
Abstract
Introduction
People with Huntington's disease (HD) are encouraged to consider end-of-life planning early on to mitigate future challenges. Initial evidence shows that undertaking planning discussions around this subject presents various barriers; however, a comprehensive evidence synthesis has not been completed to date. Accordingly, we here synthesise evidence regarding experiences of end-of-life planning discussions (EOLPD) among people with HD, their families and familial caregivers, and healthcare professionals supporting them.
Methods
Five databases were systematically searched for peer-reviewed articles addressing the research question. After screening, eight articles meeting the inclusion criteria were identified, and a narrative synthesis undertaken to develop key themes.
Results
Four themes were developed. “The value of EOLPD” details the perceived effectiveness of such discussions. “To talk or not to talk” reflect motivations to seek out or avoid EOLPD. “A clear vision of the future” encapsulates how EOLPD may provide comfort for some but fear and anxiety for others. The final theme highlights the importance of those engaging in EOLPD accessing “The right people at the right time”.
Discussion
End-of-life planning in HD remains inconsistently implemented and often process-focused, with a need for more holistic and patient-centred discussions. Further research is necessary to explore needs, expectations and experiences among HD families, and to support healthcare professionals to successfully lead on introducing these discussions. Additionally, much of the literature addressed euthanasia rather than natural death, highlighting a need for more research in the context of natural death.
Keywords
The prevalence of Huntington's disease (HD) is estimated at 4.88 per 100,000 people worldwide, 1 and in the UK has been estimated as high as 12.3 per 100,000. 2 The condition brings a range of challenges, for people carrying the gene expansion and their caregivers. McColgan and colleagues 3 describe motor disturbances that typically begin with hyperkinetic chorea, later developing into hypokinetic motor features, dystonia, bradykinesia, and changes in speech and swallow. These motor symptoms are used diagnostically for manifest HD. However, other HD-related difficulties may begin many years prior to manifest symptoms, growing in severity as the condition progresses. These include cognitive decline (impacting on skills such as executive function, insight, processing speed, attention, memory and orientation) and changes in emotion (including anxiety, depression or low mood, and irritability). These difficulties profoundly affect not only the individual, but those supporting them, bringing changes in quality of life, caregiver burden, and loss of jobs, roles and social networks.4–7
The inevitable progression of HD over time results in individuals requiring full nursing care in later stages, and medical or surgical intervention to ameliorate concerns relating to swallow and malnutrition. 3 Best practice guidance suggests that end-of-life planning discussions (EOLPD) are essential given the certainty of HD progression, and that these discussions should take place as early as possible in the HD journey. This enables the individual to prepare plans with their family and healthcare professionals while they retain capacity to meaningfully make these choices. 8
HD and end-of-life
Defining the end stage of life, and its markers, in people with HD is complex; Klager and colleagues describe prognostication of end-of-life in HD to be “the crux of the caregiving dilemma”. 9 p.77. By one definition, “end stage” in HD is suggested to be when the individual becomes fully dependent on others to maintain their activities of daily living – but this is a period of decline which can be managed over many years, differing from (for example) acute neurological or oncological conditions. 10 Moskowitz and colleagues 11 suggest that weight loss and recurrent infections could indicate approaching end-of-life in HD; however, some individuals with HD may experience such crises, recover and subsequently plateau in their deterioration, 9 whilst others may be stable for a time and die quite suddenly without such indicators, with death therefore being difficult to predict with confidence. 12 The commonest cause of death among people with HD is reported as pneumonia, which may be a clearer indicator of end-of-life 13 ; however, Heemskerk and colleagues 14 note that recurrent infections may be managed successfully prior to the final infection, such that even this risk factor is not a clear marker of end-of-life. It is also crucial to note that end-of-life in HD may be even more complex than this; individuals who carry the HD gene expansion may consider themselves to be approaching end-of-life from a much earlier point, including when they develop symptoms. From our clinical experience, this may even include people engaging with the concept of end-of-life from the point of their positive genetic test for HD, which may be years or decades before manifest HD develops. These complexities and experiences are extremely understudied in the current literature, and we will revisit this in the Discussion.
The protracted end stage and uncertainty of end-of-life in HD, and the loss of capacity to make related decisions which occur as HD progresses, dictates that considering end-of-life early is essential in order for the individual to have meaningful input into these important processes while still able. 8 A range of mechanisms are available in the UK to support people with HD in advance planning for their end-of-life, though these do of course vary internationally. 15 The term “advance care plan” encompasses several documents which can support recording of end-of-life wishes. “Advance statements” encourage individuals to express their preferences around support or preferred place of care but are not binding; decisions can still be made by others in best interests’ situations where the individual is confirmed as not having mental capacity regarding that decision. Completing documentation granting “power of attorney” for decisions around health and welfare legally allows named individuals to make related choices on behalf of the patient, although this brings its own complexities for those nominated and interactions between healthcare teams and nominated individuals are frequently sensitive and complex. “Advance decisions to refuse treatment” are legal and binding and can be used to anticipate any probable intervention to prolong life that the individual may wish to avoid. Once a palliative care pathway is agreed, a “Recommended Summary Plan for Emergency Care and Treatment” (ReSPECT) form is available for the individual (or those with power of attorney) to complete and clarify their wishes in relation to end-of-life. Finally, “do not attempt resuscitation” (DNAR) forms enable the person or their attorney(s) to refuse intervention if the heart stops beating or if the person requires ventilation to support life.
These documents all require comprehensive and collaborative EOLPD to complete. However, barriers to EOLPD in HD populations appear complex and varied. Perhaps unexpectedly, one is hope. With HD believed to be a candidate for prevention or disease modification as treatments advance, 3 individuals affected by HD and their families are understandably hopeful for a cure or a means to stay its progress. In this context, EOLPD discussions can feel inappropriate, unnecessary or unwanted, as some people with HD hope that a solution will be found before they need to consider end-of-life plans. 16
A further barrier to EOLPD is stigma and a reluctance to speak about HD at all. Prior experiences of HD can be clouded by historical stigma; Wexler suggests that this stigma “perpetuates”. 17 p.19, leaving those affected reluctant to share their experiences and resulting in a “devastating silence”. 17 p.18. People affected by HD also experience stigmatising attitudes in relation to visible symptoms such as chorea, which can result in withdrawal and reluctance to seek support.18,19 Attitudes may also be influenced by cultural differences in responses to visible illness and neurodegenerative conditions, but evidence in this regard is presently limited and presents a priority for future research.
In addition, changes in cognition (notably anosognosia, 7 or loss of insight into difficulties) and psychological rejection of distressing advancement of symptoms can result in individuals being unable or unwilling to discuss end-of-life. Some professionals may also be cautious of causing distress by beginning these conversations, meaning that EOLPD may not be raised at all. 8 However, these discussions are crucial for healthcare professionals to understand the needs and preferences of the person with HD, in order to provide and contextualise person-centred end-of-life care in future.
Review aim and rationale
Individuals with HD inevitably face progression of their condition. To provide meaningful, person-centred support, it is crucial to understand what supports and hinders good communication around planning for end-of-life among this population.
The current evidence regarding EOLPD for people with HD, taken together, presents a complex clinical picture requiring a robust synthesis. Accordingly, this review will identify and synthesise evidence examining experiences of seeking and undertaking EOLPD among people who carry the HD gene expansion, their relatives and familial caregivers, and the healthcare professionals who support them. Synthesis of perspectives of all these groups will offer a holistic overview of communication around end-of-life in HD.
Method
Search strategy
A systematic search was undertaken to identify papers describing experiences and perceptions of EOLPD among individuals with HD, their family members, familial caregivers, and healthcare professionals supporting people affected by HD. Search terms and searches were planned and conducted with guidance from a university specialist subject librarian, using the Medline, Scopus, Web of Science, APA PsycINFO and CINAHL electronic databases. Searches were undertaken in April 2024 and refreshed in October 2024. Before commencement of searches, the review was registered on PROSPERO (reference: CRD42024522893).
The following terms were used for searches, with MeSH terms included preferentially where possible: ‘Huntington*’ AND (end-of-life OR ‘end of life’ OR palliative OR death OR dying OR end stage OR ‘end stage’) AND (‘discussion’ or ‘plan*’ or ‘advance*’).
In total, 1700 articles were found. Following removal of duplicates, 1283 papers were screened by title, with a further 1218 removed at this stage. Subsequently, 65 abstracts were screened, after which 27 full articles were read in full by two reviewers. The second reviewer (SB), who has experience in psychological research into HD, reviewed the 27 papers independently of the lead author (CL). Any disagreements were resolved through discussion, with agreement reached on eight papers and one paper also referred to a third senior reviewer (SG) for a final decision. Eight papers were agreed for inclusion through this process (for inclusion criteria, see Table 1; for PRISMA flow chart, see Figure 1).
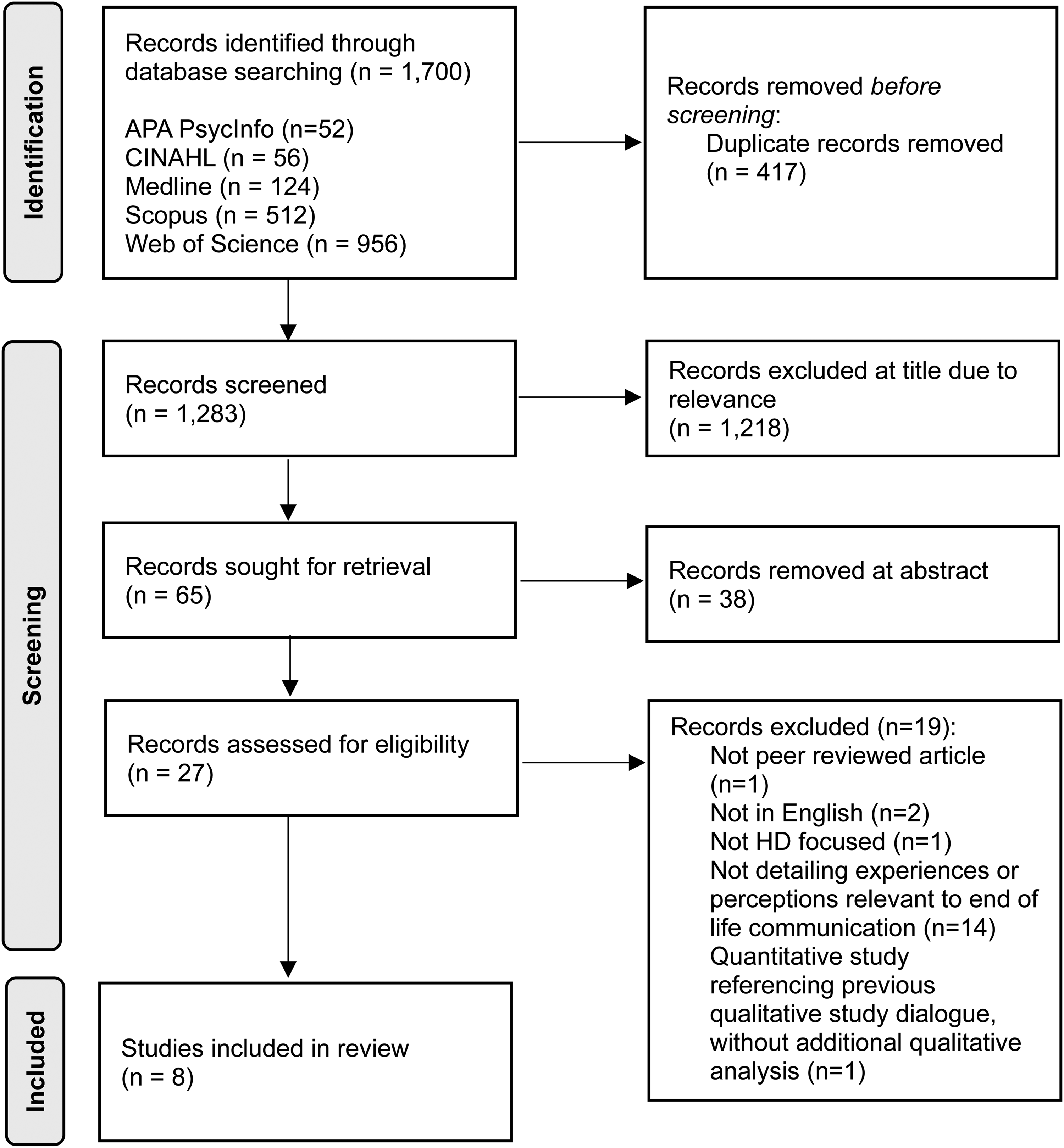
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) search process flow diagram.
Inclusion criteria for selected papers.
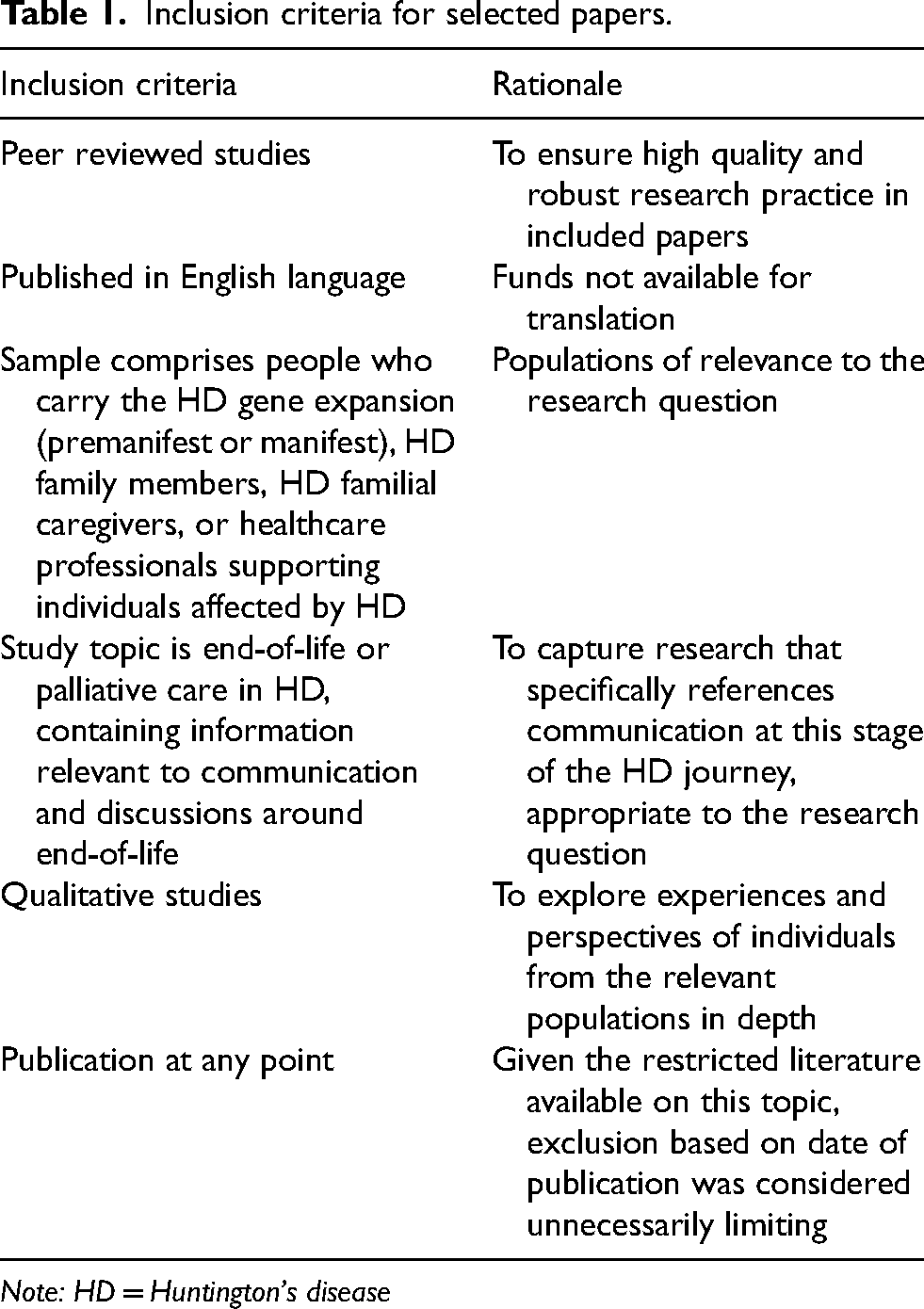
Note: HD = Huntington's disease
Quality assessment
The identified studies used a range of study methods including interview-based qualitative approaches, and quantitative studies using questionnaires and patient-reported outcomes. Accordingly, the Mixed Methods Appraisal Tool (MMAT) 20 was used to perform quality appraisals (Table 2). No papers were excluded on quality grounds, due to the limited evidence base, but limitations of the set of identified papers and potential impacts of these are outlined in the Discussion.
Outcomes of quality appraisal: criteria from Mixed Method Appraisal Tool (MMAT) – qualitative version.

Note: U = unclear; Y = yes
Data analysis
Narrative synthesis was selected to draw together the diverse studies identified, as this approach allows for a flexible integration of findings across varied approaches and relevant research questions, enabling a structured and detailed overview of findings across the literature. Narrative synthesis has been criticised for a lack of transparency and rigour
28
; to address this concern, we followed the widely-used guidance from Popay and colleagues
29
on robust and transparent conduct of narrative synthesis in systematic reviews. Following this, a four-step analysis was undertaken:
Developing a ‘theory of change’. By synthesising evidence regarding EOLPD for people with HD from the perspectives of people carrying the gene expansion, their family members and healthcare professionals, this review will offer direction to future research focusing on issues identified among the HD community around EOLPD, and contribute to wider healthcare planning around EOLPD for people with HD. Developing a preliminary synthesis of findings from included studies. Textual descriptions of study findings and tabulation of study properties was completed to develop an initial understanding of patterns and relationships between the data (Table 3). Exploring relationships within and between studies. Through coding and thematic analysis, we examined trends and similarities in the set of papers and their data, identifying contradictions and tensions, and exploring influences of different contexts and populations. Assessing the robustness of the synthesis. We assessed the methodological quality of included studies (described above), evaluated the consistency of findings across studies and the plausibility of the developed findings in context of existing literature, and reflected on limitations of the synthesis process (e.g., biases, methodological flaws, and/or issues with the evidence base including gaps or study quality issues).
Characteristics, aims and key outcomes of included studies.
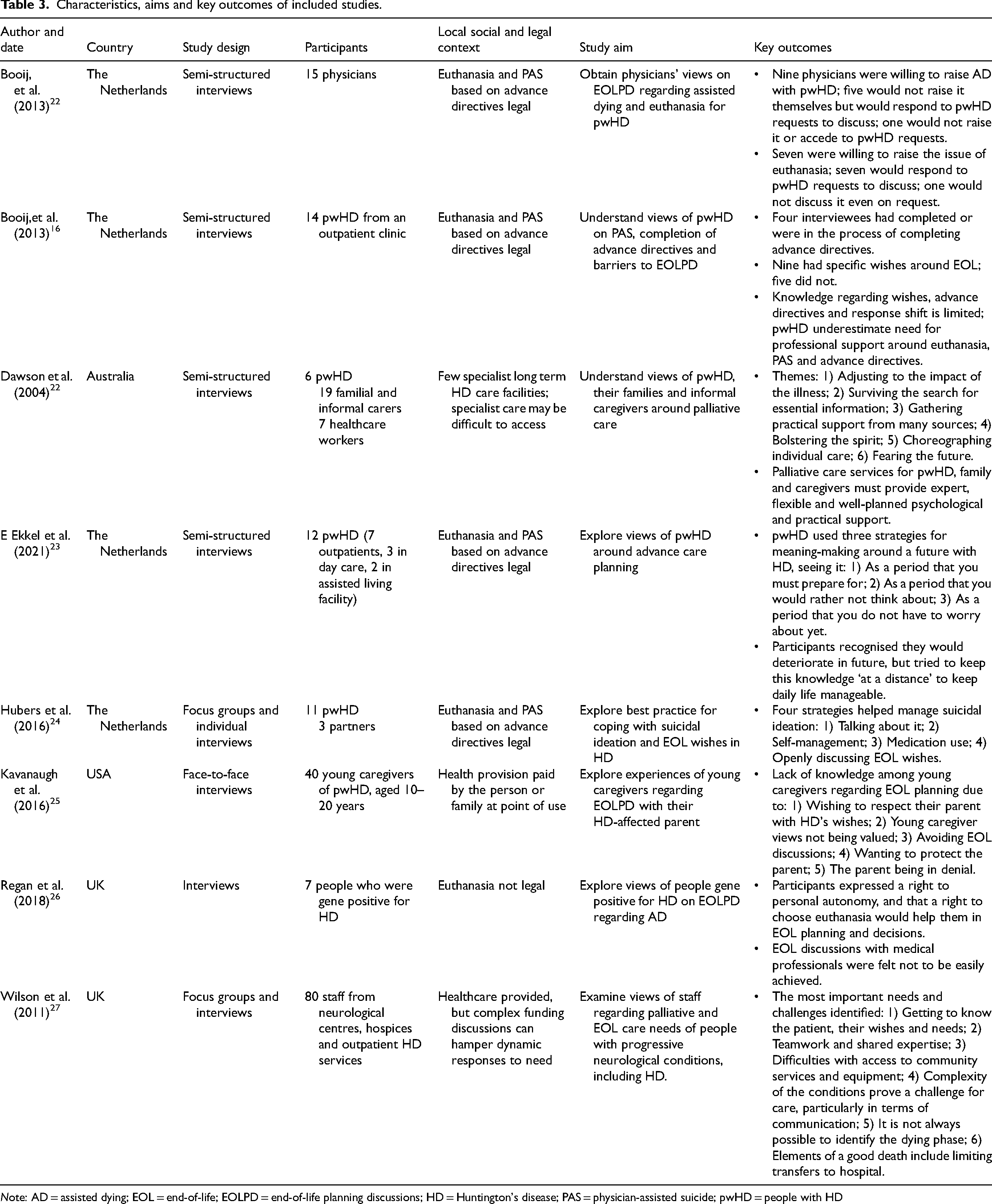
Note: AD = assisted dying; EOL = end-of-life; EOLPD = end-of-life planning discussions; HD = Huntington's disease; PAS = physician-assisted suicide; pwHD = people with HD
Results
Study characteristics
The eight identified qualitative studies included samples comprising people with HD (n = 3), young HD caregivers (n = 1), a mixed sample of people with HD, their relatives and informal/familial carers (n = 2), and healthcare professionals (n = 2; one comprising physicians only, the other mixed healthcare professionals). The studies were undertaken in the Netherlands (n = 4), the UK (n = 2), Australia and the USA (n = 1 each respectively), between 2004 and 2021.
All eight studies reported on EOLPD, but with differing foci. These foci included the effectiveness and utility of EOLPD and advance care planning for people with HD (n = 4), examining views on palliative and end-of-life needs (n = 2), supporting people around suicidal ideation and end-of-life wishes (n = 1), and understanding discussions about end-of-life within families (n = 1).
Four themes were developed. “The value of EOLPD” details the perceived effectiveness of EOLPD discussions. “To talk or not to talk” respectively reflects motivations to seek out or avoid EOLPD among people with HD, their relatives and familial caregivers, and healthcare workers. “A clear vision of the future” encapsulates how EOLPD may provide comfort for some, but fear and anxiety for others. The final theme highlights the importance of those engaging in EOLPD identifying and being able to access “the right people at the right time”, in order to develop meaningful conversations and support in this sensitive area of HD care.
Theme 1: The value of end-of-life planning discussions
In seven studies, participants described the value of EOLPD and its impacts for their lives and wellbeing. For individuals who wished for organised preparedness, EOLPD and the processes that followed them appeared to offer reassurances that plans were in place. One person with HD described the structured approach they experienced to putting an advance directive in place: “Yes, we are pro-euthanasia. I am preparing, together with my wife. The lawyer came and asked about an advance directive. And then we’ve gone back to our GP and we have the NVVE papers [papers from the Dutch Right to Die Society]”.16, p.328
For other people with HD, EOLPD was described as a source of emotional strength during challenging times. It could be helpful in managing intense distress and thoughts of ending one's life by other means: I kind of made my own crisis plan: what to do if I think I want to jump in front of a train. Because… I don’t want to end up that way. So, I made arrangements about this [euthanasia directive] and that helps.24, p.192 Our situation at home has been a lot better since he has been involved with the support group because the guys get together […] and talk about all their problems. They give each other support and so he's not so angry anymore because he can talk about it with his mates, and therefore the situation at home is calmer.22, p.127
Only one study provides physicians’ reflections on EOLPD.
21
This study, conducted in the Netherlands, explored discussions around euthanasia or physician-assisted suicide. Booij and colleagues state that “euthanasia law in the Netherlands is based (morally) on the principle of beneficence and (in terms of criminal law) the necessity of defence”.21, p.624 Physicians described the value of alleviating their patients’ stress and anxiety, with EOLPD perceived as creating a more tolerable view of the future for some. In some cases, just having these conversations was seen as reducing the likelihood of people choosing to pursue a deliberate death: A more peaceful state of mind can be achieved when a patient talks about euthanasia. Peace in the knowledge that they will get help when needed. If counselling and support are provided in most cases you will not reach the point of really considering euthanasia.21, p.622 If subjects are not talked about, they become bigger. So I believe that if you discuss it regularly it can prevent euthanasia, or to put it differently, it can have the result that patients decide they no longer want euthanasia; it is no longer necessary.21, p.622 Whenever they get a new resident […] they try and go through with that person's loved one if they can’t go through it with the person themselves. But I just think it makes things easier for that person if they’ve thought about those things beforehand. And about the sorts of choices that they normally make. Even if it's down to clothing and the music they listen to. Because how frustrating to be stuck in a room full of people playing bingo or watching (television) if they are the sorts of things that you absolutely loathe.27, p.379 I started thinking about euthanasia about 10 years ago. I saw another patient with HD who didn‘t know anything and I thought that is not what I want. And I filled in an advance euthanasia directive. And now I am further down than I, eh, I said I did not want to move to a nursing home, but now here I am, I moved here a month and a half ago. Things were not going well at home. Then we talked about it, saying if it is like this, end it. And then things change, my wishes changed. And we got a granddaughter. So now I am in a nursing home.16, p.326 It might be, for example, it is not worth it for me directly but for whatever reason I still keep my wife company. And you might drag it out another year or something … I guess it wouldn’t be just about me, but at the same time it is not about many people other than me.26, p.712 I just don’t wish to go through that process of decline. I don’t wish it for my mother, but I appreciate that other people are taking those decisions… I think my dad would feel very guilty if there were to be any intervention to end my mum's life sooner than it naturally would.26, p.712
There was also uncertainty regarding whether a plan, once laid out, would even be followed. Hubers and colleagues described a family member's frustration when doctors failed to follow requests, stating: “you have no guarantee”.24, p.192 Healthcare professionals providing end-of-life support also referenced challenges even when end-of-life documents had been successfully put in place, highlighting a lack of confidence that plans would always be followed: 1 guess the difficulty is the out of hours service, isn’t it, I think our own GP would recognise the (statement of wishes), but you get on-call doctors coming in, they don’t know the client, they tend to err on the cautious side.27, p.380
While people with HD, their family members and healthcare workers identified a range of benefits of EOLPD around care and wellbeing, there were concerns around the accuracy and representativeness of documentation, and the consistency of implementation.
Theme 2: To talk or not to talk
Six studies provided statements from individuals, families and healthcare professionals who spoke positively regarding engagement in EOLPD. One person with HD stated: “I had a conversation once with the NHP [nursing home physician] about the future… I am glad you came. Because now I have told you what my wishes are”.16, p.328 Some reported being content to simply go through the motions, accepting when the conversation was raised by their doctor and following the process with support: “Yes, I talked about it with my GP and he gave me a leaflet about euthanasia. Then I handed in the advance directive”.16, p.328
Some individuals with HD reported keenness to engage in EOLPD, while also expressing concerns around being adequately understood by their physician and having sufficient time available. Such inadequacies could cause disappointment and stress at times: “Well, it's like you’re a sort of onion – and all the layers need to be peeled off […] bit by bit actually – and that's what you can’t do if you’re only once with the doctor”.24, p.190 Another described these conversations offering some relief for their anticipatory anxiety: Someone who thinks about death already has difficulty expressing this… and has feelings of self-disapproval because of this thought […] But my experience is that it really helps when you eventually do talk about everything – with all your sorrows and misery. This always gives relief.24, p.189
Healthcare professionals expressed a wish to support individuals at the end-of-life, describing confidence around initiating and holding EOLPD. Some expressed frustration that these discussions are sometimes left too late, and therefore vital information may not be shared: People more and more are wanting to talk about [end-of-life] and are wanting to ask about it even quite early on in their condition. And it's things that we would perhaps mention at certain appropriate times, if people wanted to talk about it then they are able to… I think it's down to us as clinicians to try and gauge it right. And people will pretty soon tell you if they don’t want to discuss it.27, p.382 But it's difficult as well to build any sort of rapport with the patient… if they’re not referred until late, then they are so far, they’re so near death, that you might not be able to build up any sort of rapport with the patient, and certainly not with the relatives, or the friends or the carers… it leaves you feeling as if you’ve somehow missed out on something, as if you could have done it better.27, p.380 When I get to that point, I may be happy, you don’t know that. […] Look, because I know my brother [who also had HD] […] he was very happy. Now imagine that that is the case, well you forget things here and there […] well okay, so maybe you are living your own life.23, p.5
For others, HD was (understandably) perceived as unpredictable, provoking fear and anxiety. People with HD described an avoidance response feeling more comfortable: About the future, well, I just take it one day at a time now. […] Because in the back of my mind I know, it can manifest itself any day and then progress. Like an express train. I know that. […] No, I don’t want to think about it at all. [ …] And I don’t want to talk about it either. I don’t read about it […] [Case manager] also brings me all these booklets and leaflets […] but look, I know what it's like from experience. Second of all, I don’t have to read it because then I’ll immediately feel bad about it again.23, p.5 I don’t know how to describe it. [Talking about death] kinda made me really upset because, yeah, everybody's gonna die, but [realising or thinking] like my [parent] is gonna die, like, more than likely way before the average person.25, p.357 I never ask about this myself. Because I feel that a patient should start the conversation. I thought about this for a long time, but I feel that if a patient is afraid to talk about the subject of euthanasia, then the patient is not ready for it.21, p.622
Theme 3: A clear vision of the future
Six studies describe the advantages and disadvantages of having clear expectations of the future to guide advance planning. Many individuals with HD held a vision of a future they wished to avoid, often relating to personal experiences of HD in their family and/or anticipated future quality of life. People with HD expressed fears of replicating their relatives’ experiences and perceived suffering: “Not the way my mother suffered”.16, p.326 Also central to their fears of the future were expected losses of pleasures and freedoms: I am always creative and working with my hands. Suppose that at some point I can’t do that anymore, that could also be a consideration for me […] to say I’m done. […] Look, if, for example, my mind is still clear, you know, and I can still use my hands, but I would, for example, be fed through a feeding tube, then that wouldn’t be a big problem at all. […] Look, even if it meant I wouldn’t be able to talk very well, but I could use a computer or something, well, fine. Look, I’d still be able to communicate. But if I can’t do that anymore, so not be able to convey to others what I want, what I mean and not be able to express myself, I would really hate that.23, p.4 I am not going to leave home. I have seen that with my mother. As soon as I become dependent on others, then it is time to pull the plug. When I am not able to eat independently or be independent, that is unacceptable. If my quality of life diminishes to a point that I become dependent, then I quit.16, p.326
Contrastingly, physicians acknowledged the usefulness of prior experience, viewing them as an aid to EOLPD. “The advantage of this disease is that patients do have some idea about what their future will be like. Many of them think about the end of life”.21, p.622 In the single study detailing views of mixed healthcare professionals, participants described the importance of accurate awareness of the person with HD's situation and future; this was seen to inform practicalities regarding comfort and achieving “the good death”,27, p.382: “I think it's making life as comfortable as possible… give them the quality as best to our ability… be there to support them, family, anything for them in general”.27, p.382 A lot of hospital admissions are a response to maybe what we consider an acute period of sudden illness, a chest infection… and I think it's very difficult for the staff here to maybe recognise that occasionally it's going to be that last admission.27, p.381
Theme 4: The right people at the right time
Participants across all studies described the importance of considering who should hold EOLPD and when. However, participants from all groups (people with HD, family members and healthcare workers) also expressed concerns regarding the accessibility of specialist support with an adequate understanding of HD.
People with HD described a lack of confidence in the HD expertise of their GPs or neurologists, leaving them feeling anxious, uncontained and disillusioned: “My GP, no I never visit him. No, he is nice, but he is of no help”.16, p.328 I have the same GP as my mother had, so he knows about what should be done. But otherwise, I have no relationship with my GP. If I have any questions I visit the professor. And my GP, he doesn’t really know about the disease.16, p.328
Family members also described the importance of seeking conversations and guidance from those with specific knowledge of HD, which appeared paramount in promoting their confidence in end-of-life care: The nursing home has got to be one that's had experience with Huntington's disease, which there aren’t a great deal. […] There's all those things like the PEG feeding and those kind of issues that come up with Huntington's, they’ve got to know about it. We don’t want to just put him anywhere and find he's not getting the care he needs.22, p.128 We actually get more information out of the support group because there are people in different stages of Huntington's. That's more useful for us and it's actually since he's been involved with the support group, he's much happier because he can see other people in his situation and you don’t have to be depressed about it.22, p.127
Healthcare professionals reported struggling to access specialist support that may be required at end-of-life for people with HD, causing stress and frustration: I think one of the most frustrating things is trying to access specialists, certainly in terms of challenging behaviour, trying to get a psychologist on board is near impossible. It gets very political as well, do they have a mental health problem? […] At the end of the day, we just want to help somebody, so I find that frustrating.27, p.380 Somebody said to me, oh this patient, isn’t it a shame, she can’t talk, and I thought, oh she can’t talk, but I communicated with her so well, I’d forgotten, literally forgotten that she couldn’t talk, because she just grunts at me, and I know exactly what she says.
27
, pp.379-380
Discussion
This review provides an up-to-date narrative synthesis of evidence regarding EOLPD among people with HD, their relatives and familial caregivers, and their healthcare professionals. Four main themes were developed. The first describes “The value of EOLPD”, detailing differing views on the effectiveness of EOLPD for supporting people affected by HD. The second theme, “To talk or not to talk”, reflects counteracting reasons to seek out or avoid EOLPD. The third theme describes how “A clear vision of the future” can provide comfort for some around end-of-life, but fear and anxiety for others. Finally, those engaging in EOLPD require “The right people at the right time”, which was identified as crucial in theory but a challenge to enact in practice.
In “The value of EOLPD”, people with HD described finding planning for the future reassuring and a source of emotional strength (some of which was also reflected in the views of healthcare professionals around these discussions), and family members felt that these discussions could provide solidarity with their relative with HD. Healthcare professionals described the value they placed on opportunities to provide a person-centred end-of-life. Klager and colleagues’ description of advance directives as “the primary way to assure autonomy”,9 p.78 chimes with this idea that advance planning gives back a sense of control, indicating that best practice for HD care should involve early discussions about end-of-life. 8 This is particularly important given the unpredictability of death among people with HD.9,12,14
However, alternative perspectives demonstrated fears around EOLPD. Booij and colleagues 16 discussed response shift, the idea that people with HD may initially wish to end their life but may adapt to HD over time, potentially invalidating a pre-established advance directive. Some people with HD questioned who EOLPD were really for, or how well their views would be represented if conflicting with those of loved ones.24,26 Wider research into delivery of the ReSPECT form, for example, demonstrates that it appears to be considered “more a clinical process around end-of-life care than a person-centred plan for future deterioration”; research into engagement with related documentation in other international contexts would also be valuable to understand these potential barriers further. 30
Even when advance care plans are in place, participants feared that their wishes would not be carried out. 24 The wider evidence base substantiates these concerns, to an extent. There is a lack of clarity around advance care plans, advance directives and end-of-life planning in the literature. 31 The commonest place of death in HD is in hospital, inevitably with unfamiliar staff, 13 and research has argued that clinical realities of advance care plan implementation in the hospital context differ substantially from hypothetical scenarios planned for in advance. 32 Degenholtz and colleagues 33 likewise argue that a living will may not be guaranteed to outweigh established hospital processes. While living wills seemingly provide comfort to many in HD families (with and without the gene expansion) based on our findings, the concerns described by some unfortunately appear warranted.
There were conflicting narratives around seeking or not seeking EOLPD (“To talk or not to talk”). Some people with HD were keen to discuss end-of-life with healthcare professionals early, and the process could bring peace of mind and reduced anxiety regarding an uncertain future. 21 Relatives wished to have EOLPD with their loved one with HD, to learn how to best provide support. 25 This positivity regarding EOLPD from some participants chimes with Farag and colleagues’ 8 recommendation that such discussion opportunities are appreciated by patients, and with findings that they are not associated with negative impacts on mental wellbeing. 34
Others with HD were reluctant to engage in EOLPD, either because they were choosing to focus on hopes for the future (whether around the development of their personal HD trajectory, or for therapeutic developments such as new disease-modifying treatments), or pursuing an avoidance strategy to avoid intolerable distress or anxiety.21,23 This concurs with findings that ruminating on death may have negative impacts for mental wellbeing among people with HD, 35 and that having witnessed other family members progress and die with HD can create negative associations and expectations which impact end-of-life planning. 36 Family members likewise hesitated to raise EOLPD without initiation from their relative with HD, either fearing to distress their relative, or preferring to avoid the subject themselves. 25 These findings concur with previous work showing relatives’ avoidance of holding these discussions with people with HD. 34 It is also likely, though as yet unresearched to our knowledge, that HD family members experiencing ‘caregiver burden’, burnout and compassion fatigue may particularly struggle to engage in these difficult conversations, and this is an important topic for future study.
Healthcare professionals described taking a range of approaches. While some were confident in raising EOLPD and felt that people with HD would be able to reject unwanted discussions, 27 others would only begin EOLPD if the patient initiated them, 21 concurring with past findings that clinicians may fear causing distress. 35 The narrative in Wilson and colleagues 27 regarding these discussions being neglected until it is too late appears highly significant in light of (at least some) clinicians being unwilling to raise the conversation, especially when contrasted with Hubers and colleagues’ 24 findings regarding people with HD wanting to talk about end-of-life, but feeling their clinicians lacked the required time and expertise. The result may be a stand-off in which people with HD are willing to undertake EOLPD but feel unable due to practical barriers, while clinicians are unwilling to begin discussions without a direct prompt which may not be forthcoming.
“A clear vision of the future” described tensions between people with HD and their relatives fearing future losses, suffering and reduced quality of life,16,22,23 versus healthcare professionals’ views that past experiences, current situational awareness and future fears provide an aid and impetus to EOLPD.21,27 Regarding future planning, Wilson and colleagues 27 highlight the crucial nature of understanding what constitutes a ‘good death’ for someone with HD and leveraging good planning and familiar staff to enact it, while Klager and colleagues 9 reference the importance of planning ahead with structured advance care planning documentation, including around key decision points such as tube feeding. However, visions of end-of-life were often amorphous, lacking the specifics that healthcare professionals require to provide the desired ‘good death’, and the literature remains impoverished regarding what this actually means for HD individuals and families. What a ‘good death’ actually means will almost certainly vary cross-culturally too, and much more research is needed in this area to understand the needs of the international HD community in this regard.
Finally, “The right people at the right time” highlighted the importance of considering who should hold EOLPD and when. Across people with HD, family members and healthcare professionals, concerns were expressed around access to appropriately specialist support. People with HD expressed a lack of confidence in the professionals available to them, the time (un)available for these important conversations, and a perceived lack of understanding of HD, chiming with findings that individuals with HD prefer not to discuss end-of-life concerns with their physicians, 36 which can lead to missed opportunities.17,26 Families found relief in support groups and shared experiences but expressed longing for informed, expert support, concurring with findings that rapport with an expert in HD is crucial to successful EOLPD. 8
Healthcare professionals themselves cite struggling to access specialist support, referring to perceived gatekeeping from other services which hindered their ability to provide EOLPD and care for this specialist population. Past research has advocated for better education for healthcare professionals around the unique challenges that HD presents,9,12 recognising that general physicians may lack knowledge around key issues such as anosognosia and the secrecy within HD families which can present barriers to timely, supportive discussions. Overall, this final theme highlighted significant absences despite good intentions, with people affected by HD unsure where to gain knowledgeable, HD-expert advice around EOLPD.
Strengths and limitations
A robust search strategy underpinned this review, guided by a subject librarian. The research team hold significant diverse healthcare experience in supporting people affected by HD and other life-limiting conditions and consequently were well-placed to undertake this work. Papers were identified inclusively with no date limitations applied, ensuring a thorough representation of the evidence base. Detailed quality evaluation was undertaken to identify issues with robustness, and outcomes of this process were considered within the synthesis. Established narrative synthesis guidelines were followed throughout.
In terms of limitations, inclusion of grey literature may have offered additional insights – this was not done in order to focus on robust, peer-reviewed evidence. Regarding the evidence base itself, the included papers did not clearly report their epistemological positioning which limits understanding of the authors’ experiences and meaning-making of their findings; this should be consistently reported in the literature going forward. The high homogeneity of samples across the papers also presented limitations; all the studies were conducted in the global north, thereby excluding narratives from other cultures and contexts, with these remaining a key gap to be addressed in the literature.
Finally, and importantly, the lack of a clear definition of end-of-life in HD across the literature – as referenced in the introduction – has two implications. First, it limits the drawing of clear conclusions regarding particular points in the HD trajectory, given the variety of stages of HD represented in the reviewed literature. Second, it presents a clear priority for next steps in research, given the lengthy period between diagnosis of HD, the gradual loss of capacity and cognition, and the unclarity around markers of end-of-life deterioration, which make HD distinct from many other conditions.
Clinical implications
EOLPD should be context- and person-specific, part of a developing conversation over time rather than a one-off discussion, and engaging the individual alongside input from family where appropriate.9,12,31 This may be particularly important for those with late-onset HD, who are more likely to experience comorbid age-associated conditions in parallel with symptoms of HD. The timing of EOLPD for people with HD should also take into account HD-specific considerations around deteriorating capacity to participate in these discussions. 8
Based on our findings, healthcare professionals should be conscious that some people with HD and family members may be keen to begin EOLPD but may need an invitation to do so (while remaining mindful of their required professional and legal boundaries in their region of practice). Given that some people affected by HD may be strongly avoidant of such conversations, invitations to initiate them should be offered sensitively, with explicit acknowledgement that EOLPD will be pursued only at a time that feels right for the individual and/or family. While stigma was not expressly raised in the identified papers as an impacting factor for EOLPD, wider literature does also suggest that experiences of stigmatising attitudes in HD can impact willingness to seek support, so this is an additional factor for consideration and healthcare professionals should work to build positive rapport and minimise any felt stigma for families.18,19
The hesitation expressed by some physicians also points to a potential need to support healthcare professionals around such conversations, respecting that their own personal beliefs and preferences may influence their choices as practitioners. At times, patients may require referral on for EOLPD in their best interests if the healthcare professional feels unable to provide this. 21
It is important to note that some known issues around HD end-of-life management were not represented in our findings, which most likely reflects our focus on communication around planning ahead, rather than on the pressures and challenges of managing wellbeing and difficulties in the moment. It may also reflect that future planning is generally inadequately undertaken in relation to these known issues, per our findings. While clinical issues such as changes in movement disorder towards akinetic-rigid states, and the aspiration risk associated with severe dysphagia, are largely not referenced in our findings, they remain a crucial component in HD end-of-life management.
Future research
The current literature around EOLPD for people with HD is highly limited, and we recommend numerous routes for further research. Key areas indicated by this review include directly exploring experiences of families of people with HD who have died or are receiving end-of-life care. Examining the strengths and current weaknesses of multidisciplinary input for EOLPD will also be important, in terms of provision of specialist support for family members (e.g., information around PEG feeding), and guidance to healthcare professionals (e.g., around psychological support), which was felt to be inaccessible but crucial.
Multiple populations are underrepresented in the current literature. For example, only one paper explored experiences of young caregivers around EOLPD, yet this paper highlighted clear need for further examination of this vulnerable population. Experiences of healthcare professionals in providing end-of-life care and EOLPD are also significantly under-researched, with only two papers in total. Finally, the evidence base being entirely situated in the global north fails to represent the majority of the world with regards to HD, and consequently research to address this deficit appears strongly indicated.
Conclusion
In this synthesis of evidence relating to experiences of EOLPD among people with HD, their family members and the healthcare professionals who support them, four themes were developed which can best be summarised by polarisation. Individuals express positive and negative views around the value of EOLPD, being willing or not willing to engage in such conversations, finding comfort or fear in a vision of the future, and desiring help but being unable to obtain it. These numerous dichotomies create a lack of cohesion in the intent and usefulness of EOLPD, highlighting significant gaps in delivery from the perspectives of each population, but also demonstrating the great value of these discussions when they are successful.
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable contributions of the HD community to the research which underpins this synthesis, as well as the crucial support of the Huntington's Disease Association's consultation group ‘HD Voice’, who kindly contributed to discussions around priorities for HD end-of-life research. For the purpose of open access, the authors have applied a Creative Commons Attribution license (CC BY) to any Author Accepted Manuscript version arising from this submission.
Ethical considerations
Ethical approval was not required for this review as no new data were collected.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions (CRediT)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding (PhD fees) from the Huntington's Disease Association.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All secondary data are already available.