
Abstract
Background
Deutetrabenazine, a vesicular monoamine transporter 2 inhibitor, is one of few treatment options available for Huntington's disease (HD) chorea. There is limited data describing clinical experience with deutetrabenazine doses >48 mg daily.
Objective
Describe treatment outcomes for deutetrabenazine >48 mg daily.
Methods
A dual site retrospective cohort study of patients on deutetrabenazine titrated to doses >48 mg/day for HD chorea from April 2017 through December 2021 was conducted. Patients using concomitant strong CYP2D6 inhibitors at time of deutetrabenazine initiation, those who became deceased or lost to follow-up within six months of dose increase above 48 mg/day, or previously enrolled in a study on >48 mg daily and moving to commercial product were excluded. Outcomes were reported descriptively including therapeutic response, adverse effects (AEs), adherence (measured by proportion of days covered [PDC]), and discontinuation.
Results
Thirty patients were included: 47% female, 93% White, median age 56 years. Most patients required dose escalations for inadequate response. The rate of AEs reported before and after transitioning to doses >48 mg/day was the same. Psychiatric changes were less commonly reported at doses >48 mg/day, but extrapyramidal symptoms were more common. The median total maximum chorea score in the Unified HD Rating Scale was 13 (IQR 9–19) and 13 (IQR 7–18) at baseline and follow-up, respectively. Median PDC was 0.99 (IQR 0.94–1.00); two patients discontinued therapy due to AEs.
Conclusions
Deutetrabenazine >48 mg daily appears safe and well tolerated in patients with uncontrolled HD chorea, though no significant change in total maximal chorea score was found.
Introduction
Huntington's disease (HD) is a hereditary neurogenerative disorder characterized by deterioration in motor function, cognitive function, and behavioral skills. The most common manifestation of motor dysfunction is chorea, which is defined as abnormal, involuntary movements that can increase the risk of injury and interfere with activities of daily living. 1 Currently, there is no cure for HD, and it is estimated 7.43 individuals per 100,000 living in North America are symptomatic. 2
Deutetrabenazine is a vesicular monoamine transporter 2 inhibitor (VMAT2i) that was approved by the U.S. Food and Drug Administration (FDA) in April 2017 for the treatment of chorea associated with HD. The maximum FDA approved dose of deutetrabenazine is 48 mg/day given in two divided doses. 3 Treatment for HD chorea should be initiated if it is troublesome or bothersome to the patient, with options including VMAT2is (in the absence of depression) and dopamine (D) receptor antagonists (D2/D3).4,5 Monotherapy for the treatment of chorea is preferred to reduce the risk of adverse effects (AEs) and complications of other non-motor systems; however, combination therapy with a pre- and post-synaptic antidopaminergic medication may be indicated for patients with multiple conditions or refractory symptoms. 5 Frank et al. conducted a single arm open label clinical trial in 119 patients with HD chorea to evaluate the long-term safety and efficacy of deutetrabenazine post-FDA approval. 6 The Alternatives for Reducing Chorea in Huntington Disease (ARC-HD) investigators concluded the use of deutetrabenazine dosed twice daily allowed for better maintenance of chorea with total daily doses ranging from 6 mg to 72 mg and an average end-of-study dose of 45.7 mg/day. 6
There is a scarcity of data to support the safety and efficacy of dosing deutetrabenazine higher than current FDA recommendations, with one post-hoc analysis of 49 patients from the ARC-HD trial offering data on doses >48 mg/day. 6 The post-hoc analysis concluded that doses >48 mg/day were required in some patients to obtain control of their HD chorea; however, the analysis was limited to tolerability of higher doses and did not address efficacy. 7 Therefore, the purpose of this study was to describe safety outcomes and therapeutic response in patients receiving deutetrabenazine doses >48 mg/day.
Methods
Study design and setting
This was a multi-site, retrospective study of adult patients on deutetrabenazine who were titrated to doses >48 mg/day for HD chorea from April 2017 through December 2021 at Vanderbilt University Medical Center (VUMC) and University of Alabama at Birmingham (UAB). Patients were excluded if there was concomitant use of strong CYP2D6 inhibitors at time of deutetrabenazine initiation, were deceased or lost to follow-up within six months of dose increase exceeding 48 mg/day, or if they were previously enrolled in a clinical trial on >48 mg daily andmoving to commercial product. Both study sites are Huntington's Disease Society of America Center of Excellence (HDSA COE) clinics with an integrated health-system specialty pharmacy (IHSSP). HDSA COE clinics provide a multidisciplinary team to address all aspects of care for patients with HD. Members of the team may include neurologists, psychiatrists, social workers, pharmacists, and other healthcare professionals. IHSSP pharmacists provide comprehensive medication access, monitoring, and support services. When patients are prescribed deutetrabenazine, the specialty pharmacy team (including a pharmacist and certified pharmacy technician) ensures deutetrabenazine can be utilized safely based on potential drug interactions and laboratory results such as liver function testing and corrected QT intervals. Additionally, they complete the insurance authorization process, including appeals for dose escalations beyond FDA approved doses, and obtain financial assistance for patients as needed. Once the medication is approved and treatment is affordable, pharmacists counsel the patient extensively and communicate a monitoring plan (e.g., when patients will follow-up in clinic). After treatment is initiated, the specialty pharmacist follows up with the patient to assess efficacy, tolerability, and adherence to deutetrabenazine. This initial phone call is coordinated with the specialty pharmacy technician to schedule shipment of refill. The specialty pharmacy technician continues to follow up with patients to assess adherence monthly prior to refills thereafter. Patient concerns or issues are escalated to the specialty pharmacist who contacts the patient and/or prescriber as warranted. The study was conducted in accordance with the Declaration of Helsinki and was approved by the VUMC and UAB Institutional Review Boards on May 4, 2022and May 15, 2023, respectively, with the need for written informed consent waived.
Study objectives
The primary objective of this study was to assess safety outcomes and therapeutic response to high-dose deutetrabenazine. Safety outcomes included the number and type of patient-reported AEs and discontinuation rates and reasons. Safety outcomes were collected from the time of deutetrabenazine initiation or transition from clinical trial drug to specialty pharmacy fulfillment through discontinuation or the end of the study period (June 30, 2022). The date of AE occurrence and discontinuations were collected and categorized by occurring before or after reaching a total daily dose >48 mg.
Therapeutic response was evaluated by the changes in abnormal movement control as determined by the Unified Huntington's Disease Rating Scale (UHDRS) Total Maximal Chorea (TMC) score from dose escalation (termed “baseline” and defined as the closest score to the decision to initiate deutetrabenazine treatment) to the end of the study period (termed “follow-up” and defined as the last score in the study period). Given the potential for initial improvement after a dose escalation, UHDRS TMC scores before and within six months of a dose escalation were also evaluated for those with available scores. The UHDRS is the most used measure of function in HD and provides an overall measure of disease burden, made up from the subcategories of motor, cognitive and behavioral assessment, and functional capacity. At both sites, the UHDRS motor subsection is typically collected at every clinic visit, which occurs every three to six months for patients on deutetrabenazine. As antipsychotics are an alternative treatment recommendation for chorea and may impact UHDRS TMS score due to their antidopaminergic and postsynaptic effects, change in scores were evaluated between patients who were on antipsychotic treatment (i.e., haloperidol, risperidone, aripiprazole, quetiapine, olanzapine) and those who were not. Extrapyramidal symptoms (EPS) (akathisia, parkinsonism, or worsening movements) as an AE could be due to elevated dosages, therefore, bradykinesia sub-scores were evaluated. 8
Secondary objectives included number and type of concomitant medications used to treat HD chorea, change in the UHDRS Total Motor Score (TMS) from baseline to follow-up, adherence to deutetrabenazine calculated using proportion of days covered (PDC) for patients with medication fulfillment through the IHSSP, and dose changes. The total daily dose at the beginning and end of each clinic visit was collected. Dose changes (both increases and decreases) were evaluated as occurring before or after the patient had reached a total daily dose of >48 mg.
Data sources
Data for patient characteristics and the outcomes were collected from the electronic health record (EHR) and specialty pharmacy patient management database at each site. De-identified data were imported into a shared secured data warehouse (Research Electronic Data Capture [REDCap]) hosted at Vanderbilt University Health System.9,10
Analysis
Descriptive statistics were used to describe patient characteristics. Percentages were calculated for categorical variables; mean, median, and interquartile range (IQR) were used for continuous variables. Fisher's exact test was used to test for differences in reported AEs based on concomitant medication use. Patients had to have at least three fills to be included in the PDC calculation. Adherence was calculated using the first fill in the study period to the last fill in the study period.
Results
Baseline characteristics
Between the two sites, 30 patients (n = 17 Site 1 and n = 13 Site 2) were included in the analysis. At time of deutetrabenazine initiation, patients were a median age of 56 (IQR 47–64) years, mostly White (93%), and approximately half male (53%). Patients commonly had Medicare as their insurance type (53%). Table 1 details baseline characteristics.
Baseline characteristics.
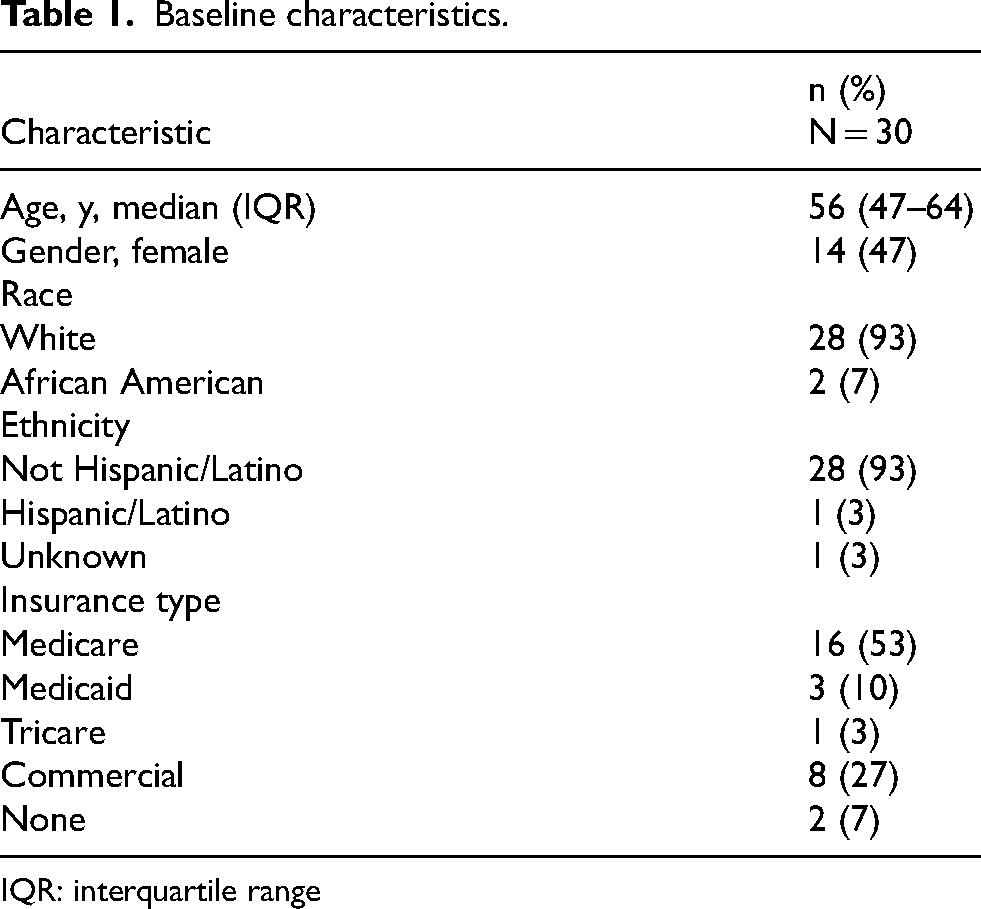
IQR: interquartile range
Reports of adverse events
Sixteen patients (53%) reported an AE at least one time on doses of 48 mg/day or less and 19 patients (63%) reported an AE at least one time on doses >48 mg/day. In total, 42 AEs were reported with 50% occurring at doses of 48 mg/day or less and 50% occurring at doses >48 mg/day. The most common AE reported, sleep changes, was similar before and after transitioning to a dose >48 mg, reported eight times in five (17%) patients before and eight times in seven patients (23%) after changing. Psychiatric changes were less commonly reported after transitioning to a dose >48 mg, reported six times in four (13%) patients before and two times in two (7%) patients after. EPS (akathisia, parkinsonism, or worsening movements) was more commonly reported after transition, reported four times in four (13%) patients before and eight times in seven patients (23%) after transition above 48 mg. Bradykinesia sub-score did not change significantly between groups (results not shown). Gastrointestinal, genitourinary, and other AEs were reported at the same rate before and after transition above 48 mg. AEs resulted in discontinuation in two patients, one at 48 mg/day dosing and one at 72 mg/day dosing. Figure 1 details AEs by deutetrabenazine dose.
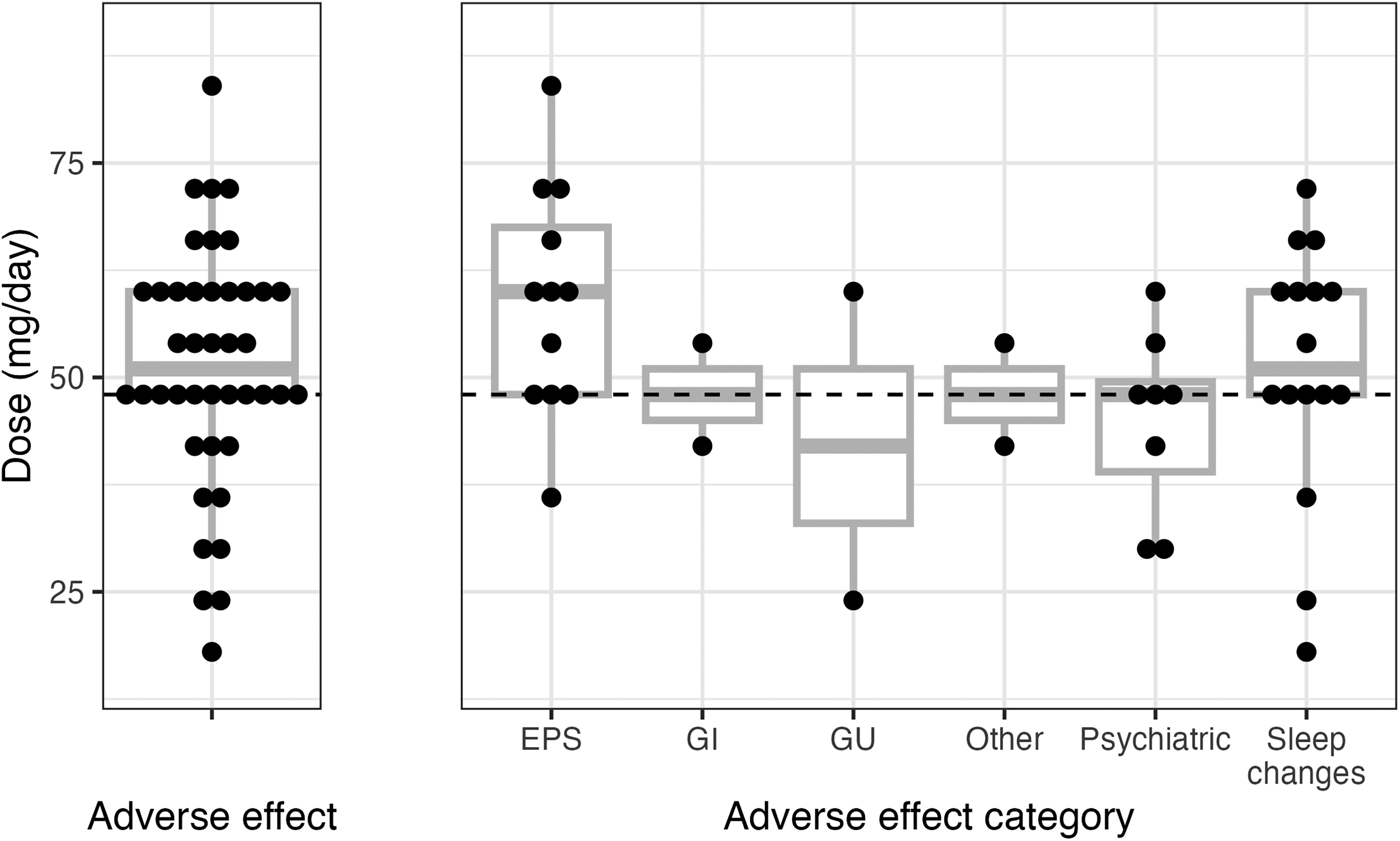
Total adverse effects reported by deutetrabenazine dose. The total number of AEs reported was the same for patients before and after transitioning to doses >48 mg/day. Psychiatric changes were reportedly more common at doses at or below 48 mg/day and EPS symptoms were more commonly reported after transitioning above 48 mg/day. Sleep changes, the most commonly occurring AE, were reported at the same frequency before and after transitioning above 48 mg/day. EPS: extrapyramidal symptoms, GI: gastrointestinal, GU: genitourinary. Other: dizziness, palpitations.
Deutetrabenazine discontinuation
Seven patients (23%) discontinued therapy during the study period with reasons including AEs (n = 2; akathisia and palpitations), death due to unknown cause (n = 2), lack of efficacy (n = 1), financial difficulties (n = 1), and administration issues (n = 1). Patients who discontinued treatment were younger with a median age of 46 (IQR 44–69) vs. 57 (IQR 52–64) years. Discontinuations occurred at doses >48 mg/day for six (86%) patients with a median time to discontinuation of 44 months (IQR 27–53). The mean dose of deutetrabenazine was 60 (IQR 57–72) mg/day at time of discontinuation. Three patients who discontinued restarted deutetrabenazine during the study period; two restarted at a dose >48 mg.
Change in UHDRS TMC score
Among 23 patients with a baseline and follow-up score available, the median UHDRS TMC score was 13 (IQR 9–19) and 13 (IQR 7 18) at baseline and the end of the follow-up period, respectively. The median time from baseline to final measurement was 38 months (IQR 26–52; range 7–81). When evaluating patients on deutetrabenazine vs. deutetrabenazine plus an antipsychotic, patients on deutetrabenazine alone had a greater change in UHDRS TMC score [13.5 (IQR 7–19) at baseline and 13.5 (IQR 8.5–21) at follow-up versus 13 (IQR 11.5–16.5) at baseline and 10 (7–12) at follow-up, respectively]. Neither change in UHDRS TMC score was statistically significant. Figure 2 details abbreviated UHDRS findings for each of these patients. In the 14 patients with UHDRS TMC scores before and within six months of escalating to a dose >48 mg, median scores were 13 (IQR 7–20) before escalation and 14 (10–17) after escalation..
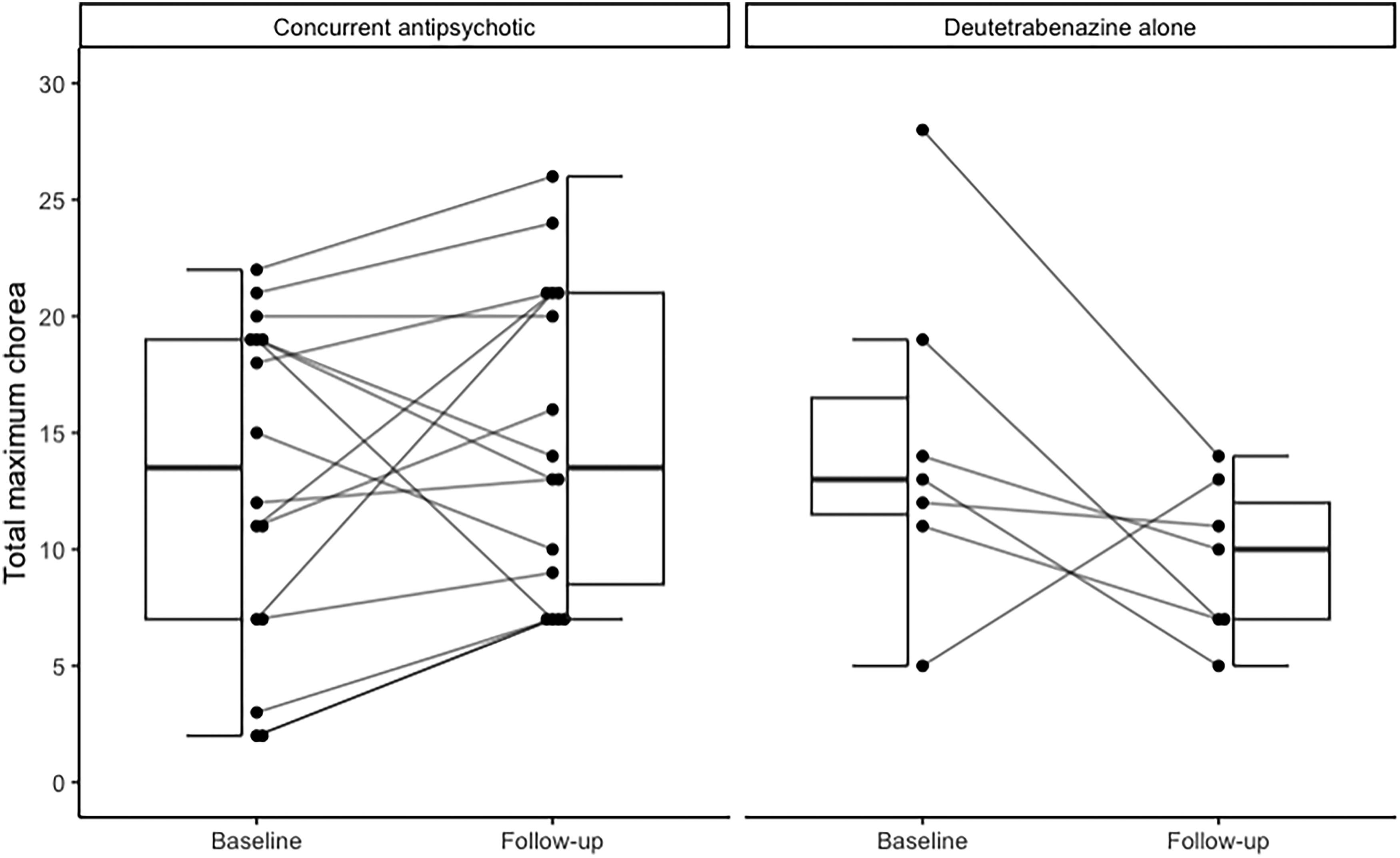
Abbreviated Unified Huntington's Disease Rating Scale (UHDRS) Total Maximal Chorea (TMC) change from baseline to follow-up. In the 23 patients with a baseline and follow-up score available, the median TMC score in the UHDRS was 13 (IQR 9–19) and 13 (IQR 7–18) at baseline and end of the follow-up period respectively.
Concomitant medication use
Most patients (n = 23, 77%) were prescribed concomitant medications for the treatment of chorea, most commonly clonazepam (n = 14, 47%), aripiprazole (n = 10, 33%), or olanzapine (n = 7, 23%). Figure 3 details concomitant medication use on the patient level. When looking at AE reports and concomitant medication use, there were no significant differences in EPS, psychiatric symptoms, or sleep changes for patients who were or were not on concomitant medications used to treat HD chorea. However, of the six patients who reported a psychiatric AE, all were on antipsychotics, compared to 13/24 (54%) who did not report a psychiatric AE (p = 0.061).

Concurrent medication use via patient-level intersection (n = 30). Most patients (n = 23, 77%) were prescribed concomitant medications for the treatment of chorea most commonly clonazepam (n = 14, 47%) aripiprazole (n = 10, 33%) or olanzapine (n = 7, 23%).
Change in UHDRS TMS
Among 19 patients with baseline and follow-up UHDRS TMS scores available, the median UHDRS TMS significantly increased from 50 (IQR 36–59) at baseline to 59 (IQR 45–64) at the end of the follow-up period (p = 0.015).
Adherence (IHSSP patients only)
Adherence
Of the 30 patients included, 25 (83%) had at least three prescription fills with the IHSSP to calculate PDC. The median PDC was 0.99 (IQR 0.94–1.00) with a median follow-up time of 25 (IQR 14–46) months. Of note, median PDC varied slightly at 0.97 (IQR 0.71–1.00) and 1.00 (IQR 0.99–1.00) for Site 1 and Site 2, respectively. A manual review of Site 1 participants with a PDC < 80% revealed that the five patients were required to utilize alternate pharmacies or the patient assistance program to continue treatment during the follow-up period, falsely lowering the median PDC at Site 1.
Dose changes
Dose adjustments occurred 104 times with 93 dose increases and 11 dose decreases. Patients were on deutetrabenazine for a median of 16 (IQR 3–27) months prior to reaching doses >48 mg/day. Overall, lack of efficacy was the most common reason for dose increases (99%). After reaching doses >48 mg/day, 24 (80%) patients continued to have dose increases. After reaching doses >48 mg/day, six patients transitioned back to an FDA-approved dose due to AE (n = 2), lack of efficacy (n = 1), financial difficulties (n = 1), non-adherence requiring retitration (n = 1), and unknown (n = 1). Overall, the most common reason for dose decrease was AEs (n = 6). The median dose of deutetrabenazine was 64.5 mg/day (IQR 57.8–72.0) with one patient reaching a maximum dose of 96 mg/day at time of study close for patients who remained on therapy. Figure 4 details dose change journeys for each patient with a change in the study period beginning with decision to increase deutetrabenazine above 48 mg/day.
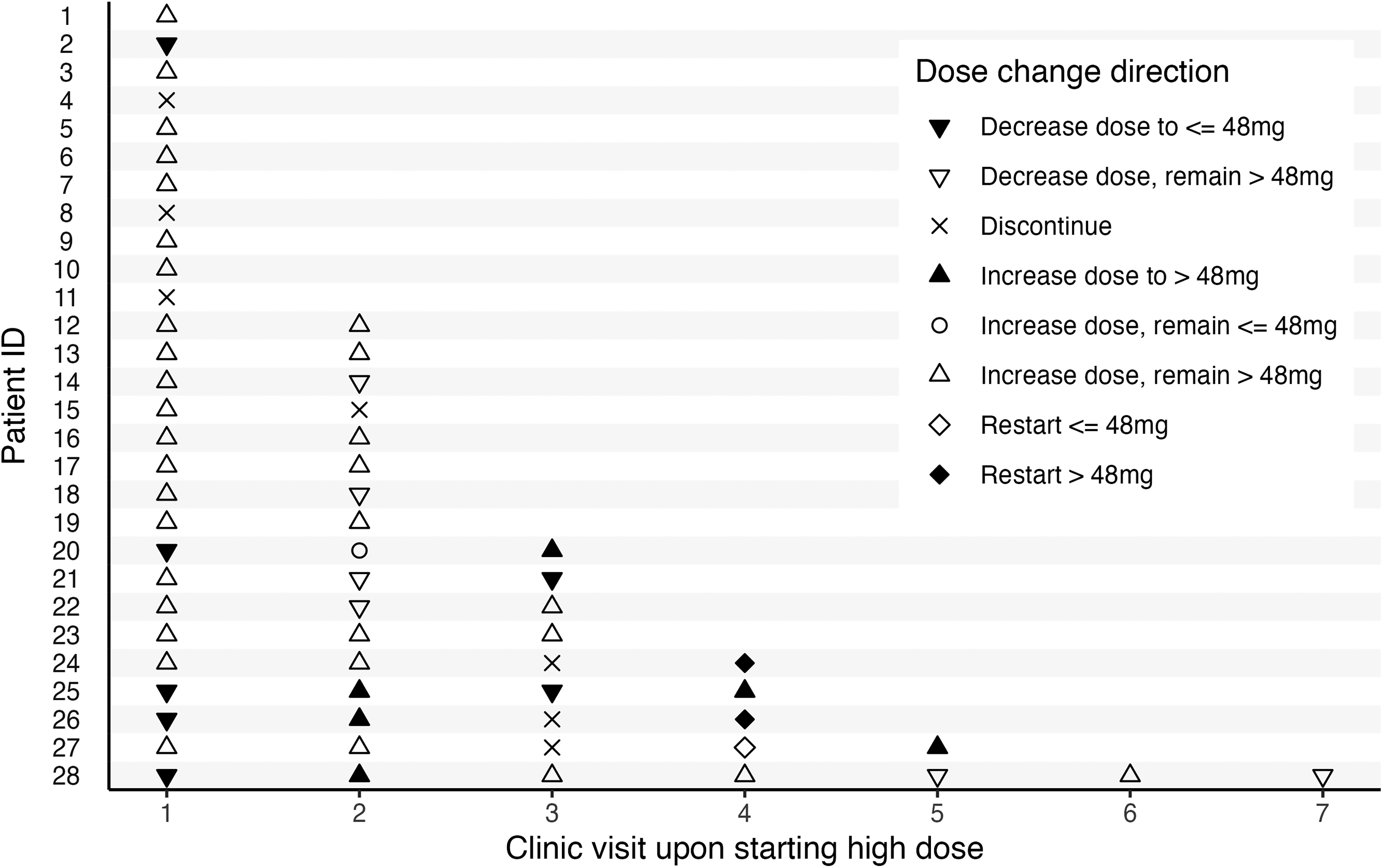
Dose change journey after reaching deutetrabenazine doses >48 mg/day. Dose change journeys for each patient beginning with decision to increase deutetrabenazine >48 mg/day are presented. The number of clinic visits after reaching the >48 mg/day dose at which each subsequent dose change occurred is on the x-axis and individual patients are on the y-axis such- each row represents one patient's journey. There were 43 total dose changes occurring in 23 patients upon reaching a dose >48 mg/day. Down arrows represent dose decreases. If the decrease resulted in the final dose remaining >48 mg the down arrow is empty; if filled, the dose decreased back to 48 mg or less. An X indicates a discontinuation. If a dose increase resulted in the final dose reaching >48 mg, the up arrow is full; if the increase resulted in the final dose remaining >48 mg, the up arrow is empty. A circle indicates a dose increase that resulted in the dose remaining <=48 mg. Diamonds indicate deutetrabenazine restarts after a discontinuation if the restart was at a dose <=48 mg, the diamond is empty; if the restart was at a dose >48 mg the diamond is full. Two of the 30 patients had no additional data after increasing to a dose >48 mg and are not represented in this figure.
Discussion
To the authors’ knowledge, this is the first real-world study to evaluate both safety and adherence outcomes utilizing an IHSSP fulfillment model in patients with HD chorea receiving deutetrabenazine dosed >48 mg/day and the first to evaluate response to therapy in the real-world setting at higher deutetrabenazine doses. Though TMC scores remained mostly stable, AEs were similar before and after transitioning to doses >48 mg/day with only two patients requiring dose reduction to 48 mg/day or lower due to an AE.
AE findings
The most common AEs reported were similar before and after transitioning to doses >48 mg/day, with sleep changes, psychiatric changes, and parkinsonism being the most common. This is in accordance with AEs described in the deutetrabenazine package insert for FDA approved dosing regimens. 3 AEs resulted in two patients reducing their dose back to 48 mg/day or lower. Two patients discontinued deutetrabenazine due to akathisia and palpitations. In the ARC-HD study, common AEs included fall, depression, anxiety, insomnia, somnolence, and akathisia while low rates of depression, suicidality, and parkinsonism. 6 A recent analysis of FDA AE reporting data found all VMAT2i had a significantly higher likelihood of parkinsonism compared to the reference product (acetaminophen). 11 Of note, suicidality was not reported by any patient included in this study. Despite the AEs reported in this study, including parkinsonism, the majority of patients continued deutetrabenazine with dose escalations as tolerated.
UHDRS TMC findings
HD is a progressive disease; thus, motor symptoms and corresponding TMC scores would be expected to worsen over time without treatment. In the current study which evaluated patients up to a median time of 38 months, TMC scores did not differ significantly from time of deutetrabenazine initiation to the last follow up in the study period, though some patients did experience improvement (Figure 2). Additionally, no initial improvement in UHDRS TMC scores was seen within the first six months after dose escalation. Results may vary based on the duration of follow-up and it is anticipated that scores would worsen over longer time periods given the progressive nature of the disease. Surprisingly, in the current study, patients on deutetrabenazine alone had a numerically greater change in UHDRS TMC score when compared to those who were on concurrent antipsychotic treatment, though this was not statistically significant. Though no conclusions may be made about effectiveness of deutetrabenazine in the treatment of HD chorea, it is notable that TMC scores did not worsen over time for patients included in the study [median UHDRS TMC score 13 (IQR 9–19) vs. 13 (IQR 7–18) at baseline and the end of the follow-up period, respectively]; therefore, it would seem that deutetrabenazine allows for maintenance of chorea control over a median of 38 months (IQR 26–52; range 7–81). Additionally, lack of efficacy was the most common reason for dose increase (99%). In the First-HD study comparing deutetrabenazine vs. placebo, mean TMC scores improved from 12.1 (standard deviation [SD] 2.7) to 7.7 (SD 3.9) in the treatment group over an eight-week titration and four-week maintenance period. 12 Frank, et al. analyzed TMC scores as part of a long-term open-label extension study for patients rolling over from a deutetrabenazine double-blind study or converting from a stable dose of tetrabenazine. 6 Participants had a decrease in TMC scores from baseline to week 8; however, minimal change was seen after that until the end of treatment or week 145, which is in alignment with results from our study. 6 While Frank, et al. noted the study design was to intentionally mimic clinical practice, it is not feasible to bring patients into clinic on a weekly basis in a real-world setting; therefore, TMC scores from baseline to week 8 are not available for analysis in our study. 6
UHDRS TMS findings
As noted, HD is a progressive disease with higher scores on the TMS notating worsening movement control. Deutetrabenazine does not treat all movement symptoms associated with HD, therefore it is not unexpected that this area of the UHDRS worsened as time passed. In the First-HD study comparing deutetrabenazine vs. placebo, mean TMS improved by a mean between-group difference of −4.0 points favoring deutetrabenazine (95% CI −6.5 to −1.5, p = 0.002). The authors noted that the majority of this improvement was due to chorea; however, total maximal dystonia scores also improved. 12 Frank, et al. also included TMS as part of their outcomes of interest. Overall, there was a mean increase of 8.2 points (95% CI 4.8–11.5) from week 8 to week 145 of treatment, which is comparable to the findings in the current study. 6
Dose changes
The time to deutetrabenazine dose escalation correlates with the clinical progression of movement symptoms with HD patients. Patients were on deutetrabenazine for a median of 16 months prior to reaching doses >48 mg/day, and the median dose was 64.5 mg/day (IQR 57.8–72.0) at time of study close for patients who remained on therapy. Even after reaching doses >48 mg/day, most patients continued to need further increases due to suboptimal response and/or disease progression. Similarly, in the ARC-HD open-label extension study, at least one-half of patients had an increase in mean daily dose after dose adjustment at week 8 to the final assessment and one-third of patients had a mean daily dose of >50 mg at final assessment. In the current study, few patients had a dose reduction to an FDA-approved dose and less than half of these were associated with an AE, which was lower than what was observed in ARC-HD. The highest dose seen in the current study was 96 mg/day, which is significantly higher than the maximum allowed dose of 72 mg/day in ARC-HD. 6
Adherence and discontinuation
The median PDC of 99% for patients utilizing an IHSSP for deutetrabenazine fulfillment is well above the commonly accepted threshold of 80% for patients with chronic disease states. 13 In fact, other studies assessing deutetrabenazine adherence have shown average PDC rates of 78.5 and 76.7%.14,15 Of the five patients in our study with PDC < 80%, all were using external pharmacies due to payer mandates or manufacturer patient assistance programs which resulted in gaps in claim information, falsely lowering PDC. The higher adherence rate seen in our study may be due to patients utilizing an IHSSP, which is generally associated with increased medication access and adherence.16,17,18 The most common reasons for discontinuation of deutetrabenazine included AEs (discussed above), death due to unknown cause, and lack of efficacy. The low rates of discontinuation related to AEs were similar to that observed in the First-HD pivotal study. 12 While the proportion of patients who discontinued deutetrabenazine were similar to another real-world, retrospective claims database study, the time until discontinuation occurred was significantly longer in the current study. 15
Limitations
There are a few limitations in the present study. Though provider notes and patient encounters were thoroughly reviewed, a lack of complete documentation in the EHR may have affected results. Both study sites employ providers who were involved in the initial clinical trials for deutetrabenazine; therefore, providers may have been more comfortable escalating doses above the FDA-approved maximum dose. Real-world claims data may not be reflective of those patients utilizing non-IHSSP, such as external pharmacies or manufacturer patient assistance programs. A major limitation includes the retrospective nature of the study with small sample size which did not allow for collection of other outcomes measures that may be used to evaluate patients with HD (e.g., total functional capacity, cognition and other motor functioning assessments) and adjusting for potential confounding factors including the progression of HD, when comparing the effectiveness of deutetrabenazine in treating HD chorea at doses >48 mg/day. However, this data is among the first to be reported from a real-world setting using clinical measures from practice and is therefore useful for clinicians managing patients with HD. Larger prospective trials are needed to determine if deutetrabenazine doses >48 mg/day are effective in reducing or maintaining chorea. However, if patients are experiencing uncontrolled chorea, increases above 48 mg/day appear to be safe and tolerable when managed appropriately.
Conclusion
The use of deutetrabenazine doses >48 mg/day appears to be safe and tolerable in patients with uncontrolled HD chorea, though minimal change in TMC score was found over a median of 38 months. Even after treatment with doses above FDA approved ranges, continued increases were prescribed in most patients due to suboptimal response and/or disease progression. Although more AEs were reported with high-dose deutetrabenazine, patients were largely adherent, and few discontinuations were attributed to AEs in both the FDA-approved dose group and high-dose deutetrabenazine group.
Footnotes
Acknowledgments
Audrey Cobb, PharmD Candidate, McWhorter School of Pharmacy, Samford University; Alyssa Lim, PharmD, MBA, University of Alabama Birmingham, Department of Pharmacy.
The project described was supported by Clinical and Translational Awards Program awards No. UL1 TR002243 and UL1 TR000445 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Ethical considerations
This study was approved by Vanderbilt University's Institutional Review Board.
Consent to participate
This study was approved as an exempt study, posing minimal risk to participants. A waiver of consent was approved.
Consent for publication
Not applicable
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SL and BD report participation in Teva Pharmaceutical Industry©'s 2023 Advisory Board Meeting on AUSTEDO® and AUSTEDO® XR
Data availability
Deidentified aggregated data used for analyses may be made available upon request.