
Abstract
This protocol describes a Campbell evidence and gap map designed to visually map existing evidence on the application of genetic and genomic testing in primary care. Beyond outlining the rationale and motivation, this protocol details the methodological steps and rigorous criteria that will guide its development. These include: 1) conducting a systematic search to identify published literature on the use of genetic and genomic testing in primary care; 2) summarising and visually mapping the available evidence; and 3) identifying gaps in the current evidence base to inform future research priorities and policy directions. The resulting map is expected to provide a rigorous yet accessible tool for researchers, practitioners, and policymakers seeking to assess the current evidence landscape and identify opportunities to integrate genetics and genomics into routine healthcare delivery.
Keywords
Background
The Problem, Condition or Issue
Traditionally, preventive and therapeutic recommendations have been based on the average patient’s expected response rather than tailored to individual variability. Over the past two decades, this one-size-fits-all paradigm has evolved toward an individualised or precision medicine model in certain diseases, incorporating a comprehensive assessment of medical history, molecular-level disease characterisation (e.g., genetic testing), and close monitoring of biological parameters using diverse tools (e.g., sensors, wearables). While rapid advances in biomedical and technological innovation will continue to reshape precision medicine, its core multidimensional definition – the integration of inherited and acquired traits, lifestyle factors, and environmental influences to personalise reproductive choices as well as disease prediction, prevention and healthcare – is expected to remain unchanged (National Research Council, 2011).
Key Terms and Definitions
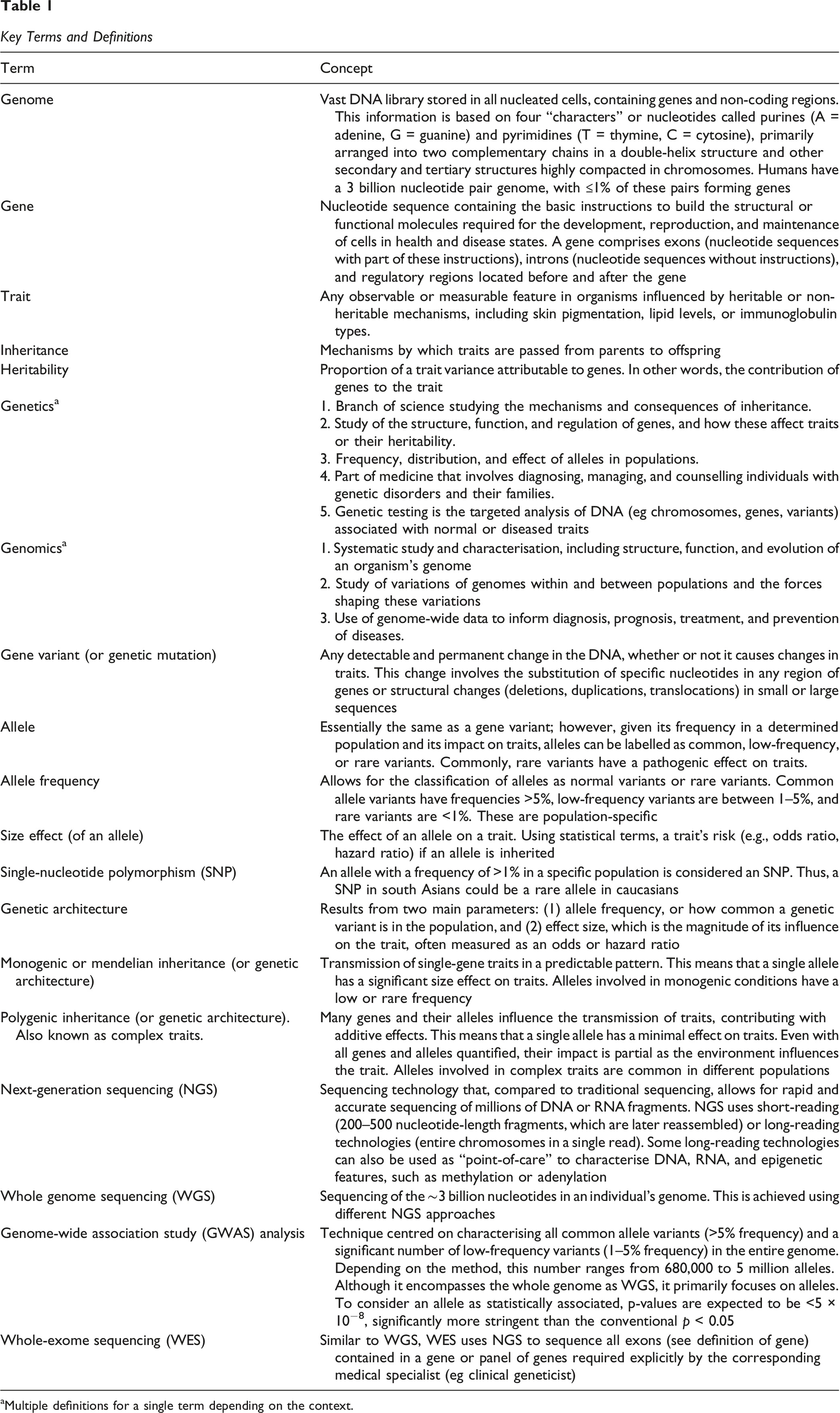
aMultiple definitions for a single term depending on the context.
Currently, decision-making in primary care relies on practitioner expertise, clinical guidelines and expert recommendations, all representing varying levels of evidence. Prediction tools, such as the Framingham score (risk of cardiovascular disease) or the CURB-65 score (need for hospitalisation in patients with pneumonia), aid clinical decisions and have strongly influenced clinical practice. Unfortunately, many conditions in primary care lack similar resources, and existing recommendations are frequently revised as new evidence emerges. In this context, genomic testing offers the possibility of generating a once-in-a-lifetime dataset, now costing under US$1000 and falling, that can inform disease risk prediction and support clinical decision-making across the life course. Integrating genomic data into primary care can enhance the management of prevalent diseases by identifying an individual’s predisposition to diseases, developing personalised primary and secondary prevention strategies, or individualising treatments to optimise efficacy and minimise adverse effects. The shift from a one-size-fits-all model to individualised approaches with population-level reach recommendations will mark a critical step toward further refining the model of primary care that aspires to be predictive, personalised, preventive, and participatory (Hood & Flores, 2012). However, the integration of genomics in primary care requires robust evidence supporting its clinical utility, understanding its multiple requirements (e.g., enough genomic facilities, specialised workforce, literacy of primary care providers, etc.), a well-defined legal framework to guide its appropriate use, and cost-effectiveness evaluations that demonstrate its benefit compared to the standard of care. In Australia, for instance, such assessments inform the Minister for Health’s decisions regarding the inclusion of medical services, procedures, and technologies in the Medicare Benefits Schedule (MBS). Addressing these supporting components across the health system and the current gaps within them is essential to unlocking the full potential of genomics-driven primary care.
The Intervention
Different approaches are used to identify research gaps and guide health and social policies. Compared with similar approaches, an Evidence and Gap Map (EGM) is a visual tool that categorises existing evidence as abundant, limited, or lacking, clearly highlighting areas of established knowledge alongside those that remain underexplored or unaddressed. The EGM methodology also plays an essential role in preventing unjustified duplication of research. It can help pinpoint areas where high-quality evidence from systematic reviews (SRs), meta-analyses (MAs), and randomised trials already exists to support decision-making. Additionally, the method helps highlight topics with sufficient primary studies, directing targeted SR/MA (Snilstveit et al., 2016). EGMs systematically map the evidence landscape, providing a clear and actionable overview for policymakers, researchers, and practitioners.
Given the increasing interest in integrating precision medicine into clinical practice, numerous narrative and scoping reviews have explored the diverse roles of genomics across multiple levels of care. Yet, a rapid assessment reveals that these reviews primarily focus on genetic testing rather than genomics, a critical limitation given their technical and regulatory differences, scopes, and target populations (Abdelhalim et al., 2022; MacEachern & Forkert, 2020). Additionally, most reviews take a broad approach, covering multiple components of precision medicine (e.g., other Omics, artificial intelligence, big data) rather than explicitly addressing genomics (Evans et al., 2024; Madhavan et al., 2018). None of these existing reviews has applied a standardised framework for systematically prioritising or mapping interventions—an essential aspect of planning EGM (Campbell et al., 2023). To address this, an EGM is needed to consolidate existing evidence on genetic and genomic testing in primary care and other care settings that may be relevant or applicable in primary care. This EGM will specifically focus on genetic and genomic testing interventions to improve the care of prevalent conditions in primary care. Doing so will identify key healthcare needs that these approaches can address and provide a structured justification for their implementation.
Why Is It Important to Develop This EGM?
This EGM aims to systematically identify and map existing evidence on the impact of genetic and genomic testing in primary care. Current evidence in primary care—or research potentially transferable to it—appears to be fragmented, low-quality, and inconsistent in terminology, spanning diverse settings with inconclusive effectiveness (Biswas et al., 2020; David et al., 2023; Edsjö et al., 2023; Haverfield et al., 2021; Schwartz et al., 2018; Walton et al., 2022; Wildin, 2024; Wildin et al., 2022a, 2022b). With rapid advancements in this field, an EGM will highlight areas with robust evidence and expose critical gaps, guiding researchers, decision-makers, and policymakers in prioritising future studies and interventions. Additionally, it will enhance evidence discoverability, supporting informed decision-making for healthcare providers, policymakers, patients, caregivers, and the public.
The knowledge generated by this EGM will offer several key benefits: - Differentiating genetic and genomic testing by outlining their benefits, technical and regulatory requirements, and associated challenges. - Prioritising interventions with sufficient studies to support systematic reviews and meta-analyses, strengthening the evidence base. - Assisting clinicians in recognising effective interventions and key characteristics of potentially practical approaches, with the necessary aids to select further and design locally applicable strategies. - Supporting policymakers and funders to accelerate the integration of PM into primary care, whether by prioritising the implementation or upscaling of effective interventions or funding research to address knowledge gaps. - Enabling research organisations to assess the reliability and quality of existing evidence, guiding the development of future research priorities in genetic and genomic testing for primary care.
Objectives
We intend to identify and synthesise existing evidence on the use of genetic and genomic testing across various levels of clinical care, focusing on its potential translation into primary care. Specifically, we seek to: - To systematically search and identify published literature on the use of genetic and genomic testing in healthcare. - To summarise and map available evidence on genetic and genomic testing in healthcare. - To identify gaps in existing evidence to inform future research and policy priorities.
Methods
Evidence and Gap Map: Definition and Purpose
EGMs are systematic evidence synthesis tools that visually present existing research relevant to a specific question (Campbell et al., 2023; Snilstveit et al., 2016). They highlight areas where evidence is available, identify gaps, and assess the quality of existing research. Typically, an EGM is structured as a two-dimensional matrix, with interventions listed as row headings and outcomes as column headings (Figure 1). Example of an EGM for Health Systems Research in Burn Care (Keshri et al., 2023)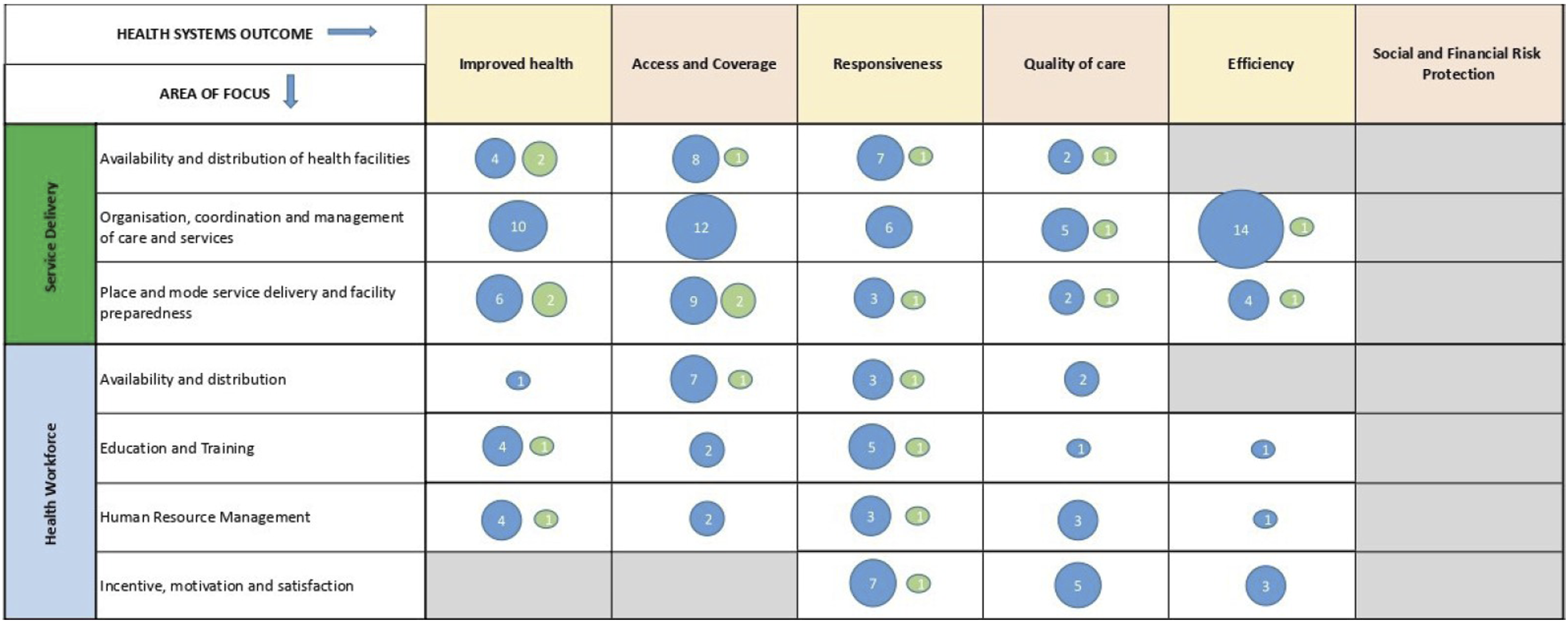
Each cell in the matrix represents studies that provide evidence for the corresponding intervention and health outcome, highlighting available research and gaps in genetic and/or genomic testing for improving healthcare across all age groups. Two EGMs are expected, one for genetic and one for genomic testing, although it will depend on the availability of evidence.
Framework Development and Scope
The conceptual framework for this EGM is grounded in the World Health Organisation (WHO) Health Systems Framework (Figure 2), which provides a shared understanding of health systems and strategies for strengthening them (WHO, 2007). This framework defines a health system through six core building blocks: service delivery, health workforce, information, technology, financing, and leadership and governance. Additionally, it incorporates key process elements (access, coverage, quality, and safety) and health system outcomes (improved health and health equity, responsiveness, social and financial risk protection, quality of care, and enhanced efficiency). To tailor this framework for genetics/genomics in clinical practice, we further categorise each building block into subdomains, drawing on significant themes from the health systems literature and insights from stakeholder consultations (Section Types of intervention/problem). Standardised operational definitions are developed for all key focus areas and health system outcome measures (Section Types of outcome measures). WHO Health Systems Building Blocks Framework (WHO, 2007)
Stakeholder Engagement
An advisory board of key stakeholders was established to help define relevant subdomains for each building block and interpret the findings. This includes academics, advocates, and policy and decision-makers from relevant Australian organisations (e.g., NSW Health, UNSW Academic General Practice Network, Ramaciotti Centre for Genomics) who are involved in primary care and the conduct of genetic/genomic testing in clinical and research contexts.
Types of Study Design
This EGM will include only completed and ongoing systematic reviews, overviews of systematic reviews, and primary studies targeting effectiveness. If multiple interventions are reported in the same publication, each intervention will be represented separately on the map. If there are various reports of a single study, these reports should be considered as a single study. Both systematic reviews with and without meta-analyses will be included. Systematic reviews and overviews will be eligible for inclusion if they are based on the population, intervention, comparison, outcome (PICO) framework and meet at least four of the five criteria expected in a systematic review (Moher et al., 2015): 1. A description of adequate search methods used to identify studies. 2. Eligibility criteria for study selection. 3. Methods for critically appraising included studies. 4. Sufficient details on the characteristics of included studies 5. Synthesis or analysis of the study findings of the included studies.
We will include experimental and quasi-experimental studies that assess the effects of interventions using randomised or non-randomised methods that allow for causal inference. Specifically, we will include study designs aligned with the Cochrane Effective Practice and Organisation of Care (EPOC) inclusion criteria (Cochrane Effective Practice and Organisation of Care, 2017): - Experimental study designs: Studies where participants were randomly assigned to either an investigational or standard-of-care intervention. - Quasi-experimental study designs: Studies in which assignment to an investigational or standard of care is determined by known allocation rules, including a threshold on a continuous variable (e.g., assignment based on age cut-offs) or geographical or econometric variation in the allocation (e.g., intervention decided by passage of law or budget constraints). Cohort studies can be included if they fulfil the above criteria. As per EPOC recommendations, we will accept studies with at least two intervention sites and two control sites. - Controlled before-and-after studies: A study in which observations are made before and after the implementation of an intervention, both in a group that receives the intervention and in a control group that does not. Allocation is influenced by other factors beyond the investigators’ control. - Interrupted time series studies: These studies collect observations at multiple time points before and after an intervention to determine whether it has a more significant effect than any underlying trend over time. To meet the EPOC inclusion criteria, the study must include at least three data points before the intervention and three after, with repeated measures in the same individuals at each time point.
Narrative and scoping reviews, non-controlled pre-post evaluations, case studies, cross-sectional studies, modelling-based studies, opinion pieces, and editorials will be excluded.
Types of Intervention/Problem
Intervention Matrix According to the WHO Health Systems Framework

Types of Outcome Measures
Outcome Matrix According to the WHO Health Systems Framework

Types of Population
This EGM will map the full range of genetic and genomic interventions and health outcomes for primary care users of all ages in the general population. It will focus on evidence on interventions that enhance clinical care among healthcare providers and improve organisational standards in agencies providing healthcare to the general population at the primary level. Using a public health approach, genomic interventions can be categorised based on their target population (Springer & Phillips, 2007): - Universal: applicable to everyone, regardless of risk. - Selective: targeting diverse high-risk subpopulations (e.g., individuals with a family history of genetic disorders). - Indicated: focusing on individuals who require genetic or genomic testing.
This categorisation provides a clearer understanding of prioritisation strategies and facilitates efficient resource allocation. While the target population is broad, this EGM excludes individuals in palliative care or end-of-life support. If a study includes data on both the general public and these excluded groups, only studies that present separate data for the public will be included. Search terms restricting the study population are detailed in the appendix document, as concept 2: primary care.
Search Methods and Sources
A pilot search strategy would be conducted under the guidance of senior author experts in EGM (KRK, AM). To ensure that this EGM is relevant and valuable to key stakeholders, the literature retrieval methods and report will adhere to high-quality standards, following published guidelines (White et al., 2020). The search will not have language restrictions, although it will be limited to research published from January 1, 2000, onwards (10 years before the initiation of the Human Genome Project). Databases include PubMed, Embase, Cochrane Library, CINAHL via EBSCO, Web of Science, Scopus via Elsevier, and OpenAlex.
A search for grey literature will also be conducted: - Some grey literature sources are captured in the Web of Science search, including Conference Proceedings Citation Index- Science (CPCI-S)—1990-present. - PROSPERO. - Open Science Framework (OSF).
Any ongoing study will be rechecked before the project’s completion. If it is still unpublished one month before submission, it will be added to a reference section titled ‘ongoing reviews’ and excluded from the EGM. Search terms are available as a separate appendix document. Relevant individuals and organisations will be contacted directly for information about unpublished or ongoing studies if no complete studies remain unpublished by the project’s completion.
Analysis and Presentation
Report Structure
This EGM may result in two primary outputs: (1) an Evidence and Gap Map focused on genetic testing, and (2) an Evidence and Gap Map focused on genomic testing. Depending on the volume, scope, and overlap of the included literature, these may be published either as two or more distinct EGMs or consolidated into a single map with clearly demarcated domains for genetic and genomic testing.
The final output(s) will include: - An interactive visual map presenting the distribution of evidence across intervention–outcome domains - Summary tables describing the characteristics, quantity, and quality of included studies - A written report providing: an overview of the evidence landscape, a narrative synthesis of key patterns and findings, identification of areas with limited or no evidence (evidence gaps), a discussion of methodological limitations and potential biases in the evidence base and mapping process.
All outputs will adhere to the methodological guidance outlined by the Campbell Collaboration guidelines (White et al., 2020) and will be designed to support evidence-informed decision-making by researchers, policymakers, and practitioners.
Filters for Presentation
Not required for this EGM.
Dependency
Each entry in the EGM will represent a single study, defined as a unique piece of research addressing a specific domain of evidence. Where multiple publications (e.g., abstracts, pre-prints, journal articles) are associated with the same underlying study, they will be treated as a single entry in the map to avoid duplication. However, studies that span multiple intervention or outcome domains or topic areas may be mapped in more than one cell within the EGM matrix. In such cases, the study will be linked to all relevant nodes of the framework, allowing users to identify cross-cutting evidence across domains while maintaining a non-redundant count of included studies.
Data Collection and Analysis
Screening and Study Selection
Searches will be completed by the first author using the corresponding databases (Section Search methods and resources) and adhering to the defined selection criteria (Section Types of study designs). All identified sources and articles will be imported into EndNote, and all duplicates will be removed to avoid duplication effort in the subsequent stages of the EGM. Two independent reviewers will screen all literature for inclusion at both the title/abstract and full-text levels. A third reviewer from the research team will resolve any conflicts that arise. To maintain objectivity, authors involved in primary studies will not participate in the screening and selection process. Literature screening will be conducted using the COVIDENCE platform. Data-mining techniques will be used in the selection process if the volume of identified records is substantially large.
Data Extraction and Management
Two team members will independently review all eligible studies, and a third member will resolve conflicts. If results are unavailable, the first and corresponding authors will be contacted to obtain missing data. If multiple reports exist for the same study (e.g., a conference abstract and a journal publication), all will be assessed to ensure that complete information is provided for the EGM. Similarly, authors involved in primary studies will not participate in this stage.
An Excel file will be used to extract data from all relevant studies. This file will be pretested with a selected sample of included studies/reviews representing the entire range of study designs eligible for this EGM. It will be refined and adjusted as necessary and then used in conjunction with all studies and reviews included. Reviewers will initially extract data from 10 articles, with responses assessed against pre-defined criteria and compared to one another. Inter-reviewer agreement and consistency of comprehension and application will be evaluated, and additional training will be initiated where necessary. Following this, weekly ongoing spot checks will be conducted on a random sample (at least 10%) of studies.
Tools for Assessing the Risk of Bias/Study Quality of Included Reviews
Two reviewers will independently use the AMSTAR 2 tool to determine the quality of systematic reviews (Shea et al., 2017). Any disagreements will be resolved by discussion. Experimental studies will be assessed for quality using the Cochrane Risk of Bias 2 tool (Sterne et al., 2019). Two reviewers will independently assess the risk of bias. A third reviewer will adjudicate discrepancies regarding the risk of bias that cannot be resolved via consensus.
Quasi-experimental and observational studies will be assessed using the Cochrane Risk of Bias Tool for Non-Randomised Studies of Interventions (Sterne et al., 2016), EPOC Risk of Bias Criteria (Cochrane Effective Practice and Organisation of Care, 2017), and the Newcastle-Ottawa Scale (NOS) for Cohort Studies (Wells et al., 2012).
Methods for Mapping
Once data extraction (3.10.2) and quality assessment (3.10.3) are completed, a final list of studies will be generated in COVIDENCE. The EGM will be developed from the final COVIDNCE list using the EPPI-Mapping tool (Thomas et al., 2010). The EGM will be piloted prior to finalisation to ensure clarity, usability, and methodological rigour. Once validated, the final version will be made publicly available online as an interactive, user-friendly tool. The map will provide a comprehensive visual summary of the existing evidence, clearly indicating where research is concentrated, where it is sparse, and where significant gaps in knowledge remain. The EGM will include multiple filter options to allow users to refine their view based on key characteristics such as mean participant age, geographical region, mode of delivery, study type, and the specific type condition/disease. These filters will enhance the utility of the map for diverse users, including researchers, policymakers, and practitioners.
The interactive map will be accompanied by a narrative report that synthesises key findings, highlights areas of evidence concentration and gaps, and outlines implications for future research, practice, and policy development. A plain language summary will also be produced to ensure accessibility for non-specialist audiences and a broader range of stakeholders who may benefit from the findings.
Footnotes
Acknowledgements
The authors have nothing to report.
Author Contributions
• Content: Braulio Mark Valencia, Marc R Wilkins, and Michael Kidd.
• EGM methods: Vikash Ranjan Keshri.
• Statistical analysis: Braulio Mark Valencia, Jialing Lin, Shona Bates, and Limin Mao.
• Information retrieval: Rafal Chomik, Chris Dietz, Peter Brown, and Patricia Mary Davidson.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ian Potter Foundation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Plans for Updating the EGM
This EGM will be updated every 2 years.
Sources of Support
The Ian Potter Foundation funds investigators of the ICFHS.