
Abstract
Background/Objective:
This study extends prior clinimetric evaluations by examining the factor structure, internal consistency, and distributional properties of the Problem Behaviors Assessment – Short Form (PBA-s) in a large sample of people with Huntington's disease (pwHD) at various stages of progression using the Huntington's Disease Integrated Staging System (HD-ISS) framework.
Methods:
Baseline PBA-s item total scores were analyzed from 14,371 Enroll-HD participants. Using HD-ISS criteria, participants were categorized as Stage 0/1 (n = 3262; 23%), Stage 2 (n = 1722; 12%), or Stage 3 (n = 9387; 65%).
Results:
Missing responses were low across items and stages. Item total score distributions demonstrated significant skew in Stages 0/1 and 2. Within Stage 3, skewness was less prevalent but still present in most distributions. In all groups, the PBA-s demonstrated moderate internal consistency, though five items exhibited weak item-total correlations. Resultant factor structures differed from those previously reported and varied by HD-ISS stage. In Stages 0/1 and 2, a three-factor model representing internalizing, externalizing, and cognitive control problems accounted for 39–42% of the total variance. In Stage 3, a five-factor solution explained 56% of the overall variance and consisted of internalizing, externalizing, cognitive control problems, suicidality, and cognitive dysfunction.
Conclusions:
While the PBA-s demonstrates adequate internal consistency, our results revealed high rates of non-endorsement (i.e., item total scores = 0) and a variable factor structure with disease progression. Thus, the PBA-s may not distinguish mild changes in behavioral symptoms that might occur in early HD-ISS stages of disease.
Plain language summary
Behavioral symptoms are a feature of Huntington's disease (HD) associated with reduced quality of life for people with HD (pwHD) and their families. Reliable and valid assessment of these symptoms are essential for the proper characterization of their frequency, severity, and longitudinal course. In this paper, we examine the measurement properties of an HD-specific measure of behavioral symptoms, the Problem Behaviors Assessment – Short Form (PBA-s). We extend prior investigations by assessing the PBA-s across stages of disease using Huntington's Disease Integrated Staging System (HD-ISS) framework. Results reveal a low level of symptom endorsement across all PBA-s items in earlier stages and a shift in symptom clustering with disease progression. These findings indicate the PBA-s may not capture minimal or mild behavioral changes that might occur in earlier stages of HD.
Huntington's disease (HD) is an inherited neurodegenerative disorder caused by a mutation in the Huntingtin (HTT) gene leading to an abnormally expanded trinucleotide (CAG) repeat. Clinically, HD is often characterized by a progressive decline in motor, cognitive and functional ability. 1 Behavioral symptoms (e.g., depression, irritability, anxiety, and apathy) are also a prominent feature of HD, though prevalence estimates vary across studies and symptom domain. 2 Nevertheless, data indicate that behavioral changes may precede the onset of motor symptoms.3,4 Moreover, behavioral symptoms cause significant distress for people with HD (pwHD) and their families and are associated with increased caregiver burden and reduced quality of life.5,6 Despite the importance of these symptoms, comprehensive or domain-specific field standard assessments of pwHD have yet to be identified.
The PBA-s, which was derived from the Problem Behaviors Assessment (PBA-HD), 7 is a widely used measure of behavioral symptoms in HD research given its relatively broad domain coverage, tolerability, and development for use with pwHD. The PBA-s consists of 11 items, each assessing a different psychiatric symptom domain: depression, suicidal ideation, anxiety, irritability, angry/aggressive behavior, apathy/loss of motivation, perseveration, delusions/paranoid thinking, hallucinations, obsessive-compulsive symptoms, and disoriented behavior. Each item is rated in terms of severity and frequency along a five-point scale for each of the two parameters; an overall item score is calculated by multiplying severity and frequency ratings. PBA-s ratings are based on information obtained in a semi-structured interview with the person with HD and a knowledgeable informant (e.g., spouse, professional carer), if available. 8
In an initial assessment of the clinimetric properties of the PBA-s, interrater reliability was found to be adequate (mean k = .74- .76). 8 A principal component analysis (PCA) with ‘delusions’ and ‘hallucinations’ items removed because of low rates of endorsement resulted in a three-factor solution (Apathy, Irritability, Affective) that accounted for 57.4% of the overall variance. 8 In a subsequent evaluation of a Spanish version of the PBA-s, the scale demonstrated acceptable internal consistency (Cronbach's alpha = .79) and a high degree of test-retest reliability (mean k = .64- .76). A four-factor structure based on severity scores was identified by factor analysis after ‘delusions’ and ‘hallucinations’ items were omitted (Irritability, Depression, Apathy, Perseverance) that explained 56% of the total variance. 9 The inconsistency in the underlying factor structure of the PBA-s may be partially attributable to differences in methodology (e.g., [PCA] vs. exploratory factor analysis [EFA], item total scores vs. severity scores). However, these incongruencies may also point to an unstable factor structure and suggest the need for further analysis.
Establishing clinimetrically sound measures of behavioral symptoms in HD is critical for the appropriate evaluation of targeted therapeutic interventions. The PBA-s was developed for use in HD research; however, data on the clinimetric properties of the PBA-s are both limited and inconsistent. Thus, the aim of this paper is to conduct an in-depth evaluation of the reliability, validity, and factor structure of the PBA-s utilizing data from Enroll-HD, the world's largest observational study of HD. 10 Specifically, our goals were to examine the frequency and distribution of scores, internal consistency, and to determine the underlying factor structure of the PBA-s. To enhance the applicability of our findings to the evolving HD research landscape, we investigated the clinimetric properties of the PBA-s as a function of disease stage in accordance with the HD-ISS framework. 11 Thus, these results may help to determine the clinimetric utility of the PBA-s across stages of HD progression.
Materials and methods
Data source and sample
Enroll-HD is a global clinical research platform and longitudinal observational study designed to facilitate clinical research in Huntington's disease. Research participants are required to complete a core battery of behavioral, cognitive, motor, and functional assessments at annual study visits. Data are monitored for quality and accuracy using a risk-based monitoring approach. All sites are required to obtain and maintain local ethical approval. See Sathe et al. for additional information on the Enroll-HD clinical research platform and study design. 10
The analyses presented in this manuscript were performed using data extracted from the Enroll-HD 2021 periodic data set (PDS-5). Enroll-HD participants with a CAG length greater than or equal to 40 who were 18 years of age or older at the time of first visit were included in the analyses. For all participants for whom an HD-ISS stage could be determined, data from the baseline administration of the PBA-s were used in the analyses.
Problem behavior assessment-short form (PBA-s)
The PBA-s7,8 is an 11-item semi-structured interview that assesses the severity and frequency of problematic behaviors commonly observed in pwHD. The problem behaviors assessed include depression, suicidal ideation, anxiety, irritability, angry/aggressive behavior, apathy/loss of motivation, perseveration, delusions/paranoid thinking, hallucinations, obsessive-compulsive symptoms, and disoriented behavior. Ten of the PBA-s items were derived from the original 40-item PBA-HD and one item assessing obsessive-compulsive symptoms was added. Severity and frequency of each item (i.e., problem behavior) during the previous four weeks are rated using a five-point (0–4) Likert-type scale and a total score for each item is computed by multiplying the severity and frequency scores (item-total score range: 0–16). The HD participant is interviewed together with a knowledgeable informant, when possible, followed by an individual interview with the informant. Ratings are based on all information obtained during the interview, including participant and informant responses and interviewer observations. Further details on the development of the PBA-s are provided in Callaghan et al. 8
Data analysis
The clinimetric properties of the PBA-s were analyzed using a Classical Test Theory (CTT) approach. Item total scores (i.e., severity×frequency) were analyzed with frequency and distribution statistics, including response rates, measures of central tendency, standard deviation, skewness, and minimum and maximum values. Data were assessed for completeness, defined as less than 10% of item data missing. Skewness (values less than −1.5 or greater than 1.5) and response frequency statistics were used to evaluate possible floor or ceiling effects. Internal consistency was assessed using Cronbach's alpha (α) with a threshold of ≥ .70. 12 Correlational analyses were performed to examine the relationship between corrected total score on the PBA-s and individual item (i.e., problem behavior) scores with correlations ≥ .40 considered acceptable. The factor structure of the PBA-s was examined using EFA on all participants with complete data at baseline using the psych package (v.2.4.1) 13 in R Statistical Software (v.4.3.2). 14 Principal axis factoring was conducted and an orthogonal varimax rotation was applied to improve the interpretation of factors. Parallel analysis was used as one source of information to determine the appropriate number of factors. 15 In addition, we examined the screeplot, factor loadings and cross-loadings ≥ .40, and interpretability of factors. 16 Bayesian information criterion (BIC) was also used to determine the value of additional factors.
Disease stage classification using the HD-ISS
The HD-ISS is a research staging system for pwHD based on biological, clinical, and functional landmarks. Stage 0 includes those with a CAG expansion between 40 and 50 but no detectable indicators of disease; Stage 1 is defined by a biomarker of pathogenesis, namely reductions in striatal volume; Stage 2 signifies the start of clinical indicators, such as cognitive and/or motor symptoms; and, finally, Stage 3 indicates functional decline. 11 In these analyses, the clinimetric properties of the PBA-s were assessed by disease stage using HD-ISS classification. However, given that neuroimaging data is not included in the Enroll-HD dataset, participants in Stages 0 and 1 could not be distinguished and, thus, comprised a single group. 17
Results
Sample descriptives
The sample included 14,371 Enroll-HD participants. Of these, 3262 (22.70%) participants were categorized as Stage 0/1, 1722 (11.98%) were categorized as Stage 2, and 9387 (65.32%) were categorized as Stage 3. Demographic and clinical characteristics of HD-ISS subgroups are presented in Table 1.
Demographic and clinical characteristics by HD-ISS stage.
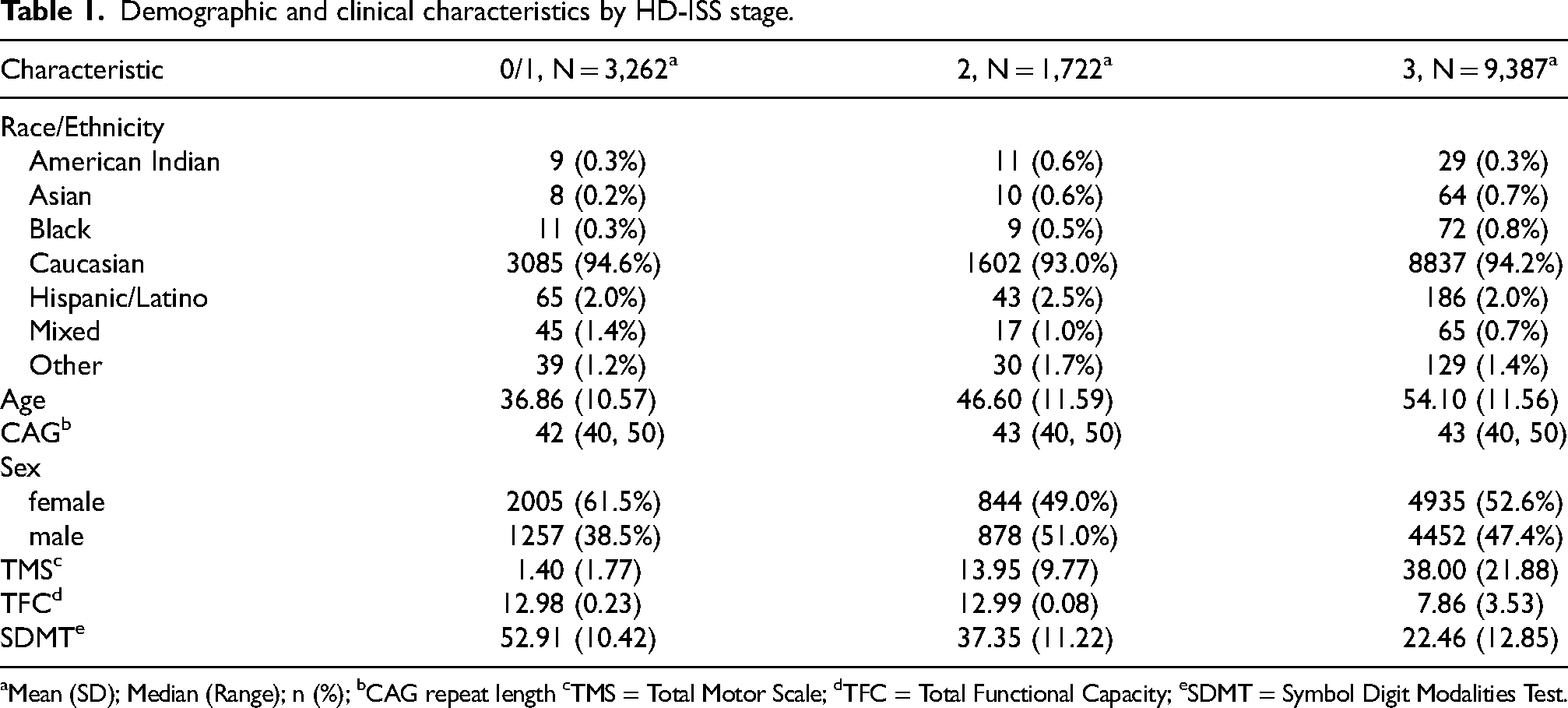
Mean (SD); Median (Range); n (%); bCAG repeat length cTMS = Total Motor Scale; dTFC = Total Functional Capacity; eSDMT = Symbol Digit Modalities Test.
Data completeness
Of all participants, 99.6% were administered the PBA-s; these rates were similar across stages (99.47–99.88%). Of those administered the PBA-s the percentage of missing responses was below 0.5% across all PBA-s items in Stages 0/1 and 2, indicating a very high completion rate. Rates of missingness were somewhat higher among Stage 3 participants, but below 2.0% for each item. Missing data were excluded from analyses (i.e., imputation was not performed). 18
Floor and ceiling effects
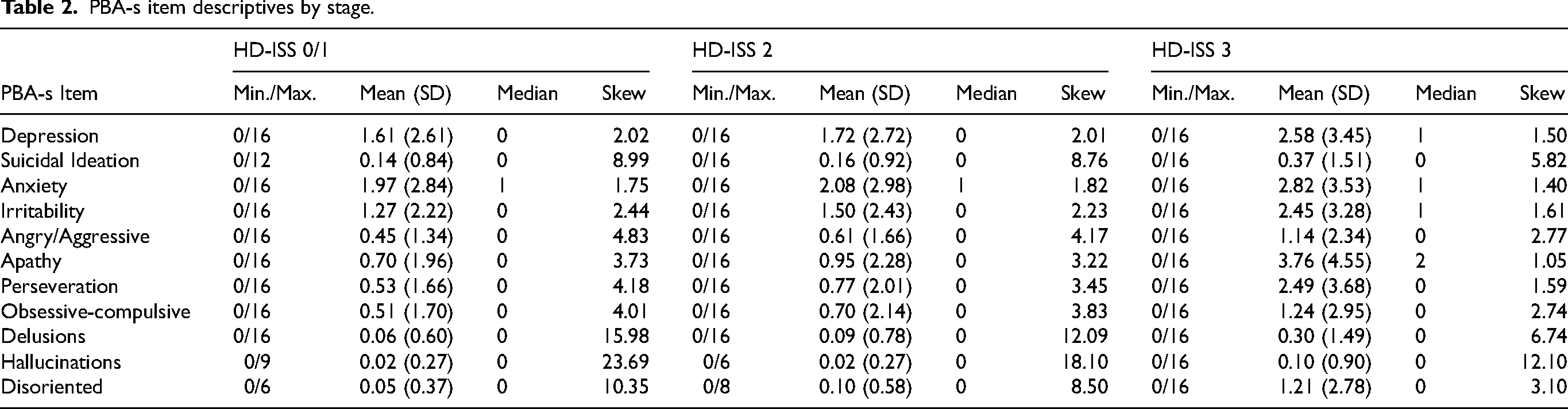
The modal PBA-s item total score was 0 (i.e., absent; never/almost never) in all HD-ISS stages, suggesting low levels of problematic behaviors overall. Item total score distributions were generally highly positively skewed, reflecting a high proportion of low scores, particularly in Stages 0/1 and 2 where all skew values exceeded the specified threshold (1.5). In Stage 3 participants, most PBA-s items also exhibited a right skew except for depression, anxiety, and apathy. The mean score at the 75th percentile was 0 for suicidal ideation, delusions, hallucinations, and obsessive-compulsive items across all HD-ISS stages, and 78–99% of participants had total scores of 0 on these items, suggesting a low base rate for the presence of these symptoms. When examined separately, severity and frequency scores also demonstrated significant skew and low rates of endorsement (i.e., scores > 1) across stages. Together, these results demonstrate the presence of significant floor effects for most PBA-S items (see Table 2).
PBA-s item descriptives by stage.
Internal consistency
Cronbach's alpha exceeded the .70 threshold (.73–.76) in all groups, indicating moderate internal consistency across item total scores. Corrected item-total correlations (r) were above .40 for six of the eleven items, however, suicidal ideation, delusions, hallucinations, obsessive-compulsive symptoms, and disoriented behavior fell below this cut-off across stages. Removal of items with low power for discriminating between high and low overall PBA-s scores resulted in minor improvement in Cronbach's alpha (Table 3).
PBA-s internal consistency statistics by stage.
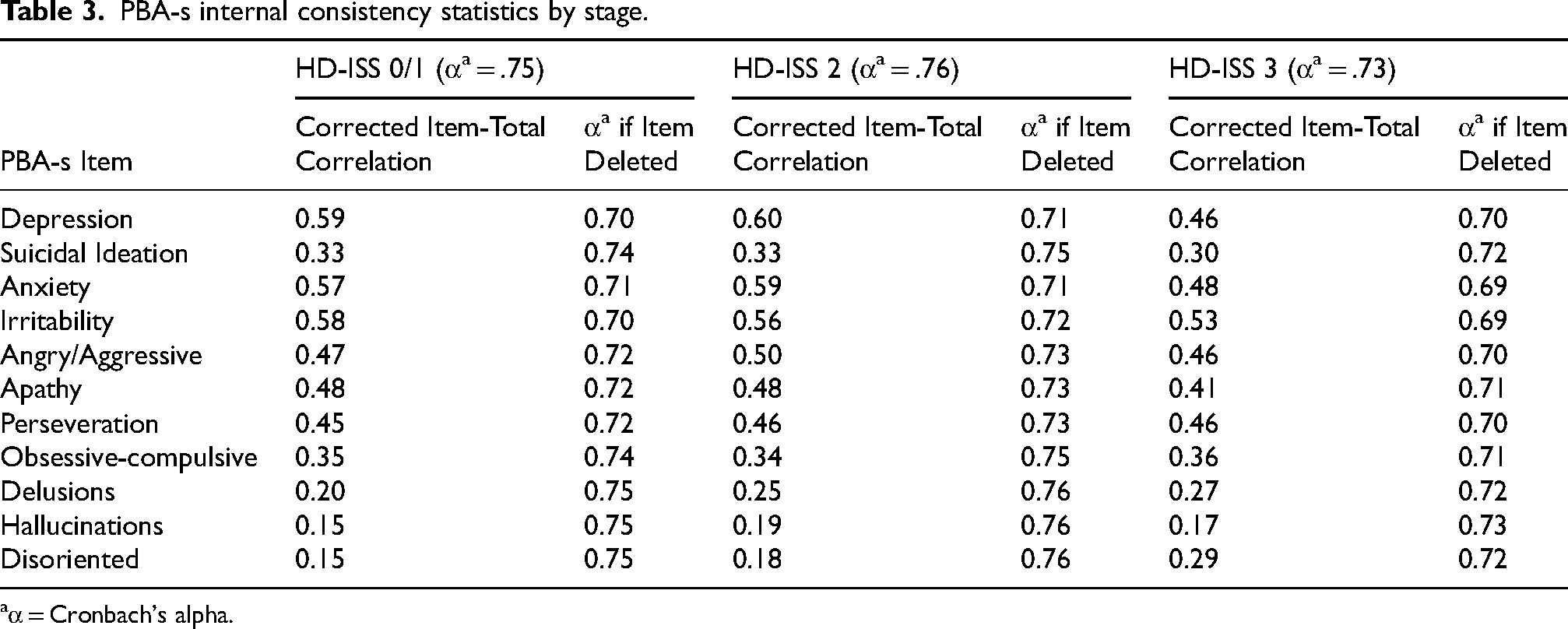
α = Cronbach's alpha.
Factor structure
Unidimensionality is not assumed on the PBA-s (i.e., no total is score computed), therefore, a factor analysis was conducted to examine the number and nature of factors underlying the PBA-s across stages of disease. As in previous research,8,9 delusions and hallucinations items were not included in the factor analysis given their extremely low endorsement rates. While rates of endorsement were similarly infrequent for both suicidal ideation and disorientation items, these items were retained in the analysis to allow for comparison with prior findings.
Examination of the inter-item correlation matrix indicated factor analysis was appropriate (i.e., items were sufficiently inter-correlated). 19 Analysis of BIC statistics suggested a three-factor solution for HD-ISS 0/1 and 2 groups, accounting for 39.2% and 41.6% of the total variance in PBA-s item scores, respectively, consisting of items representing internalizing problems (depression, anxiety, apathy), externalizing problems (irritability, anger), and cognitive control problems (perseveration, obsessive-compulsive symptoms). In these stages, suicidal ideation and disoriented behavior did not load onto any factor. In Stage 3, analysis of the BIC statistics suggested a five-factor solution that explained 55.5% of the overall variance. Inspection of the Varimax rotated factors revealed an interpretable structure with moderate to high loadings. The first factor included items corresponding to externalizing problems (irritability, anger), a second factor consisted of items relating to internalizing problems (depression, anxiety), a third factor represented suicidality (suicidal ideation), a fourth factor included items reflecting cognitive dysfunction (apathy, disoriented behavior), and a fifth factor comprised of items indicative of cognitive control problems (perseveration, obsessive-compulsive symptoms). Factor loadings are displayed in Table 4. Similar results were obtained with an oblique rotation method (promax) (see Supplemental Material).
PBA-s factor solutions and item loadings by stage.
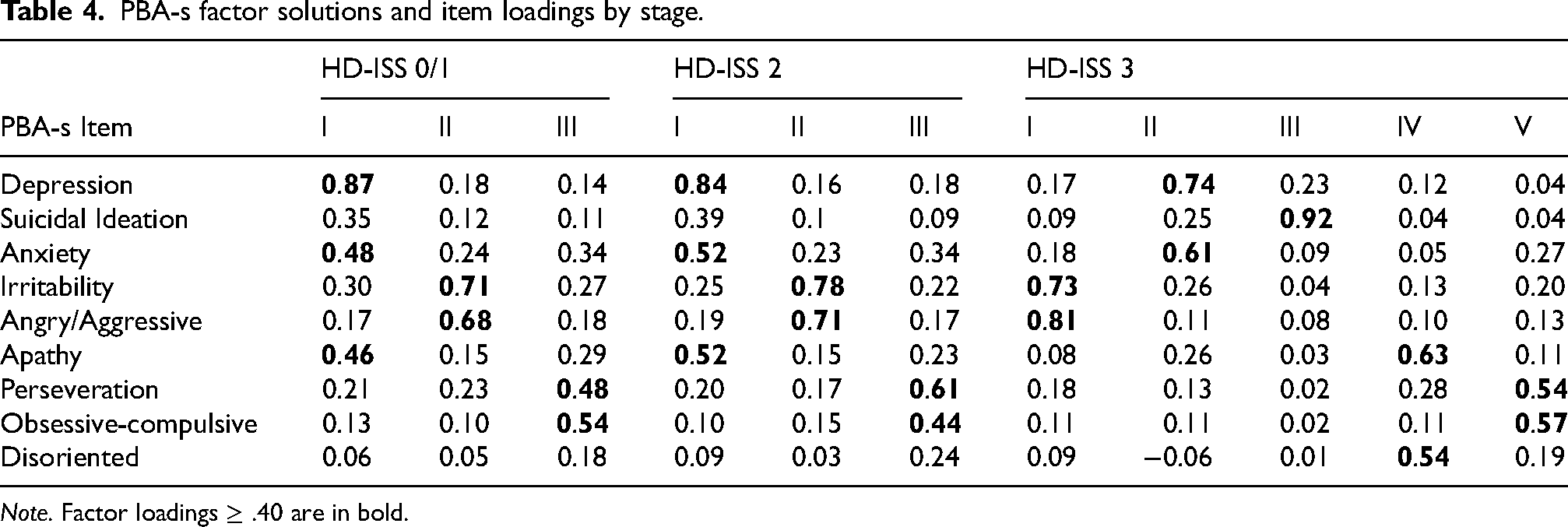
Note. Factor loadings ≥ .40 are in bold.
Discussion
The purpose of these analyses was to evaluate the clinimetric characteristics of the PBA-s within and across HD-ISS stages. The scale was generally well-tolerated with less than 1% of data missing in earlier disease stages and below 2% in Stage 3. Consistent with previous studies, 9 our data indicated that internal consistency of the PBA-s was moderate across stages. Several items with low rates of endorsement (i.e., suicidal ideation, delusions, hallucinations, obsessive-compulsive symptoms, and disoriented behavior) unsurprisingly exhibited weak associations with PBA-s total score.
Significant skewness was prevalent across items and stages, where the majority of participants had low PBA-s scores. While the course and severity of behavioral symptoms is variable in HD, substantial data indicate these symptoms are a prominent and prevalent feature of the disease, 2 particularly in later stages of progression.3,20,21 In our data, less skewness was observed in HD-ISS 3, however, scores generally fell within the mild range. This is in contrast to a number of prior studies that report moderate to severe levels of symptoms such as depression,22,23 anxiety, 23 irritability, 24 and apathy21,24 in later stages of HD (i.e., after clinical motor diagnosis), using other measures. Importantly, even in earlier stages of disease (i.e., prior to clinical motor diagnosis), reported prevalence of depressive disorders, anxiety disorders, and clinically significant apathy is 15–20%.25–27 It is possible that the observed skewness in our data reflects low base-rates of these phenomena. Alternatively, these findings may suggest a floor effect in which the PBA-s is unable to differentiate between lower levels of behavioral symptoms. Given these distributional properties, the PBA-s may have limited utility as a screening tool or clinical research outcome measure for detecting milder levels of problem behaviors that may be present prior to HD-ISS 3.
Previous investigations of the factor structure of the PBA-s have yielded variable results. It is unknown whether reported variations in the underlying factor structure of the PBA-s may be attributed to study sample characteristics (e.g., disease stage composition) or differences in statistical approach (i.e., model or estimation methods). Despite their clinical significance, psychotic symptom items (i.e., hallucinations and delusions) were not included in our examination of the PBA-s factor structure to allow for a direct comparison with prior investigations.8,9 In our data, a three-factor structure was identified in Stages 0/1 and 2 comprising of internalizing problems (depression, anxiety, apathy), externalizing problems (irritability, anger), and cognitive control problems (perseveration, obsessive-compulsive symptoms), while suicidal ideation and disorientation items did not load onto any factor, likely as a result of low rates of endorsement. However, in Stage 3, a different factor structure emerged consisting of five constructs: internalizing problems (depression, anxiety), suicidality (suicidal ideation), externalizing problems (irritability, anger), cognitive dysfunction (apathy, disorientated behavior), and cognitive control problems (perseveration, obsessive-compulsive symptoms). Though there is some overlap (externalizing problems, cognitive control problems factors), the factor structure we observed in both early (HD-ISS 0/1 and 2) and later (HD-ISS 3) stages of disease progression largely differs from that previously reported in mixed premanifest/manifest 8 and predominately manifest 9 HD samples. Therefore, previously reported factor structures may not accurately describe typical symptom associations specific to HD-ISS stages.
The increased number of factors observed in HD-ISS 3 suggests that HD-specific behavioral domains may not be clearly distinguishable until later in the disease course (i.e., in conjunction with or subsequent to the onset of motor, cognitive, and functional decline). The shift in apathy from the internalizing problems to the cognitive dysfunction factor and the emergence of suicidal ideation as a single-item “factor” independent of depression, anxiety, or other psychiatric symptoms is especially noteworthy. The change in the placement of apathy within the factor structure is consistent with apathy being a common feature of depressive syndromes, which may be similar in early HD-ISS stages to those seen in the general population. However, apathy also often emerges as a distinct expression of impaired frontal lobe circuitry and has been specifically linked to damage to anterior cingulate lobe feedback circuits, which pass through the affected striatal region in HD. 28 Thus, while subtle symptoms in earlier stages might have resulted in broader factors, as HD progresses, specific symptoms (i.e., suicidal ideation, apathy) may become more prominent, leading to greater distinction among factors. This is further supported by longitudinal data indicating apathy progresses with disease course. 27
The PBA-s item domains are fairly broad and may encompass multiple constructs. For example, the PBA-s apathy item assesses “loss of interest”, “emotional blunting”, “lack of perseverance”, “reduced spontaneity” and a “can’t be bothered” attitude. However, apathy has long been conceptualized as a multidimensional syndrome, consisting of dissociable subtypes (i.e., cognitive, behavioral, emotional apathy), each with distinct neurobiological underpinnings.29–31 Importantly, some data suggests that prevalence and severity of apathy may vary by subtype (i.e., cognitive, behavioral, emotional apathy) over the course of HD; for example, an increase in behavioral apathy has been reported after clinical motor diagnosis. 32 The multidimensional nature of apathy may explain the observed shift in its loading in earlier versus later stages. It is possible that PBA-s scores fail to capture the nuances of HD-specific behavioral symptomatology, particularly in early HD, and as symptoms evolve across stages of HD progression.
Limitations
It is important to note several limitations to our findings. First, our sizeable HD sample varied in its clinical characteristics but was not racially diverse (94% Caucasian), thus, our findings may lack generalizability. Second, few efforts to cross-culturally validate the PBA-s have been undertaken, therefore, it is uncertain whether the PBA-s is appropriate for use in different cultural and ethnic groups. Nevertheless, the Enroll-HD study includes participants from around the globe (23 countries). Third, it is not assumed that items on the PBA-s represent a single unifying construct and, thus, examination of certain clinimetric properties such as mean inter-item correlation (consistency) of the PBA-s may be limited in interpretability. The interpretability of identified latent factor structures may also be obfuscated as a result of significant skew across PBA-s items and HD-ISS groups. Additionally, the factors that emerged consisted of few items with relatively low loadings, potentially limiting the generalizability of our results.19,33 However, the latter weaknesses in our data may have been mitigated by a large sample size.
Conclusions
In summary, the goal of this paper was to evaluate the clinimetric properties of the PBA-s in a large sample of people with HD and discuss implications for its utility across stages of disease progression using an evidence-based classification system. The PBA-s demonstrated moderate levels of internal consistency, however, issues with skewness indicate the PBA-s may fail to capture milder but potentially meaningful changes in frequency and severity of behavioral symptoms in earlier stages of disease. Future studies utilizing structured clinical interviews may help to clarify the frequency and severity of behavioral symptoms in early HD. Results from our factor analysis were inconsistent with prior reports and varied across HD-ISS defined stages. These data raise concerns about the appropriateness of the PBA-s for assessing attenuated levels of behavioral symptoms that might occur in earlier stages of disease; however, it may be a useful measure for characterizing more marked behavioral changes that might be present in later stages. Thus, there is an existing need for valid, reliable, and robust measures of behavioral symptoms suitable for use across all stages of HD.
Supplemental Material
sj-docx-1-hun-10.1177_18796397261423978 - Supplemental material for A clinimetric evaluation of the problem behaviors assessment short form (PBA-s) within the context of the Huntington's disease integrated staging system (HD-ISS)
Supplemental material, sj-docx-1-hun-10.1177_18796397261423978 for A clinimetric evaluation of the problem behaviors assessment short form (PBA-s) within the context of the Huntington's disease integrated staging system (HD-ISS) by Docia L Demmin, Matthew W Roché, Jatin G Vaidya, Douglas R Langbehn, Rebecca LM Fuller, Sarah ZWeingast, Cristina Sampaio and Glenn T Stebbins in Journal of Huntington's Disease
Footnotes
Acknowledgements
Biosamples and data used in this work were generously provided by the participants in the Enroll-HD study and made available by CHDI Foundation, Inc. Enroll-HD would not be possible without the vital contribution of the research participants and their families. We also thank the individuals who contributed to the collection of Enroll-HD data: ![]() .
.
Ethical considerations
All Enroll-HD sites are required to obtain and maintain local ethical approval.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
D.L.D., M.W.R., R.L.M.F., and C.S. conceived of the project. The analyses were informed by D.R.L. and G.T.S. and conducted by J.G.V. All authors contributed to the interpretation of the results, writing of the manuscript, and approved of the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.L.D., M.W.R., R.L.M.F., S.Z.W., and C.S. are employed by CHDI Management, Inc. as advisors to CHDI Foundation, Inc. J.G.V., D.R.L., and G.T.S. are paid statistical consultants for CHDI Foundation, Inc. D.R.L. is also a paid biostatistical consultant to the Huntington Study Group, Sage Pharmaceuticals, Prilenia, Guidepoint Consultants, and Uniqure for designing Huntington's disease trials and an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability
Enroll-HD is a clinical research platform and longitudinal observational study for Huntington's disease families intended to accelerate progress towards therapeutics; it is sponsored by CHDI Foundation, a nonprofit biomedical research organization exclusively dedicated to collaboratively developing therapeutics for HD. Core datasets are collected annually from all research participants as part of this multi-center longitudinal observational study. Data are monitored for quality and accuracy using a risk-based monitoring approach. Datasets and biosamples from several studies are made available through the Enroll-HD platform: ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.