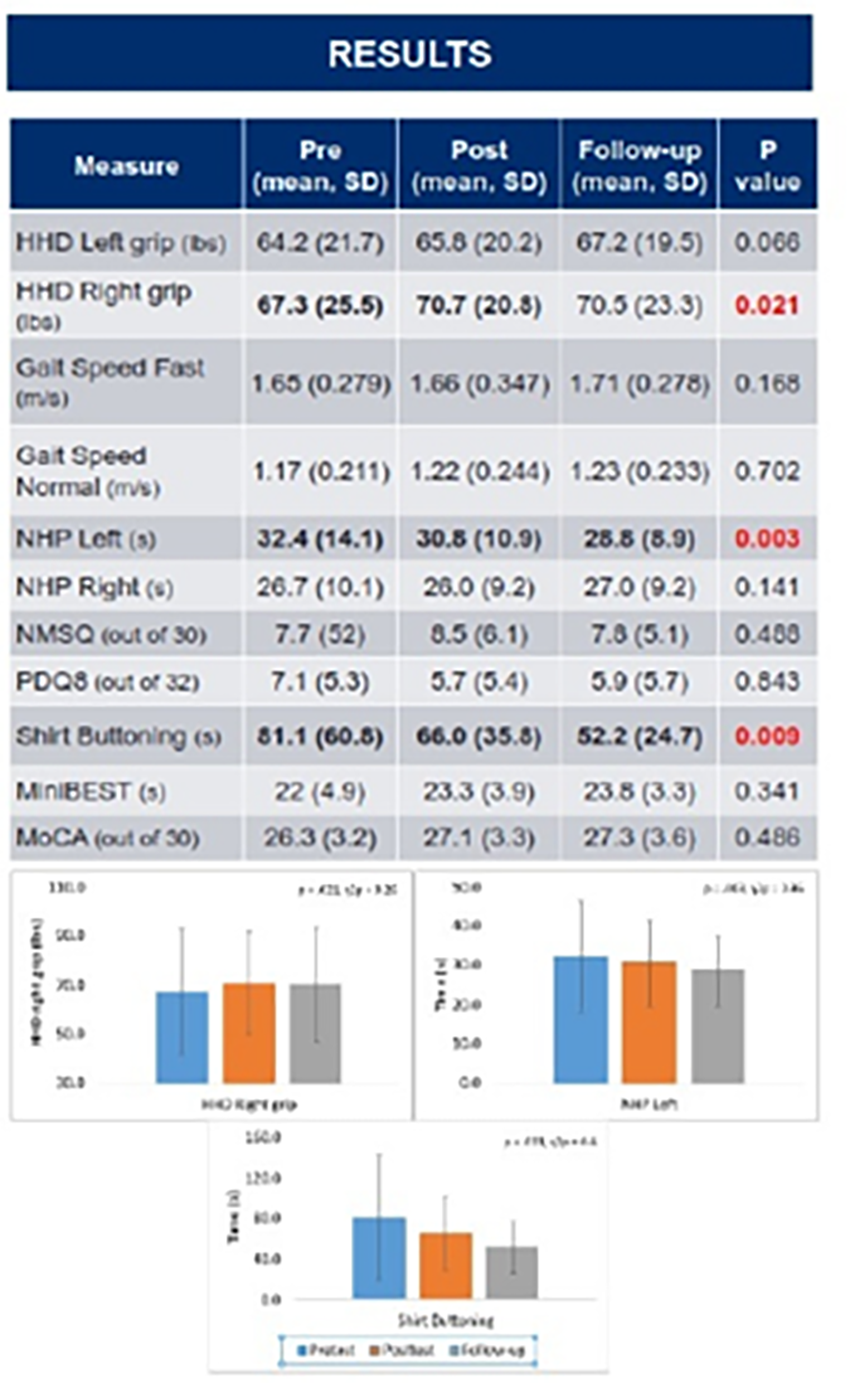
P45.38
1 Midwestern University, United States
2 Creighton University, United States
3 United States
Introduction and Background Parkinson disease (PD) results in resting tremors, rigidity, bradykinesia, and postural instability. These symptoms can limit activity and socialization. Pickleball has been shown to improve coordination, cardiovascular fitness, and mental health in healthy adults. To date, no studies have assessed the feasibility of pickleball for people with PD. The purpose of this study was to assess the feasibility of a pickleball program for people living with PD.
Methods 16 participants were enrolled in a 6-week pickleball program twice a week for one hour each. The sessions were led by a certified pickleball coach and assisted by at least one physical therapist and 3-5 physical therapy students. Students were assigned to guard those in the fall risk category. All participants completed fall safety training during the first session. Each session included warmup, learning of rules, drills, game play and cool down. Feasibility variables included retention rate, attendance rate, adverse events, safety events, and resources. Adverse events were defined as any injury or issue related to participation that required a participant’s withdrawal from the study. A safety event was defined as an event that either led or did not lead to injury but did not result in withdrawal.
Results Fifteen participants (10 males, 5 females) with history of PD (H&Y range = I-III) completed the entire program. Sixteen participants started the program, however, one person withdrew due to an unrelated medical issue, for a retention rate of 93.8%. The attendance rate was 83.3%. Four participants required guarding based on fall risk. There were no adverse events and two safety events. One participant fell on arrival prior to the scheduled study time and gained medical clearance to return the following session. Another participant had a fall without injury during a study-related activity and immediately resumed activities. Equipment needed included eight pickleball paddles, balls, a net, and an indoor space. Other resources included a coach, volunteers to ensure safety, and at least one physical therapist to supervise the students.
Conclusions A pickleball program for people with PD was feasible, with high attendance and retention rates, no adverse events, and low number of safety events. Resources, such as a place to host the program, equipment, and volunteers are needed. The volunteers were essential to prevent falls during the sessions for those with increased fall risk.

P45.39
1 Kirk Gibson Center, United States
2 University of Michigan-Flint, United States
Introduction: Parkinson’s disease (PD) management increasingly recognizes the role of socialization and regular exercise in improving function, quality of life, and slowing disease progression. To overcome financial barriers and social isolation, the nonprofit Kirk Gibson Foundation in collaboration with InMotion®, established the Kirk Gibson Center for Parkinson’s Wellness—a facility that provides free access to PD-specific movement and educational programs within a supportive and welcoming community to improve quality of life for those living with PD.
Methods: Through extensive outreach—Kirk Gibson's personal story, media coverage, webinars, open houses, newsletters, and a dedicated website—the Center generated strong community interest and enthusiasm around its opening. Since August 2025, 333 Members with PD have completed baseline assessments and are eligible to participate in over 100 weekly PD-specific classes. Members were assigned to one of four functional levels using previously published cut-offs for outcome measures: Montreal Cognitive Assessment (MoCA), Five Times Sit-to-Stand, Timed Up and Go (normal and cognitive), 3-Meter Backward Walk, gait speed (normal and fast), Six-Minute Walk Test, and a novel floor transfer test (Borchers et al., 2019). Assessors considered Member goals and personal factors—such as age, time since PD diagnosis, fall history, and balance confidence—to recommend a class level aligned with each Member’s optimal challenge point (i.e. sufficiently challenging to promote improvement while remaining safe). Member surveys, coach feedback, and 6-month reassessments will guide ongoing class placement. Voluntary post-class survey responses consistently included five-star ratings, highlighting strong Member satisfaction with the program.
Results: Since launch, the Center has built a team of >20 PD-specialized Coaches, registered over 1,000 people with PD as Members, and engaged more than 50 volunteers. Assigned functional groups (Group 1: n=49, Group 2: n=69, Group 3: n=107, Group 4: n=108) showed statistically significant differences across all outcome measures (p < 0.001).
Conclusion: The Kirk Gibson Center provides a community-based model for people with PD and their families offering PD-specific movement and educational programs in a supportive community environment. Functional stratification may facilitate long-term participation by fostering success, social connection, overall member satisfaction, challenge, and safety.
P45.40
1 FuerteVida Parkinson No Limits, Spain
2 University of Rome Tor Vergata, Italy
3 Neurosciences and Cell Biology Institute, City St George's University of London, London,, United Kingdom
4 Neurosciences and Cell Biology Institute, City St George's University of London, United Kingdom
5 Department of Neurology, IRCCS INM Neuromed, Italy
Introduction: Parkinson’s disease (PD) is a complex neurodegenerative condition affecting both the body and the mind, resulting in reduced quality of life and suffering in personal relationships. Especially for women, many subtle aspects of the broad spectrum of symptomatology are often overlooked and insufficiently managed by medications alone. In fact, gender differences and social expectations may increase the physical and emotional burden for women, also affecting body perception and the expression of femininity.
Objectives: Be Woman Project aims to improve quality of life, psychological and physical well-being of women with PD, identifying their specific needs and offering a tailored and olistic approach of rehabilitation.
Methods: Be Woman Project is a one-week outdoor therapeutic program, where an all-female team of professionals is combining Parkinson No Limits Method activities with Mindfulness and Compassion-based meditations, adaptive sports and the power of nature for a full immersion experience in the beautiful island of Fuerteventura (Canary Islands, Spain). All proposed inputs focus on psychoeducation, emotional regulation and psychological support to foster a stronger sense of self and develop a new life project for the future. After the one-week period of group activities on the island, participants continue to receive support through monthly online group meetings, aimed at enriching international communities of women with PD and strengthening relational bonds.
Be Woman Project is also a scientific research protocol: neuropsychological assessment is conducted both before and after treatment. Preliminary results are presented in a separate poster.
Results and Conclusion: Be Woman Project is feasible and effective to imporve quality of life and psychological well-being for women with PD. Now in its 4th edition, the project stands out as an international and innovative outdoor therapeutic program that truly enriches the personal experience of its participants
P45.41
1 Adewunmi Desalu Parkinson's Foundation, Nigeria
Background: Access to multidisciplinary Parkinson’s disease (PD) care in low- and middle-income countries (LMICs) remains limited due to a shortage of neurologists, fragmented systems, and poor awareness (Dotchin et al., 2021; Okubadejo et al., 2020). In Nigeria, people living with Parkinson’s disease (PwPs) face stigma and cultural misconceptions that associate tremors and rigidity with witchcraft or aging (Owolabi et al., 2018). These beliefs delay diagnosis, limit adherence to treatment, and deepen isolation and distress.
To address some of these gaps, the Adewunmi Desalu Parkinson’s Foundation (ADPF) developed a Revolving Program Model, an integrated, facility-based but community-oriented framework that combines clinical referrals, physiotherapy, therapeutic, psychosocial, support group, and welfare interventions for holistic PD care.
Objective: To describe the design, implementation, and outcomes of the ADPF Revolving Program as a scalable model improving quality of life, functional independence, and social inclusion among PwPs in Nigeria.
Methods: A mixed-methods design was applied at the ADPF Parkinson’s Center in Lagos. The program integrated medication support, physiotherapy, psychosocial counseling through support groups, dance therapy (Nigerian music), handwriting classes, non-contact boxing, caregiver education, and community awareness. Quantitative measures assessed medication adherence, motor function (UPDRS-derived), and caregiver burden (Zarit scale). Qualitative interviews explored participants’ experiences, stigma reduction, and program acceptability.
Results: Preliminary findings revealed improvements in medication adherence, mobility, and emotional well-being. Caregivers reported reduced stress and improved coping. Participants demonstrated increased confidence, self-esteem, and willingness to discuss symptoms openly. Community education and support groups strengthened morale and social participation, reducing stigma and isolation. The revolving model’s low-cost structure enhanced sustainability and engagement.
Conclusion: The ADPF Revolving Program shows that an integrated, multidisciplinary, and culturally grounded approach can transform Parkinson’s care in low-resource settings, offering a replicable model for Sub-Saharan Africa.

P45.42
1 University Hospitals of Derby and Burton, United Kingdom
2 Derby County Community Trust, United Kingdom
Background: Parkinson’s is the fastest-growing neurological condition globally, affecting around 153,000 people in the UK in 2023 and costing £277 million annually in unplanned hospital admissions (Parkinson’s UK). Regular physical activity (≥2.5 hours/week) helps manage symptoms, enhancing balance, strength, mood, sleep and quality of life. However, NHS Trusts, including Derby, lack the resources to deliver lifelong programmes. This project explored whether collaboration between NHS Foundation Trust services and community organisations could embed sustainable, cost-effective Parkinson’s care.
Methods: Participants with Parkinson’s were recruited from NHS and community settings via social media and flyers. Inclusion criteria were independent mobility and cognitive ability to follow instructions. A specialist physiotherapist assessed falls risk and supervised sessions. Parkinson’s UK, the Walking Football Association, the English Football League, and Derby County Community Trust co-funded two programmes: (1) monthly sessions (45-minute warm-up and drills, 30-minute gameplay), and (2) weekly sessions (30-minute warm-up and drills, 30-minute gameplay). Participants completed a service evaluation after 12 months.
Results: 16 participants (median age 65, two female) completed the 12-month programme. All (100%) were “extremely likely” to recommend it. 63% reported noticeable to considerable improvement in physical endurance, 56% in their quality of life and 75% in social wellbeing. No serious adverse events occurred.
Conclusion: A partnership between the NHS and community organisations successfully delivered a safe, inclusive, and cost-effective physical activity programme that improved quality of life for people with Parkinson’s. Future studies should expand and refine this collaborative model.

P45.43
1 Yes, And…eXercise!, United States
Background: Support groups are a vital yet inconsistently integrated part of Parkinson’s disease (PD) care. In 2024, our national survey of 499 participants revealed overwhelming consensus—99 percent of support group leaders (SGLs) and 84 percent of attendees identified emotional and informational support as crucial for living well with PD. Yet only 35 percent reported meaningful engagement from local medical professionals. These findings underscore a critical gap between healthcare and community support.
Objective: To deepen understanding of this gap, Phase 2 of our research expands the investigation to include Health Care Providers (HCPs)— including Movement Disorder Specialists, Neurologists, General Practitioners, Nurses, PTs, OTs, Social Workers and SLPs —to explore how they perceive, recommend, and collaborate with PD support groups. The study aims to triangulate perspectives from SGLs, attendees, and HCPs to identify systemic barriers and actionable strategies for integrating psychosocial support into routine care.
Methods: Phase 1 (2024) combined quantitative surveys and 12 qualitative interviews with SGLs and attendees across the U.S. Phase 2 (2025–2026) will use a mixed-methods design: a concise nationwide HCP survey (pilot Jan 2026; rollout Mar 2026) followed by 15 in-depth interviews with HCPs (June–July 2026). All tools are co-designed with PMD Alliance to ensure clinical and community relevance.
Preliminary Findings: Support group leaders emphasized emotional connection, shared problem-solving, and community validation as defining elements of “support,” while many attendees cited variability in quality and limited referrals from clinicians. Early informal discussions with HCPs suggest divergent beliefs about the efficacy, safety, and structure of support groups, revealing both enthusiasm and hesitation toward formal endorsement.
Conclusions and Next Steps: By uniting patient, leader, and provider perspectives, this two-phase study seeks to redefine “support” in PD care as both clinical and communal. Anticipated outcomes include evidence-based recommendations for provider education, referral pathways, and creative engagement models (e.g., prescriptive wellness) that make support groups accessible, inclusive, and sustainable. Results will be disseminated through PMD Alliance, WPC 2026, and subsequent publications, with the ultimate goal of reframing connection as a core therapeutic intervention for Parkinson’s disease.
P45.44
1 American Parkinson Disease Association, United States
2 Iowa State University, United States
Background: Residents of rural areas experience unique and significant barriers that limit equitable access to Parkinson’s disease (PD) care and support. These include shortages of movement-disorder specialists, limited access to reliable health information, long travel times, internet deserts, and few opportunities to build experiential connections. To address these disparities, the American Parkinson Disease Association (APDA) launched pilot initiatives in Iowa and Missouri, states where 31–40 percent of residents live in rural communities (Unity Point Health, 2019; America’s Health Rankings), to test sustainable outreach models grounded in local partnerships and hybrid delivery.
Objective: To develop, implement, and evaluate long-term rural outreach models that expand access to PD education, strengthen local connections, and integrate APDA programs into existing community systems.
Methods:
Both models were built on trusted local collaborations and prioritized removal of cost and travel barriers. Iowa: A Journey Through Parkinson’s Disease—a three-session education series developed by Iowa State University Extension—was delivered through Iowa’s 99 county offices. The program covers PD causes, symptoms, and treatments, and concludes with a “handoff” to APDA for continued support and services. APDA collaborates with program organizers to ensure participants remain connected to PD-specific resources and community opportunities after completing the series. Missouri: A doctoral capstone project, Educational Outreach to People Living with Parkinson’s Disease in Rural Missouri, conducted a needs assessment identifying key strengths and barriers in rural PD communities. Findings guided partnership development, supporting materials, and a beta-tested program protocol for future implementation.
Results: Both pilots showed high community interest and engagement. Participants valued PD-specific education delivered locally and appreciated learning from familiar community organizations. Early feedback emphasized that trusted partnerships helped overcome stigma, distance, and logistical barriers.
Conclusion: Effective rural outreach requires nuanced, partnership-based approaches that reflect the dynamics of local communities. Building trust, tailoring content geographically and culturally, and sustaining collaboration with local partners and volunteers are key to ensuring equitable access to information, care, and connection for rural families affected by Parkinson’s disease.
P45.45
1 University of Texas Health Science Center at Houston, United States
Background: Community programs organized by nonprofits can fill gaps in care by providing support and resources between clinical visits. They are particularly effective in reaching disadvantaged populations, building trust, and maintaining relationships, serving as a potential tool to reduce disparities in Parkinson’s disease (PD) care.
Methods: We conducted a survey study of adult participants with a confirmed PD diagnosis living in the Houston metropolitan area. Questions explored factors influencing attendance at PD-specific nonprofit programs hosted by Parkinson’s specific nonprofit organizations: logistics, knowledge-related, and cultural aspects. Additionally, participants completed a health-related quality of life assessment (EQ-5D-5L) and Duke Social Support Index – Social Interaction Subscale (DSSI). The target enrollment is 256 participants, with 64 in each racial/ethnic groups: Non-Hispanic (NH) white, NH Black, NH Asian, Hispanic. Enrollment is still ongoing.
Results: Forty-nine participants were recruited, with 28 (57.1%) being male. Twenty-three (46.9%) identify as NH white, 4 as NH black (8.2%), 5 as NH Asian (10.2%), and 17 as Hispanic (34.7%). The median age is 71 years old (SD = 10.1), with a median EQ-5D-5L Index Score of 0.745, median DSSI score of 8, and median H&Y value of 3. Most respondents were retired (67.3%, n=33), with others working (18.4%, n=9) or not working for other reasons (14.3%, n=7). Despite only 19 participants (38.8%) being aware of PD-specific community organizations, 42 (85.7%) expressed interest in attending events. The most desired events were exercise classes (73.5%, n = 36), education events (57.1%, n = 28), and speech classes (55.1%, n = 27). The top motivators of event attendance were convenient location (75.5%, n = 37), mental and physical health benefits (73.5%, n = 36), and ability to bring a loved one (65.3%, n = 32). The main barriers were lack of awareness (81.6%, n = 40), lack of motivation (30.6%, n = 15), and mild symptoms (28.6%, n = 14).
Conclusion: Preliminary findings suggest strong interest in PD-specific community programs. Convenient location, health benefits, and social support are key motivators, whereas lack of awareness remains the primary barrier. Tailoring events to address barriers and capitalize on motivators may improve engagement and help reduce disparities in care for individuals with PD.
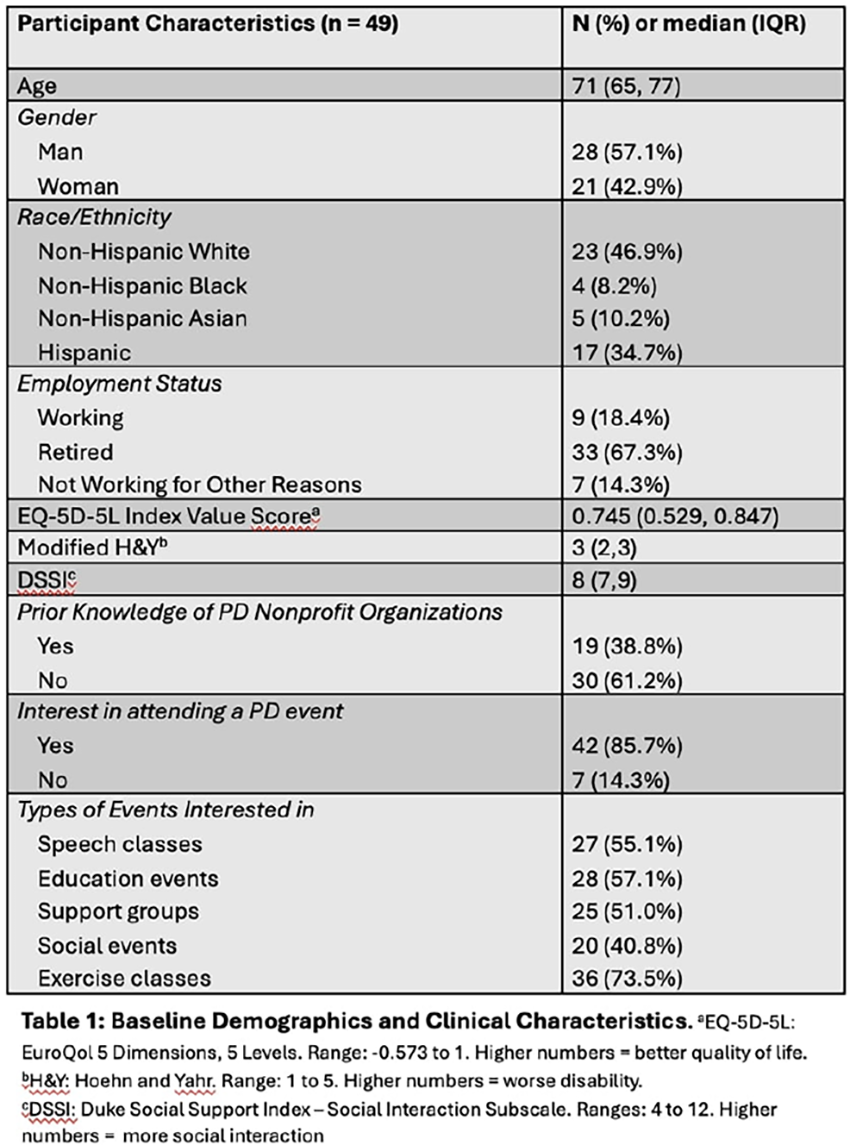
P45.46
1 Arizona State University, United States
2 Barrow Neurological Institute, United States
Background: Exercise has been shown to help improve motor symptoms, such as bradykinesia and tremor, as well as non-motor symptoms, all of which can reduce physical function and quality of life (QoL) in people with Parkinson's Disease (PD). Aim: The aim of this study was to investigate the impact of exercise engagement on physical function and QoL in people with PD longitudinally. Methods: This observational study assessed physical activity, physical function, and QoL over a two-year period (baseline, 3 months, 6 months, 9 months, 1 year, and 2 years) in adults with a physician diagnosis of PD. Physical function and QoL were assessed with three standardized self-report questionnaires: Parkinson's Disease Questionnaire (PDQ-39) is a 39-item questionnaire with 8 dimensions of functioning and well-being, Neuro-QoL Mobility evaluates lower extremity function, and Neuro-QoL Positive Affect assesses an individual's overall sense of purpose. Exercise during the previous 3 months was assessed with a self-report questionnaire that listed 44 exercise activities. For each activity the participant checked, a subsequent question asked the frequency (times/week or times/month). The intensity of each activity, measured in METs (Metabolic Equivalents of Task), was obtained from the 2024 Compendium of Physical Activities for adults (<60 y/o) and older adults (60+ y/o). METs/week was calculated for each participant by multiplying the frequency of each activity by its MET value and then summing all activities. A linear mixed model was used to investigate the impact of exercise (METs/week) on each questionnaire score over 2 years, adjusting for age, sex, and years since PD diagnosis. Results: 73 participants (56.2% men) with a mean (±SD) age of 67.8±8.1 years (range 45-90 years) and diagnosed with PD 8.1±6.9 years earlier are included in the analysis. METs/week averaged 30.1±21.2 at baseline and 29.3±21.7 at 2 years. Scores on the PDQ-39, Neuro-QoL Mobility, and Neuro-QoL Positive Affect averaged 19.6±13.7, 48.9±9.2, and 53.4±8.2 at baseline and 25.0±18.0, 45.2±9.7, and 53.1±8.5 at 2 years, respectively. Higher METs/week had a significant positive effect on Neuro-QoL Mobility (effect 0.02, p = 0.04) and Neuro-QoL Positive Affect (effect 0.03, p = 0.01), but not on PDQ-39 (effect -0.03, p=0.13). Discussion: These results indicate the importance of exercise on physical function and QoL in people with PD.
P45.47
1 Parkinson Wellness Recovery, Tucson AZ USA, United States
Background Anxiety and depression affect up to half of people with Parkinson’s (PwP) and markedly reduce quality of life. Mindfulness-based interventions (MBIs)—including seated meditation, Mindfulness-Based Cognitive Therapy/Stress Reduction (MBCT/MBSR), and mindfulness-informed yoga—are low-risk, scalable options, but their efficacy in PD requires focused synthesis.
Objective To review randomized and controlled studies of mindfulness/meditation in PD with primary outcomes of anxiety and depression, and secondary outcomes of motor function (UPDRS III) and health-related quality of life (HRQOL).
Methods Searches (through 2025) identified RCTs, assessor-blinded trials, and systematic reviews/meta-analyses enrolling adults with PD and evaluating MBIs versus active/attention controls or usual care. We extracted design, sample, intervention components, adherence, and validated outcomes (e.g., HADS, BDI, STAI, PDQ-39, UPDRS III).
Results A large RCT (n=138) found mindfulness yoga reduced anxiety and depressive symptoms and improved HRQOL, with motor outcomes comparable or superior to stretching/resistance exercise. An assessor-blinded RCT of mindfulness meditation similarly improved psychological outcomes and was feasible/acceptable. A 2023 meta-analysis pooling 8 trials (n≈337) reported significant improvements in UPDRS III (MD ∼ −6.3) and cognition, while noting heterogeneity and small samples. Newer work (2025) combining meditation + yoga showed benefits on anxiety, inflammatory markers, motor symptoms, and HRQOL. Adverse events were rare; dropout rates were low to moderate.
Conclusions Mindfulness and meditation show consistent benefits for anxiety/depression in PD, with promising effects on motor function and HRQOL. Given low risk and patient acceptability, MBIs are reasonable adjuncts to standard care for PwP seeking non-pharmacologic supports for mood and daily functioning. Future trials should standardize protocols, include active comparators, and extend follow-up to test durability and mechanism (e.g., stress biology, cognition).
Practical Implications (for Living Well with PD) Offer structured, accessible MBIs (brief group sessions + home practice), screen mood with simple tools, and adapt practices to mobility/energy levels to support sustained engagement. Note that the WPC has a mindfulness/meditation room.
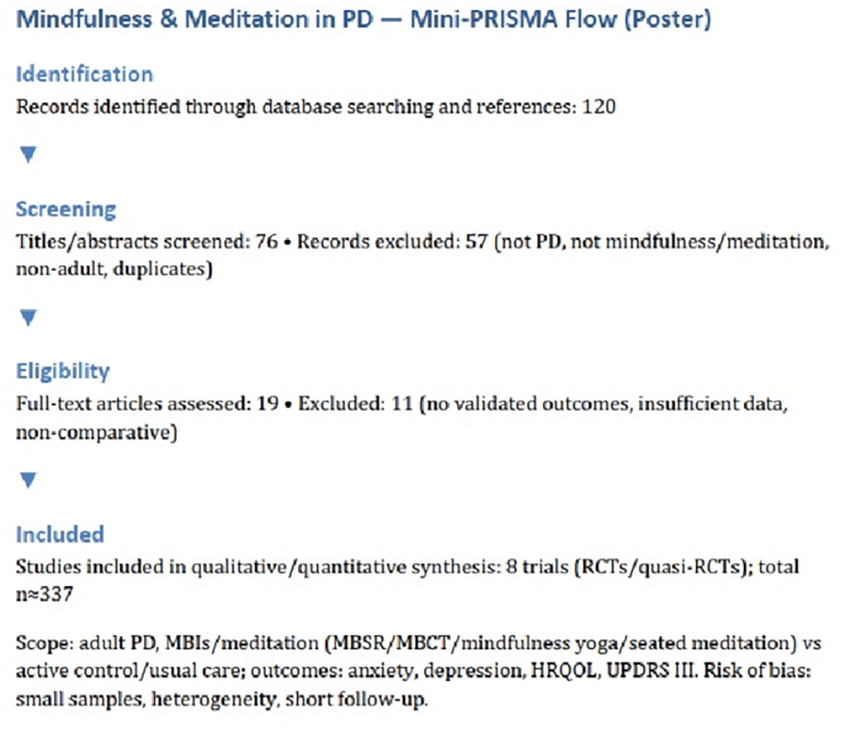
P45.48
1 Kinectic Art, United States
2 Independent, United States
Being creative has been shown to have a positive effect on well-being by promoting a positive sense of self, lowering stress, and developing social relationships. With advances in technology, it is now possible to promote creativity for all stages of life. This presentation introduces a web-based hand-tracking application that encourages intentional creativity by combining reaching movements and hand gestures into interactions with visually striking three-dimensional objects, encouraging sustained aesthetic engagement.
The platform utilizes standard webcam technology to track hand and arm movements in real-time, requiring no specialized equipment beyond a modern web browser and internet access, making technological art accessible and equitable. Users control aesthetically rich 3D objects or real-world experiences like waterfalls and blooming flowers through reaching movements and hand gestures, guiding them toward spatial targets. Upon successful target acquisition, the system provides immediate positive reinforcement through celebratory visual feedback, creating a reward cycle that encourages continued practice. The visual language deliberately diverges from medical aesthetics, instead emphasizing artistic expression and immersive experiences that exist as engaging activities in their own right.
This approach creates the opportunity for common Parkinson's motor symptoms including bradykinesia and diminished fine and gross motor control to transform from everyday challenges into artistic opportunities. Rather than framing movements as "exercises," the platform positions them as creative interactions in which users receive immediate feedback on their ability to move their hands with intended speed and placement. When practicing fine motor skills feels less like treatment and more like an enjoyable, creative experience, adherence increases and practice becomes self-motivated.
The platform is freely accessible via web browser, eliminating financial barriers, the need for specialized hardware or clinical settings, and encouraging sustained social engagement. The tool represents an exploration of how game design principles, aesthetic consideration, and accessible technology can converge to reimagine therapeutic engagement. By prioritizing joy, creativity, and visual beauty, this platform explores how technological advancements can promote well-being and expression for people living with Parkinson's disease.
Platform available at: https://www.kinectic.art/game

P45.49
1 Houston Area Parkinson Society, United States
Mind & Motion is an educational wellness series carried out through Houston Area Parkinson Society (HAPS). Founded in 1974, HAPS is one of the oldest independent Parkinson’s social service organizations in the U.S., offering free, comprehensive support to individuals with Parkinson’s and their families across the eight-county Houston area.
Recognizing that Parkinson’s affects all aspects of life and to reduce fall risk, Mind & Motion's program aimed to improve self-management, quality of life, and balance confidence.
Since Parkinson’s can touch every area of life, HAPS’ comprehensive approach includes therapeutic, social and educational resources tailored to match what Houstonians have told us they want and need. This includes balance education and fall prevention programming. Because people with Parkinson’s are at higher risk for falls, the approach to wellness education needed to be comprehensive to include topics related to balance, movement, thinking, mood, and sleep.
Held weekly at a local church, Mind & Motion included 30 minutes of education followed by 30 minutes of progressive balance exercises, and ending with mindfulness practice. Topics included fall prevention, hand strength, stress management, sleep hygiene, cognitive training, and fatigue. Participants received handouts, home exercise worksheets, and mindfulness guides.
Of the 36 attendees, 23 were individuals with Parkinson’s and 13 were caregivers or family members. On average, 31 participants attended each session. Pre- and post-program surveys, including the Falls Efficacy Scale and PDQ-8, showed that nearly all participants reported improved quality of life and balance confidence.
One month later, 19 participants completed a follow-up survey. Most continued using mindfulness and balance strategies, with 78.94% practicing deep breathing techniques regularly. Two-thirds reported sustained improvements in quality of life.
The program fostered community, sparked friendships, and connected participants to additional HAPS services such as ongoing exercise or support groups. People commented on the enthusiasm of the speaker and teacher making a difference in their interest in attending class, the quality and relatability of the content, quality exercises chosen for the handouts, and music making the classes fun. Due to its success, Mind & Motion has since been replicated, with plans for future expansion.
LIVING WITH PARKINSON'S: Advancing research: collaborations, fundraising, trials, campaigns
P46.01
1 Parkinson Vereniging, Netherlands
2 Radboudumc, Netherlands
Introduction In 2013, the Dutch Parkinson’s Patient Association (Parkinson Vereniging, PV) created a working group of patient researchers (PRs), i.e., people with Parkinson’s and carers who ensure that the patient’s voice is included in research. The group (32 members in 2025) brings diverse backgrounds and is trained to add value from the patient perspective. Their role ranges from assessing study feasibility, relevance, outcomes, clarity of lay summaries, patient information, communication of results, and potential for reuse to implementation. A second mission is to make patient representation in research as self-evident as research itself. The aim of this exploration was to evaluate the PRs’ experiences.
Working procedures of PRs in research When researchers seek involvement, PV assigns two or three PRs. Using a structured role-phase matrix, they clarify mutual expectations and remain engaged throughout the project. The group meets online about 10 times a year and once in person to exchange experiences, present projects, and share best practices, using a standard outline for consistency.
Method All members of the PR-group received a survey, covering demographics and questions about their motivation for being a PR.
Results Requests from researchers have grown in number and scope. On average, PRs became involved in 22 new projects per year, with a steep increase in 2024, when PRs participated in 38 new projects. This increase was partially driven by funding requirements for patient involvement. The group’s role is increasingly recognized; PRs became members of the Dutch Parkinson Scientists network, attended its annual congress, and contributed actively to its program. Principal investigators reported clear benefits: patient-friendly protocols, increased trial participation with less dropout, sharper focus on real-world impact, improved communication to the public, and strengthened researcher motivation. PRs often raised strategic questions about the meaning and future application of findings, influencing both fundamental and applied research directions.
Conclusion In the Netherlands, the Parkinson’s community’s voice is now firmly present in research—valued for its practical, human, and strategic contributions. The PV working group will continue to enhance its processes and share its model internationally, supporting the principle: Nothing about us without us.
P46.02
1 Northeast Ohio Medical University, United States
In 2004, neurologist Dr. Stanley Fahn and educator Eli Pollard launched a bold experiment: a global Parkinson’s congress where patients, care partners, clinicians, scientists, therapists, advocates, and industry leaders would learn together as equals. At the time, Parkinson’s organizations often competed rather than collaborated. Dr. Fahn, respected worldwide, believed the field needed unity but knew entrenched egos and silos would resist. He chose Pollard, an advocate with no medical background but exceptional skill in building bridges, to design something new.
The first World Parkinson Congress (WPC) convened in Washington, D.C., 2006. For the first time, people living with Parkinson’s sat beside researchers and physicians, asked questions, and co-moderated sessions. The event was transformative and sometimes uncomfortable; a public confrontation over a terminated clinical trial revealed the need for transparency and partnership. Fahn and Pollard viewed that tension as proof of concept: progress demanded shared truth.
By Glasgow 2010, people with Parkinson’s were helping plan sessions, shape agendas, and guide research priorities. Each Congress deepened that integration. Younger clinicians returned to their institutions seeing patients as collaborators, not subjects. Rehabilitation professionals and social scientists, once peripheral to neurology meetings, found a home at WPC. This “interdigitation,” Fahn’s term for weaving disciplines and lived experience, became the Congress’s hallmark.
Over two decades the WPC model has inspired global initiatives: PD Avengers, Parkinson’s Africa, and long-distance awareness rides such as Biking to Barcelona (2023) and Pedal to Phoenix (2026). Its informal culture, speakers staying to lead workshops and share coffee with attendees, became the secret sauce that sustains collaboration long after each meeting ends.
Today the WPC draws thousands from more than 60 countries, blending science, creativity, and human connection. Dr. Fahn’s vision and Pollard’s leadership proved that inclusion is not a risk but a catalyst. The WPC Effect shows that when every voice is valued, walls fall, innovation accelerates, and hope expands. What began as an experiment endures as a movement.
P46.03
1 University College London, United Kingdom
2 Expert by Experience, United Kingdom
3 Newcastle University, United Kingdom
Introduction: The Edmond J. Safra Accelerating Clinical Trials in Parkinson’s Disease (EJS ACT-PD) Initiative has designed a multi-arm, multi-stage (MAMS) clinical trial to test treatments that may slow or stop PD progression. From the outset, people with Parkinson’s (PwP) and carers /partners (CPs) have been central to shaping the protocol, ensuring the trial is acceptable, meaningful, and a positive participation experience for PwP. As the project has expanded from trial design to trial delivery, the scope of patient and public involvement and engagement (PPIE) has also grown.
Methods: PwP and CPs form the dedicated PPIE Working Group, supported by trial delivery and patient engagement professionals. Two to three PPIE representatives also sit on every initiative Working Group (WG) and trial Study Management Group (SMG), providing input on trial innovation, treatment selection, funding and commercialisation, digital measures, biosample collection, recruitment and retention, and communications. Structured processes support PPIE input across the project: every WG meeting includes a standing agenda item for PPIE feedback; debrief sessions are held with WG chairs; and a standard reporting form documents PPIE input and responses. New PPIE members are recruited as needed, through national calls supported by Cure Parkinson’s and Parkinson’s UK, bringing fresh perspectives. A Community Advisory Panel (CAP) provides insight on accessibility, inclusivity and underserved groups, while a wider PPIE network offers rapid additional input when required.
Results: This integrated approach has had a major impact on design and delivery of the EJS ACT-PD trial. Co-produced decisions include offering participants options of either in-person or remote visits based on preference; trial medication delivered directly to participants’ homes; a maximum participation period of three years for participants; use of digital devices trial and tested by the PPIE WG; and the use of participant-reported questionnaires to evaluate whether the trial treatments are working. PPIE members have also co-drafted participant documents, including information sheets, recruitment materials, and feedback questionnaires.
Conclusions: PwP and CPs are active partners in the process of shaping the trial and considering real-world constraints on trial design. They continue to play a significant role in managing how the trial is delivered and in developing future objectives.
P46.04
1 Public contributor, United Kingdom
2 Northumbria University, United Kingdom
3 University of Southampton, United Kingdom
4 Newcastle upon Tyne Hospital NHS Foundation Trust and Northumbria University, United Kingdom
What attracted me to the project
The iSupport-PD study involves adapting and developing a digital intervention for Care partners (CP) of people with Parkinson’s (PWP) with cognitive changes. Successful outcomes could offer flexible, accessible support to CPs through the often unexpected, complex and evolving journey. The premise of iSupport-PD is close to my heart as a CP to a PWP and in my professional background in education and digital delivery. I know digital resources can empower individuals to learn at the pace and structure that suits them, rather than enforced linear learning.
My previous experience I am keen to participate in research that improves quality of life or leads to better interventions and have taken part in numerous clinical studies. My partner was diagnosed with Early Onset Parkinson’s in 2008 aged 51; my CP experience is long-standing and deeply personal. I volunteer with Parkinson’s UK (PUK) and chair a large PUK branch.
My involvement in iSupport-PD
I was invited to join the iSupport-PD Patient and Public Involvement and Engagement (PPIE) team and later undertook the role of the PPIE lead. I was keen to join as I recognised that cognitive changes have a huge impact on the CP. I wanted to use my lived experience (LE) to help shape the research that could genuinely support others.
Contributions as a PPIE team member
Evaluated the original iSupport Dementia digital intervention and identified changes needed for Parkinson’s CP Developed study documents e.g. participant information sheets, study adverts, questionnaires and advised on recruitment strategy Participated in Think Aloud interviews, sharing insights based on my experience and as a PUK volunteer Evaluated ongoing developments for intervention usability, accessibility, and practical relevance
Attend PPIE and full team meetings
Contributions as PPIE lead Attend and contribute to monthly research team meetings Facilitate communication with the PPIE team Visited PUK support groups and research events to promote recruitment and provide a LE voice to show the real-world relevance of the project
Reflections on my involvement I now have a deeper understanding of the structure, demands and rigour of the research process. I feel genuine respect from the research team for the experience and knowledge I bring as a contributor with LE and through my professional background. I plan to remain with the team as the research develops and continue contributing to this vital area of work.
P46.05
1 UCB, Brussels, Belgium
2 UCB, Raleigh, North Carolina, United States
3 CARLDEN Inc., Bethesda, Maryland, United States
4 The Ken and Ruth Davee Department of Neurology, Northwestern University, Chicago, Illinois, United States
5 Community Advocate, Charlotte, North Carolina, United States
6 Community Advocate and Educator for Parkinson’s Disease, Loughborough, United Kingdom
7 The Michael J. Fox Foundation for Parkinson’s Research, New York, United States
8 Parkinson’s Foundation, New York, United States
9 Parkinson’s UK, London, United Kingdom
Introduction: Engaging often underrepresented communities in clinical research can enhance recruitment, retention and representation of real-world diversity in clinical studies. In 2025, UCB launched the Parkinson’s Health Equity Research and Development (R&D) Community Leaders Board, bringing together US and UK physicians, community advocates, patient advocacy groups, people with Parkinson’s (PwP) and care partners who partnered with UCB to design strategies to support more inclusive studies.
Methods: The 13-member Board collaborated to identify barriers and recommend actionable solutions to address diversity in Parkinson’s disease studies. Over four structured meetings, members aligned on priority topics where UCB could drive meaningful change and recommended implementable strategies for these. The final session consolidated insights and outlined next steps for sustained impact.
Results: Following a rigorous prioritization process, two critical topics emerged: 1) How might UCB design more inclusive studies? 2) How might UCB increase knowledge of R&D and clinical trials among partner populations? Efforts were focused on supporting PwP from Black, African, Caribbean, Hispanic (US) and Indian and Pakistani (UK) communities, with potential to impact broader communities. Topic 1 solutions: training community leaders to gather actionable insights on study designs; community listening sessions to gather PwP/care partner input on study designs; co-designing studies with a specific community to build trust, upskill and gather true-to-life insights. Topic 2 solutions: community-developed short videos, addressing knowledge gaps and highlighting clinical study benefits; longer video content to engage through storytelling; establishing a community-focused delegation to attend and present at national/international Parkinson’s events. Selected solutions are under discussion with UCB’s Parkinson’s teams to build trust and motivate community engagement with upcoming clinical studies.
Conclusion: The Board united 13 influential and diverse voices from the Parkinson’s community to recommend community-driven, patient-centric solutions to enhance awareness, recruitment, retention and representation in UCB clinical studies. Board feedback has been very positive, with ongoing collaboration to implement select solutions. UCB is exploring how these practices could be applied to other therapy areas, recognizing that increased inclusion ultimately improves outcomes for all patients.
P46.06
1 Cure Parkinsons's, United Kingdom
Introduction/Goals Cure Parkinson’s (CP) is a medical research charity dedicated to funding projects that aim to slow, stop, or reverse the progression of Parkinson’s. To achieve this, CP funds preclinical and clinical research focused on disease modification in Parkinson’s, aiming to identify and support the most promising treatments. Applications are evaluated four times a year by an independent committee of research scientists, clinicians, regulatory experts, and people with Parkinson’s (PwPs).
In 2023, we launched a new initiative, the Research Committee Internship Programme, involving early career researchers (ECRs) in the research funding process. The goal is to provide ECRs with first-hand experience of how funding decisions are made, building their skills and confidence for future careers in Parkinson’s research.
Methods: Annually, ECRs involved with preclinical or clinical Parkinson’s research are invited to apply for a one-year, voluntary internship on CPs Research Committee. Successful applicants attend the committee meetings and are actively involved in presenting and reviewing funding proposals, contributing to discussions, and observing how funding decisions are reached. The interns gain valuable mentorship from experienced committee members and experts in the Parkinson’s field.
Results Since its launch, the internship has supported five ECRs from four different UK institutions. Feedback has highlighted the value of the experience in shaping career development and providing a deeper understanding of what makes a strong research proposal. The interns reported increased understanding of funding processes, including understanding how funding priorities are set, stronger research design skills, the importance of scientific rationale and meaningful patient and public involvement in research, and greater confidence in applying for their own grants in the future.
Conclusions: This programme fosters networking opportunities, supporting ECRs in developing connections within the Parkinson’s research community. By investing in ECRs through this unique initiative, CP supports the development of future leaders in Parkinson’s research, ensuring they are better equipped to design impactful studies to meet the needs of funders, clinicians, and PwPs. The programme also helps develop a more connected, collaborative research community, accelerating progress towards a cure for Parkinson’s.
P46.07
1 Egyparkinson's Rescource center, Egypt
2 Egyparkinson's, Egypt
3 Egyarkinson's, Egypt
Background: Parkinson’s disease (PD) is a progressive neurodegenerative disorder that presents increasing challenges in Africa, where healthcare systems are often constrained by limited resources and insufficient awareness. In Egypt, the absence of dedicated support structures for patients and caregivers created ,unequal access for care which is a significant gap in comprehensive care and advocacy.
Objective: This abstract aims to present the establishment and development Egyparkinson’s , the first and only Parkinson’s disease support group in Egypt, and to highlight its role in awareness, patient care, and research within a resource-limited African context.
Methods: EgyParkinson’s was established in 2023 with the mission and vision of empowering patient and caregivers, stigma reduction ,equal access to medication and care through multidisciplinary team and advocacy. Activities included: (1) collaborations with rehabilitation centers across Egypt to expand access to therapy services; (2) partnerships with sponsors for medication coverage; (3) organization of nationwide awareness campaigns targeting both healthcare professionals and the public; (4) the formation of a Research Committee to address unmet scientific questions related to Parkinson’s disease; and (5)Egyparkinson’s EgyParkinson’s Game Development Committee developed the Shake It Up and DopaDash game as an interactive awareness game that guides players through the journey of Parkinson’s disease, introducing the key characters who support the patient including the physician, physiotherapist, nutritionist, researcher, and caregiver. DopaDash transforms awareness into action as a therapeutic rehabilitation game designed to enhance movement, cognition, speech, and emotional wellbeing. Using a dynamic spinner and evidence-based challenge cards, DopaDash can be played individually or in group therapy sessions, encouraging cooperation, laughter, and motivation.
Results: EgyParkinson’s has successfully implemented nationwide awareness campaigns, built trust with partners to ensure holistic care for the patients and caregivers, and facilitated access to medications that’s one of the parkinson’s patients challenges across Egypt.
Conclusion: Supporting groups in limited rescources countries have critical role of patient and caregivers by combining awarenessand advocacy, acess to care, medical support and research, the initiative provides a replicable model for improving outcomes in Parkinson’s across the region.

P46.09
1 Cure Parkinson's, United Kingdom
2 Highway Pharmaceuticals, United States
3 University College London, United Kingdom
4 University of Sheffield, United Kingdom
Introduction: To date, clinical trials of treatments aimed at modifying the progression of Parkinson’s disease (PD) have largely focused on monotherapy approaches. However, PD is a complex condition with different biological pathways potentially at play, meaning in order to observe an impact on clinical progression, a synergistic interplay between multiple agents may be required.
The medical research charity Cure Parkinson’s (CP) is interested in exploring combination therapies and their potential for disease modification in PD. Alongside this, we are keen to encourage researchers to consider combination therapies earlier in the drug discovery process.
Methods: In June 2025, CP convened a workshop to discuss the key considerations needed to develop and test rationally designed combination therapies to slow the progression of PD. The meeting involved individuals with a range of research-related expertise, as well as people living with the condition. Attendees of the workshop evaluated case studies from other disease indications, discussing recent examples of successful combinations to understand how they were developed before moving on to discuss requirements for designing combination therapies specifically for PD.
Results: By considering the recent approval of Auvelity, a combination of dextromethorphan and bupropion for the treatment of major depressive disorder, it was clear that understanding the mechanism by which combinations of agents are producing a synergistic effect is paramount. Following discussions to examine the intellectual property and regulatory implications, attendees began to suggest an initial framework that could be used to implement a combinatorial approach in PD. Outcomes included mentorship of early career researchers and the inclusion of questions in grant applications to provoke applicants to consider possible combinations, as well as designing specific funding calls.
As a result, CP launched a £2 million funding call, inviting clinical and preclinical applications from around the globe to test rationally designed combination therapies in PD.
Conclusion: Combination therapies represent an, as yet, unexplored avenue for disease modification in PD. Through understanding the different biological pathways involved in the condition and learning how to successfully develop a combination therapy from other disease indications, it is hoped that combination therapies could accelerate the quest to find a cure for Parkinson’s.
P46.10
1 UCB, United Kingdom
2 UCB, Belgium
3 Adelphi Values Patient-Centered Outcomes, United Kingdom
4 Parkinson’s Europe, United Kingdom
5 Parkinson’s Foundation, United States
6 Lund University and Skåne University Hospital, Sweden
7 University of Padua, Italy
Introduction Incorporating the patient voice in drug development is key to ensuring clinical studies use appropriate tools to assess outcomes that are important to patients and reflect their lived experience. To identify the most relevant concepts to measure in future Parkinson’s disease (PD) trials, a qualitative interview study was conducted with people with Parkinson’s (PwP), caregivers, and clinicians. A steering committee was formed to foster active, meaningful patient engagement and obtain expertise at key points in the study.
Methods The steering committee included four expert clinicians experienced in managing and treating PwP, two patient experts, and a patient advocacy group representative. Members shared written input on the study design, eligibility criteria, study documents, interpretation of interview findings, and refinement of a conceptual model depicting the lived experience of PD. The committee also took part in meetings to discuss collated feedback and reach consensus on actions.
Results Feedback on the study documents highlighted restrictive eligibility criteria (e.g., requiring a Hoehn and Yahr stage), complex participant-facing language (e.g., informed consent form content), unclear wording (e.g., interview guide questions), and concerns about participant recall, burden, and sensitive topic handling. Eligibility criteria were revised to improve inclusivity and alignment with study aims, and study documents were updated to improve clarity and accessibility. The committee advised on symptom prioritization, expected and unexpected findings (e.g., frequency of reporting for selected symptoms), and possible explanations for the interview findings, and highlighted comparisons with existing research and study limitations. Input on the conceptual model led to more patient-friendly wording, and the addition, removal, merging, and reclassification of symptoms. Learnings were identified to enhance steering committee involvement in future qualitative studies.
Conclusion Steering committee insights strengthened the study design and materials, interpretation of findings, and relevance of the conceptual model. Their contributions supported a deeper understanding of the lived experience of PwP. Findings will inform the development of a patient-centered strategy for measuring meaningful outcomes in PD trials. Future PD research should embed early community engagement with clear timelines, roles, and feedback mechanisms to optimize meaningful contributions.
P46.11
1 Patient/caregiver author, United States
2 Davis Phinney Foundation, United States
3 SIG - Black Diaspora, United States
Introduction: People living with Parkinson’s experience multiple visible and invisible symptoms that impact daily life and worsen over time. Although no cure exists, hope remains for a PD treatment to slow or prevent disease progression. One promising treatment is glial cell line-derived neurotrophic factor (GDNF) that can be delivered directly to the brain via gene therapy. GDNF gene therapy has potential to promote the survival of dopamine-producing brain cells critical for movement and coordination. Here, in patient-friendly language, we present outcomes from an early-stage study of AB-1005 (GDNF gene therapy) for PD and communicate patient/caregiver experiences of living with PD. These results are important and must be made accessible to our community.
Methods: In this early-stage study, participants with mild or moderate PD (grouped based on time since diagnosis and motor [movement] exam scores) received AB-1005 during a 1-time neurosurgical procedure. The study was primarily performed to assess side effects over 18 months; numerical changes in motor and nonmotor assessments after AB-1005 treatment were also analyzed. Additionally, patients/caregivers shared their experiences of PD symptoms and impact on daily life, along with their hopes and expectations for future treatments.
Results: 11 participants with PD (6 mild, 5 moderate) were treated only with AB-1005. Side effects were observed <30 and ≥30 days after AB-1005 treatment; >35% were temporary and did not interfere with daily activities. No side effects were related to AB-1005 treatment. In participants with moderate PD, motor scores improved by up to 49%, and increased time with no/nontroublesome dyskinesia was observed. Motor scores were stable in participants with mild PD, and nonmotor scores were stable in both groups. PD medication use was reduced by 27% in the moderate PD group. According to patients/caregivers, the most difficult PD symptoms were tremors, mood-related symptoms, and sleep disruption; unpredictability and inability to work or be spontaneous were the biggest limitations of PD.
Conclusion: Efforts to understand the burden of PD on patients/caregivers are crucial for advancing and communicating clinical research and treatment. Results from this study suggest that AB-1005 is well-tolerated and may benefit people with mild to moderate disease by preventing disease progression and reducing existing medication burden.
Published in: Van Laar AD, et al. Mov Disord. 2025;40:1297–1306.
P46.12
1 Amprion Diagnostics, United States
When my husband Jeff began showing uncharacteristic behaviors in his early 60s -- impulsive spending, obsessive behaviors , and severe depression -- we entered what I now call the “diagnostic odyssey.” Over the next several years, world-class neurologists and cutting-edge biomarker tests offered conflicting answers from Lewy body disease to corticobasal syndrome to frontotemporal lobar dementia. Only after Jeff’s passing did his autopsy reveal the truth: corticobasal degeneration with no Lewy body or Alzheimer’s pathology.
This presentation will explore what our story reveals about the real-world complexity of diagnosis in Parkinson’s and related disorders, and how we can build a smarter, more compassionate diagnostic ecosystem. As both a nurse and a caregiver, I witnessed firsthand how overlapping symptoms, evolving biomarker science, and conflicting data can delay accurate diagnosis and access to appropriate trials. Yet I also saw how caregiver insight, which is consistent, longitudinal, and deeply human, can serve as a vital piece of clinical evidence.
By reflecting on Jeff’s journey, I aim to spotlight systemic gaps and propose a collaborative model where caregivers, clinicians, and researchers share data and decision-making. I’ll discuss how false-positive biomarkers can distort research enrollment, why autopsy validation must be linked to trials, and how integrating caregiver-reported outcomes into real-world data can strengthen diagnostic accuracy.
Ultimately, Jeff’s story isn’t about loss, it’s about learning. His life and autopsy now inform ongoing global discussions about biomarker validation and trial design. By reframing the diagnostic odyssey through lived experience, we can shorten the path to answers for future families and ensure that every patient enrolled in a study truly helps advance the science and fight against these devastating diseases.
P46.13
1 BIAL Portela Ca, Portugal
2 Laboratory of Clinical Pharmacology and Therapeutics, Faculdade de Medicina, Universidade Lisboa, Lisbon, Portugal; CNS-Campus Neurológico, Torres Vedras, Portugal, Portugal
3 Department of Neurology, ULS Alto Ave, Hospital da Senhora da Oliveira, 4835-044 Guimarães, Portugal; Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal; CNS - Campus Neurológico, 4710-452 Braga, Portugal, Portugal
4 BIAL – Portela & Ca S.A., Coronado, Portugal, Portugal
5 BIAL - R&D Investments, S.A. Coronado, Portugal, Portugal
6 BIAL – Portela & Ca S.A., Coronado, Portuga, Portugal
7 Paracelsus-Elena Klinik, Kassel, Germany; Deptartment of Neurosurgery, University Medical Center, Goettingen, Germany, Germany
Background: Sleep disturbances and NMS are common and challenging to manage in people living with PD (PwPD). By optimizing levodopa, the catechol-O-methyl transferase inhibitor OPC may alleviate specific PD-related sleep issues and NMS burden in PwPD and motor fluctuations.
Objective: To assess the effect of opicapone (OPC) on different sleep complaints and non-motor symptoms (NMS) in fluctuating PwPD with sleep disturbances.
Methods: The 6-week, open-label, single-arm OpicApone in Sleep dISorder (OASIS) trial evaluated the efficacy of OPC 50 mg in treating sleep disturbances as levodopa add-on therapy. Primary endpoint was change from baseline to Week 6 in PD Sleep Scale-2 (PDSS-2) total score. This post-hoc analysis evaluated changes in specific PDSS-2 items and Movement Disorder Society-sponsored NMS rating scale (MDS-NMS) domains at Week 6.
Results: Of the 16 PwPD included, 15 completed the treatment. At Week 6, patients experienced improvements in several sleep issues, as indicated by the mean (standard error [SE]) reductions in the scores for poor sleep quality in the previous week (-1.1 [0.3]; -42%), sleep latency (-0.9 [0.4]; -50%), sleep fragmentation (-1.3 [0.4]; -39%), and non-restorative sleep (-1 [0.3]; -41%) (Figure 1a). Participants also reported significantly less difficulty moving or turning in bed (-0.9 [0.3]; -35%) and significantly less tremor upon waking (-0.7 [0.3]; -39%) (Figure 1a). The mean (SE) MDS-NMS score significantly decreased by -28.9 (7.3; p=0.0015), with a -6.4 (2.6; -31%; p=0.025) point reduction in the sleep/wakefulness domain (Table 1), reflecting improvements in insomnia (-2.8 [1.1]; -43%; p=0.03) and unintentional daytime sleep episodes (-2.2 [0.8]; -41%, p=0.02) (Figure1b). Reductions were seen across other MDS-NMS domains, including depression (-27%), anxiety (-35%), apathy (-31%), gastrointestinal (-27%), and pain (-26%).
Conclusions: Add-on OPC improved sleep-related symptoms by >30%, including insomnia and restorative sleep, while alleviating nighttime and morning motor symptoms. It significantly reduced NMS burden, particularly sleep disturbances and daytime sleepiness, indicating its potential to address both motor and non-motor challenges in people living with fluctuating-PD, sleep-related disturbances and high NMS burden.
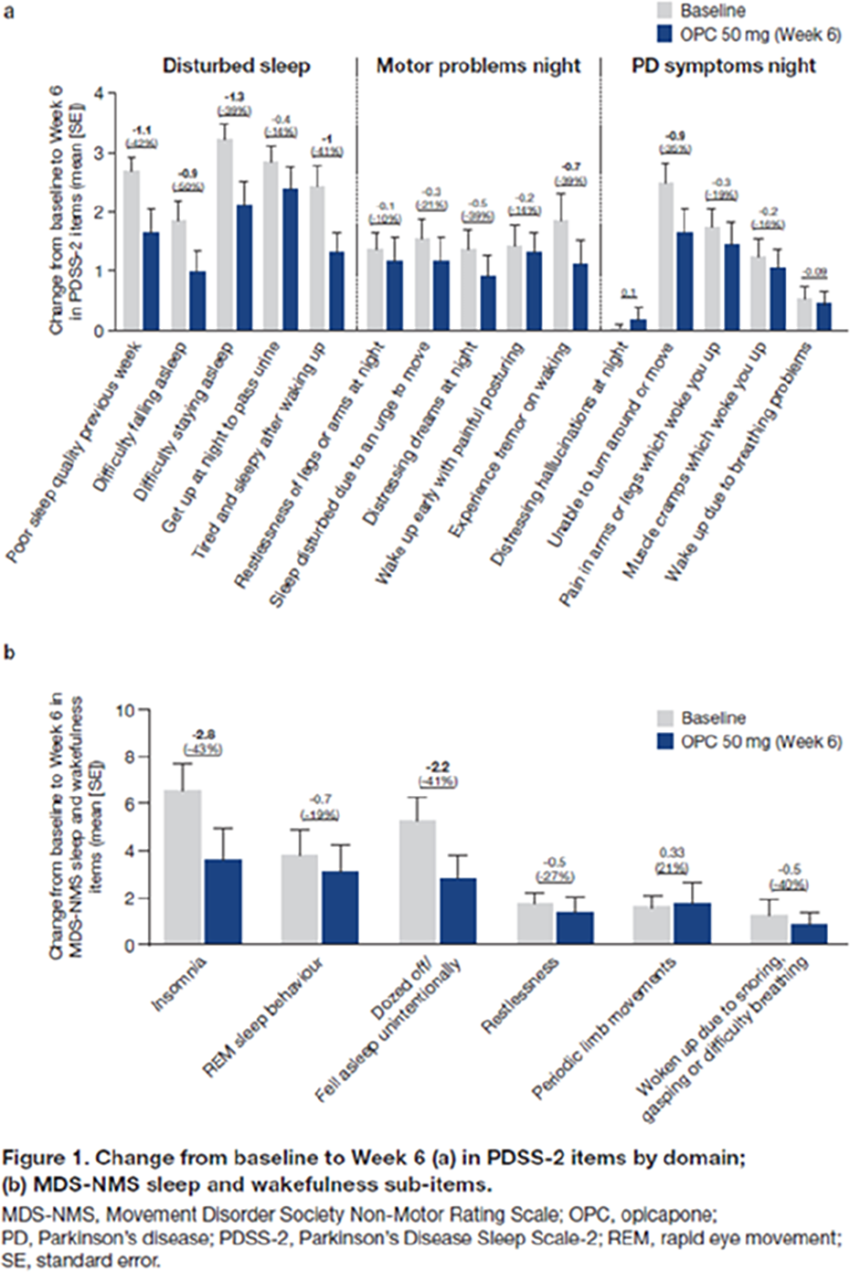
P46.14
1 Critical Path Institute, United States
2 Parkinson's Research Advocate, United Kingdom
3 Parkinson's Research Advocate, France
4 Parkinson's Research Advocate, United States
5 Parkinson's Research Advocate, Canada
6 Parkinson's Canada, Canada
7 The Michael J. Fox Foundation, United States
8 Parkinson's Europe, United Kingdom
9 Parkinson's UK, United Kingdom
10 Cure Parkinson's, United Kingdom
11 Parkinson's Foundation, United States
12 Stanford University, United States
13 Perceptive, Inc., United States
Introduction: Neuroimaging is an important aspect of Parkinson’s disease (PD) clinical trials. It can be used to enrich the trial, to monitor brain changes over time, and to monitor any changes in the brain related to the investigational drug. Imaging, however, can also impose a burden on participation in clinical trials for people living with PD (PwP). Recognition of this burden by providing ease, comfort, and education is paramount.
Methods: The Critical Path for Parkinson’s Consortium (CPP) is a not-for-profit public-private-partnership under the auspices of the Critical Path Institute. The consortium brings together relevant stakeholders to develop solutions for facilitating the drug development process. CPP’s Advisory Council brings together PwP, care partners, and patient advocacy organizations with the purpose of understanding the unique issues associated with participation in clinical trials from the lived experience perspective. CPP’s Advisory Council convened to review the need for participation in neuroimaging studies and to discuss the challenges.
Results: While there was general recognition around the importance of imaging, concerns were expressed regarding long duration of the procedures, possible radiation exposure, discomfort and pain, and claustrophobia. Sharing the imaging results with participants and guidance on how to interpret clinical findings were found to be an important aspect of participation. PwP also stressed the need for a strong human touch in imaging, with clinicians demonstrating empathy and respect throughout.
Conclusions: Providing extensive information on the imaging procedures that recognizes that real people are involved is critical to the informed consent process. Educational materials that have been developed by patient advocacy organizations may help with preparation for these procedures. Collaboration between PwP, patient advocacy organizations, pharmaceutical industry, and CPP may provide the necessary understanding for the informed participation in neuroimaging studies in clinical trials.
P46.15
1 Roche Pharma Research and Early Development (pRED), Roche Innovation Center, F. Hoffmann-La Roche Ltd, Basel, Switzerland
2 RADIORG, Belgium; EUPATI Fellow, Belgium
3 Parkinson's UK, United Kingdom
4 Parkinson's UK, United Kingdom; Parkinson's Europe, United Kingdom
5 Shake It Up Australia, Australia
6 Special Interests Group (SIG) Black Diaspora, Morgan Hill, CA, United States
7 Davis Phinney Foundation, United States
8 Parkinson's Europe, United Kingdom
9 EUPATI Fellow, Netherlands; My Moves Matter, Ireland
10 American Parkinson Disease Association, United States
11 Parkinson's Research Foundation, Australia
12 Michael J Fox Foundation, United States
13 F. Hoffmann-La Roche, Switzerland
14 Cure Parkinsons, United Kingdom
15 The Michael J. Fox Foundation for Parkinson’s Research, United States, United States
16 YUVEDO Foundation, Germany
17 Patient and Public Involvement Contributor, United States
Introduction Meaningful innovation in Parkinson’s disease (PD) requires that the perspectives and priorities of people with Parkinson’s (PwP) are integrated throughout medicines and diagnostics development. Traditional drug development has often underrepresented the lived experience of patients and their community, resulting in outcomes that may not fully reflect what matters most to the community. At Roche, we have developed a structured, multimethodology approach to ensure that the voices of PwP inform not only individual studies and products, but also our overarching strategy in Parkinson’s disease and neurology.
Methods We engage PwP and the broader community through multiple complementary channels. These include: a product-agnostic Global Advisory Council and product-specific advisory boards; 1:1 consultations with PwP, care partners, and community leaders; and qualitative and quantitative market research via interviews, focus groups, and surveys. Additionally, social media listening is used to identify emerging topics of relevance across geographies and cultures. Depending on the decision context, we select the most appropriate engagement method and participants—for example, individuals with direct lived experience, care partners, or those with specific expertise in research, healthcare systems, or advocacy. Insights gained through indirect methods are validated via direct engagement to ensure accuracy and representativeness.
Results This multimethod approach has enabled Roche to incorporate PwP perspectives into diverse aspects of PD research and strategy, including patient and caregiver journeys, study design and burden, inclusivity, meaningful outcomes, communication of study materials and results, and identification of educational and healthcare system gaps; examples will be presented. Our Global Advisory Council operates as a two-way exchange, allowing members to bring forward their own topics and priorities, fostering a collaborative partnership model that enhances trust and relevance.
Conclusion Embedding the voice of PwP and the community across the research continuum strengthens the scientific and ethical foundation of PD drug development. By using context-driven, multimethod engagement and validating insights through direct dialogue, Roche ensures that our efforts address what truly matters to PwP, care partners, and the community. This participatory model offers a replicable framework for meaningful patient involvement across therapeutic areas.
P46.16
1 Critical Path Institute, United States
2 Parkinson’s Research Advocate, United States
OBJECTIVE: To highlight the development and impact of the CPP Integrated Database, a global resource supporting new drug development tools that aim to improve clinical trials and, ultimately, the lives of people with Parkinson’s disease (PD).
BACKGROUND: CPP is a precompetitive consortium led by the Critical Path Institute (C-Path) and brings together industry members, regulatory agencies, academic experts, nonprofit organizations, and people with lived experience. CPP’s mission is to close critical gaps in the development of PD treatments through data-driven strategies that have been reviewed by regulators worldwide. For people with PD, this means a faster path to more effective treatments and trials designed with real-world needs in mind.
METHODS: CPP has established a patient-level item-level database by applying specific data standards to harmonize data across multiple sources of data from across the world. This includes six observational cohorts from the US, Europe, and Japan, and 17 clinical trials.
RESULTS: Several examples will be highlighted, showing how the CPP Integrated Parkinson’s Database is being leveraged to advance our understanding of PD in research across the globe. C-Path’s core competencies in data are unique in their ability to acquire data from diverse sources across geographically diverse populations. In the ten years since its launch, CPP has: 1) Achieved regulatory acceptance of the use of Dopamine Transporter neuroimaging as an enrichment biomarker for early-stage PD trials; 2) Engaged FDA and EMA in regulatory review of a model of disease progression; and 3) Advanced digital health technologies to improve detection of disease onset and progression. This integration created a single, standardized resource containing data from more than 16,000 participants worldwide, representing one of the largest PD research datasets available.
CONCLUSIONS: The CPP Integrated Parkinson’s Database represents a unique resource for improving our understanding of PD. New research findings are emerging from the use of this database and the development of tools to improve clinical trials, such as biomarkers, progression models, patient-centered endpoints, and trial simulations. For people living with PD, this means better-designed trials, more sensitive tools to track progression, and a stronger chance of getting effective therapies sooner.
P46.17
1 Critical Path Institute - Critical Path for Parkinson's Consortium, United States
2 Parkinson's Canada, Canada
3 Cure Parkinson's, United Kingdom
4 Parkinson's UK, United Kingdom
5 Patient Research Advocate, Critical Path for Parkinson's Consortium Advisory Council Member, United Kingdom
6 The Michael J. Fox Foundation, United States
7 Patient Research Advocate, Critical Path for Parkinson's Consortium Advisory Council Member, Ireland
8 Patient Research Advocate, Critical Path for Parkinson's Consortium Advisory Council Member, France
9 Parkinson's Foundation, United States
10 Patient Research Advocate, Critical Path for Parkinson's Consortium Advisory Council Member, United States
11 Patient Research Advocate, Critical Path for Parkinson's Consortium Advisory Council Member, Canada
Objectives People living with Parkinson’s disease (PwPD) and their care partners provide essential insight into managing symptoms and progression. In October 2023, the Critical Path for Parkinson’s (CPP) Consortium, a public–private partnership sponsored by the Critical Path Institute, Parkinson’s UK, and industry members, launched its Patient Advisory Council to ensure the patient voice directly shapes development of meaningful drug development tools, in alignment with the U.S. Food and Drug Administration’s (FDA) guidance.
Methods CPP partnered with six non-profits: The Michael J. Fox Foundation, Cure Parkinson’s, Parkinson’s Foundation, Parkinson Canada, Parkinson’s Europe, and Parkinson’s UK, to co-develop a recruitment strategy prioritizing diversity in, disease stage, motor symptoms, and caregiving roles. Eleven members from the U.S., Canada, Europe, and the U.K. volunteered to participate, representing PwPD at different stages of disease and care partners. The council meets quarterly to provide structured, lived-experience feedback on defining gaps and research priorities for drug development.
Results The Advisory Council has discussed key topics including cognition, imaging, biological staging, and clinical trial endpoints. Their perspectives have been integrated into discussions with CPP’s multi-sector partnerships, ensuring that drug development reflects what is most meaningful to patients.
Conclusions CPP’s PD Patient Advisory Council offers a structured forum for embedding lived experience into the drug development process. By providing input the council is contributing valuable insights for the development of tool meaningful to PwPD and care partners, while highlighting some of the gaps and barriers to participation in clinical trials. Guided by FDA’s emphasis on patient-focused drug development, the council’s contributions are helping lay the foundation to optimize clinical trials that better reflect the priorities of the Parkinson’s community.
P46.18
1 Parkinson's Foundation, United States
2 Genomic Medicine Institute, Cleveland Clinic., United States
3 Indiana University School of Medicine, United States
4 Columbia University, United States
5 Genomic Medicine Institute, Cleveland Clinic, United States
6 Parkinson’s Foundation, United States
Background: Hispanic and Latin American populations have been historically underrepresented in Parkinson’s disease (PD) genetic research, limiting diversity and equity in scientific discovery. To address this gap, the Parkinson’s Foundation expanded its PD GENEration initiative (offering no-cost genetic testing, counseling, and education) in 2024 through a collaboration with the Latin American Research Consortium on the GEnetics of Parkinson’s Disease (LARGE-PD) to enhance inclusion across Latin America.
Description and Methods: Between 2024 and 2025, PDGENE and LARGE-PD jointly organized educational and recruitment events in Mexico, Colombia, El Salvador, and the Dominican Republic. Each event was tailored to local regulations, cultural context, and site capacities. Programs integrated presentations on PD genetics, genetic counseling, and research participation with opportunities for on-site enrollment, led by trusted local clinicians and institutions. Materials were culturally tailored adapted to regional literacy levels and community values to enhance trust, inclusivity, and accessibility.
Results and Impact: Across the four countries, approximately 700 individuals attended the events, yielding 240 new PDGENE enrollments: 82 in Mexico, 52 in Colombia, 17 in El Salvador, and 89 in the Dominican Republic. During this period, Hispanic/Latino representation in the study overall increased. The initiative also strengthened long-term collaborations with hospitals and local clinicians, establishing a sustainable, replicable framework for culturally tailored community engagement. Attendees and site leaders emphasized the importance of accessible educational content and direct interaction with research teams. These outcomes demonstrate that community-driven approaches enhance trust, participation, and equity in PD genetic research across Latin America.
Conclusions: Integrating educational outreach with participant recruitment represents an effective and sustainable strategy to address barriers to participation and enhance diversity in PD genetic research. Leveraging physician leadership and culturally responsive educational approaches fosters trust, increases awareness, and promotes sustained engagement among underrepresented populations. This regional model shows how empowering communities through inclusive education can transform representation and advance equity in Parkinson’s research across Latin America and the Caribbean.
P46.20
1 PD Avengers, Canada
2 PD Avengers, United States
3 Cure Parkinson's, United Kingdom
4 Weill Cornell Medicine, United States
5 University of California San Francisco, United States
6 University of California, San Francisco, United States
Introduction: Written by women with Parkinson’s (PD) for women with PD in partnership with Fox Insight (FI), this initiative comprises a comprehensive series of surveys mapping women’s experiences across key life stages, including pre-, peri-, and post-menopause, and the psychosocial impact of PD. A companion survey addresses fertility, pregnancy, and childbirth before and after diagnosis. Conducted within FI, this represents the first large-scale effort to systematically capture women’s lived experiences with PD across these critical life stages.
Background: Understanding when PD symptoms first emerge in women may illuminate how hormonal transitions influence disease onset, mask early symptoms, or delay diagnosis. The study team—Dr. Soania Mathur (family physician), Kat Hill (maternity nurse), and Dr. Kristi LaMonica (researcher)— collaborated with an advisory group of women with young-onset PD, originated out of a World Parkinson’s Congress working group, whose clinical and lived experience informed survey design. The work was supported by Helen Matthews (Cure Parkinson’s), the FI team, and Dr. Roberta Marongiu, who contributed to data analysis.
Methods: Listening sessions with PD women on their experience before and after diagnosis informed survey design. Questions addressed symptom evolution and medication adjustments during key hormonal phases: pre-, peri-, and post-menopause, and across pregnancy, childbirth, and postpartum. In collaboration with FI, the surveys were piloted in North America and the UK to ensure linguistic and cultural alignment.
Results: The Experiences of Women Living with Parkinson’s Survey series includes:
Women’s Health and Homelife Survey (closed); n=640 PD women respondents Pre Menopause survey (closed); n= 95 PD women Peri-Menopause survey (closed); n=126 PD women Post-Menopause survey (closed); n= 2531 PD women Fertility, Pregnancy and Childbirth survey (live); n=1005 respondents (935 with PD).
Conclusions: There is a striking interest from women with PD to share their experiences highlighting unmet needs that remain under-recognized by healthcare providers. These span the life course - from delayed diagnosis to inadequate support during fertility, pregnancy, and menopause. Ongoing collaboration with researchers aims to leverage this unique dataset to advance understanding of hormonal, reproductive, and neurological health interactions in women with PD, and to guide more inclusive, responsive care.
P46.22
1 Arizona State University, United States
Introduction: Postural instability in people with Parkinson’s disease (PwPD) is associated with delayed and diminished reactive responses to sudden surface movements, increasing the risk of falls. Daily activities often require maintaining balance while performing an additional cognitive or motor task, which may further impair balance control. However, it remains unclear how dual-task interference influences reactive balance control in PwPD. This study aimed to investigate this relationship.
Methods: Nine individuals with PwPD participated in a reactive balance assessment conducted using an instrumented split-belt treadmill. Unexpected forward or backward slip perturbations were applied to evaluate dynamic balance responses. Each participant completed a single-task condition (ST) and three dual-task (DT) conditions (DTL1–DTL3) involving a visuomotor tracking task performed with a joystick. Increasing dual task levels introduced greater target speed and trajectory randomness. Reactive balance control was quantified using the Margin of Stability (MoS) parameter. Statistical comparisons between ST and DTL2, and between DTL1 and DTL3, were performed using paired-sample t-tests or Wilcoxon signed-rank tests when normality assumptions were not met.
Results: In the first analysis (ST vs. DTL2), five of nine participants showed a reduction (worsening) in MoS during backward slips, and six of nine during forward slips. A mild trend suggested that dual tasking may negatively impact reactive balance control during forward slips (p = 0.113), but not backward slips (p = 0.521).
In the second analysis (DTL1 vs. DTL3), increasing the cognitive task difficulty did not produce consistent changes in reactive balance control across perturbation directions.
Conclusion: The slip perturbation represents a strong biomechanical stimulus that can induce rapid, reflexive balance responses, potentially overpowering the subtler effects of concurrent cognitive demands. Participants who were cautious or fearful of falling may have prioritized physical stability over task engagement, reducing dual-task interference. This variability may explain inconsistent findings across individuals. Limited engagement at higher task difficulty could also account for minimal differences between DTL1 and DTL3. Future work will assess task engagement and cognitive load to better explain these interactions in PwPD.
P46.23
1 Remepy Health Ltd., Israel
2 Remepy Health Ltd., United States
Objective: Develop a structured patient advisory group to iteratively improve a Parkinson’s disease (PD) app for deployment in a forthcoming Phase 3 clinical trial.
Background: PD’s progressive dopaminergic loss drives motor and non-motor burdens that can exceed medication control. We developed the DopApp™, a digital treatment consisting of a proprietary daily protocol combining multisensory motor, psychological, and cognitive training. A prior randomized, 3-week pilot study (n=42; levodopa-treated PD patients) comparing DopApp™ with a placebo-app showed greater gains in motor function, mood, activities of daily living, and fMRI resting-state connectivity in parallel motor and limbic circuits, with module-specific engagement predicting domain-matched benefits. These signals motivated patient-led optimization.
Methods: We established the patient advisory program with 11 individuals with PD from the pilot study. Selection emphasized demographic diversity; PD status (MDS-UPDRS); demonstrated critical thinking in prior feedback; app engagement; and a collaborative mindset. Program goals were to (1) improve user experience via structured feedback, (2) identify everyday needs unmet by existing tools, and (3) build an enduring community that informs iteration.
Results: Advisory discussions emphasized the need for personalized, flexible programs that adapt to individual routines, integrate with daily life, and shift from rigid daily to flexible weekly activity goals with minimum completion targets and optional extra sessions. Participants stressed the importance of minimizing cognitive load by delivering concise, primarily visual guidance, such as short daily videos, instead of lengthy text or large content libraries. They also recommended that the app combine lived-experience “life hacks” with optional recommendations for specific tools, focusing on simple and creative solutions accessible to users with varying levels of digital literacy. Finally, participants underscored the value of maintaining an active co-creation community through regular touchpoints and collaboration between users and the product team.
Conclusions: A structured, criteria-based patient advisory program is feasible and rapidly converts lived experience into product requirements—personalization, routine integration, flexible scheduling, and bite-sized visual guidance. These outputs are informing final refinements to the app for deployment in a large Phase 3 clinical trial.
LIVING WITH PARKINSON'S: Other
P47.01
1 Parkinson Voice Project, United States
Sensory deficits, particularly self-perception of voice, significantly contribute to voice and speech difficulties in Parkinson's disease (PD). Individuals with PD frequently believe their voice is louder than it actually is, leading to a disconnect between how they feel they sound and how others perceive them. This compromised internal feedback loop makes it difficult for them to accept that their speech may be too soft or unclear, even when they recognize they are often not heard.
SPEAK OUT!® Therapy addresses this sensory disconnect by helping individuals adjust their perception of vocal effort and output. The therapy emphasizes speaking with INTENT—deliberate, effortful speech—which not only strengthens vocal muscles but also supports the muscles involved in swallowing. Untreated speech disorders in PD can progress to serious swallowing complications, making early and consistent intervention critical.
The adjustment process requires sustained engagement, often six months to two years, and includes daily practice, weekly SPEAK OUT! Therapy Group, and Refreshers every 3-6 months. A key factor in successful outcomes is the involvement of a Care Partner. They are essential in reinforcing therapy goals, offering the best cue to elicit intentional speech, and providing emotional support. During the initial SPEAK OUT! Evaluation, Care Partners witness the stark contrast between speech with and without INTENT—often hearing their loved one’s “old” voice for the first time in years.
Care Partners are trained to replace habitual prompts like “I can’t hear you” with personalized cues encouraging effortful speech. Their continued support ensures adherence to home practice routines and helps maintain vocal strength. They also learn to recognize when their person with Parkinson’s needs rest and can offer intentional breaks from cueing to support recovery after demanding activities.
By bridging the gap between sensory perception and vocal reality, SPEAK OUT! Therapy empowers individuals with Parkinson’s to reclaim their voice. The active involvement of Care Partners enhances the therapeutic process, making them indispensable allies in the journey toward clearer, stronger communication.
P47.02
1 New York University, United States
BACKGROUND. Parkinson’s disease (PD) impairs gastrointestinal function in up to 70% of patients. When severe gastroparesis or paralytic ileus develop, oral levodopa absorption becomes unreliable or impossible. Alternatives are needed. Vyalev (foslevodopa/foscarbidopa), approved by the US FDA in October 2024, is the first 24 hour continuous subcutaneous levodopa infusion system. Clinical trials showed about three more hours of “On” time per day without troublesome dyskinesia vs oral therapy. CASE DESCRIPTION. This report is based on one patient with advanced PD who, after paralytic ileus preventing gastrointestinal absorption, had only weeks to adopt Vyalev therapy. Her research background supported critical appraisal of system design and potential improvement areas. RESULTS. Vyalev restored stable motor control when oral therapy was unfeasible. Three main challenges to wider adoption were noted: (1) Infection control. Infusion site infections occurred in 28% of Vyalev users vs 3% with placebo infusions. Manufacturer instructions recommend alcohol pads, yet infection prevention studies show that 2% chlorhexidine gluconate (CHG) in 70% isopropyl alcohol provides longer antimicrobial protection and lowers catheter related infections by 40–49%. Findings from catheter studies may apply to Vyalev’s short cannula. CHG based antisepsis and monitoring of infection outcomes may enhance safety. (2) Skin irritation. Erythema and discomfort occur at infusion sites (∼62%), possibly due to acidity of foslevodopa or repeat antiseptic exposure. Barrier sprays or dressings may reduce irritation without compromising sterility, while pH buffered formulations or improved cannula materials could further decrease local reactions and discontinuations. (3) System complexity. Multi-step assembly—vial adapters, syringes, cartridges, tubing, and pump setup—requires dexterity and precision, increasing contamination risk and caregiver dependence. Simplified, pre-assembled components could enable more patients with PD to manage therapy independently.
CONCLUSIONS. Continuous subcutaneous levodopa infusion addresses a crucial gap in managing advanced PD when oral dosing fails. Stable plasma levels and fewer motor fluctuations improve life quality. Future Vyalev iterations integrating CHG based infection control, gentler skin protection, and simplified device design could lower infection (28%) and discontinuation (5%) rates, supporting safer, more autonomous treatment as PD advances.
P47.03
1 Parkinson's Foundation, United States
2 Parkinson's Foundation People with Parkinson's Advisory Council, United States
Introduction For people with Parkinson’s disease (PD) and their loved ones, a planned or unplanned visit to the hospital can be stressful. People with PD are at a higher risk for experiencing challenges in the hospital, frequently related to medication management and mobility issues. These issues often result in further complications and ultimately may lead to an increased length of stay.
After a difficult hospital experience, many people are unsure of what next steps to take, if any. Documenting what happened can often be helpful to a person with PD or their care partner to more effectively process the difficult experience, determine next steps, and identify relevant and useful resources and areas for support.
Methods To address the issues outlined above, the Parkinson’s Foundation created a community-facing resource tool in collaboration with members of the PD community, including the Foundation’s chapter field staff, People with Parkinson’s Advisory Council, and an interdisciplinary team of PD clinicians who provided review and feedback. The final product is an interactive questionnaire, formatted as a Microsoft Form and accessible on the Foundation’s website. This resource tool guides users through a series of robust, PD-relevant questions about their hospital stay and provides suggestions for receiving support, accessing Parkinson’s Foundation hospital safety resources, and steps they can take to help prevent future harm during a hospital visit.
Results The Processing a Challenging Hospital Experience resource will be available on the Foundation’s website in December 2025. Additionally, the resource will be distributed by the Foundation’s chapter field staff to community members and featured in national promotion materials for Patient Safety Awareness Week in March 2026, including social media posts, email newsletters, and hospital safety webinars.
Users will have the option to submit their answers anonymously, share their experiences with members of the PD community to help raise awareness, and/or request direct outreach from a member of the Parkinson’s Foundation’s Helpline. Forms can also be downloaded by the user and saved for reference during a future hospital stay.
4-Late-Breaking Poster Presentations
BASIC SCIENCES: Etiology, genetics, epidemiology, and toxicants
LBP01.01
1 Colorado State University, United States
2 Insilico Medicine, United States
Parkinson’s disease (PD) is characterized by selective nigrostriatal dopaminergic neurodegeneration resulting in progressive decline of motor and cognitive function. Although the etiology of PD is not fully understood, there is mounting evidence associating risk of PD with cumulative exposure to environmental agents, including industrial solvents, pesticides, air pollution, heavy metals, and infectious pathogens. Viral infections, in particular, are linked to neuroinflammatory activation of glial cells that may represent a critical early mechanism in the progression of PD. Our group has demonstrated that infection with the neurotropic alphavirus, Western equine encephalitis virus (WEEV), results in significant astrocytosis preceding dopaminergic neuron loss and motor dysfunction. We have also shown that overexposure to heavy metal manganese (Mn2+) during juvenile development potentiates nigrostriatal inflammation following infection with a non-neurotropic strain of Influenza virus H1N1. Accordingly, we postulated that astrocytic NF-kB signaling in Mn-primed mice is central to the neuroinflammatory response to WEEV infection and subsequent dopaminergic neurotoxicity. To test this hypothesis, we treated wildtype or astrocyte-specific NF-kB knockout mice with Mn2+ in drinking water during juvenile development, followed by adult infection with WEEV at 3 months of age. We then assessed histopathologic changes in PD-relevant brain regions using high content imaging and AI-based image analysis. Compared to vehicle treated, mice exposed to Mn2+ during juvenile development followed by WEEV infection developed more viremic infection and mortality, increased astrogliosis, and disease-associated changes in microglial morphometry. Dopaminergic neurodegeneration was similarly amplified in Mn-primed mice compared to mice infected with WEEV alone. These phenomena were all dramatically attenuated in astrocyte-specific NF-kB KO mice, despite an increase IBA1+ cell number in the substantia nigra. Together, these findings suggest a critical role for astrocyte-mediated neuroinflammation in the context of an environmentally-relevant viral model of PD.
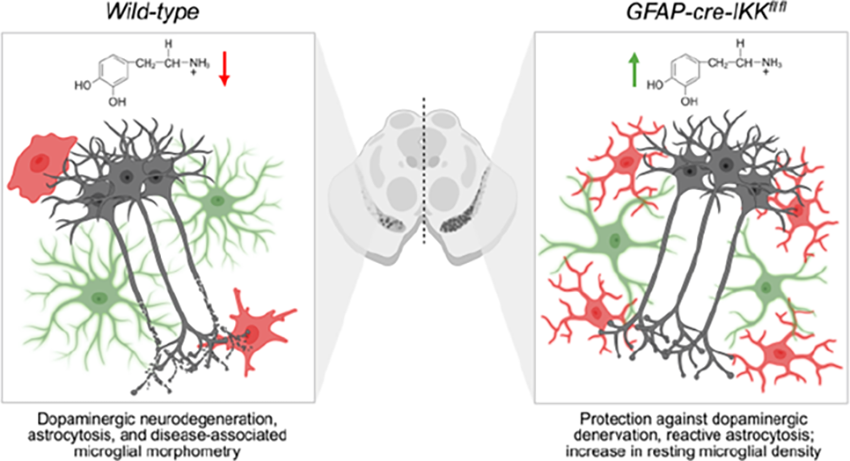
LBP01.02
1 UAB, United States
Environmental exposures increase Parkinson’s disease (PD) risk by initiating neurotoxic pathways that result in neurodegeneration. We and others have previously shown that exposure to industrial byproducts, like the organic solvent trichloroethylene (TCE), induces neurotoxicity within the dopaminergic system and recapitulates hallmark PD pathology, such as alpha-synuclein (αSyn) aggregation, oxidative stress, and endolysosomal dysfunction in adult mice. Mitochondrial dysfunction has been postulated to be a central component of toxicant induced PD; however, the endolysosomal system may play a more integral role in the sustained and persistent neuropathology that drives disease phenotype from environmental risk factors. As TCE exposure is well documented as a PD risk factor in human population studies (Odds Ratio 1.7; CI: 1.39-2.07), we used this toxicant as a model system for understanding the temporal relationship between early toxic mechanisms that drive PD-related neurodegeneration.
We have previously published that dopaminergic neuron loss in mice occurs after 12 weeks of 100 ppm TCE inhalation exposure, the current US OSHA regulated workplace exposure limit. To assess initiating neurotoxic changes that occur prior to neuron loss, we exposed adult, wildtype mice to 100 ppm TCE for 4 weeks and measured a significant reduction of cathepsin D protein within dopaminergic neurons (p<0.0001) prior to measurable neurodegeneration, and elevated accumulation of lysosomal degradation products within neuron populations (SCMAS; p<0.0001). We also observed that TCE exposed mice displayed increased insoluble, aggregated αSyn (MJFR 14-6-2; p<0.0001) in brain lysates. To assess more sensitive measures of TCE-induced toxicity prior to neurodegeneration, adult, wildtype mice were exposed to 100 ppm of TCE for 6 weeks, and their ventral midbrains were collected for a high throughput single-nuclei RNA sequencing analysis. Following exposure, animals that were exposed to TCE saw a significant upregulation in genes related to lysosomal acidification in dopaminergic neurons (FDR < 4.035536e-09), with KEGG ontology terms indicating the lysosomal pathway as the primary altered pathway following TCE exposure. This effect indicates that toxicant-induced endolysosomal dysfunction and improper lysosomal acidification may be a key factor in initiating PD pathogenesis, which could also help explain the lasting effects of neurotoxicity in the context of PD risk across the lifespan.
LBP01.03
1 Rutgers University, United States
It is well-documented that environmental risk factors and gene-environment interactions play critical roles in disease pathogenesis in the majority of Parkinson’s disease (PD) cases. Decades of epidemiological, mechanistic, and post-mortem studies show an association between specific environmental exposures and increased risk of PD. However, despite long-standing recognition of the role of environmental risk factors, significant knowledge gaps remain about how these exposures contribute to disease pathogenesis, and the environment has been largely neglected in the PD research field. Work to assess PD-related neurotoxicity largely relies on in vivo animal models, which are considered the most physiologically relevant systems for neurotoxicity testing, disease modeling, and drug screening. However, in vivo models have several limitations, and emerging new approach methodologies (NAMs) offer efficient, translatable methods to assess neurotoxicity and disease mechanisms. In this study, we aimed to recapitulate our two-hit in vivo mouse model in which developmental exposure to the organochlorine pesticide dieldrin, a known risk factor for PD, increased neuronal susceptibility in both the α-synuclein pre-formed fibril (PFF) and MPTP models. Using Lund human mesencephalic (LUHMES) cells, we adopted a 3D neurosphere model widely used as a neurotoxicity screening tool because it shows improved differentiation, survival, and cell-to-cell interactions compared to 2D cultures. Here, we replicate work from other labs demonstrating the dopaminergic-like phenotype of LUHMES 3D neurospheres, confirming 1) expression of dopaminergic and neuronal markers using ddPCR and western blots, and 2) susceptibility to 1-methyl-4-phenylpyridinium (MPP+) toxicity, assessed by ATP and neurite outgrowth assays. We demonstrate that these neurospheres are also susceptible to dieldrin toxicity at concentrations consistent with those measured in the brains of exposed mice in our in vivo paradigm, showing a dose-dependent reduction of ATP levels and neurite outgrowth. To recapitulate the two-hit effects observed in our animal model, we tested the effects of dieldrin pretreatment during differentiation on post-differentiation susceptibility to MPP+ to establish a novel paradigm for dissecting the molecular mechanisms underlying the effects of environmental toxicants on PD risk.
BASIC SCIENCES: Mitochondria, Oxidative Stress
LBP04.01
1 JPMorgan Chase, United States
2 James H. Quillen College of Medicine, East Tennessee State University, United States
3 Seeds Scientific Research & Performance Institute, United States
Parkinson's Disease (PD) involves a failure of mitochondrial quality control, with the mechanism for identifying unhealthy mitochondria for degradation remaining unclear. The new Superoxide Sentinel Hypothesis proposes a signaling pathway by which the mitophagy machinery is able to select low-quality instead of healthy mitochondria for degradation. PD risk factors disrupt this signaling pathway by depleting cytoplasmic NAD+ and NADPH pools and uncoupling nitric oxide synthase (NOS) resulting in a halting of selective mitophagy. Clinical strategies should focus on identifying disruptions of these signaling pathways as potential causes of PD and on optimizing cytoplasmic NADPH redox potential and NAD(P)H availability. The Superoxide Sentinel Hypothesis describes a mechanism for initiating mitophagy in which superoxide acts as a mitochondrial sentinel, produced when one or more of the cofactors FAD, FMN, or coenzyme Q fail to transfer electrons efficiently, thereby exposing their free-radical intermediates to react with molecular oxygen. Many mitochondrial enzymes and pathways utilize these coenzymes, including pyruvate dehydrogenase, the Krebs cycle, the electron transport chain, and enzymes involved in anabolic and catabolic processes. SOD2 then converts this matrix space superoxide into hydrogen peroxide, some of which leaves the mitochondrion as a messenger to initiate a cytoplasmic response involving factors like DJ-1, NRF2, NF-κB, Ca2+, and calmodulin contingent on sufficient NADPH redox potential to prevent NOS uncoupling. Nitric oxide, produced by one of the NOS isoforms, enters the mitochondrial matrix and reacts with superoxide to form peroxynitrite, which triggers mitophagy by means of depolarizing the mitochondrial membrane potential. This depolarization occurs through either opening the mitochondrial permeability transition pore or by peroxynitrite breakdown into free radicals that deplete NADPH, which drives increased nicotinamide nucleotide transhydrogenase (NNT) activity that transfers hydride ions from NADH to NADP+ to restore mitochondrial NADPH levels driven by the transport of protons down their gradient. Depolarization leads to mitochondrial PINK1 stabilization and Parkin recruitment, which in turn recruit autophagosomes to the organelle for degradation. You can read the full analysis at https://doi.org/10.1016/j.redox.2025.103979.
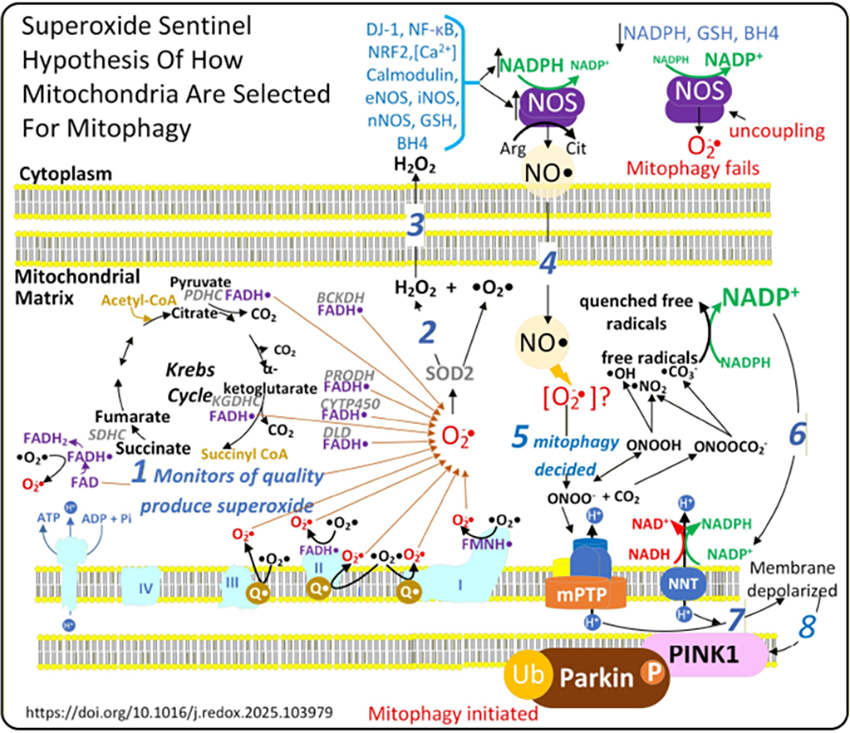
BASIC SCIENCES: Pathology
LBP05.01
1 Weill Cornell Medicine, United States
Background: Alpha-synuclein (αsyn) is the pathological hallmark of several neurodegenerative disorders that often show overlapping clinical features. 18-Fluorodeoxyglucose (FDG) positron emission tomography (PET) has been used to capture downstream physiological consequences of αsyn pathology, typically at relatively late stages characterized by posterior cortical and occipital hypometabolism. Therefore, the early-stage and potentially compensatory association between αsyn pathology and increased metabolic activity remains poorly understood.
Method: We leveraged 657 participants from the Alzheimer’s Disease Neuroimaging Initiative (mean age 74.66±7.87 years; 294 females; 141 αsyn–positive) who had undergone seed amplification assay (SAA) Cerebrospinal Fluid (CSF) αsyn assay as well as FDG-PET, Aβ-PET, and structural Magnetic Resonance Imaging (MRI). We performed voxel-wise analyses on FDG-PET scans to compare metabolic differences between αsyn–positive and αsyn–negative individuals stratified by cognitive status (cognitively impaired [CI] and cognitively unimpaired [CU]), adjusting for age, sex, and Aβ status. Multiple comparisons were addressed using a voxel-wise cluster-defining threshold of p < 0.005 (uncorrected), followed by cluster-level FDR correction at p < 0.05.
Results: Figure 1 results revealed distinct disease- and region-specific αsyn-related metabolic patterns. In the CI group (Figure 1a; n=157), the metabolic profile was heterogeneous, with hypermetabolism in the basal ganglia, thalamus, and precentral gyrus alongside robust hypometabolism in the temporo-occipital and precuneus regions. Interestingly, in the CU group (Figure 1b; n=500), FDG-PET showed αsyn-related hypermetabolism in regions including the thalamus, insula, and precentral gyrus. After cluster-wise FDR correction (FDR < 0.005), three significant hypermetabolism clusters were observed in the CI comparisons: 1- Left Precentral Gyrus (MNI: –24, –21, 53; peak Z maxima = 3.68, FDR-p = 0.026); 2- Right Thalamus (MNI: 12, –19, 7; peak Z maxima = 4.17, FDR-p = 0.011); 3- Right Basal Ganglia (MNI: 29, 1, –7; peak maxima Z = 4.30, FDR-p = 0.077). None of the results in CU group survived after cluster-level FDR correction. However, as shown in Figure 1c, the thalamic hypermetabolism pattern is the only region where we observe robust overlap between the CU and CI analyses results.
Conclusions: Our findings suggest that thalamic hypermetabolism may represent an early signature of αsyn pathology.

BASIC SCIENCES: Animal models of Parkinson's and Parkinsonism
LBP06.01
1 CEA, France
2 CEA, MIRCen, Laboratoire des Maladies Neurodégénératives, France
3 Université de Bordeaux, CNRS, IMN, UMR 5293, France
4 Benjamin, France
Synucleinopathies are characterized by the pathological aggregation of alpha-synuclein (α-syn), a normally monomeric presynaptic protein. In Parkinson’s disease (PD), these aggregates form Lewy bodies and neurites, contributing to neurodegeneration. Compelling evidence shows that α-syn aggregates propagate in a prion-like manner, recruiting monomers and spreading between cells. This was first observed in fetal neuronal grafts implanted in PD brains, where host-derived α-syn inclusions appeared. Experimental models using viral vectors to overexpress wild-type or mutant α-syn in rodents and primates, as well as inoculation of brain homogenates from transgenic mice or synucleinopathy patients, or synthetic α-syn preformed fibrils (PFF), have demonstrated α-syn propagation and dopaminergic degeneration. Importantly, α-syn can adopt structurally distinct fibrillar forms or “strains” that differ in their biochemical and pathological profiles. In vivo studies show that these strains induce distinct patterns of α-syn pathology and neurotoxicity, supporting the hypothesis that strain-specific properties contribute to clinical heterogeneity in synucleinopathies. Here we performed bilateral inoculation of 18 primates both in the substantia nigra (AAV-CBA-aSynA53T or PBS) and putamen (PFF, patient-derived α-syn or PBS). All NHPs underwent motor and cognitive assessment longitudinally as well as PET imaging at baseline, 6, and 12 months post-injection (moPI). Post-mortem analysis included tyrosine hydroxylase immunocytochemistry to detect α-syn-mediated nigrostriatal alterations. We assessed the seeding propensity of the various α-syn inocula by quantifying phosphorylated and aggregated α-syn.
Preliminary results show motor and cognitive deficits of different severity according to the inocula, and suggest that the combination of AAV injection in the SN and PFFs or patient-derived α-syn in the putamen significantly exacerbates the phenotype and accelerates the appearance of disease symptoms. This was further confirmed by PET imaging, looking at the activity of the dopamine transporter (18F-FE-PE2I) and the D2 receptor (18F-Fallypride), as well as a radioligand binding α-syn. Post-mortem and biomarker studies are currently ongoing. Our findings support the relevance of α-syn strain diversity and dual-hit models in reproducing the complexity of synucleinopathies and, to the best of our knowledge, offer a robust and valuable platform for therapeutic and biomarker testing.
LBP06.02
1 Massachusetts Institute of Technology, United States
2 Wellesley College, United States
3 MIT, United States
4 Caltech Institute of Technology, United States
Parkinson’s disease (PD) is a progressive neurodegenerative disorder marked by dopaminergic neuron loss and alpha-synuclein (α-syn) aggregation. Although motor symptoms define diagnosis, evidence suggests PD pathology may originate in the gut decades earlier. Gastrointestinal dysfunction, enteric α-syn accumulation, and environmental toxin exposure support a gut-to-brain propagation model, yet epigenetic mechanisms mediating this axis remain unclear.
We established a chronic environmental mouse model recapitulating prodromal PD and investigated gut–brain interactions and epigenetic modulation. A 5-day transient rotenone exposure followed by 9 months observation produced persistent gastrointestinal dysfunction without overt motor deficits. Rotenone-treated mice exhibited a 48% reduction in dopaminergic neurons. They also showed a 46% increase in whole-gut transit time, reduced colonic length and contractility, increased crypt depth (134 µm vs 84 µm), and elevated acid mucin goblet cells (20.7 vs 2.4), indicative of constipation and compromised mucus barrier integrity. This model dissociates gastrointestinal pathology from motor symptom onset, capturing a prodromal therapeutic window.
To dynamically monitor gut–brain signaling, we developed an implantable neurotechnology platform with LED-embedded fiber probes in the proximal colon for localized optogenetic stimulation. In healthy mice, 20 Hz stimulation (10 ms pulse width, 45 min) induced epigenetic remodeling, including increased global DNA methylation. Following a 2-month successful implant, we are deploying this platform in rotenone-induced PD mice to longitudinally map the temporal relationship between gastrointestinal dysfunction, motor decline, and epigenetic changes, enabling real-time correlation of prodromal and symptomatic features.
These findings identify early physiological and epigenetic signatures of environmentally triggered PD progression, reinforcing the gut as a critical interface for disease initiation and intervention, and providing a platform for future mechanistic and therapeutic studies.
LBP06.03
1 Department of Anatomy, Korea University College of Medicine, Seoul, South Korea
Introduction: Parkinson’s disease (PD), the second most prevalent neurodegenerative disorder, is characterized by α-synuclein pathology, a key hallmark of the disease. The molecular mechanisms underlying α-synuclein aggregation, particularly in idiopathic PD (IPD), remain unclear. Post-translational modifications (PTMs), including phosphorylation, ubiquitination, and SUMOylation, have been implicated in α-synuclein aggregation. The SMG, anatomically connected to the brainstem via cranial nerves, exhibits α-synuclein pathology comparable to that of the SN. We hypothesize that RNA signatures in SMG tissue may share molecular biomarkers with SN tissue that contribute to α-synuclein aggregation in patients with IPD. Recently, we identified common neuronal molecular markers using RNA sequencing data from submandibular gland (SMG) tissue and substantia nigra (SN) tissue in patients with Parkinson’s disease (PD). This study aimed to validate these molecular markers in a 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-induced mouse model.
Methods: Differentially expressed genes (DEGs) from bulk RNA-seq of SMG tissue in PD patient datasets were compared with neuronal DEGs from single-nucleus RNA-seq of SN tissue obtained from postmortem PD brain datasets. We identified approximately 13 common neuronal DEGs between the SMG and SN tissues of PD patients. A subacute MPTP mouse model was generated by serial intraperitoneal injections of 30 mg/kg/day MPTP for 7 days. Animals were sacrificed 14 days after the final MPTP injection, and SN tissues were collected for PCR analysis. Prior to sacrifice, behavioral tests confirmed Parkinsonian features in the animals.
Results: The 13 common neuronal DEGs identified in both SMG and SN tissues from PD patients were validated in the MPTP mouse model using PCR analysis. Among them, three target molecules were selected for downstream mechanistic studies. These molecules are known to be involved in molecular pathways including ubiquitin activity, chromatin structural regulation, and mitochondrial function.
Conclusions: The identified DEGs may represent potential molecular markers implicated in the pathogenesis of Parkinson’s disease. Ongoing investigations are focused on elucidating the underlying mechanisms in PD animal models.
LBP06.04
1 H.Lundbeck A/S, Sweden
2 2Motac France SAS, France
Chronic levodopa treatment is associated with the development of motor complications, adding complexity to disease management in advanced Parkinson’s disease (PD). Dopamine agonists (DA) are generally associated with fewer motor complications than levodopa, but are generally insufficiently efficacious in advanced PD. The limited efficacy of most DAs likely reflects predominant D2/D3 (D2-like) dopamine receptor activity with insufficient D1-like pathway engagement, essential for motor control. In contrast, apomorphine activates both D1-like and D2-like receptors, which may explain its superior motor efficacy; however, it is not orally bioavailable.
Lu AF28996 is an orally administered prodrug that is converted in vivo into a potent D1/D2 receptor agonist. In this study, we evaluated the acute and chronic effects of Lu AF28996 in the 6-hydroxydopamine (6-OHDA) PD rodent model using both motor assays (rotational response and motor asymmetry in the cylinder test) as well as the standard abnormal involuntary movement (AIM) scale for assessment of treatment-induced dyskinesias.
In 6-OHDA-lesioned rats, acute administration of Lu AF28996 produced a dose-dependent long-lasting increase in rotational behavior as well as an alleviation of the 6-OHDA-induced motor asymmetry seen in the cylinder test. This restorative effect on motor function was maintained during a once-daily chronic treatment period of 15 days. In addition, de novo treatment with Lu AF28996 resulted in minimal treatment-induced dyskinesias during the chronic treatment period compared with levodopa, which served as a comparator. When switching levodopa-primed dyskinetic rats from levodopa to Lu AF28996, there was a gradual and substantial reduction in the severity of AIMs over time, while the effect on motor asymmetry in the cylinder test remained intact.
In summary, acute and chronic Lu AF28996 administration to 6-OHDA rats resulted in long-lasting alleviation of motor function but with fewer treatment-induced dyskinesias than with levodopa. Future research in additional translational models is warranted to assess the therapeutic potential of Lu AF28996 in advanced PD.
LBP06.05
Man Kumar Tamang1, Divya Mondhe1, Sunil Srivastav1, Alex Lehn1, John O'Sullivan2, Rob Adam2, Richard Gordon1
1 Translational Neuroscience Laboratory, School of Biomedical Sciences, Faculty of Health, Queensland University of Technology, Translation Research Institute, Brisbane, Australia
2 Centre for Clinical Research, The University of Queensland, Brisbane, Australia
Background: Paraquat (PQ) is a commonly used agricultural pesticide. Previous human studies have shown link between exposure to pesticides and increased risk of Parkinson’s Disease (PD). PQ is known to induce systemic oxidative stress and neuroinflammation. The environmental toxins could affect the brain and neuro-behavioural outcomes through gut microbial alterations along the gut-brain axis. Altered gut microbiome and some non-motor symptoms have been reported to occur before overt motor impairments appear in PD patients. There are limited pre-clinical studies showing impact of environmental toxins on the gut-brain axis relevant to PD. Our study aimed to determine the impact of PQ on gut microbiome and PD relevant neuro-behavioural changes in mice. Methods: Adult C57BL/6J mice were orally exposed to PQ for two weeks. Control mice were administered with sterile saline. Faecal samples were collected at baseline prior to exposure, as well as two weeks after PQ exposure. Samples were processed for high resolution functional metagenomic sequencing to assess microbiome composition and function. Results: We found that PQ treatment resulted in gut microbial dysbiosis, characterized by reduced species richness and microbial evenness. Furthermore, Principal Coordinate Analysis with PERMANOVA testing revealed significant shifts in the gut microbial community following PQ exposure. Differential Abundance Analysis revealed depletion of critical anaerobic bacteria, as well as other species involved in oxidative stress and inflammation linked to PD. Interestingly, microbiome shifts were evident even prior to the onset of motor symptoms but coincided with changes in anxiety and depression, a key non-motor feature of PD pathology with links to gut dysbiosis. Conclusion: Overall, our study shows significant gut microbiome alterations following environmental exposures such as PQ. Our ongoing studies are assessing other neurotoxicants and heavy metals linked to PD to understand if early changes in the gut microbiota could be associated with chemical exposures.
BASIC SCIENCES: Brain physiology, electrophysiology and circuitry
LBP07.01
1 University of Florida, United States
Progressive loss of basal forebrain cholinergic projection neurons is predictive of cognitive deficits in dementia with Lewy bodies and Parkinson’s Disease dementia, and α-synuclein aggregates accumulate in the basal forebrain of patients. These aggregates have been shown to impair synaptic transmission, leading to reduced glutamate and dopamine release and excitotoxicity. However, it remains unclear how α-synuclein aggregation impairs cholinergic neurons in the basal forebrain, acetylcholine release from basal forebrain neurons, and postsynaptic cholinergic signaling and plasticity.
Using the preformed fibril model to induce α-synuclein pathology, we investigate how α-synuclein aggregation alters cholinergic circuit function and synaptic plasticity in the prefrontal cortex.
To determine how this pathology impacts cortical circuits, we performed whole-cell electrophysiology recordings from layer V pyramidal neurons in the prelimbic medial prefrontal cortex. Initial analyses revealed consistent changes in intrinsic membrane properties, including increased rheobase and decreased membrane resistance, indicating reduced neuronal excitability and suggesting altered intrinsic physiology that may shape downstream plasticity.
To assess both circuit recruitment and baseline synaptic tone, we recorded evoked and spontaneous excitatory postsynaptic currents. α-synuclein pathology sensitizes cortical neurons to cholinergic input and dysregulates synaptic plasticity mechanisms critical for executive function, with enhanced long-term depression that evolves across disease progression. Responses differ between neurons with and without Lewy-like inclusions, highlighting cell-specific vulnerability. Pharmacological experiments demonstrate that M1 muscarinic receptors gate cholinergic-induced synaptic depression, with positive allosteric modulation further enhancing sensitivity in pathology-bearing neurons.
Similar patterns are observed in spontaneous synaptic activity. Imaging confirms predominantly postsynaptic changes and shows no detectable basal forebrain cholinergic deficits at early stages, suggesting cortical dysfunction precedes overt degeneration.
Together, these findings show that α-synuclein pathology reshapes intrinsic neuronal properties and sensitizes prefrontal circuits to cholinergic signaling through M1-dependent mechanisms, identifying postsynaptic cholinergic dysregulation as a key contributor to circuit dysfunction and a potential therapeutic target.
LBP07.02
1 University of Florida, United States
Lewy body dementias (LBD) are a group of neurodegenerative disorders characterized by the accumulation of α-synuclein aggregates, leading to cognitive, motor, and psychiatric symptoms. Among these manifestations, executive dysfunction stands out as a prominent and debilitating feature, significantly impacting daily functioning and quality of life. Despite hallmark executive function impairments in patients with LBD, the mechanisms by which α-synuclein aggregation contributes to cognitive dysfunction remain poorly understood. The prefrontal cortex, a central hub for executive processing and a region exhibiting robust Lewy pathology, represents a critical candidate for investigation. To examine how α-synuclein aggregation disrupts prefrontal circuit function, we employed pharmacological, electrophysiological, and behavioral approaches in the pre-formed fibril (PFF) mouse model at 6 weeks and 3 months post-injection. We assessed the impact of pathological α-synuclein on layer V pyramidal neurons within the prelimbic medial prefrontal cortex (PL-mPFC). To distinguish between neurons with and without pathological α-synuclein inclusions, we used a novel auto-fluorescent aggregate binder enabling real-time identification of Lewy-like inclusion-positive (LLI+) and inclusion-negative (LLI−) neurons during patch-clamp recordings. At both 6 weeks and 3 months post-PFF injection, LLI+ neurons displayed elevated intrinsic excitability accompanied by a reduced rheobase, indicating a robust hyperexcitable phenotype that emerges early and persists as pathology progresses. In contrast, LLI− neurons exhibited reduced intrinsic excitability and an increased rheobase at 3 months, revealing a paradoxical hypoexcitable phenotype. Notably, the emergence of this hypoexcitability coincided with behavioral deficits in executive function. Using a pairwise visual discrimination task with reversal, we observed intact performance at 6 weeks, whereas by 3 months PFF-seeded mice showed impaired task acquisition and reduced reversal accuracy, consistent with declining cognitive flexibility. Together, these findings demonstrate that α-synuclein pathology produces cell-type–specific and temporally evolving alterations in prefrontal circuit excitability that parallel the onset of executive dysfunction in LBD, providing mechanistic insight and potential targets for therapeutic intervention.
LBP07.03
1 Indiana University School of Medicine, United States
Degeneration of dopamine (DA) neurons in the basal ganglia is a hallmark of Parkinson’s disease (PD). The most effective treatment to alleviate motor symptoms is the use of Levodopa, however, its prolonged use leads to dyskinesia and episodic psychosis events. At this time, there is no treatment to delay or stop the progression of PD. Recent studies have shown that the development of dyskinesia can be treated using glycine transporter type 1(GlyT1) inhibitors. Interestingly, using a GlyT1 inhibitor in the striatum increases glycine concentration, leading to the activation of striatal glycine receptors (GlyRs), increasing dopamine release and promoting neuroprotection. Using patch clamp electrophysiology, we previously demonstrated that GlyRs are highly potentiated by the activation of dopamine receptors. These results implicate a direct interaction between dopamine, dopamine receptors, and GlyRs. Here, using a PD mouse model of selective neurotoxic disruption (6-OHDA), patch clamp electrophysiology, and ex vivo photometry, we showed that the function of GlyRs in medium spiny neurons (MSNs) are affected by the loss of the dopaminergic terminals. Specifically, we found GlyR-evoked currents decreased at 7, 14, and 21 days following 6-OHDA lesion. To further elucidate the mechanism behind these results, we used GlyR α1-subunit KI mouse model to disrupt intracellular interactions involved in GlyR potentiation mediated by G-protein. Preliminary data suggests that at 30 days post-lesion, the physiological and behavioral effect in KI mice is more pronounced than in wildtype controls. Photometry recordings also uncover changes in striatal DA release in response to exogenous glycine application. Collectively, these data suggest a specific role of striatal GlyRs in mediating dopaminergic tone, which could be involved in the progression of PD. Ultimately, elucidating the relationship between glycine, GlyRs, and DA release may reveal new targets for therapeutic intervention to treat PD.
BASIC SCIENCES: Neuropharmacology
LBP09.01
1 CBX Therapeutics, Israel
Introduction Levodopa remains the standard of care in Parkinson’s disease (PD), but motor fluctuations and variable response necessitate improved dopaminergic strategies. Real world evidence suggests cannabis may improve PD symptoms. We developed an integrated preclinical program advancing rational cannabinoid combinations from in vitro screening to in vivo validation in Parkinsonian models to enable clinical translation.
Methods A stepwise discovery funnel prioritized candidate formulations. We prepared combinations from 7 cannabinoids library (THC/CBD/CBG/CBC/CBDV/CBT/CBN). After defining non-cytotoxic ranges, dopamine (DA) secretion by PC12 dopaminergic cells was measured using ELISA, followed by dose–response profiling and in vivo efficacy testing in MPTP-induced PD mice using Pole Test and Rotarod assays.
Results In Vitro Screening Across 120 combinations, 10%, 55%, 25% and 10% showed minimal, moderate-high, high and very high enhancement in DA release, respectively. CBD-dominant formulations increased DA release relative to minor-only mixtures, while presence of THC showed greater potency but higher variability.
Dose–response profiling revealed distinct patterns, including biphasic activation (THC), biphasic modulation (THC/CBD), and U-shaped responses (CBD and minor). This systematic combinatorial approach demonstrated that DA release depends on defined synergistic multi-component interactions.
In Vivo Validation Most promising combinations representing pharmacodynamic classes were advanced to in vivo evaluation (CBX-95, CBX-94, CBX-38, CBX-4). In the Pole Test, CBX-38 showed significant improvement vs. disease and L-dopa (p<0.001), while CBX-4 also outperformed L-dopa. CBX-38 matched levodopa in Traverse Down Latency and remained superior to disease controls across endpoints. In the Rotarod assay, CBX-38 and CBX-95 improved performance vs. disease (p<0.01), with CBX-95 also surpassing L-dopa (p<0.05). In vivo data confirmed translational potential of CBX-38 and CBX-95 demonstrating functional motor improvement across PD-relevant endpoints.
Conclusions Systematic combinatorial screening identified pharmacodynamic classes with meaningful motor improvement. Integrated analysis identified CBX-38 as the primary First-in-Human candidate, with CBX-95 being secondary. CBX-38 is the lead candidate with consistent superiority over L-dopa. Together, these results support advancement toward First-in-Human clinical evaluation.

BASIC SCIENCES: Prevention, neuroprotection and neuroplasticity
LBP11.01
1 Pell Bio-Med Technology Co., Ltd, Taiwan
Disease-modifying therapies for Parkinson’s disease (PD) remain an unmet medical need. Neuroinflammation and dopaminergic neuronal degeneration are central pathological features of PD. Targeting inflammatory signaling pathways may represent a disease-modifying strategy. PP021 is a novel short peptide identified through in vivo screening of bio-active molecules isolated from rabbit skin inflamed by vaccinia virus infection. The present study evaluated its anti-inflammatory activity, brain penetration, neuroprotective effects, and preclinical safety profile.
PP021 suppressed IL-6 and iNOS expression and reduced nitric oxide production in LPS-stimulated macrophages via inhibition of NF-κB signaling. Following a single 10 mg/kg oral dose, PP021 was detected in mouse brain within 30 minutes, confirming blood–brain barrier penetration. We next assessed the therapeutic efficacy in a subacute MPTP-induced PD mouse model that may recapitulate motor impairment with dynamic functional fluctuations. Oral intake of PP021 (1, 10, 50 mg/kg; oral gavage; BID for 10 days) successfully led to dose-dependent improvement in motor performance. Compared with PD mice without treatment, PP021-treated mice showed significantly reduced pole descent time, prolonged rotarod latency, decreased fall frequency, and increased grip strength (p<0.05–0.001). In addition, treatment of 50 mg/kg per dose exhibited efficacy comparable to or greater than treatment with Madopar (100 mg/kg). IHC analysis of brain tissues confirmed significant preservation of tyrosine hydroxylase–positive (TH+) neurons in the substantia nigra across various doses of PP021 treatment groups (p<0.05–0.001), with noticeable dose–dependent responsiveness.
Comprehensive safety pharmacology revealed no adverse effects on the central nervous, respiratory, or cardiovascular systems. In 28-day GLP repeat-dose toxicity studies, the NOAEL was 1000 mg/kg/day in rats and 500 mg/kg/day in Beagle dogs. No genotoxicity was detected, and toxicokinetic analyses showed no drug accumulation in either species.
In conclusion, our findings demonstrate that orally administered PP021 inhibits inflammatory signaling, penetrates the blood-brain barrier, preserves nigral dopaminergic neurons, and improves motor deficits in an established MPTP PD model, with a favorable nonclinical safety profile supporting first-in-human trial. Phase I clinical trials in China and the United States will start in May 2026.
BASIC SCIENCES: Genetic and other Cellular Models of Parkinson's, including iPSCs
LBP12.02
1 University of Massachusetts Amherst, United States
Neural organoids are a model system that recapitulate the brain in structure and function. Typical methods involve differentiating stem cells into various brain regions separately and can be studied in isolation or fused together to form assembloids. This fusion occurs once the regions have been differentiated which does not reflect brain development in vivo. During development, gradients of morphogens pattern the neural tube into the different brain regions. Our method uses a gradient-producing device to pattern multiple brain regions into the same organoid in a more physiologically relevant manner. These organoids include regions of striatal cells and midbrain cells, for studying the nigrostriatal pathway that is involved in Parkinson’s disease. Organoids are validated via immunocytochemistry and electrophysiology, and are being developed for potential use as a drug testing model. These organoids will allow for better studying of PD by incorporating the striatum into the model system with physiologically relevant neural connections.
LBP12.03
1 Genentech, United States
aSynuclein aggregation is a defining hallmark of pathology in Parkinson's disease (PD). A9 dopaminergic neurons of the substantia nigra are preferentially vulnerable to this pathology. Human iPSC-derived A9 dopaminergic neurons offer a physiologically relevant platform to model synuclein aggregation-induced toxicity and to identify genetic regulators that modify neurotoxicity in synucleinopathies.
Here, we optimized upon the biphasic WNT activation protocol to consistently differentiate A9 dopaminergic neurons across multiple iPSC donor lines. We identified initial seeding density and CHIR concentration as critical parameters for tuning the magnitude of WNT signaling required to reliably specify midbrain floor plate identity. Using this optimized differentiation, we developed an aSyn-fibril seeding model by systematically varying alpha-synuclein expression levels in both iPSC-derived dopaminergic neurons and NGN2-induced neurons. We found that alpha-synuclein expression level and the extent of somatic aggregation are key drivers of neurotoxicity in the seeding model, establishing a quantitative framework linking aggregation burden to neuronal loss.
Leveraging this system, we performed a pilot CRISPR knockout screen targeting PD-associated GWAS genes and identified lysosomal dysfunction as a strong enhancer of synuclein aggregation-induced toxicity. Together, these results establish a scalable iPSC-based platform for dissecting the genetic architecture of synuclein-driven neurodegeneration in dopaminergic neurons.
LBP12.05
1 Gateway Institute for Brain Research, United States
Introduction: Midbrain organoids have emerged as a quintessential model for Parkinson’s Disease (PD), as they harness the potential to recapitulate intricate networks that become compromised in PD. The utilization of these minibrains creates more opportunities for understanding how PD can be targeted and treated through specific cellular mechanisms. The goal of this study was to 1) investigate the feasibility of a patient-specific midbrain organoid model 2) employ this model by differentiating five PD patient-derived and five healthy control induced pluripotent stem cell (iPSC) lines and 3) transition the model to higher-throughput experiments including drug-screening.
Methods: Patient and healthy control peripheral blood mononuclear cells (PBMC) were isolated from blood and reprogrammed into iPSCs. These iPSCs were then entered into the midbrain organoid differentiation protocol using a spinning bioreactor system. A single spinning bioreactor system can grow up to 1000 organoids in each vessel. Organoids were then transferred to different plate types to examine electrical activity, dopamine production, transcriptomics, proteomics, and presence of dopaminergic proteins via immunofluorescence. Upon the completion of full characterization of the midbrain organoids, a long-term drug screening study commenced.
Results: Midbrain organoids cultures using the aforementioned protocol were electrically active, produced dopamine, and displayed the dopaminergic phenotype that is indicative of cells within the human midbrain. Organoids were transferred to different plate types and successfully used for metabolic assay development and combinatorial drug testing.
Conclusions: The High-Throughput Midbrain organoids show promise as a sustainable PD model that can be used to generate a personalized therapeutic framework. Through this study, we were able to successfully differentiate five patient-derived PD and healthy control cell lines into midbrain organoids. The model is robust enough to adapt to different cell lines while still displaying the midbrain phenotype. Moving forward, we will continue to characterize this model and begin to transition to automated systems for bona fide high-throughput screening methods.
LBP12.06
1 University of Pennsylvania, United States
Misfolding and intercellular spread of α-synuclein (aSyn) are central to Parkinson’s disease (PD) pathogenesis, yet human-specific mechanisms are difficult to examine in standard animal models. To understand the human aSyn pathology and cell-to-cell propagation in human neurons, we have developed a three-dimensional (3D) anatomically-relevant human model of the nigrostriatal pathway. This sophisticated in vitro testbed consists of three compartments: human iPSC-derived dopaminergic (DA) neurons, human iPSC-derived striatal medium spiny neurons (MSNs), and 2cm long dopaminergic axonal tracts that connect the segregated DA and striatal neuronal populations. Pathology in one population was initiated by injecting aSyn preformed fibrils (PFFs) and cell-to-cell spread was analyzed using immunohistochemistry (IHC), ELISA and seed amplification assay (SAA). IHC results showed evidence of early synucleinopathy in 40-50% cells in both the neuronal populations in comparison to unseeded controls when PFFs were injected to the DA neurons. Further, we found time-dependent aggregation of pSer129+ inclusions in the DA neurons when MSNs were injected with PFFs. ELISA results revealed higher aggregated aSyn and lower total synuclein in the DA axon tracts in comparison to the healthy control, indicating abundant misfolded aSyn in the neurites. Further, SAA performed on cell lysates confirmed the presence of competent aSyn seeds, indicating the capacity to spread pathological aSyn protein. In conclusion, this novel in vitro human testbed recapitulates key features of PD-related aSyn pathology and cell-to-cell spread. This promising platform enables mechanistic investigation of human PD pathophysiology and offers a tractable system for testing modulators of aSyn uptake, seeding, transmission and clearance, thereby accelerating the translation of aSyn-targeted therapeutics and biomarker strategies.
COMPREHENSIVE CARE: Exercise and Physical Activity
LBP14.01
1 University of Tennessee, United States
2 The Cole Center for Parkinson's and Movement Disorders, United States
3 Black Dog Fitness, United States
4 University of Tennessee Health Science Center Office of Research Support, United States
Introduction: There is growing evidence to substantiate the modifying impact of adaptive exercise on physical functional capacity and quality of life across all stages of Parkinson’s disease progression. The goal of this study was to explore the effects of community-based adaptive exercise of varying intensity and length on the physical functioning of people with Parkinson’s disease in relation to relevant clinical data.
Methods: This was an IRB-approved exploratory study of retrospective performance-based assessment and clinical data for N=25 consenting individuals with Parkinson’s disease who participated in one of three adaptive exercise classes.
The performance-based assessment data collected at baseline and at one subsequent assessment included, 1.) Fullerton Advanced Balance Scale (FAB), 2.) 30 sec Sit to Stand (STS), and 3.) the Timed Up and Go (TUG). Time-equivalent clinical data derived from medical records included: co-morbidities, prominent motor, and non-motor symptoms as well as medication load - Levodopa Equivalent Daily Dose (LEDD) - and demographic variables.
Primary analysis focused on
Comparing changes in performance-based functional capacity (FAB, TUG, and STS) and medication usage over time Comparing the primary endpoints (FAB, TUG, and STS) between different classes while controlling number of classes taken.
Results: The sample population was all Caucasian with an average age of 68.5±7.25.
After robust regression analysis (α<0.05 significance level), FAB scores at assessment 2 were significantly and positively associated with the number of completed classes once adjusted for baseline FAB scores (p=0.04). TUG scores were negatively related to the number of classes, though the significance varied in sensitivity analyses, showing the effect of outliers in small samples. STS scores were not significantly associated with the number of classes taken. Changes in levodopa equivalent intake were significantly and positively related to the number of classes taken regardless of regression adjustment (p=0.00).
When comparing results by class, participants showed significant differences only in FAB scores. The levodopa dosage, number of classes taken, and time between assessments were not statistically different between members of different exercise classes.
Conclusion: Performance gains in balance (FAB scores) are optimistic outcomes. Increasing sample size to improve normality and linearity of data will enhance assessment of relationships.
COMPREHENSIVE CARE: Alternative & complementary therapies/ Creativity
LBP15.01
1 Nova Southeastern University, College of Osteopathic Medicine, United States
2 Nova Southeastern University, United States
3 International Association for Human Values, United States
4 St Lukes Health System, United States
Introduction: Parkinson's Disease (PD) is a neurodegenerative condition with common symptoms including tremor, stiffness, imbalance, sleep disturbance and fatigue. Stress is a significant exacerbator of PD symptoms and is also experienced by care partners (CP). The SKY Breath and Meditation practice (SKY) has been documented to reduce symptoms of stress and anxiety, and improve sleep. No published research exists evaluating using SKY in those diagnosed with PD. The purpose of this study is to determine the feasibility and efficacy of SKY on the psycho-physiological well-being in individuals diagnosed with PD (iPD) and CPs. Methodology: The IRB 2024-434-NSU was approved. This mixed methodology feasibility study evaluated the effects of SKY in a cohort of iPDs and CPs using measures of quality of life, stress, anxiety, fatigue, and affect. The standardized SKY technique was modified for the iPDs to avoid fatigue. The program consisted of 2 phases. Active Learning Phase 1 was a 10-12 hour in person training (4 day morning program) that was delivered to the iPDs and CPs separately. Practice Phase 2 consisted of daily home practice accomplished via audio recording, handout or virtually live instruction for 6 weeks. At the end of week 1, participants also attended an in-person session to reinforce the technique. Additionally, iPDS and CPs were instructed to practice SKY daily and to attend the mandatory live weekend instructor guided session. Participants logged their daily breathwork practice. Validated measures included MDS-UPDRS, Parkinson's Quality of Life Questionnaire, Parkinson Anxiety Scale, Parkinson Disease Fatigue Scale, Perceived Stress Scale, Positive and Negative Affect Schedule and Parkinson's Disease Carer Questionnaire. Measurements were taken pre-intervention, week 2, and post-intervention. RedCap was used to collect the data. Focus groups were conducted post-intervention to share participants’ experiences. Qualitative data is being analyzed by MAXQDA software. Quantitative data is being analyzed using repeated measures ANOVA with p ≤ 0.05. Results: Twenty iPDs and 8 CPs were consented and participated. Preliminary quantitative data analysis showed improvements in the majority of outcomes. Qualitative data analysis showed improvements such as lowered medication usage, sleep quality, interpersonal relationship quality, and self-efficacy. Conclusions will be available prior to the conference.
COMPREHENSIVE CARE: Lay/professional health literacy & Public thought
LBP16.01
1 Pontificia Universidad Católica del Perú, Peru
Background: In Peru, the lack of formal long-term care infrastructure means that Parkinson's Disease (PD) management relies heavily on informal female caregivers. These women navigate a complex emotional landscape defined by two phenomena: anticipatory grief, the distress of witnessing the inevitable progression of PD; and ambiguous loss, where the patient is physically present but cognitively or personality-wise "absent." This study explores these experiences and identifies systemic gaps in health literacy and psychological support.
Methods: Using a qualitative approach, we conducted narrative life history interviews and focus groups with female informal caregivers in Lima, Peru. The study focused on their perception of PD progression, their emotional coping mechanisms, and their interaction with the healthcare system.
Results: Most caregivers manage multiple unpaid roles without formal training in PD care. A dual emotional burden was identified: anticipatory grief linked to the loss of future plans and ambiguous loss triggered by the fluctuating nature of PD symptoms (on/off periods and cognitive decline). Resilience is linked to the quality of preexisting bonds, yet it is often undermined by social isolation. There is a critical deficit in health literacy; caregivers often do not understand PD non-motor symptoms, leading to high levels of "medical uncertainty" and distress. Institutional support is nearly non-existent. Public health protocols in Peru do not address the caregiver’s mental health needs or provide tools for managing the specific grief associated with neurodegenerative decline.
Conclusions: To build future-focused health systems, we must recognize informal caregivers as vital actors. Integrating health literacy and specific psychological interventions for ambiguous loss and anticipatory grief into primary care is essential. This shift from patient-centered to family-centered care is a priority for gender equity and the sustainability of Parkinson's care in the Global South.
LBP16.02
1 University of Rochester, United States
The experiential learning experience, titled A Day in the Life of Parkinson’s, at the University of Rochester School of Nursing, is meant to give insight to nursing students on real-life scenarios that patients with Parkinson’s Disease (PD) encounter, including medication management, mobility challenges, and emotional support. Nursing students engage in activities such as planning out weekly administrations of common PD medications, assisting with activities of daily living (ADLs), participating in movement exercises and face the challenges of going out into the public eye. Emphasis is placed on fostering empathy and patient-centered care through role-playing exercises that highlight the physical, emotional, and social elements of PD. Discussion is also conducted regarding the family care giver role in caring for those with PD. After the experiential learning experience is complete, students write a detailed reflection on their thoughts, feelings and overall key takeaways from the day.
At The University of Rochester School of Nursing we have represented what the Parkinson’s Foundation has accomplished, through their “Patient Experience” booth at sponsored events. Research on the progression of the disease, led participants through various activities to promote what patients with PD experience. This has shown to be impactful for participants as these activities highlight the physical, mental and emotional components of PD. (Parkinson’s Foundation. (12/24.)) By preparing nursing students with comprehensive knowledge about PD, these educational efforts are preparing future healthcare professionals to provide more empathetic, informed, and effective care to patients and their caregivers living with Parkinson's disease.
References
Keep on moving! Parkinson’s Foundation. (2024, December 30). https://movingdaywalk.org/event/moving-day-rochester-ny/
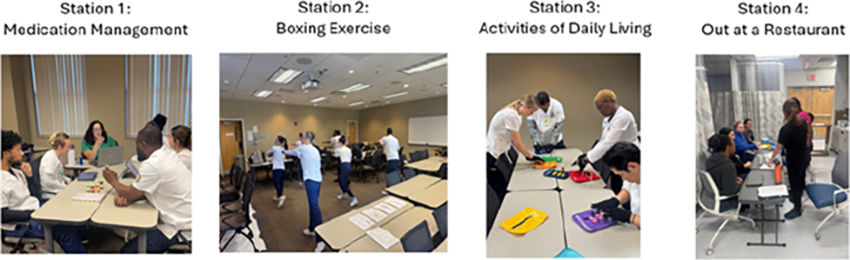
LBP16.03
1 Richard Novati Catholic Hospital, Ghana
INTRODUCTION (i)Background A knowledge gap about Parkinson's disease (PD) often exists amongst healthcare professionals who have the first responsibility to champion awareness of the disease. The level and accuracy of knowledge of a disease can influence attitude and perceptions about the disease. Although, PD is not a common everyday hospital presentation, increased awareness of this information deficit can help stakeholders identify interventions that will improve healthcare personnel's knowledge, attitudes and perceptions about PD.
(ii)Objectives To evaluate general understanding or knowledge, attitudes and perceptions of PD among healthcare professionals and identify knowledge gaps amongst same using a convenience questionnaire.
METHODS A convenience sample survey was carried out among healthcare professionals of the Richard Novati Catholic Hospital, Sogakope, Ghana.This survey included multiple-choice questions and rating-scale questions. The results were collated and analyzed.
RESULTS Of the 59 subjects surveyed and on the PD knowledge questions, most questions were answered correctly except the question on whether PD is curable and which 65.5% respondents answered correctly PD is not curable and about 29.2% believe PD is curable and 5.2% did not know the answer. On the attitude questions, only about 39.7% agree they have the confidence in diagnosing PD. About 38.6% agree they have the confidence in managing patients with PD. About 26.8% agree that caring for patients with PD is burdensome. About 73.2% strongly agree their willingness to undergo further training on PD. About 61.4% strongly agree PD management should be prioritized in the district hospitals. Finally, on the perception questions, about 39.7% of respondents strongly agree that patients with PD face stigma in Ghana. About 35.1% strongly disagree that district hospitals in Ghana have adequate resources to manage PD patients. About 71.9% of respondents agree that community misconceptions delay patients from seeking care.
Conclusion Misconceptions about PD among healthcare personnel stems from their perceptions about the disease despite some academic knowledge of the disease. This affects attitudes to managing patients with PD. Identification of this knowledge and attitude gap is vital towards allocating education resources, and the findings described herein will form the basis for effective educational interventions for healthcare personnel on PD.
COMPREHENSIVE CARE: Disability and quality of life
LBP17.01
1 Auburn University, United States
BACKGROUND: Relatedness, a basic psychological need within Self-Determination Theory (SDT), is central to motivation and emotional well-being and may be especially critical in Parkinson’s disease (PD) support group settings, where shared experience and interpersonal connection are foundational. Individuals with PD often experience reduced personal agency and social participation, reflecting thwarted psychological needs. Although SDT has been widely applied in health and rehabilitation contexts, little research has examined if PD support groups foster relatedness. This study investigated the psychosocial impact of a PD support group offering multidimensional support, including exercise, educational programming, and social connection, and examined how support valuation influences relatedness.
METHODS: Eleven adults with PD who attended at least one local PD support group meeting in the past year completed a survey assessing relatedness, depressive symptoms, disease severity, and perceived value of support types (informational, social, exercise). RESULTS: Participants reported high levels of relatedness (M = 44.1, SD = 7.9) and, on average, minimal depressive symptoms (M = 3.1, SD = 2.5). Informational support was most frequently identified as the most valued support type (n = 8), followed by social support (n = 3). Although not statistically significant, there was a trend toward a group difference in relatedness based on support valuation, F(1,9) = 4.84, p = .055, such that participants who valued social support most reported higher relatedness (M = 51.3, SD = 5.5) compared to those who valued informational support most (M = 41.4, SD = 7.0).
CONCLUSIONS: These findings suggest that while informational support is often prioritized by individuals with PD, social support may play a particularly important role in fostering relatedness within support group settings. Participants who valued social support reported higher relatedness, highlighting the importance of interpersonal connection alongside education. Designing support groups that intentionally cultivate social connection may enhance basic psychological needs while still providing multidimensional support. Larger samples are needed to better understand how support types influence feelings of connection and to inform the design of PD programs.
This work has been accepted for a poster presentation at the annual meeting of the Southeast region of the American College of Sports Medicine on February 27, 2026.
LBP17.02
1 PD Avengers, Canada
2 Department of Neurological Surgery, Weill Cornell Medicine, New York, NY, United States
3 Russell Sage College, Albany, NY, United States
4 _, United States
5 University of California San Francisco, San Francisco, CA, United States
6 Cure Parkinson’s, United Kingdom
Parkinson’s disease (PD) affects physical function, appearance, and daily activities, which may profoundly impact self-image and identity. These effects may be particularly important for women; yet remain poorly studied. The Female Health and Home Life Survey was developed and implemented through the Fox Insight platform to assess women-specific experiences in PD, including the impact of PD on self-image. The survey included 3,589 women with PD (mean age 67.6 years; mean age at diagnosis 60.0 years). Analyses were conducted across the full cohort and stratified by age at diagnosis (young-onset PD ≤50 years [YOPD] vs late-onset PD [LOPD]), menopause stage at diagnosis, and disease duration (≤3 years, 3–10 years, >10 years). Overall, 57.5% of women reported that PD negatively affected their self-image. This impact was greater in YOPD compared to LOPD (63.6% vs 57.2%) and highest in women diagnosed during peri- (70.2%) and pre-menopause (64.6%) compared to post-menopause (56.7%). The negative impact increased with disease duration, affecting 55.1% of women diagnosed ≤3 years, 59.4% at 3–10 years, and 66.2% at >10 years. Motor symptoms were the most frequently reported contributors, followed by speech changes, dyskinesia, facial masking, urinary symptoms, and body changes. YOPD women reported greater impact from rigidity, dyskinesia, and weight changes, while urinary incontinence and drooling were more frequently reported by LOPD women. Menopause-stage differences were observed. Rigidity was reported more frequently in pre- and peri-menopausal (11.3–11.5%) vs. post-menopausal women (9.4%), weight gain in pre-menopausal (6.9%) vs. peri- and post-menopausal women (4.7–4.9%), and urinary incontinence more frequently in post-menopausal (8.4%) vs. pre- (5.9%) and peri-menopausal women (7.1%). Most symptoms increasingly affected self-image with longer disease duration, including body-related changes such as dry skin, hair changes, weight changes, and urinary symptoms; while, tremor impact remained stable. PD negatively affects self-image in most women, particularly those diagnosed younger, during menopause transition, and with longer disease duration. These findings identify self-image as an important and under-recognized component of PD impact and underscore the need for improved, women-centered care addressing physical, psychological, and quality-of-life outcomes.
COMPREHENSIVE CARE: Health accessibility/ Underserved populations
LBP20.01
1 LSVT Global, United States
2 Emma Shah SLT, United Kingdom
3 The Nairobi Hospital, Kenya
4 Poonam Shah, SLT, Kenya
5 Jinagna Shah, SLT, Kenya
Parkinson’s disease (PD) is the fastest-growing neurological disorder globally, with cases projected to more than double by 2050, disproportionately affecting low- and middle-income countries (Su et al., 2025). People with Parkinson’s (PWP) in countries like Kenya face significant stigma, often rooted in poor awareness, supernatural beliefs, and misinterpretations of symptoms (Fothergill-Misbah, 2023). Stigma for PWP may be exacerbated by communication impairments such as soft voice, mumbled speech, and facial masking, which can lead to which can lead to isolation and withdrawal from social interactions (Miller et al., 2006). These challenges highlight the need for accessible and culturally responsive evidence-based speech treatments that address both the physical and social impacts of communication in PWP.
Through collaboration with the Association of Speech and Language Therapists Kenya (ASLTK), our collective goal was to explore how to make evidence-based speech treatments, like LSVT LOUD, accessible to speech-language therapists (SLTs) and PWPs alike.
A pilot LSVT LOUD treatment program was held at Inspire Wellness Center, Ltd. in Nairobi under the direction of seasoned LSVT LOUD SLT Emma Shah. Seven clients with PD underwent assessments and trial therapy over one week. Clients demonstrated measurable improvements in vocal loudness, with many reporting enhanced communication effectiveness at home. One client shared, “I am speaking now like a Kenyan who is not sick.”
Cultural adaptations played a critical role in the program’s success. For instance, ten languages were used including Kikuyu, Kiswahili, Kimeru, Gujarati, French, Kalenjin, Dholuo, Kikamba, Kikisii and English. Challenges included limited resources for printing materials, translating assessment tools, and scheduling issues due to travel constraints.
At this time, 15 SLTs from the ASLTK have been trained in LSVT LOUD and full implementation of the 16-session protocol is underway. Data from these sessions will be shared along with adaptations required to successfully implement LSVT LOUD in Keyna. We will also provide strategies and resources to raise awareness, educate, and offer practical, evidence-informed speech exercises for PWPs who live in remote villages or who experience other barriers to accessing the full treatment protocol. Attendees will gain practical insights into training clinicians in underserved regions and the need to tailor interventions to align with cultural contexts.
LBP20.02
1 Auburn University, Costa Rica
2 Auburn University, United States
Background: Gait and mobility impairments are well-established consequences of Parkinson's Disease (PD). However, the social and environmental factors that affect Physical Activity (PA) participation and engagement in this population are uncertain, particularly in a third-world country like Costa Rica, where access to specialized rehabilitation and community support varies significantly. This situation may create unique barriers for people with PD (PwPD), further impairing motor function and reducing independence. This study investigates how perceived social and environmental support relate to self-reported PA and functional mobility in PwPD in Costa Rica.
Methods: 9 people with PD (8M/1F; age 59 ± 8; 5 ≤ high school degree) completed a survey on five support aspects using a Likert scale: Support for independence during activities of daily living (ADLs), community, family, and hospital/clinical support. They also self-reported frequency of PA, weekly moderate activity time, and standing tolerance before fatigue (minutes). Spearman correlations were used to analyze the preliminary relationship between support factors and functional outcomes.
Results: In this pilot study, a pattern of interconnected support emerged. Support for independence during ADLs, family, and hospital support showed positive correlations (r = 0.81, 0.67, 0.83; p ≤ 0.05, respectively), suggesting that these resources work together and that PwPD with strong family support also tends to benefit from greater clinical and independence support during ADLs. Support factors are also linked to PA outcomes. ADLs and Family support are moderately related to time spent in PA (r = 0.63, 0.66; p > 0.05), showing that emotional and independence support may enable longer exercise sessions. Community support had a stronger association with performing PA with others (r=0.79, p=0.01), suggesting that social belonging is a key to exercise engagement among PwPD. Preliminary trends suggest that longer PA sessions are associated with greater standing capacity before fatigue (r = 0.46).
Conclusions: This study shows how support factors promote PA engagement, potentially improving standing tolerance in PwPD. Understanding social and environmental influences helps identify how external conditions facilitate or obstruct mobility in developing countries such as Costa Rica. This knowledge is crucial for future interventions that foster community support to motivate PwPD to engage in PA and promote independence.
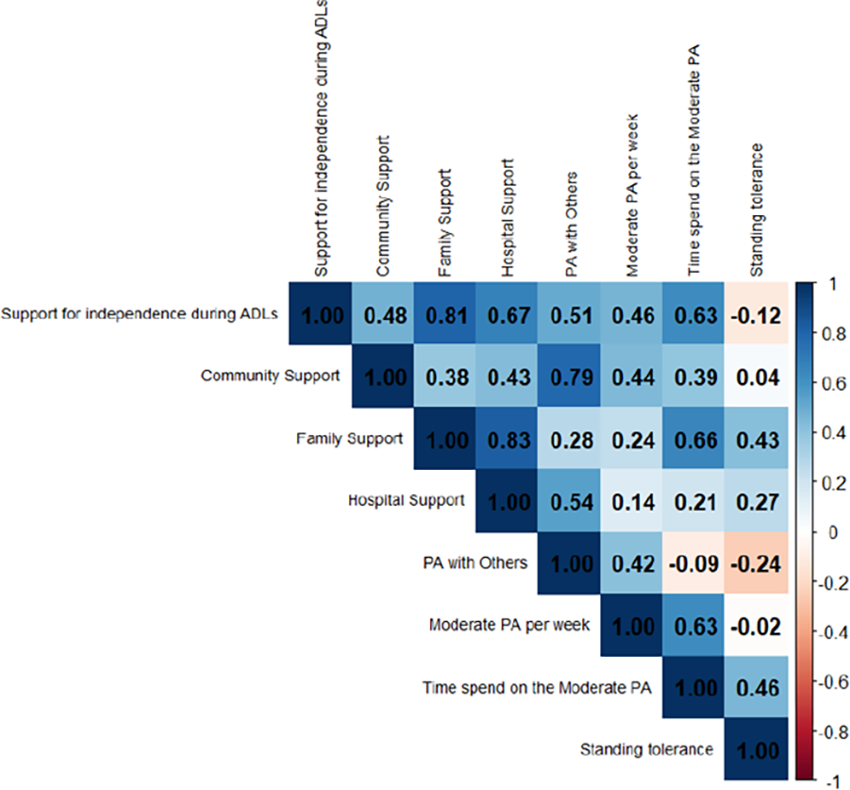
COMPREHENSIVE CARE: Self-management, empowerment, coping strategies
LBP23.01
1 PJ Parkinson's, United States
Parkinson’s Disease (PD) is a progressive neurodegenerative disorder accompanied by bradykinesia and rest tremors. PD motor symptoms fluctuate from day-to-day, which not only impacts the quality of life in PD patients, but also imposes a challenge on healthcare providers, as they would need data beyond a simple visit to gain an in-depth understanding of the disease in their patient. Furthermore, PD may result in frequent changes in prescribed medications, where non-adherence can cause the patient harm. PD has been recognized as the “fastest growing neurological disorder in the world,” with the amount of people expected to be living with PD worldwide projected to increase 112% from around 12 million patients in 2025 to 25.2 million by 2050. With the projected increase in PD prevalence worldwide, mobile health applications can monitor fluctuating symptoms and document patient adherence to their treatments, especially since 91% of Americans own a smartphone (∼96% for people under 50 years old and 78-90% for Americans over 50 years old). Despite the potential of smartphones to improve PD management, bradykinesia and tremor side effects present barriers to using the applications consistently. For example, as uncovered by usability studies, small buttons and icons, small fonts, dropdown menus challenge how PD patients interact with and understand a mobile application. Therefore, mobile health applications focused on PD management see high attrition rates, with Lee et al., 2025, finding that ∼40% of patients stopped after 6 weeks and ∼60% of patients stopped after 10 weeks. This study aims to develop a mobile health application that can maintain consistent usage from PD patients after 6 weeks, so they can learn how to build habits and manage their fluctuating PD symptoms and treatment. Specific features include incorporating a motor-accessible interface design for PD patients, direct prompts to the PD patient, the endowment effect, and social rewards. Usability studies and contextual inquiries with PD patients at PJ Parkinson’s will be conducted to uncover challenges associated with current PD management apps. Then, the management application will be developed in co-creation with patients. Finally, the application would be deployed in a controlled setting during PJ Parkinson’s treatment sessions, where the frequency and duration of app usage will be measured to assess the effectiveness of the software application in maintaining engagement and building habits.
LBP23.02
1 Radboud University Medical Center, Donders Institute for Brain, Cognition and Behaviour, Department of Neurology, Center of Expertise for Parkinson’s and Movement Disorders, Netherlands
2 Radboud University Medical Center, Research Institute for Medical Innovation, Department of Neurology, Center of Expertise for Parkinson’s and Movement Disorders, Netherlands
BACKGROUND: People with Parkinson’s disease (PwP) are faced with progressive motor and non-motor impairments that profoundly affect their functioning in daily life. A promising approach to empower PwP is to strengthen self-management skills: the ability to manage symptoms, treatments, physical and psychosocial consequences, and a healthy lifestyle. However, the development of personalized self-management interventions for PwP is hindered by insufficient insight on its determinants. This study investigates disease-related determinants of self-management.
METHODS: We analyzed cross-sectional data from 337 participants in the Dutch PRIME-NL cohort. Self management was evaluated using the 13 item Patient Activation Measure (PAM 13), which assesses knowledge, skills and confidence for self-management of one's health. Disease progression (disease duration), depressive symptoms (Beck’s Depression Inventory-II), anxiety (State-Trait Anxiety Inventory), apathy (Apathy Evaluation Scale-12PD), cognitive performance (tele-MoCA), motor symptom severity (MDS-UPDRS part II), autonomic dysfunction (SCOPA-AUT) were included as candidate determinants. We used linear regression analyses to examine associations of each potential determinant with PAM-13 scores, in two analysis blocks: (i) adjustment for age and gender; and (ii) a multivariable model in which all candidate determinants were adjusted for each other.
RESULTS: In age- and gender-adjusted models, the following determinants were significantly associated with lower self-management: longer disease duration, and worse apathy, depression, anxiety, cognitive performance, motor symptoms and autonomic dysfunction. In the multivariable model, only apathy (β=0.91, SE=0.12, p<0.001), anxiety (β=-0.16, SE=0.05, p=0.003), older age (β=-0.18, SE=0.09, p=0.049) and gender (β=-4.09, SE=1.31, p=0.002) remained independently associated with self-management. The model explained 32% of the variance in self-management.
DISCUSSION: These cross-sectional results suggest that apathy and anxiety are central disease related determinants of self management in PwP. This highlights the potential to address motivational and emotional symptoms when fostering self-management in PwP. Given the cross-sectional nature of the current analyses, some caution is warranted in the causal interpretation of these data. These results will be integrated with an ongoing longitudinal analysis of self-management trajectories in PwP in the PRIME-NL cohort.
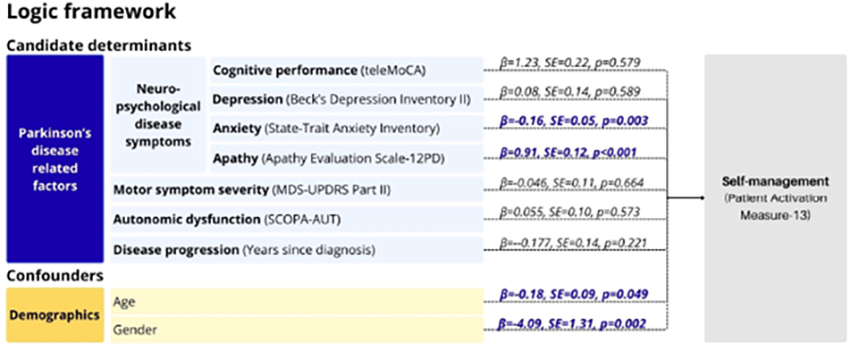
COMPREHENSIVE CARE: Multidisciplinary/Interdisciplinary teams
LBP24.01
1 North York General Hospital, Canada
2 University of Toronto, Canada
Introduction: Parkinson’s disease (PD), the fastest-growing neurological disorder globally, predominantly affects those aged 65+ (82% per Canadian Ontario Brain Disorders Report). This observational study evaluated a group-based interprofessional PD education program, preceded by individualized consultation, for improving quality of life (QoL), self-management knowledge/confidence, and lifestyle behaviors (medication adherence, exercise, sleep, stress reduction) in older adults with PD.
Methods: Patients referred to North York General Hospital’s Fanny Bernstein Living Well with Parkinson’s program received a one-time consultation by physiotherapist based on fall risk concerns and pharmacist with 18 years PD experience to address barriers by collaborating with physicians (e.g., sleep disorders, mood, orthostatic hypotension, pain, motor fluctuations etc.) Exclusions: MMSE <20, Hoehn & Yahr ≥4, language barriers, consent refusal. The 8-week program (2-hr weekly sessions, in-person/virtual) included (1) interprofessional presentations/discussions (PD diagnosis and symptoms, treatment, emotional well-being and mindfulness, cognition, nutrition, future care planning and care-partner support); (2) physiotherapist-led exercises (balance, gait, flexibility, movement strategies for daily living and fall prevention); (3) goal-setting with exercise log and mobility diary; (4) peer support with alumni sharing; community PD program and support groups.
Results: 72 patients completed the study (50 male and 22 female; mean age 74.7±6.4 years; Rockwood Frailty Scale 4.4; disease duration 3.2±1.9 years; Hoehn & Yahr 2.2±0.7). PDQ-39 Summary Index improved from 45.7 (baseline) to 35.1 (3 months post; P<0.05), with reductions in depression, loneliness, anxiety, stigma, fatigue, pain. PD knowledge increased 8/20 to 17/20; self-management confidence 4/10 to 8/10; Exercise Self-Efficacy Scale 25.5/40 to 32/40; falls decreased from 31 to 7 (all P<0.05). Lifestyle gains: levodopa adherence “often”→ “almost always”; exercise “occasionally”→ “almost daily”; community PD exercise “almost never”→“≤1/week”; relaxation/sleep hygiene “never to 2/week”→“≥3/week.”
Conclusions: This 8-week interprofessional program with pre-consultation significantly improved QoL, self-management, fall risk, and adherence to medication, exercise, mental wellness, and sleep hygiene in older adults with PD.
LBP24.02
1 North York General Hospital, Canada
2 University of Toronto, Canada
Introduction: Freezing of gait (FOG) is a debilitating symptom of Parkinson's disease (PD) that increases falls, fear of falling, and loss of independence
Methods: In this randomized controlled trial, PD patients with FOG (Hoehn & Yahr II–IV; FOG ≥weekly; able to walk 10 m; MMSE ≥15; caregiver present) from the North York General Fanny Bernstein Living Well with Parkinson’s Program were allocated to intervention (n=15) or control (n=15) groups. Both groups received pharmacist-led medication optimization, PD exercise videos, and a FOG cueing sheet; patients and blinded physiotherapist (PT) assessor were masked. The intervention added a 5-week, twice-weekly 1-hour group program (max 5 patients/class) with FOG education, balance/weight-shift training, gait strategies, motor learning via video review, and task-specific practice (turning, gait initiation, doorways, transfers, entering elevator), plus progressive home exercises with a weekly exercise log.
Primary outcomes: New Freezing of Gait Questionnaire (NFOGQ); blinded FOG Assessment (FOGA) across 4 tasks (stand/walk, 360° turns, doorway passage) ± mental math distraction; Timed Up & Go (TUG); falls (past 4 weeks). Groups were balanced at baseline (age ∼75 years, PD duration ∼8 years, Hoehn & Yahr 2.8), levodopa daily dose ∼ 8 tablets/day , mild cognitive impairment with MMSE ∼23.
Results: NFOGQ improved significantly in intervention (22.7±3.0 to 16.9±5.2) vs control (22.8±3.8 to 23.5±3.7; p=3.15×10−8). FOGA scores decreased in intervention for most tasks (e.g., doorway: 1.47±0.64 to 0.87±0.74, p=0.00052; counterclockwise turn + distraction: 1.73±0.46 to 1.07±0.80, p=0.0043), with shorter completion times (all tasks + distraction: 200.8±120.2 s to 136.1±70.1 s, p=0.0002). TUG improved (38.9±31.8 s to 27.3±16.6 s, p=0.0018) despite longer baseline. Controls worsened (e.g., all tasks time: 151±210 s to 155±121 s no distraction; 186±219 s to 269±250 s + distraction). Falls: 3 intervention vs 10 control (p=0.027).
Conclusions: A structured, motor-learning-based group program significantly reduces FOG severity, improves mobility, and lowers falls in high-risk PD patients compared to self-directed resources.

COMPREHENSIVE CARE: Rehabilitation sciences (PT, OT, SLP)
LBP25.01
1 University of Utah, United States
Purpose: The SPEAK OUT!® Therapy Program, developed by Parkinson Voice Project, is a standardized speech therapy program that helps individuals with Parkinson's disease (PD) improve dysarthric speech. Through individual and group therapy, the program targets increased loudness, clear articulation, breath support, vocal quality, intonation, and facial expression. The effectiveness of the program was first demonstrated in a peer-reviewed publication in 2020 (Behrman et al., 2020). That study reported speech benefits of 40 individuals with idiopathic PD who completed four weeks of SPEAK OUT! therapy. Following therapy, the authors reported significant increases in mean intensity, variation of intensity, variation of fundamental frequency, and cepstral peak prominence. The participants from this original study have been followed for seven years, and we now report a longitudinal perspective of the benefits of the SPEAK OUT! Therapy Program.
Methods: From the 40 participants reported in Behrman et al. (2020), 12 participants are still alive and active in the SPEAK OUT! Therapy Program. Active participation means they attend weekly speech therapy group sessions and practice at home daily. These participants completed additional speech assessments at 1 year, 2 years, and 7 years following their initial enrollment in the original study. Each assessment included sustained vowel production, reading “The Caterpillar Passage”, spontaneous speech monologue, and patient-reported outcomes using the Voice-Related Quality of Life instrument.
Results: Participants who remained in the SPEAK OUT! Therapy Program maintained improvements in intensity, fundamental frequency, and cepstral peak prominence. After 7 years of treatment, the improvements from baseline were still significant in vocal intensity (t = 5.493, p < 0.001), standard deviation of fundamental frequency (t = 3.836, p = 0.003), and CPPS (t = -3.531, p = 0.005).
Discussion: This longitudinal study reports outcomes of individuals in the SPEAK OUT! Therapy Program after 7 years of participation. This presentation will highlight the detailed acoustic changes from baseline to 1 year, 2 years, and 7 years later. These data contribute to the evidence that SPEAK OUT! is an effective program for treating hypokinetic dysarthria secondary to idiopathic PD.
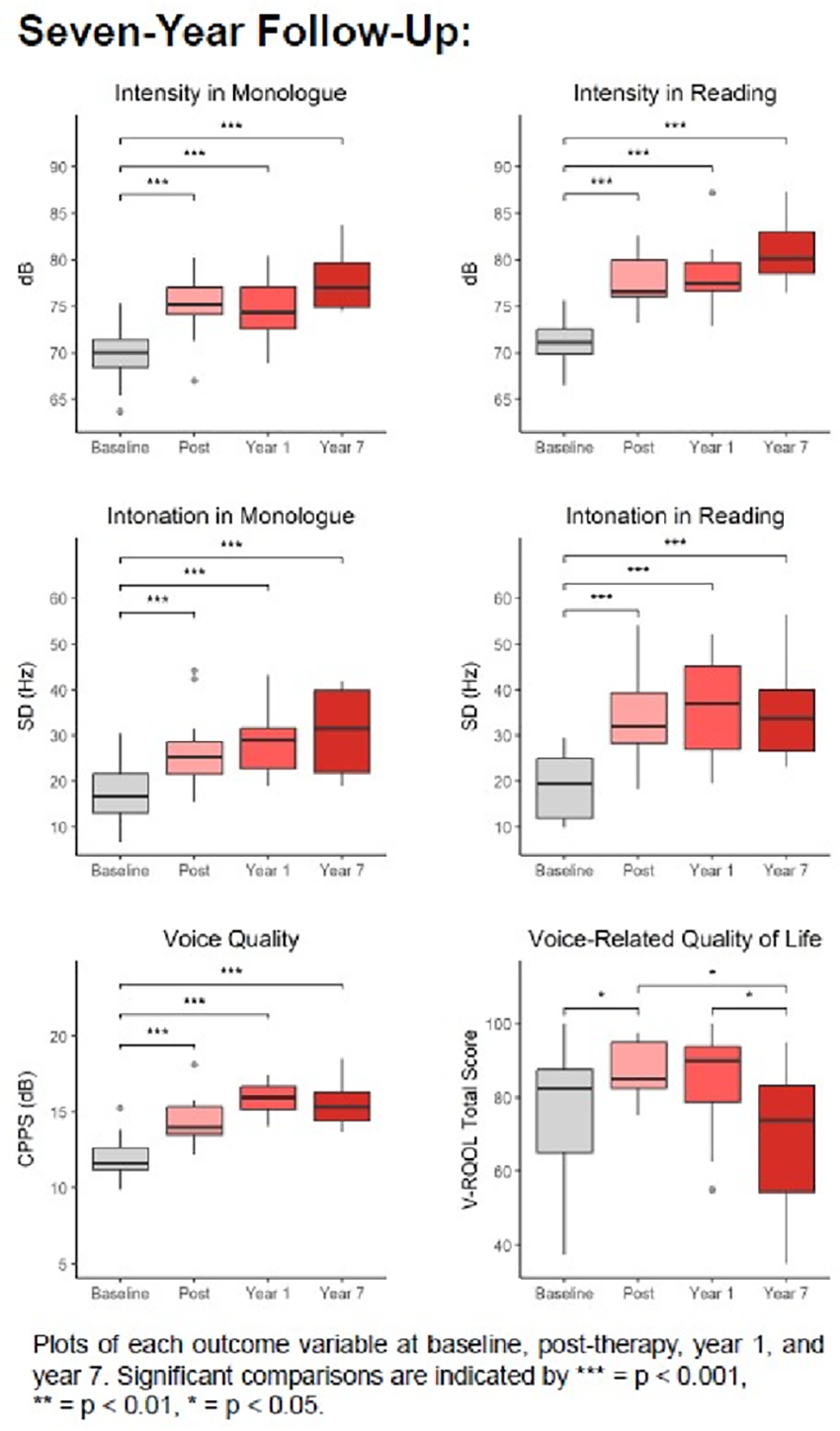
LBP25.03
1 California State University, Fresno, United States
Background: Turning is one of the major causes of falls in persons with Parkinson’s Disease (PD). Despite the high prevalence, there is limited literature on interventions to ameliorate turn mechanics. A possible avenue is to provide interventions across postural control, gait agility, and turning activities. The purpose of the study was to discover if multimodal interventions would improve turning mechanisms in persons with PD.
Methods: The study implemented an ABA intervention protocol with the following outcome measures: Fullerton Advanced Balance Scale (FAB) and a computerized gait mat that analyzed gait velocity and turning mechanics. Interventions included three modules: flexibility and agility training, postural control, and gait/turning interventions, delivered 2 times per week for 8 weeks. Statistical analyses were repeated-measure ANOVA for gait velocity and the Friedman’s test for the FAB. Turning mechanics was analyzed via descriptive analysis. The protocol was approved by the University Human Subjects Committee with each participant signing a consent form.
Participants: There were 10 participants recruited from the local community. Mean age= 69.9, SD 6.1, 8 males and 2 females, with participants ranging from Hoehn and Yahr stages I -3.
Results: FAB scores showed significant results, χ2(2) = 6.82, p = .03, with a Bonferroni correction revealing significance between test 2 and 3, Z= -2.46, p = .014, and a large effect size r =0.77. For gait velocity, the results were significant, F(2,14) =12.094, p < .001, revealing a moderate effect size, η2p = 0.63. Post hoc analysis showed significant differences between test 1 and test 3 under the Bonferroni adjustment, p = .003. Nine of the 10 participants showed adaptations during a 90-degree turn: 40% improved their step strategy, 20% reduced the number of steps during a turn, and 40% increased step length.
Discussion: The intervention program specifically targeted postural and limb agility as the foundational mechanism to enhance motor performance during 90-degree turns. An unexpected outcome was the transition from a step-out to a crossover turn, which is the typical turn strategy for adults. Individuals with PD can vary their turns by 3 distinct methods, which suggests a possible avenue for reducing falls. Future research will need to continue investigations to replicate these findings.
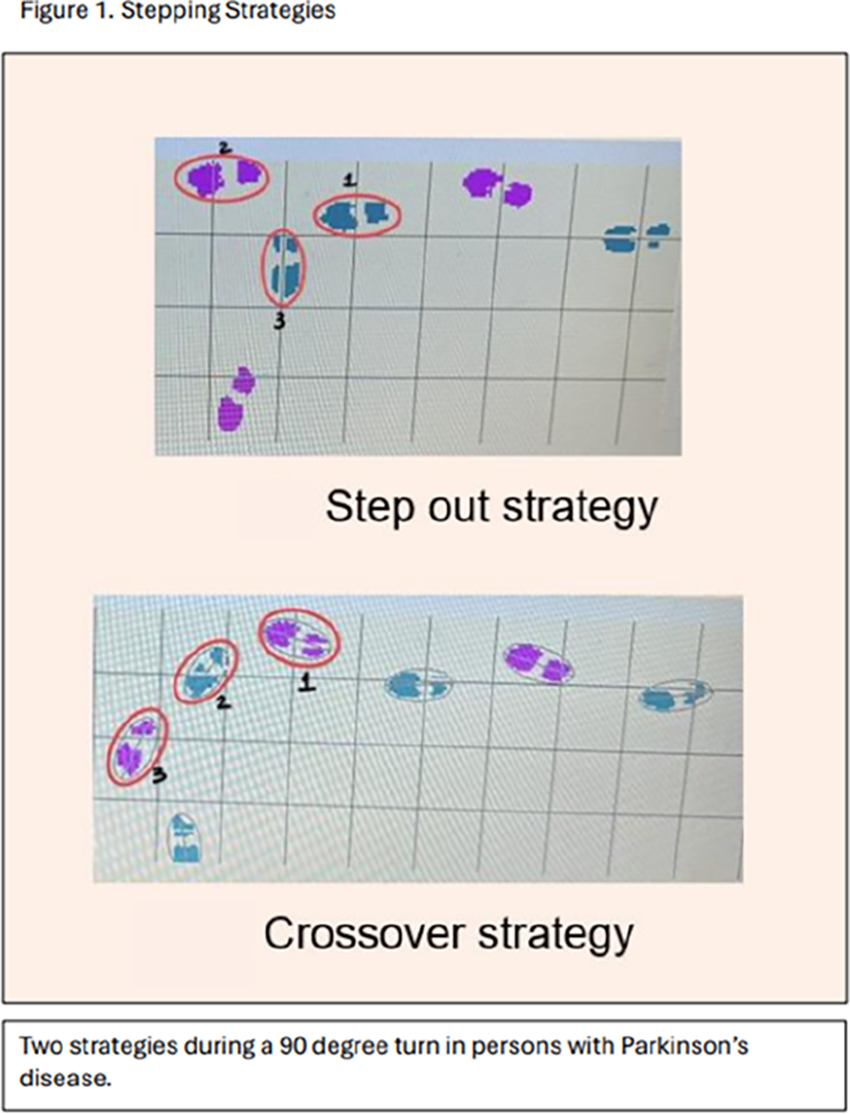
LBP25.04
1 Federal University of Goias, Brazil
2 Baptist Theological College of Brasília, Brazil
3 Brasília School of Music, Brazil
4 CEDANS – Center for Advanced Neurological Diagnostics, Brasília, Brazil, Brazil
5 Sírio-Libanês Hospital, Brazil
6 Wells Specialized Training for Parkinson’s Disease, Brazil
7 Academia Citta (Exercise and Wellness Center), Brasília., Brazil
Parkinson’s Disease (PD) compromises motor, vocal, emotional, and social functioning, significantly affecting quality of life. Growing evidence suggests that group singing interventions can improve communication and wellbeing outcomes in neurological populations. Within rehabilitation sciences, community-based interventions integrating physiological activation and psychosocial support are increasingly recognized as valuable components of comprehensive PD care. This longitudinal pilot study examines rehabilitation outcomes of a community-based choir intervention based on principles of Neurological Music Therapy for people with Parkinson’s (PwP) and their caregivers in Brasília, Brazil. A participatory mixed-methods design was implemented in a community-based therapeutic choir initiated on October 2, 2025. Twenty-two volunteers participated (15 PwP; 7 caregivers/family members). Weekly 90-minute sessions included postural alignment, targeted respiratory and vocal exercises (e.g., lip and tongue trills, explosive consonants for diaphragmatic activation), designed to support respiratory control and oropharyngeal coordination relevant to speech and swallowing function, rhythmic stimulation, collective singing, and structured group interaction. Baseline assessments were conducted on December 20, 2025, using structured questionnaires (PwP and caregiver versions) and systematic participant observation. Measures focused on perceived vocal function, communication, emotional wellbeing, and social participation. A second assessment is scheduled for April 2026 (six months from program onset) and will incorporate salivary biomarkers (cortisol and immunoglobulin) to explore physiological correlates of sustained participation.
Preliminary findings indicate perceived improvements in vocal projection, communication confidence, emotional wellbeing, and social engagement. Participants reported enhanced self-esteem, motivation, and sense of belonging, alongside reduced social withdrawal and stigma. High adherence and caregiver involvement underscore the feasibility and acceptability of the intervention.
Structured choral participation may represent a scalable, low-cost complementary rehabilitation strategy supporting communication, respiratory-vocal function, psychosocial resilience, and quality of life in PwP. Ongoing longitudinal evaluation aims to better characterize its multidimensional therapeutic effects within multidisciplinary Parkinson’s care.
CLINICAL SCIENCES: Symptoms, signs, features & non-motor manifestations
LBP27.01
1 Merz Therapeutics, Germany
2 Department of Neurology, Medical University of Graz, Austria
3 Movement Disorder Unit, Neurology Department, Complejo Hospitalario Universitario de A Coruña, Spain
4 Movement Disorder Unit, Neurology Department, Hospital de la Santa Creu i Sant Pau, Spain
5 IQVIA, Germany
Introduction Despite available dopaminergic medications with varied mechanisms of action, up to 40% of patients with Parkinson disease (PwP) develop motor and non-motor response fluctuations (OFF episodes) within a few years of starting dopaminergic treatment. OFF episodes substantially impact quality of life but are challenging to identify due to symptom variability between patients. This study aimed to (1) identify concepts of patients’ experiences (signs, symptoms, and impacts), of OFF episodes in PwP, and (2) develop a preliminary conceptual model that depicts the experience of PwP.
Methods A targeted literature review was conducted in Medline, Embase, and Cochrane for articles published during 2015–2025 that included patient-reported signs, symptoms, or impacts before or during OFF episodes in PwP (aged ≥19 years). Identified concepts were extracted and used to develop a preliminary conceptual model. Concepts with a prevalence of ≥50% and/or reported as one of the top three most bothersome, severe, or urgent to treat were prioritized.
Results Of 1,033 identified publications that underwent abstract/title review, 65 full texts were reviewed and eight selected for data extraction. A total of 132 concepts relating to the experience of PwP during OFF episodes were identified: 64 non-motor symptoms, 24 motor symptoms, and 44 impacts. Concepts were classified into 29 concept categories. Signs and symptoms with the highest reported prevalence that were also reported among the top three most bothersome, severe, or urgent to treat by PwP during OFF episodes were fatigue (100%), tremor (85%), memory problems (80%), and difficulty walking (75%). Tremor was reported as both the most severe and most urgent to treat symptom. The most prevalent impacts were impact on leisure activities (90%), difficulty with household tasks (90%), difficulty communicating (80%), and frustration (70%). Most impacts reported among the top three most bothersome to PwP during OFF episodes were in the categories of social functioning, impact on daily activities and work, and psychological/emotional impacts.
Conclusion This study highlights the varied experiences of PwP during OFF episodes, which are shown in a preliminary conceptual model. Insights on bothersomeness emphasize the substantial burden due to both motor and non-motor symptoms and their impacts on activities of daily living. This research underscores the need for better awareness of the burden of OFF episodes and their management.
LBP27.02
1 University of Toronto, Canada
2 University of Ottawa, Canada
BACKGROUND: Parkinson’s disease (PD) is a heterogeneous disorder with diverse motor and non-motor features. Traditional subtyping based on clinician-rated or biomarker measures may overlook aspects most meaningful to people with PD (PwP). The PD Patient Report of Problems (PD-PROP), a large-scale collection of verbatim reports from the Fox Insight study, was curated using a human-in-the-loop natural language processing and machine-learning framework, enabling identification of PD subtypes grounded in patients’ experiences. We aimed to explore heterogeneity and identify data-driven subtypes in early PD using self-reported most bothersome symptoms.
METHODS: Data were obtained from the Fox Insight longitudinal study via the Fox DEN (Data Exploration Network) in July 2025, including PD-PROP, baseline demographics, and self-reported outcomes (PDQ-8, UPDRS-II, NMS-QUEST, PDAQ-15, EQ-5D-5L). We included 10,464 individuals (mean age 65.0±10.1 years; 54.5% male) with self-reported PD duration <3 years and valid baseline PD-PROP. Sixty-seven curated symptoms were classified into 30 motor and non-motor domains by consensus. Exploratory subtyping used K-means clustering with serial clustering in up to three hierarchical layers for clusters containing more than 1000 participants.
RESULTS: Among 10,464 participants with PD duration <3 years, a four-cluster solution was identified. Serial clustering was applied across two additional layers, yielding a final nine-cluster structure: Cluster 1 (Fatigue/Sleepiness, n=374), Cluster 2 (RBD/Fluctuation, n=453), Cluster 3 (Urinary Dysfunction/Tremor, n=872), Cluster 4 (Tremor/Pain, n=681), Cluster 5 (Tremor-Dominant, n=3593), Cluster 6 (Postural Instability/Dysarthria/Cognitive Difficulty, n=1103), Cluster 7 (PIGD-Dominant, n=1734), Cluster 8 (Pain/Dystonia, n=959), and Cluster 9 (Pain/Fatigue/Insomnia, n=695). The RBD/Fluctuation cluster showed the greatest cognitive impairment, non-motor burden, and poorest quality of life. Over time, the Postural Instability/Dysarthria/Cognitive Difficulty cluster demonstrated the steepest decline in quality of life.
CONCLUSION: Patient-reported symptom profiles from PD-PROP identified nine distinct PD subtypes with diverse clinical phenotypes and progression patterns. To our knowledge, this is the first study to use PROP data to systematically investigate clinical heterogeneity in PD. These findings underscore the value of patient-reported measures in capturing early disease variability.
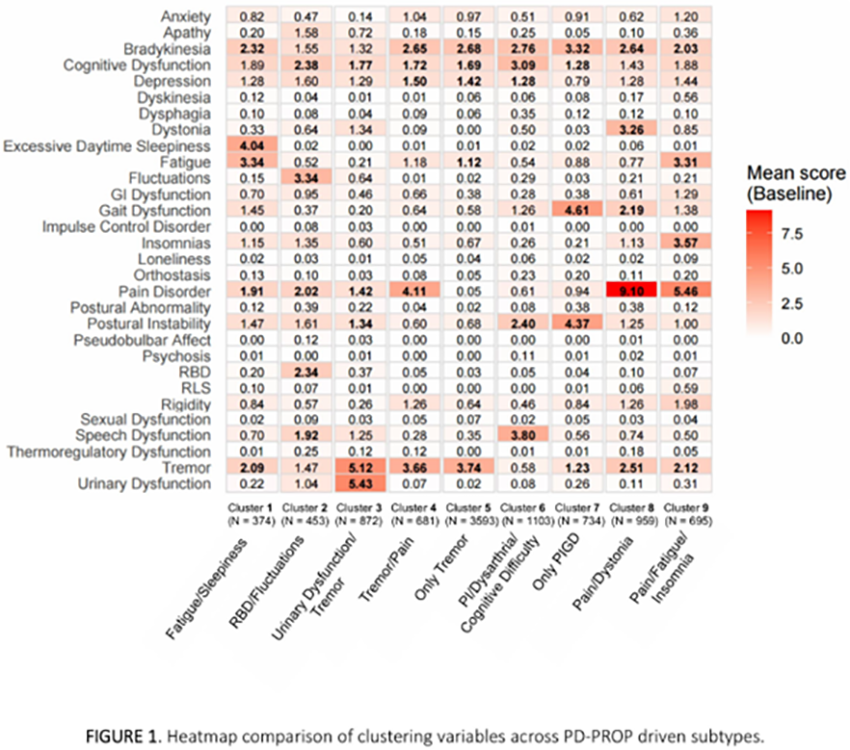
LBP27.03
1 University of Florida, United States
The pathogenesis of Parkinson’s disease (PD) begins many years before the onset of overt motor, cognitive, and behavioral symptoms. Common preclinical symptoms include constipation and bowel dysfunction. Inflammatory bowel diseases (IBD) cause chronic inflammation of the gastrointestinal tract and extraintestinal symptoms, including nervous system involvement. Attributed to the role of the gut-brain axis in PD development, IBD may be a viable preclinical marker for parkinsonism. Recent data indicate that IBD is associated with a 30% increased risk for PD. This study investigated if there are early-stage functional imaging changes in IBD. Based on prior work in early-stage PD, we aim to determine if the function of corticostriatal regions is impaired in IBD using task-based functional MRI.
Thirteen healthy controls were -age and -sex matched to IBD (n=13) individuals. All IBD participants were diagnosed by physicians at the University of Florida and have no known neurological disorders. We used a block-design unimanual grip task requiring repetitive force contractions and visual feedback to drive blood oxygen-level dependent (BOLD) activity changes. A two-way ANCOVA was conducted to analyze group differences in BOLD activity by hemisphere of the brain, covaried by age and sex.
We found decreased functional activity in IBD within the motor cortex, thalamus, caudate, anterior dorsal and ventral putamen, and posterior dorsal and ventral putamen compared to controls (pFDR < 0.05). There were no significant hemispheric or interaction effects. Our findings indicate deficits in visuomotor integration regions of the brain during the sensorimotor task. This pilot study suggests that individuals with IBD show mild motor impairments compared to controls without clinically overt motor symptoms.
CLINICAL SCIENCES: Epidemiology, genetics and risk factors
LBP29.01
1 NysnoBio, United States
2 Feinstein Institutes for Medical Research, United States
3 Juntendo University, Japan
4 Parkinson's Association of San Diego, United States
5 NysnoBioMetrix, United States
NysnoBio is advancing genetic therapies for the most common genetic early onset form of PD, Parkin-PD. Our gene therapy program has advanced to IND-enabling studies, and preparations for first-in-human clinical trials are in progress. Our WPC presentation will highlight the results of our brain imaging studies defining a specific disease network revealed by FDGPET, and results of a Parkin-PD patient survey defining patient needs beyond current therapies. First, we have recently completed a neural network imaging study identifying a specific network signature for Parkin-PD which is fully contained in the broader Parkinson’s Disease Neural Network pattern, both of which are distinct from healthy controls. This result suggests that the movement disorder that defines Parkin-PD is also disrupted in the sporadic PD neural network, indicating therapies that can ameliorate the movement disorder aspects Parkin-PD may also be useful for sporadic PD patients. Our strategy is to test our Parkin gene therapy in Parkin-PD patients, and upon demonstration of positive clinical benefit for UPDRS Part III, the therapy can be tested in the broader sporadic population. Second, we have formed a patient advocacy group for Parkin-PD patients, to better understand the practical needs of this population regarding therapeutic intervention. We will present the results of our patient survey, outlining specific needs of Parkin-PD patients, and how current treatments fail to mitigate movement disorder symptoms, and what therapeutic interventions could improve quality of life.
LBP29.02
1 bioXcelerate AI, United Kingdom
2 Cure Parkinsons, United Kingdom
Parkinson’s disease (PD) - a complex neurodegenerative disorder characterised by dopaminergic neuronal loss and Lewy pathology - remains a major unmet need in neurodegenerative therapeutics. Although large-scale genome-wide association studies (GWAS) have uncovered numerous genetic signals, substantial challenges remain in translating these loci into actionable therapeutic insights. The key difficulty lies in linking genetic signals to specific molecular mechanisms and identifying processes that may be targetable for intervention.
Recent advances in genetic colocalisation provide a powerful framework for linking GWAS signals to specific molecular traits (e.g. gene expression). Colocalisation is particularly well-suited to the complexity of PD, where disease aetiology may be shaped by interactions between genetic risk and diverse molecular layers, including transcriptomics, proteomics, and metabolomics. By assessing whether PD-associated loci share a causal variant with molecular traits, this approach enables more confident inference of biological mechanisms underlying disease risk.
Using an integrative multi-omics approach, we analysed a large European GWAS meta-analysis of PD (Nalls et al. 2019) alongside over 4,000 publicly available molecular datasets spanning e/pQTLs, spliceQTLs and metabolite QTLs from blood and brain. Through systematic causal inference analysis, we can identify molecular traits whose changes may help explain how genetic risk leads to PD.
Our analysis identified causal links between PD and more than 30 molecular traits encompassing genes, proteins, metabolites and splice variants. By embedding our findings into a PD-specific knowledge graph (KG), we constructed phenotype networks that highlighted different biological functions that may be newly relevant to PD. Protein targets such as EFNA1 and HIP1R emerged as implicated in both PD and cardiometabolic/lipid traits. Augmenting the KG with a clinician-curated list of candidate targets revealed additional links to calcium signalling and fibroblast growth factor (FGF) biology, suggesting additional mechanistic routes for further investigation.
This framework demonstrates how causal inference integrated with multi-omic data can accelerate the discovery of biological mechanisms and molecular targets relevant to PD. This layered approach enables the identification of genetically supported and mechanistically informed features that may hold promise as potential therapeutic targets in PD.
CLINICAL SCIENCES: Sleep Disorders
LBP31.01
1 Başkent University, Turkiye
2 Atatürk Sanatoryum Training and Research Hospital, Department of Neurology, Turkiye
3 Turkish Medicines and Medical Devices Agency, Turkiye
4 Unıversity of Health Sciences.Atatürk Sanatoryum Training and Research Hospital, Department of Neurology, Turkiye
5 Atatürk Sanatoryum Training and Research Hospital, Department of Emergency Medicine, Turkiye
Objective: To compare the short-term effects of levodopa–benserazide prolonged-release and levodopa–carbidopa–entacapone on subjective sleep quality in patients with idiopathic Parkinson’s disease (PD).
Methods: In this randomized, open-label, crossover study, 30 patients with idiopathic PD and nocturnal hypokinesia received levodopa–carbidopa–entacapone (100/25/200 mg) and levodopa–benserazide prolonged-release (125 mg) on two consecutive nights in randomized order. Subjective sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI) at baseline and on the morning after each treatment. Non-parametric tests were used for statistical comparisons.
Results: Median PSQI scores decreased after initiation of bedtime dopaminergic therapy, suggesting improved subjective sleep quality, although overall differences were not statistically significant. Sequence-based analysis showed a significant PSQI improvement in patients receiving levodopa–benserazide prolonged-release on the first treatment night, whereas no significant change was observed in the reverse sequence. A significant reduction in PSQI scores was found between baseline and the first treatment night. The greater improvement in the levodopa–benserazide–first sequence coincided with more frequent use of background long-acting dopaminergic therapy.
Conclusions: Short-term bedtime dopaminergic therapy was associated with improved subjective sleep quality in PD. Although levodopa–benserazide prolonged-release showed greater benefit when used as the initial treatment, this finding should be interpreted cautiously due to potential confounding from concomitant therapy. Individualized nocturnal treatment strategies may be warranted.
CLINICAL SCIENCES: Diagnosis (differential, accuracy)
LBP32.01
1 Krembil Brain Institute, Canada
2 Centre of Addiction and Mental Health, Canada
Background: Up to 62% of individuals with Parkinson’s disease (PD) experience cognitive impairment, and around 30% of patients with PD develop dementia. An early diagnosis could reduce caregiver burden and increase treatment rates. However, there is currently no standard biomarker for PD that can be used in clinical practice. Numerous studies have found that imaging is instrumental in the tracking of PD and that machine learning can assist with detection, although many machine learning models cannot be validated past the research stage. Structural MRI is useful, as it can be used to assess changes in anatomy. It is possible that MRI can be used with machine learning to distinguish stages of PD. Therefore, this research aims to 1) develop a validated MRI-based machine learning model to identify PD.
Methods: The sample includes around 1000 subjects acquired from the Parkinson’s Progression Markers Initiative. All MRI is three-dimensional and preprocessing was done through SPM and Matlab. To assess the MRI, I am using a convolutional neural network structure, which can analyze images without losing anatomical connections. Models are constructed using the Python programming language and data is split into training, validation, and test sets. The neural network model is first being created to distinguish patients with PD, healthy patients, and patients with prodromal PD. Models where most subjects classified by the model as PD also exhibit signs of PD will be prioritized.
Results: The models are currently being created and tested for the task of detecting PD and prodromal PD. I predict that the final model for this task will be able to detect subjects with PD with over 80% accuracy, and that the model will less accurately detect prodromal PD.
Conclusions: Through machine learning, I will create a model that can be adapted into clinical settings for diagnosis and assessment of PD. If my model can be implemented into clinical practice, more patients with PD may receive treatment to delay progression and reduce the effect of symptoms on the patient’s wellbeing.
CLINICAL SCIENCES: Co-morbidities
LBP33.01
1 Department of Neurological Surgery, Weill Cornell Medicine, New York, NY, United States
2 PD Avengers, Canada
3 Russell Sage College, Albany, NY, United States
4 _, United States
5 University of California San Francisco, San Francisco, CA, United States
6 Cure Parkinson’s, United Kingdom
Women with Parkinson’s disease (PD) experience unique hormonal, reproductive, and psychosocial challenges that remain under-recognized in clinical care. To better characterize women-specific experiences and unmet needs, the Female Health and Home Life (FHHL) Survey was developed and implemented through the Fox Insight platform to systematically assess women’s health experiences in PD. The FHHL Survey included 3,589 women with PD as of November 2025. Participants were predominantly White (97.5%), with mean age of 67.6 years and mean age at diagnosis of 60.0 years. Analyses were conducted across the full cohort and stratified by age at diagnosis (young-onset PD ≤50 years, YOPD; late-onset PD >50 years, LOPD) and menopause stage at diagnosis (pre-, peri-, post-menopause). As anticipated based on the known average PD age at onset ∼ 60-65 years, most participants had LOPD (95%) and were diagnosed at post-menopause (89%), with sufficient representation of YOPD (n=158), pre-menopausal (n=198), and peri-menopausal (n=176) women for subgroup analyses. Across groups, only 2.5–13.8% reported being asked by healthcare providers about menstrual cycle or menopause effects on PD symptoms, and 84–90% were not offered management strategies related to hormonal status. Hesitancy to discuss hormonal health was higher in YOPD (20.7%) and pre-menopausal women (74.9%) compared to LOPD (87.9%) and post-menopausal women (88.6%), primarily due to lack of awareness, perceived provider disinterest, or limited provider knowledge. Among pre-menopausal respondents (only responders to these questions), 50.9% used menstrual tracking apps, and 90.7% indicated willingness to use tools integrating hormonal and PD symptom tracking. Preventive care measures, including bone density screening and vitamin testing, were offered at a low rate, but comparison with the general population will be needed to draw conclusions. This large-scale survey identifies major gaps in PD care related to hormonal health and menopause. Hormonal factors are rarely addressed in clinical practice, and many women reported unmet needs and barriers to discussing hormone-related symptoms. These findings highlight the need for improved clinical education, standardized assessment of hormonal health, and development of women-specific management strategies to improve care and quality of life for women with PD.
LBP33.02
1 Washington University School of Medicine, United States
Parkinson Disease (PD) is clinically defined by bradykinesia, rigidity, and/or tremor; however, dystonia is a common and often disabling motor manifestation across the disease course. Although up to two-thirds of individuals with PD experience dystonia, its phenotypic spectrum and relationship to PD subtypes remain incompletely characterized. It is unclear whether dystonia in PD reflects a secondary motor complication or identifies biologically distinct PD phenotypes.
We conducted a retrospective cohort study to characterize clinically significant dystonia in PD using a botulinum toxin (BoNT) treatment as a proxy indicator. We identified 399 individuals with a diagnostic code (332 G20) for PD who received BoNT injections. Patients treated exclusively for sialorrhea or non-dystonic indications were excluded. At the time of this analysis, detailed chart abstraction had been completed for 172 participants; 100 individuals had clinically confirmed PD and were treated specifically for dystonia. Among these 100 participants, 48% were female. Mean age at initial PD visit was 51.75 ±8.2 years, suggesting enrichment for relatively early PD in this subgroup. Notably, age at initial injection demonstrated a bimodal distribution, raising the possibility of age-dependent dystonia phenotypes within PD. The mean age for first injection was 60.86 ± 8.2. Approximately half of the individuals received injections in a single body region, whereas the remainder received injections across multiple regions, indicating that multifocal dystonia may be more common than previously recognized. These preliminary findings highlight clinical heterogeneity in PD-associated dystonia and suggest the presence of potentially distinct age- and distribution-based subtypes. Ongoing analyses in the full cohort will evaluate temporal relationships between PD diagnosis and dystonia onset, regional distribution patterns relative to other motor features, and association with non-motor symptoms. Improved phenotypic resolution of dystonia in PD may refine mechanistic models and inform phenotypic-specific management strategies.
CLINICAL SCIENCES: Fluid and tissue Biomarkers
LBP34.01
1 ABLI Therapeutics, Inc., United States
2 Clintrex Research LLC, United States
3 ABLi Therapeutics, United States
4 Inhibikase Therapeutics, United States
5 CND Life Sciences, United States
6 Beth Israel Deaconess Medical Center, United States
7 Johns Hopkins University School of Medicine, United States
8 Johns Hopkins University Medical Center, United States
Introduction: Risvodetinib is a brain-penetrant selective inhibitor of the non-receptor Abelson Tyrosine Kinases c-Abl1 and c-Abl2. C-Abl has been implicated in the initiation and progression of Parkinson’s disease, and its inhibition correlates to histological and behavioral benefits in animal models and in humans with untreated PD. As part of the Phase 2 ‘201 Trial’, tissue and plasma biomarkers were evaluated to better understand the effect of risvodetinib on the underlying processes of neurodegeneration in placebo and risvodetinib-treated participants.
Methods: The 201 Trial (NCT05424276) was a 12-week, randomized, double-blind, placebo- controlled trial evaluating 50 mg, 100 mg and 200 mg once daily oral doses of risvodetinib in early untreated PD. The primary endpoints were safety and tolerability. Fourteen secondary endpoints evaluated motor and non-motor features of disease in the central, autonomic, enteric and peripheral nervous systems. Monthly plasma samples evaluated steady-state concentrations of risvodetinib and provided the opportunity to evaluate the effect of treatment on pathways of neurodegeneration (reviewed in DOI: 10.1002/mds.28858 ). A subset of patients volunteered for tissue biopsy enabling the analysis of the effect of risvodetinib treatment on pathological alpha-synuclein deposits within the affected neurons of disease.
Results: Alpha-synuclein pathology was substantially reduced in response to treatment as analyzed by tissue biopsy of cutaneous neurons along the length of the body. Serum samples identified Parkinson’s disease-specific upregulation of neurodegenerative pathway markers c-Abl, activated c-Abl and phosphorylated alpha-synuclein as well as the downstream effectors of mitophagy and cell-death, PARIS and AIMP2, respectively. As of this writing, the effect of risvodetinib treatment on these pathway markers remained under analysis, but are anticipated to be presented at the meeting. The reduction of alpha-synuclein pathology occurred simultaneously with a nominally statistically significant improvement in MDS-UPDRS Part II.
Conclusions: Risvodetinib is a selective inhibitor of the c-Abl kinases that has a direct effect on reduction the underlying alpha-synuclein pathology of PD. Mechanistic analysis is further elucidating how c-Abl inhibition may lead to disease-modification and/or slowing of disease progression in early untreated PD.
LBP34.03
1 Beth Israel Deaconess Medical Center, Harvard Medical School, United States
2 CND Life Sciences, United States
Background: Parkinson’s disease (PD) is characterized by progressive pathological alpha-synuclein (P-SYN) deposition in the central and peripheral nervous system. Both the Braak hypothesis and the newer Brain/Body hypothesis of synuclein proliferation suggest the gastrointestinal tract as a major portal of disease. Although multiple autopsy studies have confirmed the presence of P-SYN within the GI tract, routine sampling of tissue through GI biopsies has never achieved satisfactory utility for clinical care. The objective of this study is to develop a novel method for detection of P-SYN within superficial colon biopsies that can be obtained during routine colonoscopy.
Methods: After consent, participants with a clinical diagnosis of Parkinson’s disease (PD) who were undergoing routine colonoscopy were asked to have four superficial 3 millimeter colon biopsies taken, two from the ascending and two from the descending colon. Samples were fixed, frozen and sectioned into 50 micrometer sections. Tissue was stained for P-SYN and protein gene product 9.5. Complete confocal imaging of the slides at 20x magnification with 2 um Z-plane steps was taken through the tissue. Digital quantitative analysis of intra-axonal P-SYN deposition was measured (NerValence, CND Life Sciences).
Results: A total of 4 patients have completed colonoscopy. Two patients had a low probability of PD and two patients had a high probability of PD (based on duration of disease, response to Levodopa, comorbid clinical features, and disease confirmation by a movement disorder specialist). Both patients with a high probability of PD had a history of constipation and had multiple P-SYN positive regions within all 4 biopsies. The two patients with a low probability of PD had no history of constipation, and biopsies were P-SYN negative.
Conclusions: In this pilot study, we demonstrate that P-SYN is present in routine colon biopsy samples from patients with PD and a history of constipation. Further study is required to define the number of biopsies, location of biopsies, sensitivity and specificity, but this preliminary data strongly suggests a potential role for immunostaining of colonic tissue in the evaluation of patients with PD.
LBP34.04
1 Banner Sun Health Research Institute, United States
2 Banner Health, United States
3 BAI, Phoenix, United States
Background: Although therapeutic strategies for Parkinson’s disease (PD) have advanced considerably, reliable and objective tools to monitor symptomatic change remain limited. Assessment of motor features, particularly bradykinesia, relies largely on clinical rating scales that are vulnerable to inter-rater variability and may fail to detect subtle disease progression or treatment effects. The absence of validated fluid biomarkers that correlate with, or predict, motor severity continues to hinder accurate disease tracking and therapeutic evaluation. This study sought to identify cerebrospinal fluid (CSF) biomarkers associated with bradykinesia that could serve as objective indicators of symptomatic burden and progression in PD.
Methods: CSF (n = 1,472) samples were obtained from participants enrolled in the Parkinson’s Progression Markers Initiative (PPMI). Biomarker quantification was performed using the Alamar NULISA™ CNS panel at Banner Sun Health Research Institute. Cross-sectional and longitudinal associations between baseline biomarker levels and bradykinesia were evaluated using logistic regression and mixed-effects models, adjusting for age, sex, and PD treatment status.
Results: Participants had a mean (SD) age of 66.4 (7.0) years, and 46.5% were female. At baseline, CSF analysis identified DDC as the most significantly upregulated protein associated with bradykinesia. Longitudinal analyses demonstrated that higher CSF levels of p-TDP43, IL-2, and PGK1, along with lower CSF levels of CCL11, were associated with subsequent development or worsening of bradykinesia.
Conclusions: In this large, well-characterized PPMI cohort, we identified distinct CSF proteomic signatures associated with bradykinesia in Parkinson’s disease. CSF DDC emerged as the most robust cross-sectional correlate of bradykinesia severity, while multiple proteins demonstrated significant associations and predictive value for longitudinal progression. Notably, several biomarkers linked to inflammatory signaling, synaptic function, and metabolic pathways were associated with both current symptom burden and future development of bradykinesia. These findings support the potential utility of fluid-based proteomic markers as objective indicators of motor symptom severity and progression in PD. Further validation in independent cohorts and mechanistic studies are warranted to determine their clinical applicability for disease monitoring and therapeutic trials.
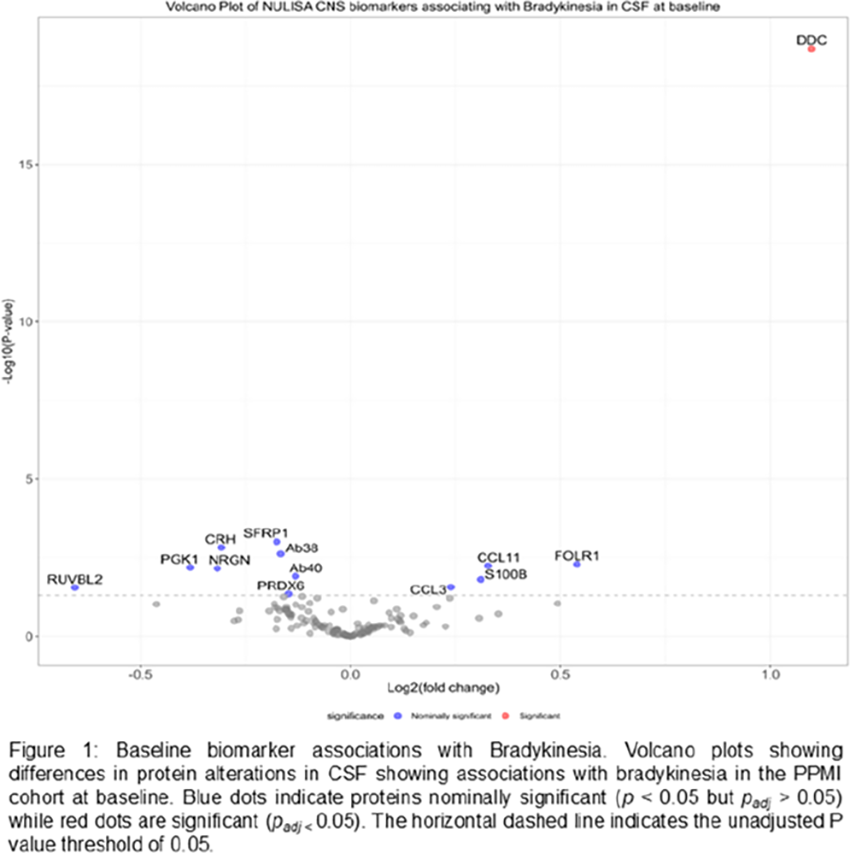
LBP34.05
1 Banner Sun Health Research Institute, United States
2 Banner Health Research Institute, United States
3 Banner Health Research Institue, United States
Background: Parkinson's disease (PD) is one of the most prevalent neurodegenerative disorders worldwide. Although its clinical diagnosis is primarily based on motor symptoms, cognitive impairment is a frequent and debilitating non-motor complication that can progress to Parkinson's disease dementia (PDD). Early identification of patients at risk for cognitive decline remains a major clinical challenge. Biomarker-based approaches offer a promising strategy for detecting early molecular changes associated with subsequent cognitive deterioration in PD.
Methods: We included n = 235 participants mean [SD] age 61.58 [9.39] years; 78 females [30.2%] from the Parkinson's Progression Markers Initiative (PPMI), all with a clinical diagnosis of PD. Among these participants, 54 mean [SD] age, 65.7 [8.2] years; 14 females [38.5%] developed cognitive impairment within 4 years of follow-up, while 181mean [SD] age, 60.4 [9.4] years; 65 females [27.84%] remained cognitively stable over the same period. Baseline cerebrospinal fluid (CSF) samples were analyzed using the NULISAseq CNS and Inflammation panels. Differential expression analyses were conducted in R.
Results: Higher baseline concentrations of multiple phosphorylated tau (p-tau) species—including p-tau231, p-tau217, and p-tau181—were observed in individuals who subsequently developed cognitive impairment. In addition, neurofilament light chain (NfL), a marker of axonal injury, was significantly elevated at baseline. Nominal differences were also observed in immune- and glial-related markers, including TREM1, CD80, IL2RB, CXCL9, and GFAP, suggesting altered immune activation and astroglial responses in individuals who progressed to cognitive impairment.
Conclusion: In this preliminary analysis of the PPPMI cohort, core Alzheimer's disease (AD)–related biomarkers—particularly phosphorylated tau species—together with NfL, emerged as the strongest predictors of subsequent cognitive impairment in PD. These findings imply coexisting AD-related pathology and axonal degeneration as key contributors to cognitive decline in PD. Furthermore, our multi-analyte proteomic approach identified parallel alterations in immune and astroglial markers, suggesting that neuroinflammatory and glial dysregulation may act synergistically with tau-mediated and neurodegenerative processes to drive cognitive deterioration in PD.

CLINICAL SCIENCES: Pharmacological therapy
LBP35.01
1 Nano PharmaSolutions, United States
Nano PharmaSolutions (NPS) is developing NT-301, a nasal powder of Apomorphine freebase (APO-FB), to treat “off” episodes Parkinson’s disease (PD) patients. Dopaminergic therapy, particularly levodopa, remains the cornerstone of PD treatment; however, as the disease progresses, many patients develop motor complications, including end-of-dose “off” episodes and dyskinesias associated with long-term levodopa use.1
Apomorphine hydrochloride (APO-HCl) is approved globally for “off” episodes via subcutaneous (SC) injection and continuous infusion pumps in the US, Europe, UK, and Australia. An APO-HCl sublingual film (KYNMOBI®), was approved by the FDA and Health Canada but later withdrawn. Sublingual delivery improved convenience but was limited by oral irritation and ulceration likely related to formulation acidity (pH ∼4), prolonged administration time (∼3 minutes hold time), delayed onset of action, and shorter duration of clinical benefit.2
Despite its efficacy, SC Apomorphine has limitations, including the burden of carrying injection devices, injection-site reactions related to the acidic formulation (solution pH 2.5–4.0)— e.g. discomfort, pain, swelling, redness, and warmth—and difficulty administering injections while motor control is impaired. NT-301 is a single-use drug–device combination containing Apomorphine freebase in a nasal powder form, offering a more convenient, tolerable, and non-invasive route of delivery. Unlike APO-HCl injectable products, NT-301 forms a neutral pH solution (∼7.2) upon dissolution.
A randomized, double-blind, placebo-controlled Phase 1 study was conducted in Australia to evaluate the safety, tolerability, and PK of single ascending doses of NT-301following antiemetic prophylaxis with domperidone. Dose-proportional systemic exposure was observed across the 1–4 mg dose range. NT-301 was generally well tolerated, with no clinically significant adverse events reported. A single instance of mild, transient nasal irritation was observed among 39 NT-301 administrations.

LBP35.02
1 H.Lundbeck A/S, Denmark
Introduction: An open-label, phase 1b trial (NCT04291859) evaluated the safety, tolerability, and exploratory clinical effects of Lu AF28996 in patients with advanced Parkinson’s disease (PD) and motor fluctuations persisting despite optimized non-invasive anti-parkinsonian medication. Lu AF28996, an oral D1/D2 receptor agonist, has a pharmacokinetic/pharmacodynamic profile that may provide sustained dopaminergic stimulation, consistent with a functional dopamine analog, to stabilize motor fluctuations. Here, we present preliminary results from a prespecified subgroup of patients with persistent OFF-time despite prior treatment optimization.
Methods: Participants were required to have ≥2h OFF-time causing significant disability (with or without dyskinesia), persisting despite prior treatment optimization attempts, with consistent medical record documentation of past/current PD medication. Participants were required to be receiving symptomatic treatment including ≥400mg/day of standard oral levodopa and ≥1 adjunct anti-parkinsonian treatment targeting motor fluctuations. Participants received Lu AF28996 twice daily for ≥41 days. Descriptive analyses based on the evaluable population as of 17/11/25 at end of up-titration period (efficacy) and across whole trial period (safety).
Results: Participants (n=22): mean age of 66 years, 10 were male and 20 Hoehn and Yahr stage 2–3 (in ON-state). Baseline mean OFF-time and mean Good ON-time were 4.4h (SD:1.6) and 10.6h (SD:2.1), respectively (standardized Hauser diary); mean MDS-UPDRS Part III score was 16 (SD:6) and mean daily levodopa dose was 847mg (SD:643).
Efficacy was assessed as change from Baseline at Week 6. Robust improvements in mean OFF-time and Good ON-time, were reported: –2.2h (SD:2.3) and 2.8h (SD:2.1), respectively. No clinical deterioration in motor function was observed (MDS-UPDRS Part-III score) despite a marked (∼40%) mean levodopa dose reduction. Treatment-emergent adverse events (AE) (≥3 participants) included nausea (n=7), dizziness (n=4), headache (n=4), vomiting (n=3); most AEs were mild, and no unexpected safety signals were observed. The safety profile was consistent with a dopaminergic mechanism of action.
Conclusions: Lu AF28996 demonstrated favorable tolerability, and robust improvements in motor fluctuations in patients with advanced PD and persistent OFF-time (≥2h) despite prior treatment optimization attempts, warranting onward clinical development in a similar patient population.
LBP35.03
1 Gateway Institute for Brain Research, United States
Parkinson’s Disease (PD) is a progressive neurodegenerative disorder characterized by the progressive loss of dopaminergic neurons, leading to severe motor and non-motor impairment. While its etiology is highly heterogeneous, most current therapeutic strategies rely on single-target interventions. With PD projected to affect 12 million people by 2050, there is a critical need for disease-modifying therapies that account for the sporadic and diverse nature of the disease, which often eludes “one-size-fits-all” clinical trial design. We developed a systematic precision-medicine framework that integrates patient-specific transcriptomics with logic modeling. This framework utilized bioinformatics tools to construct personalized transcriptomic signatures from patient samples. These signatures were mapped onto comprehensive PD-associated biological network models, which were converted into directed graphs for computational analysis. We applied ternary logic modeling to simulate disease progression and cellular state transitions. Finally, we performed in silico perturbations using publicly available drug interaction databases to evaluate the efficacy of single and combinatorial therapeutic interventions across all network graphs. The logic modeling approach successfully characterized disease-modifying changes and by ranking drug candidates based on their ability to revert personalized signatures to a control state, we identified several high-priority combinatorial targets. These computational predictions were validated against publicly available clinical study data and further confirmed in vitro using a PD injury model, where the predicted combinatorial treatments showed superior efficacy in restoring cellular viability compared to monotherapies. Our study demonstrates that combining personalized transcriptomics with logic-based network simulations can identify potent, patient-specific therapeutic strategies. By shifting from cohort-wide signatures to individualized mechanistic modeling, this approach provides a scalable pipeline for discovering the next generation of disease-modifying interventions in Parkinson’s Disease.
CLINICAL SCIENCES: Surgical therapy, including cell and gene therapy
LBP36.01
1 Xiangya Hospital & Center for Medical Genetics, Central South University,, China
2 The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, China
3 Nuwacell Biotechnologies Co., Ltd, Hefei, China, China
4 Department of Neurology, Xiangya Hospital & Center for Medical Genetics, School of Life Sciences, Central South University, Changsha, China, China
5 The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei;, China
Background Inherited Parkinson’s disease (PD) accounts for 10-15% of cases. PRKN mutations are the most common cause of autosomal recessive early-onset PD marked by early dopaminergic neuron loss. Cell replacement therapy represents a promising approach for PRKN-PD. We developed clinical-grade hypoimmune iPSC-derived dopaminergic progenitor (iDAP) cells (Product ID: NCR201) and conducted a clinical study to evaluate their efficacy in inherited PD patients. Here, we report the 6-month safety and preliminary efficacy results of one PRKN-PD patient receiving transplantation of NCR201.
Methods A 37-year-old PRKN-PD patient (onset age 22) received robot-assisted bilateral stereotactic putaminal transplantation of 4 million NCR201 cells. To complement the cell’s low-immune profile, a minimized immunosuppressive regimen was initiated intraoperatively and maintained for 6 months. Clinical efficacy was rigorously evaluated via the MDS-UPDRS, Non-Motor scale, and [18F]-FP-CIT PET imaging.
Results NCR201 consists of high purity >90% iDAPs (FOXA2+), and achieved high yield >80% of mDA (TH+) after transplantation. GLP studies confirmed a favorable efficacy, safety, and low- immune profile in rodent and NHP models.The robotic-guided procedure and minimized immunosuppression were well tolerated, with no drugs-related adverse event reported. Rapid motor recovery manifested by Day 28 after surgery. At 6 months, the MDS-UPDRS III score decreased from 39 to 10 in OFF state and from 24 to 10 in ON state, with notable resolution of rigidity and postural instability. The mean daily OFF time was eliminated at Day28 (4.5 to 0 h) and sustained through the 6 months. Improved non-motor symptoms enabled oral medication cessation and a full return to normal life by 6 months. [18F]-FP-CIT PET imaging at 3- and 6-months confirmed a significant increase in striatal radiotracer binding, providing objective evidence of successful graft engraftment and functional dopaminergic maturation.
Conclusions As the first hypoimmune iDAPs product entering clinical trial, the latest results demonstrate a favorable safety profile and robust functional recovery in one PRKN-PD patient. The close correlation between clinical improvement and restored dopaminergic neural innervation presents a prove of concept for NCR201 cell replacement therapy in PRKN-PD intervention. These preliminary findings warrants an expanded study involving more inherited PD patients with long-term observation.
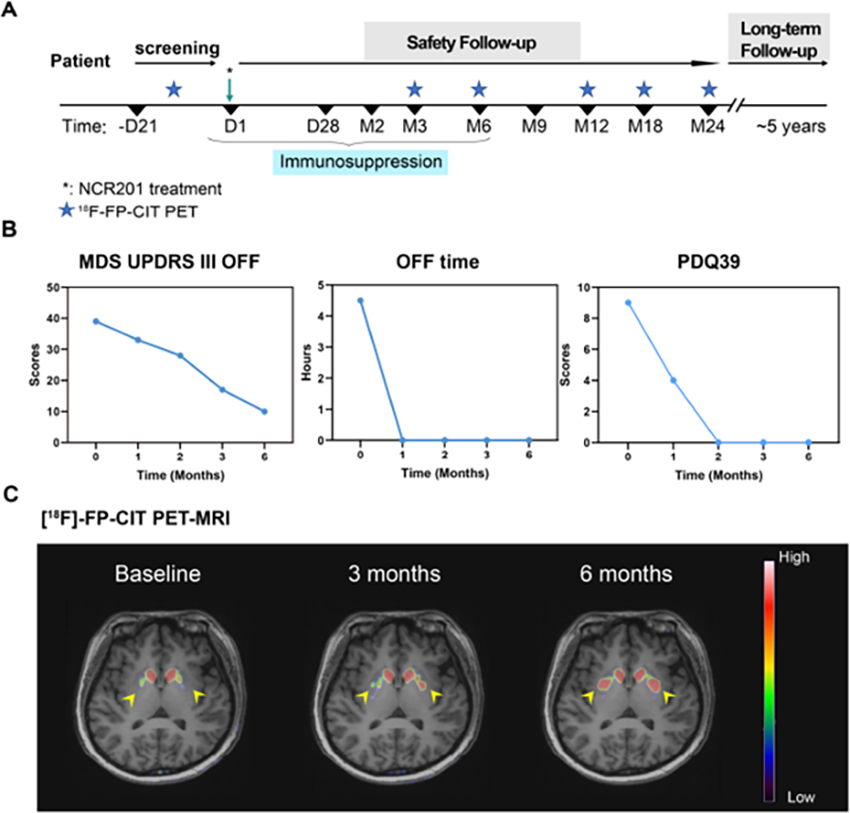
LBP36.02
1 ISSCR, United States
2 University of Cambridge, United Kingdom
3 University of California, Irvine, United States
4 University of Connecticut, United States
5 STEM-PD Trial, United Kingdom
The rapid advancement of stem cell–based approaches for Parkinson’s disease (PD) has led to increased clinical trial activity and growing interest among clinicians and patients. At the same time, the proliferation of unproven stem cell interventions underscores the urgent need for authoritative, evidence-based education to support informed clinical decision-making and patient care.
To address this need, the International Society for Stem Cell Research (ISSCR), in partnership with Harvard Medical School, developed an open-access, accredited continuing education course focused on stem cell medicine for PD. Building on prior global needs assessments in stem cell education, this disease-specific course translates emerging scientific and clinical evidence into practical knowledge for healthcare professionals.
The course is delivered as an on-demand, online program and consists of six modules. Module 1 provides an overview of Parkinson’s disease, including its history, pathology, and current standards of care. Module 2 examines competing advanced therapeutic approaches for PD, including infusion, surgical, gene, and immunotherapies, and places stem cell–based approaches within the broader treatment landscape. Module 3 focuses on the scientific basis of stem cell therapies in PD, including the rationale for dopamine cell replacement, advantages and limitations of cell-based therapies, and how stem cell–derived dopamine cells are generated and evaluated in preclinical models. Module 4 reviews the evolving clinical trial landscape, highlighting trial design and early outcomes. Module 5 explores considerations for the future adoption of stem cell–based therapies, including regulatory, clinical, and implementation challenges, and addresses the risks associated with unproven stem cell interventions. The final module centers on the patient perspective and features an interview with a participant in a stem cell PD clinical trial, emphasizing diagnosis, treatment decision-making, and lived experience one year after therapy.
This course equips clinicians, scientists, patients and their families, healthcare providers, and the science-interested public with critical knowledge to navigate the rapidly evolving field of stem cell medicine in PD and supports the responsible translation of research advances into patient care.
LBP36.03
1 Pacific Northwest University of Health Sciences, United States
Deep brain stimulation (DBS) of the globus pallidus internus (GPi) is an established treatment for advanced Parkinson’s disease (PD). While motor benefits have been well described, variability in cognitive and psychiatric outcomes suggests that electrode position within pallidal subterritories may influence patient-centered outcomes. We conducted a systematic literature review to evaluate the relationship between GPi electrode subterritory placement and cognitive or neuropsychiatric outcomes in PD.
The literature search was conducted using the terms in PubMed: (“deep brain stimulation” OR DBS) AND (Parkinson*) AND (“globus pallidus internus” OR GPi) AND (electrode placement OR contact location OR subterritory OR posterolateral OR medullary lamina OR sensorimotor) AND (“quality of life” OR PDQ-39 OR mood OR cognition). Filters included human subjects, English language, and publications from 2005–2026. Studies were included if they reported GPi DBS with defined electrode location or subregion targeting and assessed cognitive or psychiatric outcomes, even if PDQ-39 was not used. Case reports, non-human studies, and studies reporting only motor outcomes were excluded. The initial search yielded 20 studies, and 7 studies met inclusion criteria after initial screening.
Across included studies, GPi DBS was associated with stable motor improvement, while cognitive and psychiatric outcomes varied by stimulation subterritory. Stimulation of posterolateral sensorimotor regions and contacts bordering the medullary lamina was consistently associated with more favorable cognitive and psychiatric profiles. Studies utilizing imaging-guided targeting or intraoperative electrophysiologic localization demonstrated narrower therapeutic windows when stimulation extended beyond sensorimotor subregions. Although heterogeneity in methodology and outcome measures limited quantitative pooling, qualitative trends were consistent.
These findings suggest that subterritory-specific targeting within the GPi influences cognitive and neuropsychiatric outcomes in PD. Precision placement in sensorimotor regions, particularly along the medullary lamina border, may optimize patient-centered outcomes while maintaining motor benefit. Further standardized prospective studies are needed to define optimal intrapallidal targeting strategies.
LBP36.04
1 The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, China
2 Nuwacell Biotechnologies Co., Ltd, Hefei, China, China
Background Cell replacement therapy offers hope of a long-term, disease-modifying treatment for Parkinson’s disease (PD). The challenges remained to increase the yield of midbrain dopaminergic neurons (mDA) after transplantation, and to further lower the immunogenicity. We developed clinical-grade hypoimmune iPSC-derived dopaminergic progenitor (iDAP) cells and conducted clinical study (NCT06583291) to treat idiopathic PD patients. Here, we report 12-month safety and efficacy results of 7 patients.
Methods The clinical-grade hypoimmune iDAPs (Product ID: NCR201) were manufactured by Nuwacell Biotech under GMP conditions using standardized iPSC banks. Comprehensive assays were performed to ensure cell identity, purity, and safety.Eligible patients were 45 to 75 years of age, a H&Y 2 to 4, and a stable medication regimen for at least 3 months. 7 patients underwent robot-assisted bilateral putaminal transplantation of 4 million NCR201 cells, with a minimized immunosuppressive regimen initiated intraoperatively and maintained for 6-12 months. Clinical and safety evaluations were performed at baseline and predefined follow-up intervals.
Results NCR201 consists of high purity >90% iDAPs (FOXA2+), and achieved high yield >80% of mDA (TH+) after transplantation. GLP studies confirmed graft survival, and a favorable efficacy, safety, and low-immune profile in rodent and non-human primate models.In the clinical study, all 7 patients completed the 12-month follow-up. The surgical procedure and immunosuppressive regimen were well tolerated. No drug-related serious adverse events or tumorigenic growth were observed. At 12 months, the mean MDS-UPDRS III score decreased from 55.3 to 34.0 in the OFF state and from 37.3 to 30.4 in the ON state. The mean daily OFF time was reduced by 6.42 hours (from 6.85 to 0.43 hours), while Good ON time increased by 7.82 hours (from 4.11 to 11.93 hours). Improvements in non-motor symptoms were noted as early as Day 20. [18F]-FP-CIT PET imaging showed a significant increase in striatal signal intensity as early as 3 months, and persisted through 6 and 12 months.
Conclusions This clinical result demonstrated that in 7 idiopathic PD patients the NCR201 cell replacement therapy achieved functional engraftment, leading to rapid, substantial, and sustained improvements in both motor and non-motor symptoms. As the first hypoimmune iDAPs product entering clinical trial, these findings showed early promise of NCR201 as a transformative treatment for PD.

CLINICAL SCIENCES: Clinical trials: design, outcomes, recruiting etc.
LBP37.01
1 Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
2 Institute of Bioimaging and Complex Biological Systems (IBSBC), National Research Council (CNR), Segrate, Milan, Italy
3 Department of Molecular and Translational Medicine, University of Brescia, Brescia, Italy
4 School of Medicine and Surgery, University of Milano-Bicocca, Tecnomed Foundation, Monza, Italy
5 Department of Molecular Medicine, University of Pavia, Pavia, Italy
6 Department of Pharmaceutical Sciences (DISFARM), University of Milano, Milan, Italy
Background: Parkinson’s disease (PD) is driven by pathological aggregation and propagation of α-synuclein, leading to synaptic, mitochondrial, and network-level dysfunction. GBA1 mutations represent the strongest genetic risk factor for PD and are associated with earlier onset, accelerated progression, and increased pathological burden. Experimental evidence suggests synergistic toxicity between α-synuclein and tau, yet translational in vivo evidence across biological scales remains limited. SYNchronPD aims to define how α-synuclein accumulation and its interaction with tau drive neurodegeneration across molecular, cellular, and network levels, with particular focus on GBA1-associated PD, using an integrated human–animal–computational framework.
Methods: WP1 (Human) - 160 participants across preclinical and clinical PD stages, stratified by GBA1 status, undergo comprehensive clinical and neuropsychological assessment, blood-based biomarker profiling, and multimodal MRI. Tau pathology is assessed in vivo using PET with [18F]PI-2620. In a subset, skin biopsies are used to generate patient-specific hiPSC-derived dopaminergic neurons for network-level electrophysiological analyses. WP2 (Animal) - GBA-L444P/+ and wild-type mice injected with α-synuclein or α-synuclein/tau fibrils undergo behavioral testing, in vivo MRI and PET imaging, and post-mortem molecular analyses of synaptic, axonal, and mitochondrial pathology. This work package includes the preclinical validation of novel α-synuclein PET tracer ([18F]Syntacasyn). WP3 (Computational) - Multimodal data obtained from both WP1 and WP2 will be analyzed using advanced statistical and computational approaches to identify vulnerable network hubs and generate subject-specific “virtual brain” models of pathology propagation and compared on their functioning.
Status: The study started in February 2026 and has an expected duration of 36 months. Human research has been approved by the local Ethics Committee, and animal experiments by the Institutional Animal Care and Use Committee.
Conclusion: SYNchronPD provides a translational framework linking molecular pathology, brain network dysfunction, and clinical heterogeneity in PD, supporting biomarker development and precision medicine strategies in genetically defined populations.
Acknowledgment: This work is supported by the Ministry of University and Research (FIS2 - FIS-2023-00979)
LBP37.02
1 Unıversity of Health Sciences.Atatürk Sanatoryum Training and Research Hospital, Department of Neurology., Turkiye
2 Atatürk Sanatoryum Training and Research Hospital, Clinical Biochemistry, Turkiye
3 Ankara University Medicine Faculty, Department of Biochemistry, Turkiye
4 Atatürk Sanatoryum Training and Research Hospital, Department of Neurology, Turkiye
5 Atatürk Sanatoryum Training and Research Hospital, Department of Emergency Medicine, Turkiye
Background Levodopa combined with carbidopa and entacapone (LCE) and levodopa combined with benserazide (LB) are both commonly used treatment options in every stage of Parkinson's disease (PD). Although both combinations aim to enhance dopamine bioavailability and improve motor symptoms, their short-term biochemical effects remain to be clarified.This study aimed to compare the short-term effects of LCE and LB on plasma dopamine levels in patients with early-stage, unilateral Parkinson’s disease.
Methods This prospective, single-center, randomized controlled study included patients diagnosed with early-stage Parkinson’s disease presenting with unilateral motor symptoms. Participants were randomly assigned to receive either LCE or LB therapy. Venous blood samples were collected before drug administration and at 90- and 180-minutes post-administration to measure plasma dopamine levels using high-performance liquid chromatography (HPLC).
Results Both LCE and LB led to increases in plasma dopamine concentrations within the first 180 minutes. However, no statistically significant difference was observed between the two treatment groups, nor within groups over time, in terms of dopamine elevation(p>0.05, all values).
Conclusion In this study, no significant difference was observed in the short-term effects of LCE and LB combinations on plasma dopamine levels in patients with early-stage Parkinson’s disease with unilateral involvement. Further large-scale, multicenter studies with extended follow-up are required to assess long-term clinical outcomes, including motor response duration and adverse effects.
LBP37.03
1 Sydney University, Australia
2 Gaitway Neurophysio, Canada
3 Cardiac Health Institute, Australia
4 Royal North Shore Hospital, Australia
Parkinson’s disease is the most rapidly increasing neurodegenerative disease and is remarkably complex, with a high degree of heterogeneity in symptomology. The disease is relentlessly progressive, with deterioration in the clinical signs and symptoms expected, although the rate of progression is difficult to predict and varies from person to person. While medication intervention early in the disease trajectory can create a so-called “honeymoon period” where symptoms can appear stable or even improve somewhat, the trajectory over years is an inevitable deterioration in motor and non-motor symptoms, which significantly impacts health-related quality of life in all patients. There is no pharmaceutical treatment that can reverse, halt or slow the progression of PD.
Photobiomodulation (PBM) is the use of non-thermal light to affect cellular processes. We have previously demonstrated in a number of clinical studies that PBM treatment has the potential to improve some clinical signs and symptoms of Parkinson’s disease. This improvement has been shown to last for up to 3 and 5 years in some cases. The objective of the study reported here was to assess the effectiveness of continued at-home PBM treatment for a period of 7 years. We report a case series of 6 participants who have continued at-home treatment with transcutaneous abdominal laser (using a class 1 laser) plus a transcranial LED ‘helmet’ device. All participants continued an exercise program focussed towards Parkinson’s disease. Results include changes clinical motor signs, including MDS-UPDRS-III (motor) scores, measures of mobility and gait, such as walk speed and timed-up-and-go, and measures of balance, and fine motor skills. Non-motor symptoms including cognition, health-related quality of life, sleep quality, and sense of smell will also be reported. Results have demonstrated a prolonged maintenance of improvements in both motor and non-motor symptoms over many years with a slowing of the progression normally seen in Parkinson’s disease.
These results suggest that continued at-home treatment with PBM is able to slow the progression of symptoms of Parkinson’s disease, at least in some patients and strengthen the case for a larger, long-term randomised, placebo-controlled clinical trial.
LBP37.04
1 Cambridge Stem Cell Institute, Jeffrey Cheah Biomedical Centre, Cambridge Biomedical Campus, University of Cambridge, Cambridge, UK and Department of Clinical Neurosciences, University of Cambridge, United Kingdom
2 Department of Neurosurgery, Skåne University Hospital, Lund, Sweden, Sweden
3 Novo Nordisk Foundation Center for Stem Cell Medicine (reNEW), Department of Biomedical Sciences, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark and Department of Experimental Medical Science, Wallenberg Neuroscience Center and Lund Stem Cell Center, Lund University, Lund, Sweden, Denmark
4 Department of Experimental Medical Science, Wallenberg Neuroscience Center and Lund Stem Cell Center, Lund University, Lund, Sweden, Sweden
5 Clinical Memory Research Unit, Department of Clinical Sciences in Malmö, Lund University, Lund, Sweden, Sweden
6 Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK, United Kingdom
7 Department of Brain Sciences, Imperial College London, London, UK, United Kingdom
8 Department of Neurology, Skåne University Hospital, Lund, Sweden, Sweden
9 Clinical Studies Sweden - Forum South, Skåne University Hospital, Lund, Sweden, Sweden
10 Lund Stem Cell Center and Division of Neurology, Department of Clinical Sciences Lund, Lund University, Lund, Sweden, Sweden
11 Department of Neurology, Skåne University Hospital, Lund, Sweden and Department of Clinical Sciences and Wallenberg Center for Molecular Medicine, Lund University, Lund, Sweden, Sweden
Introduction Parkinson’s disease (PD) is characterised by the progressive loss of nigral dopaminergic neurons, resulting in disabling motor features. Intracerebral transplantation of stem cell-derived dopaminergic progenitors to replace lost endogenous dopaminergic neurons represents a new restorative approach to treating PD. We report the 12-month outcomes from the STEM-PD clinical trial, evaluating a cryopreserved, off-the-shelf dopaminergic progenitor product derived from the RC17 human embryonic stem cell line (NCT05635409).
Methods STEM-PD is a first-in-human, open-label, multi-centre trial in individuals with moderately advanced PD. Participants received bilateral intraputamenal grafts of the STEM-PD product at two escalating doses (n=4/dose), followed by 12 months of immunosuppression. Seven participants completed the 12-month follow-up. The primary outcome of the trial was safety and tolerability of this treatment, assessed by the number and nature of adverse events, and the absence of space-occupying lesions on cranial MRI, in the first 12 months following transplantation. Secondary outcomes included measure of clinical features including dose of medication and an assessment of graft survival using [18F]F-DOPA PET imaging.
Results No serious adverse events related to the cell product were observed and [18F]F-DOPA PET imaging indicated early evidence of graft survival at 6 and 12 months. Seven of the eight participants substantially reduced their Levodopa Equivalent Daily Dose. No graft-induced dyskinesias were observed. Ongoing follow-up to 36 months will assess long-term safety, clinical benefit and dopaminergic function.
Conclusion The 12-month outcomes from the STEM-PD clinical trial have shown that the cell product is safe and well-tolerated. There were also early indicators of clinical improvement, as well as cell survival on dopamine PET imaging. Our results are in line with the data reported in several other recent trials of transplanted pluripotent-derived dopaminergic cell products. These findings support the continued development of this therapeutic approach, including evaluation of the STEM-PD product in larger patient cohorts.
LBP37.05
1 Brigham and Women's Hospital, United States
2 Brigham and Women’s Hospital, United States
3 Tiziana Life Sciences, United States
Introduction Multiple System Atrophy (MSA) is a rapidly progressive neurodegenerative disorder characterized by autonomic dysfunction, parkinsonism, and cerebellar impairment, for which no disease-modifying therapies exist. Neuroinflammation and microglial activation are increasingly recognized as key drivers of disease progression in MSA. Foralumab, a fully human anti CD3 monoclonal antibody delivered intranasally, has demonstrated immunomodulatory effects in clinical trials in multiple sclerosis and Alzheimer’s Disease. Here, we investigate intranasal foralumab as a strategy to attenuate microglial activation in MSA.
Methods TILS-025 (NCT06868628) is a Phase 2a, open-label study enrolling up to 10 subjects with MSA, conducted in collaboration with the Mass General Brigham MyTrial-MSA and Harvard Biomarkers Study 2.0 program. TILS-025 includes a 6-month treatment phase of intranasal foralumab (50 μg per dose), with at least 6 months of pre-treatment observational data when available. Key inclusion criteria include Clinically Established or Clinically Probable MSA according to 2022 MDS criteria; age 30–85 years ; and stable dopaminergic therapy for ≥4 weeks prior to enrollment. Exclusion criteria include other causes of parkinsonism, significant cognitive impairment (MoCA ≤20), low affinity TSPO binders, recent immunosuppressive therapies, and contraindications to nasal administration. Primary endpoints include changes in microglial activation measured by [F18]PBR06 TSPO PET and changes in MDS-UMSARS scores. Secondary measures include regional brain atrophy on volumetric MRI, autonomic and quality-of-life assessments, and immune biomarkers from blood and CSF.
Results To date, four participants met eligibility criteria and have been dosed without significant protocol deviations. Preliminary baseline demographics, efficacy, and safety findings will be presented.
Conclusion This Phase 2a trial provides the first longitudinal assessment of intranasal anti CD3 therapy in MSA. By integrating imaging, biomarker, and clinical outcomes, the study is designed to examine whether intranasal foralumab reduces microglial activation, stabilizes or improves clinical symptoms, and modulates inflammatory biomarkers.
LBP37.06
1 Institute for Neurodegenerative Disorders, United States
Background
Long-term Parkinson’s research depends on strong participant engagement and clear communication. The IMPaCT Program—composed of undergraduate life-science students—supports participant interactions, gathers experiential feedback, and reduces site burden. The program provides early exposure to clinical research, influencing students’ future scientific and medical pathways. Participants contacted represented multiple PPMI clinical cohorts with diverse experiences and logistical needs. Engagement records collected between June 1, 2025, and February 17, 2026, revealed opportunities for operational refinement informed directly by participant commentary.
Objective
To evaluate participant-reported experiences across PPMI cohorts during IMPaCT outreach and document how feedback shaped workflow and process improvements.
Methods IMPaCT Program students completed 377 engagement calls to study PPMI Clinical study participants. The resulting dataset of the engagement call records (June 1, 2025–February 17, 2026) spanning multiple PPMI cohorts, was analyzed for satisfaction ratings and thematic content. Themes were identified across communication, travel logistics, procedural experiences, and questions related to clinical-study results.
Results
Participants reported high satisfaction (mean 4.79/5; 96.3% ≥4). Common themes included communication-clarity concerns, travel challenges, lumbar-puncture experiences, and questions about access to study results. Among those interviewed, 67.3% requested an additional support call. IMPaCT students generated 208 referrals and 31 site-feedback reports, contributing to two workflow updates. Their 1,018 hours represented a part-time FTE equivalent, yielding an estimated $8,450 in benefit-cost savings while providing meaningful exposure to clinical research and supporting future entry into medical and scientific careers.
Conclusion
The IMPaCT Program improved participant experience across PPMI cohorts, strengthened communication clarity, and enhanced operational efficiency. Participant feedback directly informed workflow improvements, protocol clarity, and communication refinements. This undergraduate engagement model is cost-efficient, scalable, and supports research capacity while reinforcing the value of integrating participant-centered structures to refine processes and sustain longitudinal clinical studies.
LBP37.07
1 University of California San Francisco, United States
2 Center for Health + Technology, University of Rochester, United States
3 Clintrex, United States
4 University of Rochester, United States
5 Evergreen Health, United States
6 Selkirk Neurology, United States
7 California Movement Disorders Center, United States
8 University of Colorado Anschutz, United States
9 BoroNeuro, United States
10 Unaffiliated, United States
11 University of Texas Health Science at Houston, United States
12 Beth Israel Deaconess Medical Center, Harvard University, United States
13 Texas Movement Disorder Specialists, United States
14 University of Pennsylvania, United States
15 Neuro Care Center, United States
16 Mount Sinai, United States
17 University of Michigan, United States
18 Pentara Corporation, United States
19 Photopharmics, Inc., United States
20 Atria Health + Research Institute, United States
OBJECTIVE To present preliminary efficacy results of an investigational specialized phototherapy device for treatment of Parkinson’s disease (PD) symptoms through an entirely remote, decentralized phase 3 clinical trial.
Background Current treatments for Parkinson's disease do not adequately address non-motor symptoms, including sleep quality, depression, and fatigue. Of these, few are non-pharmaceutical therapies. Previous studies suggest that specialized phototherapy may be an effective intervention to enhance circadian function and improve PD symptoms (1).
DESIGN We conducted an entirely remote, decentralized phase 3 clinical trial of a non-invasive specialized phototherapy device, akin to a tablet computer. This trial design was selected given the favorable safety profile of the therapy, ability for home use, and a geographically dispersed participant population with limited mobility. Participants were randomized to receive a high intensity active or lower intensity control light therapy for one hour every evening for six months. All study activities, including study visits and therapy use, occurred remotely in the participant’s residence. The primary outcome measure was the change in quality of life as reported in the Parkinson’s Disease Questionnaire-39 (PDQ-39). The trial design was reviewed with the FDA prior to commencing.
RESULTS From February 2024 to October 2025, 350 participants were enrolled from 17 states across the U.S. Enrolled participants averaged 67.5 years old, had Parkinson’s disease for 6.3 years, and 48% identified as female. The initial study results assessing efficacy of light therapy, including changes in primary outcome PDQ-39 and secondary outcomes MDS-UPDRS parts 1+2 and PD-HI, will be presented for the first time at the 2026 WPC conference. Safety and tolerability of specialized light therapy will be assessed with adverse events and study completion compared between treatment groups.
CONCLUSIONS To our knowledge, this is the largest and longest clinical trial assessing the efficacy and safety of phototherapy for Parkinson’s disease. If efficacious, specialized phototherapy could supplement existing pharmaceutical therapies to improve the quality of life of individuals with Parkinson’s disease.
References
Sun W, Yan J, Wu J, Ma H. Efficacy and Safety of Light Therapy as a Home Treatment for Motor and Non-Motor Symptoms of Parkinson Disease: A Meta-Analysis. Med Sci Monit Int Med J Exp Clin Res. 2022 Jan 7;28:e935074-1-e935074-17.
LBP37.08
1 Roche Pharma Research and Early Development, Neuroscience and Rare Diseases, Pharmaceutical Sciences, Roche Innovation Center, Basel, Switzerland; University of Exeter Medical School, London, United Kingdom
2 Roche Pharma Research and Early Development, Neuroscience and Rare Diseases, Pharmaceutical Sciences, Roche Innovation Center, Basel, Switzerland
3 F. Hoffmann-La Roche Ltd, Basel, Switzerland
4 Roche Products Ltd, Product Development Safety, Welwyn Garden City, United Kingdom
5 Department of Neurology, Cedars-Sinai Medical Center, Los Angeles, California, United States
6 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, London, United Kingdom; Department of Neurology, Royal London Hospital, Barts Health NHS Trust, London, United Kingdom
7 Centre for Preventive Neurology, Wolfson Institute of Population Health, Queen Mary University of London, London, United Kingdom; Department of Neurology, Homerton Healthcare NHS Foundation Trust, London, United Kingdom
8 Department of Neurology, Centre of Expertise for Parkinson and Movement Disorders, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Centre, Nijmegen, Netherlands
9 Department of Neurology, Amsterdam University Medical Centers, Amsterdam Neuroscience, University of Amsterdam, Amsterdam, Netherlands
10 Department of Neurology, University Medical Center Groningen, University of Groningen, Netherlands
11 Department of Neurology, University of Pennsylvania, Philadelphia, United States
12 Parkinson’s Disease and Movement Disorders Institute, Department of Neurology, Weill Cornell Medicine, New York, New York, United States
13 Rocky Mountain Movement Disorders Center, Englewood, Colorado, United States
14 Wayne State University School of Medicine, Henry Ford Hospital, Michigan, United States
15 Institute for Neurodegenerative Disorders, New Haven, Connecticut, United States
16 Hertie Institute for Clinical Brain Research, Department of Neurodegeneration, Center of Neurology, University of Tübingen, Tübingen, Germany
17 Department of Neurology, Northwestern University Feinberg School of Medicine, Chicago, Illinois, United States
18 Department of Neurology, Heersink School of Medicine, University of Alabama at Birmingham, Birmingham, Alabama, United States
19 Clinical Ageing Research Unit, Newcastle University and Newcastle Upon Tyne Hospitals, Newcastle, United Kingdom
20 Neurodegeneration Imaging Group, University of Exeter Medical School, London, United Kingdom
21 Pharma Product Development, F. Hoffmann-La Roche, Ltd, Roche, Basel, Switzerland
Introduction: Damage-associated molecular patterns and pathological alpha-synuclein released from damaged or dying neurons are associated with increased NLRP3 inflammasome markers and abnormal microglial response in PD brains. This study aimed to evaluate the effect of selnoflast, an NLRP3 inhibitor, in persons with early-stage PD.
Methods: A total of 57 people with early-stage PD (modified Hoehn & Yahr Stage 1−2.5, treatment naïve or on stable symptomatic therapy, with confirmed abnormal dopaminergic imaging) participated in this 4-week, Phase Ib study to evaluate the safety, pharmacokinetics, and pharmacodynamics of selnoflast.
Results: Baseline characteristics and adverse event profiles were largely similar between the 39 selnoflast-treated participants and the 18 participants on placebo. The NLRP3 inhibitor selnoflast was brain penetrant and modulated NLRP3-related biomarkers. A significant change in TSPO-PET was also observed. New biomarker results will be presented.
Conclusions: Selnoflast showed a favorable safety profile. The findings concerning peripheral and central NLRP3-related biomarkers suggest that NLRP3 inhibition could be a viable therapeutic strategy for early-stage PD.
LBP37.09
1 Harvard Medical School, Massachusetts General Hospital, Boston, MA, United States
2 Deciphera Pharmaceuticals, LLC, Waltham, MA, United States
3 Sendai-Nishitaga Hospital, Sendai, Japan
4 David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, United States
5 National Hospital Organization, Utano National Hospital, Kyoto, Japan
6 Miller School of Medicine, University of Miami, Miami, FL, United States
7 The Parkinson’s and Movement Disorder Institute, Fountain Valley, CA, United States
8 Swedish Neuroscience Institute, Seattle, WA, United States
9 School of Medicine, University of Michigan, Ann Arbor, MI, United States
10 Evergreen Neuroscience Institute, EvergreenHealth Medical Center, Kirkland, WA, United States
11 Department of Neurology, Brigham and Women’s Hospital, Boston, MA, United States
12 Department of Neurology, Dysautonomia Center, Langone Medical Center, New York University Grossman School of Medicine, New York, NY, United States
13 Department of Neurology, National Hospital Organization Osaka Toneyama Medical Center, Toyonaka, Japan
14 ONO Pharmaceutical Co., Ltd., Osaka, Japan
15 University of Kansas Medical Center, Kansas City, KS, United States
16 Parkinson’s Disease and Movement Disorders Center of Boca Raton, Boca Raton, FL, United States
17 Wayne State University, Detroit, MI, United States
18 Norman Fixel Institute for Neurological Diseases, University of Florida, Gainesville, FL, United States
Objective: To assess the safety and preliminary efficacy of ONO-2808 in multiple system atrophy (MSA).
Background: MSA is a neurodegenerative disorder characterized by glial α-synuclein cytoplasmic inclusions and progressive degeneration across motor and autonomic pathways for which disease-modifying treatments are urgently needed. ONO-2808 is a first-in-class, oral, selective sphingosine-1-phosphate receptor 5 agonist that preclinically reduced α-synuclein accumulation and promoted remyelination. We report a 24-week analysis of the ONO-2808 phase 2 trial.
Design/Methods: This randomized, double-blind, placebo-controlled, phase 2 trial (NCT05923866) enrolled participants with MSA diagnosed per Movement Disorder Society Criteria with symptom onset within 5 years. Randomization was 1:1:1:1 to ONO-2808 low-, medium-, or high-dose once daily, or to matching placebo. Primary endpoints included incidence of treatment-emergent adverse events (TEAEs) and drug-induced liver injury per independent data monitoring committee. Exploratory efficacy endpoints were evaluated, including adjusted mean change from baseline (CFB) in a modified Unified Multiple System Atrophy Rating Scale (mUMSARS) score (adjusted sum of 9 items; scores ranging from 0–27; higher scores indicating greater impairment) at week 24. Additional data from the blinded rollover period (week 32) will be presented. Assessment of exploratory endpoints and the open-label long-term extension (up to 80 weeks) are ongoing.
Results: Ninety-two participants were randomized to ONO-2808 (low-dose, n=23; medium-dose, n=23; high-dose, n=23) or placebo (n=23). TEAE incidence was similar between placebo (91%, 21/23) and ONO-2808 (93%, 64/69), with no unexpected safety signals. Transaminase elevation occurred in 12% (8/69) of participants across ONO-2808 doses; all were reversible and none met Hy's law criteria. Differences (95% Cl) in mUMSARS score CFB at week 24 between ONO-2808 low-dose, medium-dose, and high-dose and placebo were 0.47 (−1.42 to 2.36), −1.06 (−2.99 to 0.88), and -0.60 (−2.55 to 1.36), respectively. A dose-dependent trend in attenuation of MRI volumetric loss and improvement in orthostatic hypotension were observed. There was a stronger positive trend and dose response observed for the MSA-P subtype on mUMSARS than for the overall population.
Conclusions: ONO-2808 demonstrated acceptable safety. Safety and exploratory efficacy results at 24 weeks support continued clinical development for patients with MSA.
CLINICAL SCIENCES: Digital health, E-health and technology
LBP39.01
1 Translational and Clinical Research Institute, Newcastle University, United Kingdom
2 The Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom
3 Active Orbit, 5&6 Manor Court Manor Garth, Scarborough, North Yorkshire, United Kingdom
4 Department of Computer Science and INSIGNEO Institute for in silico Medicine, The University of Sheffield, United Kingdom
5 National Institute for Health and Care Research (NIHR), Newcastle Biomedical Research Centre (BRC), Newcastle University, Campus for Ageing and Vitality, Newcastle upon Tyne, United Kingdom
6 School of Engineering, Nancy Rothwell building, East Booth Street, University of Manchester, United Kingdom
Introduction As suboptimal medication adherence is common in people with Parkinson’s [1] and can increase symptom fluctuations, it is essential to explore non-adherence rates and improve this. Current research determines adherence based on retrospective questionnaires and diaries, which are prone to recall bias and cannot capture real-world medication behaviour [2]. Digital health technology may improve this, by objectively monitoring real-world medication behaviour, and improving adherence.
Aim Explore real-world medication adherence in PwP using medication reminder technology and identify factors which influence it.
Methods Fifty-five PwP interacted with a smartwatch over a week [3]. Smartwatches were linked to a smartphone application which sent audible and/or vibrating medication reminders to the smartwatch, with participants clicking “Yes” (med taken) or “No” (med not taken) on the watch face. Intakes were also recorded outside of prescribed times. Participants were classed as adherent to medication timings if ≥80% of their weekly intake was within 30 minutes (pre/post) of prescribed times. Participants were classed as adherent to prescribed intakes if they recorded ≥80% of their weekly intake. Mann-Whitney U tests compared clinical and demographic factors between adherers and non-adherers, and regression assessed their impact on timing adherence.
Results Forty-two PwP were included in analysis [28 male, average number of PD med intakes /day: 5]. Across the week, 83% were adherent to medication timings, and 90% adhered to their prescribed number of daily medication intakes (Figure 1). Average daily adherence rates were 96% (SD=6) in the adherent group, and 58% (SD=23) in non-adherers. Of the clinical and demographic factors, only cognitive function was significantly different between groups, with non-adherent participants scoring significantly lower on the Montreal Cognitive Assessment test (p=0.026), and cognitive function accounting for 17.6% of variance in timing adherence.
Discussion Non-adherence rates were lower than previous research, suggesting that smartwatch reminders may improve medication adherence and management in PwP. In line with previous literature, reduced cognitive function may negatively affect adherence and should be considered clinically.
Malek N et al. 2015
Grosset K et al. 2006
Packer E et al. 2023
Figure 1. Percentage of participants who were adherent/non-adherent to medication times and number of medication intakes over a week.

LBP39.02
1 Theremia, France
INTRODUCTION. Levodopa-based drugs (LD) remain the gold standard of Parkinson disease treatment, yet maintaining patients within the narrow therapeutic window that maximizes "on" time while limiting dyskinesia is a persistent clinical challenge. This window further shrinks in advanced stages, and marked interindividual variability demands highly personalized dosing. In current practice, regimen adjustments rely on trial-and-error titration guided by patient-reported outcomes during visits spaced months apart, a process that can take several months to converge on a satisfactory regimen. Patient hospitalization can accelerate this process but places a substantial burden on healthcare systems and is not scalable. This motivates the development of automated tools for individualized LD dose optimization.
METHODS. We present a closed-loop dose adaptation algorithm that refines LD dosing to optimize therapeutic efficacy based on real-time patient feedback. The optimization is designed to be data-efficient, aiming to identify near-optimal regimens within a few iterations. The system sequentially proposes promising regimens and updates an internal model using the patient's self-assessment of motor and non-motor symptoms, and a preference global rating between the current and previous day. We ensure that all proposed dosages are pharmacologically coherent by integrating a pharmacometric model for the prescribed levodopa formulation, which takes into account patients' features such as age and Hoehn and Yahr stage.
Safety constraints are enforced at every iteration, including clinician-defined minimum and maximum amounts for single intake, limits on daily dose variation, and overall daily dose caps. The algorithm jointly optimizes the timing and magnitude of individual doses and allows variations in the total number of daily intakes within a predefined range chosen by the clinician.
IMPACT. In-silico results demonstrate identification of optimal LD dosing within a few weeks in contrast to the several months often required by standard care. These findings suggest that the proposed approach may improve symptom control with a short automated titration, reducing healthcare burden. Future research is required to extend the algorithm to complex treatment combinations, for which an unified pharmacometric model is typically not available.
LBP39.03
1 Theremia - Paris Brain Institute, France
2 Theremia, France
3 Theremia - INRIA PreMeDICaL, France
4 Paris Brain Institute, France
BACKGROUND. Parkinson’s disease is a complex condition in which treatment decisions depend on motor and non-motor symptoms, treatment-related adverse effects, and patient characteristics. In practice, clinicians naturally balance these multidimensional outcomes when selecting therapy. However, most randomized clinical trials assess efficacy using primary or secondary endpoints that do not fully capture the multidimensional considerations underlying real-world benefit-risk assessment. Although essential, such estimators simplify how overall clinical benefit is evaluated.
METHODS. We propose a framework to estimate treatment effects that reflect neurologists’ preferences when multiple outcomes must be considered simultaneously. Clinicians compare pairs of multidimensional outcome profiles and indicate which is clinically better overall, encoding trade-offs such as accepting mild adverse effects for improved motor control. These judgments are used to learn a probabilistic preference model accounting for uncertainty and inter- and intra-clinician variability. To make this process feasible in practice, an active learning strategy selects the most informative comparisons, limiting the number of queries while preserving accuracy. Once trained, the preference function automatically evaluates and ranks new outcome profiles, enabling scalable and reproducible assessment of overall benefit. Treatment effects are then estimated by comparing expected outcomes under different treatments for individuals with similar characteristics. A treatment is preferred if it is more likely to produce an outcome profile judged better overall by the model. Performance is assessed by the ability to reproduce neurologists’ decisions and by comparing model-recommended treatments with observed prescriptions.
IMPACT. This framework extends treatment effect estimation to multidimensional settings without a predefined hierarchy between outcomes. It formalizes clinicians’ implicit prioritization into a reproducible decision rule. When integrated into a causal inference framework, this approach allows us to estimate treatment effects from observational data and to compare treatments for individual patients in a way that better reflects how clinicians weigh benefits and risks in daily-routine practice.
CONCLUSION. By aligning statistical estimation with clinicians’ priorities and trade-offs, this approach provides a decision-support tool for personalized treatment selection in Parkinson’s disease.
LBP39.04
1 Magnes AG, Switzerland
2 School of Exercise and Nutrition Sciences, Faculty of Health, Queensland University of Technology (QUT), Brisbane, Australia, Australia
3 Magnes AG, Hardturmstrasse 253, 8005 Zurich, Switzerland, Switzerland
4 School of Exercise and Nutrition Sciences, Faculty of Health, Queensland University of Technology (QUT), Brisbane, Australia, Switzerland
Introduction Gait impairments, including increased variability and freezing of gait (FOG), contribute to instability and elevated fall risk, which can negatively affect mobility and quality of life in people with Parkinson’s disease (pwPD). External sensory cueing has been shown to improve certain aspects of gait performance; however, the effects of phase-specific vibrotactile stimulation on gait consistency remain unclear. This study investigated the effects of swing-phase vibration on gait parameters and consistency in pwPD with a history of freezing.
Methods Eight pwPD, identified as freezers according to the New Freezing of Gait Questionnaire (NFOG-Q), participated in the study. Gait was assessed during the ON-medication state across three conditions: no vibration (baseline), with vibrotactile cueing during the swing phase (from toe-off to initial contact), and no vibration immediately after performing bouts with vibrotactile cueing during swing phase (no vibration post swing) to investigate any carry-over effects. In total, 1112 strides were considered for the analysis, 384 baseline values (average per subject 48±20), 381 with swing vibration (average per subject 48±23), and 347 post-swing vibration (average per subject 43±17). Metrics analyzed included stride length, duration, velocity, strike angle and heel clearance. Mean values and variability (coefficient of variation) were compared. Statistical analysis was performed using the Wilcoxon signed rank test for significance testing (p < 0.05) and Cohen’s d for effect size estimation.
Results With vibration during the swing phase, we observed significant increases in velocity (increased in 6/8 subjects, +4% average change, p=0.04, d=1.15) and heel clearance (8/8 subjects, +2.6% average change, p=0.01, d=1.65).
The effect persisted beyond intervention: Significant increases in stride length (7/8 subjects, +5.9% average change, p=0.02, d=0.96), velocity (8/8 subjects, +7.9% average change, p=0.01, d=1.16), and heel clearance (7/8 subjects, +3.2% average change, p=0.04, d=0.67) were observed. The variability of stride length (in 6/8 subjects, -0.84% average change, p=0.04, d=-0.85) and velocity (in 7/8 subjects, -1.6% average change, p=0.02, d=-1.09) also decreased.
Conclusion Preliminary results suggest swing-phase vibrotactile cueing improves gait stability in Parkinson’s disease. Larger studies are needed to confirm persistence and clinical impact.
LBP39.05
1 Cedars SInai, United States
2 Kneu Health Limited, United Kingdom
Background: The rising prevalence of Parkinson’s disease (PD) is placing increasing strain on healthcare systems worldwide. Current routine in-person visits limit the ability to objectively monitor symptom fluctuations, optimize medications in a timely manner, and provide proactive care. Scalable, digital tools that integrate into clinical workflows are needed.
Objective: To report real-world implementation of a fully deployed, patient-facing smartphone platform for remote PD monitoring at Cedars-Sinai, the first US medical center to implement the complete clinical solution in routine practice.
Methods: A multimodal smartphone platform (Kneu Health) was designed to objectively quantify PD symptoms through structured digital assessments of voice, gait, balance, finger dexterity, tremor (rest and postural), reaction time, and cognition. Data are processed into clinically interpretable metrics and visualized on a secure clinician dashboard integrated within the electronic health record. The platform was deployed at Cedars-Sinai in Los Angeles and 11 NHS hospitals in the UK. Sites used the system for 6–24 months in routine care. More than 700 patients participated (∼150 at Cedars-Sinai), completing over 750,000 individual digital measures. Clinical utility, workflow integration, patient acceptability, and service impact were evaluated.
Results: Cedars-Sinai became the first US center to implement the fully deployed end-to-end clinical platform, embedding dashboard review into standard consultations and actively using the system to conduct remote monitoring calls based on real-time patient data. Smartphone-derived motor features were sensitive to day-to-day symptom variability and supported management decisions. Over 90% of patients reported the technology was easy to use, with sustained improvements in confidence, disease understanding, and engagement. Clinicians reported improved efficiency and focused remote and in person consultations through objective longitudinal data review.
Conclusions: This work demonstrates successful real-world deployment of a fully integrated smartphone-based monitoring platform for PD across US and UK healthcare systems. Cedars-Sinai represents the first US site to operationalize the complete clinical solution, actively using the platform to support data-driven remote monitoring calls and proactive care. The approach is acceptable to patients, demonstrates measurable impact and supports scalable digital transformation in PD management.
CLINICAL SCIENCES: Neuroimaging
LBP40.01
1 University of Pavia, Italy
2 Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
3 Neurology Unit, Neuromotor and Rehabilitation Department, AUSL-IRCCS di Reggio Emilia, Reggio Emilia, Italy
4 Nuclear Medicine Unit, Azienda Unità Sanitaria Locale-IRCCS of Reggio Emilia, Reggio Emilia, Italy
5 Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena, Italy
6 IRCCS Mondino Foundation, Pavia, Italy
7 Istituti Clinici Scientifici Maugeri IRCCS, Nuclear Medicine Unit of Pavia Institute, Pavia, Italy
8 Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden
9 Vita-Salute San Raffaele University, Milan, Italy
10 Department of Molecular Medicine, University of Pavia, Pavia, Italy
Introduction: Parkinson’s disease (PD) carrying GBA1 mutations (GBA-PD) is characterized by faster disease progression and more severe cognitive decline than sporadic PD (NM-PD), but its neurobiological substrates remain unclear. Here, we employed a multimodal neuroimaging framework to investigate neurotransmitters’ network alterations in the GBA1 continuum.
Methods: Analyzed data from: (i) 76 drug-naïve PD (dnPD) patients form the Parkinson’s Progression Markers Initiative (PPMI); 60 advanced phase PD (apPD) patients and (iii) 60 asymptomatic GBA1 carriers, stratified based on the presence of REM sleep behavior disorder (GBA-RBD+ and GBA-RBD-). A group of healthy controls (HC) served as normative reference. Participants underwent structural MRI, DAT-SPECT and clinical assessments. Neuroimaging analyses included estimation of: (i) striatal dopaminergic uptake; (ii) dopaminergic pathway molecular connectivity and (iii) structural covariance analysis within dopaminergic, noradrenergic and cholinergic networks. Connectivity matrices were generated using Pearson correlation (FDR-corrected). Altered connectivity was defined as loss/gain of connections relative to HC.
Results: In dnPD, GBA-PD showed higher rates of RBD than NM-PD. Notably, GBA-PD showed a higher caudate/putamen ratio and less severe dopaminergic molecular alterations compared to NM-PD (9% vs 27%; p<0.001), suggesting less severe dopaminergic degeneration. This was confirmed by structural covariance analysis, which showed greater connectivity alterations within the dopaminergic network in NM-PD (81% vs 53%; p<0.001), but greater disruption of noradrenergic and medial cholinergic pathways in GBA-PD (p<0.001). Similar findings were observed in apPD, where GBA-PD exhibited higher prevalence of RBD compared to NM-PD, while NM-PD showed greater molecular connectivity alterations in dopaminergic network (62% vs 26%; p<0.001). In prodromal cohort, GBA-RBD+ showed significantly greater structural alterations in noradrenergic and medial cholinergic networks compared to GBA-RBD-, despite similar alterations in the dopaminergic network.
Conclusions: Since early disease phase, GBA showed greater extra-dopaminergic networks, supporting the hypothesis of distinct topography of regional vulnerability. These neurobiological alterations may underlay the clinical phenotype of GBA-PD and support further evaluation of extra-dopaminergic pathways as early biomarker in GBA1 carriers.
LBP40.02
1 University of Florida, United States
Atypical forms of parkinsonism such as Multiple System Atrophy (MSA), and Progressive Supranuclear Palsy (PSP) are often misdiagnosed as Parkinson’s Disease (PD). To address this concern, our lab recently developed the Automated Imaging Differentiation for Parkinson’s (AIDP). The AIDP is a robust support vector machine (SVM) model paired with free-water imaging that discriminates PD vs MSA/PSP (AUROC 0.96) and MSA vs PSP (AUROC 0.98).
In the efforts of further optimizing this process, we evaluated whether diffusion scans with lower number of gradient directions can yield comparable model performance metrics as the ones obtained in the previous study. We used diffusion MRI scans from both prospective and retrospective cohorts. The prospective cohort included a total of 249 participants, 40-80 years of age. The retrospective cohort had a total of 396 participants. Neurologists reviewed videotaped examinations, MRI scans, and clinical scales, and provided their blinded diagnosis for all subjects. Diffusion MRI scans were obtained using 3T scanners across at least 30 directions. Using a custom MATLAB script, we created two new datasets limited to only 15 and 6 diffusion directions to evaluate if reducing the number of directions reduces model performance.
Models were trained on free water (FW) and free-water-corrected fractional anisotropy (FAt) across 132 brain regions of interest using five-fold cross-validation. For every set of directions, we trained and tested 50 different models. The models were trained on both prospective and retrospective cohorts, while testing was performed using the independent prospective cohort only. Overall, model performance remained comparable across direction sets. DeLong’s tests showed no significant differences between the original number of directions, and 15 and 6 directions. Thus, reduced directions can maintain model performance accuracy of AIDP while enabling shorter scan times. These findings can directly impact diagnostic imaging costs by making them more accessible while also providing a reliable classification tool for physicians.
LBP40.03
1 Institute of Medical Science, Temerty Faculty of Medicine, University of Toronto, Canada
2 Brain Health Imaging Centre, Centre for Addiction and Mental Health, Canada
3 Edmond J. Safra Parkinson Disease Program, Neurology Division, Toronto Western Hospital, University Health Network, University of Toronto, Canada
Introduction: Cognitive impairment is a common non-motor symptom of Parkinson’s disease (PD), yet its mechanisms remain unclear. Apolipoprotein E4 (APOE4), a genetic risk factor for Alzheimer’s disease, has been associated with PD-related cognitive impairment, though findings are inconsistent. Notably, APOE4 has been linked to cortical morphometric alterations in regions relevant to PD-related cognitive impairment. However, no study has examined whether APOE4 is associated with cortical morphometric changes that may affect cognition in a PD cohort. This study investigated whether APOE4 is associated with cognitive function in PD through cortical morphometry.
Methods: Baseline structural MRI data from the Parkinson’s Progression Markers Initiative (PPMI) were analyzed in 51 PD APOE4 carriers and 120 non-carriers. Beyond traditional morphometric measures previously examined (gray matter volume and cortical thickness), additional metrics were analyzed using FreeSurfer: surface area, folding index (cortical folding complexity), and mean curvature (local cortical geometry). Sixty-eight regions (34 per hemisphere) were analyzed using the Desikan–Killiany atlas. Cognition was assessed using Montreal Cognitive Assessment (MoCA) scores alongside domain-specific tests. ANCOVAs tested group morphometric differences. Relationships between significant regional morphometric measures and cognitive scores were further analyzed using Pearson correlations and regression models for covariate adjustment. Significance was set at p < 0.05, with Bonferroni correction for each hemisphere.
Results: Exploratory uncorrected analyses (p < 0.05) revealed trends of surface area group differences in the left inferior parietal and rostral anterior cingulate cortices, and right parahippocampal and posterior cingulate regions. Folding index group differences were found in the left inferior parietal and medial orbitofrontal cortices, and right parahippocampal, pars orbitalis, and posterior cingulate regions. Mean curvature differences were observed in the left caudal middle frontal and medial orbitofrontal cortices. However, no group differences and associations with cognitive scores survived Bonferroni correction.
Conclusion: APOE4 in PD may be linked to subtle cortical morphometric differences in default mode, limbic, and executive control regions. Larger samples and longitudinal studies are needed to validate these findings and assess their relevance to PD-related cognitive impairment.
LBP40.05
1 University of Michigan, United States
Background: Freezing of gait (FoG) is a debilitating mobility disturbance that becomes increasingly resistant to dopaminergic pharmacotherapies with advancing Parkinson’s disease (PD). The pathophysiology underlying the response of FoG to dopaminergic is poorly understood. Our recent whole brain vesicular acetylcholine transporter positron emission tomography (VAChT PET) imaging studies implicate the degeneration of cholinergic pathways, including hippocampal, thalamic-limbic, paralimbic (insula) and cerebellar regions in levodopa-unresponsive FoG.
Objective: We aimed to investigate whether specific cholinergic system changes are associated with FoG responsiveness to levodopa treatment in PD patients.
Methods: Thirty six PD subjects (31M/5F) completed [18F] fluoroethoxybenzovesamicol ([18F]FEOBV) vesicular acetylcholine transporter positron emission tomography (VAChT PET) and underwent videotaped clinical assessments for FoG on and off levodopa.
Results: Sixteen subjects had L-dopa-unresponsive FoG. Voxel-based analyses of [18F]FEOBV PET (false discovery rate-corrected at P < 0.05 and adjusted for levodopa-equivalent dose) showed cholinergic losses in the peri-aquaductal gray (PAG), left superior collicus (SC), interstitial nucleus of Cajal (inC), periaqueductal gray matter (PAG) & nucleus of Darkschewitsch upper tegmental regions.
Conclusion: Cholinergic losses in the upper mesencephalon in levodopa-nonresponsive FoG may relate to animal findings of primitive motor behaviors observed in animals. The SC plays a central role in mediating innate defensive behaviors in response to looming visual stimuli. The inC is critical for control of eye and head movements, especially vertical and torsional gaze. PAG freezing refers to this brainstem structure's role in triggering the "freezing" response—a crucial defensive behavior (passive immobility) to threats—with different PAG regions (dorsal vs. ventral) linked to distinct types of fear, including panic attacks (dPAG) or sustained fear/anxiety disorders (vPAG). The nucleus of Darkschewitsch is an excitatory pathway from the PAG to induce such freezing motor behavior. These findings may relate to the human panic disorder subtype of FoG in PD. Such a FoG subtype may be a naturally protective defense mechanism but given the high inherent risk of FoG-associated falling, may become counterproductive. Future research should test this heuristic model.

LBP40.06
1 Cornell University, United States
Risk for Parkinson’s disease (PD) rises sharply with advancing age, and PD diagnosis is also associated with demographic factors, including sex and race. It is now understood that subcortical modulatory nuclei show some of the earliest signs of proteinopathy-related neurodegeneration, even in otherwise healthy aging. Within this system, the substantia nigra pars compacta (SN) is identifiable by neuromelanin, a pigment produced as a by-product of dopamine synthesis that accumulates within dopaminergic neurons and can be visualized with turbo spin echo Magnetic Resonance Imaging (MRI) sensitive to neuromelanin. Because degeneration of the SN is a hallmark of PD, and because the neuromelanin-sensitive signal is often treated as a proxy for dopaminergic cell health, characterizing how the SN signal differs across the lifespan is essential for understanding the temporal course of disease vulnerability in PD-related brain regions.
Here, we examined the neuromelanin-sensitive SN signal in 143 adults with no history of neurodegenerative disease who completed turbo spin-echo MRI alongside cognitive and behavioral assessments. SN signal was quantified using individualized manual tracings as well as automated individual alignments of a standard mask, and evaluated across whole-SN, hemispheric, and exploratory nigrosome-informed regions using intensity and contrast-to-noise metrics against multiple background references. Across the healthy adult lifespan, we found little evidence that broad SN signal varied as a function of age, sex, race, or cognition—unlike the pronounced SN signal reductions consistently reported in PD. The segmentation approaches and control regions yield different absolute signal intensity and CNR values, but the overall pattern of SN stability persists. Exploratory analyses indicated a potential localized right-sided effect in Nigrosome 2, though this finding requires confirmation using multiple methods to distinguish the nigrosomes in the SN.
These findings suggest that in nonclinical aging, the SN signal is relatively stable across demographic groups and that even slight SN signal differences are likely to reflect disease-related processes. Prior work has suggested a potential inverted U-shaped trajectory of SN signal across the lifespan, but this pattern has not been systematically re-examined in a large and demographically diverse cohort. Given that Locus Coeruleus (LC) degeneration is already established to precede SN degeneration in PD, this may suggest that the SN is not less vulnerable, but operates on a later degenerative timescale, such that substantial SN changes are required before broader cognitive correlates become detectable These findings may also indicate that the selective vulnerability of regions such as the SN and LC is not fully explained by neuromelanin-related signal properties alone.

CLINICAL SCIENCES: Prodromal States
LBP42.01
1 Radboud University Medical Center, Netherlands
2 Queen Mary University London, United Kingdom
Introduction Exercise may delay or prevent the onset of Parkinson’s disease (PD). The Slow-SPEED trials in the Netherlands, United Kingdom and United States are the first long-term randomized trials of exercise in prodromal PD. We report an interim update from the Netherlands (Slow-SPEED-NL), which will recruit 110 participants. This analysis examines recruitment feasibility; participant characteristics; generalizability and motivators and barriers to exercise at baseline based on the first subsample.
Methods Slow-SPEED-NL is a two-year remote exercise trial in persons with video-polysomnography confirmed isolated REM sleep behavior disorder (iRBD). Participants are recruited via sleep centers in the Netherlands and Belgium. Screening includes a telephone assessment and a 4-week eligibility period during which physical activity must remain below 10,000 steps/day. Baseline data were collected using a Fitbit smartwatch, validated questionnaires, the University of Pennsylvania Smell Identification Test, and a custom survey on exercise motivators and barriers.
Results Of 123 participants screened, 35 were excluded after pre-screening and 40 after the 4-week period, mainly due to declining participation or high physical activity (>10,000 steps/day). To date, 48 participants have enrolled over 18 months. Mean age is 67 (SD 6) years; 83% are men; 97% of Dutch origin; 26% had abnormal MoCA scores; and 82% had olfactory deficits. Compared to international iRBD cohorts, participants showed similar clinical profiles but more years of education. Physical activity averaged 7,797 (SD 1,550) steps/day and 24 (SD 20) minutes/day of moderate-to-vigorous activity, higher than in early PD cohorts and comparable to healthy older adults. Walking (95.7%) and cycling (72.3%) were common. Motivation to exercise was high (91.4% ≥7/10). Maintaining independence (78.5%) was a key motivator; weather a common barrier (53.1%).
Conclusion This interim analysis indicates recruitment is feasible, although many in this source population are already too physically active. The sample has multiple prodromal features and resembles international iRBD cohorts, but has more years of education. Participants are highly motivated to exercise, mainly for intrinsic reasons. These findings inform future PD prevention and exercise trials. Recruitment is expected to finish in 2026, after which results will be updated. We aim to triangulate results with the ongoing trials in the United Kingdom and United States.
LBP42.02
1 Center for Health + Technology (CHeT), University of Rochester, Rochester, NY, United States
2 Department of Neurology, University of Rochester, Rochester, NY, United States
3 College of Nursing and Health Sciences, University of Massachusetts Dartmouth, Dartmouth, MA, United States
4 Institute for Neurodegenerative Disorders, New Haven, CT, United States
5 Feinberg School of Medicine, Northwestern University, Chicago, IL, United States
Objective: To identify and characterize meaningful symptoms and sex-based differences in symptom patterns among individuals with prodromal Parkinson’s Disease (PD) vs Healthy controls (HCs).
Background: Little is known about sex-based differences in prodromal PD. Clarity regarding prodromal symptom patterns is needed for development of high-yield PD screening tools, timely diagnosis, and optimal care.
Methods: We conducted a double-blind, cross-sectional, mixed methods interview study. All prodromal participants and all but 5 controls were recruited from the Parkinson’s Progression Markers Initiative (PPMI). All participants completed an online symptom survey followed by a 2-hour 1:1 online interview via Zoom using symptom mapping to systematically explore any symptomatic changes from normal occurring within the past 5 years. Content coding was conducted by two independent coders who were blinded to group allocation. After unblinding, Mann-Whitney U and Ordinal regression were used to evaluate for differences in symptom patterns between prodromal PD vs HCs, controlling for age and sex, with subgroup comparisons for males and females.
Results: A total of 95 participants completed interviews (2024-2025) and 89 were included in the final analysis (48 prodromal PD, 41 HC). There were no significant differences in MoCA, MDS UPDRS Total and Part III, and H&Y staging between groups. In the prodromal PD group 97.9% were white and 66.7% were female, while in the HC group 90.2% were white and 43.9% female. Striking differences in symptoms patterns were observed for prodromal PD vs HCs within male vs female subgroups. Significant Symptom differences between prodromal PD vs. HC men included constipation (p=<0.0001), hyposmia (p=0.004), drooling (p=0.013), personality changes (p=0.013), active dreaming (p=0.014), anorgasmia (p=0.014), fatigue (p=0.03), bradyphrenia (p=0.032), and nocturia (p=0.033). Fewer differences were found between prodromal PD and HC women, but included active dreaming (p=0.0009), hyposmia (p=0.017), urinary incontinence (p=0.014), and other forms of urinary dysfunction (p=0.035).
Conclusions: This is the first blinded interview study to explore symptoms in prodromal PD. Preliminary data suggests that there might be important differences between the symptoms experienced by men vs women in prodromal PD. Further research is needed to replicate findings and best inform development of screening tools and clinical outcome assessments.
Acknowledgments: PPMI – a public-private partnership – is funded by the Michael J. Fox Foundation for Parkinson’s Research and funding partners: https://www.ppmi-info.org.
LIVING WITH PARKINSON'S: Government Advocacy/Campaigns/ Public Policy
LBP44.01
1 Vibrar com Parkinson, Brazil
2 Camara Municipal de Agudos, Brazil
3 Camara Municipal de São Vicente, Brazil
4 Vibrar com Parkinson; Doc Concierge, Brazil
5 Vibrar com Parkinson; Associação de Superação do Parkinson do Estado da Paraíba (ASPEPB), Brazil
6 Associação de Superação do Parkinson do Estado da Paraíba (ASPEPB), Brazil
7 Universidade Federal do ABC (UFABC), Brazil
Vibrar Com Parkinson, a Brazilian civil society initiative dedicated to advocacy and support for people living with Parkinson’s disease (PD), developed the Red Tulip Lanyard as a voluntary and human-centered visual identification strategy for individuals with PD. Parkinson’s disease frequently presents with invisible or fluctuating symptoms, which may lead to misunderstanding, stigma, and inadequate responses in public environments, healthcare settings, and essential services.
The Red Tulip is an internationally recognized symbol of Parkinson’s disease awareness. In this context , we designed the Lanyard incorporating this symbol for into a discreet and respectful identification tool, enabling individuals to communicate their condition when desired. The initiative aims to improve social awareness, facilitate communication in situations of vulnerability, promote timely and appropriate assistance, and validate the lived experience of people with visible motor symptoms , regardless of disease stage or symptom .
The community-based initiative evolved into formal public policy. On September 26, 2023, Municipal Law No. 5,761/2023 was enacted in the city of Agudos, State of São Paulo, officially recognizing the Red Tulip Lanyard as an identification instrument for people with Parkinson’s disease. Following this pioneering legislation, similar laws have been approved in multiple municipalities across Brazil, expanding institutional recognition and reinforcing local inclusion policies.
More recently, federal legislation has begun to be considered in the Brazilian National Congress to formally institute and recognize the Red Tulip Lanyard nationwide. This legislative progression represents a significant step toward integrating Parkinson’s-specific visibility measures into broader disability and public health frameworks.
The Brazilian experience demonstrates how grassroots advocacy can inform and shape public policy, promoting social inclusion, autonomy, and dignity for people living with Parkinson’s disease. As a low-cost, scalable, and culturally adaptable intervention, the Red Tulip Lanyard presents strong potential for international replication as a practical policy tool to enhance awareness, accessibility, and rights-based approaches within Parkinson’s care and disability inclusion strategies worldwide.
LIVING WITH PARKINSON'S: Living Well with PD
LBP45.01
1 University of Maryland School of Medicine, United States
2 Parkinson Foundation, United States
3 University of Maryland, United States
4 University of Rochester, United States
Background: People with Parkinson's disease (PD) often misunderstand palliative care, with 68% associating it with hospice or "giving up." A PCORI-funded randomized trial by Dr. Benzi Kluger showed that outpatient palliative care improves quality of life (QOL) without increasing caregiver burden. The PEACE-PD (Disseminating PCORI-Funded Study Results on Palliative Care to Improve Quality of Life for People with Parkinson's Disease) project seeks to demystify palliative care, promote informed discussions, and enhance daily living for people with PD and their care partners.
Methods: A multidisciplinary team of palliative care experts and patient advocates leads PEACE-PD using a virtual dissemination approach. A Patient and Care Partner Advisory Panel (PCAP) co-develop accessible messages and a digital toolkit (PDF guide, videos, infographics) for distribution via trusted advocacy channels. In partnership with the Davis Phinney Foundation (DPF) and University of Maryland Medical System (UMMS), activities include bi-monthly virtual PCAP meetings, message testing with DPF and UMMS participants, toolkit launch on the DPF Learning Lab and UMMS portal, training of "Palliative Care with Parkinson’s Champions," and five Zoom community events co-facilitated by trained PCAP members.
Results: PCAP members and DPF Ambassadors (people with PD and care partners from across the U.S.) refined key messages for the toolkit, including: “The need to enjoy life does not end with serious illness,” “Palliative care approaches improve patient and care partner outcomes,” and “Palliative needs begin at diagnosis, fluctuate over the illness course, vary individually, and include death and bereavement.” Drawing from Kluger's trial, palliative care improved patient QOL, reduced caregiver burden, enhanced symptom control, and lessened anxiety/grief. Toolkit feedback highlighted value in the digital guide (e.g., questions for providers, palliative vs. hospice distinctions, resources, lived experience testimonials).
Conclusion: PEACE-PD empowers people with PD to live better by translating evidence into relatable, accessible tools, breaking down barriers to palliative care, and ultimately improving quality of life.
LIVING WITH PARKINSON'S: Advancing research: collaborations, fundraising, trials, campaigns
LBP46.01
1 American Parkinson's Disease Association, United States
Background: Parkinson’s disease (PD) researchers are navigating an increasingly unstable funding environment. In May 2025, APDA surveyed 74 investigators to understand the impact of recent federal funding changes. Seventy-six percent reported disruptions to their research programs, and 51% experienced direct funding loss through institutional or individual awards. These findings highlighted immediate risks to research continuity.
Objective: To describe APDA’s rapid development of the Bridge Funding program to support investigators facing unexpected funding gaps and to highlight early indicators of demand.
Methods: In response to survey findings, APDA developed the Bridge Funding Awards within months and announced inaugural awards in October 2025, supporting three investigators to start in January, 2026:
Donghe Yang, PhD Memorial Sloan Kettering Cancer Center Characterizing development of human dopaminergic neurons from stem cells Helen Hwang, MD, PhD Washington University School of Medicine Studying inhibitors of alpha-synuclein fibril growth Franchino Porciuncula, PT, DScPT, EdD Boston University Examining whether rhythmic auditory stimulation reduces cognitive demands of walking in PD Total Bridge Funding awarded: $205,000.
Results: Survey findings demonstrated widespread instability:
76% reported funding-related disruption 51% reported loss of institutional or personal funding
As expected, demand for APDA funding was particularly strong in 2026. APDA received 366 LOIs in January 2026, an increase from 290 LOIs in 2025, despite restricting applications to within the U.S.
Conclusion: APDA’s Bridge Funding program demonstrates the value of rapid-response philanthropy in supporting promising Parkinson’s research during periods of funding uncertainty. Subsequent LOI trends suggest sustained need for flexible support mechanisms that help ensure continuity of scientific progress.
LIVING WITH PARKINSON'S: Other
LBP47.01
1 Merz Pharma UK Ltd, United Kingdom
2 Merz Pharma UK Ltd, United Arab Emirates
Introduction: Focus groups provide an important opportunity to gather patient perspectives on PD and its treatment, with the overarching goal of enhancing clinical care. The objective of this meeting was to gather insights from patients with PD and their caregivers across three interconnected themes: the lived experience of OFF periods, reactions to an inhaled treatment recently launched in the UK [levodopa inhalation powder] and preferences for educational support.
Methods: This UK-based focus group included 8 patients with PD (five male) and 2 carers. All patients were currently taking PD medications, including some on advanced (non-oral) therapies, and all were experiencing daily OFF periods. Participants engaged in facilitated focus group sessions exploring each of the three key themes.
Results: OFF periods were viewed as among the most debilitating aspects of PD, yet were often misidentified or poorly understood by patients. Patients described a variety of physical (motor) and non-motor symptoms during OFF periods, in addition to emotional, cognitive, and social disruption, which they considered equally impactful. Timing of OFF periods varied significantly, with all patients experiencing 1–2 per day.
The concept of inhaling medication was generally accepted by patients and most expressed openness to an on-demand treatment option. Several potential positive aspects of the inhaler compared to oral or injectable rescue therapies were highlighted, including rapid onset of action, reduced stigma, gastrointestinal bypass/lack of food interaction, and discretion of use.
Regarding education, a clear divide in digital confidence was evident, with some favoring digital tools and others preferring printed materials or in-person support. In general, participants preferred videos featuring real people with PD over animations or clinical demonstrations. PD nurse specialists were viewed as key educators and sources of support; however, inconsistent access and lack of integration across services were highlighted.
Conclusions: Novel insights from this PD patient focus group highlight the complex experience of OFF periods and the critical need for accessible education and support. The inhaled device was generally viewed positively by patients as an on-demand option for treating OFF periods, provided it is supported by accessible patient-centered training.
Disclosures: Preparation of this abstract was supported by Merz Therapeutics, Global Medical Affairs.
AUTHOR INDEX
Aamodt, Whitley, LBP37.08
Aarsland, Dag, P42.02
Abbott, Maggie, P45.49
Abdesselem, Houari, P34.01
Abid, Nauman, P36.06
Abler, Victor, P35.10
Abosnwber, Yara, P01.10, P01.11, P02.01
Abushanab, Karime Raygoza, P14.32
Acevedo, Gabriela, P39.01
Acevedo, Marty, LBP29.01
Acheson, Jonny, P45.23
Ackerman, Peter, P37.06
Aco, Paulo, P38.10
Adam, Rob, LBP06.05
Adam, Robert, P10.07
Adamkovič, Peter, P45.07
Adams, Dan, LBP37.07
Adams, Jamie, P37.32, P37.33, LBP42.02
Adams, Jamie L., P28.07, LBP37.07
Adams, Robert J, P10.05, P10.08
Adamson, Ashley, LBP01.02
Adamson, Jeanie, P45.29
Addison, Clare, P45.23
Adetulubo, Henry, P10.16
Adileu, Erika, P27.18
Adler, Charles, P01.12
Aertsen, Veerle, P46.15
Afanasiev, Elia, P06.04
Agarwal, Pinky, LBP37.07, LBP37.09
Agarwal, Veena, P37.43
Agin-Liebes, Julian, P25.29, P25.33
Agley, Ledia, P14.09
Agoriwo, Mary, P14.34
Aguiar, Marcos, P17.05, P29.05
Aguilar-Calvo, Patricia, P05.04, P05.06
Aguillon, David, P01.21
Ahmad-Annuar, Azlina, P01.16
Ahmed, Ezaz, P32.07
Ahn, Jiyun Wendy, P25.25
Aiello, Carmen, P13.11
Aigbirhio, Franklin, P40.18
Ajnassian, Michael, P01.22
Akalu, Mussie, P46.16
Akande, Rayo, P40.05
Åkesson, Elisabet, P14.11
Akbudak, Ömer, LBP31.01
Akinola, John, P45.41
Akpalu, Albert, P14.34
Alam, Nazia, LBP37.06
Alberts, Jay, P25.51
Albin, Roger, LBP40.05
Albitar, Orwa, LBP37.08
Alcala, Francesca, P25.06, P37.44
Alcalay, Roy, P12.05
Alcalay, Roy N., P37.23, P46.18
Alcauter, Sarael, P29.12, P40.03, P40.04
Alcock, Lisa, P37.18, LBP39.01
Aldhahwani, Bayan, P38.12
Aldhahwani, Bayan M., P22.01, P25.46
Aldred, Heather, P45.39
Aldred, Jason, P35.01, P36.03, P36.04, P37.10, LBP37.07
Alefanti, Ioanna, P15.09
Alegre-Esteban, Manuel, P38.03
Alemany, Mäelys, P04.05
Alen, Natalie, P27.05
Alessandri, Elena, P15.02
Alessandri, Kevin, P02.03
Alessi, Dario, P06.18
Alessi-Fox, Christi, LBP37.07
Alexander, Brooke, P23.02
Alexander, James, P14.09
Alexandratou, Ioanna, P15.09
Alfaidi, Maha, P35.20
Alfonso, Arisly, P24.04
Al-Jassar, Gemma, P13.12
Allan, Amanda, P10.19
Allard, Simon, P35.09
Alleman, Laurent Y, P01.07
Allen, Natalie, P23.05
Allendorfer, Jane, P14.10
Allgar, Victoria, P23.14
Allison, Jennifer, P37.43
Allison-Ottey, Sharon, P46.05
Allnutt, Mary Alice, P34.03
Alomar, Jehan, P38.12
Alomar, Jehan A., P22.01, P25.46
Alonso, María Sancho, P07.05
Alonso, Paco, P43.32, P43.33
Alphonso, Helene, P27.04
Alstrup, Aage KO, P06.03, P06.09, P06.10
ALTELAAR, Marteen, P09.07
Alty, Jane, P14.01, P32.01, P39.06
Alves, Guido, P28.04, P34.05, P42.02
Amara, Amy, P14.04
Amedi, Amir, P37.37, P37.45
Amine, Myassar, P46.07
Amlani, Bharat, P35.07, P35.13, P35.14, P35.15, P35.16, P35.17, P35.18
Ammar, Sara, P46.07
Ananthakrishnan, Ananya, P39.08
Ancer-Rodríguez, Patricia, P26.06
Andersen, Julie, O104, P02.08
Andersen, Katrine, P06.10, P34.01
Andersen, Katrine B, P06.09
Anderson, Adam, LBP40.06
Anderson, Caleb, P02.03
Anderson, Dakota, P11.05
Anderson, Rylee, P30.03
Andrews, Charlotte, P29.06
Andrews, Lily, LBP29.02
Andrews, Shan, P12.10
Andruska, Kristin, LBP37.07
Andrzejewska, Ewa, P35.20
Angelini, Lorenza, P39.23, P39.25, P39.26
Angermair, Paula, P15.03
Anikeeva, Polina, LBP06.02
Animdife, Walter, P14.34, P43.31
Annett, Lucy, P15.02
ANNICOTTE, Chloé, P09.07
Antonelou, Roubina, P15.09
Antonini, Angelo, P46.10
Anzures-Cabrera, Judith, P37.20, P40.05
Apokotou, Olympia, P35.22
Appelberg, Annicka, P23.01
Arango-Quintero, Paola Andrea, P38.03
Arauzo, Noelia Peña, P42.01
Arboleda-Bustos, Gonzalo, P01.21
Ardle, Ríona Mc, P14.34
Aref, Donya, P35.20
Arenas, Roy Llorens, P39.10
Argenziano, Giacomo, LBP40.01
Argibay, Uxia, P06.07
Argyrou, Charlie, P10.19
Aries, Ali, P25.40
Aristieta, Asier, P06.12, P06.13
Armengol, V.Diego, P24.04
Armengou-Garcia, Laura, P38.03
Arnold, Emma, P20.12
Arnold, Philipp, P12.12
Arnone, Annachiara, LBP40.01
Arrar, Ambrine, P06.02
Arredondo, Marco, P02.06
Arriagada-Concha, Héctor, P30.05
Arrue-Gonzalez, Mercedes, P03.06
Arsac, Jean-Noël, P06.02
Ascherio, Alberto, P37.33
Ashkenazi, Yarden, P37.07
Ashton, Nicholas, LBP34.04, LBP34.05
Asis, Angelica, P46.14, P46.17
Aslam, Sidra, P01.12
Aspinall, Bryony, P13.06, P46.04
Ǻström, Daniel Oudin, P38.02
Atkinson, Louise, P46.03
Atorrasagasti-Villar, Ainhoa, P38.03
Atri, Alireza, P01.12
Atrian, Farzaneh, P02.06
Aufauvre, Claire, P06.02
Auffret, Manon, P19.01
Auinger, Peggy, P37.33
Auld, Grace, P38.05, P39.17
Aulet-Leon, Margarita, P30.02
Avantaggiato, Federica, P38.07
Avenali, Micol, LBP37.01, LBP40.01
Avery, Leah, P27.05
Avila, Cesar, P01.21, P29.12
Avion, Sabela, P39.30
Awad, Lou, P39.14, P39.15
Awad, Louis, P39.24, P40.07, P40.08
Ayala, Patrice, P45.36, P45.37, P45.38
Ayele, Wdasie, P37.02
Ayhan, Zilan, P05.03
Azcarate, Ignacio, P37.23, P46.18
Azoidou, Viktoria, P14.22, P20.04, P30.15, P39.09, LBP42.01
Bäckström, David, P28.04
Böttger, Tabea, P20.06, P24.03, P37.13
Babarinde, Adetayo, P25.36, P25.47
Babarinde, Adetayo A., P25.42, P27.12
Babcock, Daniel, P08.02
Badin, Romina Aron, LBP06.01
Baekelandt, Veerle, PCO3, P11.02
Baghoydan, Sophie, P39.24
Bahrinejad, Sepehr, P11.01
Bailey, Lorna, LBP37.08
Baird, Abigail, P30.06
Bailey, Suzanne, P46.17
Baillot, Louis, P02.02
Bakalidou, Daphne, P15.09
Baker, Katherine, P27.05, P27.06
Baker, Teresa, P39.14, P39.15, P39.24, P43.20
Bakshi, Nikul S., P46.05
Baldassarre, Antonio, P15.02
Bale, Claire, P18.04, P19.02, P37.32, P46.15, P46.17
Balech, Patricia Risden, P14.13
Baleche, Patricia Risden, P14.20
Ballabio, Andrea, P02.04
Ballard, Lachane, P23.02
Ballardin, Demetra, P09.05
Ballmann, Christopher, P14.10
Balsamo, Barbara, LBP07.02
Balsamo, Giuseppe, LBP07.01
Bandmann, Oliver, P37.03, P37.04
Banisadr, Ghazal, P35.08, P35.09
Bank, Netherlands Brain, P05.03
Bannister, Kirsty, P27.06
Bantle, Collin, LBP01.01
Banuelos, Amanda, P14.32
Barajas, Jordan, P37.34, P39.13, P46.22
Barbier, Emeline, P01.07
Barbier, Emmanuel, P11.01, P32.02
Barbieri, Fabio A., P40.01
Barbosa, Egberto, P38.04
Barbosa, William, LBP42.02
Barela, José Angelo, P14.35
Barker, Roger, O69, O120, P10.06, P37.03, P37.04, LBP36.02, LBP37.04
Barker-Detwiler, Justin, P43.15
Barmpoutis, Angelos, LBP40.02
Barnes, Haley, P37.47
Barnhill, Lisa, P01.22
Barolli, Thayane Habache, P37.15
Baron, Thierry, P06.02
Barrasa, Inma, P28.01
Barrera, Alberto, P46.16
Barret, Olivier, LBP06.01
Barthe, Louis, P09.05
Barthel, Maria, P20.06, P37.13
Bartholomé, Emmanuel, P39.10
Bartlett, Michèle, P37.18, P46.14, P46.17
Bartlett, Michele, P37.32, P37.43, P46.03
Bartlett, Mitchell, P06.12, P06.13, P06.15, P07.04
Bartliff, Caroline, P25.17
Bartolomeu-Pires, Sandra, P37.43
Bash, Ryan, P05.04, P05.06
Basha, Nardin, LBP06.01
Basirat, Anahita, P30.04
Basu, Purbita, P26.01
Battistella, Ingrid, P04.04
Baumgartner, Alexander, LBP37.07
Baumier, Raphaëlle, P06.02
Baxter, Jazmine, P37.09
Baykal-Caglar, Eda, P46.14, P46.17
Bayramov, Aydin, P36.08
Bazan-Wigle, Jennifer, P14.27, P25.03, P25.49
Beach, Thomas, O98, P01.12
Bechtold, Toni, P15.02
Beck, James, P12.05, P37.33
Beck, James C., P37.23, P43.18, P46.18
Beck, Judith, P14.25
Beckers, Debby G.J., P37.14
Bek, Judith, P14.41, P27.19, P39.31
Belachew, Shibeshih, P39.10
Belafsky, Peter C., P37.07
Belaire, Bailey, LBP34.01
Belden, Christine, P01.12
Bell, Stephanie, P38.01
Bellaire, Bailey, P31.02, P32.04, P34.07, P34.08, LBP34.03
Bellières, Camille, P06.02
Belloli, Sara, LBP37.01
Bellucci, Arianna, LBP37.01
Belnavis, Alexander, P10.20, P33.01
Beltre, Melba, P31.04
Bement, Ben, P43.27
Benabderrazik, Rita, P29.03, P38.06
Benavoli, Patrick, P01.13
Bennett, Venetia, LBP15.01
Benskey, Matthew, P02.05
Bensmail, Ilham, P34.01
Bentley, Cintra, P37.02
Benvengo, Stephanie, P37.33
Benykoub, Amine, P37.24
Berchol, Rose, P17.05, P29.05
Berendse, Henk, P05.03
Berendse, Henk W., P34.06
Beretta, Victor, P37.36
Beretta, Victor Spiandor, P37.35
Bergamino, Maurizio, P40.10
Berge, Jan Erik, P42.02
Berger, Anna-Karin, P38.02
Bergmann, Ken, P39.30
Bergmann, Lars, P35.01, P35.02, P37.17
Bergmans, Bruno, P29.01
Bergquist, Filip, P35.01
Bermudes-Mendoza, Jesús, P26.06
Bernard, Kelsey, P02.09, P12.02
Bernardo, Greta, P04.06
Bernasconi, Corrado, P39.10
Bernstein, Alison, P11.04, LBP01.02, LBP01.03
Berti, Elena, O64, P14.24, P15.06, P17.06, P45.26, P45.40
Berti, Luca, P45.26
Bestwick, Jonathan, P29.03, P29.08, P39.09
Bestwick, Jonathan P, P38.06
Bevilacqua, Laura Menegatti, P30.01
Beyene, Kassu M., P45.46
Bezard, Erwan, P02.03, LBP06.01, LBP06.04
Bezchlibnyk, Yarema, P36.04
Bhadra, Esha, P20.04, P29.08, P39.09
Bhatia, Perminder, P37.29
Bhattacharya, Ritika, LBP12.05
Bhavsar, Nilay, P01.09
Bhullar, Sukirat, P39.14, P39.15
Biagioni, Milton, P37.05, P46.10
Bianchi, Joana, P35.12, P37.39
Bibb, Abigail, LBP01.01
Bicknell, Brian, P15.14, P15.15, P25.52, LBP37.03
Biercewicz, Monika, P27.01
Biering-Sørensen, Bo, P35.18
Biglan, Kevin, P37.33
Billakanti, Vamshi, P01.10, P01.11, P02.01
Bilodeau, Anthony, P02.04
Binck, Sylvia, P27.14, P27.16
Binder, Luisa Bandeira, P30.01
Bindila, Laura, P04.06
Bindoff, Aidan, P32.01
Bingol, Baris, LBP12.03
Bircan, Mert, P35.21
Birznieks, Gunther, P35.22
Bischof, Gérard, P28.03
Bishop, Christopher, P40.10
Bitaraes, Larissa, P25.50
Bittencourt, Julia, LBP35.03
Bjartmarz, Hjalmar, LBP37.04
Bjordal, Ellen Marie Thinn, P42.02
Bjorklund, Anders, LBP37.04
Blackburn, Hannah, P38.05
Blacker, David, P45.35
Blackwood, Indhira, P24.01
Blake, Kathleen, P24.07
Blanchard, Joel, P01.06, P01.08
Blauwendraat, Cornelis, P01.16, P37.23
Bledsoe, Ian, P37.47
Bleinroth, Gabriel, P29.02
Bloem, Bas, P20.10, P23.06, LBP23.02, LBP37.08
Bloem, Bastiaan, P14.22
Bloem, Bastiaan R., P15.03, P23.04, P26.02, P37.14, LBP42.01
Blokhuis, Sterre, P23.06
Boari, Daniel, P43.11, LBP44.01
Boari, Daniel C., P40.01
Boas, Liliana Vilas, P42.03
Boccon-Gibod, Philippe, P46.10
Bock, Meredith, P27.08
Bodmer, Rolf, P04.06
Boehm, Gary, P27.04
Boesen, Thomas, P06.03
Bogaarts, Guy, P39.23, P39.25, P39.26
Bohnen, Nicolaas, P27.09, P40.15, LBP40.05
bohnen, Nicolaas I., P14.30
Boileau, Isabelle, LBP40.03
Boiser, Joey, P37.25
Boiten, Walter A, P05.01
Bolduc, Cyril, P04.06
Bolen, MacKenzie, P01.09
Boles, Claire, P46.14, P46.17
Bolhalter, Stephan, P15.02
Bommarito, Silvana, P27.17
Bonifati, Vincenzo, P05.01
Bonni, Azad, P37.20, LBP37.08
Boon, Bram, P26.02
Borchers, Emily, P14.27, P25.49, P45.39
Bordelon, Yvette, LBP39.05
Borges, Brandeci, P01.21
Borges, Vanderci, P29.12
Borghammer, Per, P06.03, P06.09, P06.10, P34.01
Borich, Michael, P07.07
Bornemann, Tina, P37.05
Bortolozzi, Analia, P06.07, P07.05, P10.09
Bosman, Monique, P46.01
Bossert, Irene, LBP40.01
Bothwick, Nicola, P12.05, P37.23, P46.18
Botta, Ragasudha, P37.32, P46.14, P46.16
Bottiroli, Sara, LBP40.01
Bouet, Severine, P37.21
Bougea, Anastasia, P15.09
Boulainine, Oumnia, P17.04
Boularand, Sylviane, P06.18
Boulet, Sabrina, P11.01, P32.02
Bounsall, Katie, P23.14, P39.12
BOURDON, Stéphanie, P40.06
Bourinet, Emmanuel, P06.01
Boutet, Valerie, P06.18
Boutsikari, Eleni, P15.09
Bouwman, Sanne, P24.09
Bowden, Alillia, P25.46
Bowr, Abigail, P27.11
Boyle, Evan, P34.10
Boyle, Gary, P46.14, P46.17
Boyle, Thomas, P39.09
BP, Kailash, P01.08
Bradley, Emily, P26.04
Bradley, Helena, P46.10
Bradshaw, Patrick, LBP04.01
Brady, Stephen, P14.07
Braga-Neto, Pedro, P01.21
Braganza, Alyssa, P13.02
Brahmachari, Saurav, P10.01, LBP34.01
Bramich, Sam, P39.06
Bramich, Samantha, P32.01
Bramoulle, Yann, LBP06.01
Branson, Chantale, P37.47
Brauer, Sandy, O32, O83
Brazel, David, P34.10
Brennan, Cameron, P36.06
Brennan, Lily, P37.03, P37.04, P37.18
Bressman, Susan, P29.11, P31.04
Breve', John JP, P05.01
Brigas, Helena C., P43.22, P46.13
Briggs, Aidan, LBP01.01
Brinton, Roberta, P37.32, P37.48
Brittain, Katie, P14.34
Brockman, Kathrin, P37.19, P37.32
Brockmann, Kathrin, LBP37.08
Brolin, Kajsa Atterling, P29.06, P29.08
Bronstein, Jeff, P01.22, P39.03
Brooks, Annie, P24.10, P47.03
Broome, Kieran, P38.01
Brotchie, Jonathan, P35.20
Brouwer, Kaley, P25.15, P45.34
Brower, Kaley, P24.13
Brown, Ethan, P01.17, P27.08
Brown, Ethan G., P37.47
Brown, Graham, P46.15
Brown, Harry, P05.02, P10.14, P12.11, P35.06
Brown, Jodi, P45.28
Brown, Philip, LBP39.01
Broyant, Quentin, P08.01
Brubaker, Logan, P14.07
Bruce, Elikem, P14.34
Bruce, Elikem Ame-, P43.31
Bruggeman, Arnout, O66, O101, P29.01
Brugna, Omar, LBP39.01
Brundin, Patrik, P37.19, P37.20, LBP37.08
Bruno, Michiko, P01.17, P15.11
Brunson, Greg, P31.03, P35.10
Bucher, Olivia, P38.10
Buckley, Thomas, P37.01
Budu, Caroline, P29.08, P39.09
Buetow, Emily, P24.07, P43.16, P43.19
Buff, Susan, P37.11
Bui, Bang, P02.07
Bui, Bang V, P06.06
Buitrago-Pocasangre, NIck, P37.24
Burciu, Roxana, P27.11, P37.01, P38.11
Burdick, Daniel, P37.28
Burgos, Pablo, P25.06, P25.41, P25.43, P37.44
BURIN, Alessio, P09.07
Burmeister, Tim-Simon, P10.17
Burré, Jacqueline, O10
Burton-Freeman, Britt, P26.07
Busch, Gregory T., P39.27
Buser, Andrew, P25.46
Bustos, Bernabe, P01.16
Bustos, Gonzalo Arboleda, P29.12
Butler, Tracy A., LBP05.01
Byatt, Hilary, P47.01
Byrd, Erica, P37.47
Célinain, Corinne, P06.18
Caallison, Susan, P45.44
Caboy, Lark, P37.23, P46.18
Cabrera, Jocelyn, P39.03
Caceres, Valentina, P01.18, P20.09
Cadoret, Alice, P30.01
Caggiano, Eloise, P21.02, P43.20
Calabrese, Rosaria, LBP40.01
Calandrella, Daniela, P13.11
Callado, LLuis F, P10.09
Callegari, Sylvie, O9
Callen, Antoni, P30.05
Callisaya, Michele, O44, P14.01, P39.06
Camacho, Marta, P10.02, P10.10, P28.04, P40.18
Camastra, Chiara, LBP32.01
Camboe, Ellen, P20.04, P29.08, P39.09
Camgrand, Eva, P24.08
Caminiti, Silvia Paola, LBP37.01, LBP40.01
Campbell, Clyde, P46.15
Campos, Edevaldo, P29.05
Campos-Vargas, Silvia, LBP20.02
Canning, Colleen, P23.05
Capato, Tamine, P20.10, P38.04
Capotosti, Francesca, P12.07
Caprau, Rodica, P06.13
Carau, Rodica, P06.12
Cardoso, Tiago, P02.02, P04.01
Cardoso, Viviane, P43.11, LBP44.01
Carey, Danielle, P14.19
Carli, Giulia, P27.09, P40.15, LBP40.05
Carlin, Daniel, P01.19
Carlone, Michael, LBP12.02
Carlson, Jonathan, P36.04
Carlson, Lydia, P15.10, P28.08, P35.19
Carlson-Kuhta, Patricia, P25.38, P39.05
Carlson-Kuhta, Patty, P25.43
Carnaby, Giselle, P25.08
Carnicella, Sébastien, P11.01, P32.02
Carnicer-Caceres, Clara, P03.06
Caroen, Scott, P01.10, P01.11, P02.01
Carolina R, Ganivet, P03.06
Carpenter, James, P37.03, P37.04, P37.18
Carpentier, Jessica, P01.07
Carrillo, Laura, P37.32, P46.14, P46.16, P46.17
Carroll, Camille, O76, P23.14, P37.03, P37.04, P37.18, P37.40, P37.41, P37.43, P38.05, P39.08, P39.12
Carroll, Camille B, P37.42
Carter, Gillian, P23.09
Carter, Jade, P22.01, P25.46, P38.12
Carter, Valerie, P14.36, P25.26
Cartner, Helen, P13.06, P46.04
Carvalho, Augusto, P37.36
Carvalho, Eduardo Dias, LBP25.04
Casal, Carme, P06.07
Cassidy, Emma, P14.05
Casso, Isabel, P15.02
Cassy, Andrew, LBP36.02
CASTANO, Chrystelle, P40.06
Castelo, Paula Midori, P27.17
Castelo Rueda, Maria Paulina, P04.06
Castillo-Ribelles, Laura, P03.06
Castillo-Sanchez, Pablo, P03.06
Castonguay, Sierra, P14.33
Castro, Jeanelle, P06.15
Castro, Sandra, P10.03
Catalogna, Merav, P37.37, P37.45
Catherine, Kestner, P25.34
Caulfield, Margaret, P37.23, P46.18
Caulfield, Margaret E., P43.18
CAUSIN, Ellen, P24.08, P35.05
Cavaioni, Pietro, P12.06
Cavallieri, Francesco, LBP40.01
Cavanaugh, James, P39.24, P40.07, P40.08
Cavo, Annge, LBP12.05
Cedarbaum, Jesse M, P37.24, P39.30
Cellan-Jones, Rory, P44.03
Cerino, Eric, P14.36
Chávez-Luévanos, Beatriz, P26.06, P29.13
Chagas, Sandra, P43.11
Chai, Yaqiong, P40.11
Chakrabarty, Samit, P41.02
Cham, Momodou, P14.34, P43.31
Chambers, Nicole, LBP07.02
Chan, Vicky, P20.07
Chana, Pedro, P29.12
Chana, Pedtro, P01.21
Chandra, Shivika, P45.45
Chandra, Sreeganga, PCO2, P34.03
Chang, Chih-Kang, P39.14, P39.15
Chang, Ih, P37.25
Chang, Sherry, LBP11.01
Changizi, Barbara Kelly, LBP37.09
Chanwimalueang, Theerasak, P39.02
Chapa-Ancer, Karla, P26.06
Chaparro-Solano, Henry Mauricio, P01.21
Chaparro-Solano, Mauricio, P29.14
Charter, Shelly, P45.44
Chatzipirpiridis, George, P25.45, LBP39.04
Chaudhuri, K. Ray, P27.06, P35.02
Chavez, Jorge Borja, LBP16.01
Cheminon, Maxime, P17.04
Chen, Aobo, LBP36.04
Chen, Chih-Yang, P06.16
Chen, Keiwei, P10.20
Chen, Rob, LBP40.02
Chen, Robert, LBP32.01
Chen, Sarah Mitchell, P37.02
Chen, Tiffany, P39.03
Chen, Xuejie, P27.08
Cheng, Cynthia, LBP24.02
Cheng, Jiani, P13.01, P13.07
Chesire, Amy, P12.05
Chi, Jinhua, P35.06
Chiang, Gloria Chia-Yi, LBP05.01
Chiang, Ming Sum Ruby, P06.18
Chien, Chester, LBP11.01
Chin, Andrew, P39.14, P39.15
Chitnis, Tanuja, LBP37.05
Chodosh, Joshua, P37.02
Chohan, Harneek, P29.03, P38.06
Choi, Eu Jene, P04.02
Choi, Ko-Eun, LBP06.03
Chou, Kelvin, LBP40.05
Choudhury, Parichita, P01.12
Chouhan, Dimple, LBP12.06
Chowdhury, Kashfia, P38.05, P39.17
Chriss, Ariana, P01.06
Christensen, Kristina B, P06.09
Christiansen, Cory, P45.28
Christou, Evangelos, LBP27.03
Chrones, Lambros, P31.03, P35.10
Chrysovitsanou, Chrysa, P15.09
Chu, Yaping, P36.10
Chung, Eun Ju, P40.17
Chung, Sun Ju, P12.01, P36.01
Ciambur, Constantin Bogdan, P03.01
Cicero, Steven, LBP37.05
Cipparonne, Elizabeth, P38.07
Cisneros, Aliah, P25.39
Ciucci, Michelle, P06.08
Ciucci, Michelle R., P06.19
Clark, Karen, LBP37.07
Cleveland, Lesli, P25.35
Cline, Victoria, LBP15.01
Cochran, Joy, P14.03, P14.37
Cochrane, Robert, P45.43
Cocks, Naomi, P25.02
Coenen, Volker, P36.02
Cogan, Wendy, P46.12
Cognard, Tilio, P19.01
Cohan, Charles, LBP12.05, LBP35.03
Cohen, Ohad, LBP35.03
Coimbra, Madeleine, P06.18
Coizet, Veronique, P27.13
Colón-Semenza, Cristina, P16.02, P43.20
Colbert, Brett, P37.37, P37.45, P46.23
Cole, Cassandra, P01.09, P10.16, P10.21, P10.22
Coley, Denise, P37.12, P46.15, P46.19, P46.21
Coley, R Bernard, O36, P46.11, P46.19, P46.21
Coley, Robert B., P46.15
Coley, Robert Bernard, P37.12
Colini Baldeschi, Arianna, P12.07, P12.08
Collier, Timothy, P06.15
Collier, Timothy J., P02.05, P36.10
Collins, Helen, P37.43
Collins, Sally, P37.03, P37.04, P37.43
Colombo, Aurora, P13.11
Colon-Semenza, Cristina, P14.29, P14.39
Columna, Luis, P13.13
Combs, Hannah, P30.06
Comella, Cynthia L., P37.47
Comes, Georg, P35.03, P35.04
Comi, Cristoforo, O47, O123
Comyns, Kathleen, P27.08
Con, Evrim Sude, P28.01
Conde, Luis Bernal, P02.05
Cong, Cen, P39.08
Conrad-Bruat, Isabelle, P37.21
Consortium, ProPark, P34.06
Conte, Cindy, P14.38
Contento, Angela, P13.08
Conti, Elysabeth, P37.21
Converse, Madeline, P37.34, P45.46
Convey, Victor Mc, P28.06
Cool, Nicole, P45.03
Cooley, Ambriel, P30.03
Coon, Cheryl, P37.32
Cooper, Antony, P29.07
Cooper, Jack, P29.07
Cooper, Kay, P25.04
Coral, Anny, P01.18, P20.09
Coral-Zambrano, Anny, P37.23, P46.18
Corcos, Dan, O96, O135
Corcos, Daniel, P14.01, P14.02, P25.18
Cordero-Espinoza, Lucia, P02.03
Corenblum, Mandi, P02.09, P11.05, P12.02
Coric, Vladimir, P37.06
Cormac, Ryan, P27.05
Cornejo-Olivas, Mario, P01.21, P29.12
Corpa Cipolla, Maria Eduarda, P14.35
Correa-Gallego, Valentina, P35.07, P35.13, P35.14, P35.15, P35.16, P35.17, P35.18
Correal, Sara, P20.11
Cortes, Carolina Navarrete, P27.17
Corti, Corrado, P11.02
Corvol, Jean-Christophe, P37.21, LBP39.03
Costa, Ellen, LBP44.01
Costa, Ellen Cristyanne, P43.11
Costa, Fulviany Cristina Lazari, P43.11
Costa, Raquel, P46.13
Costes, Safia, P06.02
Couchouron, Joël, P37.21
Coulombe, Vincent, P04.06
Counsell, Carl, P28.04
Cowd, Elaine, P37.41
Cowell, Rita, P05.06
Cowen, Stephen, P06.12, P06.13, P07.04
Cox, Madeline, LBP12.05
Crabb, Lauren, P25.53
Craig, Stephanie, P17.08
Crary, Felix, P01.06, P01.08
Crary, John, P01.06, P01.08
Crawford, Victoria, P37.30
Crespo, Andrea Merriam, P13.12
Creuwels, Lambert, LBP35.02
Criscuolo, Antonio, P30.05
Crist, Kathleen, P30.06
Criswell, Susan, P40.12
Crone, Julia S., P15.03
Cronin-Golomb, Alice, P40.07, P40.08
Crosiers, David, P29.01
Croucher, Rebecca, P37.43
Crowell, Jason, P20.05, P32.05
Crowley, Suzanne, P18.01
Crozier, Kaylie, P45.28
Cruz, Kelli, P45.05
Cruz, Rosa Elba Hernandez, P43.13
Cucca, Alberto, LBP35.02
Cui, Changxu, P04.02
Cullen, Kacy, LBP12.06
Cummings, Steven R., P37.47
Cunningham, Amaya, LBP37.06
Curle, Annabel, P10.06
Curtis, William, LBP04.01
Cushen, Samantha, P26.04
Cutting, Emma, LBP37.04
Cwiekala-Lewis, Klaudia, P27.01
d'Alencar, Matheus Silva, P25.28
D'Cruz, Nicholas, P25.19, P25.54
D'Urso, Giulia, LBP37.08
Déon, Catherine, P06.18
da Silva, Denilson Feijoreiro, P25.27
da Silva, Paloma Rodrigues, P25.27, P25.28, P25.32
da Silva, Renato Marques, P43.11
da Silva, Suzane Weber, P15.13
da Silva Neto, Francisco, P38.04
da Silva Salin, Mauren, P14.13, P14.20
Da Viega Said, Angélica, P27.17
Daadi, Elyas, P02.06, P35.11
Daadi, Etienne, P02.06, P35.11
Daadi, Marcel, P02.06, P35.11
Dabée, Guillaume, P02.03
Dadar, Mahsa, P01.12
Daigmorte, Chloé, P24.08
Dal koyuncuoglu, Beyza, P25.09
Dalal, Bhavin, LBP47.01
Dallal-York, Justine, P25.33
Dallemand, Alexia, P37.22
Dalm, Brian, P36.04
Damasceno Mendes, Caio Henrique, P02.08
Danaila, Téodor, P17.04
Dangla, Marjorie, P24.04
Daniel, Nathalie, P37.21
Daniels, Rebecca, P38.11
Dannenbaum, Julia, P20.12
Darbandsari, Paria, P14.29, P14.39
Darweesh, Sirwan, O1, O15, P14.22, P15.03, LBP23.02
Darweesh, Sirwan K.L., LBP42.01
Das, Piyali, P05.04, P05.06
Dashtipour, Khashayar, P35.10
Dave, Aditi, LBP15.01
Davenport, Lisa, LBP14.01
Davidson, Rory, P37.40, P37.42
Davies, Emma, P37.43
Davies, Sarah, O133, P17.03, P38.01
Davis, Emma, LBP25.01
Davis, Oliver, P12.10
Dawkins, Polly, P46.15
Dawson, Ted, LBP34.01
Dawson, Ted M., P10.01
Dawson, Valina, LBP34.01
Dawson, Valina L., P10.01
Day, Cindi, P45.03
Dayal, Viswas, P26.08
Dayalu, Praveen, LBP37.09
De Bartolomeis, Francesca, P14.24, P15.06, P17.06, P45.24, P45.25, P45.40
De Bie, Rob M. A., LBP37.08
De Cesar, Aude, P06.02
de Fabregues, Oriol, P37.17
de Groot, Dave, P14.01
De Groote, Friedl, P38.13
De Jesus, Russell, LBP25.01
de Lataillade, Adrien de Guilhem, P10.12
De León, Rebeca, P01.18, P20.09, P46.18
De Leon, Maria, P13.12
De Leon, Rebeca, P37.23
de los Angeles Soto Linan, Victoria, O91, P34.13
de Mattos Aranha, Luiza, P25.27, P25.30, P25.32
de Mello, Celina Malebran, P25.21
De Miranda, Briana, LBP01.02
de Morais Faria, Christina, P14.32, P25.42
De Natale, Edoardo Rosario, LBP37.08
De Pablo Fernandez, Eduardo, P38.06
de Pablo-Fernández, Eduardo, P29.03
de Paiva, Tamara Ferreira, P14.32, P25.42, P25.47
de Paula Magalhães, Jordana, P14.32, P25.23, P25.24, P25.42, P25.47
De Renzis, Francesco, P35.13, P43.22
de Souza, Aline Trucillo, P37.35
De Vleeschhauwer, Joni, P25.54
de Vries, Christian, P13.12
de Vries, Nienke M., P23.04, P26.02
DE VRIES, Rens, P09.07
de Wilde, Henk, P11.06
de Witte, Lot, P01.06, P01.08
de Xivry, Jean-Jacques Orban, P38.13
Dean, John, P14.28, P43.25
Dean, Thomas, P45.04
DeAngelis, Tami, P43.20
Dear, Blake, P13.02
DEBETS, Donna, P09.07
Deerhake, M. Elizabeth, P37.24
Deeson, Eric, P46.03
Defebvre, Luc, P37.17
Defendorf, Sara, LBP42.02
DeFranco, Meredith, P15.08, P45.13
Deh, Edem Stephen Komla, LBP16.03
Dehay, Benjamin, O47, LBP06.01
Deierborg, Tomas, P12.08
Dekker, Marieke CJ, P39.30
Del Din, Silvia, P38.05, P39.17, LBP39.01
del Mar Gimeno-Rodriguez, Maria, P38.03
Deleidi, Michela, P10.11
Delevoye-Turrell, Yvonne, P15.02
Delva, Aline, P29.01
DeMarch, Erica, LBP39.04
Demirtas, Alp, LBP23.01
Denkinger, Marisa, LBP34.04
Denkinger, Marissa, LBP34.05
Denney, Linda, P30.03, P39.18
Dennis, Anthaea-Grace Patricia, LBP32.01
Deprets, Stephanie, P06.18
Derkinderen, Pascal, P10.12
DeRosa, Eve, LBP40.06
Desai, Aarav, P43.09
Desai, Amey, P41.02
Desai, Divya, P25.05
Desai, Radhika, P14.26
Desai, Tanvi, P43.09
Descaillot, Roxane, P06.02
Deshayes, Natasja, P05.03
DeSimone, Jesse, LBP40.02
Desplats, Paula, P01.19
DeTabola, Luis, P37.01
Dettmer, Ulf, P02.05, P12.03
Devenney, Etain, P45.27
Devos, David, P01.07, P30.04, P37.21
Devoto, Daria, P13.11
Dey, Kamalesh, P20.04, P29.08, P39.09
Dey, Sankar, P26.01
Dey, Sumit, P29.06
Dhall, Rohit, P37.25, P37.26
Dhingra, Juslyn, P14.12, P39.07
Di Blasio, Andrea, P14.24
Di Leva, Francesca, P11.02
Di Rocco, Alessandro, P38.07
Diaféria, Giovana, P27.17
Diamond, Scott, P03.02
Dias, Cassia, P25.13
Dias, Lorrane Esterfane, P25.24
Dias, Rebeka, P27.18
Dias, Rebeka Amanda, P21.03, P21.04, P25.50
Diaz, Kasandra, P35.19
Diaz-Taveras, Graciela Maria, P38.03
Dibble, Leland, P25.51
DiBiaso, Peter, P46.14, P46.15, P46.17
Dieckhoff, Kari, LBP34.04
Diederich, Nico, P27.16
Diederich, Nico J, P27.14, P42.03
Diesing, Sarah, P13.05, P25.12, P25.14
Digraskar, Saumya, P05.04, P05.06
Dilliott, Allison, P37.23, P46.18
Dillon, Tyaisha Blount, P43.12
Din, Silvia Del, P37.18
Dinacci, Daria, P15.02
Dini, Megan, P37.23, P37.30, P46.18
Dinku, Abegeya, LBP37.06
Dobert, Jan Philipp, P12.12
Doblas, Francisco, P20.11
Dolhun, Rachel, P46.21
Domínguez-Fraustro, César Arturo, P40.03, P40.04
Domingos, Josefa, P14.28, P43.25
Donadio, Vincenzo, P34.09
Donald, Alex, P32.07
Dong, Ryan, P02.05, P10.18
Dorney, Casey, P37.33, LBP42.02
Dorsey, E. Ray, P37.33, LBP37.07
dos Santos Ghilardi, Maria Gabriela, P29.12
Dos Santos Soares, Açucena Rodrigues, P02.08
Doshier, Kirby, P27.04
Doucet-Beaupré, Hélène, P04.01
Drake, Danielle, P34.14, P34.15
Drew, Cheney, P15.05, Pc37.09
Drews, Janika, LBP27.01
Driver-Dunckley, Erika, P01.12
Drysdale, Emily, P01.19
Drzezga, Alexander, P28.03
Du, Peng, P26.08
Duarte-Zambrano, Felipe, P01.21, P29.12
Dubios, Laurent, P06.18
Dubman, Sue, P37.32, P46.16
Dubroux, Malvina, P10.11
Ducotterd, Fiona, P46.09
Duda, John, P43.16
Duda, John E., LBP12.06
Duffen, Joy, P37.03, P37.04, P37.43
Duffy, Orla, P25.16
Dufloux, Jean-Louis, P37.21
Dugay, Philipe, P06.18
Duguey, Olivier, P06.18
Duits, Annelien A., P23.04
Duncan, Ryan, P25.36, P25.47
Duncan, Ryan P., P25.42, P27.12
Dunson, Kayla, P06.05
Dupee-Polcari, Brandy, LBP37.05
Dupré, Nicolas, P34.13
Durand, Tony, P10.12
Durcan, Thomas, P02.02, P02.04
Durphy, Jennifer, P36.04
Durrleman, Stanley, P37.32
Dutta, Rishi, P32.07
Dutton, Lauren, P12.06
Duval, Erin, LBP29.01
Duval, Manuel, P20.05, P31.02, P32.05, P34.07, P34.08, P34.09, LBP34.03
Duvvuri, Sridhar, P37.25
Dwyer, Danielle, P14.07
Dzialas, Verena, P28.03
Dziwis, Christine, P35.21
Eberhard-Bensaid, Noam, P14.12, P39.07
Eberling, Jamie, P46.14
Eberly, Gari L., LBP06.02
Ebise, Hayao, P38.08
Edirisinghe, Indika, P26.07
Edwards, Hillary, LBP45.01
Edwards, Luke, P36.05
Ehab, Karim, P46.07
Ehlenberger, Peter, P17.09
Eidelberg, David, LBP29.01
Ek Olofsson, Henric, P36.07
Eklund, Nicole, P39.14, P39.15, P39.24, P40.07, P40.08
El Kodsi, Daniel, P28.01
El-Agnaf, Omar, P34.01
Elci, Okan U., LBP37.09
Elhussein, Malaz, LBP47.01
El-Kodsi, Daniel, LBP37.05
Ellis, Terry, P39.14, P39.15, P39.24, P40.07, P40.08
Ellis, Theresa, P43.20
Ellis-Doyle, Romy, P37.43
Ellmore, Timothy, P37.39
Elpidoforou, Michail, P15.09
Emektar, Emine, LBP31.01, LBP37.02
Emmanouilidou, Evangelia, O75, O131
Emmery, Laura, P14.41
Emore, Ufuoma, O52
Engel, David, P38.09
Enriquez, Silvia, P43.30
Enseki, Carol, P45.04
Erb, Rowena, LBP24.02
Eretz-Kdosha, Noy, LBP09.01
Erickson, Madeline, P27.02
Erkamp, Nadia, P35.20
Erlich, Shai, P37.45
Escalada-Cebadero, Leire, P25.11
Eshed, Gadi Maayan, P37.07
Esko, Jeffrey, P05.06
Espay, Alberto, P37.33
Espay, Alberto J., P35.10, P37.47, P39.30
Espinoza, Eric, P14.05
Espinoza, Eric E., P45.34
Espinoza, Freydell, LBP40.02
Espinoza, Stefano, P11.02
Espinoza-Vinces, Christian, P38.03
Esposito, Samantha, P37.24
Esquivias-Farías, Juan Manuel, P40.04
Esquivias-Farias, Juan M., P40.03
Essam, Farida, P46.07
Estrada-Bellmann, Ingrid, P26.06, P29.13
Eubanks, Jim, P37.26, P37.28
Evancho, Alexandra, P14.10
Evans, Amy, LBP37.04
Evans, Samantha, P21.05
Even, Mathieu, LBP39.03
Evers, Christiana, P24.07
Evers, Luc, O5, O118
Evidente, Danica, P32.06, P34.14, P34.15
Evidente, Virgilio Gerald, P34.14, P34.15
Evidente, Virgilio Gerald H., P32.06
Førland, Per Tore, P42.02
Fabbri, Margherita, P24.08, P35.05
Fabrizio, Ryan, LBP37.06
Facheris, Maurizio, P35.23
Faggiani, Emilie, P02.03
Falconer, Drew, P14.28, P37.10
Falk, Torsten, P02.09, P06.12, P06.13, P06.15, P07.04
Fan, Rebecca, P05.02, P10.04, P10.14, P35.06
Fan, Rebecca Z., P12.11
Fang, Zih-Hua, P01.16
Faouzi, Malika, P15.11
Farahnik, Joshua, P21.05
Fargo, Keith, P37.02
Faria, Christina DCM, P25.23, P25.24, P25.47
Faria-Costa, Lucas, P29.06
Farley, Becky, P14.27, P25.49
Farmer, Jill, LBP37.07
Farmer, Kyle, P10.03
Farrell, Kelly, P25.44
Farrer, Matthew, P03.07
Fasano, Alfonso, P36.06, P37.10
Faulkner, Joanne, P45.06
Fauvel, Tristan, LBP39.02
Fauvelle, Florence, P11.01, P32.02
Fayard, Audrey, LBP06.01
Fazal, Shaline, LBP37.04
Febbo, Eli, P02.08
Feher, Kip, LBP35.03
Fehlmann, Bernhard, P37.22
Feldman, Matthew, P24.04
Feng, Xiaoshu, P31.03
Fenyi, Alexis, LBP06.01
Fereshtehnejad, Seyed-Mohammad (Sam), O11, O86, LBP27.02
Ferguson, Christine, P14.10
Ferguson, Dominique, LBP12.05
Ferguson, Owen, P02.04, P04.01, P34.13
Fernández, Marisol Gomes, P27.15
Fernández-del-Olmo, Miguel Angel, P39.11
Fernandez-Toledo, Elias, P29.06
Ferraro, Federico, P05.01
Ferreira, Joaquim J., P46.13
Ferrell, Betty, P13.08
Ferrer, Cyril, P36.09, P37.31
Ferris, Jennifer, LBP14.01
Festanti, Andrea, P39.23, P39.25, P39.26
Feyeux, Maxime, P02.03
Fiallos, Katie, P01.18, P20.09
Figueiro, Mariana, P31.04
Figueroa-Amaro, Jovany, P14.39
Filice, Angelina, LBP40.01
Finch, Spencer, P29.06
Fineman, Julie, P14.40
Finke, Megan, P37.23
Finkelstein, David, P02.07
Finkelstein, David I, P06.06
Fischetti, Pietrina, P25.31
Fisher, Stanley, P35.08, P35.09
Fiske, Brian, P37.11
Fiske, Eldbjørg, P34.05, P42.02
Fitch, W.L., P01.10, P01.11
Fitzgerald, James, P36.02
Fitzgerald, Kate, P24.01
Flanagan, Richelle, O139, P26.04, P26.08, P27.07, P39.21, P39.29, P46.15
Flanders, Emily, P27.02
Flannagan, Richelle, P37.32
Fleisher, Jori, PCO14, O63, P37.02
Flores-Ocampo, Victor, P29.06
Floro, Nicole, P36.06
Flynn, Allyson, P14.14, P23.05
Flynn, Christine, P25.48
Foco, Luisa, P11.02
Foletti, Amanda, P15.02
Foley, Christopher, LBP29.02
Follett, Jordan, P03.07
Foltynie, Thomas, P37.03, P37.04, P37.18, P37.40, P37.41, P37.42, P37.43, P38.05, P39.17
Foltynie, Tom, O49, O82
Fonseca, Miguel M., P46.13
Foote, Kelly, P36.04
Forbes, Jodie, P09.03, P46.03
Fornaguera, Jaime, P29.12
Fornari Caprara, Ana Leticia, P01.14, P01.15, P01.20, P37.38
Forsaa, Vegard Asgeir, P42.02
Forsgren, Lars, P28.04
Forti, Esther R., P29.11
Fortinsky, Richard, P14.39
Fortuna, Tyler, P34.02
Fosberry, Christine, P17.03
Foster, Erin, O117
Foster, Justin, P14.42
Fothergill-Misbah, Natasha, P14.34, P43.26, P43.31, P45.27
Fougerat, Anne, P06.02
Fox, Cynthia, LBP20.01
Fraga, Angeles Sanchez, P37.31
François, Amaury, P06.01
François, Patricia, P37.21
Frank, Andrew, P32.03
Franke, Sigrid, P35.13
Frankel, Natalie, LBP37.06
Fransen, Nina, P05.03
Frantzen, Veslemøy, P34.05
Frantzen, Veslemøy Hamre, P42.02
Franzén, Erika, P14.11
Franzen, Erika, O97, O114
Frasier, Mark, P34.02
Fratenali, Alessandro, LBP40.01
Frazão, Andre Helene, P25.28
Frazzetta, Giulia, P36.09
Freedman, Dan, P43.06
Freeman, Roy, P20.05, P31.02, P32.04, P32.05, P34.07, P34.08, P34.09, LBP34.01, LBP34.03
Freeman, Thomas, LBP12.05
Freisens, Selena, P35.03, P35.04
Frick, Markus, P13.12
Friedman, Benjamin, P17.07, P24.13, P25.15, P45.34
Frieg, Hendrike, P20.06, P24.03, P37.13
Friend, Alex, P10.02, P10.10
Friend, Alexander, P40.18
Frommel, Bridget, LBP39.05
Frosi, Gabriella, P01.12
Frost, Joshua, P01.16
Frucht, Steven, P10.19
Fryer, Tim, P10.10, P40.18
Fuentes, Alberto, P40.10
Fujii, Shinya, P39.28
Fujimori, Koki, P38.08
Fujita, Hiromi, P03.03
Fukuchi, Claudiane A., P40.01
Fullem, McKayla, P15.10, P28.08
Fuller, Rebecca LM, P39.30
Fumel, Jules, P30.04
Fung, Victor SC, P37.17
Furlanetto, Bruno, P14.35
Furman, David, P02.08
Fuzzati, Marie, P37.21, P43.34
Gámez-Valero, Ana, P05.05
Gøtzsche, Casper, P13.12
Gabriel, Anja, P13.12
Gadala-Maria, Camila, P20.11, P24.01
Gagnon, Bernadine, P25.11
Gago, Miguel F., P46.13
Gaillard, Damien, P06.02
Galati, Salvatore, P15.02
Gales, Jón P., P42.01
Galicia, Christian, P03.08
Gallagher, Casey, P43.18, P46.17
Gallagher, David, P29.08, P39.09
Gallagher, Rosemary, P45.15
Gallardo, Ignacio, LBP07.01, LBP07.02
Gallichio, Joann, P15.08, P45.13
Gallo, Luca, LBP40.01
Galper, Jasmin, P34.11
Galvelis, Kamalini Ghosh, P37.23, P37.30, P43.18, P46.18
Gamble, Kimberly J., P46.05
Gamet-Payrastre, Laurence, P06.02
Gandhi, Sonia, P10.03, P37.03, P37.04
Ganong, Erika, P43.01
Gan-Or, Ziv, P01.03, P29.04
Gant, Katie, P36.09, P37.31
Gao, Fay, P01.17
Gao, Fay, P15.11, P37.47
Gao, Weimin, P10.18
Garçon, Guillaume, P01.07
Garavaglia, Giulia, P13.11
García, Diego Santos, LBP27.01
García-Ramos, Rocío, P35.15
Garcia, Denilson Feijoeiro, P25.30, P25.32
Garcia, Julya Morais, P37.15
Gardner, Joan, P24.05
Garlanka, Mihit Sai, P05.06
Garraux, Gaëtan, P18.05
Garrido, Alicia, P42.01
Garzillo, Kevin, P08.02
Gasser, Jori, P13.13
Gassner, Heiko, P28.07, P39.17
Gatti, Sabrina, P06.14
Gatti, Sabrina Ayelén, P26.05
Gatto, Emilia, P01.21, P29.12
Gaudart, Cécile, P11.01
Gauss, Taylor, P43.27
Gaveel, Ties J., P23.04
Gavra, Vasilina-Zafeira, P12.09
Gazit, Eran, P28.07
Gazizova, Yulia, P39.20
Gelfond, Jonathan, P25.18
Gemos, Anya, P28.01
Genbrugge, Margot, P25.19
Genet, Elisabeth, P06.18
Gentile, Giovanna, P04.06
Genzano, Valerie, P24.05
Geoffroy, Chloe, LBP39.02, LBP39.03
Gerhardt, Greg A, P36.07
Gerretsen, Philip, LBP32.01
Getchell, Nancy, P27.11
Getz, Marjorie, P16.04
Geut, Hanneke, P05.01
Gharabaghi, Alireza, P36.02
Ghasemzadeh, Hassan, P10.20
Ghisays, Valentina, LBP34.04
Ghosh, Debosmita, P26.01
Ghosh, Soumyabrata, P42.01
Ghosh Galvelis, Kamalini, P12.05
Gibbons, Christopher, P20.05, P31.02, P32.04, P32.05, P34.07, P34.08, P34.09, LBP34.01, LBP34.03
Gibbons, Colin, P20.05, P32.05
Giehl, Kathrin, P28.03
Gifford, Larry, P43.03, P43.21, P45.02
Gifford, Matthew, P39.10
Gil, Xavi López, P07.05
Gilat, Moran, P25.19, P25.54, P38.13
Gilbert, Breelyn, P28.01, LBP37.05
Gilbert, Rebecca, LBP46.01
Gilbert, Rebecca, P20.07, P20.08, P21.02, P43.24, P46.15
Gilby, Jonathan, P14.09, P14.15
Gill, Baljeet, P30.03
Gilleran, Clara, LBP37.06
Gillick, Jennifer, P45.33
Gillis, Arnelle, P17.08
Gilmozzi, Valentina, P04.04, P04.06, P04.07
Giordani, Lola, LBP39.03
Giovannoni, Gavin, P29.03
Giove, Rossana Angela, P13.11
Gipchtein, Pauline, LBP06.01
Girges, Christine, P37.18, P38.05, P39.17
Girnadi, Megan, P14.19
Giusti, Veronica, P11.06
Glaab, Enrico, P27.14, P27.16
Glass, Tiffany J., P06.19
Glenat, Valérie, P06.18
Glenn, Gretchen, P43.16
Godinho, Catarina, P43.25
Godley, Patricia, P17.09
Godsey, Laurie, P45.28
Goh, Lina, P23.05
Gokarn, Rishab, LBP37.06
Goldberg, Edward, P36.02, P36.03, P36.04, P36.05
Goldman, Jennifer, O21, O79, P37.32
Goldman, Samuel, P01.17
Goldman, Samuel M., P37.47
González Monje, Mariana Hernández, P39.30
Gonzalez, Marlen, LBP40.06
Gonzalez-Latapi, Paulina, P46.05
Gonzalez-Robles, Cristina, P37.03, P37.04, P37.18, P37.41, P37.43
Gonzalez-Sepulveda, Marta, P06.14
Gopal, Pallavi, P34.03
Gora, Charles, P04.06
Gordon, Richard, P01.10, P01.11, P02.01, P09.06, P10.05, P10.07, P10.08, P34.04, P34.12, LBP06.05
Gorelik, Shai, P46.23
Goris, Maaike, P25.19
Gosselin, Gary, P43.10
Gosset, Pierre, P01.07
Govaerts, Anneke, P29.01
Gow, Sonia, P14.28
Grace, Bola, P37.32
Gracia-Casals, Michelle, P24.04
Graff-Guerrero, Ariel, LBP40.03
Graham, Emma-Louise, P14.19
Grahn, Jessica, P15.02, P23.08
Gram, Hjalte, P06.03, P06.09, P06.10, P10.17
Granholm, Ann-Charlotte, P36.07
Granit, Volkan, P37.06
Grant, Elaine, P14.40
Graves-Swinney, Everett, P43.17
Green, Bianca, P46.05
Green, Charles, P37.39
Green, Ralph, P29.11
Greenamyre, J. Timothy, P10.03
Greenland, Julia, O88, O125
Greenwell, Kate, P13.01, P13.06, P13.07, P46.04
Greenwood, Andrew, P15.02
GREGGIO, Elisa, P09.07
Grellier, Gawain, P06.01
Grey, Elisabeth, P18.04, P19.02, P24.12
Grey, Lis, P19.02
Griffiths, Hannah, LBP16.02
Grigoriadou, Niki, P12.09
Grimani, Irene, P15.09
Grimes, Kelsey, P32.03
Grinspan, Augusto, P36.09, P37.31
Gros, Priti, P14.25
Grosset, Donald, P27.06, P29.08
Groves, Natalie, P09.06
Grubor, Irena, LBP37.04
Grunenwald, Felipe, P06.14
Gu, Haiwei, P10.04, P35.06
Gu, Ivy, P29.11
Guarin, Diego, P39.01
Gudesblatt, Mark, P37.34
Guevara Agudelo, Fredy Alexander, P34.13
Guijarro, Cristi, LBP29.02
Guillermier, Martine, LBP06.01
Guillou, Titouan, LBP39.02
Guinart, Nadia, P43.17, P43.28
Gullotta, Fabiana, P37.19
Guo, Jifeng, LBP36.01
Guo, Joshua, P39.10
Gupta, Resmi, P35.01, P35.02
Gurevich, Tanya, P37.07
Gury, Thierry, P06.18
Gustincich, Stefano, P11.02
Gutierrez, Pedro Paulo, P14.35
Guza, Zach, LBP14.01
Hébert, Marc, P34.13
Højer, Astrid-Maria, LBP35.02
Ha, Connie, P12.10
Ha, Su Hyeon, P39.04
Haak, Maria, P13.04, P23.01
Haar, Shlomi, P37.18
Haas, Aline Nogueira, P15.13
Hackney, Madeleine E, P14.41
Hafler, David A, P37.24
Hagell, Peter, P13.04, P23.01
Hager, Megan, LBP01.01
Hagerbrant, Lynn, P14.40
Hagey, Mackensie, P35.23
Hagstrom, William, P34.10
Haines, Jamie, P20.01, P23.02
Hakanson, Sierra, P30.03
Hall, Deborah A, P39.30
Hall, Dominic, LBP07.02
Hall, Emily, P43.16
Hallack, Andre, P25.17
Halliday, Glenda, O74, O105
Halpern, Angela, LBP20.01
Halstead, Edward, P14.32
Halter, Valérie, P15.02
Hamana, Katy, P14.18, P15.05, P17.01, P37.09
Hamilton, Calum, P38.05
Hamilton, Rebecca, P37.09
Hammer, Lauren H., P37.47
Han, Chao, LBP36.01, LBP36.04
Hand, Annette, P13.01, P13.06, P13.07, P27.05, P27.06, P46.04
Hand, Robert, P14.07
Handler, Alison, P46.14, P46.17
Handley, Emily, P39.06
Hanley, Davron, LBP34.04, LBP34.05
Hanratty, Megan, P45.49
Hans, Felipe, P17.05
Hansson, Oskar, LBP37.04
Hanton, Katherina, P09.06
Hantraye, Philippe, LBP06.01
Harding, Katherine, P24.06
Hardouïn, Jérôme, P02.03
Hare, Orla, P15.15, P25.52
Hares, Orla, P15.14, LBP37.03
Harinsuit, Pynn, P39.03
Harlow, Tanya, P16.01
Harmer, Linda, P37.25, P37.27, P37.28, P37.29
Harmon, Leah, P34.03
Harris, Brian, P39.24
Harris, Celeste, P30.06
Harris, Kent, LBP29.01
Harris, Pamela, P20.11
Harrison, Krista, P27.08
Harrison, Rob, P23.12
Harrison-Jones, Glynn, P43.22
Harry, Bronwen, LBP37.04
Hartman, Rebecca, LBP12.02
Hasanov, Teyyub, P36.08
Hashish, Sara, P34.01
HASSEN, Sirine, P40.06
Hastings, Nataly, P35.20
Hatano, Taku, P23.11
Hatcher, Meredith Rollins, P37.26
Hattori, Nobutaka, LBP29.01
Haunton, Victoria, P23.14
Hausdorff, Jeff, P39.16
Hausdroff, Jeffery M, P28.07
Hauser, Robert, P35.08, P35.09
Hauser, Robert A., P35.02, P37.27
Haworth, Hazel, P23.09
Hay, Meredith, P02.09
Hayat, Liav, P37.07
Heck, Christian, LBP36.03
Hei Yu, Kenny Kwok, P36.06
Heick, John, P25.26
Heitner, Renee, LBP24.01, LBP24.02
Helland, Monica, P34.05
Heller, Gillian Z, P15.14
Hellqvist, Carina, P13.04, P13.09, P23.01
Helman, Emily, P05.04
Hemm, Jessica, P37.02
Hemming, Rebecca, P14.18
Henchcliffe, Claire, O50, O81, P36.06, LBP36.02
Henderson, Davin, P34.04
Hendricksen, Monica, P14.05, P25.15
Hendrix, Kent, LBP37.07
Hendrix, Suzanne, LBP37.07
Henriksen, Tove, P35.01
Henry, Anastasia, O28, O60, P12.10, P34.02
Hensley, Ripley, P16.02, P47.03
Herkes, Geoff, P15.14, P15.15, P25.52
Herkes, Geoffrey, LBP37.03
Herman, Carolyn, P14.12, P39.07
Hernández, Imma, P43.30
Hernández-Vara, Jorge, P05.05
Hernandez, Gerson, P37.48
Hernandez, Jose Alquicira, P10.19
Herrera-López, Mayra, P26.06
Hersh, Bonnie, P39.10
Hess-Pino, Stacey, P20.02
Hetrick, Natalie, P13.08, P37.33
Heutink, Peter, P01.16
Hicks, Andrew, P12.06
Hicks, Andrew A., P04.04, P04.06, P04.07, P11.02
Hiden, Hugo, P28.07, P37.18
Higashi, Ryunosuke, LBP37.09
Higgins, Carmen, P43.27
Higgins, Robyn, P17.03
Higgins, Sean, P32.01
High, Michael, P45.47
Hill, Derek, P37.32
Hill, Emma, P37.12
Hill, Kat, P46.20, LBP17.02, LBP33.01
Hill, Kathryn, P29.07
Hinson, Vanessa, P35.21, P45.03
Hiramatsu, Satoe, P38.08
Hirata, Kosei, P01.06, P01.08
Hirato, Tetsuya, P06.16
Ho, Gary, P12.03
Hoang, Anh, P02.07, P06.06
Hoang, Phuong, P37.47
Hobbs, Aimee, P15.07
Hockensmith, Shelley, P25.03, P25.49
Hockey, Kate, P37.18, P37.40, P37.42, P46.03
Hodges, Priscila D., P01.18, P20.09, P46.18
Hodges, Priscila Delgado, O134
Hoenig, Merle, O77, O109
Hoesl, Florian, P15.02
Hoffman, Lisa, P14.02, P24.01, P24.05
Hogg, Elliot, LBP39.05
Hohl, Kristen, P14.05, P17.07, P24.11, P24.13, P25.15, P25.34
Hojjati, Seyed Hani, LBP05.01
Holenz, Joerg, P46.13
Holiga, Štefan, P40.05
Holley, Andrew, P35.08
Holliday, Parres, P14.33
Holmes, Jeffrey, P13.02
Holmes, Mary Beth, P39.24
Holstege, Henne, O70, O103
Homola, Jaclyn, P35.02
Honda, Karina Yumi Tashima, P37.15
Hong, Chaerin, P39.13, P46.22
Hong, Jin Yong, P40.17
Hong, Young, P10.10, P40.18
Honisch, Claudia, P04.06
Hoogendoorn, Lea, P46.01
Horak, Fay, P25.06, P25.38, P25.43, P38.09, P39.05
Horan, Nicolas, LBP37.05
Horlings, Corinne, P42.01
Horne, Jeremey, P23.05
Horrillo-Maysonnial, Alejandro, P38.03
Horsager, Jacob, P06.09, P06.10, P34.01
Hosny, May, P46.07
Hou, WeiJia, P14.08
Hourcade, Stephane, P06.18
Houson, Hailey, P05.04
Hoyt, Audrey, P12.05, P37.33
Hu, Michele, P27.06, P29.08, P37.32, P38.05
Hu, Michele T., P37.18
Huang, Yuan, P37.24
Hubbard, Michelle, P15.08
Huber, Jessica, P27.02
Huber, Jessica E., P25.37
Hue, Trisha F., P37.47
Huete, Adolfo Jiménez, P28.05
Hughes, Rachel, P46.09
Huh, Jaewon, P05.06
Hulbert, Sophia, P15.07, P23.12
Hulst, Lova, P25.19
Hummers, Eva, P20.06, P37.13
Humo, Muris, P06.02
Humphryes-Kirilov, Neil, P29.07
Hunt, Kevin, P35.23
Hunter, Heather, LBP39.01
Hunter, Sue, P25.40
Hursey, Amelia, P46.14, P46.15
Husain, Aneeq, LBP35.03
Hussain, Sarrah, P20.04, LBP37.07
Hussain-Ali, Shafaq, P37.32, P46.03
Hussein, Samer, P02.02
Hutchison, Calli, P25.03, P25.45
Hutson, T. Noah, P40.12
Huxford, Brook, P20.04
Iakovakis, Dimitrios, P18.05
Ianzer, Danielle, LBP44.01
Ianzer, Manoel Francisco Madeira, P43.11
Ibrahim, Ahmed, P04.03
Ichimura, Daisuke, P39.28
Igarashi, Pamela, P25.13
Ikeda, Kazuhito, P06.16
İlbars, Hilal, LBP31.01
Imbert, Jacques, P06.02
Imery, Peter, P25.51
Imitola, Jaime, LBP36.02
in 't Veld, Sjors G.J.G., P34.06
Inca, Miguel, P01.18, P20.09
Inches, Jemma, P37.43, P38.05
Ingram, Alexandra, P24.04
Ingrassia, Angela MT, P05.01
Intorcia, Anthony, P01.12
Iosif, Ana-Maria, P30.02
isa, Kaoru, P06.16
Isa, Tadashi, P06.16
Isaacson, Stuart, P35.08
Isaacson, Stuart H., LBP37.09
Ishida, Ana Beatriz, P37.36
Ishida, Ana Beatriz Nakasone, P37.35
Ishii, Atsushi, P11.05
Ishii, Takaya, P38.08
Ivy, Cynthia, P39.18
Iyengar, Reethi, P37.10
Jónsdóttir, Sonja R., P42.01, P42.03
Jackson, Jhia, P45.48
Jackson, Lauren, LBP42.02
Jacob, Nina, P15.05, P37.09
Jacobs, Laura, P46.14, P46.17
Jaffee, Michael, LBP27.03
Jagid, Jonathan, P36.04
Jaime, Eduardo Salinas, P27.03, P27.15, P28.05
Jain, Shreya, P14.12, P39.07
Jain, Tarang, P25.26
Jain, Trishala, P13.10
James, Ray, P20.02
James-Cruz, Rachael, P27.04
Jammot, Matthias, P39.14
Jan, Asad, P06.03
Jan, Caroline, LBP06.01
Janer, Alba, P43.30
Jang, Beomjin, P01.08, P10.19
Jann, Kay, P40.11
Jansen, A. Elizabeth, P25.51
Januario-Neves, Ines, P02.03
Jaunarajs, Karen, LBP01.02
Jayabalan, Nanthani, P09.06, P10.05, P10.08
Jehu, Deborah A, P14.41
Jeka, John, P37.01
Jenkins, Mary, P13.02
Jennings, Danna, P39.10
Jensen, Poul H, P06.03
Jensen, Poul Henning, P06.09, P06.10, P10.17
Jeong, Chanhee, P39.04
Jeong, Claire, LBP12.03
Jericó-Escolar, Judith, P06.07, P10.09
Jeyachandra, Christine, P23.10
Jha, Ashwani, P37.18
Jiao, Luyan, LBP36.01, LBP36.04
Jiao, Yang, P14.08, P31.01
Jimenez, Adriana, P20.11
Jimenez, Alberto Jaramillo, P42.02
Jimenez, Patricia Lopez, P43.13
Jimenez Moreno, Cecilia, P13.12
Jimenez-Shahed, Joohi, P35.08, P36.06
Jin, Yan, P10.04
Jo, Sungyang, P12.01, P36.01
Joers, Valerie, P01.09, P10.13
Johansson, Annika, P12.08
Johansson, Hanna, P14.11
Johnson, Aishwarya Mary, P09.06, P10.07
Johnson, Eric, P14.26
Johnson, Rebecca, P34.14
Johnson, Stephanie, P25.20
Johnston, Jennifer, LBP29.01
Jolain, Bruno, P37.12
Jones, Chris, P37.09
Jones, Joanne, P10.06
Jones, Julie, P14.09, P14.19, P25.04, P25.20, P27.05
Jonkman, Laura, P05.03
Jorgensen, Shasta, P46.16
Joseph, Letha, P18.03
Joseph, Theresita, LBP37.05
Joseph, Vincent, P04.06
Joshi-Apte, Tanish, LBP33.02
Jost, Wolfgang H, P35.01
Jouy, Christophe, LBP06.01
Joyeux, Yoann, P37.08, P37.21
Jun, Jin-Sun, P26.03
Just, Mie K, P06.03, P06.09, P06.10
Köchli, Sabrina, P15.02
Kaddouh, Firas, P37.48
Kahanawita, Lakmini, P10.10
Kahl, Katrina, P46.21
Kajzinger, Krisztina, LBP37.08
Kalbe, Elke, P14.11
Kalf, Hanneke, P24.09
Kalia, Suneil, P36.06
Kallevåg, Øystein, P42.02
Kallhoff, Lydia, P24.02
Kalvakuri, Sreehari, P04.06
kam, Tsz Yan, P13.03
Kamem, Lisa, P37.06
Kancharla, Harsha, P39.03
Kanel, Prabesh, P14.30, P27.09, P40.15, LBP40.05
Kang, Gail, LBP37.07
Kang, Suk Yun, P40.17
Kang, Young-Abraham, P25.43
Kannarkat, George T., LBP12.06
Kanthasamy, Anumantha, P10.08
Kanthasamy, Anumantha G, P10.05
Kanzler, Christoph M., P39.10
Kapelle, Willanka, P23.06
Kaplan, Jessica, P17.09, P43.16
Karageorghis, Costas, P15.02
Karapetsas, Athanasios, P06.18
Karppanen, Jenna, P19.03
Karslake, Jason, P46.16
Kasten, Meike, P29.08
Katrib, Chirine, P37.21
Katz, Michael, P46.15
Kauffman, Marcelo, P01.21, P29.12
Kaur, Gurkirat, P11.06
Kausek, Christina, P17.09
Kawauchi, Dory, P39.03
Kayatekin, Can, P06.18
Kayhanian, Saeed, LBP37.04
Kayo, Isabel, P38.04
Kazanski, Meghan, P14.41
Kelley, Christy M., P05.08
Kelliher, Caitlin, P46.17
Kelly, Rachel, P10.17
Kennedy, Connor, P14.07
Kennedy, Deanna, P14.38, P25.53
Kennedy, Terry, P25.07
Kenny, Jack, P01.16, P29.08
Kentros, Michalis, P03.08
Kerchner, Geoffrey A., P37.19, P37.20, LBP37.08
Kern, Drew, P36.04
Kern, Drew S, P37.17
Kernohan, Prof George, P25.16
Kerr, Graham K., LBP39.04
Kershaw, Rachael, P38.02
Kesar, Trisha, P14.41
Kestner, Catherine, P25.15
Khashan, Tarek, P10.19
Kheirbek, Raya, LBP45.01
Khemani, Pravin, PCO4, O17, LBP37.09
Khurana, Vikram, P28.01, LBP37.05
Kiat, Hosen, LBP37.03
Kieburtz, Karl, LBP34.01
Kim, Ain, P05.03
Kim, Han-Joon, P39.04
Kim, Hosung, P40.02, P40.11
Kim, Jeffrey, P02.06, P35.11
Kim, Mi Sun, P36.01
Kim, Min Seung, P40.17
Kim, Minji, P40.11
Kim, Richard, LBP37.05
Kim, Ryul, P26.03
Kim, San Jin, P40.17
Kim, Seok Hun, P15.08
Kim, Yeji, LBP06.02
Kim, Young Ah, P15.03
King, Alexa, P38.05, P39.17
King, Anna E, P32.01
King, Laurie, P25.06, P25.38, P25.43, P37.44, P39.05
Kipnis, Danielle, P14.40
Kirby, Nigel, P37.09
Kirchner, Martin, P13.12
Kirk, Cameron, P38.05, P39.17
Kirkeby, Agnete, LBP37.04
Kitos, Alex, P39.06
Klæstrup, Ida H, P06.09, P06.10
Klæstrup, Ida Hyllen, P10.17
Klaassen, Remco V, P01.02
Klee, Trevor, P46.09
Klein, Christine, P01.16, P29.08
Kleindel, Alisha, P45.09
Kleinschmidt, Lina, P14.04
Klingstedt, Therése, P06.03
Klint, Carl, LBP34.01
Kluge, Annette, P45.05
Kluger, Benzi, O121, P13.08, LBP45.01
Knight, Christopher, P38.11
Knight, Lindsay, P36.09, P37.31
Knowles, Tuomas, P35.20
Knudsen, Karoline, P34.01
Koberstein, Greg, P14.06, P24.02
Koca, Ekin, P39.10
Kojiri, Tomoko, P23.11
Koliqi, Viosa, P37.02
Konradi, Andrei, P10.03
Koo, Brian B, P37.24
Koolman, Tiara SZ, P01.02
Koopmans, Ingrid, P35.23
Kopil, Catherine, P37.32
Kopkow, Christian, P24.03
Kopli, Catherine, P46.15
Kordower, Jeffrey H., P10.18, P36.10
Korell, Monica, P01.17, P27.08, P46.20, LBP17.02, LBP33.01
Korkmaz, Nora, LBP37.06
Koros, Christos, P15.09
KORTHOLT, Arjan, P09.07
Korucu, Aysu Akbaş, LBP31.01
Korucu, Osman, LBP31.01, LBP37.02
Kostrzebski, Melissa, LBP37.07, LBP42.02
Kotter, Mark, P35.20
Kotz, Sonja, P30.05
Kouba, Tomáš, P27.03
Kouli, Antonia, P40.18
Kouli, Antonina, P10.10
Kovacs, Gabor, P05.03
Kozauer, Nick, P37.06
Kozlowska, Justyna, P29.07
Kozlowska, Zhana, P29.07
Krüger, Rejko, O12, O87, P27.14, P27.16, P42.01, P42.03
Krainc, Dimitri, O26, O62
Krane, Catherine, P45.44
Krantz, Leilani, P39.03
Krasko, Maryann, P06.08
Krasucki, Lauren, P14.02
Kraus, Alison, P25.22
Kremer, Philip, P35.23
Krenek, Nancy, P25.53
Krening, Emma, P15.11
Kriesel, Dana, P37.47
Krishna, Vibhor, P36.04
Krishnamurthy, Anushree, P06.09, P06.10
Krishnan, Rajaraman, P06.18
Krueger, Chris, P46.11
Krueger, Christopher, P46.15
Krystal, Andrew, P31.03
Ksendzovsky, Alexander, P39.27
Kuan, Wei-Li, P35.20
Kubler, Raphael, P01.06, P01.08
Kuehni, Claudia E., P18.01
Kuhl, Maggie, P46.05, P46.15
Kuhn, Andrea, P36.02
Kukreja, Pavnit, P35.01, P37.17
Kulic, Luka, LBP37.08
Kumar, Dileep, P40.13, P40.14
Kumar, Rajeev, LBP37.08
Kuncheva, Zhana, LBP29.02
Kuri, Ashvin, P29.03, P38.06
Kustermann, Thomas, P40.05
Kuzkina, Anastasia, P28.01
Kwasny, Damian, P37.22
Kwok, Kevin, P46.14, P46.17
Kyritsis, Konstantinos, P18.05
Kyrousi, Christina, P12.09
Lázaro-Figueroa, Alejandra, P40.03, P40.04
Lévesque, Martin, P02.02, P04.01, P30.01, P34.13
López-Gil, Xavier, P06.07
L’Italien, Gil, P37.06
La Monica, Kristi, LBP17.02, LBP33.01
La Villa, Pablo Miguel Cortadi, P27.03, P27.15, P28.05
Laban, Rhiannon, P20.04
Labib-Kiyarash, Esther, O119, P46.11, LBP45.01
Labrecque, Nathalie, P06.04
Lacaze, Marie, P02.03
Lacey-Solymar, Gillian, P44.03
Lachica, Isaiah, P07.07
Lagos-Villaseca, Antonia, P30.05
Laguna, Ariadna, P05.05, P26.05, P43.30
Lai, Yanhao, P05.02, P10.04, P10.14, P35.06
Lakhdar, Latifa, P06.02
Lamb, Jasmine, P37.40, P37.42
Lambert, Christian, P37.18
Lambrecht, Stefan, P37.22, P39.20
LaMonica, Kristi, P46.20
Lamotte, Guillaume, P14.01
Landers, Merrill, P25.23, P25.24, P25.36, P25.47
Landers, Merrill R., P14.32, P25.42, P27.12,
Landsbaum, E.Amanda, P45.44
Lane, Rachel, P01.10, P01.11
Lanfranchi, Vita, LBP39.01
Lang, Martin, P04.04, P04.06, P04.07
Lange, Johannes, P34.05, P42.02
Langlais, Paul, P12.02
Lanzer, Danielle Alves, P43.11
Lao-Kaim, Nick, LBP37.04
Laouafa, Sofien, P04.06
LaPelle, Nancy R, P37.41
Lapi, Suzanne, P05.04
Larsen, Jennifer, P14.17
Larson, Jonathan, P45.48
Larsson, Helena, P13.04, P23.01
Lasmarrigues, Romane, P10.11
Lau, Brian, P12.10
Laughrey, Cassie, P45.05
Laun, Olivia, P28.01, LBP37.05
Laurell, Katarina, P13.09
Lavdas, Alexandros, P04.06
Lavelle, Aonghus, P39.21
Lavisse, Sonia, LBP06.01
Lavoie-Cardinal, Flavie, P02.04
Lawniczak, James, LBP35.03
Lawrence, Sarah, P37.30
Lawson, Rachael, P27.06, P28.04, P29.08
Lay, Rick, P46.03
Lazzari, Fulviany, LBP44.01
Le Gouellec, Audrey, P32.02
Leach, Samantha J., P37.05
Leal, Thiago Peixoto, P29.12
Leavy, Breiffni, P14.11
Lebel, Manon, P30.01
LeBlanc, Colleen, P43.27
LeBlanc, Randy, P43.27
Lecht, Shimon, LBP09.01
Leclair-Visonneau, Laurène, P10.12
Lecourtois, Sophie, LBP06.01
LeDoux, Mark S., P37.47
Lee, Christina, P39.14, P39.15
Lee, Dasom, P39.04
Lee, Dong Goo, P04.02
Lee, Edward, P34.03
Lee, Grace, P39.22
Lee, Hyunglae, P39.13, P46.22
Lee, Inyoung, P37.17
Lee, Jennifer, P23.08
Lee, Jihyun, P12.01
Lee, Kelsey, P13.02
Lee, Kyungsung, P39.04
Lee, Pei Ying, P02.07, P06.06
Lee, Seungmin, P39.04
Lee, Soyoung, P09.04
Lee, Stephen, P25.44
Lee, Sun Joo, P25.10, P45.10
Lee, Yoomin, P01.03
Leedom, Matt, P07.06
Leedom, Matthew, P07.01
Lees, Andrew, P29.03
Legutke, Beatriz, P37.36
Legutke, Beatriz Regina, P37.35
Lehéricy, Stéphane, PCO8, O35
Lehman, Claire, P37.32, P46.14, P46.17
Lehn, Alex, P10.07, LBP06.05
Lehn, Alexander, P10.05, P34.12
Lehn, Alexander C, P10.08
Lehosit, Jessica, P17.09
Leinweber, Juliane, P20.06, P37.13
Lemon, Lynell, LBP37.06
Lemstra, Evelien, P05.03
Lenizky, Markus, P27.19
Lenkei, Zsolt, P09.05
Leonard, Hampton, P29.06
LEPETIT, Alexis, P40.06
Lerner, Aaron, LBP42.02
Lessard, Nicole, P25.34
Leto, Dara, P12.10
Letourneau, Saul, P46.03
Letro, Grace Helena, P01.21, P29.12
Leung, Sally, P22.01, P25.46, P38.12
Leutert, Stephanie, P46.15
Levanon, Noa, P39.16
Leventhal, David, P14.25
Levesque, Martin, P02.04, P04.06
Levine, Todd, P20.05, P31.02, P32.04, P32.05, P34.07, P34.08, P34.09, LBP34.01, LBP34.03
Lewis, Annie, P21.01, P24.06
Lewis, Henry, P39.03, P43.07
Lewis, Maria, P14.18
Lewis, Patrick, P01.01
LeWitt, Peter, LBP37.08
LeWitt, Peter A., LBP37.09
Li, Dongli, P25.17
Li, Juan, P32.03
Li, Katie, LBP37.05
LI, YAN, P28.04
Li, Yihang, P06.18
Li, Yuanyuan, P29.09, P29.10, P40.16
Liander, Christine, LBP35.02
Liang, Tsao-Wei, P14.07
Liberelle, Maxime, P08.01
Liddle, Trevor, P37.40, P37.42
Liebert, Ann, P15.14, P15.15, P25.52, LBP37.03
Lightsey, Priscilla, P25.53
Liguori, Rocco, P34.09
Lilja, Daniela, P35.18
Lillethorup, Thea, P34.01
Lim, Shen-Yang, O23, P01.16
Lin, Amy, P16.01
Lin, Rui, P38.09
Lin, Steve, LBP11.01
Lind, Amber, P37.27
Lindemann, Michael, P37.22, P39.20, P39.23, P39.25, P39.26
Lindgren, Hanna, LBP06.04
Lindop, Fiona, P27.05
Lindvall, Olle, LBP37.04
Linn, Sara, P43.17, P43.28
Liot, Sophie, P37.21
Lipsmeier, Florian, P37.22, P39.20, P39.23, P39.25, P39.26
Lira, Jumes, P37.44
Lithander, Fiona, O33, O122, P26.08
Lithgow, Gordon, P02.08
Litmer, Claire, P38.10
Liu, James, LBP34.04
Liu, Jun, P29.09, P29.10, P40.16
Liu, William, P25.06, P25.38, P37.44
Liu, Yize, P32.07
Lizarraga, Karlo, P37.33
Lobbestael, Evy, P11.02
Lobo, Marcelo, LBP25.04
Lockette, Kevin, P25.07
Loftus, Andrea, P25.02
Loging, William, LBP35.03
Lombana, Patricia Téllez, P43.32, P43.33
Lombardi, Kylie, P45.09
Lomnicki, Tekki, P45.34
Longhurst, Jason, P25.36, P25.47, P27.12
Longhurst, Jason K., P25.42
Look, Mele, P15.11
Loor Ortiz, Shirley Liliana, P27.10
Lopes, Bruno, P01.21, P29.12
Lopez, Claudia, P37.48
Lopez, Janel, P45.05
Lopez, Tatiana, P01.21
Lopez-Grancha, Mati, P06.18
Lopez-lennon, Cielita, P25.51
Lorente-Picón, Marina, P06.14
Lorenzo-Rivera, Julia, P03.06
Lott, Jason P., P13.12
Lotti, James, P12.03
Lotz, Christian, P45.04
Louie-Gao, Melinda, P36.06
Lousada, Kátia, P17.05, P29.05
Louviere, Michael, P43.27
Lovegrove, Chris, P14.15
Low, Roberto, LBP25.04
Lowell, Emilie, P25.29, P25.33
Lowry, Erin, P46.16
Lozano, Andres, P36.06
Lu, Yun, P37.30
Luauté, Jacques, P17.04
Lubert, Veronika, P15.02
Luca, Corneliu, P36.03, P36.04
Ludwa, Angee, P45.39
Lugo, Victoria, P37.01
Lumsdon, Jack, P14.34
Lunaris, Charlie, P06.19
Lunnon, Katie, P12.08
Luque-Casado, Antonio, P39.11
Luszeck, Tyler, P14.06, P24.02
Luthra, Nijee, P14.01
Luthra, Nijee S., P37.47
Luz, Rafael, P27.18
Ly, Sothary, P02.02
Lydon, Aoife, P46.10
Lyles, Kenneth W., P37.47
Méndez, Mariana Fraustro, P40.04
Möllenhoff, Kathrin, P28.03
Müller, Christiane, P20.06, P37.13
Müller, Martijn, P46.16
Müsch, Kathrin, LBP39.04
Ma, Mei, P14.08
Mañago, Mark, P45.28
Maas, Bart, P23.06
Mabry, Senegal Alfred, LBP40.06
Macedo, Taynara, P21.03, P21.04, P27.18
Macena, Rauisa Gonçalves, P25.27, P25.30, P25.32
Machado, Venissa, LBP37.08
Machado-Hitau, Anaïs, P02.03
Machewitz, Tobias, P13.12
Mackay, Ana, P25.21
Macklin, Eric, P37.33
MacLean, Mhairi, P38.05
Macleod, Angus, P18.04, P19.02, P28.04
Macpherson, Chelsea, P25.33
Madan, Allison, LBP29.01
Maddumage Dona, Shanshika P., LBP39.04
Madhavan, Lalitha, P02.09, P11.05, P12.02
Maebe, Hanne, P29.01
Maebe, Jo, P29.01
Maetzler, Walter, P28.07, P39.30
Mafra, Margit, P14.13, P14.20
Magan, Kristin, LBP42.02
Mageto, Richard, P14.33
Magri, Patricia, P14.13, P14.20
Mah, Greta, LBP24.01, LBP24.02
Mahant, Padma, P23.07
Maher, Samer, LBP24.01
Mahlknecht, Philipp, P42.01
Mahoney-Sánchez, Laura, P10.03
Main, Alyssa, P25.18
Mairano, Paolo, P30.04
Majethia, Priya, LBP07.02
Makarious, Mary, P29.06
Malagon, José Miguel Pinilla, P43.32, P43.33
Malandraki, Georgia, O7, O106, P25.29
Malandraki, Jaime Bauer, P25.29
Malatt, Camille, LBP39.05
Malaty, Irene A, P35.01
Malekmohammadi, Mahsa, P36.03
Malheiros, Guilherme, LBP44.01
Malik, Aryan, P06.12, P06.13
Malin, Eirwen, P15.05, P37.09
Malito, Rachele, LBP40.01
Malkoc, Asiye, P12.06
Mallet, David, P11.01, P32.02
Malliaras, Geroge, P35.20
Malpetti, Maura, P40.18
Mammen, Jennifer, P13.08, LBP42.02
Mançano, Alquiandra, P29.02
Manak, Thomas, P37.02
Mancini, Maria, LBP37.01
Mancini, Martina, O6, O140, P25.06, P25.38, P25.43, P37.44, P38.09, P39.05
Mancino, Emaryn, LBP34.01
Manee, Erika, LBP12.05
Manffra, Fabio, LBP44.01
Manffra, Fabio André Becco, P43.11
Manfredsson, Fredric, O128, P02.05, P40.10
Manfredsson, Fredric P., P05.08, P10.13, P10.18, P36.10
Mangiante, Carlo, LBP39.04
Manhoudt, Gert, P23.04, P26.02
Manor, Yael, P37.07
Mantri, Sneha, P23.03
Manuel, Douglas, P32.03
Manzi, Danni, P18.04, P19.02
Maple-Grødem, Jodi, P28.04, P34.05, P42.02
Marano, Maria, P46.17
Marcelino, Camila Wells Damato, LBP25.04
March, Susan, P45.04
Marchisella, Giuliana, LBP40.01
Marciano, Sabina, P11.03
Marcotte, Sarrah, P20.05, P31.02, P32.05, P34.07, P34.08, P34.09, LBP34.03
Mardell, Mark, P44.03
Marek, Ken, P37.19
Marek, Kenneth, P37.20, LBP37.08
Mari, Zoltan, P37.25, P37.27
Mariani, Diane, P37.02
Mariani, Louise-Laure, LBP39.03
Marinelli, Olivia, LBP24.01, LBP24.02
Marinho, Daniela, P43.22, P46.13
Marini, Stephanie, P04.07
Marinissen, Erik Jan, P46.01
Mark, Julian, P01.09
Marks, Scott, P46.15
Marks, William, O29, O72
Marlonsson, Ares, P36.07
Marmion, David, P10.18, P40.10
Marongiu, Roberta, O138, P01.19, P46.20, LBP17.02, LBP33.01
Marques, Renato, LBP44.01
Marques, Taina, LBP34.04
Marras, Connie, LBP27.02
Marsden, Jonathan, P14.15
Martí, Eulàlia, P05.05
Martí, Maria Jose, P42.01
Martí, Vicent Teruel, P07.05
Martínez, Miguel Inca, P46.18
Martínez-Vicente, Marta, P05.05
Martinez, Claludia, P20.11
Martinez, Claudia, P43.28, P43.29
Martinez, Derek, P36.04
Martinez, Miguel Inca, P29.14
Martinez-Lemus, Juan, P35.12, P45.45
Martinez-Lemus, Juan D, P37.39
Martinez-Martin, Pablo, P39.30
Martinez-Ramirez, Daniel, P01.21
Martinez-Valbuena, Ivan, O2, O14
Martinez-Vicente, Marta, O61, P03.06
Martino, Lucila, P29.05
Martins, Fabricio, LBP44.01
Martins, Marlènes, P02.03
Martins, Pedro, P38.04
Martuscello, Regina, P37.31
Mas, Sara, P43.30
Masese, Peter, P43.26
Massad, Rania, LBP15.01
Massucco, Sara, P34.09
Masurier, Morgane, P24.08
Mata, Ignacio F., P01.18, P01.21, P20.09, P20.11, P29.14, P46.18
Mata, Ignacio Fernandez, P29.12
Matarazzo, Michele, O59, O112
Mathur, Soania, P37.32, P46.20, LBP17.02, LBP33.01
Matos, Luiza, P25.50, P27.18
Matsumoto, Riki, P06.16
Mattei, Daniele, P01.06, P01.08
Matthews, Helen, P37.32, P46.14, P46.15, P46.17, P46.20, LBP17.02, LBP33.01
Matthies, Cordula, P36.02
Matuk-Pérez, Yamil, P40.03, P40.04
Maurenbrecher, Henrik, LBP39.04
Mauri, Nadine, P32.03
Maurissens, Tim, P38.13
Mavroyianni, Ioanna, P15.09
May, Benjamin, P02.08
May, Matthew, P37.12, P46.15
Maya, Stephanie, P04.05
Mazmanian, Sarkis, PCO12, O42
Mazzá, Claudia, P39.10
Mbegbu, Mimi, P10.18
McAlpine, Connor, P37.03, P37.04
Mcbride, Heidi, P06.04
McCarthy, Andrew, P13.01, P13.06, P13.07, P46.04
McCarthy, Danielle, P17.02
McCarthy, Michael, P14.36
McCartney, Daniel, LBP29.02
McClure, Samuel, P40.09
McComish, Rachel, P38.05, P39.17
McCormick, Allyson, P16.02
McCrossin, Mara, P25.31, P38.07
McFarland, Nikolaus R., LBP37.09
McFarthing, Kevin, P37.03, P37.04, P37.11, P37.41, P46.03
McFetridge, Lisa, P28.04
McGarry, Andrew, LBP34.01, LBP37.07
McGarry, Bebe, P45.04
McGinley, Jennifer, P21.01
McGrath, Carmel, P26.08
McHale, Dawn, P43.16
McIsaac, Patrice Tara, P45.37
McIsaac, Tara, P45.36, P45.38
McKay, Lucas, P14.41
McKee, Kathleen, P14.01
McLauchlan, Duncan, P37.09
McLernon, David, P28.04
McWilliams, Tim, LBP42.02
Mead, Kara, P37.24
Meakin, Carmen, P30.03
Meana, Jose Javier, P10.09
Mearns, Desirae, P16.03
Mecheri, Yasser, P29.06
Medel, Maria, P03.06
Medina, Alex, P29.12
Medina-Rivera, Alejandra, P01.21, P40.03, P40.04
Mehanna, Raja, P28.06, LBP37.07
Mehta, Shyamal, P01.12, P40.09
Mehta, Swati, P13.02
Meijerink, Hannie, P37.14
Meinders, Marjan, P23.06, P24.09, P46.01, LBP23.02
Meinders, Marjan J., P15.03
Meinert, Edward, P39.08, P39.12
Meissner, Wassilios, P37.21
Mejia, Elena, P10.19
Meles, Sanne K., P26.02
Melki, Ronald, P03.01, P12.09, LBP06.01
Melo, Joster, LBP44.01
Melo, Victória Sena, P25.23
Meloy, Angela, P14.03
Menard, Caroline, P30.01
Mencacci, Niccolò, P01.16
Mendonça, Felipe, LBP25.04
Menees, Kelly, P10.21
Menees, Kelly B, P10.13
Meneghini, Alessandra Bornhausen, P14.13, P14.20
Meneghini, Chiara, LBP37.01, LBP40.01
Meng, Cheryl, P01.17, P27.08, P37.47
Merchak, Andrea, P01.09
Merchant, Imran, P43.04
Meredith, Jasmine, P06.15
Merkel, Kelly, P23.07
Merkouris, Spyros, P12.09
Merritt, Carolyn, P45.16
Messler, Jordan, LBP35.03
Mesto, Nour, P06.02
Mestre, Tiago, P39.30, LBP27.02
Metevier, Marla, P14.39
Methawasin, Kulthida, P39.02
Metman, Leonard Verhagen, P36.04
Metra, Elisa, P11.01
Metzakopian, Emmanouil, P02.04
Metzler-Baddeley, Claudia, P37.09
Meulien, Didier, LBP35.02
Meyer, Bill, P45.15
Meyer, Christopher, LBP34.01
Meyer, Nadean, P45.15
Meyer, Sophie, P29.03
Meyer, Sophie I, P38.06
Mghendi, Brenda, P43.26, P45.27
Miamoto, Milena Satie, P25.27, P25.30, P25.32
Michalak, Zuzanna, LBP37.08
Mikulski, Heather, P39.23, P39.25, P39.26
Milanese, Vanessa, O113
Mild, Breeann, P38.10
Millard, David, P45.06
Millasseau, Vanille, P11.01, P32.02
Millecamps, Magali, P27.13
Miller, Aidan, P10.15
Miller, Allegra, P37.02
Miller, Ashley, P15.08
Miller, Laurel, P37.43, P46.03
Miller, Rebecca, P24.01
Miller, Stephanie, P38.10
Millett, Michael, LBP07.01, LBP07.02
Mills, Georgia, P37.03, P37.04, P37.18, P37.40, P37.41, P37.42, P37.43, P46.03
Mills, Jodie, P25.16
Milow, Mark, P16.02
Minakawa, Eiko N., P03.03
Minar, Michal, P45.07
Minyard, Rachel, P25.53
Miquel-Rio, Lluis, P06.07, P10.09
Mir, Pablo, P35.01
Miraglia, Dominic, LBP37.06
Miranda, José Garcia Vivas, P25.28
Mirdamadi, Jasmine, P07.07
Mirelman, Anat, O31, O107, P28.07, P39.16
Mischley, Laurie, P20.12, P21.05, P38.14, P13.12, P23.07
Mitchell, Eleanor, P14.22
Mitchell, Gary, P17.08, P23.09
Mitchell, Kyle, P37.47
Mitrotti, Pierfrancesco, LBP40.01
Miyazaki, Masayuki, P03.03
Mochizuki, Hideki, O89, O127
Modugno, Nicola, P14.24, P15.06, P17.06, P45.40
Moehle, Mark, LBP07.01, LBP07.02
Mohamed, Moutaz Bellah, P10.13
Moindrot, Nicolas, P06.18
Molcho, Shira, P37.37
Molinero-Martín, Elvira, P39.11
Mollenhauer, Brit, P42.01
Molohan, Cathy, PCO15, P46.15
Molpeceres, Elba, P07.03
Mondal, Rajib, LBP06.02
Mondal, Snehasree, P26.01
Mondhe, Divya, LBP06.05
Mondhe, Divya Onkar, P10.05, P10.08, P34.12
Monje, Mariana, P37.33
Monnet, Annabelle, P37.19, P37.20, P39.20, P40.05
Montes, Ramon Ortega, P14.31, P15.12
Moore, Lisa, P36.05
Moore, Sarah, P27.07, P39.21
Moors, Tim, P05.07
Moors, Tim E, P05.01
Mora, Javier Pagonabarraga, LBP27.01
Moreau, Caroline, P30.04
Morella, Martino Luca, P01.02, P05.01
Moreno, Emma Muñoz, P07.05
Moresco, Rosa Maria, LBP37.01
Morez, Margaux, P08.01, P09.07
Morgan, Prue, P21.01
Morgante, Francesca, P15.06, P17.06, P36.02, P45.40
Morin, Béatrice, P02.02, P04.01
Moro, Elena, O45, O58, P37.28
Morris, Alan, P35.09
Morris, Huw, P01.16
Morris, Meg, P14.25, P24.06
Morris, Paul, P46.03
Morrison, Neil, P18.04, P19.02
Morse, Michael, P39.30
Morte, Silvia Della, P14.24, P15.06, P17.06, P45.40
Mortensen, Anne, P13.13, P14.43
Mortiboys, Heather, P46.09
Mosberger, Jasmine, LBP06.02
Mosier, Nina, P39.07
Moura, Marcos, P17.05, P29.02, P29.05
Moustaklis, Apostolis, P18.05
Moya-Galé, Gemma, P25.11
Mracskó, Eva Zsuszsanna, LBP37.08
Muñoz, Braulio, LBP07.03
Muñoz-Moreno, Emma, P06.07
Muelhardt, Nicoletta Milani, LBP37.08
Mufson, Elliot J., P10.18
Muhammed, Kinan, LBP39.05
Muller, Martijn, P37.32, P46.14, P46.17
Muller, Scott, P36.10
Muller, Valentina, P01.21, P29.12
Mullin, Stephen, P37.43
Mullins, Daniel, LBP45.01
Muncinelli, Sandra, LBP44.01
Muncinelli, Sandra Elisa, P43.11
Murawska, Magdelena, P20.12, P38.14
Murdock, Chloë, P39.03
Murphy, Claire, P37.03, P37.04, P37.18
Murphy, Kathryn, P37.33, LBP37.07
Murray, Nicole, P20.05, P32.05
Musgrave, Olivia, P14.14
Mustakos, Richard, P36.03
Myers, Brett, LBP25.01
Nóbrega, Kátia Cirilo Costa, P37.15
Nachalon, Yuval, P37.07
Nachtigall, Eduarda, P05.05
Nackaerts, Evelien, P25.54
Naeser, Margaret, P15.14, P15.15, P25.52
Naiem, Tasneem, P46.07
Naisby, Jenni, P27.05, P27.06
Naismith, Sharon L, P32.01
Naito, Tatsuhiko, P10.19
Nakako, Tomokazu, P06.16
Nakamura, Tomoya, P39.19, P39.28
Nakanishi, Etsuro, P06.16
Nakayama, Tatsuo, P06.16
Namini, Ashley, P15.14
Napiórkowski, Natan, P39.23, P39.25, P39.26
Napolitano, Carla, P30.05
Napolitano, Gennaro, P02.04
Narcis, Oriol, P01.06, P01.08, P10.19
Nascimento, Isaíra Almeida Pereira Silva, P37.15
Nascimento, Isaira, P27.18
Nasir, Habib, P28.01
Nasstrom, Elin, P12.08
Natarajan, Aishwarya, LBP12.05
Nativ-Zeltzer, Noga, P37.07
Naumann, Nina, P06.10
Navangul, Anaya, P46.15, P46.17
Navarra, Jordi, P30.05
Nayak, Soubhagya, P39.13, P46.22
Nazeen, Sumaiya, P28.01
Neatrour, Isabel, P28.07, P37.18
Neely, Kristina, LBP17.01
Neighbarger, Noelle, P01.09, P10.16, P10.21, P10.22
Neighbarger, Noelle K, P10.13
Nejtek-Salvatore, Vicki, P27.04
Nelander, Jenny, LBP37.04
Nemazanyy, Ivan, P10.11
Nemykina, Yuliya, LBP14.01
Nesbit, Jamie, P45.36, P45.37, P45.38
Neto, Pedro Braga, P29.12
Newman, Ronnie, LBP15.01
Ng, Dominick, P32.07
Ng, Jessica, P37.47
Ng, Rita, P25.48
Ng, Roy, P35.20
Ngure, Margaret, P35.03, P35.04
Nguyen, Christine, P02.07
Nguyen, Christine To, P06.06
Nicewaner, Melissa, P37.23, P46.18
Nicholas, Doreen, P25.35
Nicholson, Tracy, P37.26, P37.29
Nieuwboer, Alice, O67, P25.19, P25.54, P28.07
Nighah, Krishan, P38.02
Nijkrake, Maarten, P24.09
Niketeghad, Soroush, P36.03, P36.05
Nikolcheva, Tania, P37.19, P37.20, P37.22, P39.20, P40.05
Nilsson, Peter KR, P06.03
Nisbet, Alex F., P06.19
Nishikawa, Noriko, P23.11
Nishimura, Akihisa, LBP37.09
Nitz, Kim, P43.19
Nobile, Marcelo Almeida, P43.11
Nobrega, Katia, P21.03, P21.04, P27.18
Noguchi, Hirofumi, P45.18, P45.20
Noh, Yoo-Hun, P39.04
Nojonen, Tanja, P19.03
Nonnekes, Jorik, P20.10
Nordahl, Timothy, P40.07, P40.08, P43.20
Norris, Scott, LBP33.02
Nouh, Moustafa, P06.04
Novak, Dan, P37.33
Novello, Salvatore, P11.06
Novio-Vasquez, Fernando, P03.06
Noyce, Alastair, P01.16, P14.22, P20.04, P29.03, P29.06, P29.08, P30.15, P37.18, P39.09, P42.01
Noyce, Alastair J., P32.01, P38.06, LBP37.08, LBP42.01
Noyce, Alistair, P39.06
Nunes, Luiz, P29.05
Nuttall, Sofia, P25.17
Nuytemans, Karen, P29.12
Nyadimo, Vivian, P45.27
Nyengaard, Jens R, P06.03, P06.09, P06.10
O'Brien, John, P40.18
O'Malley, Katy, P46.03
O'Meara, Marie, P35.01
O'Neal, Suzanne, P45.36, P45.37, P45.38
O'Shea, Timothy, P06.05
O'Sullivan, John, P10.07
O’Keeffe, Fiadhnait, P27.07
O’Shea, Emma, P27.07
O’Sullivan, John, P09.06, P34.12, LBP06.05
Obergasteiger, Julia, O108, P02.02, P02.04, P04.01
Obinu, Marie-Carmen, P06.18
Odin, Per, P35.02, P46.10
Oeda, Tomoko, P37.17, LBP37.09
Oehlwein, Christian, P37.25
Ofori, Edward, P10.20, P14.42, P33.01, P37.34, P40.09
Ofori-Atta, Blessing, P25.51
Oh, Ji-Hye, P12.01
Oh, Thomas, P02.06, P35.11
Oh, Yoonsang, P40.02
Ojemann, Steven, P36.04
Ojigho, Daisy, P14.12, P39.07
Okeno, Jared, P43.26
Oksas, Catherine, P30.02
Okun, Michael, P36.04, LBP40.02
Olanow, C Warren, LBP34.01
Olguin, Patricio, P01.21, P29.12
Oliinyk, Anna, P35.20
Olsen, Nick, P29.07
Olson, Scott, P35.12, P37.39
Ondo, William, P37.26, P37.27
Onilari, Sola, P37.12
Onoe, Hirotaka, P06.16
Onuigbo, Chiamaka, P35.12, P37.39, P45.45
Onuk, Koray, P37.10, P37.17
Onyeachu, Precious, P39.12
Oosterbaan, Annelien, O16, O51
Oosterhof, Thomas, P14.22
Oosterhof, Thomas H., LBP42.01
Ophey, Anja, P28.03
Oprescu, Florin, P17.03
Orcioli-Silva, Diego, P14.35
Ordóñez, Antonio Jesús Lara, P08.01
Oren, Sheila, P37.37, P46.23
Orme-Smith, Megan, P25.04
Oronsky, Bryan, P01.10, P01.11, P02.01
Orozco, Yuraima, P13.13
Orozco-Vélez, Jorge Luis, P01.21
Ortiz, Bianca Lopez, P29.11
Ortiz, Omaniel, P14.39
Ory-Magne, Fabienne, P37.17
Ossard, Gaëtan, P03.01
Ostreicher-Kedem, Yael, P37.07
Ostrem, Jill, P30.02
Ott, Laurent, P30.04
OTTMANN, Christian, P09.07
Otto, Robin, P37.02
Ouellet, Victor, P25.43
Ouyang, Bichun, P37.02
Owens, Nicole, LBP37.09
Özdemir, Sedat, LBP37.02
Ozgun, Mete, P25.09
Ozsezer, Yakup, P36.08
Pérez-Carbonell, Laura, P29.03, P38.06
Pérez-Carbonell, Laura Laura, P32.01
Płonka, Marta, P39.23, P39.25, P39.26
Pachicano, Marcelo, P10.13
Packer, Emma, LBP39.01
Padgett, Parminder, P25.44
Padhi, Piyush, P10.05
Pagano, Gennaro, P37.19, P37.20, P37.22, P39.20, P40.05, LBP37.08
Pahwa, Rajesh, P37.25, P37.27, LBP37.09
Paire-Ficout, Laurence, P17.04
Paiva, Izabel, LBP37.06
Pal, Shankar, P26.01
Paladino, Sandra Luft, P14.13, P14.20
Pallab, Md. Rezwanul Akter, P07.01, P07.06
Pallmann, Philip, P37.09
Pang, Karen, LBP06.02
Pang, Menglan, P39.10
Pantazopoulou, Marina, P12.09
Pantelyat, Alexander, P10.01
Paolantonio, Paolo, P15.02
Paolone, Giovanna, P11.02
Papadopoulou, Marianna, P15.09
Papagiannakis, Nikolaos, P15.09
Papanastassiou, Alexander, P36.04
Papapanagioutou, Vasileios, P18.05
Papastefanaki, Florentia, P35.22
Pape, Lise, P39.18
Parab, Ashwini, P37.17
Parades, Deyran, P27.08
Pardini, Andrea Lima, P43.11
Pardon, Magalie, P06.18
Paredes, Deyran, P46.20, LBP17.02, LBP33.01
Parent, Jourdan, P20.05, P31.02, P32.05, P34.07, P34.08, P34.09, LBP34.03
Parent, Martin, P04.06
Park, Gilsoon, P40.02, P40.11
Park, Hyejung, P06.18
Park, Jade, P31.04
Park, Jang Woo, P40.17
Park, Jongsil, P09.04
Park, Sarah, P23.08
Parker, Anita, P46.21
Parkinson, Mark, P27.05, P27.06
Parkkinen, Laura, PCO1
Parkyn, Brandon, P27.01
Parlar, Sitki Cem, P01.03
Parmar, Malin, LBP37.04
Parmar, Raveena, P06.15
Parra, Juan Carlos, P35.01
Pasaye, Erick Humberto, P40.03, P40.04
Patel, Bina, P10.02
Patel, Sapna, P37.24
Patjane, William, P43.20
Patterson, Kenneth, P17.09
Patterson, LiAna, P24.13
Paul, Ashley, P24.01
Paul, Gesine, LBP37.04
Paul, Kimberly, P01.22
Paul, Morgane, P43.34
Paul, Serene, P23.05, P39.30
Pauly, Claire, P27.14, P27.16, P42.01, P42.03
Paumier, Katrina, P34.10
Pautet, Sylvain, P12.07
Pavese, Nicola, LBP37.08
Pavese, Nicola, O90, O124, P37.19, P37.20
Pavone, Federico, LBP39.02, LBP39.03
Payne, Kayleigh, P27.02
Paz, Verónica, P06.07, P10.09
Peña, Rosa, P20.11, P43.20
Peña, Susana, P01.21, P29.12
Peñuelas, Nuria, P06.14
Peabody, Taylor, P36.03
Peattie, Alexander, P10.10, P40.18
Pedata, Anne, P46.16
Pedersen, Mads, LBP35.02
Pederson, Viviana, P06.12
Pederson, Vivianna, P06.13
Pedlow, Katy, P25.16
Pedrosa, David, P36.02
Pedrotti, Giulia, P04.04
Peerbolte, Tessa Femke, LBP23.02
Peeters, Marloes, LBP39.01
Peixoto-Leal, Thiago, P01.21
Pellecchia, Jacqueline, LBP34.01
Pellegrino, Nathália Mendes, P40.01
Pelowski, Matthew, P15.03
Pena, Rosa, P20.07, P21.02, P43.24, P43.29, P45.44
Peng, Amy, P43.23
Penn, Melissa, P13.12
Pensyl, Claire, P37.02
Penuela, Sara, P37.01
Peralta, Modesto III, P34.13
Peralta, Modesto R., P04.06
Perani, Daniela, LBP40.01
Perdrix, Esperanza, P01.07
Pereira, Heloisa, P27.18
Pereira, Joana B, LBP40.01
Pereira, Nathalia, P27.18
Pereira, Nathalia Brito, P37.15
Perez, Carlos, P10.19
Perez, Mikaela Rosen, P10.19
Perez, Ruth G., P02.05
Perez, Sylvia E., P10.18
Perfetto, Eleanor, LBP45.01
Periñan, Maria Teresa, P01.16, P29.06
Perkins, Jacque, P37.47
Perlman, Susan, LBP37.09
Perrier, Prunelle, P06.02
Perulli, Mia, P08.02
Peterson, Daniel, PCO5, O18, P25.25, P37.34, P39.13, P39.18, P40.09, P46.22
Petrey, Beth Farber, P36.03
Pettigrew, Tiffany, P10.18
Petty, Rebecca, P37.41, P37.42, P37.43
Phillip, Cheri, LBP39.05
Phillips, Julia, P32.06
Phillips, Justin, P20.05, P32.05
Philpott, Carl, P14.22
Picón, Marina Lorente, P04.06
Piccini, Paola, LBP37.04
Pichiecchio, Anna, LBP37.01
Pichler, Irene, P04.04, P04.06, P04.07
Pickett, Kristen, P13.13, P14.43
Piemonte, Maria, P25.50, P27.18
Piemonte, Maria Elisa, P21.03, P21.04
Piemonte, Maria Elisa Pimentel, P25.13, P25.27, P25.28, P25.30, P25.32, P28.06, P37.15, P37.16
Pierce, Carmen, P37.02
Pigeon, Caroline, P17.04
Pihlstrøm, Lasse, P05.01
Pilcicka, Aleksandra, P37.11, P46.09
Pilitsis, Julie, P36.04
Pillutla, Sree Vani Poorna, P11.05
Pincherle, Alexander, P42.03
Pinheiro, Márcia Resende, LBP25.04
Pino, Miguel, P25.41
Pintchovski, Sean A., P10.03
Pinzon, Maria Mora, P13.13
Piotto, Martial, P32.02
Pisani, Antonio, LBP37.01
Pischedda, Francesca, P11.02, P12.06
Pitton Rissardo, Jamir, P01.20
Pitzer, Kenneth, P37.11
Pizzillo, Clemie, P20.11
Plagenz, Jake, P16.01
Plitnick, Barbara, P31.04
Poewe, Werner, P42.01
Pol, Rodriguez-Carreras, P03.06
Poliakoff, Ellen, P15.02
Politis, Marios, LBP37.08
Pollard, Eli, P24.01
Pollard, Elizabeth, P24.05
Polymeropoulos, Christos, P35.22
Polymeropoulos, Mihael, P35.22
Poma, John, O4
Pombo, Eva, P02.09
Pomeshchik, Yuriy, P12.08
Pompe, Nils, P32.02
Ponce-Fernández, Carlos, P40.03, P40.04
Pongmala, Chaetkew Fay, P14.30, LBP40.05
Pongmala, Chatkaew, P40.15
Popa, Daniela, P07.02
Poplin, Alenka, P13.10
Popp, Werner, P37.22, P39.20
Porcher, Raphaël, P37.21
Porciuncula, Franchino, P39.14, P39.15, P39.24, P40.07, P40.08
Porrill, Sophia, P14.10
Porter, Gillian, P14.36
Porto, Michelle, P37.33, LBP37.07
Posey, Janna Jernigan, P10.21
Post, Bart, PCO13, P23.06
Posthumus, Matthijs, P37.14
Postma, Elbrich M., P23.04, P26.02, P37.14
Poston, Kathleen, PCO6, O3, O13, P46.14
Postuma, Ron, O137
Postuma, Ronald, P37.19
Postuma, Ronald B., P37.20
Potashman, Michele, P37.06
Powers, Jim, P45.44
Pradas, Eddi, P03.06
Prades, David, P43.30
Pramstaller, Peter, P12.06
Pramstaller, Peter P., P04.04, P04.06, P04.07, P11.02
Prasad, Aakash, P26.08
Prawitt, AnnaLisa, P45.09
Press, Iggy, LBP35.03
Preston, Camille, LBP07.01, LBP07.02
Preston, Elisabeth, P14.14
Prettyman, Richard, P45.23
Previero Luz, Larissa Isabelle, P14.35
Price, Beverley, P46.14, P46.17
Prieto, Laura, P13.13, P14.43
Prince, Cherolyn, P14.23
Prins, Eva M., LBP42.01
Prinssen, Eric, LBP37.08
Pross, Nathalie, P37.12, P37.20, P37.22, P39.20, P40.05
Prudon, Nicolas, P02.03
Prutton, Kendra, LBP36.02
Pryor, Brian, P37.01
Przychodzen, Bart, P35.22
Pu, Kelly, P23.03
Pugh, Cheryl, P37.03, P37.04, P37.40, P37.42
Pulliam, Haley, P40.12
Pullman, Mariel, P29.11
Punjani, Nahid, P33.01
Puri, Natasha, P12.10
Pushparatnam, Kuhan, P46.03
Pyke, Wesley, P18.02
Pyle, Ian, P37.31
Qian, Ruobin, LBP36.01, LBP36.04
Quaegebeur, Annelies, P10.06
Quah, Corrine, P39.09
Queiroz, Rodrigo Guimaraes, P05.04
Quinn, Caitríona, P14.11
Quinn, Joseph, P38.09
Quinn, Lori, P14.40, P22.01, P25.33, P25.46, P38.12, P46.21
Quintana, Rosa, P46.14, P46.17
Quintana Pena, Valentina, P01.16
Quintero, Jorge, P36.07
Quiros, Olivia, LBP37.06
Qureshi, Ferhan, P34.10
Qureshi, Irfan, P37.06
Rábano-Suárez, Pablo, P39.30
Racelo, Lynn, P01.17, P27.08, P37.47
Racette, Susan B., P45.46
Rafferty, Miriam, P14.02, P14.05, P17.07, P24.11, P24.13, P25.15, P25.34, P38.10, P45.34
Rafiei, Forouzan, P14.41
Raghunathan, Anusha, P25.46
Ragothaman, Anjanibhargavi, P39.05
Rahman, Saifur, P35.20
Rai, Shreya, P28.01
Raikes, Adam, P37.48
Rainbow, Daniel, P10.06
Raineri Tapies, Martinna, P01.18
Raitt, Jane, P45.23, P45.23
Raj, Towfique, P01.06, P01.08, P10.19
Rajput, Ria, P41.02
Ralph, Abigail, P06.04
Ramachandran, Sujith, P15.14, P15.15
Ramalingam, Nagendran, P02.05, P12.03
Ramaswamy, Bhanu, P27.05
Ramdhani, Ritesh, P36.04
Ramirez, Daniel Martinez, P29.12
Ramirez-Virella, Jariel, P36.10
Ramirez-Zamora, Adolfo, P36.03
Ramstack, Megan, P14.43
Ranchet, Maud, P17.04
Rane, Neha, P18.02
Ranghetti, Alessandra, P13.11
Rao, Tejala, P20.04
Raphael, Karen, P14.21, P47.02
Rascol, Olivier, P24.08, P35.05, P37.21
Rautenberg, Josiah, P02.09
Ravache, Rosicler, P14.13, P14.20
Ravier, Magalie, P06.02
Ravindran, Priyadarshini, P12.12
Raychaudhuri, Soumya, P10.19
Raymond, Deborah, P29.11, P31.04
Raymond, Frédéric, P34.13
Ready, Megan, P20.01
Real, Caroline C, P06.03, P06.09, P06.10
Reaume, Carlin, P25.05
Rebholz, Heike, P09.05
Redd, Hannah, P14.05, P17.07
Reddy, Abhinav, P14.12, P39.07
Reddy, Vijaya L, P37.24
Redon-Munoz, Pau, LBP39.02
REDOUTE, Jérôme, P40.06
Reed, Hope, P14.32
Rees, Kelly, P45.01
Reese, Ben, P36.03
Rege, Kavita, P42.01
Regmi, Sanjib Mani, P43.02
Rehbein, Carlos, P14.29, P14.39
Reid, Jennifer, P14.40
Reid, Tony, P01.10, P01.11
Reilly, Hema, P46.05
Reinbacher, Rene, P27.07, P39.21, P39.29
Reinhardt, Jessica, LBP07.01, LBP07.02
Rendon, Ruby, P43.15
Rentería, Miguel E., P40.03, P40.04
Reyes, Óscar, P39.10
Reyes, Adriana, P37.12, P37.19
Reyes, Paula, P40.03, P40.04
Reyes, Sol, P10.13
Reyes-Pérez, Paula, P29.06
Rezeli, Melinda, P12.08
Ribeiro, Maria Eduarda, P25.23, P25.24
Riboldi, Giulietta, P10.19
Ricci, Benedicte, LBP37.08
Ricciardi, Lucia, P15.06, P17.06
Ricciardi, Luciana, P45.40
Richard, Irene, LBP37.07
Richard, Yaashwini Laura Selwyn Selwyn, P06.06
Richards, Kirsten, P45.33
Richards, Yaash, P02.07
Richardson, Eric, P43.01
Richardson, Kelly, P25.37, P27.02
Richfield, Edward, P18.04, P19.02, P24.12
Rideout, Hardy, O27, P03.07, P03.08
Rieder, Melissa, P05.07
Riekschnitz, Diana, P12.06
Riela, Ilaria, P13.11
Rigg, Aileen, P18.04, P19.02
Riley, Elizabeth, LBP40.06
Riley, Kathryn, P45.36, P45.37, P45.38
Ringel, Claudia, LBP27.01
Rio, Lluis Miquel, P07.05
Rioux, Véronique, P04.06, P30.01, P34.13
Rippon, Daniel, P13.06
Rissardo, Jamir Pitton, P01.14, P01.15, P37.38
Ritter, Robert, P35.12, P37.39
Rittman, Tim, P10.06
Ritz, Beate, P01.22
Rivadulla, Nolo, P43.32, P43.33
Rivera, Monica, LBP25.03
Ro, Kumhee, P44.02
Roberts, Angela, O55, O68
Roberts, Melissa, P12.10
Roberts, Meredith, P14.04
Robichaud, Sarah, P14.25
Robinson, Fiona, LBP20.01
Robinson, Liz, P46.12
Robson, Hailey, P25.37, P27.02
Rocha, Emily M., P10.03
Rochester, Lynn, P14.34, P27.06, P28.07, P37.18, P38.05, P39.17, LBP39.01
Rochester, Tarah Breanne, P25.08
Roddewig, Lea, P20.06, P37.13
Rodríguez, Mayela, P01.21
Rodríguez Oroz, María Cruz, PCO9, O37, P27.03, P27.15, P28.05
Rodrigues, Giulia Torres, P14.35
Rodrigues, Luiz Henrique, P14.13, P14.20
Rodrigues, Rubia, P38.04
Rodrigues, Rute, P37.36
Rodrigues, Rute Vieira e Magalhães, P37.35
Rodriguez, Diego, P28.01, LBP37.05
Rodriguez, Mayela, P29.12
Rodriguez, Raphael, P07.08
Rodriguez, Tabitha, P11.04
Rodriguez-Martin, Daniel, P14.31
Rodriguez-Oroz, Maria Cruz, P38.03
Roe, Courtney, P37.33
Rogers, Katherine, P23.09
Rogers, Rebecca, P14.10
Rogus-Pulia, Nicole, O43, O54
Rohl, Jenn, P46.14
Rohl, Jennifer, P46.17
Rojas, Sandra, P30.05
Rolland, Anne-Sophie, P01.07
Rolli-Derkinderen, Malvyne, P10.12
Romero, Klaus, P37.32
Romero-Laboureur, Eugénie, P03.01
Romero-Maysonet, Lilliana, P22.01
Romero-Ramos, Marina, PCO10, O39, P06.09, P06.10, P10.17
Roper, Jaimie, LBP20.02
Roper, Katherin E, P10.05, P10.08
Roper, Katherine, P10.07
Roque, Antonio C., P25.28
Rosa, Bruna, P25.13
Rosa, Hans, P29.05
Rosal, Angenelle Eve, LBP40.03
Rosato-Siri, Marcelo, P12.06
Roscher, Patrick, P14.03
Rose, Dawn, P15.02, P23.08
Rosen, Mikaela, P01.06, P01.08
Rosenfeld, Sheera, P24.07, P24.10, P43.16, P47.03
Rosenfeldt, Anson, P25.51
Rosenthal, Liana, LBP34.01
Rosenthal, Liana S., P10.01
Ross, George Webster, P01.17, P15.11, P25.07
Rossi, Ben, P14.16
Rossi, Jason, P03.02
Roudieres, Sebastien, P06.18
Rowe, James, P10.06
Rowsell, Kira, P39.09
Roy, Akash, P10.01, LBP34.01
Roybon, Laurent, P12.07, P12.08
Royo, Victor, P43.30
Roytman, Stiven, P40.15, LBP40.05
Rozemuller, Annemieke, P05.03
Rubin, Lyubov, P25.31, P38.07
Rubinsztein, David, O57, O115
Rubrecht, David, P46.11
Rudisch, Denis Michael, P06.08, P06.19
Ruffner, Joshua, P37.23, P46.18
Ruiz-Contreras, Alejandra Evelyn, P40.03, P40.04
Russell, David, P46.14
Russell, John A., P06.19
Ruston, Francisco Contreras, P25.21, P30.05
Rusz, Jan, P27.03
Rutley, Rachel, P25.40
Rutten-Jacobs, Loes, P37.12
Ruzza, Paolo, P04.06
Ryan, Barry, P29.07
Sánchez, Karen, P29.02
Sánchez-Ferro, Álvaro, P39.30
Saade, Joseph, P32.03
Sachs, Judith, P45.01
Sacilotto, Elena, P13.11
Sadeghirad, Habib, P10.06
Sadighian, Hooman, P02.06
Safa, Laura, P30.03
Safarpour, Delaram, P37.10, P37.17
Saffie-Awad, Paula, P01.04
Saint-Hilaire, Marie, P20.02, P39.14, P39.15, P43.20
Saint-Hilaire, Marie-Helene, P39.24
Sakellariou, Dikaios, P17.01
Salari, Mehri, P28.06
Salehe, Said, P05.02, P10.04, P10.14, P12.11, P35.06
Salido, Tiffany, P14.03
Salloum, Layla C.S., P40.01
Salm, Sandra, P24.03
Salokhiddinov, Marufjon, P40.13, P40.14
Saltarrelli, Jerome, P35.12
Saltmarche, Anita, P15.14, P15.15, P25.52
Salvatore, Michael, P03.05, P27.04
Samiotaki, Martina, P12.09
Samuel, Debbie, P26.08
Samuel, Shanon, P05.04
Sanchez, Raymond, P37.25
Sandmann, Thomas, P12.10
Sandoval, Ivette, P02.05, P36.10, P40.10
Sandoval, Ivette M., P05.08, P10.13, P10.18
Sani, Sepehr, P36.04
Sansare, Ashwini, P25.53
Santamaria, Anna, P43.30
Santos, Francielle, P38.04
Santos, Gabriel Venas, P25.27, P25.28, P25.30, P25.32, P37.15, P37.16
Santos, Heloisa Pereira, P25.30, P37.16
Santos, Larissa Bitarães Rodrigues, P25.27, P25.30, P25.32, P37.15
Saporta, Nira, P37.37, P37.45, P46.23
Saraceno, Taylor, LBP37.05
SARACHO, ROBERT HIRIGOYEN, P43.14
Sardi, Sergio Pablo, P06.18
Sarle-Valles, Pau, P03.06
Sarmiento, Ignacio Keller, P01.16
Sarna, Justyna, P37.17
Sarno, Marina, P24.04
Sarrafha, Lily, P12.10
Sarraudy, Marie, P07.02
Sarriés-Serrano, Unai, P06.07, P10.09
Sarva, Harini, P36.06, LBP37.08
Sarvestan, Javad, LBP39.01
Sasaki, Jhony, LBP44.01
Satagopam, Venkata, P42.01
Satani, Nikunj, P37.39
Satterwhite, Angela, P17.09
Saunders, Tim, P39.06
Saunders-Pullman, Rachel, PCO16, P10.19, P29.11, P31.04
Sauvee, Mathilde, P32.02
Savıcı, Volkan, LBP37.02
Savchenko, Ekaterina, P12.08
Savica, Rodolfo, P28.06
Sawada, Makoto, P39.19, P39.28
Sawamoto, Nobukatsu, P38.08
Sawamura, Masanori, P06.16
Scampavi, Louis, P35.06
Scanlan, Kathleen, P25.38
Scelsi, Marzia, P39.20
Schade, Sebastian, P42.01
Schaefer, Rebecca, P15.02
Schaepers, Miriam, P10.02
Schaer, Alessandro, LBP39.04
Schambach, Christopher, P37.47
Schapira, Anthony, P37.03, P37.04
Scheiner, Linda, LBP37.08
Scheperjans, Filip, O92
Scheschonka, Astrid, P35.03, P35.04, LBP27.01
Schiess, Mya, P35.12, P37.39, P45.45
Schiff, Gilat, P36.09
Schlossmacher, Michael, P32.03
Schmid, Franz R., P15.03
Schmidt, Michelle Vanessa, LBP36.03
Schmidt, Minna, P02.08
Schmidt, Ronny, P35.20
Schmier, Katrina, P37.33, LBP37.07
Schmit, Matthew, P06.12, P06.13
Schmit, Nora, P20.06, P37.13
Schneider, Kevin, P02.08
Schneider, Ruth, P12.05, P37.33, P37.47
Schneider, Ruth B., LBP42.01
Schrag, Anette, P14.09, P29.03, P37.03, P37.04, P37.18, P38.06
Schroeder, Jens, P02.03
Schubbe, Emily, P20.01
Schuh, Artur, P29.12
Schuller, Adam, LBP01.01
Schumacher-Schuh, Artur, P01.21
Schuurman, Rick, P36.02
Schwamborn, Jens, O126
Schwartz, Cathe, P14.16
Schwarzschild, Michael, P37.33
Schwarzschild, Michael A., P37.47
Schwingenschuh, Petra, LBP27.01
Sciani, Juliana, P29.02
Scianni, Aline Alvim, P25.23, P25.24
Sconfietti, Ileana, P13.11
Scott, Brittany, P45.29, P45.30, P45.31, P45.32
Scott, Kirsten, P10.10
Scott, Nicholas, P35.20
Scott, Peter, P27.09, P40.15
Scott, Peter J. H., P14.30
Sedhed, Jenny, P14.11
Seeds, William, LBP04.01
Segala, Vanessa Techio, P14.13, P14.20
Seibyl, John P, P37.24
Sellier-Montaigne, Loïc, P10.12
Selvaraji, Sharmelee, LBP06.02
Semeraro, Fernanda Marino, P25.30, P37.16
Senft-Daniel, Isabell, LBP23.01
Senn, Olivier, P15.02
Seppi, Klaus, P37.20
Serini, Matilde, P13.11
Seritan, Andreea, P30.02
Serpieri, Valentina, LBP37.01
Serrano, Geidy, O99, P01.12
Seshadri, Sandhya, P13.08, P37.02
Sesia, Thibaut, P06.03
Seto, Todd, P15.11
Settle, Sydney, P45.44
Seuschek, Caitlyn, P24.11
Sevitz, Jordanna, P25.29, P25.33
Sfikas, Evangelos, P15.09
SGAMBATO, Véronique, P40.06
Shah, Emma, LBP20.01
Shah, Hiral, P43.29, P43.29, P46.21
Shah, Jinagna, LBP20.01
Shah, Megha, P35.01, P35.02, P37.10
Shah, Nami, LBP42.02
Shah, Poonam, LBP20.01
Shahid, Anisa, P29.03
Shahid, Anisa J, P38.06
Shahkhali, Morvarid Ghamgosar, P29.04
Shakeshaft, Clare, P37.03, P37.04
Shaltouki, Atossa, P10.03
Shambetova, Cholpon, P29.06
Shapiro, Benjamin, P14.07
Shariati, Nima, LBP37.08
Sharma, Anuj, P13.10
Sharma, Samya, P39.03
Sharp, Deborah, P25.37, P27.02
Shaw, Krisha, P14.39
Shearer, Georgette, P46.09
Sheedy, Tiana, P39.24
Shelly, Shahar, P37.45
Shelton, Erin, P14.16
Shen, Changyu, P39.10
Shepherd, Victoria, P17.01
Sherman, Scott, P06.15, P37.48
Shi, Jiong, LBP36.01, LBP36.04
Shiell, Anushka, P43.24
Shih, Ludy C., LBP37.07
Shill, Holly, P01.12
Shima, Atsushi, P38.08
Shin, Jung Hwan, P39.04
Shin, Tammy, P25.39
Shiozawa, Kaymie, P39.14
Shivacharan, Rajat, P36.02, P36.03, P36.04
Shonhard, James, P10.06
Short, Alison, P15.02
Shpiner, Danielle, P24.04
Shpunt, Dina, P37.07
Shrader, William D., P10.03
Shrewsbury, Steve, LBP35.01
Shukurova, Gunay, P36.08
Shuler, Marshal, P26.08
Shulman, Joshua, P01.16
Shuman, Ruby, P15.11
Siadati, Abdolreza, P36.04
Siddiqui, Mustafa, P36.04, P37.47
Siddiqui, Omer, P35.23
Siderowf, Andrew, O110, LBP37.08
Sieberts, Solveig, P37.33
Siegel, Sharon, LBP15.01
Silva, Bruna Hiromi Tateyama, P37.15
Silva, Jocelyn, LBP42.02
Silva, Paloma Rodrigues, P25.30, P37.15, P37.16
Silva, Verónica Paz, P07.05
Silva-Batista, Carla, P25.06, P25.38, P37.44, P39.05
Silverdale, Monty, P27.05, P27.06
Silverstone, Ilana, P45.12
Silvestri, Erica, P11.02
Šimek, Michal, P27.03
Simervil, Esdras, LBP35.03
Simitsi, Athina-Maria, P15.09
Simon, Sarah, P29.11
Simonet, Cristina, P29.03, P30.15, P32.01, P38.06, P39.09, LBP37.08
Simonson, Anna, P14.16
Simpson, Ian, P29.07
Simpson, Joelle, LBP27.03
Simu, Mihaela, P35.01
Simuni, Tanya, P37.06, P37.19, P37.20, P37.32, P37.33, LBP37.08, LBP42.02
Sinclair, Rachel, P17.09
Singer, Carlos, LBP37.09
Singh, Alpana, LBP34.04
Singh, Arun, P07.01, P07.06
Singh, Dharmesh, P40.13, P40.14
Singhal, Tarun, LBP37.05
Singleton, Andrew, P01.16, P37.23
Singleton, David, P37.18
Sirico, Thiago, P37.36
Sirico, Thiago Martins, P37.35
Siu, Carroll, P46.03
Siu, Tin Wai Tiffany, P24.04
Sivaramakrishnan, Anjali, P25.18
Skjærbæk, Casper, P34.01
Skorvanek, Matej, P39.30
Slodkowska-Barabasz, Joanna, P13.01, P13.07
Sloutsky, Regina, P40.07, P40.08
Ślusarz, Robert, P27.01
Smaller, Kevin, P14.05
Smalley, Alan, LBP39.01
Smallman, Kim, P15.05, P37.09
Smayda, Kirsten, P39.24
Smeyne, Michelle, P11.04
Smeyne, Richard, O85, O95, P11.04
Smieszek, Sandra, P35.22
Smigorski, Krzysztof, LBP37.08
Smiley, Adrianne, P24.01, P43.18
Smilowska, Katarzyna, P28.06
Smit, Augustus B, P01.02
Smith, Emma, P06.15
Smith, Laura, P20.04, P30.15
Smith, Laura J, P38.06
Smith, Morganne, P26.07
Smith, Reuben, LBP37.04
Smith, Ryan, P13.10, P35.19
Smith, William, P30.02
Smuniewsky, Kevin, P45.03
Snyder, Sandy, P25.37
Soh, Sze-Ee, P21.01
Sohur, U. Shivraj, LBP37.09
Soileau, Michael, P35.08, P37.26, LBP37.07
Sokolov, Amit, P36.09
Solano, José, P30.01
Soliz, Jorge, P04.06
Song, Rhayun, P44.02
Sorace, Anna, P05.04
Sordyl, Ronika, P18.02
Sorgato, Eduarda Hahn, P15.13
Sori, Sheila, P14.12, P39.07
Sortwell, Caryl, P06.15
Soto, Isabel, P27.04
Soto, Stephanie, P45.36, P45.37, P45.38
Soto Linan, Victoria, P04.06
Southgate, Alex, LBP29.02
Souto, Arthur, P05.05
Soutrenon, Rémi, P27.13
Souza, Adriana, P17.05
Souza, Aline, P37.36
Souza, Carolina, O78, O116
Sovera, Andrea, P02.03
Sowden, Ryann, P18.04
Spee, Blanca T.M., P15.03
Speelberg, Daniël, P23.06
Sperandio, Olivier, P03.01
Spicer, Timothy, P35.06
Spindler, Lennart, P40.18
Spindler, Meredith, LBP37.07
Srivastav, Sunil, P01.10, P01.11, P02.01, P34.04, LBP06.05
Stack, Lucy Collins, P27.07, P39.21
Stacy, Mark, P35.21, P35.21
Stadelmann, Martina, P15.02
Stalker, Andrew, LBP37.07
Stancati, Jennifer, P36.10
Standaert, David G., P37.10, P37.17, LBP37.08
Stanton, Harley, P39.06
Stark, Patrick, P23.09
Stebbins, Glenn, P27.08
Stebbins, Glenn T, P39.30
Steece-Collier, Kathy, P06.15, P36.10
Stefan, Arianna, P11.02
Stefanis, Leonidas, P12.09, P15.09
Steffen, Douglas Korbes, P14.13, P14.20
Stegemöller, Elizabeth, P15.10, P35.19
Stegemoller, Elizabeth, P13.10, P28.08, P45.44
Step, Kathryn, P29.06
Stephenson, Diane, P37.32, P46.14, P46.16, P46.17
Steppe, Maxime, P24.09
Stevens, Evelyn, P37.02, P43.18, P46.05, P46.10, P46.14, P46.17
STEVERS, Loes, P09.07
Stewart, Charlotte, P37.40, P37.42
Stiep, Tamara, P37.47
Stiles, Elizabeth, P14.16
Stiles, Sydney, LBP07.03
STINSON, FRANK, P45.22
Stocchi, Fabrizio, P37.19, P37.20
Stoessl, A. Jon, PCO7, O19
Stojak, Margaret, P25.38
Stokes, Ashley, P40.10
Stone, Britt, P45.21
Stott, Simon, O48, O80, P37.11, P46.06, P46.09
Strachan, Olivia, P45.42
Strafella, Antonio, LBP32.01, LBP40.03
Strand, Tillan, P13.09
Straniero, Valentina, LBP37.01
Stratton, Jo Anne, PCO11, P06.04
Strazdins, Rachel Lane, P02.01
Strong, Jennifer, P12.04
Strunge, Ethan, P14.07
Sturkenboom, Ingrid, P24.09
Sturkenboom, Ingrid H.W.M., P37.14
Su, Emily, P14.01
Subramanian, Indira, P23.10, P37.32
Sue, Carolyn, P32.07
Suescan, Jessika, P10.08, P34.12, P37.39
Sullivan, Aideen, P27.07, P39.21, P39.21
Sullivan, Jim, P35.23
Sullivan, John O, P10.05, P10.08
Sultana, Ayesha, P13.01, P13.07
Sultana, Razvan, P29.07
Sun, Wesley, P10.03
Sun, Yubing, LBP12.02
Sundaram, Bharathy, P36.04
Sung, Chang Ohk, P12.01
Surmeier, Dalton, P29.07
Surtchev, Yana, P06.12, P06.13
Susic, Adam, P30.03
Sutcliffe, Lou, P37.18
Suttman, Erin, P25.51
Swan, Matthew, LBP37.07
Swanson, Alexandria, P20.05, P32.05
Swanson-Fischer, Christine Swanson-Fischer, P34.02
Sweeney, Kathleen, P24.11
Swift, Hannah, P38.10
Swillens, Julie, P24.09
Swink, Laura, P45.28
Sykes, Jenna, P15.14, P15.15
Téllez, José Gabriel Pinilla, P43.32, P43.33
Téllez, Natalia Pinilla, P43.32, P43.33
Türkeş, Gülsüm Feyza, LBP37.02
Tabar, Viviane, P36.06
Tachiki, Jeremy, P02.08
Tackney, Mia, P37.18
Tada, Mitsunori, P39.28
Taggart, Lara, P14.36
Tagliati, Michele, LBP37.08, LBP39.05
Takahashi, Ryosuke, O111, P06.16
Takata, Julia, P15.11
Takata, Yukiko, P45.18, P45.20
Takeda, Atsushi, LBP37.09
Takeshige-Amano, Haruka, P23.11
Talman, Lauren, P38.09
Tamang, Man Kumar, LBP06.05
Tamarelle, Dorothee, P06.18
Tamir, Tal, P37.37
Tan, Ai Huey, O20, O102, P01.16
Tan, Echo, LBP39.05
Tan, Eng-King, P28.06
Tanco, Sebastian, P03.06
Tang, Joyce, LBP24.01, LBP24.02
Tanner, Caroline, P01.17, P27.08, P37.32, P37.33, P46.20
Tanner, Caroline M., P37.47, LBP17.02, LBP33.01
Tansey, Malú, P01.09, P10.22
Tansey, Malu, P10.16, P10.21
Tantistirapong, Suchada, P39.02
Taoufik, Era, P35.22
Tapies, Martinna Raineri, P20.09
Tarakad, Arjun, P37.25
Tardelli, Erica, P25.13
Tarolli, Christopher, P37.33
Tarudji, Aria, P36.10
Tarylor, Nicholas, P24.06
Tassorelli, Cristina, LBP37.01, LBP40.01
Tat, Lyvin, P29.11
Tate, Adam, P43.08
Tatter, Stephen, P36.04
Tavares, Maria Clotilde Henriques, LBP25.04
Tavera, Graciela María Díaz, P27.03, P27.15
Taveras, Graciela María Díaz, P28.05
Tay, Yi Wen, P01.16
Tay, Yi-Wen, P29.06
Taylor, Kirsten, P37.22, P39.20
Taylor, Sabrina, P39.24
Taymans, Jean-Marc, P08.01, P09.07
Teixeira, Cristina, P43.11, LBP44.01
Teixidó, Laura, P43.30
Teneketzi, Martha, P05.01
Tente, William, LBP37.05
Terrens, Fleur, P21.01, P24.06
Tervonen, Tommi, P13.12
Teunissen, Charlotte E., P34.06
Thai, Kenny, P15.11
Thalamas, Claire, P35.05
Thaler, Avner, P39.16
Tharp, Emily, P35.12, P37.39
Tharp, Marla, P37.02
Theologidis, Vasileios, P06.03, P06.09, P06.10
Theophilopoulos, Alex, P33.01
Therkelsen, Malthe, P10.17
Thezenas, Jeremie, P20.03
Thilakaratne, Ramishka, P25.02
Thomann, Alessandra Elena, LBP37.08
Thomas, Cathi, P39.24, P43.20
Thomas, Cathi Ann, P20.02
Thomas, Kustermann, P39.20
Thomas, Maria, P15.02
Thomas, Rhys Williams, P37.09
Thomas, Tia, P37.39
Thompson, Ellie, P46.06, P46.09
Thompson, Tom, P14.15
Thorman, Emma, P24.12
Thornton, Jennifer, P01.23
Tien, Ong, P01.16
Tieu, Ethan, P10.14
Tieu, Kim, P05.02, P10.04, P10.14, P12.11, P35.06
Tilmont, William, P02.03
Timmerman, Kelly, P01.07
Timmermans, Evelien, P34.06
Ting, Lena, P07.07
Tiwari, Anupama, P12.03
Tjalkens, Ronald, LBP01.01
Tobin, Emily, P40.09
Todd, Olivia, P26.07
Todde, Sergio, LBP37.01
Toga, Arthur, P40.11
Togeretz, Kaley, P15.14, P15.15, P25.52
Toledo, Alejandro G., P12.08
Toledo, Elias Fernandez, P29.12
Tolentino, Kalehua, P15.11
Tolleson, Christopher, LBP14.01
Tolosa, Eduardo, P42.01
Tomlinson, Julianna, P32.03
Tomlinson, Max, P45.11
Tonietto, Matteo, LBP37.08
Tonino, Paula, P12.02
Toomey, Eibhlín, P27.07
Torrandell-Haro, Georgina, P37.48
Torres, Martha Suárez, P25.21
Torres, Murilo, P37.36
Torres, Murilo Lorecetti, P37.35
Torres-Carmona, Edgardo, LBP40.03
Torres-López, María, P06.07
Torres-Russotto, Diego, P37.29
Torrez, Luis, P46.15
Torricelli, Roberta, P01.16
Tosin, Michelle HS, P39.30
Tosserams, Anouk, P20.10
Tournerie, Clotilde, P10.02
Toyooka, Keiko, LBP37.09
Tröster, Alexander, O24, O53
Tragord, Bradley, P25.18
Trebilcock, Emma, P23.12
Trejo, Manuel, P39.18
Trejo-Ayala, Roberto, P26.06, P29.13
Tremblay, Cecilia, P01.12
Trenam, Kate, P46.05
Trenkwalder, Claudia, P42.01, P46.13
Trifirò, Giuseppe, LBP40.01
Trinca, Ana, P27.17
Trinh, Elizabeth, P27.08
Trinh, Joanne, P01.16
Triolo, Fabio, P35.12, P37.39
Tripolitsioti, Theofania, P03.07
Troche, Michelle, O93, P25.29, P25.33
Trotman, Hannah, P17.01
Trudeau, Louis-Eric, P06.04
Trueblood, Peggy, P14.03
Truong, Daniel D., LBP37.09
Truran, Lindsay, P15.02
Tsika, Elpida, P12.07
Tsuji, Keiko, P37.44, P39.05
Tsukada, Hideo, P06.16
Tumas, Vitor, P01.21, P29.12
Turgutyan, David, P36.05
Turner, Travis H, P39.30
Turton, Susan, P13.01, P13.06, P13.07, P46.04
Tyner, Christina, P35.22
Tyo, Mirinda, LBP42.02
Tyrrel, Emily, LBP37.06
Tysnes, Ole-Bjørn, P28.04
Tzoulis, Charalampos, P18.01
Uchida, Yuki, P23.11
Udayar, Vinod, P05.01
Uemura, Norihito, P06.16
Ueno, Shin-ichi, P23.11
Ullén, Susann, LBP37.04
Ulloa-Bravo, Jimmy Santiago, P38.03
Ulven, Callahan, P30.03
Unda, Shila Dama, P45.27
Uno, Yuki, P39.19, P39.28
Unwin, Richard, P35.20
Urushido, Yukiko, P23.11
Uthke, Therese, P45.09
Vaidya, Ariv, P28.01
Vaillancourt, David, P39.01, LBP27.03, LBP40.02
Vajargah, Amir Rajabi, P29.04
Valdovinos, Blanca, P37.33
Valencia-Ustarroz, Miguel, P38.03
Valenete, Enza Maria, LBP40.01
Valente, Enza Maria, LBP37.01
Valles-González, Beatriz, P25.21
VALLET, Anne-Evelyne, P40.06
Valoti, Ermanno, LBP37.01
van Barschot, Pauline G.M., P37.14
van Bennekom, Denise, P35.13
van de Berg, Wilma, P05.03
Van de Berg, Wilma D.J., O56, P05.07, P34.06
van de Berg, Wilma DJ, P01.02, P05.01
Van de Sijpe, Sarah, P10.17
van den Berg, Sanne, LBP23.02
Van Den Berge, Nathalie, P06.03, P06.09, P06.10, P10.17
van der Haas, Johannes, P10.12
van der Heiden, Monique, P26.02
van der Valk, Jurrian, P35.23
van der Wel, Annemiek, P23.04
van Eimeren, Thilo, O73, P28.03
Van Emde Boas, Miriam, P14.30, P27.09, P40.15, LBP40.05
van Geluk, Hans, P26.02
van Horne, Craig, P36.07
Van Hout, August, P40.15
van Ingen, Manon M., P34.06
Van Laar, Teus, P26.02, LBP37.08
Van Mele, Femke, P03.08
van Midden, Vesna, P29.06
van Nijen, Chinouk, LBP39.04
Van Rompuy, Patricia, P18.05
Van Vliet, Trinette, LBP37.04
van Wetering, Janna, P34.06
Vanbellingen, Tim, P15.02
Vancil, Janiece, P03.05
Vandenberghe, Wim, P25.19, P25.54
VanderSleen, Katelyn, LBP01.03
Vanegas, Melissa Naranjo, P20.12
Vaou, Eleni Okeanis, P35.02
Vaou, Okeanis, P25.18, P35.09, P36.04
Varoqui, Camille, P10.11
Vasile, Alexandra, P20.01
Veit, Kelly, P25.29
Velasco-Orozco, Miguel, P28.02
Velasquez, Erika, P12.08
Velastegui, Carla, P47.03
Velez, Jorge Luis Orozco, P29.12
Velez-Pardo, Carlos, P29.12
Velilla, marc, P06.14
VenMeeteren, Emma, P14.23
Vequaud, Philippe, P06.18
Vermorgen, Sanne, P05.03
Vernetti, Patricio Millar, LBP37.09
Versees, Wim, P03.08
Vethe, Rune, O65
Viñuela, Angel, P01.21, P29.12
Vicent, Maria Jesus, P03.06
Vickers, James C, P32.01
Vijiaratnam, Nirosen, P38.05, P39.17
Vila, Miquel, P05.05, P26.05
Villagrasa, Alejandro Cano, P25.21
Villalobos, Ruby, P20.11
Villalobos, Yolianys, P24.04
Villamediana, Pablo Lecumberri, P27.15
Villamil-Cabello, Eduardo, P39.11
Villino-Rodriguez, Rafael, P38.03
Vinke, Saman, P36.02
Vintimilla, Antonio, P14.03
Vishwanath, Abhilasha, P07.04
Visser, Hester, P35.08
Visser-Vandewalle, Veerle, P36.02
Vizcarra, Joaquín, O30, P39.30
Vo, Huong Giang, P04.06
Voelker, Wendy, P14.16
Voloboueva, Ludmila, P34.10
Volpicelli-Daley, Laura, P05.04, P05.06
Volta, Mattia, P11.02, P12.06
Von Handorf, Kristi, P23.08
von Ramm, Stella, P24.03
Voss, Margaret, P37.02
Vozdek, Roman, P04.07
Vulin, Johann, P06.02
Wada, Keiji, P03.03
Wadsworth, Danielle, LBP20.02
Wagner, Jackson, P14.38
Wald, Mike, P39.10
Walden, Sarah, P24.04
Waldo, Emily, P01.21, P29.12
Waldvogel, Daniel, P15.02
Walker, Jenna, P17.03
Walker, Jessica, P01.12
Walker, Richard, P14.34, P27.06, P45.27
Wallace, Sophie, P46.10
Wallings, Rebecca, P01.09, P10.16, P10.22
Wallock, Kristin, P25.34
Walser, Ronald, P14.03
Walsh, Conor, P39.14, P39.15
Walter, Carmen, P35.03, P35.04
Walters, Teel, LBP01.02
Walz, Cordelia, P24.05
Wan-Albert, Ling, P25.48
Wang, Cuiling, P29.11
Wang, Jin, P14.08
Wang, Lucia, P44.01, P45.17
Wang, Pan, P39.10
Wang, Silu, P14.41
Wang, Siting, P37.10, P37.17
Wang, Wei-en, LBP40.02
Wang, Xiaoye Michael, P39.31
Wang, Xiuyuan Hugh, LBP05.01
Wani, Dipti, P22.01, P25.46, P38.12
Waring, Molly, P16.02
Warnecke, Tobias, O71, O100
Washburn, Rachel, P45.28
Waters, Sheena, P29.03, P38.06
Watford, Patricia, P25.20
Wathes, Rowan, P18.04
Watson, Caleb, LBP17.01
Watters, Valerie, P02.02
Watts, Joel, P30.01
Weaver, Jen, P45.28
Weber, Jon, P13.12
Webster, Katherine, LBP42.02
Webster, Katie, P25.17
Webster, Sam, P34.15
Weddle, Jordan, P10.22
Weiner, Howard, LBP37.05
Weinrich, Madison, P14.38, P25.53
Weintraub, Daniel, O84, O94, P37.33
Weintraub, David, P36.04
Weissleder, Christin, P10.11
Welch, Jessica, P38.05
Weller, Joanna, P37.34
Welsh, Timothy N, P27.19
Wendel, Nicholas, P39.24, P43.20
Werner, Milton, LBP34.01
Wessels, Kristy, P36.03
Wetherholt, Hannah, P24.10, P47.03
Whelan, Eimear, P25.20
White, Audrey, P06.12, P06.13
White, Kelly, P37.06
White, Meghan Darling, P25.37
White, Simon, P40.18
Whitehead, Michael, P35.20
Whittingham, Sara, P01.05, P45.14, P46.02
Whyatt, Caroline, P15.02
Wichmann, Rose, P24.05
Widner, Hakan, LBP37.04
Wiedemann, Jonas, P38.02
Wijesinghe, Sasvi, P10.06
Wilberding, Rachel, P14.43
Wile, Daryl, P14.33
Wilhelm, Jennifer, P25.38
Wilkinson, David, P18.02
Wilkinson, Luke, P45.42
Willi, Romina, LBP39.04
Williams, Jenee, P37.12
Williams, Joy, P25.39
Williams, Lindsay, P25.35
Williams, Pete, P02.07
Williams, Rachel, LBP17.01
Williams-Gray, Caroline, O22, P10.02, P10.10, P28.04, P40.18
Williamson, Nicola, P46.10
Wills, Anne-Marie, LBP37.09
Wills, Jordan, P25.11
Wilputte, Isabelle, P37.05, P46.10
Wilson, Mel, P14.19
Wilson, Renee, P37.33
Winter, Sarah, P23.07
Wise, Adina, P31.04
Wong, Annie Li, P43.16
Wong, Harvey, P35.23
Wong, Joshua, P36.03
Wong, Vickie, P02.07
Wong, Vickie HY, P06.06
Wonnacott, Sheila, P37.43, P46.03
Woodhouse, Helen M, P10.05
Woods, Paige, P06.05
Woods, William, P10.02
Woolnough, A.C., P45.15
Worley, Sandie, P25.29
Wragge, Nicole, P14.23
Wu, Annie, P01.19
Wu, Carol, LBP11.01
Wyant, Kara, LBP37.07
Wylie, Karen, P25.02
Wyse, Richard, P29.07, LBP29.02
Xavier, Laura, LBP33.02
Xhukellari, Henri, P06.11
Xian, Zizheng, P10.05, P10.08
Xiao, Yuge, P46.17
XIE, Jing, P40.06
Yagihara, Hiroko, P03.03
Yajid, Malika, P06.18
Yake, Addison, P37.23, P46.18
Yamaguchi, Misa, P23.13
Yamakado, Hodaka, P03.03, P06.16
Yamashita, Tomoko, P38.08
Yan, Connie H, P37.17
Yanes-Castilla, Claudia, P06.07, P10.09
Yang, Mengxi, P31.04
Yang, Mengxi (Cathy), P29.11
Yang, Minhua, P39.10
Yanouri, Omar, LBP01.01
Yao, Elvin, P20.07, P20.08, P21.02, P43.24, P45.44, LBP46.01
Yao, Lingyan, LBP36.01
Yarmahmoudi, Fatemeh, P06.03
Yarnall, Alison, P27.06, P28.04, P37.18, P38.05, P39.17
Yarnall, Alison J, LBP39.01
Yarnall, Alison L, P28.07
Yasumizu, Yoshiaki, P37.24
Yatsugi, Harukaze, P39.19, P39.28
Yee, Melvin, P25.07
Yeshaw, Wondwossen, P12.10
Yiannakou, Yan, P37.40, P37.42
Yinesu, Tsion Terefe, P19.04
York, Michele, P30.06
Yorke, Amy, P14.27, P45.39
Yoshida, Kenji, P38.08
Yoshimoto, Masaru, P23.13
Young, Christa, P14.06
Young, Tyler, P24.02
Ysselstein, Daniel, P35.23
Yu, Eric, P29.04
Yu, Geraldine, P14.40
Yu, Jae, P25.31
Yu, Junying, LBP36.01, LBP36.04
Yu, Shelly, P43.21
Yu, Taewook, P22.01, P38.12
Yucel, Meryem, P40.07, P40.08
Yumoto, Ryo, P39.28
Zabre, Erika, P14.05
Zabre, Erika V., P17.07
Zachayus, Jean-Luc, P06.18
Zadikoff, Cindy, P37.25
Zait, Anat, P37.07
Zajac, Jenna, P39.24
Zamarian, Laura, P42.01
Zanigni, Stefano, P38.02
Zanon, Alessandra, P04.06
Zanon, Ilaria, P11.06
Zanon, Nathalie, P37.21
Zauber, Sarah E., P38.10
Zeighami, Yashar, P01.12
Zeissler, Marie-Louise, P37.03, P37.04, P37.18, P37.40, P37.41, P37.42, P37.43, P46.03
Zelatis, Aleksandra V, LBP17.02, LBP33.01
Zenner-Dolan, Sarah, P37.32
Zesiewicz, Theresa, P36.04
Zhang, Ai, LBP12.03
Zhang, Diana, P32.07
Zhang, Le, P37.24
Zhang, Lina, P43.20
Zhang, Peter, P31.03, P35.10
Zhang, Wei, P13.12
Zhang, Ying, LBP36.01, LBP36.04
Zhao, Cong Zhi, P36.04
Zhao, Da, P02.07
Zhao, Darren, P06.06
Zhao, Yu, P10.19
zhizhong, zhu, P31.01
Zhong, Min, P29.09
Zhong, Min, P29.10, P40.16
Zhou, Amy, P24.11
Zhu, Shuyi, P40.10
zhu, zhizhong, P14.08
Zimmerman, Eric, P25.51
Zimmermann, Ellen, LBP27.03
Zinnhardt, Bastian, LBP37.08
Zirra, Alexandra, P20.04, P29.06, P29.08, P39.09
Ziv, Aviv, P39.16
Ziv, Daniella, P46.23
Ziviani, Elena, P04.06
Zoeller, Sara, P39.14, P39.15, P43.20
Zollar, Jillian, P02.09
Zollinger, Charles, LBP37.07
Zolnierczyk, Pawel, P11.06
Zubcakova, Jana, P45.07
Zuckerman, Daniel, P37.30
Zunke, Friederike, O8, P12.12
Zurawski, Sarah, P14.43
Zurzolo, Chiara, P04.05
Zuzuarregui, Rafael, P37.47
Zvagelsky, Tatiana, LBP09.01