
Abstract
Background
People with Huntington's disease (HD) experience physical, cognitive, and psychiatric manifestations that can result in housing in settings that are inappropriate for care requirements.
Objective
The aim of this scoping review was to examine the existing literature on effective housing and support models for people with HD.
Method
Five major databases (MEDLINE, CINAHL, SCOPUS, PsycINFO, and EMBASE) were systematically searched for studies that reported qualitative and/or quantitative findings on housing and support models for people with HD. Key findings from eight eligible studies were integrated to provide preliminary information about housing and support for this population.
Results
No studies included in the review specifically provided data on the effectiveness of housing and support models for people with HD. However, important insights regarding the challenges facing this population in accessing appropriate housing and supports were revealed. Findings highlighted the importance of good quality disability and health supports from adequately trained staff. People with behavioral manifestations, poor physical status and psychosocial concerns were more likely to be living in residential aged care than in their own home. The role of positive behavior support and supporting caregivers were highlighted as important considerations.
Conclusions
There is limited research on effective housing and support models for people with HD. Due to the wide variety in sociocultural variables and disease manifestations, it is unlikely that a single best-practice model exists. Housing and supports should be flexible and adapted to individual needs.
Introduction
Huntington's disease (HD) is a genetic progressive neurological disease. Although the disease is rare (up to 7.5 per 100,000 in European, American and Australian populations, 1 the disease burden is high, and life expectancy is compromised. HD affects global cognitive functioning and includes cognitive, physical and psychiatric manifestations that worsen progressively. 2 The usual disease onset is between 30 and 50 years of age, but the age range varies from very young to late age. The prognosis from the age of diagnosis to death is typically 17–20 years which reflects a relatively long duration of progressive disability.3,4 Currently, there is no cure or effective treatment to alter the course of HD. 5 Due to the complex clinical manifestations, people with HD require support from a specialized multidisciplinary team, including neurologists, psychiatrists, occupational therapists, psychologists, social workers and speech therapists. 6 Despite all people with HD developing complex care needs, clinical manifestations experienced by individuals can vary significantly and have an unpredictable trajectory.7–9 As a result, implementing appropriate supports and housing that meets the person's needs and preferences while also matching these to the progression of the disease can prove challenging.
People with HD experience a range of clinical manifestations, including involuntary movements known predominantly as chorea, cognitive impairments, psychiatric and behavioral manifestations, and speech and swallowing difficulties. 2 As the disease progresses, people typically experience dementia characterized by progressive disorientation and confusion, personality changes, severe cognitive deficits, restlessness, aggression and agitation. 10 Psychiatric manifestations combined with the genetic nature of HD can thus place a significant strain on family relationships, causing breakdowns, stress and caregiver burden.11,12 Further, in comparison with other neurological diseases, people with HD experience increased levels of spiritual and existential distress and a high suicide risk.3,13 As a result, informal carers of people with HD are typically required to provide psychological and practical support while concurrently being flexible and adequately planning for changing or future circumstances. 14 A recent study found that many families of people with HD provide extensive daily care, with responsibilities increasing as the condition progresses. Caregiver burden emerged early and intensified over time as cognitive, behavioral, and functional impairments increased. 15 Informal caregiving arrangements can be further complicated when there is experience with other affected family members. Additionally, some caregivers may themselves carry the HD gene expansion, either knowingly or unknowingly, adding to the emotional complexity and future planning challenges. 16
A study by Ekkel et al. 17 described the disease characteristics and functional impairments for a cohort of people with HD in a Dutch residential aged care (RAC) facility. The study highlighted the heterogeneity in the physical, cognitive, emotional, and social functioning of 173 residents. Participants had an average age of 58.3 years, and impairments varied widely, with 46–49% exhibiting mild impairments in activities of daily living and cognition, while 22–23% had severe impairments. Notably, 80.3% of residents were prescribed psychotropic medications, and 74% displayed neuropsychiatric impairments. The findings highlight the complexity of support required for this population and suggest that the multidisciplinary teams of people supporting people with HD must be equipped with expertise across diverse domains to address the varied needs of this population.
Current recommended support models for people with HD include a combination of specialist nursing care, disability housing, multidisciplinary community-based services, paid and informal caregivers, and palliative care. 18 Due to the specialized nature of the services required, combined with the limited number of specialist service providers, accessing required care can be difficult for people with HD. Unsurprisingly, the uncertainty of access to necessary housing and supports can exacerbate stress and pressure experienced by people with HD and their informal support systems.18,19
Internationally, people with disability and complex needs who require supports live in a range of housing options, outside of RAC: at home supported by family, in group homes (i.e., shared living arrangements with two or more people with disability), with parents at home (beyond the age that people would usually live with parents), and in the community (either in government funded or private housing) with paid and/or unpaid support. 20 Compared to people with conditions causing fixed deficits such as stroke, 21 people with HD face a protracted disease course with complex and changing needs. Institutionalized settings typically become the only housing option that can meet their support needs as access to 24-h care becomes necessary.2–4,22 Consequently, many people with HD face admissions to RAC early to midway through their disease process due to a lack of alternative specialized housing and support options that consider their preferences.23–25
For younger people with HD, RAC may not be the preferred option. RAC is designed primarily for older adults and lacks the specialized support and social engagement opportunities that younger people require. 26 Young people living in RAC continuously report a lack of community participation and social interaction, limited choice in everyday activities, and poor mental health outcomes.26,27 Opportunities to engage in meaningful activities are often limited, and basic human needs such as privacy, physical, nutritional, sexual and emotional needs can be overlooked.26–29 It is noteworthy that there is a dearth of research into the experiences of younger people with progressive neurological disorders living in aged care, with research primarily focusing on those with conditions causing fixed-deficits, or presenting aggregate findings comprising people with progressive and non-progressive disorders.26–29
The funding and regulatory frameworks governing housing and support for people with disability vary significantly across countries, making direct comparisons and a unified best practice approach challenging. For example, models of aged care in the US and UK differ in funding sources, admission criteria, and oversight, with some systems operating under social care models and others under medical care frameworks. These differences shape access and appropriateness of housing and support services, highlighting the importance of jurisdiction-specific solutions.
In Australia, the National Disability Insurance Scheme (NDIS), a non-means tested federal scheme, provides reasonable and necessary funding for housing and supports (e.g., Allied Health and disability support workers) for people under 65 with a permanent disability.30,31
Regarding support to live in the community, the NDIS funds Supported Independent Living (SIL) and Specialist Disability Accommodation (SDA). SIL is most commonly used in shared living arrangements, funding paid support to help participants with activities of daily living. 32 SDA funding, provided to a very small proportion of NDIS participants, subsidizes the cost of renting dwellings registered with the National Disability Insurance Agency (NDIA) that meet certain accessibility criteria. People aged over 65 years who require housing and support can access this through the aged care system, which includes the Commonwealth Home Support Programme and residential aged care services funded under the Aged Care Act 1997. 33 Unlike the NDIS, aged care services are means-tested, and funding levels may vary depending on an individual's income and assets. 34 Although there are initiatives to increase the support and housing available to people with HD, only three states (NSW, Victoria and WA) have specific residential facilities for people with HD, with very limited places available for people with HD. 35
Despite the availability of novel housing and support options through the NDIS, there is limited evidence on what constitutes effective models of care for people with HD. 36 Given the complex, unique and changing support needs of people with HD, a scoping review was employed to explore effective housing and support models for people with HD.
Methods
A scoping review method was selected to map and further understand the state of the current literature around housing and support models for people with HD. 37 Scoping reviews allow for a wide exploration of literature across a range of study designs and questions beyond intervention effectiveness, can facilitate the identification of gaps in research and practice, and can contribute to the development of primary research studies. 38 This scoping review followed the stages outlined by Arksey and O’Malley 37 : (1) Identifying the research question; (2) Identifying relevant studies; (3) Study selection; (4) Charting the data; (5) Collating, summarizing and reporting the results; and (6) Consultations. The reporting of the methods and results was guided by the PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. 39 The review was guided by the research question; “What are the effective housing and support models for people with Huntington's Disease?”.
Search strategy
A search strategy was devised by the authors in consultation with a research librarian. Four concepts were selected to represent four major concepts relevant to the research question: HD, housing and accommodation, models of care and outcomes.
The search strategy was entered into five databases including, MEDLINE, Scopus, PsycINFO, Embase and CINAHL. Following the screening process, the reference lists of included full text articles were hand searched. Forward citation searches as well as author citation searches were completed for included full text studies. Reference lists of relevant systematic reviews exploring housing for people with disability were manually searched for any further studies not captured by the search strategy.
Inclusion criteria
Inclusion and exclusion criteria were developed prior to the screening of abstracts. To be included in this review, peer reviewed articles published between January 2010 and September 2024, written in English were required to report original quantitative and/or qualitative data relating to outcomes associated with housing and support/service models for adults over 18 years old with HD. Studies reporting the perspectives of participants with HD, informal caregivers and allied health professionals were considered eligible. Studies were required to have extractable data relating to people with HD and were excluded if they were not published in a peer-reviewed journal, or had a predominant focus on a population outside of people with HD.
Screening
On completion of the literature search, all citations were imported into Covidence, a web-based bibliography management system, and duplicate studies were removed. Titles and abstracts of eligible studies were independently screened by two reviewers using the inclusion and exclusion criteria outlined above. An interrater agreement rate of 86% was obtained following title and abstract screening. Conflicts were resolved through discussion between the two independent reviewers. A PRISMA flow diagram outlining the study selection process is provided in Figure 1. All 253 eligible full text articles were reviewed by three members of the research team. An agreement rate of 94% was reached, with disagreements resolved by senior investigators (JD and DW) through discussion and consensus. A total of eight studies met the inclusion criteria. No additional articles were included through citation searches or reference lists.
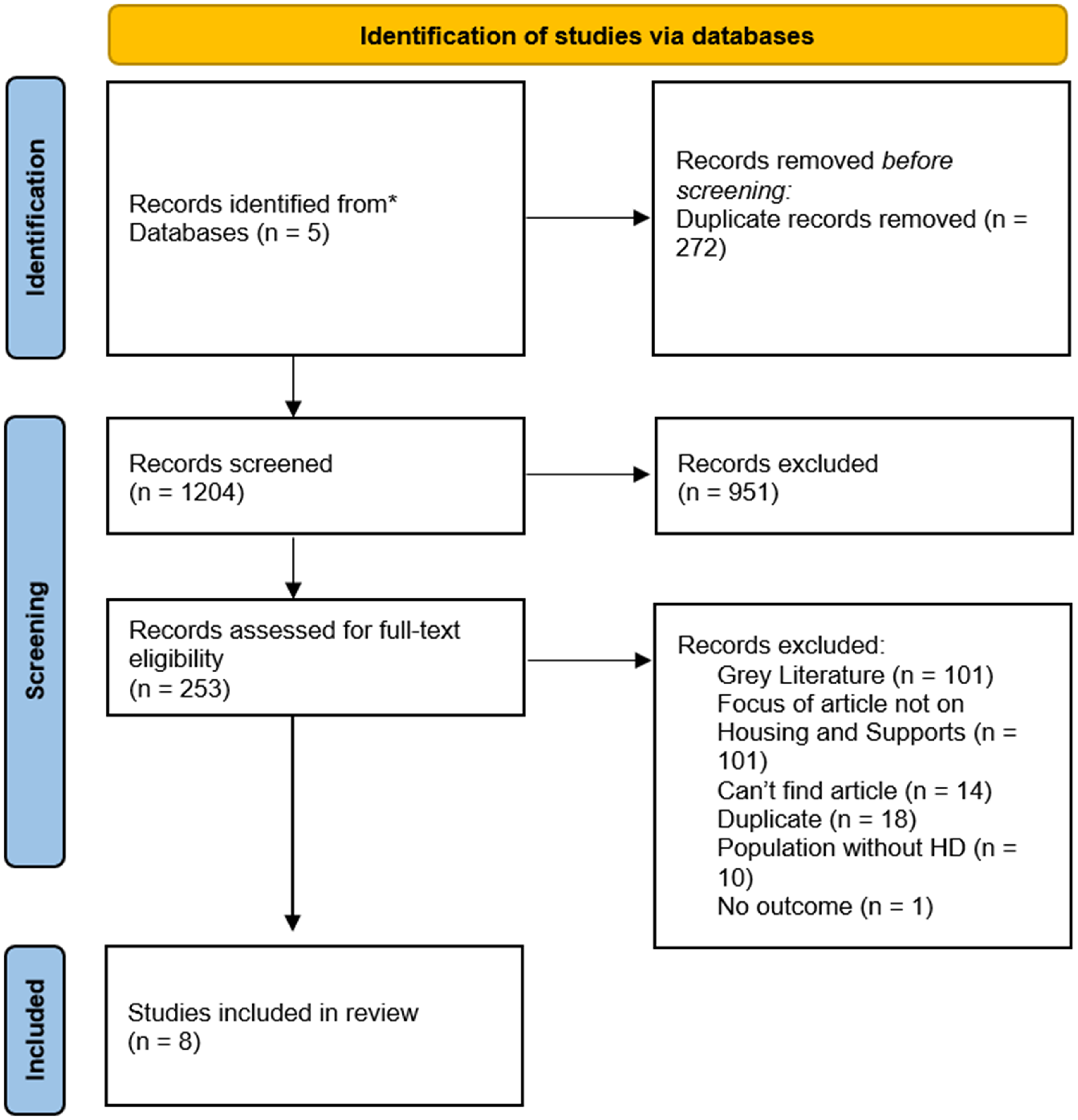
PRISMA flow diagram.
Charting the data
Data extraction was initially conducted by three reviewers independently (ED, EGK, HJ). Data extraction tables were created in Microsoft Excel to extract and prepare the data for analysis. Data charted were: author; study aim; year of publication; study setting; study design; participant recruitment methods; sample size; participant type (e.g., person with disability, informal caregiver, allied health professional); participant age; participant gender; stage of HD; outcome measures used; study outcomes associated with housing and support models for people with HD; main findings; study limitations; conclusions and implications of research.
Collating, summarizing and reporting the results
All data were extracted individually by reviewers ED, EGK and HJ. Extracted data were then combined to ensure uniformity across data extraction processes and prevent the omission of important data. Findings were compared across studies to identify similarities and differences, with these summarized in a table. Findings were then integrated across studies to establish overarching principles related to the housing and support needs of people with HD. Initial findings of the scoping review were presented to a reference group of professionals working with people with HD (n = 5) and a reference group of family caregivers of people with HD (n = 4). Input was provided at a group level, and feedback was recorded and de-identified. Both reference groups agreed that the scoping review findings accorded with their experiences and understanding of housing and support for people with HD.
Results
Half of the studies were conducted during or prior to 2011, and the most recent study was published in 2024. The studies were conducted in several countries including the Netherlands, USA, United Kingdom (UK) and Australia. Four studies were quantitative, three included mixed methodology and one was qualitative (see Table 1). The study settings included an outpatient department, an ambulatory care setting, nursing homes, a neuropsychiatric ward and the community. Seven studies included people with HD, two studies included caregivers, and three studies involved health professionals and others with HD expertise. Regarding the aims of the quantitative studies, one explored the feasibility and acceptability of an outpatient clinic, 40 and the other three studies examined factors that were related to hospital discharge outcomes.41–43 For the mixed methods studies, one presented staff perspectives on providing end of life care for people with HD, 22 and the other two studies explored perceptions of healthcare and factors that influence how people with HD live with the disease.44,45 A qualitative study explored the experiences of case management for people with HD. 46
Study characteristics.

Participant characteristics
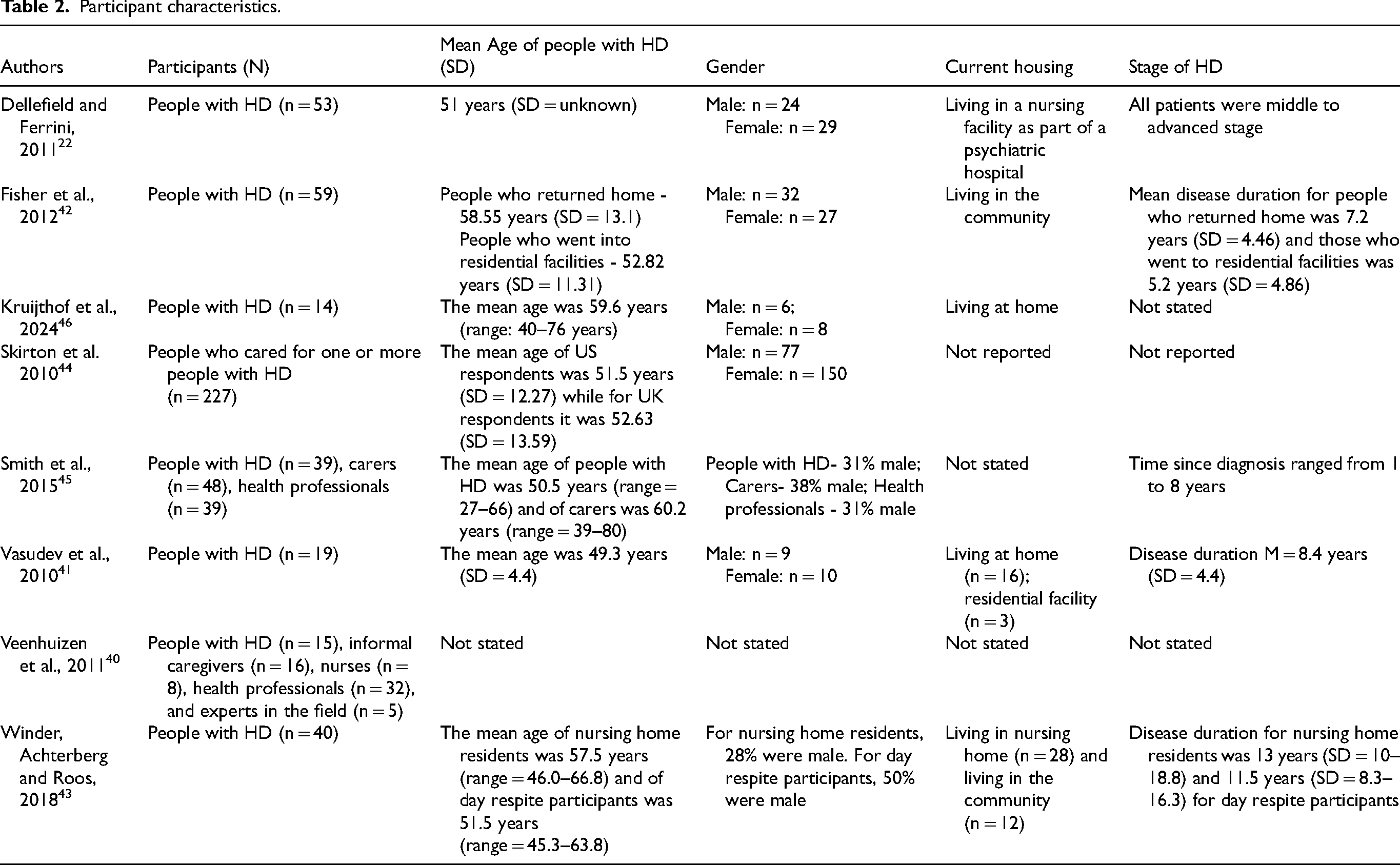
As depicted in Table 2, the studies included relatively small samples of patients with HD ranging from 19–59 participants. One study included a larger sample of caregivers of people with HD (N = 227). The average age of people with HD included in the studies varied from 49–63 years. Although the stage of HD was measured differently in the studies, overall, the studies tended to be focused on people at the middle and advanced stages of the disease. The proportion of males and females with HD were similar although caregivers were more likely to be female. People with HD involved in the studies were living in a range of housing and support models including community, aged care facilities, other facilities, a neuropsychiatric ward and in the community.
Participant characteristics.
Housing and support for people with HD
Overall, no studies specifically sought to investigate effective housing and support models for people with HD. Nonetheless, the integrated findings of the eight studies provided relevant information about the key influences on where and how people with HD are supported. These have been organized across four themes including: (1) demographic factors and disease manifestations associated with community versus institutional living; (2) barriers to sustaining care in the community; (3) service models that facilitate community living; and (4) features of high-quality specialist residential care.
Factors associated with community versus institutional living
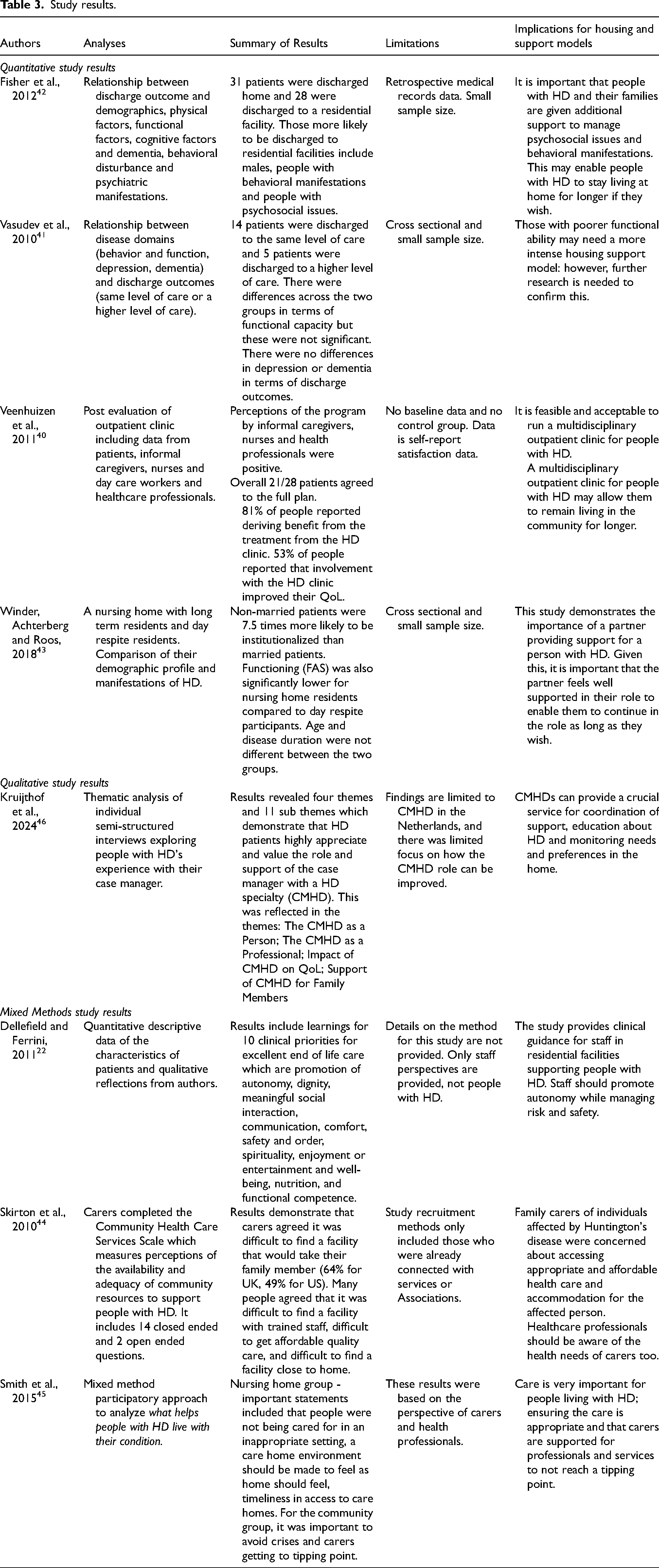
Three studies41–43 described the differences in the characteristics of people discharged to or living in residential care versus those living in the community (see Table 3). Factors included demographics, physical, cognitive and psychological functioning, behavioral manifestations and psychosocial issues (i.e., financial concerns, breakdown in formal and/or informal supports, unstable housing and caregiver stress). Considered together, the findings highlighted that people with behavioral manifestations, poor physical and cognitive status and psychosocial issues were more likely to be living in residential facilities than in their own home. For example, in Fisher et al. 42 people in hospital with behavioral manifestations (i.e., irritability and aggressive behavior) and those experiencing psychosocial concerns were significantly more likely to be discharged to residential care than back home. Physical and functional impairment levels did not significantly differ between those who were discharged home versus those into residential care. Vasudev et al. 41 found that people discharged to a higher level of care from a neuropsychiatric hospital had higher support needs in activities of daily living; however, this was not statistically significant and based on a small sample size. Winder et al. 43 found that although greater functional impairment was associated with living in a RAC facility, having a domestic partner was the strongest predictor of people with HD continuing to live at home.
Study results.
Barriers to sustaining care in the community
Several studies identified systemic and interpersonal barriers to sustaining care in the community, particularly as the disease progresses. A mixed methods survey of caregivers of people with HD in the USA and UK highlighted the difficulties in sourcing appropriate housing and support for the person with HD. 44 Challenges included finding housing and support models with high-quality care, appropriately trained staff with expertise in HD and being in a location that can be easily accessed by friends and family. Caregivers of younger people with HD reported difficulty with finding age-appropriate activities and housing options, as they were largely designed for older adults.
Behavioral manifestations emerged as a key barrier to sourcing and maintaining housing and support arrangements in two studies.44,45 Inadequately trained health professionals and support workers, combined with an unwillingness to upskill in HD, resulted in disruptive moves between care facilities and increased burden on family and friends to provide frequent guidance and supervision to support workers. 44 Caregivers reinforced the need for health and disability support workers to be flexible and learn to work with an individual's routines, needs and preferences. Sometimes, due to the behavioral consequences of deviating from very specific care routines, using paid supports to attend to other domestic and family duties freed up the primary family caregiver to support the person with HD. 45 Where flexibility was not granted, one caregiver reported that “no help is better than inflexibility”. 45 (p264)
Given the progressive nature of HD, timeliness of adaptations and supports was crucial. When there were delays to the receipt of these, the person's disease may have progressed rendering the modifications or equipment redundant. 45 Smith et al. 45 noted that those making decisions about funding for housing, equipment and supports should gain information from informal caregivers as the person with HD may have limited insight into their functional impairments, resulting in insufficient or delayed modifications, equipment and supports.
Service models to support community living
There were two models of support reported that facilitated people with HD to remain at home: (1) outpatient clinics, and (2) specialist case managers. Addressing the complex needs of people with HD and their families, Veenhuizen et al. 40 reported on the acceptability and feasibility of a multidisciplinary outpatient clinic for people with HD living at home. The clinic included assessment by a range of professionals including an elderly care physician, psychologist, occupational therapist, speech and language pathologist, social worker and case manager. A care plan with specialized support for implementation at home was developed including goals across physical, housing, social and psychological domains. The care plan was reviewed every six months and adjustments made as needed. The data on feasibility and acceptability was generally positive with 81% of participants reporting benefit from the intervention, and caregivers reporting that people with HD were able to remain at home for longer due to the intervention. It is noteworthy that the data in this study are self-report, and it is unclear whether this intervention significantly influenced the trajectory of living in the community versus requiring supported disability housing.
A study by Kruijthof et al. 46 explored the experiences of people with HD receiving case management through a specialized HD service in the Netherlands. Case managers specializing in HD (CMHDs) worked closely with a person's medical and allied health team to provide a coordination service that was easily accessible for people with HD. The CMHDs provided advice, such as recommending personal alarms and home modifications, and linked people with services that provided personal care. Engaging with this service enhanced peoples’ confidence in maintaining independence and a continued ability to remain living at home for longer periods. Having expertise in HD meant that CMHDs could have discussions with people about their current support needs as well as planning for the future as the disease progresses. The findings of this study highlight the role of CMHDs in supporting the housing and broader support needs of people with HD.
Features of high-quality specialist residential care
Dellefield and Ferrini 22 revealed key insights from a nursing facility with HD expertise, including the promotion of autonomy, dignity, meaningful social interaction, communication, comfort, safety and order, spirituality, enjoyment, entertainment and well-being, nutrition, and functional competence. Dellefield and Ferrini 22 described the most successful approach to supporting people with HD as the promotion of autonomy and choice while monitoring safety. The authors described the changing support needs during the course of the disease, such as cognitive support (e.g., environmental prompts for ADLs) earlier in the disease, and equipment such as wheelchairs and chairs with specific foam and shape for extended sitting without restraints during the latter stages of the disease. People's bedrooms were designed to facilitate independence and reduce risk of injury. 22 The rooms were restraint free, kept at a cool temperature, and were usually single occupancy. HD-suitable furniture and equipment, such as low beds with padding, grab rails and therapeutic seats were provided in addition to room modifications such as padded walls and the removal of curtains. 22 (p191) As verbal communication skills diminished, staff reportedly drew upon observation and prior needs and preferences to best facilitate choice and control. Staff and family members received education about HD to improve effective communication skills. Nutritional support needs also increased as the disease progressed with some people opting to receive a feeding tube during the advanced stages of living with HD. The nurses included in this study reported striving to provide meaningful social connections and promote a safe and secure environment while undertaking a person-centered approach.
Discussion
Although the included studies provided valuable insights into the housing and supports for people with HD, none deliberately sought to evaluate effective housing and support models for this population. This scoping review highlights the need to conduct further targeted primary research into the housing and support needs and preferences of people with HD, and for further enquiry into the existing models of housing and support for this population internationally. Notwithstanding the dearth of relevant literature, the studies included in the review identify important factors that influence housing and support. These include support needs and preferences, implications for hospitals, and the importance of caregiver support. Unsurprisingly, the findings from this scoping review suggest that there is no “one size fits all” model of housing and support for people with HD. Rather, housing and support models need to be flexible and adapted to individual needs.
Support needs and preferences
The support needs and preferences of people with HD were complex and varied as the disease progressed. Early in the disease, these needs included psychological and social support.22,45 Behavioral manifestations emerged as a predictor of hospitalization and discharge to RAC, 42 and the need for support to manage challenging behaviors emerged strongly as a need for caregivers. 45 As the disease progressed, support needs increased and included mobility aids such as wheelchairs, equipment, specialized furniture and home modifications to improve the ability to navigate the home safely without injury or property damage.22,45 Given the significant functional decline that can occur in HD, there was a need for increased supports to be approved and implemented quickly. This aligns with findings from Bayen et al. 15 who identified high levels of caregiver burden related to behavioral and cognitive symptoms, reinforcing the need for support models that reflect the evolving and multifaceted nature of care preferences in HD. Case managers with expertise in HD provided a crucial role in supporting people to prepare for and navigate these changes. 46
Caregiver training and support are crucial for the sustainability of people being supported to remain living at home. Disability support workers providing paid support, either at home or in residential care settings, require training and supervision in order to provide a high level of support to people with HD. Smith et al. 45 emphasized a need for the extraction of knowledge located at HD centers of excellence into localized multi-disciplinary teams. A key component of training and support for informal and paid caregivers needs to focus on managing behavioral manifestations using Positive Behavior Support; an intervention that can improve quality of life and reduce behavioral manifestations in people with progressive neurological disorders. 47 This may enable people with HD to live at home for longer, if that is their preference, and to receive more appropriate support if living in supported residential housing. However, such preferences may not always be achievable due to limited insight into disease impact, caregiver distress, and the availability of suitable care options.
A home-like environment for those living in supported housing models was emphasized as important. 45 Specialist HD facilities staffed by multidisciplinary teams were highlighted as important given the unique physical, cognitive, behavioral and existential needs of people with HD. Dellefield and Ferrini 22 outlined the specialized equipment needs of people with HD during the mid to advanced disease stages admitted to their facility, including chairs that were specifically designed for people with very limited mobility to remain comfortable and to be able to sit without restraints. While their study highlighted the importance of promoting autonomy and choice, there were also principles relating to providing comfort, safety and well-being. Recent research into individualized housing models for people with disability and complex needs, including people with progressive disorders, found that a transition from RAC to individualized housing was associated with improved social integration and quality of life. 48 Given the unique manifestation trajectory of people with HD, further targeted research is needed into group versus individualized housing and support models for this population.
Implications for hospitals
Given the role of psychosocial challenges and behavioral manifestations in predicting discharge location, there is potential for hospital settings to intervene early in the admission to target housing needs, source funding and provide Positive Behavior Support intervention and training to caregivers and other community supports. Discharge from hospitals back into the home environment requires extensive support and consideration for people with disability and complex needs.49,50 This can include education for family members and paid supports, disability housing, home modifications, equipment, medical and disability supports and access to community-based Allied Health. A case manager with expertise in HD should be sourced as a conduit and point of coordination between hospital and the community. 46
Caregivers may reach a critical point where a person with HD must receive additional or emergency care which may result in admission to hospital. 41 Such junctures present a need for urgent decision making about whether it is possible to sustain living at home with supports, or whether there is a need to transition to disability specific housing. The latter was a concern noted by Skirton et al. 44 who highlighted the difficulties of locating housing with access to staff with expertise in HD, within reasonable proximity to the person's existing communities. A thorough investigation into the HD housing and support models across different countries would provide a useful comparison against findings by Skirton et al. 44
Caregiver support
Caregiver burnout emerged as a risk factor in the sustainability of informal caregiving arrangements once the person with HD's functional impairments increased. Smith et al. 45 emphasized placing equal value on the perspectives of the caregiver and person with HD. Listening to the current support needs or concerns expressed by caregivers, particularly if the person with HD is unaware of the impact to changes in their behavior, can facilitate the provision of more timely and appropriate support. A focus on caregiver needs can identify psychological distress and/or the need for counselling support. 42
Veenhuizen et al.'s. 40 study on the feasibility of an outpatient clinic highlighted the importance of a multidisciplinary team in supporting people with HD and their caregivers. The multidisciplinary team facilitates staying at home for as long as possible and is actively engaged in in-home care. A case manager is the primary point of contact, assisting the team to monitor the patient and train caregivers on HD progression and changes in behavior. Consistent support and monitoring of a person with HD living at home has the potential to extend this living arrangement for as long as possible and, as noted by the study's authors, extend the timeframe in which people with HD can remain living in the community. Although the data on feasibility and acceptability of the clinic was generally positive, it is difficult to draw conclusions about the effectiveness of the model given that no outcomes were assessed at baseline or follow-up and there was no comparison group. Further research should explore the feasibility and effectiveness of this service for people and how this would vary in metropolitan, regional, rural and remote settings.
In the absence of detailed literature on caregivers of people with HD, drawing upon the research into caregivers of people with dementia, which also can encompass a combination of cognitive, physical and behavioral manifestations, may provide helpful insights into interventions that reduce caregiver burden and enhance their capacity to continue providing support as the disease progresses. Yaffe et al. 51 described a need to simultaneously focus on the needs of the person with disability and the caregiver as a unit or dyad to reduce caregiver burden, enhance the person's independence, and reduce costs associated with moving into residential care. Further research should examine the unique experiences of caregivers of people with HD, comprehensively exploring their specific needs and how these change as the disease progresses.
Research implications
The research into housing and support needs for people with HD is very limited. This scoping review has demonstrated that there is a need for further research to understand the effectiveness of housing and support models for people with HD. Given the needs of people can change as the disease progresses, it is important to understand how different models can support people at different stages of the disease. Because HD is both progressive and complex, it is important to recognize early signs that a person may need to transition to a higher level of support. The studies in this review point to functional decline, behavioral manifestations and caregiver burden as key triggers for a move into residential care. Despite this, there are no clear tools or guidelines to guide people on how and when to plan these transitions. Future research should focus on developing clear, reliable ways to guide these decisions to ensure that people with HD and their families are supported at the right time and in the right way.
There is a notable lack of data on HD housing needs, including population-level demographics, residential settings, and support models. In order to evaluate the effectiveness of housing and supports for people with HD, there is a need to first gain a better understanding of their housing and support needs and preferences. Future mixed-methods research should define the housing and support needs of people with HD more precisely. In addition to qualitative investigation, this includes demographic data, disease stage, impairments, quality of life, formal and informal care hours, and associated costs. These represent critical factors in understanding service demand and resource allocation in health and disability sectors. Further, there may be opportunities to evaluate administrative and quality assurance data from organizations providing support to people with HD against these needs and preferences. In the absence of available data, future studies should employ a co-design informed action research methodology for the development of HD-specific services targeting housing and supports.
Summary and conclusions
The eight included studies provided different insights that were influenced by the stage of disease and subsequent support needs and preferences of people with HD and caregivers, and geographical location. For those earlier in the course of living with HD, outpatient clinics emphasized building capacity to ensure people with HD can remain home as long as possible if that is their preference, and if this option is otherwise viable.40,46 For those with mid to advanced HD who could no longer live at home, the emphasis shifted to purposely designed facilities.22,45 A range of factors that can influence a person with HD moving into supported housing earlier than necessary were identified, including behavioral manifestations, psychosocial disadvantage, caregiver burnout and/or not having family that are able to provide support.42,43 There was a lack of confidence in the choices presented to caregivers, a scarcity of HD-trained staff and limited housing options within a preferred location.42,44 Overall, current published research highlights the need to strengthen support for caregivers to sustain home-based care where appropriate, while also ensuring specialized housing and support options are available when living at home is no longer feasible.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable as no additional datasets were generated or analysed during the current study.